#Mental health education
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Forty percent of Tumblr users are between the ages of 18 to 25.
Text
Clinical studies be like
1 billion random boys were tested. results show that 0% of girls are autistic* 👍
1 billion autistic males were tested. results show that 0% of autistics are female* 👍
1 billion minors were tested. results show ADHD stops at age 18, often to be replaced by plain laziness* 👍
*certified😎 totally credible source✨ we are pros🤓 with coats🥼
#rants & reflections#clinical studies#healthcare reform#mental health education#autism research#undiagnosed neurodivergent#neurodiversity#late diagnosed adhd#late diagnosed autistic#self diagnosis is valid#autism in girls#autism in women#autistic girl#autistic women#adhd in women#adult adhd#adhd adult#audhd struggles#audhd things#adhd autistic#audhd brain#audhd problems#autistic thoughts#autism diagnosis#adhd diagnosis#educated self diagnosis#pro self diagnosis#self diagnosed autistic#self diagnosed autism#self diagnosed adhd
380 notes
·
View notes
Text
As someone with BPD, I'd just like to try to clear some things up.
People with BPD do/are:
DO have trouble regulating their emotions and their impulses
DO struggle with healthy relationships and attachments to others
DO have an intense fear of abandonment and will do whatever it takes to avoid being abandoned
DO have an unstable sense of self and their identity
DO suffer from chronic self-harming and/or suicidal behaviours
DO experience feelings of emptiness or hollowness
DO have erratic moods and emotions that can change drastically from moment to moment
DO frequently engage in impulsive behaviours
ARE able to feel real love towards other people
ARE able to be treated
ARE able to live happy, well-rounded lives
ARE able to form healthy relationships
DO deserve respect
DO deserve support
DO deserve love
People with BPD do/are not:
DO NOT act the way they do for attention (the self-destructive behaviours people with BPD sometimes engage in stems from a need to cope with our emotions and thoughts, not out of attention-seeking)
ARE NOT intentionally or maliciously manipulative (manipulative behaviour is pre-planned and intentional. People with BPD engage in their behaviours as a reaction to their intense emotions. While we may act in ways that attempt to control how others behave, we are typically doing so to try to ease or prevent our own emotional pain, not to hurt others.)
ARE NOT dangerous or violent (people with BPD are much more likely to hurt themselves than others)
HAVE NOT all experienced childhood trauma (many people with BPD have experienced childhood trauma, but many have not. Childhood trauma is a risk factor, not a cause.)
ARE NOT all AFAB (while a larger percentage of those diagnosed with BPD are assigned female at birth, many of those who are assigned male at birth also suffer from BPD, and some evidence shows that it may be more equally distributed among both sexes)
ARE NOT untreatable (there are lots of treatment options available! DBT is the most common, but there are many other options as well.)
ARE NOT all abusers (abuse is not linked to any one mental illness. People with BPD may struggle to form healthy relationships and this can lead to abusive dynamics, however ANYONE can be abusive regardless of their mental health.)
ARE NOT all the same (BPD is a spectrum and it affects all of us a little bit differently. Not everyone is going to experience it exactly the same as someone else, and it's important to recognize that we're all individuals.)
ARE NOT rare (BPD is actually pretty common. It's estimated that around 1-2% of the population are diagnosed BPD. That's around 156,000,000 people, and that's not even counting those who are undiagnosed.)
ARE NOT horrible, unfeeling monsters (we are literally just people)
ARE NOT unworthy of love (EVERYONE is worthy and deserving of love)
#bpd#actually bpd#borderline personality disorder#mental health#mental health awareness#bpd awareness#mental health education
330 notes
·
View notes
Note
Hello! I just wanted to say that I've been using some of your posts talking about ASPD to help me better understand it to write an OC I'm writing. I have a question though, do you mind talking about more symptoms of ASPD that I should keep in mind when writing her?
Hi! Very glad to hear that my posts have been helpful and its cool that you are aiming for good representation!
When it comes to how ASPD symptoms should be written and which ones should make it into literature, theres different opinions, so this is gonna go a bit beyond your question I guess? Just to get a roundabout view.
1. Recovery Position
• First thing to rly keep in mind is that the intensity of the symptoms, the way they present and the way the character would deal with them, absolutely depends on where they are in recovery.
��� It also depends on what you understand as recovery, be that the reducing of overall symptoms so they are less often present, the act of reducing the harm that is done by your symptoms (ex: trough redirection, or actively learning prosocial behavior) or just learning to find a way to live in society the way you are. No ones view on recovery or the way they go about it (or if they decide not to) is in any way better or superior, but it is an aspect that does change how many symptoms you show in which way, so its important to think about when writing a character.
2. Covert/Overt Symptom Presentation
• Another thing to think about, depending on what fits into your story, is the question as to whether your character is very obviously antisocial, or whether they go about it in a more covert secret way. Can they control which symptoms they show when? Or are they lost to their impulses and emotions? Do they come from a background where hiding their symptoms was essential, or were they able/forced to present obviously?
• Theres also a more mixed presentation where some symptoms are more obvious and others are not, depending on stuff like what meets your needs best, how much control you have and whether or not you've done any active work on the symptoms yet, etc.
• Then you can also think about the personal opinion of your character on symptom presentation. Do they believe that they should get to just be themselves? Are they of the opinion that people just have to deal with their symptoms and accept them that way? Or do they think that they have to hide some symptoms in order to fit into society better? Have they potentially adopted some prosocial ways of thinking and model their presentation after that? Depending on what it is, it will obviously look different.
3. The Causes of their ASPD
• Depending on the type of trauma they went trough that made them develop ASPD, presentation will differ. Its highly individual of course, but theres some themes, like people who come from violent households often being violent themselves, people who were neglected struggling with the social aspects like empathy & remorse, people who were lied to/manipulated/berated all the time adopting similar manners, people who had to commit crimes and/or witnessed those often continuing to do so because its normal to them, etc.
• The other aspect is genetics, where certain tendencies can be given from parent to child or grandparent to grandchild, such as impulsive tendencies, the type of temper someone has, access (or denied access) to certain parts of the brain that are responsible for prosocial emotions, etc. Those genetics mix with the trauma and sometimes push the presentation in certain directions, so its a thing to keep in mind.
• Some CD/ASPD symptoms can also develop/be made worse trough bullying, intense experiences in childhood/teens, hanging around with people who engage in/normalize certain behaviors, etc. (ex: kids with delinquient tendencies who hang around other kids with those, may be more likely to develop that as a continous behavior). So its also worth thinking about who your character was around while they grew up, who influenced them how and what was normalized to them.
4. The Current DSM-V ASPD Criteria
• When it comes to the core symptoms of ASPD, theres 3 out of 7 DSM criteria points your character should meet. It doesn't matter which ones, but it has to be at least three! Your character should also be older than 18, have shown conduct disorder symptoms before they turned 15 and have their ASPD symptoms even in absence of other comorbidities, substances and/or episodes (Criterion B-D which I am not quoting, but thats it summed up)
• The 7 criteria points recognized in the DSM-V are (and I quote):
A. A pervasive pattern of disregard for and violation of rights of others, occuring since age 15 years, as indicated by three (or more) of the following:
1. Failure to conform to social norms with respect to lawful behaviors, as indicated by repeatedly performing acts that are ground for arrest.
2. Deceitfulness, as indicated by repeated lying, use of aliases or conning others for personal profit or pleasure.
3. Impulsivity or failure to plan ahead.
4. Irritability or aggressiveness, as indicated by repeated physical fights or assaults.
5. Reckless disregard for safety of self or others.
6. Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations.
7. Lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated or stolen from another.
• Everything after "as indicated by" is an example of a possible presentation. The DSM-V acknowledges that there are other possible ways in which symptoms can show up.
5. The Alternative ASPD Model in the DSM-V
• This is not used to officially diagnose people with ASPD, but is one idea, as to how personality disorder classification could work in the future. It looks at the symptoms as dimensions, under which possible experiences could fall and mentions quite a few things the current criteria doesn't, so I'll quote it below as well:
A. Moderate or greater impairment in personality functioning, manifested by characteristic difficulties in two or more of the following areas:
1. Identity: Egocentrism, self esteem derived from personal gain, power or pleasure.
2. Self direction: Goal setting based on personal gratification, absence of prosocial internal standards, associated with failure to conform to lawful or culturally normative ethical behavior.
3. Empathy: Lack of concern for feelings, needs or suffering of others, lack of remorse after hurting or mistreating another.
4. Intimacy: Incapacity for mutually intimate relationships, as exploitation is primary means of relating to others, including by deceit and coercion, use of dominance or intimidation to control others.
B. Six or more of the following seven pathological personality traits:
1. Manipulativeness (an aspect of antagonism): Frequent use of subterfuge to influence or control others, use of seduction, charm, glibness, or ingratiation to achieve ones ends.
2. Callousness (an aspect of antagonism): Lack of concern for feelings or problems of others, lack of guilt or remorse about negative or harmful effects of ones actions on others, aggression, sadism.
3. Deceitfulness (an aspect of antagonism): Dishonesty and fraudulence, misrepresentation of self, embellishment or fabrication when relating events.
4. Hostility (an aspect of antagonism): Persistent or frequent angry feelings, anger or irritability in response to minor slights and insults, mean, nasty or vengeful behavior.
5. Risk taking (an aspect of disinhibition): Engagement in dangerous, risky and potentially self damaging activities, unnecessarily and without regard for consequences, boredom proneness and thoughtless initiation of activities to counter boredom, lack of concern for ones limitations and denial of the reality of personal danger.
6. Impulsivity (an aspect of disinhibition): Acting on the spur of the moment in response to immediate stimuli, acting on a momentary basis without a plan or consideration of outcomes, difficulty establishing and following plans.
7. Irresponsibility (an aspect of disinhibition): Disregard for - and failure to honor - financial and other obligations or commitments, lack of respect for - and lack of follow trough on - agreements and promises.
Note: The individual is at least 18 years of age.
6. Other Common Experiences
• Theres a few experiences that quite a few people with ASPD report, that have not explicitly made it into the criteria. Sometimes these are examples for certain symptoms and/or are implied, sometimes these have been studied but haven't been written as a requirement for diagnosis and sometimes these are not supported by science/still debated by science.
• Apathy, a total lack of emotion, overall muted emotions or having trouble to access certain emotions, is something some people with ASPD talk about a lot. There is no scientific consensus yet, as to whether this is an ASPD symptom. Some theories suggest it falls under PTSD (absence of positive emotions & tendency to experience negative ones and/or having dissociated away from the emotions and/or having put up a sort of non permanent barrier as a form of protection), depression (common comorbidity, anhedonia & apathy can both be part of it), other PDs (schizoid, borderline episodes, etc.) or something else entirely. While its not sure whether its caused by ASPD, or not, a lot of people with it seem to report differences in their capability to feel a full range of intense emotions.
• The criteria talks about aggressiveness and physical fights, which is not the only way in which this symptom seems to commonly present. Harming animals, homicidal ideation, dealing with aggressive thoughts & urges without actually acting on them, verbal aggression, taking out aggression on self or property, etc. are also often reported.
• The current criteria doesn't mention it at all and the alternative talks about a complete inability to form bonds, but community consensus seems to be, that while forming emotional bonds is harder & happens more rarely, it is still possible. The intensity differs (some describe the bond as a logical construct, some only do platonic bonds, some only do romantic bonds, some describe deep obsessiveness, etc.) as does the number of people they find themselves bonded with. Theres also a significant amount of people in the community that describe a phenamenon similar to BPDs FP (aka a bond to a person that is defined by the symptoms of the personality disorder).
• There is some debate on whether or not an absence of prosocial inner standards makes it impossible or more difficult to define personal morals and understand how morality works. Some people with ASPD say they have no difficulties, some report that they struggle with the understanding part, some say they struggle with upholding those norms and others struggle with both. It seems like ASPD could make it more difficult to understand and/or respect the way societies morals work for some, which makes room for conflict.
• Personality Disorders are what we call egosyntonic, which usually means that they are in alignment with what we as people think is the correct way to feel, think and act. This doesn't mean that its inherently impossible to change the way you think/feel/act and that recovery is impossible, but it may make it more difficult to break out of the patterns (if that is what one wants). Some people show little problems in this area, some need a lot of outer assistance and others either can't or don't want to change.
7. Other Things To Keep In Mind
• You should probably think about whether your character fits the psychopathy subtype & if yes which definition of it you want to use (theres different theories)
• ASPD can influence every aspect of your life, so it may interfere with things in such a roundabout way that you wouldn't even think about it at first (ex: Disregard for safety of self => Disregard for your own health => You get ill carelessly => You dont take ur meds responsibly, or put off a doctors visit for months/years => You end up with longterm damage => You don't treat it responsibly => You get more ill => Death. Which happens to ppl without ASPD too, but can indeed be a presentation of that symptom.). Additionally comorbdities interact & interfere with ASPD symptoms and may alter/add onto presentation!
• You could also always add the ASPD stigma into the mix and how your character responds to it/how it influences them. Does it make them not wanna recover? Does it make them wanna recover even more to prove everyone wrong? Are they trying to get into therapy but no therapist wants them? Is it on a court record and causing problems that way? Do they lose relationships/friendships? Does it change the way they see themselves or others? etc.
• The key with ASPD characters is not to just make them into good people or portray them as angels and also not to always make them into the cruel villain. The key is to show that they are an individual, a human being, a single example for what this disorder can present as. If you can somehow portray that the presentation of ASPD in your character is just how this specific character is and is not how the disorder inherently presents itself, you nailed it! Cus u'll have ASPDers who want to just stay the way they are and who are exactly what you'd imagine a cruel villain to be like, you have ASPDers who you couldn't ever distinguish from a prosocial person, cus they learned to blend in and you've got ASPDers who decide that they wanna do a 180 and behave in the most prosocial way possible and then you have everything in between and beyond. So as long as your character would meet criteria, as long as you're not spreading misinfo and as long as its clear that its just one example of a possible presentation, you're good in my opinion (but this is indeed just my opinion and others may disagree).
Note: If you need examples for the specific symptoms, you can ofc send another ask, this is more of a general overview of what exists, cus going into detail on each would make this post wayyy too long.
#actually aspd#aspd#mental health#mental health education#antisocial personality disorder#aspd awareness#aspd safe#aspd things#aspd thoughts#aspd tag#writing#writing advice#writing help#mental heath awareness#aspd stigma#how to write a character with aspd#writers advice#how to write#questions#asks#asks open
98 notes
·
View notes
Text






i am cluster b but i do not have aspd so same as last time pls tell me if i got anything wrong 👍🏻
#digital art#art#digital painting#digital sketch#mental health#aspd#anti social personality disorder#cluster b#stigma#mental health comic#mental health education#mental health stigma
35 notes
·
View notes
Text

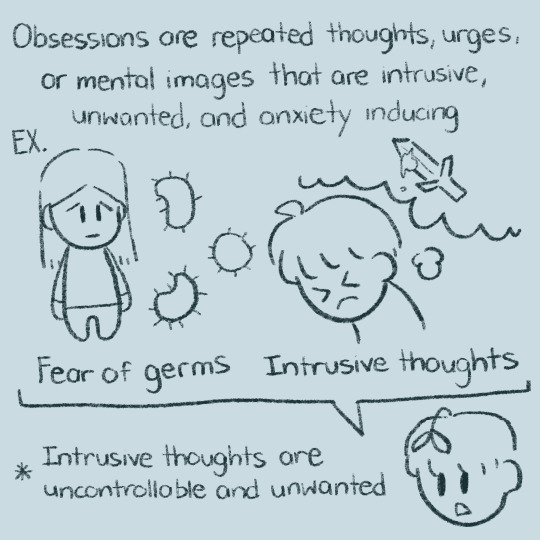
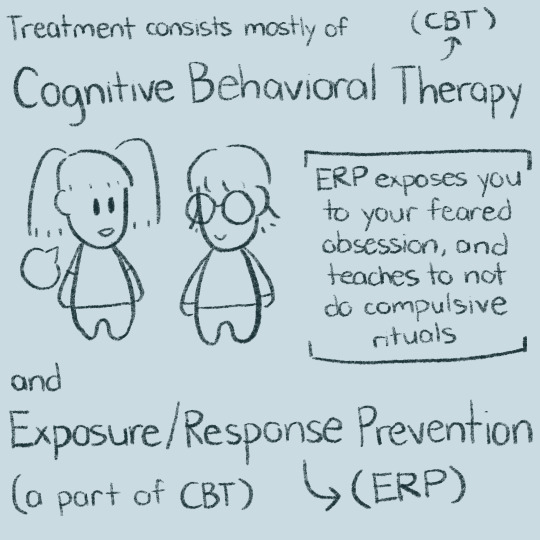
— from coping with ocd: practical strategies for living well with obsessive-compulsive disorder by bruce m. hyman and troy dufrene
#actually ocd#ocd#mental health education#ocd awareness#pure ocd#mental disorders#mental illness#I am anti psychiatry but this is useful info idk#I am learning to navigating those contradictions#like recognizing mental compulsions can be really useful for understand how your brain is coping with the anxiety#and try to work to do less compulsions as they actually increase anxiety#I need a break from my brain#and revolution#words words words#fountain pen
11 notes
·
View notes
Photo

(via When Anxiety Turns to Anger: A Hidden Struggle)
This comes from the Heart
#psychiatry#shrinks in sneakers#doctor#anxiety#anxiety disorder#anxiety tips#anxiety help#mental health#mental health matters#mental health education#mental health is health
3 notes
·
View notes
Text
im all for educating children on disorders and health and shit early in life for multiple reasons but partly because when i was a kid i had what i now know was a tic attack wherein i forcefully laughed (so much so that i was purple in the face and choking) and waved my arms for 4+ hours while at a school orientation thing and when i asked my friends what the fuck just happened one was just like bro didnt you know the fae kill people in the most beautiful ways and i just fucking. accepted that as the answer and told zero people about what happened. and when i was diagnosed with tourettes like 3 or 4 years later i was like oh shit so thats what that was
#tourettes#mental health#education#child education#mental health education#neurodivergent#kids will just make shit up if they cant explain things#its just the way shit goes#you gotta tell them what the fuck is up bro#kids#children#tics
23 notes
·
View notes
Text
There’s a post that says “Dear Taylor swift, mental illness is not an aesthetic” but believe it or not people with mental illnesses are actually more than welcome to turn their experiences into a creative outlet if they fucking want to.
With all due respect (which is none) your gate-keeping and fake-claiming vibes are not welcome here. Not in the swiftie tags, not in the mental health tags, not anywhere.
#ttpd reaction#ts ttpd#the tortured poets department#mental health art#mental illness art#mental health advocate#mental health education#anti fakeclaiming#fuck fakeclaimers#anti gatekeeping#mental health resources#art therapy#creative outlet#creativity#creative process#artists on tumblr#recovery art#trauma art#post traumatic growth
2 notes
·
View notes
Text
There needs to be more common education on mental illnesses, because in middle school my friends and teachers would comment on the fact that my hands were cracked and bleeding because I washed them so much, and I had no words to describe the absolute need I had to wash them constantly.
#personal#ocd#mental health#mental health education#I finally discovered what I had because my parents saw something was obviously wrong with me and did education on it#not everyone is that lucky#rain’s ruminations
6 notes
·
View notes
Text
If you knew
how to Love...
You would never feel the need to
say an unnurtured word, statement
or, ask questions
based on self- entertaing curiosity
But always because you are concerned.
🪶 Armaan. 🧭
Remember Darling, when you are connecting with another Life.
Tip for this writing 📮♥️
#love#love quotes#love quote tumblr#life quotes#how to talk to people#love quote life quotes#inspiring quotes#romantic#spilled ink#love poetry#poetry#mental health#mental illness#positive mental attitude#writer#writerblr#mental health support#mental health education#how to talk to anyone#how to love#writers on tumblr#self development#self help#self reflection#self love#self improvement#selfishness#self care#donate if you can
2 notes
·
View notes
Text
Knowing and admitting you need help is one thing
but knowing what help you need or how to acquire it or where to even start is a whole other thing entirely.
Anyone have any tips or resources for this?
#audhd#cptsd recovery#borderline personality disorder#late diagnosed autistic#actually autistic#neurodiversity#disability resources#mental health resources#adhd resources#bpd help#did osdd#chronic illness#chronic pain#mental health help#mental illness#accessibility#intersectionality#healthcare#mental health education#executive dysfunction#self care#mental health community#autistic community#late diagnosis#unmedicated#living with adhd#adhd autistic#adhd help#adhd problems#adhd community
191 notes
·
View notes
Text
Early Signs of Schizophrenia and Prevention Strategies!
Schizophrenia, a complex and often misunderstood mental disorder, affects millions of individuals worldwide. It is characterized by a range of symptoms that impact thoughts, emotions, and behavior. While the exact cause of schizophrenia remains elusive, early detection and intervention are crucial for managing the condition effectively. In this article, we delve into the early signs of…

View On WordPress
#Cognitive health#Early detection#Early intervention#Mental health awareness#Mental health education#Mental health prevention#Mental health promotion#Mental health support#Mental wellness strategies#Preventing schizophrenia#Psychiatric disorders#Psychosis signs#Schizophrenia awareness#Schizophrenia risk factors#Schizophrenia symptoms
2 notes
·
View notes
Text
ASPD: The Desire for and Run from Intimacy
This post will only contain my personal opinion and experience. It may not be applicable to all other people with ASPD and may likewise be relatable to people who do not have it.
I am only going to be talking about emotional intimacy, but this post is definitely also applicable to the other type of intimacy!
I'll make myself pretty vulnerable in this post, by discussing my personal experience, so you better not make me regret that!
Abbreviations:
ASPD = Antisocial Personality Disorder
ASPD is a disability caused by prolonged childhood trauma (with many possible variations), that develops in order to protect the brain from said trauma, or rather to help the brain deal with it in some way!
While the consequences of this in the context of intimacy, look different for every person with ASPD, many do report: a difficulty with developing bonds, having problems trusting people & giving away control, losing feelings for people quickly and abruptly/getting "bored" of people, responding extremely to arguments, having problems dealing with peoples emotions/ problems with being close to people etc.
This may be due to a variety of factors, but does often tie back to having no or few positive experiences with intimacy, having not learned how to exist in relationships properly/a lack of being socialized, not having the necessary prosocial emotions and mechanisms to deal with it and other similar things.
While this causes some people with ASPD to develop a brain, that does not have a need for emotional intimacy at all, others develop a brain, that craves the emotional intimacy it has been denied, but which will also fight said intimacy at every turn.
Thats as much generalized info as I can give you, as the exact representation of this is highly individual, but I will offer my personal experience on the following slides!
What you need to know is that I was accidentally neglected for huge parts of my childhood and teens and did not get my emotional and social needs met most of the time, while also knowing that my parents were theoretically capable of that, as they were giving everything I lacked to my sibling.
This caused me to grow up with a burning desire for intimacy, while being disappointed by people time and time again, failing to actually develop the things needed to experience this intimacy and partially growing to resent it and viewing it as "weak" and "bad".
Ever since then I have been stuck in what I like to call the "ASPD stages of running". Theres different points in getting close to people (in any nature of a relationship), that'll send me running and feeling like I am "weak" for wanting it, or as if being close to people is the worst thing that could happen.
The stages (simply put) are:
1. Desiring/Daydreaming about my dream relationship
2. Looking at peoples relationships/Looking at people with the intent of getting closer to them
3. Talking to people (online or irl)
4. Getting closer / being friends with people
5. Being friends with people for longer
Optionally:
6. Getting so close that a romantic relationship may happen
7. The moment of getting in the relationship / the days after
8. Being in the relationship for a bit
At any of those stages, I'll very likely have one or multiple moments where my ASPD will try to get the better of me and will try to convince me to just run away, drop contact and never talk about it again. Even just admitting to this and talking about it is hard as fuck, because it is so deeply ingrained in my brain to see emotional intimacy as a weak and dangerous thing.
What this will look like exactly really depends on the person and situation, but things that have happened in the past were:
• blocking the person and everyone I am friends with and pretending I am no longer alive
• my brain fixating on their faults in order to give me a good reason to hate them so I don't get closer to them and can hold them at arms length
• responding less often/more dryly or ignoring messages entirely
• not replicating the energy of the conversation/relationship
• staging an incident so I ruin the relationship
• running at the first signs of a disagreement
• avoiding people when they are emotional
• feeling uncomfortable around people as a whole => isolating
• beating myself up about letting it happen again
• impulsively bumping the relationship to another stage, just to immediately regret it (in a "fuck that has consequences" way)
• shutting off all my emotions, dissociate or otherwise make sure to stop the feelings (or just lose them automatically)
To put it in a shorter and more simple way, I'll usually either get the fuck outta there, or make sure to change the relationship/my personal position in the relationship to a more comfortable and less vulnerable and intimate level. This may also just look like me shutting off, becoming distant, or seeming mad, when all I am is overwhelmed by the intimacy and grossed out that I actually need and desire that.
As you can possibly imagine, that is not the most useful thing, as it causes issues in relationships, cuts friendships short and makes dealing with people a lot harder!
The most frustrating thing about this for me though is, that even if the most perfect friend or partner came along and even if the relationship would work at first, I am very very likely to crash it against the wall, simply because my brain cannot handle having the things, that it needs and desires.
It desires a hug and runs from the one who offers it.
It needs help and bites the hand that does.
It needs love and gets grossed out by whoever offers it.
It wants attention and can't handle it when it gets it.
It wants gifts, but doesnt know what to do when it gets them.
Whatever it wants, it can't have, so it keeps wanting, keeps yearning, keeps desiring and has to watch itself be unable to accept any of it.
And if that sounds painful, thats because it is.
Its a vicious kind of pain when you have to watch yourself ruin yet another thing, because your brain can't handle it, while you scream at it in frustration to get its act together, because it also is everything you desperately need.
ASPD sucks when it comes to intimacy and it especially sucks when it comes to talking about it, or being honest about these problems. It developed to protect me from being too "weak" to deal with the trauma and now its practically preventing me from showing any "weakness" or seeking out what previously hurt me. Which wouldn't be this bad, if I didn't still have this kid in me that just wants to be loved and daydreams about all the things, the ASPD hates.
When your shell disagrees with your core and you're not strong enough yet to break your shell, what does that really leave you with, other than curling up into a spiky ball and letting the shell do its job? I know I still need the protection, but I wish it wasn't actively preventing me from learning to live without it.
First posted on my instagram (same @)
#actually aspd#aspd#mental health education#antisocial personality disorder#mental health#antisocial#aspd awareness#aspd feels#aspd thoughts#aspd things#aspd mood#intimacy
390 notes
·
View notes
Text




tell me if theres misinformation in here please, i used several sources but i could still be wrong
#ocd#ocd tag#obsessive compulsive disorder#obsessive compulsive behavior#mental health stigma#mental health#art#digital art#digital painting#digital sketch#original comic#mental health comic#anxiety#intrusive thoughts#intrusive thinking#education#mental health education
20 notes
·
View notes
Text
Doing less means letting go of the whack-a-mole approach to OCD, of jumping from one scary thought, concluding it must be OCD nonsense, and then jumping to the next scary thought until that one has been neutralized. Instead what is needed is a shift in attitude and mindset; a move from “I have to get rid of these thoughts” towards a stance of “I can get better at accepting mental chatter as it comes and goes.” Sufferers can strive to recognize that the volume (or loudness) of the subject matter or content is not an indicator of its importance. We all walk around with a degree of mental chatter or “the committee,” a term used by members of Alcoholics Anonymous to describe their awareness of the mental activity going on. What sets apart the OCD sufferer from those without the condition is the OCD sufferer’s acute awareness of the chatter and the predisposition to judge or attribute meaning to the chatter.
— molly schiffer, help! I have OCD about what’s OCD (emphasis mine)
#ocd tag#actually ocd#mental health#mental health struggles#ocd awarness#ocd recovery#mental health education#mental health tips#words words words#quote
5 notes
·
View notes