#did-research.org
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
When you start to try to fact check information about DID it is absolutely insane how much of it seems to be from DID Research.
Like from what we have caught alone, did-research.org seems to be the earliest source for:
DID only appearing before the ages of six to nine
OSDD-1 being divided into OSDD-1a and OSDD-1b
The average number of alters is 12 for males and 15 for females
Especially the first one makes me feel like I'm loosing my goddamn mind because it's constantly cited as a "gotcha" in syscourse, but there is no earlier source for that we can find besides did-research.org.
#did resarch#did-research.org#syscourse#we haven't even really done a deep dive into the website or anything this is just what we've found from trying to look up other things#then we realize we can't find any studies or anything to prove it so we look it up. then sure enough it's just pulled by them out of nowher#like this keeps happening#the website is also way too focused on people who fake DID in a way that just. completely comes across as someone trying to spread an agend#on top of this was one of the biggest blogs back in the day that spread fakeclaiming and they were giving unsoruced misinformation then too#and it just comes across as one of those sources you find that's written by a DID skeptic but they try to hide it
42 notes
·
View notes
Text
i've been in and out of my mind since the 8th. it feels too easy to "disappear" and have Ares take my place, and i cannot even look into how to compose myself because i am disallowed by him.
#it's hard to explain what happened in a way that doesn't seem absurd to an onlooker.#even the concept of 'disallowment' feels difficult or i am unwilling to explain out of anxiety.#delete later.#i don't know. can i just replace my speech with a link to 'did-research.org'...
1 note
·
View note
Text
Harry Du Bois, the skills + DID/OSDD coding
a compilation of most of my thoughts on harry as a system (note: i am system im not just like. pulling stuff out my ass)
1. Structural Dissociation Theory crash course
so for this point i'm going to give you a crash course structural dissociation theory (do not use me as a source for ur knowledge on it this is very like. base level and just to establish context)
structural dissociation states that we all start as multiple different facets, and that as we grow up, these facets all fuse into a cohesive personality. however, in DID/OSDD, ongoing trauma proves it safer to NOT fuse these facets and instead develop dissociative and amnestic barriers between them to varying degrees. these facets cope by developing into individual personalities, and if traumatic events persist, the brain may split more personalities to try and cope with this. this gives us two bits of information that i'm going to use throughout this
1. there is no "original", just alters that host for long periods of time and/or identify with the body the most
2. amnestic & dissociative barriers are fluid. in times of rest, these barriers may start to come down between some alters, but not necessarily all.
**NOTE: these are not hard and fast rules and vary from system to system. it's also vastly different if you have Polyfrag DID or Complex DID. since I don't hc Harry as polyfrag or complex tho, i'm not gonna get into that
2. Harry (the system)
so it's pretty easy to establish that harry has a good handful of childhood trauma. being born in a military hospital + town and growing up there means he probably saw and/or heard a lot of death and sickness. we also know his father left based on the logic passive in the measurehead conversation

we also know from the reaction speed passive when you find out your name that harry was born in a time all these were concerns. most likely, hunger, considering how through the game hunger + eating is an undertone w/ harry
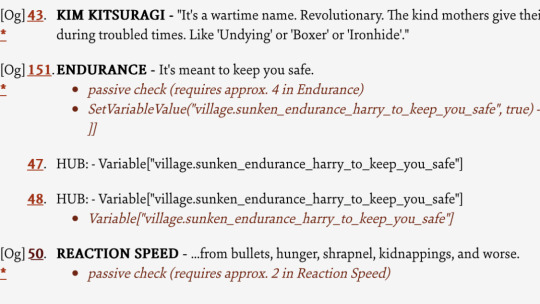
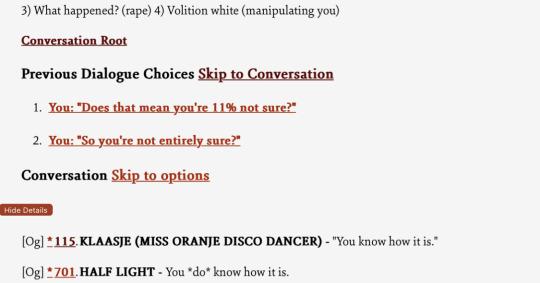
we also have the klaasje half-light passive implying that harry's been raped (might not have occurred during childhood, but still a contributing factor to trauma)
my point being bro has enough childhood trauma and then some to create a system.
we also see a LOT of amnestic barriers between harry and the rest of the skills. besides the obvious not remembering anything, we see the skills remembering things that harry doesn't.
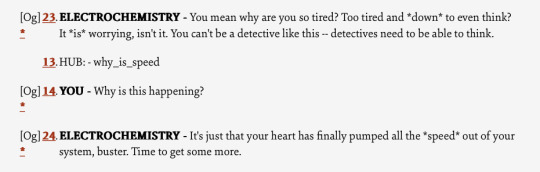
for example, EChem remembers that harry took speed some point recently, while harry himself doesn't
we also see that the skills have distinct personalities and opinions separate from each other. shit we've got a communist (rhetoric) and a fascist (endurance) living in the same fucking body. half light is immediately suspicious of everyone and everything while empathy tries to understand everyone even to their own detriment. and volition and echem need a whole post of their own. thats some pretty strong dissociative barriers
3. Harry (the alter)
to be quite honest with you i think harry as we, the audience, know him is a brand new split, an introject* of an old host that has either fused with another alter or gone dormant. he's trying to fill a different harry du bois's shoes- someone he is fundamentally similar to, but is, at his core, not
*Definition from did-research.org: Introjects are alters that are based off of an outside person or figure. Introjects may or may not see themselves as the individual that they represent.
knowing nothing about yourself, even what you look like, is a common feeling for new splits (in our experience). with the high amnestic barriers separating harry from the rest of the system, it makes sense that the first time he is conscious he is totally lost about his own identity, where he lives, or what his occupation even is.
losing facts about basic reality is probably a dissociative response. things the brain knows (see encyclopedia filling in gaps once given a prompt about something like Fillipe the Conquerer) but doesn't want the new host to know for fear of not being able to function.
4. Certain Alters with Functions
some of the skills fall into alter "archetypes" (not all alters will, even in like. real life systems) and im just gonna list them out here:
ones with subtextual backing:
Volition: Caretaker + Apparent Normal Part
Half-Light: trauma holder
Electro-Chemistry: symptom + trauma holder
Authority: protector
Logic: apparent normal part
ones that are just my headcanons:
Interfacing: little
Endurance: ex-persecutor
Inland Empire: ex-caretaker
here ends my post of articulate thoughts, if u have any like. follow up questions feel free to shoot me an ask. might take me a minute tho
279 notes
·
View notes
Note
Do you have any idea where the myth of "None, OR, Not a lot of amnesia = OSDD" and "blackout amnesia = DID" came from? I heard it since 2016, and posts for a search of "osdd1b amnesia" bring up the same so I guess the idea recently circulates as well. In 2016, me and my friend thought we had OSDD instead of DID because we didn't always have amnesia. I was under the impression OSDD1B has No Amnesia except for emotional, correct me if I'm wrong? (yada yada insert disclaimers about 1B here lol)
Did-research.org is typically the source of these kinds of myths. Did-research is run by another tumblr blogger with a similar educational background to myself.
The site is quite old and the wording is very clunky and unclear in a lot of places. This is also where the myth about osdd 1a alters comes from (if you have full alters, it's 1b, even if they're you at different ages).
So, to clarify for others, osdd 1b (Obligatory "doesn't actually exist") has EMOTIONAL AMNESIA ONLY.
Emotional amnesia is a fancy way to say "dissociation." A disconnect between memory and emotion.
DID can have SO MANY different types of amnesia.
Amnesia only for childhood trauma with full system communication? DID.
Amnesia between some alters and not others? DID.
Blackout amnesia? DID.
Gray out? Probably DID, depending on who's defining it.
47 notes
·
View notes
Note
You know what, I'm sick of u endos, u want proof take a read.
did-research.org
I've seen that site before. Heck, I've cited it years ago in some discussions on DID when I was too lazy to get real academic sources and was okay settling for a glorified blog ran by a random psych student that hasn't been reviewed or endorsed by professionals.
The thing is, it doesn't address non-DID plurality at all.
Alright, you're new to this game, right? You've probably been on TikTok for a while or isolated in your remote anti-endo communities where people will accept a random psych student's webpage as a valid source while telling you that the science is on your side and keeping you blissfully ignorant of reality.
So let me just say... welcome to Tumblr.
If you want to talk about sources and proof here, you've gotta do better.
So I'll raise your random student blog (that doesn't even support your point) with the Plurality chapter of Transgender Mental Health.



This book is written by Dr. Eric Yarbrough, a Distinguished Fellow of the American Psychiatric Association, which is the highest honor the APA gives. The book itself was also both reviewed and published by The American Psychiatric Association's publishing division.
#syscourse#pro endogenic#pro endo#anti endogenic#anti endo#plural#pluralgang#multiplicity#sysblr#systems#system stuff#psychology#psychiatry#did-research#actually plural#actually a system
51 notes
·
View notes
Note
This is more of a question rather than something regarding misinfo, but is there a specific term for what the, like, ORIGINAL is called? We use the term "core" since that's what we found once, but we've also heard people refer to them as the "host" or the "body" and we wanted to know if there was a correct term or if "core" is something we shouldn't use since we've never heard anyone else use the term "core", although we don't meet new people, especially systems, very often which may be apart of it.
So sorry if this is worded wrong or weirdly!!!!
techincally the term for the "original" is core, but the term core is very debated,, it has been used by people but whether a "core" exists or not is argued over " There is currently a debate over the existence of cores because it does not easily fit with the theory of structural dissociation. Not all systems have a part that could be identified as a core. "
the idea of a core doesn't completely fit with the theory of how DID forms, since if we go off the theory of structural dissociation there would be no "original" or "first" alter (as before alters are formed it'd just be fragments / parts of an identity, not a integrated identity,, if that makes sense?)
it kind of depends how you refer to it / how you use the term core. i would say that overall, the term is disliked since it goes against the theory of structural dissociation,, though did-research.org says that a core could be fit into it as; "one has to examine the theory as it exists on a spectrum to conceptualize how an early failure of integration could still allow one part to integrate before others." which i guess could make sense in a way? it depends.
really its more of a personal thing i think,, most systems don't like the term but if you like it i can't stop you from using it. there's not much else to say. ((also calling them the original is also widely disliked too, but its pretty much the same thing))
apologies if this doesn't really answer your question, i'm unsure what to say
#- dreambee#anti endo#endos dni#system#did osdd#osddid#did#traumagenic system#answered asks#didosdd#plural#anti misinfo#sourced#requested info
39 notes
·
View notes
Text

Ok so I did because I was curious to see what was actually there.
So first now of course we have the AI overview.


Firstly thought to form and typically strong word choice there very persuasive/sar. Secondly what do they actually link in the overview? Two blogs and WedMD. So I guess now what does WebMD say because I hope we aren't using blogs as our sources here.

Again with the weak word choices. Using likely then stating 99% instead of 100. What about that last 1%?
So now let's scroll down the page and see what we find.
Firstly we have did-research.org which has a disclaimer page stating not all information on the page is necessarily accurate and there is already some well known things on that website that are questionable in their accuracy when you look at the science on the topic. Also basically just one person's blog so not a reliable resource.
Next in the list one of the blogs linked in the AI overview. They seemed to actually be citing some good sources though...

...still that use of weak language.
Next we have "how do new alters form" asked on r/DID and I decided to check to see if anyone added a source to their answer to give it the benefit of the doubt. They didn't and I shouldn't have to explain why this is a bad source.
After that we have the othe blog from the AI overview the fact it cites did-research.org as a source immediately knocking it even further down in credibility and all of their other sources use that same weak language.
Then we have quora with "how are new alters in DID systems created? Can it happen randomly?" Again I checked for any sources and found none.
And finally after going through all those sources we finally get to a credible one which does actually support their argument until you read what it is about. "Formation and Functions of Alter Personalities in Dissociative Identity Disorder" It isn't talking about every case where alters are present just the cases where the individual has DID and nowhere does it say you need DID to have alters. It also starts to use the same weak language when it actually gets to the actual descriptions of alter formation.
I'm just wondering how they think the first thing that pops up is supporting their point when it takes me to the seventh to find anything. Also most endogenics aren't claiming to have DID and most don't. Most also don't use the word alters. So I really don't see why they think they have proved anything. If your sources aren't talking about endogenic plurality they are not evidence for or against it.
23 notes
·
View notes
Text
> give a proendo but traumagenic system a chance because theyre our coworker and we dont want bad blood
> after a while, breaks the boundary that we set of “please don’t bring your views into our server or speak to us about them”
> open a ticket and politely reminds them of the boundary set
> gets aggressive, cites did-research.org and calls me and my partner names
anyway here are the highlights from the mod chat/our friends losing their shit with landline since hes the main handler of drama



#aurora (he/him)#landline/hi8 (he/hxm)#nuke txt (syscourse)#nuke img#they dont have our tumblr so they will not see this#im still so flabbergasted#actually did#anti endo#did#did community#did osdd#did system#polyfrag did#osdd did#system discourse#system#traumagenic system
12 notes
·
View notes
Text
Not-so-friendly reminder that you cannot be a system without trauma.
Some more proof; done by me, a person living with DID.
This is not syscourse, this is fact.
According to the Diagnostic and Statistical Manual of Mental Illness (DSM-5), a history of childhood abuse and neglect is prevalent in 90% of cases of dissociative identity disorder (DID). The remaining cases involve medical trauma, terrorism, and childhood prostitution. Ninety percent is overwhelming. Other research claims that rates of abuse and neglect in DID are actually much higher.
DID develops in response to severe, recurring trauma in childhood. Children are not fully equipped to cope with continued, severe instances of abuse, so they may develop dissociation as a survival skill, which can then develop into DID. It makes sense, then, that the rate of childhood abuse and neglect in people with DID is so high.
https://www.healthyplace.com/blogs/dissociativeliving/2016/04/the-undeniable-connection-between-did-and-child-abuse
The authors interviewed 102 individuals with clinical diagnoses of multiple personality disorder at four centres using the Dissociative Disorders Interview Schedule. The patients reported high rates of childhood trauma: 90.2% had been sexually abused, 82.4% physically abused, and 95.1% subjected to one or both forms of child abuse. Over 50% of subjects reported initial physical and sexual abuse before age five. The average duration of both types of abuse was ten years, and numerous different perpetrators were identified. Subjects were equally likely to be physically abused by their mothers or fathers. Sexual abusers were more often male than female, but a substantial amount of sexual abuse was perpetrated by mothers, female relatives, and other females. Multiple personality disorder appears to be a response to chronic trauma originating during a vulnerable period in childhood.
https://pubmed.ncbi.nlm.nih.gov/2044042/
Causes
The main cause of DID is believed to be severe and prolonged trauma experienced during childhood, including emotional, physical or sexual abuse.
The development of dissociative identity disorder is understood to be a result of several factors:
Recurrent episodes of severe physical, emotional or sexual abuse in childhood.
Absence of safe and nurturing resources to overwhelming abuse or trauma.
Ability to dissociate easily.
Development of a coping style that helped during distress and the use of splitting as a survival skill.
While abuse is frequently present, it cannot be assumed that family members were involved in the abuse.
Dissociative identity disorder (DID) is the result of repeated or long-term childhood trauma, most frequently child abuse or neglect, that is often combined with disorganized attachment or other attachment disturbances. DID cannot form after ages 6-9 because individuals older than these ages have an integrated self identity and history. Trauma later in life can lead to posttraumatic stress disorder or complex posttraumatic stress disorder, other dissociative disorders including other specified dissociative disorder, somatic symptom disorders, or possibly borderline personality disorder, but DID requires an unintegrated mind to form.
https://did-research.org/origin/
Other helpful links!!
DSM-5 on DID and
A explanation of each DD
NAMIs fact sheet on DID
Please see this account for OP
A PDF research paper done on the link between DID and childhood abuse
My own multi-part research thread
A post about biomarkers in the brains of pw/OSDDID
#Sage speaks#host posts#Mystic speaks#Mystic - 🧜🏻♀️#co-con#did is a disorder#did research#did#did is caused by trauma#you cannot have DID without trauma#stop faking DID you clowns#I was not traumatized for it to be used for clout chasing#endos aren't real#tw endos#endo dni#anti endo#fuck endos#anti endogenic#endos do not interact#endos fuck off#endos stop being shitty#endos are not valid#truamagenic system
244 notes
·
View notes
Text
this is an important thing i want to talk about. im mostly refering to Emesis Blue fandom here, but it goes for any fictional media. ‼️please read even if you don't like Emesis Blue this is a general important message‼️
sorry for the rant but. can we please stop using "split/multiple personality disorder" in the context of "i think this character has it because 2 evil sides. its his other personality coming out!". actually can we also stop using those names too? MPD as a name has been outdated since 1994.
like.. as someone with DID (Dissociative Identity Disorder, "MPD"s ACTUAL name.) it's so fucking heart breaking to see people still have this mindset in 2024. like please before you even let a disorder's name out of your mouth please actually research even a tiny bit. one little thing you say can be so harmful.
I should also state im specifically talking about those who don't have said disorder of course. for example, i as a person who is medically recognized as having DID like to headcanon Postal Dude with DID. i usually keep it to myself unless i go in full depth to make sure i am not demonizing it or misrepresenting it. (i do have a post explaining it on my alt. i use it to cope.) generally, i think if someone has said disorder and they headcanon even a villain or a bad person character with it, they are allowed to
the issue comes when people without this condition come into play, and dont even respect the topic a little bit. this is where i talk about Emesis Blue.
No guys, pills do NOT give you DID. DID only comes from repeated childhood trauma.
no, DID is NOT the "2 personalities 1 is evil" disorder.
i hate ever mentioning my disorder onto this specific blog but this is the only way ill reach people. please stop misrepresenting disorders, especially using their VERY OUTDATED names and views.
im bringing up emesis blue specifically because someone's art i REALLY liked did emesis blue art, and i was instantly met with this in their tags.

please, this goes for ANY FICTIONAL MEDIA, please stop representing DID this way. it is super harmful.
please do not witch hunt people either. i know not everyone is gonna know every thing, or be up to date. i know people arent constantly researching disorders like i like doing, i just want people to know that these representations of us are super harmful and we need to stop them please.
thank you so much for reading. please reblog so more people see. im sorry for this on my main.
if you want to learn more about DID, i would recommend this site as a start. https://did-research.org/origin/structural_dissociation/
im also not FORCING YOU to research every little thing about disorders or at all, just please do not severely misrepresent them in such a harmful way.
thank you.
#lemonmeat#rant#important#important psa#did#dissociative identity disorder#actually did#endos dni#emesis blue#tf2 emesis blue#dr fritz ludwig#fritz ludwig#osddid#did osdd#actually dissociative#tw demonization#medic tf2#tf2#team fortress 2#tf2 medic
12 notes
·
View notes
Note
I was wondering if you could write a saiki & reader oneshot fic with a reader who has DID & C-PTSD and paranoid tendencies? I understand that that might be a bit too hard to write but just in case I got some recorces that might be handy, here is the link to DID listing from my own copy of the newest version of the DSM https://www.dropbox.com/sh/htaraej65e34tg9/AADBATmelRQFUBfTMxaJ3W6wa?dl=0 as well as this website that has a lot of good info on it https://did-research.org/ and this page I found that has a brief overview of C-PTSD https://my.clevelandclinic.org/health/diseases/24881-cptsd-complex-ptsd but I also recommend quickly reading thru the different types of flashbacks (shouldn't be that hard to find info on)
The main idea is that because of the mix dissociation,switching,paranoia, different types of flashbacks etc that the readers thoughts are very fucking confusing to saiki (feel free to use this premise for any kind of plot you want just try not to make it overly angsty is all I ask, well as un-angsty as you can get with C-PTSD anyways lol) I just wanna see more y/n / reader inserts that I can actually relate to but the saiki K fandom is so small
Can be platonic or romantic
Hi!! So sorry for the late reply, I researched as much as I could so if theres anything remotely wrong or different please tell me! Ngl, im not very sure i like how it turned out, nevertheless I hope you enjoy :))
Also i totally get that its hard finding stuff for saiki k which is the reason why i write for it in the first place, they totally deserve more recognition!! Feel free to send more requests in the future!!
⤑Back to navigation
Content: somewhat angsty but not really, i tried to be as vague as possible so as not to trigger anyone, reader suffers from trauma, DID, CPTSD, swearing, fluffy ending? slightly oc saiki
Summary: Saiki was used to listening to many types of thoughts, and at one point, nothing he heard surprised him. However when you came around, he was beyond confused. What sparks as a little curiosity might turn into something more.
✧・゚: ✧・゚:✧・゚: ✧・゚:✧・゚: ✧・゚:
ღNo matter what
He was used to it, or at least that's what he used to tell himself. Throughout the years he had heard all sorts of thoughts, at one point, he learned to tune them out when need be, having listened in on weird enough ideas that now don't surprise him anymore.
When you came in the picture, he was...baffled, to say the least. Confusing wasn't even close of a word to express how he felt. Your thought process was anything but simple. At times it'd be a fuzzy mess almost as if you lost part of your memory, other times, you'd think as if you were a completely different person, contradicting many of your previous thoughts. But what disturbed him most was the series of traumatic thoughts that would cross your mind. Flashbacks he realized in that moment.
In the beginning he felt annoyed, as per usual. Often times, he'd find you in class with a dazed expression, which to be frank, he had seen enough times to not give it a second thought. But then his attention would be caught when your mind would wander and you'd start thinking in a very unusual way. They were so unlike the person you presented to be, so much so that Saiki was left perplexed and in need to understand exactly what was going on.
The more it happened the more worried he'd be. There were days where you acted a certain way, and other days where you acted completely different. He could tell you weren't being fake trying to act differently for attention, after all, your thoughts lined up with the you acted and the things you said. Rather, it was the abrupt changes in your behaviour that had him thinking for far longer than he normally would.
Along the way, he also picked up how you'd flinch if you were in sudden physical contact, the way your shoulders would tense and the way your heart beat would speed up. Saiki wasn't stupid of course, he was aware that all of this was caused by some form of trauma.
He knew not to pry, yet his heart strings pulled everytime he saw you having a bad moment. So he began to follow you, in disguise of course, and even if he seemed like a stalker, he couldn't help it. Eventually he began to connect the dots, your reactions, behaviors, everything. It made sense now.
Unconciously, his words began to soften around you, his touch became gentler, he looked out for you in ways he had never done so with others. You began to notice but in no way did you mind, if anything, Saiki was someone you took great comfort in. What started of small slowly grew into something neither of you expected.
Of course, that didn't make it any less hard for either of you. Like right now. You were laying in Saikis bed, your head resting on his shoulder as you watched a movie, when suddenly a specific scene had triggered an anxiety attack. Your mind was racing through flashbacks of the many disturbing events you had gone through. Saiki was up almost immediately, having read your mind and sensed your reaction.
His touch was soft, his hands cupping your face so gently you'd think he was scared to break you, which he was. He was in no way someone who could comfort others easily. Nevertheless he tried his best. He attempted to lower your heart rate, rubbing small circles against your back as his other hand held the back of your head. No words were needed, they never were. He had, in a way, been there for you, way before you two even became a thing, so none of this was a surprise for either of you.
That didn't ease the guilt in your heart any less. You always felt bad. You knew Saiki could read you, literally. And well, it wasn't pretty. Countless times you had attempted to push him away, yet he never budged.
"'m sorry" you mumbled against his shoulder as your rested your head on it.
He cupped your face in his hands, pulling you to look at him.
`I won't let you push me away. The things you went through won't make me see you any differently, because to me you'll still be someone I cherish'
Your eyes welled up as you looked him deep in the eyes, finding nothing but love for you. Still cupping your face, he ran his thumbs under your eyes, wiping the tears away. He leaned forward, pressing a gentle kiss to your forehead.
'I love you'
"No matter what?"
`No matter what'
#headcanons#masterlist#saiki kusou no psi nan#saiki kusuo#saiki no psi nan#kusuo saiki#saiki k#saiki fanart#ao3 saiki#the disastrous life of saiki k#disastrous life of saiki k#saiki kusuo no psi nan#saiki x reader#saiki icons#saiki headcanons#saiki imagines#saiki reactions#saiki oneshots#saiki k headcanons#saiki k imagines#saiki k fanart#saiki k x reader#saiki k no psi nan#saiki k fanfic#saiki ff#saiki fanfic#anime masterlist#anime edit#anime and manga#anime gif
91 notes
·
View notes
Text
Resources we recommend to learn about Dissociative Identity Disorder (DID) and Otherwise Specified Dissociative Disorder (OSDD):
YouTube:
Multiplicity And Me
Jess is now recovered from DID, but she has previously posted tons of educational videos on DID that are backed by studies and professionals. We recommend this channel to systems and to professionals wanting to learn more in depth detail about not only DID, but communication with the system, alter roles and internal relationships.
Websites (UK):
The NHS website
DID-research.org
Mind
Whilst I know we don't have a lot of resources, these are the places in which we have learned about DID. With both MultiplicityAndMe and DID-research sourcing their information from research papers, the DSM and ICD as well as professionals who specialise in trauma and dissociation, these are the sources of information we trust and recommend the most.
The NHS website and Mind do have information on dissociative disorders. Although this is just basic information and not in depth, it's still a good read if you need a basic definition of dissociative disorders and their symptoms.
If you have any more recommendations for YouTube channels that do educational videos on dissociative disorders (that are also backed by research papers & professionals), please feel free to recommend them, and we'll check them out!

#actually did#diagnosed did#did osdd#did system#dissociative identity disorder#endos dni#actually dissociative#actual did#anti endo#dissociative disorder
37 notes
·
View notes
Text
Referencing this post that I replied to; other than my gripes about the ToSD being very colonialist in it's assumptions, the OTHER large issue I have with how ToSD is talked about in online spaces is that everyone applies a circular reasoning / argument as to how ToSD is absolute and correct.
For simplicity of discussing it without the pre-occuring discussion:
[...] before you state that its impossible for people to experience themselves as plural without trauma and that said person DEFINITELY has trauma they don't know about, please provide a genuine literature review or MULTIPLE sources (because one source is not enough to make a claim) with empirical research that has been replicated across studies that are NOT just on white / western cultures that proves that all people integrate into one state of self without trauma. I'm not asking for research that proves that "trauma causes DID" because that is unethical and there is no reason to expect that literature to exist, I'm asking for the null hypothesis that people will always - across all cultures and backgrounds - fuse into one person. The fundamental statement that underlies the ToSD is a huge assumption in its own that is largely unfounded in literature. Even the famous did-research.org (which is not a strong source, its written by a person who is a PhD candidate, its a nice source for convenience but its secondary) acknowledges that it is based on the ASSUMPTION that people fuse. Unless there is proof that people across all cultures always fuse to one identity state, using the ToSD to say it "proves" that all people fuse is a circular argument / circular reasoning as "The ToSD operates on the assumption that all individuals fuse into one identity" then "The ToSD states that trauma causes this fusion into one identity to be disrupted thus causing DID" then "therefore ToSD proves that people will fuse into one unless they have DID, thus using itself as proof for the premise". The ToSD can't both be based on the assumption that all individuals fuse unless disrupted by trauma AND also be the proof that all individuals fuse unless disrupted by trauma.
It's not all that much better of a circular argument than the assumption that god exists, that the bible is right because god exists, and the bible says god exists, so god is proven to exist.
If you change "god" with "fuse into one person unless disrupted by trauma" and bible with "ToSD" its the exact same arguement.
So unless there is literature out there that accounts for intersectionality and cultural awareness and is actually replicated to the standard that it should to be considered anything more than a "finding" in science; the argument is circular and not much better than the classic biblical circular argument.
You can't both have something based on an unproven assumption AND have that prove the unproven assumption.
#sysconversation#this one just really bugs me whenever I think about it#its bad science and bad scientific literacy#vent#vent tw#this one is kind of a vent
12 notes
·
View notes
Text
Masterlist of information and resources for dissociative disorders, including dissociative amnesia, depersonalization-derealization disorder, and dissociative identity disorder (+ subtypes)
**THESE RESOURCES AND INFORMATION ARE NOT TO BE USED TO SELF-DX YOURSELF. THESE ARE MEANT TO BE A STARTING POINT TO LEARN MORE ABOUT THE DISORDERS. IF YOU FEEL LIKE YOU MIGHT HAVE ONE OF THE FOLLOWING, DO MORE RESEARCH ON YOUR OWN. AND IF YOU CAN, SEE AND TALK TO A PROFESSIONAL. FURTHERMORE, I CAN BE WRONG! THESE ARTICLES CAN BE WRONG! YOU CAN SEND US ARTICLES/PAPERS ON ANYTHING HERE TO CORRECT US, AS LONG AS IT IS NOT A CARRD OR SOMETHING ALONG THOSE LINES. THIS IS A STARTING POINT, A LAUNCHPAD IF YOU WILL, NOT THE FINISH LINE. **
I would also like to remind you that all systems are different. Systemhood is a spectrum, and you will see this in multiple articles on this masterlist.
Many of these articles come from did-research.org. If anyone has any other articles or papers for any of the following topics, please either dm me or send an ask. Do not reblog/comment with the article/paper.
**Some links may contain mentions of cult abuse and/or ritual abuse. This will be mostly in the polyfragmented area of this masterlist.
An overview of dissociative disorders
Resources for dissociative disorders
Expert questions and answers (the switching one in this is not very accurate, I touched on it more in the DID portion of this masterlist)
What causes dissociation (focuses more on DID but still important. please note that it's very long and wordy.)
6 DID myths (another long and wordy one. touches on the following: the belief that DID is a “fad”, the belief that DID is primarily diagnosed in North America by DID experts who overdiagnose the disorder, the belief that DID is rare, the belief that DID is an iatrogenic disorder rather than a trauma-based disorder, the belief that DID is the same entity as borderline personality disorder, and the belief that DID treatment is harmful to patients. Iatrogenic, in this instance, means "induced in a patient by the treatment or comments of a physician" according to the National Institutes of Health)
7 DID myths (easier to read, and covers different topics. Confirms there is not a limit to how many alters a system can have.)
Even more DID myths (NOTE. This article will say that different alters can have their own mental health issues. Please refer to "Can alters have different disorders than the body?" in the Dissociative Identity Disorder section of this post.)
You can find the start of the DSM-5 information on dissociative disorders here, page 336
A quick overview of Dissociative Disorders (this one has OSDD and subtypes)
DISSOCIATIVE AMNESIA:
What it is + cases/examples
More information, explanations of treatment, and other important Q&A's
Other information (basically a summary of the above two, but might be a little easier to read)
Amnesia in Dissociative Amnesia
More types of Amnesia in Dissociative Amnesia
DEPERSONALIZATION-DEREALIZATION DISORDER:
Causes, Symptoms, and more
Living with the disorder, treatment, diagnosis, and more (the overview/symptoms and causes isn't entirely accurate, but still provides a baseline)
A more compact version of the above two (but less in-depth)
An easier to read version of the above two (least in depth but covers the basics)
The most in depth (but also hardest to read and contains a lot of long words and sentences without a lot of breaks. tiny font too)
DISSOCIATIVE IDENTITY DISORDER:
Overview of DID
What causes DID? (scroll down to "Risk Factors")
What causes DID? (part 2)
The Theory of Structural Dissociation (the very long and complicated version)
The Theory of Structural Dissociation
Problems with the Theory of Structural Dissociation
What are alters?
Different types of alters (This one goes into detail not only about what alters are, but different types of them and how they help the body/mind. There is some misinformation sprinkled within, so don't take anything as a total fact until you do further research.)
Different types of alters (this one is easier to read and created by a system who is/was in therapy. I am uncertain if the system is diagnosed, but the basic alters and basic functions match up with many diagnosed DID systems.)
Notes on non-human alters (and why you can have entire systems of just non-human alters)
Fictives (this was literally the only article i could find. please send me more.)
A paper that talks about DID and fictives (this one was sent to me and I was unable to read it due to personal reasons)
Is there a limit to how many alters a system can have? (A woman who was diagnosed with DID was reported to have 2,500 alters)
Is there a limit to how many alters a system can have? (A center in Utah who specializes in DID confirms as many as 4,500 alters have been reported)
Is there a limit to how many alters a system can have? (Researchers are still unsure, but up to 4,500 have been reported. Scroll down to "multiple personalities")
Fragments (the most basic definition)
Fragments (scroll down to F)
Fragments
OSDD and UDD
An overview of the types of OSDD
OSDD Type 1 (You can find OSDD-1B and OSDD-1A in there)
OSDD Type 2 and OSDD Type 3 (there was barely any information on these two outside of wikipedia and other not-really-professional blogs that i had access to, but I tried my best)
OSDD Type 2 and OSDD Type 3
OSDD Type 2 and OSDD Type 3
OSDD Type 4 (this will take you to a page called "Trance Disorder". That is what it's called in the ICD-11) (Possession Trance Disorder is also similar, you can find that here)
P-DID/Partial DID
Splitting, is it always trauma based? (the short answer, no. Direct quote: Many individuals cannot split unless a split is strictly necessary for their protection, functioning, or ability to remain hidden as a system. That said, there are exceptions. Some individuals may become so used to using splitting as a coping mechanism that they may split easily in response to seemingly minor stressors. For example, if an individual finds going to the doctor triggering, an alter may split that exists only to attend medical appointments. In some cases, systems may be so destabilized that even trauma processing leads to the creation of new parts.)
Polyfragmented DID: the very very basics
Polyfragmented DID: notes from a diagnosed polyfragmented DID system
Polyfragmented DID (you can find it on the side bar)
More notes on polyfragmented DID from a system, unable to tell if the system is diagnosed or in therapy
Comorbid disorders
Can alters have different disorders than the body? (I couldn't find a link, but short answer, yes and no. Neurodevelopmental disorders are things that are shared by all headmates, since it's all the same brain. So things like autism, ADHD, conduct disorders, those all are implemented into the brain and therefore all alters will have them. For stuff like eating disorders however, one alter may struggle with an eating disorder while others might not. Different alters can also present different symptoms/severity of a disorder.)
This is a post about a system(?) talking about fusion and their experiences
Integration and Fusion (or in simpler terms, integration is the act of breaking down amnesia barriers and building communication. Fusion is the act of fully integrating two parts into one.)
Dormancy (I could not find a good/reliable link, but it's basically when an alter "goes to sleep" for a period of time. This period of time can be long or short, and can happen for a multitude of reasons.)
Final Fusion and Functional Multiplicity
Time loss, Co Fronting, and Co Consciousness
Switching (covers passive influence too)
Passive Influence defined
Basics types of amnesia, not necessarily system related
More types of amnesia
The three most common types of amnesia from the system community, not necessarily scientific
-Emotional amnesia: where you don’t remember any emotions that you were feeling during the memory.
-Greyouts: when you remember what happened but have no memories of it, as if someone told you about the event and you might be able to recall certain details, but you weren’t there.
-Blackouts: when you don’t remember anything about what happened, and you often don’t remember that you missed something.
Innerworlds
Subsystems
Apparently Normal Parts and Emotional Parts
Primary Structural Dissociation
Secondary Structural Dissociation
Tertiary Structural Dissociation
You can find more resources here
A helpline that can help you understand and manage PTSD, dissociative disorders, and trauma can be found at (410) 825-8888 according to the National Alliance on Mental Illness
Crisis Text Line is a Text and Online Chat service provides 24/7 free support to those struggling with various mental health issues, including DID. Online chat: crisistextline.org Text: 741741
NAMI offers a volunteer helpline staffed by knowledgeable professionals who can answer your questions and connect you with valuable resources within your area. Call: (800) 950-6264 Text: Text "Helpline" to 62640
Basically every hotline you could need
Once again, these resources and information are not to be used to self-dx yourself. That means do not read this information and immediately say "oh yea i have this disorder". This is meant to be a starting point to learn more about dissociative disorders. If you feel like you might have any, do more research on your own. And, if you can, see and talk to a professional about it. These articles can be wrong. I can be wrong. We accept articles/papers/studies on anything here to correct us. Our only request is that it is not a carrd or something along those lines. This information is a starting point, and is not final.
Another good post about the basics of DID (not dissociative disorders in general, just DID and subtypes) can be found here
#traumagenic did#did alter#did system#actually did#traumagenic system#did osdd#endos dni#anti endo#tw cult#tw cult mention#tw abuse#tw abuse mention#dissociative identity disorder#polyfrag did#polyfrag system#polyfragmented#osdd did#osdd#osdd 1b#osdd 1a#osdd type 1#osdd type 2#osdd type 3#osdd type 4#actually dissociative#dissociative amnesia#derealization#depersonalization#depersonalization derealization disorder#dpdr
51 notes
·
View notes
Text
Kind of a shot in the dark, but does anyone know of a medium-length post where someone rants about how the did-research.org site is not actually a good community resource for learning about DID and OSDD-1 in-depth with accuracy? I think it was made relatively recently. If you know the post I'm talking about, I'd be grateful for a link. I'm very curious as to what they had to say because when we initially read through the site there were some parts that felt questionable to us and I was wondering if that post had gone into detail about any of the parts that felt questionable to us. This is NOT a post to syscourse under, please do not syscourse here. I only tagged syscourse because the post was made in response to system discourse, I think.
10 notes
·
View notes
Text
so this poll has been up for a couple days now, and we are startled to learn that nearly 30% of responders believe that childhood trauma is not a requirement or prerequisite for developing complex dissociative disorders.
we’ve had multiple people either comment or send an ask to tell us studies have shown that cdds can form due to trauma after childhood. so far though, no one has been able to link a single article or source to back this claim.
we do believe childhood trauma is the catalyst that causes complex dissociative disorders to develop, and we’d like to provide some sources to demonstrate why we think this way.
did-research.org claims that complex dissociative disorders form from childhood trauma. on their website they link to other resources, and provide explanations and examples to demonstrate why childhood trauma is necessary for complex dissociative disorders to develop.
a visual understanding of how alters / parts are formed by trauma in did and osdd by the ctad clinic - we love this handy, easy-to-digest video! we actually used this video when explaining our disorder to some of our loved ones.
this post from @multiple-myselves includes citations for a plethora of academic articles (we believe 18 in total!) which attempt to disprove (but were unable to) that dissociative disorders do in fact form from childhood trauma. these studies point to trauma as a prerequisite for cdds.
this article by the american psychiatric association also demonstrates the link between dissociative disorders and repeated, overwhelming childhood trauma.
here’s a pdf of the haunted self, by onno van der hart, elliot r. s. nijenhuis, and kathy steele, a book which first explored structural dissociation as we know it and laid the groundwork for the tosd
this article from beauty after bruises puts a ton of misconceptions about did and other dissociative disorders to rest - including the misconception that dissociative disorders can form after childhood!
this systemic data review from 1990-2022 shows that, while the cutoff age is somewhat contested, there is overwhelming evidence that dissociative disorders form as a response to childhood trauma.
are dissociative disorders under researched? without a doubt. does that mean we should cast aside or refuse to acknowledge the research that does exist? absolutely not! hopefully these sources can help others learn more about dissociative disorders, and understand how childhood trauma plays a key role in their development.
there are tons more resources out there on how dissociative disorders work, and why childhood trauma is a requirement for cdds to form. please take some time to educate yourself, and feel free to ask questions or start a discussion!
#syscourse#complex dissociative disorder#osdd did#did osdd#dissociative identity disorder#pluralgang#plurality#multiplicity#trauma#childhood trauma
104 notes
·
View notes