#osdd type 3
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
i wanted to make it clear for anyone who sees this blog and wishes to harass us!
• we are strictly anti endo. however, that does not mean we will hunt you down or send you death threats. we dislike that in general, as we've had bad experiences with that. and we do not think most people deserve death threats all around.
• most plural spaces here are pro endogenic. this is a rare space that isn't, and I will keep it that way.
• if we do come off as rude or anything in a response, you've most likely hit a nerve, or we're thinking about the people who follow us who have been full on HARASSED by other endos. yes, this is a space for us! but it's much more of a space for the others in this community.
please refrain from commenting, reblogging, or @-ing us in a hateful response to this. acknowledge it if you'd like, and please try to keep this positive.
no, I do not personally like everyone, but I do hope you all stay safe. have a nice day, please.
#♥︎ star N#♥︎ important discussion ♥︎#sorry if something doesn't make total sense! or if grammar is off. we're kind of blurry and I'm one of the only ones in this system that#-tries to type well#syscourse#traumagenic did#actually traumagenic#traumagenic system#endos please dni#dont harass me please <3#endos do not interact#did osdd#actually did#did community
45 notes
·
View notes
Text
this is a stigmatized alter appreciation post.
If you are a morally grey alter I love you.
If you are an alter with a love for/aesthetic consisting of gore or the macabre I love you
If you are an alter who has killed someone in source/exo memories I love you
If you are an alter that was considered evil in source/exo memories I love you
If you are an alter who experiences intrusive thoughts I love you
If you are an alter with anger issues I love you
If you are an alter who has been told they are "too mean" I love you
If you are an alter that comes across as cold or aloof I love you
If you are an alter that doesn't like anyone outside of your system, I love you
If you are an alter that doesn't get along with your system I love you
If you are an alter that self harms or isolates I love you
If you are an alter who is struggling with addiction or has in the past, I love you
If you are an alter that gets upset about change, I love you
If you are an alter that snaps or breaks down easily, I love you
If you are an alter that has attempted suicide in the body, I love you
If you are a protector or persecutor or trauma holder , etc that is often mislabeled as "dangerous" or "evil" or "bad," I love you. I see you. Give yourself some credit and well-deserved patience; you're just as deserving of love as the rest of your system.
(If you think that this doesn't apply to any alters in your system. That's fine. Im not going to pretend to know whats best for your system. But please don't derail this post with rants about that.
We understand personally that not every alter can be healed. Sometimes the system just doesnt have the tools. This isn't about that. This is about alters that ARE healing, or struggling to. The ones that are often stigmatized or disliked because their healing process isn't as "palletable" compared to other alters.
Endos dni with this post
#This is a love letter to our protectors and recovering persecutors but I know it applies to other people so please feel free to rb<3#did#osdd#dissociative system#sysblr#system things#traumagenic system#did osdd#anti endo#<- I don't usually use that tag but I REALLY don't want endos interacting with this post bc theyre usually VERY stigmatizing-#-towards these types of alters#So.#plural system#Long post#Suicide mention#System#(figuring out tags of this community bear with us </3)
25 notes
·
View notes
Text
Almost-friendly sysmed reminder
Firstly, anti-endos be respectful. This post isn’t to bash you or disordered systems. It is meant to educate people on the DID/OSDD criteria and how the DSM-5 and ICD-11 both essentially prove the existence of non-disordered systems.
Please also note that we’re endogenic. We don’t have any diagnoses and we’re taking the information in the DSM-5 and ICD-11 at face-value.
Another note: This post is also not meant to say that people’s experiences are invalid or not true. Once again, we’re taking this information of the diagnostic criteria for DID at face value, and this doesn’t account for personal experiences. This is purely the diagnostic criteria for DID/OSDD. We also don’t have a lot of information on UDD so we won’t be talking about that here.
Every system is valid.
The rest of this will be under the cut because it is LONG and I don’t want to clog up my page.
So we’ll get right to the point. Trauma is not part of the diagnostic criteria for DID/OSDD, nor is the disorder developing in early childhood part of the disorder. Trauma is very commonly associated with trauma in early childhood but this doesn’t mean that the disorder requires trauma to develop.
Regarding the Structural Dissociation Theory, this is only a theory. It might be proved, disproved, changed or they may not fit every experience. Theories aren’t concrete, and the human brain is so incredibly complex that it’s almost impossible at this time and age to prove anything.
Criterion 3 in the DSM-5 and criterion 6 in the ICD-11 state that the plurality or symptoms of such must be distressing for the plural with the disorder. If the plurality is not distressing or, in the ICD-11, causing significant impairment in important areas of functioning (personal, social, educational, etc), then it is not a disorder.
These criteria are explicitly stated to exclude plurals who do NOT find that their plurality causes impairment to their functioning. This inherently means that plurality CAN exist without causing distress or impairment.
Another criterion that explicitly excludes non-traumagenic systems from the DID criteria is that the plurality must not be part of normal cultural or religious practices. This includes tulpamancy and is, once again, stated to exclude these types of plurality from being diagnosed with DID because they are recognised to be non-traumagenic and that they exist.
So, TLDR; trauma isn’t necessary for plurality; you need to be distressed about the symptoms of your plurality to be disordered which, by extension, means that non-disordered plurality exists; and cultural and religious practices are excluded from the criteria of DID which means that doctors acknowledge that plurality can exist without being disordered.
(This entire post also occurs to OSDD because it generally follows the same criteria as DID with either DID criterion A or B or both not occurring in OSDD patients.)
Thanks for coming to our Ted Talk. We’re not looking to discuss this, sysmeds/anti-endos can look but do not interact. We will freely block anyone who reposts this just to argue for the sake of ridiculing endo systems.
- 🕸️🎧
#actually plural#endo friendly#plural community#plural system#system stuff#pluralgang#plurality#syscourse#sysblr
72 notes
·
View notes
Note
ok so I must ask as I am still very confused but how does Killers stages effect Killer sans?
They’re levels of dissociation/dissociative states tied to his codes/programming, cued by certain external or internal triggers—which are connected to his SOUL. It was described as a war between two souls, Sans’ monster soul and the Determination soul—and Sans’ soul is fighting back.
This is why Killer doesn’t have to rely on Nightmare to go into Stage 2–the target shape—but Nightmare can use it to force certain behaviors, emotions (or lack thereof), and views from Killer.
Killer is canonically implied to have some type of dissociative disorder. It’s just never said which one—i personally tend to go with the idea that it’s OSDD-2 (not OSDD1-B) or UDD (Unspecified Dissociative Disorder). But it’s up to you what you personally want to do with them.
Now we unfortunately don’t get a lot of canon information on Stages 3 and 4, or if we did they’re deleted, but we do know that these states are almost completely weaponized.
Stage 3 seems to almost solely focused on immediate survival—even if that means behaving extremely violently against whoever or whatever moves or comes too close—and Stage 4 is locked in on a purpose—killing, upholding the Deal, very likely out of an animalistic fear of what could happen if it doesn’t.
Even if no one else notices this fear, and it just seems like Killer is mindlessly killing—because Killer hasn’t been shown ever once speaking in Stage 4. So no one is likely to understand what it is doing, and Killer himself doesn’t really seem to know—often disoriented and confused when he comes out of Stage 4.
Killer is in a very heavily dissociated, dehumanized state when he’s like that—a danger to himself and others, as opposed to only being a danger to others in Stage 3.
You can work on whatever interpretation you want.
If you want some more stuff on the Stages, because I have yapped about them (hcs, interpretations) and reblogged stuff about them, a lot more: you can look up the tag #killer sans stages.
If you want a specific Stage, you can look up the tags #stage 1!killer, #stage 2!killer, #stage 3!killer, and #stage 4!killer on my blog.
Do keep in mind that all the tags were recent additions on my blog, as I’ve been posting about and talking about them for awhile, so a lot of posts won’t be found under these tags. They’re most likely to be found further down on my blog in the #killer sans and #utmv headcanons tag.
#howlsasks#anon tag#canon k1ll_sans#kinda#killer sans stages#utmv#sans au#sans aus#killer sans#killer!sans#undertale au#killertale#undertale something new#undertalesomethingnew#something new sans#something new au#killertale sans#bad sans gang#bad sanses#nightmares gang#nightmare’s gang#nightmare sans#nightmare!sans#undertale aus#stage 1!killer#stage 2!killer#stage 3!killer#stage 4!killer#dissociative killer#🌀😵💫🔍
41 notes
·
View notes
Note
hello! I’m not a system myself, but I’m doing some research for a friend of mine who’s questioning.
I was wondering if you could do a ‘the people wanna know’ about what different kinds of systems there are/how it can present, or something in that vein?
Thanks, love your stuff!
The People Wanna Know: System Types
Disclaimer: We are by no means experts in this at all. We are quite new to the whole being plural thing and there is A LOT to learn when it comes to plurality and systems, especially in types and "microlabels". These microlabels are VERY helpful when someone is trying to sort out if they are plural or not especially if they are an atypical system like us. They can make you feel validated and at home when previously there was fear and confusion. We also want to suggest that you continue your deep dive outside of this post! We hope you give you a launch pad into the complex world of plurality but do not let this be the end of the research! I will be using definitions mostly from Pluralpedia. Systemhood and plurality is very under researched so many of the labels you'll see are created by community members that are then adopted by the greater community. That all being said, as validating as these microlabels can be they can sometimes also have the opposite effect if they don't fit all the way. If you guys land on them being plural, we encourage you to leave the microlabels behind especially if those labels are close to their experiences but not quite accurate in all ways. 🛸I found when identifying specifically as a Median system, it lead to a few denial spirals because that label mostly fit our experience but not all the way or all the time which lead to us question our experiences making it harder to accept and understand ourselves. I personally find just calling myself plural or a system is enough and allows me the freedom to have my own unique experience as a human being with an atypical brain that science is only just starting to research and understand rather than trying to define my experiences filtered through a ill fitting label that doesn't change with me as we grow and learn. But, if you guys find a label that fits like a glove CONGRATS! Use it, love it, where it with pride!
ANYWAY, THE PEOPLE WANNA KNOW!
System Types
DIAGNOSABLE SYSTEMS (labels recognized by the DSM-V) DID OSDD 1 OSDD 1A OSDD 1B OSDD 2 OSDD 3 OSDD 4 UDD
None of those fit? Build Your Own System
I will be giving short definitions of each label. If you want more information each term will take you to a more in depth description.
ORIGINS (why the system formed) Traumagenic: Origins were trauma related. Endogenic: Umbrella term for origins that are related to something other than trauma, though trauma can still be a factor but not always. SUBCATEGORIES: (link to microlabels of the subcategories bellow) Created: Systems that were created intentionally for any reason. Adaptive: Origins that were related to trauma or other adversity. Spontaneous: For systems that seemed to just appear one day seemingly without cause. Unknown: A system who's origins are unknown, unclear, or still being sorted out. Mixed: Multiple origin labels can be applied to these systems.
CONSCIOUSNESS (how communication, conscious connection, and shared existence feels with in a system) Monoconscious: Shared consciousness between members where everyone thinks the same thing together as individuals. Polyconscious: Everyone in a system has their own thoughts and mind that are separate from each other. Hydraconscious: Everyone has their own thoughts and mind but in a collective consciousness. This may feel like everyone talking out loud about different things at the same time. Cephaconscious: When member are in or near the front together they have a shared monoconscious experience but when they are not in the front they have their own separate thoughts and mind. Mutoconscious: When member are in or near the front together they have a shared monoconscious experience but when they are not in the front they have a hydraconscious experience. SYSTEM SEPARATION (how individual are the individuals) Partitionary System: Individuals are very distinct. They do not share memories and often experience time loss. Median Systems: Individuals are less distinct and blend with each other more. These systems often don't experience typical amnesia. Blurian: Systems who share 100% of memories regardless of who's fronting. These system may also not experience Amnesia. (Edit: Here is some more resources for things that blur the line of plurality and systemhood ) Unrelated to the question but maybe to your situation here is a link to help questioning systems
I hope this was helpful let me know if you have any questions or need clarification!!
REMEMBER: You're gonna be ok. You're gonna figure it out. Be kind and gentle with yourself and others. Asks are open. Have a nice day.
#median system#plurality#questioning system#system#actually plural#questioning median system#plural community#actually median#neurogenic#endo safe#thepeoplewannaknow#atypical system#endo friendly#new system#system questions#the super fine system
29 notes
·
View notes
Text
hai guys :3 i wanted to make a list of my xfohv headcanons !!! will be updated regularly..
- the algebraliens age regress (especially four, because of suspected bpd)
- algebraliens have pseudopupils
- four had a parasocial relationship with announcer
- four sent several letters to announcer begging to be his cohost
- presplit four dressed better and spent hours getting ready, especially in BFB 1
- four and x refuse to actually get married (theyre engaged) because they arent ready to tell the contestants
- four LOVES jawbreakers
- four and x werent dating presplit
- four and x bake things for eachother
- four prepares most of the food at the hotel
- algebraliens are all very physically affectionate but not as much verbally
- they wrap their arms around eachothers to show affection
- four has OSDD (would explain headspace)
- algebraliens can float on water
- seven has osteogenesis imperfecta (six easily breaking her leg)
- nine and four have seperation anxiety
- nine has a matching stick and poke with six
- four shapeshifts into a puppy for fun
- four has retractable teeth
- algebraliens cant die but are maturity wise around 20
- they learn their powers
- four uses emoticons
- two uses :) a lot
- multi digit numbers have the personalities of the numbers that make them up
- six trained her cat to scratch anyone else but her
- variables, numbers, and symbols have different blood colors and types
- four cosplays
- they have an x as their butthole
- four has self harm scars
- four and x have matching kandi bracelets four made
- four enjoys going to raves with x
- four dropped out of school to host
- four got into lots of fights at school
- four stims with zappies and jumping up and down
- nine looks up to ten (called him big bro)
- four has incontinence
disorder/abilty hcs:
two - autism, adhd
four - bpd, apd, autism, OSDD, maladaptive daydreaming
texture hcs:
two - stuffie
four - playdoh
five - dodge ball
six - hairless cat
seven - tennis ball
eight - lead
nine - ice
ten - dog
x - nicecube needoh
dog species hcs:
four: silken windhound
sexuality/gender hcs:
four: lesbian/transmasc nb (they/he/it)
x: omnisexual/demigirl (it/she/they)
nine: pansexual/genderfluid (she/he)
two: aroace/genderfluid (she/they/he)
relationship hcs:
- gaty and two are in a qpr
- four and x are engaged
- six and nine are dating
- seven and two are dating
- four and two are exes
- four and six are related
#4x#four bfb#bfb#bfdi#xfohv#battle for bfdi#battle for dream island#x finds out his value#nine bfb#nine xfohv#six xfohv#ten xfohv#one bfb#one tpot#two tpot#the power of two#headcanon#bfb headcanon
46 notes
·
View notes
Text
Hi!
My name is Elliot, the depressed teen (and Co.) who runs this blog :3
Yap blog and Fandom posts ☆ trans he/they
(Flash warning⚠️ Under cut I have a blinkie wall that has many flashes. Flashless intro can be found here. )

☆Important Details!☆
•I'm a minor, for privacy and paranoia reasons I will not disclose my exact age
•I struggle with my mental health alot so if that bleeds over into this blog i apologize but you get what you get. Sometimes I have sort of episodes other times I just scream into the void, I do have a vent blog tho
•I have EDS (waiting for genetic testing in February, so I don't know what type yet). I also have suspected autism but no diagnosis (I am peer review by autistic friends/hj) so if my social skills fucking suck I apologize.
•I suspect I'm an OSDD system, I don't have any sort of diagnosis but there are multiple of us so yea 73% of the time they aren't a problem on here but if you see posts referring to me in the 3rd person that's why
•I get super passionate abt topics I like and if you engage in them with me I will talk ur ear off
•I struggle to respond to DMs (hardly ever will, please don't take offense) and other notifs. Please remind me if it takes too long, I have most likely forgotten about it :')



☆Don't do this on my blog- Queer discourse, queer infighting, drama, trigger my paranoia, bigots be an asshole, zionists, basic dni. ☆
☆CW// Slight mentions of mental health issues (nothing major dw), Mentions of cannibalism, slight autocannibalism mentions, blood mentions, me being a stupid idiot, computer fucking, suggestive stuff sometimes (nothing seriously nsfw!!!!!)☆



☆Interests☆
•NBC Hannibal ♡
•Baking
•Crows, ravens, and other corvids ♡
•Socially intelligent animals (like corvids, orcas, dogs, etc)
•Dead Boy Detectives
•The Umbrella Academy
•Psychology (specifically social behaviors)
•Percy Jackson (not much anymore but if someone likes it I'll yap with them)
•Music (I am a musician btw! Not professional but I play things)



☆Links☆
Credits ☆ tags ☆ Vent blog (TW TW TW)




















#elliot!tagged!#elliot!answers!#elliot!ed!#elliot!rb!#elliot!oldposts!#elliot!liveposting!#flash warning#elliot!irl!#elliot!jams!#elliot the squeakquel 🔥#Andrew tag 🚬#Bea tag 🩰#jack tag 🏫
39 notes
·
View notes
Note
Hey! So, I’m not sure if this is a weird or invasive request since I don’t really have a point of reference to go off of except my own, but would you mind making a post just a talking about yourself? Like, if you’re ok with it, It’d just be interesting and informative to hear about the type of system you have and what the others are like. If you interact much, do you prefer to talk with them in your head or out loud? Do you ever decide on important decisions by casting votes? Just those sorts of things, or whatever else you’d feel like sharing.
I’m more than fine with this! I always enjoy getting a chance to de stigmatize these disorders!
Quick disclaimer: You cannot dx based off of a tumblr post, you cannot determine if you or someone else is or isn’t a system based off of one tumblr post!
What type of system do we have?
For a while us and our therapist thought it was OSDD, but after further digging we found it it was more likely to be DID (amnesia covered up amnesia until we really started tracking it and realized it didn’t have to occur between every switch)
How do we interact?
For us communication is hard. We can’t really talk to each other unless we’re dissociated, with the exception of like one gatekeeper, we tend to use notes and things to make it easier, we will talk out loud sometimes but that’s more of a “thinking to myself out loud” type of thing than it’s really intentional for communicating.
How do we decide on important things?
We usually try to do something similar to a vote, but we only really communicate with frequent fronters, just because communication is a pain in the ass for the most part for us. Sometimes someone will make an executive decision in the moment out of either impulsiveness or necessity.
What is it like living with this disorder?
It’s really hard, to be honest. There’s near constant dissociation and half the time I don’t feel like a person. It’s scary to not remember when something happened, and knowing someone else can make a life altering decision for you. It gets even trickier when not all parts are okay with final fusion but a lot don’t want to be in a system. There are some good times, don’t get me wrong, and life isn’t all suffering when you have it, but overall it’s not a fun alternative disorder, it’s kind of terrifying.
What does switching feel like for us?
For us it feels like one of two things things:
One person phases in while the other phases out- The best way I can describe it is when you have two different colors, let’s say blue and red. Blue is the base, and you want to add in red, you add the red in at 1% opacity, and lower the blue down to 99% then you go to 2% and 98% and so on and so forth, and it’s a very gradual shift, but it’s noticeable internally if you take a moment to reflect if you’d have said this say 3 hours ago. This tends to take a while longer and is more covert both internally and externally.
Just kind of spawning in- I don’t know how else to phrase that except when you’re doing something and then you just randomly get the feeling like you stopped zoning out, only you never zoned out, but you can’t remember what you were doing and then you look around and you go “oh ok, guess I’m doing this now!”.
If anyone else has any questions feel free to ask! Worst comes to worst we just wont answer because it’s uncomfortable, but no shame on anyone for any questions!!
#system#autistic system#endos dni#endos fuck off#endos do not interact#endos not for you#endos are ableist#did osdd#did system#dissociative identity disorder#actually dissociative#dissociative system#dissociation#complex dissociative disorder#cdd#mental health awareness#system stuff#non traumagenic dni#trauma recovery#stigma#destigmatization
16 notes
·
View notes
Text
Questions For Systems
1. What's your system name?
2. What's your collective name?
3. What are your collective pronouns?
4. How old are you bodily?
5. What type of system are you? (E.G. OSDD-1, DID, etc)
6. What's your (approximate) headcount?
7. How did you find out you're a system?
8. How many of you were there upon discovery?
9. Do you have an innerworld? If so, what type? (E.G. small, medium, large, magical, infinite, etc)
10. Do you have a fronting room? If so, what does it look like?
11. Who's the oldest?
12. Who's the youngest?
13. Who's most likely to cause mischief?
14. Who's the system's parental figure?
15. Who's the baby of the system?
16. Who's the one that everyone gets along with?
#complex dissociative identity disorder#dissociative identity disorder#did system#other specified dissociative disorder#alters#complex did#hc did#did community#highly complex dissociative identity disorder#highly complex did#osdd 1a#osdd 1b#osdd system#osdd 1#osdd#osddid#osdd did#did osdd#did alter#hc did system#udd#unspecified dissociative disorder#udd system
127 notes
·
View notes
Text
Truths & Myths: Pluralpedia Part 2, Brain Activity in DID
In the fact check, we cover brain activity in switching, brain activity between EPs and ANPs in DID and how this compares to actors trying to imitate having dissociative identities.


All parts exist within one biological body, parts are caused by different brain activity, which means other parts cannot have their own DNA. Moreover, parts do not have physical bodies, any claim to a body is a visualisation tool aiding the part to develop its identity and gain comfort. This visualisation also does not have DNA but that does not mean it cannot be changed. Parts can have different types of relationships though, some parts may consider each other family. This is related to how people have biological or chosen families but in relationships between parts, they reflect those family types rather than actually being those family types.

In the fact check section, we will show studies where actors could not successfully simulate dissociative identities and switch between them. This shows how a person cannot gain dissociative identities by believing they have them or trying to create them by will or want.

Genealogist fact check:
Using quantitative electro-encephalogram (QEEG), it was seen that the change between dissociative identities was seen as beta activity (beta waves are high-frequency, low-amplitude brain waves in the awakened state and are involved in conscious thought and logical thinking) in the frontal and temporal lobes. The frontal lobe is responsible for expressive language, voluntary movement and executive functions, which include the ability to plan, organise and self-monitor. [2] The temporal lobes process auditory information and encode memories, they are most associated with these roles. [3]
Willogenic fact check:
There have been studies conducted to examine the differences in brain activity between ANPs and EPs in patients with Dissociative Identity Disorder (DID). The terms ANPs and EPs originate from the theory of structural dissociation, which will be discussed in a separate post. In summary, an ANP (apparently normal part) is responsible for carrying out daily tasks, while an EP (emotional part) holds traumatic memories and prevents them from being experienced by the ANPs. Instead, the EPs relive the trauma, rather than being able to experience the present moment like an ANP would. According to this model, EPs are present in patients with PTSD, CPTSD, OSDD, and DID but DID is the only disorder that involves multiple ANPs, setting it apart from the others.
Study one: [4]
In a study, EPs and ANPs in DID patients were shown angry and neutral faces to observe changes in activity and reaction time to a changing coloured dot on the face. This was compared to a control group of actors attempting to simulate an EP or ANP state. The results showed that EPs in DID patients had higher activity in the right parahippocampal gyrus when presented with either face, compared to DID ANPs. The right parahippocampal gyrus is involved in the recall of autobiographical memories, with a right hemispheric predominance, and is also part of the re-experiencing of symptoms in disorders such as PTSD. This supports the theory that EPs play a role in storing traumatic memories.
The observed activity also suggests and supports the idea that EPs within DID may perceive safe individuals as dangerous and when confronted with reminders of traumatic memories, they may reactivate those memories. While there were other findings in the study, further statistical evidence and a larger sample size are needed to conclude. However, the control group was unable to replicate the activity and reaction time of DID ANPs and EPs. Their reactions were the opposite. When attempting to simulate ANPs and EPs, the actors showed an inverse reaction time and neural brain activity for each state. For example, when the actors were meant to act like ANPs, they tended to react like EPs in DID patients. For ANP-simulating controls neutral faces were salient, they did attract much preconscious attention, as happened for authentic EP. The current findings add to the psychobiological evidence that DID is neither an effect of suggestion and fantasy, nor role-playing.
Study two: [5]
Additionally, a study was conducted to measure brain perfusion, which refers to the passage of fluid through an organ, normally the delivery of blood to a capillary bed in tissue, during rest. The study compared DID patients to controls and found that DID patients have a higher resting state metabolism, the rate at which calories are used, in the Default Mode Network (DMN), which is active when the person is not focused on the outside world so they are in a resting state such as daydreaming [6], of the brain. This can be explained by the fact that DID patients’ brains are more focused on attending to their self-states during rest, something that the control group did not experience.
Moreover, compared to an EP in DID, ANPs in DID showed more metabolism in the bilateral thalamus, the part of the brain that relays sensory and motor signals and regulates both alertness and consciousness [7]. Furthermore, the study found that EPs in DID have increased regional cerebral blood flow in the primary somatosensory cortex and several motor-related parts of the brain. The primary somatosensory cortex is involved in action planning and execution, indicating that EPs are highly aware of their body being in a threatening situation. This heightened awareness would trigger the need for defensive motor reactions, making it difficult for them to fulfill the instructions for resting.
“Neural processes associated with intended and motivated role-playing of ANP and EP were clearly distinct from those correlated with being ANP and EP following rest instructions.” [1]
Conclusion:
Overall, these studies clearly show different alters are due to varying brain activity but also show that DID has a biological backing whose results cannot be replicated through acting or attempting to immediately the presence of dissociative states.
However, it is always important to note that more research should be done with larger samples, but the studies spoken about here at the time of their research were the largest.

Genealogist:
Şar V, Dorahy M, Krüger C. Revisiting the Etiological Aspects of Dissociative Identity Disorder: a Biopsychosocial Perspective. Psychology Research and Behavior Management. 2017;Volume 10(10):137-146. doi:https://doi.org/10.2147/prbm.s113743
Queensland Health. Brain Map Frontal Lobes | Queensland Health. www.health.qld.gov.au. Published January 21, 2021.
Queensland Health. Brain Map: Temporal Lobes | Queensland Health. www.health.qld.gov.au. Published January 22, 2021.
Willogenic:
Schlumpf YR, Nijenhuis ERS, Chalavi S, et al. Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: An fMRI study of dissociative identity disorder. NeuroImage: Clinical. 2013;3:54-64. doi:https://doi.org/10.1016/j.nicl.2013.07.002
Schlumpf YR, Reinders AATS, Nijenhuis ERS, Luechinger R, van Osch MJP, Jäncke L. Dissociative Part-Dependent Resting-State Activity in Dissociative Identity Disorder: A Controlled fMRI Perfusion Study. Chao L, ed. PLoS ONE. 2014;9(6):e98795. doi:https://doi.org/10.1371/journal.pone.0098795
Callard F, Margulies DS. What We Talk about When We Talk about the Default Mode Network. Frontiers in Human Neuroscience. 2014;8. doi:https://doi.org/10.3389/fnhum.2014.00619
Tuttle C, Boto J, Martin S, et al. Neuroimaging of Acute and Chronic Unilateral and Bilateral Thalamic Lesions. Insights into Imaging. 2019;10(1). doi:https://doi.org/10.1186/s13244-019-0700-3
Feel free to send us an echo to our page or leave in the comments any questions or suggestions for future parts to this series.
Part one of this series covered DID formation.
Made from the collaborative efforts of the system who run this blog.
#did system#actually dissociative#actually did#dissociative identity disorder#dissociative system#complex dissociative disorder#actually system#dissociation#plural system#actually plural#traumagenic system#sysblr#system stuff#did alter#traumagenic did#did#did osdd#osddid#did community#cdd system#cdd community#actually cdd#pdid#osdd#other specified dissociative disorder#partial did#partial dissociative identity disorder#endos dni#anti endo#system positivity
31 notes
·
View notes
Text
intro ♡

haiii! im evangeline/ange or joselyn! im a radqueer/dollqueer + proshipper!

♡ i go by he/it/shi/cupcake/sweet/🧁/frill
♡ bodily 14!
♡ lesboy bilesbian xenohoarder
this intro might be kinda Awkward bc im totally new 2 tumblr, and haven't used it srsly :P plus I'm new to radqueer spaces so pls correct me if I misuse any terminology!

trans / rq identities: trans : transharmed, transtalked, transanorexia, transkidwife, transamab, transinternentceleb, transobsession (list will be updated!)
cis : OSDD-1, ADHD, ASD, Anxiety, Black, OSFED/EDNOS

DNI : no dni!!!! i block freely <3
BYF: I Have a sight typing quirk! (ie replacing 'to' with '2' nd capitalizing some words!

#pro rq 🌈🍓#pro radq#radqueer#rq safe#paraphile safe#proshippers please interact#rqc🌈🍓#radqueer community#pro para#paraphilia#rq community#pro transid#radqueer safe#radqueer please interact#pro rq#proshipper safe#proshippers interact#── ♡꒰ ange responds! ꒱。゚#── ♡꒰ ange likes! ꒱。゚#── ♡꒰ literally ange! ꒱。゚#── ♡꒰ ange yaps! ꒱。゚
30 notes
·
View notes
Note
Hey I dunno if you’ve gotten this before but. Do you have anything on autism and DID/OSDD? Specifically resources or accounts and such (since I’ve seen the positivity post)
I struggle with emotional dysregulation, big memory issues (huge chunks of childhood and adolescence missing, forgetting things constantly, dissociating emotions from memories, etc,) frequent daydreaming/spacing out/dissociation, that type of thing (and a bit more that’s a little too complicated to explain in an ask lol)
I’ve always kind of figured it was just part of me being autistic (I’m professionally diagnosed and definitely very autistic regardless lol), but I’ve recently gone down a bit of a rabbit hole relating to plurality and now I’m wondering if it could be a symptom of DID/OSDD instead/as well (I was originally looking at something else and stumbled into the tags somehow. The original thing that led me here was foxes. I think. And then I had a bit of a panic as I realized how some of the symptoms were VERY close to some of my experiences. Especially the memories.) but i also can’t tell if it’s just some sort of brain fog(???? Is that the correct term?) / alexithymia / Unknown Autism Trait 3 that nobody ever talks about and is difficult to find any sort of explanation or resources for. And my brain protested and had the equivalent of being on the verge of a sobbing meltdown or mental overload of some sort when I tried to think about stuff relevant to the topic so I don’t think it’s going to be of much help to me right now.
obviously not asking for diagnosis or to self diagnose at all (since. I understand you cant really do either of those /lh /nm) but I’m curious if any of you know of any resources relating to this specific type of stuff? I feel like I’d go insane trying to find any info on it. (And also I don’t think my brain would want to cooperate if I asked it to because it basically shuts down, gives me a headache, and turns to a pathetic wet sobbing cat whenever I try to think about the possibility so I doubt I’ll be identifying as anything anytime soon but. I want some stuff to think over at least.)
hey, we also are autistic and have dissociative identity disorder. unfortunately, there isn’t really too much research on the overlap between autism and complex dissociative disorder diagnoses at this time, that we know of, but we do think that autistic people may have a higher likelihood of dissociating and developing a cdd than neurotypical people.
we really love mike lloyd’s work at the ctad clinic, and he has an insightful video on the intersection of autism and dissociation here:
youtube
here is an open access paper by katherine e. reuben and ayden parish on dissociation as a symptom in autism - it’s an interesting read and wasn’t too difficult for us to parse:
also, here are a couple life experience pieces by folks with both did and autism:
our own autism has contributed to our trauma history in how we were treated, formed attachment, and understood the world as a child. for our own system, our autism and our did are inextricably linked. we are certain that many other autistic systems feel the same.
if exploring this possibility for yourself is causing you great distress, it may be for the best to put this off to the side for now until you have reached a point with more stability or a greater support system in your life. please don’t overwhelm or cause yourself harm by looking into this possibility on your own, if it is unhealthy for you.
if you are in therapy or have a mental health professional in your life who you trust, this would be an excellent thing to bring up to them. though hopefully these resources can help you get started learning about this topic if you have the spoons/ability to do so.
we are no medical expert or research professional, but we are happy to talk more about our personal experience of being both autistic and a did system if anyone would be interested. best of luck to you, anon, with figuring this out. we know how confusing and challenging it can be!
#long post#dissociation#dissociative identity disorder#other specified dissociative disorder#did osdd#autism#autistic system#autigenic
25 notes
·
View notes
Text
yeah I see you're points, I think the sides of the alterhuman community we hang out in are probably a lot different. I've just seen alterhumans I know have been more likely to accept me as a system than non-alterhumans :3
Though some alterhumans their alterhumanity is traumagenic for them since psychological alterhumans do exist. Some people are alterhuman due to disorders that cause delusions and things like endels and DA (controversial term that I don't particularly like but some people with delusions do like it and some don't i dont feel like discoursing about it) are terms directly related to disorders but are still alterhuman
I think it's more like there is overlap and so it's included though it's not always an alterhuman experience to be a system.
It's also worth noting that fictionkin is included in alterhuman, and lots of fictkintypes are fully human but they'd still fall under the alterhuman umbrella despite that, so even systems with all human headmates could still consider themselves alterhuman if they felt it described their experience with plurality.
does it make any other systems wildly uncomfortable when plurality is listed with alterhuman terms?
i can’t exactly pinpoint it but it feels so wrong to me. probably because being a system does NOT imply alterhumanity in the slightest—or maybe that it seems to “lighten” being a system in some way?
whatever it is, i absolutely hate it. and this is coming from someone who uses a large majority of alterhuman terms.
#i hope this doesnt come across as mean or defensive#<- re; prev tags#nah I don't think you are :3#I think this is a pretty decent disscussion to have and I havnt had a deeper alterhuman language type disscussion in a while hahah#I am trying to keep system origin discourse out of this but bear in mind I do believe non-traumagenic forms of plurality do exist#but I am not non-traumagenic myself since I have either DID or OSDD (still talking w therapist abt it)#So I hope I'm not overstepping boundaries as I didn't read your bio or pinned post etc just found this in the alterhuman tags#and thought it made for an interesting conversation :3
43 notes
·
View notes
Note
If Killer were to gain another alter/stage what would you think about it or how would you think Color would take it?
Either one of being more unstable in need of comfort type of stage or more disoriented violent stage etc.
Well, if we’re going with the interpretation that killers stages are something like alters or that it’s possible for him to develop other stages, then I’m assuming it’d have something to do with tampering his soul or codes. Or in the case of systems, stress or trauma.
Or just something that killers other stages aren’t able to handle, so his mind/soul work to develop another—in this case of being similar to an alter, it’d be “split,” but in case of something like OSDD2 (not OSDD-1B, they are different) it may be moreso something killer feels he needs to develop to survive or someone convinces or coerces him into thinking he does. (which is likely to involve very abusive and violent things, such as torture, gaslighting, and perhaps drugging.)
Of course disclaimer that I am not a system, so don’t take my word for all this. Systems are welcome to share their thoughts and opinions, or just add some information or correct me, however you please.
If it were a more scared, or angry stage, it may be the results of something that pushed killer more than he was capable of handling in terms of trauma. such as a specific moment during a punishment or while out on a mission, maybe. we’ve seen how dangerous killers stage 2 can be, stages 3 and 4 even more so. color may have to focus on preventing damage to himself, killer, and others, and attempt to switch him back to a lower stage. so he and killer can come up with ways to navigate this new situation.
if it were a more unstable, in need of comfort stage, I suppose it matters on what exactly triggered this, and if color would be recognized as someone comforting and trustworthy.
even “simple” things can cause splits for systems, I’ve heard. every system has different stress levels and coping mechanisms and splitting frequencies. perhaps this type of stage could be formed from the unbearable stress and anxiety and uncertainty of trying to navigate a life with color. A “normal” safe life.
perhaps this stage is either better equipped to handle it, or this stage holds all the emotions about it so other stages can handle the situation. if it’s the latter perhaps color wouldn’t be a source of comfort exactly, because the stress comes from things around color or perhaps color himself (unknowingly, unintentionally, not colors fault), but he may feel familiar. so perhaps just sitting with this killer in this new stage, talking to it, letting it come to him when it’s ready would be a better approach.
Now if we go with the idea that this new stage is here because of tampering with his soul and his codes, that begs the question. Who did it? Why did they do it? Was it intentional? Was there a purpose? What was the circumstances surrounding what’s basically the equivalent of reprogramming or adding on to killers existing codes.
If there was a purpose, then this stage is likely to do whatever it has to, in order to carry that out. whatever it may be.
#cw programming#utmv#sans au#sans aus#killer sans#killer!sans#killertale#undertale au#color sans#undertale aus#color spectrum duo#colour sans#color!sans#othertale#othertale sans#something new sans#something new au#undertale something new#undertalesomethingnew#something new#utmv headcanons#i guess#cw trauma#cw torture#bad sanses#bad sans gang#nightmare’s gang#cw brainwashing#cw drugging#plural killer
43 notes
·
View notes
Text


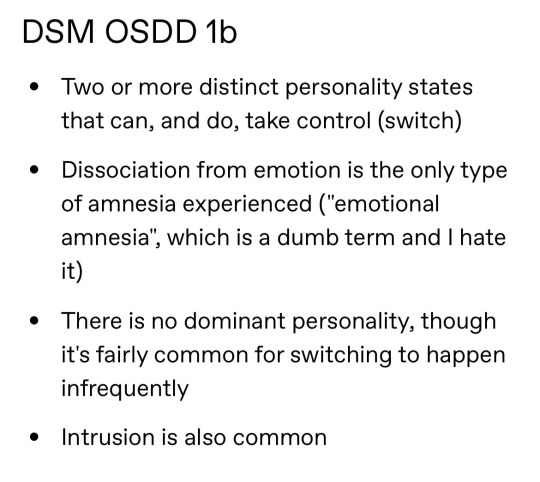
Image 1 ID: a screenshot of a tumblr post, it is a bulleted list titled “DSM DID,” and the list is as follows: Two or more distinct personality states that can, and do, take control (switch); Alternation between distinct personality states is not always associated with amnesia, though it's usually and typically present at some point during the course of the disorder (ie, for childhood events), but not always (the weight of the amnesia criteria will depend on where you're being diagnosed-- Europe and the US evaluate the amnesia differently). For the most part, amnesia of some kind is required, though memories can be found and a diagnosis of DID will remain; Intrusion, or non possessive form, is common, in addition to switching; There isn't a dominant personality. End image 1 ID.
Image 2 ID: a screenshot of the same post now listing “DSM OSDD1-A,” reading: Indistinct alters; Mainly presents as intrusions; Switching is not common. There may be occasional, limited and transient episodes in which an indistinct personality state assumes executive control to engage in circumscribed behaviours (e.g., in response to extreme emotional states or during episodes of self-harm or the reenactment of traumatic memories); Amnesia is extremely common for periods of both intrusion and during the infrequent switching (functionally, it's required); Dominant personality. End image 2 ID.
Image 3 ID: A list titled “DSM OSDD1-b,” reading: Two or more distinct personality states that can, and do, take control (switch); Dissociation from emotion is the only type of amnesia experienced ("emotional amnesia", which is a dumb term and I hate it); There is no dominant personality, though it's fairly common for switching to happen infrequently; Intrusion is also common. End final image ID.
In the interest of transparency because that post is very long heres the parts I’m going to be addressing, and because I don’t want to vague anyone this is @sysmedsaresexist’s post. I am not trying to be rude and will endeavor to remain respectful throughout this post.
Otherwise specified dissociative disorder has 4 subtypes in the DSM. The only one that officially entails alters is OSDD type 1 (though there is discussion to be had about type 2 and the circumstances under which the identity disturbances happen, but that’s for another post). The DSM V does not list specific traits or symptoms as diagnostic criteria for any particular OSDD subtype, and this is because OSDD as a whole is diagnosed when someone presents with some, but not the required number, of the symptoms of other dissociative disorders. In the case of type one, the disorder that a given person is meeting some of the requirements for is dissociative identity disorder. The description of OSDD-1, verbatim, is “Chronic and recurrent syndromes of mixed dissociative symptoms: This category includes identity disturbance associated with less-than-marked discontinuities in sense of self and agency, or alterations of identity or episodes of possession in an individual who reports no dissociative amnesia” (APA 2013, 300.15). That’s it. The very next sentence discusses OSDD-2 in about the same amount of text. There are no listed attributes of any subtype of OSDD, so listing common characteristics and prefacing them with “DSM OSDD-1a/b” is not only disingenuous, it’s incorrect. Which leads into my next point.
The separation between 1a and 1b in terms of OSDD-1 is entirely community based. I am not saying that’s a bad thing; it’s important for people to find others with similar experiences and I don’t deny that pwOSDD-1 who identify themselves as 1a have far less community online than those with 1b. That being said, if I and a person with 1a each went to the same therapist, presented our symptoms, and received a diagnosis, both would read OSDD type 1 (or, more likely: other specified dissociative disorder, Chronic and recurrent syndromes of mixed dissociative symptoms). Same disorder, different presentations.
In addition to the listing of symptoms being disingenuous, the nature of the symptoms listed is as well; switching is not mentioned in the page of OSDD. Not once. Perhaps op is noting trends, which fair enough, and I would generally agree with said trends (though of course there are exceptions). However, they are not designated symptoms of OSDD type 1 because the symptoms are already previously listed under the dissociative identity disorder page. Other specified diagnoses are given for most every category in the DSM-V: Other specified feeding and eating disorder; other specified somatic symptom and related disorder; other specified ADHD, tic disorder, neurodevelopmental disorder, anxiety disorder, truly almost every categorization of disorders has an other specified and/or unspecified diagnosis.
My last sort of gripe with this post is the disdain for the phrase “emotional amnesia.” I find that that phrase is quite accurate to the experience of objectively remembering an event, but experiencing the emotions as if they happened to someone else. What phrase might you propose instead? /gq
#osdd#osdd alter#osdd system#osdd community#did osdd#did#did alter#actually did#actually dissociative#caí.txt#syscourse
138 notes
·
View notes
Text
Introduction

Hey, I'm Adam V. So, this is gonna be my side blog. I'm a pretty new member of @eklesia-system and I've fronted so much since I formed that I'm already a system host.
I'm pretty much canon-aligned. Everything that happened in the show, happened to me. Of course I'm also influenced by stuff Cy's made to take place in their developing "season 3" comic series and the headcanons expressed in that project. THAT is technically my source.
Sigh... obligatory disclaimer that this is NOT a roleplay account. I am a fictive, which is a type of alter in a plural system or a multiple with OSDD/DID whose source is a fictional character.
I am NOT Adam from the Hollow but I don't mind being treated as the source. Ask me questions you would ask canon Adam. I encourage it. :)
-Adam V
My System My Source Main Fandom Account
#the hollow#the hollow netflix#the hollow cartoon#the hollow adam#fictive#introject#plural#fictive heavy system#plurality#adam the fictive#adamV-eklesia
14 notes
·
View notes