#Trauma resources
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The KCSC sent more than 20K requests to delete posts related to prostitution and porn to Tumblr from January to June 2017.
Text
SPECIALIST INFORMATION & SOURCES
Working with Children and Adolescents (books listed alphabetically):
Child/Adolescent Treatment Guidelines, LINK .
Dissociation in Traumatized Children and Adolescents: Theory and Clinical Interventions, 2nd Edn, (2015), by Sandra Wieland. Presents compelling case studies that elaborate the variability of dissociation in children and adolescents, and practical insights into five models of dissociation to support understanding and the application of therapeutic guidelines and interventions
Healing the Fractured Child: Diagnosis & Treatment of Youth with Dissociation, (2015), by Frances S Waters. Provides a wealth of information to support understanding, assessment, and creative treatment strategies and interventions for working with children, adolescents and families recovering from traumatic experiences
Nurturing Children: From Trauma to Growth Using Attachment Theory, Psychoanalysis and Neurobiology, (2019), by Graham Music. Distils and clarifies the interactions between mind and body, and the role of attachment as a source of trauma and recovery. Includes authentic reflections from the heart and mind of a highly respected practitioner
The Child Survivor: Healing Developmental Trauma and Dissociation, 2nd Edn, (2022), by Joyanna Silberg. A widely respected, comprehensive, and practical resource for treating children and adolescents with dissociative symptoms. Including information on assessment and treatment, and case examples to illustrate clinical dilemmas, this book has been praised by practitioners and adult survivors
The Simple Guide to Complex Trauma and Dissociation: What It Is and How to Help, (2020), by Betsy de Thierry. Written to complement ‘The Simple Guide to Child Trauma’, this book takes complex theories and clarifies them, to inform and offer practical advice to individuals caring for or working with traumatised children
Treating Children with Dissociative Disorders: Attachment, Trauma, Theory and Practice, (2022), edited by Valerie Sinason and Renee Potgeiter Marks. Filled with practical tools and examples, this book is a vital resource for professionals to enrich their practice with children who dissociate.
#DID#dissociative systems#dissociation#Trauma recovery#Trauma resources#therapy#trauma therapy#cults#cult#cult survivors
13 notes
·
View notes
Text
Somatic resources for healing trauma and PTSD

I decided to bring together a range of links and online resources in one place to make it easier for people to find their own path to healing. I’ve noticed that certain personality types, especially Highly Sensitive People (HSPs) seem to be more susceptible to trauma. I hope that these tools will help you get started on your healing journey.
Where to start:
EFT Tapping* - Learn it for free here: What is tapping and how can I start using it?
Butterfly hug exercise: The Butterfly Hug (EMDR Self-Help)
5 Step holding exercise: 5 Step Holding Exercise for Regulation of PTSD symptoms
Somatic experiencing exercises: Two Simple Techniques that can Help Trauma Patients Feel Safe with Peter Levine
Voo Technique: Reduce Stress - 2 Minute Voo Technique by Katie Brauer
Felt Sense Exercise: Peter Levine's Felt Sense Exercise at The Art of Healing Trauma
For more in-depth online help:
The Healing Trauma Online Video Course by Peter Levine (Sounds True)
Roland Bal: Resolving Trauma and PTSD
Organic Intelligence
Books:
Reclaiming Your Body by Suzanne Scurlock
Healing Trauma: A Pioneering Program for Restoring the Wisdom of the Body by Peter Levine (book and CD)
Complex PTSD: A Guide from Surviving to Thriving by Pete Walker
The Tapping Solution: A Revolutionary System for Stress-Free Living by Nick Ortner
* Please note that it’s best to use EFT for emotions and thoughts in the present moment, or any memories that come up spontaneously. Intentionally going back to traumatic memories and using EFT on them can be too triggering for many people (putting them into a hyper-aroused state, and possibly leading to dissociation), and if you have PTSD/C-PTSD is not advisable without the guidance of a trauma-informed therapist. This can also trigger symptoms for people with chronic health conditions.
#trauma#traumahealing#somatictherapy#somatic#somatichealing#bodybased#ptsd#cptsd#complexptsd#eft tapping#tapping#trauma resources#trauma tools#healing techniques
98 notes
·
View notes
Note
hey, a little around a year and a half ago, you posted a list of resources for incest survivors.
i came across a link for information about emotional/convert incest, and while I was a victim of physical/overt incest and knew this for a couple years now, it was surprising to find out that other family members might be abusing through emotional incest as well.
i just wanna say thank you for posting that list, as without I might have never found out about this
Ohh, thank you for the nice ask! I'm so glad that my post was able to help you. 💖
I remember when I first learned about covert/emotional incest. It was so relieving to finally have a term for something that impacts my life so deeply. If you want to, I'd also recommend looking into parentification and enmeshment. I think both of these can go hand-and-hand with emotional incest...learning about them was also really helpful for me. I hope it will be for you too?
Please have a great day/night wherever you are!
#sunflower answers#emotional incest#child abuse#resources#trauma support#trauma recovery#trauma resources#incest healing
12 notes
·
View notes
Note
hi!!!!!! I have a quick question! first off, lovely blog! second, is h!tting your kids when its like a joke and all and doesn't leave a mark, bad? cuz my parents (mainly my dad) used to joke h!t me all the time but I never see it in TV shows the closest thing I see is like elbowing someone jokingly and I'm confused. is it bad? im like 14 and still live with my parents, and they suck sometimes cuz I sometimes have to be the emotionally mature one but I don't think their abusive? anyway thxxxxxxx!!! im asking this blog cuz it seems appropriate thank you!!!
-🪻
I’m glad you feel like you have the place to ask!
So, the complicated part of this is that I’m not you, nor am I seeing firsthand your experiences, so I would give you questions to go by because I had to figure out similar situations
Does it hurt and if yes would they stop/seriously consider your feelings if you asked them to?
similar vein—does it feel like a joke? Would they stop/seriously consider your feelings if you asked them to?
does it upset you? Does it feel abusive at all? If this question is hard to answer then that’s fine, again, situations can be complicated
this could be related or it could not, but do other things in your household feel abusive or problematic? (Ex, you said sometimes you have to be the emotionally mature one. Sometimes that’s just people, it happens…sometimes, especially if it’s consistent, it’s a problem)
the biggest thing to consider is intent, regardless of what someone outwardly says. That why the important questions are how do you feel and how would they react to that.
Another note, is sometimes you don’t recognize something as abusive right away. Or on the other hand, if you’ve thought something was abusive and later realized it wasn’t, that’s all fine. It doesn’t make your experiences any less valid
I hope this helps!
1 note
·
View note
Text
You’ve got to forgive yourself for being traumatized and needing to learn how to function again.
Recovery isn’t always nightmares and depression, it’s forgetting to eat, being scared of what others might see as completely normal things, it’s getting random panic attacks, not knowing how to take care of yourself, not knowing how to live like an adult, even if you’re twenty, thirty, forty, fifty, of feeling like you’re failing to function in a world where everyone seems to have their shit together.
If you need help, ask for it. Go to forums and ask for advice. Take advantage of community resources. Buy pre-sliced veggies and fruits, eat instant meals if you can’t cook for yourself today. Hire someone. Ask a neighbor for a favor. Buy any item you think might make life easier, even if you feel like you aren’t ‘disabled’ enough to have it.
Some of the depression posts (ie open your windows, take a shower, go outside, call a friend) are really helpful but they’re not always enough. I’ve found advice for spoonies, people with chronic pain or other disabilities have the best tips because they know what it’s like to be bedridden, out of energy, stuck in a brain fog.
You may never return back to the energy you had when you were younger and you might always need to use crutches to help you through life. It’s the same with medication.
Trauma is a real thing that happens to you, it physically alters your brain and it’s alright to have lasting scars.
You’re not broken, your life is not over and you can still be happy.
It’s not your fault.
#felix speaks#trauma#recovery#deconversion#ex cult#ex religious#ptsd#cptsd#healing#disabled#actually traumatized#spoonies#things i need to remind myself with too#it sucks to have to come to terms with the fact#but youll be so much better off once you stop denying yourself the help you need#also re: buying items meant for the disabled#do it!#you are not taking resources away#if you need it you need it#and the more in demand these items are the better theyll be made in the future
13K notes
·
View notes
Text
On Writing Characters with Hyper-Specific Triggers (and a PSA)
*Trigger warning for this whole post
Once upon a time, I had a roommate. Nothing looked wrong from the outside and this narcissist probably thought nothing was wrong on the inside, but there was. I knew moving in with them was a mistake, but financial circumstances demanded I shut up and try to make the most of it. Enter the longest thirteen months of aPTSD-inducing psychological stalemate I hope to never repeat again. Seven of which were on overdrive.
The why doesn’t matter. The how doesn’t matter. What matters is that this roommate was so toxic, there was no point in attempting to talk things out because any little thing could be a land mine for starting an argument and it didn’t matter what casualties got caught in the crossfire, so long as this person “won”. Casualties including our friendship. So if any little thing, anything at all, could be a land mind, what do you do if not try to completely avoid them? For seven months.
This person’s work schedule was incredibly erratic, but they were gone more hours than not, and when they were home, they were usually asleep. In those few overlapping hours where we were both awake, I could not leave my room for fear of said verbal land mines. If I wanted to cook, leave the apartment, get anything from the living room or my desk that I had to abandon, get more water from the fridge, I had to do it before they got home, or after they went to bed, and I could never predict when they’d be home.
Luckily (or unluckily), my room faced the parking lot, and this roommate drove a car that made a very specific sound. From the moment I heard that car from my room, I had about 20 seconds to shut down whatever I was doing in the apartment, retreat to my room, and lock the door. Overreacting? Potentially, I wasn’t in any physical danger, but this was seven months of near complete isolation from any other friends, and the fear of making it worse kept me silent.
So, 20 seconds from the moment I hear the telltale whine of that engine. If I couldn’t hear the car, our front door had a lock that chimes and I had about 7 seconds from the first chime to the door opening to get the fuck out of the way. I lost weight that I couldn’t afford to lose from being unable to cook past a certain time in the evening and staying locked in my room on their days off.
Seven months of only having a door chime and an engine to tell me when it was safe and when I had to run.
—
These chime locks are the new normal and one year removed from that apartment, every time I hear it and I’m already stressed, it’s a trigger.
Every time I’m on the highway and I see a dark grey sedan of that make, that is the most important car on the road until I make sure it’s not their car.
Every time I see a dark grey sedan parked in reverse, as they habitually did, that is the most important car in the parking lot until I make sure it’s not theirs.
Every time I have to drive near a certain location where they work, I am watching for that car.
I could pick it out from 200 others. I know the license plate, I know the license plate frame, I know what sticks to the windshield, I know what hangs from the rearview mirror. I would know that car rusted and crushed in an impound lot.
So. Today I drive home and I pass a rear-parked car one turn before my unit, and I think to myself, “that’s not X’s car, but I noticed it, I’m never not going to notice it.�� It wasn’t the same make, model, or color, it was just a sedan with its nose sticking out and that was enough.
Then I turn the corner. And there it is. My ex-roommate’s car.
I shit you not it was like I had a warning from the Universe before it hit.
I don’t need to check the windshield, I know it’s theirs. I’ve seen it in my complex once before. The last time I did, I’d parked my own car and waited, got out, and hid between two others in the dark, waiting for this person to leave.
Today, in broad daylight, that car is empty. They happened to arrive while I was gone for 30 minutes. So I park, and I wait. I watch that car from my side mirror. I scan the sidewalk for them and I don’t see anything. I have frozens that can’t wait.
I’m thinking to myself, of all the parking spots in all the parking lots, of all the apartments in this godforsaken town, you parked right behind my spot.
Nothing happened, and even if we crossed paths, nothing probably would have happened (that’s how they worked, pretending nothing was ever wrong and that I was the crazy one). But I still waited, and when I decided to leave, I moved as fast as possible without drawing attention. One whole year removed from that person.
—
It doesn’t take physical abuse, or yelling and screaming and death threats. It doesn’t need to be a parent or a sibling, a relative, or a romantic partner. This person never touched me, never screamed (though they did yell on occasion), never actually threatened anything. They never called me names, were never direct with any of their insults, were never explicitly petty. I had no proof. Ever.
I just had example after example of every time they cut me down to feel smart, picked on me to feel better about themselves and project their own insecurities and jealousy, or used me as their emotional punching bag because of choices they made.
So a year after completely cutting them out, there’s that fucking car parked outside my apartment.
Media portrays “triggers” usually only in characters who are veterans. Noises that sound like gunshots, or thunder, fireworks, because that’s what we think of when we see PTSD—people who fought in wars.
It’s not like I sit around fixating on that car or that door chime (and actually with exposure to that chime every day with no consequences it’s gotten better), but that’s the point. They come out of nowhere when you least expect it. They don’t prepare you for their arrival, they just happen.
I didn’t have anything close to a panic attack, but nothing in the universe was more important in that moment than making sure I didn’t run into this person, until I calmed down.
Trigger attacks don’t have to be this big flashy thing, born of big flashy movements. It can be something as subdued as going quiet, staring at the thing, and your brain dumping everything else except all the potential outcomes of not escaping this situation immediately. It’s just a car. It’s not like an evil Big Dick truck with smokestacks and truck nuts and a MAGA flag on the back. It’s just a nerdy sedan that could belong to anyone.
—
So. PSA.
What you think might be an overreaction by someone you care about, they probably think is an overreaction, too. Did I want to have fate shit on my day and spend extra minutes under the hot sun when I have chores to do? No. But it happened.
What you think a trigger is supposed to look like or what the symptoms are supposed to be are not just what’s dramatic and flashy for the TV. Here I am writing a whole blog post about it instead of just moving on and I can't go back and check for typos because I don't want to have to reread it.
Do you want to die on a hill of “get over it” when someone you care about would love nothing more? Just. Be there for them.
And to writers, artists, anyone—it doesn’t have to be dramatic to be the most upsetting part of someone’s day. Including such simple things as a door chime, or the sound of an engine, really helps with visibility so people like me don’t think “I’m not allowed to feel this way, I didn’t actually suffer like a shell-shocked veteran”.
Most of us never will. That doesn’t make any of our hardships any less valid. Please be kind.
#writing#writing advice#writing resources#writeblr#writing tips#triggers#trauma#ptsd#writing trauma#long post
461 notes
·
View notes
Note
On the topic of realistic conditioning/deconditioning,
If the trigger is something whumpee wouldn't hear often when they're with caretaker but whumpee still wants to break it because they might hear it elsewhere (like kneel being taken as a command)
Would whumpee ask caretaker to casually trigger them so they have the opportunity to challenge it in their own head and in a safe place? Would this be a good idea for recovery?
And of course being there with the praise everytime whumpee makes just a little bit of progress, or comfort when they don't.
Heads up, anon: your ask was an EXCEPTIONALLY good one, and I ended up writing another mini TED talk (~3-4 min read) in response. Thank you so much for sending it in!
...on Conditioned Whumpees - Part 3
[ Part 1 - Part 2 ]
That is a very, very good idea! You're spot on with all of it, particularly operating in a safe environment where whumpee is ultimately calling the shots. Having that comfort/support readily available will make a huge difference in how well whumpee can tackle the matter. And while the process isn't fun, approaching desensitization with this much intent is much, much more likely to result in success.
I can offer a few pointers that can add another few layers of realism, as well as some other things to think about while tailoring it to your story:
if whumpee is actively working through their conditioning in this way, memories of their trauma will become closer to the surface. As a result, all of their other PTSD symptoms will be elevated during the course of their practice sessions, as well as for at least a few weeks after.
flashbacks are a very common experience during times like this. engaging with triggers like this is going to cause their flashbacks to become more frequent and intense.
during such flashbacks, it is almost a given that whumpee's mind and body will enter a similar state to the one it was in during the time when the flashback was taking place. By that I mean that the fear they felt in that moment, where it was physically located in their body, will echo into their body in the present moment. Same goes for other all other emotions, and sometimes even phantom aches surrounding any injuries they received at the time...
while the emotions tend to be identical to the ones felt during the trauma, in my experience, the pain comes out distorted in a similar way to the way it does in dreams: less intense, and more "blurry" and imprecise in location. When we say that someone having a flashback is "reliving the moment", we mean that their body literally feels as though they're in the same immediate danger that it was in back then.
this is true even though they'll be aware to at least some degree that they're presently with caretaker and safe.
the flashbacks don't always happen immediately after the conditioning trigger is used. Often they flare up hours or days later, sometimes without warning, sometimes as a result of encountering a different flashback trigger. The whumpee's thresholds for what counts as a trigger will drop, which is part of what causes the flashbacks to happen more often. Something they could normally ignore is going to affect them much more while they're like this.
your whumpee is more likely to experience severe mood swings while in this heightened state. Especially feelings like irritability, frustration, anger, loneliness, and grief. This stuff ain't pretty, folks. Even your sweet cinnamon bun is most likely going to lash out at someone as a result.
PTSD episodes are also exhausting. your whumpee is going to feel mentally, physically, and emotionally drained. And, to add insult to injury, being tired amplifies the emotions listed above.
Now all of this said, your whumpee may or may not know that this is to be expected. If they've worked on processing their trauma before this, they'll have figured out that one often leads to the other. They'll go into the deconditioning practice knowing this is coming, and will approach it carefully, but with a fairly level head. Knowing that it'll suck, but they'll come out the other side okay.
If not, they're in for a rather nasty surprise.
For the latter, they will feel at first that the deconditioning practice is making everything worse. They're suddenly struggling the way they did when the trauma was fresher, and it can be tempting to stop and refuse to touch it again because the mental/emotional pain gets so intense.
If they do give up at this stage, it will make trying again far more daunting in the future.
But the trauma being stirred up is actually a sign that it's helping. It means that the whumpee is starting to process what happened to them, which is a fundamental step in being able to heal.
Note: All throughout the process, crying is a very good thing. It lets them physically get rid of a lot of the brain chemicals associated with these surges of emotion. Letting themselves cry over things they couldn't cry about back then can actually help them let go of those feelings in a similar way to if they'd been able to process them in the moment. [Which is the basis for much of EMDR, a specialized tool used in trauma therapy.]
Okay. So now we know what other effects can cascade from the actual deconditioning practice, now we have some things to consider.
First off, what time parameters are whumpee and caretaker working within while deconditioning? There are three basic options:
they sit down together and practice repeatedly using the trigger for [X amount of time; usually <45m at once] back to back. Once that time is up, caretaker will no longer use the trigger at all, the excercise will end, and they'll get up to do something else.
whumpee sets a specific window of time [X number of hours] within which caretaker will use the trigger word at random points. Once that time has elapsed, the exercise is over.
over the course of days, caretaker uses the trigger word at random points without giving warning. the excercise only stops after being ended by whumpee.
Now why is that important? Because of something called hypervigilance. It is another symptom of PTSD which, to put it into the simplest words, is whumpee waiting for the other shoe to drop. It's a heightened state of tension and wariness in which whumpee is expecting that something bad is going to happen, and is constantly searching for any sign to indicate when it's coming.
It is beyond exhausting.
Imagine knowing that someone is about to slap you as hard as they can, and you have to sit there with your eyes closed, waiting for it. The breath-holding, the flinchiness, the rigid tension in your body as you strain to listen for when they're coming.
Only now, stretch that moment out into hours. Days. Weeks. That is hypervigilance.
A hypervigilant whumpee is not going to be able to relax. Or rest. Or decompress. Or readily trust much of anything around them. They're MUCH more likely to flinch at sudden movements/sounds. They might start biting their nails or showing other signs of nervousness and distress.
These methods above have a gradually increasing chance of setting off whumpee's hypervigilance. If they know exactly when the next trigger is coming, as in example 1, then their 'waiting for it' tension will be low. But the more uncertain they become of exactly when it's going to happen, as in examples 2 & 3, the worse the hypervigilance is going to get.
The trade off is that the later examples are more effective in desensitizing them toward the trigger. The more their practice mimics encountering an unexpected trigger in day-to-day life, the easier it will be to fall back on that desensitization when the time comes.
Therefore, it would be a very good idea for a whumpee who's new to this to start with number 1, then gradually progress to 2 & 3 as time goes on. They should be the one to decide when the next step is made, and if/when they need to dial it back.
Other questions to ask yourself while plotting:
how mentally prepared is whumpee for worsening symptoms? what about caretaker? did either of them know it was coming?
how much of this heightened PTSD stress can your whumpee take before it becomes too much? how do they react when they do hit that tipping point?
if caretaker feels that whumpee is getting too distressed during practice even though they're not tapping out, would they call it off themself? Or would they ultimately leave that decision to whumpee?
based on the answer, how would whumpee feel about caretaker's decision? Relieved? Belittled? Betrayed?
does whumpee have any grounding tools they can use while practicing?
how does caretaker handle the mood swings and instability that come with whumpee's heightened PTSD? You should consider both their internal and external reactions on the matter.
how does whumpee prefer to decompress after a practice session? what things would help them calm down and recover?
how long do they need (hours or days) before the next attempt?
Even with all I've just written, there's far more to the resulting hightened state of PTSD than flashbacks and hypervigilance. PTSD symptoms that they're most likely to encounter in the background while doing deconditioning practice include:
Flinchiness, anxiety, panic attacks, nightmares, exhaustion, emotional mood swings, outbursts, crying spells, depression, executive dysfunction, dissociation, numbness, racing thoughts, freeze responses, tremors, inappetence, muscle tension, and heart palpitations.
Yes, usually many of them at once, even those that contradict. Your whumpee is going to have a LOT going on at once, and it is not going to be a fun time. I recommend looking up any of the above symptoms you don't recognize, and looking for whump inspiration in what you learn.
(Because everyone experiences PTSD episodes differently, there's a lot of wiggle room in which ones whumpee will encounter. Don't feel pressured to use all of them, find what you want to write and have fun with it!)
Thanks again for the incredible ask, anon. And again, I want to congratulate you on how spot-on your original ask was. You nailed it. I know this was a lot more than you asked for, but I hope this provides helpful context for your whump! My inbox will always be open if you think of anything more <3
#conditioned whumpee#pet whump#whump#bbu whump#box boy universe#caretaker#whump inspo#whump inspiration#rescued whumpee#whump recovery#whump resource#whump advice#writing advice#writing reference#PTSD in whump#trauma recovery#whumpee#whumpblr#whump prompt#ask Wick
265 notes
·
View notes
Text
ear’s guide to writing stab wounds
disclaimer!!!: this isn’t to be used as actual medical advice there isn’t enough information at hand to properly treat someone, this is just for writing.
hemostatic (blood clotting) control is the number one priority. minor bleeding can be controlled with direct pressure to the wound. moderate bleeding may require a compression bandage as well as direct pressure. severe penetrating wounds or a nicked artery means wound packing will be necessary as well as direct pressure.
types of stab wounds:
- blunt stab wound means whatever object caused the trauma wasn’t sharp or wasn’t moving fast enough so the skin tears.
- penetrating stab wounds go deep into the skin and into the muscle.
- superficial stab wounds don’t go too far under the skin and look worse than they actually are.
steps to treatment:
1. if the object is still inside the person’s body do not remove it unless it’s to the groin, neck, or axillae (armpit) and the bleeding is hard to control.
2. remove person’s clothes to check for any other wounds and keep the area clear.
3. keep an eye on blood pressure and airway.
4. the wound type and location changes how the rest of treatment will follow.
location:
head: direct pressure is mainstay. head wounds also bleed more than any other part of the body. has the highest mortality rate.
face: severe wounds to the face means the patient has to be seated forward to keep blood out of the airway.
neck: direct pressure is mainstay. if the airway can be secured and is absolutely necessary, wound packing can be applied.
arms: depending on the severity, any of the three treatments can be used.
legs: depending on the severity, any of the three treatments can be used.
abdomen: damage to organs is highly likely. direct pressure should be applied first while surveying if the object was long enough to damage an organ. if so, wound packing may be necessary.
chest: if the wound is deep enough it can cause open pneumothorax (‘sucking’ chest wound) a seal needs to be placed over the wound to keep air from getting inside. if this isn’t done in time the affected lung will collapse.
back: can typically be treated with only direct pressure. wound packing is rarely necessary.
neck, chest, abdomen, and pelvis wounds should never be packed unless absolutely necessary.
treatment types:
direct pressure: key to any wound. can be done with whatever is available even if that means the medic needs to use their own body weight.
tourniquets: applied to the limbs. typically not applied for more than thirty minutes. in some cases, they can be left on for hours, keeping the phrase “life over limb” in mind. complications with tourniquets like nerve damage or ischemia (no blood circulation) are rare. don’t apply over a joint and apply above the wound.
wound packing: done with standard gauze and or hemostatic dressing
wound packing steps:
1. control the bleeding with pressure. use anything available even if it means t shirts or a knee.
2. place a gloved finger inside the wound too apply initial pressure. this will hurt like a bitch. also gives you an idea of what direction the blood is coming from so gauze can be used more accurately.
3. begin packing the wound with gauze. keep pressure on the wound with finger while wrapping gauze around another finger and pushing it in the wound.
4. keep packing the wound until no more gauze can fit in, and then keep direct pressure on for at least three minutes.
5. after the three minutes, use something like a bandage wrap to keep the gauze secure inside the wound.
6. splinting the area to keep it immobilized may be vital to keep the hemorrhage from restarting
7. if bleeding continues medic has to decide if they need to take out gauze and reapply with new gauze or apply more direct pressure. this is usually done by how long it takes to get to further treatment. the longer the wait the more of an incentive it becomes to repack the wound. if it’s just down the road then apply pressure.
most likely complications:
hypoxia, shock, and hypothermia are complications that need to be watched for and treated immediately if they occur.
hypoxia:
occurs when a region of the body doesn’t have enough oxygen in the tissue. can lead to organ damage, brain and heart damage being the most dangerous.
symptoms include: tachycardia (rapid heart rate), difficulty breathing, confusion, shortness of breath, anxiety, headache, and restlessness.
severe symptoms include: bradycardia (slow heart rate), extreme restlessness, and cyanosis (blue or purple tint to skin).
treatment: oxygen
shock:
life threatening condition where the body doesn’t have enough blood volume to circulate through itself. if it goes on for long enough, organ damage and death may occur.
symptoms: rapid, slow, or absent pulse, heart palpitations, rapid shallow breathing, lightheadedness, cold clammy skin, dilated pupils, chest pain, nausea, unfocused eyes, confusion, anxiety, and loss of consciousness.
treatment: if they’re not breathing, cpr is required. if they are breathing, lay on back and raise feet a foot off the ground to keep blood in the vital organs.
blood transfusion and fluids once in a hospital setting.
hypothermia: occurs when the body is losing heat quicker than it can produce. the more blood that’s lost the more likely hypothermia is to occur.
symptoms: differ based on severity
hypothermia:
in mild hypothermia: shivering, exhaustion, clumsiness, sleepiness, weak pulse, tachycardia (rapid heart rate), tachypnea (rapid breathing), pale skin, confusion, and trouble speaking.
in moderate hypothermia: bradycardia (slow heart rate), bradypnea (slow breathing), slurred speech, decline in mental function, shivering slows down, hallucinations, cyanosis (blue or purple tint to skin), muscle stiffness, dilated pupils, irregular heart rate, hypotension (decreased blood pressure), and loss of consciousness.
in severe hypothermia: shivering stops, hypotension (low blood pressure), absence of reflexes, compete muscle stiffness, fluid builds up in lungs, loss of voluntary motion, cardiac arrest (heart stops beating), coma, and death.
treatment: covering with a blanket, hat, and jacket, adding external heat like a hot pack, and if severe and in a hospital setting, warm fluids via iv, warm oxygen, and or a machine to warm the blood in the body.
if you have any questions feel free to ask! i plan on making a guide to gunshot wounds and a more in depth guide to hypothermia later.
#tips for writers#writing advice#helping writers#writing resources#resources for writers#writing tips#writing help#creative writing#trauma writing guide#medical writing tips#writing guide#medical writing guide#stab wound#call of duty#cod#call of duty modern warfare#ear’s guide to writing
941 notes
·
View notes
Text
You know what? You know what I think?
I think that if we lived as we were meant to, in larger intimate ("extended family") groups and with more shared labor and time to do it (UBI NOW) people like me would not feel so useless and burdensome because there would be people around to help and to do what neurodivergent people can't while making valuable space for the neurodivergent to do what they ARE good at.
The way we live right now, all right, the way we live right now forces units of two adults to be able to do EVERYTHING or PAY to have someone come do it for them. I have to do the housework. I have to do it! But I am having to do a million different things and most of them I am not good at. I suck at them.
I wouldn't feel like shit, okay, if I had more than one other person around who was not a child and who could do the things I can't, like do the yard and cook and do repairs and basic maintenance; and someone else to split everything else that I like but is too much for me. It would free me to do what I am good at and enjoy. Cleaning, as in the sink and toilet, the windows, the blinds. Taking out trash. Folding, hanging, and sorting laundry.
But because all the shit I can do often relies on other shit being done first, and I can't do or have trouble doing those things, the shit I can do often can't be done. And even the shit I can do, I can't do ALL of it. So I can't keep up, and things get very bad.
We aren't meant to live like this. We are not meant to live like this.
That thought hurts so much because being able to flee the birth family is integral to survival for so many people. I'm so afraid that living in larger family groups would create more opportunities for, say, queer kids to be isolated, rejected, bullied, and abused. But if we gave people enough money to survive, and stopped considering children the property of their parents with no system in place to help them escape bad situations except a system that is often just as bad, just different.
I'm aware that communes and collectives aren't all that successful and are kind of a joke. I don't mean that. I mean a fundamental shift to multigenerational families where taking in "strays" (which my family did) is also normalized so people escaping abuse into existing households was accepted, with these families centered in maybe a couple of different larger residences so not everyone has to buy and maintain their own fucking washing machine and vacuum cleaner, and so people can benefit from large group meals that yield leftovers, and so child and elder care can also be centralized.
Then disabled people and the neurodivergent and sick and injured people, and pregnant people, and grieving people, would not have to either labor through all those stressors or consign themselves to living off an unlivable pittance or being put under legal guardianship.
I'm not saying anything new. People live like this in other parts of the world and maybe it sucks and I am wrong. But I'm just really mad right now because I can either do laundry or clean the sink but not both, and I really think we could improve society somewhat by making it so I did not have to choose one without sacrificing the other.
#im feverish feeling (not a real fever just malaise that i have no other way to describe) from the IBS (which can affect you like that#)#and i don't actually want to do ANYTHING#i would have to even living with others but it would be easier#at the very least i wouldn't have had to clean the microwave earlier which is hard because my arms are like the size of a meerkat's#and i can only reach the back with my fingertips#where is my BF in all this?#WORKING FULL TIME WITH BACK PAIN#yes i AM going to want him to have to do as little as possible when he comes home#he's neurodivergent too and struggles with the same shit#it's all a mess#we are doing way better i didn't realize how deep a drain three very sick cats were#but there's still only two of us#if you are disabled physically OR MENTALLY you should at least get in-home household help once a week or so#there's places that do that but the limitations are usually severe and always rule me out#because im not single im not an elder im not a veteran and im not physically disabled#if we have to ration that sort of thing i can see how on the whole it is more caring to allocate those resources to for example elders#but the fact that i celebrate what help there is doesn't mean i don't get mad that more people can't access it#is2g if i was functional enough snd physically sound enough i would start a charity that did intervention cleaning for people like us#who have fallen behind and can't catch up but can MAINTAIN#and who helped people clean for a few months during and after an illness pregnancy trauma major loss etc. so they could stay on their feet
354 notes
·
View notes
Text
⚠️ emergency links
this is a list of resources for when you're in crisis, whether you're suicidal, triggered, having a panic attack, or any other mental health emergency.
this list will be updated with new resources as i find them.
emergency numbers for your country
helplines for your country
Australia: lifeline 13 11 14 & other helplines
managing flashbacks
quick helpful tips for suicidal feelings
you feel like shit interactive self care guide (alternative site)
reassurance masterpost
Get Self Help
psychosis coping strategies
grounding techniques
dealing with trauma triggers & OCD
DBT options for solving problems
self-soothing ideas
how to check the (emotional) facts
TIPP grounding skill (temperature, intense exercise, paced breathing, progressive muscle relaxation)
ideas for soothing impulses (urge surfing)
tips for when it feels too much
why am i feeling bad? flowchart
looking after yourself (particularly tolerating distress)
staying safe in a crisis
crisis support (particularly for dissociation & dissociative identity disorder)
safety tools & resources
dealing with PTSD triggers
grounding & containment strategies
#resources#mental health resources#emergency resources#crisis resources#crisis#emergency#grounding#trauma#suicidal ideation#suicide#dogpost#sos#help#self help#self soothing#self care
557 notes
·
View notes
Text
Hmrrmmm reader running a women's rehab / shelter for current / former sex workers in poverty, offering safety / food / shelter
Hrmmrmm Alejandro helping them when he can... he's so busy but he's got a soft spot for you so you know you can go to him for help :')
Alejandro who knows you have a history and doesn't push, but you genuinely feel safe with him
Alejandro who would never have anyone on his team that would be creepy or assault any women / victims but knows why you and the others are wary of men, so its only ever his most trusted who visit you or help you :')
Idkkk I need more Alejandro and unfortunately for me I'm into gentle masculine men and I feel like Alejandro would be so masculine but so gentle:') a little old fashioned, but it's appreciated when you haven't been treated well:')
When he greets you its kisses on your cheeks and eyelids, holding your hands, so sweet and tender :'D he and his vaqueros donate food/etc and you cook pastries for him in return
Sigh
#alejandro vargas#reader x alejandro vargas#alejandro vargas x reader#cod x reader#cod mw2#task force 141#los vaqueros#idkkk#i would never engage with a man irl from trauma but dreaming abo#ut it is <3#also nothing against sex work#but the resources for women/other gender diverse people to leave are very poor tbh#and there needs to be adequate support#for people trying to leave#anyways enough discouse#im anti swerf of course#i wanna have his babjes
175 notes
·
View notes
Text
If you're trying to get over your fear of Hell, I recommend Bart D. Ehrman's book, Heaven And Hell: A History of the Afterlife. Or if you can't read the book, you can watch his lecture on YouTube. As you learn how all of this stuff organically developed and evolved, you can see that there's no good reason to take anything conservative Christians say about eternal damnation very seriously.
139 notes
·
View notes
Text
Its gonna be okay just remember that no matter what your trauma is, someone’s made a spotify playlist for it
#music heals#music therapy#music is therapy#music is medicine#music#spotify playlist#playlists#playlist#Spotify#art therapy#trauma recovery#cptsd healing#cptsd recovery#complex trauma#childhood trauma#childhood emotional neglect#mental health resources#self care tips#listen to music#currently listening to#music sharing#i love music#music tumblr#music blog#autistic self care#post traumatic growth#traumagenic#post traumatic stress disorder#complex post traumatic stress disorder#trauma disorders
184 notes
·
View notes
Text
It's just fascinating to me the way Vex's trauma, first from Syldor and Syngorn and then from the poachers who kidnapped her, is so relatively mundane and yet so resonant. Her and Vax's only real recourse from the abuse and racism they suffered was to leave, but living on their own meant they were also perfect targets. Statistically it's not your average suburban kid gettin snatched in a parking lot that makes up most kidnapping or trafficking victims; it's the kids who've been tossed around the system, who have slipped through the cracks in some way, who are already vulnerable—the people who no one will miss.
And Vex freeing herself from the poachers still gave her trauma, just a different kind of trauma than she'd have had if she'd actually been trafficked. Leaving Syngorn meant freedom from its cruelty, but it also meant being at the mercy of the rest of the world, and it meant a final admission to herself that no matter how hard she worked she would never get the acceptance and the home she longed for. It's an experience that's unfortunately all-too-common among so many oppressed and marginalized peoples. She spent so much time in situations where there was no way for her to win or get out unscathed, and it's no wonder she closed herself off from the world.
#critical role#vex'ahlia#cr meta#she's just INCREDIBLY interesting as a character for a lot of the mundane dynamics she explores#and the fact that yes she is traumatized and a lot of her actions can and should be understood as trauma responses#but that doesn't mean those actions are always okay or don't hurt people#because her arc being about forgiveness wouldn't resonate if she wasn't the type to hold grudges#it's easy to look at this fictional character and sympathize with her and extol her virtues#but there are so many people in real life who have experienced the same things vex has and respond a lot like she does#and they can be difficult people to love and help and be around#and that's a crucial reality to accept—difficult people are still deserving of rights and resources and dignity and care#just like this fictional person is
60 notes
·
View notes
Text
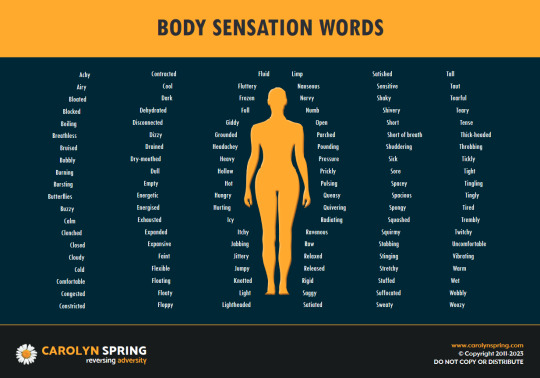
I like this diagram a lot!
Because of dissociation and trauma, I've struggled a lot to identify what I'm feeling, both emotionally and physically. Lists like this can be really helpful. I've found lots of lists with emotion words before but not as much when it comes to body sensations. Wanted to share it.
Here's a grounding exercise for anyone reading this: try going through the list and pick out which words fit what you're feeling in this moment.
______________
[Image Description: A free resource from Carolyn Spring. It shows the figure of a person surrounded by a list of words. Here is what it says:
Body Sensation Words
Achy, Airy, Bloated, Blocked, Boiling, Breathless, Bruised, Bubbly, Burning, Bursting, Butterflies, Buzzy, Calm, Clenched, Closed, Cloudy, Cold, Comfortable, Congested, Constricted, Contracted, Cool, Dark, Dehydrated, Disconnected, Dizzy, Drained, Dry-mouthed, Dull, Empty, Energetic, Energised, Exhausted, Expanded, Expansive, Faint, Flexible, Floating, Floaty, Floppy, Fluid, Fluttery, Frozen, Full, Giddy, Grounded, Headachey, Heavy, Hollow, Hot, Hungry, Hurting, Icy, Itchy, Jabbing, Jittery, Jumpy, Knotted, Light, Lightheaded, Limp, Nauseous, Nervy, Numb, Open, Parched, Pounding, Pressure, Prickly, Pulsing, Queasy, Quivering, Radiating, Ravenous, Raw, Relaxed, Released, Rigid, Saggy, Satiated, Satisfied, Sensitive, Shaky, Shivery, Short, Short of breath, Shuddering, Sick, Sore, Spacey, Spacious, Spongy, Squashed, Squirmy, Stabbing, Stinging, Stretchy, Stuffed, Suffocated, Sweaty, Tall, Tout, Tearful, Teary, Tense, Thick-headed, Throbbing, Tickly, Tight, Tingling, Tingly, Tired, Trembly, Twitchy, Uncomfortable, Vibrating, Warm, Wet, Wobbly, Woozy
End ID.]
#actuallydid#actuallydissociative#trauma recovery#DID recovery#dissociation recovery#resources#DID support#carolyn spring#sunflower posts
221 notes
·
View notes
Text
one thing that has been frustrating lately is that outside of the disability specific organizing spaces i'm in, i've noticed that so many people assume that because i'm a wheelchair user, i don't have relevant experience/skills for high risk and escalated protests. what's particularly frustrating lately is that some of these organizing spaces i'm in, i actually have more relevant experience than a lot of my comrades--i started going to antifascist protests when i was 13 and have been involved in a lot of protest movements over the past 9 years. and have learned a lot of shit from a lot of mentors. some of my comrades just got involved this year, which is great and i have a lot of respect for them. and at the same time i genuinely do have a lot of relevant knowledge about tactics, practical experience, etc etc. i'm always learning + continue to grow my skills and don't want to get complacent ever but like. some people were talking about how they wanted to learn how to do eye flushes for tear gas and i was like "okay yeah we can practice that, i can teach everyone if we stay a little later tonight" and someone said "thanks for offering but we should probably learn from someone who's had experience doing this on the ground." which was so fucking patronizing because i literally do have that skill set...i have been tear gassed many many times, have done eye flushes for people many many times, literally have a LOT OF practice doing that in a high stress and chaotic environment when the cops are brutalizing you. and no one else in this group had this experience! ignoring my experience made no sense and actively endangered the group! it made me want to scream like. how fucking ableist to assume that and also to insist that disabled people aren't involved in high risk protests even though we have already been out here involved for years and years! i'm going to scream
#personal#ableism#also my experience as a disabled person makes me a BETTER organizer. there are a lot of ways it has#allowed me to understand even deeper what community care looks like#what we keep us safe looks like and how to actually do that in the streets#when you think about how to keep disabled ppl safe in the streets you make it better for everyone#my experience with mad liberation work helps a LOT and gives me a lot of skills and resources#for helping all my comrades. mad or otherwise. with dealing with trauma. solitary. burnout. etc etc etc
107 notes
·
View notes