#medical writing guide
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text
ear’s guide to writing stab wounds
disclaimer!!!: this isn’t to be used as actual medical advice there isn’t enough information at hand to properly treat someone, this is just for writing.
hemostatic (blood clotting) control is the number one priority. minor bleeding can be controlled with direct pressure to the wound. moderate bleeding may require a compression bandage as well as direct pressure. severe penetrating wounds or a nicked artery means wound packing will be necessary as well as direct pressure.
types of stab wounds:
- blunt stab wound means whatever object caused the trauma wasn’t sharp or wasn’t moving fast enough so the skin tears.
- penetrating stab wounds go deep into the skin and into the muscle.
- superficial stab wounds don’t go too far under the skin and look worse than they actually are.
steps to treatment:
1. if the object is still inside the person’s body do not remove it unless it’s to the groin, neck, or axillae (armpit) and the bleeding is hard to control.
2. remove person’s clothes to check for any other wounds and keep the area clear.
3. keep an eye on blood pressure and airway.
4. the wound type and location changes how the rest of treatment will follow.
location:
head: direct pressure is mainstay. head wounds also bleed more than any other part of the body. has the highest mortality rate.
face: severe wounds to the face means the patient has to be seated forward to keep blood out of the airway.
neck: direct pressure is mainstay. if the airway can be secured and is absolutely necessary, wound packing can be applied.
arms: depending on the severity, any of the three treatments can be used.
legs: depending on the severity, any of the three treatments can be used.
abdomen: damage to organs is highly likely. direct pressure should be applied first while surveying if the object was long enough to damage an organ. if so, wound packing may be necessary.
chest: if the wound is deep enough it can cause open pneumothorax (‘sucking’ chest wound) a seal needs to be placed over the wound to keep air from getting inside. if this isn’t done in time the affected lung will collapse.
back: can typically be treated with only direct pressure. wound packing is rarely necessary.
neck, chest, abdomen, and pelvis wounds should never be packed unless absolutely necessary.
treatment types:
direct pressure: key to any wound. can be done with whatever is available even if that means the medic needs to use their own body weight.
tourniquets: applied to the limbs. typically not applied for more than thirty minutes. in some cases, they can be left on for hours, keeping the phrase “life over limb” in mind. complications with tourniquets like nerve damage or ischemia (no blood circulation) are rare. don’t apply over a joint and apply above the wound.
wound packing: done with standard gauze and or hemostatic dressing
wound packing steps:
1. control the bleeding with pressure. use anything available even if it means t shirts or a knee.
2. place a gloved finger inside the wound too apply initial pressure. this will hurt like a bitch. also gives you an idea of what direction the blood is coming from so gauze can be used more accurately.
3. begin packing the wound with gauze. keep pressure on the wound with finger while wrapping gauze around another finger and pushing it in the wound.
4. keep packing the wound until no more gauze can fit in, and then keep direct pressure on for at least three minutes.
5. after the three minutes, use something like a bandage wrap to keep the gauze secure inside the wound.
6. splinting the area to keep it immobilized may be vital to keep the hemorrhage from restarting
7. if bleeding continues medic has to decide if they need to take out gauze and reapply with new gauze or apply more direct pressure. this is usually done by how long it takes to get to further treatment. the longer the wait the more of an incentive it becomes to repack the wound. if it’s just down the road then apply pressure.
most likely complications:
hypoxia, shock, and hypothermia are complications that need to be watched for and treated immediately if they occur.
hypoxia:
occurs when a region of the body doesn’t have enough oxygen in the tissue. can lead to organ damage, brain and heart damage being the most dangerous.
symptoms include: tachycardia (rapid heart rate), difficulty breathing, confusion, shortness of breath, anxiety, headache, and restlessness.
severe symptoms include: bradycardia (slow heart rate), extreme restlessness, and cyanosis (blue or purple tint to skin).
treatment: oxygen
shock:
life threatening condition where the body doesn’t have enough blood volume to circulate through itself. if it goes on for long enough, organ damage and death may occur.
symptoms: rapid, slow, or absent pulse, heart palpitations, rapid shallow breathing, lightheadedness, cold clammy skin, dilated pupils, chest pain, nausea, unfocused eyes, confusion, anxiety, and loss of consciousness.
treatment: if they’re not breathing, cpr is required. if they are breathing, lay on back and raise feet a foot off the ground to keep blood in the vital organs.
blood transfusion and fluids once in a hospital setting.
hypothermia: occurs when the body is losing heat quicker than it can produce. the more blood that’s lost the more likely hypothermia is to occur.
symptoms: differ based on severity
hypothermia:
in mild hypothermia: shivering, exhaustion, clumsiness, sleepiness, weak pulse, tachycardia (rapid heart rate), tachypnea (rapid breathing), pale skin, confusion, and trouble speaking.
in moderate hypothermia: bradycardia (slow heart rate), bradypnea (slow breathing), slurred speech, decline in mental function, shivering slows down, hallucinations, cyanosis (blue or purple tint to skin), muscle stiffness, dilated pupils, irregular heart rate, hypotension (decreased blood pressure), and loss of consciousness.
in severe hypothermia: shivering stops, hypotension (low blood pressure), absence of reflexes, compete muscle stiffness, fluid builds up in lungs, loss of voluntary motion, cardiac arrest (heart stops beating), coma, and death.
treatment: covering with a blanket, hat, and jacket, adding external heat like a hot pack, and if severe and in a hospital setting, warm fluids via iv, warm oxygen, and or a machine to warm the blood in the body.
if you have any questions feel free to ask! i plan on making a guide to gunshot wounds and a more in depth guide to hypothermia later.
#tips for writers#writing advice#helping writers#writing resources#resources for writers#writing tips#writing help#creative writing#trauma writing guide#medical writing tips#writing guide#medical writing guide#stab wound#call of duty#cod#call of duty modern warfare#ear’s guide to writing
964 notes
·
View notes
Text
Writing this Final Fantasy 7 fanfic is kind of a weird experience, because I try to stick to the tone of the original work, and Final Fantasy 7 can get darker in tone than what I'm used to. Do I warn for "Canon Typical Hojo"???
Actually, I notice that there's quite a few Final Fantasy 7 stories on AO3 tagged with "Content Warning: Hojo", or "Hojo Being Hojo", so I guess I do? Also, "Bad Dad Hojo", which is relevant since the story is about Chadley. Hojo is not winning any father of the year awards in that one scene in Rebirth where he acknowledges Chadley's existence. Enslaving your kid to work in your evil science lab is also not great parenting.
I don't normally dislike fictional characters, but I think I do dislike Hojo. I don't really... want to look at him. Is this one of those "confront characters" I keep hearing about? It was hard to even analyse him so his actions would make sense in the story. I think he's someone who once experienced not being the smartest person in the room, and made it his life's mission to make sure that never happened again.
This story is also making me like MAI, after being indifferent to her for a while. I'm going with Chadley accidentally creating a person while trying to create an AI assistant, with neither of them having realised it yet. That gives them an interesting dynamic! At least to me.
I just hope I have the energy to edit this story into making sense, so I can finish it. And also to keep playing the original game up to when this story is set. The canon story stuff is happening in the background, and I know roughly what happens, but I really should play through it as well.
#Final Fantasy 7#Final Fantasy 7 Remake Trilogy#Chadley#Hojo (Final Fantasy)#MAI (Final Fantasy)#There's a bit near the end I need to fix in the outline but otherwise I'm happy with the general plot#Since Chadley has a canon age (15) I assume he ages normally and that Hojo raised him from an infant#'Dorky but rebellious human teenager' would be a weird assistant choice for Hojo to make from scratch anyway#And the Rebirth strategy guide describes him as having gone through Hojo's medical procedures without saying Hojo created him#So I think Chadley's upbringing probably had a huge effect on him#In what I've got so far Hojo's presence is felt some time before he actually shows up#I can't promise this story will be any good but I am really enjoying writing it
7 notes
·
View notes
Note
y/n type fic - you're the household's new familiar, and as the guide has some expertise from her volunteering, she is the one to inspect you physically. in her unhinged nurse outfit obv. whatever medical kink stuff you like, go wild
-
#wwdits#wwdits kink meme#kink meme#writing prompt#reader insert#the guide x reader#medical kink#doctor kink#the guide wwdits
17 notes
·
View notes
Text
#Sriina#books#education#medical books#medical writing#A Guide for Medicos#Educators and Researchers#Online book store
1 note
·
View note
Text


URGENT!!!Help Abdul Salam Al-Anqar and his family get through this war in Gaza!!!
(URGENT) THEY ARE AT €3,445 OUT OF €50,000 GOAL
I was asked by @nader5555 to make this, if u cannot donate please please share this post. Copy pasted from a message i was sent:

"Only a Few Hours Left Before We Enter Our First Year of War, Genocide, Starvation, and Displacement A Final Plea from the Heart of Hell: Save Us Before Hope Dies 💔🔥 I am Abdel Salam, and I have nothing left but words written by a trembling hand ✍️. The war has not only destroyed our lives; it has taken everything from us. Our home, which was once our refuge, is now a pile of rubble 🏚️.
My car, my only source of livelihood, was destroyed in a sudden strike 🚗, and the work that sustained us is now a distant memory 💼. Today, I live in an endless nightmare. Under a sun that burns everything in its path 🌞🔥, my family and I sit in a worn-out tent, a tent that shields us neither from the summer heat nor the winter cold ❄️. Insects 🦟 invade the place, diseases consume our bodies 🩺, and my younger siblings cry from hunger and thirst 🍞💧. We have no clean water or a crumb of bread to ease our hunger. Each passing day deepens the weight of this hell we live in.

My Daughter Eman is Dying from Malnutrition 😨 My daughter Eman suffers from malnutrition; I have nothing to feed or treat her with. The deterioration of her health is killing me slowly. Every glance in her eyes, every pain she endures, crushes my heart 💔. How can I explain to her that what was once our hope has now turned into nothing but a mirage? The Night Only Adds to Our Pain 🌙 The night does not bring us rest; it only adds to our pain. We sleep on hard ground, feeling the cold in every bone of our bodies 🥶, with nothing but pieces of cardboard 📦 to cover us. My wife Aya cries in silence 🥺 as she watches our daughter’s future fade before her eyes. My mother Eman suffers from illness and needs urgent medical care 🩺💊.

My Father Ahmed is Sick with Cancer and Needs Emergency Treatment My father Ahmed, who is sick with cancer, needs emergency treatment outside Gaza, and the cost of his treatment is at least $10,000, not including accommodation. As he suffers from severe pain, I cannot provide the treatment he needs due to our dire situation.

My Siblings Are in Constant Suffering ⚰️ My brother Omar was unable to continue his studies due to the situation. My brother Nader could not take his high school exams, and my younger brother Mohammad suffers from brittle bones and needs treatment we cannot afford. Every day we live brings us one step closer to the end. Death surrounds us from every side: if not from hunger 🍽️, then from illness 🦠. And if not from illness, then from the despair that devours our souls. Where is Humanity? Where is the World? 🌍💔 We want to leave the devastated Gaza Strip to escape the machinery of destruction and killing and the severity of hunger and poverty. The cost of travel for each person is $5,000, and we are a family of seven members, bringing the total cost to $35,000.
Where are the compassionate hearts? Are you waiting for us to disappear into the depths of this suffering? Are you waiting until death takes us before you act? We are drowning, and we don’t have enough strength to scream for help 🆘. Will you let this cry go unanswered? 😭 Your donation today is our last thread of hope. With the little support I received, I was able to buy a simple phone 📱 to reach out to you. But the bitter truth is that what I and my family need is much greater. We are not asking for much; just enough to save our lives from this hell 🔥. Every donation, no matter how small, could be the difference between life and death for us 👐. Don’t Let Us Disappear in the Darkness of Suffering 🌑 Don’t let our story end here. Be the light that guides us to salvation 🕯️✨.
With every tear, with every pain, I write this final plea to you, Abdel Salam."
taglist
@butchniqabi @xinakwans
@batekush
@appsa
@nerdyqueerr
@butchsunsetshimmer
@biconicfinn @stopmotionguy
@t4tvampireisms
@strangeauthor
@bryoria @shesnake
@legallybrunettedotcom
@lautakwah @sovietunion
@neechees @evillesbianvillain @antibioware
@akajustmerry @dizzymoods
@ree-duh @neptunerings
@explosionshark
@heritageposts
@ibtisams
@schoolteacher
#my art#**mine#free palestine#free gaza#gfm#palestine gfm#b00st#help#mutual 4id#donation link#boost#signal boost#art#artists on tumblr#digital artist#digital art#artblr#save palestine#palestine#all eyes on palestine#free plaestine#gaza#from river to sea palestine will be free#artists#please help#important#edit: changing photos per nader5555's request
13K notes
·
View notes
Text
A general cane guide for writers and artists (from a cane user, writer, and artist!)
Disclaimer: Though I have been using a cane for 6 years, I am not a doctor, nor am I by any means an expert. This guide is true to my experience, but there are as many ways to use a cane as there are cane users!
This guide will not include: White canes for blindness, crutches, walkers, or wheelchairs as I have no personal experience with these.
This is meant to be a general guide to get you started and avoid some common mishaps/misconceptions in your writing, but you absolutely should continue to do your own research outside of this guide!
This is NOT a medical resource!!! And never tell a real person you think they're using a cane wrong!
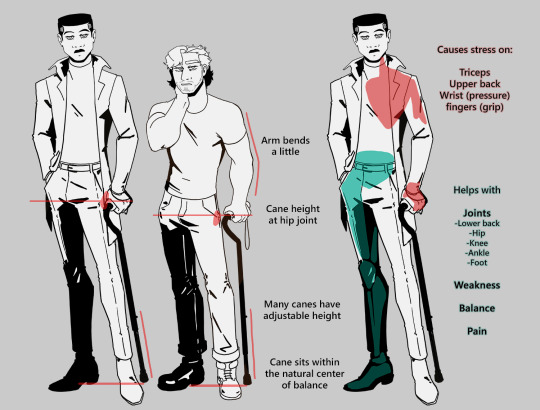
The biggest recurring problem I've seen is using the cane on the wrong side. The cane goes on the opposite side of the pain! If your character has even-sided pain or needs it for balance/weakness, then use the cane in the non-dominant hand to keep the dominant hand free. Some cane users also switch sides to give their arm a rest!
A cane takes about 20% of your weight off the opposite leg. It should fit within your natural gait and become something of an extension of your body. If you need more weight off than 20%, then crutches, a walker, or a wheelchair is needed.
Putting more pressure on the cane, using it on the wrong side, or having it at the wrong height can make it less effective, and can cause long term damage to your body from improper pressure and posture. (Hugh Laurie genuinely hurt his body from years of using a cane wrong on House!)
(some people elect to use a cane wrong for their personal situation despite this, everyone is different!)
(an animated GIF of a cane matching the natural walking gait. It turns red when pressure is placed on it.)
When going up and down stairs, there is an ideal standard: You want to use the handrail and the cane at the same time, or prioritize the handrail if it's only on one side. When going up stairs you lead with your good leg and follow with the cane and hurt leg together. When going down stairs you lead with the cane and the bad leg and follow with the good leg!
Realistically though, many people don't move out of the way for cane users to access the railing, many stairs don't have railings, and many are wet, rusty, or generally not ideal to grip.
In these cases, if you have a friend nearby, holding on to them is a good idea. Or, take it one step at a time carefully if you're alone.
Now we come to a very common mistake I see... Using fashion canes for medical use!
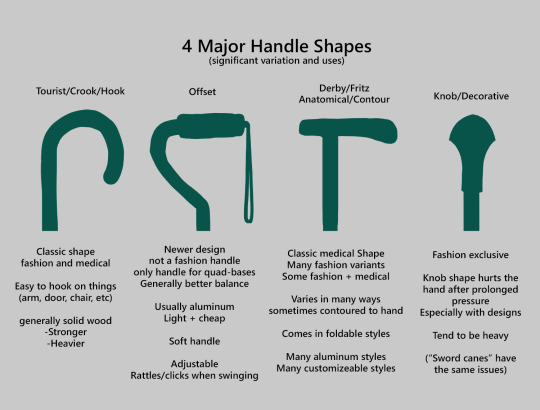
(These are 4 broad shapes, but there is INCREDIBLE variation in cane handles. Research heavily what will be best for your character's specific needs!)
The handle is the contact point for all the weight you're putting on your cane, and that pressure is being put onto your hand, wrist, and shoulder. So the shape is very important for long term use!
Knob handles (and very decorative handles) are not used for medical use for this reason. It adds extra stress to the body and can damage your hand to put constant pressure onto these painful shapes.
The weight of a cane is also incredibly important, as a heavier cane will cause wear on your body much faster. When you're using it all day, it gets heavy fast! If your character struggles with weakness, then they won't want a heavy cane if they can help it!
This is also part of why sword canes aren't usually very viable for medical use (along with them usually being knob handles) is that swords are extra weight!
However, a small knife or perhaps a retractable blade hidden within the base might be viable even for weak characters.
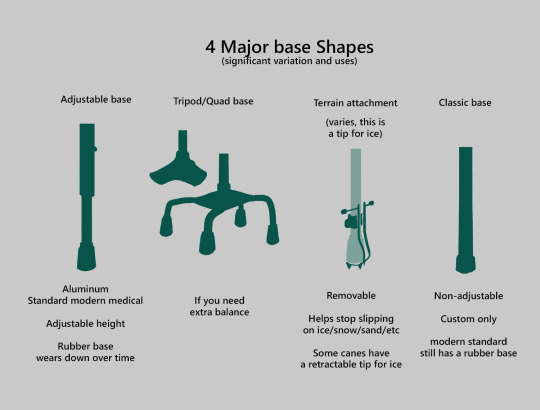
Bases have a lot of variability as well, and the modern standard is generally adjustable bases. Adjustable canes are very handy if your character regularly changes shoe height, for instance (gotta keep the height at your hip!)
Canes help on most terrain with their standard base and structure. But for some terrain, you might want a different base, or to forego the cane entirely! This article covers it pretty well.
Many cane users decorate their canes! Stickers are incredibly common, and painting canes is relatively common as well! You'll also see people replacing the standard wrist strap with a personalized one, or even adding a small charm to the ring the strap connects to. (nothing too large, or it gets annoying as the cane is swinging around everywhere)

(my canes, for reference)
If your character uses a cane full time, then they might also have multiple canes that look different aesthetically to match their outfits!
When it comes to practical things outside of the cane, you reasonably only have one hand available while it's being used. Many people will hook their cane onto their arm or let it dangle on the strap (if they have one) while using their cane arm, but it's often significantly less convenient than 2 hands. But, if you need 2 hands, then it's either setting the cane down or letting it hang!
For this reason, optimizing one handed use is ideal! Keeping bags/items on the side of your free hand helps keep your items accessible.
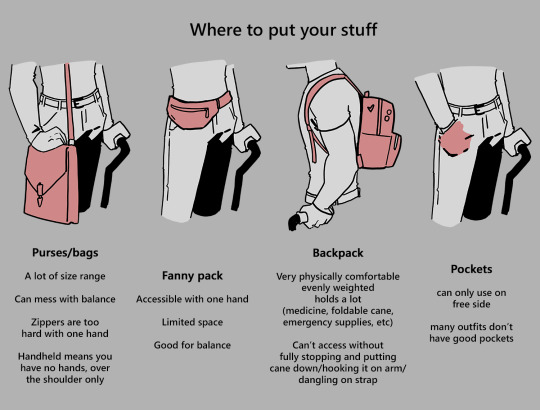
When sitting, the cane either leans against a wall or table, goes under the chair, or hooks onto the back of the chair. (It often falls when hanging off of a chair, in my experience)
When getting up, the user will either use their cane to help them balance/support as they stand, or get up and then grab their cane. This depends on what it's being used for (balance vs pain when walking, for instance!)
That's everything I can think of for now. Thank you for reading my long-but-absolutely-not-comprehensive list of things to keep in mind when writing or drawing a cane user!
Happy disability pride month! Go forth and make more characters use canes!!!
#mobility aid#cane user#writing tips#writing advice#drawing tips#art tutorial#art tips#art reference#art resources#art help#my art#long post
93K notes
·
View notes
Text
I found an extremely dope disability survival guide for those who are homebound, bedbound, in need of disability accommodations, or would otherwise like resources for how to manage your life as a disabled person. (Link is safe)
It has some great articles and resources and while written by people with ME/CFS, it keeps all disabilities in mind. A lot of it is specific to the USA but even if you're from somewhere else, there are many guides that can still help you. Some really good ones are:
How to live a great disabled life- A guide full of resources to make your life easier and probably the best place to start (including links to some of the below resources). Everything from applying for good quality affordable housing to getting free transportation, affordable medication, how to get enough food stamps, how to get a free phone that doesn't suck, how to find housemates and caregivers, how to be homebound, support groups and Facebook pages (including for specific illnesses), how to help with social change from home, and so many more.
Turning a "no" into a "yes"- A guide on what to say when denied for disability aid/accommodations of many types, particularly over the phone. "Never take no for an answer over the phone. If you have not been turned down in writing, you have not been turned down. Period."
How to be poor in America- A very expansive and helpful guide including things from a directory to find your nearest food bank to resources for getting free home modifications, how to get cheap or free eye and dental care, extremely cheap internet, and financial assistance with vet bills
How to be homebound- This is pretty helpful even if you're not homebound. It includes guides on how to save spoons, getting free and low cost transportation, disability resources in your area, home meals, how to have fun/keep busy while in bed, and a severe bedbound activity master list which includes a link to an audio version of the list on Soundcloud
Master List of Disability Accommodation Letters For Housing- Guides on how to request accommodations and housing as well as your rights, laws, and prewritten sample letters to help you get whatever you need. Includes information on how to request additional bedrooms, stop evictions, request meetings via phone, mail, and email if you can't in person, what you can do if a request is denied, and many other helpful guides
Special Laws to Help Domestic Violence Survivors (Vouchers & Low Income Housing)- Protections, laws, and housing rights for survivors of DV (any gender), and how to get support and protection under the VAWA laws to help you and/or loved ones receive housing and assistance
Dealing With Debt & Disability- Information to assist with debt including student loans, medical debt, how to deal with debt collectors as well as an article with a step by step guide that helped the author cut her overwhelming medical bills by 80%!
There are so many more articles, guides, and tools here that have helped a lot of people. And there are a lot of rights, resources, and protections that people don't know they have and guides that can help you manage your life as a disabled person regardless of income, energy levels, and other factors.
Please boost!
#signal boost#please reblog#I'm so so glad this has gotten the traction that it has!#chronic pain#chronic illness#disability#fibromyalgia#cfs#chronic fаtiguе ѕуndrоmе#actually disabled#spoonie#me/cfs#cfs/me#long covid#important#invisible disability#ehlers danlos syndrome#lyme disease#chronically ill#cpunk#cripplepunk#it's a bummer that it's so US centric but if you're outside of the US you can look into similar programs#I hope that other countries have options like these#the US seems so behind when it comes to medical care and disability resources. and i mean it is#but it's good to know all of your rights as a disabled person or if you ever become disabled
24K notes
·
View notes
Text
LaDS Men React To An Unexpected Pregnancy

AN: Pregnant reader. Not the boys. That genre is currently unexplored on this blog but not for long 🤭👺
Pairing: LaDS boys x Fem reader
Ingredients: 75% fluff, 25% angst.
My Fav: Rafayel's (new segment because I want to discuss which ones I liked best when writing)

Xavier:
You pass out during a mission. That’s how you find out. In the Hunter Association’s medical ward, you stare at the positive report in stunned silence.
The nausea hadn’t just been Xavier’s cooking.
How even…? You sit there, frozen, until he walks in, finding you pale and unmoving.
A child.
He leans against the wall, the report in his hand. God.
He had vanished the day he found out. Left you bitterly alone. But you didn’t need him, you could raise the child on your own. If Xavier was too weak to accept the truth, so be it.
But he returns. You don’t know where he went, only that when he comes back, he is broken.
"I couldn't change it." He falls to his knees. "The world remains unchanged," he repeats, voice hollow.
The destruction he had accepted, the grief he had worn like armor, now, it becomes unbearable. Because for the first time, he isn’t sure if he can ever manage to save it for his child.
Rafayel:
He dreams of it. Strange dreams.
He’s not one to obsess over omens, but even he, in his eternal wisdom, cannot decipher what a colony of seals playing with marbles is supposed to mean.
Then, one afternoon, he dreams of a baby seal. It coos at him, glumphing closer, making infant-like noises.
And in the dream, he bends down to pet it. Only for you to pick it up instead.
He jolts awake. Hands immediately over his stomach. Breath unsteady. No...not him...it was you. You picked the seal, that meant-
Then he stumbles out of bed, nearly tripping over himself in his rush to find you.
Drives like a madman. He counts the days. Two months. He counts the signs.
His heart refuses to slow down.
Barging into the Hunter’s Association, he’s chased by guards, by an exasperated receptionist, but none of it matters.
When he finds you, he grips your shoulders, searching your face. How could he have missed it?
By the tides, he was a fool.
And then—he feels it. A whisper, warm and murmuring, like the gentle pull of the waves.
A half-formed yawn, ringing softly in his mind.
The presence of his child.
Now all he has to do is tell you.
Zayne:
You watch Zayne eat dinner, half-listening as he talks about his day. He absentmindedly bites into another baby carrot.
Not just baby carrots, baby corn, baby potatoes, those tiny tomatoes.
"How’s dinner, Zayne?" you ask, feigning nonchalance.
He nods, smiling. "It’s good. Very healthy."
"Notice anything?"
He hums in thought. "You’re trying Italian cuisine these days." He places his hand over yours, gentle. "But you don’t have to cook if you’re tired after work."
He’s too kind to mention the small incident with the oven last week. To be fair, the bun in the oven analogy is a classic.
A week. A whole week of hints, and still, he hasn’t caught on.
Sighing, you give up on subtlety. "Darling, did you visit the pediatrics ward today?" you ask, pushing food around your plate.
"I didn’t have time. Had to miss the volunteering event for surgery."
You grin. Taking his hand, you guide it over your stomach. "Well, luckily for you, we’ll have one right here soon."
His mouth hangs open. Eyes darting between you and your stomach before his fingers brush over the nonexistent bump.
"Really? Are we—"
"Yes, you dummy!" You pull him into a hug. "I’ve been trying to tell you for days."
For a man obsessed with your health, he somehow had been ignorant of the biggest of surprises. Unplanned or not, you were going to give him the longest late night shift of his life.
Sylus:
The timing could have been better, he muses, wiping blood off his cheek.
But he had been too lax.
Not that it mattered. Everything was under control.
"Clean up," he orders, snapping his fingers. Shadows slither forward, dragging the remains of his enemies into the abyss.
The news of a child had changed things. He had let fate play its part for too long. Now, it was his turn.
Whatever slow-moving scheme he had let linger, ended now.
There was no way in hell he was letting you go on any mission while carrying his child.
Aether Core be damned. EVER be damned to NEVER. He would wipe them out if he had to.
For now, though, he had other priorities.
Leaving you safe at home, he finishes this last errand. Your only battle at the moment is morning sickness which, much to his surprise, isn’t just limited to mornings.
He wipes his hands clean, heading for his bike.
One last stop. You wanted pickles.
He smiles, revving the engine. Soon, only cars.
And then, he’s gone, speeding into the night, back to you. Back to his family. To cuddle the little dragon who gives you unrivaled heartburn and kicks like a menace at 18 weeks.
Caleb:
He knew.
Some would say he saw it coming, but just because he kept track of your cycle didn’t mean he could predict your ovulation exactly.
He was just…good at math.
Mental math.
And taking you to a convenience store for cough drops, right next to the pregnancy tests, had been pure coincidence.
Not that he totally snuck a glance at you eyeing them. And if he excused himself to grab a snack right then? Also not planned.
You hand him the test. "I think I’m pregnant."
He goes through all the expressions shock, surprise, joy, tears. So dramatic that it fools no one.
Seriously, he’s atrocious at being subtle about it.
Instantly proposes. Shotgun wedding because the baby will need a family.
Grins like a madman when it turns out to be twins.
Secretly, he’s very, very proud.
Heavens, he thinks smugly, I really am amazing at math.
#love and deepspace#love and deepspace sylus#love and deepspace caleb#love and deepspace headcannon#love and deepspace x reader#sylus x reader#xavier x reader#rafayel x reader#zayne x reader#zayne love and deepspace#caleb x reader#fluff#love and deepspace reaction#fem reader#pov caleb grows concerning with every piece i write
4K notes
·
View notes
Text
The Anatomy of Passing Out: When, Why, and How to Write It

Passing out, or syncope, is a loss of consciousness that can play a pivotal role in storytelling, adding drama, suspense, or emotional weight to a scene. Whether it’s due to injury, fear, or exhaustion, the act of fainting can instantly shift the stakes in your story.
But how do you write it convincingly? How do you ensure it’s not overly dramatic or medically inaccurate? In this guide, I’ll walk you through the causes, stages, and aftermath of passing out. By the end, you’ll be able to craft a vivid, realistic fainting scene that enhances your narrative without feeling clichéd or contrived.
2. Common Causes of Passing Out
Characters faint for a variety of reasons, and understanding the common causes can help you decide when and why your character might lose consciousness. Below are the major categories that can lead to fainting, each with their own narrative implications.
Physical Causes
Blood Loss: A sudden drop in blood volume from a wound can cause fainting as the body struggles to maintain circulation and oxygen delivery to the brain.
Dehydration: When the body doesn’t have enough fluids, blood pressure can plummet, leading to dizziness and fainting.
Low Blood Pressure (Hypotension): Characters with chronic low blood pressure may faint after standing up too quickly, due to insufficient blood reaching the brain.
Intense Pain: The body can shut down in response to severe pain, leading to fainting as a protective mechanism.
Heatstroke: Extreme heat can cause the body to overheat, resulting in dehydration and loss of consciousness.
Psychological Causes
Emotional Trauma or Shock: Intense fear, grief, or surprise can trigger a fainting episode, as the brain becomes overwhelmed.
Panic Attacks: The hyperventilation and increased heart rate associated with anxiety attacks can deprive the brain of oxygen, causing a character to faint.
Fear-Induced Fainting (Vasovagal Syncope): This occurs when a character is so afraid that their body’s fight-or-flight response leads to fainting.
Environmental Causes
Lack of Oxygen: Situations like suffocation, high altitudes, or enclosed spaces with poor ventilation can deprive the brain of oxygen and cause fainting.
Poisoning or Toxins: Certain chemicals or gasses (e.g., carbon monoxide) can interfere with the body’s ability to transport oxygen, leading to unconsciousness.
3. The Stages of Passing Out
To write a realistic fainting scene, it’s important to understand the stages of syncope. Fainting is usually a process, and characters will likely experience several key warning signs before they fully lose consciousness.
Pre-Syncope (The Warning Signs)
Before losing consciousness, a character will typically go through a pre-syncope phase. This period can last anywhere from a few seconds to a couple of minutes, and it’s full of physical indicators that something is wrong.
Light-Headedness and Dizziness: A feeling that the world is spinning, which can be exacerbated by movement.
Blurred or Tunnel Vision: The character may notice their vision narrowing or going dark at the edges.
Ringing in the Ears: Often accompanied by a feeling of pressure or muffled hearing.
Weakness in Limbs: The character may feel unsteady, like their legs can’t support them.
Sweating and Nausea: A sudden onset of cold sweats, clamminess, and nausea is common.
Rapid Heartbeat (Tachycardia): The heart races as it tries to maintain blood flow to the brain.
Syncope (The Loss of Consciousness)
When the character faints, the actual loss of consciousness happens quickly, often within seconds of the pre-syncope signs.
The Body Going Limp: The character will crumple to the ground, usually without the ability to break their fall.
Breathing: Breathing continues, but it may be shallow and rapid.
Pulse: While fainting, the heart rate can either slow down dramatically or remain rapid, depending on the cause.
Duration: Most fainting episodes last from a few seconds to a minute or two. Prolonged unconsciousness may indicate a more serious issue.
Post-Syncope (The Recovery)
After a character regains consciousness, they’ll typically feel groggy and disoriented. This phase can last several minutes.
Disorientation: The character may not immediately remember where they are or what happened.
Lingering Dizziness: Standing up too quickly after fainting can trigger another fainting spell.
Nausea and Headache: After waking up, the character might feel sick or develop a headache.
Weakness: Even after regaining consciousness, the body might feel weak or shaky for several hours.
4. The Physical Effects of Fainting
Fainting isn’t just about losing consciousness—there are physical consequences too. Depending on the circumstances, your character may suffer additional injuries from falling, especially if they hit something on the way down.
Impact on the Body
Falling Injuries: When someone faints, they usually drop straight to the ground, often hitting their head or body in the process. Characters may suffer cuts, bruises, or even broken bones.
Head Injuries: Falling and hitting their head on the floor or a nearby object can lead to concussions or more severe trauma.
Scrapes and Bruises: If your character faints on a rough surface or near furniture, they may sustain scrapes, bruises, or other minor injuries.
Physical Vulnerability
Uncontrolled Fall: The character’s body crumples or falls in a heap. Without the ability to brace themselves, they are at risk for further injuries.
Exposed While Unconscious: While fainted, the character is vulnerable to their surroundings. This could lead to danger in the form of attackers, environmental hazards, or secondary injuries from their immediate environment.
Signs to Look For While Unconscious
Shallow Breathing: The character's breathing will typically become shallow or irregular while they’re unconscious.
Pale or Flushed Skin: Depending on the cause of fainting, a character’s skin may become very pale or flushed.
Twitching or Muscle Spasms: In some cases, fainting can be accompanied by brief muscle spasms or jerking movements.
5. Writing Different Types of Fainting
There are different types of fainting, and each can serve a distinct narrative purpose. The way a character faints can help enhance the scene's tension or emotion.
Sudden Collapse
In this case, the character blacks out without any warning. This type of fainting is often caused by sudden physical trauma or exhaustion.
No Warning: The character simply drops, startling both themselves and those around them.
Used in High-Tension Scenes: For example, a character fighting in a battle may suddenly collapse from blood loss, raising the stakes instantly.
Slow and Gradual Fainting
This happens when a character feels themselves fading, usually due to emotional stress or exhaustion.
Internal Monologue: The character might have time to realize something is wrong and reflect on what’s happening before they lose consciousness.
Adds Suspense: The reader is aware that the character is fading but may not know when they’ll drop.
Dramatic Fainting
Some stories call for a more theatrical faint, especially in genres like historical fiction or period dramas.
Exaggerated Swooning: A character might faint from shock or fear, clutching their chest or forehead before collapsing.
Evokes a Specific Tone: This type of fainting works well for dramatic, soap-opera-like scenes where the fainting is part of the tension.
6. Aftermath: How Characters Feel After Waking Up
When your character wakes up from fainting, they’re not going to bounce back immediately. There are often lingering effects that last for minutes—or even hours.
Physical Recovery
Dizziness and Nausea: Characters might feel off-balance or sick to their stomach when they first come around.
Headaches: A headache is a common symptom post-fainting, especially if the character hits their head.
Body Aches: Muscle weakness or stiffness may persist, especially if the character fainted for a long period or in an awkward position.
Emotional and Mental Impact
Confusion: The character may not remember why they fainted or what happened leading up to the event.
Embarrassment: Depending on the situation, fainting can be humiliating, especially if it happened in front of others.
Fear: Characters who faint from emotional shock might be afraid of fainting again or of the situation that caused it.
7. Writing Tips: Making It Believable
Writing a fainting scene can be tricky. If not handled properly, it can come across as melodramatic or unrealistic. Here are some key tips to ensure your fainting scenes are both believable and impactful.
Understand the Cause
First and foremost, ensure that the cause of fainting makes sense in the context of your story. Characters shouldn’t pass out randomly—there should always be a logical reason for it.
Foreshadow the Fainting: If your character is losing blood, suffering from dehydration, or undergoing extreme emotional stress, give subtle clues that they might pass out. Show their discomfort building before they collapse.
Avoid Overuse: Fainting should be reserved for moments of high stakes or significant plot shifts. Using it too often diminishes its impact.
Balance Realism with Drama
While you want your fainting scene to be dramatic, don’t overdo it. Excessively long or theatrical collapses can feel unrealistic.
Keep It Short: Fainting typically happens fast. Avoid dragging the loss of consciousness out for too long, as it can slow down the pacing of your story.
Don’t Always Save the Character in Time: In some cases, let the character hit the ground. This adds realism, especially if they’re fainting due to an injury or traumatic event.
Consider the Aftermath
Make sure to give attention to what happens after the character faints. This part is often overlooked, but it’s important for maintaining realism and continuity.
Lingering Effects: Mention the character’s disorientation, dizziness, or confusion upon waking up. It’s rare for someone to bounce back immediately after fainting.
Reactions of Others: If other characters are present, how do they react? Are they alarmed? Do they rush to help, or are they unsure how to respond?
Avoid Overly Romanticized Fainting
In some genres, fainting is used as a dramatic or romantic plot device, but this can feel outdated and unrealistic. Try to focus on the genuine physical or emotional toll fainting takes on a character.
Stay Away from Clichés: Avoid having your character faint simply to be saved by a love interest. If there’s a romantic element, make sure it’s woven naturally into the plot rather than feeling forced.
8. Common Misconceptions About Fainting
Fainting is often misrepresented in fiction, with exaggerated symptoms or unrealistic recoveries. Here are some common myths about fainting, and the truth behind them.
Myth 1: Fainting Always Comes Without Warning
While some fainting episodes are sudden, most people experience warning signs (lightheadedness, blurred vision) before passing out. This gives the character a chance to notice something is wrong before losing consciousness.
Myth 2: Fainting Is Dramatic and Slow
In reality, fainting happens quickly—usually within a few seconds of the first warning signs. Characters won’t have time for long speeches or dramatic gestures before collapsing.
Myth 3: Characters Instantly Bounce Back
Many stories show characters waking up and being perfectly fine after fainting, but this is rarely the case. Fainting usually leaves people disoriented, weak, or even nauseous for several minutes afterward.
Myth 4: Fainting Is Harmless
In some cases, fainting can indicate a serious medical issue, like heart problems or severe dehydration. If your character is fainting frequently, it should be addressed in the story as a sign of something more severe.
Looking For More Writing Tips And Tricks?
Are you an author looking for writing tips and tricks to better your manuscript? Or do you want to learn about how to get a literary agent, get published and properly market your book? Consider checking out the rest of Quillology with Haya Sameer; a blog dedicated to writing and publishing tips for authors! While you’re at it, don’t forget to head over to my TikTok and Instagram profiles @hayatheauthor to learn more about my WIP and writing journey!
#hayatheauthor#haya's book blog#haya blogs#writing community#quillology with haya#writing tools#writer things#writing advice#writer community#writing techniques#writing prompt#writing stuff#creative writing#ya writing advice#writing tips and tricks#writer tools#writers of tumblr#writer blog#writers block#quillology with haya sameer#writers on tumblr#writerscommunity#writer stuff#author help#author advice#author#writing inspiration#writeblr#novel writing#on writing
6K notes
·
View notes
Text
hello hi i’m making writing guides on injuries in an emergency setting is there anything specific y’all might wanna see? i work in a pre hospital setting so i’m not writing anything pertaining to in hospital care.
#writing tips#writing guide#medical writing guide#medical writing tips#trauma writing tips#trauma writing guide#pls y’all let me give you knowledge some medical inaccuracies y’all write is driving me insane#pls#pls pls#ear’s guide to writing
17 notes
·
View notes
Text
A Humanitarian Appeal from the Depths of Suffering🥹:
The War on Gaza, Our Losses, and the Struggles We Endure



In these difficult and painful times😔, I find it hard to find words that truly express the depth of the suffering I, 💔😓
along with my family, am going through. I am writing this message from a place of desperation and need, as a doctor working in a hospital in Gaza. Life here has become a constant battle for survival, and each day brings new challenges that test our will to continue😭.



We were once living a peaceful and stable life🙂, building our hopes and dreams😥, working towards a future for ourselves and our loved ones🥺.
However, the recent war on Gaza has turned our world upside down😢. I have lost my job💔,
and with it, my only source of income, due to the destruction of the facilities where I worked😭.
The physical destruction around us has been devastating😓, and many projects I was involved in to support the families of patients have come to a halt😢. The economic losses are staggering, and the road to recovery seems almost impossible😥.


The war on Gaza has not only taken our peace of mind but has also brought with it an unbearable level of suffering😓.
The cost of living has skyrocketed,
and we are struggling to meet even the most basic needs of daily life😣.
The situation has become unbearable, and it feels like we’re trapped in a vicious cycle of poverty, fear, and despair.
How can a family survive when they cannot even afford food, let alone the necessities of life?😭😥💔
As a doctor, I stand at the frontline, trying to save lives amidst the wreckage of war😢.
I treat the injured, manage critical cases, and do my best to bring comfort to those who need it most. 🥹
However, at the same time, I face personal struggles that are just as overwhelming😢. The hospital is in dire need of medical supplies and personnel, and we are doing all we can to save lives with limited resources. But the pain of seeing my own family suffering while I try to help others is a constant burden.
How can I help those in need when I cannot even provide for my loved ones?😣😣


Today, as I face this immense struggle😔,
I turn to you, dear reader, with a plea for help🙏🏻😥.
This is not just a request for personal assistance🙏🏻🥹, but a desperate call for hope and a chance to rebuild my life and support my family.
I need your help to share my story😓, so that it reaches as many people as possible.
Your support, through donations and sharing this story, will allow me to help my family escape the horrors of war and start a new life abroad, where we can live in safety and dignity🙏🏻🥹❤️.
I need the resources to travel abroad to continue my education l😔and provide a future for my family🙏🏻😓. Pursuing my studies and advancing my career in medicine is my way of ensuring that I can make a lasting difference, both for myself and for the people of Gaza. But I cannot do this alone.
The funds I am seeking will help me cover travel expenses, medical costs for my family, and the basic needs that we are struggling to meet each day😥.

The financial burden is overwhelming😭,
and without your support, I fear that my dreams, and the future of my family, will slip further out of reach😥😭💔.
Every donation, no matter how small, will make a difference.
Every act of kindness, every person who shares this message, will help light the way for us in this dark time🙏🏻😢.
I humbly ask you to help me spread this story. Share this story with your friends, family, and networks. Let it reach those who have the means and the will to help🥹🥺❤️.
Together, we can make a difference. Your kindness, your generosity, and your willingness to stand by us will mean the world💝🥹🙏🏻.


In these dark times, solidarity is the light that can guide us😔💔. Your support is not just an act of charity; it is an act of humanity❤️❤️.
You are not only helping an individual, but you are also supporting a family in dire need of hope and a better future😃❤️.
I will forever be grateful for any assistance you can provide, whether it’s a financial contribution, sharing this story, or offering a kind word of encouragement.
Your help will give us the strength to continue, and it will remind us that in the midst of all this suffering, there is still hope, there is still kindness, and there are still people who care😃❤️.

Thank you, from the bottom of my heart❤️❤️, for your time, your attention, and your compassion.
Together, we can create a future where we can live with dignity, rebuild what has been lost😔, and give our children the hope they deserve💝🥹🙏🏻.
Solidarity is Hope, and Helping is Life💚❤️💛🖤🇵🇸 .
vetted by \
@90-ghost (number 212)
@mangocheesecakes ,
@sayruq
@el-shab-hussein
@nabulsi
#free palestine#palestine#free gaza#palestine news#gaza genocide#palestine genocide#gaza#i stand with palestine#palestinian genocide#viva palestina#long live palestine#all eyes on palestine#free palastine#palestine will be free#end the genocide#stop the genocide#genocide#gofundme gaza#gofundme#gaza news#gaza strip#gazaunderattack#free free gaza#help palestine#pray for palestine#support palestine#strike for palestine#save palestine#palestinians#free plaestine
3K notes
·
View notes
Text
this is a new post being made for ammar @ammarfamily2 as i checked the post i had been using and it has now been flagged as "potentially mature content". out of concern for this possibly suppressing pings, i have made this one instead.
the below text is copy pasted from the previous
samah’s original campaign and account are shared by 90-ghost, but it was shut down as her organiser’s bank account was deactivated
proof samah asked me to use my paypal / ko-fi account here
unfortunately ammar needs some medication to make sure he is well after the operation he had 3 days ago - namely, he needs painkillers and antibiotics
samah has told me that it is going to cost $1263 for his post-surgery care - because she will have to pay 20% fees to get this money to her, i have it up as $1600.
his condition without having immediately received the post-surgery medication already worsened enough that he had to return to intensive care last night
in 3 days he has had surgery, left the hospital, and failed to receive the medication needed to keep him well after the surgery, then became ill enough to go back to the hospital.
we truly do not have enough time and i worry for him, please let's do what we can for him
$766 / $1600
let me know for ping removal
@shikse @gh4ul @sundung @fandom-master-mind @aconstantallegory
@proffittproductions @romdocitizen @knownoshamc @the-awkward-reblobber @peachyleechy
@soft-sunbird @dannyketch @cramenjoyer @oreobunny2 @soopertiddies
@inthecornerofyourbedroom @aurorae-return @spindly-counting @depressedthembo @moronicprincess
@the-mold-under-your-bed123 @nyenyel @linz-creations @we-eat-our-young @koscheiy
@cyclopsboxhead @iactuallytryingtolovemyself @kyoukris @thepurevessel1 @birdsbeesknees
@meadow-sea @divortion @skricrich-yellowtooth @brotherblasphemous @bisexuel
@something-writing @lgbtiqrefugeesblog @blvvdyindustries @morelinesandscribbles @danielladadasworld
@wellsbering @tolbachik @superdragonjpeg-thing @afropiscesism @ihavenotfallenyet
@fly-sky-high-09 @cherry-shrimp @insanitysmiles @wirehairwiredstare @everypores
@fantasynovel @ohlorde @theinconvenientlifestyle @sea-shame @faacethefacts
@buttfacemcgee @craigthetourguide @blomstermjuk @mythiedew @springacres
@thatonetreetho @milanesa-enthusiast @tacit-semantics @3lawzdef1ant @fiapple
@pupindaturd @playthemz @yourlocalamoeba @bi0lizard @leovaldeeeznuts
@my-little-resource-guide @moremorehino @utane-uta-town @avvrat @zuzecadyke
@gayos-emerald @manisthebastard @elidoesdumb2 @spooperdedooper @neoneone0
@gingerweed-man @rhymeswithpurple9 @funkworms @fantasykiri5 @autechres
@kneecapremover @esrah-rah-rasputin @pandycake-blog @soupygremlin @kurtwagnermorelikekurtwagnerd
@smilepilled @321butz @monika-396 @erameteors @rosawo7
@lindacube @fluoresensitivearchived @rhmis-user-2020 @jonesthebonelord @lordmimi
@choccybug @rubitheracoon @theprotagonistisdead @roseyange @yourlocaldreamrgirl
@sayhellotosomethingscary @a-sky-of-diamonds @yeahhiyellow @flowerkith
@mbookcovers @dorawnfredread @mysticfandeer @anarchafemme @missgirlsthings
@junipersramblings @chronicsheepdeprivation @win-rrar @shizukateal @queerlyblack
@hexxeh @knavewoods @katherinefh @variouscontent @thelorewriter-inator
@galaxy-of-great-possibilities @vor765wm @brain-cel @voidlesslove @onlineengima
@metal-king-slime @seraphalpha @maidthings @mxwhore @inkskinned
#free palestine#free gaza#palestine#gaza strip#all eyes on palestine#mutual aid#all eyes on gaza#gaza fundraiser#gazaunderattack#gaza gofundme#war on gaza#stand with gaza#gaza aid
2K notes
·
View notes
Text
weather the storm
dr. jack abbot x female!wife!reader

wc: 1.8k
summary: you take you and jack's son to the er in the middle of the night when he's sick, but your marriage happens to be on the rocks atm
warnings: reader and jack have 11 year old son, medical inaccuracies, mentions of marital differences/separation, mentions of surgery/medical procedures, established relationship, light angst but happy ending, not canonically accurate, reader has her dogs out
a/n: i don't know why i'm struggling so bad to characterize/write for abbot but i hope this does him justice. i def think he's more goofy in the show but this is a more sensitive situation so idk? i hope you like it okay!!! ugh!!!! i want to write sm more for him so maybe it will come easier to me
You were deep in sleep when you felt a familiar small hand grasp your shoulder. Your eyes shot open and you inhaled sharply as you sat up on your elbow. Your son’s face came into your weary vision. He was grasping your arm and bent over the bed, a distressed look on his face.
“Mom.” He spoke in a pained whisper.
“Benjamin?” You blink and clear your eyes, anxiety skyrocketing at the sight of Jack and your son’s form. You grab onto his arm that’s gripping your body and squeeze. “What’s wrong? Are you hurt?”
His voice is soft and broken, “My side. My side really hurts.”
You sit up immediately and push the covers back. “Your side?”
You run your hands over his arms and move the one that’s covering his midsection, lifting his pajama top. It looks normal to the eye.
“Here?” You place a gentle hand on him.
He nods, grimacing.
You curse under your breath and stand, guiding Ben to sit on the edge of your mattress. It’s definitely his appendix and you’re praying to yourself it hasn’t ruptured.
You grab your phone off the nightstand. “You’re okay, baby.” You reassure him as you dial Jack’s number.
You know it’s a shot in the dark. Jack was working an overnight shift again and you had been separated for two months now. Your marriage was one full of love and a deep connection to each other, but lately you’d been struggling. He’d been working nights full time and barely saw you. He tried to make time for Ben, which you appreciated, but it was a different story for you.
You started spending more time at work in his absence and found yourself desperate for his attention. And when you reached a breaking point you pushed him away. You two fought like you’d never fought before and things buried deep inside came to the surface. After the two of you cooled down, you spoke with a marriage counselor and a brief separation was suggested.
So, here you were. At home in the house you used to share, the bed that you still kept to your side of. Jack had gotten a small townhouse closer to the hospital and stopped by for the occasional dinner and to pick up Ben. But, as the phone rang you internally begged him to pick up, all drama aside.
You get his voicemail. Realistically, you know the ER can get chaotic at night, but you can’t help the curse that escapes again. You toss the phone down and grab your shoes from near the closet, the ones you swore you’d pick up days ago.
You help Ben move to the car, holding his groaning form up. You hide your fear and anxiety and whisper reassurances to him.
The dashboard reads 2:38 am as you drive the fastest and safest way you can to the hospital. You park and help your son to the familiar ED’s waiting room. It’s less busy than you would have thought, the night shift seeming to usually catch the weirdest cases.
The receptionist is one you recognize thankfully, and her eyes shoot up when she sees you and Ben.
“I think it’s his appendix.” Your voice shakes.
Ben leans into you, his eyes tearing. “Mom-”
“It’s okay. You’re okay. We’re here now.” You repeat.
The receptionist pages back and Dr. Ellis exits the locked doors with a nurse not a moment later.
“Abbot?” She uses your last name as she rushes over and assesses Ben’s state. The nurse follows with a wheelchair and she helps you sit Ben in it.
“I think it’s his appendix. Jack didn’t pick up and I have no idea if it’s ruptured-”
Ellis cuts off your rambling, “Don’t worry, we got him.”
You follow her as they put Ben in a room and start an IV. You step forward and run a hand over your son’s hair, trying to comfort him.
“Is Dad here?” He groans.
“He’s in Trauma 1.” Ellis answers, giving you a look as she pulls the ultrasound over.
“He’ll be here in a little, baby.”
Ben nods but drops his head back defeatedly.
Ellis moves closer to her boss’s son and speaks gently. “I’m going to lift your shirt and check out what’s going on, okay, kid?”
Ben nods and she puts the soft gel on the wand, moving it over his abdomen. She watches the screen and Ben holds onto your hand, wincing softly.
Ellis hums to herself, before placing the wand back and wiping your son’s side. “Good news is it’s not ruptured yet. I’m going to admit him to General Surgery and they’ll get him in pre-op.”
“He needs surgery?” You thought you’d heard of doctors being able to reverse appendicitis with medication.
She nods. “It’s pretty inflamed, I’m not sure the antibiotics would work in time to stop a rupture.”
“Okay, yeah, yeah. Thank you. Can- can you just get Jack when you have a chance?” You know he’s working and you’re not in the best place but you want him here.
“Of course.” She takes a moment to explain what’s going on to Ben before exiting. You sit on the edge of the mattress and squeeze Ben’s hand, trying to soothe him.
Jack had been in Trauma 1 when you had entered the ER. A GSW had come in through the ambulance bay and the patient was critical. He had spent the first 10 minutes coding him, then working to stabilize him enough to send him up to the OR.
When he finally exited and shoved off his gown, exhaling a deep sigh, he wasn’t in the mood to find out why Ellis was moving towards him in such a grim way.
He went to glance up at the board but Ellis’ tone caught him off guard.
“Dr. Abbot,” Her inhale was shaky, “Your son is in South 15.”
His world stopped. His years of training and education abandoned him in that singular moment. “What?” His voice was barely audible.
“Your wife brought him in, looks like appendicitis. It’s inflamed and I don’t think there’s time for antibiotic treatment. He’s getting prepped for General Surgery-” He didn’t stay to hear her finish. His movements were controlled but hurried as he moved to the curtain he would find you behind.
He shoved the curtain back and took in the scene before him. You were sitting on the small hospital bed, still in your tank top, striped pajama pants, and familiar worn flip-flops you’d had since before Ben was even born. You were whispering soft words to your son. Your son, whose face was scrunched up and who was lying back in a hospital gown, IV dripping into his arm.
You turned at the curtain’s movement and sighed deeply in relief. Ben glanced up.
“Dad.”
Jack was by his side in an instant. “You okay, buddy? What happened?”
You stood and watched Jack run his hand over Ben’s hair, pushing the curls he’d inherited from the man back.
Ben spoke softly, “My side started hurting, it woke me up. I woke Mom up and she brought me here.”
“I tried to call. I got here as quick as I could-” You continued.
“You did everything right.” Jack nodded, his voice soft and eyes firm.
He grabbed a pair of gloves from the box on the wall and pulled the ultrasound machine back over.
You knew he trusted Ellis and her professional opinion, but he also wanted to make sure his son was okay for himself.
Ben laid back as his dad examined his abdomen. You ran a hand over your bedhead and watched Jack shift into the all too familiar doctor he was. His expression unreadable, his movements precise.
He wiped the machine and his son’s stomach before speaking, “You’ll be okay, kid. One less appendix for you.” He smirked, winking at the young boy.
Ben smiled weakly at his dad and you let out the breath you’d been holding. Hearing that everything would be okay from Jack was the most reassurance you could get at that moment.
A few more nurses came in, giving Jack sympathetic glances and prepping Ben to head to the OR. When Ellis came back in and gave the all good, you pressed a long kiss to your son’s head. Jack squeezed his hand and whispered ‘I love yous’ in his ear. You watched as they wheeled him towards the elevator.
You knew he would be okay and that he was in the best hands, but your eyes watered. The night was catching up with you. A sob wracked through you and Jack watched your shoulders shake.
He stepped close behind you, his hands finding your shoulders and his mouth pressing a soft kiss to your head.
“It’s okay.” His voice was quiet and that was all you needed to let the tears fall.
Turning in his arms, you fell into his chest. His familiar hands, rough and calloused, wrapped around your crying form and his head came to rest on yours.
It was overwhelming. Ben needing surgery in the middle of the night and Jack not being there next to you to know or help. You let yourself cry for a while, before pulling back. You said nothing as you let Jack lead you to the elevator.
He kept his arm around you as you moved to the surgical floor. He sat with you in the waiting room, even finding a PTMC hoodie to wrap around your shoulders. He didn’t push you. He let you lean on him and intertwine your fingers with his.
“Do you need to go back down to the ER?” You sniffle, head on his shoulder.
“Shen can manage. I told him to page me only if there’s an emergency. I’m not going anywhere.” He squeezed your hand.
You lift your head and his eyes meet yours, serious and soft.
“I’m sorry,” you start, “about everything. Tonight- the whole night, I just kept wishing you were there with me. That I didn’t have to worry about calling or you being across town if something happened.”
A tear escapes as you continue, “I don’t like this. Not knowing where we stand. It’s killing me. I miss you, Jack. All the time.”
His face contorts in emotion and he swallows before responding in that soft tone of his. “I miss you too. All the time. I’m sorry, baby. I thought- I thought this would help. That you’d feel better away from me.”
Your head shakes and a few more tears fall. “I don’t, I don’t. I want you to come home.”
His thumb catches your tears as he takes in your words. His touch is soft and casual, a motion you’d found comfort in for years.
His jaw visibly clenches and his nod is firm, but it carries the emotion you know he’s feeling. “I want that, too. I want you, Ben, all of us together.”
“Together.” You repeat and clutch his hand tighter.
He pulls you into his arms and you let him. You fall into him for the first time in months with no second guesses. No imaginary lines being crossed.
You feel his lips graze your hairline and you pull back slightly, hands cupping his face. His lips find yours easily and it feels brand new again. Your heart full and your mind at ease.
“We’ll be okay.” His words wrap around you like his arms and you know in all certainty they’re true.
#jack abbot#dr jack abbot#jack abbot x reader#jack abbot x you#jack abbot x female reader#jack abbot fanfic#the pitt#the pitt hbo#the pitt fanfiction#the pitt x reader#jack abbott#my fics#do not copy#not my gif
1K notes
·
View notes
Text
I'm getting depressingly good at identifying the formula for Pop Academic Books About ADHD.
Regardless of their philosophy it pretty much goes like this:
1. Emotionally sensitive essay about the struggle of ADHD and the author's personal experience with it as both a person with ADHD and a healthcare professional.
2. Either during or directly following this, a lightly explicated catalogue of symptoms, illustrated by anecdotes from patient case studies. Optional: frequent, heavy use of metaphor to explain ADHD-driven behavior.
3. Several chapters follow, each dedicated to a symptom; these have a mini-formula of their own. They open with a patient case study, discuss the highly relatable aspects of the specific symptom or behavior, then offer some lightweight examples of a treatment for the symptom, usually accompanied by follow up results from the earlier case studies.
4. Somewhere around halfway-to-two-thirds through the book, the author introduces the more in-depth explication of the treatment system (often their own homebrew) they are advocating. These are generally both personally-driven (as opposed to suggested cultural changes, which makes sense given these books' target audience, more on this later) and composed of an elaborate system of either behavior alteration or mental reframing. Whether this system is actually implementable by the average reader varies wildly.
5. A brief optional section on how to make use of ADHD as a tool (usually referring to ADHD or some of its symptoms as a superpower at least once). Sometimes this section restates the importance of using the systems from part 4 to harness that superpower. Frequently, if present, it feels like an afterthought.
6. Summation and list of further resources, often including other books which follow this formula.
I know I'm being a little sarcastic, but realistically there's nothing inherently wrong about the formula, like in itself it's not a red flag. It's just hilariously recognizable once you've noticed it.
It makes sense that these books advocate for the Reader With ADHD undertaking personal responsibility for their treatment, since these are in the tradition of self-help publishing. They're aimed at people who are already interested in doing their own research on their disability and possible ways to handle it. It's not really fair to ask them to be policy manuals, but I do find it interesting that even books which advocate stuff like volunteering (for whatever reason, usually to do with socialization issues and isolation, often DBT-adjacent) never suggest disability activism either generally or with an ADHD-specific bent.
None of these books suggest that perhaps life with ADHD could be made easier with increased accommodations or ease of medication access, and that it might be in a person's best interest to engage in political advocacy surrounding these and other disability-related issues. Or that activism related to ADHD might help to give someone with ADHD a stronger sense of ownership of their unique neurology. Or that if you have ADHD the idea of activism or even medical self-advocacy is crushingly stressful, and ways that stress might be dealt with.
It does make me want to write one of my own. "The Deviant Chaos Guide To Being A Miscreant With ADHD". Includes chapters on how to get an actual accurate assessment, tips for managing a prescription for a controlled substance, medical and psychiatric self-advocacy for people who are conditioned against confrontation, When To Lie About Being Neurodivergent, policy suggestions for ADHD-related legislation, tips for activism while executively dysfunked, and to close the book a biting satire of the pop media idea of self-care. ("Feeling sad? Make yourself a nice pot of chicken soup from scratch and you'll feel better in no time. Stay tuned after this rambling personal essay for the most mediocre chicken soup recipe you've ever seen!" "Have you considered planning and executing an overly elaborate criminal heist as a way to meet people and stay busy?")
Every case study or personal anecdote in the book will have a different name and demographics attached but will also make it obvious that they are all really just me, in the prose equivalent of a cheap wig, writing about my life. "Kelly, age seven, says she struggles to stay organized using the systems neurotypical children might find easy. I had to design my own accounting spreadsheet in order to make sure I always have enough in checking to cover the mortgage, she told me, fidgeting with the pop socket on her smartphone."
I feel a little bad making fun, because these books are often the best resource people can get (in itself concerning). It's like how despite my dislike of AA, I don't dunk on it in public because I don't want to offer people an excuse not to seek help. It feels like punching down to criticize these books, even though it's a swing at an industry that is mainly, it seems, here to profit from me. But one does get tired of skimming the hype for the real content only to find the real content isn't that useful either.
Les (not his real name) was diagnosed at the age of 236. Charming, well-read, and wealthy, he still spent much of his afterlife feeling deeply inadequate about his perceived shortcomings. "Vampire culture doesn't really acknowledge ADHD as a condition," he says. "My sire wouldn't understand, even though he probably has it as well. You should see the number of coffins containing the soil of his homeland that he's left lying forgotten all over Europe." A late diagnosis validated his feelings of difference, but on its own can't help when he hyperfocuses on seducing mortals who cross his path and forgets to get home before sunrise. "I have stock in sunburn gel companies," he jokes.
6K notes
·
View notes
Text
MOONSTRUCK | p. jisung
pairing: werewolf!hufflepuff! jisung x hufflepuff!fem. reader genre: best friends to lovers, hogwarts/supernatural au, angst, smut. wc: 18.3k+ summary: after a cruel prank leaves jisung cursed, he withdraws from everyone—including you, his closest friend. but secrets can't stay hidden forever, and when a full moon pulls you into the darkness he's tried so desperately to conceal, there's no going back. content warnings: werewolf lore & transformation, drug usage, rut/mating behavior, rough sex, biting/marking, mild breeding kink, oral (f receiving), multiple orgasms, knotting, bulge kink, mentions of bruising & blood, mild body horror, brief medical talk (contraceptive), aftercare. lmk if i missed any! a/n: nearly a month in the making and i can finally say i’m satisfied enough to post this lol. i’m actually really happy with how it turned out—and i finally got to write about werewolves, which has been on my list forever. canonically, werewolves in the HP universe (and most lore tbh) are dangerous nocturnal creatures and primarily bloodthirsty. but for this fic, i took a step away from that and leaned into the rut aspect instead because why not ;) pls don’t judge the cover, i had picsart and a dream lol. btw moonstruck by enhypen and nda by billie eilish are two songs u should listen to while reading this!
ps: i don’t know why i was under the assumption that everyone knows hp terms but i realized that is not the case after my mark fic 😭 so even though i didn’t use too many obscure ones here, here’s a little reference guide just in case: legilimens– someone who can read minds or emotions squib– a non-magical person born into a magical family (in this fic, it’s thrown around more like calling someone useless/coward) wolfsbane– a potion that allows werewolves to keep their mind during a full moon; in hp lore they still transform, but in this fic it's not a full transformation. feel free to message me if anything else was confusing! happy reading<3

You didn’t expect your seventh year at Hogwarts to feel like grieving someone who was still alive.
Three months ago, Park Jisung was still your best friend. Now, he can’t even stand being near you.
The suddenness of this change was something you couldn’t wrap around your head. But things don’t always fall apart all at once. Sometimes they drift until you’re left staring across a room at someone who used to know everything about you and wondering when they became a stranger.
He was the very first friend you made at Hogwarts. You remember how he barely spoke to anyone, and you sat next to him in Transfiguration class just because there was an empty seat. You charmed your quill into a frog that wouldn’t stop croaking, and when he finally cracked a smile, it felt like you’d won something important.
He was awkward and soft-spoken, unsure of himself in the way most boys are before they grow into their limbs. But you liked him instantly. Probably because he liked the same books as you, or because he never made fun of you for being nervous on a broom.
He even held your hand during your first flying lesson, hovering near you the whole time so you wouldn’t be scared. Years later, you found out he was just as scared of heights as you were and only pretended not to be to make you feel safe.
By fifth year, you spent so much time together that you could finish each other’s sentences. By sixth, you were bringing blankets to the highest tower in the castle and naming stars until you both fell asleep mid conversation. There wasn’t a single version of your life in Hogwarts that didn’t include him.
You thought seventh year would be just like that….
You were wrong.
After a summer of sending each other daily letters, pages and pages of thoughts, jokes, and half-sincere promises to never grow up, you returned to school thinking nothing could change.
And at first, it didn’t.
You walked to classes together, fell asleep with your legs tangled on the same couch, pretending not to hear the way people whispered about it the next morning, and snuck out of the common room after curfew not caring that you’d get caught.
The Astronomy Tower was your favorite place, you discovered how pretty it looked at night in your third year.
It was quiet that evening, the wind tugging at your robes as you leaned over the battlement. Jisung set down the little paper packet he’d smuggled from the kitchens—honey biscuits, still warm—and nudged it toward you.
“Payment for helping with my Potions homework,” he said, trying to be casual, though the tips of his ears were already pink.
You laughed and took one, bumping his shoulder with yours. “You’d owe me a whole bakery if this were the price.”
He smiled softly. The moonlight caught in his hair, and for a second you forgot the chill entirely.
“Close your eyes,” he said suddenly.
You arched an eyebrow but obeyed. Something light, wool‑soft, was placed around your shoulders. You opened your eyes to find his black‑and‑yellow scarf wrapped there, smelling faintly of cedarwood soap and parchment ink—purely, unmistakably Jisung.
“You’re shivering,” he mumbled, eyes on his shoes. “Couldn’t have my star‑chart partner freeze.”
You swallowed a reply that felt too big, and instead reached for his hand where it rested on the stone ledge. Your fingers threaded with his, easy as blinking. He stiffened for a second then squeezed back. When you looked up, his gaze was already fixed on you, wide and bright, as though the whole sky were reflected there instead of above your heads.
Neither of you moved for a long while. Orion wheeled overhead, the biscuits cooled, and the castle bells tolled curfew far below. But the only thing you really noticed was the warmth of his palm against yours, and the way your heart tripped every time he glanced your way and smiled shyly.
You learned just how soft‑hearted Jisung was that day on the Astronomy Tower.
Which is why, a few weeks into seventh year, it struck you as utterly wrong when rumors reached you that he’d been seen tagging along behind Lee Seungmin. Seungmin was everything Jisung wasn’t—loud, sharp‑tongued, the sort of Slytherin who thought shoving first‑years into suits of armor was a hobby and swapping curse ingredients under the table was a joke. He hexed quills to peck at classmates and bragged about detentions like they were trophies.
Jisung, by contrast, apologized when he bumped into someone and brought extra quills for anyone who forgot theirs. He flinched at raised voices and fed the barn owls after hours because he worried they were lonely.
So hearing his name linked with Seungmin’s felt like hearing that rain was falling upward. At first you laughed it off, because surely someone must have mixed him up with another quiet Hufflepuff. But then Jisung started arriving late to meals, dodging your study sessions, mumbling vague excuses you’d never heard from him before.
That was when you realized the rumor wasn’t a mistake—and that something was very, very wrong.

Seventh Year
September settled over the castle in a bright rush of golden leaves and new parchment, and for a while everything felt the way it always had. You and Jisung were crossing the courtyard—still laughing about his theory that Professor Lockhart polished his hair with Mrs. Skower’s Extra‑Shine—when a voice cut through the chatter behind you.
“Oi, Park!”
You both turned. Lee Seungmin jogged toward you, grinning widelys. You didn’t bother hiding your sigh.
“Still on for tonight?” he asked, dropping his voice as he leaned in toward Jisung.
“I’m not sure. I’ve got a Potions essay to finish.” Jisung shifted akwardly.
Seungmin smacked him on the back, too hard to be friendly. “Come on, you’ve bailed twice already.”
You stepped forward, folding your arms. “Don’t you have that same essay, Seungmin? It’s half the term grade.”
He turned, as if noticing you for the first time and smirked “Why bother? Snape’s going to fail me anyway.”
“Typical,” you muttered.
“I’ll let you know later,” Jisung said quickly, cutting between you before another jab could leave your mouth.
Seungmin’s gaze lingered on you, faintly mocking, before he turned away with a humorless laugh. “Sure thing, Park.”
The moment he was out of earshot you exhaled. “Since when are you and Seungmin… close?”
“We’re not,” Jisung said, scratching at the back of his neck. “He just hangs around sometimes.”
You searched his face. “You two have nothing in common.”
“It isn’t a big deal,” he insisted, but the laugh that followed sounded fake.
“It is if you’re sneaking off with someone like him,” you said, sharper than you meant to, but the worry was too much to hide.
Jisung’s gaze dropped to his shoes. “I didn’t think it was worth mentioning.”
You didn’t say anything after that. You just walked the rest of the way to class in silence with a sense of unease settling on your chest.
That was when the distance began to show.
First, he started seating two rows over in Charms, smiling apologetically whenever you glanced his way but never moving back. He stopped leaving crooked little jokes on the margins of your Transfiguration notes or looking at you and trying not to laugh whenever Professor Lockhart messed up a spell.
He still spoke to you, yet every conversation felt stitched together, as if he were acting out a script. One afternoon you finally asked, “Are we all right?” He nodded so quickly you had a hard time believing it.
The next time you saw him with Seungmin it was well past curfew.
You had just left the library after wrestling Arithmancy proofs and stopped short as soon as you rounded the corner near the dungeon stairs. There was Seungmin leaning against the wall and Jisung half‑turned away, both speaking in low murmurs. You caught only fragments of Seungmin’s lazy drawl and Jisung’s tight replies. Then Seungmin laughed sharply, and your best friend flinched as though struck.
Your loud footsteps made both of their heads snap up.
“Y/N,” Jisung blurted, striding toward you as if to block your view. “Why are you out so late?”
“I could ask you the same.” You said arching a brow.
Behind him, Seungmin offered a thin grin before slipping down the stairs into the darkness of the dungeons.
Jisung pressed a hand to his eyes. “I was heading back to the dorm.”
“What did he want?”
“He—” Jisung’s voice faltered and for a heartbeat you saw the words gather behind his lips but he swallowed them down. “It’s nothing.”
“Nothing?” Your voice cracked on the word. “Come on, Ji.”
“I’m just tired,” he whispered. “Can we talk tomorrow?”
Silence pooled between you, at last you forced a smile neither of you believed. “All right. Tomorrow.”
But tomorrow never arrived—at least, not the kind where he told you what was wrong.
Because the next day Jisung never came to class at all.
Two whole days slid by without a glimpse of him and you were so on edge you kept glancing over your shoulder, half‑expecting his soft voice behind you. Or hoping he might walk into the library with that shy lopsided smile, asking if you had spare parchment which he always ran out of because his handwriting was too big and messy.
But he wasn’t anywhere, and no one seemed willing to notice besides you.
By lunch on the second day you couldn’t keep silent. Renjun was halfway through a Honeydukes bar, mumbling that chocolate boosted cognitive function, when you leaned across the table and murmured, “Do you know what’s going on with Jisung?”
He froze mid‑bite. “What?”
“Renjun,” you said, low and tight, “you know he hasn’t been to class, or in the common room. He isn’t anywhere.”
“I thought he was sick,” Renjun offered with a shrug that felt rehearsed.
“He isn’t in the hospital wing, and he hasn’t answered any of my owls.”
A flicker of something, maybe guilt, crossed his face. “Maybe he just… needs space?”
Your gaze sharpened. “Did something happen?”
“No,” he blurted too fast. “No, not that I know of.”
“Renjun.”
“I swear, I don’t know.” He wouldn’t meet your eyes. That was answer enough, but you let it drop for now.
That evening, heading back from a prefect meeting, you passed the hidden entrance to the Slytherin common room and heard voices up the corridor.
You weren’t trying to eavesdrop—until one word snapped you still.
“Jisung.”
“Snape got to him before—”
“—thought he was going to die, mate—”
“—Seungmin won’t shut up, keeps saying it wasn’t meant to go that far—”
A rush of blood pounded in your ears as you picked up bits of the hushed conversation. You edged closer and caught sight of Jay and Niki—Seungmin’s friends—half hidden in the shadows, whispering behind cupped hands.
Your fingers curled into fists at your sides. Your thoughts finally being confirmed; Something happened to Jisung and Seungmin was at the heart of it.
You didn’t sleep a minute that night. Every time you shut your eyes, the conversation replayed in your head until dawn bled through the curtains and you were already out of bed, fury keeping you upright.
You found Seungmin loitering outside the Great Hall, laughing too loudly at something Jay and Niki had said. You crossed the marble floor without a second thought.
“Where is he?”
The smile slipped from Seungmin’s face. He cocked his head, all polite confusion. “Sorry, where’s who?”
“Drop the act,” you said, stepping close enough that he had to tilt his chin to keep eye contact. “I heard your lackeys talking last night. Where’s Jisung?”
Jay and Niki exchanged a look but said nothing..
Seungmin gave a thin, brittle laugh. “You’re hearing ghosts, sweetheart. Why would I bother with Park?”
“A better question,” you started, voice cold, “is why you’ve been so attached to him lately. You don’t exactly run in the same circles, so what did you talk him into?”
Something sharpened in Seungmin’s eyes and he leaned in by a fraction. “Careful with what you’re accusing me of.”
“Or what?” You didn’t move. “You’ll do to me what you did to him?”
For a heartbeat his mask slipped, just long enough to confirm you’d scored a direct hit.
“I didn’t touch him,” he said, almost gently. “Whatever mess Park’s in? He walked into it himself”
“Liar.”
He dipped his head, a mock‑sympathetic smile curling at his mouth. “You think you know him so well, huh? Ever think that maybe he finally got tired of you shadowing him like a needy bitc—”
Your wand was at his throat before the last word finished leaving his lips. The corridor went silent except for your breathing.
“You know nothing about us,” you said, voice shaking with contained fury. “If he’s hurt, I’ll make sure everyone here knows exactly whose fault it is.”
Seungmin’s gaze flicked to the tip of your wand, then back to your face. A slow, poisonous smile spread. “Ask too many questions, Y/N, and you might choke on the answers.”
He stepped back with his hands raised in surrender, and strolled away. Jay and Niki followed in uneasy silence. You lowered your wand, fingers trembling with adrenaline.
His parting smile told you everything about his involvement. But you still didn’t have clear answers.
So you went to seek the other person allegedly involved. Snape.
When you descended into the dungeons, the silence was immediate and unnatural. No one ever came this far during free periods; only Professor Snape’s office existed at the end of this corridor, buried deep in the coldest, most isolated part of the castle.
Faint green flames floated midair along the walls, suspended in enchanted sconces that made no sound and cast no warmth. They pulsed gently, like breathing, and their glow warped the stone around them, making the shadows twist in ways that defied logic.
You hated it down here. Even now, in your seventh year, walking this corridor alone made your heart thud against your ribs like it wanted you to turn back.
But you were desperate.
Snape looked up slowly when you stepped into his office without knocking, his quill pausing mid-sentence on the parchment. His expression went from mildly irritated to coldly displeased in an instant.
“Is knocking a forgotten concept these days?” he said dryly.
“Professor,” you began quickly, not even trying to hide the urgency in your voice. “I need to talk to you.”
Snape set down his quill, arching a single eyebrow. “Then I suggest you start talking, and make it quick.”
You swallowed. “It’s about Jisung… Park Jisung. He’s been missing for days, and no one seems to know anything. Or at least, they’re pretending they don’t.”
His gaze sharpened and for a second, you thought you saw a flicker of caution behind his eyes before he quickly masked it.
“I fail to see why you’re bringing this to me,” he said coolly, leaning back in his chair. “Missing students are a matter for the headmaster.”
“Don’t,” you snapped before you could stop yourself. Snape’s eyes narrowed dangerously, but you pressed forward anyway. “I overheard some students talking. They mentioned your name…said you found Jisung somewhere. Something happened to him, didn’t it?”
Snape’s eyes flashed briefly. “And you believe the idle gossip of students because…?”
“Jisung wouldn’t just disappear on his own like that. I know something happened to him,” you shot back, voice shaking. “And I believe you know exactly what.”
He watched you silently for a moment. You could feel him weighing something behind his guarded stare. Finally, he exhaled sharply.
“Miss Y/N,” he began slowly, voice heavy with thinly veiled warning, “there are things within these castle walls and beyond them that you are better off not knowing.”
“That’s not your choice to make,” you said immediately.
“On the contrary,” he replied calmly. “It is precisely my choice. And you will do well to remember that.”
Your fists clenched at your sides, frustration prickling hot behind your eyes. “Professor, please. Jisung’s my best friend. If he’s hurt… if something’s happened… I need to know.”
Something shifted in Snape’s expression at your words, almost looked like regret. When he spoke, his voice was almost gentle, which frightened you more than his scorn.
“Sometimes the worst harm you can do to someone is to keep prying.”
He paused, holding your gaze steadily. “Park is alive. That is all you need to know. Now leave.”
You stood frozen for a second, his words sinking in painfully. Jisung was alive—yet somehow, that felt worse. It meant something had happened… Something terrible.
Your jaw tightened. “You can’t keep this hidden forever,” you whispered fiercely.
He leaned forward, eyes piercing yours in the darkness of the room.
“We’ll see.”
You turned away, storming from his office without looking back. Snape hadn’t denied anything which meant there’d definitely been an incident and it was serious enough that Jisung couldn’t be seen right now. He was alive, but he was hurt, and whatever happened to him was being deliberately hidden.
A few days later
The day started like any other.
You pushed cold eggs across your plate, half listening to Renjun’s gentle attempts at conversation while the Great Hall hummed as if a student hadn’t been missing for a week. But suddenly, a hush rolled through the room.
You felt Renjun touch your arm.
“Y/N.”
You looked up, and followed his gaze toward the doors. The breath caught in your throat.
Jisung was standing just inside the oak doors.
He was bent at the shoulders, eyes flicking over the Hall as if he didn’t remember ever being there before. His robes hung wrinkled and loose and there were red scratches carved along his neck and cheek. He was paler than before and the shadows beneath his eyes made him look years older than when you’d last seen him.
Without greeting anyone, he drifted to the far end of the Hufflepuff table nowhere near his usual seat beside you.
You were on your feet before the thought finished forming.
Renjun caught your wrist. “Y/N, maybe wait—”
You shook him off and crossed the hall, every step echoing in the sudden quiet.
“Jisung?”
He flinched but kept his gaze on the empty plate. “Not now, Y/N.”
“You’ve been gone a week,” you whispered, voice trembling. “I was so worried—”
“I said not now.” The snap in his voice was sharp enough to cut. He glanced up and the terror in his eyes chilled you to the bone.
You reached for him, but he stood so abruptly your balance faltered. Without another word he strode the length of the hall and disappeared through the doors, leaving a silence that seemed to bend the rafters.
You stood frozen, heat flushing your face as dozens of eyes slid away. Renjun appeared at your elbow and talked softly. “Let him breathe.”
You nodded, though the emptiness in your chest insisted otherwise.
Jisung returned to lessons, but only in body. He answered professors in one‑word murmurs and offered classmates strained smiles that meant please don’t talk to me. At meals he sat alone, two yards of empty bench marking the space where laughter used to live.
He moved faster when he saw you in the corridors. He no longer waited outside classrooms or drifted toward your chair in the library. His robes hung loose as if he’d lost weight along with sleep, and his hands shook whenever he raised his wand. Sometimes you caught him staring through stone walls at something only he could see.
You tried with soft hellos in the common room, and owls folded with careful questions but every attempt slid off the wall he’d built overnight. The harder you reached, the farther he retreated, until all that remained between you was silence and the memory of how easily you’d once shared the same breath.
2 days later
Jisung sat on the edge of his bed, head buried in his shaking hands. His palms were marked with crescent-shaped indentations from how hard he was clenching his fists.
He kept hearing it.
The snap of branches in pitch-black darkness. The sickening crunch of claws sinking into damp earth. The guttural snarl vibrating through his bones moments before razor-sharp teeth pierced his shoulder. The thick warmth of blood soaking through his robes.
Sometimes it came to him in dreams. Other times, he’d be awake, in class, or walking down the corridor. A sound, or a smell and he was back in the forest.
Snape had said the wolfsbane would help and it had in a way. At least, it kept the full transformation at bay. But it didn’t stop the memories, it didn’t quiet the noise in his head.
His senses were too sharp now, every creak of the floorboards, every flicker of candlelight, every rustle of parchment felt louder. Sometimes he thought he could hear people’s heartbeats, smell their sweat before they entered a room. His insides constantly felt overwhelmed with unbearable energy. He felt trapped in his own skin, moments away from tearing free of himself. Sometimes he felt too much, and other times… he felt nothing at all.
Worst of all, though, was you.
He couldn't stand to be near you anymore. Not because he didn't want to, but because your scent now stirred something dangerous within him. It made his chest ache unbearably, tightened his throat with longing and thirst.
A part of him urged him to get far away from you. But another darker, more primal part whispered the opposite… to scent you, to sink into you, to lose control entirely. But he refused to drag you into his nightmare. He wouldn't allow it, no matter how much it tore at him.
He could remember most of what led him into the forest, up to a certain point.
He remembers Seungmin saying he wanted to hang out and they met near the edge of the Forbidden Forest, where one of the slytherins handed out something called shadeleaf. It was an iridescent petal folded into itself like a capsule. Illegal, of course. Banned by the ministry for its hallucinogenic properties and its tendency to react differently based on magical affinity.
Jisung didn't even know why he was there. This wasn’t his scene at all. The guys were drinking something out of a flask that smelled like burnt sugar and smoke. Jay was lighting up a rolled spell-scroll with charmed embers. Niki already looked half out of it, eyes glazed.
When Seungmin started showing an interest in him a few weeks ago, Jisung had been flattered. He'd only ever made two close friends at Hogwarts, so someone new noticing him felt good. That was the only reason he went along with him. He wanted to be accepted.
“Is it safe?” Jisung asked nervously.
“Come on, park,” Niki chuckled, placing a shimmering petal on his tongue. “Don’t be a Squib.”
“What's the worst that could happen?” Seungmin grinned, handing one to him. “You trip a bit? See some weird shit? Wake up with a headache?”
Jisung hesitated, staring at the thing in his palm. It pulsed faintly with a color he didn’t have a name for.
He didn't want to do it, but they were all watching him. So he took it.
The effects hit almost instantly. His vision went fuzzy first; he could only see edges warping and light bending at impossible angles. Then his tongue tingled and throbbed, and his body felt too hot.
“Shit, this is strong,” Jay laughed.
“It’s not that bad,” Seungmin said, puffing from the smoldering scroll between his fingers.
None of them looked as affected as Jisung.
"Come on, Park," Seungmin said, draping an arm casually yet firmly around Jisung’s shoulders. "There’s a spot a little deeper in. We hang out there all the time."
Jisung couldn’t hear properly anymore, everything sounded underwater. He followed anyway.
He couldn’t say how long they walked. It felt like hours, though in reality it was probably mere minutes before his knees gave out, sending him sprawling onto the cold forest floor. His head spun violently, vision fractured.
He tried to speak, to call out but his voice didn't work, the forest blurring darker and darker until only silence and blackness swallowed him whole. He didn’t know when they left him. Just that at some point, he was alone.
The last thing he remembers was seeing bright, yellow eyes and feeling immense pain…
He woke up choking on his own blood.
His body jerked violently, lungs burning as he struggled to take in air. He felt strong hands grip his shoulders, pulling him upright with urgency. Through blurry, half-open eyes, he caught the outline of a wand glowing faintly in the dark. He barely recognized the familiar cadence of Professor Snape’s voice echoing through the haze.
“Park… Can you hear me?” Snape’s voice was clipped, edged with tension he’d never heard before.
Jisung managed only a strangled groan. He couldn’t speak, his throat was raw, filled with the metallic tang of blood. Breathing felt impossible, each gasp shallow and painful, as if his lungs were full of lead. He felt wetness soaking through his clothes and pooling beneath him. He didn't know if it was sweat or blood. Probably both, his clouded mind whispered darkly.
He was certain of only one thing—he was going to die here.
“You’ve been attacked,” Snape explained urgently, casting quick charms that rippled warmly across Jisung’s battered body. “I need you to remain as still as possible while I attempt to slow the bleeding.”
The word attacked echoed faintly in Jisung’s mind. Attacked by what? His thoughts swirled sluggishly. He couldn’t focus enough to piece anything together.
Snape pressed a small vial to his lips. The Hufflepuff hesitated, eyes flickering up weakly, his question dying soundlessly on cracked lips.
Snape seemed to understand instantly. “It’s Wolfsbane.”
The word crashed over Jisung with crushing weight, his mind snapping painfully back to clarity. Wolfsbane. A potion for…
His stomach twisted violently, nausea gripping him as realization cut sharply through the fog in his mind.
He’d been attacked by a werewolf.
It felt impossible. He wanted to deny it, wanted to believe it was just some twisted nightmare brought on by the drugs he’d foolishly taken. But the pain burning through his shoulder and the dark, grim expression on Snape’s face all made denial impossible.
With trembling lips, Jisung allowed Snape to tip the bitter potion into his mouth, grimacing weakly as he forced himself to swallow it down. It tasted vile but he had no energy left to protest.
He collapsed back against the cold forest floor, limbs heavy, vision fading once more as Snape continued muttering charms, trying to keep him tethered to consciousness.
“Stay with me, Park,” Snape’s voice commanded, sharp but oddly comforting. “You’re not going to die tonight.”
But Jisung wasn’t sure he believed him.
The darkness rushed back in, heavy and thick, pulling him under again as Snape’s frantic movements blurred and faded away.
His memory is fuzzy from then on.
One moment he was lying in the dirt, blood soaking the ground beneath him. The next, he was being levitated through narrow hallways, his body wrapped in magic and warding charms.
The room was dark, except for a wandlight hovering near the ceiling. He was placed on a dusty mattress on the floor. His skin felt stiff with blood, every muscle felt like it had been peeled apart and sewn back together with barbed wire.
He recognized the Shrieking Shack from an article he’d read once about the most haunted places on Earth. That’s where they were right now.
The shack was colder than he imagined. This was the place they used to tell ghost stories about in the common room. The place kids dared each other to peek into on Hogsmeade weekends. It smelled like old wood and dust. Snape moved through it like he’d been here before—like this was routine.
He cast a dozen silent spells before even speaking. Layers of enchantments wrapped around the rotting floorboards, the shattered furniture, the warped windows.
“You must take this Wolfsbane every day,” Snape said curtly, setting a tray on the floor beside the creaking mattress. “Or I’ll force it down your throat.”
Jisung didn’t answer. Snape paused, studying him with that unreadable stare.
“You’ll stay here until the full moon passes,” he said. “You’ll say nothing when you return.”
Jisung blinked slowly, the weight of it sinking into his bones. ‘When you return… or If’.
Then Snape turned to go but he stopped in the doorway.
“You are not the first,” he said, voice low. “It will be painful but you’ll survive.”
And with that, he was gone.
The silence was the most unbearable part of being in the Shack. Not even the pain or the way Jisung’s bones ached like they were preparing to snap apart. It was the silence that made him feel like he’d go crazy any minute.
He tried to sleep, but whenever he tried he’d blink awake to phantom sensations of fur brushing his skin, fangs pushing against his teeth, and a sweet scent of honey curling through the cracks in the floorboards.
It wasn’t the full moon yet but his body was already responding to it. The Wolfsbane kept him from changing completely, but it didn’t stop everything. His skin itched as if it was being stretched and he realized he’d grown a few inches taller overnight. His eyes were also becoming sensitive to even the faintest flickers of light, and they were a dark shade of yellow that glowed whenever the moonlight hit them.
It might’ve been on the second night or the third, he couldn’t remember well, but Snape came in and told him that the full moon would be at its peak and he would feel the effects more despite the potion.
Jisung lasted about two hours before the pain began. It wasn’t sudden. It crept in slowly, like frostbite, numbing his fingers first. Then his wrists and his legs. He thought maybe this was it—maybe he’d just fade out before anything happened. Then it spread up his spine and into his skull, where it bloomed behind his eyes like fire.
The pain was so much bigger than his body. It burned and it shredded him, as if his bones were being broken and rebuilt at the same time, like his skin wasn’t big enough to hold him anymore. He scratched at his own arms until his nails cracked and bled. It got so unbearable he slammed his head against the wall hoping he would knock himself out but he couldn’t.
He clawed at the walls, tore at the floorboards and bit into the wood until his mouth filled with splinters and blood. He howled until his throat tore raw. And still, it didn’t stop
He lost count of how many times his limbs broke and reformed. His jaw cracked open so wide he thought it might dislocate, teeth pushing through bloody gums. He was sobbing or at least, he thought he was. It was hard to tell over the sound of his own growling.
The transformation stopped halfway and started again the next day. He never fully transformed but he felt the pain of his body trying to fight against it every single time.
He stopped counting days after that.
Hunger and exhaustion tangled with grief and fear until all that was left was the throb of his body and the steady hum of magic in his blood. He didn’t think about the pain anymore. Or the bite. Or Seungmin. Or the forest.
Mostly, he thought about you.
He tried not to, but you wouldn’t leave him. Your face, your laugh, your voice, it all circled him like the moonlight through the slats in the wall.
The way the thought of you made his body burn now.The way your honeyed scent used to be comforting but now made his lungs tighten and his mouth water. He didn’t understand why he was feeling this way.
On the seventh day he woke up soaked in sweat, shivering uncontrollably. The moon had passed. He could feel it in the way the ache in his bones was retreating and his mind was clearer.
Snape arrived at dawn.
He said nothing about the mess of blood and broken furniture in the room. He just studied Jisung who was sitting slumped against the wall. He pulled out his wand and started casting diagnostic spells over his body.
“You’ll return to class tomorrow,” he said. “If anyone asks, you were ill.”
Jisung didn’t move.
Snape continued impassively. “You are not to mention the Wolfsbane, the forest, or what you’ve become. Do you understand?”
Jisung finally looked at him, barely able to lift his head properly. “That’s it? Just… go back like nothing happened?” His voice came out hoarse.
Snape’s eyes narrowed faintly. “No. That is not it.”
He stepped closer.
“You will take your potion every cycle, no matter what. And you will not seek out the other boys involved, nor will you retaliate.”
Jisung’s jaw clenched. He wanted nothing more than to rip Seungmin’s throat apart, but he knew that was just the wolf thinking.
“And most importantly, you will stay away from her.” Snape said, his voice dropping at the last word.
Jisung sat up sharply, knowing exactly who he was referring to. “Why?”
The professor’s expression didn’t soften. “Because the wolf doesn’t care that she’s your friend. It doesn’t care about boundaries or guilt or decency. It responds to need.”
Jisung’s chest tightened, throat dry.
“The first few transformations are the worst,” Snape continued, pacing slowly now. “Your body hasn’t adjusted. Your instincts haven’t aligned with your mind. You will feel urges…violent, territorial, carnal urges that you can’t control. Those urges will turn into fixations... Especially for someone you already had feelings for”
“I don’t–” Jisung started.
“You don’t need to lie, Mr. Park.” Snape cut him off, “I am a very skilled Legilimens, you know? I can see your mind and I see how it’s filled with thoughts of her.”
Jisung looked away, jaw trembling slightly. Snape stopped in front of him.
“Her scent” he said quietly. “It already triggers you, doesn’t it?”
Jisung didn’t answer. That sweet scent of honey and parchment that he kept smelling through the rotting floors and the dried blood, he figured out it was you. It reminded him of that night at the Astronomy tower.The Shrieking Shack might be a few miles away from Hogwarts castle but he could still somehow smell you.
“You feel it in your chest, in your teeth, in your gut” Snape said, voice like a scalpel. “You want her.”
Jisung’s breathing picked up.
“That is the beginning of your rut.”
“Rut?” he repeated, barely above a whisper.
Snape nodded. “It’s a biological response. Wolves enter a heightened state after the full moon cycle. Some experience it more than others, especially younger ones who’ve recently turned”
Jisung’s heart was pounding now, nauseatingly fast.
“You may feel sudden impulses or worse you might want to act on those impulses.”
He felt sick. “I’m not— I would never hurt her.”
“I’m not concerned about your intentions,” Snape said coldly. “I’m concerned about your self control. A werewolf’s instincts are hard to resist and if you lose control, Mr. Park… She will pay the price.”
“So stay away from her,” Snape said with finality. “It’s the only way to keep you both safe.”
Jisung sat there shaking, the weight of what he’d become pressing down on his spine like a second body.
He couldn’t go back. Not like this.
“I’m not ready,” he said hoarsely.
Snape didn’t turn. He stood by the window, watching the last of the night dissolve into grey morning.
“You won’t ever be,” he said simply.
Jisung clenched his jaw. “I don’t want to see her. Or anyone. I—I can’t trust myself.”
“You must learn to live with your current situation.”
“Why can’t I just… stay here?”
Snape turned at that. His eyes were cold and calculating.
“Because people are already asking questions,” he said. “Students, staff. Your friend.”
Jisung’s heart stuttered at that.
“She’s worried,” Snape continued. “Rightfully so. You disappeared without warning. She’s been to my office several times. She’s even confronted the student who got you into this predicament, pulled out a wand at him. I don’t know how much longer I can keep her from endangering herself trying to find you.”
Jisung lowered his head, guilt flooding every nerve.
“Rumors are spreading, too.” Snape added. “A few students are saying they saw you with Mr. Lee that night. Some think you were injured, others that you’re in trouble. You’ve already been gone too long.”
Jisung swallowed hard. “So I just walk into the Great Hall acting like I’m normal?”
Snape didn’t blink. “Yes.”
His stomach turned. “And if someone sees the scars?”
“You’ll say you had an accident in the forest.”
“And you’ll back me up?” he asked bitterly.
“If I must.”
Jisung exhaled shakily. “And Y/N? We—we’re always together, she’ll find it weird if I suddenly cut her off”
“You’ll keep your distance regardless. If she asks questions, you deflect. If she pushes, you walk away. You’re not safe around her”
He bit his lip hard, so hard it almost bled. “She’ll know something’s wrong.”
“Then hope she’s smart enough not to get too close.”
The doors to the Great Hall had never felt so heavy. Jisung stood in front of them for nearly five minutes, staring at the carved wood. Behind them, he heard laughter, casual conversation, normalcy.
He wasn’t ready.
But Snape’s words echoed in his skull.
"You’ve already been gone too long."
He took a breath and pushed them open.
All the noise overcame him like a wave, the plates clinking, voices overlapping, owls fluttering through the rafters. It all felt loud in a way it hadn’t before, as if someone had turned the world’s volume up just to punish him.
He kept his head low and his pace steady. One foot in front of the other. Just like Snape said. Act like nothing happened.
He could feel all eyes on him almost instantly. First years stopping mid-bite and a few seventh-years whispering across the Gryffindor table. Someone, he thought maybe Jay, froze with a goblet halfway to his lips.
And then you. He didn’t have to loo, he felt the second your eyes landed on him, making something twist deep in his chest. That same unbearable tightness he’d felt in the shack whenever he let himself think about you. About your laugh echoing across the common room. About your fingers brushing his when you passed him a quill and how it used to mean nothing, and now it meant everything.
He knew you’d notice the hollow look in his eyes, the bruises blooming like violets on his neck and the bandage peeking out from beneath the collar of his robes. You’d find it weird that he didn’t sit near you, didn’t even glance your way. But he tried to ignore those thoughts and just focus on the plate in front of him even though his stomach turned at the smell of food.
You stared at him from your seat. It took you several long, painful seconds to process what you were seeing.
Jisung—your best friend, who’d been missing a week without a word—just walked into breakfast looking like he’d seen hell and barely made it back out.
His robes were loose like he’d lost weight and his eyes were ringed with dark circles, exhaustion written clearly in every line of his face. There were cuts visible, thin red marks down his jaw, a deeper scar stretching beneath his collar, fading bruises on the backs of his hands. His hair was tangled, his posture painfully tense.
You felt a sick sense of relief after seeing him, despite his appearance. But most of all you felt angry. You felt everything all at once, a hot rush of emotions almost too intense to handle.
Jisung avoided your gaze completely. He picked at the food in front of him, not really eating, just pushing it around his plate.
He felt you approaching before you spoke. Your scent hit him first, warm and familiar, yet unbearably intense. His jaw clenched tight, fingers curling into fists beneath the table. He didn’t look up even when you stood near him. He simply couldn’t trust himself to see your face and not fall apart.
You called his name quietly and he almost cried at the sound of your voice. But he didn’t move, not even when you stepped closer.
Slowly, he raised his head, gaze finally meeting yours You went still, eyes widening just slightly. He knew instantly what you saw—the darkness in his stare, the shadowed bruises, the fresh scars. The way he looked wrong.
He couldn’t bear your pained eyes, so he snapped at you. Something he’d never do before, but Snape told him to deflect. So he yelled and walked away, trying to ignore how hurt you looked.
This was what Snape meant. You’re not safe around her.
You couldn’t eat after that. Not with the way he’d looked at you.
Jisung had always been soft-spoken, a little awkward, a little shy—but never cold. And you didn’t need a Healer to tell you that whatever he’d gone through wasn’t some stomach bug or routine cold. You weren’t stupid.
You saw the tremble in his fingers when he reached for his fork. You saw the way he flinched when someone behind him dropped their goblet. You saw the bruises just under his collar and the bandages.
Something happened to him.
You sat back down but your heart was still up at the other end of the table with him.
“I need to know,” you murmured, more to yourself than to Renjun.
He sighed. “Y/N…”
“Don’t say it,” you snapped quietly. “Don’t say I should give him time. Don’t say he’ll come around. I know him, Renjun. He’s scared. You don’t just disappear for a week and come back with claw marks on you neck.”
Renjun went quiet.
That silence told you more than anything else.
“Okay, I’m tired of this… You know something, don’t you?”
He avoided your gaze. “It’s not my place to say.”
That hurt. “Is it mine to not know?”
You stood abruptly, grabbing your bag. “If no one’s going to tell me the truth, I’ll figure it out myself.”
Over the next few days, you tried to get close to Jisung in every way you could think of. You waited for him outside the greenhouses after Herbology, hoping to catch him alone. You switched seats in Charms just to be nearer, and sometimes you even loitered in the corridor after Potions, telling yourself you’d walk him back to the common room.
Despite your best efforts, he continually slipped away.
He offered awkward excuses about having somewhere to be, or sometimes said nothing at all and just walked past. Most of the time, he barely managed to look at you, as if doing so caused him physical pain. This wasn’t an icy kind of avoidance, nor was it tinged with anger. It felt worse than either of those possibilities—it was as though he found everything about you unbearable, but still couldn’t muster the energy to explain why.
Once, you nearly cornered him after lunch. He was leaning against the corridor wall outside the Great Hall, head tipped back, looking utterly exhausted. In that unguarded moment, your eyes met his, and you thought you glimpsed your old friend beneath the tension he carried. Summoning the nerve you’d been collecting all day, you stepped forward.
“Can we talk?” you asked softly.
For a split second, it seemed like he might say yes. His mouth opened as though he wanted to form the words but then Professor Snape’s voice echoed from behind you.
“Miss Y/N.”
You turned around to find Snape standing there, unruffled as always, robes hanging in sharp lines. He inclined his head in an almost polite manner yet still carried the weight of an order.
“I need you to come to the dungeons,” he said in a measured tone. “There are ingredients that require sorting. I trust your handwriting is still legible.”
You tried to protest, but as soon as you turned back, Jisung had vanished. From that moment on, it became a pattern: every time you got too close to him, Snape appeared with some new task for you—an extended office hour to discuss a mistake in an essay, a request to reorganize outdated potions, or a perfectly timed interruption just as you were about to speak with Jisung privately.
On a rational level, you knew it was ridiculous to think Snape was orchestrating this on purpose; however, it was impossible to ignore how consistently he managed to swoop in whenever you finally had a chance to approach Jisung alone. You didn’t know why your professor was so intent on calling you away, and truthfully it wasn’t the main issue gripping your mind.
All you could focus on was Jisung.
He looked so different—worn down, scared, ashamed, like he was carrying a secret that weighed on his shoulders every moment of the day. Every time you tried to reach him, he withdrew further. It broke your heart, because you weren’t trying to fix him or make him talk if he didn’t want to. You just wanted to be there, to stand by him instead of watching from a distance.
Yet no matter how hard you tried, the boy who used to seek you out for study breaks and late-night jokes now seemed determined to avoid you. And the more distance he forced, the more you wanted to find out what had really happened, because this Jisung—the one who flinched when you spoke and looked away when you caught his eye—felt like a stranger wearing your best friend’s face.
It was late, far too late for anyone else to be out of bed. So when you heard commotion up in the Astronomy Tower during one of your prefect rounds, you instinctively climbed the stairs to inspect, your wand held loosely in your fingertips.
The castle had felt too quiet lately. Ever since Jisung came back, everything had been off balance. You’d even taken extra patrols just to keep your mind busy. You weren’t expecting to find anything up there except maybe a few rowdy owls.
But when you pushed open the heavy wooden door to the Astronomy Tower, you froze at the sight.
Jisung was there, hunched against the railing, his robes half-open, hands gripping the stone balustrade so tightly you saw his knuckles pale even from across the room.
"Jisung?" you said softly, hesitant.
His head snapped up instantly, and your breath caught in your throat.
His eyes were wild, pupils blown wide, irises shimmering unnaturally gold beneath the moonlight. Sweat gleamed across his pale forehead, his hair was messy and damp, sticking to his face. His breathing came harsh and fast, almost feral.
You took a cautious step forward. "Jisung, are you okay?"
"Stay back," he choked out, voice strained and rough. "Don't come closer."
But you saw the tremble in his arms, the feverish brightness in his eyes. He looked sick. He looked scared.
"What’s wrong? Let me help—"
"No." He shook his head violently, squeezing his eyes shut as if fighting himself. "You can't—I'm not—"
He trailed off, stumbling forward as if pulled by some invisible force toward you. He was breathing heavily, lips parted as he seemed to taste the air between you.
"Jisung—"
Your voice cut off as his gaze snapped sharply to yours again, something raw and dangerous flaring in his eyes. It sent a shiver racing down your spine, and you instinctively backed away half a step.
"Leave," he hissed, the word barely recognizable through his clenched teeth. His whole body seemed rigid with tension. "Please, leave before—"
He broke off with a gasp, doubling over as though a wave of pain had just wracked through him.
You rushed forward instinctively, panic clouding your caution. "Jisung!"
He moved faster than your eyes could track. One moment he was curled into himself and the next he had you pinned against the cold stone floor, wrists pressed tightly beside your head, his face inches from yours, breath hot and erratic against your neck.
"Ji—" Your voice cracked. "What are you—"
He inhaled deeply against your throat, his body trembling against yours. "God, you smell so—" His voice was ragged and broken, almost a sob. "I can't—I can't stop it, I—"
He pressed closer instinctively, hips pinning you hard against the floor. His lips grazed roughly against your neck, sharp teeth skimming dangerously along your pulse point. Your heart slammed against your ribs, fear tangled confusingly with something hot in your lower belly.
"Jisung, please," you whispered, half plea, half gasp. "You're scaring me."
Those words seemed to pierce through whatever haze had overtaken him. He jerked back, eyes wide, suddenly horrified at himself. His gaze flicked down to your wrists, already bruising beneath his grip, and he stumbled away as if burned.
"No," he whispered, horror and guilt bleeding openly into his expression. "I didn't—I wouldn't—"
You stayed frozen on the floor, chest heaving as you watched the agony twist across his face.
"What’s happening to you?" you breathed, sitting up slowly.
He stared at you, anguished, hands still trembling at his sides.
"I'm sorry," he whispered brokenly. "I—I'm so sorry."
Before you could say another word, he turned sharply and bolted down the stairs, leaving you alone, shaking, and terrified.
The Hufflepuff common room was quiet when you walked in. Most students had gone to bed, but Renjun sat alone on the couch.
You didn’t give him a chance to pretend he didn’t see you coming.
“You’re going to tell me what happened.”
Renjun sighed, not looking away from the fire. “Y/N…”
“No,” you said, standing in front of him. “No more deflecting. You’ve known something since the day he came back.”
He rubbed his hands over his face. “I don’t know the whole story.”
“Then tell me what you know.”
Silence.
You crossed your arms. “Do you really think I’m going to stop asking? You’ve seen him. You know he’s not okay. And no one’s saying anything, and I’m losing my mind because—” your voice cracked, just slightly— “because that’s my best friend.”
Renjun’s shoulders slumped. He looked like he aged ten years in a second.
“Seungmin and his friends... they planned something,” he said quietly.
Your chest went still.
“I only heard a conversation between Professor Sprout and Professor Snape,” he continued. “But apparently they were hanging out near the edge of the Forbidden Forest. Seungmin gave Jisung something. A potion or… some kind of enchanted hallucinogen.”
Renjun looked up at you, guilt heavy in his eyes even though he hadn’t been there. “They led him into the forest, Y/N… And something attacked him.”
You stared at him, voice thick with dread. “Something?”
Renjun hesitated. “Snape... Snape was the one who found him.”
You felt cold all over. “What was it?”
He looked away.
“Renjun. What was it.”
His voice dropped to a whisper.
“A werewolf.”
A gasp got stuck in your throat.
“I don’t know how bad it was,” Renjun said softly. “But apparently Professor Snape had to lock him up for a week while he went through the transformation.”
Tears stung behind your eyes. “Why didn’t you tell me?”
“Because I didn’t want to believe it myself….”
You sank into the chair across from him, everything too heavy to stand.
“A werewolf,” you whispered.
He nodded and suddenly, so many things clicked at once. Suddenly it all made sense.
After Renjun told you, you couldn’t sleep.
You sat in your bed staring at the ceiling until the sun started bleeding through the windows, and then you slipped out of the dorms without a word. You went straight to the library and stayed there all morning.
Madam Pince gave you a curious glance when you asked to go into the Restricted Section after looking through every other possible book in the regular shelves and finding nothing of value. You dropped Professor Babbling’s name as your excuse—said you were doing independent research for an Arithmancy paper. She didn’t ask further, just handed you a list of approved titles and waved you through.
You didn’t touch a single one of them. Instead, you searched for everything you could find on werewolves.
They were mostly old, dusty books with creaking spines and brittle pages. Most seemed to be more folklore than facts but you found a text buried near the bottom of a shelf, half its title burned off the spine.
Lycanthropy and Lunar Madness: A Clinical Compendium.
The chapters were brutal. You read about the first changes, the muscle pain, the sensory overload. The way magic in the blood would flare, fight back, burn from the inside out. You read about the violence, how the mind slips away when the full moon peaks, how instincts override everything else.
But what caught your atention the most was this:
“In cases of recent infection, the afflicted may experience an attraction fixation, often triggered by proximity to a familiar person. This response is especially common in individuals whose first transformation occurs during adolescence or early adulthood.
The instinct is not always sexual, but it is always possessive. The werewolf’s senses recognize the person as a source of comfort or danger. When comfort, the fixation can lead to obsessive behavior, rut-like symptoms, and irrational aggression if the person is perceived as threatened or unattainable. When danger, it can lead to avoidance or attack. Scent is the most common anchor. Once imprinted, it is nearly impossible for the werewolf to ignore.”
Your throat tightened. You re-read the paragraph five times.
It made sense, too much sense. His distance, his flinching, the way he couldn’t look at you anymore.
Your scent.
You remembered how he looked at you that morning in the Great Hall. How he barely breathed when you stood too close and how he wouldn’t meet your eyes when you asked what happened. And last night in the Atronomy Tower, he said you smelled good and it looked like he wanted to eat you alive.
You closed the book with shaky hands and then checked out four more. You didn’t stop reading until your eyes blurred. You didn’t eat or go to class.
By the time the sky outside the window started darkening, you were sitting at a corner table, surrounded by open tomes and loose parchment covered in frantic notes—everything you could find about Wolfsbane, Snape’s potion-making reputation, the legal status of werewolves in magical Britain, and every known case of student infection in the last fifty years.
You turned the page again.
Magical Intervention
“Wolfsbane Potion, taken daily during the week of the full moon, prevents transformation but does not erase the instinctual response. It is crucial that young werewolves are supervised during their first year of turning, especially if they experience early signs of rut.
If left unmonitored, the werewolf may become a threat not only to others—but to themselves.”
You found another book next. Not on lycanthropy, but on magical trauma. It mentioned Professor Snape by name.
“A known expert in dark creatures and cursed bloodlines, Professor Severus Snape has played a role in the treatment and monitoring of several underage werewolf cases, particularly after the war.”
You sat there for a long time, staring at the page, your mind buzzing. Snape knew, he was involved and he wasn’t just keeping the secret, he was managing it.
Which meant whatever happened to Jisung—Snape had seen it before. And he’d chosen not to tell you a thing.
You sat there in silence, your hands numb on the table. Snape had told him to stay away from you, that much was obvious now. But no one had told you what being near him could do.
You weren’t afraid of him. But for the first time, you understood why he was of you.
You left the library as the sky was starting to pale with early morning light, the forbidden books still echoing in your thoughts. You didn’t bother going to class again. You went directly to Snape’s office instead and waited there. When he finally arrived, he paused mid-step at the sight of you.
“Miss Y/N,” he said flatly. “You are not scheduled to meet with me.”
“No,” you said, stepping forward. “But I’m not leaving until you tell me the truth, sir.”
His eyes narrowed. “I beg your par—”
“Did you know?” you cut in, voice trembling with restrained rage. “Did you know what would happen to him?”
“I’m not sure what you’re referring to.”
“I know that Jisung got attacked by a werewolf.”
Snape stilled.
“I went to the restricted section,” you continued. “I know what werewolves go through. I know about the rut cycle. The way someone can trigger it just by being close… Did you know it would be me?”
He didn’t speak, and that silence was an answer.
You took another step toward him. “You told him to stay away, didn’t you?”
Still silent.
You laughed bitterly. “What, were you going to wait until I ended up on the courtyard floor with his teeth in my neck before you decided to warn me?”
“Lower your voice,” Snape said sharply, eyes flicking toward the empty corridor.
“No,” you snapped. “You don’t get to tell me what to do now when you left me in the dark about everything.”
“He is alive and you’re safe because of me,” he said sharply. “Do not mistake silence for neglect.”
“He’s barely alive,” you fired back. “He’s walking around like a ghost and you expect me to believe that’s your idea of help?”
“You think you want the truth but the truth is messy and dangerous. And the truth, Miss Y/N…” he stalked closer to you, almost menacingly “… is that your friend is not who he was anymore.”
“I know that!” you shouted, voice cracking. “But you made him think he was dangerous.”
“He is.”
“No,” you said fiercely. “He’s just scared and you’re feeding it.”
Snape’s eyes narrowed. “You have no idea what a werewolf in rut is capable of.”
“I do now.” You stepped closer again, voice trembling. “I’m not stupid or fragile. And I’m not going to stay away just because you think it’s better that way.”
“Miss Y/N—”
“No,” you snapped. “You can’t “protect me” by locking him away like some creature. He’s not a danger to me. What’s dangerous is isolating him, making him ashamed of something he didn’t choose.”
Snape’s mouth pressed into a thin line.
“And what will you do, then?” he asked. “If he loses control?”
“I’ll help him.” You exhaled, hands trembling. “I’m not afraid of him and he needs someone who isn’t.”
There was a long pause. Snape looked at you with something like pitty. Then he spoke, carefully.
“Then you’d better learn how to handle what’s coming.”
Knowing about Jisung’s condition didn’t bring the relief you thought it would. If anything, it made everything worse. Because now you understood that there was almost nothing you could do to save him from himself. And, like Professor Snape said, the safest option was to stay far away.
And you tried, but it was so hard.
You'd find yourself turning to complain about Professor Binns's endless lectures, only to realize it wasn't Jisung beside you, but Renjun—quiet, studious Renjun who never dared utter a complaint in class.
Or when you walked toward the kitchens out of habit, thinking maybe you'd sweet-talk the elves into some pumpkin tarts, only to remember it was Jisung who always did the charming.
Or when the night sky looked especially clear and you found yourself wanting to stargaze but realizing no one else knew how to trace constellations on your palm with their fingertip. And you couldn’t even remember their names without Jisung pointing them out to you.
Renjun tried. He filled the empty seat at meals, nodded at the right moments when you rambled, even agreed to sneak out once or twice. But he wasn’t Jisung. He didn’t know your weird inside jokes, didn’t lean his head on your shoulder when he got sleepy, didn’t touch your wrist when you got nervous.
You missed him so deeply it ached.
So, when you saw him slipping out of the common room one night you followed him without a second thought.
He moved quickly across the grounds, his hooded shape skimming the moonlit grass. You jogged to keep up, keeping low behind hedges and statues until he stopped beside the Whomping Willow. Your breath caught as he pressed a knot at the roots and the tree froze mid‑sway, its branches locking in eerie stillness. Then, an entrance yawned open.
You hesitated. Every instinct screamed that going after him was a terrible idea. But the thought of him hurting or worse, hurting alone was too much to bear.
So you followed.
The tunnel led you into the Shrieking Shack. A chill raced down your spine the moment you stepped inside. Rot and mildew clung to the walls, the floorboards seemed like they would give way with each step, and it smelled like old nightmares in there. You had to bite down on your lip to keep from gagging but you kept going, following the sounds of his ragged breathing upstairs into a dusty room.
You opened the door cautiously, barely an inch—but before you could fully register what was happening, Jisung lunged. He grabbed your arm, yanking you roughly inside and pinning you to the sagging mattress with a strength that startled you.
"Jisung—!" you gasped.
He loomed over you, eyes wild, glowing gold in the darkness. His expression was pained, almost feral.
"What—are you doing here?" he growled through gritted teeth. His voice was deep and barely recognizable.
You stared up at him, wide-eyed. “I—I was worried. You missed all your classes…”
Something dark flared in his gaze, and he dropped his head, panting harshly against your throat. He inhaled deeply, shuddering as he pressed closer instinctively. Your breath hitched sharply, your body reacting involuntarily to his closeness.
"You shouldn't have come," he whispered brokenly, hands trembling where they gripped your wrists.
You swallowed, feeling his hips press involuntarily against yours and realizing exactly what was happening.
"Your rut," you whispered breathlessly, realization flooding you. "It's started, hasn't it?"
A helpless whimper slid from his throat as his hips rocked against you once more, his erection pressing unmistakably through his trousers. The desperate sound he made sent heat pooling in your stomach, despite the fear and confusion swirling inside you.
“You smell so fucking… good” He let out another ragged noise, and you reached out instinctively, resting a trembling hand against his cheek. His skin burned under your palm. He looked almost delirious, golden eyes flickering between human fear and something more feral.
You’d spent the past week reading about werewolves and their ruts, absorbing every detail you could from hidden texts and restricted tomes. You knew that once the rut hit, the urge for physical intimacy would become nearly unbearable. You also knew it was dangerous for you to be near him like this.
But as you stared at your best friend, trembling and half-broken with need, your heart clenched. You couldn’t just walk away.
“Jisung,” you said carefully, your voice shaking. “Did you take the Wolfsbane?”
He shook his head, eyes squeezing shut. “I don’t know… I think I didn’t—” He broke off, a pained groan tearing from his throat as he rocked forward, hips searching for contact.
Swallowing hard, you remembered the passage in the book. How an afflicted werewolf needed a trusted partner to help ease the rut’s consuming effects.
It felt like your heart was in your mouth.
“You—” he gasped, voice faint. “You can’t stay. I—if I hurt you—”
You cupped his other cheek, forcing his gaze to meet yours. “You won’t,” you promised, though a part of you wasn’t entirely sure.
“Y/N,” he groaned, hips rutting forward again. “Don’t. Don’t touch me right now, I swear—”
“I want to help you,” you said softly. “Please let me.”
His pupils dilated immediately and he let out a shaky breath, leaning into your touch. The heat radiating from him was overwhelming but despite your own hammering pulse, you didn’t draw away.
Because somewhere deep inside, you knew this was the only way to help him.
His grip on your waist was bruising, claws just barely retracted. His body was sweat-slicked and trembling, panting through gritted teeth as he pressed himself flush against you.
“I warned you,” he growled, voice shaky with restraint. “I told you to leave.”
You pulled him closer up and felt how he shook under your touch. “You can have me”
He didn’t wait another second. Your clothes were suddenly nothing, the fabric ripped under his desperate hands. Your skin was bare before you had time to register the sound of seams tearing. His mouth found your throat instinctively, tongue tasting your pulse before he bit.
You winced at the pain and his hips rutted against your thigh, hard and frantic, his cock felt thick and straining through his trousers. He was whining soft, broken sounds between gritted teeth, like each second without you wrapped around him was tearing him open from the inside.
“You smell—fuck, you smell so good,” he gasped into your skin, humping against you harder. “I need—i need to be inside, I need—”
You spread your legs, breathless, head spinning from the force of it all. “I’m here, Sungie.”
He didn’t prep you, didn’t pause for a second—just spit on his fingers and shoved them inside you hard and fast. Stretching you wide while whispering obscenities you couldn’t even make sense of.
“So fucking tight—fuck—gonna ruin you—fill you up, knot you, make sure no one else ever gets to—”
You didn’t even realize he’d taken his cock out until you felt him line himself up with shaking hands, barely getting the tip in before he snapped his hips forward, burying himself inside you in one brutal thrust.
You cried out and Jisung growled, slamming his hand beside your head, forehead pressed to yours, golden eyes glazed over.
“Mine,” he gasped. “Fuck… Mine. Mine. Mine—”
Suddenly, he shoved your knees up, pressing them tightly to your chest as his hips snapped forward, rough and desperate. You cried out sharply, feeling stretched too wide, overwhelmed by the rawness of him filling you again and again. His teeth dragged harshly against your throat, marking you repeatedly, as if he couldn't bear the thought of anyone mistaking you for anything but his.
You sobbed beneath him, your body caught between pain and a pleasure that blurred into something unbearable. Part of you wondered numbly if it would have changed anything if you'd told Jisung it was your first time—if it would've made him pause, slow down, be gentler. But you knew it wouldn't have mattered. He wasn't fully himself, and even if some part of him wanted to stop, he couldn't.
You felt it then, the swelling at his base. His knot beginning to expand, stretching your entrance wider with every punishing thrust. Panic mixed with need, your mind spinning as your walls spasmed around him.
“Gonna knot you,” he panted desperately, voice breaking as he slammed into you harder. “Can’t stop—fuck, you feel so perfect—gonna keep you like this forever—”
He thrust deeply one last time and locked himself inside, his knot catching and sealing him within you. You screamed, body jolting at the sudden fullness, the pressure almost too much. He shuddered violently above you, his cum flooding hot and deep, twitching through aftershocks that made your thighs quake and your vision blur.
You barely had time to gasp a breath before his knot began to soften, still pulsing faintly inside you. But Jisung didn’t stop, not even for a moment.
Before you could recover, he flipped you roughly onto your stomach, the mattress creaking sharply beneath you. He pressed into you again slowly, his breathing ragged and hot against your sweat-damp back. You trembled uncontrollably beneath him, arms shaking, barely able to keep yourself upright.
“Jisung, wait—” your voice broke, a thin plea lost beneath the rasp of his breath.
But he didn’t acknowledge your begging. One hand pinned your hip firmly, the other flattened between your shoulders, forcing you down into the sheets until you couldn’t move. You felt the ache building again as he pushed inside you once more, pushing mercilessly against your walls. Your thighs burned, your body instinctively arching to escape the overstimulation, but he wouldn’t allow you to shift away.
The moment he felt how wet and open you still were, the last shred of his restraint shattered. His rhythm turned frantic, his hips slamming into yours so fiercely the air was knocked from your lungs with every brutal stroke.
You moaned helplessly into the sheets, fingers clawing at the mattress as your body surrendered. He wasn’t speaking now, wasn’t asking if you were okay—all you heard were harsh, ragged sounds torn from his throat, desperate noises so primal and raw they made your skin burn hot with shameful need.
His movements grew rougher, your bodies locked in a rhythm that erased any remaining thought from your mind. Your senses narrowed until all you knew was the brutal heat between your thighs and the ache of him stretching you. You took every thrust, helpless to stop, unable to do anything but accept the ruthless force of his body on yours.
His teeth bit sharply into the back of your shoulder, fangs scraping against your skin until you gasped in pain. His grip tightened, fingers bruising your hips as he pounded into you without mercy, branding you with every brutal snap of his hips.
With one final thrust, he buried himself impossibly deep, and you felt the knot swell again—filling you, stretching you beyond limits as he locked himself inside with a guttural growl.
His whole body jerked, cock throbbing violently as he spilled into you again. It was so much cum it leaked around the thick swell of his knot, your walls clenching tight, helpless to hold it all in. He held still, panting, hands trembling as he stayed buried in you, locked and pulsing.
He stayed inside you for what felt like forever, body trembling from release, your muscles fluttering weakly around him. His breath came in uneven bursts against your skin.
But even then, you could feel that he wasn’t finished.
He rutted again and let out a feral sound low in his throat, one that sounded more like a growl than a moan. And then he was moving just enough to slip free with a wet sound that made both of you shiver.
His hands moved to your waist, lifting you. He dragged you onto your back again, spread your thighs wide, and settled between them with a single-minded hunger that made your whole body pulse with anticipation.
His gaze dropped the moment he pushed back in and he groaned, eyes locked between your legs with an obsessive intensity. Your walls clenched around him as his cock slid in with zero resistance. His breath hitched, and he stopped for just a second.
His mouth parted when he saw the shape of him pushing inside you, deep enough to press against your belly, the bulge rising with every brutal thrust. He pressed his palm against it and let out a wrecked moan. The sight of his cock inside your belly driving him halfway mad.
“Fuck,” he choked. “That's me? inside you?”
You tried to answer, but all that came out was a gasp as he rocked into you harder.
He watched your stomach move with every stroke, how your cunt took all of him, again and again, walls fluttering around his cock like your body was desperate to keep him.
He was mesmerized. Staring with wide, hungry eyes as hips snapped forward with more force. One of his hands grabbed your thigh, the other pressing to your lower belly as he kept thrusting, rougher this time, watching the bulge disappear and return with every movement.
“Fuck,” he groaned. “you’re made for this—fuck—you’re made to take me like this—”
You could feel the knot swelling again, dragging harder against your soaked, overstretched entrance, until your legs started to shake. He braced both hands on either side of your hips, growled deep in his chest, and slammed forward. The knot forced its way in with a brutal stretch that made your eyes roll back.
His whole body jerked, head falling forward as a strangled moan left his lips. His cock twitched violently, knot fully buried, and you felt the rush of his cum flooding you again, deeper this time, deeper than anything had ever been.
His eyes were still locked on your lower stomach, wide and blown out with awe. The bulge in your belly pulsed with each twitch of his knot, round and taut with the sheer amount he’d pumped into you
“Look at that,” he whispered, almost dazed. “Look what I did to you.”
He reached out again, fingertips brushing against your stomach and the possessiveness in his voice made your body clench all over again.
“I'm inside you.”
He blinked, his eyes flickering to your face as he really looked at you for the first time.
You were trembling, bruised, and barely able to keep your legs from shaking. Your eyes were glassy, your body completely spent beneath him. And something in him seemed to return.
His hands gentled against your skin as he eased out of you slowly, knot slipping free with an aching stretch that made you whimper. You gasped at the sudden emptiness, but he didn’t leave you long. He kissed your thigh once, softly, as if in apology, and then lowered himself between your legs.
You barely had the strength to lift your head. “Ji—what are you doing…”
But he didn’t answer. Just held your thighs gently in his hands, spreading them open again but this time with reverence, not greed.
Then he licked a single, languid drag of his tongue that made your hips twitch weakly. He groaned low in his throat at the taste of you.
You whimpered, the oversensitivity almost unbearable but his hands kept you grounded. Thumbs rubbing soothing circles into your hips, mouth moving with an aching kind of care. He sucked gently at your clit, tongue flicking in slow passes, easing the pain into something warmer.
You threaded trembling fingers through his hair, tugging gently.
His mouth grew more desperate by the second, tongue dipping lower and teasing at your entrance where his cum was still leaking out. He groaned at the taste, sucking softly, messy and slow, like he couldn’t get enough of it. Of you.
He buried himself there with his nose pressed into your skin, mouth drinking you. You let out a soft cry, hips twitching against his face, and his grip tightened just enough to hold you still as he circled your clit again, tender but insistent.
“I need to make it better,” he murmured into your skin, voice hoarse and reverent. “Let me—please…”
You didn’t answer but the way your legs shook around his head told him everything. So he stayed there—worshipping the mess he made, tongue moving slow and devoted, lips soft and endless. He lost himself in you.
The first thing you noticed when you woke up was the pain.
It was deep and dull at first, but the moment you shifted, it sharpened—radiating through your thighs, your lower back, your hips. Your skin felt hot, stretched too thin in some places, sore in others. You winced as you tried to sit up, limbs trembling slightly from the effort.
Jisung was already awake. He was sitting on the edge of the bed, facing away from you, his robes wrapped tightly around him. His shoulders were stiff.
You swallowed through the dryness in your throat. “Ji?”
He stood up without looking at you.
You watched him move across the room, hands twitching at his sides like he didn’t know what to do with them. He picked up your clothes from the floor—torn in multiple places, seams ripped from how desperately he’d removed them the night before—and with a flick of his wand, the fabric mended itself slowly in the air.
“Get dressed,” he said flatly. “I’ll help you get back to the hospital wing.”
You blinked. “Back to the—what?”
He turned then, just slightly, just enough to look at you briefly. His eyes were guilt-ridden.
“You’re hurt,” he said. “I can see it.”
Your mouth opened, but no words came out.
“And I’m going to Snape later,” he continued. “I’m going to ask him to relocate me during the next cycle. Somewhere far from here.”
You stared at him, stunned. “Jisung, you don’t have to—”
“I do,” he snapped. “Because this—” He gestured toward you, his voice colder now. “This shouldn’t have happened.”
Your heart twisted.
“I told you to stay away,” he said. “And I didn’t mean that to sound cruel. I meant it because I knew I’d lose control. And I did… and now look at you.”
He walked toward the cracked mirror, stopped a few feet in front of it, and gestured for you to come closer.
You hesitated.
“Please,” he said, quieter now. “Just… come here.”
You stood slowly, legs shaking slightly under your weight. You wrapped yourself in the blanket and stepped toward the mirror.
Your reflection made your breath hitch.
There were bruises on your neck, angry bite marks along your collarbone and shoulder. Finger-shaped welts on your hips and thighs. Your lips were still swollen from where he’d kissed you too hard. Some of the marks looked deep. Others looked like they might last days, if not longer.
“I didn’t know I was capable of this,” Jisung said behind you, voice cracking.
You looked at him through the mirror. His face was pale, jaw tight.
“I’d rather suffer the worst pain a rut could ever give me than ever touch you like that again.”
“Jisung—”
“No,” he cut you off. “You don’t understand. I didn’t even care if I was hurting you. I couldn’t think. You could’ve cried, begged, screamed, and I still would’ve—”
He stopped himself, breathing hard.
“I’m not going to let this happen again. I’ll talk to Snape. I’ll take whatever dose he gives me. I’ll lock myself somewhere no one can find me.”
You stepped forward, reaching for him, but he flinched when your fingers brushed his sleeve.
He turned his face away. “Get dressed,” he said quietly. “Please.”
There was nothing else to say.
He handed you your clothes without looking at you again. When you were dressed, he silently moved to support your weight down the stairs and back toward the tunnel beneath the Whomping Willow.
Your legs ached with every step. Jisung’s arm was around your waist, holding you upright as you moved slowly down the path back to the castle, your freshly repaired clothes felt stiff and uncomfortable against your bruised skin.
You hadn’t said a word since leaving the Shrieking Shack. Neither had he.
His touch wasn’t warm, or comforting. It was careful and detached. Like he was holding you not out of care, but out of obligation.
Your heart hurt more than your body. You two had been close for so long. Even after he’d changed, after he came back cold, distant, guarded you still felt more warmth than right now. Like he was reaching for you even when he didn’t realize it. So seeing him acting like this was almost unbearable.
You tried to tell yourself it wasn’t rejection or shame. That he was just protecting you, trying to keep you safe. But it still felt like being left behind.
You didn’t even realize how close you were to the castle until the path curved and the first archway of the courtyard came into view.
“Park.”
Professor Snape stood just beyond the arch, his arms crossed over his chest, black robes billowing faintly in the wind. His gaze flicked over the two of you quickly. His eyes dropped to the way you leaned into Jisung, to your limp. And then he saw the bruises. Even with your collar pulled tight, they peeked out, the edges of bite marks and the faint discoloration just beneath the skin.
Snape’s eyes narrowed.
“Come here,” he said, voice cold.
Jisung didn’t move.
Snape stepped forward. “Now.”
You felt the panic rise in your chest immediately.
“Professor, wait. It’s not—he didn’t—” You reached for his sleeve. “He didn’t force me.”
Snape’s eyes snapped to yours, and for a moment, you almost stepped back. His expression didn’t change, but something in it darkened like your words had confirmed what he already suspected.
“I didn’t ask what he did,” he said sharply. “I asked him to come with me.”
Jisung’s jaw was clenched so tightly it looked painful. He didn’t say a word, just let go of you carefully.
You nearly stumbled from the sudden absence of support.
“I can explain—” you tried again, but Snape raised a hand.
“This is not your responsibility,” he said, more quietly this time. “And you are in no condition to be standing here arguing.”
He turned to Jisung once more.
“Park. Now.”
And without looking back at you, Jisung walked toward him.
You stood there trembling, arms wrapped around yourself, the chill settling deeper into your bones now that he was gone.
Jisung stood in the doorway of Snape’s office with his head hung low. The potions master had stepped away to ensure you made it safely to the hospital wing and to explain the delicate situation to the healers. Minutes stretched on endlessly until finally, he heard the sharp clack of Snape's shoes approaching.
“Go in,” Snape ordered coldly, gesturing toward the open door. The Hufflepuff obeyed silently.
Snape shut the office door behind them with a flick of his wand. The room smelled of ash and damp parchment, but Jisung could still smell your scent stronger than anything else; it clung to him, saturated his senses.
“Sit,” Snape instructed curtly.
Jisung lowered himself into the hard chair opposite the desk, shoulders slumped. He couldn’t bring himself to meet Snape’s eyes.
“How is she?” he asked softly, voice raw.
“She’ll live,” Snape replied coolly, summoning a few vials and herbs onto his desk. “Madam Pomfrey is treating the bruising you saw fit to decorate her with.”
Jisung’s head snapped up, panic clear in his gaze. “I—I bit her. More than once.” The admission spilled out before he could stop himself, heavy with guilt and shame. “Does that mean—”
“No,” Snape interjected sharply. “The curse passes only when the biter is fully transformed under the full moon. You were saturated with Wolfsbane, half-shifted but not contagious.”
Jisung exhaled sharply, gripping the chair arms until his knuckles whitened. Relief flooded him, but Snape wasn't done.
“However,” Snape continued, voice lowering dangerously, “do not delude yourself into believing she was truly safe. Had you missed even one additional dose, or had the moon been at its peak, she would already share your curse, and that responsibility would lie entirely with you.”
Jisung flinched. “I know. I—I keep hurting her. I keep losing control, and no matter how much I try to stay away, something just…pulls me back. I don’t know how to stop it.”
Snape regarded him for a moment in silence before speaking, voice softer but still edged with steel. “That’s because it is no longer a matter of mere control. You've complicated things significantly, Park.”
Jisung looked up slowly, eyes wide with apprehension. “What do you mean?”
Snape folded his hands on the desk, expression severe yet composed. “By marking her during your rut, you've effectively chosen Miss Y/N as your mate.”
Jisung’s breath caught, his throat tightening painfully. "Mate? I—what does that mean?”
“It means,” Snape explained, calm and clinical, “that your wolf has identified her specifically as an anchor. Such mate-bonds occur most commonly during adolescence, particularly around a first transformation. It's why you find yourself physically unable to stay away for long.”
Jisung swallowed, panic bubbling up again. “Is it dangerous? Will I hurt her more?”
“Not inherently,” Snape said evenly. “But the bond is permanent, Park. Your wolf will always crave her presence—most intensely near the full moon or during rut. Ignoring it will only worsen your aggression.”
“Then…what can I do?” Jisung asked desperately. “How do I keep her safe?”
“You must never skip your Wolfsbane. Take it every evening at sundown and report to me regularly so we can adjust dosage accordingly. Furthermore, and pay attention to this, you must manage your bond carefully. You cannot fight it entirely so stay close to her but with awareness, not indulgence. ”
Jisung flushed deeply. “But… after everything I've done, how can I risk being close to her again?”
Snape leaned forward slightly. “The greater risk lies in distance, your instincts will spiral. Proximity is crucial but do not confuse instinct for entitlement.”
Jisung nodded slowly, the weight of responsibility settling heavily onto his shoulders. “Does she…know?”
“She soon will,” Snape replied quietly. “But it is essential she hears it clearly from you. Be honest and thorough. Do you understand me, Park?”
“Yes, sir,” Jisung whispered. “I won't fail her again.”
Snape regarded him a moment longer, then produced a fresh vial of Wolfsbane, setting it decisively on the desk. “Good. Now leave before I decide silence is insufficient punishment.”
Jisung rose unsteadily, clutching the vial to his chest. He walked slowly to the threshold, feeling every step heavy with responsibility. Just as he reached the door, Snape spoke once more.
“Park, if you truly care for the girl, learn how to live with the wolf without letting it consume her.”
The door sealed shut behind him, and Jisung stood for a long moment in the corridor, the potion trembling slightly in his grip.
You lay on one of the hospital wing beds, half-covered by a sterile white blanket, the curtains drawn tightly around you. The air was too quiet, every sound outside muted by the silencing charm Madam Pomfrey had casted when she left you there.
You picked at your cuticles absently, barely noticing the sting where skin peeled back. Your hospital gown gaped at the shoulders, revealing the bruises along your arms in the shape of fingers. Jisung’s fingers. You should’ve been horrified and maybe you were a little bit but there was something strangely comforting about them. His hands had held you through something painful, but they had held you. It made you feel... needed. Like you mattered to him again.
Your thoughts scattered when the curtain parted and Madam Pomfrey stepped through, her face tight with concern. Behind her came Professor Sprout, head of Hufflepuff house. And just before the curtain fell shut again, you caught the edge of black robes retreating down the ward—Snape. He’d definitely told them everything.
You bit your lip and dropped your gaze.
“Hello, dear,” Pomfrey said gently. When you didn’t answer, she cleared her throat. “To begin with, I’d like to offer you a calming draught for the pain.”
“I’m fine,” you said quietly, though your whole body ached. You didn’t want to take anything that would fog your thoughts. You needed to stay alert to explain the situation.
“Well…” she murmured, unconvinced. “Then I’ll start with the surface wounds.”
She gestured toward the scratches and crescent-shaped bites along your shoulders and collarbone. You stayed still while she worked.
Professor Sprout stepped closer, arms folded tightly across her chest. “Miss Y/LN,” she began carefully. “There’s no need to be guarded with us. We’re not here to punish you… but there are a few matters that need to be addressed.”
You nodded wordlessly, eyes fixed on a wrinkle in the bedsheet.
“Madam Pomfrey will heal what she can,” she continued. “But the bite marks will take several days to fade. Magical injuries of this nature are… stubborn.”
“I understand,” you murmured. The marks didn’t bother you.
Professor Sprout hesitated, color rising faintly in her cheeks. “We also understand that Mr. Park was… in a heightened state when you were intimate.”
You saw her flinch slightly at her own words and you almost pitied her. There was no elegant way to discuss something like this. You nodded once.
“Am I correct to assume no contraceptive charms were cast beforehand?”
Your brows pulled together. You’d never studied contraceptive spells properly. You knew they were meant to be used before any intimacy though and given how everything had happened there hadn’t been time for anything like that. You shook your head slowly.
Professor Sprout exchanged a brief look with Pomfrey before exhaling slowly. “Very well. Madam Pomfrey will now perform a diagnostic charm to ensure no unintended consequences arise from your… encounter.”
You nodded again, tending slight when Madam Pomfrey raised her wand and murmured a spell. A pale lavender glow swept across your lower abdomen then faded without a flicker.
“No conception,” she announced softly. “Everything is normal.”
A breath you hadn’t realized you were holding slipped out and you noticed Professor Sprout’s shoulders ease a fraction.
Pomfrey lowered her wand, relief softening the stern set of her mouth. Then she hesitated, studying you over the rims of her spectacles.
“Dear, may I give you some practical advice?”
You nodded, cheeks still furiously warm.
She lifted her wand again. “There are several reliable contraceptive charms you can use. The simplest is Praeventa Conceptum. It’s quick, painless, and lasts a whole day.”
Professor Sprout cleared her throat delicately but said nothing.
Pomfrey demonstrated. She pointed her wand at her own midsection. “Circle once, clockwise, like so.” A pale halo of light traced the motion. “Then speak Prae‑ven‑ta Con‑cep‑tum. Stress on the second syllable of each word. The charm settles just beneath the skin and it’s a mild warming sensation, nothing more.”
You mimicked the motion in the air, whispering the incantation under your breath. A faint peach‑colored glow sparked at your wand tip and faded.
“Good,” Madam Pomfrey said, satisfied. “Remember, the charm must be renewed daily, and it is far more reliable when cast prior to any sexual activity.”
“Thank you,” you murmured, both grateful and faintly embarrassed.
Professor Sprout offered a small, reassuring nod. “Better to learn here than under far less ideal circumstances.”
Pomfrey tucked her wand away. “Knowledge is its own protection.”
“Again, you are not at fault for any of this,” Sprout added, voice firm. “Last night’s events were influenced by circumstances far beyond your control.”
“Is he okay?” you asked softly.
A shadow crossed the professor’s eyes. “Mr. Park is with Professor Snape now, discussing the seriousness of missing future doses of Wolfsbane.” Her tone suggested ‘discussion’ meant something closer to a dressing‑down. “He’ll be monitored closely.”
“It wasn’t his fault,” you said, fingers worrying the edge of the sheet. “I followed him there, fully aware of the consequences. I just wanted to help… and I don’t regret it.”
Madam Pomfrey’s brows knit, but it was Professor Sprout who spoke first. “Miss Y/L/N, no one here is assigning blame. What matters now is that both of you are safe, and that Mr. Park remains diligent with his potion.” Her gaze softened. “Your loyalty is commendable, but your well‑being is equally important.”
You nodded, swallowing the dryness in your throat. “I know.”
Pomfrey dabbed a final line of salve across the deepest bite mark. “You’ll be sore,” she said gently, “but you’ll heal. Rest here tonight, at least until breakfast.”
The curtain swayed gently as they left you alone, and you stared ahead thinking only of the warmth of his breath, the panic in his voice, and the way he’d whispered “you shouldn’t have come” like it had broken him to see you there.
But you would do it all again.
Madam Pomfrey cleared you for release just after sunrise. You dressed in silence, fingers brushing over the gauze she’d left on the deepest bite. She offered one last vial of bruise balm and a faint smile before sending you off.
It was Saturday, thank Merlin. There were no classes so most students were still sleeping. You were relieved as you stepped out of the hospital wing, and saw nothing but an empty corridor.
Though still a strange, hollow pressure settled in your chest. You missed Jisung.
You weren’t sure if it was the residual ache in your muscles, or the fading imprints he’d left on your body, but you felt the absence of him like it was stitched into your skin. You needed to see him.
And then, as if your thoughts conjured him, he appeared.
Jisung was standing at the other end of the hallway, just beyond the shaft of sunlight spilling in from the tall windows. He looked stunned to see you, like he hadn’t meant to be here, like his feet had brought him without his permission.
You hesitated.
Snape had surely warned him again—more strictly this time—to stay away from you. But still, Jisung took a step forward and you followed.
You met in the middle of the hallway, stopping close enough that your chests nearly touched. It wasn’t until you were standing in front of him that you realized how much he’d changed. He was taller now, just slightly, but it was enough to notice. His shoulders were broader, his presence heavier, like the wolf was still there beneath the surface.
He stared at the bruises along your collarbone, what little was visible through the open neck of your shirt. You saw the way his throat bobbed, how his eyes flickered with guilt.
“Are you—?”
“I’m okay, Ji,” you cut in gently, offering him a small smile. “Perfectly fine.”
“I’m so sorry.”
He exhaled shakily, and his hand reached for yours tentatively. You almost gasped at the contact. It had been so long since he touched you first. His fingers threaded through yours like they were remembering how easily he did this all the time before.
“You don’t have to be,” you whispered. “You didn’t do anything wrong.”
Your other hand rose instinctively, brushing against his cheek. He leaned into the touch immediately, eyes fluttering closed.
“Did Snape scold you too badly?” you asked, voice soft and teasing.
Jisung cracked a smile. “Yeah, I have to clean the Quidditch stands every day this winter without magic.”
Your eyes widened. “Seriously?”
He laughed. “I’m joking.” He paused, eyes searching yours. “Though honestly… I think I deserved one.”
You squeezed his hand gently. “You’ve been punished enough.”
He didn’t respond, just looked at you like he was still trying to figure out if this moment was real.
The corridor felt suddenly too small, so without speaking, you guided Jisung toward the nearest side door that opened onto the courtyard. The November air was sharp, but sunlight spilled across damp flagstones and carried the faint scent of wet leaves.
You walked side by side, your shoulders brushing now and then. After a long stretch of silence, Jisung spoke in a quiet voice. “Do you remember fifth year… when we hid in Greenhouse Three during that thunderstorm?”
You smiled. “And you spent the whole time pretending not to be scared of lightning.”
He huffed a soft laugh. “I kept thinking about that last night. How you held my hand and told me storms always pass.” He glanced at you, guilt and wonder warring in his eyes. “I wanted to go there initially. But then I smelled you, and I went to the Shack instead, thinking you wouldn’t follow me into a place like that.” He laughed bitterly. “I should’ve known better.”
The admission loosened something tight inside you. “Storms pass, Ji,” you said. “Even the ones inside us.”
He stopped, turning to face you fully. “Does this one? Because I can still feel it.” His gaze flicked to your neck where a bruise peeked above your collar. “I feel every mark I left on you like they’re on my body, too.”
You lifted a hand to his chest, just over his heartbeat. “You didn’t hurt me.”
He looked at you, like he almost believed it, but the tension in his jaw said otherwise. “Snape told me… the biting… it wasn’t random.” he dropped his gaze and bit his lip nervously “I… marked you.”
Your breath hitched, but you didn’t interrupt.
“He said you’re my mate now,” he said quietly. “That the wolf chose you. That’s why I can’t stay away. Why I can’t stop smelling you, hearing you even when you’re not around. Why it feels like something’s ripping open in my chest when I try to stay away.”
You stood still, eyes locked on his.
“He said I shouldn’t fight it. That if I try to pretend the bond doesn’t exist, it’ll make it worse. That I just have to be… careful and gentle with it. With you.” He exhaled, voice tight. “He said if I really want to protect you, I have to learn how to live with the wolf, not push it down.”
“What did you say?” you finally asked.
“I told him I’d do anything to keep you safe,” Jisung said. “And I meant it.”
You reached for his hand and he let you take it, though his fingers twitched.
“The bond… is that why you came to the Hospital Wing corridor?”
He nodded, shame creasing his brow. “I woke up and… I was already walking there. I didn’t think.”
“Then next time, think and tell me,” you said. “We’ll handle the need together. On our terms.”
He swallowed. “Snape says if I miss a potion… you’ll be in danger first.”
“Then you won’t miss it.” Your tone brooked no argument. “Even if I have to brew it myself.”
A faint smile ghosted his lips. “You’d sit through that smell?”
“I’d sit through worse.” Your thumb stroked over his knuckles.
He exhaled shakily, some of the tension easing, though the gold still flickered behind his eyes like embers. “I’m not safe yet,” he warned.
“That’s okay,” you answered, stepping close until your foreheads touched. “I’m not scared.”
For a while you simply stood in the sunlight, listening to the distant chatter of students who knew nothing about storms or wolves or the way a heartbeat could echo in someone else’s chest. His hand tightened around yours, and instinctively you looked up, meeting his gaze.
His eyes flickered down to your lips, hesitation clear in the tense line of his jaw. Before he could withdraw, before he could overthink it, you stepped on your tippy toes and pressed your mouth gently to his.
It began softly, a cautious brush of lips but it escalated quickly. His mouth opened hungrily, tongue sliding against your teeth, and you gave in with a low sigh. His hand found your waist first, pulling you closer, then slid up to cup the back of your neck, angling your head so he could deepen the kiss. Your fingers tangled through his messy hair, tugging gently. He groaned into your mouth, hips pressing forward instinctively until you were pinned softly against the rough stone wall.
“I can’t lose control again,” he murmured urgently against your lips but still he kissed you harder, as if he couldn’t pull away even if he wanted to.
“You won’t,” you promised breathlessly. “This is fine.”
His hips snapped forward again, pressing you tighter to the stone behind you. You knew you were out in the open—anyone could pass by and see—but caution melted beneath the heat of his mouth trailing down your neck. The dull soreness from the previous night faded to a faint pulse, replaced by something hungrier, as he sucked gently at your throat.
“Ji—” your voice shook softly, hands gripping his robes tighter. “You’re… you’re not still in rut, right?”
He pulled back just enough to meet your gaze. “No. No, I don’t think so,” he panted roughly, almost like he was convincing himself too. “It doesn’t feel the same as last night, but—” He exhaled shakily, pressing his forehead to yours “I want you. Fuck, I want you so bad—I don’t think I’ll ever stop wanting you.”
A helpless moan escaped you at the raw admission, your pulse quickening under his mouth when he kissed you again—softer now, more controlled, as if he was proving to himself he could do this without falling apart.
“I won’t let myself hurt you again,” he breathed, lips brushing your skin between each whispered word. “But you need to tell me if it’s too much”
You shook your head slightly, pulling him closer still, holding him like he was the only thing keeping you upright. “Ji, nothing’s ever too much with you. Just stay here… stay with me.”
He shivered, his breath hitching as he kissed you again, trying to ground himself in the feeling of you rather than the wild instinct still whispering beneath his skin.
Someone laughed nearby, close enough to remind you exactly where you were.
Jisung froze against you, his forehead dropping to your shoulder with a soft groan. “We need to move,” he muttered “If anyone sees—”
“Then come on,” you said grabbing his hand.
He followed without another word.
You tugged him along a narrow side-corridor, the secret path behind the Herbology wing that only upper years and rule-breakers bothered with. Past the old broom cupboard, beyond the faded tapestry of a witch laughing drunkenly into her wine goblet, your footsteps were quiet, your pulse anything but. It hammered through your veins, in your fingertips, your throat—everywhere Jisung’s hand stayed locked in yours.
Soon you stood outside Greenhouse Three, abandoned since the storm in your fifth year shattered half its glass panes. Now, ivy and moss crawled along the cracked glass walls, and no one had bothered to repair it, leaving the space forgotten and overgrown.
You slipped through the splintered wooden door, pulling him gently behind you.
Inside, sunlight spilled across broken tables and tangled greenery. Plants had grown wild, illing the air with the scent of damp earth, crushed leaves, and something faintly sweet. You felt your chest tighten from the memory of your younger selves hiding here together.
Jisung remembered it too, you could see it in the softening of his eyes, the way his shoulders relaxed slightly. He caught your lips again, slow at first, but deepening fast, pulling a moan from your throat. Your hands gripped the front of his shirt, pulling him in until you tasted him fully.
“I want you inside me,” you whispered against his mouth, fingers trembling as you tugged at his clothes again.
He groaned softly, forehead pressing to yours. “Say it again.”
Your breath shuddered. “I want you to fuck me, Ji. Right now.”
He kissed you once more, messy and desperate, before stepping back just enough to undo his belt. His hands shook slightly, desire evident as he freed his cock—already hard and flushed, leaking at the tip as he positioned himself between your thighs. You lay back on one of the old greenhouse tables, cool beneath your skin but sturdy enough for this.
Jisung dragged the head of his cock through your folds, groaning openly at how wet you were, coating him perfectly. He pressed gently against your entrance, one hand braced beside your head, the other gripping your hip, thumb stroking tenderly.
He met your gaze, eyes filled with heated care. “Tell me if it’s too much,” he rasped, voice thick with want but edged with concern.
You cupped his cheek softly, eyes locked on his. “It’s perfect. It’s always perfect with you…Just fuck me, Ji.”
And he did.
The first thrust was slow, a deep stretch that pulled a gasp straight from your lungs. His cock slid in inch by inch until he bottomed out, and then he just held there, buried inside, groaning like he’d finally found home.
“Holy fuck,” he whispered, his voice breaking. “You’re so tight, you feel so—shit—you feel like you were made for me.”
You clenched around him involuntarily and he hissed, head dropping to your shoulder as he fought the urge to move too fast.
But control didn’t last long. His hips started to roll into yours, picking up a rhythm that got harder with each thrust. The sound of skin slapping echoed off the glass, mixed with your breathy moans and the desperate groans breaking in his throat.
You wrapped your legs around his waist, heels digging into his back, dragging him deeper.
“Yes, yes—right there—don’t stop,” you gasped.
“I won’t,” he growled. “I can’t.”
He drove into you harder, the table creaking beneath you as he pounded into your soaked cunt like he was trying to carve the shape of himself into your body. You arched under him, nails raking down his back through his shirt, gasping every time he bottomed out and hit that spot that made your toes curl.
He pulled out just enough to watch his cock slide back in.
“Look at this,” he breathed, one hand dragging down to your stomach, pressing just above your pubic bone. “Can feel myself right here.”
You could tell Jisung was obsessed with seeing himself inside you, it made his thrusts hit deeper just so he could feel himself in your lower belly. You moaned brokenly, the pressure making it worse, the angle driving you insane.
“Fuck, fuck—I’m gonna come,” you choked. “Don’t stop—please, don’t—”
“I want to feel it,” he growled. “Come on, baby. Come for me.”
Your body clamped down around him, walls spasming hard enough to make Jisung curse violently. He fucked you through it, rough thrusts stuttering until his own orgasm took him.
With a strangled groan, he slammed into you one last time and came hard, cock twitching deep inside you as he filled you again with thick spurts that made your pussy slicker than before.
He collapsed over you, forehead buried in your neck, both of you panting like you’d run for miles. His cock was still buried inside you, twitching with aftershocks.
You dragged your fingers through his hair gently, voice hoarse. “That didn’t feel like your rut.”
He laughed, breathless. “No. That was just me.”
“Are you okay?” he whispered into your neck, voice raw and reverent. “Did I hurt you?”
You shook your head slowly. “You didn’t. You were perfect.”
He sighed against your skin, relief loosening his shoulders. Then, gently—so, so gently—he pulled out, groaning as his cock slipped free from your cunt. The mess between your legs was immediate, warmth spilling down your thighs, and you whimpered at the sensitivity.
“I got you,” he murmured, already reaching for his wand.
He muttered a quiet cleaning charm, careful not to touch you until you nodded. His hand brushed your knee, then your thigh, his fingers trembling as he whispered the incantation again and wiped away the rest with his robe sleeve.
When he was finished, he kissed the inside of your knee, then your hip, then your stomach like it was part of some silent apology only your skin could understand.
“I’m gonna help you down,” he said, voice soft.
You nodded, and he wrapped his arms around your waist, lifting you slowly from the table and holding you close while your legs adjusted. You swayed once, but he caught you instantly.
“You’re shaky,” he murmured.
“You fucked my legs numb, Park,” you whispered, trying to smile, and he let out a breathy laugh, burying his face in your neck.
“I’m never letting you go again,” he mumbled. “Not even if Snape drags me out of your bed himself.”
You held onto him tighter, forehead pressed to his collarbone. “You better keep that promise.”
He kissed your temple. Then your cheek. Then the corner of your mouth.
“I will,” he said. “Forever.”
He helped you sit on the edge of the table while he redressed—pulling his trousers back up, refastening his belt with one hand while the other stayed on your knee like he couldn’t bring himself to stop touching you. When he was done, he reached for your discarded panties, blushing faintly as he held them out to you.
“I should’ve asked first,” he said quietly. “Back then. In the shack.”
You looked up at him, heart aching. “You couldn’t. And I already told you… I don’t regret it.”
He nodded, but the guilt lingered behind his eyes. So you took his hand and laced your fingers through his again.
“We’ll be okay,” you said. “You and me.”
“We will,” he whispered.
You dressed in silence together, stealing soft glances and touches, letting the heat cool but not disappear. And when you finally stepped out of the greenhouse, blinking into the pale afternoon light, Jisung’s arm was already around your shoulders holding you close and as steady as the heartbeat you’d heard pounding through his chest not long ago.
And this time, when he kissed you, it wasn’t desperate or rushed. It was quiet and certain.
Like a promise kept.
eeeeek feedback is greatly appreciated! i love reading ur comments and anons <3
#nct x reader#nct dream x reader#nct smut#nct dream fic#nct imagines#nct dream smut#nct dream scenario#jisung x you#park jisung x reader#park jisung smut#park jisung x you#nct jisung x reader#nct jisung smut#nct fanfic#nct dream fanfic#nct dream x you#nct dream x y/n#nct dream x female reader#nct fic#nct angst
970 notes
·
View notes
Text

SOLID WORK; dr jack abbot x dr!reader
words: 4,700+
content warnings: my minimal medical knowledge, doctor humor, abbot’s filthy mouth, some smut, fluff <3
notes: i am so beyond new to this fandom and to tumblr so please stick with me but i couldn’t not write this🫶
・❥・
”Solid work.”
My breathing slows as I start to process the complexity of the procedure I had just performed. I’d probably be blushing at Dr Abbot’s praise if it weren’t for the adrenaline coursing through me.
“That was your save. Not mine.”
Trust me - I am never jumping to credit a man with my work but that was the truth. I may have physically done everything but the idea and the instructions that made it possible were all Dr Abbot.
I look back down at the patient. I tell myself it’s to make sure this is all real. That I really just did that. But if I am being honest it’s to avoid Dr Abbot’s unwavering eye contact.
“Hey-“
He is not gonna let me. I look up to meet his gaze. So rock solid but somehow so warm all at once. He may as well be staring right through me.
He lightly rests his hand on my forearm to stop me from going for the suture. To stop me from giving him anything other than my undivided attention.
“-you are the smartest person in here. Take the win.”
I can’t help the exasperated smile that spreads across my face. He’s right. I’ve only got a couple months left of residency. I should just take the fucking win for once in my life.
Abbot, much to my surprise, smiles back. And he has dimples because of course he does.
He’s calm under pressure, he lies on official paperwork to get a teenage girl the abortion she has every right to, he’s the actual smartest one here, he’s kind to everyone in this ED regardless of the stress he is under, and…he still has his hand on my arm.
His hand. The veins there don’t hurt the eyes either.
We must both realize his lingering touch at the same time because he is clearing his throat and pulling away. He reaches for a surgical instrument he doesn’t need. Picks it up and then puts it down.
I swear there is a faint blush on his cheeks but if I think about that too long one will appear on my own.
“Let Whitaker stitch this up. Go home - get some rest. Your shift ended hours ago.”
“I love Whitaker but he is so slow we may as well let the wound heal all on its own.”
Dr Abbot laughs. Genuinely, truly laughs as we exit out of the trauma bay. So loud that Robby looks over and asks if he’s okay.
Don’t get me wrong. Dr Abbot has a wonderful sense of humor. A wicked one, actually. But it’s one of those dry, witty kinds. Not the animated, giggly kind.
I tell myself it’s not a bad thing that I’m proud to have gotten a good laugh out of him. That it’s not a bad thing that it gave me butterflies. That’s it’s not a bad thing that I am laying in bed wondering how the hell I am going to get him to do that again.
・❥・
Jack lets out a low moan as he recovers. His eyes are dazed, his head slightly tilted back but not so much so that he can’t keep eye contact with me.
His hand that held the makeshift ponytail in my hair starts to massage my scalp as the other hand reaches for my chin and tilts my head up to meet his strong gaze.
Once he’s got me where he wants me, his thumb travels from my chin to my lips, swiping what’s left of his release off of it.
“My good girl. So good for me, yeah?”
My thighs involuntarily clench together at his words. He knows it too. I nod as his thumb presses further into my mouth, my lips wrapping around it.
His mouth quips into a smirk, “Solid work, doctor.”
I roll my eyes and bat his hand away. Standing up from my knees on my own. Ignoring his arms trying to gently guide me up instead.
“That! That is exactly what I am talking about!”
“I have no idea what you’re talking about, baby.”
Jack just laughs as he grabs my wrist, turning me back towards him. He’s quick to have me pinned up against our shower wall - his strong thigh spreading my own apart as he plants long slow kisses across my neck.
“You know exactly what I’m talking about.”
Back when I was a resident, otherwise known as a couple months ago, Jack consistently praised what I was doing by saying “Solid work.”
The way he did always made me dizzy. His voice would drop an octave and he’d look me straight in my eyes while he said it. There is nothing inherently sensual about the phrase but it took me a while to realize he was not complimenting the other residents like that.
Him saying it during sex started as a joke. Harkening back to when, as he puts it, I was so painfully oblivious to his flirting. To which I responded, “That was flirting?”.
He said it again to me at work the next day. Being completely and utterly genuine. I don’t even remember what I did but I did it well and he is always the first to acknowledge that. So he was confused when I just huffed in annoyance and peeled out of the room without so much of a glance at him.
I wasn’t annoyed at him. I was annoyed that now all I could think about was him. His hands, his biceps, his tongue. Everything. And I still had six hours of my shift to go.
He followed me into the on-call room I was going to find some refuge in. He locked the door behind him - closed the curtain for good measure.
“What’s wrong? Are you okay?”
And then I felt bad. He thought something was actually wrong. That no way I’d ever brush him off like that when he was just trying to compliment me unless something was seriously wrong.
His eyes bored into mine, genuine concern and love pouring out of them. And here I was just being a brat.
I tried to be sly about the way my eyes trailed the veins bulging out of his biceps. I tried to be sly about the way I was imagining my hands tugging on his salt and pepper curls that were just slightly askew from a couple hours work. Unfortunately for me, Jack can read me like a book.
“Did you just stomp out of the ED because you’re needy?” Jack couldn’t contain the grin that spread across his face at the realization.
“Well maybe if you weren’t always going Mr Christian Gray on me with the praise-“
“I don’t even know who that is but all I said was ‘Solid work’-“
Jack stops himself as he remembers the past couple nights. When he was saying the same thing in a much different context.
I can’t say I’m entirely innocent. Or innocent at all really. I love throwing in a ‘sir’ every now and again at work to tease Jack. So he does the same to me with other phrases - constantly.
And he said the same thing in that on-call room that he is saying to me right now, “But what I do know is how fucking wet you are for me. So stop pouting and let me taste you, yeah?”
He swipes a finger through my soaked folds before he’s the one sinking down to his knees as I try to keep mine from buckling.
・❥・
“Solid work, Dr Abbot.”
I smile down at my sparkling new engagement ring and then up at the love of my life.
“Seriously? You can tease but I can’t?”
“What’s that saying again? Happy wife, happy life?”
Neither of us can wipe the huge grins off of our faces. No one knows we’re engaged yet. Just how we wanted it.
A couple of months ago, right after I had taken an attending job at The Pitt, Jack had broached the topic of marriage. We’d talked about it before. We both knew we were spending the rest of our lives together. But we hadn’t actually talked about the timeline of it all - the logistics.
Jack was always extremely hyper aware about how our relationship affected me. He didn’t want it to interfere with my career or all of my hard work. So as much as he would’ve walked down the aisle six months ago, he wanted everything to be on my terms.
“Hypothetically - if I were to propose, say within the next month - would you say yes?”
“Hypothetically - if I ever say no to a marriage proposal from you - please get me a psychiatry consult.”
Jack laughed - in an airy way where you could tell he was relieved. I kissed him. There was no universe in which I ever said no to a proposal from him.
He pestered me with questions. He wanted direction but not so much so that I wouldn’t be surprised when the time came.
I told him I didn’t want anything fancy. No big party although I did want to have a small gathering with our friends and family at some point afterwards. A nice sized diamond but not gaudy. No grand gestures - just him being him is all that I wanted.
And he executed perfectly. Because when does he not. It was our first night in the new home we had bought. He said we could get a hotel while we waited for our furniture to be delivered. But I wanted to do one night with no furniture, an air mattress, some candles, and a pizza delivery.
“Like camping.” I had said.
“You hate camping.”
I laughed because he was right but he obliged me anyways. He carried me over the threshold and I made a joke about how he’s got to be careful - being old and all.
Then he carried me right over to the air mattress, said something like “Can an old man do this?” and went on to coax four orgasms from me - one from his fingers, one from his tongue, one from his thigh, and finally one from where I wanted him most.
When we were done, I threw on one of his old tshirts and a pair of boxers. He just had on an old pair of sweats and a white tee. We stared into each others eyes like two lovesick teenagers until he said “Come here - I gotta show you something.”
“Babe, the house is empty.”
“Get over here smart ass.”
Jack picked up a candle and lead us over to the fireplace. He set the candle on the mantle as I read what was now engraved into the stone ‘The Abbots - Est 2025’
“So this is why you were getting all of those random tools from Amazon.”
Ever the handy man he is. Then he was on his knee. His bad one. To which I told him he didn’t have to do that. And then he said he would even if it killed him. And I think I said something stupid like “Not on my watch.”
I don’t even remember what he said after that. He doesn’t either. We both blacked out from sheer happiness. All I really remember is him asking me to do him the honor of being his wife and me pulling him up off of his knee and saying ‘Duh!’ as fast I could before kissing him. Over and over and over again until that air mattress was just a deflated extension of the wood floor beneath it.
・❥・
Dana’s hand rests on my thigh gently. My leg stops shaking. My mind doesn’t stop racing though.
I'm not an anxious person. If anything, I can be relaxed to a fault. But I am an intuitive person - and something is wrong.
Where is he?
“Relax. When is that man ever late?”
“That’s why I’m worried.”
You would think I didn't have my own license or car the way Jack insists on driving me everywhere. He tells me it is to keep our insurance from being sky high. I may or may not be a bit accident prone when behind the wheel. I tell him it's because he's obsessed with me. He always huffs a laugh and murmurs something about two things being true at once.
The Pitt makes sense. Ever since Jack started taking on more day shifts to balance out our conflicting schedules, a lot of times we are arriving and leaving here together. But on the off chance we are not, he is still picking me up. Always with some kind of treat in hand - usually a McDonalds Diet Coke much to Jack's dismay.
Jack takes the saying 'If you're not early - you're late' far more seriously than anyone I have ever met. The day shift typically gets off at 7 PM which means he is usually here to gossip with Robby on the roof by 6:35 PM.
“Go - take a case! He’ll be here to pick you up before you know it.”
My dissents are quickly met with Dana shooing me from the nurses station and personally squaring my shoulders to the board.
I haven’t even read the first name when Robby appears at my shoulder.
“Where is your fiancé?”
“Say that any louder and you’re going to be my next patient.”
“Yeah because you two are so inconspicuous with the whispering and the giggling and the big honking rock on your finger and the-“
“-disappearing to 'clean' the on-call room.” Dana finishes Robby’s sentence as they both double over in laughter.
Dana, Robby, and Collins are the only people in the ED that know about Jack and I’s relationship.
Collins knew I had feelings for Jack before I even let myself go there. Robby knew Jack had feelings for me before he let himself go there. So they took matters into their own hands.
Collins had a $100 on Jack breaking first. Robby $100 on me. And he had an extra $100 to spare when he bribed Dr Ellis to ask me to take her night shift for a week. Oh, how that backfired on him.
Three shifts later and Robby was $200 in the hole.
Six months later, I was moved out of my city apartment and into Jack's house.
Dana offered to drive me home after shift one night. Because it was cold and rainy and my apartment was close by. My apartment that I no longer lived in.
Jack wasn’t picking me up - he was out of town at a conference. I insisted on taking an uber, the bus, walking - anything that meant not explaining to Dana why my new address was the same as Dr Abbot's. She wouldn't take no for an answer and yelled "Oh, I knew it! Bridget owes me $100!" when I finally fessed up.
One year later, almost to the day that Robby had to pony up on his bet with Collins, I had an engagement ring on my finger.
Tonight, after he picks me up, Jack and I are going to pilates together.
It was only a matter of time before Robby and Collins gave it another go and I bet Jack that Robby would fold before Collins.
What's the point in betting money when we share a bank account? Seeing Jack in the pink pilates grippy socks he does not know I got him will be priceless.
“Well, when you find him please tell him that he is late for our date on the roof."
"Stop dragging him up there - you already have a date tonight!"
"Yeah, one in which I need his advice on."
"Oh please, you're talking to the wrong Abbot if you need advice on how to woo Collins." Dana interjects. Not everyone in the ED knows about Jack and I but they do know Heather and I are best friends.
"Oh, I wasn't aware you two had tied the knot already. Do you want me to change your name on the board? I can do that right now actually. Does HR know? It'll just take a moment-" Robby teases.
I grab the remote out of Robby's hands as he laughs, "Okay fine - go have your little roof date but do not take long!"
"Well, we'd already be done if he wasn't late. Where is he by the way? He is never late for anything.”
“Yeah, don’t remind me.”
I step forward, my elbows on the counter of the nurses station and my head now in my hands as I groan.
“Relax. It’s Jack - we couldn’t keep him away from this place even if we wanted to. Especially with you in here.” Robby squeezes my shoulder and is off to what I assume to be the roof.
I check my watch before I stand back up to scan the board for real this time - 6:50 PM.
Where is he?
I pull my phone from my pocket. There’s no new message from Jack lighting up my home screen but I open up our conversation anyways.
From Jack: I miss you
From Jack: I can’t believe Langdon is getting to hang out with you right now and not me
From Jack: If you stay at that damn hospital any longer we’re gonna have to start forwarding all these packages you order there
Little does he know one of those many packages holds his new pilates socks.
To Jack: Oh please - as if more than half aren’t all your little go bag gadgets
To Jack: And to think our colleagues think I’m the drama queen
“Incoming - Trauma 1!”
I’m happy for the distraction. I’m gowned, gloved, and ready to go before the patient is even rolled in.
The doors to Trauma 1 fly open - but not with a patient. Just Dana.
“I’m going to get Robby! You should not have to do this.” Dana is staring pointedly at me before she’s off. I don’t even get a chance to respond.
Weird. I know I’ve only been an attending for a couple months but Dana had more confidence in me on my first day as an intern than she did just now.
I now understand why as the patient is rolled in front of me.
There he is.
Unconscious. Cold. Clammy. And slightly bloody from a small cut on his forehead.
My world stops.
“Heart attack.” Langdon is here.
Somehow all I can think of is Jack’s text from earlier. I want to laugh but I can’t. What if I never get one again? I’m supposed to see him in pink pilates socks tonight. Not in a body bag.
“CLEAR!”
Suddenly all the pieces from the past couple days are coming together and I cannot believe I didn’t catch it sooner. Can’t believe he didn’t catch it sooner!
“CLEAR!”
His dizziness. The increase in massages of his amputated leg. The quick heart beat. The rash.
I hear the commotion around me. But I’m not processing any of it until it’s directed at me.
“I said CLEAR! Move!”
This cant be happening. So I decide that it’s not going to.
“No!” My voice comes out way more feeble than I meant. Way more feeble than anyone in this ED has ever heard me.
“Well I hope you enjoyed being Abbot’s favorite because you’re going to kill him and your career in one go.”
“Langdon - he is not having a heart attack.”
“Yes he is!”
“No he isn’t - take off his leg!”
“Take off his leg?! Okay, you’re literally going insane. And I’m supposed to report to you?! I know I went to rehab but oh my gosh - CLEAR!”
“I’m going to clear you out of this trauma bay if you do not get out of my way.”
You know how they say a new mom could lift a car off of her new born baby? I’m pretty sure that’s the phenomenon I am experiencing right now. I don’t exactly know what other worldly force is taking over me right now but I do not question it. I am watching myself from outside of my body as I spring into action.
I shove Langdon to the side as I lift up Jack’s pant leg to remove his prosthetic. The prosthetic that noone else in this room would’ve known he had.
He doesn’t keep it a secret but he doesn’t exactly advertise it either. Especially when he refuses to sit down on a double shift. Ironically enough, that’s probably why he is on this table.
I spot what I’m looking for immediately but Langdon is the one who speaks it out loud, “Pressure ulcer - he’s in septic shock.”
“Thanks for finally using your brain Dr Langdon but we’re going to be using mine from here on out.”
“Blood ox is 91.” Someone yells. I don’t know who. What I do know is that 91 is dangerously low.
“Scalpel.” I demand.
“What are you going to do?”
“We need to drain this fluid before his organs start to fail.”
The first and only time Jack taught me this procedure it was his save. Now it has to be mine.
I tell myself that one day we will be sitting in front of our engraved fireplace. Old. Like, actually old. Not the fake old that Jack tries to pretend he is. With kids and grandkids - telling them the story of how Jack saved his own life through the transitive property. So I better get to work.
“Scalpel. Now.”
Langdon slams the scalpel into my hand. I ignore the looks around the room. The looks that say ‘The only person qualified to perform something like this in an ED is the patient’.
“Your funeral. And his.” I ignore Langdon.
I must have cut the most perfect incisions of my life. Performed the most flawless procedure anyone has ever seen from me. I don’t remember any of it.
The loud beeping slows. His blood pressure rises. Then his blood oxygen. Then the bag I drained is full and being disposed of by Dana.
When did she get here?
Robby’s hand is on my shoulder, trying to pull me away.
When did he get here?
I hear him tell Whitaker to get a suture and close up the wound. Oh, the irony. Credit where credit is due - Whitaker has gotten much quicker under Jack’s patient teaching. Thank fucking goodness.
I think of the first real laugh I got out of Jack. My eyes start to tear up but I stop myself. I will hear that laugh again. Over and over and over again. So much so that I would get sick of it if that was even possible.
Robby is apologizing profusely into my ear. He has nothing to be sorry for. But I can’t manage any words. So I just let him move me out of Whittaker’s way but I do not leave Jack’s side.
I can’t seem to register anything beyond Jack’s face that I’m seemingly trying to force into consciousness with my stare alone.
“Where the hell did you learn that?”
My head turns to Whitaker at his question but it swivels so fast back to Jack I think I give myself whiplash. Because I don’t speak - he does.
“Solid work, doctor.”
I’ve never been happier to hear those words come out of his mouth.
“Oh my god.” My hand clamps over my mouth as my head dips to Jack’s chest, my arms wrapping around his shoulders.
My adrenaline tank plummets to zero and I am absolutely sobbing into Jack’s chest. Whatever was coursing through my veins during that procedure is coming out in what feels like gallons of tears and hiccups.
I don’t care who’s in the room. I don’t care that everyone is slack jawed and staring and so beyond confused. I don’t care that out of the corner of my eye I see Perlah slapping a $100 into Princess’s palm.
All I care is that Jack’s hand has found its way into my hair and when I place my shaking hand on top of it to make sure it’s real - it is. Even better - it’s warm and dexterous and alive.
He’s alive and he’s here.
He gently guides my head out of his chest. I lift my chin up to look at him - give him the eye contact I know he is seeking. That we both are.
“Baby - I’m okay. I’m okay, I’m safe, I’m here. I’m not going anywhere.”
His voice is as steady as ever. His heart beat matching it. The beat that was so faint what seems like moments ago.
I let it calm me down. I place a kiss to his chest and lean up to do the same to his forehead. My hand tangles in his salt and pepper curls as I hold his sweaty forehead to my lips and then bring my own forehead down to meet his. I close me eyes and breath him in.
He’s alive and he’s here.
“Welcome back, brother.” Robby manages to choke out through a couple tears of his own.
“Just wanted to make sure you guys weren’t getting lazy at the end of your shift.”
We all crack a smile but only Robby speaks, “Does this mean I have to work a double?”
“Not if you go park my car. It’s in the ambulance bay.”
I speak a full sentence for what feels like the first time in days, “You drove here?”
“We had a date. Plus, I wasn’t feeling quite right.” Jack nods down towards his amputated leg like it’s nothing but a minor inconvenience.
I dig into his pocket and toss Robby his keys. Robby calls for a CT and a room with a bed before ushering himself and everyone else out to give us some privacy.
“And how are you feeling now?”
“I’m feeling like I’d like to make the woman who just saved my life my wife.”
My hand immediately flies to the small cut on his forehead. The blood dry and crusty, “How hard did you hit your head? We’re already engaged.”
Jack chuckles, places his hand on mine and squeezes, “I barely hit my head when I fell out of the car. I’m fine - I just really don't want to live another moment without being able to call myself your husband.”
So we don’t. Not really anyways. I make Jack get every fucking scan in the book that I think we hit our insurance deductible in under an hour. He humors me by lying in the bed in one of the ER rooms as I pump a myriad of fluid and antibiotics into him.
After a few hours his blood oxygen is perfect. So is his blood pressure and his heart rate. I don’t think I’ve taken my eyes off of him once. Or my hands. Running my hands through his hair, caressing his forehead, squeezing his forearm. Just to reassure myself he is here.
He understands what I’m doing. Hears what I cannot say. He grabs my hand on its next pass through his hair and presses a kiss to every single knuckle before speaking, “Baby, I’m sorry I scared you. I scared myself honestly. But I promise, I am not going anywhere. Ever. And I am so sorry you had to go through that. You should have never had to operate on me. I don’t know how you did that. I mean if it was flipped. If I saw you come in like that-“
His voice falters, his bottom lip quivers and he pulls me into the tightest hug as we both begin to cry. I think if we could crawl into eachothers skin, we would.
We stay there like that for a while. Until Jack grabs my face, kisses every single part of it, then whispers “I love you so much but I think if you pump anymore fluid into me you’re going to water board me.”
As if on cue, Robby whips the curtain open, “To the roof we go!”
“You can’t be serious.”
Robby holds up some kind of certificate as Collins and Dana round the corner.
In the hours I spent nursing Jack back to health, I went to the bathroom one time. And only because I hadn’t gone the last four hours of my shift and I own a huge water bottle.
In that one bathroom break, Jack had managed to get Robby ordained online and enlisted Dana and Collins to ‘decorate’ the roof.
We’re still gonna have our wedding ceremony and the reception and the whole ordeal. But I agree with him - I can’t go another second not married to him. Not after today.
So we go up to the roof. Jack still in his hospital gown and me in my scrubs. Robby officiates, Dana sings because she can’t help herself, and Collins ‘witnesses’ which really means crying.
Jack is kissing me before Robby can even say, “You may kiss your bride.”
When we come up for air, Robby claps both of us on the back and says, “Solid work, you two.”
I just kiss my husband again. Because he is alive and he is here
#jack abbot#dr abbott#dr abbot x reader#dr abbot x you#jack abbott#the pitt#dr abbot smut#dr abbot fluff#dr jack abbot x reader#dr jack abbot fanfic#dr jack abbott#dr jack abbot x you#the pitt hbo#jack abbot x reader#jack abbot x you#jack abbot x female reader#jack abbott x reader#jack abbott x you#jack abbott x female reader
797 notes
·
View notes