#there are more personality disorders out there you know
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The average Tumblr user visits about 67 pages every month.
Text
Reference Guide to Writing Drug Withdrawal
So your character has a substance use disorder (or physical dependence to a substance for another reason). This post will tell you how to write a scene (or story) in which they go through withdrawal.
NOTE: THIS POST DOES NOT INTEND TO COVER ANYTHING EXCEPT WITHDRAWAL, WHICH IS A VERY SMALL PART OF SUBSTANCE USE DISORDER AND PHYSICAL DEPENDENCE.
Substance Use Disorders and Physical Dependence:
Substance use disorders are chronic illnesses in which a person continues to use a substance (commonly nicotine, alcohol, cocaine, opioids like heroin or fentanyl, benzodiazepines, etc...) even when acquiring or using the substance can be dangerous or cause significant problems in their life (such as problems with money, safety, law enforcement, job security, child services involvement, or physical problems like wounds, infections, side effects, hangovers, and withdrawal). Substance use disorders are a common cause of physical dependence.
Physical dependence is also it's own problem and can occur for other reasons too. For example, many people take prescription medications that they would go through withdrawal from if stopped abruptly (say, because the pharmacy couldn't fill it in time and they ran out). Assuming that the medication is being taken as prescribed, physical dependence in itself does not mean someone has a substance use disorder.
So what is withdrawal? Withdrawal (sometimes called "detox") is the process by which a body stops being physically dependent on a substance. Generally speaking, it is unpleasant. This is because when a body is exposed to a substance repeatedly, it changes how it functions to accommodate that substance. When the substance is removed, there is a period of time where the body has to re-adjust to not having the substance.
For example, alcohol is very similar to the neurotransmitter (brain chemical) GABA. If you drink a lot of alcohol (more than about 4 drinks per day) for longer than about a month, the body decreases the amount of GABA it makes naturally to accommodate the "fake" GABA from the alcohol. If the alcohol is suddenly removed, the body doesn't have enough GABA, and the effects of not having enough GABA result in withdrawal symptoms.
The difference being, someone taking a medication they no longer want to take can slowly reduce the dose to minimize withdrawal symptoms. Someone with a substance use disorder usually finds cutting back nearly impossible. Because of this, managing physical dependence in someone with substance use disorder generally means giving them a similar substance which they get from a pharmacy and take continuously (methadone, buprenorphine), or a similar substance they can then taper off of in a controlled way (benzodiazepines, gabapentin).
Specific Withdrawal Syndromes:
Alcohol/Benzodiazepines:
These are the only two substances that result in a potentially life-threatening withdrawal syndrome, and it's essentially the same syndrome. As stated above, when taken for either 2 weeks for benzodiazepines or 4 weeks for alcohol, the body decreases the amount of GABA it produces naturally. GABA is the "brake pedal" in the brain, slowing things down and decreasing the amount of activity. If you don't have enough GABA, you get too much activity, which can result in severe anxiety, insomnia, seizures, hallucinations, high blood pressure, temperature, and pulse rate, heart arrhythmias, and confusion.
6-12 hours after a person's last drink, they will experience insomnia, anxiety, tremors, and headache.
12-24 hours after a person's last drink, if untreated with benzodiazepines or gabapentin, they may start to experience hallucinations (they typically know they are hallucinating at this point).
24-48 hours after a person's last drink, if untreated, they may start to experience seizures.
48-72 hours after a person's last drink, if untreated, they may start to experience a severe symptom known as delerium tremens. This is a state where they are hallucinating severely and they don't know they are hallucinating anymore. This is also a state where the person has heart rhythm problems that could result in death. This is the most dangerous period during withdrawal.
If a person makes it through 72 hours, they are usually in the clear as far as life threatening symptoms go, though they may experience mild symptoms like headaches and insomnia for long periods afterwards.
Note that medication for alcohol or benzodiazepine withdrawal like other benzodiazepines, phenobarbital, and gabapentin are given only for the first 5 days of withdrawal, tapering to lower doses each day. This gets the person through the dangerous part hopefully with no life threatening symptoms. It does not mean all symptoms are controlled, but they are hopefully kept on the milder end while the brain learns to make it's own GABA again.
Opioids:
Opioids include a range of drugs including prescription medications like oxycodone, hydromorphone, and morphine, as well as street drugs like heroin. Today, the street drug supply in many places is heavily adulterated. Many samples of heroin (and even "pressed pills" made to look like prescription opioids) contain the much stronger opioid fentanyl (which increases risk of overdose) and the sedative xylazine (which causes wounds) in addition to the expected heroin or oxycodone.
Opioids work by pretending to be endorphins- another neurotransmitter usually used by the body to reduce pain and stress. Similarly to GABA in alcohol use, the body reacts to having sustained high amounts of fake endorphins by decreasing the amount of endorphins it makes itself. This means, when the opioids are no longer present, the body can't make itself feel good or recover from pain.
There are many parts of the body that endorphins work in, including the brain, gut, nerves, and spine. When they are removed, symptoms include:
Nausea and vomiting.
Diarrhea.
Insomnia.
Anxiety.
Increased body temperature.
Racing heart.
Muscle and bone pain.
Sweating.
Chills.
High blood pressure.
There is not really a universal timeline for these symptoms like there is with alcohol. For someone who primarily uses short-acting opioids, withdrawal begins 8-24 hours after the last use (though anxiety and cravings can start much sooner). For people who primarily use long-acting opioids, withdrawal can take up to 36 hours to begin following the last use. Generally, symptoms peak within 1-3 days after they start, and acute symptoms last 10-14 days.
Unfortunately, someone who has an opioid use disorder will frequently experience cravings for very long periods of time (potentially the rest of their life) after they stop use. For this reason, people do significantly better at reducing or stopping use over the long haul if they are taking an opioid replacement drug like methadone or buprenorphine.
Methadone and buprenorphine are prescription medications that a person goes somewhere each day to get (methadone) or picks up each day from the pharmacy (buprenorphine). The drugs essentially make it so the person won't go into withdrawal and will have significantly fewer cravings for as long as they take the drug.
The management of opioid withdrawal is usually done by switching the person from a street drug to one of these opioid replacement drugs. However, it is important to note that methadone doesn't work immediately (usually it takes about 2-5 days of titrating it up to get it to a high enough dose to work, longer if the person has a very high tolerance). Buprenorphine requires a certain amount of time in withdrawal (usually a day or two) before it can be given, or it can make withdrawal worse instead of better (something called precipitated withdrawal).
Once someone is on one of these medications, they can choose to stay on them (recommended) or taper off (nice to be off meds in theory, but high rates of return-to-use).
Cocaine/Amphetamines:
Instead of pretending to be a neurotransmitter, stimulants like cocaine and amphetamines prevent the body from re-absorbing the neurotransmitter dopamine, leading to a whole bunch of it hanging out in the brain. This increases concentration and energy and boosts mood. However, taken over long periods of time, the brain kind of burns out and fails to respond to the high levels of dopamine.
You may have heard that amphetamines and cocaine don't have withdrawal states. That would be a myth. People who use stimulants repeatedly for long periods frequently have a withdrawal that is essentially the opposite of the effects of stimulants- they feel very tired, have trouble focusing, and feel depressed because their brains can't use dopamine the same way they did before the drug use. This may last for weeks after cessation of stimulants.
Unfortunately, unlike with alcohol and opioids, there's not a ton that can be done for this withdrawal. There have been several studies, including testing medications like the antidepressant mertazapine, the migraine medicine topiramate, as well as naltrexone and buproprion (also an antidepressant).
In Conclusion:
There is so much more to drug use, substance use disorder, and physical dependence than I am covering in this post. I am just covering a small part of physical dependence, however the cause, by discussing the effects and common treatments for withdrawal.
Thank you all for reading this far! I hope you learned something and will use it in your writing!
#whump reference#writing reference#whump#drugs#medications#drug withdrawal#substance use disorders#which is a better way to put it than addiction tumblr#physical dependence
83 notes
·
View notes
Text
Most of Stranger Things is within Will’s head…
Including El, the Mind Flayer, Vecna, and more characters...
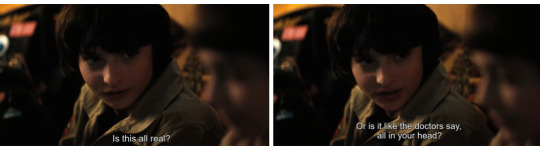
A lot of people aren't going to like this or agree but- if you are willing to read this at risk that you won't like it... try to keep an open mind and keep that curiosity door open.

(Above is a direct cut from Will to this line...)
I just want to begin by saying: I believe Will is the center of this show. I know many disagree, and place other characters at the center but let me explain to you why I believe the show is mainly about him.
The show begins with Will, as his disappearance is the catalyst for every single event to follow.
If you take a step back, and look at the show as a whole… making Will the center makes the most narrative sense. Without Will… there is no Stranger Things.
(GIF from @/kaypeace21's post here)
Lonnie hammering a nail into the wall while we cut to Mike poking a hole into a piece of paper visually tells a lot. Remember guys, this show is all about showing and not telling. Here they are showing us that the abuse Lonnie has inflicted unto Will caused the gate to open. The Upside Down exists due to Will's trauma. This is because the Upside Down is Will's mindscape.
DID and Internal Worlds

Will has experienced trauma far more severe than we are explicitly told. His trauma mainly leads back to his father. If you are prepared to read about the depths of said trauma, read this post. Not for the faint of heart though, my friends.
In Will's case, his trauma as led to a specific rare mental health condition called: Dissociative Identity Disorder.
Dissociative identity disorder (DID) is a mental health condition where you have two or more separate personalities that control your behavior at different times. When personalities switch, you’ll have gaps in your memory. The identities are usually caused by living through trauma. x
This means I believe that many of the characters we know and love were created from Will's mind. There are common alter roles within a DID system, and this show has been assigning different characters to some of these roles this whole time.
Now, this is NOT a new theory. The creator of this theory is kaypeace21 (one of the original Byler theorists!) Check out her posts here and here. While I agree with a lot of what she has to say, I do think she jumped the gun a bit with some things... specifically: the Persecutor Alter... more on that soon (not to fault her at all! As Vecna did not even exist prior to ST4).
Let's go back to the Upside Down being Will's mindscape:
Many individuals with dissociative identity disorder (DID) have an internal world in which they or their alters can manifest as themselves and interact. These internal worlds, which are also known as inner worlds or headspaces, can range in size and complexity. x
The Upside Down = Will's internal world. Those that inhabit that world or arose from said world are likely Will's alters. Yes, that includes El, the Mind Flayer, Demogorgons, etc. and of course: Vecna.
Here's another visual clue! A hole in the wall (an opened gate...) at the Byers' house that may have "always been [there]".
I know we are told the gate had opened prior to Nov 6, 1983, and that El had been the one to open that door/gate. But... that's because El herself is Will. She is a personality that had developed from him.
Now, lets talk common DID alter roles and how some of our favourite characters fill these roles to a tee.
El, the Gatekeeper Alter
I talk about the Willel theory here but I'll explain it briefly. El is "the gatekeeper", she is the one who Will lets "front" most of the time. Because remember guys... Will "likes to hide".
El was even compared to D’art (who came from Will…) see post here.
Also worth noting: Will's abduction in the shed is compared to... the first atomic bomb (used in an act of war) called "Little Boy". Post about that comparison here. What occurs during a nuclear reaction? Nuclear fission. Fission meaning: SPLITTING INTO TWO! Just as we see with the Phineus Gage comparison. That exact moment was when "El" emerged from the UD (Will's mindscape) into "reality". Leading to her becoming... a literal gatekeeper for Will.
She also helps solve Will's dilemma of to stay or to go, as Will himself stays (in the UD) and El goes.
So... what do I mean by “the gatekeeper"?
A gatekeeper is an alter that controls switching or access to front, access to an internal world or certain areas within it, or access to certain alters or memories. x

Now. Remember guys, we literally see her closing the gate and she (allegedly) was the first to open said gate. She also is heavily associated with repressed memories (the whole NINA plot...)

El has always been protecting Will from facing his trauma and facing himself. That is why we see her "save" him multiple times, why she takes on the role of Mike's romantic partner, why she takes the brunt of the bullies at Lenora, and why Will looks on like a helpless bystander... It is not due to resentment nor cruelty but fear. Will has been hiding behind her this whole time. He is not ready to face his memories, trauma, and the world. Not yet...
The Mind Flayer, the Demon Alter

In abusive groups, a young child can be severely traumatized in order for abusers to intentionally create an alter, and the alter can be tricked into believing they have been possessed by, and have become, a demon. X
This one is pretty self-explanatory, as we literal have a "possession" plot line involving Will. Though, instead of being "possessed", this alter of Will's was fronting.
Vecna, the Persecutor Alter

This is the one I'm most excited (and nervous) to talk about because it is SO fascinating and it matches his character perfectly.
So basically, Vecna is NOT Henry Creel. Vecna is an alter of Will's existing in his hive mind. Hear me out about this.
What I believe is that Henry Creel (or perhaps Edward Creel), was a real person that Will had heard about resulting in him creating an alter based on him. This is called "Factive Introject":
An alter with the form, personality, and possibly the psychological backstory e.g. memories of an outer-world person, whether a relative, a celebrity, or even an acquaintance. x
I believe that when we see "Henry" within both the Rainbow Room AND the Upside Down... this is Will's alter. (The Rainbow Room is likely another inner world of Will's...).
Are you still with me on this? Because lets get into the real evidence here.
What is a persecutor alter?
Persecutors are alters that purposefully harm the body, system, host, core, or other alters, sabotage the system’s goals or healing, or work to assist the system’s abuser(s). x
I know that sounds pretty scary, and some easily dismiss persecutor alters as "evil" BUT they are not. Viewing any alters this way is harmful. All alters' goals are to protect the system, even if they may do so in misguided ways.

x

Most persecutor alters start out as protector alters… which exactly what we see in the show! “Henry” is kind and protective towards El (who is another alter).
Then he decides to “kill” the other kids/alters (I say kill but they will still live on in the mind.)
Lets look at the exact terms used to describe the effects the persecutor alter has on the system...
X
Headaches…
Internal bullying…
Increased blank spells…

Interference with function…

Self-multilation…
Still have doubts on this? Let’s continue…
x
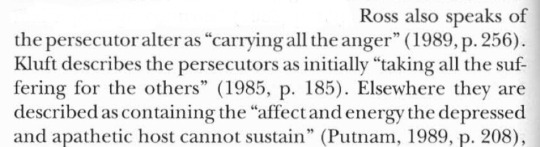
As I said, the persecutor alter is not "evil", it is a misguided protector. Its goal is to protect and often does this by taking on all the suffering experienced by the host and the alters...
But why? Why does the persecutor alter do such things if the goal is to protect?
X
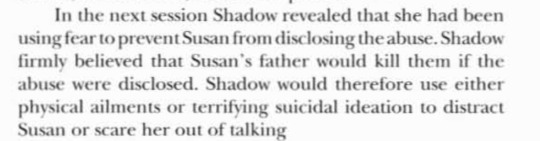
To prevent the host and alters from disclosing their abuse. Think about this for a moment. What did Chrissy, Fred, Patrick, and Max all have in common (other than trauma)? They all were seeing the student counsellor Ms. Kelley and revealing to her aspects of their trauma and abuse.
Vecna, as the persecutor alter, was having NONE of that and thus… “killed” them to protect the system. As he feared the consequences for Will/the system as a whole.
This is VERY telling for Will, because he has long been afraid of opening up about his abuse, trauma, and everything…

We see this emerge in many forms:
The Byers phone frequently going unanswered throughout the show due to Will’s fear of opening up/communication.
Lonnie telling Jonathan to keep his mouth shut for his mom’s sake…
The rats in ST3. To “rat” = to snitch.
El’s bullying in ST4. Angela repeatedly refers to her as a “snitch” even though she never did snitch.
Papa/the Demogorgon/Neil, the Abuser Alter
x I’m going to go right out and say this: “Papa” represents Will's abuser. We see him abuse El, Henry and others in a manner similar to what Will had experienced with Lonnie.

That’s why he’s called “Papa”, as he is a representation of the abusive papa of Will: Lonnie Byers.
Like Henry Creel, he is also likely based off a real person... Richard Brenner perhaps?
"That's what I have to do to keep her close to me. I don't want her going out. Men only want her for one thing and then they hurt her. She doesn't need anyone else but me." In addition to intimidating her so that she would not seek contact with men and risk further abuse, [the abuser alter] was also possessively trying to strengthen her attachment to him. X
This perfectly applies to Brenner's relationship with El, Henry and the others. He wants to isolate them to "protect" them from further abuse. We see this clearly as Brenner prevents El from leaving NINA, at all costs.
Again, even the alter representing the abuser should not be seen as “evil”. It’s complicated. All alters are aspect of the host, they are not evil. There are good intentions behind the bad actions.
Other Alters…
So, I believe other characters are also alters of Will’s such as:
Max, Billy, Chrissy, Fred, Patrick, Eddie, Argyle… and more. This post is getting far too long for me to expand on that just yet though.
Mike is “The Key” but… he’s not the only key

Let’s not forget about Ms Kelley and her key necklace!
Although Mike’s love will be an incredibly important aspect to saving Hawkins and saving Will… Will also needs to open up, face his trauma, and reveal his truth. Keeping all of this bottled up inside is causing far more problems…
When it comes to treatment for DID, there are different methods. Some include:
Identifying and working through past trauma.
Managing sudden behavioral changes.
Merging separate identities into a single identity. x
The latter being a highly controversial one, and it may not be the right choice for everyone with DID.
Within the show however? We will likely see merging or fusion of some of the characters in the end (we likely already have too...)
We already have foreshadowing of fusion between Will and El:
Robin and Steve discussing the act of "combining" to "solve all [their] problems".
Dustin hugging El and Will only to have El visually disappear during their hug.
El ending the season standing alone in the Upside Down.
In DID there's also a concept called integration, which may not be as extreme as fusion.
The individual must then make the choice of to what extent they want to integrate their alters as part of their healing. Again, some degree of integration is inevitable. The individual must integrate traumatic materials in order to heal from PTSD. As well, enough integration between alters must occur to allow for easy communication, a lack of dissociative amnesia between parts, and a consistent sense of being grounded in the present and in the body. The individual must be able to take responsibility for all of the system's actions, and all alters in the system should work together towards the same goals. x
Basically, Will must become insightful of his condition and see all aspects of himself (all alters) as helpful (even if they may be misguided). It will NOT help him to simply "kill" any alters, that will not work. He must accept himself for who he is. He must learn to love all aspects of himself.
I won’t touch on it here, but I will just mention that I’m very confident the show will end with another realm/internal world that’s beautiful and full of life. Implying that Will has finally found some peace of mind. I talk about it in this post.
#I don’t think you guys are ready for this one………….#most controversial post yet#stranger things#Stranger things theory#Will Byers#byler#Vecna
62 notes
·
View notes
Text
I don’t remember if it’s suggested on these or not but one handy free place that’s been a huge help for me has been library’s they offer free resources entertainment and events sometimes the events where I am at least the events come with snacks if you stay till the end they often give away said snacks.
And there not a thing everywhere but friendship centres or community centres are also great resources and often have food bank like programs and events to meet and be a part of a community along with some free food.
Buy nothing/ free groups on fb etc are also popping up in both cities and small communities
There’s often condition specific support groups to be found if not in person then online my family’s found ones for cvs, thyroid disorders and more of our conditions on fb etc
I couldn’t find the link but there was a really good cookbook book/file floating around here with different low $/low spoon food ideas/ recipes. I’ll send a link if I find it
take my hand for a moment
your objective from this point on is to survive
the election results are going to take a few days. The world is going to be very tense. I want you to take all the things you like to do to distract yourself and splurge on them. I want you to go eat your favroite foods and spend time with friends. I want you to do what you gotta do to make sure you can make it through the week.
There are people out there who want you to survive. There are people out there who are just as scared as you are.
We'll get through this. We will find a way
18K notes
·
View notes
Text
Also preserved in our archive
Dr Aspa Paltoglou hears from physician Dr David Joffe about what’s needed from our discipline; from Janina Bradshaw about what Psychotherapists can do; and from occupational therapist Kirsty Stanley.
Iam a psychologist – a Senior Lecturer in Psychology at Manchester Metropolitan University – and I have felt a bit useless in the last five years. From where I stand, I can see overwhelming evidence that Covid-19 has terrible and long-term consequences for people's health, and I have questioned whether Psychology is the specialism holding the key to dealing with Covid-19.
Many times I have wished I was a virologist, or an engineer that could help clean indoor air, or somebody that could develop vaccines against Covid-19, so that I could contribute to the eradication of Covid-19 and successful interventions for Long Covid. Or maybe a politician, so that I can pass laws for issues such as universal masking in healthcare and other public settings, clean indoor air in all public spaces, more research grants on Covid-19 vaccines and for Long Covid interventions.
I have written for The Psychologist about my personal approach to continuing pandemic precautions, and the support I have received in this. But there's another side to that – the Covid misinformation and minimisation I have seen. The idea that Covid poses no greater risk to the large majority of the population than the flu, which is simply not true. The overemphasis on the negative impacts of lockdowns, over the fact that there were 'no good options' at the time and without such measures many more would have died. Sometimes there is no mention of the possibility that Covid-19 infections could be responsible for cognitive deficits and decline in the population. Some people continue to suggest that Long Covid is primarily a psychological disease. The notion that ME (which has considerable overlap with Long Covid) can be treated by graded exercise and CBT has contributed to deterioration and death of patients – have we learned nothing?
And here's the thing: from what I have seen, Psychologists themselves have not been immune to this minimising of Covid, or the sharing of misinformation. With that in mind, I was keen to seek out broader conversations around the edges of our discipline, to ask other professionals how Psychology can support themto deliver effective care to Long Covid patients.
First, I contacted Dr David Joffe, a physician, researcher and Vice-Chair of the World Health Network Long Covid Working Group.
Thanks for your time, David. Can we start with one area where you think psychological help is important for Long Covid sufferers?
Yes. There are several examples of cognitive and emotional impairments associated with Covid-19 infections and Long Covid. We already know that the fronto-temporal injury mediated by hypoperfusion – decreased blood flow through an organ – will considerably affect mood. The incident rate of post-infectious depression is considerable. There are also several ways repeated in which Covid infections can lead to cognitive impairments and increased risk of Alzheimer's disease. Similarly, Yunhe Wang and colleagues noted in Naturethis year that 'compared with contemporary controls, infected participants had higher subsequent risks of incident mental health at 1 year, including psychotic, mood, anxiety, alcohol use and sleep disorders, and prescriptions for antipsychotics, antidepressants, benzodiazepines, mood stabilizers and opioids.'
The incidence of PTSD as a consequence of prolonged Intensive Care exposure and a life-threatening illness are also vital to consider. That can sometimes manifest as 'survivor guilt'. Furthermore, injury to the hippocampus and amygdala have been clearly established and are linked to PTSD.
There is also clear evidence of Dopa Senescence with rising cases of REM sleep Behaviour Disorder and an increase speed of neurodegenerative processes following infection. The integrative role of dopamine and serotonin imbalance are clearly another marker of this process.
What is Dopa Senescence?
Yang and colleagues recently demonstrated direct Dopamine cell aging and death. The usual pathways of cellular recovery are damaged. The virus causes direct cell death, but also prevents the usual cascade of enzymatic repair from being activated… hence the term senescence. This is what we are so worried about. I have 20+ Long Covid patients with laboratory-confirmed REM sleep Behaviour Disorder. The average age is about 40. It's primarily a condition we used to see in older men with a high rate of Parkinson's or Lewy Body Dementia. Will they be the same? Time will tell.
Which psychological therapies could be relevant, and why?
We need psychotherapists and other psychological practitioners to treat phobias and PTSD. Many Long-Covid sufferers have significant issues with phobia related to the risks of repeated infections in a world devoid of mitigation. It's essential we get supportive psychological therapy, from CBT to strategies to improve impulse control and reduced socialisation.
Addressing the phobias could help them continue taking effective Covid-19 precautions, such as wearing well-fitted respirators, without any unwanted psychological distress.
What else would be helpful?
Therapies such as Dream Rehearsal Therapy and other non-pharmacological treatments have been used for a long time, and are known to be very effective in treating some psychological disorders such as PTSD in parallel with pharmacotherapy. We need Neuropsychologists to measure cognitive challenges and suggest therapies.
In terms of research, as a Sleep Physician with expertise in neurocognitive dysfunction and driving in OSA, there's a critical role of Neuropsychologists for both primary and secondary evaluation of metrics, such as short-term memory, attention, concentration, visuospatial agnosia and apraxia. Repeated measures following a therapeutic intervention, or merely as a guide to rate of progression will be critical. At this point, there is little data to determine the risk and rate of progression in those with prior normal function. We just don't know.
Are there also emerging concerns as the virus changes?
Yes – with the Omicron variant, the evidence for greater neurotropism (i.e. the ability of a virus to invade the nervous system) has been realised. And there is a growing concern of rising ADHD as a consequence of direct putamen injury. This will have considerable implications for those practising in Educational and Child Psychology.
Last but not least, the toll on partners who are now carers, and kids who have disabled parents, should not be underestimated. Couples Counselling and Supportive Family Counselling should be considered crucial. These roles have been underestimated and severely underfunded. I have mentioned the damage to kids. They are not protected against Long Covid. As an Adult Physician, I am not positioned to advise in this regard, but they have been poorly treated in general.
Would you also have an overall message for our readers?
Yes. Although we need the input of Psychologists, please do not psychologise ME/CFS or Long Covid. The Psychology community needs to understand that this is a direct organic, neurological condition, with a plethora of complex outcomes, including severe consequences for autonomy and quality of life. The presence of depression, dementia, and PSTD are clearly evident from the vast body of literature.
The ME/CSF community have long railed against the 'Psychologising' of their conditions. The evidence for interventions such as Graded Exercise and CBT in isolation have been questioned and debunked. That community were right to warn us of potential missteps being repeated for a condition with vastly more neurological sequelae, and immense disability.
It is crucial that issues around plans for Rehabilitation and 'Return to Work' strategies appreciate that the vast majority of Long Covid patients will never achieve anything close to their prior function. Mental and physical pacing, reducing workload, and supporting people to manage these tasks can be helpful strategies. But there needs to be a recognition that these patients will likely not return to baseline.
Clinicians cannot manage the psychological damage alone. Psychologists must be properly educated and informed to realise the consequences. Let's see the back of those that consider this a malingering condition, or one that will improve with 'a bit of CBT'.
Thank you Dr Joffe for your insightful comments… I think they will empower practitioners and researchers to focus their efforts in the right direction. Long Covid is a physiological condition with some psychological and neurological consequences; Psychologists can help address these consequences, but we should not expect psychological therapies to be anywhere near sufficient to treat Long Covid.
There is still a lot we don't know about Long Covid. We need to learn, fast, and get this right as Psychologists.
Next, I approached Psychotherapist Janina Bradshaw. Here's what she had to say.
Long Covid or Post-Covid condition is a complex and multi-faceted syndrome, with over 200 symptoms listed under this broad umbrella term. The latest figures from ONS suggest at least two million people in the UK may have this condition. This includes over 100,000 children and young people. It is a massive and growing problem.
Many with the condition feel neglected and overlooked by the medical establishment – research is under-funded and there are no known cures (although there are some treatments and therapeutics in trial).
There is a danger that Long-Covid (LC) could be psychologised, in a similar way to CFS/ME – which is also a complex condition which for many years has been viewed as being of largely psychological aetiology. It has sometimes seemed that with a very complex condition that we don't know much about, if medicine doesn't have the answer, it must be the patient that is 'at fault'. We might see this as medical gaslighting. Given that government and the medical establishment's response to Covid can appear to be to downplay the ongoing impact, many with LC may be left feeling disenfranchised, rejected or even harmed.
I do want to emphasise that although there is some overlap in symptoms between CFS/ME and LC (particularly Fatigue, and Post Exertional Malaise [PEM]), LC is a much more heterogeneous condition than CFS/ME. Many with new onset health conditions (which includes but not limited to Diabetes, Heart Conditions such as POTS and pericarditis, Cognitive Decline and 'brain fog', other autoimmune conditions, plus the re-activation of viruses such as EBV) may not even realise that these new onset conditions are as a result of their previous Covid infections. At present, the medical establishment are not fully making these links either, despite there being many studies which point to Covid as a precipitating factor.
If you were a previously relatively health and active person, it may be assumed that this loss of health status is a major issue to adapt to. At present, we do not know if people will ever resume their previous functioning. It is the role of therapists to assist people with their process of coming to terms with this.
As a therapist, I want to stress that LC has a clear physiological basis, requiring medical input and much more research to begin to address the physical basis of this condition. However, I do think that therapy practitioners have a role in assisting LC patients in coming to terms with the grief and anger they may be feeling as a result not only of developing LC, but also due to the lack of an adequate response to the pandemic which has resulted in lack of appropriate treatments. Given that health and social care workers, teachers and others who work on the 'frontline' are over-represented in the LC population, as well as people from more deprived economic backgrounds and those from ethnic minorities and women, therapists have a role in offering a listening ear. It's about allowing expression of the grief and anger, and also acknowledging and supporting people to find their voice in the face of such systemic injustice.
Another issue I think is important to reflect on as psychotherapists is this: why are so many people so willing to accept the continuing immense impact the Covid is having on the population? My impression is that grief and trauma from the start of the pandemic, coupled with the inadequate and deceitful conduct of government, plus a lack of public health messaging, has left many people so unable to face this ongoing reality that they are heavily in denial. They are unable to grasp the very real harms that repeat Covid infections are having on them and their children. There is probably also a lot of guilt that people will have to face if they realise how their actions are contributing to this ongoing harm.
Repeated Covid infections increase the chance of developing Long Covid, so prevention should always be an important part of our strategy to deal with Long Covid. Psychotherapists could help and empower individuals to use protection such as masking and help them deal with the psychological conflicts of being one of the few to still being Covid cautious in a world that seems willing to ignore Covid-19.
From my part, I will do everything I can to help people with Long Covid. I believe psychotherapy can have a positive effect in the lives of the people that suffer from this debilitating illness.
I thank David and Janina for their thoughtful input.
Finally we spoke to Kirsty Stanley, an Independent Occupational Therapist and Health Lead at the charity Long Covid Kids, about the issues she is seeing.
Understanding the wide ranging co-morbidities that can occur following COVID-19 infection is essential for appropriate diagnosis and management. Children and young people (CYP) can display similar Long Covid symptoms to adults, but they are far less likely to be offered medications for Long Covid's common co-morbidities such as Postural Orthostatic Tachycardia Syndrome (PoTS), instead only being offered self management options. Additionally CYP can develop Paediatric Acute Neuropsychiatric Syndrome, an equally misunderstood neuro-inflammation condition, that can initiate tics, emotional regression and hallucinations, which can respond to antibiotic treatment. Many families feel forced to seek expensive support from private practitioners. Gastrointestinal symptoms are also extremely common and can present as disordered eating but may be mistaken for eating disorders.
Post Exertional Malaise (PEM), also known as Post Exertional Symptom Exacerbation (PESE), can be a particularly troubling symptom for the CYP, their parents or caregivers and professionals to understand. The delayed onset of symptom exacerbation following physical, cognitive and emotional exertion can make it seem like CYP are functioning well. The subsequent inability to attend school due to these severe symptoms then sees some families at risk of fines or, in growing numbers of cases, referred to social care for neglect, or fabricated and induced illness claims. Whilst professionals should always be alert to the possibility of abuse, it should also be recognised that the negative and long lasting impact on families of false claims is immeasurable.
Where adults may find equipment, aids and adaptation readily provided, children have regularly been told to avoid using wheelchairs due to the risk of 'deconditioning'. We need to recognise that without vital mobility aids many can become stuck at home, or indeed in bed, unable to engage in daily life. CYP talk about the loss in friendships, as peers move on with their lives whilst they struggle to engage with activities where they need to pace or plan energy. Finding community with other disabled peers can be useful for identity – identifying as disabled is not something that should be labelled as negative.
The impact of medical gaslighting can not be underestimated. The very real risk of psychologising Long Covid is that CYP end up masking symptoms of anxiety, depression, self harm and suicidal ideation. Psychologists need to support around re-building trust with healthcare professionals, to ensure that the disbelief young people have experienced in their formative years does not continue into health inequalities in future.
Occupational Therapists are among the professionals well-placed to consider people holistically. Whilst we inevitably wait for large scale biomedical research, drug and treatment trials, we should not underestimate the positive impact that addressing the person's social environment can have. Evidence from ME/CFS demonstrates that where CYP are appropriately supported to rest and pace during their early illness they do have a significant likelihood of recovery (for multiple reasons this is sadly less likely for adults). Education for parents, caregivers, and those working in schools and colleges, can better facilitate a supportive environment where CYP are not pushed beyond their energy limitation, but facilitated to succeed within it.
Psychologists and Occupational Therapists can be advocates for the CYP voice to be heard. Together we should campaign for clean air, particularly within educational establishments, because the risk of Long Covid rises with repeated Covid-19 infections.
#long covid#covid 19#covid#mask up#pandemic#public health#wear a respirator#still coviding#wear a mask#sars cov 2#coronavirus#covid conscious#covid is airborne
18 notes
·
View notes
Text
Not every violent, manipulative, and/or abusive character is a narcissist or a psychopath folks 🙄
#narcissist in particular has a specific list of criteria#it's not just douche who's full of themselves#there are more personality disorders out there you know#sorry i just saw a redditor come to the realization that armand is a narcissist#which like. i really don't think so? he lacks several of the defining traits#(grandiosity/excessive need for admiration/fantasies of power fame or weath/etc)#lestat fits narcissism much better and we can see the stark contrasts between the two characters#though even for lestat he could just as easily have hpd#i know narcissist is the trendy label to slap on everybody (real or fictional) who's toxic these days#but it does mean a specific thing and you should probably at least double check it actually fits what you're describing first
4 notes
·
View notes
Text

green beetle black beetle
#star wars#the original trilogy#boba fett#darth vader#hi. sorry for star war jumpscare. genuinely#i feel like ive kinda been on an art hiatus lately due to health stuff#i got diagnosed with a parathyroid disease recently (wahoo) so now i know why i have been feeling so bad! need more tests though#anyway. in the mean time most of the entertainment my brain can handle has been like. youtube clip compilations of shows and movies#not even the actual shows or movies. literally just sections of them on youtube#i wish i was joking#the only reason i know what happens in succession is because i have watched it in disjointed order in youtube compilations. not joking#anyway so ive learned a lot more about star wars than i ever. thought i would#mostly just the original trilogy and prequels. some of the old comics & books are interesting too#(sick to my stomach) i like darth vader he has like the same personality as ganondorf except he had no good reason for doing anything#when vader/anakin does literally anything weird or unacceptable it like. makes me laugh so hard its like jerma when he sees a car accident#boba fett’s costume design has been rotating in my head a lot too it’s very good#he’s very colorful and like. matte/unpolished compared to vader and it makes them a cool duo visually#those 2 are my favorites. vader why is the space cowboy the only person aside from sidious or tarkin who is allowed to get mad at you#sidious is my 3rd favorite. he sucks so bad as like a person that you just. you have no expectations of him except just being evil#so its just really funny like everything he does is horrible and he’s so happy all the time like good for him#i’m making it sound like ive never seen star wars before. i have i just never really cared about it until i got an endocrine disorder lmao#but yeah idk art may continue to be slow while im figuring out treatment stuff#if anyone reading this also has or has had hyperparathyroidism im wishing the strength & radiance of 1000 beautiful horses upon you
81 notes
·
View notes
Text
Okay I actually really hate this take I’m sorry. Anakin was not possessive or selfish and that’s not what the Jedi taught him.
The way I think of it is that Jedi pursue inner peace by disconnecting themselves emotionally from situations, they feel empathy in a very detached way. That’s what having no attachments means. It’s in the word. The Jedi are Detached from reality as it is perceived by humans.
The Force gives Jedi a glimpse of what it is to be a 4th dimensional entity with consciousness no trapped in a single moment in time. So to a certain extent they don’t actually perceive time linearly and thus do not feel they’ve lost something because it still exists in the past.
So now that we’ve established that yes Jedi are detached from the present let’s move onto the more problematic statement about selfishness and possessiveness.
It is not selfish to want unconditional love. That’s basic human nature. Anakin, a person who clearly suffers from borderline personality disorder which comes with symptoms such as fear of abandonment, an unstable view of the self, devaluing or overvaluing relationships to the point placing of one’s self-worth entirely in another person’s hands, and more, literally needs unconditional love and support. And he developed this disorder in large part because of the Jedi order and the way they treated him. He was simultaneously considered the “chosen one” and considered a burden or a problem. He had to change everything about the way he thought to fit the prescribed mold of what a Jedi should be, and he was held to higher standards because of his perceived “chosen one” status and people were disappointed when he failed to meet them. I know from experience how truly awful it is to be told “i know you can do better” in a disappointed voice when you’re honestly trying your best.
And that’s not even touching on how in Phantom Menace he created strong bonds with both Qui-Gon and Padmé only to have both of the ripped away right after he’d left behind everything he knew and loved. After the movie he was around nothing familiar or comfortable. He didn’t know Obi-Wan and he knew that Obi-Wan hadn’t actually wanted him as an apprentice or even in the Jedi order. So he was surrounded by a bunch of people who all thought he didn’t belong and only let him stay because of a dead man’s wishes. He was NINE and being told that everything he ever learned was wrong and backwards and leads to being evil and that he needs to be perfect for anyone else to think he belonged because even the smallest mistake would just confirm their preconceived beliefs about him.
And that’s not even mention Sidious’s manipulation. Anakin never would have become anything like Vader without Sidious leading him.
Also! There is a difference between possessive and protective! Anakin is protective! He has lost so much he’s clinging desperately to what he has! He wants to protect the one good thing in his life. He doesn’t try to control Padmé, they actually have a very healthy relationship, it’s the situation that’s toxic. Anakin doesn’t view Padmé as a possession, I don’t know why anyone would think that. Oh wait the Clovis arcs. Right. Those exist and other people actually consider them canon. That’s a whole ‘nother rant about writing that I’m not going to get into here. But let’s make this one thing clear, Clone Wars Anakin and movie Anakin are 2 totally different characters psychologically because of the awful reception of the prequel trilogy when it came out.
"no attachments" in SW literally just means "don't be selfish and possessive". that's it. that's all there is. doesn't mean jedi can't have friends and loved ones. they can. just. don't be possessive and selfish about it. don't murder thousands of people in an effort to save one.
#star wars#jedi order#jedi#anakin skywalker#mental illness in fiction#the jedi code is bullshit#bpd#anakin has bpd he needs unconditional love#that is not selfish!!#and there’s a difference between possessive and protective!
6K notes
·
View notes
Text
PwNPD, I'm making a video on why I would argue that the use of the word "narc" in the context of a narcotics officer/someone who would snitch to the cops does not negate the derogatory meaning. However, I wanted to hear what the rest of you had to say on it since I think feedback will help me create a more satisfactory script.
Unless you are someone from the opposition who has a different point than 1. just stating the definition of the word as if I don't understand it or 2. mocking people because "then wouldn't it be pronounced narse?" ...Yeah, I've already heard those 'arguments'. I'm primarily looking for feedback from pwNPD that are of the same opinion as me, but may have different argumentation I didn't think of. Anonymous asks are allowed on my blog, so if you don't want your name attached then I am happy to receive feedback that way.
I DO plan on integrating anything helpful into my video, so I may end up messaging people if there's anything that stands out and may need further discussion privately. I will be sure to give proper credits where it's due.
Other than that, either way you fall in the discourse, feel free to answer the following poll. "Narcissist" includes anyone who identifies as one, whether you have NPD traits, self dx or are clinically diagnosed. I may make a follow-up poll later if I end up feeling there wasn't a good enough variety of options.
#XANDER TXT#🌼 NPD#ACTUALLY NARCISSISTIC#NARCISSISTIC PERSONALITY DISORDER#NPD#NPD TRAITS#NPD ADJACENT#NPD SAFE#(LET ME KNOW IF YOU WANT TO BE NOTIFIED WHEN THE FINAL VIDEO COMES OUT)#(IT WILL BE AN UNLISTED VIDEO SINCE ITS SPECIFIC TO TUMBLR AND NOT A BROADER YOUTUBE AUDIENCE)#(PLEASE AND THANK YOU)#(OH AND OBVIOUSLY REBLOG IF YOU WANT TO SO THIS REACHES MORE PEOPLE)
34 notes
·
View notes
Text
The craziest thing is that I know exactly what’s wrong with Armand and could write a thesis on it but I have NO idea what’s wrong with Louis he’s a psychological mystery to me
#like what Daniel said psychologists will be clamoring to figure out what’s wrong with him#it’s also worse because he’s such an unreliable narrator we hardly know what the truth is#the differences between Louis and lestat’s physical fight?? you start thinking Lestat was just pounding the hell out of him#but then we see the fight again in s2 and Louis is about to kill lestat#AND YET WE CANT BELIEVE EITHER AS THE TRUTH#we only know that Lestat did drop him and that they fought but we can’t trust either version#Louis also suffers from a perpetual victim complex#but it makes a lot more sense in the show since he’s a black queer man living in the early 20th century#so we can start to really understand how he got to this point#but book louis was a perpetual victim and ANNOYING#I cannot wait for s3 when we are out of louis hea#not that Lestat is better… but he’s a bit more truthful??? that’s insane to say#I mean he lies a lot but he doesn’t self delude as much 💀 different personality disorder ig#but also ghost Claudia!!!#it’s the way no one in this show tells the truth ever 💀#iwtv#louis de pointe du lac
37 notes
·
View notes
Text
Organizing & contamination OCD Will Solace 🤝🏼 OCPD Annabeth Chase friendship forever in my head.
#🌞#See. The point is that I think Will has severe issues with anxiety-tied organization & possibly contamination OCD (as a stretch of being#a doctor) so his behaviors mostly include anxious overthinking of organization and attempts to quench the OCD need#with rituals and compulsions. But at its core it is an anxiety disorder and I do think it's pretty much canon that Will is an anxious guy#who has his shit together because he has healthy coping mechanisms (in his idea of healthy).#Meanwhile Annabeth seems to have a strong trauma surrounding the need to fend for herself and take care about herself since she comes#from a way more unstable and hectic household than Will does. Childhood neglect and parental issues with 'Beth could easily result in#anger-tied personality disorder such as OCPD. Where the need for perfectionism and 'JUST LET ME DO IT' come not out of irrational#anxiety but rather out of a existing traumagenic personality disorder that convinced you that YOU are the only person who can do#something right.#Ultimately Will is OKAY with others taking care of things but he gets anxious when he handles things bc he overthinks.#'Beth does not overthink but she cannot handle having others take care of things bc she fended for herself her whole life & is traumatized.#But yeah also they're friends.#I am definitely not projecting bc I have organization&contamination OCD and i know how it feels.#rrverse#pjo#will solace#annabeth chase
25 notes
·
View notes
Text
violently forcing myself to have better days
#everyone’s different and this isn’t true for everybody of course:#but a lot of the time we have more control over things than we can see in a difficult moment#like for example#a negative thought is inevitable and not something you can just stop. however you CAN decide from there how you let it effect you#it’s way easier said than done but you genuinely can be like hey I’m going to have a good day today#I like to set my intentions for the day and not allow my trauma nightmares to dictate how my whole day goes#but in order to do that I have to consciously decide that I deserve better and then create that for myself#does this make sense?#do things you know you enjoy/ things that make you feel better. take care of yourself. create little healthy routines to do each day#even if it’s just for 5 or 10 minutes#you have to act to make a genuine positive change in your life and circumstances#tried to say this as well as I could but I struggle w articulating exactly what I mean#like my thoughts are too complex to translate into words#anyways though I just wanted to add this- this post is not to make anybody feel bad whatsoever.#if you struggle with certain disorders and such it genuinely might be close to impossible for you to actually be able to have that control#and that’s okay. it doesn’t make you any less of a person and it is not your fault that you experience those difficulties#I just wanted to remind people that it is possible to control certain aspects of your life and it is possible to snap yourself out of it#I know I need to remember this as often as I can#that’s why I shared it#I hope this makes sense I do not know if it does lmao#(the tags)#my thoughts are so jumbled up. idk what other word to use lmao
38 notes
·
View notes
Text
who up seeing their disorder in a fictional character but feel like its not their place to put a name on it
#id have to be waterboarded before i can talk abt how i see a lot of my adhd and personality in mitsumi iwakura let alone post it#idk how to talk abt this without feeling like im talking over or invalidating ppls experiences relating with a character#someone was talking abt how ppl tie laios' autism to special interest and social difficulties but not much else which kinda flattens it#and then went into a respectful in depth analysis of other autistic behaviour that laios exhibits and it wasnt phrased meanly#its fascinating and important to me to hear someone explain a little bit abt traits that they recognized and often go overlooked#because it does help me learn more about it. but i think thats also where hesitancy kicks in when it comes to depicting it accurately#like i have adhd and some of my adhd symptoms overlap with autism (time blindness and pattern seeking behaviour) but that only means#it feels familiar to me even without having autism. on top of that traits arent always cleanly determined as being /caused/ by#a disorder. to understand my environment i compare it to something unrelated but similar to make it more familiar and for the longest time#i thought that was a personality thing and not an information processing thing since i loved playing pretend in my head as a kid#so if you make a character who experiences that hoping to reach people that also experience that and tell them its not weird or#smth youre making up like. thats the goal. ppl who dont get it arent expected to it just means it doesnt cater to them but it helps them#become familiar to it yk? since i dont have autism myself i dont feel confident i can depict it properly or explain it in my own words#but that doesnt mean im trying to dismiss it or try and cut it out completely.. ill just leave the floor open to someone who /can/#a lot of issues around fanon depictions are when smth is baselessly popularized or a characters personality and behavior is flattened#especially to fit them into a trending meme. its harmless and its supposed to be for fun but it gets tricky when you drag things that#need to be carefully explained beforehand or else it gets lost in translation. like that tweet abt 'hyperfixating' on cooking pasta#once it becomes popular language usually the original meaning is left out for the sake of simplifying it for everyone that when it#circles back theres a sort of hesitancy like. am i using it the way it was intended or am i unknowingly using the popularized version of it#actually thats probably why i felt wrongfooted during diagnosis bc it felt like i was misusing the words i heard to describe what i felt#i /know/ i see a lot of myself in mitsumi because our minds are always somewhere else and we tend to put good faith first and for me#that personal connection is enough. but idk it feels like its always gonna have to be 'palatable' first before i can talk abt it openly#mad respect to writers and creators who stick to their story even if theres the looming fear of ppl misinterpreting it and letting them#have it.. its been almost 2 weeks and i am so close to deleting that m3 dunmeshi drawing bc ppl keep saying chilchuck wouldnt have 200 HP#IT LITERALLY SAYS I MADE IT WHILE WATCHING EP 1. I USED EARTHBOUND LOGIC AND I WASNT EVEN TAKING IT SERIOUSLY CHILL#yapping
20 notes
·
View notes
Text
For everyone who wants to have a more layered, not so nice portrait of Sisi I can recommend Karen Duve's historical fiction "Sisi". The book is a vignette of Sisi's Europe travels in her fourties until her marriage planning for her niece Marie Wallersee.
I generally like Duve's historical fiction at she's not shy to unapologetically depict unlikeable traits in women. Especially with Sisi she's incredible skilled at recreating her complicated character. Her graciousness towards her sister, her flightly attention, her egoecntrism, the strong contrast between Franz who wakes up at in the middle of the night and does try to execute his govenrmental function to a T, in contrast to Sisi who commits one political faux-pas after another as a consequence of her having realized how she's a poltiical body not a person in her function. Yet she's reckless, tornments Lady Festetics, doesn't take life seriously in spite of the political power she holds. She projects onto the innocence of nature and despises people yet is offended when she isn't treated like the royalty she bears. The Hungarian cause was important to her once however, after the failed succession she dissasociated and only engages with Hungarian nobility for romatic and lipservice to herself. She makes a virtue out of her heavily disordered eating, is fatphobic- A cold mother yet blames her children for not loving her. Over all, there're many fecetts of her character captured, weaved together in a colourful tapestry. If you like the character is up to each reader - what does matter is the author capable of recreating a woman with a very difficult character, her qualities, her failings which make sense in a single person.
I don't know how good any translation is however, the original writing is delightfully sarcastic. Sisi herself is certainly not nice or aspirational however it has some enjoybale snide remarks on the poltiics of the time, or the meanest but most deserved burn against Emperor Franz. ("Nobody marries a 15 year old out of the desire to entertain a intellectually stimulating conversation with their spouse.")
It came out in a funny time in which two Sisi movies came out which were weirdly projecting on feminist themes onto Sisi's persona. Sure but Sisi herself was her most important cause, it is more a public facination with her persona, and her prominence in central European popculture that make a movie of feminist issues projected on a popular figure marketable. Whereas I don't think that movies are as deep or realistic as they like to think I think "Corsage", and "Sisi und ich" (with the one and only Sandra Hüller) strongly work with Sis as more tornmented, difficult character, opposing the once so prevalent demure idea as portrayed in the Romy-Schneider-trilogy.
I honestly think that the problem with quite a bit of Sisi media is a larger problem with historical fiction.
It's that fiction really struggles to know how to portray women who are shy and sensitive and have a rich internal life. It's the "well behaved women rarely make history" interpreted as a certain kind of plucky, outgoing personality in fiction that makes it difficult to know what to do with someone who spent a lot of time within themselves. Elisabeth was, by all accounts, someone who was literary, poetic, and had an extensive internal life that not many people were privy to. She's not an ideal female protagonist, at least not by most norms of fiction.
She's not a "well-behaved" woman. But it often comes in the form of internal retreat and strategic assertions of her own beliefs. It doesn't track as well with how fiction tends to think of historical women.
To a degree, it works better in mediums that can be a bit less literal. The Elisabeth musical does it by externalizing the concept of death and playing out her internal conflict. But on the other hand, recent art films (about figures like Marilyn Monroe or Diane) have been such a mixed bag when it comes to portraying the internal life of a famous woman and not fixating on the tragic elements.
34 notes
·
View notes
Text
has anyone ever written a no capes DC AU where Jason's pit rages are switched into OCD/intrusive thoughts?? because that's a concept i literally can't get out of my mind. i tried to write a pit rage once and i noticed the way i'm describing it is a literal projection of my intrusive thoughts back when my ocd was that awful. so i thought i might try to write something like an OCD!Jason fic but if anyone's read something like that before please let me know!!
#as a side note i saw a lot of discourse about the nature of a lazarus rage and more specific ally the way it is handled in fics#and a lot of people were saying it's wrong to imply the rage can make someone do things they don't actually want to do#because that would erase jason's whole philosophy when he wanted to kill criminals#and would instead make it a case of 'crazy person doing bad things because he can't control himself'#and i agree with that sentiment 1000%#like obviously i cant tell you how tro write your fics lol#but i feel like the reasoning and philosophy behind his actions is a part of Jason that can't and shouldn't be erased#so an ocd au would WORK with this character#because like i know a lot of people don't know this but intrusive thoughts have absolutely nothing to do with your real feelings#i mean when you have ocd & you keep thinking about killing someone it's not because you're a dangerous murderer who really wants to kill pp#and maybe i just really want to write a blorbo going through the same shit i did and coming out alive and still loved by his family— SUE ME#jason todd#red hood#DC#DC Comics#lazarus pit#lazarus rage#headcanons#mental issues#obsessive compulsive disorder#ocd#ocd headcanon#fanfiction#writing#ocd!jason todd
9 notes
·
View notes
Text
I uh. Finished the first chapter draft for Ouroboros. Little sneak peaks below the cut I suppose.
“Deep down, you know that something has changed. You can’t quite put your finger on it yet.
-
That’s what it is. You’re alive.
-
Death does not always mean an end. It is simply a pit stop on a very long highway. You still have many miles to travel.
It is best if you get back in your car and begin to drive again.
-
How long can you take it? The way you have a mouth but no voice to speak through.
Can you take it?
-
You realize you are being rebuilt. It is uncomfortable and itchy knowledge. You feel it in the prickling numbness at the tips of your fingers, the eternal ache in your temples, and most of all, you fear.
Your aches and pains are all fear.
You are no longer human.”
#the ouroboros cycle#oh god. here we go#I like this sequence a lot for a few reasons#it’s just ambiguous enough that there’s some wiggle room for interpretation#lines can be twisted in one way by one person or another by a different one#I like when writing does that quite a bit#definitely gonna be editing this but here’s something out of the rough draft as a treat#since a lot of the plot is set out already in my other post I’m just gonna have to figure out how I want to shape the narrative effectively#kepler is a very layered character to me and he’s even more compelling because we still don’t know anything important about his past#which leaves the community to whip up whatever interpretation makes sense to us on a personal level#we’re given so much to work with for Kepler yet so little at once#we know his surface level traits and flaws already but we don’t know HOW he got to that point#ugh warren kepler#throwing bricks at him#probably should’ve asked this earlier in the tags but would you folk prefer fic updates on here or ao3#or both#oh and before I forget#a lot of the story revolves around some pretty deep mental health struggles for a while#such as a disorder similar to dehumanization (not fully classifying it as such because there are some nuances that stray away from ->#some of the typical aspects of dehumanization disorder)#that’s one of the big ones but there will be others#which I’ll make note of before any content that contains anything of the sort (along with other tags that are featured)#I think that’s all for now#wolf 359#w359#warren kepler#daniel jacobi#isabel lovelace#renee minkowski#kepcobi
10 notes
·
View notes
Text
girl who sucks at making OCs needs to make a DnD character send help
#I did make one who was rad but then got vetod by the DM and now I handed in a half-elf wizard but she's just so basic#she literally has no personality send help#and also idk what direction should we take because I have no idea what the other people will be like in the party#and I'm the only girl player there so I don't want for that to be like be a thing and bring a stereotipically girly character#and I could make her like a standard bookish wizard which obviously stands very close to me and would be super easy to play#but that's so cliche and I don't want to be like everyone's mom in game if everyone else is just running around and fucking shit up#but I know that I'll have a harder time playing a more reckless and careless character and if there isn't going to be someone#thinking for the team and we just go headfirst into stuff that also sucks.#and like I like to be someone who thinks about the solutions it just can't just be me being the party pooper if you get me#but poor wizard girl is just so mid with her 'my parents wanted me to be an X wizard but I'm gonna be an Y wizard instead' backstory#like wow such rebellion you're gonna show them girl#but at this point I'm a week behind schedule so I need to have a character like for yesterday#and I don't want to just copy others' dnd characters from D20 but they have like a group cohesion and individual arcs and that's so cool#and I suck at making up little men#miaing#mia's dnd adventures#I'm stressing so much over just making a character and meeting strangers bringing a character with anxiety disorder wouldn't even be rp#I guess great that my sorcerer got vetoed how would I play out being the face of the party
18 notes
·
View notes