#hiv viral load
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s reach among the 26-to-35-year-olds in the US is 11%.
Text
youtube
Call : +917997101303 | Whatsapp : https://wa.me/917997101505 | Website : https://fidicus.com
మీరు ఇష్టపడ్డ వాళ్ళకి HIV ఉందని తెలిస్తే? What to do if your Loved one Has HIV AIDS ? Treatment Cure
In this video, we discuss important steps to take if your loved one is diagnosed with HIV. Learn how to offer emotional support, encourage medical care, and understand treatment options like antiretroviral therapy (ART). We'll also cover ways to reduce stigma, promote a healthy lifestyle, and emphasize the importance of regular check-ups. Together, we can ensure that your loved one lives a long, healthy, and fulfilling life with the right care and support.
Dr. Bharadwaz | HIV AIDS | Health & Fitness | Homeopathy, Medicine & Surgery | Clinical Research
#HIVSupport #LivingWithHIV #HIVAwareness #HIVCare #SupportAndHope
#DrBharadwaz #Helseform #Fidicus #Clingenious
#ClingeniousHealth #HelseformFitness #FidicusHomeopathy #ClingeniousResearch
#FidicusHIV #HIV #AIDS #HumanImmunodeficiencyViruses #AcquiredImmuneDeficiencySyndrome
#Treatment #Cure #Prevent #Relieve #Medicine #Vaccine
#AlternativeTherapy #AdjuvantTherapy #AlternativeMedicine #AlternativeSystem
Specialty Clinic Fidicus HIV highest success with homeopathy Improve Wellness | Increase Longevity | Addresses Questions
#infectious diseases#viral load#hiv#undetectable#hiv viral load#hiv undetectable#undetectable viral load#hiv positive and undetectable#undetectable equals untransmittable#hiv positive#hiv prevention#how to stop the spread of hiv#what is a viral load#aging with hiv#human immunodeficiency virus#living with hiv#aids#hiv medication adherence#what does undetectable mean#am i undetectable#hiv comorbidities#untrasmittable = undetectable#treatment#care#Youtube
0 notes
Text
things that do exist and can play a significant role in illness but always make me Very Suspicious when they come up:
the vagus nerve
heavy metal toxicity
mold poisoning
#wanna guess what book they keep coming up in?#mast cells united#also sibo.#and candida.#'viral/bacterial load' outside specific contexts like hiv is rapidly climbing the list through this book too.
4 notes
·
View notes
Text
HIV and COVID
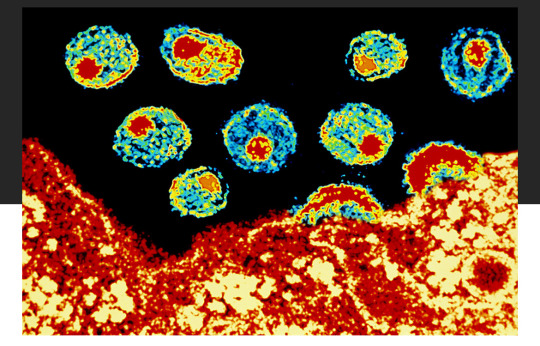
A major barrier to preventing the spread of HIV is accurate test results.
There is a high chance there are many people with HIV that have it and do not know. We do not know how long this undetected time period is (lentiviruses are often associated with long periods of time of virus activity that goes undetected- 5 to 10 years or more), but there is a chance many individuals with HIV go undiagnosed for many years. Individuals during this time before an HIV diagnosis complain of fatigue and many undiagnosed disabling symptoms during that time period. HIV is able to cause changes to immune cells that prevent HIV tests from finding the infection. Some people get negative HIV tests when they are HIV positive. This means you could be HIV negative, but still have HIV in your blood and can spread HIV to other individuals.
Getting a COVID vaccination (and sometimes other vaccinations like the flu vaccination) can help the body identify HIV hiding in the body. This allows earlier treatment and intervention. Once HIV has been identified, it also reduces the risk for all individuals in our population to be exposed to more severe infections.
Getting tested regularly for HIV used to be part of our federal public health recommendations.
This just further emphasizes why this information is so important to know and healthcare needs to start testing for more diseases in more people and do these tests more often.
People often assume their infection came from an unfaithful partner, but in reality HIV has been spreading unknowingly to many in the medical community and still in the public sphere no one is talking about it like the huge deal it is.
This potential means people could be raped as a child, never have sex again, never encounter drugs, and then be miserable & living with an active HIV infection into their early 20s and they would never know. Once they got a positive test result they would have no idea where the infection even came from.
Our entire understanding of these types of diseases has to change and the seriousness of this topic has to be addressed by the world. This was theorized as a mechanism of HIV spread due to how many people were getting diagnosed but had no identifiable cause of their HIV, but now it’s proven and right in front of us. This is disastrous.
To everyone that told the truth about how they didn’t know how they got these types of diseases & how they had no idea where they got it from then faced judgement from others and even the medical community- you aren’t crazy.
On behalf of everything these types of diseases did to destroy families, relationships, and your body, I’m going to apologize right now for all the individuals that I know won’t ever give you an apology for what they did and what they said.
I believe you. I always did.
Without you telling your truth , we never would have been able to figure this out about HIV.
HIV is spreading in “HIV negative” individuals to other individuals as some researchers theorized.
The mRNA vaccination technology developed is now the foundation for the next generation of HIV treatment and disease control. We must continue to push and advocate for improving the lives of all people with disease and we all just took a huge step forward.
You do not have to be sexually active to develop HIV. Your sexual trauma doesn’t have to define your life for the rest of your life- you are stronger than you know and braver than you feel.
Find a place to get tested for HIV here:
I still recommend getting a NAT or “viral load” test done as the first test to see if you have HIV.
I think considering what we know about HIV and in consideration of all the things we still don’t know that this is the safest option. Any other test for this condition available today has too high of a chance of producing a wrong result. I find it extremely uncomfortable we still use the other types of tests in the hospital and doctor office settings.
If you choose to order a test through an online service be aware some tests only tell you about either HIV-1 or HIV-2 and will not always provide you information related to type 1 and type 2.
For example, here:
This will provide you information related to ordering a test that looks for both types of HIV instead of just one strain of HIV.
Stay safe.
#hiv#virus#sick#chronically ill#chronic pain#chronic illness#chronic fatigue#pain#doctor#medicine#viral
687 notes
·
View notes
Note
would you like to tell us about your research on virginity?
but also...wdym STIs aren't as scary as we think??? I was told most of them are incurable? I know you can make aids untrasmittable and that they've even succeded in curing it a couple times but that's about it. I would love to be educated about this
yeah, the basic idea with the virginity project was that the whole concept of virginity is pretty bullshit in the context in which it was initially significant, namely cisgender women being penetrated by cisgender men, so as soon as you take it outside of that context by introducing gay and trans sexuality it totally falls apart. I mean, hell, it stops working if you even look at two cishet people doing literally anything OTHER than penis-in-vagina sex. I tripped up so many people initially when I started asking questions like "okay, so you don't think a woman loses her virginity from a man going down on her. so what if it's two women? what's the difference?" and just really getting people to face down their very penis-centered view of the sex, to the result of several people telling me that it kind of made them reevaluate what they actually think of as the first time they had sex. it's also fascinating to either read other people's accounts or discuss firsthand how queer people have either tried to make themselves fit into the binary of virginity - queer man disagreeing over whether or not you have to have penetrative anal sex to lose your virginity or oral sex is sufficient, a fascinating case of a lesbian who felt that have sex with other cis women didn't "count" and asked a cis male friend to have sex with her just so she could feel satisfied that she'd lost her virginity - or abandon it entirely. Hanne Blank's book Virgin was a formative starting point, and it really exploded for me from there.
as for the STIs - hey, bad news! you fell victim to the scare tactics used to make people afraid of sex! almost all sexually transmitted infections are very easy to treat and cure with the right medicine, which is why it's important to get tested regularly and check in with your healthcare provider at the first sign of something amiss. pubic lice, scabies, trichomoniasis, gonorrhea, chlamydia, syphilis - all of those are pretty easy to get rid of with some help from your doctor and a run to the pharmacy!
the major exceptions are the 4 H's: herpes, HIV, HPV, and hepatitis B.
herpes is with you forever but is an incredibly mild companion to share your body with, considering most people never experience any notable symptoms and those who do can curb the severity with medicine.
it's also worth noting that herpes is so common as to be virtually ubiquitous; the World Health Organization consistently estimates that somewhere around 80% of the world's adult population is carrying herpes simplex virus 1 or herpes simplex virus 2. a great deal of those people don't even get it from having sex, but rather by catching HSV-1 from a parent or other people they come is close contact with as a child.
you're actually thinking of HIV (human immunodeficiency virus) when you mention AIDS becoming untransmittable, but that's still a very good thing! the care available for people with HIV has come incredibly far since AIDS first became known and claimed so many lives, and today it's more than possible for people infected with HIV to live long, healthy lives by taking the proper medication to manage their viral load.
with management, people with HIV will not develop AIDS (which happens when the immune system is sufficiently depleted by HIV) and by consistently taking their medication people with HIV can become undetectable (the viral load in their body is too small to be detected or measured in tests), at which point they are unable to transmit the virus to other people.
HPV (human paillomavirus) comes in many different strains, most of which are absolutely harmless and go away on their own after a couple of months or years of freeloading in your body. I cannot emphasize this enough: HPV is so common that virtually everyone who has sex has, will have, or has had it in their lives, and the vast, VAST majority of those people will never be troubled by it literally at all.
the trouble comes from a few strains of HPV that can cause genital warts, and a few others that can cause cancers in the throat, anus, cervix, vulva, vagina, and penis. while HPV can't be treated, you can reduce your risk of developing cancer by getting the HPV vaccine if you haven't already and, if you have a cervix, getting regular Pap smears to catch early warning signs of cancerous developments.
hepatitis B is a viral infection that targets the liver. in rare cases it can cause chronic health problems that can be very dangerous, but I have to emphasize that's not common. in most adults who get hep B, there will be no symptoms and it will resolve itself in a matter of weeks. the infection is riskiest in children, but at least in America most people have received vaccines against hepatitis B as babies since the 90s.
in conclusion: get your shots, take your medicine, use protection, get tested, and talk to your doctor, but know that if there's one thing humans are good at it's figuring out how to manage STIs. we've been doing it for a long time - most sexually transmitted infections and parasites have been with us since before we we became modern humans - so we're really good at it!
473 notes
·
View notes
Text
Dominique Pelicot, one of the worst sex offenders in modern French history, has been sentenced to 20 years in prison for drugging his then wife, Gisèle, and inviting dozens of men to rape her in her home in the south of��France over almost a decade.
The historic trial of 51 men was held in public after Gisèle Pelicot waived her right to anonymity so that “shame could change sides”.
Alongside Dominique Pelicot, guilty verdicts were returned on Thursday for all the accused men including a nurse, a soldier, a journalist, a prison warden and delivery drivers, aged from 26 to 74. Forty-seven were convicted of rape, two of attempted rape and two of sexual assault.
Pelicot’s co-defendants received jail terms of between three and 15 years. Two of these men had their jail terms suspended.
Some of the sentences handed down by the panel of judges were lower than those that had been suggested by the state prosecutor. “Shame!” shouted one feminist campaigner outside the courthouse in Avignon.
Gisèle Pelicot, a 72-year-old retired logistics manager, looked on with her sons and daughter as the men’s sentences were read out by the head judge. She has been hailed as a feminist hero worldwide for opening the doors to the trial, and members of the public outside the courts have cheered daily for the woman who said she was “determined that things change in this society”, in particular the “macho, patriarchal society that trivialises rape”.
Dominique Pelicot, 72, a retired electrician and former estate agent, was given the maximum sentence of 20 years for drugging and raping his then wife and inviting men to rape her which she was in a comatose state. The court heard that he crushed sleeping tablets and anti-anxiety medication into her mashed potato, coffee or ice-cream and invited dozens of men to rape her over a nine-year period from 2011 in the village of Mazan, Provence, where the couple had retired.
After videos of the rapes by him and other men were found meticulously categorised on his computer hard drive in a file labelled “abuse”, Dominique Pelicot admitted the charges in court, telling judges: “I am a rapist.”
He was also convicted of placing hidden cameras in bathrooms and bedrooms in his own home and that of his family to make and distribute naked images of his adult daughter and the wives of his sons.
Fifty other men were on trial alongside Dominique Pelicot.
Charly Arbo, 30, a former vineyard worker who raped Gisèle Pelicot on six occasions, including on her 66th birthday when he was 24, was sentenced to 13 years in prison. Video evidence showed he also proposed drugging and raping his own mother with Dominique Pelicot, but he said he did not go through with it.
Romain Vandevelde, 63, a former forklift driver who raped Gisèle Pelicot on six occasions over six months between 2019 and 2020, was sentenced to 15 years. He had known he was HIV positive at the time of the alleged rapes and had not worn a condom. His lawyer said that because he had been on HIV treatment since his diagnosis in 2004 he had an undetectable viral load and could not transmit the virus.
Cédric Grassot, a software technician who used to run a record shop in Avignon, was sentenced to 12 years for raping Gisèle Pelicot at her home in 2017. During the trial, he had turned to Gisèle Pelicot in court, and said: “I was your rapist. I was your torturer.”
Jean-Pierre Maréchal, 63, a former lorry driver, was sentenced to 12 years for using the same technique to drug and rape his own wife, and organising for Pelicot to rape her with him.
(archive)
264 notes
·
View notes
Text
Yes, there's hope in the fight against Long Covid.
Hope doesn't come in the form of natural immunity or subpar vaccines rolled out after waves of illness have already peaked. It comes in the form of clean indoor air, widespread masking, and better treatments. In that vein, the NIH is finally launching a new batch of clinical trials focused on Long Covid, five total, dedicated to different aspects of the condition. Institutes like Mount Sinai are running clinical trials on repurposed HIV drugs. So is HealthBio, a startup working on immune diseases. (They're testing maraviroc and atorvastatin.) Post-Viral Trials News is sharing updates as they roll in. Of course, the NIH and FDA need steady pressure to make sure they're funding trials that focus on a range of options. Given the urgency of the crisis, we should be doing far more. As Harvard economist David Cutler has said on developing treatments for Long Covid, "There is no amount that's overdoing it." We're talking about a $16 trillion crisis.
We're talking about an urgent need for dozens of expedited clinical trials for drugs that already exist, which have shown effectiveness in preventing and treating Long Covid in its various incarnations. We're talking about making those drugs accessible right now for off-label use, so that Covid survivors can finally get the help they need.
Long Covid is an emergency.
We're going to talk about prescription treatments first, and then supplements and extracts you can find yourself. Up front, you can try services like RTHM and CURE ID that aim to connect patients with treatments without endless waits. (I'm not endorsing them. I'm just telling you they exist.)
Let's dig in.
Healthcare largely abandoned monoclonal antibodies during the first Omicron wave, but some of them remain effective in higher doses as postviral therapies. We've also found new ones. For example: A study in Nature offers 5B8 as a therapy for fibrinogen, a protein in your body that binds to the Covid spike protein during infection. Afterward, that protein starts to behave differently, "forming pro-inflammatory blood clots" that lead to cardiac and brain dysfunction, especially in young patients with mild infections. It also suppresses your natural killer cells, weakening your immune system. So, damaged fibrinogen is the culprit behind a lot of the "mysterious" health problems we're seeing.
As the authors show, "fibrin-targeting immunotherapy may represent a therapeutic intervention for patients with acute Covid-19 and Long Covid." The monoclonal antibody 5B8 "provides protection...without adverse effects." The sooner you get it, the better it works.
A 2024 study in the American Journal of Emergency Medicine also found that the monoclonal antibody regeneron helped Long Covid survivors recover. Researchers "expressed surprise at the swift and comprehensive improvements observed in the patients," adding that "regardless of the duration of their Long Covid experience, significant progress was noted within a mere 5 days of receiving the Regeneron treatment." It might work because it helps your immune system eliminate residual amounts of virus or viral fragments, or it might replace damaged antibodies that attack your cells.
A 2022 study found that another monoclonal antibody, Sotrovimab, helped survivors with persistent viral loads after initial infection who were still reporting fatigue, chest pain, and trouble breathing months after infection. As the researchers note, the patients showed "rapid improvement of symptoms and inflammation markers as well as negative swabs."
Yet another 2022 study in Clinical Infectious Diseases found that a monoclonal antibody treatment called Leronlimab could help Long Covid patients recover by boosting their immune system in cases where Covid downregulated it, causing a drop in their CCR5 levels, a receptor found on a range of cells that fight pathogens, including your CD4 lymphocytes.
The Long Covid Action Project is also developing a list of drugs that desperately need clinical trials and faster deployment. They stress the need for monoclonal antibodies and antivirals like pemivibart, azvudine, ensitrelvir (Xocova), and sofosbuvir. They'll be releasing a full list later this year.
So while these monoclonal antibodies might not save your life during early infection, they can help your recovery.
There should be more clinical trials and off-label use.
Interferon treatments, specifically Interferon-Lambda, have shown the potential to help with immune system problems and cognitive deficits (caused by brain inflammation) after Covid infections.
Also:
A 2022 study in Frontiers in Immunology found that high doses of immunoglobulin have shown "a significant to remarkable clinical benefit" in treating a full range of brain, heart, and lung problems in Long Covid patients. A major 2023 study in Frontiers in Neuroscience confirmed that immunoglobulin lead to significant improvement in neurological problems. As researchers in a third study on immunoglobulins and Long Covid state, we already use this therapy to treat a variety of chronic inflammatory diseases, as well as flu, HIV, and measles. (The NIH has included immunoglobulins in their new clinical trials.)
HIV drugs have also shown promise for helping Long Covid patients. A 2023 study in Clinical Infectious Diseases found that Tenofovir reduced someone's Covid risk regardless of whether they had HIV. A range of studies have supported the use of Tenofovir, Darunavir Ethanolate, and Azvudine for Covid. As we noted earlier, clinical trials are currently testing HIV drugs for Long Covid.
Another study in Antiviral Research found that cobicistat, used to boost HIV antivirals, also fights Covid and leads to a significant reduction in overall risk. The researchers found that higher doses work better. They also found that higher doses work better for ritonavir, one of the key components of Paxlovid. By the way, ritonavir has been used in HIV treatments since the mid-1990s.
The research on repurposed HIV drugs points to the potential of many antiretroviral therapy (ART) medications for Long Covid, given that viral persistence plays a large role in most cases.
When you consider that Paxlovid itself contains an HIV antiviral, it sounds a little less extreme to compare Covid to HIV and discuss repurposing existing drugs.
Finally, studies have shown that molnupiravir and metformin have shown effectiveness against Covid. In particular, a 2024 study in Clinical Infectious Diseases found that metformin prescribed in the early stages of a Covid infection led to a 41 percent drop in Long Covid risk.
Other research has revealed that sometimes it takes a combination of these drugs to help patients recover. In a 2022 study in Clinical Infectious Diseases, researchers used nanopore technology to identify the specific variants patients were infected with and select the most effective treatments for that variant. In one case, a Long Covid patient with severe Paxlovid rebound only got better after doctors prescribed Paxlovid again and added remdesivir. Nobody had thought to try that yet.
It worked.
These are the drugs that demand renewed attention and clinical trials, given that most research on Long Covid points to ongoing infection, viral persistence, and the disruption of your immune system, which could mean a downregulated or weakened immune system or an overactive one. We especially need clinical trials that match drugs with specific conditions.
Specialists are going to decide the right dose for prescription drugs. Generally, the research indicates that if a standard dose doesn't work, a higher dose might as long as it doesn't trigger side effects. A combination of drugs can work when a single drug fails.
What can you do if you don't have access to these drugs?
This:
A major 2023 study in Cells found that eriodictyol, a flavonoid extracted from yerba santa, can help with the brain inflammation caused by Covid infections that leads to cognitive deficits and fatigue. Researchers have found that at least part of the "brain fog" from Long Covid happens when the virus triggers immune cells to attack the brain. Eriodictyol can also be derived from citrus fruits, tomatoes, and grapes. As the authors explain, a range of flavonoids "have been reported to prevent neuroinflammation, provide neuroprotection, and reduce cognitive dysfunction, especially brain fog."
The authors of the Cell study list flavanoids liposomal luteolin, oleuropein, and sulforaphane as all beneficial for recovering brain function. They identify formulas called BrainGain and FibroProtek containing flavonoids that helped Long Covid patients with severe brain fog in previous studies. Those contain luteolin. They ultimately recommend ViralProtek, which combines several flavonoids, "alone or together" with eriodictyol.
These formulas aren't just managing symptoms. According to the studies, they're helping you clear viral remnants and rehabilitate your immune system. They inhibit your microglia and mast cells, immune cells that often drive the brain inflammation behind Long Covid cognitive problems.
What else?
A 2022 study in Molecules found promise in nattokinase, "a popular traditional Japanese food made from soybeans fermented by Bacillus subtilis var." Not so coincidentally, nattokinase also "decreases the plasma levels of fibrinogen," the same protein that drives thrombosis in Long Covid patients and indeed "has drawn central attention in thrombolytic drug studies," as well as tumor treatment. It also inhibits the replication of bovine herpes virus. Clinical trials have found no adverse effects from eating natto. In this particular study, the researchers found that nattokinase degrades the Covid spike protein, inhibiting infection. As they conclude, "nattokinase and natto extracts have potential effects on the inhibition of SAS-cOv-2 host cell entry."
Martha Eckey describes natto extracts in more detail here, along with benefits, recommended dosage, and possible side effects. Respondents to her survey reported the best results when they took Solaray's natto extract along with serrapeptase, an enzyme and commonly used drug in Japan and Europe that helps your body break down proteins. A large number of patients reported improvement after taking the natto-serra combination, often within a week or two. Many of them also benefited from adding lumbrokinase, an enzyme shown to facilitate healing.
Like natto, lumbrokinase breaks down fibrin. We're seeing a theme here. Any kind of treatment that breaks down fibrin, whether it's a monoclonal antibody or an enzyme, helps after a Covid infection.
Take a look for yourself:

Eckey discusses cromolyn for brain inflammation and neurological issues, and some people have said it helps with other problems. She also wrote this great post about protecting kids from Long Covid.
A lot of it also applies to adults.
Another surprising study in Viruses from 2021 found that grapeseed extract (V. vinifera) contained dozens of flavonoid compounds that inhibited viral replication, including for Covid. The researchers used concentrations from 500 μg/ml down to 10 μg/ml.
Studies have even found that taurine supplements can do a lot to reduce your Covid risks, including Long Covid. A 2024 study in PLoS One found that the amino acid can serve as both a biomarker and a target for treatment in Long Covid. As they write, taurine has already "shown benefits such as reducing depressive behavior, improving memory, and mitigating age-related issues by addressing cellular senescence, chronic inflammation, DNA damage, and mitochondrial dysfunction." It can play "a potential protective role" in "alleviating the burdens of PCC." If that weren't enough, "taurine supplementation has demonstrated diverse therapeutic properties, including anti-oxidation, anti-aging, antiepileptic, cytoprotective, and cardioprotective effects in many diseases." Yes, even taurine from energy drinks. (And I guess it's a good thing I drink them.)
A standard diet contains about 40-400 mg of taurine per day. Medical use often starts at 6 grams a day.
There's a reason why many of these treatments don't get the attention they deserve, and Timothy Ferriss of all people describes it very well in the opening to The 4-Hour Body. As he learns from talking with a wide range of doctors and medical researchers, the industry frowns on any kind of treatment that doesn't look or feel "elite" enough. There's not a lot of incentive for major research on supplements or cheap, widely available drugs because they're just not cool enough, even if they work. For drug makers, it can't just work. It also has to generate enough profit.
That's what happens when you privatize medicine.
As a society, we have to overcome that. This shortcoming isn't going to help us address the myriad public health challenges of the future.
It's a little ironic that the catchphrase "do your own research," once levied against anti-vaxxers, is now used to insult Long Covid survivors and advocates who are trying desperately to find treatments. The difference is that we're not rejecting medicines.
We're simply not getting them.
This article can't replace a doctor or a nutritionist, but it offers a comprehensive starting point for anyone who needs it. You can do more digging and confirm what's here. You could also just make a list of all the things discussed here and take them to someone you trust, and go from there.
It's crucial for us to develop a range of treatments and therapies for Covid that go beyond the mainstream reliance on Paxlovid and vaccines, conveniently dominated by a single pharmaceutical company.
It won't last forever.
In fact, research has shown that Paxlovid leads increasingly to rebound infections in which "the virus can return unimpeded by the drug, bringing the risk of disease and even death."
That's the part left out by corporate media. Rebound doesn't simply mean another round of Paxlovid. It means decreased effectiveness.
It means evasion.
Just like our mediocre vaccines, Covid is developing resistance to Paxlovid. According to an article in Nature, researchers around the world are now quietly racing to develop alternatives. No doubt, viral evolution offers one of the unspoken reasons why many of us find it so hard to access the drug now. The elites are terrified of losing the thing that enables their denial and wishful thinking.
Here's what one researcher said:
“This type of approach helped to improve HIV drugs, and we think it’s a good way to improve antivirals against SARS-CoV-2,” says Sho Iketani, PhD, assistant professor of medical sciences at Columbia University’s Vagelos College of Physicians and Surgeons and Aaron Diamond AIDS Research Center, who co-led the research..."
Western countries are well behind the curve on these fronts. Japan now offers a drug called Xocova (ensitrelvir), arguably more effective than Paxlovid, and it's been sitting in the FDA approval queue for about a year. China approved HIV antivirals for Long Covid back in 2022. While some healthcare workers in Europe and North America know about combining and repurposing drugs, many of them are still busy pretending Covid is over.
It's time for government agencies to pull their heads out of the sand and do their jobs. If there had been more urgency over the last four years, and less favoritism toward one or two drug giants, we would already have these treatments deployed. As things stand, we need leaders to not only run these long overdue clinical trials but also prepare to scale up production considerably, while making sure that everyone has access, not just those with platinum insurance plans. We could already be doing that for emergency off-label use now. Why aren't we?
Although it's infuriating and demoralizing it took us so long to get here, it's encouraging to know that teams of scientists around the world have been working on this crisis and producing results. We just need the gates unlocked.
There's no time to waste.
Let's get moving.
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#still coviding#public health#wear a respirator
95 notes
·
View notes
Text
Things that can go in/pass through the vagina just fine:
penis (and/or semen)
sex toys made of body-safe materials
condoms (male and female)
lube
infants you are actively giving birth to
all that other shit that comes outta there during childbirth
period blood
mucus your body naturally produces so long as it doesn't smell or look weird
tongue
fingers
tampons and menstrual cups
IUD or other insertable birth control methods
ovulation tests
medical devices used during pap smears and pelvic exams or IVF treatments
dilators for those who've had bottom surgery
medications as directed by your doctor(like estrogen cream to prevent vaginal atrophy when on testosterone)
Things that should not go in there!!!
soap, oh my god do not put soap in there holy shit
food
flavored condoms/lube
douching fluids
crystals/special rocks
blood that isn't yours
pregnancy tests(you're supposed to pee on them)
sex toys made out of non-body safe materials unless you put a condom on them
stuff that isn't sterile or hasn't been cleaned properly
no fr like if you are doing anal you NEED to clean your penis/sex toy or at least swap to a new condom before putting it in the vagina holy fucking infections batman
anything you're allergic to(this includes everything on the safe list, if you're allergic to it it's not safe)
the body parts/bodily fluids of someone who has an STI unless you guys have protection(condoms, dental dams, latex gloves, you're taking PrEP/medications to keep your HIV viral load low enough that you can't pass it on, ect.)
Not a comprehensive list ofc but like since it does seem we occasionally need the reminder here ya go. If you're unsure about anything planned parenthood has a lot of sex education material up on their website, def check it out!!
143 notes
·
View notes
Text
"Five people have gone into remission thanks to advancements in medicine — and a sixth patient may also now be free of HIV.
One of the biggest breakthroughs in HIV/AIDS prevention in recent years is the widespread use of PrEP (pre-exposure prophylaxis).
This drug therapy, approved by the Federal Drug Administration in 2012, has been a key player in preventing HIV transmission through sex or injection drug use. Antiretroviral drugs, such as PrEP, also slow the replication of the virus and prevent it from progressing to AIDS.
Although PrEP has become a more accessible treatment for the virus, scientists have been hurriedly working towards cures for HIV for decades — and we’re finally seeing some results.
In February of this year, scientists in Germany confirmed a fifth-ever patient had been cured of HIV after receiving stem cell transplants that include genetic mutations that carry a resistance to HIV.
But it looks like a sixth patient may soon be able to join this very exclusive club.
The man, referred to as the “Geneva patient,” underwent a stem cell transplant after cancer treatment, though these cells did not include the HIV-resistant genetic mutation.
Still, he went off antiretroviral therapy for HIV in November 2021, and his viral load remains undetectable.
Instead, doctors are researching whether a drug called ruxolitinib may be partially responsible for his recovery.
Ruxolitinib decreases inflammation associated with HIV by blocking two proteins, JAK1 and JAK2. This helps kill off “reservoir cells” that lay dormant in the body and have a potential to cause rebounds in patients with HIV.
Experts say the AIDS crisis can end by 2030 across the globe — as long as leaders prioritize this goal.
A new report from UNAIDS shows a clear, optimistic path to ending the AIDS crisis. (This looks like a 90% reduction in cases by 2030.)
The organization’s report includes data and case studies that show that ending AIDS is a political and financial choice — and that governments that have prioritized a path towards progress are seeing extraordinary results.
By following the data, science, and evidence; tackling inequality; and ensuring sufficient and sustainable funding across communities, the global community could wipe out the AIDS pandemic by the end of the decade.
The report demonstrates that progress has been strongest in the countries and regions that have the most financial investments, like eastern and southern Africa, where new HIV infections have been reduced by 57% since 2010.
Investments in treatments, education, and access to care have also led to a 58% reduction in new HIV infections among children from 2010 to 2022 — the lowest number since the 1980’s.
Plus, the number of people on antiretroviral treatment around the globe has risen from 7.7 million in 2010 to 29.8 million in 2022.
The moral of the story? This goal can be achieved, if world leaders put their minds — and wallets — to it.
A region in Australia might be the first place in the world to reach the United Nations targets for ending HIV transmission.
Researchers believe that the central district of Sydney, Australia is close to becoming the first locality in the world to reach the UN’s target for ending transmission of HIV.
Specifically, new infections among gay men have fallen by 88% between 2010 and 2022. In fact, there were only 11 new HIV cases recorded in central Sydney last year, and almost all HIV-positive Australians are on antiretroviral drugs.
... "These numbers show us that virtual elimination of HIV transmissions is possible. Now, we need to look closely at what has worked in Sydney, and adapt it for other cities and regions across Australia.”
Namibia is ahead of schedule in UN targets to end HIV/AIDS.
Although the virus is still the leading cause of death in Namibia, the country is well on track to hit 95-95-95 UNAIDS targets before its 2030 deadline.
In Namibia, 92% of people know their HIV status, 99% of people living with HIV are on treatment, and 94% of people living with HIV who are on treatment are virally suppressed.
In addition to these exciting statistics, new infections have plummeted. The estimated rate of new HIV infections in Namibia is five times lower than it was in 2002, according to the Centers for Disease Control & Prevention.
These encouraging numbers are thanks to the investment and strategic response of PEPFAR, but also to the willingness of local governmental agencies and organizations to adhere to the UN’s Fast-Track approach.
Breakthroughs are being made in HIV vaccine therapies.
Long before we were all asking each other “Pfizer or Moderna?” about our COVID-19 vaccines, scientists have been researching the potential of mRNA vaccines in treating some of the world’s deadliest diseases — like HIV.
And with the success of our mainstream mRNA vaccines, an HIV inoculation remains a goal for researchers across the globe.
Last year, the National Institutes of Health launched a clinical trial of three mRNA vaccines for HIV, and similar studies are being conducted in Rwanda and South Africa, as well.
CAR T-cell clinical trials are underway to potentially cure HIV.
This spring, UC Davis Health researchers have dosed the second participant in their clinical trial, which poses the use of CAR T-cell therapy as a potential cure for HIV.
The study involves taking a participant’s own white blood cells (called T-cells), and modifying them so they can identify and target HIV cells, ultimately controlling the virus without medication.
The first participant in the study was dosed with anti-HIV T-cells last August, and the trial is the first of its kind to utilize this technology to potentially treat HIV.
Of course, the trials have a long way to go, and the lab is still preparing to dose a third participant for the study, but CAR T-cell treatments have been successful for lupus and forms of cancer in the past...
“So far, there have been no adverse events observed that were related to the treatment, and the two participants are doing fine.”
Guidance on how to reduce stigma and discrimination due to HIV/AIDS is reaching people around the globe.
While the stigma surrounding HIV and AIDS has significantly decreased — especially towards the LGBTQ+ community — with advancements in treatment and prevention, discrimination is certainly not gone.
While most people now understand HIV/AIDS better than they did decades ago, those most impacted by the virus (like gay men and low-income women and children) still face ongoing barriers to care and economic security.
It is vital to maintain awareness and education interventions.
After all, experts suggest that eliminating discrimination and stigma are key factors in reducing disease. And not eliminating stigma impedes HIV services, argues UNAIDS, “limiting access to and acceptance of prevention services, engagement in care, and adherence to antiretroviral therapy.”
Luckily, UNAIDS provides guidance on how to reduce stigma and discrimination in the community, workplace, education, health care, justice, and emergency settings.
The goal is to, of course, decrease stigma in order to decrease disease, but also to provide folks with the culturally significant support they need to live safe, integrated lives — with or without disease.
For instance, a 2022 study conducted in Northern Uganda showed that local cultural knowledge passed through Elders was a successful intervention in reducing HIV-related stigma among young people.
“Research in school settings has shown that the use of local cultural stories, songs, myths, riddles, and proverbs increases resilient coping responses among students and strengthens positive and socially accepted morals and values,” the study’s discussion reads.
So, while an uptick in acceptance gives us hope, it also gives us a directive: Keep telling the accurate, full, and human stories behind HIV/AIDS, and we’ll all be better for it. "
-via GoodGoodGood, August 3, 2023
#hiv#hiv/aids#aids crisis#public health#medical research#vaccines#australia#namibia#united nations#queer issues#trans issues#lgbtq issues#lgbtq community#infection prevention#good news#hope
274 notes
·
View notes
Text
Just finished Love In The Big City and I don’t know, it’s a sad story but I don’t feel crushed by it nor wanted a pretty little bow in the form of a “happy ending” for it.
I didn’t read the book so I’m basing on the show only: the ending was fitting. Though they could’ve explored a few things better, some nice ideas that were not fully fleshed out in the final episodes.
Now, the production value here? Whew, it leaves an impression, and so does the acting, role of a lifetime for Yoonsu — threw himself in this role, his Young feels authentic, real, he brings his A game and uses it to the max.
Personally, an important part of the story was jarring for the wrong reasons (to me). Everything surrounding Young’s status as HIV-positive left me shocked by the way they deal with it in South Korea (assuming the show portrays accurately), because from where I’m from it’s not handled that way at all, with patients having access to meds that lower the viral load to undetectable levels and alternative for the partners to prevent infection through sex, all of that for free, I was surprised seeing them dealing with his condition that way. Cultural difference that really made a difference for me here. Young and Gyu ho would hardly have the problems they did in the show with the right medical counseling.
Other than that I thought it was lovely show, albeit melancholic and moody — it’s like the sad gay cousin of Sex and the City. It’s witty, sexy, well acted and barely avoiding depression.
12 notes
·
View notes
Text
in relation to the last reblog, some things about HIV. (it's not really a proper educational post (tm) just some facts and misconceptions that i wanna bring so please do your own research if you're able).
HIV is transmitted through blood and sex.
HIV is NOT transmitted through air, saliva, common dishes, household items, etc.
PrEP = pre-exposure prophylaxis. treatment that you get if you regularly participate in risky activities to prevent getting HIV. if you regularly participate in risky activities (share syringes with someone, have unprotected sex), you may consider using PrEP. YOU NEED TO BE HIV- TO USE PrEP!! usage of PrEP if you've already got HIV is dangerous! HIV may develop resistance to the anti-retroviral drug you intake for PrEP, and it can make treatment more difficult!
PEP = post-exposure prophylaxis. treatment that you get as an emergency if you get at risk suddenly (had unprotected sex with someone whose status you don't know, were sexually assaulted, don't remember whether you used condoms or not, condom slipped/teared, shared syringe with someone, etc). it is an EMERGENCY MEASURE that couldn't be used on a regular basis. if you're exposed at risk on a regular basis, consider using PrEP.
PEP needs to be started NO LATER THAN IN 72 HOURS after exposure. the earlier you start, the higher the effectiveness is.
what does it mean: after exposure, you'll have HOURS to contact with medical provider/center/place where you can get PEP and start treatment. so it's better to research opportunities beforehand. maybe get a supply, if it's legal. but at least you need to find a place where to go in emergency case.
the most risky activities are: usage of same syringe for injections, unprotected sex with contact of genitalia and anal, sexual assault (PEP is recommended). consencual oral sex has very very very low risks (PEP is not recommended). anyways, if you think you have been exposed at risk, you should contact your medical provider or centers that specialize in HIV prophylaxis and treatment. it's better to contact in any doubts.
idk how it works in other countries, but where i live we have (some) HIV/AIDS centers where people can get tested, get PrEP, PEP, and help with access to antiretroviral treatment. places that you can research: HIV/AIDS centers, planned parenthood, reproductive clinics, queer-specialized places, etc.
HIV IS NOT ADDICTS-ONLY DISEASE. HIV IS NOT QUEER-ONLY DISEASE. HIV IS NOT MARGINALIZED PEOPLE-ONLY DISEASE. marginalized groups have their risks because of stigma, ostracization, medical neglect, etc. BUT no one is immune to HIV. A LOT OF, and i mean it, generally privileged people get and transmit HIV because they're sure they will never get it.
there are MORE THAN ONE HIV STRAIN. and you can get more than one HIV strain. so if you're living with HIV and going to have risky activity with someone living with HIV and you've not gotten it one from another, YOU STILL NEED PROTECTION. (if you both don't have undetectable viral load).
UNDETECTABLE = UNTRANSMITTABLE. if someone lives with HIV and has undetectable viral load, they can't transmit HIV to someone else. which means you can have unprotected sex with them (if you all don't have other STDs), they can give birth and don't transmit HIV to the children, etc.
HIV IS NOT THE ONLY STD. there are others, and their transmission differs from HIV transmission. for example, oral sex is risky for gonorrhea. so DON'T NEGLECT CONDOMS!
HIV and STDs are not the worst things in the world. most STDs are either curable or controllable, and you can live fine with them. and anyways, no disease should be stigmatized.
HIV and STDs aren't dirty. thinking that "only dirty shameless people can get HIV/STD" is a) discriminatory; b) factually incorrect - everyone can get STDs; c) prevents people from getting tests and treatment; d) promotes the spread and evolution of STDs.
anti-retroviral therapy may be expensive/inaccessible in lots of places. research the situation where you live and your opportunities in case you'll need HIV-associated treatment (PrEP, PEP, anti-retroviral treatment).
people who know that they have HIV are not the "dangerous" ones. the "dangerous" ones are people who have never gotten tested, who are sure that HIV is not something that they can get, and who ask you to have a sex without a condom.
i'm sorry if i say obvious things here, but i'm not sure about public awareness around HIV and thought that if someone can be surprised that person living with HIV can have children without HIV, then these things should be articulated.
10 notes
·
View notes
Text
Now an international team of researchers has discovered a new genetic variant in people of African ancestries that appears to restrict HIV replication after an infection sets in. Though more research is needed to confirm their findings, the discovery is a huge step forward for HIV research, which has long neglected African populations. "The findings may explain why certain people in these populations have a lower viral load, which slows down the virus from replicating and transmitting," says pathologist and study author Simon Mallal from Murdoch University in Perth, Australia. The discovery, from a combined analysis of nearly 3,900 individuals, could also pave the way to developing new antiviral drugs as previously identified genetic variants have done in the past.
Continue Reading
86 notes
·
View notes
Note
Been living with HIV for nearly a decade. You will feel pretty crappy for a while even when you are undetectable. Once your body sorts everything out you will be right as rain with a few time you feel icky here and there. The better news is that the CDC has stated transmission from sexual fluids is impossible with an undetectable viral load. Steer clear of alcohol within a few hours of taking your pills and if you take anything for heartburn (not tums or anything like. Stuff like nexium or Prevacid) then make sure you take your anti-retrovirals first then and then wait two hours before you take the heartburn stuff. Take your stuff religiously and you and your girlfriend will be perfectly safe.
this ask made me kinda upset when i got it. .. i have known abt everything u said. i was posting at the time abt being stressed abt access to medications. having hiv does affect how ppl want to interact w me sexually even if i am undetectable. the acute infection did change me forever, i am weaker now. im nauseous all the time... "Long term toxicological effects of antiretroviral treatments can sometimes cause secondary morbidities even when the viral count is low." idk.. whatever, hope u survive
also fuck the cdc
13 notes
·
View notes
Text
COVID-19
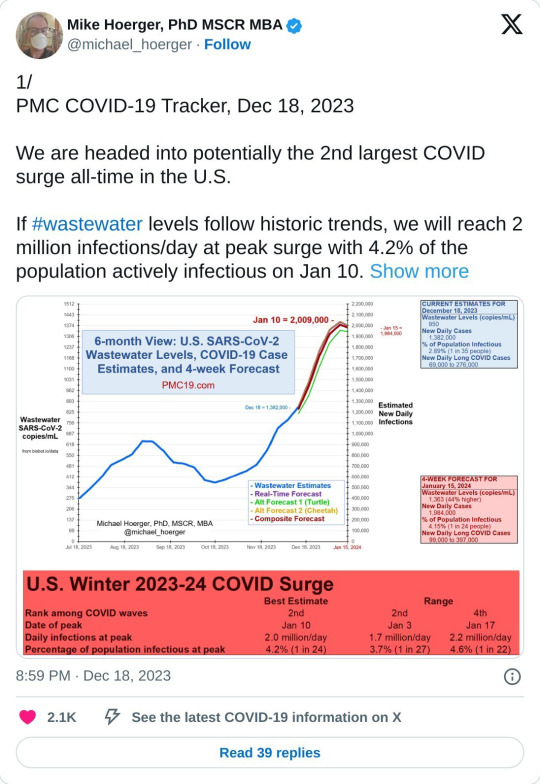
We are currently in the largest COVID surge of all-time in the US.
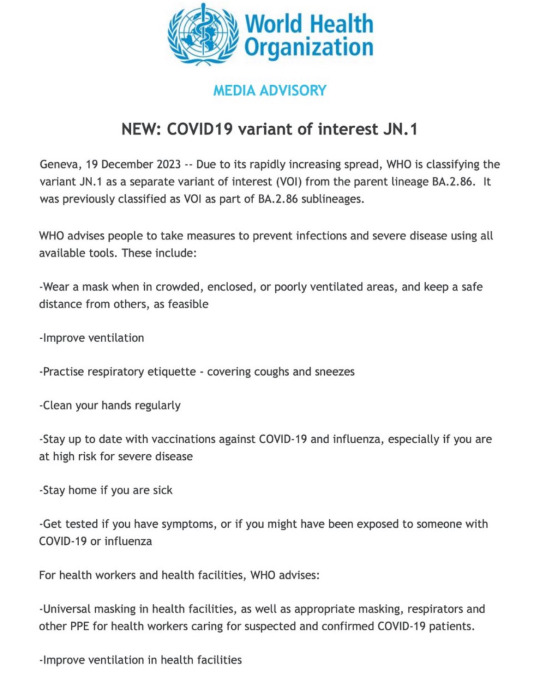
There is also a new variant that is not protected by the previous vaccine.
Please start back masking and please get the COVID-19 booster (schedule with your local pharmacy).
Wastewater counts are obscenely high right now, belying the official case numbers. Considering that we've stopped collecting or reporting most COVID data, wastewater is the best way we have to judge the actual infection rate now. Wastewater is collected from washing our hands, going the bathroom, etc. We shed COVID into the water system and based on the concentration of COVID in waste water, we can get very accurate estimates of how many people are infected at one time.
We are currently seeing ten million new infections a week, and can expect that to greatly increase within the next three weeks.
* If you've stopped masking, please start again, for your own safety and the safety of your community. Many hospital systems are already trending toward being overwhelmed right now; wear a mask when in crowded, enclosed, or poorly ventilated areas, and keep a safe distance from others, as feasible.
* Avoid unnecessary gatherings where possible.
* Ventilate your spaces well (Corsi-Rosenthal Box).
* Reevaluate casual habits (touching face, respiratory etiquette—covering coughs and sneezes, clean your hands regularly, stay home if you are sick, get tested if you have symptoms, or if you might have been exposed to someone with COVID-19 or influenza)
Please be aware of Long Covid.
COVID impacts the immune system similar to HIV in that it hides in the body and continues to wreak havoc in the various organ system by driving inflammation and disrupting the immune response. It causes neurological, vascular, and immune dysfunction.
Patients with long COVID generally have symptoms that fall into three categories or phenotypes: fatigue, neurocognitive symptoms such as brain fog or headaches, and cardiovascular symptoms such as shortness of breath, heart arrythmias, exercise intolerance, and blood clots. Patients may have more than one type, and some also have symptoms like constipation, diarrhea, or loss of taste and smell that don’t seem to fit neatly into one of the three groups.
This is a period where we need to act with more care. Not a time to panic, but a time to be more cautious.
If you contract COVID, these are some helpful things that work to reduce viral load in the hope of minimising symptoms. And your chance of developing Long Covid:
* Brush & floss as usual
* Mouthwash (CPC (cetylpyridinium chloride, an ingredient in many/most commercial mouthwashes), cooled green tea, salt water)
* Green Tea (drink on an empty stomach if possible; can also be used for swishing/gargling once it has cooled; if green tea isn't doable for you, black tea is an alternative)
* Nasal Spray (if chemicals in nasal spray causing an issue for you, saline nasal spray also an option)
* Vitamin C supplement
* Antihistamines
* Other prophylactics to consider: Nattokinase, Grape Seed Extract, EGCG supplements
* Natto (if this is something you already eat, or would like to try. It's fermented soya beans and is popular in Japan
* Mask & Vaccinate!! A fully vaccinated individual is five times less likely to continue to have any symptoms or ill-effects three months after their initial infection compared to someone who has not been vaccinated.
Not a medical professional but compiled resources from medical professionals and individuals with disabilities including long COVID.
Free Palestine. Free Congo. Free Sudan. Free Tigray. Stop Cop City. Eyes on the Mass Graves in Jackson.
Please SHARE & Please participate in the Global Strike for Palestine 1.21-1.28.
#covid#covid19#long covid#covid isn't over#covid 19#coronavirus#corona#free palestine#free gaza#free congo#free sudan#freepalastine🇵🇸#freedom#black liberation#israel is committing genocide#israel is a terrorist state#end occupation#human rights#hawai'i#land back#decolonization#nakba#jason todd x reader#free tigray#stopcopcity#copcity#congo genocide#save congo#mass graves in jackson#jackson mississippi
14 notes
·
View notes
Text
Virtual elimination of HIV isn't enough if it doesn't include everyone
New Post has been published on https://qnews.com.au/virtual-elimination-of-hiv-isnt-enough-if-it-doesnt-include-everyone/
Virtual elimination of HIV isn't enough if it doesn't include everyone
Remember the government’s commitment to eliminating HIV by 2025? The problem with virtual elimination is who it leaves behind.
Virtual elimination of HIV sounds great in the news or a press release, but what is it really saying?
The advancements in medicine and people’s understanding of HIV and those who live with it have been decades in the making.
So why is the stigma surrounding the disease still so high?
All virtual elimination means is that we have reduced new diagnoses to such a degree that it is no longer considered a public health threat.
This is important, but so is addressing the voices and experiences of those who live with HIV.
They are the ones advocating, challenging discrimination and bringing more and more awareness every day.
The science is clear.
An undetectable viral load poses zero risk of HIV transmission.
So why does social stigma seem to trump that medical reality?
Is it because the ‘virtual elimination’ carrot keeps being dangled in front of our noses?
Transmissions have reduced, but has the stigma?
HIV
HIV doesn’t discriminate, and nor should our response
Last year on World AIDS Day, Living Positive Victoria’s Board President Craig Brennan spoke about who virtual elimination leaves behind.
“Virtual elimination refers to reducing new transmissions of HIV to negligible numbers within a specific population.”
“But here’s the issue.
“Selective statistics mask the realities of marginalised communities that continue to experience HIV at disproportionately higher rates.
“We cannot claim victory based on the success of privileged demographics while others remain vulnerable and underserved.
In Australia, we’ve seen incredible strides in HIV prevention, particularly among well-resourced populations and predominantly in white gay men.
“But HIV doesn’t discriminate, and nor should our response.
“Communities that don’t fit this mould include multicultural populations, Indigenous people, and heterosexual men and women.
“Transgender individuals continue to face significant barriers in accessing care and prevention. These populations are sidelined completely in the discussion of virtual elimination.”
World AIDS Day 2024 Photo by Dean Arcuri
Our response must be inclusive.
“The discussions around virtual elimination as a goal often overlook the realities faced by these communities.” Brennan said,
“Structural inequity, lack of access to healthcare, and historic injustices continue to disproportionately impact health outcomes for Indigenous people.
“HIV is intertwined with broader systemic issues like poverty, housing instability, and a lack of culturally safe services.
“Declaring we have virtually eliminated HIV in Paddington while in neighbouring suburbs, Indigenous communities are left grappling with these challenges feels at best disingenuous.”
“The emerging narrative risks erasing the experiences of women.
“Particularly women of colour and transgender women, who often face gender-based violence, economic inequality, and social stigmas that increase their vulnerability to HIV.
“Their stories are frequently lost among our broader success stories, and they continue to remain at risk.
“To genuinely move towards ending HIV, we must be brutally honest with ourselves.
“Virtual elimination isn’t enough if it doesn’t include everybody.
“We must ensure the populations most at risk are not left behind as we declare progress in more privileged demographics.
“Our response must be inclusive.
“Our response must be equitable, and it must reflect the full scope of the epidemic, not just convenient statistics.”
Last year, the Albanese Government invested $43.9 million to help Australia eliminate transmission of HIV by 2030.
This was through a range of measures recommended by the National HIV Taskforce.
But we don’t have to wait till we see a headline saying we can ‘eliminate HIV’ to make things better now.
For people living with HIV, and our community as a whole.
youtube
For the latest LGBTIQA+ Sister Girl and Brother Boy news, entertainment, community stories in Australia, visit qnews.com.au. Check out our latest magazines or find us on Facebook, Twitter, Instagram and YouTube.
2 notes
·
View notes
Text
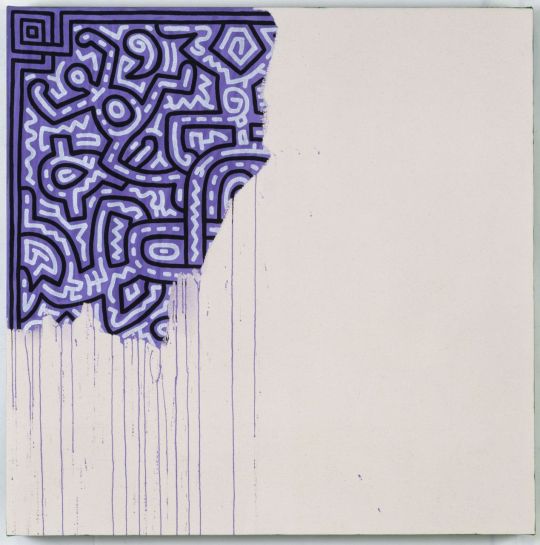
That post where someone used AI to finish Keith Haring's final piece, "unfinished painting," really, really got me like a punch in the gut. Maybe it's because I was a wee thing during the AIDS epidemic and grew up wearing a red ribbon on my coat. Maybe it's because I knew people personally affected by AIDS. Maybe it's because the deaths of people like Keith Haring, Ryan White, Ariel Glaser and Freddie Mercury from AIDS stayed with me. But just - you don't. You. Fucking. Don't.
Keith Haring did not simply leave the painting behind. He wanted it that way.
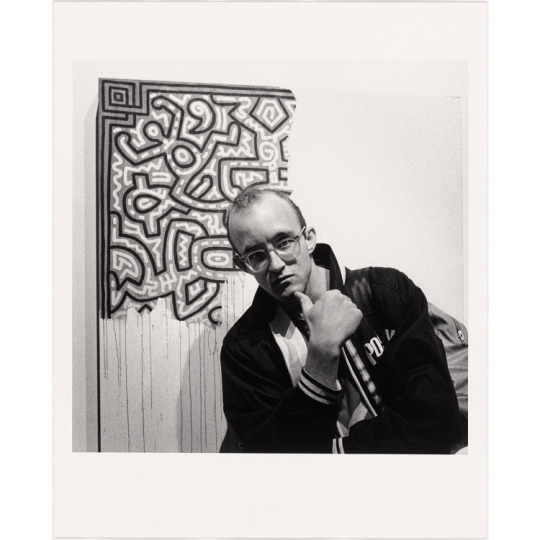
Yeah, the original story behind the piece was "sad." THAT WAS THE FUCKING POINT. It WAS sad that someone who was 31 years old died of a virus the government had made it clear they didn't give a fuck about researching, because oh, it seemed to affect gay men (the original name that a lot of people used was "Gay Related Immune Deficiency" if there's any doubt there) and they didn't care when that demographic died. It WAS sad that kids with HIV were harassed out of school and had to get court orders to attend in some cases, that adults with HIV lost their jobs and became pariahs because they had HIV/ADS, and that when people died of AIDS a lot of undertakers wouldn't even take their bodies. It WAS sad that so many people with AIDS were abandoned by their families and left to die completely alone, without even hospital staff comforting them. It WAS sad that people with AIDS often kept it a secret as long as they could because if anyone knew, it would cause immeasurable harm to them and their families.
HIV/AIDS now has treatments that can reduce viral load to undetectable levels. People with HIV and AIDS can live long lives. That's not everywhere in the world, BTW. But it only got that research and development and was taken seriously because AIDS activists put their blood, sweat and tears into it, and made sure that the legislators could not ignore them. This stuff isn't a secret. It's not ancient history. People who were involved with AIDS activism wrote books, made films and documentaries, sang songs, took photos, and so many of them are out there ready for you to read. People who remember and survived the AIDS epidemic are very much alive, including some who miraculously got through the 80s and 90s with HIV.
Keith Haring's final piece represents the loss of life, the loss of potential, the fact that someone who made glorious images come to life was now stopped in his tracks. It has always looked to me as though the painting is crying. Don't know if that's what he intended, but it's how it came across to me. Not just his tears, the sorrow of the entire situation was there on that canvas.
Any of of his friends could have finished his piece, if that was what he wanted, or what they felt was right. To feed it into AI and finish it is to erase all of the emotion this picture was created with.
So here's how it's supposed to be.
#keith haring#AIDS#HIV#I have not seen a red ribbon on anyone's jacket in a long time. Maybe it's time for me to wear mine again
13 notes
·
View notes
Text
Americans with well-treated HIV can no longer be barred from enlisting in the U.S. military, a federal judge ruled Tuesday, striking down the Pentagon’s last remaining policy limiting the service of those with the virus. “Defendants’ policies prohibiting the accession of asymptomatic HIV-positive individuals with undetectable viral loads into the military are irrational, arbitrary, and capricious. Even worse, they contribute to the ongoing stigma surrounding HIV-positive individuals while actively hampering the military’s own recruitment goals,” wrote Judge Leonie Brinkema of the U.S. District Court for the Eastern District of Virginia. In her ruling, Brinkema mentioned her landmark 2022 decision that ended the Defense Department’s long-standing policy of forbidding service members who were diagnosed with HIV after enlisting from deploying in active duty outside the continental U.S. and being commissioned as officers. “Modern science has transformed the treatment of HIV, and this Court has already ruled that asymptomatic HIV-positive service members with undetectable viral loads who maintain treatment are capable of performing all of their military duties, including worldwide deployment. Now, defendants must allow similarly situated civilians seeking accession into the United States military to demonstrate the same and permit their enlistment, appointment, and induction,” she wrote. Research has shown that people with HIV who have an undetectable viral load thanks to antiretroviral treatment, as is the case for the vast majority of people on HIV treatment, cannot transmit the virus to others through sex. Advances in care and treatment of the virus have extended the lifespan of people with the virus to near normal. People with well-treated HIV are effectively healthy. However, they are still at higher risk of various health conditions related to aging, including heart disease and various cancers.
3 notes
·
View notes