#reading the first part to start and the dsm as a follow up
Explore tagged Tumblr posts
Last Seen Blogs





Text
#heres a good article on mocd. again please speak with a mental health professional if you believe you may have a form of ocd. i recommend#reading the first part to start and the dsm as a follow up#as while the dsm can be overly clinical it still helps narrow down diagnostic criteria#and give you an avenue for conversation with a professional#mick mack
4 notes
·
View notes
Text
How Law Treats Your Depression
Crossposted from my AO3 - https://archiveofourown.org/works/44915341
TW’s: SH (not explicit detail, but talked about, and checking the healing of it), mentions of manipulation, depressive thoughts, symptoms of anxiety and depression.
I wrote this when I was goin through a rough patch. No romance exactly, just fluff. It makes me want to cry every time I read it so I’m sorry in advance if it makes you feel the same way.
The symptoms Law lists are from the DSM 5 and my own experiences.
----
You raised your hand, shaking from anxious hesitation. The door seemed to loom in front of you, being an impenetrable shield to your glimmer of hope for a cure.
“Oh, are you going to see the captain?” said a voice behind you. You nearly jumped out of your skin, spinning around with your fist still raised. You calmed once you laid eyes on Bepo. You exhaled with a small smile.
“Uh… I... I think… well, it can wait” you managed to get out, stumbling over your words. Bepo cocked his head.
“It’s okay, Come in with me. I just have a quick question and then you can talk to him.” His wide body was accidentally corralling you towards the door as he knocked twice.
“Come in” said a voice gravely with exhaustion. Bepo smiled at you and gestured for you to open the door. You gulped but followed his silent request. Will Law even help me? I’m not technically part of his crew. Still, he healed Luffy after Marineford. I’m part of the Strawhats and we’re allied but… your anxious thoughts garbled the mundane question and answer that occurred between Bepo and Law, and before you realized it, the bear was leaving the room with a small pat on your shoulder.
“So?” Law said, cocking an eyebrow at you. Your heart thudded.
“Uh… it… It’s not too big of a deal” you began, trying to scramble for words to voice your request.
“But you’re a doctor, right?” you asked. You cringed at the dumb question. This was why you proposed this whole internship in the first place! Sure, learning about the submarine would help your crew eventually somehow, but… you had to follow through on your real reason for coming here.
“Are you feeling okay?” Law asked. There was a tone of professionalism in his voice now, different than the regular voice he used as a captain.
“Yeah I’m fine!” you replied automatically with a forced smile. His brow furrowed.
“Then why do you need a doctor?” he prodded. You swallowed, looking down. Your heart thudded and your stomach dropped.
“If… If I tell you some hypothetical symptoms, would you be able to give m… uh… the patient, a cure?”
He leaned back in his chair, his hands steepled under his chin.
“Maybe. There may not be a cure exactly, but medicine or surgery could help. Or both” he said, shrugging. You didn’t like the gleam in his eye when he mentioned surgery.
“Oh” you muttered disappointedly. Law sighed and gestured to a seat.
“Sit. Tell me about the patient’s hypothetical symptoms.”
You sat stiffly in the chair, bouncing your leg nervously as you steadied your breath.
“Where should I start?” you asked, glancing at the captain. He hummed in thought.
“Start with the physical symptoms. Aching? Discomfort? Sweating? Redness? Exhaustion?” he rattled off easily. You furrowed your brow, thinking. Back to when your symptoms really acted up.
“Um… exhaustion for sure. They sleep a lot, and minor tasks seem to make them tired. Not like physically exerted, but just like they need a break mentally?”
“Any other physical symptoms?”
“Hmmm… does crying count?”
“From physical pain?”
“No… but sometimes it’s accompanied by a fast heartrate and hyperventilating. Oh, and a decreased appetite” you reported factually, gazing upwards as you thought. Law hummed.
“What about mental symptoms?”
“M-mental?” your heart dropped. This was the part you were worried about.
“Mental distress often leads to those physical symptoms.”
You held back a scoff. Mental distress? It’s not that big of a deal.
“Symptoms like what?” you asked quietly. You refused to look at the doctor.
“Low self esteem past the normal amount, feeling like a weight is holding you down, feeling worthless or guilty for things that aren’t your fault, decreased concentration, and loss of interest in things the patient used to like” he listed. He hesitated before he continued in the same even tone “thoughts of hurting themselves or others, and thoughts of killing themselves.”
You flinched at the last two. This guy really does not pull punches when it comes to medical stuff you thought with an internal shudder.
“It sounds way worse when you say it out loud” you muttered under your breath.
“I have a hunch this patient has a combination of two illnesses- depression and anxiety- which are very common together. Should I list the symptoms of anxiety, and you can tell me if it seems to fit?”
You sighed, but nodded.
“Worrying excessively about things and finding it difficult to control the worry, muscle tension, restlessness, easily mentally fatigued, mind going blank or difficulty concentrating, irritability, sleep disturbance…” he listed, trailing off.
“Basically, worry and stress that goes beyond the norms. So, like not about being embarrassed, or away from people, or during a panic attack. Of course, panic disorders are basically part of anxiety disorders and are just an intense episode of an accumulation of different symptoms, which you mentioned with the fast heartrate and hyperventilating. There’s also probably some other symptoms yo- uh- the patient doesn’t notice during the time, or doesn’t know it’s a symptom”
You tried to absorb the onslaught of information thrown your way. You rubbed your temples. Law seemed to notice your struggle.
“I know it’s a lot of information all at once” he said sympathetically. You sighed. There was only one question you had. You looked into the captain’s grey eyes.
“Is there a cure?”
The captain hesitated, but leaned forward in his chair, resting his elbows on his desk and met your gaze resolutely.
“No”
Your heart dropped, and your lungs constricted. Your throat burned as you fought back tears.
“There’s no cure, but there’s medicine that can help.”
“Right” you muttered as you stood. You had your answer. You needed to leave.
“Wait.”
You paused, hand on the door. You didn’t look back.
“What’s been done to treat it before? It’ll help me narrow down a more effective medicine.”
You huffed, hiding your distraught behind a veil of humor.
“Nothing. Been rawdoggin this bitch the way God intended” you said, keeping your voice light. You heard a snort behind you.
“I’ll give you what I use then. We’ll start with that.”
You froze. I’m not alone? He has it too? You turned slowly in shock. He met your gaze.
“If it doesn’t seem to work, call me, and we’ll try something different. Eventually if we exhaust all the medicine, there is a more radical solution. It’s for treatment resistant forms of depression.” You took a few steps toward him.
“Why do you call it an illness? Aren’t I just weak?”
A small, soft smile escaped Law’s lips as he looked at you in a rare moment of gentleness.
“No. You’re not weak. It has to do with chemicals in your brain. Doctors aren’t exactly sure what triggers it, and it’s usually triggered by different things in different people. But it’s a chemical imbalance that occurs, and the medicine is to help correct that balance. Of course, talking to people is also incredibly important. Have you talked to anyone in your crew about it?”
You shook your head absently, mystified that there was a real reason you felt this way.
“No. They don’t know. They might suspect, but I’ve never said anything. I couldn’t bring myself to tell sweet, innocent Chopper that I wanted to hurt myself on purpose” you said easily.
“Have you?”
You flinched at the question, wrapping your arms around your middle.
“Does it matter?”
“Yes”
You glared at him.
“A little” you finally muttered.
“How?”
“Does that matter?” you said defensively.
“As your doctor, yes” he said gently. You bit the inside of your lower lip to stop yourself from spouting venom. He’s not attacking you or demanding to know for selfish reasons. He needs to know. You took a deep breath and slunk over to your previous seat to collapse in it. You held your head in your hands.
“I try not to, you know. I resist for as long as possible until I finally can’t find any logic against not doing it” you say eventually.
“How do you do it?” he repeats, softly. You sigh, looking to the side. You tell him. The words just flow out, accompanying the tear tracks down your cheeks in a delicate dance of pain and regret. When you’re done explaining, he stands slowly, approaching you slowly.
“I’m going to check the healing of it. That’s all. I just want to be sure it’s healing properly so you don’t have further issues when you’re better” he said softly, holding out a hand. I wish it didn’t heal you thought before pushing the negativity away.
“You sound so sure I’m going to get better” you said as his hands delicately grazed over the area.
“You will. Maybe not cured, but better.” You hummed, welcoming the companionable silence. A thought occurred to you, and you snorted. Law stepped back and raised a brow.
“Something funny?”
“Isn’t it ironic that the so-called ‘Surgeon of Death’ is helping me with… this?” you said, waving your hand in the air as if to gesture to your mental state. He rolled his eyes.
“Yes, yes. Very funny” he said flatly.
“Well at least I’m that” you teased.
“You’re so much more than that. If you can’t see it, trust those around you to. They see you the same way you see the positives in others” Law said, holding your gaze. You stopped breathing, eyes widened with shock.
“What, have you never had anyone tell you that?” he asked, looking at your expression. He leaned back against his desk, halfway sitting on it as he crossed his arms. You could only shake your head as you remembered to breathe. He grunted.
“Well. Remember it. Come back here same time tomorrow to pick up the medicine too. We’ll talk a little more too.”
You didn’t move, too shook that someone cared about you enough to do this.
“I’m sorry” you whispered. Tears gathered in your eyes again.
“Why?” Law seemed bewildered at the idea.
“I must’ve manipulated you somehow to care about me. To go through this… you don’t have to. It’s okay. I’ll be fine. I’ll live”
“I guarantee I am the last person on this ship you could manipulate” he said. Something warm and slightly heavy plopped on your head. A white hat brim entered your field of vision. You shrunk down further, starting to sob.
“You’re part of my crew, even temporarily. Even if I wasn’t your captain, I’m your doctor. You only told me the symptoms that you hide so well, not even saying at first that it was you who had it. How could you have manipulated me?”
He knelt in front of you, producing a tissue and handing it to you. He rested his hand on your head, securing his hat.
“If you see a good person who’s sick, would you help them if you could?” he asked gently. You nodded slightly, wiping the snot dripping from your nose.
“Then why wouldn’t I help you? You deserve basic human decency and respect, you know. Right now, you’re treating yourself worse than your enemies.” He said softly. Your sobs increased at his words. He sighed.
“C’mere.” He lifted you up bridal style and took your seat, holding you on his lap. You pushed him away.
“Hey. It’s okay. You’re not hurting me. You’re not manipulating me. I’m doing this of my own accord. When’s the last time you had a real hug like this?”
You shuddered in a breath, unable to speak through your sobs. His warm hand rubbed your back, and you let your head fall onto his shoulder.
“T-t-thank… you” you wailed.
“Always” he muttered.
--
“Are they okay?!” Shachi whisper-yelled as Law passed him the hallway with you cradled in his arms.
“They will be” he replied quietly. He didn’t want to disturb your tear-induced sleep. You looked peaceful, finally. He saw the pain in your eyes, the pain you had inflicted on yourself. Shachi nodded in understanding and continued on his way. Law carried you gently to your bunk and tucked you under the blankets. He removed his hat, knowing it would make you feel guilty if he let you sleep with it. Smoothing stray hair away from your face with his hand, he unthinkingly dropped a gentle kiss on your forehead. A light blush dusted his cheeks with the realization of what he’d done. He stood quickly and walked quietly from your sleeping form.
“Sleep well”
#one piece x reader#trafalgar law#trafalgar one piece#trafalgardwaterlaw#trafalgar d law x reader#one piece fluff#fluff#tw depressing stuff#tw self doubt#tw self harm#angst and fluff#feels#one piece feels#one piece fanfiction#no smut#romance if you squint#you're not alone
145 notes
·
View notes
Text
breaking down the "Debunking Sysmeds" carrd (just for kicks 😍) part 1!!
was sent this carrd by a friend and it's been a while since i've interacted with endo logic so here we go! <3 let's break it down section by section because whew girlie is chock full of bonkers misinformation! henceforth, i will be referring to the person who made the carrd as the "creator" and using they/them pronouns, as i do not know their pronouns (please let me know if anyone does!).
----------
THE "CLAIMS AND REBUTTALS"
if y'all don't stop using 20 different fallacies in your arguments... it'll be all over for you... seriously!
----------
the first point the creator tries to rebuff is the argument of "DID/OSDD-1 is a trauma disorder." starting off strong, i see! their response is essentially that nowhere in the diagnostic criteria within the DSM-V or ICD-11 does it say that DID/OSDD requires trauma. immediately going to stop you there - it may be to the creator's benefit to read any other page of the DSM. the third sentence on the intro page for trauma-related disorders is:
"Placement of this chapter reflects the close relationship between these diagnoses and disorders in the surrounding chapters on anxiety disorders, obsessive-compulsive and related disorders, and dissociative disorders"
additionally, had the creator read the ENTIRE DID entry, not just the diagnostic criteria, they would have found this lovely quote, found in the "development and course" section of the DID entry:
Dissociative identity disorder is associated with overwhelming experiences, traumatic events, and/or abuse occurring in childhood.
within this section, the creator also discusses an article written by allen j frances, the person responsible for the changing of MPD to DID, in which he discusses the abundance of false diagnoses of DID following the recognition of it as a disorder after the release of the DSM-IV in 1994. firstly, the creator of the carrd incorrectly stipulates that frances renamed MPD to DID in the DSM-V. secondly, the creator uses frances' criticism of increased DID diagnoses to demonstrate that the diagnostic criteria isn't to be trusted.
what.
so, to reiterate, we should trust the DSM-V when it doesn't emphasize trauma in the diagnoses (false), but we also shouldn't trust the DSM-V because of an article written by someone who had nothing to do with the DSM-V?
----------
the second point the creator decides to rebut is "Science says Endogenic systems don't exist." now, much of this argument is rooted in a few "studies" the creator has linked, which i will analyze more in a separate section reserved specifically for source analysis. but! one really interesting part of this section is the comparison between endogenics (an internet community and internet term) to "marginalized religions such as Shamanism" which is a direct quote.
something i really need endos on the internet to understand is that you can't compare your just-realized "system" of non-traumatic origins to the spiritual practices of highly religious individuals who have been practicing their religions for decades, engaging in extreme asceticism, and doing really intense internal reflection. and you especially shouldn't throw in words like "marginalized" to your argument. at what point does that become cultural appropriation?
i also find it soooo interesting that the creator refers to the otherkin and alterhuman communities as something that has "existed long before the term DID/MPD/OSDD-1/DDNOS." the first recorded use of "otherkin" was in 1990 in a newsletter from an elf club in kentucky, and it has been predominantly an online community. the concept of DID (MPD at the time) first appeared in the DSM-III in the 1970s.
the creator also refers to endogenic systems as something people "believe" in, which is... questionable in it's own right. it is interesting that they brought this point up in the section in which they are trying to combat the idea that science does not back up endogenic systems, as religious beliefs (with no proof, something that people simply "believe" in) and science (which is backed up by decades of research) aren't exactly comparable.
----------
the third point rebutted is the statement "You're not a system, you're schizophrenic/psychotic." honestly, not a big issue with this one. i've never heard anyone say this personally, but i can totally see it happening, and it definitely shouldn't be done. no one can really tell you what you're experiencing, so i take no issue with the creator on this one! i don't think this at all supports the existence endogenics, though.
----------------
i don't want to make this too long, so i'm going to write out the remainder of the points on a part 2!
#syscourse#discourse#anti-endo#anti endo#radinclus#endogenic#multiplicity#systems#plural#critinclus#syscourse tw
25 notes
·
View notes
Text
I'm not very good at being loved, or loving back, but I'm going to keep trying gdi
I've spent most of my life completely detached from other people; up until 2012 or so, I even fit the diagnostic criteria for schizoid personality disorder. I'm just now learning what it feels like to touch someone else's soul and let them touch mine. Even with the friendships I've had for a decade, I have only recently begun to truly understand what it is to be loved and to love someone else. It's terrifying and beautiful.
I read about schizoid personality disorder when I was maybe 14 years old, and even then I thought it was an eerily apt description of what was going on in my mind. To clarify, the criteria for SPD from the DSM-5 are as follows (American Psychiatric Association, 2013)
A persistent pattern of disinterest from social interactions and a limited variety of expression of emotions in a close personal settings, starting in early adulthood and there in an array of contexts, as shown by at least four (or more) of the subsequent:
neither wants nor likes close relationships, counting being part of a family
almost constantly picks introverted activities
has little if any, thought in engaging in any sexual experiences
seldom derives pleasure from any activities
has no close friends other than immediate relatives
appears apathetic to the admiration or disapproval of others
shows emotional coldness, detachment, or flattened affectivity
This described me to a T. I wouldn't seek out relationships of any kind, and I put no effort into deepening or even maintaining the ones that formed incidentally through school or work. My favorite activities were those that didn't require socializing--playing the piano (as a soloist), reading, and video games (before online playing was a thing). I didn't care about sex and sexual relationships (still true; different reason). My only close relationship was with my sister, and even she didn't know 75% of what was going on in my head. I didn't care about other people's opinions of me, because I thought other people were completely irrelevant. And even the activities I liked best rarely made me feel any kind of long term pleasure because I was just so... disconnected. Dissociated. I felt completely hopeless constantly and questioned if a life like mine was worth living.
Things started changing a little bit when I got into writing fanfic and participating in fandom. That was the first time I found myself enjoying being part of any kind of community. I started to make friends with people in the same fandom circles as me, but they weren't just incidental friendships based on proximity--they were based on shared interests. For the first time, I had friends that I would actively seek out instead of being totally indifferent to whether they were around or not.
I started weekly therapy when I started grad school in 2015, then added various kinds of group therapy as time went on. And after the first 2 years of this, it became very apparent that I did NOT have schizoid personality disorder. What I had was abandonment trauma, chronic depression, and severe PTSD from my frankly horrific childhood. I had built walls around myself that were so thick that no one could hurt me. I was in a state of near-constant dissociation, fueled by increasingly severe self harm, to escape the incredible amounts of pain I'd suffered and had never been able to take the time to process.
Schizoid personality disorder has no known causes and no concrete treatment. When I thought I had that, I felt like I could never change, so there was no point trying to. I felt like I was damned to this kind of half life forever. But PTSD, depression, and abandonment trauma were things that I could change, at least I'm theory. That gave me hope. Maybe there was more to life, and maybe I could have some of it.
Once I realized all this, I started working on the long, slow process of tearing down those walls and finally processing the old, festering pain.
Friends, it has been a Very long, Very slow process.
Dissociating from the pain didn't make it go away. Tuning back in means that now I'm feeling it. It's not great, in fact, it's been pretty fucking terrible. I cry a lot. I'm angry a lot. I scream into my pillow a lot. I've cut down on self harm dramatically, but there are still times where being in my mind hurts so much that I get desperate enough to do it. Or desperate enough to knock myself out with drugs or alcohol. Because god, I went through some Bad Shit. I went through it alone. I went through it silently. And then I carried it with me for a lifetime as it slowly rotted into something more toxic and dangerous than the original pain. A cut on the palm of your hand hurts. But if you don't take the time to clean it immediately, it gets infected, and then it hurts a lot more. Then it leads to sepsis, maybe even to amputation or death.
I have come so close to death from this infection. Cleaning the wounds is slow and painful, but at least I'm no longer getting sicker. Now at least I'm starting to recover.
The defensive walls have been a little easier to work through, but not much. I often feel like an abused dog that learned to see all humans as equally and inherently dangerous. Like that poor dog, when I meet someone new, I'm afraid to take the chance that maybe THIS person is actually ok and not dangerous. How can I tell the difference? What if I'm wrong and get hurt again? What if I get hurt so badly this time that I can't recover from it?
But sometimes, somehow, I DO get up the courage to take that chance. I used to think it's because I'm stupid, but maybe it's because I'm hopeful. Fine line between those two things. But I think I'm hopeful.
I am hopeful because sometimes when I take the chance and let down my guard, I am rewarded with joy and...love? I am rewarded with feelings I didn't know existed. I am rewarded with something that makes me think that this life is absolutely worth living. I am rewarded with the things that I only barely thought possible.
Sometimes I do get hurt, though. And in those moments, I flinch back behind my walls. I castigate myself for being foolish and trusting people when I know all people are dangerous. But then, eventually...I let down my guard for someone else.
You see, I have to remember that I have never been hurt so badly by anyone that I couldn't recover from it. Even as a small, helpless child I survived terrible things. I survived everything they threw at me, even when I was powerless and alone.
And now? I am no longer powerless. I am no longer alone. I am no longer small and helpless. If I survived those terrible things back then, I can certainly survive anything now.
So I am hopeful.
1 note
·
View note
Text
Actually 🤓
The isstd doesn't say that. TPA is literally the only one saying that, and people like you parroting it.
It says you're supposed to treat the whole system as a collective, and it goes on to discuss system accountability. I DARE you to find the section in the isstd that says that.
But honestly, I'm going to find it for my followers first, so.
It basically boils down to, use the client's preferred language unless it poses a danger. Yes, including people focused language.
And I quote:
Alternate Identities: Conceptual Issues and Physiological Manifestations
The DID patient is a single person who experiences himself or herself as having separate alternate identities that have relative psychological autonomy from one another. At various times, these subjective identities may take executive control of the person’s body and behavior and/or influence his or her experience and behavior from “within.” Taken together, all of the alternate identities make up the identity or personality of the human being with DID.
It goes on to give a few clinical definitions by different researchers.
Many terms have been developed to describe the DID patient’s subjective sense of self-states or identities. These include personality, personality state, self-state, disaggregate self-state, alter, alter personality, alternate identity, part, part of the mind, part of the self, dissociative part of the personality, and entity, among others (see Van der Hart & Dorahy, 2009). Because the DSM–IV–TR (American Psychiatric Association, 2000a) uses the term alternate identity, this term is used in the Guidelines for consistency.
Clinicians should attend to the unique, personal language with which DID patients characterize their alternate identities. Patients commonly refer to themselves as having parts, parts inside, aspects, facets, ways of being, voices, multiples, selves, ages of me, people, persons, individuals, spirits, demons, others, and so on. It can be helpful to use the terms that patients use to refer to their identities unless the use of these terms is not in line with therapeutic recommendations and/or, in the clinician’s judgment, cer- tain terms would reinforce a belief that the alternate identities are separate people or persons rather than a single human being with subjectively divided self-aspects.
So what this is talking about is... for example, someone religious who believes that some or all of their alters are demons. Clinicians shouldn't play into that. The interplay of religion and psychology is incredibly dicey, but a clinician shouldn't engage with an alter that believes it's a demon and has traits, like indestructible or something. No, the clinician is supposed to help the demon understand it's stuck in this body, and if the body goes to jail or dies, it's game over for everyone, demon included.
Next, we move to:
TREATMENT GOALS AND OUTCOME Integrated Functioning as the Goal of Treatment
This is always my favorite part to show people who haven't read the Treatment guidelines :)
We start:
Although the DID patient has the subjective experience of having separate identities, it is important for clinicians to keep in mind that the patient is not a collection of separate people sharing the same body. The DID patient should be seen as a whole adult person, with the identities sharing responsibility for daily life. Clinicians working with DID patients generally must hold the whole person (i.e., system of alternate identities) responsible for the behavior of any or all of the constituent identities, even in the presence of amnesia or the sense of lack of control or agency over behavior (see Radden, 1996).
Treatment should move the patient toward better integrated functioning whenever possible. In the service of gradual integration, the therapist may, at times, acknowledge that the patient experiences the alternate identities as if they were separate. Nevertheless, a fundamental tenet of the psychotherapy of patients with DID is to bring about an increased degree of communication and coordination among the identities.
You see, that's important, because:
Helping the identities to be aware of one another as legitimate parts of the self and to negotiate and resolve their conflicts is at the very core of the therapeutic process. It is countertherapeutic for the therapist to treat any alternate identity as if it were more “real” or more important than any other. The therapist should not “play favorites” among the alternate identities or exclude apparently unlikable or disruptive ones from the therapy... The therapist should foster the idea that all alternate identities represent adaptive attempts to cope or to master prob- lems that the patient has faced. Thus, it is countertherapeutic to tell patients to ignore or “get rid” of identities (although it is acceptable to provide strategies for the patient to resist the influence of destructive identities, or to helpcontrol the emergence of certain identities at inappropriate circumstances or times).
Then it gives a few more examples of counter productive things, and we finish off with:
Kluft (1993a) has argued that the most stable treatment outcome is final fusion—complete integration, merger, and loss of separateness—of all identity states. However, even after undergoing considerable treatment, a considerable number of DID patients will not be able to achieve final fusion and/or will not see fusion as desirable.
Accordingly, a more realistic long-term outcome for some patients may be a cooperative arrangement sometimes called a “resolution”—that is, sufficiently integrated and coordi- nated functioning among alternate identities to promote optimal functioning.
So no, it doesn't only promote fusion, either.
Anyways. We're so off point. Within the community, alters and CDDs tend to be parts focused, plural is people focused. That's just facts. They overlap and there are always exceptions and people exploring boundaries, but that's the general consensus.
I never said there weren't flaws with the psych system, I said that plural is not a blanket term, it's opt in. As another person said, it's opt in, not opt out. Do not use plural as a blanket for CDD systems. The lowest score on every poll is CDD and plural. There are two other polls, fyi. Tumblr CDD systems don't like to be called plural, and I explained why. I have given you links and history.
Use system as a blanket, not plural.
"System" is the alternative. It is the blanket.
You think I'm arguing about things I'm not. Welcome to tumblr, pwCDDs prefer system, and I explained why.
As for why you shouldn't trust lunastusco, well, they literally just denied a thing I linked in my first post. Like... it's right there?? The person who first coined plural is linked in my post, explaining why, and lunastusco really just said, "nahh, that's not true." Would you like my debunks of LB Lee's articles? :)
God sysmeds are often so sure that they're special for their system being formed from trauma and how hard it is after going through trauma, and like
Trauma IS hard. But not everyone who has experienced trauma also has DID/OSDD. If trauma was the unifying factor here, why would so many people who have PTSD or have otherwise experienced abuse or traumatic events be ableist and shitty about systems? Who do you think is more likely to support you as a system: a singlet who has experienced trauma and knows NOTHING about DID/OSDD other than what they've seen from books/movies/etc (which is most people), or another system who happens to have been formed through means other than trauma?
Also not everyone who has DID/OSDD even wants to call themselves a system, so yes, systemhood IS an identity -- because even people with DID/OSDD can choose what terminology/framework they identify with.
"Plural" is an inclusive descriptor. Even only looking at people diagnosed with DID/OSDD-- it would be incorrect to call them systems if they don't consider themselves systems, while "plural" is a better way to include people with DID/OSDD who don't identify as systems but understand they are multiple people/facets/alters/parts/whatever.
That last part, the plurality, is the only thing that everyone with DID/OSDD have that makes it possible to understand each other. Traumatized people without DID/OSDD are not going to understand. But plural people without DID/OSDD might.
As a last note, incorrectly defining endogenic as a "system without trauma" means you don't understand trauma. There are many types of trauma people often experience without realizing. Medical trauma, religious trauma, trauma from the fucking COVID-19 pandemic-- the list goes on. I'm not sure anyone can really go through life without experiencing trauma at one point or another. Which would mean "systems without trauma" probably don't exist, sure-- but that's not the definition of endogenic. Endogenic systems just become systems first and may experience trauma later.
So nope, the trauma isn't what makes you special. Guess again.
(Signed, a system diagnosed with DID.)
77 notes
·
View notes
Text
How to Properly Self-Diagnose
This is a highly requested post! Especially after our last post, many people asked how they would go about properly doing research and some specifically asked for this post. So here we go!
1. Notice your symptoms and track them. Determine if it's a one time thing, or if it's repeated for several months. Usually when self diagnosing, you already have a disorder in mind but not always. If you don't, try and see what disorders your symptoms match with and start researching those. If you do, determine if your symptoms are repetitive and cause some type of distress in your life.
2. Research!! Do research from credible sites, the DSM-V's section on the disorder, read posts from lived experiences, /ask/ about lived experiences, etc. Learn what it's like to have this disorder and what it's like to live with it and see if your experiences match up. This is also the time to research similar disorders (such as OSDD-1a and BPD). This helps you determine which disorder you're most likely to have. This is not tests online. Do not do a test online and say you have a disorder. Some can help determine if your symptoms do in fact line up, but they can't be your reason of self diagnosis.
3. Factor in family history. Many disorders have a part in genetics which will make a person more likely to have it. Some examples would be depression, anxiety disorders, personality disorders, and what people typically think of when they hear neurodivergent (autism and ADHD). For example, we've self diagnosed with BPD after tons of research and learning the body's mom has it. Paired with our symptoms and the trauma we faced, it's likely for us to have BPD as well.
4. If possible, reach out to a professional. Explain your symptoms, and say you've done some research yourself and you /may/ have the disorder you've been researching. They will take time to diagnose it, of course. But professionals can also think more rationally than you can and be less biased when it comes to diagnosis.
5. Remember it's okay to not know. Sometimes, it's not the disorder you've been researching and you can't tell what it is. It's okay to not know and to wait to get professional help deciding what it is.
6. Always be openminded that you may be wrong. If you get professional help and they diagnose you with something different but it explains your symptoms, it's important to believe them. They explained your symptoms with their diagnosis and they generally have a wider range of knowledge on different types of disorders.
7. When self diagnosing multiple disorders (like us with BPD and DID), first determine if they're comorbid or not. Then look at the symptoms for each. BPD and DID heavily overlap, but there are other differences that helped us. BPD cannot cause alters or a system, BPD doesn't cause amnesia, BPD doesn't cause constant dissociation (which we experience). DID doesn't cause the intense fear of abandonment, the idolization of FPs and those unstable relationships, black and white thinking, etc. We experience all of those symptoms, which is why we've self diagnosed with both. Follow a similar pattern and notice if your symptoms can just be caused by both or if you have the overlapped ones and ones that don't overlap from both disorders.
8. If you misdiagnose, it's okay!! Communities won't bash you if you do the proper research and simply just misidentify your symptoms. My advice for this would be to apologize for intruding on a community that isn't yours and to apologize for any harm and misinformation you may have done (intentionally or not).
#osdd system#did system#did alter#did osdd#dissociative system#osdd#osdd community#osdd support#osdd things#adhd#autism#personality disorder#bpd tag
344 notes
·
View notes
Text
Is Shakespeare's Richard III a Psychopath?
It is once again Shakespeare Richard III hours on this blog. A question that's come up in multiple conversations I've had with people in the past is whether or not Richard is a psychopath. With the disclaimer that this is not a strictly literary question and that it's hard to put modern psychiatric diagnoses on fictional characters from 400 years ago, etc., I looked up the actual DSM V criteria for Antisocial Personality Disorder and I think reading it actually highlights some interesting things that are going on the first tetralogy.
So let's go through the diagnostic criteria; all the letters here are criteria that need to be met:
A. Impairments in self-functioning, either in "identity: ego-centrism; self-esteem derived from personal gain, power, or pleasure," or "self-direction: goal-setting based on personal gratification; absence of prosocial internal standards associated with failure to conform to lawful or culturally normative ethical behavior," AND impairments in interpersonal functioning, either in empathy or intimacy.
B. Pathological personality traits: antagonism, characterized by manipulativeness, deceitfulness, callousness, and hostility, and disinhibition, characterized by irresponsibility (defined here as not following through on agreements, promises, or obligations), impulsivity, and risk-taking.
C. "The impairments...are relatively stable across time and consistent across situations."
D. "The impairments...are not better understood as normative for the individual's developmental stage or sociocultural environment."
E. "The impairments...are not solely due to the direct physiological effects of a substance... or a general medical condition...
F. "The individual is at least age 18 years."
Looking through A and B, we're checking a lot of boxes based solely on the text alone. But C and D are where things get interesting.
As many boxes as I was able to check going through those first two criteria, most of them are not stable or consistent throughout the three plays Richard appears in. When we first meet him at the end of 2H6, he is ruthless but more than capable of pro-social behavior, helping the "old" and "feeble" Salisbury three times in battle by going into the middle of the danger, bringing him away, and then keeping him safe (see the beginning of 5.3.) Up until he emerges as a villain in 3.2 of 3H6, Richard is portrayed as brutal to his enemies but loyal to his family and allies. He even calls out Clifford's killing of Rutland, an innocent child, as morally wrong. And that's not even speaking of his monologue in 5.3 of Richard III, before the Battle of Bosworth field, where he feels incredibly guilty and regrets everything.
That leaves us in kind of a weird place, to be presented with a character who displays all these dysfunctional and harmful traits, but only in the middle of his story.
But it's D that raises the real questions and I think helps you see something that's going on in the tetralogy. Is anything Richard does nonnormative for a sociocultural environment full of warfare, murder, and backstabbing for political gain that's been getting worse and worse over the course of four plays? I don't really think anything he does is completely unprecedented. Part 2 is full of nobles plotting against and killing each other and even starting rebellions to gain and keep power. Humphrey is pretty harsh during his stint in power. Clifford later kills Rutland. And let's look back at some of Richard's early ruthlessness in light of this: his father York (who also breaks his agreement with Henry to end the war) praises his brutality. This behavior is not only normalized, but encouraged. Richard's bloody rise to power and paranoid rule are kind of just the logical conclusion of everything that's been building up over the course of the tetralogy.
So I guess my answer to the original question is no, I don't think so. You do have to meet all the letters to qualify for diagnosis, and I didn't even quote the language about "impairments in functioning" - Richard functions just fine until there's no more fighting - but more importantly, trying to view Richard as pathological pins everything on one individual in a narrative that chronicles the downfall of a civilized society into one where this stuff is normal. Maybe part of the point is that he's a product not just of family or interpersonal dynamics but of his larger social environment, and maybe that's why, in the end, even he is able to recognize that it isn't right.
10 notes
·
View notes
Text
Let’s talk about depression
In my latest book ‘The Power of Death’ I talk about this topic in depth. I will post the links to it at the end of this post if you are interested in reading it. If there is one part of the book that resumes the message that I wanted to transmit, it’s Mikasa’s (The main character) press conference at the end of the last chapter.
It’s okay if you don’t read the whole book, but at least, read the following extract from the book (some stuff removed to avoid spoilers):
Standing behind the podium Mikasa started the conference by saying,
"Paradis island doesn't have studies about the topic we are about to discuss, but other countries do. In the United States, in 2019, a total of 47,511 Americans died by suicide and an estimated 1.38 million attempted it. [2] What about other countries? you may ask, well, overall, suicide was in the top 10 leading causes of death across Eastern Europe, Central Europe, high-income countries within the Asia Pacific, and Australasia. Within regions and countries, though, suicide rates soared among people with lower social and economic status. [3] This data comes from research made by the Institute for Health Metrics and Evaluation in Washington, Seattle. [4] This goes without mentioning that for every suicide, it is estimated that there are seven to ten people intimately affected."[8]
Mikasa stopped to take a sip of water and looked back at the audience to continue her speech,
"Untreated depression can, and possibly will lead to suicide, death. In biology, homeostasis is the state of steady internal, physical, and chemical conditions maintained by living systems. [5] Depression does have an impact on this. Research shows that the hippocampus is smaller in some depressed people. For example, in one fMRI study published in The Journal of Neuroscience, investigators studied 24 women who had a history of depression. On average, the hippocampus was 9% to 13% smaller in depressed women compared with those who were not depressed. The more bouts of depression a woman had, the smaller the hippocampus. [6] The hippocampus is not the only area of the brain affected by depression, the Amygdala, and Thalamus are also affected.[6] Depression is, and should be treated as, an illness that, if left untreated, can be lethal. Just remember the statistics I gave you about suicide at the beginning of my speech. With that data as the base of my argument, it is safe for me to say that depression is one of the top life-threatening illnesses having, in some countries, the top mortality rate overall."
A woman from the public raised her hand and when allowed to talk she said,
"How can you call an illness to something that can be 'cured' by just talking to a so-called doctor about your issues?"
Mikasa gave the woman a serious look and said, "Therapy, is not just talking. Psychotherapy stands over years of research and development going as back as the 19th century. There is extensive evidence of its effectiveness. Also, most cases of depression treatments include medication."
Then a man shouted, "So now doctors will give our kids a bunch of pills just because the child is feeling a little sad?!"
"Several tests are usually performed before a psychiatrist gives a diagnosis of depression. Tests like: physical exams, lab tests, psychiatric evaluation, and the country's manual of mental health like for example the DSM-5 which is the Diagnostic and Statistical Manual of Mental Disorders from the American Psychiatric Association, is applied. After that, the psychiatrist might do more testing to see if medication is an option. Because they are physicians, psychiatrists can order or perform a full range of medical laboratory and psychological tests which, combined with discussions with patients, help provide a picture of a patient's physical and mental state. Their education and clinical training equip them to understand the complex relationship between emotional and other medical illnesses and the relationships with genetics and family history, to evaluate medical and psychological data, to make a diagnosis, and to work with patients to develop treatment plans.[7] In other words, for a doctor to prescribe medication to your child, it has to first do an extensive evaluation on the kid before even start to consider medication in the first place. If in the end, medication is needed, then it would mean that your kid is not only 'feeling a little sad', it means that there is a deeper problem that needs to be addressed and the physician will have a lot of evidence to back up his claim.", Mikasa said.
She stopped talking and pinched the bridge of her nose out of frustration, then she looked seriously at the same man she was addressing before, and said, "Would you rather lose your child to suicide or seek valid, scientific-based help to save the kid's life?"
The man was frozen in place. He was not expecting to be put in the spotlight this way. Mikasa noticed the teenage kid who was seated next to him with his head bowed to the floor. Before he could answer Mikasa said,
"Do you even know how depression feels like? To have your own mind to conspire against you? To illogically feel worthless, alone, like nobody can understand you, or at least, nobody that hasn't been through the same darkness as you. Do you know how it feels when people tell you worthless crap like, 'get over it', or 'just stop being sad' like being sad is just an option you chose because apparently, you like to torture yourself? Have you ever contemplated to end your life out of desperation to get an out, a break, from your own mind?"
By this point, the kid was looking straight at Mikasa with tears pouring down his eyes. Mikasa knew she was getting through him. She grabbed the microphone and started to walk while resuming her speech,
"To feel like you are constantly drowning. To feel like an ungrateful ass because logically, you should be happy because you have everything. But you aren't... Thinking that there must be something really wrong with you for you to feel this way without an apparent reason. To feel lost, alone with this feeling that is eating you inside slowly until it gets to the point where you desperately want to rip your soul out of your body. When it gets so bad that causing physical pain to your body is an option since, at least, for a brief moment, your mind focuses on the physical pain which is better for you because the emotional pain is so much greater than a little cut on your forearm."
The man realized that she was no longer addressing him but the person seated next to him, his own son. Mikasa stood right in front of his son and looked at him in the eyes. She lowered the microphone and while brushing her fingers through the kid's scars on his forearm she said to him,
"You are not alone."
Then, she showed him her own scars and the kid stood up pulling her in for a hug while repeatedly saying, "Thank you"
Reporters were recording the whole encounter. It was real. Depression was real, and it was being recorded. The father of the kid sat back down while looking at his son in shock. Trying to find the words to say he just pulled him in for a hug while saying,
"I'm sorry. I didn't know."
"You never really asked.", the boy replied.
"I'm sorry. I will do better. You deserve better.", his dad replied with a broken voice.
Mikasa lifted the microphone again to talk and said, "Depression is a silent killer. It could be your child, partner, parent... it could be closer to you than what you think. So before you speak about the topic remember that. Your words could be hurting one of your own for your lack of empathy."
She walked towards the podium again to start answering reporter's questions,
"What would you say to someone who is going through this?"
Mikasa lowered her head lost in thought and said, "You don't need to have a traumatic event in your life to have depression. Depression is not just sadness and is not only caused by personality type or environmental factors. Genetics and biochemistry are also a big part of it, and those two have nothing to do with how much crap you've been dealt in life. What I am trying to say it's that, it's okay to not be okay, you don't need a reason to, and you don't need to feel worse about it for not having a reason. Being sad is not a right you earn after a certain amount of societally accepted shit has happened to you. Just seek help, see the situation logically, and not let people bring you down. If possible, educate others on the topic. Be the change you want to see in the world."
She paused, thinking of her own struggles with depression, and the stability and peace she finally felt once the pills started to work on her. Sure, dark thoughts still lingered at the back of her head, but, it was no longer unbearable, now, it was manageable. With time and therapy, she had managed to live with it, minimizing their negative effect on her. With this in mind, she said,
"Do not get frustrated if anti-depressants don't work at first, sometimes it takes a couple of tries with different types of medications to get the one that works for you. Researchers are exploring possible links between the sluggish production of new neurons in the hippocampus and low moods. An interesting fact about antidepressants supports this theory. These medications immediately boost the concentration of chemical messengers in the brain (neurotransmitters). Yet people typically don't begin to feel better for several weeks or longer. Experts have long wondered why, if depression were primarily the result of low levels of neurotransmitters, people don't feel better as soon as levels of neurotransmitters increase. The answer may be that mood only improves as nerves grow and form new connections, a process that takes weeks." [6]
She paused and looked at the crowd. Then, she said,
"In the meantime, stay alive, even if it feels against your will. Do not give a permanent solution to a temporary problem, because trust me, it DOES get better."
Stay Alive
Feel free to share this to raise awareness. This book has all the things I wish someone had told me in my darkest moments, and I hope, it can help someone out there who is going through the same painful path in life. Remember, it's not your fault, you are not alone.
Resources used in this part:
[1] Oswego City School District Regents Exam Prep Center. Archived from on 25 October 2012. Retrieved 12 November 2012. URL: homeostasis
[2] American Foundation for Suicide Prevention: suicide-statistics
[3] global-suicide-rates-study
[4] Global, regional, and national burden of suicide mortality 1990 to 2016: a systematic analysis for the Global Burden of Disease Study 2016: content
[5] Gordon., Betts, J. Anatomy and physiology. DeSaix, Peter., Johnson, Eddie., Johnson, Jody E., Korol, Oksana., Kruse, Dean H., Poe, Brandon. Houston, Texas. p. 9. ISBN 9781947172043. OCLC 1001472383.
[6] What causes depression? Harvard Medical School: what-causes-depression
[7] What Is Psychiatry? from the American Psychiatric Association. URL: what-is-psychiatry
[8] Lukas, Christopher; Henry M. Seiden (1997) [1987]. Silent Grief: Living in the Wake of Suicide. Northvale, New Jersey: Jaron Aronson. p. 5. ISBN 0-7657-0056-5.
Book Summary:
Mikasa is a woman suffering from clinical depression. There is one thing that she is sure of: she wants to die. But when she received some unexpected news that makes her death wish a reality, she starts to wonder if that was really what she wanted. She starts a journey to discover the truth about her biological parents that gave her up for adoption when she was a baby. This journey will guide her to cross paths with someone as broken as her, someone that hates her to death for what her biological family did to him. Will she have the courage to, for once, fight to live? or will she let him drag her to hell with him?
The book is tagged as an ‘Attack on Titan’ Alternate universe fanfic but honestly you don’t need to know anything about the anime to read it. The story has nothing to do with it so feel free to read if you haven’t seen it.
You can find the story in the following links:
Archive of our own:
https://archiveofourown.org/works/30452145/chapters/75087657
Wattpad:
https://www.wattpad.com/story/264598251-the-power-of-death
14 notes
·
View notes
Note
Hey, I just read your post on ADHD/EFDD and was just wondering if you have read any research articles on this and if you have, could you tell me which ones because it all sounds super interesting and I need to choose a topic for my psych lit review and I’m thinking about doing something to do with all the stigma around and misconceptions about different mental health disorders.. it’s totally okay if not tho, I know it’s a big ask, but thanks anyway
That sounds like such a great topic!!! I would be HONORED to help :D
The first person I think of when discussing the term EFDD is Dr. Russell Barkley. He’s one of the leading ADHD experts, and has been a spearhead for studying executive dysfunction in people with ADHD for decades. Very much ahead of his time compared to the DSM. I’ve had his book “Taking Charge of Adult ADHD” recommended to me so many times, but have yet to read it.
Here’s some free stuff, though!
[reblogs appreciated because Tumblr hates posts with links and I wanna make sure this anon sees it!]
I tried to include some short stuff and longer stuff, some articles, images, videos, and comic recs, so you can choose based on your current energy and focus level :) I’ve also bolded links and key points of each source if you like skimming. Let’s go!
...................................
Here’s an interesting article/study on EFDD! They found that “ADHD [is] associated with deficits in inhibition, managing one’s attention, self-directed speech and rule-following, self-motivation, and even self-awareness [...] ADHD therefore involves deficits in self-restraint, [...] selfsensing and imagery, self-control of emotion, and self-directed play for problem-solving.”
Thank you for motivating me to look up some articles, because I learned some new things, too! For instance, they assert that ADHD could also be called SRDD (Self-Regulation Deficit Disorder), but conclude the article by saying either SRDD or EFDD fits better than ADHD, and that the terms could be used interchangeably, because SR (self-regulation) and EF (executive function) are effectively talking about the same things. So his assertion is that even if the name ADHD never changes, it can still be scientifically classified as either of the other terms. I believe in recent years he’s preferred EFDD more and more.
[note that the above article/study is from 2011, back when we were on the DSM-IV, so a lot of research has been done since then]
...................................
If that article’s a bit wordy or you want something more visual and up-to-date, here’s a really detailed PowerPoint presentation used during the 2018 ADHD Symposium! It’s long but well-organized so you can just read the big headers or you can read all the bullet points explaining it. Keep in mind this was a lecture, so some of it probably made more sense in person. I’m glad I read this, because I realize the terminology I’ve used is slightly off: according to the Symposium, there aren’t “subtypes” of ADHD, but the different names (ADHD-PI, ADHD-PH, and ADHD-C) are really just used to show the prevalence of certain symptoms in that individual. So they’re all terms for ADHD, but “subtype” was poor word choice on my part.
Oh! I just found a video of him giving a lecture in 2012 using many of the same PowerPoint slides! Here ya go! It’s a bit longer than the other videos I’ve linked below (13min), but it might make the slides easier to interpret :)
...................................
If you want a really short and basic overview, here’s a video explaining 5 main ways executive functions affect the brain and how they work differently in people with ADHD. [I put the video below as well if you wanna stay on tumblr] It’s from 2010, but it holds up. It only covers 5 big ones, so remember (if you can) that executive function affects EVERYTHING and the symptoms will affect everyone differently and at different levels.
This is just the most basic overview and a good place to start:
youtube
...................................
Here’s one where he talks about our Time-Blindness! (below) I was going to pick a couple favorite quotes to give you an idea, but that’d wind up being a transcript of the whole video because HE GETS IT. This is from 2014, but I CANNOT recommend it enough!!! He mentions that ADHD doesn’t have a deficit of attention, but rather a deficit of intention. He describes us as having a near-sighted sense of time, and talks about deadlines, “laziness,” etc.
ALSO he talks about how our brains DON’T CONNECT our knowledge to our performance (back of brain to front) like everyone else’s, so we have the same level of knowledge and intelligence, but can’t access and use it the way others can. This is why teaching skills and organization/memory/time-management tips isn’t helpful -- we can learn them, but our knowledge and action centers are separated, so actually doing them/sticking with them is just as hard as before.
If you don’t watch the whole thing, at least skip to 3:29 cause that part’s really funny and relatable (ok the whole thing is relatable):
youtube
...................................
And of course, I highly recommend the YouTube channel How to ADHD! I have a couple friends who work on it, and they REALLY know their stuff! (They’re the ones who taught me during a game night that RSD isn’t a real term and it should be called “rejection-sensitivity” as part of the emotional dysregulation umbrella)
I went looking and found this video (below) has the BEST explanation of it that I’ve seen in such a concise, entertaining way. I hadn’t seen this one before, but it even covers some of the things I mentioned in that post your ask is about! Especially the Internal Restlessness that I mentioned as the true “hyperactivity” we all share; even though some of us also express outward hyperactivity, both presentations come from the same restlessness in our brains.
youtube
^^^This has some great examples, visuals, animations, and different ways of explaining and thinking about our symptoms! If you want more about this, the description has a bunch of links to their sources! Jessica and everyone else who works on this channel is great at making the videos watchable for people with ADHD (even if we have to rewind sometimes)
Here's Jessica's official Twitter @HowtoADHD! (I was today years old when I found out that she follows me)
...................................
And if you want something REALLY short and simple, here’s a 2 minute animation comparing living with ADHD to trying to film a movie with a director who keeps falling asleep [below]
youtube
....................................
If you like comics:
My favorite ADHD comic artists are: ADHD Alien [@ADHD_Alien on Twitter and @adhd-alien on Tumblr]; Dani Donovan [@danidonovan on Twitter and @danidonovan on Tumblr -- we’re somehow twitter mutuals and she is such a sweetheart. She has some really good infographics, too!!]; ADHD Bri [@AdhdBri on Twitter and @adhdbri on Tumblr]; and dreamadept [@yume_dango on Twitter and @yume-dango on Tumblr]
They’re all well-researched, funny, genuine, intelligent, insightful, talented artists who depict ADHD in a very accurate and relatable way. Go check ‘em out and support them! :D
....................................
I’m gonna stop there for now, but PLEASE feel free to add on to this with other sources, questions, videos, thoughts, comic artists, etc.!!! Hope this helps someone out there!
#adhd#actuallyadhd#efdd#executive function deficit disorder#how to adhd#dr. russell barkley#I hope you see this in time for your essay!!!#tried to give you a variety of sources and places to start#quinpost#quinanswer#oof I'm sure I forgot some adhd comic artists I love but maybe I'll remember later lol#Anonymous
107 notes
·
View notes
Text
#TheBirthOfChaos #DSM #SOA #Mayans #RP Part Two
Written by: @HackerSister @InkedPrincessMC @ReyesAtHeartMC @BikersRose @InkedWithPetals @EZReyesDSM @ReyesMayans @AShotOfAPatch

Juana "Juice" Ortiz: Juice groaned at the sound of her phone buzzing at the table beside her head. It was too fucking early and didn't people know she had a fucking hangover.
The patch party for the new San Bernadino prospect lasted well into the next morning. And Juice was feeling the weight of it. In and on her head. Groaning she swipes the message open and reads the text. #Bishop? It took her a minute to register the Santo Padre Prez name. "Fuck," she muttered to herself. She popped the tab of her favorite Red Bull flavor, dragon fruit, and opened her laptop on the table. Santo Padre needed to update its firewall. It was way too easy to hack into their traffic cams.
She watched as a dark van pulled through a light near the corner a block from the clubhouse of the Santo Padre charter. It would be sus on any other day but the day a charter president goes missing multiplied that by a thousand.
After zooming in on the plates she runs a trace. It would take a couple hours for the results. Just enough time for me to haul her ass down south. She turns on her mobile hotspot, to keep shit going while she drives. Then tuck everything safely in her saddlebags.
Hopefully the early ass time of day would mean traffic would be at a minimum.
:::::::::::::::::::::::::::::::::::

Nikki Lowman: I was riding back from Charming from seeing my father, I had just stopped at the gas station to fuel back up to get me back to Santo Padre, I had a voice on my phone from Alexis, pressing the button and Listening to the call, I frantically paid for the gas
and got back into my Motorcycle, heading home, As I pulled up outside my apartment I pulled out my cell and begins to dial #Ez cell but there was no answer. Yeah, This was definitely frustrating knowing #Bishop was taken and #Hank was attacked inside the « clubhouse. I dialed @ReyesAtHeartMC hoping she would know where #Ez was at. The ringing tone felt like forever until a voice was heard on the line.>>
::::::::::::::::::::::::::::::::::::::

Malia Reyes: I stirred as I hear my cell ringing as I reach over answer the call “Hello?” Nikki’s voice was troubled as she explained what had happened, I was definitely wide awake now.
“I think he said he was staying with my pops, I’ll keep trying to ring him. I’ll drive over there to see where he’s at, I’ll meet you at the clubhouse once I’m done.”
I couldn’t believe what I had just heard, The Prez being taken and #Hank being knocked out cold. I quickly got out of bed and got dressed, heading out to the truck and heading towards my pops house to see if #Ez was there. My head was on overdrive wondering what the hell happened.
Pulling up to the house and getting out, quickly rushing to the door and walking straight inside. “Ez you here?” Quickly rushing to the bedroom where he’d stay but it was empty. My pops walks out. “ Malia, ¿qué pasa?” Looking over at him as I look around.
“ Pop, ¿Has visto a Ezkiel?” He shook his head as I walk over to him as I place a kiss on his cheek as I head back out to the truck. “I’ll call you later.” I had to time to stick around as I jump into my truck and head to the clubhouse, I tried to figure out where Ez was at, Pulling into the yard and shutting off the engine. I get out and rush inside. “Any news?”
::::::::::::::::::::::::::::::::::::::::::

Rosa Diaz: It could have been minutes after I called @InkedwithPetals for help or it could have been hours. But the time seemed to drag agonizingly long. Time was crucial. The chances of something happening to #Bishop multiplied with each ticket of the clock.
I kept my head about me, trying to keep from focusing on the worst-case scenario. It wouldn't help anyone to panic. I sat with #Hank on the floor. He'd be more comfortable on the couch but I hadn't had nearly enough Wheaties to hoist him up.
Fortunately, his breathing remained steady and his eyes finally fluttered open. I give him a soft smile, "Don't try to get up, Viejo. Help is coming."
I lift my eyes to the door hearing @ReyesAtHeartMC come through the clubhouse doors, "In here." I call out, "There's nothing yet."
::::::::::::::::::::::::::::::::::::

Alexis Alvarez: [I parked my truck in the lot outside the clubhouse barely giving Marcus time to follow me. #Hank on the floor. My Nikes squeaked on the floor as I knelt in front of the teddy bear of a biker.] Stay put old man. I've got this. [#Hank stared at me, his words were a bit slurred but clear to me. "You came. Get those pendejos." I nodded kissing his cheek.] You know I will. [I looked up seeing a familiar face smiling at me. "Lexi." #Chuckie was odd, but he took care of things, first with SAMCRO and now here with the Mayans.
I smiled hugging #Chuckie lightly.] Good to see you, Chuckie. I'm going to need the keys to the shed. Can you do that for me? [A simple nod, but I knew he was probably just as freaked out as everyone else. Marcus stared at me. "Alexis, no!" Fury flashed in my eyes as I stood toe to toe with my godfather.] Who the fuck are you to tell me anything? Especially today. Do you ride? Wear a patch? Vote? Hold a gavel? Nope. You are the cartel's little bitch now. Shut the fuck up and sit down. [I took the keys from Chuckie and turned to Rosa.]
I will bring him home. I'm not that motherfucker behind me. [I ran out to the shed opening the doors. My breath caught for a minute as two bikes were covered with tarps. One I was keeping for Abel and the other was Esai's. As I walked over to my husband's Harley, I patted the handle of the other Harley. Now wasn't the time for tears. I slung my leg over Esai's bike and started it. Clipping my helmet in place I put on my Raybans whispering into the air.] I'm coming Tio. Just hang on. [I pulled out of the shed looking at #Chuckie.] Lock it up. [I looked at Malia and nodded.] Either one of your brothers show up, slap them and send them after me. Juicy shows up? Tell her I have my burner. I'll be back as soon as I can.
3 notes
·
View notes
Note
The last chapter of UWS, right when catra and adora meet up at the bakery before their date
HEY GIRL I’M SO SORRY THAT I HAVEN’T GOTTEN AROUND TO THIS WHEN YOU WERE SO NICE AND THOUGHTFUL TO HAVE SENT IT IN i COMPLETELY UNDERESTIMATED MY AMOUNT OF FREE TIME BUT HERE WE GO I HOPE THIS IS WHAT YOU HAD IN MIND!

So a little backstory about the last chapter: usually a chapter of about 16k-20k will take me about a month, if I’m lucky not to have enough off days. I got this chapter done, (I think it was about 33k words?) in about three weeks. I was full on sprint writing because I wanted to be done before season three dropped on what was either August 3rd or 4th? Anyways, I was eating, breathing, sleeping upper west side. Almost all of the big plot points I’d spent a lot of time dreaming up for the past nine months so they ended up just flowing out of me. I’m still amazed I got it done and it was cohesive enough for the audience because I was spent.
I got this chapter up, lost my mind over season three- especially because I’d written Angella in this chapter and it gave me and quite a few readers EMOTIONAL WHIPLASH- and then I took the entire month of August up from any writing.

I have no idea why Rob was Scottish but I am LAYING IT ON THICK WITH THAT SHOW DON’T TELL RIGHT THERE. I was exhausted by the time I was writing this part, because I write linearly, so I just wanted to be done.
I get asked this question enough to say I’m not sure what the significance of the migraines was in upper west side. There’s no canon equivalent, so I think I was just putting a little bit of me in Catra to I dunno, help with realism? At this point I’d only suffered with chronic pain- fibromyalgia to be specific- but back in April of 2020 I started experiencing migraines and my first thought was “HOW COULD I DO THIS TO CATRA?” Life imitates art.

This will be discussed more in cruel summer, but I wrote Catra as having Borderline Personality Disorder. I’ve never been fully diagnosed with BPD, but I’ve struggled with some syndromes of it, and she comes across that way to me in canon (she fits a DSM-V profile to the letter, almost). I’ve always wanted to have mental illness as a fundamental element of any of my stories because in my own life, I’ve experienced many barriers there and there’s just almost no positive rep for M.I, especially not unconventional disorders like BPD.
So Catra is talking about how she cycles through the entire spectrum of human emotions as a result of everything that’s happening to her, but also just how her psyche is reacting to it. To me, if you feel anger really intensely, the flip side can be feeling happiness really intensely, and I can testify to that.

For being completely exhausted I don’t think that first paragraph is actually too bad.
Catra has such a unique voice in Upper West Side; it’s what I believed her voice would be like if she’d been raised in the modern world, so there’s a lot more cursing and aggravation and even sarcasm, because not only is this the modern world, she’s also about three years older than she was at the end of canon.
One of the things that I think is being expressed here is the idea of resilience. Catra is resilient by nature, she’s a born fighter, and so she breaks but she gets back up. I think the biggest difference between her and Hordka- and the reason why Catra survives such an onslaught of abuse and mistreatment but doesn’t need Adora to whisk the bad out of her- is that Catra is psychology resilient. And I put her through the wringer in this universe so I wouldn’t her resilience to be very loud and apparent.

Entrapta is, without a doubt, a cyber criminal in the uws universe. But as they say, BE GAY. DO CRIME.
They won’t be ghosts for much longer, Catra.
But look at that progress! One thing that I think is really jarring for people when they start she’s god and I found her is that Catra seems to have regressed to being against the vulnerability she seemed so open to in this scene, but I’m never not dealing with some sort of cognitive distortion in a character’s head. When you’re mentally ill, you can be pro-recovery and can be making changes and strides, but you’re going to get set back, and it’s much easier at the start to get moved back to square one than say after months or years of therapy and meds. One thing that I hope people who move through this universe remember is that Catra is at the beginning right here. She’s having one of many hundreds of epiphanies you have when you are going through recovery. In Cruel Summer, we’re going to see how she’s moved forward and what she’s doing to keep herself moving forward.
I think I got the idea of the “curiosity killed the cat” motif when I was making a pinterest board for this story. See, pinterest boards DO work for inspo!
“Walk cock excuse for a human.” I stand by that ASDFHGJK

I love the line in Alessia Cara’s song “My Kind” (which was a HUGE inspo for uws, that whole album was) “I wish we could’ve told those little girls they’re gonna be okay”/ “Wish somebody would’ve told me that we'd be alright.” It just hits me so hard. So there’s a repeated element I want to carry through the universe of “If my past self could see me now, she wouldn’t be so ready to give up 24/7”
I love writing thirsty!Catra, almost as much as I love writing thirsty!Adora.

Okay, just how obvious is that I know nothing about alcohol? I grew up Mormon, and I’d drink now but I can’t because, you know, meds, so I feel like I'm always overcompensating when I write about drinking.

I really, really like working in motifs.

My, my, my, how the turn tables. Definitely a nod to Season 2 when we all lost our minds.
This moment feels very finale Best Friend Squad, which we’ll see more of in Cruel Summer.
Writing a character with a broken arm, I have to say, was strange. The cast is just one more out of a million things to keep track of in your working memory. Writing Upper West, especially as the seasons continued to drop, sometimes felt like I was balancing stacks and stacks of plates on my head, hands, and one foot while trying to whistle Beethoven.
I love that she keeps Sea Hawk’s bracelet and that she adds her “What Would Scorpia Do” to it and wears both.

I have spent hours listening to AJ and Aimee’s voices. Between the actual episodes, youtube clips, and interviews because I am so worried that my characterization is not going to transfer to readers. When AJ is playing Catra as teasing, she sometimes will go up in her register and so that’s what I was going for when she’s teasing Bow.
Also, writing PDA is hard.

Because I go hard on the angst, I have to go hard on the fluff, of course.
And the humor.

I THOUGHT HAVING THEM BE AT THE WINDOW WAS THE FUNNIEST THING IN THE UNIVERSE I’LL HAVE YOU KNOW.
Writing confident and flirty Adora is sooooooo fun, especially because I don’t think that’s really how the fandom thinks of her, but she can be like that in canon, so I like to bring her out when it’s appropriate. And because, obviously, Catra is whipped for her.

WRITING KISSES IS SO, SO, SO DIFFICULT. THREE SO’S OF DIFFICULTY. It can so easily become gross or unbelievable, but I didn’t want every single time they kissed to be the same, so then they each have to be different in some way.
Catra’s mentality of doom is a result of years of trauma and untreated mental illness. It’s branching off of learned helplessness that she and Adora both suffer from. It also sets up for the universe to be explored more beyond the end of this story.

For those who didn’t catch it, the last line of upper west side and the first are the same: “Bright Moon, ugh.” She speaks it here, instead of thinking it. That was the plan from the very beginning to have them kiss in front of the bakery and for her to say this.
Thank you SO much for sending this ask and letting me divulge all of my random thoughts about this scene. I had a blast and I hope it lives up to expectations! Thank you for reading!
You can find upper west side here, and the follow up series, she’s god and I found her, here, and keep a look out for the third series, cruel summer, coming soon!
#upper west side#she's god and i found her#upper west side: cruel summer#AGAIN SORRY IT TOOK ME SO FREAKING LONG#I hope this is what you had in mind
27 notes
·
View notes
Text
Common Sense Meets the Autism Spectrum:
| a Parental Aide for ALL |
Last month was Autism Awareness Month, and in honor of that I've whipped up a little Parental Aide to help all grown-ups understand neuro-divergence a tiny bit better. I meant to post it here during the last week of April, but I forgot because of the craziness with Finals... But since Autism and neurodivergence doesn’t just magically go away at the end of April, here’s a little skim of it now:
I've recently been chatting with a new consultation client / parent whose child has been recently diagnosed with Autism, and it got me thinking about the unfortunate nonsense surrounding the entire societal black hole of neuro-atypical / neuro-divergent presentations, especially in 'unusual' cases.
The first thing that needs to be said is IT'S A SPECTRUM, and it's honestly a comprehensive population spectrum, which means that EVERYONE IS ON IT.
Yes, say it with me: Everyone is on the Autism Spectrum.
From being perfectly, generically neuro-typical humans to rage-murder psychopaths to non-verbal, high-physical autistic kids to sociopathic con-artists. It's a SPECTRUM.
Accepting that is the first part of understanding it. And it's sometimes helpful to know in order for parents still in diagnosis shock to have something that reconnects them to their child. If you've recently received a diagnosis and you've dissociated at all, or know someone who is in that situation, knowing that the parents and the child involved are both still on the same spectrum, can help.
(It's a sense of cohesion and sameness that parents dream up for offspring, and can be problematic if over-done, which is why parents sometimes force their hobbies / goals onto children or react poorly to LGBTQ+ explorations / self-discoveries, both of which are fodder for plenty of other posts).
Once the spectrum is accepted, we can move on to understanding it better, and to diagnosing attributes of it that are affecting our lives. Knowing these attributes can help us navigate them, even in a capacity where the effect of them is not so severe that we call it a neurodivergence.
There's a stigma with mental illness, and autism is a trigger word regarding that, but it shouldn't be. We don't (as much, any more, at least) shame people who don't have clinical anxiety, but still exhibit crowd skittishness or phone distress or choice paralysis. And, honestly, mild autism frequently presents as anxiety, in our current popular understanding, as it's often limited to one or two aspects of life that provoke dramatic aversion responses where as actual, general anxiety is usually a more evenly distributed with lower-key hesitance / avoidance. Mild autism also presents as ADD / ADHD (and in my opinion the ADD / ADHD diagnosis tools are essentially boiling things down to 'not a psychopath but probably autistic, but not like the autism in in the popular imagination').
We accommodate the small symptoms of both autism and anxiety, adjust what we can and power through what we can't.
That adjustment is a lot easier when we know the triggers for the distress.
Now, the scaling systems I'm about to share are not professional, not part of the DSM, and not a tool of formal diagnosis. Consult a licensed professional before taking any big steps, but take a look at these scaling systems to help start a conversation (even if it's only with yourself). I might have another post on adjustment strategies, because these don't really address the links between presents-as-anxiety and autism, but for now, we're just gonna look at how to start asking questions and how to wrap your brain around the biggest bit of the autism concept.
Again, none of this is a diagnosis or a practical guide on how to cope, but it is helpful to be generally informed enough to start recognizing issues / asking questions about what else might be affected by a given place on a scale.
So, Autism is a spectrum, right?
Well, technically, it's multiple spectrums.
There are several sub-spectrums that layer over each other.
The crux of it, the most basic version specific to autism, is this:
Understands Emotion -- vs -- Does NOT Understand Emotion.
Now there are varied layers of that, such as 'displayed' emotion (like in facial expressions), or 'tonal' emotion (like voice tones), or even 'conceptual' emotion (as in the basic cause / nature of emotionality).
Plenty of kids understand Tonal Emotion (hearing and recognizing the difference between Mum is angry and Mum is happy), but not Conceptual (this is called being young, and usually gets grown out of as kids actually experience {and label} more emotions, the process starts at age 3 or 4, but honestly continues for most of life). Or kids may be able to hear tonal changes and interpret them accurately, but they don't read faces well (this is either a significant indicator of some sort of disconnect or, can indicate that the facial expressions they have seen shift do not shift in a way that is consistent with tonal changes {like if a parent is angry and tries to hide it with a smile}.). Some kids can track the changes in tone and expression but can connect them to a concept (such as 'fear' which doesn't develop as a concept to children until about age 5~7, even in horror-story situations, like children in warzones, only get a really nuanced concept fear a year or two earlier).
The second BIG scale to assess things on is intro- or outro-spective, and it's a 2-for1:
- misunderstand -- VS -- understands OWN emotions
-- vs --
- misunderstand -- VS -- understands OTHERS' emotions
AND misunderstands or understands the CAUSES of emotions in self / others, and why those causes and interpretations may be different for various individuals (which requires understanding the concept of there even being varied individuals, a process that ).
This is the line between "I like it, so others DO" vs "I like it, so others MIGHT", that is difficult for young children. Having a distinct sense of a separate self is actually a complicated psychology process, and it takes over a year for most infants to even recognize that they have a reflection. If understanding the self/others division stays extremely difficult passed age 7-ish, we maybe should look more closely. But at the same time, it's rarely before that 5~7 range when kids begin to understand that shopping for a birthday present for a friend involves thinking about what the friend would like, and not what the kid themselves like.
And there's still gonna be moments of grown-up fan-rage at why don't people ship my ship?, but all we might wanna do is limit time on Reddit or Tumblr when in anxiety mode.
The final BIG spectrum used in understanding these autism specific neuro-disconnects is one that revolves around concern for the disconnect:
Does not fully understand all aspects of Emotion and CARES that they don't.
-- vs --
Does not understand and does NOT CARE.
This disconnect leads to Performative Emotion, which means acting the part of emotional responses without a full understanding of all aspects of them. Sometimes this is good, as in exhibiting quiet displeasure even though I think this warrants screaming because, I don't wholly understand what I or others feel, but I do understand the appropriate / expected response. It can also be very bad, as in someone who understands the emotional response to pretend to have when a pet dies and is aware that doing so can cover that the pet was killed intentionally by said someone.
The last relevant spectrum isn't one that most people find critical, but I think it's important to delineate this one from the caring aspect. The previous note is specifically about caring in regards to the subjects understanding of emotion--and exclusively their understanding of emotion.
It is not a measure of concern for other respects of life, that spectrum is:
Sympathy -- vs -- Empathy
Now, defining terms is important here.
- Sympathy = care for how others feel
- Empathy = understanding / comprehension of how others feel
Someone who self-refers as an 'Empath' is actually expressing a high sympathy response, as in, I understand your pain so well, I feel it myself. What they mean to say, is that they understand the feeling and its causes well, and they care so much that they cause themselves to experience it.
This is also the line between Sociopaths and Psychopaths, as most people know it. The truth is a lot more nuanced, but basically, a Sociopath often lacks Sympathy, but has Empathy, where a Psychopath most often lacks both.
A Sociopath understands that they have a disconnect, cares that they do, and hides it by performing the emotive responses they are aware are appropriate (for the most part, occasionally making some exceptions due to exhaustion with the performance, or a lack of genuine care allowing for selective exploitation--making them great sales people / CEO's / business people / lawyers / writers / con-artists / Sherlockian private detectives etc).
A Psychopath either doesn't understand they have a disconnect, doesn't care that they do, or both. They rarely perform emotions and therefore often draw people in who feel trapped and in need of counter culture. They make great cult leaders, but not much else (occasionally business people, but some of them are cult leaders by a pseudonym). They truly CANNOT conform, and that can be seductive / freeing to others, but they also cannot conceive of anyone who decides to follow them ever changing their mind or not experiencing exactly the same emotions / emotive responses to stimuli as they do.
BOTH are considered extreme presentations of their respective trait.
People with both very high and very low sympathy get exhausted around others.
Because experience other's emotions or pretending to care about others' emotions is HARD. It's work and it's exhausting on both ends.
People with both very high and very low empathy get anxious in not being around others for prolonged periods.
High-Em usually worries over current states (ie, what if something happened to them or what if they hate me now), whereas Low-Em usually worries over reunions (did I forget something someone else would've remembered, birthday, holiday, or that I was gonna bring you something we discussed).
And, as always, Presentations vary. HUGELY.
But sometimes, being told you're looking at an abstract a picture of a dog, helps you spot the dog in the ink squiggles.
'Normal' isn't a fixed point, it's a range within every single subject presenting mild deviations that come together to form an average in a single person, and are then averaged again across populations.
Such data can always be understood better. And better understandings allow better accommodations to be made.
Therefore, a given person's place on any part of any one of these spectrums needs to be assessed and reassessed constantly.
Also, if you're interested in learning more / supporting Autism Advocacy, check out a few more resources, but for the love of god DO NOT give money to Autism Speaks. Take a looks at THIS and do some research of your own! ^_^
Again, this is just a vague baseline, and it doesn't address symptoms like Face Blindness (in ability to recognize people by faces) or stimming (self-stimulation or emotive overwhelm release) or even environmental sensitivity (extreme dislike / like of certain noises, colors, light levels / sources, tactile sensations). Even so, it might be informative enough to start getting a conversation started and it'll be helpful for me to refer back to this one while making other Spectrum related posts.
^_~
For more on what I’m getting up to (and for more timely updates), check me out on Patreon!
2 notes
·
View notes
Text
Okay, im gonna say something that is probably going to get misinterpreted if you never done some deep research about it. But please read it untill the end.
Have people who follow me heard about the "adhd only exists in america"?
It's basically about how ahdh is only diagnosed in very especific countries. Such as Brazil and USA for example. Said countries are the same countries where there are very especific pharmacology companies, that sell the basic compounds necessary for making adhd medicine either to other companies or to the goverment's health systems.
Besides that, in every other country in the world, that are almost no, or none at all, records of adhd recorded.
But how could that happen? If it is listed as a disease?
Well, the first ever study who identified it, was payed by the same company who started selling methylphenidate hydrochloride, as the the medicines called "concerta (transleted as fix it, so you could fix your kids behaviour by druging them)", that is the basics to make all the adhd medicine.
The doctors who released the first studies, that lead to ahdh being classified as desease, later testified that the were forced to lie about the number of pacients used and the results, that in fact, they hadn't had any valuable findings after all the years and private money spent. But they had to come up with something. So they used symptons of other known diseases that were harder to diagnose and associated with low educational ratings to give it a broader spectrum of possible symptons. Such as depressions, bypolar, people who were prived of develepmental stages and never learned how to properly focus on matters at hand, people who have brains lesions, etc. And all of this only came to light recently in the scientific community.
But suddenly, information about adhd spread about it in media, schools, internet and whenever you'd go to a doctor's office, you could probably have it, so you would get just the free sample of a miraculous medicine, that is an opioid, wich gives you tons of energy and focus, numbs part of your emotions, but also makes you an addict. Perfect sale. Also makes you feel super whenever you take, minus all the side effects.
Also, schools systems, every goverment rep and so on were kept out of it, out of the blame, so goverments founded it. Because it was kids fault they were neurodivergent and teachers fault for not noticing. So you dont have to improve schools, just send them to private doctors. Because the medicine isn't free.
Also, there is a high incidence of people near college entrance exams, or near job interviews, tests and etc buying medicine such as aderral in bulks without any prescription (in places where you need it) so they can sleep less and keep focused to study for example. Wich further consolidates the notion the "you can do it if you work hard" idea plus giving high profits to the medic companies.
But how did it get onto the dsm for example? Well, diseases manuals and what not are both based and founded by doctor's papers and doctor's groups. As long as you pay for both, you can make it happen.
For example, if you have different kinds of autism you need different kinds of assistence. But a few years ago one manual used in brazil put them all into one category cause it was cheaper when processing into the health system. That way they didnt need to pay for different facilities or personal. And the medic community approved it.
What does that mean to people diagnosed with adhd? Does it mean your life is a lie?
NO. It means you may have other neurodivegert condition, or, in some cases, no condition at all. Because people where paid to sell you medicine. And so, you have been given addictive medicine that both boosts your focus and numbs your emotions for such a big part of your life, that you became unable to cope with them without it.
What about people who were diagnosed with it? Well, in my personal experience, i now about 30 people who were misdiagnosed with adhd. Both therapists and people from other areas and social classes, neurodivergent and not, me included. We all had the same complaints/symptons, that "suddenly" disapeared after the quit the medication, went after good psychiatrists and doctors and worked on it.
Since i have been misdiagnosed i have been actively researching this and have become a psychologyst. My personal experience, my studies, people, and professors have the same opinion.
You dont need to agree if you dont want to. Just try to make sure you arent sacrificing your money, your physical and mental health over a misdiagnose.
2 notes
·
View notes
Photo
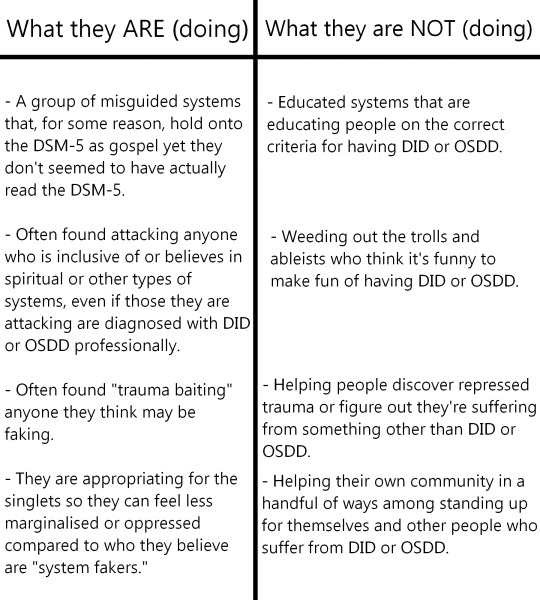
Long Post Incoming!!!
To start off, “trauma baiting,” as I would describe it, is: bullying someone to the point they admit their trauma and abuse even though they don’t want to, saying anyone is faking their trauma for any reason, bullying or harassing someone for “not having bad enough” trauma, in anyway making someone relive their trauma, or actively convincing someone they have repressed trauma that they’re unaware of (with the intentions of either proving them to be fake or proving their origins are actually traumagenic as opposed to any other origins).
As said in the last post, all gatekeepers want to do is look like their doing something helpful and productive when they aren’t doing any productive that only harms people. A fair number of Ex System Exclusionists have admitted that being in that community was harmful, draining, and negatively affected their mental health. Even though they fit the criteria that Sysmeds are looking for, it was harmful for them because they felt like they always had to be on their toes and put up a mask for anything another Sysmed might call them out on. Anything that might get them seen as fake or get them “cancelled.” Tldr; it’s a community full of hate and, just like the kin gatekeepers, they open up a perfect path for trolls and other people to sneak their way into the community. Really all a troll or anyone else has to do is put on a mask, watch what they do and say, then copy them. Though, I would say that Sysmeds are just a bit less trusting than kin gatekeepers. Also, while they like to say they’re helping others and what have you, most Sysmeds are pretty racist! They refuse to even hear of cultures that have had or still do have spiritual plurality woven into their daily lives and beliefs. Not to mention all of the religions and other similar beliefs they completely deny as truth. I personally took a course in college where spiritual plurality in other cultures and religions was a pretty big focus in that class! Their belief systems are taken very seriously and most of the cultures we touched on rarely allowed outsiders, even to study their culture to understand them better. However, these aren’t the only religions that hold such views. Possession is the biggest type of Spiritual Plurality in most first and second world countries. Something that even Christians and Catholics often believe in. It’s not usually to the extent of sharing a body with another soul for the rest of or most of your life and tends to be focused around Demon Possession, but it’s there. It’s still a popular belief.
As for not actually reading the DSM-5, well see for yourself.


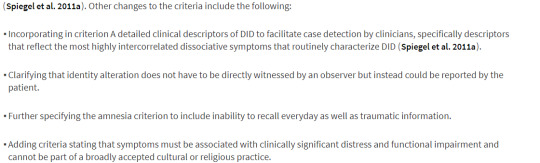


While Sysmeds like to go around claiming that trauma is needed for DID or OSDD, that isn’t actually in the criteria for either! Both are often found with people who do have trauma, but that isn’t always the case.
"In the DSM-5, the dissociative disorders are placed next to, but are not part of, the trauma- and stressor-related disorders."
“yeah osdd is just amnesia + less differentiated alters (1a) or no amnesia + more differentiated alters (1b).”
Also, I would just like to mention that this is the DSM-5; it’s the Fifth (5th) installment or update to this criterium that Psychologists, Therapists, and Psychiatrists, are supposed to use as a guide to diagnose patients. They are no where near done with research for any of these mental illnesses or disabilities to say that this is the end all be all of criteria and symptoms (even if it did say that trauma was needed for diagnosis). DID, OSDD, Schizophrenia, Depression, Anxiety, etc aren’t colds. They aren’t like cancer or diabetes or anything like that. You can’t just look at someone’s throat who has a cough or their blood or other parts of their physical body and go “yep this is what you have” with one hundred (100) percent certainty. Hell, even physical science, which is normally much easier to research, still has its flaws and misdiagnosis. Added onto that, this is only a guide for professionals when it comes down to it. Even something that seems simpler to diagnose isn’t always going to be easier to diagnose in people. Just like a cold or the flu (or, hell, most other things), not everyone exhibits all of the same symptoms.
They may one day be able to prove or disprove spiritual plurality, who knows. Only time will actually tell. Having a belief in spiritual plurality doesn’t actually harm anyone. Those that believe their plurality is directly linked to spiritual (or sometimes other) things, usually aren’t searching out any sort of therapy for their plurality. Most wouldn’t even admit to a therapist or any other professional that they are plural without some very deep trust between them. Also, just because somebody believes their plural origins to be linked to neurodivergence, spiritual things, or anything besides trauma doesn’t mean they can’t have trauma. Anyone can have trauma. It also doesn’t mean that they can’t have DID or OSDD. Just let people label themselves how they want. Just because someone labes themselves as “endogenic” (or what have you), doesn’t mean their forcing anyone else to and it doesn’t give anyone the right to attack and hate on them.
(Sources for the DSM-5: here and here. Along with the actual DSM-5. Greysdawn has a good post on all of this as well).
No matter how you slice it, exclusionists are all the same. It’s just a question of “who are they hurting?” Nixe already went into the similarities of Transmeds and Sysmeds (System Exclusionists) but let us run down the line in simple terms, shall we?
Sysmeds exclude based on people’s beliefs, a person’s identity, and whether or not they’re accepting of “outsiders.” Transmeds exclude based on people’s beliefs, a person’s identity, and whether or not they’re accepting of “outsiders.” TERFs exclude based on a person’s identity and whether or not they’re accepting of “outsiders.” SWERFs exclude based on a person’s job, their beliefs (to an extent, depending on the SWERF), and whether or not they’re accepting of “outsiders.” Kin Exclusionists or Gatekeepers exclude people based on their beliefs, identity, and whether or not they’re accepting of “outsiders.” Basically the same rings true for just about any other exclusionist group. Sure specific vocabulary changes to fit the community, but it’s all the same in the end. It’s consistently about keeping out the people who “don’t belong,” making sure the ones that do belong follow strict beliefs and guidelines or be cast out. No exceptions. These groups only care about the strict goals they have in mind.
To sign off this time, I leave you all with probably one of my biggest sayings:
Humans are diverse in everything. Looks, emotions, thoughts, beliefs, personalities, and actions. We’re meant to be diverse. That’s why we have so much control over ourselves - our own free wills. We’re not monkeys or any other animal destined to always be looking for food, mating, then dying. We have passions, hobbies, complicated thoughts, complicated feelings, and best of all; complicated relationships. Not only with each other but with society as whole, objects, our own pets, other animals, and with ourselves sometimes. We decide our own morals, our own beliefs, our own ways of living life. It’s probably the best thing about being human. You never know what’s going to happen or how you’ll conquer the hardships. We plan ahead, but all we really know is the destination and not what’ll happen there.
#tom#tom speaks#alucard#alucard speaks#host#host speaks#cruxen#cruxen speaks#syscourse#syscourse informational post#sysmeds cry me a river challenge
27 notes
·
View notes
Text
Director’s Cut 1: Andrew ‘Pope’ Cody

“I find it difficult to find any redeeming qualities in this character. He is a person with spot on DSM antisocial personality disorder, with sociopathic traits and without the charming facade. But the mental health professional in me also sees him as neurodiverse, on the spectrum. At any rate, I can’t find any allure or menacing sexuality in him. How did you find redeeming qualities within Pope? And how the heck did you come up with a female OC who can interpret his cues and find warmth and attraction from him? I enjoy your fics about him, others I’ve read have basically torture porn.”
Wow, okay, Andrew. You’ve picked a really interesting one here. So, lets start with some background... Which I will try to condense as much as possible.
Also, for ease of talking, I’m going to give our Reader back her OC name and therefore when I refer to ‘Elaiyna’ that’s your reader character! 😁 Background I was never meant to write for Andrew Cody from the movie. My first watch of the movie left me cold and, to be honest I still find it very difficult to watch even now. (The movie is great for sure, but it’s not one I rewatch often.) Without a long explanation as to ‘why’, I watched the movie so that I could watch the US TV show version of Animal Kingdom. Which I highly recommend!
Where as Movie!Andrew I couldn’t get into at all, Show!Andrew I fell in love with. It took me one episode to come up with my OC and a decent story line. Although I never actually wrote it out I had many plot points saved on a document for how Andrew/Elaiyna’s relationship would play out. So really, you have Shawn Hatosy to thank-!
Who, super side note, deserves an Emmy for this. And also can someone please get him and Ben in an interview to talk about Andrew - I will beg!

When I decided to start writing and posting for Andrew here (considering I had the plot points and we were taking the Mendos as far as we could) - I essentially wrote a mix of Show!Andrew and Movie!Andrew. Honestly tipped in favour of the show. But very recently I’ve tried to write much more for Movie!Andrew as I’m 99.9% sure that’s who everyone reading my work is reading for anyway!
How did you find redeeming qualities within Pope?
The only real answer is Show!Andrew. I love him so much, and they explore a lot with his character - as they of course have time to, that a 1hr30 movie doesn’t - so it’s very easy to find redeeming qualities in a character that’s at a very different stage to his movie counterpart (and yet is still the same character and recognisable as the same character... Show!Andrew is the build up to the man we get in the movie, if you will.). Show!Andrew has that same... creepy/awkward vibe, but also has a lot of sweet, decent human being moments that give you his more redeeming qualities (without spoiling anything major his relationship with Lena, Baz’s daughter, is a good example).
But also I view Andrew in the movie very differently to the way that I believe most people do. Movie Andrew doesn’t scare me. Sure, he does scary things, but to me he just comes across as very awkward. Like, he knows what a situation calls for and kinda adapts to that - or he says things because he’s like “That’s what people say in this situation right?” at least that’s how I interpret him. No matter how incorrect that is. Like there’s no social queues in his character, he doesn’t really fit into those kinds of situations (or function well!) but he observes everything. So he knows that “If X happens, say/do Y. Because that’s what people do.” regardless of his own “feelings” etc. I don’t think he has emotional intelligence and there’s a definite disconnect between think and feel and... I guess instinct? That ‘primal brain’ thing.
I mean I know it’s interpretation but that scene where he carries Nicky to bed and then like strokes her hair back and then tells Jay “She’s beautiful.” Doesn’t give me any other vibe other than Andrew having observed this and his brain going ‘Oh, yeah, Andrew - then compliment her to her boyfriend. That’s a thing people do.’ Just the way my brain works I guess.
The obvious follow up question would be “Okay, so you love him in the show. But you write for him in the movie. So... you gotta have something redeeming there right? Now you’re leaving Show!Andrew on a shelf? Correct - I kinda feel like Andrew has at least some ‘relationships’ to which he actually feels something. Which is why I’m reluctant to place the “Psychopath” tag on him. Look at his relationship with Baz for instance (honestly, that supermarket scene is my very favourite.) - I just get this “friends” vibe. Like real friends, maybe even best friends. Andrew cares enough about him to want vengeance (I’m not down for thinking this is just him wanting to be a criminal I genuinely think this is a reaction to losing his best friend - and arguably his stability.) And I mean, he cares about his family. Even if not in the traditional ‘sense’ of caring.
I also want to give a quick shout out to @mandy23b - as Andrew is her favourite, and conversations with her on how she views him really help me shape Andrew in my head. For example she has a lot of headcanons about how he grew up (eg: potential physical abuse) that I am happy to adopt. So, my own personal headcanons / adopted head canons about him also help to make him redeemable.
And how the heck did you come up with a female OC who can interpret his cues and find warmth and attraction from him?
Oh my gosh, Elaiyna. Okay, well aside from again her starting with Show!Andrew and me basically lifting their entire relationship and giving it to Movie!Andrew there’s a lot about her that I guess ‘prepares’ her for him.
First - they meet because the Cody’s case her car (...Ready For It?), assume she has a lot of money and try to rob her. She knows who he is before they form a relationship - the barrier of “oh by the way I’m a career criminal” is broken instantly. Second - Although she’s an only child her parents have fostered a lot of children over the years (More details in ‘Flaws’) and so she’s used to a lot of siblings and the bonds between siblings. Added to this it’s not hard to imagine that some of these foster children might have had neurodivergancies of their own and therefore she’s also used to people that act like Andrew does. Third - David ( ‘Flaws’ and ‘Last Habit’) her eldest foster sibling is a Police officer, and they have a close relationship. Figure she could learn a lot from him. Both on crime/criminals and then maybe neurodivergant criminals too. He’s bound to have at least some stories that might help her. Fourth - Not to make some kind of robot comparison for our Boi here but, she works in IT. She’s the CIO for her firm. Draw your own conclusions on relationships with something/one with basically zero emotional output.
I find your comments on other fics you’ve read very interesting. Because to me Andrew just isn’t sexual. (I might be in the minority, because other fic writers I’ve talked to tend to put him in ‘physical only’ / highly sexually charged relationships) He’s never read that way to me. ‘4 In the Morning’ is the first time I’ve thought to write something that is sexy for him. Although I have alluded to sexual elements of their relationship in other fics. Their relationship to me has always been on a quiet understanding level. He observes and learns about her and is fairly quiet about it. Elaiyna is more extroverted, but also observes and learns about him very quickly. So instead of PDA and verbal “I love you’s” they have this non-verbal communication that isn’t always physical either. Although touch sometimes plays into it. Because that just the kind of relationship that I see him in - sex is rare, and when it happens it’s not because of this big “I love you” romantic build up - it’s spontaneous. That part of his primal brain is kicked in and it’s like “Okay. We’re doing this now.” For his character I understand the “draw” to write something like that (even though, like I say, I don’t see him being interested.) but I’m just very much a romantic... 😅 So I want to write something Romantic even for a Mendo who you wouldn’t necessarily fit into a romantic role. Their story still has “romantic” tenancies. Like it’s a loving relationship it’s just a different kind of love. I don’t feel like he would necessarily know that he loves her, or even comprehend what ‘love’ is. But he knows he feels something for her that’s very different to how he feels about other people. Which is why when Elaiyna does say ‘I love you’ it’s not reciprocated with words - and rarely with actions. She knows he loves her, even if he doesn’t know it. Their relationship is very ‘quiet’ but she knows that’s just how he is - and he will show “affection” as he deems fit and appropriate to show it. Even if - again - it’s not a “typical” way of showing it. And when he wants affection himself it’s more, “I am hugging you now on MY terms. But in 5 seconds I will walk away as if nothing happened.” He is more often enough the one to initiate anything PDA and Elaiyna will wait for him to come to her. If her read on him is *just* right then she’ll initiate, but then there’s the consequences of getting it wrong and Andrew pushing her away... I definitely base a lot of the beginning of their relationship on them just finding each other fascinating. He’s completely different to any other man she’s ever met, and he’s never met someone so interested in him that doesn’t try to change him and/or however he treats her is met more with understanding than conflict.
I say I love all my OCs, of course I do. But Elaiyna is one I really had to think about building because of Andrew’s own personality. It had to make sense for her to be with someone like him - their relationship had to make sense and keep him (mostly) in character. So she needed to be able to interpret his cues, as you so nicely put it 😊 But I think I gave her the right tools to do this, and, with Show!Andrew she got the right base to jump from.
I know this is super long, but I hope it helps in your understanding of how I’ve built Andrew’s relationship with his S/O! 🙏 And more importantly answers the questions you have!
---
Thank you SO much for asking! If anyone else wants a Fanfic directors cut for any of my fics please ask! I would love to answer any questions! 🥰😘
#Andrew Cody#Andrew Pope Cody#Pope Cody#Animal Kingdom#Long Post#HOLY SHIIIIT L O N G post#Ask me more questions guys please!!!#I mean you're gonna get some super in depth Answers!#(Ralph Anderson to come!)
17 notes
·
View notes
Note
Hey, I’ve been reading a lot of your BNHA metas, (they’re all absolutely awesome btw) and I was wondering about two things, what kind of mental illness do you think Shigaraki has? And I read a post somewhere that speculated that he might have suffered a tbi when his father hit him with the tree sheers, do you think that might be true?
Hello anon, thank you for your ask!
I will try to answer your questions the best I can, however beforehand I think it’s important to note that I don’t really like diagnosing characters outside of like specific examples where the authors tell us this is the disease they were attempting to portray, or headcanons. Shigaraki clearly shows signs of mental illness, but I don’t think Horikoshi writes characters by looking up a list of symptoms in the DSM and then writing them based on that.
Also yes, the two clearest examples of mental Illness (Shigaraki, Twice) are both villains but I have faith that the mental illness of Shigaraki is an instance where it’s used to humanize him and show how much of a victim of a system both characters are, rather than just to give the villain traits that are abnormal and therefore creepy and dangerous.
I can’t give you a specific dianogisis but I can give you a more in depth look at several symptoms that Shigaraki displays.
Excoriation

Excoriation disorder is an obsessive-compulsive spectrum mental disorder that is characterized by the repeated urge or impulse to pick at one’s own skin to the extent that either psychological or physical damage is caused. In Shigaraki’s case it’s clearly a stress response that is aggravated the more violent, unstable or dangerous a situation he is put into.

Which is why I find claims that Shigaraki is content with violence, or likes being a killer and is comfortable living this way to be false. Because Shigaraki’s own body constantly rejects him. He feels a compuslive need to scratch and harm himself because his body cannot handle the stress of being violent. It’s a stress response because Shigaraki does not actually on some level want to be doing these things, and living in a constant state of stress and harm makes him more compelled to vent his stress by following his compulsions.
The compulsion he feels can sometimes get so bad that in childhood he was rolling around the floor, crying and frantically scratching his whole body. This is not what All for One said and him holding back his urge to kill, but rather Shigaraki responding to the stress. Shigaraki is seven and was put in front of two homeless people who were threatening to harm him and he already came from a physically abusive household. He’s in unbelievable stress with no healthy way of venting it, and thereofre he compulsively self harms.
GAME TALK

In general Shigaraki uses a lot of game talk. This is not so much a symptom of mental illness necessarily as it is a coping mechanism, but the goal is for Shigaraki to distance himself from reality. Basically it’s a mechanism for rgaining control because if you imagine life as just one big game where you are the player, you feel much more in control then some random kid who lost his family in a freak accident then got picked up by a super villain. Gamespeak is also a way of being deeply impersonal with the situation, in case it goes bad Shigaraki can say it’s just game over. It’s a layer of distance between him and reality, like I said, escapism to cope. His insistence of using game terminology for everything could also be seen as a “special interest” but once again that depends on your intepretation Shigaraki shows a whole cluster of symptoms that overlap with a lot of things.
HIGH ATTENTION TO DETAIL
Shigaraki in a fight where he and AIzawa are jumping around trying to kill each other, Shigaraki is able to notice a detail as minute as when the hair falls over Aizawa’s eyes it stops, and also that his quirk was weakening because the tiny seconds long windows were getting shorter and shorter.
This is an extremely small detail to notice. Hyper-sensitizing, or hyper-attention to detail is another sign of mental illness, because usually the brain filters out superfluous details like this because otherwise noticing everything in that fine detail would overwhelm the senses.
Immaturity


Shigaraki is completely unable to handle his negative emotions like a well-rounded adult. Though, I dislike how All Might and the others phrase it in this discussion because it is a pretty ablist description (downright sick in the head, a toddler’s sense of feeling like he can do whatever he wants). (the ablist part is that they’re using symptoms of his clear mental illness to dehumanize him.)
Regardless, Shigaraki of course does act like a man child, constantly talking about games, giving up easily, not having the patience to converse with others especially in situations he does not want to be in, throwing tantrums.
Children who are abused and neglected especially to the extreme extent that Shigaraki has, show long term developmental (that is term for the process of growing into a full adult) and behavioral problems. To the point where some studies have shown even the brain’s chemistry is permanently effected and the brain grows differently.
Children need a stable environment, and also positive role models for what adults act like to grow into full fledged adults, Shigaraki had neither of those. In fact he was also raised almost entirely outside of society except for the first five years of his life, so there is also no outside influence on his upbringing as well, which is why he is like a child, egocentric, unable to handle his emotions, because mentally he was never given the chance to develop past one.
ISOLATION

This is something that Shigaraki showed at the start of the series, but also has shown to develop past. At first he never left his room and from the several trash bags it’s quite obvious he spent long periods of time in there without taking care of himself or the environment around him in any significant way.
Shigaraki is no longer isolating as a result of having gotten closer to the league, he is basically available to them at all times and does not shut them off in any significant way. Which in this quick tangent we can also talk about symptoms Shigaraki does not have. Shigaraki is able to read a room pretty clearly, and knows how to hide himself in a crowd enough to keep Deku hostage with no trouble at all, and even leave the scene with Uraraka there without provoking her into attacking him or tipping her off what he was doing right away. Shigaraki is fairly competent at reading other people and he does have social skills so he’s not like someone who never sees the light of day or cannot interact with others and is clueless on how people think.

He’s also shown to be capable of making emotional connections with other people, and also of being considerate to those people’s needs. Which also shows that Shigaraki is capable of communication and also has an awareness of the feelings of other people and the ability to empathize, he is just choosy about who he makes connections with. He is definitely not someone unable to form an emotional connection with another person.

Shigaraki also shows a pretty flagrant disregard for all social norms, but that can be a result of being raised outside of society all of his life.

Shigaraki also likes to piss people off on purpose, almost like he is testing their boundaries and what he can get away with the same way a child playing around might.
Dissociation

We have seen Shigaraki experience Dissociation in both senses of the word. First we have seen him physically detach himself from his feelings, and his own body in the middle of a fight and still continue on in a fugue-like state.

He experiences dissociation in the sense of the word meaning periods of detachment to your body, drifting away from your consciousness, severe feelings of alienation from himself, extreme difficulty concentrating or holding focus to the moment, his perception of both time and the area around him slipping to levels that are borderline hallucinogenic.
Dissociation is a mental process where a person disconnects from their thoughts, feelings, memories or sense of identity.
Shigaraki also displays traits of what is more classicly known as Dissasociative identity disord. He has two names, and clearly considers the life of Shimura Tenko to be separate from Shigaraki Tomura for a long time at the start of the manga. It might not be full on DID, but he at least dissociated his memories away from himself long enough that he forgot all of them like those memories belonged to another person, not Shigaraki but rather Tenko.

Shigaraki also foils Twice pretty heavily who developed actual dissociatve identity disord. He even shares similiar symptoms of speaking to himself when he speaks to the hand of “father��. I am not saying he has full on DID like I said I’m not diagnoising just that he displays several symptoms of it. He also came from an abusive household at an incredibly young age, which is where DID most commonly manifests.
Shigaraki also shows signs of flashbacks when his memories return at inconvenient times during fights when direclty exposed to violence, or he experiences a trigger reminding him of his past. Flashbacks are a symptom that have the most in common with Post Traumatic Stress Disorder.
To answer your question on whether Shigaraki has a brain injury from when his father hit him with shears, there is evnidence suggesting he could have suffered brain damage, especially in the symptoms that he shares with Twice. However, at the same time Shigaraki also would have developed brain damage either way. Post Traumatic Stress Disorder is something that permanently rewires the brain after exposure to trauma. His brain has suffered a traumatic injury regardless of whether or not it was the garden sheers that did him in.

Suicidal Ideation / Self Harm
Shigaraki in general wishes to not exist, or to destroy everything so it will not exist anymore. Even if it’s not a direct wish for suicide that symptom is called suicidal ideation. It’s intrusive and persistent thoughts of suicide. The likely cause is once again, Shigaraki is absolutely not comfortable living like this, and is constantly overwhelmed with stress and pain and is seeking an escape.

Shigaraki also actively seeks out harm. The same way he obsessively compulsively scratches, he puts himself into harmful situations like the extremely painful hellish surgery the doctor said he did not even have to endure if he did not want to. He feels compelled to harm himself, even when he is not fighting against someone else. He inflicts harm on himself becauseit is once again an unhealthy way to process his emotions. Oncce again all of these symptoms are there not to make Shigaraki out to be terrifying and incomprehensible because he is mentally ill, but rather to show he is a human being caught within the cycle of abuse with extremely unhealthy methods of coping with that fact.
#Anonymous#metasks#shigaraki tomura#mha meta#shigaraki meta#my hero academia#shimura tenko#tomura shigaraki
258 notes
·
View notes