#i have a couple of chronic issues which could be causing these symptoms but i think me not being able to maintain relationships irl
Text
tfw you read a really sad story which actually happened and you understand every single decision of the person writing it. I can literally picture me living their life. some of the details they mention are so accurate that it's downright scary lol
#i usually don't talk about very personal stuff on here#but for a long time now I've been feeling lonely#the ppl i used to be close with irl have moved away and while we do keep in touch#usually I'm the one who reaches out#and while i get they're busy i feel like I'm the one keeping those relationships going#my colleagues don't know I'm not very social#i guess they know I'm not a social butterfly but they don't know how lonely i really am#and being lonely hurts#it also seems to zap my energy and motivation to do things#when I'm at work there is so much i want to do once i get home#but then i just can't seem to muster the energy to actually do them#i also find it hard to care about things#i have a couple of chronic issues which could be causing these symptoms but i think me not being able to maintain relationships irl#isn't exactly helping#either#i know loneliness kills#literally#if you're aiming for a long life having good relationships is more important than quitting smoking or giving up alcohol#statistically speaking#about me
0 notes
Text
Health Update
First, I want to say thank you to everyone who reached out or commented on the latest installment of Where's Mommy? to wish me good health. I am so grateful for all of you 💚
However, the health issue I'm currently dealing with isn't due to a virus or bacteria, and there's a possibility it won't get better.
A little history.
Back in 2022, there was a two week period where I felt like my blood sugar was dropping, and I was very symptomatic. There was a moment where I slumped down a wall at work because of it, and they had to dump sugar packets from the break room into my mouth to rouse me. It was a very scary time.
After those two weeks, I went to my Primary Care Physician who ordered blood tests and had me purchase a glucometer to test my blood sugar several times a day. However, during the two weeks she had me do this, I never got a reading below 70, and the same symptoms did not develop as they did prior. My blood work came back clean, and without a reading lower than 70, my PCP dismissed it and told me I was having anxiety attacks, lol. She told me to come back if the symptoms came back, and they never did.
Backing up a couple more years.
Without revealing too much of my medical history, I have a chronic illness called POTS (postural orthostatic tachycardia syndrome). It's a dysautonomia or a dysfunction of the autonomic nervous system, the system that controls all of the automatic functions of the body. It was caused by my battle with Lyme Disease in 2010 and is currently incurable. I was diagnosed with POTS in 2018, after being told for 6 years that I had anxiety, lol.
POTS is not a very well-known illness, but it's getting more attention these days. It garners a host of different symptoms, including tachycardia, chronic fatigue, brain fog, orthostatic intolerance, migraines, gut issues, syncope, dehydration, blood pooling, etc. Everyone's POTS presents differently, and most people with a POTS diagnosis live on disability. I made the choice not to.
Fast forward to 2024.
Fast forward again to this past Wednesday.
Well, I finally was able to get a POTS specialist in my state this year. A huge win! When I had my initial consultation, I had mentioned the low blood sugar episodes in 2022 and asked if it could be related to POTS. The doctor told me that they don't see POTS patients having low blood sugar issues, but we're concerned enough to refer me to an endocrinologist. Another big win!
I had my consultation with the endocrinologist, and he ordered more blood tests, some of the same tests as before, and some different (y'all, they took like 20 vials from me). He also gave me a CGM (continuous glucose monitor) to wear for 14 days so they can track my highs and lows to see if they can catch anything.
Well, the next night, my blood sugar dropped below 70, 20 times, and 55, 9 times. Which means I was woken up 9 times throughout the night. I got only about 2 hours of sleep, and still had to go to work the next morning. But, once again, it went back up by itself without any intervention from me.
Y'all, it caught A LOT in just the first day, actually night. My blood sugar dropped below 70, 11 times, and below 55, 4 times while I was sleeping. Now, because anything below 55 is considered critical and could be fatal, there is an alarm that cannot be overridden and will sound. It sounds like a smoke alarm. So, I was awoken 4 times.
The odd thing is that my blood sugar dropped, then went back up on its own. I didn't eat or drink anything. Blood sugar doesn't really do that, so I thought it was odd. This also begs the question: If I'm asymptomatic at 53, then what level was I at in 2022 when I had symptoms? Honestly, I don't want to know.
Here is a nifty graph!

All of the red is considered low blood sugar, below 70, and anything close to that 50 line is considered critical low blood sugar. And again, I did not eat anything during the night.
There are four major anomalies with my low blood sugar occurences:
Most cases of hypoglycemia are seen in diabetics, I am not diabetic
Most cases of hypoglycemia seen in non-diabetics are sporadic, mine are consistent
Hypoglycemia is normally corrected by consuming sugar, mine auto-corrects
When blood sugar drops, it creates symptoms, I do not get symptoms
There are only a handful of things that can cause hypoglycemia in a non-diabetic and even less consistently at night time. The doctor has already ruled out insulinoma (insulin producing tumors in the pancreas), so that leaves even less, and also the good old "we don't know what's wrong with you".
I'm not going to lie. This whole thing terrifies me. There's no telling how long my blood sugar has been doing this, and it only takes one dip below 50 for me to slip into a coma and die in my sleep. Luckily, my blood sugar does this crazy autocorrect thing, and I haven't died yet! Humor makes this easier.
Right now, I'm emotionally, mentally, and physically exhausted. Adding this on top of my already difficult life with POTS has been hard to cope with, and I'm crying a lot.
Hopefully, I'll get results soon, and my endocrinologist can figure out why this is happening and how to manage/fix it if it can be managed/fixed. Maybe I've got a completely new illness, and you'll find me in a medical journal! Wouldn't that be something.
Anyway, thanks for the continued support. I have a lot of IRL support from friends and family, but while I go through this process, I may seem distant, my posting might be sporadic, I may not keep my fic posting schedule, etc. And when I have an update, I promise to let y'all know!
Much love 💚💚💚
Steph
54 notes
·
View notes
Text
JJ Maybank character analysis
How parentification shaped JJ's personality
Part 2
Victim role, low self-esteem and compulsive caregiving
Especially in the first season of Outer Banks there are moments where JJ is not fully respected by his friends, the Pogues, and he often accepts this dismissive treatment. For instance, his ideas are frequently brushed off, and he is called names like "dumbass," reinforcing his belief that he is not valued or taken seriously. JJ tolerates this treatment, likely due to his low self-esteem and his desperate need to maintain these relationships, as flawed as they may be.
Additionally, JJ voluntarily gets himself into situations where he simply can't win, exemplifying his compulsive caregiving and martyr complex. For example, he confronts a group of Kooks alone to defend his friends, even though he knows he is outnumbered and likely to lose the fight. This behavior underscores his willingness to sacrifice himself for the sake of others, even when it is detrimental to his own well-being. He also constantly highlights how the Kooks have the advantage, which, while often true, also shows how he puts himself in the victim role more than the other Pogues.
JJ's low self-esteem is most poignantly visible in his interactions with Kiara in Season 3 Episode 4.
youtube
JJ feels uncomfortable when Kiara is getting close to him
When Kiara confesses her love for him, JJ's immediate reaction is to dismiss it. Kiara tries to confront him again, reminding him of an affectionate moment on the boat where they almost kissed. But JJ shrugs her off, recollecting the moment as "just weird", later admitting that he has issues getting close to someone.
Considering that JJ probably had a lifelong experience with parentification, it has caused him to prioritize others' needs over his own, leading to poorly developed emotional boundaries and a lack of understanding of his own desires. Coupled with his low self-esteem from his abusive upbringing, JJ struggles to believe he deserves love and affection. So when faced with Kiara's romantic interest, he feels confused and uncomfortable, questioning his worthiness and feeling that someone as stable as Kiara couldn't genuinely want to be with him.
Another point is that the potential relationship with Kiara represents a significant change and requires vulnerability, which JJ finds unsettling due to his need to always be strong and in control. This internal conflict makes the near-kiss feel strange and out of place for him. When admitting to his feeling of unworthiness, describing it as "not even having a home or parents" Kiara offers him help, which he refuses, illustrating once again his difficulty in accepting care from others.
JJ's low self-esteem and compulsive caregiving are deeply rooted in his responsibility thrust upon him from a young age and the lack of nurturing from his father which led JJ to develop a skewed sense of self-worth, believing that his value lies in what he can do for others rather than who he is. However, this can also expose JJ to extreme stress and anxiety. This is notably seen when JJ and John B. encounter smugglers threatening Miss Lana at her house in Season 1, Episode 2.
youtube
JJ's decision not to help Miss Lana once the smugglers are gone can be attributed to a combination of emotional overload, psychological exhaustion, and his complex relationship with trust and authority.
Contrary to his usual impulsive and confrontational nature, JJ experiences an anxiety attack, urging John B. to leave rather than confront the danger. This reaction can be interpreted as a symptom of his chronic stress and trauma of having experienced his abusive father. The sound of someone being beaten and threatened might evoke a generalized trauma response, leading to anxiety and a desire to escape the situation. This reaction could be seen as a form of PTSD, where certain triggers cause an overwhelming urge to flee rather than fight.
******I am sorry. This time I had to hurry and I wanted to get this done before going on holiday tomorrow. Thanks you so much your support, for reposting and giving me thumbs up!!! I find JJ to be a very interesting character with surprisingly much depth for a series like Outer Banks, probably because he is portrayed most relatable and realistic. If you have any other suggestions and ideas on what to do next, let me know.******
#jj obx#jj outer banks#jj maybank#character analysis#outer banks#parentification#low self confidence#low self worth#low self image#compulsive behavior#caregiving#victim mindset#emotional boundaries#emotional abuse#anxiety attack#obx s1#obx s2#obx s3#kiara carrera#jj x kiara#kiara obx#relationship#ptsd#trauma response#friendship dynamics#emotional exhaustion#emotional overload#self worth#confrontation#sacrifice
18 notes
·
View notes
Note
hiii!! i was wondering if u have any advice on getting taken seriously and getting care in an emergency department as a chronically ill/disabled person?
i've had progressive muscle weakness, fatigue, nerve issues, and pain for like five years that hasn't been properly diagnosed (been told it was fibro but. doesn't seem to fully fit that anymore. idk if anything will show up on tests but even if it doesn't i feel like the more correct diagnosis would be ME. my current gp thinks i have [seronegative] myasthenia gravis but gps can't order emgs so can't diagnose it), and recently have been having trouble breathing that seems like it's due to muscle weakness in my chest and follows the same patterns as my other muscle weakness.
my gp can't do anything to help (and referrals always get declined because the system is overwhelmed) and can only advise that i go to the hospital, been to one hospital who sent me home because my oxygen saturation was fine (even though from what i've read shortness of breath caused by muscle weakness doesn't show in oxygen saturation til it's Very Very bad, at the time i could only speak a couple syllables per breath and my peak flow was around half of what it usually is), i asked my gp what to do and he told me to try the further away hospital and explain that i haven't been able to get care at the closer one.
my mum is going to take me in a couple days (unless i really can't breath in the mean time obviously) and i'm nervous because i usually get dismissed, or they'll do a couple tests but not the ones that would actually show the conditions that i might actually have. i don't know how to advocate for myself without getting seen as overreacting, or get care for a chronic condition that has become urgent because usually if it's been happening for a while they'll say to just talk to ur gp but. my gp can't do anything.
(note: i know ur only supposed to go to the emergency room for things that are really urgent and the fact that i'm waiting a couple days might make it not urgent. my gp has said this is the best thing i can do though because there's literally no other avenue for me to get care and with my breathing the way it is i am even more restricted in what i can do than i have been before.)
oh god, i’m so sorry you’re in this position and am sending so much love to you. obligatory disclaimer that i’m not a medical professional, just Some Guy with a couple degrees, a girlfriend in medical school, and a whole lot of medical trauma.
that being said, my only advice is to lie. lie your ass off, lie like your life depends on it, most importantly lie in an informed fashion - which is easy in this case because you pretty much know what you have, you just need them to do the test you want. the doctor thinks they’re creating a clinical picture on a blank canvas and you need to give them a paint-by-numbers.
here are the factors i would consider and the narrative i would construct if i was in your position, but it’s your body, your experiences, and your care (or lack thereof), so all of this is just my opinion and your mileage absolutely may vary:
most importantly, make sure anyone with you in the ER is on the same page. a lot of doctors assume patients are lying by default because they suck, so if somebody contradicts you, you’re probably screwed. when my gf takes me to a doctor’s appointment, we have a “what are we lying to them about” meeting ahead of time. you know your mum best, so you probably know what approaches she would/wouldn’t be on board with, but i’d initiate that conversation like “i’m concerned this hospital might dismiss me like the other one did, so i’m planning to say XYZ to hopefully get them to take me more seriously” and not “Some Guy on tumblr told me to lie my ass off” lol
next, make your symptoms match the textbook. downside to this, i definitely recommend not bringing up ME/CFS because they can’t/won’t test for or treat it (i have a friend in the UK who almost certainly has ME/CFS and just got sent to even more physical therapy). here’s where it helps that your GP is pretty sure they know what you’ve got (whether you actually have that or not): research myasthenia gravis (i recommend continuing education sites geared towards clinicians), know what’s on that list, and (with some exceptions) say you have those symptoms. my personal strategy is three-tiered:
lies of creation: unless it’s something immediately life-threatening or something they can concretely disprove, say you have symptoms of your disease even if you don’t. ER doctors don’t give a shit if they can say you need to wait it out and go to a specialist, regardless of that being unrealistic and your symptoms being unlivable, so you need something urgent and serious. (my gf says “they might be worried if you’re having trouble swallowing. maybe.”) myasthenia gravis typically waxes and wanes, so even if you’re able to do something when they examine you, it would be totally realistic for you to not have been able to a couple of hours ago (eg, when you arrived to the ER). for example, i told the NHS i totally had a positive MRI in the US that i was having delays getting access to the records of, even though my MRI didn’t show a speck of inflammation, because at least that got me a couple months of flare medication while they confirmed and an NSAID when they decided i was in remission rather than literally nothing. obviously you can’t tell them you’re seropositive because they’ve unfortunately got that record, which means you’re already fighting an uphill battle, which leads to my favorite sub-category lie of creation: anything you’ve read or believe or know that works in your favor, your GP told you. memorize what percent of people with myasthenia gravis are seronegative - don’t lead with that, because doctors hate when people are educated about our conditions or know what’s wrong with us, but if they say “we won’t do an EMG because you can’t have myasthenia gravis because of your bloodwork,” then you can be like, “my GP said that’s pretty common, like, about X% of people don’t show up on the test, and they’re really convinced i have this.”
lies of exaggeration: increase frequency of symptoms, impact on your activities of daily living, rank on a scale. familiarize yourself with what the numbers on the pain scale generally mean in terms of ability, and elaborate - “my pain is at an 8, it’s really hard to XYZ.”
lies of omission: this ER doctor was an asshole and still would’ve fucked me over regardless, but the instant i said “yes” when he asked if i experienced acid reflux, he stopped listening to a single word i said. i was experiencing acid reflux, and i knew that symptom happened with IBD, celiac, and a host of other serious conditions, but he instantly decided that was all that was going on with me, tried to send me home with just an antacid during the worst pain of my life, and led to me experiencing malnutrition and all my hair falling out due to the severe delays in accessing care. my recommendation for “instant dismissal” (or worse, “instant institutionalization”) symptoms to omit are: acid reflux; menstrual cramps or really anything related to menstruation; anything they could dismiss as covid - if they try to dismiss your breathing issues as covid, say you’ve tested negative this week even if you haven’t had a test. if you’ve had covid and you’re certain it’s not in your chart (assume it’s in your chart if you’ve ever said it to a doctor), say you’ve never had covid. if they still try to say it’s covid, stress that this has been going on for years before covid; anything psychiatric.
so, what i would do:
“i have X, Y, and Z symptoms. my GP thinks i have myasthenia gravis and is working on referring me, and said to go to A&E if A, B, or C got worse. A, B, and C have [measurably gotten significantly worse since the last time you went to A&E] - i’m having trouble breathing, swallowing, and [other].” hope that they decide to do an EMG on their own.
if they try to send you home or try to do useless tests, say “my GP mentioned that i really need an EMG in order to get the treatment that would help me be able to breathe, swallow, [other]. will this test also do that?” (one of the instances where you strategically ‘play dumb’ because doctors hate when we know things)
if they still won’t do anything helpful, either you or your mum say: “i’ve/they’ve had these symptoms for five years and it’s never been remotely this bad. i/they seriously can’t breathe, swallow, [other] - how do we manage these symptoms before we can get to a specialist?” i’m white and, having been super professional/polite until then, this is the point where i start crying; you know your circumstances best and whether that will incur racism, etc, upon you from the medical system.
if they still want to send you home, i (again, being white) would at that point firmly request a second opinion. they still might send you home with nothing; i did all of this shit and received 50 pills of 50mg tramadol in addition to the antacid, and probably an angry note in my file, and not a millisecond of further testing.
i say this with love and from experience, in the interest of minimizing trauma and devastation: you need, to the best of your ability, to go to the emergency department with the expectation of receiving no care. i recommend a buddy, a reminder, and a reward: message a bitter crip or someone else who Gets It throughout the process and have support in place for if/when you get home with new medical neglect and trauma; remind yourself that your symptoms are real and serious and, in my gf’s words, “if your GP thinks you have myasthenia gravis, you almost definitely have something neuromuscular going on.” i like to make posters of my reminders (example here: link); do something that will make you feel better afterwards - my go-to is buying a new stuffed animal after experiencing medical trauma. i have a lot of them lol
for more advice on coping with medical neglect before and after appointments/visits, see my post here (link). if you don’t know anyone who’ll understand or be available and helpful to support you during your trip to A&E, feel free to dm me and i’d be happy to give you my WhatsApp. i wish you so much luck and you’ll be in my thoughts, i really hope it goes as well as possible - you deserve quality, compassionate, thorough care. if you’re comfortable with doing so and feeling up for it i’d really value an update afterwards 💓💓💓
88 notes
·
View notes
Text
Kaplan-Myrth: COVID is back, so let's take care of ourselves and others - Published Aug 1, 2024
The numbers are up, and when September rolls around, we will be vulnerable again. Let's not be complacent about protection.
Two weeks ago, I tested positive for COVID-19. Last week, I cancelled patients in my medical clinic because I was too sick to work.
For anyone who is counting, that is my fourth infection. Never from work — even when I see patients who are COVID-19 positive — because I require masks at all times in clinic to keep staff and patients safe. This infection was from an extended family gathering at which we let down our guard.
Article content
“A couple at the party tested positive for COVID-19,” my uncle informed me the day after his 70th birthday party. Although I spent most of the time outside on a patio, I ventured inside a few times to see relatives who were more comfortable in the air-conditioning, as did my husband and children, and we forgot to mask. What was meant to be a happy reunion was sullied by each of us, one by one, testing positive.
It is summer 2024, and we are inundated again with sick patients as COVID-19 levels surge across Canada.
We are all sick and tired of COVID-19. I do not want to hear that a patient goes into hospital for surgery and gets COVID-19 pneumonia, or that children or seniors are coughing to the point that they vomit. For some people the symptoms seem milder, but we know that the effects of COVID are cumulative and unpredictable, that it can cause damage to the heart, lungs, brain, vascular and endocrine system, even with mild symptoms, and can lead to serious long-term disability.
Physicians are writing medical notes for leaves of absence for months or years for previously healthy young patients who have brain fog, fatigue or heart arrhythmias and chronic shortness of breath.
Article content
Happily, because many people are up to date with their latest COVID-19 vaccine, far fewer are dying from COVID-19 now than early in the pandemic. However, the vaccine does not prevent people from spreading COVID-19, and many people are still highly vulnerable: infants, seniors, people with disabilities, people who are immunocompromised.
COVID-19 is airborne and highly contagious. Ottawa Public Health issued a reminder this week to Ottawans to use “all layers of protection” against it. That includes vaccine (and boosters as appropriate); improved ventilation and use of HEPA filters in workplaces; masking indoors and in crowded outdoor gatherings; use of rapid antigen tests; and avoiding others when contagious. Caution:
Do not to be fooled by false-negative Rapid Antigen Tests (RATs); assume you have COVID-19 if you have close contacts who test positive and/or have symptoms. Swab the inside of your mouth as well as your nose. If possible, retest at day five, seven, and 10, and do not forget that you could be contagious for up to 14 days.
Waste-water testing will continue in Ottawa, thanks to advocacy from public health, but in many places across Ontario and Canada people will have no way to make informed decisions.
Article content
Donatemask.ca is a non-profit organization in Canada that helps distribute masks and RATs to those who cannot access or afford them. Unfortunately, workplaces are pushing employees to work at the office, are reluctant to provide adequate medical leave, and encourage people who are sick to return prematurely.
Ottawa Public Health’s 2021 pinned post says, “We’re all experiencing this differently. Don’t compare yourself to others. Don’t compare it to ‘how it was before.’ Just do the best you can, and if that varies from one day to the next, that’s ok.”
When OPH wrote that in 2021, there was still a sentiment that we were “in this together,” although even then we were not doing enough for the most vulnerable. My 2024 caveat: If we set our societal baseline as consideration of the wellbeing of others, then we can accept that individually we will be imperfect.
COVID-19 tearing through the community now is not the end of this. When September rolls around, we will be vulnerable again. So, I gently remind you to use the preventative tools at your disposal to take care of yourselves and each other.
Dr. Nili Kaplan-Myrth is a family physician and Ottawa-Carleton District School Board trustee.
#covid#mask up#pandemic#covid 19#coronavirus#wear a mask#sars cov 2#still coviding#public health#wear a respirator
6 notes
·
View notes
Note
HI ITS ME CHRONIC PAIN ANON BACK AGAIN... here's my thoughts on who of the human cast is Aware That They Have Chronic Pain Issues. srry ppl were discussing and im like, Wow, Time For Me In Hc Central
june's issues start to really develop and get bad post-game (in my headcanons), so for a long period of time she literally has no one to talk to about it bc she's self-isolating. she eventually tells nannasprite about it when nanna is guilt-tripping her into getting up (nanna voice: Whatever works, hoohoo!), and nanna is like. this is my only granddaughter. i will do whatever i can for her. (i love june & nanna's dynamic. could u tell.) jasprose also is like GIRL!!! You Are In Pain!!! nanna & jasprose team up of the century to get june egbert to Acknowledge Her Problems
dave NO clue NO idea WILL not talk about it. maybe EVENTUALLY tells karkat about it but i don't think she ever seeks out a diagnosis or tries to get one. hes got old ingrained trauma about seeing doctors, which is something he's trying to get over, but like, he already has 4 bajillion other things to unpack about his childhood and healthcare systems are not historically good about chronic pain, a dismissal of their symptoms might set them back in that regard. they're just homebrewing this shit for now.
rose: yeah, she knows. she doesn't talk about it in those terms, though. instead of saying "i have a horrible migraine and cannot get out of bed" she tells kanaya to text the gc that she's afflicted by the Broodfester Woes and cannot join them this evening. theyve sort of picked up by now what that means but she thinks it's funnier this way.
jade: HMMM. i think she put herself through her denial paces but actually i think going grimbark essentially caused her to not feel her chronic pain (a side effect of condy's semi-control over her body), and when she got shunted back into her body she had to face the reality where she DIDNT hurt all the time like wow thats how ppl normally feel? what the fuck????
jane: oh absolutely fucking not does not know. unlike jade, his pain got WORSE during crockertier. yet it still takes literally two decades for him to finally acknowledge that his stuff is NOT normal and the fact that her whole friend group has chronic pain doesn't help, which kind of sucks. jane voice: well sometimes i can get out of bed when i have a headache and rose can't, so clearly its not the same (as if jane doesn't force himself out of bed even when he really shouldnt!!!). roxy has to be the one to tell him.
roxy: yeah she knows it's chronic pain. she's been worried about getting cirrhosis for years, and so has been keeping up to date on her physical health as a result. she figured it out pretty quickly after a couple flareups. trickster mode made it worse for her.
dirk: hal has been telling him for YEARRRRRRRRS that his carpal tunnel is just that, carpal tunnel. and yet. AR: Dirk, if you do not take better care of yourself, you are never going to be capable of building me a body of my own. TT: 1. I'm fine. 2. I'm not building you a body anyways, so the point is moot. anyways he accepts it during the game bc he's like you know what. might as well admit it to myself. good thing, too, because it only gets worse after a couple decapitations.
jake: has pretty much always known, deep down, but like. she lives on an ISLAND. the hell is he going to do about it? no, better not to think about it. someday they'll be able to deal with it, but that day isn't today, and theres so much to do. so he represses it DEEPLY. normal action hero jake english doesn't have chronic pain, of course. she's a heroic manly lead, after all... (the deconstruction of that mindset sort of makes them acknowledge it, though.)
ANYWAYS I JUST RAMBLED AT YOU FOR A COUPLE HUNDRED WORDS HOPE U HAVE, A GOOD DAY/NIGHT/WHAT EVER
YYAYYY no you're so good nonnie thank u forever and ever
19 notes
·
View notes
Text
Minette watches Medici, part 23 (Lost Souls)
-So, this is the culmination of Lorenzo's villain arch. He's fully the bad guy now. And I... Didn't hate that. The writing around that wasn't terrible, although it also wasn't exactly awe-inspiring either. My main problem with this episode is in the other half of this episode's emotional core - Lorenzo and Clarice's health complications, because the writing around that was an unmitigated dumpster fire.
-To start with, let's talk about the historical Lorenzo's health. The thing is, he has suffered from an array of chronic health issues since he was a young man, at the time thought to have been the result of gout, though I've seen modern research dispute this; Wikipedia links a paper that claims Lorenzo de' Medici suffered from acromegaly and his death might's been a result of complications from that.
-Either way, you'll notice that the IRL version is actually better written than the show one. Not only does Lorenzo launch the house of Medici into unprecedented heights despite his chronic health issues (the Handicapped Badass trope and all that), but his premature death is properly foreshadowed instead of Lorenzo suddenly starting to limp, causing doctor to announce he is dying of... Gout? Yeah, that's another thing. Gout ISN'T A DEADLY DISSEASE. You can't die from gout, you just can't. Now, it does contribute to kidney diseasses that can actually kill you, and also is a result of a garbage lifestyle (bad diet, lack of excersise, that sort of thing) that can cause other, more lethal complications. But it never kills you on its own. Like, you could maybe justify some of the inaccuracy by "well, the renessaince doctor wouldn't know any of THAT", but this still leaves us with how sudden the deterioration of Lorenzo's health is in the show and how mild his symptoms are compared to real life. Neither of which is a good change, to be honest.
-But at least he doesn't just drop dead of completely unexplained reasons like his poor wife! Like, if I were to hazard a guess, I'd say Clarice died of a miscarriage, except she doesn't even bleed??? She just collapses, at first seemingly in tears of guilt, but not in physical pain... And then Lucrezia D is carrying her home? And in a few minutes (and seemingly a couple of hours at most in-universe) of screentime, she is just dead?! Did she died of broken heart or some shit?! Look, real Clarice died of tuberculosis, and I know in the show it would probably just sound like a rethread of Simonetta's death. I get that changing it to miscarriage makes a lot of sense considering that was indeed something potentially lethal back then, also Clarice had several in her life, so it's not a bad idea in principle. I also get that the writers were trying to tie Lorenzo's personal tragedy to his professional downfall. But in so doing, they rendered a powerful scene of Clarice being overwhelmed by guilt and despair over her husband's actions kinda silly by almost implying guilt and despair killed her?
-And don't get me wrong, it is a very powerful scene! I actually liked it a lot! Even the previous scene of Clarice learning Lorenzo sold their little girl to pope's failson isn't bad, especially since it retroactively gives more narrative weight to Lorenzo's previous disgust at another very young girl, Caterina Sforza, marrying a papal failson (well, failnephew, but you know).
-I am a bit miffed at the show's inconsistency around just how corrupt the renessaince papacy is. Like, at first, it doesn't seem nearly as bad as it is in The Borgias, but then Lorenzo apparently considers asking the pope to name his 14-year old son a cardinal perfectly normal, or at least nothing that a strategic match cannot fix??? It also begs the question why the fuck would the pope even agree to that considering he should still be mad about Sarzano, but okay.
-The one and only thing that I liked, nay, loved about Clarice's death... We got one last Clarice x Lucrezia D moment out of it! I know I shouldn't celebrate my girl dying, but like. Look at the pathetic little breadcrumbs they feed us shippers this season. I can't let my obsession starve to death, you know!
-I am not sure whether what Lorenzo did to poor Anna the beggar counts as bribery or gaslighting, but I guess the grey area was the point. Either way, I liked it! And I liked her giving money to Savonarola, overcome with guilt! See, I can be fair to this show, even if I am tired of it and can't wait for the final episode!
-I liked other things too, like Lorenzo going full villain mode and Piero grieving Tomasso. Even if Piero's actor... Look, Tewkesbury from Enola Holmes was 16, it's a bit more understandable if he doesn't hit every note. He isn't completely terrible in this, just... Not good.
-I only noticed in this episode that Savonarola is played by an Italian and dubbed. And I noticed, because the dub of his speech at the beginning, while passionate, clearly did not go as hard as the actor's expressions suggest he did in the original audio.
-Okay, that was exhausting. Onto the final episode!
4 notes
·
View notes
Note
ok, so I have this problem. I dissociate. A lot. It causes me to loose my balance, and I also have knee pain, occasional back pain, and mild hip pain. I do not use a walking aid. I’m 13, which, in my opinion is too young, but there are days where I go rlly slow. How do I explain 2 people that I’m not doing it on purpose, it’s cause it hurts. Also, how do you go about navigating crowds on bad days?
First of all, I am so sorry that you're going through this! This is a really difficult situation that you're in and I'm sorry that people around you are not seeing and understanding that. Secondly, my direct messages are open and it might be easier for me to better answer your questions if we can have a conversation about it, and/or if you have other questions, you're welcome to reach out there! As a disclaimer, I'm not a doctor so I can only share from my experience and my perspective. My lengthy answer is under the read more !
The part you asked for:
Communicating lived experiences, like how your chronic pain and balance issues impact you, is particularly difficult since others aren't experiencing what you do, so they have a hard time understanding what it's like to have that level of pain and can often assume you must be exaggerating. Comparing your pain to pain they're familiar with helps them understand (ex. "it feels like when you bump your knee really hard, but my pain doesn't go away after a couple minutes"). The approach you'll take depends on a lot of factors, like their ages, your relationships with them and how open they are to trying to understand what you're experiencing. Unfortunately, some people won't even try to understand, sometimes you have to let those people out of your life if they're not willing to try, but sometimes people (in particular parents) are actually scared of confronting the situation because of what it means for you+your future; you can continue reminding those people that you are still in pain and need help/accommodations if they don't acknowledge it at first. You can share resources/info about chronic pain with them, and/or tell them your pain level at certain times with a numerical pain scale.
There's a loose formula I use for general communication that is based on DBT therapy which is: "I experience this, this is how it impacts me, this is how it impacts our relationship, this is what you can do to help me and help our relationship". Coming up with a solution yourself for the situation helps set clearer expectations and what the other person can expect from you rather than putting it on them to find a solution.
How I typically explain it is, "I have chronic pain and other health issues that impact how quickly I'm able to do things. I often experience uncontrollable moments of pain that appear unexpectedly. Concretely, that means it takes me more time to do the same things that you do. I do my best to make preparations in advance to manage my symptoms, but they sometimes appear unexpectedly and I cannot control them. It would really help me if you could let me know (X time/days in advance) if there's something I need to be ready for at a specific time, that will give me a better chance to be there/ready on time". I personally timed how long it takes me to do the activities I need to do to get ready, so I know that if it's a bad pain day, I'll need to add another 30 minutes to an hour to accommodate that.
On bad days, I avoid crowds. But I understand that you probably aren't able to do that; you can maybe suggest going at an earlier time when things are less busy though? The quick version is: I bring sunglasses (even for indoors), headphones/earbuds (I have the Skullcandy Sesh Evo, they're noise-cancelling - I leave one halfway out in case I need to hear something & play lofi music), a medical face mask (it feels reassuring/protecting) and a water bottle. If you're grocery shopping and get overwhelmed, you can communicate that and say you're going to go wait outside. If you're at an event, you can excuse yourself to the bathroom for some distance. You're going to have to accommodate yourself in ways that may seem socially weird to others, but your health and comfort is more important than those social rules.
For the long explanation:
I prepare before I even get into that situation.
So for prep, I make sure I eat a proper meal. I take a 1h30 nap that allows me to reset my body and sensory experiences. I do a guided deep breathing exercise (1-2 minutes following a YouTube video is enough) and my stretches to help with pain. I take my pain medication early enough for it to take effect before leaving. I make sure I'm wearing sensory friendly clothes.
I carry with me at all times a Ziploc bag of "essentials" that contains stuff like lip balm, lotion, ear plugs (for when I need to fully tune out what's around me), mints/gum (helps anxiety/nausea) & additional pain meds. I put my essentials pack into my backpack and in my backpack I have a snack (like a granola bar) and a large water bottle. You can also put the sunglasses+earbuds/headphones in when not in use. Yeah it kinda sucks to carry a backpack, but I find the weight/presence of it grounding and my anxiety is reassured knowing I have everything I need on my person. You can use any type of bag for this btw. Having a cane forces people to give me space and makes them generally more understanding of my whole situation when I'm wearing sunglasses indoors; a mask can sometimes have a similar affect depending on where you live. If you're standing in line or a place that isn't moving much, you can actually ask people if they can take a couple steps back to give you more space.
Additional input:
My dissociation is brought on by my pain rather than the opposite. So I'll experience a higher level of pain, and in order for my brain/body to be able to cope with that, I dissociate (it's an involuntary response but I can recognize a lot of my triggers). My therapist very gently explained to me that while dissociating is annoying, it does serve a purpose and you don't always need to try to forcibly ground yourself. It's a maladaptive coping tool, but it's what you have available right now and sometimes using more helpful coping tools can only happen when you have more control in your life. That doesn't mean you shouldn't try learning them now, but it's important to not get mad at yourself for having that response.
I'm not very familiar with having balance issues due to pain or dissociating. What I assume is happening is that your dissociation is causing a warped perception, which is causing you to have balance issues. It may also be a different underlying cause (vertigo, inner ear infection, blood sugar fluctuations, iron deficiency, just to name a few). It's really hard to unravel all of these things to see what's connected and what might be a different issue all-together. This is where I mention you should go to a doctor if you haven't already, my heart goes out to you if that's not an option for you at the moment but I can reassure you that you will be able to get medical help eventually.
Lastly, there is no age too young to encounter disability. For example, it's hypothesized that fibromyalgia can be triggered by traumatic events, which can occur at any age. But to clarify, it is definitely not the norm for a thirteen year old to be experiencing these issues! I had to do a lot of research by myself and present that to doctors for them to know how serious I was about my difficulties. When/if you can, I'd recommend booking multiple appointments in one day to save time considering wait lists. Having all your test results, x-rays and other medical info already done and readily available helps to cut down the wait time for a diagnosis by a lot. For me, a diagnosis allowed me to accept myself and my situation better, and let me allow myself to use the accommodations that were necessary. Wishing you the best & thank you for reaching out!
2 notes
·
View notes
Text
Medical update (long post, don’t read if you’re not interested)
A lot of my followers probably know that I’ve had neck issues for the past couple of years and migraine problems for a long time before that.
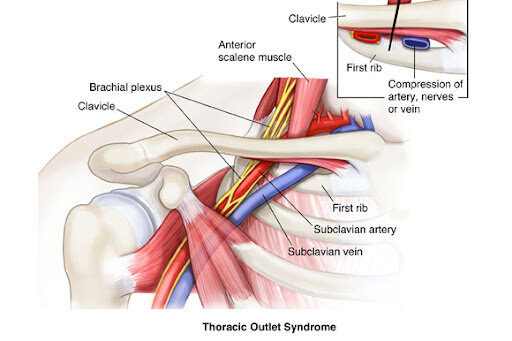
Within the past 3-4 months I’ve made significant progress with this issue because I finally got a diagnosis for what was happening from a reputable orthopedic doctor in my area. I have severe neurogenic thoracic outlet syndrome, which essentially amounts to an orthopedic issue where a biological irregularity in my first rib traps the nerves in my thoracic outlet behind my clavicle. This happens mostly when my shoulder muscles become too relaxed--For example, it happens when I’m sleeping and I roll over into the wrong position, or when I get extremely drunk or high (which I used to do very often). It is mostly in my left shoulder, but I also have an irregularity in my right shoulder. In addition to this being a biological issue, it was probably exaggerated by my years of violin playing.
The pain from this condition is chronic and excruciating. It causes me to have severe migraines where it feels like there’s an extreme amount of pressure behind my eyes. These migraines also cause me to get vertigo and nausea when they’re bad enough.
I’ve been getting migraines and vertigo since college, but college is also when I started weightlifting, and strengthening the muscles in my shoulders helped to lessen the severity of some of the symptoms--So much so that I thought the problem had gone away even though I didn’t know the cause of the problem.
This turned out not to be true; a whiplash injury (long story) made the pain flare up again, this time to the point where I thought I was having a stroke. This injury happened during the pandemic in 2020, but the pain from the TOS lasted far longer than any of the pain from the whiplash--It was so severe because the injury caused the nerves in my shoulder to move from close to my spine over to almost the edge of my clavicle.
Of course, I had no idea what was happening at first, so it was extremely concerning and it gave me numerous anxiety attacks (literally, my nerves were in very bad shape). I dealt with this pain for almost exactly 760 days, mainly because every single doctor I saw couldn’t figure out what was wrong. But after a lot of physical therapy and the right anti-inflammatories, I finally seem to be making progress with the pain. To give you an idea of what it took, I had to first strengthen the muscles in my shoulder, and then I literally had to dig my thumb into the side of my neck in order to move the bundle of nerves back into the right place. (This hurt a lot, but the migraines hurt worse.) After two years and two months, I’m feeling somewhat normal again, although it’s definitely still a work in progress.
I’m already starting to lift weights again and I’m hoping to be able to start running this spring. Throughout all of this, only meditation (specifically meditation in the Vajrayana Buddhist tradition) has provided me with the mental fortitude to deal with the pain. The anti-inflammatories helped too, but those are only a temporary fix. I’ve learned that when it comes to chronic pain of the genetic variety, no supernatural power is going to help you--The only thing that will help you is your own mind, because ultimately you are the only one that has to deal with the pain. I’m also extremely thankful for my parents, because both of them were restless in helping me get the medical care that I needed. Specifically, my mom is the one who found the orthopedic doctor that was able to diagnose the problem.
At the end of the day, I hope this experience burned some of my negative karma, which is also just the negative karma of sentient beings in general. If you’ve supported me throughout the past couple years, thank you as well, because I quite literally could not have done it without you. My support network has been really essentially through all of this, and I’m so blessed to have some incredible people in my life.
2 notes
·
View notes
Text
Exploring Natural Remedies for Varicocele Effective Treatments Without Surgery

Varicocele is frequently an underlying cause of pain, and can lead to infertility. Being familiar with varicocele, its forms and symptoms, as well as the various varicocele treatment without surgery options can be a big help to keep the condition from becoming chronic.
Types and Symptoms of Varicocele
The degree of varicocele may be determined using the following criteria:
Grade I The varicoceles are part of the first grade and are quite small. They are able to be diagnosed or identified only through an examination of the body or imaging techniques. In general, they don't have any symptoms visible.
Grade II Varicoceles of medium size, which can be detected on physical examination even in an upright position. The symptoms could include a feeling of discomfort or a tingling sensation around the scrotum.
Class III: This is a significant dilations that are visible and feelable. The majority of them cause significant swelling and discomfort as well as the patient might start to exhibit some obvious physical changes to his scrotum.
It is important to recognize the symptoms of varicocele and the use of natural remedies is a way to cure varicocele naturally. The most frequent symptoms of varicocele are :
Pain or itchiness in the sac of the testicle, typically in the evening or after a prolonged period of standing, or following exercise.
A feeling of dragging or weight inside the testicle sac.
Dilated or swollen veins within the sac of testicle.
Testicular atrophies or asymmetry in size.
Infertility or issues in conceiving are usually identified by a fertility test.
Can Varicocele Be Treated Without Surgery?
The issue of whether it is possible to cure varicocele without surgery is somewhat complex. Although surgical procedures are popular and extremely effective, other options that aren't surgical are able to help control and ease symptoms. Non-surgical treatments do not cure the varicocele however they may provide some relief from symptoms that improves the your quality of life.
Natural Treatments and Lifestyle Adjustments
Lifestyle modifications: The symptoms are treatable through a healthy and balanced lifestyle. Exercise, a healthy BMI and avoiding being in a position for too long can decrease the pressure on the veins within the scrotum.
Wearing supportive clothing Wearing supportive underwear, or athletic support reduces discomfort and helps support the region.
Fluid intake and Diet Nutritional and healthy diet that is abundant in antioxidants, when coupled with adequate hydration, could improve vascular health. Dietary ingredients are incredibly high of vitamins C and E and flavonoids, which help improve blood vessel health and, thus, improve circulation.
Herbal remedies: Some plants are believed to have benefits in keeping veins healthy. Certain remedies are utilized by some individuals to strengthen vein walls and enhancing blood flow. These products from herbs must be discussed with a physician before using.
Tips to Prevent Varicocele
To prevent varicocele, you must take note of every factor that could contribute to its development. The varicocele natural remedies listed below could be beneficial in decreasing the chance of developing.
Avoid heavy lifting Avoid excessive straining and heavy lifting increase abdominal pressure and this can lead to the development of varicoceles. Proper lifting techniques must be followed, including the assistance of a professional when lifting large objects.
Control Constipation: Constipation for a long time results in more abdominal pressure and worsens the varicocele. A healthy intake of fibre, adequate fluid intake and regular exercise can reduce constipation.
Routine Check-ups: This implies that the patient has regular and frequent medical check-ups. It is possible to detect early particularly if someone has the signs or risk factors.
Healthy Lifestyle: Keeping an appropriate weight or BMI and being fit by exercising regularly could aid in the prevention of varicocele. It accomplishes this by increasing blood flow while at the same time, reducing tension on veins.
Complications and Fertility Problems
One of the major complications that can be found due to varicocele has to do with fertility. Varicoceles influence the production of sperm and the quality of sperm by these methods:
The increase in temperature of the testicle: Varicocele may disrupt the body's natural mechanisms to regulate temperature of the testicles or the scrotum. Testicles that are not at a normal temperature of people suffering from varicocele can affect producing sperm, and decrease the sperm count.
Hormonal Inbalance Varicoceles may influence hormone levels and bring about an imbalance that can affect the process of spermatogenesis and therefore fertility.
Reduced Sperm Quality: The oxidative stress induced due to varicocele could reduce the sperm's motility, resulting in a greater proportion of abnormalities in sperm.
Identification of varicocele early and evaluation of varicocele natural treatment options are crucial to the outcome of fertility.
Homeopathy and Varicocele
Homeopathy is a method of best varicocele treatment that makes use of extremely dissolving substances. Its principal goal is to boost the body's natural healing capabilities. Here is a listing of remedies believed to ease in the treatment of symptoms associated with venous constriction as well as discomfort that is associated with varicocele. Other remedies are touted as a way to assist in the reduction of disease-related swelling and pain which can be experienced in varicose veins as well as related ailments. Additionally, certain are recommended for their ability to help strengthen connective tissues within the body, as well as to help maintain vascular health.
This can help you determine the right remedy and dosage that is appropriate to treat your specific condition. Additionally, integrating traditional treatment with homeopathy and lifestyle changes could be beneficial in the ways of treating varicoceles.
Conclusion
Varicoceles can be very uncomfortable and may seriously affect fertility. Understanding the causes, types and possible complications is crucial to managing the disease. Nonsurgical approaches - lifestyle modifications as well as natural remedies can greatly aid in relieving symptoms and improving general health of an individual. Prevention, methods to boost fertility, and other nonsurgical treatment options for varicoceles have also been proved to be effective. Homeopathy may help in certain cases, but it is important to consult a qualified and experienced doctor to develop a disease treatment plan which will not just ease discomfort in the moment, but also guarantee long-term health.
0 notes
Text
its 5am and i can’t sleep and i have to ramble about something (a few somethings actually) bc i cannot stop thinking about it!! this is really just for me to get my thoughts out bc they’re driving me crazy, but on the off chance anyone reads this, prepare yourself: it’s about to be a very long post.
i have so many chronic issues — both physical and mental — that i’m just used to dealing with at this point, and i’m only just recently realizing how not normal they are?? the main thing that’s driving me insane lately is just my overall physical well being, like it’s just so… not good lmao. i’m extremely anemic, so i’m basically exhausted and lightheaded and dizzy and nauseous pretty much all of the time which is just awesome for me, and it’s been even worse than normal the past few months bc i have a ton of food issues that just keep getting worse (caused by a super fun combination of depression, disordered eating, constantly being sick, and just general stomach issues). my diet is really just all over the place and definitely not as nutritious as it needs to be, which as you can imagine does not help all the health issues i already have! on top of all that, i was finally diagnosed with adhd earlier this year after spending forever 1) constantly learning that a lot of things i had always thought were just “me things” were actually symptoms 2) being told by so many people around me WITH ADHD that i seemed like i had it, and 3) outright asking various psychiatrists and doctors to test me for it. because of the shortage on adhd medication, i only recently was able to get a prescription, and (this is where the relation to food comes in) literally no one — not my doctor, not the psychiatrist who prescribed it, not the pharmacist — thought to tell me that the medication i’m on lowers your appetite?? i only found out bc my mom, who’s a nurse, mentioned it one day and was shocked that i didn’t already know that was a side effect. so that sucks because i need the medication, but i also need to be eating a lot more than i currently am (especially because i’m also taking iron supplements for my anemia, and if you don’t eat enough while taking them, they make you sick). so! that’s all great for me!
i’ve also had chronic headaches since i was 11 years old that have continually gotten more frequent and more painful over the years, to the point that i get them almost every day and have taken advil, tylenol, midol, etc. so often that i’ve pretty much built up a tolerance to them and they do essentially nothing for me anymore. they’re usually just really bad headaches, but sometimes i get full-on migraines, and when i ended up in the ER in the spring (long story), the nurses told me i’m likely developing a migraine disorder. this is kind of just an unfortunate fact of life for me now since it’s been going on for eight years, but i’ve just been thinking about it a lot lately bc of a psychiatrist appointment i had a couple months ago (lots of various appointments lately but not much has gotten better… lol). when i was telling the psychiatrist about my headaches, he told me that the average person gets a headache twice a year, which just… genuinely blew my mind. like, i cannot imagine not having this problem. what a nice life that must be for the average person. and i mean, i’ve always known that i get headaches way more often than most people, but i truly could not wrap my brain around the difference being that extreme. i literally started asking everyone i knew how often they got headaches bc i was so surprised and curious, and they all told me they just never get them?? like that is insane to me, i’m so jealous.
okay last thing for now: the reason i’m still awake rn! i started struggling with insomnia when i was maybe 11 or 12, and just like with the headaches, it’s gotten worse and worse over time and i’ve just kind of grown accustomed to it. it always takes me hours to fall asleep, and i have a very hard time staying asleep — i usually wake up in the middle of the night at least two or three times a night. it’s another thing i knew wasn’t super typical, but it’s not insanely uncommon either. but that same psychiatrist had a statistic for this too, and he said that the average person wakes up in the middle of the night ONCE A YEAR (under normal circumstances, so not counting things like being sick or having abnormally high stress levels). he also asked me how long it takes me to fall asleep again after waking up in the night, and i said “not that long, like half an hour usually” and he quite literally just stared at me and said “yeah so that is long actually.” like, i know not everyone has insomnia, but this whole time i thought that everyone who DOES have it would have generally the same experience as me, and apparently that’s just not true lmao. in fact, he said my insomnia is so bad that i have what’s called terminal insomnia, so i guess this is just my life forever! how fun is that!
so that’s pretty much all i wanted to say (she said as if she didn’t just spend 30 minutes typing all of this). whenever something like this is on my mind, it makes it even harder to sleep than it already is all the time, so i figured i’d just come on here and word vomit for a while. i don’t expect anyone to read all of this (or any of it tbh), but if you have, thank you for listening! i hope you have a great day and get a better night’s sleep than me tonight :)
1 note
·
View note
Text
I feel like I want to write about death. But I'm not sure exactly where to start or what to say.
I guess I'll start with why it might be something I think about.
I met my first wife when I was finishing my freshman year of college. She wasn't in school at the time, but we were only a month apart in age. We hit it off instantly.
The next year we lived in my dorm room together, getting married shortly after I graduated.
I'm not sure if it was a perfect relationship, but early on, things were good. She realized she had a drinking problem and got sober.
Then she was in a major car accident. No broken bones, but soft tissue damage and a concussion. Back then they didn't see anything so sent her on her way once they confirmed there were no broken bones. In hind sight, she clearly suffered a TBI.
She did ok for a bit, but chronic pain crept in and she started having progressive symptoms of CTE. She started drinking again, in part to deal with the pain, in part to deal with the progressive CTE symptoms, in part to deal with the PTSD, depression, and anxiety that were getting perpetually worse.
I watched someone who had a near photographic memory and extroverted personality turn into a shut in with memory problems. Turn into someone with emotional regulatory issues.
I was on a business trip in San Francisco and she came with me. The second morning there, I woke up and the room felt far more quiet and still than it should. I reached over to touch her and her body was cool.
Logically, my brain knew it was too late, but I leapt out of bed, pulled her onto the floor. Mentally I noted that she already had livor mortis. I could smell a vomit-like smell. I started chest compressions. I could hear the fluid in her lungs as I performed compressions. It wasn't vomit she aspirated, it was that she had been gone long enough fluid had drained into them. I called 911 while I was giving chest compressions.
When they got there they performed some actions, I know they knew it was futile. it was clear she was gone.
They let me stay in the room with her until the medical examiner? Coroner? Whoever, got there to declare her death.
I called my parents, I called hers. My cousin rushed to fly up from southern California.
After I walked around San Francisco, a strange city full of strangers. I had coworkers there, but not who I considered friends.
I talked to a couple of people on the phone. I went into a brew pub and had a beer or two. I remember thinking how surreal it was that there were people sitting there having a good time and I had just gone through what I went through.
My cousin got there, we to shit faced drunk. My parents got there the next day. We went to a funeral home. I remember thinking that she would have appreciated that it looked like it could have been a stand in for the funeral home in Six Feet Under, which had been one of her favorite shows.
The autopsy found the cause of death to be "acute multidrug toxicity". A combination of alcohol, Wellburtin, and Ativan. None of them were in excessive levels, other than the alcohol. And none in concentrations out of line than she had consumed hundreds of times before. "The Heath Ledger" special she would have called it. She had honestly said before it was how she would want to go. Just stop breathing in her sleep.
Before that, we had talked, many times, about getting her into treatment. She was scared.
I had honestly started to lose her years before I lost her. She suffered, we suffered. The last few years it felt like we were just surviving.
When she died, it felt like someone set off a grenade in my chest and the pieces of a shell were left.
I consciously told myself, I was going to put the pieces back together and build something good and healthy for myself.
I had a lot of help along the way. And I would very much make the choice to get out and not collapse in on myself, especially when it was hard.
I didn't always have a straight path there, but I am in a good place now. I reconnected with a friend from high school. We have been together 5 years now and are now married.
I am happy. I have had a lot of trauma. I am here.
1 note
·
View note
Text
Coming out as a Transwoman: Answers to Frequent Questions
You may find that you have a bunch of questions now. So to help you with those here is a list of some of the more frequently asked questions I have received which I coupled with my responses. However, do keep in mind that I am only speaking about my own experience.
I never once saw you do anything stereotypical of an LGBTQ person. How do you know?
Actually, I did. Unfortunatly actions like these are stigmatized. I was pressured into either conforming as one of my male peers or else face hardship. I was therefore socialized and pressured into presenting as a man. I became so good at masking and repressing these thoughts that I ended up suffering from the symptoms of repressed childhood trauma as an adult.
Okay, so you didn’t know this because you repressed it before; why not keep doing that?
This discovery came about after years of growth and a deep desire to address a multitude of chronic issues. Thus, to chose to repress what I know can recall about myself will only exaserbate other issues. At best such efforts may allow me to survive, but I certainly could not thrive. Also, recall that I had already once repressed this knowledge. I was only able to repress these memories in that context: I was driven by a desire to avoid any more death threats or sexual assaults. We weaponize ignorance when we try to ignore inconvenient truths. Actions like these can embolden the oppressors and assailants. Finally, by repressing this truth I had to struggle with a whole host of chronic symptoms for much of my life. Some of these chronic symptoms included:
sleep issues (insomnia), fatigue, or nightmares
low self-esteem
Confusion/problems with concentration and memory
Unexplained pain and stomach distress
It’s Difficult To Control Your Emotions
Strong Reactions To Sudden Situations, Specific People, and Places
Frequently Emotionally Exhausted and Anxious
Emotion dysregulation, fear of abandondoment, and anger management issues
Thus, I am now becoming healthy with each passing day. I will speak to this more in a bit but for now, consider these two articles for more information:
Wait, does this mean you’ve changed your sexuality?
Fair question, but again no. Being trans is not about who someone is attracted to per say. Being trans is actually about externalizing my internal lifelong identity, an identity that was previously oppressed by others, and suppressed to the point of memory loss.
So if being trans is not a choice, then help me understand what made you trans. Did the culture and politics influence you? Was this just something you chose to become.
No. No. And also No. Allow me to clarify: I didn’t choose this, rather I discovered that I am trans. The following quote may be helpful: “Theories of both psychological and biological causality have been forwarded and it is quite likely there are different causes for different individuals. Lately, strong research suggests that an incorrect amount of miss-timed secretion of male hormone during stages of fetal development may create a transgendered individual - whether male or female. Biologically, nature will produce a female unless male androgens are supplied at the right times and in the right amounts. There are physiological and mental gray areas between male and female "absolutes". Additionally, there are some theories arguing a genetic model of causality.”
Not sure how to ask this question, so allow me to use a house as a metaphor: you helped me understand your thinking by unpacking the attic, and I think I understand your heart on the ground floor. However, what about…you know…
Please don’t ask. No two trans people have the same experience. Here, I align with what you and I were both likely raised to believe: that it is innapropriate to ask or make a comment about these topics.
How do you know this is healthy or safe?
I have relied upon a team of doctors and therapists to ensure I am following the WPATH standards of care for transgender individuals. Anecdotally, I have also been keeping track of my transition with a variety of metrics. Here is a handy comparison of just some of the healthy changes I have experianced during this journey:
Before coming out: negative blood work results in several key areas.
Today: all the negative results are now in a normal/expected range.
Before coming out: I carried a great deal of extra body weight.
Today: Now that I am living in the body that I want, I have successfully lost over 40 pounds with little effort.
Before coming out: I could never address/fix my minor depression, anxiety, difficulty concentrating (compounded with ADHD) and avoidance of social situations.
Today: Symptoms related to these issues are at 1/2 their strength and fading!
1 note
·
View note
Text
RE8 Ladies + S/o with chronic pain HCs
Type/cause of chronic pain is kept ambiguous, but some of the hcs might seem geared towards migraines, since that's the main thing that I personally struggle with (and these are very definitely comfort hcs). Features Alcina, Bela, Cassandra, Daniela, Donna, Mother Miranda, and as a 'lil bonus Ava. Not particularly long, but the combined length of every character is enough to be put under a read-more (About 2,500 words in total).
Alcina:
It’s difficult for her to know that you are suffering, but be unable to deal directly with the source of the problem. Chasing off unwanted nuisances or hunting down threats to the castle was one thing, trying to solve complicated medical issues was another thing entirely. If only she could tear your condition asunder without tearing you asunder.
That being said, she’ll still support you endlessly, however she can. It doesn’t matter how expensive or hard-to-access possible treatments are. If there’s something you haven’t tried, and are interested in trying, she’ll find a way for you to get it.
The biggest, and arguably most helpful, thing that she does is set up a space for you within her office. She spends quite a lot of time there for her family’s business, but doesn’t want to leave you alone on bad days. So this was her idea of a nice compromise.
There’s a very comfortable sofa that folds out, a cabinet filled with the softest blankets, and several pillows of a few different sizes. Servants are instructed not to interrupt Alcina’s work without good reason, but she has a couple who ensure your snack cabinet is always well stocked.
If there are certain environmental factors to your condition, such as sensitivity to light and sound, she does her best to reduce their effects. Lights remain dimmed (or she’ll rely on candlelight), her music will be kept quiet enough to be soothing, and she’ll refrain from taking any calls while you are with her.
Bela:
To think that Daniela once tried to claim that Bela would “never need to know any of that (medical) stuff”! Sure, there haven’t been many people who have needed (and received) treatment from her, but that didn’t mean the skill was useless. Admittedly, she doesn’t know enough to replace one of your doctors, or try to create her own version of a cure, though no one really expected that much from her.
Still, she knows enough to help soothe your pain. Obviously there are different techniques for different kinds of pain, and she does research before trying anything specific. Bela’s also aware that you’ve been dealing with this for far longer than she has, meaning that you probably wouldn’t be pleased if she came in, acted like an expert, or assumed that you hadn’t really thought about the most popular remedies. So she’s tactful with how she approaches things, always checking if you’re familiar with a subject before she tries to explain anything.
Bela ends up surprising you with a lesser-known skill of hers: Massage. Studying anatomy has given her a decent idea of the body’s more sensitive spots, and the rest she’s figured out through her own, ahem, experiences. Regardless of where you’re in pain, your girlfriend can help reduce your suffering. Okay, well, if your pain is more internal than external, it’s a bit harder for her, but she can still help you relax.
One of her favorite things to do after giving you a massage is to just pull you in close for some cuddling. Preferably you’ll be in her lap, with her arms around your waist, her chin tucked on top of your shoulder. Then she’ll do her best to whisper you praises, reminding you how strong you are, and that she’s incredibly proud of you.
Cassandra:
She’s, uh, not great at this. At least not at first. Maybe she’ll never be more than good at it, though. But she’s definitely trying! And learning! By Jove, that’s something, right?
First things first, she’s always ready to try to distract you, primarily through kisses and gentle touches. Fingers softly trailing over your skin, lips tickling your neck, featherlight in all the right places… It’s not inherently sexual (though it can quickly go that route if you ask), just intimate. It’s harder for your brain to process pain when you’re also processing pleasure, so there is some science behind Cassandra’s methods, even if she herself isn’t entirely aware of that.
While she’s not great with words, there are certain things that she manages to articulate well enough. For one, she makes sure you know that you aren’t a burden. Taking care of you- no, helping you take care of yourself- is a labor of love, if a labor at all. More than that, she knows full well that you probably don’t like feeling pitied, or coddled. That, over time, being sick ends up being beyond frustrating. She never wants you to feel like your condition defines you, or like it puts any strain on your relationship.
That said, she’ll avoid telling her family any specifics unless you do first, and ensures that the staff know how to accommodate you (without telling them why, because it’s none of their fucking business, and she’s their boss, and for fuck’s sake it’s their job to do what she tells them. Maybe she gets a lil bit overzealous with it). At no point will she ever complain about helping you, or otherwise indicate that your needs are “troublesome”.
At the end of the day, the best comfort she brings you is her presence, simply being near you, endlessly loyal, tireless in her affections. Especially considering she gets clingier the worse your symptoms get.
Daniela:
Hope you enjoy cuddling. Seriously. There’s nothing Daniela loves more than curling up with you, and that goes double for bad pain days. Some adjustments will be made position-wise if you need, but she’ll still hold you as close as possible, for as long as you need. Although she might eventually fall asleep (because damn are you comfy), she’ll play with your hair or run her fingers along your scalp until she eventually dozes off.
If you want a little more from her than light snoring, or if she feels like going above and beyond, or honestly just if she’s thinking about how much she loves you (so all the effing time), she’ll do something she’s always loved in movies/books: Reading to you! She’ll pick special books that neither of you have read before, so you can experience them together on your sick(er) days. Which does, of course, mean that it might take months to finish even a single one. Surprisingly, Daniela won’t even briefly consider reading any without you. Even if the plot is really good.
But, uh, if you wanted her to read to you on a day where you aren’t bedridden? Hell yes, my friend, she’s absolutely down for that!
On days where she’s too busy to spend hours upon hours in bed with you, or days where her ADHD is just particularly bad, she tries her best to leave you with a “substitute”. AKA a massive fucking teddy bear, in a reddish brown color, with a green bowtie. Custom ordered (The Duke did not dare tease her for it). There’s a heart stitched onto the stuffed animal’s chest, which features your first initial alongside a D for Daniela.
Additionally, she has a blanket she only brings out for you, which she periodically sprays with her favorite perfume. That way you can hold it close when she’s not around, as if you were cuddling her. For her sake, though, don’t hold the teddy bear or blanket too tightly when she is around. Homegirl here will get jealous of inanimate objects, even ones that she gave you.
Donna:
“I think I have a tea for this…” Damn right she has a tea for this. Donna has a massive garden, with dozens if not hundreds of different plants, including a variety of herbs/spices. At least one of them has to be a little helpful for you. Whether it relieves pain, helps you nap off some of your misery, or just distracts you by tasting bloody-well delicious! Besides, few things make you feel quite as loved as holding a cup of freshly brewed tea in your hands, knowing your lover made it just for you. Like a hug in a mug, it is!
Similarly to Alcina, Donna will also try to create a comfortable space for you, but isn’t likely to put it downstairs with her workshop. Instead she’ll let you take over one of the larger guest rooms, customizing it to suit your specific needs. There will be some easy to care for plants for decoration (ones that won’t mind potentially missing out on natural sunlight), a couple relaxing paintings, and a shelf near the bed with things to help you pass the time, mainly books.
Furthermore, she’ll do her best to keep you company as often as possible. She’s naturally a fairly quiet person, so you won’t have to worry about sound if that’s something you’re sensitive to. While she prefers using a sewing machine, she’ll do things by hand while you’re in pain, just to reduce the chances of you getting irritated by the sound.
Speaking of potentially irritating sounds… by god can Angie be difficult to be around when you’re ill. Thankfully, Donna is perfectly understanding of this, and, as the only person Angie ever listens to, makes sure to give the doll a stern talking to about your health. To your immense surprise, it actually works. You’re not exactly sure what was said, but Angie certainly becomes a lot more compensating afterwards. She’ll keep her antics to herself, and usually even on another side of the house from where you rest, but only for as long as you’re tucked away in your room. As soon as you set foot outside, her restraints are metaphorically removed. All hell breaks loose (as is her universe-given right as the physical embodiment of both Chaos and Entropy).
Mother Miranda:
If the two of you weren’t lovers, there’s a decent chance you would completely misinterpret her actions. She might come off as irritated, like she has bigger concerns than your health, you fragile little human. After all, she is a goddess (well, practically). But the truth is that she’s aching inside every time you have a bad pain day, knowing that (for once) she cannot cure your ailment. Maybe if she had infinite subjects with the same condition as you…
But, at the end of the day, that’s the problem. There’s only one of you. One of her beloved, her little human darling, so dangerously fragile in comparison to the scale she works on. Even with all the time in the world, which she most certainly has, she cannot cure you without taking incredible risks. With your life at stake… It is a gamble she refuses to take. You are hers, and while she hates to see you suffer, the truth is that she’ll always be selfish enough to let you endure on your own.
That doesn’t mean she doesn’t help, though, just that she doesn't do a full-out experiment on you. Instead, she keeps notes. She’ll track your activities, bedtimes/when you get up, dietary habits, when you have pain, what you do to treat said pain, how effective the treatments are, etc, etc. All of this can be very useful in establishing patterns (a skill she’s gotten very good at, in her many decades of being a scientist), which can in turn lead to less pain days.
(For example, many people with migraines find that certain foods seem to trigger a migraine, or at least increase the chances of getting one. Though admittedly they don’t always end up cutting the food out of their diet. I mean, come on, you want me to give up chocolate? You want me to drink normal milk, like an adult? Kidding, kidding, I don’t have any food triggers. Nor do I particularly enjoy chocolate milk, nor do I dislike it.)
Moving on! While her work seemingly takes precedence over your condition, Miranda is not heartless, and she does do some things to lend you more direct comfort. Specifically, she tries to work in the same room as you when she can, normally while making electronic copies of physical documents, or while looking over the details of a finished experiment. She’s not always one for cuddling, so she won’t often get in bed with you during the daytime. But at night? Yes, fine, she will wrap her arms around you, maybe one of her wings too if you like how soft they are.
Just don’t think that she secretly loves every second. It’s not like she’ll spend half an hour whispering about how sweet and adorable you are as soon as you fall asleep, or anything like that. It’s twenty minutes at the most.
Bonus!Avaskian Caldwell:
“Oh, fuckin’ mood!” Followed by a solid thirty seconds of pure regret. Seriously, though, Ava has spent xer entire life (starting at age 10) dealing with chronic migraines. For a while xe also dealt with POTS (Postural Orthostatic Tachycardia Syndrome), which meant lots of chest pain, but that (thankfully) faded as xe grew into an adult, as is fairly common with the condition. If anyone in Castle Dimitrescu understands unrelenting, unexplainable pain, it’s xer.
That being said… Ava never really managed xer chronic pain, at least not when xe was at xer worst. Xe had to drop out of school because of it. Hell, xe didn’t have a “real” job until xe was almost 23! Didn’t have a chance until things just calmed down for xer. So xe gets anxious whenever you talk about your health, worried that things are (or will at some point be) as bad for you as they were for xer. Other than that, though, you might initially think that xe doesn’t care, or didn’t understand the conversation.
Truth is, xe knows how absolutely fucking ANNOYING it can be to have to explain your health to every new person you meet (like the dozen different doctors you’ve met over the years, possibly every nurse who takes your pulse and thinks it’s a little bit high). So xe did a shit ton of research on your condition, in order to reduce how much you need to explain. Sure, xe will still have questions, and there are always aspects that only you can tell xer, but it’s a nice gesture.
As for helping you destress, xe’s pretty much a mix of Bela and Miranda. You’ll get plenty of massages (because Ava has learned from personal experience what sort of touches help with which sorts of pain), but also some scientific insight on any noticeable patterns. Lots of holding you close and telling you that you’re the coolest person in the world, and that Ava feels beyond lucky to have you.
#alcina dimitrescu x reader#bela dimitrescu x reader#cassandra dimitrescu x reader#daniela dimitrescu x reader#donna beneviento x reader#mother miranda x reader#oc x reader#avaskian caldwell#j has ocs#re8 village#resident evil: village#hcs
237 notes
·
View notes
Link
As a teenager, Sylvia Plath vividly understood the extent to which her body steered her. "If I didn't have sex organs, I wouldn't waver on the brink of nervous emotion and tears all the time," she wrote in her journal in 1950. Ten days before her death, she had come to believe that "fixed stars/Govern a life." It turns out that Plath was probably right -- more right than she could have possibly known -- about her biology and her fate. But when Plath's journals were first published in 1982, what was most obvious about her was the supercharged nature of her emotions. Whatever causal agents may have been governing Plath's life, they were blown back by the force of her personality.
As unmistakable as were Plath's volatile emotions in the 1982 journals, the heavy editing of the text necessarily made it hard to discern the patterns to her moods. Even so, there did seem to be a detectable pattern, and it did not seem then, nor had it seemed to the people closest to her during the last years of her life, to be merely a function of temperament. In the weeks before her suicide, Plath's physician, John Horder, noted that Plath was not simply deeply depressed, but that her condition extended beyond the boundaries of a psychological explanation.
In a letter years later to Plath biographer Linda Wagner-Martin, Horder stated: "I believe ... she was liable to large swings of mood, but so excessive that a doctor inevitably thinks in terms of brain chemistry. This does not reduce the concurrent importance of marriage break-up or of exhaustion after a period of unusual artistic activity or from recent infectious illness or from the difficulties of being a responsible, practical mother. The full explanation has to take all these factors into account and more. But the irrational compulsion to end it makes me think that the body was governing the mind."
For at least the past 10 years it has been generally assumed that Plath fit the schema of manic-depressive illness, with alternating periods of depression and more productive and elated episodes.
The hypothesis that Plath suffered from a bipolar disorder is persuasive. But in late 1990, another, even more intriguing medical theory emerged. Using the evidence of Plath's letters, poems, biographies and the 1982 journals, a graduate student named Catherine Thompson proposed that Plath had suffered from a severe case of premenstrual syndrome. In "Dawn Poems in Blood: Sylvia Plath and PMS," which appeared in the literary magazine Triquarterly, Thompson theorized that Plath's mood volatility, depressions, many chronic ailments and ultimately her suicide were traceable to the poet's menstrual cycles and the hormonal disruptions caused by PMS.
Thompson pointed out that Plath unwittingly recorded experiencing on a cyclical basis all of the major symptoms of PMS, as well as many others, including low impulse control, extreme anger, unexplained crying and hypersensitivity. She also suffered many of the physical symptoms associated with PMS, notably extreme fatigue, insomnia and hypersomnia, extreme changes in appetite, itchiness, conjunctivitis, ringing in the ears, feelings of suffocation, headaches, heart palpitations and the exacerbation of chronic conditions such as her famous sinus infections.
Thompson compared Plath's reported mood and health changes with the journals, letters and biographies and found that her symptoms seemed to appear and disappear abruptly on a fairly regular schedule, with clusters of physical symptoms and depressive affect followed by dramatic changes in outlook and overall physical health. Those patterns can be directly linked to the dates of Plath's actual menses, particularly in 1958 and 1959, when she most habitually noted her cycles. Judging from the pattern of Plath's depression and health in late 1952 and in 1953 until her Aug. 24 suicide attempt, Thompson posited that "it seems reasonable to conclude that this suicide attempt was directly precipitated by hormonal disruption during the late luteal phase of her menstrual cycle and secondarily by her loss of self-esteem at being unable to control her depression."
Thompson showed that a well-known journal entry from Feb. 20, 1956, is clearly traceable to Plath's menses, to which she refers directly a few days later. The journal fragment takes on new meaning in light of having been written during the physically and emotionally debilitating luteal phase of Plath's cycle: "Dear Doctor: I am feeling very sick. I have a heart in my stomach which throbs and mocks. Suddenly the simple rituals of the day balk like a stubborn horse. It gets impossible to look people in the eye: corruption may break out again? Who knows. Small talk becomes desperate. Hostility grows, too. That dangerous, deadly venom which comes from a sick heart. Sick mind, too." On Feb. 24, the same day she notes in her journal that she has a sinus cold and "atop of this, through the hellish sleepless night of feverish sniffling and tossing, the macabre cramps of my period (curse, yes) and the wet, messy spurt of blood," Plath wrote a letter to her mother blaming her dark mood on her physical health: "I am so sick of having a cold every month; like this time, it generally combines with my period."
By the fall of 1962, the poems (which Plath carefully dated as they were completed) seem to follow a pattern of metaphorical renewals and optimistic transformations for roughly two to three weeks of artistic production, then jagged, seething accusations and aggression for a couple of weeks.
Thompson's PMS theory has been largely ignored by Plath scholars. But it immediately gained two important supporters: Anne Stevenson, Plath's controversial biographer, and Olwyn Hughes, Plath's former sister-in-law, whose letters were published in a subsequent issue of Triquarterly. Though oddly defensive in tone, Stevenson's letter does commend Thompson for her "invaluable contribution to Plath scholarship ... Certainly no future study of Plath will be able to ignore the probable effects of premenstrual syndrome on her imagination and behavior." And it states that she wishes she had been able to utilize Thompson's insights in the writing of her own work on Plath.
A letter from Olwyn Hughes also congratulates Thompson for her scholarship, but unlike Stevenson, Hughes practically stumbles over herself in amazement at the PMS theory. Hughes, who was quoted in Janet Malcolm's book "The Silent Woman: Sylvia Plath and Ted Hughes" as characterizing her long-dead sister-in-law as "pretty straight poison," wrote to Thompson: "It is quite a shock to digest all this -- after thinking for so long that Sylvia's subconscious mind was her prison, and to suddenly realise it may well have been in part, or wholly, her body. But it certainly tallies with Ted's mentions -- he has always felt some chemical imbalance was involved."
Hughes further points out that Ted Hughes had spoken of Plath's ravenous appetite just prior to her periods and asks, "I wonder if that is a known characteristic of PMS?" (According to the PMS literature, it is.) But most tellingly, Olwyn Hughes explains that "one of the reasons I was so bowled over by your piece is that Sylvia's daughter, very like her physically, suffers quite badly from PMS but is, in these enlightened times, aware of it and treats it."
Dr. Glenn Bair, one of the leading experts on PMS treatment and research in the United States, confirmed to Salon that PMS is typically passed from mother to daughter. In a rare interview about her parents, Frieda Hughes told the Manchester Guardian in 1997 that after the "collapse of her health," including extreme fatigue and gynecological problems, she underwent a hysterectomy in her 30s.
After a careful review of Thompson's article, of a seven-page monthly breakdown of Plath's symptoms for 1958 through 1959 and of the documented evidence of Plath's pregnancies and postpartum symptoms of 1959 through 1962, Bair said, "If you hack through the PMDD criteria, I think that you'll find that she fits the PMDD profile."
170 notes
·
View notes
Last Seen Blogs

joy-jpg
joy’s art repository

jpgrising
Phoenix Force Rising

joymask
sun following

sukamemek
Untitled

sociallynonexistant
Library in a Corner