#Informal education
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The average Tumblr user visits about 67 pages every month.
Text
Greetings, fellow travelers! 🌎
On this blog you will find wild stories, stunning photos, quotes, random gossip, whimsy & snark, from staff and visitors to:
Museums 🏛️
Science centers 🔭
Zoos 🐼
Aquariums 🦈
Botanical gardens 🌿
& related institutions.
I have some stories of my own to tell, and I want to hear about your experiences in these places, too!
About me: I just took early retirement after working for more than 25 years as the web designer, editor, and photographer for a natural history museum. I have a BA in anthropology and a master's in museum studies. I had graduate assistantships in the exhibits, entomology, and geology/paleontology departments of the university museum where I was working towards my degree. Before that, I worked as a sort of general assistant in a small science museum. Earlier still, I volunteered with the exhibits team at a science & nature center that also had a small zoo.
My parents were both scientists - mom was a high school biology teacher (and a botanist by training) and dad was a physicist. They both loved to travel, and we did a lot of that when I was a kid. We took a few cross-country road trips, and also took trips to Canada, France, the UK and Switzerland. I've done limited travel on my own to Germany and Denmark. I've been to museums and similar places on most of these trips. I plan to share my thoughts on those experiences here.
Please join me in exploring the world of museums!
#first post#museums#research#museology#science#science center#science museum#history#history museum#living history#art museum#museum studies#Children's museum#aquariums#botanical gardens#herbarium#nature center#zoos#Wildlife center#conservation#Informal education#Exhibits#Museum trips#travel#places to visit#cultural attractions#Museum history#museum humor#travel destinations
10 notes
·
View notes
Text
Wet Beast Wednesday: sea urchins
As I continue the slow grind of covering every living group of echinoderms for this series, it was inevitable that I would eventually encounter the only echinoderm I've actually studied. Sea urchins are among the most iconic of marine invertebrates, but many people just think of them as part of the scenery. I'm here to show you that there's more to these creatures than just being spiny lumps on a rock.

(Image: a purple sea urchin (Strongylocentrotus purpuratus) being held in someone's hand. It is a round, globular animal with a dark purple color. Light purple spines emerge from it all over its body, with the longest being around the middle. End ID)

(image: a long-spined sea urchin (Diadema savignyi). It is a black sea urchin with spines longer than its diameter. End ID)
Urchin is an old-fashioned word for hedgehog, and sea hedgehog is a fitting name for these round, spiny animals. Sea urchins tend to be fairly small, with a diameter of 3 - 10 cm (1 - 4 in), though some species have very long spines that make them seem larger. The main body of an urchin is round and enclosed in a (usually) hard shell called a test made of calcium carbonate. The test is covered with a slayer of skin and muscle that controls the spines and small, pincer-like structures called pedicellaria. Within the test are the internal organs. As with other echinoderms, sea urchins are radially symmetrical as adults, with five segments arranged around the center like pizza slices. The two main body holes are found on the top and bottom of the animals where the segments converge. At the bottom is the mouth and at the top is the anus. Each segment also has a hole near the anus used to release gametes and one will have a larger pore called the madreporite, which is used to control the amount of water within the urchin's body. The mouth is a unique structure known as Aristotle's lantern, consisting of five tooth-like structures (one for each body segment) that interlock together and sharpen themselves. Behind the teeth is a rasping tongue.

(image: a close-up of an urchin's mouth, showing the Aristotle's lantern. It is a hole surrounded by a fleshy lip. Five spade-shaped teeth are emerging from the edge of the hole. End ID)
Internally, most of the body is taken up by the digestive tract and water vascular system. The digestive system lacks a stomach, with the esophagus attaching directly to the small intestine. The digestive tract forms a loop as it passes through the body. The water vascular system uses seawater to form hydrostatic pressure that moves the tube feet. All starfish, urchins, and sea cucumbers have tube feet, small, transparent, tentacle-like structures they use for movement. Tube feet are hollow and retracted into pores on the skin normally. To be used, they have to be inflated with water, which makes them stick out of the body, where they can be controlled with muscles. Tube feet end in suction cups that can be used to grab into structures around them. Seawater drawn in through the madreporite serves as the source of pressure needed for the tube feet to function. In urchins, tube feet cover the body and are used for locomotion, moving food to the mouth, and moving objects on or off the body. The main body cavity is filled with circulatory fluid that uses special cells to move oxygen and nutrients around the body. The nervous system is simple, consisting of a central nerve ring around the esophagus that branches into nerves that connect to the rest of the body. Urchins have no eyes (except for the family Diadematidae, which have eyespots), but are sensitive to light. The gonads are usually small, but during mating season they can swell to fill much of the body cavity.

(Image: a drawn diagram showing a cross-section of a sea urchin, with the different organs and body parts labeled. End ID. Source)
Sea urchins are found in oceans worldwide, from intertidal zones to the deep sea and the tropics to the poles. They are bottom-dwellers who feed primarily on algae, which they scrape up with their teeth. However, they will also take a variety of food, including carrion, aquatic plants, and other slow-moving or sessile animals like sponges, polyps, bivalves, worms, and sea cucumbers. Urchins can play a key role in regulating algae populations through their ecosystems, but they also rely on predators to keep from overeating necessary algae. Famously, California's kelp forests were almost destroyed by urchins eating the kelp after their primary predator, sea otters, were driven to near extinction. Urchin's primary defense against predators is their hard tests and spines. As most of the edible portion of the urchin is within the test, predators have to get through both layers of defense first. The spines are hollow and each can be moved independently of each other, allowing them to be positioned toward a threat. Many species contain venom within their spines as an added layer of defense. This venom is rarely dangerous to humans, but can cause swelling and painful reactions. Another layer of defense is the pedicellaria, which are good at removing small animals and parasites from the skin. The flower urchin, Toxopneustes pileolus, has modified its pedicellaria into flower-like structures that extend beyond the spines and can deliver a sting that can be fatal to humans.

(Image: a flower urchin. It is a pinkish urchin covered with flower-like structures that extend to the length of the spines. It has placed some bits of shells on top of it. End ID)
Sea urchins possess distinct males and females, though the differences are internal, making it impossible to tell which is which based on visual examination. During mating seasons, the gonads swell as they generate gametes. Urchins tend to reproduce in groups at synchronized times (possibly correlated with the phases of the moon in shallow-water species) to maximize the possibility of fertilization. When ready to mate, the gametes are squeezed to empty their contents through the genital pores and into the water column. Sperm must find egg in the water to fertilize it. Most sea urchins provide no parental care, but in some species, the female will retain the eggs in her spines to protect them. The eggs hatch into bilaterally symmetrical larvae called plutei that drift with the plankton. As they develop, a section of the larvae will develop into a radially symmetrical adult rudiment. This piece will eventually break off and become the juvenile urchin while the rest of the larva dies. Because echinoderms start out as bilaterally symmetrical larvae, we can infer that they developed from bilaterally symmetrical ancestors and the radial symmetry of adults is a more recent development.

(image: a series of photos showing the embryological development of a sea urchin from a single cell to a cluster of cells, to a bell-like structure, to growing several arms, to the eventual adult developing and breaking off. End ID. Source)
Fossils show that the oldest sea urchins had large, club-like spines that they walked on, with the modern spines being a later development. Most of those urchins died out with the dinosaurs, leaving the pencil urchins of order Cicaroida as the only living members. All other living urchins are Part of the clade Euechinoidea. Amongst them, there are still some oddballs, known as the irregular urchins of clade Irregularia. These urchins have moved away from radial symmetry, with less symmetrical segments and the anus and mouth moving from being on the top and bottom to being on the sides in the heart urchins. Heart urchins have gone from bilateral symmetry to radial symmetry and are now going back to bilateral symmetry. Heart urchin mouths don't have an Aristotle's lantern. Instead, they use strands of mucus to capture food and cilia to pull the strands back inside. Sand dollars, also known as sea cookies or sea biscuits, are also in this clade. These are flattened urchins with short and very fin spines that resemble velvet. They are burrowers who spend much of their time buried under sand and as such are rarely seen alive. The name sand dollar comes from their tests, which are similar to old dollar coins and can often be found washed up on beaches. While still radially symmetrical, sand dollars also have a secondary form of bilateral symmetry, with a distinct front and back end that often look different. Irregular sea urchins also tend to have fewer gonads and associated pores than regular sea urchins.

(image: a red pencil urchin (Heterocentrotus mamillatus) nestled among coral. Instead of spines, it has a series of long, thick, red clubs. End ID)

(image: a purple heart urchin (Spatangus purpureus). It is an urchin elongated on one direction and with a few rows of long spines amongst short ones. On the surface facing the camera is a large hole that could be the mouth or the anus. End ID)

(image: a group of irregular sand dollars (Dendraster excentricus) partially buried in the sand. They are round, flat animals with a velvety covering of tiny spines. The are sticking out of the sand. End ID)
Sea urchins have been known to humans for as long as people have lived near the ocean. Stings can occur when people step on them and can cause pain and irritation, but are rarely medically significant. That being said, some people can have allergies to the venom, which could be a big problem. Spines left in the wound should be removed, as they can continue injecting venom. Urchins are a food source for people around the world, specifically the gonads, which are the only meaty part of the animal. The gonads are often marketed as roe or corals and can be eaten raw or cooked. Urchins are also used as a model organism in embryology due to the interesting and well-studied nature of their larval development. Urchins are vulnerable to pollution, habitat loss, and over-predation. Ocean acidification due to climate change poses a major threat to them, as it reduces the quality of their tests.

(image: tow sea urchins served as food. They are upside-down with the bottoms removed. The gonads are visible within as five orange, spongy structures that take up most of the body cavity. End ID)
#wet beast wednesday#sea urchin#urchin#sea urchins#echinoderms#invertebrates#invertiblr#sand dollar#heart urchin#pencil urchin#marine biology#marine life#biology#zoology#ecology#animal facts#informative#educational#image described
706 notes
·
View notes
Text
Fish of the Day
Today's fish of the day is the collared carpet shark!

The collared carpet shark, also known by scientific name Parascyllium collar is the best known shark in genus Parascyllium.The name is derived from para an old greek word meaning dog shark or small shark, and collare, a latin word for iron band or neck chain. These sharks are in the carpet shark family, which are known for their often bottom dwelling ways, spiracles (a kind of respiratory opening) behind the eyes. The family of Parascylliidae, which genus Parascyllium makes up one half of, is defined by their small size and barbels (a whisker-like appendage) behind the chin.Collared carpet sharks in particular are found around the Southwestern Pacific, specifically focuses on the continental shelf of Eastern Australia. Found from a range of 26°S through 38°S, and 149°E to 154°E, these sharks live in temperate to subtropical zones. Their habitat is best known as reef like zones, which their bodies are adapted towards, but can comfortably spend time in sandy bottomed areas as well.


Collared carpet sharks are long and elongated, which helps them in the rocky crevices they live around. Along with fins and a tail that are proficient from balancing and navigating the uneven seabed. These fish are covered in spots, which blend them into both rocky and sandy areas. With a nocturnal lifestyle, the collared carpet shark is known for sneaking up on prey, and lunging at them. They have a diet made of fish and invertebrates, with specially shaped mouths and teeth that are made for hunting prey that hides in and around rocky fissures.

These sharks are relatively unknown when it comes to reproduction and lifecycle, with an unknown life span and maturity age. Collared carpet sharks live solitary lives, and we know little to nothing about any mating season, preference, or time span. Similar to many other carpet sharks, the collared carpet shark is oviparous, meaning that the shark is fertilized and the egg is laid before hatching. These eggs are attached to seaweed, or other vegetation before being abandoned by the parents, leaving young to fend for themselves once they hatch. This is all currently known information about the shark, and they are threatened by fishing bycatch, water pollution, and coral bleaching caused by rising temperatures and stress.

That's the collared carpet shark everybody! I hope you enjoyed learning about them, and have a wonderful day!

#fish#fish of the day#fishblr#fishposting#aquatic biology#marine biology#freshwater#freshwater fish#animal facts#animal#animals#fishes#informative#education#aquatic#aquatic life#nature#river#ocean#coral#coral reef#collared carpet shark#carpet shark#shark
439 notes
·
View notes
Text
Prompt 271
“Grandmother is visiting,” Damian suddenly said with no warning and with his usual not-quite demanding tone.
“Who?” Tim wasn’t the only one to startle, seeing as Bruce had practically froze, a downturn to his lips in a silent show of confusion.
Damian scowled. “Are you deaf Drake? Grandmother is coming to Gotham to, quote, make sure I am being properly cared for.” None of them had known that Ras was with anyone actually. At least Tim was pretty sure that would have been in the files.
“Oh?” Dick didn’t quite crouch to Damian’s height but it was a near thing. “She-” “He,” Damian corrected, interrupting him. They all exchanged a glance before Dick continued.
“Is he coming to the Manor or…”
Damian scoffed again, a tiny bit of a flush against his face. “No, Grandmother will most likely be staying with Akhi-”
Now wait one moment-
“YOU HAVE ANOTHER BROTHER?!”
#DCxDP#DPxDC#Prompts#Deadly Decisions#Danny & Ras are the homoerotic rivals that no one knows if they’re flirting or attempting a murder#It’s actually both they’re just also both Immortal#Danny to Jason: You can become a crime lord if you finish college- you’ve said you wanted to get a degree this is ur chance#Dusan (nodding): Mother has made all of us finish at least our basic education nephew#Why yes this does mean that RH has just made the heads in a duffel bag debut & the bats have no clue it’s Jason#Normally Danny wanders the universe but RAS (affectionately derogatory) HOW DARE U TRY TO HIDE THE GRANDCHILDREN#Morally Gray Danny#He’s well over 300 and that has an affect lol#Also has some fun fae vibes thx to his ghost half & human half finally balancing out#Let Jason & Damian be brothers#Tiny Damian: Akhi look I found a frog :>#Jason (newly not brain damaged & has no clue who this small child is): …. That’s great#Tiny Damian: *GASP* Akhi you can talk now :D#Fuck it- all the Al Ghuls deserve fangs from ecto contamination#Is Danny actually Dusan & Talia’s mother? No one knows and no one wants to ask the probably immortal fae being okay#Danny brought Damian a ghost hound puppy & Jason an original signed Pride & Prejudice book#How come Bruce wasn’t aware of Danyal? Talia forgot to inform him that the mother she was speaking of is in fact still alive#He disappears for a decade sometimes longer she was using past terms how was he supposed to know
3K notes
·
View notes
Text
FREE CONGO 🇨🇩
We have to talk about Congo as well, they are so in need of our awareness that they’re setting themselves on fire because no one cares enough !
Resources
#free Congo#news#current news#current events#educate yourself#stay informed#the democratic republic of Congo#fire#free oppressed people#Congolese#blm#black lives matter#black people matter#boycott apple#boycott Samsung#boycott technology#pro palestine
3K notes
·
View notes
Text
Repeat after me: kink is not a "gateway" to committing a crime.
#ki/nk#queer#queer liberation#kink education#leather pride#pride#lgbtq#consent#kink safety#sex ed#trans#transsexual#transgender#kink at pride#lgbtq issues#lgbt pride#sex and relationships#sex and sexuality#sex education#sex positive#sex positivity#kink positive#kink positivity#kink advocacy#kink informed#leather love#leather dyke#anti censorship#pro kink#pro sex work
849 notes
·
View notes
Text
To all the people who think aspec people aren't LGBTQIA+ because we aren't "discriminated against enough", here's a lovely list of reasons why you need to educate yourself:
- We suffer from dehumanisation, people actively devaluing or even erasing our humanity because of our identities (The voidpunk community is heavily supported by aspec people because of this)
- We suffer from self hatred due to feeling as if and being told we are broken, that no one can be happy unless they're in a romantic/sexual relationship, because of allonormativity and amatonormativity that actively damages our mental health
- Amatonormativity shapes laws that put us at an active disadvantage, such as giving married people financial and legal benefits
- Aspec people have been victims of conversion therapy, correctional rape, a lower quality of life, and other effects of being a marginalised and oppressed group
- We suffer from our identities being pathologised and deal with medical stigma because of this, causing many of us to feel unwelcome in and even avoid health care settings
- We suffer from our identities being erased, which can range from people completely denying our existence and people equating it to celibacy, to an almost complete absence of aspec representation in the media (It's been getting better lately, especially for alloaces and aroaces, but I have yet to ever see a canon aroallo character, and representation for those on the spectrum rather than in the extremes is often ignored)
- YOU are creating a hateful, exclusionary space in a community meant to be about inclusion. The same thing that happens to us happens to bisexual people, to polyamorous people, and other identities that are "disputed." In a community meant to be about rejecting the norm, YOU are shoving us out because we don't fit the norm of being LGBTQIA+. Because we're not enough like you.
These are only a few examples of aphobia that people like me deal with. Discrimination and oppression against aspec people stretches far beyond this.
But even if it didn't, it is disrespectful and harmful to everyone involved to gatekeep membership in the community based on oppression and discrimination.
We aren't LGBTQIA+ because we experience oppression. We are LGBTQIA+ because our existence alone goes against heteronormativity and other societal norms forced upon us.
#lgbtq#lgbtqia#aromantic#asexual#aromanticism#asexuality#ace#aro#aspec rights#aspec#aro pride#aroace#arospec#ace pride#ace rights#acespec#aro rights#this has been a psa#psa#information#important psa#aroaceprideispridetoo#we are enough#allonormativity#amatonormativity#discrimination#aspec discrimination#oppression#inclusion#educate yourself
1K notes
·
View notes
Text
i had a friend who was raped as a teenager and had a really strict mum who did not let her go out so she was really lonely. when she turned 18 she started going clubbing and since we live in a city with a big fetish scene, she started going to the kinky venue. since she was young, naive and very pretty, she was immediately roped in by older men who did bondage shootings with her and everything. she started working in the club. to me, she was clearly groomed, but she works in a fetish shop now and is fully immersed in the scene
i have a friend who answered a job ad for a secretary when she was abroad and she and her friend ran out of money but when they arrived there it was a brothel. they both prostituted themselves for several months. they were only 18. she still talks highly of that brothel, how clean and safe it was, and wants prostitution to be legal
i read the gut wrenching biography of a thai woman who ran away from home, whose parents refused her education and treated her brother very preferably while openly hating her, and entered prostitution in sex tourist destination pattaya at only 13. she was paid by men in their 50s first for her virginity, then to piss on her. she exited at 19 and developed psychosis. she defends sex buyers, hates feminists and wants prostitution to be legal
do you see where im going with this? brainwashing is real. despite the obvious facts, the grooming, the system that pushed and pulled them, the men taking advantage of them; they defend it. so yeah, we shouldnt dismiss firsthand testimony and personal experience, but always take it with a grain of salt, always contextualise, always see it as one part of a bigger picture. liberals dont do that and have duped too many people into not doing it either. „if thats her choice its none of our business“ fuck you!
#there are so many more examples from the women in the sex industry who defend it in my notes alone#mine#there were and are women who dont want women to have the right to education to vote to work etc#even if it was denied to them as well#the thing is no group is a monolith and you cant just say ‚listen to x group‘ because#there will be differences within x group so you need to form your own opinion#based on all the information you can geg
1K notes
·
View notes
Text



This afternoon, read CURSE/KISS/CUTE, my illustrated web novel for queers 18+. Features include:
hope
flirting
emotions
the inherent sexiness of change
vaguely scary deep lore (also sexy)
forcefem (woke)
jokes
It's literally free: www.dicot.moe/ckc
339 notes
·
View notes
Text
idk when people started saying antinous (of Ithaca) was younger than telemachus. i mean you can google how old antinous was but
dates fucked
"Greek youth from Bithynia"
"lover of the Roman emperor Hadrian"

this is antinous of Rome!!!!! antinous of ithaca was likely mid 20s-early 30s
#not in a disparaging manner#ik its a misread a lot of the time but ive seen people kinda spread it around in informal educational contexts#esp under epic content#the ages could be different in epic so maybe hes can be a little bit younger? but that is Not a 19 year old#ochi orates#antinous#epic the musical#the odyssey#greek mythology#tagamemnon
251 notes
·
View notes
Text
Intersex Guide!
(UPDATED: April 4th, 2025. Please reblog again if you only saw our old version. Please also reblog if you've never seen this before, to spread awareness.)
Hello and happy pride! We wished to share a passion project we have been working on for months - a guide to intersex traits and variations!
Now, a question that many ask - what is intersex? Well, we will be answering that question for you here! Anything on this post that is written in red is NOT intersex, so if you wish to skip over any of it, you can. And if you wish to get straight into the intersex types, scroll down to the read-more and start from there.
Intersex, also known as the intersex spectrum, is a term used to describe when someone's biological sex - as in the sex they are born with/what they naturally develop during puberty - is not clearly defined as the typical male or female sex traits.
(This does not include someone that was born male or female, and later chose to have their sex traits changed due to being transgender, transsex, or altersex. It also does not include males that experienced circumcision/dorsal slits or penis splitting, females that experienced genital mutilation, or males & females that indulged in modifications such as piercings and beading.)
This only applies to primary sex traits - chromosomes, genitals, reproductive organs, hormones, and hormone responsiveness. Atypical secondary sex traits (breasts, muscle tone, body/facial hair, deepness of voice) do not make someone intersex unless it is paired with "abnormalities" in primary sex traits.
Before you can understand what it means to be intersex, first we must clarify what it means to not be intersex.
A typical male has XY chromosomes, a penis, two testicles within the scrotum, a prostate, and more androgens (mostly testosterone) than females. Upon puberty, they usually (but not always) develop more facial hair & muscle tone than females, and a deeper voice than females.
(Note: A penis has a phallus, a scrotum beneath the phallus, foreskin protecting the head of the phallus, and a urethra on the head of the penis. It is straight or slightly curved when erect.)
A typical female has XX chromosomes, a vulva, two ovaries, a single uterus, and more estrogen than males. Upon puberty, they usually (but not always) develop larger breasts and wider hips than males.
(Note: A vulva has two labia, a single pea-sized clitoris, a single vaginal entry, and a urethra above the vaginal entry and under the clitoris.)
Here is a list of non-typical sex traits that, by themselves, are not intersex.
Accessory Breasts (Polymastia): Having more than two breasts. Accessory Nipples (Polythelia): Having more than two nipples. Athelia: Having only one nipple, or no nipples at all. Amastia: Having only one breast & nipple, or no breasts & nipples at all. Breast Hypertrophy/Macromastia/Gigantomastia: Having extremely large breasts Gynecomostia: Breasts on a male. The reason this is not considered intersex is because all sexes (except for people with amastia) have breast tissue, which can vary in size regardless of sex. Females can have small breasts, and males can have larger breasts than is expected. Hypotonia: Low muscle tone. Bicornuate Uterus: A heart-shaped uterus. Septate Uterus: A uterus that internally has a partition down the middle. Macropenis: A penis that is 7 inches/17.78 centimeters or larger. Macroorchidism: Testicles that are 4 milliliters or above pre-puberty, and above 30 milliliters as an adult. Macrovagina: A vagina that is deeper than 5 inches/13 centimeters. Labial Hypertrophy: Labia that is longer than average (above 2 inches/5 centimeters)
Now, onto the intersex spectrum! First, some notes.
-An intersex trait is a singular atypical trait. For example, someone with ambiguous genitals, but no other "abnormality" has an intersex trait. -An intersex variation is when multiple atypical traits are present, with at least one of them being an intersex trait. For example, someone with ambiguous genitals and fused kidneys has an intersex variation. Equally, someone with ambiguous genitals and cryptorchidism also has an intersex variation. -CTF stands for "close to female." CTF traits are characteristics that are closely associated with females (vulvas, uteruses, ovaries, estrogen as the main sex hormone, breasts, widened hips, XX chromosomes, etc.) CTF people are intersex people who call their body as a whole CTF, due to a majority (but not necessarily all) of their sex traits being CTF (ie; a person with breasts, a uterus, ovaries, and a penis might call themself CTF, even though not all of their traits are CTF in nature.) -CTM stands for "close to male." CTM traits are characteristics that are closely associated with males (a penis, testicles, androgens as the main sex hormones, increased hair growth, higher muscle mass, a deepened voice, XY chromosomes, etc.) CTM people are intersex people who call their body as a whole CTM, due to a majority (but not necessarily all) of their sex traits being CTM. -CTA stands for "close to androgynous." CTA traits are characteristics that are predominantly "androgynous", or an equal mix of "feminine" and "masculine" (ie; ambiguous genitals, ovotestes, XXYY chromosomes, etc.) CTA people are intersex people who call their body as a whole CTA, due to a majority (but not necessarily all) of their sex traits being CTA, or they have a near-equal mix of CTF and CTM sex traits. -CTN stands for "close to neutral." CTN traits are characteristics that are predominantly "neutral" (ie; small/absent/blocked off genitalia or reproductive organs, a lack of hormone production, 0X chromosomes, etc.) CTN people are intersex people who call themself CTN, due to a majority (but not necessarily all) of their sex traits being CTN.
Also, when we state that an intersex trait/variation is "fairly common", we mean that it is fairly common amongst the intersex population, not that it is fairly common in the general population. Being intersex is still classified as "rare" statistically speaking (as statistics define "rare" as 1 in 1,000 people.)
So for the sake of this post, here is how we are classifying the following:
"Fairly common" = 1 in every 5,000 (or less)
"Rare" = above 1 in every 5,000, up to 1 in every 100,000
"Extremely rare" = above 1 in every 100,000
Keep in mind that "may co-occur" means that not all of the features will be present on every single person with that variation; in fact, none of the extra features could be present. However, for chromosomal variations specifically, it is highly likely that at least 1-5 (or more) of the listed extra features will be present.
And finally, when we say that "fertility is average", what we mean is that the gonads are fully capable of producing healthy average numbers of sperm/eggs, and/or the uterus is capable of carrying healthy babies. Struggles with the sperm reaching the eggs still might occur, but if direct insemination is done (as in the sperm is directly injected), then pregnancy should occur perfectly fine.
-------------------
Penile Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the penis.
Congenital Chordee: An trait in which an individual is born with a curved penis. This curve may be on its own, or it may be curved due to webbed-skin on the scrotum connecting to the penis and holding it in a curved manner. As a lone variation, those with congenital chordee have XY chromosomes, testicles, and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 200 AMAB births.
-
Penoscrotal Transposition (PST): A trait in which an individual is born with a scrotum that is in front of the penis, rather than beneath it. A Shawl Scrotum/Donut Scrotum is a form of PST where the scrotum completely surrounds the penis like a shawl. As a lone variation, those with PST have XY chromosomes, testicles (possibly cryptorchidism, in which case the scrotum surrounding the penis is full of empty tissue), and a prostate. They may also have hypospadias. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include absent kneecaps, ureter abnormalities, an absent or underdeveloped kidney, heart disease, overgrown/protruding ribs, widely-spaced nipples, an incurved pinkie finger, a small lower jaw, a chin dimple, folded eyelids, a large/protruding back of the skull, cerebral atrophy, and intellectual disability.
-
Diphallia/Bifid Penis: A trait in which an individual has two penises (either next to each other or one on top the other.) These penises could be of the same size, or have a size difference. A urethra may be present on only one penis (possibly with epispadias or hypospadias), both penises, or they may have a single urethra that is in-between both the two penises. Erections may be possible in both penises or only in one. As a lone trait or variation, those with diphallia have XY chromosomes, testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra efficiently, depending on the urethra's placement. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include pubic bone abnormalities, an extra hole (not an anus) that leads into the rectum, an absent anus (which will need surgical intervention in order to pass waste), two colons, an extra ureter, fused kidneys, an extra kidney, a rotated kidney, an inguinal hernia, gastrointestinal abnormalities, an extra gastrointestinal tract, exposed organs on the lower abdomen, heart abnormalities, spinal abnormalities, and an absent thumb.
-------------------
Urethral Traits/Variations (not including those on the agenital spectrum)
These are traits that affect the development of the urethra.
Urethral Duplication/Double Urethra: A trait in which an individual with a singular set of genitals has two urethras. One of the urethras may not fully reach between the bladder and genitals, either cutting off before reaching the bladder (making it visible from the outside, but without a use), cutting off before reaching the genitals (making it connected to the bladder, but not visible or accessible from the outside), or cutting off in the middle (making it connected to the bladder, and visible from the outside, but a blockage existing somewhere in the middle internally.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (usually with epispadias for one or both of the urethras, however the urethras could be side-by-side as well) or clitoromegaly & fused labia, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis (usually with hypospadias or epispadias for one of the urethras, though both can be side-by-side on the penis head), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status of this variation, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include an extra ureter, an extra bladder, urinary tract infections, an extra rectum, an extra colon, an absent kidney, an abnormally-located kidney, kidney cysts, spinal abnormalities, and an opening between the windpipe and the esophagus.
-
Hypospadias: A trait in which an individual with a penis is born with a urethra that is located lower than typical. This could be lower on the head of the phallus than typical, or it could be on the shaft, the scrotum, or even underneath the phallus. As a lone variation, they have XY chromosomes, a penis/micropenis (possibly with chordee or PST), testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. They can produce semen, but it may not be able to exit the urethra depending on its placement. Fertility is average. This trait is extremely common, occurring in 1 of every 250 AMAB births. Vulval Hypospadias/Hypospadias Feminis is an extremely rare form of hypospadias that occurs on vulvas, in which a urethral opens on the vaginal wall. As a lone variation, those with vulval hypospadias have XX chromosomes, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the rarity, little is known about the fertility status of vulval hypospadias.
-
Epispadias: A trait in which an individual is born with a urethra that is located higher than typical. On a penis, this refers to a urethra that is located above the typical spot on the penis head. Ona vulva, the urethra is on the stomach or above/in the middle of the clitoris (thus splitting the clitoris into two.) As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is extremely rare. A common trait/disability that may co-occur is exposed organs on the lower abdomen.
-
Urogenital Sinus Anomaly (UGS)/Persistent Urogenital Sinus Anomaly (PUGS): A trait in which an individual has a single opening, which is a combination of both urethral and vaginal tissue, and connects to both the urinary tract and the reproductive tract. This opening could be the size of a typical vaginal entry, the size of a urethra, or somewhere in-between. As a lone variation, those with UGS have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare.
-
Persistent Cloaca: A trait in which an individual has a single opening for urination, menstruation/sexual output, and feces (being a combination of the urethra, vaginal entry, and anus.) This opening could be the size of a typical vaginal entry, the size of a urethra, the size of an anus, or somewhere in-between. It could be placed anywhere from the crotch to between the buttocks, or somewhere in the middle. Partial cloacas may occur as well, in which the anus and the vagina are combined but the urethra is still separate, or the anus and the urethra are combined but the vagina is still separate. As a lone variation, those with persistent cloacas have XX chromosomes, a vulva or clitoromegaly & fused labia, two ovaries/one ovary (unilateral ovarian agenesis) or ovarian agenesis, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. If they have a uterus and a partial cloaca, they may have a double cervix, with one cervix in each opening. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no ovaries, an embryo implant will be necessary. Alternatively, if they have no uterus or a uterus that is too small for pregnancy, but have ovaries, their eggs can be used to implant an embryo into another carrier. This trait is rare. Common traits and disabilities that may co-occur include a dilated colon, a dilated vaginal entry, urine buildup (which may cause a stretched/swollen kidneys or ureter), an absent kidney, an oddly-placed kidney, heart defects, a tethered spinal cord, and an underdeveloped esophagus.
-------------------
Ambiguous Genitals
These are traits in which a person was born with a combination of vulval and penile characteristics. Micropenises are often considered a part of this spectrum.
As a lone trait, this can come in a CTA, CTF, or CTM form.
The CTA form can have any mix of gonads, reproductive organs, hormone production, and puberty. Typically they either have XX or XY chromosomes, however occasionally they may have a chromosomal variation as well.
Those with the CTF version have XX chromosomes, two ovaries (or ovotestes), and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips.
Those with the CTM version have XY chromosomes, testicles (or ovotestes) and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice.
Ambiguous genitals are fairly common, occurring in 1 of every 5,000 births.
Bifid Scotum: A form of ambiguous genitalia where a penis is present, however the scrotum is separated in a labia-like fashion around the phallus. Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia is fused in a scrotum-like fashion. The fused labia either covers the entirety of the vulva (leaving only the clitoris) exposed, or half of the vulva (leaving the clitoris & urethra exposed, but the vaginal opening mostly or fully hidden.) There may be tissue within the labia that appears like small testicles. Clitoromegaly: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged, being over 1 inch (2.54 centimeters) in diameter. In some cases, it looks like a small penis. Combined Clitoromegaly & Fused Labia: A form of ambiguous genitalia, where a vulva is present, however the labia fuses to resemble a scrotum and the clitoris is enlarged, creating a structure almost identical to a small penis. The vaginal opening is fully hidden under the labia. Pseudophallus: A form of ambiguous genitalia, where a vulva is present, however the clitoris is enlarged significantly (beyond the typical clitoromegaly expectations) and is merged with labia, creating a significantly-sized penis-like structure. Penis & Vulva Combo 1: A form of ambiguous genitalia where a vulva is present, however the labia stretches up and merges with a penis, becoming the outer skin & foreskin of the phallus. The penis is located where the clitoris usually is (thus replacing the clitoris.) No scrotum or descended testes are present. The urethra is on the vulva, below the penis. Penis & Vulva Combo 2: A form of ambiguous genitalia where there is a penis (with no scrotum or descended testicles) that has a vulva underneath it. The vulva has labia (which is not merged with the penis) and a vaginal opening. It may also have a clitoris beneath the penis as well. The urethra is on the vulva, below the penis. Penis & Vulva Combo 3: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles) that has labia (which is not merged with the penis) and a vaginal opening, but no clitoris. The urethra can either be on the tip of the penis or on vulva beneath it. Penis & Vagina Combo: A form of ambiguous genitalia where there is a penis with a scrotum (possibly with descended testicles) that a vaginal entry tucked beneath the scrotum.
It is important to note that the term Clitorophallus is often used as an umbrella term to describe micropenises, clitoromegaly, combined clitoromegaly & fused labia, and pseudophalluses.
-------------------
The Agenital Spectrum/Agenital/Agenitalia
These are traits in which a person was born with absent, small, or closed off genitals. Anorchia & Monoorchidism fall under this umbrella as well.
Urethral Agenesis: A trait or variation in which an individual is born without a urethra. It may be visibly absent, or it may appear to be present from the outside, with a blockage of skin being within the first few centimeters or inches internally. A urethra is necessary to be surgically added, as to avoid urine buildup. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) Common traits and disabilities that may co-occur include limb deformities, an anus covered by skin (which will need surgical intervention in order to pass waste), urine buildup (which may cause a stretched/swollen kidneys or ureter), an abnormal connection between the bowel and bladder, an absent bladder (which will need surgical intervention in order for urine to have somewhere to be collected), a small kidney, kidney cysts, an underdeveloped lung, an enlarged chamber of the heart, and heart issues.
-
Urethral Hypoplasia: A trait in which an individual is born with a narrow or underdeveloped urethra. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average (implying those with testes can produce sperm, and those with a uterus can get pregnant.) This trait is rare.
-
Vaginal Hypoplasia: A trait in which an individual has a vaginal opening that is small/tight or not very deep. As a lone variation, those with vaginal hypoplasia have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible if they have a uterus that is present and large enough. If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 5,000 AFAB births.
-
Vaginal Agenesis/Vaginal Aplasia: A trait in which an individual has some or all of the external vulva (clitoris, labia, & urethra), but no vaginal opening. As a lone variation, those with vaginal agenesis have XX chromosomes, two ovaries, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry. Pregnancy is possible if they have a uterus that is present and large enough, however sperm will need to be medically injected (unless they have a vaginal entry created surgically.). If they have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring in 1 of every 4,000 AFAB births.
-
Imperforate Hymen: A trait in which an individual has a hymen that completely covers the vaginal opening. As a lone variation, those with imperforate hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. Pregnancy is possible, however embryos will need to be medically implanted (unless they have the hymen removed surgically.) This trait is fairly common, occurring in 1 of every 1,000 AFAB births.
-
Microperforate Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only one tiny hole in the hymen. Cribriform Hymen: A trait in which an individual has a hymen that fully covers the vaginal opening, with only multiple tiny holes scattered across the hymen. Septate Hymen: A trait in which an individual has a hymen that stretches across the middle of the vaginal opening, making it appear as though there are two (or more) vaginal entries (when in reality, every hole leads to the same vagina.) As lone variations, those with microperforate hymens, cribriform hymens, or septate hymens have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the hymen. All three of these variations are fairly common, with each (separately) occurring in 1 of every 1,000 AFAB births.
-
Vaginal Septum: A trait in which an individual has a vaginal opening that is partially or fully blocked by skin tissue (which is not a hymen.) A Transverse Vaginal Septum (TVS) is when the tissue runs horizontally across or within the vaginal cavity, dividing or blocking it. Depending on how deep or wide this tissue is within the vagina, it may cause the vagina to seem short/small (due to blocking the vagina mid-way), may make the cervix seem absent (due to covering the cervix), could split the vagina into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally), or could be covering the entrance to the vagina altogether. An Obstructed Hemivagina is when the tissue runs vertically across/within the vaginal cavity, and curves to block part (but not all) of the vaginal entrance, leaving one side open. This might cause the vagina to seem short/small, and might cover the cervix. It may be obvious externally or only noticeable internally. This trait almost always partners uterus didelphys, blocking menstrual output from one of the two uteruses. A Longitudinal Vaginal Septum (LVS) is when the tissue runs vertically across/within the vaginal cavity, splitting it into two entryways (creating a double vagina, which may be obvious externally or only noticeable internally.) As a lone variation, those with vaginal septums have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the holes being too small or absent, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to remove the tissue. This trait is rare.
-
Labial Hypoplasia: A trait in which an individual with a vulva is born without one or both labia. As a lone variation, those with labial hypoplasia have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Clitoral Hypoplasia: A trait in which an individual has a vulva with a small clitoris (under 0.75 inches or 1.90 centimeters.) As a lone variation, those with clitoral hypoplasia have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare.
-
Penile Agenesis/Penile Aplasia: A trait in which an individual who is expected to have a penis is born without one. They either have urethral agenesis, a lone urethra, or a persistent cloaca. As a lone variation, those with penile agenesis have XY chromosomes, two testicles/one testicle (monorchidism) or anorchia, and a prostate. If they have testes, cryptorchidism is common. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone, and will likely have increased body/facial hair, higher muscle mass, and a deepened voice. If testes are present, they can produce semen, but it may not be able to exit the urethra/cloaca depending on its placement and how the testes connect. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include twisted feet, an absent anus (which will need surgical intervention in order to pass waste), anal abnormalities, bladder abnormalities, small kidneys, kidney cysts, urine buildup (which may cause a stretched/swollen kidneys or ureter), a hole between the heart chambers, small lungs, a connection between the windpipe and esophagus, a flat nose, and rotated ears.
-
Congenital Buried Penis/Congenital Hidden Penis: A trait in which an individual is born with a penis that is mostly or entirely hidden within the skin of the abdomen, thigh, or scrotum. As a lone variation, those with congenital buried penises have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is fairly common, with the exact estimates unknown.
-
Aposthia: A trait in which an individual is born with a penis that has very little or no foreskin. As a lone variation, those with aposthia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Microorchidism/Testicular Hypoplasia: A trait in which an individual is born with one or multiple testicles that are smaller than average. Microtestes are 14 milliliters or less in adults, 3 milliliters or less during puberty, and under 1 milliliter pre-puberty. As a lone variation, those with microorchidism XY chromosomes, two testicles (possibly with cryptorchidism), a penis/micropenis or ambiguous genitals, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome.
-
Cryptorchidism: A trait in which an individual is born with one or multiple testicles that are undescended (within the body, rather than hanging in the genital area.) This trait only counts as intersex if the testicles do not descend within the first 3-6 months after birth. As a lone variation, those with cryptorchidism have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is extremely common, occurring in 1 of every 100 AMAB births, however it can also occur in AFAB and AXAB/UAB individuals too. A common trait/disability that may co-occur is testicular cancer.
-------------------
Gonadal Agenesis
These are traits that cause one or both gonads to be absent.
Common traits and disabilities that may co-occur with gonadal agenesis include an absent kidney, kidney swelling, and kidney stones.
Anorchia/Bilateral Congenital Anorchia/Testicular Agenesis: A trait in which an individual that is expected to have testicles instead has no gonads. As a lone variation, those with cryptorchidism have XY chromosomes, a penis/micropenis or ambiguous genitals (which may have a urogenital sinus anomaly or a hole between the urethra & vagina) or penile agenesis, and a prostate. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile. This trait is rare.
-
Monorchidism/Monorchism/Unilateral Congenital Anorchia: A trait in which an individual is born with a single testicle. As a lone variation, those with monorchidism have XY chromosomes, a penis, possibly cryptorchidism, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This trait is fairly common, occurring in 1 of every 5,000 AMAB births.
-
Unilateral Ovarian Agenesis: A trait in which an individual is born with a single ovary. As a lone variation, those with unilateral ovarian agenesis have XX chromosomes, a vulva, and a uterus/unicornuate uterus or MRKH syndrome. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. They are at a higher risk of infertility. If they are fertile enough, and have a uterus that is large enough, pregnancy is possible. If they are fertile enough, and have no uterus or a uterus that is too small for pregnancy, their eggs can be used to implant an embryo into another carrier.
-
Ovarian Agenesis/Bilateral Ovarian Agenesis: A trait in which an individual that is expected to have ovaries instead has no gonads. As a lone variation, those with ovarian agenesis have XX chromosomes, a vulva, and a uterus (possibly with uterine hypoplasia) or MRKH syndrome. They will not begin puberty unless they are on HRT. Due to the lack of gonads, they are infertile, however if they have a uterus (and it is large enough), they can carry a (genetically unrelated) embryo if it is medically implanted. This trait is rare.
-------------------
Other Reproductive Traits
Gondal Dysgenesis: A trait in which an individual is born with a gonad (ovary, testicle, or ovoteste) that is full of empty tissue, rather than reproductive tissue. These are known as "streak gonads." If a person has two streak gonads, they will not begin puberty unless they are on HRT, and will have no eggs or sperm. XX Gonadal Dysgenesis/Pure Gonadal Dysgenesis (PGD) is a form of gonadal dysgenesis, in which an individual with XX chromosomes is born with two streak ovaries. They have a vulva or clitoromegaly and a uterus. They will not begin puberty unless they are on HRT. Due to the lack of eggs, they are infertile, however they can carry a (genetically unrelated) embryo if it is medically implanted. Swyer Syndrome and Mixed Gonadal Dysgenesis fall under this umbrella, and Turner Syndrome often does as well. All forms of gonadal dysgenesis are rare, except for when it occurs in Turner Syndrome.
-
Ovarian Hypoplasia/Hypoplastic Ovaries: A trait in which an individual is born with one or multiple ovaries that are smaller than typical. Unilateral Ovarian Hypoplasia is when an individual is born with one ovary that is smaller than typical. Bilateral Ovarian Hypoplasia is when an individual is born with both ovaries being smaller than typical. As a lone variation, those with ovarian hypoplasia have XX chromosomes, a vulva, and a uterus (possibly with fallopian tube agenesis or uterine hypoplasia.) Their menstruation may be irregular or absent. Pregnancy is possible if they have a uterus that is large enough, however they are at a higher risk of infertility and early menopause. If they have eggs and a large enough uterus, they may become pregnant naturally. If they have no fallopian tubes, they may need medical intervention in order to access their eggs. If their uterus is too small, then their eggs can be used to implant an embryo into another carrier. This trait is rare on its own, but fairly common when partnered with Turner Syndrome.
-
Fallopian Tube Agenesis: A trait in which an individual with ovaries and a uterus is born without one or both fallopian tubes. Unilateral Fallopian Tube Agenesis is when an individual is born with only one fallopian tube. Bilateral Fallopian Tube Agenesis is when an individual is born with no fallopian tubes. As a lone variation, those with fallopian tube agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Those with fallopian tube agenesis are capable of producing eggs, however only people with unilateral fallopian tube agenesis are capable of being impregnated (as they still have one fallopian tube to transport eggs) meanwhile people with bilateral fallopian tube agenesis are incapable of transporting eggs (as they have no fallopian tubes) and will need medical intervention to access their eggs. This trait is rare.
-
Vas Deferens Aplasia/Congenital Absence of the Vas Deferens (CAVD): A trait in which an individual with testes is born without one or both vas deferens. Unilateral Vas Deferens Aplasia/Congenital Unilateral Absence of Vas Deferens (CUAVD) is when an individual is born with only one vas deferens. Bilateral Vas Deferens Aplasia/Congenital Bilateral Absence of Vas Deferens (CBAVD) is when an individual is born with no vas deferens. As a lone variation, those with vas deferens aplasia have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Those with vas deferens aplasia are capable of producing sperm, however only people with CUAVD are capable of releasing it (as they still have one vas deferens to deliver the sperm to the urethra), meanwhile people with CBAVD are incapable of releasing it (as they have no vas deferens) and will need medical intervention to access their sperm. This trait is fairly common, occurring in 1 of ever 1,000 AMAB births.
-
Seminal Vesicle Hypoplasia: A trait in which an individual has a seminal vesicle that is smaller than typical. Unilateral Seminal Vesicle Hypoplasia is when an individual is born with one seminal vesicle that is smaller than typical. Bilateral Seminal Vesicle Hypoplasia is when an individual is born with two seminal vesicles that are smaller than typical. Seminal Vesicle Agenesis: A trait in which an individual that is expected to have seminal vesicles has none, or only one. Unilateral Seminal Vesicle Agenesis is when an individual is born with only one seminal vesicle. Bilateral Seminal Vesicle Agenesis is when an individual is born with no seminal vesicles. As lone variations, those with seminal vesicle hypoplasia or seminal vesicle agenesis have XY chromosomes, a penis, two testicles (possibly with vas deferens aplasisa), and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may or may not be capable of producing semen. If they are incapable of producing semen (or have vas deferens aplasia), then they will need medical intervention to access their sperm. These traits are rare. Common traits and disabilities that may co-occur include kidney abnormalities and an absent kidney.
-
Prostate Hypoplasia: A trait in which an individual has a prostate that is smaller than typical. For adults, the mass of a hypoplastic prostate is 10 cubic centimeters or less. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
Prostate Agenesis: A trait in which an individual that is expected to have a prostate instead has none. As a lone variation, those with prostate hypoplasia have XY chromosomes, a penis or micropenis, and testes (possibly with microorchidism or cryptorchidism). During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. Their testes typically produce sperm, however the sperm is incapable of leaving the body due to the lack of prostate, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring. The rarity of this variation is unknown. Common traits and disabilities that may co-occur include ureter abnormalities, kidney abnormalities, kidney cysts, and prune belly syndrome (a condition in which the abdominal muscles above the stomach are underdeveloped or absent.)
-
WNT4 Deficiency: A variation in which an individual with XX chromosomes has a mutation in the WNT4 gene, which causes them to be born with an absent uterus, a vulva with vaginal agenesis or vaginal hypoplasia, and two ovaries. During puberty (without the influence of HRT), they will have hyperandrogenism, leading them to have testosterone as their main sex hormone, and will likely develop clitoromegaly, increased facial/body hair, higher muscle mass, and breasts. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This variation is rare.
-
Mayer–Rokitansky–Küster–Hauser Syndrome (MRKH Syndrome)/Müllerian Agenesis/Müllerian Aplasia: A trait in which an individual that is expected to have a uterus is born with a completely or partially absent uterus. As a lone variation, those with MRKH syndrome have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia) or a urogenital sinus anomaly, and two ovaries (which may be on an atypical spot of the fallopian tubes.) During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Due to the lack of uterus, they are unable to get pregnant, however their eggs can be used to implant an embryo into another carrier. This trait is fairly common, occurring 1 in every 4,500 AFAB births. Common traits and disabilities that may co-occur include a shorter height than average, abnormally located kidneys, an absent or underdeveloped kidney, heart complications, rib abnormalities, spinal abnormalities (possibly scoliosis), a short neck, a low hairline on the back of the neck, and hearing disabilities/deafness.
-
Unicornuate Uterus: A trait in which an individual is born with a uterus that has one side fully developed, while the other side of the uterus is underdeveloped (known as a Hemi-Uterus) or absent. If a hemi-uterus is present, it may or may not be functional. If it is functional, menstrual fluids will be released from it. The hemi-uterus might have a large enough opening that allows the menstrual fluids to leak into the main uterus - however, if the hemi-uterus does not have a wide enough opening, the menstrual fluids may get trapped and buildup could occur, or menstruation could take longer to end. As a lone variation, those with a unicornuate uterus will have XX chromosomes, a vulva, and two ovaries/an ovary (unilateral ovarian agenesis). The ovaries may be on an atypical spot of the fallopian tube(s). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of premature birth, miscarriage, and ectopic pregnancy. This trait is fairly common, occurring in 1 of every 4,000 AFAB births. Common traits and disabilities that may co-occur include kidney abnormalities and kidney cysts.
-
Uterine Hypoplasia/Hypoplastic Uterus: A trait in which an individual is born with a uterus that is smaller than typical. For adults, the length (from top to bottom) of a hypoplastic uterus is 2 inches/5 centimeters or smaller. As a lone variation, those with uterine hypoplasia have XX chromosomes, a vulva (possibly with vaginal agenesis or vaginal hypoplasia), and two ovaries/an ovary (unilateral ovarian agenesis) or ovarian agenesis. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. They may have hypogonadism, so their estrogen levels might be lower than females. If the uterus is smaller than 1.60 inches/4 centimeters, pregnancy is not possible, however their eggs (if they have an ovary) can be used to implant an embryo into another carrier. If the uterus is 1.60 inches/4 centimeters or larger, pregnancy is possible. however they are at a higher risk of miscarriage and premature birth, and if they have no ovaries, an embryo implant may be the only way to become pregnant. This trait is rare.
-
Cervical Agenesis/Cervical Dysgenesis/Cervical Atresia: A trait in which an individual with a uterus is born without a cervix, leaving the uterus closed off from the genitalia. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. If menstruation occurs, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a cervix. Pregnancy is possible, however embryos will need to be medically implanted (unless they have a cervix created surgically.) This trait is extremely rare.
-
Cervical Hypoplasia: A trait in which an individual with a uterus is born with a cervix that is smaller than typical. As a lone variation, those with cervical agenesis have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, and menstruation may occur without any complication, however if menstrual fluids fail to exit due to the cervix being too small, birth control will be necessary in order to prevent internal buildup, or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to expand the cervix. This trait is extremely rare.
-
Cervical Duplication/Double Cervix: A trait in which an individual with a uterus is born with 2 cervixes. As a lone variation, those with cervical duplication have XX chromosomes, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), two ovaries, and a uterus or uterus didelphys. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average. This trait is rare on its own, but fairly common when partnered with uterus didelphys.
-
Uterus Didelphys: A variation in which an individual is born with two uteruses. As a lone variation, those with uterus didelphys have XX chromosomes, possibly cervical duplication, a vulva (possibly with an obstructed hemivagina or longitudinal vaginal septum), and two ovaries (typically one fallopian tube & ovary for each uterus). During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Fertility is average, however there is a higher risk of miscarriage and premature birth. Oftentimes each uterus can be impregnated separately. This trait is fairly common, occurring in 1 of every 3,000 AFAB births. Common traits and disabilities that may co-occur include severe menstrual cramps, heavy bleeding, extra menstruation, sexual dysfunction, and an absent kidney.
-
Fallopian Tube Duplication/Accessory Fallopian Tube: A variation in which an individual is born with three (or more) fallopian tubes. The extra tubes may or may not be attached to the uterus itself. As a lone variation, those with fallopian tube duplication have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Pregnancy is possible, however there may be difficulty with eggs reaching the uterus, due to going through one of the extra fallopian tubes, which may not have a connection with the uterus. This gives a higher risk of ectopic pregnancy and miscarriage. This trait is fairly common, with the exact estimates unknown. A common trait/disability that may co-occur is endometriosis.
-
Vas Deferens Duplication/Accessory Vas Deferens: A variation in which an individual is born with three (or more) vas deferens. The extra vas deferens may or may not be attached to the testes or prostate. As a lone variation, those with vas deferens aplasia have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare. Common traits and disabilities that may co-occur include inguinal hernias, an absent kidney, and cystic fibrosis.
-
Polyorchidism: A trait in which an individual is born with three (or more) testicles. These testicles could be descended, or they could have cryptorchidism. As a lone variation, those with polyorchidism have XY chromosomes, a penis, testes, and a prostate. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. Fertility is average. This trait is extremely rare.
-
Accessory Ovary: A trait in which a person has three (or more) ovaries, with the extra ovaries being connected to the other ovaries, the fallopian tubes, or the uterus. Supernummary Ovary: A trait in which a person has three (or more) ovaries (and possibly extra fallopian tubes), with the extra ovaries (& fallopian tubes) being detached from the reproductive system, located away from the other ovaries. If they are latched onto/pressed against a different organ (ie; the intestines), they may cause abdominal pain. As lone variations, those with accessory ovaries or supernummary ovaries have XX chromosomes, a vulva, and a uterus (possibly a bicornuate one) or unicornuate uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This trait is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include extra adrenal glands, an absent kidney, an absent ureter, an extra ureter, and pouches in the bladder.
-
Ovotesticular Syndrome/Bigonadal/Ambigonadal: A variation in which an individual is born with a combination of ovaries and testicles. This could be ovaries and testes as separate gonads, or it could be a unique gonads (Ovotestes) that has both testicular and ovarian tissue within it. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. People with ovotestes have a uterus 90% of the time (possibly with uterine hypoplasia), and they may or may not have a prostate. They may have fallopian tubes, vas deferens, or both. As a lone trait, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes and a vulva or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. Those with the XY form have XY chromosomes, a penis (possibly with chordee or hypospadias) or ambiguous genitals. During puberty (without the influence of HRT), depending on the function of their gonads, they could have any combination of secondary sex traits (widened hips, breasts, increased body/facial hair, higher muscle mass, a deepened voice, etc), and they could have estrogen or androgen as a main sex hormone, or a combination of both. People with both the XX and XY forms are at a higher risk of infertility. However, for those who are fertile, most commonly, the semen is infertile, while the eggs are fertile. However in rarer cases it is the other way around, with the eggs being infertile and the sperm being fertile. This trait is rare. Common traits and disabilities that may co-occur include germ cell tumors and inguinal hernias.
-
Persistent Müllerian Duct Syndrome (PMDS): A variation in which an individual with XY chromosomes is born with a uterus (possibly a hypoplastic uterus or an incomplete one) and possibly fallopian tubes. They usually have a prostate. In some cases, they may have an ovary or ovoteste, however most often they have testicles. If they have a testicle or ovotestes structured in a similar manner, it is common to have cryptorchidism. They will have a penis, micropenis, or ambiguous genitals. During puberty (without the influence of HRT), they will have testosterone as the main sex hormone, and likely have increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypogonadism, so their testosterone levels might be lower than males. They may or may not be fertile, depending on the presence (or lack thereof) of a prostate, the function of their gonads, and the size of their uterus. If they have a prostate and functional testes, they are capable of producing sperm. If they have a large enough uterus, they are capable of pregnancy (however it may need to be medically implanted, depending on whether or not their genitals have a vaginal entry.) If the uterus is large enough to menstruate, the shedding will either exit through the genitals (if there is a vaginal entry or the urethra is connected to the uterus), or it will have nowhere to go. If it has nowhere to go, birth control will be necessary in order to prevent internal buildup (as there is no exit for the uterine shedding), or surgery could be chosen (ideally by the intersex person themself, not forced upon them) to create a vaginal entry or to remove the uterus. This variation is extremely rare.
-------------------
Hypergonadism
These are traits that cause a person's gonads to produce a higher level of hormones than in males and females.
Hyperestrogenism: A trait in which an individual has high levels of estrogen. If they have ovaries, this describes having higher levels of estrogen than females do. If they have testicles, this describes having higher levels of estrogen than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva (possibly with labial hypertrophy), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone (though it will be high), and will likely develop breasts (possibly with breast hypertrophy) and widened hips. Their menstruation could be heavy or irregular. They may also have hypoandrogenism, meaning their testosterone levels might be lower than females. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis or micropenis, and two testicles (possibly with microorchidism). During puberty (without the influence of HRT), they will either have estrogen and testosterone at near-equal levels, or have estrogen as the main sex hormone, and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. If estrogen is their main sex hormone, they may also have hypoandrogenism, meaning their testosterone levels might be lower than males. They may be capable of producing semen, but are at a higher risk of infertility. This trait is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), cold hands/cold feet, weight gain, swollen or tender breasts, bumpy breasts, a higher risk of breast cancer, a low libido, thinning hair, chronic migraines, memory difficulty, sleep disorders, and mood disorders. Aromatase Excess Syndrome (AEXS/AES)/Familial Hyperestrogenism is an extremely rare form of hyperestrogenism, caused by genetic mutations in the CYP19A1 gene, which makes the body convert more androgens into estrogen than is typical.
-
Hyperandrogenism: A trait in which an individual has high levels of androgens. If they have ovaries, this describes having higher levels of androgens than females do. If they have testicles, this describes having higher levels of androgens than males do. As a lone variation, this comes in both an XX form and an XY form. In 80% of cases the XX form is caused by Polycystic Ovarian Syndrome (PCOS), a genetic condition that causes the ovaries to overproduce hormones, which may cause cysts to develop on the ovaries. Those with the XX form have XX chromosomes, a vulva or clitoromegaly, two ovaries, and a uterus. During puberty (without the influence of HRT), they will either have estrogen and androgens at near-equal levels, or have androgens as the main sex hormones, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breasts and widened hips. If androgens are their main sex hormones, they may also have hypoestrogenism, meaning their estrogen levels might be lower than females. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis (possibly a macropenis), two testicles (possible with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may have hypoestrogenism, meaning their estrogen levels might be lower than males. They may be capable of producing sperm, but are at a higher risk of infertility. The XX form is extremely common, occurring in 5-10% of AFAB people. The XY form is rare. Common traits and disabilities that may co-occur include an early puberty (which may lead to a shorter height than average), oily skin, higher levels of acne, a high libido, bald patches, high blood cholesterol, diabetes, behavioral disorders, mood disorders, and anxiety disorders. Familial Male-Limited Precocious Puberty (FMPP)/Testotoxicosis is an extremely rare form of the XY form of hyperandrogenism, where puberty-influencing androgen production begins extremely early, causing puberty to begin between the ages of 1-5 years old.
-------------------
Hypogonadism
These are traits that cause a person's gonads to produce a lower level of hormones than in males and females.
Primary Hypogonadism/Hypergonadotropic Hypogonadism describes when the gonads themselves have low production levels. The brain is still communicating to produce the average male/female levels of hormones, but the gonads are failing to keep up with the brains-signals.
Secondary Hypogonadism/Hypogonadtropic Hypogonadism/ Central Hypogonadism describes when the brain has low levels of communication with the gonads. The brain is failing to send out typical levels of signals to the gonads, and the gonads only produce hormones when a signal is received.
Hypoestrogenism/Estrogen Deficiency: A trait in which an individual has low levels of estrogen. If they have ovaries, this describes having lower levels of estrogen than females do. If they have testicles, this describes having lower levels of estrogen than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone (though it will be low) and have the possibility of developing breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Turner Syndrome or PCOS. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, genital dryness, a higher risk of urinary tract infections, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-
Hypoandrogenism/Androgen Deficiency: A trait in which an individual has low levels of androgens. If they have ovaries, this describes having lower levels of androgens than females do. If they have testicles, this describes having lower levels of androgens than males do. As a lone variation, this comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. This trait is rare on its own, but fairly common when partnered with Klinefelter Syndrome. Common traits and disabilities that may co-occur include a delayed puberty, a low libido, less body/facial hair than average, low bone density, heart disease, sleep disorders, depressive disorders, anxiety disorders, and frequent headaches.
-------------------
Other Hormonal Variations
Congenital Adrenal Hyperplasia (CAH): A variation in which an individual has adrenal glands that produce low levels of cortisol and/or aldosterone, and as a result, produce extra androgens to make up for it (leading to hyperandrogenism.) Classic CAH is when the symptoms are obvious at infancy, while Nonclassic CAH is when the symptoms occur in later childhood/teen years or adulthood. Classic CAH can be simple-virilizing or salt-wasting. Simple-virilizing CAH is when the aldosterone levels are low, but not dangerous. Salt-wasting CAH is when the aldosterone levels are too low to regulate the salt within the blood, leading to high levels of salt in the urine, which will need supplements and medications to manage. If people with salt-wasting CAH don't get treatment, it can result in low blood sugar, high levels of acid in the blood, dehydration, vomiting, diarrhea, irregular heartbeat, shock, coma, and death. Classic CAH has both an XX form and an XY form. Those with the XX form of classic CAH have XX chromosomes, a vulva (possibly with vaginal hypoplasia or a urogenital sinus anomaly) or ambiguous genitals, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Classic CAH have XY chromosomes, a penis (possibly a macropenis) two testicles (possibly with macroorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Nonclassic CAH has both an XX and an XY form as well. Those with the XX form of nonclassic CAH have XX chromosomes, a vulva (though it may develop into clitoromegaly), two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone and will likely develop breasts and widened hips, with the possibility of increased body/facial hair, higher muscle mass, and a deepened voice. They might also develop PCOS. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility. Those with the XY form of Nonclassic CAH have XY chromosomes, a penis, two testicles , and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility. Classic CAH is rare. Nonclassic CAH is extremely common, occurring in 1 of every 200-1,000 births. Common traits and disabilities that may co-occur with all forms of CAH include an early puberty (which may lead to a shorter height than average), oily skin, and higher levels of acne.
-
Leydig Cell Hypoplasia (LCH): A variation in which an individual with XY chromosomes is born with testicles (possibly with microorchidism or cryptorchidism), which has underdeveloped or absent leydig cells, resulting in hypoandrogenism and delayed or absent puberty. They have a penis or micropenis (possibly with hypospadias), bifid scrotum, or a vulva. They also have a prostate. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though it will be low), and have the possibility of developing increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is extremely rare. Common traits and disabilities that may co-occur include a taller height than average, low bone density, and delayed or absent bone maturation.
-
17-Ketosteroid Reductase Deficiency (17 KSR Deficiency): A variation in which an individual with XY chromosomes has a genetic mutation that causes the hormone androstenedione not to convert into testosterone as frequently as it down within males, resulting in hypoandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly). They also have two testicles (possibly with microorchidism or cryptorchidism) and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
5α-Reductase 2 Deficiency (5αR2D)/Pseudovaginal Perineoscrotal Hypospadias/PPSH: A variation in which an individual with XY chromosomes has a genetic mutation that causes a lower production of dihydrotestosterone compared to males, resulting in hypoandrogenism. They have a penis or micropenis (possibly with hypospadias), ambiguous genitals, or a vulva (though it may develop into clitoromegaly.) They also have two testicles (possibly with cryptorchidism) and a prostate (possibly with prostate hypoplasia.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing sperm, but are at a higher risk of infertility (and if a vulva is present, the semen may have no way to exit, depending on how the testes are connected to the genitals.) This variation is rare.
-
Aromatase Deficiency: A variation in which an individual's body is incapable of converting androgens into estrogen, resulting in hyperandrogenism and hypoestrogenism. This begins during fetal development, and comes in both an XX form and an XY form. Those with the XX form have XX chromosomes, a clitorophallus or fused labia, two ovaries (possibly hypoplastic ovaries), and a uterus (though menstruation does not occur.) During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. Those with the XY form of aromatase deficiency have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though it will be high) and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include patches of darker/lighter skin, a taller height than average, low bone density, long limbs, inturned knees, high blood sugar, type 2 diabetes, weight gain, and a fatty liver. A person who is pregnant with a baby that has aromatase deficiency will get secondary effects of the androgens from the fetus within them. They may develop phallus growth, increased body/facial hair, and a deepened voice. These changes typically end once the baby is born.
-
Estrogen Insensitivity Syndrome (EIS)/Estrogen Resistance: A variation in which an individual's estrogen receptors do not respond to estrogen being produced. The estrogen is present, but the body is not fully using it. This may result in high levels of estrogen in the blood (due to estrogen being unused and building up), with the body only using minimal amounts of it. This comes in both an XX and an XY form. Those with the XX form have XX chromosomes, a vulva, two ovaries, and a uterus (possibly with uterine hypoplasia.) Menstruation is absent or irregular. They may also have hyperandrogenism and experience ovarian cysts. During puberty (without the influence of HRT), if they don't have hyperandrogenism, then they will have estrogen as the main sex hormone, however it will have very little effect on their physical development. If they have hyperandrogenism, then testosterone will be their main sex hormone (or even just equal to estrogen, though the estrogen is being unused), however its effects will be minimal, likely only resulting in severe acne and pubic hair. Those with the XY form have XY chromosomes, a penis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include a delayed puberty, a taller height than average, and low bone density.
-
Androgen Insensitivity Syndrome (AIS)/Androgen Resistance: A variation in which an individual with XY chromosomes has androgen receptors that do not respond to androgens being produced. The androgens are present, but the body is not fully using it. This may result in high levels of estrogen in the blood (due to estrogen being unused and building up), with the body only using minimal amounts of it. This comes in 3 forms - mild, partial, and complete. Those with Mild Androgen Insensitivity Syndrome (MAIS) have a body that is only mildly unresponsive to androgens, meaning that most of it is still in use. They have a penis (possibly with hypospadias), two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. Those with Partial Androgen Insensitivity Syndrome (PAIS) have a body that is partially unresponsive to androgens, meaning that a significant amount of it is not in use. They have a penis or micropenis (possibly with chordee or hypospadias), ambiguous genitals, or a vulva with a urogenital sinus anomaly. They have two testicles (possibly with cryptorchidism), and may have a prostate (possibly with prostate hypoplasia) or no prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice, with the possibility of breast growth and widened hips. They may be capable of producing sperm, but are at a higher risk of infertility (and if they lack a prostate, the sperm will be incapable of leaving, and thus medical intervention to extract the sperm would be necessary in order to create a biological offspring.) Those with Complete Androgen Insensitivity Syndrome (CAIS) have a body that is completely unresponsive to androgens. They have a vulva (possibly with vaginal hypoplasia, labial hypoplasia, and clitoral hypoplasia,) and two testicles with cryptorchidism. They have no prostate and no uterus. During puberty (without the influence of HRT), they will have estrogen as their main sex hormone, and will likely develop breasts and widened hips. They are infertile. All forms AIS are rare. Common traits and disabilities that may co-occur include a taller height than average, large teeth, dry skin, drier eyes than typical, light sensitivity in the eyes, and dry hair.
-
Chromosomal Variations
These are variations affect a person's chromosomes.
Swyer Syndrome/XY Gonadal Dysgenesis: A variation in which an individual has XY chromosomes, but due to a genetic mutation, they develop a CTF appearance. They have a vulva or clitoromegaly, a uterus (possibly with uterus hypoplasia), and two streak ovaries. They will not begin puberty unless they are on HRT. Due to the streak ovaries, they are infertile, however if their uterus is large enough, they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is rare. A common trait/disability that may co-occur is low bone density.
-
Mixed Gonadal Dysgenesis (MGD)/45X-46XY Mosaicism: A variation in which an individual is born with some cells having X chromosomes, and other cells having XY chromosomes. This comes in two forms. Those with the first form have a vulva (possibly with a urogenital sinus anomaly or vaginal aplasia) or ambiguous genitals and ovaries (though one or both will be streak ovaries). They may in some cases have a uterus. If both of their gonads are streak ovaries, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, meaning their estrogen levels may be low), and will likely develop breasts and widened hips. If they have a non-streak ovary, but no uterus, their eggs can create an embryo to be implanted into another carrier. If they have two streak ovaries, but have a uterus, then they can carry a (genetically unrelated) embryo if it is medically implanted. If they have two streak ovaries, and no uterus, then they are infertile. Those with the second form have a penis/micropenis or ambiguous genitals, testicles (though one or both will be streak), and a prostate (possibly with prostate hypoplasia). If both of their gonads are streak testes, they will not start puberty without HRT. If they start puberty naturally (and don't use HRT), they will have testosterone as the main sex hormone (though hypoandrogenism is common, meaning their testosterone levels may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. If they have a non-streak testicle, they can produce semen - though, if they also have prostate hypoplasia, they are at a higher risk of infertility. If both of their testes are streak, then they are infertile. This variation is rare.
-
XYY Syndrome/Jacob's Syndrome: A variation in which an individual is born with XYY chromosomes. They have a penis/micropenis (possibly with hypospadias), two testicles (possibly with macroorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism or hyperandrogenism is common, so their testosterone may be high or low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. They may be capable of producing semen, but are at a higher risk of infertility. This variation is fairly common, occurring in 1 of every 1,000 AMAB births. Common traits and disabilities that may co-occur include being taller than average, hypotonia, flat feet, abnormal feet patterns, asthma, a large head, low-set ears, flattened cheekbones, dental abnormalities, widely-spaced eyes, night-blindness, tic disorders, seizure disorders, neurodevelopmental disabilities, learning disabilities, and communication disabilities.
-
XYYY Syndrome: A variation in which an individual is born with XYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include being taller than average, hypotonia, fused forearm bones, incurved fingers/toes, radial head dislocation, a short neck, dental abnormalities, a thick lower lip, a flat bridge of the nose, a longer space between the upper lip and nose, folded eyelids, widely spaced eyes, higher levels of acne, and intellectual disability.
-
XYYYY Syndrome: A variation in which an individual is born with XYYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status, though it seems there's a higher risk of infertility. Common traits and disabilities that may co-occur include fused forearm bones, an incurved pinkie finger, facial asymmetry, a smaller than typical jaw, widely-spaced eyes, low set ears, hypertelorism, neurodevelopmental disabilities, and communication disabilities.
-
XXYYY Syndrome: A variation in which an individual is born with XXYYY chromosomes. They have a penis, two testicles, and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone, and will likely develop increased body/facial hair, higher muscle mass, and a deepened voice. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include delayed bone development, abnormal facial features, a small head, and intellectual disability.
-
XXXYY Syndrome: A variation in which an individual is born with XXXYY chromosomes. They have a penis/micropenis or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status. Common traits and disabilities that may co-occur include being taller than average, delayed bone development, twisted feet, abnormal feet patterns, long legs, long arms, incurved fingers, a slim or underweight body, frequent upper respiratory infections, a narrow chest, a prominent jaw, a small jaw, a wide bridge of the nose, widely spaced eyes, folded eyelids, a prominent forehead, an abnormal face shape, low-set rotated ears, neurodevelopmental disabilities, communication disabilities, and behavioral disorders.
-
XXYY Syndrome: A variation in which an individual is born with XXYY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, flat feet, hip dislocation, inguinal hernias, cardiovascular abnormalities, gastrointestinal disabilities, weight gain , asthma, apnea, frequent upper respiratory tract infections, lymphatic cancer, scoliosis, an incurved pinkie finger, elbow dislocation, fused forearm bones, shoulder abnormalities, a flat back of the skull, a long face, facial asymmetry, a broad jaw, dental abnormalities, a cleft lip, a thick lower lip, widely spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, movement disorders, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
-
Klinefelter Syndrome/XXY Syndrome: A variation in which an individual has XXY chromosomes. They have a penis or micropenis, two testicles (possibly with cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is extremely common, occurring in 1 of every 500 AMAB births. Common traits and disabilities that may co-occur include a low libido, being taller than average, weak bones, hypotonia, breast cancer, increased body fat, type 2 diabetes, cardiovascular abnormalities, autoimmune disorders, lung disease, narrow shoulders, dental abnormalities, neurodevelopmental disabilities, communication disabilities, learning disabilities, behavioral disorders, depressive disorders, and anxiety disorders.
-
XXXY Syndrome: A variation in which an individual is born with XXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They may be capable of producing semen, but are at a higher risk of infertility. This variation is rare. Common traits and disabilities that may co-occur include being taller than average, hypotonia, hyperflexible joints, abnormal shaping at the end of bones, flat feet, twisted feet, hip dislocation, abnormally angled hips, an underdeveloped kidney, inguinal hernias, gastrointestinal disabilities, increased body fat, frequent respiratory tract infections, asthma, cardiovascular abnormalities, scoliosis, elbow dislocation, fused forearm bones, an incurved pinkie finger, low-set sloped shoulders, a short neck, a flat back of the skull, dental abnormalities, a large jaw, a cleft palate, facial asymmetry, a flat bridge of the nose, widely-spaced eyes, upslanting eyelids, folded eyelids, drooping eyelids, crossed eyes, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, anxiety disorders, and psychotic disorders.
-
XXXXY Syndrome: A variation in which an individual has XXXXY chromosomes. They have a penis or micropenis, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is extremely rare. Common traits and disabilities that may co-occur include being shorter than average, hypotonia, hyperflexible joints, abnormal shaping for the end of the bones, flat feet, a twisted foot, abnormally angled hips, hip dislocation, an absent or underdeveloped kidney, cardiovascular abnormalities, gastrointestinal disabilities, asthma, frequent respiratory infections, scoliosis, an incurved pinkie finger, fused forearm bones, low-set sloped shoulders, a short neck, a flat back of the skull, a prominent jaw, dental abnormalities, a cleft palate, a wide nose, a flat nose, absent olfactory bulbs (resulting in an inability to smell), upslanted eyelids, drooping eyelids, widely spaced eyes, crossed eyes, near-sightedness, frequent ear infections, tremors, seizure disorders, neurodevelopmental disabilities, and communication disabilities.
-
XXXXX Syndrome/Pentasomy X: A variation in which an individual has XXXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. This variation is extremely rare. Due to the rarity, little is known about the fertility status, however it appears to be average. Common traits and disabilities that may co-occur include delayed puberty, being shorter than average, short feet, hip dislocation, immune system disorders, cardiovascular abnormalities, a small head, a flat back of the head, a small lower jaw, a flat front face, dental abnormalities, a wide nasal bridge, upslanted eyelids, widely spaced eyes, crossed eyes, low-set rotated ears, and intellectual disability.
-
XXXX Syndrome/Tetrasomy X: A variation in which an individual has XXXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is extremely rare. Common traits and disabilities that may co-occur include delayed puberty, hypotonia, hyperflexible joints, hip dislocation, kidney disorders, bladder disabilities, immune system abnormalities, autoimmune disorders, cardiovascular abnormalities, short fingers/toes, an incurved pinkie finger, dental abnormalities, widely spaced eyes, upslanting eyelids, crossed eyes, seizure disorders, learning disabilities, and communication disabilities.
-
Triple X Syndrome/Trisomy X/XXX Syndrome: A variation in which an individual has XXX chromosomes. They have a vulva, two ovaries, and a uterus. During puberty (without the influence of HRT), they will have estrogen as the main sex hormone, and will likely develop breasts and widened hips. Their menstruation may be irregular. Pregnancy is possible, however they are at a higher risk of infertility and early menopause. This variation is fairly common, occurring in 1 of every 1,000 AFAB births. Common traits and disabilities that may co-occur include delayed puberty, being taller than average, hypotonia, hyperflexible joints, flat feet, an absent or underdeveloped kidney, kidney defects, frequent urinary tract infections, autoimmune disorders, a caved-in chest, fused forearm bones, incurved fingers, widely-spaced eyes, folded eyelids, drooping eyelids, tremors, seizure disorders, neurodevelopmental disabilities, communication disabilities, learning disorders, mood disorders, anxiety disorders, and psychotic disorders.
-
SERKAL Syndrome: A variation in which an individual has XX chromosomes, but due to a genetic mutation in the WNT4 gene, they develop a CTM appearance. They have a penis or micropenis (possibly with hypospadias or penoscrotal transposition), two testicles or ovotestes (possibly with cryptorchidism), and a prostate. This variation is extremely rare. There is no information on fertility or puberty, as the only three recorded cases of this variation were terminated as fetuses. Common traits and disabilities that may co-occur include a small/underdeveloped bladder, an absent kidney, adrenal abnormalities, non-coiled intestines, small/underdeveloped lungs, heart abnormalities, a diaphragmatic hernia, and an oral cleft.
-
XX Male Syndrome/De La Chapelle Syndrome: A variation in which an individual has XX chromosomes, but due to one of their X chromosomes containing an SRY gene, they develop a CTM appearance. They have a penis/micropenis (possibly with hypospadias) or ambiguous genitals, two testicles (possibly with microorchidism or cryptorchidism), and a prostate. During puberty (without the influence of HRT), they will have testosterone as their main sex hormone (though hypoandrogenism is common, so their testosterone may be low), and will likely develop increased body/facial hair, higher muscle mass, a deepened voice, breast growth, and widened hips. They are infertile. This variation is rare. Common traits and disabilities that may co-occur include a shorter height than average and a low libido.
-
Turner Syndrome/Monosomy X: A variation in which an individual has only one X chromosome and no Y chromosome (0X.) They have a vulva, ovaries (usually hypoplastic ovaries or streak ovaries), and a uterus. Puberty may be absent or delayed. If they start puberty naturally (and don't use HRT), they will have estrogen as the main sex hormone (though hypoestrogenism is common, so their estrogen may be low), and will likely develop breasts and widened hips. If one of their ovaries is non-streak, then pregnancy is possible, however they are at a higher risk of infertility and early menopause. If they have two streak ovaries, then they can carry a (genetically unrelated) embryo if it is medically implanted. This variation is fairly common, occurring in 1 of every 2,500 AFAB births. Common traits and disabilities that may co-occur include a delayed puberty, a shorter height than average, vitiligo, moles, birthmarks, skin scarring, low bone density, outturned forearms, nail abnormalities, abnormal feet/hand patterns, flat feet, flexible toe joints, short toes, splayed toes, abnormal shape for the end of the tibia bones, inturned knees, enlarged outer thighbones, hip dislocation, an absent or underdeveloped kidney, fused kidneys, abnormally located kidneys, increased body fat, liver defects, heart defects, autoimmune disorders, thyroid gland inflammation, cystic hygroma, scoliosis, a hunched back, a short sternum, a wide rib cage, a caved-in chest, a broad chest, a broad neck, a webbed neck, a short neck, a low hairline on the back of the head, a small/underdeveloped or absent lower jaw, dental abnormalities, drooping eyelids, folded eyelids, crossed eyes, near-sightedness, prominent ears, frequent ear infections, hearing disabilities, neurodevelopmental disabilities, communication disabilities, depressive disorders, anxiety disorders, and psychotic disorders.
_______________________________________________________
_______________________________________________________
_______________________________________________________
And thats all!
Again, please reblog to spread awareness. Intersex people are highly discriminated against. Their bodies are still regularly mutilated at birth or during puberty, and they are still forced into HRT, in order to make them "look right" or "function right."
This medical abuse can cause complete infertility, a loss of sensation in genital areas (making sex unsatisfactory), chronic pain, gender or sex incongruence, and body dysmorphia.
Additionally, intersex children are often bullied at school for looking or sounding "abnormal" for their age/gender. And as they grow up, they face the same difficulties transgender individuals do - judgement for not being a "real man" or "real woman" (or for being non-binary), difficulty dating, struggles finding jobs, complications in receiving proper healthcare, and they are at an increased risk of being abused and assaulted. Many are also left out of sports or kicked out of public bathrooms as well.
This is all due to the lack of education. Tolerance and acceptance needs to be taught to children. Many doctors have no idea how to treat intersex patients, as they didn't learn about their bodies, even in advanced schooling. We need to put a stop to this.
#intersex#intersex spectrum#queer#lgbt#lgbtq#lgbtqia#lgbtqia+#education#educate yourself#educate yourselves#pride month#lgbt pride#happy pride 🌈#queer pride#body diversity#diversity#information#informative#chromosomes#hormones#hormonalhealth#genitals#reproductive rights#reproductive health#representation#reproductive justice#intersex awareness#intersex pride#intersex issues#intersex community
401 notes
·
View notes
Text
Understanding The Spectrum (updated)
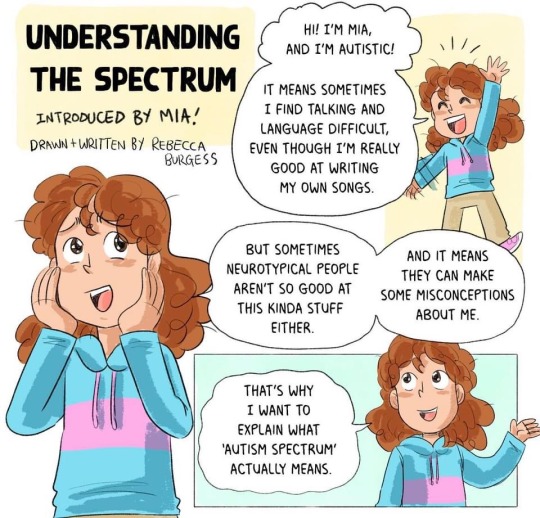
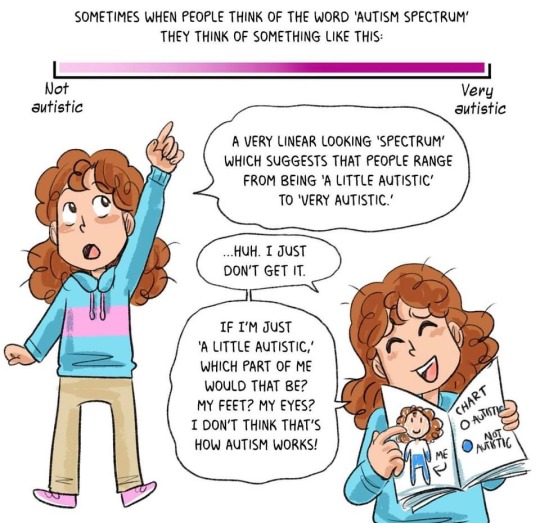

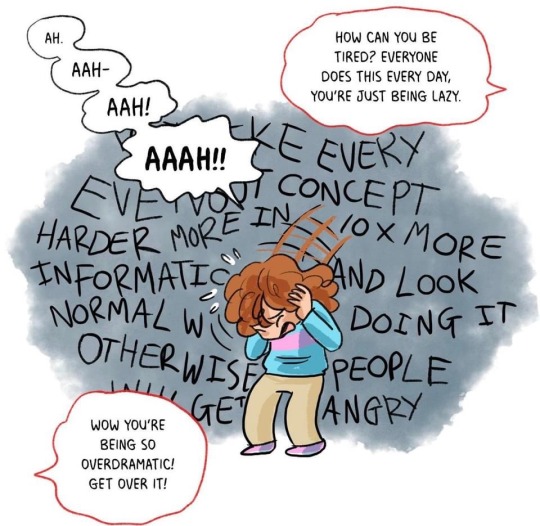
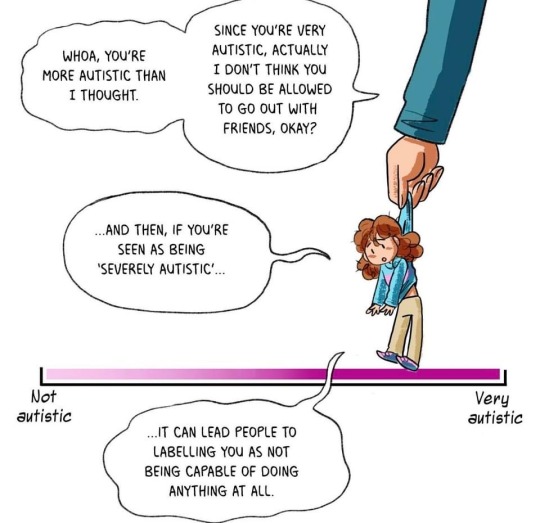
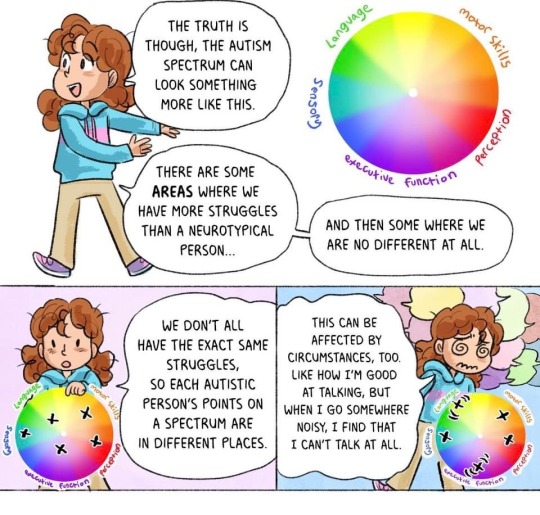
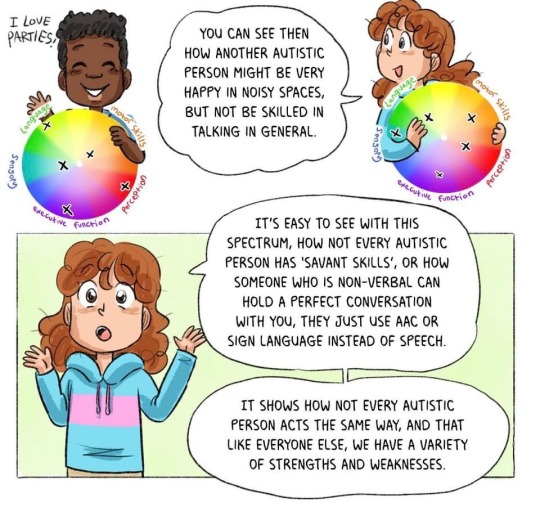


I CAN Network Ltd
#autism#autism awareness month#autism acceptance month#understanding the spectrum (updated)#informative#educational#actually autistic#neurodivergence#neurodiversity#actually neurodivergent#feel free to share/reblog#I CAN Network Ltd (Facebook)
435 notes
·
View notes
Text
Wet Beast Wednesday: moray eels
This week on Wet Beast Wednesday I'll be going over something amazing, a fish with a sense of morality. You see, the moral eel is known for, what... I think I'm reading this wrong. Oh, MoRAY eel, not moral. Well this is awkward. Hang tight, I need to go redo my research.

(Image: a green moray (Gymnothorax funebris) swimming outside of its burry, with its whole body visible from the side. It is a long, slender fish that looks a bit like a snake. A long fin starts just below the head and continues down the length of the body. The body is arranged in a wave pattern. It has a pointed snout and small eyes. Its body is a yellow-green color. In the background is the sandy seafloor, dotted with various sponges and corals. End ID)
Moray eels are true eels, meaning they are in the order Anguiliformes. Yeah, I did wolf eels, electric eels, and lamprey eels before I got around to actual eels. There are over 200 known species of moray eel in 15 genera. Like other eels, they are elongated bony fish with extra vertebrae and reduced fins. Moray eels have fewer fins than most eel species, only having a dorsal, anal and tail fin that merge together and run down the back of most of the body and underneath portion of it. They achieve motion by undulating this long fin and sometimes undulating the rest of the body as well. Moray eels aren't the fastest of fish, but they can swim backwards, something almost no fish can. The head has a long snout with wide jaws. Most species have long fangs used to grab onto prey, but a few species are adapted to eat hard-shelled prey and have molar-like teeth to crush through shells instead. Probably the coolest feature of morays are the pharyngeal jaws. This is a second set of jaws located in the back of the mouth. When the eel bites onto prey, the jaws can be shot forward to grab the food and help pull it into the throat. While lots of fish have pharyngeal jaws, morays are the only ones who can extend their pharyngeal jaws forward and use them to grab prey. Morays have smooth, scaleless skin that is often patterned to provide camouflage. The skin is coated in mucus that provides protection from damage and infection. In some species, the mucus can be used to glue sand together to help reinforce burrows. Morays lack lateral lines, a system of organs found in most fish that senses changes in water movement. Their sense of smell is their primary sense. The size of morays varies between species. The smallest species is the dwarf moray eel (Gymnothorax melatremus) which reaches 26 cm (10 in) long. The largest species by mass is the giant moray eel (Gymnothorax javanicus) which can reach 3 meters (10 ft) and 30 kg (66 lbs) while the longest species is the slender giant moray (Strophidon sathete), the longest known specimen of which measured in at 3.94 m (12.9 ft).

New reaction image
(Image: a giant moray (Gymnothorax javanicus) emerging from a burrow. It is brown and mottled with yellowish patches. Its head is pointed at the camera and it's mouth is wide open, aming it look shocked. End ID)

(Image: an anatomical diagram of the skeleton of a moray eel emphasizing the pharyngeal jaws and the muscle attachments. End ID. Art by Zina Deretsky)
Moray eels are found throughout the Atlantic, Pacific, and Indian oceans. Different species are found in different temperatures and depths, though most species live in relatively shallow, warm water. Several species can live in brackish water and a few will swim upriver and live for a time in fresh water, though there do not appear to be any species that live their entire lives in fresh water. Morays are ambush predators who rely on the element of surprise. They live in small, tight places such as holes in coral, gaps between rocks, or sandy burrows. When prey passes, the eel can lunge out and grab it. Unlike most fish, the eel cannot use suction feeding due to the shapes of their mouths. They have to rely on lunging froward and catching prey with their mouths. Their mouths are adapted in shape to push water to the sides. This reduces water resistance and avoids creating a wave that could push prey away from the eel. If an eel catches prey that cannot be swallowed whole, it will tie itself in a knot while biting on to the food. By pulling its head through the loop, the eel can rip the food into bite-sized pieces. Spending most of their times in burrows also provides protection from predators, especially in juveniles or smaller species. At night, the eels will come out of their burrows to hunt sleeping prey while the larger predators are asleep. Giant morays have also been seen engaging in interspecies cooperative hunting with roving coral groupers (Plectropomus pessuliferus). The eels can fit into small crevices the groupers can't to flush prey into the grouper's path while catching their own. Morays are mostly solitary species and many can be territorial. They are known to be shy and will retreat into their burrows if they feel threatened. They are also curious and many species are quite intelligent.

(Image: a male ribbon eel (Rhinomuraena quaesita) on a coral reef. It is a very long and slender eel with its body curved in many waves. It is brightly colored, with a blue-purple body, yellow fin and face, and a long black and white stripe running down the back half of the body. On the nostrils are two feather-like structures. End ID)
Morays reproductive strategies are poorly known and differ based on species. While many species seem to have no set mating season and will reproduce whenever they can, others will mate at the same time every year. Some species seem to have dedicated spots to lay their eggs and a few are believed to be anadromous, meaning they travel from the sea to fresh water to spawn. Meanwhile, some of the species that spend a lot of time in fresh water are catadromous, meaning they return to sea to mate. Females will lay their eggs and the male fertilize them. After this, they depart, providing no parental care. As with all true eels, moray eels begin life as leptocephalus larvae. This type of fish larvae is notable for its resemblance to a simple, transparent leaf with a head on one end. These larvae are unique and poorly understood, despite being the larval stage of a lot of different species of fish. They are unusually well developed for larvae, capable of active swimming and generally living life. In fact, some particularly large leptocephalus larvae were initially mistaken for adult fish. They feed mostly on bits of drifting organic material called marine snow and can remain in the larval stage for up to 3 years, with those in colder conditions usually taking longer to metamorphose. All leptocephalus larvae start out with no sex organs, then develop female organs, then develop male ones, becoming simultaneous hermaphrodites. They will ultimately become eith male or female and it is likely that environmental factors are the main determining factor. During metamorphosis into a juvenile, the leptocephalus can reduce in size by up to 90%, resulting in the juvenile being smaller than the larva. The process of maturation is poorly understood, but it seems that most morays will be sexually mature by three years of age.

(Image: multiple photos of a particularly large leptocephalus larva (not sure what species). It is a translucent organis, wth a body shaped like a very long leaf, narrow at both ends. In the frint is a very tiny head. End ID)
Morays are shy and generally avoid humans. Though some cultures have hunted them for food, they are often not considered a particularly good food source. Many species have high levels of chemicals called ciguatoxins in their bodies, which can lead to a condition called ciguatera fish poisoning if eaten. The largest threat to morays is habitat loss. This is especially true for the many species that live in coral reefs, which are in increasing danger due to global warming. Attacks on humans are rare and usually happen as a response to a human sticking their hand in the eel's burrow. Some of the large species could cause significant damage with a bite. Some species, usually the smaller ones, are found in the aquarium trade, thought they are not good pets for beginners as even the smallest morays are still large for aquarium fish and have some specific requirements. The curiosity many morays have has led to some becoming familiar with and even friendly to humans, often the result of feeding them. They can recognize individual humans and remember them over the course of years. Aquarium employees sometimes report that the eels will come to nuzzle and play with them and have personalities like dogs. Marine biologists and professional SCUBA divers Ron and Valorie Taylor befriended a pair of eels they named Harry and Fang at the Great Barrier Reef who would remember them and come out to visit them year after year.

(Image: a SCUBA diver hugging a large, brown moray with black spots. End ID)
youtube
(Video: A shot video showing Valeria Taylor and a moray eel she befriended)
youtube
(Video: the song "That's a Moray", a parody of the song "That's Amore" by Dean Martin)
#wet beast wednesday#i accidentally typed moron eel more than once#moray eel#eel#anguiliformes#fish#bony fish#fishblr#fishposting#eelposting#marine biology#biology#ecology#zoology#animal facts#informative#image described#that's a moray#educational#Youtube
1K notes
·
View notes
Text
Fish of the Day
Today's fish of the day is the Alabama Cavefish!

The Alabama Cavefish, scientific name Speoplatyrhinus poulsoni, is known for being one of the rarest troglobitic fish species in North America. Discovered in 1967, by the time the alabama cavefish was scientifically described in 1974, there were only about 100 fish left. On any visit to the cave, only about 10 fish have ever been seen, but they are consistently different fish, so the estimated number is a little under 100, making them critically endangered. This also makes them a possibility for the rarest cavefish in North America!

Despite the large waterways connecting caves in Key Cave National park to several other cave systems, the Alabama cavefish has restricted itself to only one cave for reasons we don't understand. A search of over 120 caves in the surrounding area revealed no populations or signs of populations. With a range consisting only of Key cave in Lauderdale county, Alabama; these fish are constantly faced by the threat of extinction, and most of their worries are based on the limited home range, and waters entering the cave. Any water with chemicals, especially fertilizers and other agricultural runoff are a large concern. That along with competition from more aggressive cavefish, and predation from nearby crawfish. Due to their living situation and delicate population, much is unknown about these fish. But, let us go over what we do know!

The diet of the Alabama cavefish consists mostly of invertebrates found in the caves: copepods, isopods, smaller cavefish, spiders, beetles, and anything else it can find that will fit in its mouth. They grow up to a size of 2-3 inches in length. They have no eyes or pigment, and hunt solely based off of sensory protrusions that dot the head and sides, a trait evolved to handle the almost complete darkness. These fish have no breeding season, and instead breed based off of the environmental signal: when the caves flood in the winter and spring. Insufficient flooding can lead to years where no breeding or spawning occurs, and when it does females carry few eggs, and even fewer eggs hatch. Their lifespans, based off of the lifespan of Northern cavefish, are an estimated 5-10 years.

#fish#fish of the day#fishblr#fishposting#aquatic biology#marine biology#freshwater#freshwater fish#animal facts#animal#animals#fishes#informative#education#aquatic#aquatic life#nature#river#ocean#alabama cavefish#cavefish#cave fish#Speoplatyrhinus poulsoni
786 notes
·
View notes
Text
loving this official US government sample card for the new driver's license standard that people'll need to fly in 2025

"Ima Cardholder"
Ace Attorney character
#ace attorney#is reposting Department of Homeland Security info like this gonna get me on a list? they want to raise awareness about the new reqs right?#listen man i was just booking a bargain bin flight and it was like “New Real ID reqs in 2025 educate yourself!!!”#and the info page had this funny image#im a good citizen dont want no trouble just informing the good people of the new Real ID act sir#dont draft me
1K notes
·
View notes