#unaffordable insurance
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Text
"This is why I'm about to quit my job."
-a Neurodivergent's Shpeil; a story and takeaway under cut
What is happening in my head: Why is he just standing there in the middle of the isle? Does he not know that he's in the way? I have to get to the next shelf, but I don't want to ask him to move, I've already asked like six times, and he's bumped into me twice. I just have to get past him somehow, then I'll be able to get the last few items I need and finish up this 712-piece order.
What actually happens: I said excuse me again, and he didn't hear me because he was talking to someone about which is better: pizza rolls or "chickie nuggies."
What happens in my head next: OH MY GOD HE IS SUCH A NUISANCE I ABSOLUTELY HATE HIM DOESN'T HE KNOW THAT HE'S A BURDEN IN THE WORKPLACE AND PEOPLE HATE IT WHEN HE SINGS PASSIONATELY TO EVERY FUCKING SONG THAT PLAYS ON THE SPEAKERS AND HE'S SLOW AND SHOWS NO REGARD FOR THE PEOPLE AROUND HIM AND WHY THE FUCK DOES HE STAND THERE SPREAD-EAGLE WHERE NO ONE CAN GET PAST HIM AND FOR FUCK'S SAKE I HATE HIS NAME TOO SOMEONE SHOULD HAVE NAMED HIM CHAD: LORD OF THE SHITHEADS BECAUSE GODDAMN AND OUR FLOOR LEAD IS JUST GOING TO TELL ME TO PICK UP HIS SLACK AND TAKE HIS CART AND FINISH IT BECAUSE HE'S TOO SLOW.
What actually happens next: I said excuse me yet again, and he heard me this time. I asked him if I could go around him, my heart beating out of my chest. He said sure, and I whipped my cart -- which is as long as a fucking countertop and about two hundred pounds at this point -- past him at high speed which probably isn't the safest choice.
The rest of the day: I stay pissed off all day, hating everyone around me, not speaking to anyone, and they all are looking at me like "goddamn I don't want to get in that bitch's way, she looks extremely unpleasant." My manager checks on me, asks me if I'm okay, and I can't explain anything to where he'll understand, so I fake a smile and say "yeah why? I'm fine. Don't worry about it, I'm just tired. Thanks for checking on me." I take out my frustration on my husband when he asks me if I want something to eat on the way home and I tell him I literally can't think straight and just want to go home and not to ask me anything again that requires making a decision or other long thought processes. My husband's in a shit mood now because he got his head bitten off by an overstimulated wife that just wants to wrap herself in a blanket and disappear from the world.
The takeaway: I don't know how many neurodivergents struggle with this particular symptom, but I'm extremely irritable around people. I want to be left alone. Being too close to too many people I don't like or hardly know causes me physical discomfort. I'm in literal mental anguish when I have to engage in conversation that I don't care for. I'm exhausted to think of meaningful responses when people talk to me. I even have a hard time responding to emails, texts, or chats, and I have a heart attack when I get a phone call. My mom has to make my doctor's appointments for me just so I don't have to get on the phone. And yet I stay working where I work because I'm terrified that I won't find anything else that pays me this much or suits my needs. I'm not disabled, and it would be extremely difficult to get disability in the US for stuff like this. So I continue to work in places I don't like, I continue to suffer around people I don't want to be around, and I continue to feel like there's something horribly wrong with me that no one else seems to have a problem with. It's just me. In my mind, I'm just messed up. I'm unlikable. I'm overlooked. I don't matter. And if I fail at this job like I've failed at all the others, I'm worthless, too. And I can't afford to fail again.
#neurodivergent#neurodivergent problems#neurodivergence#mental health#burnout#job#work#work problems#blog talk#no insurance#unaffordable insurance#untreated adhd#untreated anxiety#anxiety disorder#adhd#rsd
7 notes
·
View notes
Text
.
#personal post incoming#how tf am I suppose to stay alive?!#like this shit is expensive!#my work cut my pay 75 dollars a week because they are now offering insurance#but it’s so unaffordable and I’m on Medicaid anyways#and then my car insurance went up $50 A MONTH for no reason other than state increases#which is such a load of fucking bullshit#and my gas and electric have doubled since last year#it’s impossible to go to the store and not spend at least 30 dollars#and today my pay got fucked to hell and no one is responding to me about it and I literally don’t even have a cent in my bank account#like literally what the fuck is anyone supposed to do anymore
0 notes
Text
A Category 4 storm, Hurricane Helene, one of the largest storms to hit the Gulf Coast in a century, collided into the Big Bend area of Northern Florida on Thursday, before moving into neighboring states of Georgia, Tennessee, Kentucky, Virginia, and the Carolinas. According to media reports, upwards of 60 people have already been confirmed dead, although the death toll is expected to rise as many municipalities have yet to release official numbers as cell phone service and internet remains down and millions are currently without power. Extreme flooding has been reported in Atlanta, GA and Asheville, NC, as whole communities are left stranded and lacking proper shelter and access to clean drinking water.
As Truthout reported, “While hurricanes are no stranger to the Gulf Coast, climate change has intensified their destructive impacts, and Hurricane Helene is the just the latest case of the extreme weather events that are rising in their frequency and ferocity.” Compounding this crisis is the fact that many people on the Gulf coast lack “flood insurance, because repeated strikes by powerful hurricanes have driven up insurance rates to unaffordable levels.”
As someone from Triangle Mutual Aid reported, “The geographic scale of this disaster is beyond anything most of us have dealt with before. It’s most similar to hurricane Katrina in my experience, though over much different terrain and with people completely unprepared for it.” A recent post from Firestorm anarchist community center in Asheville, NC commented, “Our community is experiencing an ongoing crisis created by infrastructural collapse and the profound failure of capitalism to value and sustain life. No state or federal aid has yet reached Asheville, but all around us we’re seeing regular people acting autonomously to address immediate needs and meet one another with care.”
What follows is a collection of autonomous mutual aid groups and disaster relief resources that are being mobilized in the southeast in the wake of Hurricane Helene. Please consider boosting and donating to these groups and organizing support for supply chains to impacted areas.
135 notes
·
View notes
Text
My cousin's son died unexpectedly this week.
The ex-wife of one of my brothers also died unexpectedly this week.
Their families had to ask for donations to lay them to rest.
And tens of thousands of people die each year because they don't have health insurance or because health care is unaffordable.
In case you needed anyone to mourn today.
32 notes
·
View notes
Text
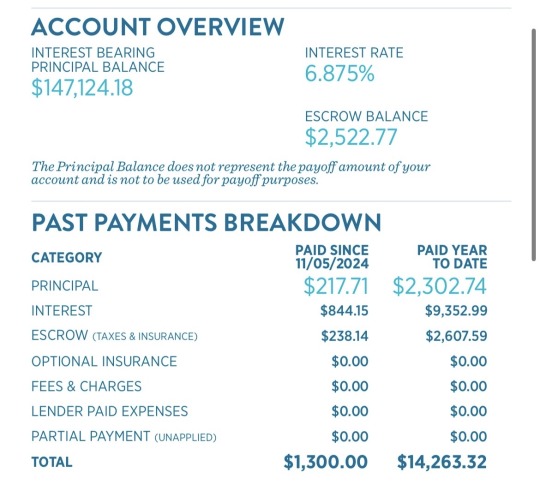
What the actual f*ck!??? How is this even legal!? I guess I’ve never looked at my mortgage breakdown. I knew I had a pretty garbage interest rate, I was waiting for rates to fall and perhaps refinance. I am absolutely blown the f*ck away!!
I pay an extra hundred bucks a month as to just keep chipping away at the principal for the loan and still!! They’re telling me, that I’ve paid, coming up on $15k on my mortgage since I bought my house last year, but I’ve actually only paid $2,300 on the actual house but I’ve given the bank $9,300 for lending me the money to purchase this piece of sh*t home, that I’ve put tens of thousands of dollars into, copious amounts of blood and sweat remodeling this thing!?!?!! WHAT THE F*CK!!!?
When I bought this POS I purchased it in Jan 2023. The listing boasted an orchard, pear trees, apple trees, peach, pomegranate and fig. When I came to see the house, I knew it needed work, but fortunately that’s what I do for a living is remodel houses.
Come to find out the pear and apple trees are infected with fire blithe, an incurable disease.
I don’t think it was the last owners, probably the ones before them but, when I opened the walls and floor, HOLY SH*T! I didn’t know termites could do that much damage! Those f*ckers covered that termite wood so well, while at the same time cursing me with the worst “craftsmanship” I have ever seen… I used to think building inspectors were a pain in my ass. I’ve never respected them more than after purchasing a home on unrestricted land.
After nearly two years of busting my ass both to pay the mortgage, and renovating this dump, I go to check the fruits of my labor, see how much I’ve paid down the house, to find I’ve paid a month of rent in a city off the actual principal of the house, while nearly 4/5ths went to interest.
I’m shocked! I’m pissed! I’m crushed!
Two f*cking years of busting my balls! Two years of living in a renovation that includes replacing the floor joists and nearly all structural studs, both interior and exterior. Two years of chasing the “American dream”, which is having a small piece of property with a very modest house on it, to find that I’ve paid $2,300 on the house itself.
The rest goes to a giant bank who harbors billions of dollars, that it acquired because it speculated (a fancy word for gambled) with other people’s money, as well as making money off having money!?
Then there’s dumbass Eugene over here, being the f*cking tool he is, just a cog in the machine, a brick in the wall if you will, being a good little serf, “just keep working just keep working just keep working.” Paying into a system he despises, lining the pockets of undeserving CEO’s and oligarchs, then some people are shocked that most of us are like, “serves him right” when a CEO of a major health insurance company gets popped!
I’m an early millennial, late GenX, I feel bad for you GenZers and beyond! Home insurance is unaffordable in many places around the country. A bank won’t give you a loan without your home being insured (don’t get me started on shistey ass insurance companies either) which kinda makes sense, so if your home burns down and ain’t worth sh*t, you don’t just walk away like, see ya ✌️ That is leading to these MASSIVE real estate companies purchasing any home they can get there hands on, not only forcing the majority of the middle class to be renters, but also fixing the price for rent, which if any of you don’t know, in any moderately big city, is out of control expensive!
For a country that decries the horrors of communism there are certain aspects of capitalism that create a subjugated class very similar communism for anyone who isn’t wealthy.
How you may ask?
One of the main principles of communism is the lack of individual ownership. Not sure if anyone’s noticed but every year there’s more you spend, but less you own.
Music and movies are no longer physical objects that one has possession of. They are now linked to a streaming service or app that requires internet, or at best downloaded into a computer.
To purchase a vehicle, especially a new one, requires a loan nearly as extensive as what a home use to cost. Vehicles are $60k-$100k anymore!! If you don’t have the credit (which is a NWO conspiracy, and that’s coming from a liberal) you can’t acquire said loan, which leaves you with the option to lease. Again. No individual ownership.
Video games are more and more becoming software that you connect to the internet to play. In my day we had clunky plastic cartridges that we owned indefinitely. Some video games now require subscriptions to Xbox live, or whatever PlayStations equivalent is, to even play the game you don’t own!
So basically what we “own” is the clothes on our back and the various “toys” we have (mine being tools, which in cruel irony are for work). The rest is consumables. Food, booze, herb, vacations, healthcare. What’s the f*cking point!?
I’m telling you my fellow Americans, Republican, Democrat, Independent, if we don’t rise up against this inequality, we, and definitely our children, will live under an umbrella of capitalism where we stay dry from any of its benefits while the rest soaks the very elite with wealth they don’t need.
The top 10% own 67% of the nations capital. That leaves us to split the remaining 33% between the remaining 90% of us. It’s f*cking absurd!!!
I know I ain’t the only dumb f*ck who works his or her butts off day after day after day, building wealth for someone else while we get but a fraction of the record profits the companies we work for make, and are told to like it or we can be replaced.
I thought I made this next thing I’m going to say up, I’ve been using this analogy for years, but just the other day I heard something similar, so I don’t know if my thought got out to the world, of if I unwittingly stole someone else’s thought years ago and claimed it as my own, but…
Let’s say we’re doing a study on a primate colony. In this primate colony there are one or two monkeys who gather as many bananas as they can, more than they could ever eat, hoarding and bogarting nearly three quarters of available bananas in this part of the jungle. The other 50-60 monkeys are left with a measly amount of bananas, whatever is left on the jungle floor that “trickled down” from these monkeys who are hoarding the majority of bananas.
We wouldn’t look at these monkeys as some kind of geniuses of bananas, or as titans of the banana industry. We wouldn’t look at them and wonder, what is wrong with these couple monkeys?! Gathering up so many bananas while every other primate in the colony struggles just to feed their baby monkeys and get by.
That’s where we’ve gotten as a society. There’s a handful of people hoarding all the damn bananas and we can’t hardly get any! Yet they’ve conned us, in a capitalistic fevor, to glorify them. See them as role models. Aspire to be just like them.
As of now there are 6 billionaires in trumps cabinet. How do these people have our best interests in mind? How do they have any basic idea what the middle class needs or desires? How can they be trusted not to focus on their bottom line as their top priority?
They don’t, they can’t and they won’t.
The last time the markets were deregulated and these “titans of industry” had the reigns, in 2007-2008, it was the greatest recession since the Great Depression.
Anyone who’s kept up with my writing might remember a study I often reference and think of. Getting a good sum of money fires off the same reward centers in your brain as doing a line or hit of blow. The same dopamine and serotonin are released in the same way.
We need to stop looking at the wealthy as people who know how to succeed and start recognizing them for what they really are.
Junkies. Looking for that next line of capital snorted up their nostril. That next hit off the glass rose stem of currency.
The whole while as they’re getting their fix from money, it’s done at our expense (no pun intended). Lessening our pay, the safety requirements we work in, our ability to collectively bargain, our employer healthcare, the labor practices, denying coverage, cutting jobs, automating jobs, working on skeleton crews, practicing predatory lending, gambling with pensions, privatizing social security.
We have to remember. Their obligation is to their shareholders. Not their customers, and certainly not their employees.
This will not change unless we rise up against them. I’m not saying with gun violence or necessarily violence in general. They need to know, that without a workforce, they can’t make money. Without a customer base, they won’t make money. Without money, how will they get the monkey off their back?
Workers of the world unite!
#politics#oligarchy#republicans#democrats#election 2024#government#gop#elon musk#trump is a threat to democracy#donald trump#liberal#news#the left#the right#democracy#billionaire#u.s. house of representatives#recount 2024#vote blue#brolargarchy#traitor trump#communist#marxism#capitalism#big banks#theft#middle class#freedom#vote democrat#america
31 notes
·
View notes
Text
A new study has revealed the worst place in Canada to buy a home, and it might surprise you. MetroVancouverHomeSource.com looked at each province's average house price and median annual income to determine its rankings. While British Columbia's housing market makes headlines over and over again for its unaffordability, it's actually Ontario that took the not-so-coveted prize with a score of 20.97 out of 100. "The average house price in the province is a staggering $931,870, while the median annual income is $41,690. Ontario also has high living costs, with high childcare, food, and household maintenance costs. However, the province has the lowest healthcare costs of all ten provinces," the report found. Apparently, BC placed a bit better for the chance of buying a home due to having "the lowest mortgage insurance premiums on average." But the average cost of a home in 2023 is higher than in Ontario — a jump compared to 2022 and remains more than double what it would cost in Alberta.
Continue Reading.
Tagging: @politicsofcanada
228 notes
·
View notes
Text
Yall I hate making personal posts like this. Genuinely. I try to keep my personal real life away from social media. But christ I'm struggling here.
I have really severe ADHD. I cannot work or function or do anything without my medication. I physically can't. But right now my medication is completely unaffordable for me.
I've been applying everywhere I can, but I live in a college town so the competition really fucks me over. I mean, which would they rather pick, a competent college student, or an adhd/autistic dropout who never learned how to mask properly?
And recently, I got dropped off my insurance plan. And thanks to me being unable to work decent jobs, I haven't earned enough to file enough taxes to qualify for affordable Healthcare. The only Healthcare I legally qualify for is a Healthcare that's $300 a month when I'm living off pocket change.
I really hate to ask, I do, especially since right now I'm without my medications so I can't get many things done, if at all, but if anyone is willing to help me out, I'm doing $5 doodle commissions. I'll work down the queue as best I can, it'll be slow but I'll do my best.
Link to my Ko-fi for assistance is below. I appreciate the help. Currently I can get a one month prescription of my medications for $45. So I'll be able to get it relatively soon but I need to save up so I can afford it each month.
If you're not able to assist that way, any advice on how to afford medications (I already use GoodRX) or any suggestions on jobs, would be greatly appreciated too.
57 notes
·
View notes
Text
If you have healthcare through the Affordable Care Act(ACA), AKA Obamacare, appreciate it now because Republicans are going to repeal it the second they get into power. You think healthcare is unaffordable now? Just wait. And I promise, even if they replace it with something else, it'll probably be just as if not more expensive than the ACA, and will likely cover fewer things. I'll be astonished if the part about covering pre-existing conditions is in their version(meaning that insurance companies aren't allowed to refuse to pay for care for illnesses that you already have when you start getting insured by them). And again, that's assuming they bother to replace it with anything at all, something that is by no means guaranteed.
Like I said, it's about to get bad.
#politics#Donald Trump#Republicans#conservatives#republican government#affordable care act#aca#obamacare
13 notes
·
View notes
Note
I'm gonna yap in here for a sec, cuz honest to god I feel you're one of the few people whom I can have a nuanced convo about this in this damned website
I REALLY havent been vibing with the glorification of people like stalin and mao here. Like, I too hate the current wild and unregulated capitalistic system we have in place, but to go and defend men who killed so fucking many is wrong as fuck.
I get wanting to question things reported by the US and th US military, that is a good instinct (as someone whose country has been negatively affected by US intervention, I dont trust the US and the military) and i also think its good to not paint everyone living in china or north korea as mindless, unemotional drones, these people lived there their whole lives and have families and emotions and bla bla. But. To go on and say that both of those govts have done nothing wrong is like ??? (And denying the ongoing uyghur genocide is also scummy as fuck)
I am also very iffed that people say that everyone who left cuba had family members that owned plantations and shit, i think the castros suck but i also think it was shitty that it was a US playground for a long time.
Sorry for the extended yapping
Yapping is always welcome.
I feel the reaction is similar to... well, any standard in the west? Christianity is king so we have to swing the total opposite and be anti-theist, ignoring how that can be deeply antisemitic, belittling, and harms minorities more than anyone else. They just see themselves as taking a swing at their oppressors, but like a kid at a party having a go at a piñata, there's other kids standing behind them that just got cracked over the dome they have no idea about.
They've been hurt by republican politics so they defensively swing so far left they to say they're democrats is an insult. Now all republicans are evil, they support Trump, don't they? They support all this evil so they're evil. These people have completely lost sight of the human condition. We aren't all knowing. We aren't all understanding. We aren't a hive mind, perception rules us and there will simply be people who see things as better another way.
Nevermind that, let's face it, people in America voted red this time because a gallon of milk costs 5$ now in a lot of places. Inflation is killing people as fast as the complete lack of healthcare and on top of it, no one is hiring. Insurance rates are insane. Housing, car, and health. Unaffordable. The wages haven't gone up since the 70s and they aren't hiring anyone. Everyone 20 to 40 is just getting fucked around. Biden did nothing to help, he got lost walking to the podium multiple times.
That's why they voted red.
These people are not online. They don't know about the insane racist bullshit. I don't know how to delicately explain that everyone I know in real life doesn't have time for the internet and has no idea what a proud boy is or what white privilege is or what's going on in California, Boston, or New York. I barely do. I worked three jobs last year and did under the table work for a few places. I have bills to pay. I have to make money to send home. My family lives in a country that couldn't even afford to be in Eurovision last year, I have 14 siblings - some of which are minors - and we are hosting people fleeing the war with Russia.
We live in one of the richest most advanced countries in the world and we can't afford to enjoy it. People see two options. Red and blue. Your third party candidate doesn't mean shit. It's red or blue. That's how America works and if you don't vote because you see yourself as above the system, oh enlightened soul, you're just giving your vote to whatever evil you see as worse.
Red promised to lower the cost of living. Blue banked on women's rights. They lost. Women voted red. They voted red the same reason countries like mine accepted communism at one point. Freedom for security.
That's the cost of communism.
Hell, that's the cost of socialism in a lot of ways. Socialized medicine sounds so good until you look at your taxes. Where do you think that free education and healthcare comes from? It all sounds like a fairytale until you've sat waiting months to see a general practitioner. Want to see a specialist? Good luck. You need a referral then you're put on a list. How long's the wait? Well, it depends. On what? If someone else gets tired of waiting. It could be months. It could be longer. Suddenly just being able to go get same day xrays starts looking good.
You couldn't pay me to go back to Europe just based on healthcare alone. I'd die. I have chronic issues, are you kidding me? You need referrals in America for some doctors, but the longest I've waited is about two weeks. You can just pay to go see a guy. You can just walk in any ol' place. I've gone in and been asked if I have a referral, said no, and seen the doctor anyway because at the time I could afford it because I was married.
I'm sorry, but Americans are so privileged. I'm staggered every day I'm here by just how oblivious you all are about being so comfortable with how terrible you all treat one another. Not saying there aren't good people, but you all get away with dog shit that would get you completely iced out of any other community in any other country and you think you can handle communism? HAH!
You can't even effectively communicate with people in your own discord servers.
Free living sounds so damn good until you get in that block, your room is the size of a prison cell, there's over 50 of you in one building and your whole floor is sharing one bathroom. You do not get to choose who you live with. If you get lucky, you might get one with multiple stalls. You have to clean it. There's no janitor that comes in and cleans the building. That's you. You and your neighbors have to clean and keep your building . The government isn't going to come cut the grass for you. They aren't going to fix your sink. You'll be put on a list for repairs. It will not be a short list.
Block living is shit I wouldn't wish on my worst enemy and these people have no concept of it.
The food is rationed. Comparable to food stamps. You only get as much as the government allows. You pay for that, it comes out of your taxes. Want to grow your own? You can't. There's no community garden in a block and you can't own land for you and your friends to start one. You can ask. You'll be put on a list. They'll get back to you. If you do manage to get that garden, you have to clean and keep it. If it gets trashy they'll take it from you. There's no "Well my chronic issues" The government does not care.
This isn't even getting into the construction of the place. That there would be multiple blocks in one place and the actual reality of overcrowding or having a job the government picks for you that you get no say in. This isn't getting into being completely out of control when it comes to your own country. Not knowing what evil is happening because they control television, radio, newspaper, books, everything. It just keeps going and going and they put up Eastern Europeans DNI because when we try to tell them they can't listen because the opposite of capitalism can't be bad.
Communism isn't the opposite of capitalism. It is it's equally fascist cousin and it has a body count just as high as any capitalist nation.
Those mass graves are deep and some people just disappeared. Work camps aren't summer camps where you ride horses and play in the streams. The Nazis and Ceaușescu are Romania's two greatest evils and the body count is something I can't even truly begin to explain. We, my people, my family, we're just gone and no one talks about it. We never got answers. "Where is our loved one" Just gone. "Where is our home?" Just gone. Our culture has to be kept so fucking secret for our own safety. We can't practice it openly still because it isn't safe and then I come online and see people say tarot is Romani culture and I just want to scream.
The west is so disconnected. Reading it in a book will never do it justice and these tankies prove it. Imagine thinking Stalin is worth following? The man who let Nazis kill his own son in a camp. Mao, with at least 80 million deaths to his name.
You can't trust what America says. You can't trust the American military about ANYTHING. The American military is a horrible dog owned by a cruel master. They abuse and kill and leech then send those people home completely unsupported and loose them on the civilian population to figure out the toll of that evil for themselves. It's inhumane. Do not trust America about these places, but why wouldn't you trust the people who suffered there? The people who survived and told what happened? Sometimes a fact is just a fact, but they don't care about that.
They only care about "the right side of history". They don't know the history. They care about social credit. They care about optics. They can't do an evil because they are so obsessed with black and white that the fact they're actively supporting a machine that's just like the one they hate so much is something they can't stomach. They can't see it because they'd be wrong. And being wrong is bad. Being bad is evil and evil is unforgivable. There is only good and evil to them. And people like you and I who don't fall into that thinking are unforgivable evil people, but they want us to believe their way of thinking is the way things should be.
They don't know what happened to people who communism found evil. The death means nothing to these people because if you disagree with them you deserve it.
They don't care about disabled people. They don't care about minorities. They themselves might be those things and yet somehow it doesn't get through they'd be seen as not worth keeping housed, healthy, and fed and end up in the same place I would. They don't care about anything, but themselves and all they see is free housing, free food, free healthcare. They see security. They don't care about the cost.
#There#I out yapped you#This isn't...my most poetic post but it felt nice to say#I hope youre having a nice day anon and feel a little less alone with this stuff#I know it can feel very isolating and scary
11 notes
·
View notes
Text
i love how any time we complain about housing pricing being too high or health insurance being unaffordable it's all like "you arent personal responsibilitying hard enough" but then when an article comes out like The Millennials Are Killing the Napkin Industry the comments are full of people being like "do these kids even know how to have fun? we used to have napkin parties all the time" and "well there goes the fucking weekend. 20 year olds just ruined this saturday's napkin party"
114 notes
·
View notes
Text
𝓘 𝓢𝕖𝕖 𝓨𝕖𝕝𝕝𝕠𝕨
Colors of Pandora Day 3: Yellow
Pairing: None (Reader Centric - Although, I do picture a WLW relationship towards the end)
Warnings: Mentions of the death of a parent, Slight grief/morning/loss, Other than that the rest is happy fluff
Word Count: 1.5K

Despite the multitude of otherworldly colors that Pandora has to offer, the moment you step on the alien moon - all you see is yellow.
The sun shines brightly in the sky, warm rays gleaming over the wide expanse of dense forest as far as the eye can see. And even though you’re first seeing this while on base - the disgusting man-made structures of steel and the whirling of machines can’t dissuade you from the excitement you feel now.
Yellow is the color of your hope.
Earth is dying, along with everything you’ve ever cared about with it. Your research has always kept you busy and the friends you had in your youth found lives of their own. It’s hard enough to keep up with relationships while struggling through adulthood, and you were always so busy anyway that most of those who were willing to reach out eventually gave up on trying. Your momma was the only friend you ever really needed anyway. Someone loyal who loved you unconditionally and who you knew would always be there for you.
The research on Pandora has found incredible breakthroughs for the medical industry. Tiny yellow glass vials that could fix everything. New serums for cancer cures and even an elixir to stop human aging - the opportunity to be healthy and live forever with those you love.
But they’re expensive. Unaffordable for someone like you, and your momma’s insurance is a huge joke.
She’s not on Earth anymore, so you don’t want to be either.
But it’s in moments of despair that you need hope. She wouldn’t want you to wallow in your grief, stricken by the pain you feel at her absence and terrified at the thought of actually being completely and utterly alone. Yellow can be cruel - fearful and cowardly, anxious beyond measure.
You refuse to think about it like that. Yellow was her favorite color. Her with her pretty yellow dresses and excessive sunflower decorations that always made the tiny and cramped apartment you both could barely afford feel more like a home than any other space. You wanted to take it all with you as you packed for the interstellar trip, but the most important thing you could bring yourself to actually pack was the small, frilly yellow flower clip she always had pinned in her hair.
It sat safely clipped on your tank top strap as you lowered yourself in for your cryosleep, letting it be the symbol you intend it to be. When you close your eyes, you believe you can feel your momma’s loving and protective hold wrapping around you - and you think you can even see the faintest hint of a soft yellow aura behind your closed eyelids.
Your momma always thought the color yellow was beautiful - radiating of love and joyfulness, a necessity in an otherwise dull and dying world. She saw the beauty in it, and now so do you.
You don’t approve of what the RDA is doing. Their destruction and carelessness for the place the Na’vi and the wildlife call home is deplorable at best. The same cycle of Earth repeating here.
It’s the negative of yellow again. A darker yellow, a more irritating shade maybe - one that begs caution when dealing with the devious and heartless people that surround you now, but still the same color you hold dear to your heart.
But they’ve offered you a chance for a new life. A new body built for the rougher terrain and the freedom to use it to further your research. It’s for them, you know that. But you feel like it's for you more.
Yellow is the color of your happiness as you walk through the Pandoran forest. Your new body moves effortlessly through the foliage, confident steps that take you across the mossy surfaces that your human feet would probably slip on if you even tried to cross. The sun in the sky is bright - too brilliant a yellow to even look up at for too long. But its rays feel amazing on your body, skin soaking up the heat as you stretch out like a cat along the soft ground of the found meadow.
The water along the meadow’s edge is blue, clean and inviting in a way the water on Earth could never be anymore. But when you hover over it and gaze into the reflection staring back at you, you see yellow. You’ve never liked your eyes before, never thought they were anything special. But they look so striking now, like twin pools of swirling honey.
You’ve always thought that happiness was dependent on the external. Good environment, good circumstances. Happiness is yellow in the same way that joy is yellow. Similar in shade and even closer in their meaning, but still so different in the end.
If happiness is yellow, bright and vibrant and soul-changing as it washes over you, enveloping you in its warm embrace and soaking into your skin, then joy is yellow too - soft and playful, almost child-like as it wells in your heart, growing and growing until it’s uncontainable and it shoots out from your being and into the world for all to see. An internal feeling that only you can manifest - a color only you can create and share with the world.
When you meet her, you know she’s going to bring you both.
She’s stealthy, a true predator, especially considering you’re not and you most definitely shouldn’t be out without protection. The gun slung across your back is useful in theory, and you’ve been trained on how to fire it acceptably, but you’re not sure if the time ever actually came time to use it if you actually could. You think it would be okay - to die at the hands of an alien animal or one of the natives. Pandora has already given you more than you could have ever hoped for after your mother passed and you think that if things ended right now, it would have all been worth it.
She could have ended it. Who knows how long she was watching you - up in the trees or hidden in the tall foliage, an arrow dipped in neurotoxins meant to kill you in less than one minute flat if the arrow itself doesn’t do the job first pointed straight at your heart.
But she didn’t.
Yellow is the color of your curiosity. The question of ‘why’ is a repeating mantra in your head because when she finally does reveal herself to you, it's like she already knows you. She’s not afraid, even smiles at your wide eyed stare - her own eyes like sparkling suns.
It’s the color of her own curiosity too.
“I watched you,” she says. “I learned. Now you watch too.”
You watch as she extends her arm out towards a nearby bush, fingers just brushing against the leaves before something explodes out of it. A gecko-like creature bursts from its hiding spot, jumping up and unfurling into a circular glowing fan as it flies up in the air. A startled laugh slips from you in amazement as a few others pop out as well, circling up overhead in a display that almost looks magical. The glow coming from the creatures is tinted yellow, and while your eyes are on them, her eyes are on you.
You see yellow in the ways she treats you. For the first time in a long time, you have a friend. A friend who cares about you, who wants to be around you. Someone who’s not your momma, but who gives off the same energetic vibe as she did.
She shows you her world and how to see it not just through your own eyes in a constant state of wonder, but through hers. Yellow is the color of your new found appreciation for the place you now call home. She guides you through it, introducing you to all that Pandora has to offer and teaching you all you can do to give back to it in return. You see yellow in the energy around you - yellow in the animals and in the dirt.
In her.
When in this body, the little yellow flower clip usually sits pinned to the waistband of your pants or tucked safely in your hair on your sleeping human form back at the lab. You want it with you always, but you can’t bear the thought of losing it somewhere out in the alien environment where you might never be able to find it again.
It’s a big thing, to not have it on your human body right now. It’s not with your Avatar body either. Or rather, not on it.
Instead, it’s clipped beautifully at the end of her songcord. It’s bigger than the rest of the beads and jewels she’s used to weave it, but it makes your heart sing to see it kept there so proudly. You know she’ll keep it safe for you.
When she catches you looking at it again, her smile is blinding. And when she steps closer to wrap her arms around you, holding you close - all you feel is yellow.
**Special thanks to @xylianasblog for the prompt!

#𝑻𝒂𝒍𝒊𝒆 𝑾𝒓𝒊𝒕𝒆𝒔 ✎#ColorsOfPandora#fem!na'vi x fem!avatar!reader#fem!na'vi!oc x fem!avatar!reader#fem!na'vi x fem!human!reader#fem!na'vi!oc x fem!human!reader
14 notes
·
View notes
Text
just so you guys know how fucked up US healthcare is
I’ve been off my antidepressants for months because it was about $150 to get a 3 month refill. anti anxiety was the same. $300 for meds I need; I’m a full time student with a part time job. $300 is an entire paycheck for me. This $300 is AFTER insurance.
So what do you do if you can’t afford meds in America? Three options, honestly:
1. You don’t get your meds
2. Don’t use insurance and have the pharmacist use GoodRX
3. See if your meds are available through mark cuban‘s online pharmacy.
For my non-Americans out there, let me explain what GoodRX is
Plenty of medical providers keep GoodRX cards at the reception desk. How does it work? Hell if I know. But if you tell the pharmacist “don’t use my insurance, use my GoodRX card instead,” they do it. and 9 times out of 10 it’s cheaper. and literally all you have to do is show them a piece of cardboard. no signup, no paying to join, nothing. it’s essentially just a reusable coupon you can use instead of insurance.
For me, tho, GoodRX only brought my meds down to being about $200 total. Still unaffordable.
Again, for my non-Americans, you may be wondering what the hell the mark cuban online pharmacy is.
Billionaire Mark Cuban created an online pharmacy that provides some very common medications for a MUCH lower price than literally anywhere else in the US.
It’s a little bit of a pain to get started, but when you do it gets mailed to your door. They take insurance, but currently they don’t take mine.
Want to know how much my meds (which, btw, went from 2 medications to 3, one of which increased dosage) cost on mark cuban’s website?
For a 60 day supply, after tax, and after paying $15 for expedited shipping, it was about $35.
Thirty. Five. Dollars.
Why the FUCK were my meds EVER over $300 when I can get them shipped to me for LESS THAN $40.
(just to break down the costs a bit more, that’s (including cost for shipping) ~$0.15 per pill online (one of my meds is twice daily) vs ~$0.90 per pill from my pharmacy with insurance, and it wasn’t even all my meds. )
11 notes
·
View notes
Text
OK I HAVE A CONCEPT!
okokokok so
bear with me i know this is going to be stupid as FUCK but just b e a r w i t h m e
Archangels and Demon lords are forced to play D&D together.
And the Nephalem is the DM running the whole thing, and its set in a semi modern world where their characters have to deal with shit like "they just got in a fight and now cant go to the hospital because they dont have insurance" and shit like that.
They are all forced to work together as a team to fight against a corrupt politician or something, but they are also dealing with weird modern problems like learning how to send an email or hotwire a fucking car.
here are some quotes from the initial conversation
"Ok Belial, roll Deception" "HA i have such a high modifier i couldnt possi-" "What did you get?" "… nat 1"
"You can't buy that, Diablo. You don't have any coin." "How do I get coin?" "Get a job, mate." "Like what?" "Idk, barista?"
"how do I send this message?" "you can try email, letters.." "what is email I want to do that one" "alright you spy a computer next to you" "I shove the message into the artifact" "you…. what?"
"I run up in front and block the attack" "Did… you just save me, Asmodan?" "Shut up, Tyreal"
"Tyrael you are our only healer and healthcare is unaffordable. if you die we are all fucked." "glad to see you care… kind of"
some other things:
Diablo's character would 100% die first and he would be mega salt about it, he always plays a Teifling (bc he wants to keep the horns)
Tyrael would play a Cleric, who the party relies on for healing bc none of their characters have Insurance to pay for hospital visits.
At the beginning of the campaign the DM has angels and demons on opposite sides of the table but by the end they are all mixed up and sitting together. He knows he did a good job when they beat a hard encounter and they all cheer and some of them even hug or highfive.
they're having a lot of fun but would never admit it outside of sessions.
And I did of course draw this.

in this senario half the party is fighting a mutant rat while the other is trying to figure out how to hotwire a car so they can run it over.
#diablo 3#diablo#nephalem#angiris council#Demon lords#archangel#malthael#tyrael#imperius#auriel#itherael#azmodan#belial#duriel#andariel#baal#mephisto#dungons and dragons#dnd#this is only kinda silly#but like what if it was kinda serious#can we end the eternal conflict with TTRPG's and snacks?#my art
139 notes
·
View notes
Text
To every American who has ever told me that I have it easy/easier because I'm in Canada,
Maybe start by reading the GODDAMN WIKIPEDIA ARTICLE!!!
I'm an sick and tired of being told that I am not suffering just as much because I am not paying as much as you are. I recognise that my unaffordable $10 000 is probably your unaffordable $100 000 but I need you to stop telling me that I have it easier.
I need you to stop saying 'our wait times are bad too!' Yes! They are! No one should have to risk their life waiting! But, like I'm recognising that healthcare is less unaffordable than mine, I am asking you to recognise that your 2-3 year wait time can be 5-15 years for me and our resources are scarcer and our travel is less accessible and our insurance covers less and government-funded healthcare means economy-based availability.
I am making absolutely no judgement about who has it worse. I'm trying to recognise that this is no longer the 1970s and that we have vastly different systems with vastly different problems and I am sick and tired of saying 'I'm suffering uniquely as a disabled person in Canada' but then having to tack on 'but, although I am unique, the Americans have it worse and I must repent' when my suffering is unconditional so my expression of it should be too.
#and if you haven't said that#make sure you haven't expressed a similar opinion (I don't care if you work in healthcare)#and if you still haven't#good for you don't tell me about it#disability#physical disability#medical#canadian healthcare#healthcare crisis
4 notes
·
View notes
Text

Hey I sold a bunch of books again so it's donation time. And now's a great time to donate if you want to join in because every donation is being tripled. Yes they hit their goal but what if: they could do even more for trans folks? Utopia.
https://secure.givelively.org/donate/point-of-pride/stand-up-for-trans-futures
Here's some copy from the donation page enumerating some of the services they help trans folks get access to:
* Free chest binders and femme shapewear discreetly delivered to recipients in all 50 states and around the world. These garments help trans folks live safely and authentically, at no cost to them.
* Permanent hair removal services for trans femme individuals, helping to remove financial and social barriers to this often essential, yet unaffordable, care.
* Gender-affirming surgeries and HRT access for those who lack the financial resources or inclusive health insurance needed to access this life-affirming care.
Okay that's all. Cheerio.
2 notes
·
View notes
Text
The dilemma in my life currently is basically my employer switched to an individual health insurance instead of group, so I have a bunch of options to choose from but they’re all kinda shitty.
My employer has given me a ‘generous’ $635 health insurance contribution toward the monthly premium, but the only affordable ones in New York are $300 or $800 (and the $800 is worse than the $300 one). The $300 NY one has a $9200 deductible and nothing is covered even if it’s in network until that deductible is met, HOWEVER the first 3 pcp visits are free if they’re in network
The $800 NY one has a $3800 deductible but the first three pcp visits are $50, and then after the first three they’re only $50 after the deductible is met. So there’s no point in paying part of my actual salary ($800-$635 contribution is $165 of my own salary money per month) for this one
Meanwhile if I say I live in my parents house in New Jersey, none of the New York providers are in network (aka my New York primary care, obgyn, etc. Are all out of network) but if I found NJ providers in say, Jersey city or Hoboken, the premium for NJ insurance is $600 (so fully covered by my employer’s contribution) and if I were to see a NJ doctor in network the copay is like $5 for PCP etc and the deductible is only $1750 or $1500 I forget
So basically I have the option to choose a NJ plan, and have to do all my doctors visits in New Jersey which isn’t that far from me especially, like I could easily get to the PATH train at World Trade Center or even walking to Christopher street PATH station, but for some reason I have a mental block that says it would be really out of the way every time I need to see a doctor
Meanwhile my current doctor is a 10 min walk away, so if I wanted to see her it would be really easy, and I COULD continue seeing her, just maximum 3 times next year if I choose the New York plan. I saw her twice this year so like this should be fine if I chose this plan but it’s sooo shitty.
But idk lately I’ve been getting yeast infections (tmi) and they won’t prescribe me a pill for it unless I go in and see them and they do tests on me aka maybe I would need to see the doctor more than 3 times a year, in which case I’d be fucked if I got either of the NY plans
The other thing is if I need urgent care if I choose the NJ option, all the NY urgent care is out of network which might be stressful in an emergency. I’ve used urgent care a bunch when I first moved to New York mostly bc I was still on my mom’s superior health insurance back so it was covered then in both NJ and NY but also bc I would go for COVID tests. But nowadays I don’t really go as much, I think I went once in October 2023 bc I cut my foot open at the beach and that’s it
This all makes me sad because why is health insurance in New York so unaffordable. The $300 and $800 NY plans are the two CHEAPEST plans offered meanwhile the $600 NJ plans like the 4th most expensive out of 25 (so the first 21 options were cheaper than $600)
Like yesterday during my jewelry class one of my classmates is a literal surgeon who works in Manhattan and used to live there, and she moved from the city to Westchester aka upstate, because living in the city with two children was too expensive. FOR A SURGEON??
The reason this came up is because there was like an article in some magazine about how people on nyc whose household income is less than $300k are eligible to apply for assistance to send their children to daycare
Apparently sending your kids to a daycare can cost $65,000/yr which is more expensive than how much it cost me to go to college for a year. They’re writing applications and asking if a parent is a legacy for a TWO YEAR OLD. What would one even say? She likes barbies and playing with legos??
Idk it all makes me so incredibly sad the possibility of leaving nyc when I’m older and being convinced to choose a NJ health insurance plan because it’s more affordable and better value is kinda proof that this might be my fate one day
2 notes
·
View notes