#these are from the dsm; the icd is a little different
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
Does anyone realize that the "everyone is valid" thing has actual diagnostic implications?
Yes, every case of DID will have differences from another. But all DID cases must meet diagnostic criteria in order to actually be DID. You can't say "everyone is valid" and "DID can look like anything" because really, it can't. At the end of the day, there are still diagnostic criteria that must be met. If anything goes and anything is valid and anything can be DID, then DID is nothing and we might as well not even classify it as a disorder at all.
Same thing as people who say that "everyone has a little bit of DID" or "everyone has parts". Yes, you act differently at work than you do at home. This does not mean that you have dissociated parts of a fragmented self, and if it did, then DID would be a redundant diagnosis and there would be no need to have it in the ICD or DSM if "everyone" had it.
#actually did#actually dissociative#ramcoa#ramcoa survivor#did osdd#did system#dissociation#dissociative identity disorder#dissociative system#osddid
558 notes
·
View notes
Text
Oh boy, lets open that can of worms
There's a LOT of discourse with endo vs anti-endo stuff (endogenic system=plural system not formed by trauma if you don't know 🙂). Like, death threats coming from both sides kinda thing. We try to stay out of it. But it's easy to accidentally stumble into it if you're not familiar with some of the nuance. So we want to share some observations as like, a crash course. (And apparently we had a lot to say lol.)
This post isn't really to debate how plurality forms. Just to give some context as to why so much hate is flying between these two groups.
Basically, you have 2 extremes. (And everyone in between obviously)
On one side you have people making up extra rules on top of the diagnostic criteria to exclude and gatekeep anyone who doesn't meet "their level" of disordered. (I've literally heard people say "you can't be a system, you're not as traumatized as me"). A lot of accusations of faking come from this bunch. Too much internal communication? Faker. Too many non-human alters? Faker. Too many or not enough alters? Faker. You can't win with them even if you have a diagnosis.
We've noticed a lot of parallels between this group and transmeds. You need to have x level of dysphoria to ride this ride. You can't be trans if you don't want xyz treatment. You need to reach my arbitrary bar of "trans enough". Enbys and everyone else are fakers. That kind of bs.
But on this side you also have a lot of people who just want to be taken seriously. They want to be validated by their diagnosis and feel hurt when people say or do things that they think will compromise that validity. They, at least initially, come from a place of sincerity not malice. But they fall into the trap of trying to be "one of the good ones".
On the other extreme you have the wild west. Things people treat as fact aren't codified with the same scrutiny as the DSM-5 or ICD-11. This breeds its own confusion and misinformation. We've seen people conflate plurality with things like maladaptive day dreaming, lucid dreaming, adhd, and (applying it to other people with ferocity to the point of harassment) metaphors of all things.
They have a spaghetti at the wall approach that reminds me of a less extreme MOGII (an attempt to define just about every possible form of gender and sexuality). It's a messy patchwork of ideas. We've seen 8 different labels that all mean the same thing and are being used by exactly no one. Redundancy and hyperspcificity, that's the name of the game. But frankly we like this if for no other reason than we want to see what sticks, what becomes mainstream.
We've seen people from this group attack people as badly as the anti-endo group. Openly mocking people for having trauma or saying vile shit like "traumagenics kys". They feel threatened by the exclusionary nature of diagnoses. But instead of taking their frustration out on the systems of power they take them out on normal people. After all if you're diagnosed, you "represent the system"... I guess. Equally bull shit.
But this is also where the edge cases go, the exclusions, those that don't fit into a neat little box. The DSM excludes people whose plurality is accepted as part of their culture or religion. These people don't suddenly stop being systems just because they're accepted, but they're distinctly not disordered. They don't meet the clinical definition of DID or OSDD. Same goes for someone whose symptoms are mild enough to not cause "clinically significant distress". You also have people who don't want to be pathologized or have been failed by the medical system.
So lastly, a warning: When dealing with plural stuff, it's very easy to go stumbling into a mine field.
Tldr: I would always rather land on the side of letting too many people in than exclude people who needed the support. However, no matter your in-group, some people take things too far. Like, ffs don't attack people.
-Taylor & Mark
#not giving this any proper tags cause I don't want a fucking maelstrom of hate coming at us lol#long post#this might be a bad idea
173 notes
·
View notes
Text
Dissociative Identity Disorder in Mr. Robot
So I have been writing little essays about Mr. Robot recently.
Dom's Sexuality, Gay Marriage and Whiterose
Back to the Future and Brainwashing
Today I wish to talk about the DID representation in Mr. Robot.
Actually I want to talk about the DID representation in the Hulk comics but there are 40 years worth of storylines involving it and it would require me to write about clinical understandings from the 1980s when it was called MPD (admitedly Mr. Robot's stumbles at the finish line with some of these same outdated treatment models) and that would take a while. Suffice to say it will happen eventually*. I shall make a new tag "Media Myself and I" and post it under that when I have more time to do it justice. Maybe I'll do others. I am uncertain. I believe I want to focus on positive depictions where there are no murder alters. The goal is to get people to want to enjoy things, not to steer them away. I have a few shows and games in mind at the very least.
Regardless… Mr. Robot is an easier topic to cover and is my hyperfocus of the moment.
So Mr. Robot is a show about isolation in the modern world. It's a show about socioeconomic stress, late-stage capitalism and what it means to enact meaningful change on a broken world.
But above all it is about the healing journey of Elliot Alderson, a man with dissociative identity disorder.
I say that at the start because Elliot's condition is never named until the final episode. In many ways a realistic depiction of a real world disorder was an afterthought noted in the final hour of the journey as a means of justifying the split personality trope and hiding a final twist. In spite of that the roadmap for the show was always leading to this destination and along the way they managed to get some fairly good representation out of the mix.
Season 2 even involves the only time I have ever seen a piece of fiction depict "blending" on screen. Blending isn't a symptom listed in either DSM or ICD manuals. It is, however, something one would hear about if they had a conversation with someone who had DID. I have used that scene to depict what it feels like to my partners.
I'm getting ahead of myself.
I love Mr. Robot. It is currently my favorite show of all time. If you have never seen it then please give it a shot. This post will be spoiler heavy and I'd hate to rob anyone the opportunity to watch S4E7 and have a pure emotional reaction to it. The show is on Amazon Prime and the full box set is available for $35-50 depending on format and vendor.
Go with my blessing.
-
The first season of the show begins with Elliot Alderson (Rami Malek) living a double life. By day a cyber security expert and by night he spends his time at his computer hacking people's accounts and satisfying a "little itch in the back of his head" that guides him to uncover the murky facts about people. The first scene of the show has him take down a cafe owner who hosts an illegal and deeply unpleasant website. I have seen individuals walk away from the first episode thinking that the show is "Dexter but with computers" but it is more lulsec activism with a Fight Club aesthetic.
The show has 4 seasons and each season depicts a different stage of Elliot's healing journey and with it completely different rules and depictions of his condition. I'll break down each season for what they do right and what they do wrong.
Season 1: Discovery
Elliot's system in season one is undiscovered but he has overt symptoms, meaning he is unaware that he has any alters but he suffers from clean breaks in his consciousness and drastically altered behavior patterns both which are a detriment to the "hidden" nature of the condition.
Commonly most people do not discover their condition until their 30s. I was 37/38 when our therapist started guiding us towards accepting our condition.
DID manifests in childhood but it's a hidden illness that does its best to go undetected. The point of the condition is to remain hidden. The internet and the educational resources it offers are helping younger individuals to recognize their symptoms and advocate for themselves at an earlier age but the standard medical understanding is that most people are developed adults before they are diagnosed.
Published statistics for DID indicate the global population of those with the condition is about 1.5% (some organizations argue the number should be higher due to how difficult it is to receive an accurate diagnosis, but 1.5% is the most consistent figure) which is rare but not to the point of never encountering it. For comparison, according to a 2023 census 1.0% of people in the USA identify as transgender. There are no tested classifications for Covert vs Overt display of symptoms but it is widely agreed that an overwhelming majority of cases within the 1.5% are covert.
We learn that Elliot is desperately lonely, abuses morphine and has paranoid delusions about men in black stalking his every move. Whenever Elliot is on screen we can never be sure what is real and what isn't, so there are times when men wearing black suits are on screen and we cannot be sure if Elliot is paranoid or delusional.
The show takes place through his perspective after all and we are a character in the show.
See… the narrative device of the show involves Elliot speaking to "friend", us. The audience. "Hello, friend." is a common refrain spoken throughout the show. The narrative begins a short while after Elliot had a complete mental breakdown and smashed up a server room, he is seeing a court appointed therapist, is socially paralyzed to the point of which we see him linger outside a birthday party and retreat home to cry in loneliness.
The entire first season Mr. Robot is depicted as another character, akin to Tyler Durden, a wild revolutionary who wants to encrypt the data of the world's largest bank in order to seal the debt records and reset everything back to 0. He starts off appearing in scenes involving the men in black stalking Elliot to mingle him in with the paranoid delusions and eventually begins interacting with him in earnest. Though the reveal is treated as a twist 8 episodes into the show Elliot does accuse the audience of knowing the entire time and he refuses to speak to us for some time, even going as far as to keep secrets from us because he cannot trust us any longer.
It's at this point that I will note that media depictions of DID tend to lean heavily on the phrase "it's a visual medium" and depict ways that characters can see, interact with and communicate with alters/parts in a dramatic setting. Off the top of my head Hulk is about the only form of fiction I've seen where the temptation to do this doesn't take over and even then the old "other face in the mirror" trope shows up there.
So for what it's worth the paranoid thinking and hallucinations are not DID symptoms and typically a person with the condition cannot see or hear their alters. In fact a testing criteria included in the MID exam is to rule out schizophrenia by eliminating the possibility that the voices heard are external or that any hallucinations exist. In Mr. Robot they are likely caused by Elliot's morphine addiction, but he gets clean after season 1 and Mr. Robot is always there.

There are some plot elements which I want to talk about but they do spoil the final "twist" of the show. So I want to warn again that anyone in the process of watching should be warned we are getting into entire show spoiler territory.
The Elliot we see in the show is the result of the stress fueled breakdown that Mr. Alderson had 6 months prior to the show starting. The timeline is fuzzy in my head but there were two triggers which set him off and began his condition flaring up (and/or caused him to lean harder into his drug addiction which in turn fueled his condition). The one we know about is that he was locked in a server room and forced to work long into the night on an issue and the already upset and stressed Elliot snapped and had a black-out.
We come to learn that he has had these his whole life but this is the first time such an incident occurred that he couldn't self-justify what had happened. He smashed up a server room, something he felt himself not capable of.
But the second trigger is the more important one.
His sister, Darlene, moved to NYC and started visiting him.

The bigger and better twist of season 1 is that Elliot and Darlene are siblings. This is hidden from Elliot and the audience for the first 7 episodes and her presence is treated much like Marla Singer from Fight Club, of whom she likely contains some inspiration, where she keeps showing up in Elliot's apartment and acting overly familiar with him.
In the earliest episodes when we are learning about Elliot's lonely life he looks at a photograph of himself and his mother at Coney Island. Due to some hallucinations we know that Magda is an abusive mother and screamed at/hit Elliot a lot. We learn more about her in future episodes and she is a truly horrible parent. Likely more than was ever depicted in the show.
The photo is actually of the full Alderson family including Darlene and Edward but is not shown as such until the reveals that Darlene is Elliot's sister and Mr. Robot is modeled after Elliot's father. The photograph is a reference to Back to the Future.

But it also is a fairly good visual representation of self-filtering information, even when it is contradictory in nature. This is common not just in DID but in all forms of CPTSD.
Complex Post-Traumatic Stress Disorder is a condition that develops during prolonged exposure to trauma and makes radical changes to the nervous system. CPTSD is considered a root of DID and it is universal for those diagnosed with DID to have a CPTSD diagnosis also.
One of the ways CPTSD symptoms manifest is "Emotional Avoidance". The nervous system is activated when triggers related to the trauma exist within the person's life. In order to function their brains push away these reminders and naturally avoid interacting with them. This causes those with the condition to become withdrawn, to isolate and to have distorted and often contradicting patterns of thought. For instance Elliot needs connection and safety that he associates with family but his family were his primary abusers and so he edits his memories to focus on positive associations such as a family trip to Coney Island that has become an obsession to him in adulthood. We later learn that Elliot's obsession with movies was born from it being his primary way of connecting with his father... which is fairly relatable.
His positive memories of his parents are held in high regard even though we know that his father "pushed him out of a window" and his mother used to put out cigarette butts on Darlene, tried to force her to commit animal cruelty and is often depicted in hallucinations as beating and screaming at Elliot.
In a case where it is impossible to avoid the traumatic trigger, for instance the return of relative who is a living reminder of his abusive childhood, the individual may begin to dissociate. Dissociation being where a person, overwhelmed by what they are experiencing has a separation from their normal state leading to a disconnect from emotions, sense of self and reality.
Episode 8 in particular contains a visual depiction of it when Elliot is having a quiet meltdown over finding out he has a 2 day deadline and his boss at work has known about the server exploit he installed all along.

(the show often uses the camera in ways to emphasize emotional walls, dissociation and isolation like this. This sequence does so by having hard cuts, shaky cam and frantic pace melt into a gliding slow lull where the background noise filters out and we can share in Elliot's distance from his situation for a moment)
Elliot's form of blocking out is extreme but has half a foot in reality (and half a foot in the logic born from the "twist" ending) in that in order to continue interacting with Darlene he views her as a member of Fsociety and edits out their connection until it is revealed in episode 7.
A small brilliancy about Fsociety is that the entire group is formed around Elliot and Darlene's need for childhood safety. The hacking elements of the show undoubtedly born from 9 year old Elliot spending time at Mr. Robot computer repair with a smile. The anon-mask that the show uses comes from an in-universe movie that Darlene and Elliot watched every Halloween and their base of operations is Coney Island. A place that both siblings seem to associate with safety and happiness...
Which is extra messed up when you factor Season 2's revelation that Darlene was kidnapped while on a family trip to Coney Island.
Darlene's panic attacks, need to feel special and her abusive upbringing are not the topic for this essay, but I wanted to make mention that Magda was such a horrible mother that a 4/5 year old Darlene thinks of being kidnapped from a family trip to Coney Island as one of her most precious childhood memories.
The desire to reach into the past and change things to create an ideal future is a heavy theme of the show and I feel it's important to note that though the Alderson siblings reject Whiterose and her scheme, they are both living in an almost literal fun house distortion of the few unambiguously GOOD childhood memories that they each have and have wrapped them around themselves like a protective blanket.
The plot of season 1 gets a lot more uncomfortable when you realize how much of Fsociety is two traumatized kids recreating positive elements of their childhood and trying to live inside of those memories while lashing out at those who took their father away from them. The entire plan is centered around events from 1995. The show takes place in 2015.
Mr. Robot himself is, of course, the ultimate symbol of that take on events.

Edward Alderson was a monster. He's referred to as such overtly in Elliot's detox fever dream. Everyone asks him who his "monster" is while handing him the key that we learn was to his childhood bedroom. A key that he hid to prevent Edward from entering his room late at night.
Yet throughout the first 3 seasons of the show we are only shown him in context of the positive memories that he and Elliot shared. Elliot was 9 years old when Edward passed away from leukemia.
At a point, Elliot is picked up from school. He has a bruise on his cheek and the scene begins with Edward asking "If I had to guess, you didn't tell Principal Howard your side.", assuring him it's okay to share his side of the story. Because Edward is convincing him to tell his side I am going to assume Elliot got into a fight but it's not impossible to assume that the school pulled Edward in to discuss the signs of physical abuse on the child. Edward would never tell Elliot to tell his side of that story so I assume it was a fight.

It's unclear if Mr. Robot is the one who participated in those fights (we only have 2 confirmed instances of Elliot's alters showing up in childhood. The window incident and the day Edward died) but Edward picks him up and protects him from his mother's wrath and bonds with him during that drive, he reveals his diagnosis to Elliot before inviting him to work with him at the computer repair store. Likely this is what leads to Elliot's hacker skills being born.
A hauntingly similar event in my own life is why I am a photographer.
Given that the majority of Season 1 has Elliot in the dark about his condition we are only given context as to why he is the way he is and see the display of dissociative symptoms which manifest from CPTSD. Mr. Robot existing at all is actually not required for this to be a good depiction of adults who grew up in abusive environments and the way they maladaptively cope.
I also want to give a little praise to the "itch at the back of [Elliot's] head" that shows up when he feels the desire to hack someone or dig deeper and the way he pushes forward with his own will until he calms down enough to let a creeping hesitation overcome him and prevent him from acting.
Passive Influence is part of DID. It's a situation where a "fronting" (that is to say part that is in control at a time) performs an unthinking action or is emotionally swayed by the influence of another part/alter that is not presently conscious. These are one of the biggest ways that the condition flies under the radar for many. When they are close to discovering proof of their condition they will often feel an unconscious push away from it. The phenomenon is fairly easily brushed aside internally as "a gut feeling" or an "impulse" but it's observable under the right conditions.
An instance I can think of in my own life is when our survival part is trying to push people away and our emotional part desperately tries to reach out. I will often find my hand grabbing a person's wrist and clinging tightly to it without even noticing that I've done it.
In the show Elliot is compelled by Mr. Robot when he feels someone is a danger or has a weakness that can be exploited. Part of him knows he needs to do something about it and so he lets himself be guided.
The season ends with The 5/9 Hack succeeding, all the financial data being encrypted and Elliot sent to prison for (minor) hacking charges.
He knows who Mr. Robot is now and he fears him as his enemy.
Season 2 (and the book): Exploration
The first 8 episodes of Season 2 are a filter for those watching the show, many drop off. Personally I love it but I can see why it's not for everyone. Season 2 is much slower than the first and Elliot is in prison for those 8 episodes. He's also imagining that prison is his mother's house.
That daydreaming coping mechanism is largely there to add a fairly unearned sense of mystery to a character development season and make things a little more visually interesting. For the most part I don't really want to focus too much on it or the way Elliot treats "us"/"friend".
The fact is that for this season Mr. Robot and Elliot are in direct conflict but they are feeling out their landscape and trying to find common ground. They are pulling in different directions but they are reacting and responding to one another. The show uses a chess match as a visual symbol of this and in such they are keeping one another in a constant state of check. They are opposed to one another but they are communicating and working things out.
So let's start by looking at the book. The book is a recreation of the in-universe journal that Elliot keeps while he is in prison. We see him writing in it during the show and the entire thing is available, it even includes little ARG elements to let you decode the messages Mr. Robot is receiving from The Dark Army.
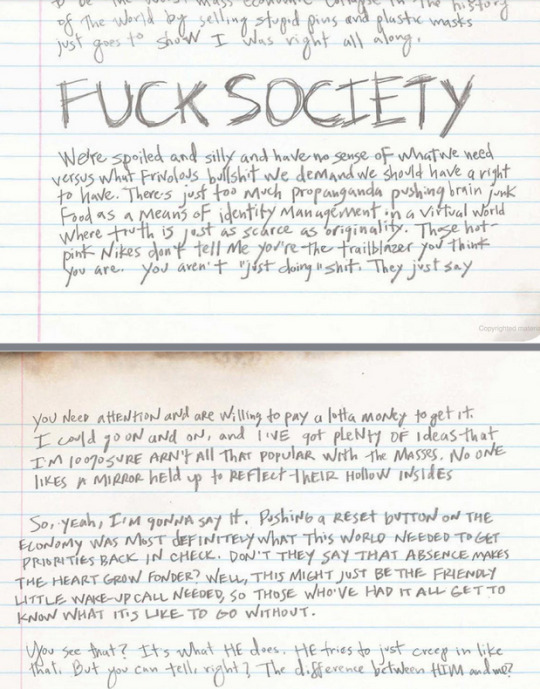
The book is detailed like this and it's possible to note when Elliot's handwriting turns into Mr. Robot's handwriting. There are even points where there is "blended" handwriting. It's easy to spot in the above image because Mr. Robot writes with a heavy hand and in all caps where Elliot is soft and uses lower case, in the top line of the second page "you NeeD atteNtioN aNd aRe Willing to pay a lotta MoNey to get it." you can see Elliot slipping from one headspace to another while becoming upset at society.
Even still if you look above the FUCK SOCIETY image you see Elliot's calmer handwriting as clear and flowing.
When we were in denial of our condition we poured through journal after journal and chatlog after chatlog hunting for evidence to prove or disprove the theory.
It was when I looked at our old gaming journals (we took notes in pen/pencil live during TTRPG sessions because memory issues are gonna memory issues) that we noticed similar. Cursive used in some phrases, individual letters separate on another, the letters g and y getting curled at times and not at other times.
Subtler than what is displayed above but no less real.
Season 2 introduces us to Ray the warden brilliantly played by Craig Robinson. He empathizes with Elliot because he speaks to his dead wife as a means of coping with grief and assumes that Elliot is the same.
He offers Elliot guidance by asking him to play chess "against himself" and this leads to Elliot and Mr. Robot playing endless games of stalemate against one another with deletion on the line for the loser. It's the same brain and neither side wants to lose (nor do they truly want to win, Elliot admits as much in Season 3 that he likes having Mr. Robot and misses him when he's not around) and as noted above with passive influence, the games are always guided to end in a stalemate because no matter how opposed they are as forces, they both want the same things.
So... how about the Sitcom episode?
Elliot breaks his promise to Ray and looks at the website that he is tasked with doing tech support on. It's--- not good.
Ray uses a combination of crooked cops and convicted Neo-Nazis to have Elliot beaten into submission so he won't report what he saw. Elliot cannot handle this and has a mental break and wakes up in a 90s 4 camera sitcom world.

Alf is there. Because old episodes of Alf are playing in the medical ward at the time Elliot is being treated for his wounds.
The entire time he is taking a beating Mr. Robot is protecting Elliot by fronting and forcing him into an inner-world fantasy.
Okay... so Inner-Worlds.
In the show we actually had one of these in Season 1 during the detox trip but I want to talk about it now and round back and talk more in Season 4.
Inner-Worlds are a thing within DID treatment. Emphasis on the word treatment. It's one of the more commonly misunderstood things within discussion on the condition because it's regularly reported as part of the experiences within those who are diagnosed with DID but it's important to know that the existence of the diagnosis indicates the existence of treatment.
During any adapted 3 or 4 phase trauma treatment program that includes parts work, whether this be Internal Family Systems model which is used for individuals who do not have DID or system mapping and stabilization for those who do, the patient must work on creating a "meeting" space to visualize (or sense out emotionally for those with aphantasia) and much of the work of developing safety and structure within comes from filling that space with comforts and generating communication between parts.
I'll talk more on the "conference table" in Season 4.
It is possible for those not going through therapy to create one outside of the context of a therapeutic alliance but the creation of one is an intentional act. Not something that comes free with your childhood trauma.
Elliot's trip to the inner-world keeps him from experiencing any of the beating that the body is receiving and at the end Mr. Robot earnestly says he only wanted to take the punches for Elliot, nothing more. Elliot falls against him, tearful and whimpers out "Thank you" before we are given the flashback of the day Edward picked up 9 year old Elliot from school after the fight and confesses his leukemia.
For the record, my heart swells every time I see Mr. Robot acting as a protector.
So, let's talk S2E9 and the "blending" incident.
Blending is what happens when two parts/alters are co-conscious and are present enough that they are sharing control of the body. It's an uncomfortable experience. Co-Consciousness means that more than one part/alter is actively perceiving the world at any given time.
It's more complicated than binary yes/no. Every one of these experiences exists on a spectrum and no two people with the condition experience it quite the same way but there are levels of presence that one has.
The following is me talking more from anecdotes and personal experience than textbooks. I like to be clear when I'm not being academic because I do not want to spread misinformation in my arbitrary analysis of TV shows that will get 20 notes on Tumblr Dot Com.
Front is to be driving the body, to have your inner monologue playing (if you have one, most people do, but it's not a given) and have your emotions interact with the nervous system if you are grounded enough to feel your experiences. As I said, it's a spectrum. Everyone gets dissociated at times and can just go into auto-pilot or a trance. That all still counts as being in front.
To be conscious but not front is to exist in an emotionally reactive state. If Fronting is driving then co-consciousness is to be in the passenger seat.
It's truly difficult to describe and my therapist doesn't even fully comprehend it despite her being the one who educates me on these topics. Presently as I type this I can only feel one of our system (5 parts) active and "with" me right now. She's not speaking but she's reacting. I can feel her apprehension to us typing this much about our personal life, little flits of paranoid thinking that we'll get anon-hate or that people from our former life will see this and judge us. It's a presence and exists on a gradient. She's "awake" right now but I do not consider her fully "co-con" because if I asked her to tell me what she thinks about this sentence I can feel an emotional reaction (apprehension) but not a direct answer akin to "I think you should edit out references to our journal and focus on talking about the show" (which is what I imagine she would say right now). That's the spectrum.
Closer to the front a part/alter is the more direct communication happens.
There's also "asleep" and "dormant" when they are unresponsive. Pretty self explanatory. Elliot's system has 5 parts(plus "friend") and until Season 4 we only really see Mr. Robot and the main character version of Elliot. Magda and Young Elliot show up in hallucinations in Season 1 and Young Elliot is co-con in Season 4. Magda never shows up outside of emotional flashbacks and the inner-world.
So after Elliot and Mr. Robot combine forces (though Mr. Robot is still working with the Dark Army and is trying to move in secret) they have moments where they rapidly switch and cannot keep straight who is fronting at any given time.
There's a scene where Elliot is in another room thinking to "friend" when he hears an argument in the next room and realizes Mr. Robot is in the argument. As he walks in, Mr. Robot is surprised to see that Elliot is aware when he is fronting and he trails off and they switch.
Mr. Robot says that something feels off about how they are acting and that they feel like they're overheating.
A later scene depicts Elliot phasing out mid-conversation on the subway and picturing himself in the next car observing Mr. Robot talking to Cisco while a passenger plays erratic music on a keyboard.
That is such a horrifyingly accurate depiction of something we live with that I was stunned to see it on screen. I've included it in some of my stories that go over living with these experiences but the idea is when we are stressed out, can't keep our head straight and are blended like this we tend to have snippets of music playing over and over in our head. We also get what I refer to as "static" and that seems to be relatable in support groups.
A++ for the show depicting something about the DID experience that simply does not get spoken about outside of the spaces of people dealing with it. It was the moment I knew they actually spoke to people who experience this stuff and did proper research that wasn't just media depictions and medical textbooks.
The final part of Season 2's wild ride I want to talk about is the "lucid dreaming" bit.
Mind awake. Body asleep. Mind awake. Body asleep.
This again goes into Overt DID which I cannot comment on as much as covert depictions but the idea is that Elliot trains himself to remain awake when Mr. Robot takes over. We have seen from the blending experience that he is starting to remain when Mr. Robot is active and so he tries to force himself to stay when Mr. Robot is active.
In therapy this would be achieved through trust, communication and awareness. It's said in communities that systems tend to become more overt as they go through treatment as they are able to identify lines, parts can advocate for themselves and there's better understanding of what "self" means for every alter.
In my experience there's also an element of trying to pretend to be consistent and whole. We were coming out transgender when our therapist guided us towards DID diagnosis and there was a lot of tearing ourselves apart because we needed to act in a certain way for our safety and inability to do so put us at risk of being targeted. In accepting our system we have stopped trying to be the same individual and that has lead to a more overt presentation. As I tell my therapist "we need to act out our gender expression anyway. Every action we take is a performance."
That is to say, Mr. Robot has never attempted to maintain the illusion that he is Elliot Alderson (albeit he never identifies himself. He's even surprised to learn that Elliot calls him that) and Elliot doesn't even know he is "The Mastermind".
In opting to remain hidden and conscious he gains a greater degree of control and agency in his situation.
These things get easier as you learn your condition, build system trust and allow yourself to experience that which you feel comfortable experiencing. With the example of the beating earlier, Mr. Robot shut Elliot out and took the beating for him and Elliot resisted but ultimately did not want to be present. In this episode he learns that if he wishes he could have pushed through and been there and experienced everything, albeit as a passenger rather than the driver.
Therapy also teaches how to "go into the back room" to maintain stability. A technique that lets you volunteer to not be involved in a situation. My system all use this whenever I (Dawn) perform erotic intimacy of any kind. They cannot handle the thought of associating with those acts and prior to treatment it would emotionally disregulate our nervous system if parts that couldn't handle the concept were to be present during those moments because parts of me would be trying to dissociate while I am trying to act. It would either trigger a switch, cause blending or make a part shut down and become unresponsive for a large period of time- one of our partners actually discovered our system this way. She saw us shut down during a scene and realized it wasn't just a "mood swing" as we had insisted.
Elliot learns how to intentionally open up and be present when Mr. Robot is active and because Plot happens he is shot and decides to use this skill to close himself off and create a stronger divide between parts.
Season 3: Rejection
If Season 2 was the pair working things out on a chess match where they keep one another in check then Season 3 is after Elliot has tossed the board and decided to shut Mr. Robot out completely.
The arc words are "battling in our own voids", in Season 1 Mr. Robot was always aware of what Elliot was doing but Elliot was unaware of Mr. Robot's actions and in Season 2 they were fairly co-conscious to the point of overheating. Season 3 the connection is shut down. Mr. Robot has no concept of what Elliot is doing and Elliot no concept of what Mr. Robot is doing.
This goes back to the Overt/Covert thing mentioned at the start. It's a rare thing even within a rare disorder to have that level of amnesia barriers between parts and so I can't really comment on accuracy. It's a frustrating season for me in that regard because Season 2 was doing so well at depicting something that I have lived through that going back to Fight Club tropes was fairly disappointing to me.
Season 3 is great by the way. It's a debate on if 3 or 4 is the best but it's close enough that there is a debate.
The real meat of the discussion, spare for the events of the final episode where they reconcile, is in how other people treat them and talk about their condition.
Angela Moss is Elliot's childhood best friend and also lost a parent to the disaster that claimed Edward Alderson's life. She discovered Elliot's condition during his breakdown in S1E8 and was brainwashed by the show villain Whiterose in S2E11 (I have a write-up of the psychological principals at play with the brainwashing here).
In Season 3 she acts as Elliot/Mr. Robot's handler and is responsible for helping Mr. Robot continue his hacktivist terrorism without Elliot finding out. She betrays Elliot and exploits his condition. She also tells people about it without his knowledge or consent, which is pretty fucking monstrous in my eyes.
Don't out a person. Just don't do it.
When Mr. Robot asks how she can tell who she's talking to she responds "Your eyes. You're never trying to look away." which is accurate enough that I messaged my girlfriend to be sappy and grateful towards her as the first time she noticed our condition she told me it was our eyes.
From a 2022 IM chat, shared with permission:
"it's ... well, it's [...] your eyes soften, kind of, when going to Cammie. Dawn has this piercing gaze, like she's looking right into my heart and soul. Camden is just very alert, noticing so many things but not the level of piercing. Cammie... her gaze is softer. More focused, but in a ... drinking everything in, rather than seeking it out sort of way"
and added today when I asked for permission to share the quote:
"(for the record, Craig draws his eyebrows down in a particular way that makes his gaze intense in a good way)"
The show works as hard as it can to never let the audience wonder who they are seeing on screen at any time. Most scenes where Rami Malek is depicting Mr. Robot it is a brief perspective view to remind us what the other characters are seeing before switching back to Christian Slater playing the character. There are a few scenes which involve Rami playing the character for a full sequence. One is the context for a flashback where we see a scene Slater performed through another character's eyes where they see Malek.
The others usually involve us being in Darlene's perspective to highlight her unease and uncertainty of what is happening with her brother.
The only scene where it is ever treated as a surprise is when Darlene plants a bug on Elliot's computer while staying overnight and is roughly interrogated by "Elliot", only to realize midway through the conversation "Jesus. It's you".
The camera cuts back to reveal it has been Mr. Robot the entire scene. They avoid that trick throughout the show so it has large impact when it actually happens.
I feel like that scene (as well as the scene where Elliot wears the real Mr. Robot jacket and gives birth to the 2 Stage plan to take down Evil Corp) are important for reminding that no matter how differently Malek and Slater play their roles, to an outside observer they are the same person and when he acts "out of character" it could easily just be an emotional outburst.
Incidentally you can see the physicality of the acting if you go back and watch it again.
The end of the season has Elliot, betrayed, alone and terrified for the safety of his sister; finally reach out to Mr. Robot and open a dialogue.
He even goes out of his way to have this discussion on the Ferris Wheel at Coney Island both as a Season 1 callback and as a sign of trust. Elliot admits in this conversation that he missed Mr. Robot while he shut him out and wants him to be part of his life and in the season finale Mr. Robot says that he wants the two of them to keep talking.
Elliot also finds out that the window incident wasn't his dad pushing him out of a window. They jumped. Elliot asks in a kind and soft way to Mr. Robot, representing both his protector and an element of the loving father he wished he had, "did you know?"
Mr. Robot, the one who jumped. The one who wanted to protect Elliot from Edward says nothing. But he finally feels an alliance form with Elliot.
The road to healing finally has opened.
Season 4: Integration and Fusion
So let's address the elephant in the room right away. The show uses the word "real" to describe the Elliot who existed before the show started and considers him to be the only legitimate alter. There is enough wiggle room within the show to think that is in-universe ignorance but the show does nothing to prevent the fumble at the finish line.
I want to say upfront and before I start dissecting this season that outdated models of DID believed that there was a crack formed in a person's sense of self and that healing involved restoring the identity prior to the crack.
This is 100% UNTRUE and it upsets me that people once believed it. DID is formed in childhood during a time of a person's life (between ages 4-9) where the child is taking in data from their surroundings and integrating it into their socialized survival mechanics to form a personality. The child is working out what traits it can exhibit to receive nurture, care and protection from other humans and will adapt to those processes. Attachment Theory goes into greater detail about how this relates to the formation of psychological disorders, especially personality disorders.
For a traumatized child they will find that their environments do not offer consistent and reliable safety and thus they are unable to adapt to a version of their reality where they are able to maintain stable safety. This may be horrifying forms of physical, emotional and sexual abuse placed upon a child and is often depicted as such but it can also be a confused child trying to get affection from a cold and distant parent or having a parent who abuses alcohol and becomes inconsistent in their ability to give affection and care. Child psychology is a heavy and depressing field, sadly.
The result is that the child never forms a permanent sense of identity. This is a large factor in the formation of Borderline Personality Disorder and is why DID and BPD are so often thrown together within medical treatment and diagnosis. It's at the point of which when my therapist gave me our diagnosis she presented a clinical list of "myths" regarding DID and "BPD is the same thing as DID" was 5 on the list of 6.
The point of this detour is to say that there is no original self. A person who has DID never managed to form a stable sense of identity in childhood and thus they find themselves acting as chameleons in their day-to-day life, adapting to what they feel they need to become in order to receive the things they need from their surroundings. It's why there is a stigma in the BPD community over the concept of being "manipulative". In reality people with that condition are unconsciously adapting to their environment as a survival mechanism. With DID the added layer of dissociation is there to help the self function even when they are forced to interact with materials that are incompatible with their ability to function.
Pre-show Elliot was living a fairly comfortable life but his emotional needs were not met and at the time he was alienated from his sister. He was miserable and lived in a society that he felt was crumbling. His daydreaming gave birth to "The Mastermind" to remove the threats from his reality and Mr. Robot who had been there all along went into Protective Sicko Mode and decided to expedite the process in a way only a protector's morality could.
We'll get into system roles a little later.
The point is that day-to-day life Elliot (Janina Fisher's book "Healing the Fragmented Self" refers to the part untouched by trauma as the "going about daily life" part) is not Real. He is not The Original. Those terms do not exist and are meaningless in this space.
True/Real/Orignal-Elliot is as much a construct as Mr. Robot. He's a version of Elliot who does not have to think about the trauma, he can just live a happy normal life. The kind that Elliot speaks often and derisively about in Season 1.

With that out of the way, I'm going to ignore the bad use of language and talk only about what is depicted on the screen and not said out loud. Because if you remove the misconception about real/original from the mixture, this is a perfect depiction of final fusion model healing.
Season 4 introduces us to the conference table in the inner world. A conference table is a therapeutic technique used in trauma therapy where you bring the alters/parts to a conference. The idea is that it needs to be a neutral ground where everyone is comfortable and able to share their thoughts and ideas. With practice it can be a space one can close their eyes and imagine, seeing their system and allowing communication to happen between parts.
Mine is based on the Minerals Gallery in the Natural History Museum in London. I refer to it as The Library. You didn't need to know that but I didn't want to discuss this section without mentioning it.
Elliot's is the conference room in Evil Corp where he and Tyrell spoke in the first episode.

Interestingly enough there are only 4 seats in this set. I'm not sure what the implication is here as in the scene depicted above Magda (Persecutor Alter) is scolding Young Elliot (Child Alter) for sitting in a chair that isn't his. They mention all 3 alters who are not present (Elliot, Mr. Robot and The Other One).
My thought is that this is the show going all in on the idea that Elliot ("Real") is not an alter and does not take a seat at the table. Which I have issues with.
I'll note as I did with the inner-world that this is a therapy technique and not something Elliot would just have in his mind. It's an accurate depiction of DID treatment but Elliot isn't being treated for DID. Krista is no way near close enough to be able to help Elliot. She's wonderful and deserves the world and more for how she handles things in this season but she's in the pre-stabilization phase of therapy where she knows more than Elliot is willing to accept and needs to wait for him to come around.
Speaking of Krista. Episode 7 is the greatest hour of television rivaled only by Ozymandias from Breaking Bad and the M*A*S*H finale. At present it has a 9.9 on IMDB.
The episode is structured as a bottle episode in way of a 5 act play depicting the stages of grief. This is the episode where Elliot peels back to dissociative layers and understands the truth. The truth of what his father did.
I won't type it.
I don't need to.
The next episode involves Elliot seeing Young Elliot and following him to a museum exhibit with a model of Manhattan. In Season 1 when Elliot had his psychotic break after realizing Darlene is his sister Darlene and Angela checked this location stating it was a place he used to go in times of crisis.
It turns out when he was young Elliot hid the key to his bedroom here to prevent Edward from getting in. All these years later adult Elliot (or "The Mastermind" if you prefer, which I do not) discovers it and has a heart-to-heart with his younger self, screaming into the emptiness that he's sorry for not protecting him. Sorry for letting him get hurt.
The scene is lit in the golden hues that symbolize safety in this show. The final season also takes place during Christmas in New York so it gets to show off that color palette more often which is great for symbolism and aesthetic.
Young Elliot shows that the act of hiding the key from their father was protecting him. It was fighting back. Sometimes surviving is the best you can do and you need to forgive yourself for not being able to do more.
God I love this show so much.
That episode ends with the scene I most want to just overtly show off to an audience.
youtube
I already loved the show. The final episode may have broken my heart a little with its talk of "Real" but this scene? This scene gets it.
Prior to the above video clip Mr. Robot cautiously approaches and says "Hey, kiddo". Something he always says. It's who he is. Regardless of anything else he, Mr. Robot, is designed from the father Elliot wishes he had and when he hears Mr. Robot-- no Edward's voice he tenses up in terror, allowing the above scene to take place with Mr. Robot so scared that he has failed as a protector by allowing Elliot to remember and that he cannot be there for him any longer because of who he is based off of.
Those with the condition commonly create alters who are based on the traits of those in the child's life at the time the symptoms developed. I... have experience.
The lines I want to focus on the most are:
Mr Robot: If I could go back in time and change everything that happened to you... just make it all go away...
Elliot: Then I wouldn't be me... *He turns to finally look at Mr. Robot* ...and I wouldn't have you.
The final arc of the show is where the "Mastermind" twist takes center stage and Elliot enters his inner-world and finds out that he created a peaceful reality for "Real" Elliot to exist in so that he is unharmed by the horrors of the world that is crumbling in reality. Mr. Robot, as a protector, wanted to expedite the whole hack and destruction of capitalism in order to rescue "Real" Elliot from the inner-world prison. In time he came to accept "Mastermind" as a part of the whole and not a rogue alter who was endangering the body and their "Host".
S4E13 lays it all down. An imagined version of Krista speaks directly to Elliot and explains the system and their functions. Mr. Robot a father and protector who could prevent Elliot from intolerable situations. Magda, a persecutor who blamed Elliot for the abuse. Young Elliot, who Elliot could push the traumatic situations on, a common thing that many do unconsciously in CPTSD situations, dissociating from the person the trauma happened to, disconnecting until they are just another version of self.
Elliot then says "I guess she doesn't know about you." referring to us, the audience.
Krista(*) looks into the camera and addresses us directly, calling us the voyeurs who pretend we're not a part of it even though we have been here for it all. She even claims we are on her side in getting "Mastermind" to accept he is a constructed personality who was there to lash out at the society that caused him so much pain.
"You loved him so much you wanted to keep him safe, no matter the cost."
The episode ends with "Mastermind" Elliot waking up in a hospital and reuniting with Darlene only to realize that she has known the entire time that the person we have been following throughout the show wasn't her "real" brother.
...and god damn it I hate this element of the show so much.
I'll accept that they had very little time to clean things up and needed to get a way to have Mastermind agree to the fusion. I'll even demonize Darlene and say she was being selfish and ignorant in saying something hurtful because she missed the version of her brother that existed before Fsociety.
But Our version of Elliot says that he loves her and she doesn't reply. Her disappointment and resignation causes Our Elliot to go back inside and agree to the fusion.
The show ends in a first person perspective of Darlene seeing her "real" brother wake up and that's it. I'm glad we never actually see "Real" Elliot, that feels fitting.
Here's the thing about that last minute fumble though.
Let's talk about Integration and Fusion. They are different things.
Integration is when dissociative barriers come down. The system is stabilized to the point of which the alters are capable of communicating openly, sharing thoughts, memories and experiences and every part has the ability to opt in or out as life goes on.
"Functional Multiplicity" is what happens when a system is in harmony, no memories are being withheld and the system is able to go about everyday life with minimal disruption or disregulation. It is a valid goal for trauma therapy and there's a decent amount of medical stigma around it being used as the goal and not a step towards the goal. Many clinicians prioritize the appearance of normalcy over the function of the individual(s).
Fusion is when you go the extra step and take this communication and sharing of memory and experience and as you tore down the dissociative barriers you tear away the division between parts.
A system is made up of parts that make up a whole person and Fusion is the process of all parts uniting to "become" that whole person. It is a valid and normal goal for treatment. It shouldn't be held up as the only legitimate method of healing but it shouldn't be demonized for being an option. I say this because I have seen some people in support communities get real upset when the topic comes up.
The final sequence of the show, prior to Elliot opening his eyes, involves the system at the inner-world conference table agreeing to go through with it and walking towards a cinema screen. Elliot says this will only work if we go too.
The family (and audience) sit down in the movie theatre and memories flood onto the screen and pour out until all experiences and emotions are shared in one pool and Elliot Alderson opens his eyes with all 5(+audience) alters fused into one.
It was almost perfect if only Darlene hadn't have rejected the "not real" brother.
The cinema screen projecting memories, all the thoughts and experiences being shared as the Alderson System accept their parts in the whole and agree to the process? It was a beautiful visualization of a healing journey.
There are imperfect moments here and there. There are great moments I skipped over such as S3E8 (I'm not up for talking about Self-Deletion today) but all in all it's the best depiction of DID for a main character we'll likely get on TV. It's a whole and complete narrative and I love it so much. It makes me feel seen.
#dawn posting#mr robot#dissociative identity disorder#elliot alderson#did#plurality#domo arigato mr alderson#media myself and i#watch me post my trauma in public#Youtube#media essays
125 notes
·
View notes
Text
Plurality is being “more than one” in some way.
Being a system is being “more than one” in some way.
Disordered? You can use the term plural or system.
Non-disordered? You can use the term plural or system.
Trauma-formed? You can use the term plural or system.
Non-traumagenic? You can use the term plural or system.
Created, intentionally or not? You can use the term plural or system.
Median/not completely separate? You can use the term plural or system.
Purely psychological? You can use the term plural or system.
Spiritual? You can use the term plural or system.
Fictive-heavy? You can use the term plural or system.
Non-human sysmates? You can use the term plural or system.
Two folks only? You can use the term plural or system.
1000+ folks? You can use the term plural or system.
Formed when you were little? You can use the term plural or system.
Formed when you were older? You can use the term plural or system.
Figured it out via tumblr or tiktok? You can use the term plural or system.
Literally the only requirement is being “more than one”. That’s how it’s been since the 1990s. The DSM/ICD/etc requirements are only for clinical cases. It isn’t the be all and end all for ALL systems, and science doesn’t prove ANYTHING about systems beyond “yeah there’s something going on here”.
Be kind to systems or plural folk different from you. The boots some of you are licking want to stomp on all of us, your system included.
We’re stronger together.
#actuallyplural#actuallymultiple#plural systems#plurality#multiplicity#syscourse#endo safe#endo positive#sysmeds fuck off
399 notes
·
View notes
Note
Hello, recently discovered we’re traumagenic with a headmate that has pseudomemories that he always has been here, I always did believe him and thought we are endo, but I have P-DID probably.
Could you explain about how does P-DID works, and systems that don’t have derealization dissociation, only other multiplicity related symptoms
/genq
I’m sending this ask again lol
Hello to you both! (we didnt get it the first time so thank you!) It took us a long time to figure out we have P-DID because it's barely talked about in dissociative disorder spaces, and unfortunately our success in finding professional help has been scattered. (Though it's going well currently!) So we hope we can help in this info!
Here's the link to the ICD-11 page on Partial DID. It starts you off on some information!
We're not a system without a dissociative disorder, but we can say that systemhood has to cause distress or impairment to qualify as disordered; to answer your second question, any system that doesn't meet those qualifications doesn't have a disorder relating to their plurality. Every system works differently, but the axis of distress or impairment is what denotes whether or not a system is considered disordered. For example, some traumagenic systems do not experience these things and therefore would not fall under a disordered status, and some endogenic systems may experience such things due to reasons like how their plurality interacts with other neurodivergencies or trauma induced after or unrelated to the system's formation.
As for how P-DID works, we realized that this is how we operated upon comparing the ICD-11 criteria & description to many different disordered systems talking on their experiences. The understanding came when we realized that the difference is not that others can't share front or communicate, as "partial" might seem to imply, but that the main fronter is incapable of completely leaving front to be replaced by another alter. For us, this manifests in the main fronter (the Prism Subsystem) being a median subsystem that is always stuck in front, despite how many times we split. To get a little personal about this, this is due to our trauma being specifically tied to being required at all times without respite, so regardless of how many parts of us we split, we're mentally unable to allow ourself to truly let go. We have many other alters & other headmates that're not part of the host subsystem, but even though they're able to use the body as well, it's impossible for the Prism's consciousness to completely disconnect from front via being "asleep" or going into headspace. If I were able to leave front, then the term DID would be more accurate, but because other members can only "partially" front, this is a distinct source of both distress and dysfunction that alters our disordered presentation to the point P-DID fits better. It's a shame the ICD-11 is not considered as often as the DSM-5.
Thank you for asking! Sorry this took a while to get to ^^
- Lucis, Prism Subsystem
#pluralgang#p-did#p did system#disordered system#traumaendo#traumagenic system#plural community#prism subsystem
17 notes
·
View notes
Note
Why do you use the term severe to describe your autistic traits?
am assume you talk about this post, which is me copy paste @birdofmay post edit, so technically it not me call self severe but sina (birdofmay) call herself severe👍
(why not own self: level 3 & severe, is diagnosis & assessment thing, don’t feel comfortable give self. feel a little different than self dx autism [which am okay with] but don’t know how explain. because regression, am wait for updated document to see.)
gonna let @birdofmay if want explain why call herself severe, but here list reason why seen people call self severe/low functioning/other things autistic community find not okay, etc:
is what they diagnosed with
hard time learn new thing or switch language because is what they know entire life (bc is again what they diagnose with)
autistic community tend focus on level 1 & low support needs autistic and then call their experience “entire autism experience.” so severe ppl find helpful call self specifically “severe” “low functioning” to specifically say their experience of autism because it tend be quite different (many same but many different)
self identity (different from be force call it by others). —especially common where people labeled severe / low functioning autism & ID (many developmental disabilities but especially these people) seen as automatically not able know self not able do decision, how other people know better, and “actually you can’t call your own self [severe/low functioning] because that bad” is another version of it even if people who say that also autistic.
“high support needs” & support needs not quite same because support need not autism specific, it describe iADLs bADLs instead of autism symptoms only, someone can be allistic and high support needs, or autistic but high support because other disabilities. severe autism specific to how autism affect them.
^ on that, levels are DSM-5 thing, most used in the US after 2013 (maybe other country also use but US biggest loudest). countries who use ICD or if diagnosed before 2013 no have levels
some people labeled severe / low functioning & hate it (again self identify vs other people call you that different bc they not self identify). that okay too.
52 notes
·
View notes
Note
Hello yes please I'd love a post about possession and mediumship and how they may or may not relate to plurality actually
Sigh...like, I guess, but I have to preface this by saying this is such a huge huge subject so this won't even scratch the surface. Possession and mediumship has been a persistent and global phenomena throughout all of human history, with each belief system having a unique and rich history that each deserve their own examination and exploration. In fact the inspiration for doing the research was seeing two sentiments in the community that kept rubbing me the wrong way being firstly "the reason there's no records of endogenic plurality is because someone might think you're possessed by a demon and perform a violent exorcism on you" and secondly "the DSM and ICD recognise Mediumship and spirit possession as a form of endogenic plurality" which aren't necessarily completely wrong when you look into it, I just think are incredibly incredibly lazy and culturally insensitive gotchas.
Demonic possession is actually a very specific phenomena which different religions have different beliefs and approaches on how to spot and what to do about it, but other forms of communication with, or connection to, non benevolent spirits was widely accepted. Even in Christianity in Europe, which I guess is what we would all immediately think of when we hear 'demonic possession', there is the Cult of Saints that existed for over a millennia. There's actually a few accounts of demonic possession that retrospectively we can say with certainty match the symptoms of DID, but really this is down to the meticulousness of the records being kept, which anyone who's researched witch trials knows can suck ass the majority of the time.
The first documented case of dissociative identity disorder (DID) was in 1584. Though not labeled such at the time, Jeanne Fery recorded her exorcism in detail (with additional details provided in the records of her exorcists), preserving documentation of symptoms that exactly match those that are found in individuals with DID today. She had multiple alters, each with their own name, identity, and identifying features and had alters that would today be described as an ISH, persecutory protectors, and child alters. Her alters were associated with actions that ranged from helping her to heal to self harm and disordered eating, were audible inside her head, and could take control of her body to allow for various actions, conversion features, and changes in knowledge and skills. The alters resulted from childhood physical and possibly sexual abuse. Jeanne Fery was actually called ”the most perfect case” of “dédoublement de la personnalité,” the most perfect case of DID, by Bourneville, the man who reissued a book about her life in 1886 (van der Hart, Lierens, Goodwin, 1996).1
But when it comes to endogenic plurality as being something non pathological, or non benevolent, it's harder to draw the same kind of parallels between endogenic plural experiences that we see and hear about today with something like the Cult of Saints while you can draw several parallels between the Cult of Saints and other practices around the globe. Also interestingly, while there's very little written about endogenic plurality, there's a metric fuck tonne written about spirit possession and mediumship. So can you take that humongous body of research, scratch out "spirit possession" and "mediumship", and write in Endogenic Plurality? Fuck no, and it would be insanely racist to try.
What we can do though, is identity and categorise commonality between them and see what insights we can gather about humanity as a whole.
To that end, these beliefs and experiences can be summed up thusly:
Voluntary Possession - usually involving some kind of trance induction, a specific entity such as a spirit, someone who's died, an angel, or a deity briefly inhabits the body for a limited time for a specific purpose, usually providing some kind of insight or perform an act of healing
Involuntary Possession - these are your demons and your devils, often accompanied by a deluge of physical and psychological symptoms such as convulsions and outbursts of rage
The Ouchies - these are bad spirits that don't possess you so much as they hang around and play mischief with your body, causing ailments and issues that aren't medically explained. Nowadays we call them somataform disorders but we used to call them hysteria as well until like the 80s.
And The Voices of Temptation - these are the devils and demons that whisper in your ear from within, tempting you to perform socially unacceptable behaviours like kissing boys and drinking too much wine.
One outlier of this that I really don't know enough about is the Jinn of Islamic faiths.
Jinn are much more physical than spirits.[31] Due to their subtle bodies, which are composed of fire and air (marijin min nar), they are purported to be able to possess the bodies of humans. Such physical intrusion of the jinn is conceptually different from the whisperings of the devils.[32]: 67 Since jinn are not necessarily evil, they are distinguished from cultural concepts of possession by devils/demons.[33] Since such jinn are said to have free will, they can have their own reasons to possess humans and are not necessarily harmful. There are various reasons given as to why a jinn might seek to possess an individual, such as falling in love with them, taking revenge for hurting them or their relatives, or other undefined reasons.[34][35] At an intended possession, the covenant with the jinn must be renewed.[36] Soothsayers (kāhin pl. kuhhān), would use such possession to gain hidden knowledge. Inspirations from jinn by poets requires neither possession nor obedience to the jinn. Their relationship is rather described as mutual.
And honestly, that sounds really really fascinating, I need to look into that much more cause wow I did not know that.
On the subject of voluntary trance possession, the best candidate for finding signs of Endogenic Plurality, rather than the potential DID of involuntary Possession, there's actually been a lot of research into this. Several attempts have been made by the medical community to pathologise voluntary possession and they've largely failed. Like at the core of it, that's why these are listed in the ICD and DSM, because we tried to explain them medically and couldn't because these practices are rarely detrimental to the practitioner, they don't constitute a disorder. There's also been some choice comments by medical professionals where they essentially blame the belief on the inherent inferiority and suggestibility of the (poc) practitioners mind.
Viewed through a psychophysiological lens there's actually been quite a bit of scientific research into the biological function of trance and possessive states and we do actually see changes in brain area activation and activity, very similar in fact to that of hypnosis. Induction into a trance state often involves the use of rhythmic drum beating, group dancing, or the use of psychotropic herbs, so called ecstatic practices.
Mediums often score highly in certain specific criteria of the Dissociative Experiences Scale but low on others and tend to score better than average on mental health scores. So are they a potential example of Endogenic Plurality? Well Endogenic is more of a self identity label where one defines themselves as being 'more than one' in some way and you find very few accounts of mediums describing themselves in this way. The spirits they channel do not exist within them outside of trance rituals, but rather come from another plane of existence temporarily connecting with our realm through the medium.
However! There may be a parallel to be drawn between the brain activity of a trance state and the auto Hypnotic model of Paul Dell. Not everyone is capable of trance and possession, just as not everyone is capable of plurality or developing DID, but they all might use the same mechanism. The same mechanism that leads to psychosomatic symptoms and the placebo effect, behind Mesmerism and hysteria.
The way that this mechanism manifests might very well be sociocognitive in nature, being used and utilised in different cultures in different but very measurable and real ways. As such I think the most we can really say that these practices and experiences are linked to plurality, and there may very well be some individual and isolated cases of plurality in these practices, but that we shouldn't overwrite and erase what these practices are within their own contexts and definitely shouldn't be using them as rhetorical arguments and gotchas, that's the devil of colonialism on your shoulder talking and you should not be listening to him
#syscourse#system community#sysblr#plural community#pluralgang#actually did#did system#sysconversation
14 notes
·
View notes
Text
Junkrat and Schizotypal Personality Disorder
Upon some close examination (and projection), Junkrat's character appears to exhibit traits suggestive of schizotypal personality disorder (STPD). His eccentric beliefs, erratic behavior, and unconventional mannerisms align with the typical features of this disorder.
Now I will say, I myself have some personality disorders so I have the need to project onto him (despite mine being cluster B & C and STPD being incluster A). This might lead me to project certain traits onto Junkrat as I analyze his character, so keep that in mind please.
On another note, if you disagree please just scroll past and don’t argue. I’m not saying this is canon or even implied, it’s just a headcanon and a silly little analysis that I wanted to do because I was bored.
Let’s get into it.
To receive a diagnosis of STPD, an individual must meet five out of the nine specific criteria. Not the full set, only partially. It is important to note that everyone’s experience with STPD will be different because of the many combinations that exist within the criteria.
I will be using the direct diagnostic criteria in the DSM-5. Though Junkrat is Australian and would use the ICD-11, I’m just not as familiar with that.
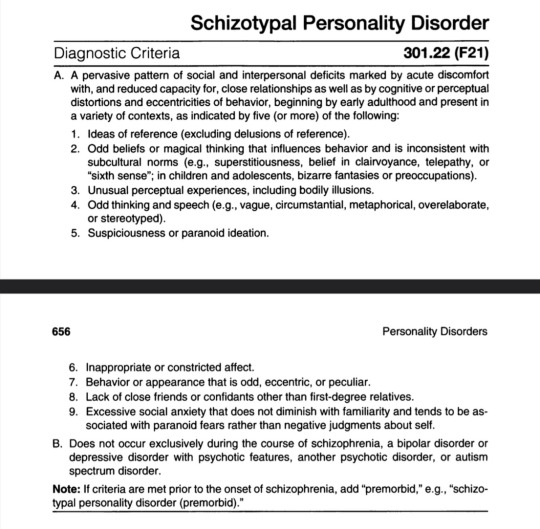
Ideas of reference (excluding delusions of reference).
Now to explain what that means; it is when someone will take an event that is unrelated to them, some random occurrence and think that they are the cause of it. They think that something is referring to them when it is not, hence the name. One of the biggest examples of this is when one will see people laughing in public and think that they are laughing at them instead of something else. [source]
There is no canon examples or interactions or so on to suggest this, through what we know of Junkrat it is highly likely he experiences this. He tends to make things about himself and often talks about himself highly. Because of this mixed bag, I will give it a half point. In personality disorders, these half points are typically counted because of the complexities of these types of disorders. 0.5/9.
Odd beliefs or magical thinking that influences behavior and is inconsistent with subcultural norms.
This is when person believes their thoughts, feelings, or rituals can influence events in the material world, either intentionally or unintentionally. This is also common in other disorders such as OCS. [source]
Now, I’d say Junkrat most definitely has this. He has extremely odd beliefs about bombs and explosives among other things, as well as general magical thinkings. In an interaction with D.Va, he considers himself famous and suggests that they both need to keep their heads down. He’s a mad scientist with many extraordinary inventions, but he does not have the popularity that she has. That’s the only canonical example we have, but I still think it’s close enough to give a point. 1.5/9.
Unusual perceptual experiences, including bodily illusions.
These experiences refer to atypical sensory perceptions or sensations that deviate from what is considered typical or normal. These experiences can occur in various forms and may involve any of the five senses: sight, hearing, taste, touch, and smell. One specific aspect of unusual perceptual experiences includes bodily illusions. [source]
Now, I can’t say we have any canon examples of this other than maybe “Mum, I did it! I’m on fire!” which could say he senses his mother’s presence and is talking to her, but this is also a very common thing to say. Just referring to your mother, especially if she has passed, and talking to her. So no point for this. 1.5/9.
Odd thinking and speech.
Now this is in reference to vague, circumstantial, metaphorical, overelaborate, or stereotyped style of language. [source]
Junkrat’s way of talking is one of the first things I think of when I think about him. He most definitely has off speech patterns, overelaborate to be specific. He explains himself to an extreme and uses an incredible vocabulary at all times, no matter the circumstances. His thinking goes along with this, given some of his strange and eccentric ideas. So I’d say he has a point. 2.5/9.
Inappropriate or constricted affect.
This is when someone cannot feel the full range of “normal” human emotions or feel the emotions with limited intensities. Both flat and blunted count towards this as they refer to different levels of emotions. [source]
Now while we do not exactly see it, it is heavily implied that Junkrat is “happy” or “maniacal” most of the time. I would say he struggles to have most of the more negative emotions, which still counts towards this. So, another point for him. 3.5/9
Behavior or appearance that is odd, eccentric, or peculiar.
When it comes to this type of behavior in STPD, it’s not just “random lol XD” type of odd. This behavior would typically be perceived as unusual or unnecessary, without being demonstrably maladaptive. This is contrasted with normal behavior, the nearly universal means by which individuals in society solve given problems and pursue certain priorities in everyday life. [source]
Junkrat is basically the perfect example of this, he is half naked most of the time, has absolutely horrid posture, is constant twitching, and a lot of other things. He is very odd and eccentric in practically every single way, so he’s definitely getting a point for this. 4.5/9
Lack of close friends or confidants other than first-degree relatives.
When it comes to STPD, the symptoms and tendencies often make it hard for one to form any long lasting relationships.
We know that other than Roadhog, Junkrat doesn’t have any friends. While Roadhog is not a first-degree relative but he is a “bodyguard” so I feel like that bypasses this. Most of the other characters are unnecessarily rude and mean to Junkrat, showing he has no real friends among them. So I would say he gets a point here. 5.5/9
Excessive social anxiety that does not diminish with familiarity and tends to be associated with paranoid fears rather than negative judgments about self.
Social anxiety is an intense, persistent fear of being watched and judged by others. This fear can affect work, school, and other daily activities. It can even make it hard to make and keep friends. [source]
Actually Junkrat is very social able with little to any self-esteem issues (though I headcanon he had a little) so he doesn’t exactly seem to have any of this, no point here. 5.5/9.
And there we have it. Five and a half out of nine points. If he was real, he could very much qualify for a STPD diagnosis. Now there’s obviously factors like you can’t have schizophrenia, bipolar, schizoaffective, and blah blah so he could possibly be disqualified; but in my eyes he’s got STPD.
Now, again, this whole analysis is all for fun, shits and giggles if you will, so if you disagree that’s completely okay! Just don’t be mean about it, it’s just a headcanon/personal belief.
#overwatch#overwatch 2#junkrat#jamison fawkes#stpd#schizotypal#schizotypal personality disorder#character analysis#analysis
29 notes
·
View notes
Note
do you have any information on p-did? I just found out we're a p-did system and i dont have much info on it. like what kind of trauma do you need to get P-DID out of all the other OSDDDID spectrums? idk where else to get credible info from so im asking blogs i know have good information on DID
P-DID, or partial DID, is the ICD equivalent of the DSM's OSDD type 1, with a couple of slight differences in description of presentation. It's a little bit more open to some presentations that are... Kind of grey areas/unmentioned or implied in the DSM.
It's all the same kind of trauma, it's just describing presentation. Depending on the age that abuse starts, the length of the abuse, the type, frequency, and severity, and your own potential for dissociation, you'll end up with different combinations of symptoms.
Here's the ICD entry for partial DID, but I'll summarize really quick.
The main point is that there's one "dominant" alter, and that switching is infrequent. More, you'll have "intrusions" from these non-dominant alters (sounding a bit like 1a here). When switching does happen, it's typically covert. Overt would imply DID. There typically is not amnesia if switching occurs (now it's sounding like 1b), but there can be.
Boiling it down, it seems to describe one ANP and multiple EP, which are somehow covert (they're usually not because they're pretty damn emotional most of the time, hence EP), but much like with OSDD, I think many systems will agree that they have multiple ANPs.
The section for boundary with DID does a pretty good job of describing how it's different, and I think it's easy to follow.
I really hope this helps!! If you have any other questions, don't hesitate to ask!
57 notes
·
View notes
Text
Wanted to talk about some common misconceptions regarding terminology I see online while talking about OSDD
NOTE: I am not a psychiatrist or researcher, I'm just a student with a little medical experience! This is also not meant to discredit anyone or anyone's experience, I'm just trying to find the roots of terminology!
So, a lot of the times I see people talk about OSDD-1a and OSDD-1b, but when reading the DSM-V and DSM-V TR, there's no mention of a 1a or 1b. There's OSDD-1, OSDD-2, OSDD-3, and OSDD-4, but no specification of 1a or 1b. At first I just chalked it up to a community created specification to differentiate symptoms, but when reading a little bit deeper, I realized there's quite a bit more to it. After asking around and running in circles to find a potential medical root for these terms, I ran into a chain of misconceptions, mostly coming from the fact people don't read the DSM and just cite other articles. So here's some stuff on the terms OSDD-1a and OSDD-1b, from a medical perspective!
Before getting into the story, I just want to show the DSM-V so it doesn't look like I'm pulling shit out of my ass when I say OSDD-1a and 1b are not listed in the DSM-V. Pages 306 - 307 list the diagnostic criteria for OSDD, including specifications of OSDD 1 through 4.


(Cut since I'm using the PDF lol)
The criteria for OSDD-1 are similar to OSDD-1a and OSDD-1b, but not exact or separated. Even if you check the DSM-V TR (pages 348 - 349), it doesn't exist in there. I also checked the ICD-11 for clues, and found no references anywhere.
For reference, here are the common criteria stated for the two:
OSDD-1a: "Members of a system are less differentiated than in classic DID, but experience amnesia." OSDD-1b: "Members of the system are differentiated from each other, but do not experience amnesia"
I pulled the wording from the Multiplicity and Plurality Wiki and Pluralpedia, which the former refers to 1a and 1b as clinical while the latter refers to it as a colloquial term. Of course neither of these are credible sources, especially since the former states a blatant falsehood. So if they're not diagnoses from the DSM, where are they from?
Even good ol' Wikipedia mentions them but cites nothing. (See [Citation Needed], and none of its sources at the bottom of the page mention 1a or 1b either.)

A common source I see people direct me to when looking for answers is did-research.org, a site that aims to provide resources for, understanding of, and awareness of dissociative disorders. The article I'm often linked to, the only one on the site that mentions 1a or 1b, explain the differences between the two and between DID in a more academic way. [Comparing OSDD-1 and DID] It also mentions DDNOS, which will be very important later. But if you go down to their sources, none of them mention 1a or 1b, and both actually predate the DSM-V, which came out in 2013. [Here's the first source listed, and here's the second!]
And if you look around the site, you'll learn that the author is not a medical professional, but a med student, and that the site is not at all for research purposes, but just for awareness.
So if this site can't lead to the origin of OSDD-1a and 1b, it's time to turn back to the wikis and blog posts that talk about them and look at their other sources, one of which is the site traumadissociation.com. Which again, does not mention 1a or 1b. But if people read the sources that are being linked to them on other articles or blog posts, they'll spot something that looks familiar.

DDNOS-1a and DDNOS-1b, two diagnoses from the DSM-IV that merged into OSDD-1, with some specifications now being diagnosed as DID. And it's not like this information is only hiding in this site. Just Google DDNOS and all of the information linking OSDD-1a to DDNOS-1a and OSDD-1b to DDNOS-1b is right on Wikipedia!


But of course Wikipedia cites faulty sources, but thank god we have the DSM-IV handy! On page 490, right at the end of the dissociative disorders section:

So OSDD-1a and OSDD-1b are not, in fact, current diagnoses, but are pretty much renamed versions of DDNOS-1a and DDNOS-1b; outdated diagnoses from the DSM-IV, which was published all the way back in 1994.
Which begs the question... Why?
Reading the diagnostic criteria for OSDD-1 is confusing, as it describes a multitude of different experiences and symptoms. OSDD as a whole almost feels like a broad swoop to cover all dissociative symptoms that can't be fit into DID. And with how damning getting diagnosed with anything can be, the confusion one must feel when getting slapped with a loaded diagnosis -- or realizing they fit into said category -- is pretty fucking confusing. So of course people want to go back to the thing that makes things a little neater.
Dissociative disorders are horribly under researched and misunderstood, and while it's so great that people are finally breaking out of the stigmatization and talking about their experiences, misinformation, large or small, can lead to more harm. Yeah, this is a minor thing with a term that can easily be uncovered if you Google for ten minutes, but I think a lot of this can reflect a larger issue within online mental health spaces.
I encourage everyone to look into what I linked, since if even one of y'all becomes a researcher that's going to make major strides for the scientific community, as well as for people who actually have dissociative disorders. Also, if I messed something up, point it out to me and I'll fix it!!
And for the love of god, please read your sources.
#osddid#did osdd#did#osdd#dissociative identity disorder#otherwise specified dissociative disorder#osdd 1b#osdd 1a#mental health
7 notes
·
View notes
Note
i don't even know if you guys are okay with this kind of ask, but im in a rough spot and any input or positivity would be delightful
cw for questioning? i don't know if i need to say that but i am haha. self fake claiming too
so uh. around a year or two ago was when I started learning about DID and OSDD. at that time, i felt like it explained a lot. like a lot a lot. the memory loss, the disassociation, the fluid identity feeling, the lack of memories before i was 13, among other things. i was really close to the host of a system I've known for years, and i was trying to figure things out. then i just lose the time, and suddenly, it's not 2021 anymore, it's 2023.
i do not have the resources to seek professional help, or i would. so I'm trying to research more. but the more i look, the more things get confusing.
for example: some people say you MUST be able to see an innerworld and hear your alters, and others say you don't. ive heard very little (that i don't even know if it was real), and can't see shit.
i know i have a lot of symptoms of DID, but i feel like even saying i could have it makes me look like im trying to latch onto a trend (which im not.)
i dunno. some people i know have said they think i have DID, but others say it's just Bipolar Disorder. it's not great and i just wish i understood everything happening
hey, sorry you’re going through a rough time trying to figure this out :(
for what it’s worth, no, you don’t need a visual inner world in order to have did. here’s the requirements (as we understand them, paraphrased from the dsm)
1. two or more distinct personality states
2. amnesia surrounding trauma, important information, or every day life events
3. symptoms that cause you to have significant distress or impairment
4. with symptoms not able to be attributed to spiritual belief/practice or
5. the effects of a substance (like drugs or alcohol)
that’s the official criteria in the dsm. here’s a link to the icd criteria - it’s a bit more complicated but there’s still no requirement of having an inner world.
if you’re a host, anp (apparently normal part), or main fronter of your system, it’s likely you won’t be able to have access to the inner world, other headmates, or many of your system’s memories at first. did works by hiding, masking, and disguising trauma, and it does this in a few different ways. one major way is by keeping those who handle day-to-day life separate from those who hold traumatic memories that otherwise would be too much to handle. in fact, it works so well as a covert disorder, many people don’t realize they have a dissociative disorder until well into adulthood, if they ever learn about it at all. so not having access to an inner world, other headmates, or certain memories is definitely normal, especially early on in the recovery process.
i understand you don’t have resources to seek professional help. here’s some free resources that may help you if you’re going to attempt self-diagnosis. we’re advocates of self-diagnosis (not everyone can afford quality mental healthcare), but it’s important to make sure you’re doing proper research.
truly we cannot recommend enough getting therapy to help with this. dissociative disorders are complex, and it can be incredibly difficult to try and navigate recovery on your own. if you tell us your country (you’re welcome to dm us) we can try to help you find affordable, state-funded, or otherwise non-profit therapy organizations in your area.
also, “self fake claiming” is a very common experience in did systems. some parts may want to deny the system’s existence as a means of protection from others, some do it to reasonably deny trauma, some do it because they’re afraid of what having a dissociative disorder might mean for them, some do it because dissociative disorders today remain heavily stigmatized. we’ve been officially diagnosed for around 6 months (after questioning for years), and we still have parts who adamantly deny that we’re a system at all. we understand this will change with time as we continue to grow, heal, and build trust and communication with each other.
sorry if this response was a bit fragmented or all over the place. we’re not trying to diagnose you here. we just want to provide you with some tools to continue your research along with dispel some worries or concerns you may have. hopefully this was able to help a little bit - best of luck to you!
🐢 kip and 💫 parker
18 notes
·
View notes
Note
If it's not too invasive, how did you get diagnosed with ASPD, and has it changed anything for you?
I don't feel too comfortable sharing a lot of details of my history online tbh but since I share stuff on my blog about mental health things and mention ASPD pretty often in the tags, here's a little summary for you from what I feel comfortable sharing under the cut.
I got misdiagnosed with BPD in my early 20s during a psych ward stay, which later turned out to be a misreading of my issues by the psychiatrist and therapists there. Over several years of receiving therapy, I eventually got diagnosed correctly (in my opinion) with ADHD, cPTSD, DID and Personality Disorder of the emotionally-unstable (read: not borderline type; the ICD makes a difference between EUPD-impulsive and EUPD-borderline, while the DSM-V lumps them together as Borderline PD which is also confusing as fuck when you don't have the borderline part of the disorder yet get told you have BPD because it's the universally more known label) and the dissocial type (ICD-10 version for anti-social PD).
In regards to the combined PDs, it just felt to me like getting the logical answer to some questions I had that I didn't know how to answer myself for a long time.
When I first got diagnosed with BPD I rejected the idea of having a PD entirely, mainly because I don't relate to more than half of the disorder's characteristics after having dug deeper into the matter. The other reason was the psychiatrist back then dishing it out together with a transphobic remark, saying that I cannot be a trans man because of my 'unstable sense of self' (that was just her team observing different alters during my stay there) and her own cissexist definitions of 'man' and 'woman'.
So when it got later changed to ASPD, I already had a clue of what was going on with me anyway due to the new found interest in human psychology and mental health conditions. I also had a complete lifestyle change from prior getting diagnosed with BPD, which got me into new hobbies and some low-key forming interest in becoming more pro-social because there's an arguable benefit of not fucking up your life to the point it could get me my freedoms revoked. Felt like I am having my shit together (which I didn't actually have, but I was good at making the dissociality more covert) for the most part until the pandemic, the lockdowns hit me with major setbacks and I pretty much regressed almost entirely to who I was pre-PD diagnosis in my early 20s.
In my last clinic stay (different one from the one mentioned above), the psychiatrist there told me that they have doubts about the PDs though, and said that my symptoms could also be explained with cPTSD which technically makes sense but... yeah, idk man.
I call bullshit because I don't have complete amnesia about my childhood and teen years and there's plenty of evidence for conduct problems that never saw any treatment during that time. Then again, I grew up in a small town in buttfuck nowhere with corrupt cops, useless social workers and plenty of crime, so I am also not surprised that I just could get away with my bullshit and I suspect that the DID also made it easier as well, since not all alters have the same intensity of anti-social symptoms and behaviours. I suspect that I have the combined PD label because some alters are more emotionally-unstable, and others are more anti-social.
I am also physically disabled (and tbh I struggle to even admit to myself that I am disabled even though a recent physical exam begs to differ) and I guess that my limited ability to get into physical altercations with other people due to said disability makes me apparently not 'violent enough' for them to give me the ASPD label I guess lol
4 notes
·
View notes
Text
mental health vent post
Anxiety attack anxiety attack aaah!!!
Anyways. For a long time I didn't look into bpd as a possible explanation for my identity issues, because I just didn't want to have that in common with Rhys. A little bit ago I did look into it, worked up the courage or whatever. Besides the dissociation, identity issues, and fear of abandonment, nothing else about it describes me. And even with the fear of abandonment, I remember seeing a comparison of the actual feelings involved behind 'fear of abandonment', which could mean a lot of specific feelings and fears and reactions, between bpd and avpd, and the bpd one I couldn't relate to at all (the avpd one very much).
Anyways. I'm just stressed about it. I've been stressed about it. I found out about osdd-1a, which is one of those things I've seen mentioned lots but didn't actually find out the details. It's something that was in an older version of the dsm, now only covered by osdd and usdd in the dsm, and not at all in the icd, but that people still use as a useful label to them to describe an experience that people have? But also there's practically nothing online about it besides the most basic overview. And if you get to more personal discussion about it, there's still hardly anything and people disagree about things. A common piece of advice strongly given about any dissociative identity thing of any kind is, 'don't jump to conclusions, talk to a therapist'. And I really really really do want to talk to a therapist, about so many things. Hopefully soon. But also I can't find anyone who says they have experience with all the things I want to talk to them about. But I guess I can just email them or have the phone consultation and see if any of them think it would be a good fit. I also just like. I don't want it to be that. Not because I hate systems but I just want it to be simpler. I don't want it to be so much. And it wouldn't even be, comparatively. The only explanations I've found so far for Identity Issues though are bpd and dissociative disorders, and it very likely to me seems to not be bpd. I really want an explanation for why I feel so wildly differently about things, and myself, and have different opinions, and priorities, and interests, and anxieties, and feelings towards people, and things I want in relationships, and an indescribable sense of self at different times. I don't feel like a cohesive person at all, and it stresses me out. And also the thing is I have one of those that's the best and I like the best and is the most Me, but I hardly ever get to feel that way any more. I want to more. It's a special occasion to me when I do. (Edit: Okay I also know it's normal to have different personas for different settings and people, but. This is still something I experience and bothers me when I'm by myself. Or it's more than one with the same person at different times.)
I feel better after getting to write this down, I'm going to try and calm down. Also I want to try grounding exercises more often because I basically am at least lightly dissociated or brainfogged A Lot of the time. Something I've done a lot is when I'm outside somewhere and I don't fully feel like I'm there, is I'll just be touching things like trees or the ground or a wall just to feel them. I also want to get in the habit of observational exercises too. Oh my goodness I didn't even talk about my memory. I went from very little memory of my history and life here to None memory of my history and life here. Only very little scraps I can pull up with conversation or prompting. I hate that. Okay okay okay I'm done, I'm going to go do something nice.
1 note
·
View note
Text
Hanzo and Obsessive-Compulsive Personality Disorder
I was joking with a friend about making the Overwatch characters have personality disorders, I realized that Hanzo very closely resembles someone with obsessive-compulsive personality disorder (also called anankastic personality disorder).
Now I will say, I myself have some personality disorders so I have the need to project onto him. This might lead me to project certain traits onto Hanzo as I analyze his character, so keep that in mind please.
On another note, if you disagree please just scroll past and don’t argue. I’m not saying this is canon or even implied, it’s just a headcanon and a silly little analysis that I wanted to do because I was bored.
Note: OCPD and OCD are not the same thing despite the similar names. Please do your own research if you want to learn more about the differences as I want to focus this on character analysis.
Let’s get into it!
Many may be shocked to know that OCPD is the most common personality disorder (not BPD like many may think). [source] So it is very likely that Hanzo could be one of these.
To receive a diagnosis of OCPD, an individual must reach four out of the eight specific criteria. Not the full set, only partially. It is important to notice that everyone’s experience with OCPF will be different because of the many combinations that exist within the criteria.
I will be using the direct diagnostic criteria in the DSM-5. Though Hanzo is Japanese and would use the ICD-11c I’m just not as familiar with that.
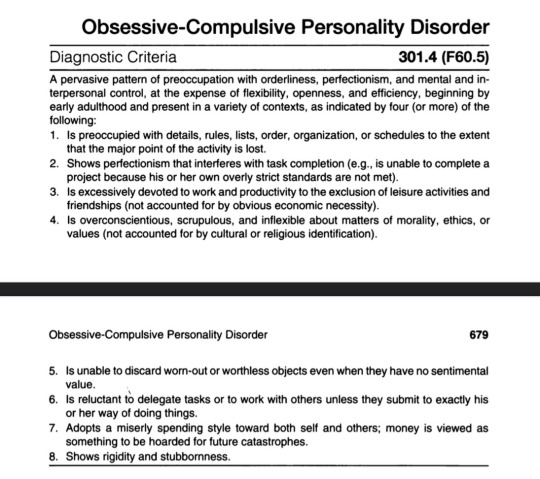
Is preoccupied with details, rules, lists, order, organization, or schedules to the extent that the major point of the activity is lost.
To maintain a sense of control, people with OCPD focus on rules, minute details, procedures, schedules, and lists. As a result, the main point of a project or activity is lost, as the criteria says. People with OCPD repeatedly check for mistakes and pay extraordinary attention to detail. They do not make good use of their time, often leaving the most important tasks until the end. Their preoccupation with the details and making sure everything is perfect can endlessly delay completion. They are unaware of how their behavior affects their coworkers. When focused on one task, these patients may neglect all other aspects of their life. [source]
Now while I personally believe Hanzo does this, from my understanding there’s no exact canon proof of him being preoccupied with these things. It could be assumed he does with all the later criteria he has that he is probably this way, but we don’t know for sure. No points. 0/8
Shows perfectionism that interferes with task completion
Nothing else matters except for being perfect. Things may never be completed because the need for it to be the best it possibly can be. Only the highest of standards for themselves. They have nothing in the tank to take care of yourself or attend to your hobbies or interests. [source]
Now while this can be explained from Hanzo being the eldest son and the pressure put on him by his father, that doesn’t negate the fact he does this. We know from dialogue with other characters he holds himself to a very high standard. So, that’s a point for him. 1/8
Is excessively devoted to work and productivity to the exclusion of leisure activities and friendships
People with OCPD may have difficulty in forming and maintaining relationships due to their perfectionist tendencies and devotion to work. They may have unrealistic expectations of themselves and others, which can lead to conflict and disappointment. [source]
This is pretty much the same as the last one. He isn’t tied to any organization and really has no friends or close ties to anyone. While there might be other explanations for this, I think it’s plausible he might not want to set himself up for disappointment. I’ll give a half point here. 1.5/8
Is overconscientious, scrupulous, and inflexible about matters of morality, ethics, or values
People with OCPD think actions and beliefs are either completely right or completely wrong. They often feel they are always right. It’s as if nothing will change their minds. [source]
Hanzo believes he is unforgivable and unworthy of anything. While this might be a more morbid belief that what is typically for OCPD, it still constitutes as one and would apply here. So sadly, he gets a point. 2.5/8
Is unable to discard worn-out or worthless objects even when they have no sentimental value.
Hoarding is a very common symptom in OCPD because of the fear of losing something.
While I headcanon this: we have no canon proof of it. No point. 2.5/8
Is reluctant to delegate tasks or to work with others unless they submit to exactly his or her way of doing things.
People with OCPD want to do things on their own without any help for fear of someone messing up their work. They typically deeply consumed in dysfunctional beliefs and genuinely see their way of functioning as the only "correct" way, where the world needs to conform to their own strict standards. [source]
This is very much Hanzo. He works by himself, a lone wolf, never with anyone else. While we don’t know if it’s exactly for the reason stated above, i would say it’s a plausible situation enough to give him a full point. 3.5/8
Adopts a miserly spending style toward both self and others; money is viewed as something to be hoarded for future catastrophes.
This one is pretty self explanatory .
Hanzo doesn’t have this, he gave away all his fortune. So, no point. 3.5/8
Shows rigidity and stubbornness.
People with OCPD are often described as “stuck in their ways” and “unwilling to change”. Such rigidity often manifests in a sense of hypermorality.
Hanzo is most definitely stubborn in every way possible. He doesn’t want to do anything except for his way. While he doesn’t have hypermorality, he is definitely ridged in his ways. Point. 4.5/8
And there we have it. Four and a half longs. If he was real, Hanzo could very much qualify for an OCPD diagnosis. There’s a lot of possible “stretching” and projecting; but in my eyes he had OCPD.
Now, again, this whole analysis is all for fun, shits and giggles if you will, so if you disagree that’s completely okay! Just don’t be mean about it, it’s just a headcanon/personal belief.
#overwatch#overwatch 2#hanzo#hanzo overwatch#hanzo shimada#ocpd#obsessive compulsive#obsessive compulsive personality disorder#obsessive compulsive pd#character analysis#analysis
14 notes
·
View notes
Note
With all of the PDs, how much of the criteria do you have to fit?
PPD: 4 or more
Suspects w/o evidence that people are planning to harm them
Preoccupied w/ doubts about loyalty & trustworthiness
Reluctant to share info about themselves out of fear that it’ll be used against them
Misinterprets innocent remarks or behaviours as threats
Holds grudges
Quick to get angry or [counter]attack people based on what they think are threats
Suspects partner of cheating
+ Must not be part of schizophrenia, other psychotic disorder, bipolar disorders, but can be premorbid to schizophrenia
SZPD: 4 or more
Doesn’t enjoy close relationships
Almost always chooses to be alone
Asexual
Finds little pleasure in activities
Lacks close friends, other than family
Appears indifferent to praise or criticism
Flat/cold emotional expression
+ Must not be part of schizophrenia, other psychotic disorder, bipolar disorders or autism, but can be premorbid to schizophrenia
STPD: 5 or more
Ideas of reference (not delusional)
Odd beliefs or magical thinking (not delusional)
Unusual perceptions/illusions (not hallucinations)
Odd thinking & speech
Suspicion or paranoia
Inappropriate or flat emotional expression
Strange behaviour or appearance
Lacks close friends, other than family
Social anxiety & paranoia about social interactions
+ Must not be part of schizophrenia, other psychotic disorder, bipolar disorders or autism, but can be premorbid to schizophrenia
ASPD: 3 or more
Doesn’t conform to social norms esp. in regards to the law
Deceitful
Impulsive
Irritability & aggression
Reckless & disregards their & others’ safety
Irresponsible
Lacks remorse
+ Must be at least 18, have had symptoms of Conduct Disorder before 15, & not be part of schizophrenia or bipolar disorders
BPD: 5 or more
Frantically avoids abandonment
Splitting, unstable relationships
Unstable sense of self
Damaging impulsivity
Self harm & suicidal behaviour
Mood swings
Feeling empty
Intense anger
Dissociation &/or paranoia
HPD: 5 or more
Uncomfortable w/o attention
Inappropriate sexual behaviour
Mood swings
Uses appearance to get attention
Speech mimics others’, lacks detail
Dramatic
Suggestible
Overestimates intimacy
NPD: 5 or more
Grandiose sense of self
Fantasies of success, power, etc
Feels special & unique
Needs admiration
Feels entitled
Exploitative
Lacks empathy
Jealous
Arrogant
AVPD: 4 or more
Avoidance b/c of fear of criticism, disapproval, rejection
Unwilling to have relationships unless certain they’ll be liked
Restrained in relationships b/c fear of shame, humiliation
Preoccupied with fears of criticism or rejection
Restrained in social situations b/c of fear
Views self as inadequate
Reluctant to do new things out of fear of embarrassment
DPD: 5 or more
Difficulty making everyday decisions
Needs others to be responsible for major areas of life
Difficulty being assertive b/c fear of loss of support
Difficulty doing things by themselves b/c lack self-confidence
Feels uncomfortable or helpless when alone
Urgently finds a new relationship when one ends
Unrealistically preoccupied w/ fears of being alone
OCPD: 4 or more
Preoccupied with details, rules etc so that the point of the activity is lost
Perfectionism that interferes with life
Workaholicism that interferes with life & relationships
Overly inflexible & hyperaware of morals, values
Things have to be done their way
Hoards money in case of future need
Rigid & stubborn
#long post#pd info#dogasks#these are from the dsm; the icd is a little different#no bold#ppd#ppd info#szpd#szpd info#stpd#stpd info#aspd#aspd info#bpd#bpd info#hpd#hpd info#avpd#avpd info#npd#npd info#dpd#dpd info#ocpd#ocpd info#diagnostic criteria#i could criticise these all day long but thats not what ths post is abouf
176 notes
·
View notes
Text
A Guide to DID & OSDD-1 —
|| The Fundamentals of OSDDID.
Written by an adult with professionally dx'd DID, who's had over two decades of lived experience and five years of dedicated research.
• What are DID & OSDD-1?
Dissociative Identity Disorder [DID] and Other Specified Dissociative Disorder Type One [OSDD-1] are complex dissociative disorders classified under "Dissociative & Conversion Disorders" in the ICD-10, and "Dissociative Disorders" in the DSM-5.
DID as defined by the ICD-10:
"A disorder characterized by the presence of two or more identities with distinct patterns of perception and personality which recurrently take control of the person's behavior. This is accompanied by a retrospective gap in memory of important personal information that far exceeds ordinary forgetfulness."
In the ICD-10, OSDD-1 is classified as "Dissociative & Conversion Disorder, Unspecified."
(Because of the difference between the ICD-10 and the DSM-5, and how common language surrounding the disorder is often based on the DSM, I will use the DSM-5 description to define OSDD-1.)
OSDD-1 as defined by the DSM-5:
"Identity disturbances associated with less-than-marked discontinuities in sense of self and agency [subtype 1a], or alterations of identity or episodes of possession in an individual who reports no dissociative amnesia [subtype 1b]."
Simply, DID is characterized by multiple identity & self states, each with their own separate narrative, somatic, and emotional experiences. These various identities can exert autonomous control when activated, and experience dissociative amnesia between each identity state.
OSDD-1 is very similar, but these identity states are less defined or distinct [subtype 1a], or the dissociative amnesia present between these identity states is most often limited to emotional experiences [subtype 1b].
(Note: These differences are subjective and can be fluid.)
• How do they develop?
OSDDID is developed through multiple factors, including: a genetic baseline for dissociation; unstable family dynamics; disorganized & fearful attachment to one's caregivers; repeated, intense trauma; and unresolved, inescapable stress in early childhood.
• What is dissociation?
Dissociation is defined as a disconnection & lack of continuity between thoughts, memories, surroundings, actions, and identity.
A natural response to trauma & inescapable situations, dissociation helps to disconnect one from their current experience. When a young child is in an inescapable situation, they will dissociate away from certain thoughts, feelings, actions, behaviors, and the experience itself.
This act helps the mind to compartmentalize these experiences, allowing the child to function in day-to-day life.
However, when these situations are repeated, overwhelming, and are unable to be processed in a safe environment (often because one doesn't exist), their dissociation turns pathological, or disordered.
Their dissociation bleeds into everyday life, and causes issues in function.
• How does dissociation develop into OSDDID?
Dissociation is the very base of these disorders, causing not only amnesia, but functioning as the formula for how these identity states - often called parts or alters - develop and interact with each other and the world around them.
Our fiancé wrote a thread explaining how alters form in simple terms and an easy-to-follow example. You can find it here (thread no longer exists 😭).
To get a little more in-depth, the currently accepted theory regarding the development of OSDDID and the formation of alters is "[the theory of] Trauma-related Structural Dissociation of the Personality." It states that when a child dissociates during inescapable situations, those experiences are compartmentalized into neurobiologically predetermined "action systems."
Essentially - alters are, at a very base level, a manifestation of these action systems.
From the ToSD:
"These systems are conceptualized as evolutionary based action systems that serve major functions, predominantly survival of the individual in the face of major threat, survival of the species, and management of daily life."
Alters are divided into two classifications according to the ToSD: ANPs and EPs.
I've written detailed, informative threads on these classifications. You can find them here.
[ANPs]
[EPs]
• What really are alters?
Objectively, alters are the dissociated identity states that form along the predetermined action systems described in the previous section.
Simply, they are compartmentalized experiences that have developed their own sense of identity.
In a subjective sense, alters are individual identities within a single person, who have their own ways of perceiving and interacting with their experiences & the world around them.
Alter identities vary in personality, as well as gender, orientation, age, appearance, and more.
These variations in identity and personality are due to the inherent differences in life experience caused by mental "barriers" formed through dissociative amnesia.
Your identity is the sum of your entire life experience. When you can't remember and/or feel connected to bits and pieces of your life, your identity will differ based on what experiences you DO remember and/or feel connected to.
For example, an alter who was only active during childhood is likely to identify as a child, since that's the sum of their lived experience. This lived experience identity will also factor in subjective beliefs formed through socialization & cultural "rules."
Example: a male child who's told "boys don't cry" may form an alter that identifies as a girl, whose function is to express emotions in a way a boy "can't."
It's important to recognize that the identity of an alter is very real, and very important to that individual alter.
That said, these identities don't exist in a vacuum, and may include harmful beliefs one learned in childhood, and in subsequent traumatic experiences.
Alter identities deserve acceptance, validation, and critical examination.
Their identity is as real as anyone else's, but may need to be more deeply assessed by the person with OSDDID and their mental health team.
- Transcribed from a twitter thread by @/ColubridC with his permission. Link to OG thread : https://twitter.com/ColubridC/status/1410820188950327299?t=jr7g56CEzp2kgWvB5yezow&s=19
#dissociative identity disorder#dissociation#osddid#did/osdd#educational#actually did#actually dissociative#dissociative system#psychology#twitter thread
24 notes
·
View notes