#symptoms of Heart valve
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
25% of US internet users with an annual income of $80-100K use Tumblr.
Text
youtube
India has emerged as a premier destination for heart valve replacement surgery, offering world-class medical care at a fraction of the cost compared to Western countries.
#Heart Valve Replacement india#Heart Valve Replacement Surgery india#Heart Valve Replacement Surgery Cost in india#heart valve replacement surgeon in India#heart valve replacement hospital in India#symptoms of Heart valve#valve replacement procedure#types of heart valve replacement#why choose india for heart valve surgery#Medical Care Surgery India#Youtube
0 notes
Text
Me: *gets my test in which I am supposed to give a diagnosis to a patient*
My patient: *Has ALL of the textbook symptoms of TWO DIFFERENT HEART ISSUES, a bunch of general symptoms that can be attributed to both of them, and a HEART ATTACK in history, which can cause one, but not the other, but both of them can lead to each other, and there's literally ZERO INDICATION which one is the main one*
Me: WHAT AM I SUPPOSED TO DO WITH THIS?!!?!?!!!
#HOW ARE YOU EXPECTING ME TO GIVE A FINAL DIAGNOSIS WHEN I HAVE NO INFO TO DIFFERENTIALLY DIAGNOSE WHO'S THE PROBLEM#I CAN'T DO THIS. ISCHEMIA CAUSING MITRIAL STENOSIS AND MISTRIAL STENOSIS WITH ADDITIONAL ISCHEMIA SYMPTOMS ARE TWO DIFFERENT THINGS#I CAN'T TELL YOU A DIAGNOSIS WITHOUT KNOWING WHICH PART OF THE HEART BROKE FIRST#(it was more of a question of 'who do we blame the CRVF on' and I did put stenosis as the main one but still)#also I should never listen to my groupmates because one of them threw me off even more by saying that right ventricular failure because of#Mitral valve stenosis can't happen. it CAN. it DOES.#what a total failure of a day honestly#med school diaries#med school shenanigans#med school stuff#med school#med student
2 notes
·
View notes
Text
God I swear I’m not trying to be all doom and gloom talking about my health I know it’s annoying I just really need a break and everyone irl is already done with my shit bc I’ve been too anxious to go back to the doctor bc the last one told me I’d just have to deal with it and potentially get more surgeries and I’m 23 dude. It took nearly 3 years before my doctor even agreed that that surgery was necessary and it didn’t even fully fix my shit it just lessened the pain — which I’m grateful for, don’t get me wrong! But I haven’t had full limb function in my left arm since I was 15 and they made it sound like the surgery would fix it and then acted like I was overreacting when it didn’t. And my left leg has been deeply fucked for nearly as long, and at least slightly fucked at least since I hit double digits, and has gotten progressively worse. So like I know, I get it that I need to go to a doctor, but why would it go better now? What’s going to make a doctor take me seriously now?
I want to be angry, but I’m too tired.
#chronic health#chronic pain#cpunk#cripple punk#tw surgery#I was told (in a nonprofessional capacity) that I should be screened for ehlers danlos syndrome#which matches a lot of my symptoms#and my parental units want me to get screened for pots#and a heart murmur#and mitral valve prolapse#and asthma but I’ve been tested for that within the last 5 or 6 years and seem to be fine in that regard at least#I don’t want to keep doing this man#I would really like to be healthy#I miss ballet a fuckton#and martial arts#and just being able to go places with my friends without having to plan out how to avoid fainting or pain flares#maybe hEDS#I don’t want to clutter up the actual tags with my hypothetical shit#tw vent#fever’s vibe check#feverdreamsandlucidnightmares
4 notes
·
View notes
Link
Heart Valve Expert in jaipur - Dr. Ravinder Singh Rao
Make an appointment with your doctor if you have any persistent signs or symptoms of Heart Disease that concern you. If you don’t have any signs or symptoms, but you are worried about your risk of Heart Disease, discuss your concerns with the Heart Valve Expert In Jaipur, Dr. Ravinder Singh Rao. Hence, call us Tel: +91-7891791586 and get more information
#Heart Valve Expert in jaipur#Best Heart Expert in Jaipur#Symptoms Of Heart Valve Disease#What Causes Heart Valve Disease#Heart Valve Disease Treatment#Dr. Ravinder Singh Rao
0 notes
Text
I wanted to put this one the previous post but it was long and this is a tangent but- In regards to the hypothetical "If House was my doctor I'd just tell him everything. Rip to all his other patients but I'm different."
The whole point of the show is that you wouldn't. Like a major theme of the show is about how the various shames and stigmas and habitual dishonesties that plague our societies both metaphorically and literally kill us. "Everybody lies" isn't just a cynical catchphrase, it's the shows thesis. Because of how we operate as a society, everyone feels compelled to suppress and hide things and that inevitably leads to suffering.
And there are plenty of episodes where this is obvious, ie "I cheated on my partner and gave them an STD." But there's also much more of "This little girl went through early puberty and because of the way our society stigmatizes women's bodies her single father never discussed puberty with her and she was so afraid and ashamed of her new pubic hair that she tried to shave it without telling anyone and mutilated herself, leading everyone to think she'd been abused and throwing off the whole case until House figured out her hormones were going crazy because she'd been exposed to her father's low T medicine, which he hid because of how our society regards masculinity, which he started taking because he began dating a younger woman (because of shame stemming from our society's unrealistic expectations wrt sex in relationships) which he was hiding from his kids, because of shame regarding our societies toxic views on monogamy."
A particular episode stands out as a really good example. S06E15 "Private Lives," which aired in 2010 but was fairly prescient about where social media was heading. The patient was a blogger who documented literally every moment of every day for her followers. She made it very clear she left *nothing* out, from her and her boyfriend's sex life to, eventually, asking for feedback from her followers on whether to get her heart valve replaced with one from a pig or a "vegan" plastic one. She handed the whole blog over to House as soon as he took the case and the team poured through the whole thing. Surely this is proof you're wrong about everybody lying, the team says to House. She's give us her whole life and you still can't find out what's wrong! Spoiler, it turned out the crucial symptom that allowed House to put it all together? Was the one thing she *didn't* include in the blog- Her bowel movements. Shame and stigma around talking about *poop* nearly killed this woman. It was also a detail that should have been picked up immediately by a normal doctor, who would have asked about her bowel movements as part of the standard checklist of diagnostic questions. But this woman was so confident that she'd laid out every relevant detail of her life in her blog, she wouldn't answer those questions, obfuscating what she was actually ashamed of underneath a pile of curated, rationalized, narritivized junk she could pretend was proof of a lack of shame and not simply a skill at creative writing.
When I say "I'd just tell House everything" is ridiculous, I don't just mean "well, because of the way the show works, you HAVE to be hiding SOMETHING." I mean literally, you- because you are a human being- are ashamed of *something.* And because you are a human being, the more info you try to give House the more deeply you will bury whatever it is you're actually ashamed of. And, because of the way the show works, that *will* end up being the key to what's making you sick.
3K notes
·
View notes
Text
oh, in the majority of cases my mom says "no, I never could, but your dad can and I always found it funny". that's actually why I'm asking her lol. the reason this whole possible EDS thing slipped by me until now, even with all the medical shit caused by my unstable joints years ago is exactly because my sister and my dad (and possibly even my grandpa) are also like this, so I thought it was normal for your joints to bend weird ways and for your skin to be stretchy like that, and so on 😅 so now I'm gathering info from people not related to me on the paternal line to see what is actually normal and what is not.
demonstrating possible ehlers-danlos symptoms and asking my mom "can you do this?": so far all answers have been negative. very helpful anon might have been onto something. 😨
#the ONLY thing my mom checked out on was that her ankle was prone to dislocating#my dad however checks just about every other symptom (except for dislocation funnily enough. running theory is he got lucky)#including heart valve problems which i really hope i will not have ever! 🙃#i don't actually know abt my grandpa but i remember him demonstrating super bendy fingers as a party trick#so i feel like this is from his line
32 notes
·
View notes
Text
The Difference Between Heart Attack, Heart Failure, and Cardiac Arrest
I think fiction has done us a huge disservice when they conflate the above, but even my nursing students were kind of on the edge of not understanding this, so we're gonna talk about it here.
Heart Attack: A blockage in the coronary arteries
A heart attack, also called a myocardial infarction, is when one of the arteries that supplies the actual muscle of the heart gets blocked by a blood clot. When this happens, the muscle the artery was supplying starts to die. The more muscle impacted, or the longer the heart attack goes untreated, the worse the outcome for the patient.

Symptoms of this are different between men and women:

Treatment for a heart attack usually involves inserting a small tube into the wrist or groin, snaking it up to the blocked artery, and stenting open the blockage, thus returning blood flow to the heart muscle.
Heart Failure: A problem with the heart's ability to pump
Heart failure occurs when the heart is not beating hart enough or well enough to adequately get blood out to the body. This can occur for several reasons. It can be because of damage from a heart attack, because a valve in the heart isn't working right, from poorly functioning electrical system, or from long term exposure to untreated high blood pressure.
The symptoms of heart failure come both from blood collecting "in front" of the heart waiting to get pumped (swelling, shortness of breath, weight gain), and not enough blood getting pumped out to the body (dizziness, fatigue).

Heart failure is treated with medications that make the heart beat more normally and get rid of excess fluid to take workload off the heart. It can also be treated with surgery if the problem is with a valve, or with a pacemaker if the heart is beating too slowly.
Cardiac Arrest: A problem with the heart's electrical system
The heart beats in a synchronized way because it is made of muscle cells that are responsive to electricity. Special cells called pacemaker cells generate small electrical currents, which wash over the heart. When the cells are stimulated with that current, they contract, creating a beat.
Cardiac arrest occurs when that normally organized current becomes disorganized, and lots of cells, not just the pacemaker cells, start making their own currents. This can happen because of a lack of oxygen, too much or too little of particular electrolytes like potassium, an electrical shock, or damage to the muscle from a heart attack.
See below for a comparison between the normal electrical activity of the heart (top) and the disorganized rhythm of ventricular fibrillation:

When the electrical rhythm is disorganized, the heart isn't beating, just quivering, and no blood gets out to the body. This is treated with CPR to keep some blood flowing to vital organs, medications that can stabilize the heart's electrical system, and defibrillation. Defibrillation works by stopping the heart with an overwhelming amount of electricity and letting it restart (hopefully) in a normal rhythm.
If someone has no electrical activity in their heart (known as asystole), defibrillation won't work, but sometimes medication will.
170 notes
·
View notes
Note
Let's say a character with some sort of crazy hearing/sensory enhancements has the ability to pick up on the sound of someone's heart beat. If they had this ability... theoretically, would they be able to hear a heart attack before the person felt it? What would it should like? How much notice would they be able to provide??
Ooh, really good question, anon.
The answer is... potentially.
In order to explain why, we have to talk a little about what hearts sound like to the people who are trained to listen to them.
A healthy heart has 2 sounds per beat- Lub and Dub, also called S1 and S2. You can hear this in your own heart or a friend's if you have a stethoscope (or just an ear you can press against a friend) and listen at one of these locations:
You'll hear a heart that probably sounds like Lub-Dub Lub-Dub Lub-Dub, etc... The Lubs are S1 and the Dubs are S2. One Lub-Dub (S1-S2) cycle is a single heart beat.
But there are other sounds that can be heard if someone has a problem with their heart. For example, if one of the heart's 4 valves has a leak in it, you might hear a "Shhh" sound somewhere between or around the Lub and Dub. Like Lub-Shhh-Dub or Lub-Dub-Shhh. Depending on which part of the chest the "Shhh" sound is audible, you can tell which valve is faulty.
You might also hear an S3 or S4 sound. S3 and S4 are "extra" sounds that occur during the heart cycle. An S3 sound is like a "Uhh" and happens at the end of the Dub (Lub-Dub-Uhh). An S4 sound sounds like a "Buh" and weirdly enough happens before the Lub (Buh-Lub-Dub).
For the purpose of your question what we really want to focus on is that S4 sound. This is a sound that almost universally occurs in the early stages (first 1-3 days) of a heart attack.
See, the S4 sound is the sound of the top of the heart (atrium) straining as it tries to push blood into a damaged, overgrown, or swollen lower part of the heart (ventricle). Since heart attacks cause damage to the ventricle(s), you get this sound pretty soon after the damage starts occurring. You can even tell where the damage is in the heart (left or right) by where on the chest you hear the S4 most clearly.
But since heart attacks are not the only reason for damage to the ventricle, hearing an S4 sound does necessarily mean that a heart attack is currently occurring. It could have been that the person has had a heart attack in the past and they have scarring on their ventricle(s). It could also mean that they have had high blood pressure for a long time and their left ventricle is bigger and stiffer than it is supposed to be. It could be that they have heart failure and there is more pressure in their ventricles than there should be. It could be that they had an infection in their heart that left scarring in the past. It could be a problem they were born with.
Since these are all chronic problems, what your character would have to notice is a sudden start of an S4, probably combined with other symptoms. When the S4 sound starts, these symptoms might not be the "classic" heart attack symptoms yet. They might be feeling "off" or more out of breath than usual, or more tired than usual, or they might have some mild nausea or indigestion.
Your character might be able to provide at least a few hours of notice before the more classic symptoms show up.
196 notes
·
View notes
Note
Hey Joy, this isn't a question so much as a way for me to convince myself I'm not a hypochondriac, lol. Lately, I've been experiencing symptoms of fatigue, brain fog or memory issues, light-headedness, etc, that are uncommon for my age (30). I have related disorders such as anemia, anxiety, & ADHD that may be contributing to these symptoms, although they seem to have gotten worse or appear more frequently now than when I was initially diagnosed with those disorders. My work allows me to read & interact with disabled people with rare diseases, so I often find similarities with their medical issues. At first, I thought this was all just burnout or something related to the lockdown during COVID. I just saw my doctor and had blood work done to check my levels, and I may have a heart condition (tachycardia, mitral valve prolapse). I've fallen asleep at work before because I can't keep my eyes open, even after a full 8 hours of sleep. I can get dizzy from standing up too fast & can't seem to be on my feet for very long without discomfort & pain (I used to work retail, how did I ever do it?). I've researched some of my symptoms and found ME/CFS and POTS as possible conditions. Do you think it's a possibility I have these, or is it just my anxiety? Thank you! (P.s. Hunger Pangs is on my tbr!)
I obviously cannot tell you with any certainty what is wrong--and I am glad you are seeing doctors about it already and may have possible answers wrt tachycardia and the mitral valve.
What I will say is that there are many types of dysautonomia, of which POTS is one, and that what you are describing sounds very familiar to me as someone with two known types of dysautonomia.
The fact that this is hampering your quality of life to the point where you fall asleep at work, are unable to stand without getting dizzy, and are experiencing chronic pain, is enough of a reason to pursue further testing for things like dysautonomia and, yes, possibly even ME/CFS though given your history of anemia, I'm inclined more toward dysautonomia because the two often go hand in hand.
Also, it is normal to feel anxiety experiencing these types of symptoms. Even if it turns out to be a symptom of your anxiety, doesn't make the experiences any less real and debilitating, and you deserve treatment that will help improve your quality and comfort of life. And there is treatment and things you can do that will make you feel better. Getting your anemia under control should be a top priority if it isn't already. Mines was allowed to go untreated for years until we found out my iron anemia was being caused by pernicious anemia (b12 deficiency), and the iron anemia I'd been plagued with since birth suddenly cleared up.
Years and years of blood transfusions and infusion treatments, and the whole time I needed b12. Who knew? Certainly not my old doctors.
Anyway. If your symptoms are at the point where you are recognizing yourself in things like POTS? It's time to pursue that with your doctor. Don't put it off because you think it's not that bad or others have it worse. Everyone deserves to feel well.
Good luck.
200 notes
·
View notes
Text
Myxomatous Mitral Valve Disease vs Dilated Cardiomyopathy (Part 1)

Hope you are ready to do some learning today! I didn't want to bog down Nadia's post too much so I figured I'd do something a little more in depth, separately. I also hope that the information here might help anyone seeking information about either disease. Might want to go and make yourself a drink and/or a snack because this will be a long read.
What is MMVD? Myxomatous Mitral Valve Disease also called Degenerative Mitral Valve Disease is the most common cardiac disease affecting dogs. It is an acquired disease (aka "adult onset") that is most typically seen in small breed geriatric dogs. It is characterized by a progressive thickening of the Mitral valve, which is the valve on the left side of the heart - in other words, the valve that connects the left ventricle (LV) to the Left Atrium (LA). The thickening results in it becoming more rigid and overtime it loses the ability to close properly, causing a leak (or regurgitation) from the left ventricle to the left atrium. Over time, the valve has a tendency to become so fibrinous that the leak becomes more important with time, and for some dogs with very advanced MMVD the valve may not even really close much at all anymore.
Because of the leak, over time the left ventricle and the left atrium will enlarge. When the left atrium becomes severely enlarged the patient will progress to congestive heart failure. Because of the stiffening of the valve the chordae tendineae that hold it together are also at risk of rupturing as the disease progresses. When a dog ruptures a major chord, they are at risk of an acute episode of CHF without dilation of the left atrium (because the left atrium does not have a chance to adjust or adapt to the sudden backflow) and patients in this situation will often require critical hospitalization care for 24-48 hours before normalizing. In some very uncommon or rare cases the disease can be self limiting. We have seen it in one or two patients where the dog actually improved after being in B2, with the heart reducing in size because the mitral valve thickened so much it started plugging the leak again. What causes MMVD? It is unknown what exactly causes this process. In certain breeds there is a very strong genetic, hereditary and familial component like in Cavalier King Charles Spaniels, Dachshunds, Cocker Spaniels, Yorkies, Pomeranians and others. It mostly affects small breeds, but any dog breed can get MMVD. How is it diagnosed? MMVD can only truly be diagnosed exclusively via cardiac ultrasound (echocardiography) by a cardiologist. It can be listed as a differential with the help of other diagnostic tools like x-ray, auscultation (presence of a heart murmur on the left side), age/breed of the patient and clinical symptoms (late stages). There are other diagnostic, clinical tests but they are non-specific blood tests that can merely serve to further refer out to a Cardiologist. Can you treat it? Yes. The primary treatment for MMVD will be the administration of Pimobendan once the disease progresses to moderate stage MMVD classified as ACVIM B2. Because it is so prevalent in dogs there is empirical data on it, and one in particular the groundbreaking EPIC study has helped establish very specific guidelines for the classification of Moderate Stage MMVD and the early (pre-clinical) administration of pimobendan. In order to be classified as B2 and qualify for early administration of pimobendan the dog must meet 4 criteria:
Grade III heart murmur or higher
Left Atrium/Aortic (LA/Ao) ratio of 1.6 or higher
Left Ventricle Internal Diameter in Diastole Normalized for weight (LVIDDN) of 1.7 or higher
VHS (Vertebral Heart Score) of 10.5 or higher on xray
Where an echo is not possible, in order to qualify for pimobendan, it is recommended to wait until the the VHS is equal to 11.5 or higher. What is miraculous about the EPIC study is that it offers proof that administering Pimobendan to a dog in B2/moderate MMVD will slow down significantly the progression of the disease. The median time it takes for a B2 moderate MMVD to progress to a Stage C heart failure is 766 days without the administration of Pimobendan. With pimobendan that median increases by 60% 1228 days. Once a dog reaches CHF typically the prognosis is 6-12 months post diagnosis of CHF. With pimobendan it adds about 10% overall time without clinical signs or quality of life issues. Some Cardiologists will also prescribe an ACE Inhibitor (Angiotensin-converting-enzyme inhibitors) alongside Pimobendan even while still in Moderate/B2 stage, while others will prescribe it rather only once the dog progresses to a Stage C (aka severe stage with congestive heart failure). Once the dog reaches Stage C, typically a diuretic will be added to the treatment. Management can include adjusting dosage of the medication and on occasion adding in additional diuretics, or if exhibiting new cardiac symptoms, adding additional medication. For example in large breed dogs you can see Atrial fibrillation, and in some individuals you'll also see Ventricular Premature Contractions (VPCs or PVCs which doberman people will be familiar with due to its role in DCM) so medications can be added to control these aspects too. Now what is interesting with MMVD is that there are currently two surgical procedures/interventions with very limited availability. One is an open heart surgery that is curative and consists in repairing the Mitral Valve. There is the JASMINE Animal Referral Hospital in Japan where the procedure was developed by Dr Uechi Masami, who has then gone on to train teams in the UK at the Queen Mother Hospital Royal Veterinary College as well as a team in France at HOPIA. Currently Dr Uechi is performing mitral valve repair procedures at the University of Florida in the USA, with the goal to try and train as many teams in the USA and around the world. The likelihood of this surgery ever becoming widespread or common place or even accessible to most people is fairly low, given the high demand, and how resource intensive it is both in equipment and specialized teams. The other very recent intervention is the TEER mitral valve repair, a minimally invasive procedure that consists in installing a clamp on the mitral valve to bring it back closer together and thus reduce or eliminate the leak. Can I do anything to prevent it? While there's nothing you can do to prevent MMVD from occurring, if you intend to purchase a puppy from a small breed or medium breed, especially one of the breeds known to have high prevalence of the disease, it is imperative to ask the breeder if the parents have been screened and are being monitored for cardiac disease by a cardiologist, whether that's with a yearly auscultation or a yearly echocardiogram (because MMVD is always associated with a murmur, for regular owner it is acceptable to auscultate yearly, and only do an echo if/once a murmur is heard). Ask about the pedigree also. I strongly encourage you to start screening/monitoring for it when your dog reaches 4-5 years for at risk breeds. Breeding animals should be screened before being bred and then yearly thereafter. If you are unsure whether your breed is considered at risk, you can check the recommended tests for your breed on the OFA website. If you adopt a pup from a rescue or shelter with an unknown genetic background, I would strongly encourage you to ask your vet to properly auscultate during your yearly vet visits and physical exams, and I would request a referral to a cardiologist (if required in your area, our cardiology department doesn't per se require a referral anyone can call and book) even if your dog only has a Grade I-II murmur.
#myxomatous mitral valve disease#degenerative mitral valve disease#cardiology#veterinary cardiology#OFA#health testing#health tests#MMVD#DMVD#ACVIM#EPIC study#canine heart diseases
16 notes
·
View notes
Text
Erlinda Rodriguez, 21 (USA 1969)
Erlinda Rodriguez was seen at an ER in May of 1969. One month ago, she had been exposed to infectious hepatitis and was now suffering from symptoms consistent with it. She had missed a period, but told her doctor that she knew she wasn’t pregnant because she had an IUD. The doctor did not perform a pelvic exam.
X-ray studies of Erlinda’s gastrointestinal organs and gallbladder were ordered. The only abnormality was “nonvisualization of the gallbladder” and a repeat of the X-ray had the same results.
In June, Erlinda was seen at an obstetric clinic because she still had not had a period. Had the ER doctor performed a pelvic exam, it would have been immediately obvious that her IUD had come out. She was pregnant.
Pelvic exposure to radiation was estimated at 10 to 12 rads. Abortion under certain circumstances had already been legalized in New Mexico, and Erlinda and her husband feared the possible effects of radiation on their baby. She was promptly approved by a committee for a “therapeutic” abortion. Had the committee said no, Erlinda could have lived.
The hospital that carried out the abortion did not have a specialized vacuum uterine aspirator (which can still be lethal even when properly equipped). They had substituted a portable vacuum laboratory pump with a suction trap. It is unknown if Erlinda knew about the equipment substitution when she agreed to the abortion.
On June 30, 1969, Erlinda was put under sedation and her cervix dilated for the “safe and legal” abortion. After the cannula was put into her cervix, the vacuum device was turned on.
Immediately, a massive amount of bloody froth began to foam out of Erlinda’s body. The machine was turned off, but it was too late. Someone had connected the suction tube to the pressure outlet. Erlinda’s uterus had been pumped full of vacuum exhaust.
The tubing was reconnected and the abortion carried out, along with the removal of blood so full of air that it was frothy. The anesthetist was told to watch for signs of an air embolism. Only 30 seconds after having pressurized vacuum exhaust pumped into her body, Erlinda’s blood pressure was undetectable. Her heart rate dropped to 50 bpm and she had to be intubated, at which point she was noticed to be blue.
A cardiovascular surgeon was brought in six minutes after the massive drop in vitals. Closed chest massage was used for one minute, but Erlinda had no pulse. Her chest was opened for cardiac intervention.
Erlinda’s heart was so massively distended from a massive air embolism that it was nearly sphere-shaped. About 11 minutes after the embolism, needles were used to create vents in her heart. Air hissed under enormous pressure from each vent site.
After intensive efforts, Erlinda’s heartbeat was brought back to a strong sinus rhythm, but the damage had been done. She never regained consciousness and spent her last weeks comatose. She had to have a breathing tube and feeding tube put in. Decorticate rigidity indicated severe brain damage. Several urinary and respiratory infections later, Erlinda died on September 17, 1969.
The autopsy revealed extensive cerebral necrosis, tracheobronchitis, pulmonary edema, bronchopneumonia and gallstones.
Erlinda’s death was preventable on many levels. First, a pelvic exam after she reported missing periods would have immediately found the dislodged IUD before the radiation exposure could ever happen. Second, the study that reported her death recommended screening for pregnancy before conducting pelvic X-rays. The exposed pressure outlet on the hospital’s substitute equipment was unacceptably risky, and greater care with preparation would have found that the tubing was connected to the outlet valve before it was turned on. All equipment also should have been tested before it was actually put into anyone’s body.
Adding to the tragedy, we now know that the chance of X-rays during pregnancy harming an unborn baby is very small. According to the CDC, there is scientific disagreement on whether or not the amount of radiation in a diagnostic X-ray is sufficient to seriously harm an unborn child (although a large number of pelvic X-rays still warrant consideration and care). Erlinda died without knowing that her child was probably fine.
(Erlinda is Patient ER)
#tw abortion#pro life#pre roe legal#unsafe yet legal#tw ab*rtion#tw murder#abortion#tw malpractice#tw negligence#tw neglect#death from legal abortion#abortion debate#pregnant people deserve better#tw eugenics
8 notes
·
View notes
Text

“According to Eastern medicine be it Indian, Chinese, Tibetan or Thai, the left side of the body is totally different from the right side. Even some Buddhist monastic traditions include within their precepts for monks to sleep on their left side. Although it sounds weird resting and sleeping on the left side has many health benefits.
The lymph drains to the left.
The left side of the body is the dominant side of the lymphatic system. Most of the lymph drains down to the thoracic duct which is located on the left side. In its path the lymph transports proteins, glucose metabolites and waste products that are purified by the lymph nodes to be drained to the left side.
Derived from the above it is common to deduct in Eastern medicine that the diseases of the left side of the body may be due to chronic congestion of the lymphatic system.
The priorities of the body.
According to ayurveda congestion occurs in the body following certain priorities. If the lymphatic system is digested, the liver and blood are subsequently saturated with toxic substances. Primary symptoms of congestion present on the left side of the body before moving to the right side where they make their later appearance.
Feeling bored after a meal?
The Indian suggestion is that if you take a break after eating, do it lying on your left side. The rest should not exceed 10 minutes and is different from the evening nap which is usually 20 minutes or more.
Stomach and pancreas hanging to the left side. When you lie on your left side both naturally hang allowing for optimal and efficient digestion. Food is driven to move naturally through the stomach and pancreatic enzymes are secreted in a paulatin way and not in a single stroke, which happens if you lie down on the right side.
Laying on your left side your liver and gallbladder hang from your right side. Resting on the left side allows them to hang and secret their precious enzymes into the digestive tract, emulsifying fats and neutralizing stomach acids.
When the digestive system is stimulated this way your digestive cycle is shorter and doesn't leave you stranded for the rest of the afternoon. Try resting 10 minutes on your left side after eating.
Feel energized and not tired after eating.
Try to eat in a relaxed way mid-day and don't forget to rest on your left side and check that you will feel more energized and with better digestion.
Sleeping magic from the left side.
Best elimination.
The small intestine flushes toxins through the ileocecal valve (VIC) on the right side of the body at the start of the large intestine. The large intestine travels down the right side of your body, crosses your stomach and descends down the left side.
Through the VIC, sleeping on the left side allows gravity to stimulate bodily waste into the large intestine from the small intestine more easily.
As the night passes and continue sleeping on your left side the debris moves more easily toward the downward column and morning removal will be easier.
Best cardiac function.
More than 80% of the heart is located on the left side of the body. If you sleep on the left side the lymph drained to the heart will be driven by gravity taking work out of your heart while you sleep.
The aorta, which is the largest artery in the body, comes out from the upper part of the heart and is arched left before going down to the abdomen. By sleeping on the left side, the heart pumps blood more easily into the downing aorta.
Sleeping on the left side allows the intestines to move away from the cava vein that brings blood back to the heart. Noticeably the cava vein rests on the right side of the thorn, so when you lie down on the left side the viscera move away from the cava veina. Again gravity makes the heart job easier.
The sparrow is on the left side.
The spleen is part of the lymphatic system and is also on the left side of the body. Its function is that of a large lymph node which filters the lymph and additionally filters the blood. When you lie on the left side the fluids return to the basin is easier and is more easily produced by gravity.
The lymphatic system drains all cells in the body through contractions and muscle movement and not by heart pumping. Helping the lymph drain into the pelvis and heart with gravity is a simple way to purify your body.
And while there are no scientific protocols on it, sleeping on the left side does make sense. Understanding ancestral wisdom based on knowledge of modern anatomy clears up many doubts about the reasons that exist in the east to sleep a certain way.”
Original article written by Dr. John Doull
[Leila L'Abate]
#sleep#Physiology#left side#Leila L'Abate#Dr. John Doull#quotes#articles#lymphatic system#Body Alive
25 notes
·
View notes
Text
Lea's home
Chapter 2 pt.2
The climb up to her room is filled with worry, anxiousness and a little bit of lust.
My thoughts are running everywhere: I don't want to be fired; I hope she hasn't found out; I want to steth her; I hope Lea's safe; How did she learn about this; I want to palpate her neck vein; I need to fix this; I want to palpate her heart; I want to keep my job; I need to steth her-
Just a jumble of all too many things.
Before I know it, I'm at her door. I hear the shower going inside. I lightly knock on the door and hear a soft "come in". I make sure the corridor is empty, and slip inside her room. My heart pounds as I scan the room and wait for her to come out.
Promptly I hear the shower turn off, and after a few seconds Mrs. Nicole emerges from her bathroom, draped in nothing but a bathrobe, her hair wet and dripping, her face flush from the warm water, but with her glasses still on. She locks her foxy eyes on me, and walks towards her bed and sits on it, before tapping the space beside her motioning me to sit beside her on the bed.
"How've you been doing?" she asks, her silky voice alluring me, holding me in place.
"I'm doing well Mrs. Nicole. Lea and her family has treated me well, and work is going smoothly." I speak fast and slurred, trying to focus on calming my nerves. I quickly sneak a glance at her breasts against my wish and quickly flick my eyes away, noticing her very clear pulse on her neck and under her left breast, pounding away steadily and at a slightly quick pace, probably from the shower.
What I wouldn't give to place my steth there-
"And how is college? Is your studies progressing smoothly? I hope nothing's hindering your progress towards your goal" her voice is dropping steadily, doing things to me. A warm sensation grows in my lower abdomen.
"Everything's going smooth Mrs. Nicole, I'm keeping up to date with all my material." Why's she bringing up this small talk?? Is this a way to intimidate me? Is she indirectly threatening to ruin my college life?
"That's great, my dear" she says, with a hand reaching towards me a stroking my cheek. Is she....by any chance.....drunk?
"Mrs. Nicole, are you okay? Is there anything I can do for you?" I mean, she did call me to her room, and she has yet to tell me why.
"I hear you're a medical student, yes? You see, I am getting old, and with my age I am noticing a few problems. Every now and then, I feel slightly out of breath, and my heart palpates a lot. It lasts for a few minutes at a time. Do you have any idea what these symptoms are?"
Omg. Is this what I think it is? This can't be real. She's asking me about a heart related issue? How do I interpret this? Is she genuinely asking for my advice, or is she insinuating that she knows I do "heart checkups" on Lea?
Wait.... whatever it is, doesn't this also mean that this is my chance to finally palpate her? Finally, after dreaming about it for so long, I finally have a (questionable) reason to palpate her beautiful breast.
"are you currently feeling palpitations?" She nods eagerly, her eyes widening a bit.
"I might need to palpate your chest area, do you mind?"
"Yes dear, please, and feel free to move around my boobs, I know they're in the way and I've seen doctors having to move them aside."
I waste no time and immediately palpate over her bathrobe, above her breasts and slowly make my way down. I gently untie the front of her robe and palpate her sternum, feeling a slight sternal heave. My brain is now divided into 2 parts: Analyzing the meaning behind a sternal heave, and bathing in the sensation of how amazing her heart is. I make my way to her point of maximal impulse, and it's almost like her heart is eager for me to touch it, pushing its apex as close as possible for me to feel it with minimal efforts.
"Wow Mrs. Nicole, your heart is really amazing" I say, quickly following up with "I can feel a heave, but I might need a stethoscope to carefully listen to the valves before I give any further advise. Unfortunately I don't have mine on my right now..."
She gets up and quickly makes her way to a small compartment in her desk and pulls out a Littman stethoscope and makes her way back to me. She stands in front of me, and hands me the steth. "Wear it" She commands, and I put it on without missing a beat.
I start putting things together slowly: Why does she have a steth? How does she know that sometimes doctors move breasts of heavier build people to properly hear their heart? I can't believe I'm thinking this, but is it remotely possible that....she's a cardiophile, like me? Or is this just my wishful thinking?
"Steth me, now." She orders, and i place the cold steth on her bare skin, in the pulmonic position and there I hear it: the beautiful strong heartbeat of a sexy woman, right at my fingertips.
Bu-thump Bu-thump Bu-thump
I stutter out a "It looks fine Ma'am."
She removes my hand of her chest and beckons me to get up. She then leans on the headrest of her bed, scoots her legs over to one side, and pats the other side.
"This position might help you hear clearer."
My mind is completely blank. I do as she says and obediently sit. She then says "I gave you the tool, now use it properly. Steth me."
I go in order saving the best for the last, first her aortic valve, her pulmonic, her tricuspid, and finally my favourite: the mitral valve.
Bu-thump Bu-thump Bu-thump Bu-thump
As I go in order, her heart rate picks up from a 90 bpm to a 120 bpm, and she now starts panting, her cheeks becoming more flushed. Her pounding heartbeat is becoming more and more visible, her PMI becoming more clearer and prominent. Her neck veins are pulsating hard, and it takes all my will power to not feel it. She places one of her hands on my own and pushes it strongly to her chest.
"What are you hearing? Describe it to me."
"I hear your valves, pushing hard and fast. It sounds beautiful and strong." All my medical knowledge leaves me, and I am left alone with my leud thoughts, my pounding heart and the most beautiful muse in front of me. All I would ever need.
"I can make it go faster.....for you....." she says, slowly, looking at me intently. With her eyes fixed on me, she pulls my other hand toward her chest, slowly caressing herself with my hand. Her eyes flutter close and she bites her lip, stifling a small moan threatening to escape.
"Your heart... it's pounding so hard.... I want it to go faster."
She looks at me surprised. Now I'm the one giving her instructions. It seems to have caught her off-guard. I stop stething her and she whimpers a bit. I pull off her glasses, revealing her full face, cute and flushed, now seemingly under my control.
"Don't stop your moaning. Moan for me. Make your heart go faster for me." Her hands have become weak and fall away, and allows my fingers to play around her nipple which has been hard for a while, begging for attention. I rub it slowly, twisting it and squeezing it gently, watching the once strong woman crumble under my touch, her fierce face melting into a flushed mess due to my touch.
I fully understand why she called me to her room. She's wanted this from me. She must've noticed me staring at her and knew I was the one she needed. The way her body quivers, tells me she's wanted this for a long time now. Getting drunk was her way of letting it happen. So now, I must give her what she's asked for.
"My heart's beating fast, steth me" she tries taking control but I don't budge. I look at her coldly, waiting for that magic word.
"Please!" She begs. That's more like it. I put my weight against her body and press the steth into her chest, and she moans. The warm feeling was now fully raging in my clit, throbbing with my heartbeat.
"Can I *huff* please... listen *huff* to yours? Please?"
I remove the steth, my ears feeling lonely, and place them in hers, and guide the bell to my own apex. My heart leaps out with excitement, hammering away strongly, as if showing her who's heart is best.
"Touch yourself" I order her, and her hands go down and insert inside easily, her underwear wet in anticipation. She rubs her clit and listens to my heartbeat hammering inside, pounding harder as I watch her twitch and moan. My heart is doing this to her. I did this.
She tried to reach for my vulva but I swat her hand away, "Did I tell you to do this? No. You only touch what I tell you to." She whimpers and nods.
Seeing this strong and powerful woman obey my every word is everything I've dreamed of with her.
I lay down on her chest, listening to her raw heartbeat. This pushes her to her climax, and I feel the wave of orgasm hit both of us. As I continue to touch her nipples, and slip my other hand into her clit and rub sensually with her fingers, both covered and wet, panting and heaving, her moaning loudly. With a final quiver, she cums and collapses down into the headrest, and I leaning on her chest. We listen to each other's heartbeats in silence till we both calm down and our breathing gets regulated.
"I've wanted you to listen to my heart since Lea introduced you here" she says, in between small breaths. "I also noticed how your relationship changed recently and how she watches your heart every time you're in the room. I wanted that for me, too."
I look at her, mildly shocked that she noticed. Maybe it takes one cardiophile to understand another.
"I thought I lost that, but I noticed you never stopped looking at me. Every time you're in the room my heartbeat picks up and you notice it. Every time it shakes visibly, you're the only one who notices. I've wanted you for a long time, and I was happy when it looked like you wanted me too."
I'm filled with happiness, and am so grateful that she was on my side. I knew that Mrs. Nicole would never betray me, and that I could trust her and her heart. Because today, her heart was mine to control. She belonged to me.
I let her listen to me for a while until she fell asleep, and I monitor her heart go back to a steady 60 bpm. Her neck veins go back to being slightly visible, and her apex pulses against her chest slowly.
I let my fingers linger on her neck, her breast, her nipples and her clit, slowly massaging it. I finally get up, turn off the light, and leave the beautiful Mrs. Nicole alone.
I pack up my things and leave the house, just on time to see Lea pulling up. I wish her good night knowing that if I stayed a bit longer she would call me to her room as well, and I'd had enough work out for now.
As I reach home, I think on how now, I have 2 very different yet very beautiful hearts that belong to me, and how I look forward to playing with them in the future.
83 notes
·
View notes
Photo

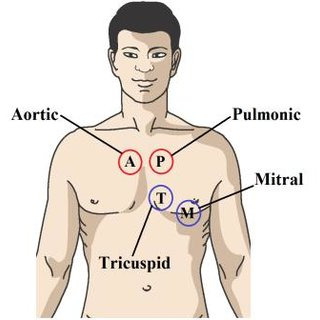
Symptoms Of Heart Valve Disease
Make an appointment with your doctor if you have any persistent signs or symptoms of Heart Disease that concern you. If you don’t have any signs or symptoms, but you are worried about your risk of Heart Disease, discuss your concerns with the Heart Valve Expert In Jaipur, Dr. Ravinder Singh Rao. Hence, call us Tel: +91-7891791586 and get more information
#Heart Valve Expert in jaipur#Best Heart Expert in Jaipur#Symptoms Of Heart Valve Disease#What Causes Heart Valve Disease#Heart Valve Disease Treatment#Dr. Ravinder Singh Rao
0 notes
Text
The body will fall away
January 24, 2022. Monday. 8:39pm
Good time to start a new journal.
Just as a new chapter in life rolls out.
Cardiologist nurse, 4:40 pm today said “You have moderate aortic stenosis.”
A callus has formed on the aorta valve, causing blood to, well, I guess, be pushed back into the heart..I’m not sure.
Nurse said that people who have it go on to live another 30, 40 or 50 years longer. Really. Doesn’t she know that I’m 66 1/2. Maybe 5 or 6 hours longer. Or days! (I’m joking here :))
So, just as in the New Dimensions Post Cast poet’s poem, death comes to visit.
He was sitting there, holding my arm, as I reviewed a journal awaiting the nurse at Stanislaus Cardiology.
He encouraged me to get the book out there as soon as possible.
Earlier, a teeth cleaning. My gums were parted, they could see the bone. Cavity, a major one.
So, a bit unnerving, but death is inevitable.
As James Hillman said on learning that his death from cancer was imminent “It shocks the conscious."
The teeth, the heart say “The body will fall away”
End of entry
Notes:
Late summer 2023, I returned to the Cardiologist’s office to get the results of an echo test on my heart. The nurse said now the stenosis was severe.
Knowing this, I still swam from just off Alcatraz island to Aquatic Park, San Francisco ion September 23, 2023. As a Doctor friend of mine told me before the swim “If you don’t feel symptoms before the swim, do it. If you die out there, you will have died doing something you love to do."
I finished the swim in 1 hour 20 minutes. I felt fine.
New Dimensions Radio is a weekly program the features interviews with progressive authors and thinkers. It began in 1973.
James Hillman was an author, philosopher and progressive thinker who died in 2011.
I had a talk yesterday with a friend of mine who is a few years older (I’m 68). He also has heart issues, different than mine, though. We both agreed, it’s not the quantity. It’s the quality of life that counts.
#1/24/2022#journaling#writing#aging aortic stenosis#death is inevitable#quality over quantity#Alcatraz swim#dying doing what you love#risk
11 notes
·
View notes
Text
Engine Repair Instruction Full Guide
Engines are the heart of any vehicle, powering everything from your daily commute to long road trips. Knowing how to repair an engine can be a game-changer, whether you're an enthusiast who loves getting your hands dirty or someone looking to save money on mechanic bills. This guide will walk you through the entire process of engine repair, from diagnosing problems to reassembling your engine and ensuring it runs smoothly.

Understanding the Basics of an Engine
Before diving into the repair process, it’s crucial to understand how an engine works. Most vehicles use an internal combustion engine, which combines fuel and air, ignites it, and transforms that explosion into mechanical energy.
Components of an Internal Combustion Engine
The main components include:
Cylinder Block: The engine's core where combustion occurs.
Cylinder Head: Houses the valves and spark plugs.
Pistons: Move up and down to create the force needed to turn the crankshaft.
Crankshaft: Converts the pistons' up-and-down movement into rotational motion.
Camshaft: Controls the opening and closing of the valves.
Valves: Regulate the flow of fuel and air into the engine and exhaust gases out.
How an Engine Works: A Simple Explanation
An engine works by pulling in a mixture of air and fuel, compressing it, igniting it with a spark (in gasoline engines), and then expelling the exhaust gases. This cycle—intake, compression, power, and exhaust—happens in each cylinder and repeats hundreds of times per minute.
Tools and Equipment Needed for Engine Repair

Whether you're performing a basic repair or diving into more complex work, having the right tools is essential.
Essential Tools for Basic Repairs
Socket Set: For removing and tightening bolts.
Wrenches: Different sizes for various engine parts.
Screwdrivers: Flathead and Phillips for screws and clips.
Pliers: For handling wires and small parts.
Torque Wrench: Ensures bolts are tightened to the correct specifications.
Specialized Equipment for Advanced Engine Work
Engine Hoist: For removing the engine from the vehicle.
Cylinder Hone: Prepares cylinders for new piston rings.
Compression Tester: Checks the health of each cylinder.
OBD-II Scanner: Diagnoses engine codes and issues.
Safety Gear and Precautions
Gloves: Protect your hands from cuts and chemicals.
Safety Glasses: Shield your eyes from debris.
Work Boots: Offer protection against heavy parts or tools.
Diagnosing Engine Problems
Accurately diagnosing engine problems is the first step in any repair process. Understanding the symptoms can save time and prevent unnecessary work.
Common Symptoms of Engine Issues

Check Engine Light: Indicates a problem detected by the car's computer.
Strange Noises: Knocking, tapping, or grinding sounds can signal internal damage.
Excessive Smoke: Blue smoke might mean burning oil, while white could suggest a coolant leak.
Loss of Power: Often linked to fuel or air delivery issues.
Step-by-Step Diagnostic Process
Listen and Observe: Note any unusual sounds, smells, or behaviors.
Check Engine Light Codes: Use an OBD-II scanner to retrieve error codes.
Perform Compression Test: Assesses the health of your engine’s cylinders.
Inspect Fluids: Look for contamination or leaks in oil, coolant, and other fluids.
Step-by-Step Guide to Reassembly
Prepare Your Workspace: Ensure that your workspace is clean, organized, and well-lit. Lay out all the parts and tools you'll need in the order of reassembly. Keep the engine manual handy for specific torque specs and sequences.
Install the Crankshaft: Place the crankshaft back into the engine block, ensuring it is seated correctly. Use assembly lube on the main bearings to prevent damage during the initial startup. Torque the main caps to the manufacturer's specifications.
Insert the Pistons: Install the pistons and connecting rods. Be sure to align the piston rings correctly and use a ring compressor to insert the pistons into the cylinder bore. Attach the connecting rods to the crankshaft and torque the rod bolts to spec.
Install the Camshaft and Timing Components: If your engine uses a timing chain or belt, install it according to the timing marks on the camshaft and crankshaft gears. This step is crucial for ensuring the engine's valves open and close at the correct times.
Attach the Cylinder Head: Place the cylinder head gasket on the engine block, followed by the cylinder head. Torque the head bolts in the correct sequence and to the proper specifications. This ensures a good seal and prevents head gasket failure.
Install Valves, Lifters, and Pushrods: If applicable, install the engine's valves, lifters, and pushrods. Make sure they are properly aligned and that the lifters are seated correctly in their bores.
Reassemble the Valve Train: Install the rocker arms and adjust the valve lash according to the engine manual. Proper valve lash is critical for engine performance and longevity.
Reattach External Components: Begin reattaching external components like the water pump, oil pump, timing cover, oil pan, and intake manifold. Replace any gaskets and seals during this process to prevent leaks.
Reconnect the Fuel and Ignition Systems: Reinstall the fuel injectors, spark plugs, and ignition wires. Ensure all electrical connections are secure and properly routed to avoid short circuits or malfunctions.
Final Checks: Before moving on, double-check all connections, bolts, and components. Make sure nothing is left loose or unconnected.
Applying Proper Torques and Specifications
Every engine has specific torque settings for each bolt. Over-tightening can strip threads or warp components, while under-tightening can lead to leaks or parts coming loose. Use a torque wrench and follow the manufacturer's specifications closely.
Double-Checking Work for Mistakes

It's easy to miss a step or make a mistake during reassembly. Double-check your work:
Ensure all components are installed in the correct order.
Verify all bolts are torqued to spec.
Check for any leftover parts or tools in the engine bay.
Testing the Repaired Engine
With the engine reassembled, the next step is testing it to ensure everything is functioning properly.
Preparing for Initial Startup
Before starting the engine, perform a few preparatory checks:
Prime the oil system: This can be done by cranking the engine with the fuel system disabled until oil pressure is achieved.
Fill the engine with fresh oil and coolant.
Double-check all electrical connections and fuel lines.
Checking for Leaks and Unusual Noises

Once you start the engine, pay close attention to any unusual noises or leaks:
Oil Leaks: Check around the oil pan, valve covers, and front and rear seals.
Coolant Leaks: Inspect the radiator, hoses, and water pump area.
Unusual Noises: Listen for knocking, tapping, or whining sounds, which could indicate an issue with the timing components or internal parts.
Fine-Tuning and Adjusting the Engine
After the initial startup, the engine may require some adjustments:
Timing Adjustments: Use a timing light to set the ignition timing.
Idle Speed: Adjust the idle speed according to the manufacturer’s specifications.
Fuel Mixture: On carbureted engines, you may need to adjust the air-fuel mixture for optimal performance.
Common Engine Repair Mistakes to Avoid
Engine repair is complex, and mistakes can be costly. Here are some common errors to watch out for:
Misalignments and Incorrect Torques
Misaligned timing components can lead to poor engine performance or damage.
Incorrectly torqued bolts can cause leaks, parts failure, or engine damage.
Overlooking Small Parts and Connections
Small parts like washers, clips, or gaskets are easy to overlook but crucial for preventing leaks and ensuring proper function.
Electrical connections: Double-check that all sensors and connectors are properly seated.
Skipping Diagnostic Steps
Skipping steps in the diagnostic process can lead to unnecessary repairs or missed issues. Always perform thorough diagnostics before and after repairs.
Maintaining Your Engine After Repair
Proper maintenance is key to ensuring the longevity of your newly repaired engine.
Importance of Regular Maintenance
Regular maintenance, such as oil changes, air filter replacements, and coolant checks, is essential to keep your engine running smoothly and prevent future problems.

Tips for Extending Engine Life
Use high-quality oil and filters.
Avoid hard driving until the engine is fully warmed up.
Regularly check and maintain fluid levels.
When to Seek Professional Help
While DIY repairs can save money, some issues are best left to professionals, especially if you encounter complex problems or lack the necessary tools and expertise.
Dealing with Advanced Engine Repairs
Some engine repairs are too complex for the average DIYer. Here's when to consider professional help:
Understanding When It’s Beyond DIY
Extensive internal damage: Cracked blocks or severely worn bearings usually require professional expertise.
Advanced electrical issues: Problems with engine management systems often need specialized diagnostic tools and knowledge.
Overview of Complex Repairs: Timing Belt, Engine Rebuilds
Timing Belt Replacement: Involves precise alignment of engine components and is critical for preventing engine damage.
Engine Rebuilds: This is a time-consuming and complex task that often requires professional machining and specialized tools.
Working with a Professional Mechanic
When the repair is beyond your capabilities, working with a professional mechanic ensures that the job is done correctly and safely. They have the tools, experience, and resources to handle complex engine repairs.
Cost Considerations in Engine Repair
Engine repair costs can vary widely depending on the scope of work, parts required, and whether you do it yourself or hire a professional.
Estimating Costs for DIY vs Professional Repair
DIY Repairs: Typically cost less but require an investment in tools and time.
Professional Repairs: Can be expensive but come with the assurance of experience and often a warranty.
Budgeting for Tools, Parts, and Time
Consider the cost of any special tools or equipment you might need, as well as the cost of replacement parts. Factor in the time required, especially if the vehicle is your daily driver.
Understanding the Cost of Mistakes
Mistakes can be costly. Stripping a bolt, breaking a part, or incorrect assembly can lead to additional expenses. Always weigh the risks before starting a major repair.
Conclusion
Recap of Key Points
Engine repair is a rewarding but challenging task that requires careful planning, the right tools, and attention to detail. Whether you’re fixing a minor issue or performing a complete rebuild, following the correct procedures is crucial for success.
Encouragement for DIY Enthusiasts
For those who love working on their vehicles, engine repair can be a satisfying and cost-effective way to maintain your car. With patience and persistence, even complex repairs can be tackled with confidence.
Final Thoughts on Engine Repair
Always approach engine repair with a clear plan and the right resources. Don’t hesitate to seek professional help when needed, and remember that regular maintenance is the best way to avoid major repairs.
FAQs
How do I know if my engine needs repair?
Common signs include unusual noises, excessive smoke, loss of power, and a check engine light. Regular diagnostics can help catch issues early.
Can I repair my engine without professional help?
Basic repairs like replacing gaskets or sensors can often be done at home with the right tools. However, more complex tasks like engine rebuilds may require professional expertise.
What are the signs of a failing engine?
Signs include knocking noises, excessive oil consumption, smoke from the exhaust, and persistent overheating.
How long does it take to repair an engine?
The time required varies greatly depending on the complexity of the repair. Simple repairs might take a few hours, while a full rebuild could take several days or longer.
2 notes
·
View notes