#medical misconceptions
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
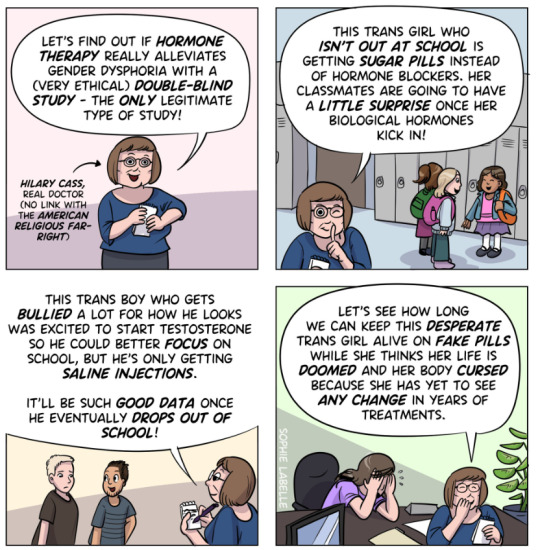
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
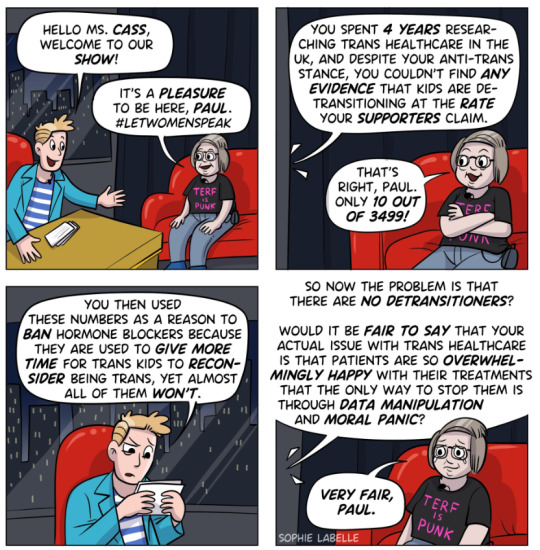
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone. There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
384 notes
·
View notes
Text

fuck it. plaguesona
#i thought of this a couple weeks ago on the bus a couple seats away from someone loudly coughing into the open air#i think something snapped and i decided to make a fuckin. medieval ass plague sona. horseman of pestilence fursona#this is also why i was asking abt animals with medical symbolism.. originally i wanted a two headed snake like the staff of caduceus#but it turns out thats actually hermes symbol. the real symbol for medicine is the rod of asclepius which looks pretty similar#the difference is that theres only one snake and its twined around a stick. ironically mercy from overwatch's weapons are named after#the caduceus despite the misconception LMAOOO#snakes were the most consistent medicine related animal i could find even across multiple cultures so it couldve really worked#if i could actually draw scalies.. one of my earliest sketches had a cobra with a syringe at the end of its tail like a rattlesnake#and it had markings similar to the syringe tube but i didnt have much else going on so i scrapped it#i was also recommended animals with less obvious ties to medicine like jellyfish and horseshoe crabs and learned something new ^_^#im not confident i could pull off a non-mammal furry but they were really good ideas i might put into smth else.. i also thought of#axolotls bc of their regenerative thing and growing back limbs but i think that would suit smth like a surgeon or amputation...#possums and bats were also an option bc theyre actually really resistant to most diseases like rabies but i feel like ppl wouldnt know that#if they saw it so it looks a little ironic at a glance. rabbits rats and mice were my second option bc of animal testing and lab rats#less obvious reference but the moon rabbit in chinese mythology is loosely connected to medicine bc it makes the elixir of life#otherwise lab mice in a pharmacy / modern medicine setting seemed fitting and jerboa tails remind me of cotton buds#and. ironically. jerboas are more closely related to elephants than rats and mice. can you believe it#my art#myart#my oc#sona#plaguesona#cottonbud#fur#furry art#character design#ref sheet#oc ref sheet
131 notes
·
View notes
Text
so... apparently I've been writing Sammelweis' name wrong the entire time. It's Semmelweis, just like the doctor Ignaz Semmelweis.
I do wonder if she's going to have a heavy-handed reference to the real-life Semmelweis. Look him up, his story and role in the founding of antisepsis practices is incredibly interesting if you're into medical history like me.
#reverse 1999#semmelweis#certified storm moments#she's an npc in the rougelike mode that's introduced in the uh... 1.5 patch I think? or is it 1.6 i can't quite remember#i was curious on what her fullbody looked like and i thankfully found this on danbooru#why is your waist so tiny tho. maam your belt is crushing your organs! let your abdomen breathe jfc#you may not know this about me but i really love looking up medical history and pathology. its a really fascinating topic to me#modern medicine is such a miracle and i am intrigued on how things lead to the medicine and practices we currently have. how did#people back in the day deal with certain diseases and what was the misconceptions and what they got right but didn't quite know#the explanation of#jesus the tags turned into an essay of why i like this
48 notes
·
View notes
Text
My least favorite misconception about tfc Heavy and Medic is that they didn’t like each other and Cheavy never respected or liked him
That’s the complete opposite
Cheavy and Cmedic cared and were inseparable when around each other, they cared and valued each other’s work. We can tell that from the only two voice lines in the game being what (many including myself) believe to be Cheavy yelling for Cmedic for help, tho his tone could be better, he still asks semi-politely for help (audio clip below)
And explicitly on Cmedic’s own official wiki page it states that he’s literally Cheavy’s best friend! (photo below)

The reason I think this misconception is so widespread in tf2/tfc spaces is because we only see how Cheavy interacts with Medic, who he explicitly says he doesn’t trust. Also Medic had been experimenting on both him and the tfc mercs for who knows how long and spent their entire medical budget on expensive animal organs. I would too be made if the guy who thought would act like a professional was doing this stuff the you and the people you’ve spent more the 40 years of your life with (photo below)

TLDR; saying tfc Medic and Heavy hate each other is wrong and you’re just uneducated
#tfc#team fortress classic#tf2#team fortress 2#tfc heavy#Classic heavy#tf2 Medic#team fortress 2 medic#tfc medic#classic medic#tf2 comics#I just hate that misconception about their characters#and especially about Cheavy’s own character#it’s not that he hates all medics#he just hates Medic in particular
208 notes
·
View notes
Text
What kind of cruel joke is it that a Ratchet fictionkin, a FIELD MEDIC, was born into a family that believes that doctors are evil power hungry people who just want to stuff you with more pills so they can make more money??? That's not true at all, but that's what I grew up on. My parents were so paranoid about doctors; I hadn't seen a doctor since I was in kindergarten, and only within the last four months began going to regular checkups. I didn't have a gp until I was 20, this is ridiculous.
I wanted so badly to be a doctor as a kid(now I know why, smh), but I couldn't tell my parents that because it would end in a lecture on the corruption of mankind. Jokes on you, I'm not even human, but that's neither here nor there. I always just said I wanted to be a veterinarian, because that was the closest thing...
I binged shows like Bones, NCIS, ect, because it gave me a peek into a world that felt forbidden. I read medical books of every kind, as it fascinated me. I wanted so badly to help people, to be there for them in their darkest hour and tell them it would be ok. And then make it ok. When someone got hurt, I would feel awful that I couldn't help them the way I wanted to.
In my alterhumanity I found the answers as to why I was so fascinated by something I was told was so awful. I am a medic. I carry my first aid kit with me every time I leave the house, I always have an extra bandaid or bottle of hand sanitizer, or burn kit, or treat for a sniffling kid who let me patch them up. Echoes of the life that feels so familiar to me, echoes of a life that feels right, feels like mine. And now that I know who I am, I want to shout it from the rooftops.
I am Ratchet. I am a medic. I am here, and I will be here for any who need a guiding hand.
#tfp ratchet fictionkin#fictionkin vent#otherkin#nonhuman#transformerskin#transformersprimekin#tw mention of medical misconceptions#tw medical
8 notes
·
View notes
Photo

be strong everyone, keep living your best you
(combination with recent national events and a coworker calling T “steroids” just makes me nervous and scared for everyone’s safety and well being)
#trans day of visibility#sona#beeble#okay but fr tho i had to explain to this man that T doesnt cause fucking roid rage#like bro?#you can't OD on T because it TURNS INTO ESTROGEN#i had to tell him my medical doctor and not my therapist told me that before he believed me#the lack of understanding and misconceptions is what scares me the most with people#im just furious#trying to tie it to gun laws and the recent tragedy in tennesee#trans people shouldn't own guns until they're stable bro that's horrible wtf#anyways 2 years on t and my gender is great#ill stop rambling now#done diddly doodle#lmao i cant spell anyways
75 notes
·
View notes
Text
HELLO TUMBLR DOT COM HERE IS SOME MENTAL HEALTH INFORMATION FOR YOU
So, a lot of terms get thrown around without people really knowing what they mean, especially when it comes to mental health awareness. I am definitely guilty of this, which is why when i am corrected i am trying to make a point to share the correction with others.
So. I was talking with my therapist an came around to the fact that I come up with stories in my head to fall asleep, something that people frequently say is Maladapative Daydreaming. But my therapist informed me that no, its not.
Maladaptive Daydreaming is only maladaptive if it is actively impeding function.
So, if your stories you come up with before bed aren't screwing over you or your sleep schedule, by all means, continue to make fanfiction in your head!
I am not a medical professional, if your doctor says you shouldn't be doing something, listen to them, not me
#mental health#mental health advice#Mental health matters#maladaptive daydreaming#Don't treat this as actual medical advice I'm begging you#I'm just passing on info to fix a misconception
21 notes
·
View notes
Text
most L take of all time to be like "well if you support trans people being able to change their bodies medically you should support people taking o/zem/pic for wl"
#like wow doing the medical change that people constantly discourage which youll likely experience oppression for & potentially be ostracized#by loved ones or even killed for etc etc is really the same thing as doing the medical thing thats encouraged even when its knowingly going#to be detrimental to your health bcus its pushed byboth fucked up beahry standards & misconceptions abt what 'health' is are totally the#same thing.#texticles
4 notes
·
View notes
Text
Common misconceptions about asthma
Asthma, a chronic respiratory condition, is often misunderstood. Here are some common misconceptions about asthma: Misconception 1: Asthma is only a childhood disease. Reality: While asthma often begins in childhood, it can develop at any age. Adults can also develop asthma even if they did not have it as children. Misconception 2: Asthma is contagious. Reality: Asthma is not contagious. It…

View On WordPress
2 notes
·
View notes
Note
So random question, I recently got my drivers permit and was asked if I wanted to be registered as a organ donor. I said no because my drivers Ed teacher said not to, because if we put organ donor on our permit/license and then get into a car accident paramedics will not try and save us, is this actually true?
No no no no NO. If your driver’s Ed teacher said that they are extremely freaking ignorant. Being an organ donor does NOT mean that we won’t try to save you. What it means is that if you die you are giving permission to donate your organs so that others whose organs are dying may have a chance to keep living. It could be as simple as corneas to as complicated as a heart.
Being an organ donor does not at all in any way, shape, or form affect your care. We will always try to save you, sweetheart.
#you ask skye answers#lovely anon#Congrats on getting your learner’s permit btw!#Skye talks medical stuff#Idk how this is a misconception but I’ve heard it before and it blows my mind#Makes us sound like vultures just waiting to find ways for people to die
11 notes
·
View notes
Text
Relief from Jellyfish Sting Pain
There is a popular misconception that if somebody is stung by a jellyfish, you can relieve the pain by urinating on the area of the sting.
#poll#tumblr polls#tumblr poll#misconceptions#science#science misconception#animals#animal misconception#jellyfish#sea life#sea creatures#medical misconception
4 notes
·
View notes
Text
I hate when someone tells me something that is Simply Incorrect, but in a way that I can't correct them without feeling like a know-it-all killjoy
like when my dad was moving out of state and let me take a bunch of open liquor bottles, including two bottles of absinthe, and he let me know that one tasted better but the other one had stronger ~effects~ which he went on to describe, and I had to be like 'woooah :O okay cool' instead of 'absinthe is not actually psychoactive and what you were feeling was a placebo if anything'
#I had never even HAD absinthe before he gave me his I just am a person who collects miscellaneous information at random#anyway this was years ago and I have finished the good bottle and the 'woooOOOooo ~green fairy~' one remains largely untouched#because putting more wormwood in absinthe still doesn't make it drug you but it DOES! taste VERY bad!!#a less fun example is one time my nurse practitioner was like 'you need to drink 8 glasses of plain water every day'#and I had to be like :) okay well! the 8 glasses of water thing is a common misconception and you are giving it to me as medical advice#but it feels safer to nod and smile than risk casting myself as a 'well I'VE done my OWN RESEARCH' guy at the dr's office#anyway I just kinda collect fun facts but I never know how to bring them up in situations like this lmao#people hate to be corrected but *I* hate to let people go around believing something that's not true and I dunno how to resolve that#usually what I do is say nothing but then google it later like 'that WAS incorrect though-- wasn't it?' (it was)#about me#potions
5 notes
·
View notes
Text
obsessed with how people call any critique or questioning of the big pharma industries surrounding meds for mental illness and neurodivergence “ableist med shaming”. we are never escaping this prison that society has crafted around us.
#these medications are . not great in many ways and conversations need to be had 😭#as someone who’s been on 4 diff ssris and is currently on them#I hate hate hate the way psychiatrists treat them and gps give them out to even mild depression cases#overprescribed with their negative side effects undermined just to get mental health treatment responsibility off your bac#efficacy of half these meds is questionable too in terms of their harm reduction but go off I guess#don’t even get me started on ssri polypharmacy and this concept of perpetually increasing doses + therefore adverse effects until ‘it works’#putting people on insane cocktails without even being in good therapy like you can’t make this shit up#personally I can’t wait to get off my meds#the idea that once you’re on them and stable you should never stop taking them#it’s just the drug companies trying to like their pockets 😭#some people may need meds forever but for that to be your aim from the onset of taking them ? :/#most mental illnesses aren’t even chemical imbalances that’s literally a medically proven misconception
3 notes
·
View notes
Text
i realized a little while ago that i’ve never explained why johanna goes from absolutely hating doctors in her canon verses to being in the medical field in her modern verses. in the victorian era, there was less of a divide between doctors that helped you when you got sick and psychiatry. since foggs was absolutely horrible ( as were most ‘mental hospitals’ of the time ), johanna doesn’t know much of a difference between the two in canon. she associates all types of doctors with her experience in an insane asylum. those kinds of doctors hurt her and caused a lot of trauma.
in her modern verse, she knows who her father is and she feels a tremendous amount of guilt because of it. in canon, she is aware of how corrupt turpin is and carries that guilt with her, too. johanna is both of their next of kin. she gets their inheritance which doesn’t help that guilt. because of this guilt, she feels the strong need to help people. while living with turpin, she made plans to become a nurse since it’s a more traditional female occupation and that’s what turpin wanted her to become. a teacher or a nurse or something in that nature ( whether or not he would allow her to actually pursue that career after graduating from university is doubtful ).
however, johanna cannot handle the sight of blood. it makes her nauseas and anxious and it’s been the cause of flashbacks for her before. even before she was almost murdered, she couldn’t stand the sight of blood. for that reason and partly because she wanted to spite turpin by not going into a traditionally feminine role, she decided to become a medical assistant. that way she gets to help people. maybe try to shrug off some of that guilt from the hurt the actions of her biological father and her former guardian caused. this way, she won’t have to deal with a lot of blood either.
johanna decided she wanted to work with children because maybe she might be able to notice patterns of abuse they’re going through before it escalates. she wants to prevent any more situations like the one she was in. she wants to be financially independent because that was something turpin held over her head a lot. this way, she gets to be. johanna is very happy with her chosen occupation and being able to be financially independent means the world to her.
edited to add that johanna still doesn't like going to the doctor for herself in her modern verse. this is mostly because she's trying to hide her ed and poor sleeping habits from everyone and if anyone can and will figure that out about her, it's the doctor. she also knows that doctors ask about mental health/well-being and she does not want to go to a mental health professional. just as in canon verses, she does not like any kind of mental health professional and refuses to trust them because of her experiences at foggs.
#i should probably address the misconceptions about her job#she doesn't repair people's wounds or readjust bones or anything like that#she does the pre-check up stuff like taking temperatures and things like that#jo does know how to sew stitches and minor things like that but she isn't a doctor you know?#why am i rambling so much tonight?#*❈ ‣ 𝘩𝑜𝑤 𝑐𝑎𝑛 𝑦𝑜𝑢 𝑟𝑒𝑚𝑎𝑖𝑛 𝑠𝑡𝑎𝑟𝑖𝑛𝑔 𝑎𝑡 𝑡𝘩𝑒 𝑟𝑎𝑖𝑛? — ( headcanon. )#medical tw#hospital tw#abuse tw#murder tw#death tw#ask to tag /#ed tw#anorexia tw#eating disorder tw
2 notes
·
View notes
Text
Can a Chihuahua Be a Service Dog in 2024? Shocking Truth and Facts!
In recent years, service dogs have become more recognized and accepted worldwide. These dogs are trained to help people with physical or mental disabilities. They make daily life easier and give their owners more confidence. While big dogs like Golden Retrievers and German Shepherds are often thought of as service dogs, Chihuahuas can also be great at this job. This article will provide the…
#adaptability#agility#Americans with Disabilities Act#anxiety#behavioral traits#breed discrimination#Chihuahuas#deep pressure therapy#disabilities#emotional support#grooming needs#health issues#independence#legal requirements#loyalty#medical alert tasks#misconceptions#mobility assistance#positive reinforcement#psychiatric service dog tasks#service dogs#skepticism#socialization#supervision#support#tasks#training#training methods#unique skills
1 note
·
View note