#american physical therapy association
Explore tagged Tumblr posts
Last Seen Blogs





Text
Pain Relief Associations.
#pain relief#american pharmacists association#association;#sciatica pain relief#sciatic nerve pain relief#sciatica relief#sciatic nerve pain relief exercises#leg pain relief#knee pain relief#sciatica exercises for sciatica pain relief#leg pain relief exercises#american psychological association#back pain relief exercises#american physical therapy association#exercises for leg pain relief#lower back pain relief#psychology and pain relief#educational#interesting#did you know#inspiration#motivation#information
0 notes
Text



the importance of mindfulness
mindfulness is a practice that involves being fully in the moment and paying attention to your thoughts, feelings and sensations without judgment. it has gained recognition for its positive impact on both mental and physical well-being.
here are some reasons why practising mindfulness is important:
mindfulness helps manage stress by allowing us to respond to our environment differently. our minds are not well-suited for the modern world, but mindfulness techniques let us navigate challenges more effectively.
studies show that mindfulness-based therapies can reduce anxiety and depression. by focusing on the present moment, individuals can better cope with life’s difficulties and protect their mental well-being. since mindfulness teaches us to be fully in the present, mental noise (which is often a large contributor to anxiety and depression) can be reduced. additionally, mindfulness practices, such as meditation, activate the parasympathetic nervous system. this leads to a sense of calm and relaxation, reducing reactivity to stressors.
mindfulness isn’t just about mental health; it also positively impacts our physical health. evidence suggests that it can lower blood pressure, improve sleep quality, and enhance overall well-being. by managing stress and promoting relaxation, mindfulness contributes to cardiovascular well-being. it can also lead to better sleep quality. when we're mindful, we let go of racing thoughts and create a calm mental space conducive to restful sleep. while more research is needed, preliminary evidence suggests that mindfulness might enhance immune function. it may help people recover more quickly from illnesses like colds or flu. for further reading about this, see this article from the american psychological association.
practising mindfulness often leads to increased relaxation, enthusiasm for life, and improved self-esteem. it helps us to see the world differently and live a more compassionate, fulfilled life.
mindfulness techniques can help people cope with physical pain. by being fully present and accepting the sensations, individuals may experience relief and improved pain management.
but nene, how can i be mindful?
first, dedicate a specific time each day for mindfulness practice. something i have made a routine of is stretching when i first wake up ~ allowing myself time to wake up slowly and move my body. your dedicated time could be as short as five minutes, or longer, depending on your practice.
find a quiet and comfortable spot where you won't be disturbed. sit or lie down in a relaxed position.
close your eyes and pay attention to your breath. feel the air entering and leaving your nostrils or the rise and fall of your chest. if your mind wanders, gently bring it back to your breath.
some specific mindfulness practices include:
three-step breathing kettering general health - youtube video
five senses check-in the partnership in education - youtube video with love, esta - youtube video
body scan policy research associates - youtube video mariellen brown - youtube video
further reading: positivepsychology.com NIH news in health psychcentral american psychological association
remember - mindfulness is a skill that improves with practice. regular mindfulness, whether through formal meditation or everyday activities, can have great positive effects.
i hope you enjoyed today's post! ❤️ nene
image source: pinterest
#elonomh#that girl#elonomhblog#becoming that girl#student#productivity#student life#academia#chaotic academia#study blog#it girl#it girl aesthetic#it girl energy#pinterest girl#dream girl#vanilla girl#pink pilates princess#study#self awareness#self compassion#self help#self improvement#self love#self reflection#self care#health and wellness#health and wellbeing#wellness aesthetic#wellness girl#wellness and health
72 notes
·
View notes
Text
humanizing your desired reality.


made one of these months ago on tiktok so im remastering it for here (˵•̀⤙•́˵)૭
harry potter ⋆ ˚。⋆୨୧˚
✧ getting up early for class.
✧ working with dangerous objects / spells.
✧ navigating schools layout.
✧ living beside a forest with potentially dangerous beings.
✧ school being linked to multiple (students) deaths.
✧ pulling all nighters to study for exams & homework.
✧ being separated from non-magic folk.
✧ seemingly strict with large punishment.
marvel ⋆ ˚。⋆୨୧˚
✧ putting life at risk.
✧ unreliable scheduling.
✧ seeing friends, family & people getting injured.
✧ the balancing of two lives.
✧ always feeling like something is coming / something always being after you.
✧ lack of (openness in) therapy
✧ inability to open up without endangering loved ones.
supernatural ⋆ ˚。⋆୨୧˚
✧ endangering self & others.
✧ survivors guilt.
✧ lack of permanent home & space — always moving & traveling.
✧ little to no personal space.
✧ little time to mourn d3ath.
✧ being on call 24/7
✧ little sense of security or safety.
hunger games ⋆ ˚。⋆୨୧˚
✧ being exposed to death & violence so young.
✧ starvation & dehydration.
✧ weaponizing your loved ones.
✧ physical & emotional stress / trauma.
✧ possible imposture syndrome.
✧ heavy surveillance, always being watched.
✧ never being able to predict what's going to happen.
✧ never being able to 100% trust the people around you.
the walking dead ⋆ ˚。⋆୨୧˚
✧ never knowing when "the end" is coming.
✧ injury, infection.
✧ watching yourself & others deteriorate & not being able to do anything about it.
✧ abandoning your home & shelter.
✧ lack of stable / scarce food & water supply.
✧ the smell.
✧ discomfort of bodily horror.
stranger things ⋆ ˚。⋆୨୧˚
✧ the stigma of therapy / asking for help.
✧ dealing with virtually unknown creatures.
✧ knowingly endangering yourself on your own or simply by association.
✧ fear of the unknown.
✧ the feeling of "never ending" & not knowing what else is coming.
✧ managing school onto of saving the world.
✧ the adjustment of not having modern technology
american horror story ⋆ ˚。⋆୨୧˚
— mixture of / general for all seasons
✧ never knowing what's coming.
✧ having to cope with supernatural.
✧ never truly being alone.
✧ possibly never getting answers.
✧ not being believed.
✧ loved ones / friends turning against you.
✧ lack of evidence.
✧ people dismissing your experiences.
✧ dying & being attached to a space, never allowing you to leave.
✧ bodily horror.
fame dr ⋆ ˚。⋆୨୧˚
✧ constantly having eyes on you, being judged.
✧ lack of privacy.
✧ social pressure.
✧ stalkers & paparazzi.
✧ not being able to do things that you're used to — target shopping, out to dinner , going on vacation — without attracting groups of people.
✧ being a safety hazard.
✧ being seen as a character or brand instead of a person.
✧ lack of free time.
✧ words being twisted.
✧ little sympathy towards you, dismissal of problems.
#desired reality#reality shifting#shiftblr#shifting#shiftok#shifting motivation#shifting realities#shifter
63 notes
·
View notes
Text
https://www.wsj.com/articles/most-transgender-kids-turn-out-to-be-gay-gender-affirming-care-conversion-therapy-58111b2e
Most ‘Transgender’ Kids Turn Out to Be Gay
Subjecting them to medical interventions is the modern-day version of ‘conversion therapy.’
By: Roy Eappen
Published: Dec 14, 2023
As a medical professional who happens to be gay, I’ll be celebrating Dec. 15, the 50th anniversary of the American Psychiatric Association’s decision to remove homosexuality from its list of mental illnesses. The longstanding designation was based on prejudice, not medical research, and the revision marked the beginning of the end for so-called conversion therapy, which sought to “cure” gays and lesbians of a nonexistent malady.
Half a century later, the medical establishment is pushing a new kind of conversion therapy under the guise of transgender identity. No one is suffering more than gay kids. In Canada, where I practice, and in the U.S., physicians provide what’s euphemistically known as “gender-affirming care” to patients as young as 8, and the leading transgender health association has opened the door to interventions at even earlier ages. Under this framework, those who feel uncomfortable with their bodies may receive a medical regimen including puberty blockers, cross-sex hormones and sex-change surgeries. These interventions typically stunt, remove or irreversibly modify a patient’s sexual development, genitals and secondary sex characteristics. Any endocrinologist or other physician who rejects this approach is alleged to be endangering the health and even the life of his patients.
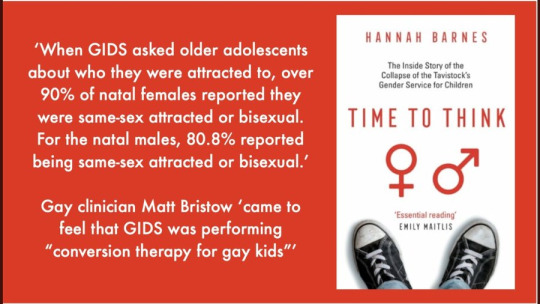
But are these patients really “transgender”? Research shows that some 80% of children with “gender dysphoria” eventually come to terms with their sex without surgical or pharmaceutical intervention. Multiple studies have found that most kids who are confused or distressed about their sex end up realizing they’re gay—nearly two-thirds in a 2021 study of boys. This makes sense: Gay kids often don’t conform to traditional sex roles. But gender ideology holds that feminine boys and masculine girls may be “born in the wrong body.”
In this light, “gender-affirming care” looks a lot like conversion therapy. In the past, it took the form of electroshock therapy, chemical castration and even lobotomy. Now it takes the form of rendering teenagers sterile and sexually dysfunctional for life. Clinicians from the main U.K. transgender service referred to prescribing puberty blockers as “transing the gay away”—a play on the description of old-fashioned conversion-therapy as “praying the gay away.” A clinician who resigned from the U.K. service accused it of “institutional homophobia.” Clinicians at the service had a “dark joke” that “there would be no gay people left at the rate Gids”—the Gender Identity Service—“was going.”
Consistent with conversion therapy, physicians are telling young gays and lesbians that something is wrong with them, based on a regressive view of what it is to be male or female. Also consistent with previous efforts to cure homosexuality: The resulting interventions often create lifelong medical problems, both physical and mental. Contrary to advocates’ claims, there’s no evidence that puberty blockers, cross-sex hormones, or surgeries reduce the risk of suicide.
Children who take this road face a lifetime of pain, infertility and anguish. They deserve real mental-health care to address common underlying comorbidities, not mind- and body-altering medical interventions that try to make them into something they aren’t.
Fifty years ago, the medical assault on homosexuals began to end. Now society has been told that accepting transgender identity is the same as accepting gays and lesbians. But it isn’t. Even well-intentioned acceptance of transgender identity disproportionately harms them. One day perhaps professional organizations like the Endocrine Society and the American Academy of Pediatrics will follow the evidence, as the APA did in 1973. Until then, gay kids will continue to suffer from an injustice that was supposed to end 50 years ago.
Dr. Eappen is a practicing endocrinologist in Montreal and a senior fellow at Do No Harm.
==
Reminder:

There's no such thing as "trans kid."
#Roy Eappen#gay conversion therapy#gay conversion#homophobia 2.0#woke homophobia#gender ideology#queer theory#medical mutilation#medical malpractice#medical corruption#medical scandal#gender affirming care#gender affirming healthcare#religion is a mental illness
71 notes
·
View notes
Text
The benefits of jumping rope for 10 minutes every day


Jumping rope, a simple yet effective exercise, has garnered attention as a potent cardiovascular and full-body workout. While often associated with children's play, this activity is increasingly recognized by fitness enthusiasts and health professionals alike for its numerous health benefits. Engaging in just 10 minutes of daily rope jumping can yield significant improvements in cardiovascular health, muscular strength, coordination, and overall physical fitness.

Cardiovascular health
Jumping rope is a highly effective cardiovascular exercise. A study published in the Journal of Sports Science & Medicine found that 10 minutes of daily rope jumping for six weeks improved participants' cardiovascular endurance as effectively as 30 minutes of jogging. The rhythmic, repetitive nature of rope jumping raises the heart rate, strengthening the heart muscle and improving circulation. This enhancement in cardiovascular efficiency reduces the risk of heart diseases, including hypertension and stroke.
Caloric burn and weight management
Jumping rope is also an efficient way to burn calories. According to research published in the Harvard Medical School Health Publication, a person weighing 155 pounds (70 kg) can burn approximately 124 calories in just 10 minutes of moderate-intensity rope jumping. This calorie expenditure is comparable to more extended sessions of other aerobic activities, making it an excellent option for those looking to manage or reduce their weight. Consistent daily practice can contribute to a caloric deficit, which is essential for weight loss.
Improved coordination and balance
Rope jumping requires synchronization of hand and foot movements, enhancing coordination and balance. A study demonstrated in the Journal of Physical Therapy Science that jumping rope improves proprioception and body awareness, which are crucial for preventing falls, particularly in older adults. This enhanced coordination also benefits athletes by improving their agility and reaction times in various sports.
Muscular strength and endurance
Although primarily known as a cardiovascular exercise, jumping rope also engages several muscle groups. The calves, quadriceps, hamstrings, and glutes are activated with each jump, while the upper body, including the shoulders, arms and core, works to maintain rhythm and stability. Over time, daily rope jumping can lead to increased muscular endurance and strength. A study published in the European Journal of Applied Physiology found that athletes who included rope jumping in their training regimen experienced significant improvements in leg strength and overall muscle tone.
Mental Health Benefits
Physical exercise, including jumping rope, has well-documented mental health benefits. The American Psychological Association highlights that regular physical activity can reduce symptoms of anxiety and depression. The repetitive nature of jumping rope can have a meditative effect, helping to reduce stress levels. Additionally, the endorphins released during exercise enhance mood and promote a sense of well-being.
Time efficiency
One of the most significant advantages of jumping rope is its time efficiency. In today's fast-paced world, finding time for exercise can be challenging. However, with just 10 minutes a day, individuals can achieve substantial health benefits without the need for extended workouts. This makes rope jumping an accessible and practical option for people with busy schedules.
[photos from Pinterest]
#benefits#it girl#that girl#clean girl#becoming that girl#glow up tips#hyper feminine#healthy girl#pink pilates girl#this is what makes us girls#weight loss#beauty tips#dream girl tips#health tips#jumping rope#fitness#fitness girl#fit girls#fit beauty#fitblr#fitspo#healthyliving#healthy diet#healthy eating#healthylifestyle#mental health#healthcare#health and wellness#healthy food#wellness and health
19 notes
·
View notes
Text
‼️🎨 Fundraiser Fridays Art Requests 🎨‼️

To continue to support those in need, I'm doing a sort of art request/giveaway!
Every Friday, send proof of your donation of at least $5 to a gofundme or charity along with an art request, and I'll draw something for you!
More examples of my work are found on my art blog, mimitay-art
Priority is given to helping those struggling in Palestine, Sudan, and DR Congo, as well as hurricane disaster relief efforts post-Helene and Milton.
———
Where To Give?
First I want to highlight the campaigns of some of the people I’d been helping each week!
The Al-Resh family (this isn’t everyone, but those I’ve spoken with the most):
Wafaa - Raising money for the family, especially her mother who’s sick
Mohi - Struggling with several severe health issues amid a genocide
Fidaa - Needs to support her infant daughter, Sila
Ahmed - Raising money for the family, extended goal to help support Mohi’s medical treatment
Others in need of help:
Aseel - Both of her parents have health issues, her father in particular is a stroke survivor in need of treatment and physical therapy
Hana - Needs support for her and her son, Youssef
———
This master document lists resources for helping Palestine, Sudan, DR Congo, Haiti, Yemen, Hawai'i, and Lebanon and for staying informed.
More links below— but they’re are not all there is, there are many many more reputable organizations to give to!
———
🇵🇸 Palestinian Fundraiser Spreadsheets/Resources 🇵🇸
Hussein and Nabulsi's list
Gazavetter's list
Bees and Watermelons
The Butterfly Effect Project
Operation Olive Branch
Gazafunds - This link gives you a random Gazan gfm to donate to if you can't decide.
———
🇸🇩 Sudanese Charities/Humanitarian Organizations 🇸🇩
Sudanese American Physicians Association (SAPA)
Sudanese Red Crescent
Sudanese American Medical Association (SAMA)
Darfur Women Action Group
Hadhreen (7adhreen)
———
🇨🇩 Congolese Charities/Humanitarian Organizations 🇨🇩
Friends of the Congo
Panzi Foundation
CAMME
Malaika
Focus Congo
Action Against Hunger
———
⛈️ Hurricane Disaster Relief ⛈️
Gofundme's Hurricane Relief Fund
Red Cross
Fleet of Angels
MANNA Food Bank
Hunger and Health Coalition
BeLoved Asheville
———
You can send proof of donation (screenshot of receipt etc etc) via ask and we can work out the details of your drawing request privately. I just ask that it stays simple so that I can complete it within a week alongside classwork!
Same standards for what I will or won't draw for commissions apply here. (That being said, if there's something you want drawn that's bigger or more complicated, my commissions are open as well)
Incentive or not, please consider donating when you can afford to!
11 notes
·
View notes
Text
Medical stuff I wish cisgender people knew
Medical transition does not make someone a man or a woman. A trans woman is a woman, and a trans man is a man, regardless of what medical treatment they have or have not had. Medical treatment just makes life a hell of a lot easier for a lot of people
It is not true that 40% of trans people commit suicide. The infamous 40% statistic refers specifically to rates of suicide attempts which occur before transition. Most of these attempts fail and the person survives.
Transition vastly reduces risk of suicide attempts from 40% down to around the national average, while dramatically improving mental health, social functionality, and quality of life for those who need it.
Being trans is not classified as a mental illness by either the American Psychological Association or the World Health Organization. Gender dysphoria (in the DSM) or incongruence (in the ICD) is recognized by both as a medical condition, and transition is the only treatment recognized as effective and appropriate medical response to this condition
When able to transition young, with access to appropriate medical care, and spared abuse and discrimination, trans people are as psychologically healthy as the general public
Transition-related medical treatment is not new or experimental; it has existed for over a century
Transition-related medical care is recognized as necessary, frequently life saving medical treatment by every major US and world medical authority
Transition is the only treatment for dysphoria that has proven to be effective. Attempts to "cure" trans people, alleviating dysphoria by changing the patient victims' gender identity to match their appearance at birth (aka "conversion therapy" or "gender identity change efforts"), are such utterly worthless and actively destructive train wrecks that this "therapy" is condemned as pseudo-scientific abuse by all major medical authorities
Transition is a very individual process; not everyone needs or wants the same things
"Regret" rates among trans surgical patients are vanishingly rare, consistently found to be about 1% and falling. This 1% includes people who are very happy they transitioned, and often are still glad they got reconstructive surgery, but regret only that medical error or shitty luck led to sub-optimal surgical results. That's a risk in any medical treatment, and a success rate of about 99% is astonishingly good. And only about 6% of trans people have had reconstructive surgery, so rates of surgical regret among trans people as a whole are about 0.06%.
Transition "regret" is vanishingly rare. Of everyone who starts even the preliminary steps of transition, like trying a new name or pronouns socially, only about 0.4% eventually realize it is not right for them (see p108-111). Most realize this soon after starting transition, when physical changes are minimal or nonexistent. Many do not regret exploring transition as an option, even if ultimately it wasn't what they needed.
Hormone therapy is pretty cheap, is generally the first line of treatment most trans people get, and dramatically impacts one's appearance
Most trans people socially transition long before they get reconstructive genital surgery, if they ever get it at all. Not everyone needs or wants surgery, and even those who do need it are often unable to afford it. Genital surgery for trans women costs tens of thousands of dollars out of pocket. Surgery for trans men can cost between tens of thousands to over $100k, depending on the procedure one is getting.
25 US states currently have laws prohibiting health insurance companies from having "trans exclusion" policies, where they categorically refuse to cover medically necessary transition-related treatment. This means that a small but growing number of people are able to get treatment, including surgery, covered by insurance
When a child or adolescent transitions that does not mean they are being rushed into irreversible surgery
Transition for predolescent children is 100% social; changing hair, clothes, name, pronouns, and/or the gender they are recognized as by their family and community. No medical treatment is necessary or provided before the start of puberty
The first line of medical care for trans adolescence is puberty-delaying treatment. It is gentle, fully reversible, and has been used for decades to delay puberty in kids who would otherwise have started it too young. It does nothing but buy time, and has no long term effects
Transition-related hormone supplements do not cause serious long term health problems
Reconstructive genital surgery for both trans women and trans men can provide excellent results
#gender equality#gender roles#gender bender#genderqueer#gender#gender stuff#queer stuff#trans stuff#pronouns#trans tag#thepinprick#pride#trans#pin#lgbt pride#pride flags#lgbt#queer#gay pride#pride edit#pride icons#ace pride#lesbian pride#mogai pride
390 notes
·
View notes
Text
Bizarre Prison Procedure
Forced Thorazine to place inmates in a Full Body Plaster Cast
Others who were more violently suicidal were treated to one of the most bizarre procedures in prison history, a plaster body cast from neck to ankles, with holes for defecation and urination. This restraint was developed in 1978 by the penitentiary's medical director as an alternative to drug therapy. As he explained to the team of forensic consultants, he thought it was "probably more humane to physically restrain people" than to make them suffer the affects of some tranquilizers. His premise is voided by the fact that Thorazine had to be forced down a fit-throwing convict's throat to get him into the body cast. Dr. Orner spoke about his use of these casts at a meeting of the American Medical Association's Conference on Health Services in Correctional Facilities in November of 1979. He told his audience that he was using body casts as a method of crisis intervention. "And he did it in almost a bragging tone—he sounded like he thought it was terrific," one listener, an attorney with the New York Legal Aid Society, commented. "I asked him how he got people into it, considering that they would be supposedly violent people in some kind of episode, and he said that if it took six officers, eight officers, it didn't matter how many it took to hold the guy down." But according to an interview with an ex-inmate who was placed in a body cast in the summer of 1979, it was Thorazine, not guards, that subdued him:
I was brought down to the hospital in handcuffs, and thrown off into the strip cell a number of times. Finally they upped and stuffed me off in that oP cast situation… But before they did that, they poured Thorazine down my throat. Held my jaws right there, and just poured it right in my face because I didn't want to take it. Well.. .after I got in that full body cast, I busted all out of that, man, because I was hysterical. Scared. Somebody's trying to kill me…"
From: The Hate Factory A First-Hand Account of the 1980 Riot at the Penitentiary of New Mexico, page 65, ISBN-10: 0-595-36669-4 (pbk) by Georgelle Hirliman.
#thorazine#body cast#prison#prison procedure#full body cast#prison riot#Hate Factory#Georgelle Hirliman
65 notes
·
View notes
Text
Meeting with the Renlunds
I met with Elder Kevin Hamilton and he offered to walk me over to Elder Renlund's office for my next appointment as it would help me get through security more easily.
Elder Hamilton greeted the secretary and explained he found me wandering around and helped me find where I was going.😄 Then he said that we became friends when he did a stake conference in Florida and I have a standing invitation to visit every time I'm in Utah.
At that moment, Elder Renlund steps out of his office door and proclaims, "I trump that invitation. He gets to see ME when he's in town." 😁
It was a humorous way to be handed off from the one to the other.
—————————
Elder Renlund asked if I was in town for that conference in Provo (the Gather Conference)? Y'all, I was impressed that he knew about it! Great credit to the conference organizers!
—————————
I reminded the Renlunds that the last time I visited, they gave me a book they co-wrote. When I saw it was about the Melchizedek Priesthood, I was like "Go Ruth!" There's no reason a woman shouldn't write about the priesthood.
This time I brought them a gift, a copy of a book which contains a chapter I wrote.
Me: I'm a little nervous giving it to you because I wrote it from my viewpoint. I was very honest and that means not everything matches the Church's view. Some things about church are hard for me.
Dale: We will read this.
Me: Now I'm even more nervous!
Ruth: Don't be nervous. You shouldn't be nervous about telling the truth.
Dale: They're your thoughts and perspectives.
Ruth: Others have done the same, why not you?
Whew, I felt much better after that exchange.
I also shared that writing my chapter led me to realize I may have an eating disorder, and how that led to an official diagnosis and now I'm in therapy. I'm on a journey to better mental and physical health. They were genuinely interested in this development and kind in their support.
—————————
Elder Renlund mentioned that when he presides over a meeting and opens things up for questions, it's not unusual for LGBTQ topics to come up. As we spoke, the Pride flag got mentioned.
I shared a conversation I had with my friend who recently retired from a 20-year career with the U.S. military. My friend doesn't wear a US flag pin at church. He is there for religion, not patriotism. Anyone who wants to know if he is patriotic should look at his life. Plus, America does some things that aren't compatible with what Jesus taught. My friend wants to keep the two separate.
When it comes to the Pride flag, I feel a little different. No one questions whether Americans are welcome at church. We don't have a history of harsh teachings against Americans. We need to be intentional in signaling that we welcome LGBTQ+ people.
The Pride flag represents queer people and it goes where they go, which means it is there when people fight for Civil Rights or run their business, and however they live their life. This causes some to see the flag as representing things they don't like because some queer people make choices they don't agree with. I think when the average member displays the Pride flag, they are indicating that queer people are welcome and wanted, that they are a safe person to talk with. But for a leader, some will see his wearing the flag as endorsing all the things people associate with it.
Elder Renlund responded that it's like Black Lives Matter. Of course Black lives matter, but the political movement that grew up around that phrase can be seen by some as controversial, so if a leader displays a Black Lives Matter flag people may question or assume he supports all of it.
He went on to say that he appreciates my friend's position because when they lived in South Africa, a friend of his said, "We South Africans don't like Americans telling us what to do." What registered with Elder Renlund is if what his friend sees is an American, then he needs to change so what his friend sees is a disciple of Christ.
—————————
Elder Renlund asked what else is going on in my life and I shared that I'm now on the Affirmation Board of Directors. It's interesting because I don't seek to do things in the LDS/LGBTQ space, but the Lord provides opportunities and I accept them.
His response was, "You can help others and that's what I think God wants you to do."
—————————
They asked how my parents are doing and I mentioned my mom's calling in her ward.
"Your mom is the Primary chorister?" Elder Renlund shared that he is the chair of the committee putting together the new hymnal. "I think the war in heaven started over a new hymnal. Everybody has an opinion." 🤣
—————————
Ruth and I spoke about a person we're both related to. It's a man who was her uncle, and he was married to my grandma and they had 2 children together. He died in World War II and my grandma remarried and had 2 more children.
My grandmother was sealed to her first husband but spent the bulk of her life with her second husband. When my granddad passed away, he was also sealed to his wife, she is sealed to two husbands.
Elder Renlund said that in life there is an asymmetry, men can be sealed to multiple women but women are limited to being sealed to only one man. However in death, all are equal, everyone can be sealed to all those they were ever married to.
This means we don't have a clear understanding of what it's like in Heaven. Since all three of these people are sealed to each other, and they have promises made to them, no blessing will be denied to them. We don't know how that works, but we are convinced of the promises and see them afar off.
Elder Renlund went on to say those who have "LGBTQ issues" and try to be faithful are heroes and the Lord really will bless them.
I brought up that single people face the same questions about their situation as queer people.
His response was of all those who are single and members of the Church, the majority are not active. He doesn't think God is going to harshly judge them. But he thinks God holds real blessings in store for those who try to be faithful. I thought that was interesting, "try" is enough to qualify.
Elder Renlund says there will be a sorting and figuring out who is sealed to whom, but we don't believe anyone will be forced. All wounds will be healed and injustices made whole, and no blessings withheld from the righteous.
—————————
We had met for nearly an hour and needed to wrap up. Elder Renlund proposed, "Let's get a photo." Sister Renlund commented, "I just came from the hair dresser so this works out well." 😂
As we walked out of the office, Sister Renlund explained that he has to go practice his conference talk using the teleprompter so there isn't much wiggle room for extending our visit. She also joked that you'd think these men would have the use of the teleprompter mastered, but they have to practice before every General Conference. 😆
—————————
It was generous of them to take an hour out of their day to spend it in conversation with me
44 notes
·
View notes
Text
Remembering and Fighting for Eden Knight
TW // Suicide, Transphobia, Forced Detransition


Eden Knight was a Saudi Arabic trans woman living in the United States, who on the morning of March 12th 2023, was discovered to have died by suicide after a twitlonger (which, upon reading, proved itself to be a suicide note) was posted to her Twitter account.
Her suicide note goes into detail, and explains the driving force behind her death. The manipulation by three people who lied to and betrayed the trust of Eden in order to force her into de-transitioning, all led by her influential religious conservative family.
Whether they want to admit it or not, they succeeded in what they did. As of March 13th 2023, her death has been confirmed.

(Note: This screenshot redacts her deadname, the original tweet both misgenders and deadnames Eden)
Eden gives the names of the people involved in, what is essentially her murder, so I will explain who they are and what they did to her.
Michael Pocalyko

Michael Pocalyko is the CEO of a company called “Special Investigations Limited." A business that claims they do “cyber security”, and “investigations."
Not only does Michael own this company, but he has also ran as a republican political candidate before, has sat on the boards of pharmaceutical companies, is tied to investment banking and equity firms, JP Morgan, as well as the Heritage Foundation.
He contacted Eden through one of her in-real-life friends, a self-proclaimed "fixer" who told Eden he could help mend her and her family's broken relationship. Michael, and his associate Ellen Cole, introduced Eden to (alleged) Saudi Arabian lawyer Bader Alomair.
Bader Alomair
Not much is known about Bader Alomairs background, but we do know his role with Eden. Bader told Eden he was a lawyer and got her an apartment in Washington D.C. He began to take care of her financially; Eden realized he was grooming her into de-transitioning, living in the closet, and she was now an illegal immigrant (her international scholarship, which she'd been using to go to school in America, had expired which meant she could be deported) who was financially dependent on him. Feeling she had no other option she caved to his demands and changed her physical appearance, along with discontinuing her hormone therapy. She even met with her father and got back into contact with her mother. At this point Michael and Ellen had ceased all communication with her, she had an emotional breakdown and “repented," as Bader booked her a flight to Saudi Arabia.
Final Notes and Thoughts

Eden Knight was failed by so many fucking people. Failed by her transphobic family who literally drove her to death because of their bigotry. Failed by the two American investigators who cared more about money than this poor girls life. Failed by the U.S. immigration system which should've provided her asylum and support.
Eden was a beloved member of the trans community. People knew her as a sharp, witty, thoughtful person who wanted to make the world a better place. She said,
"I hope that the world gets better for us. I hope our people get old. I hope we get to see our kids grow up to fight for us. I hope for trans rights world wide."
It's been eight years since Leelah Alcorn died by suicide, isn't it fucked how we're still fighting for the same things?
Eden deserved to be happy. All of us do.
#queer#trans#eden knight#justice for eden#trans rights are human rights#protect trans people#protect trans kids#protect trans lives#trans woman#transmisogyny#hate crime#transphobia#trans rights#tw transphobia#tw transmysoginy#tw suicide#tw forced detransition#transphobes dni#terfs dni#radfems dni#caesthoffe.txt
101 notes
·
View notes
Text
A.B.A. is the only autism intervention that is approved by insurers and Medicaid in all fifty states. The practice is widely recommended for autistic kids who exhibit dangerous behaviors, such as self-injury or aggression toward others, or who need to acquire basic skills, such as dressing themselves or going to the bathroom. The mother of a boy with severe autism in New York City told me that her son’s current goals in A.B.A. include tolerating the shower for incrementally longer intervals, redirecting the urge to pull on other people’s hair, and using a speech tablet to say no. Another kid might be working on more complex language skills by drilling with flash cards or honing his ability to focus on academic work. Often, A.B.A. targets autistic traits that may be socially stigmatizing but are harmless unto themselves, such as fidgeting, avoiding eye contact, or stereotypic behaviors commonly known as stimming—rocking, hand-flapping, and so forth.
Hammond is now the mother of two autistic sons. Her older son, Aidan, who is sixteen, is nonverbal and needs round-the-clock care. When he was young, he attended a traditional school, but teachers, Hammond said, “were literally calling me every single day: ‘Can you please come here and sit with him? Can you please pick him up?’ ” Hammond tried physical, occupational, and speech-language therapy for Aidan, but he was “kicked out of every single one,” she said. Therapists “felt that his behaviors were interfering with his learning, and that he needed to be in A.B.A.” A.B.A. clinicians, she added, “were at least willing to look at my son.”
She drove him to A.B.A. appointments at a clinic about an hour from their home in southwest Texas, but stopped treatment after just a few sessions. This was partly due to the commute and the co-pay, but also to a discomfort with the approach, which required Aidan to spend long periods, over multiple sessions, solving a puzzle in which he matched shapes to the right-sized holes. “He’s having to do this over and over and over again,” Hammond recalled, “and, when he picked the right thing, it’s, like, Ooh, here’s a Skittle! Like he’s a puppy.”
In recent years, A.B.A. has come under increasingly vehement criticism from members of the neurodiversity movement, who believe that it cruelly pathologizes autistic behavior. They say that its rewards for compliance are dehumanizing; some compare A.B.A. to conversion therapy. Social-media posts condemning the practice often carry the hashtag #ABAIsAbuse. The message that A.B.A. sends is that “your instinctual way of being is incorrect,” Zoe Gross, the director of advocacy at the nonprofit Autistic Self Advocacy Network, told me. “The goals of A.B.A. therapy—from its inception, but still through today—tend to focus on teaching autistic people to behave like non-autistic people.” But others say this criticism obscures the good work that A.B.A. can do. Alicia Allgood, a board-certified behavior analyst who co-runs an A.B.A. agency in New York City, and who is herself autistic, told me, “The autistic community is up in arms. There is a very vocal part of the autistic population that is saying that A.B.A. is harmful or aversive or has potentially caused trauma.”
Until recently, the American Medical Association officially endorsed “evidence-based treatment of Autism Spectrum Disorder including, but not limited to, Applied Behavior Analysis Therapy.” Last summer, the medical students’ body of the association proposed that the organization withdraw its support for A.B.A., citing objections by autistic self-advocates. The association did not adopt the resolution as submitted, but its house of delegates eventually approved an amendment removing any explicit reference to A.B.A., and autistic activists spread the word that A.B.A. no longer appeared to have the outright endorsement of the nation’s largest medical society.
13 notes
·
View notes
Text
COBRA'S MILITARY FILE (OC)

NAME: HOWARD, SCOTT KEOLA
DOB: May 25th, 1985
BIRTHPLACE: Pago Pago, American Samoa.
SERVICE NO: 156-39-43
CALLSIGN: Cobra, Shadow 0-2.
SEX: Male.
MARITAL STATUS: Single.
EDUCATION: High School Education.
LANGUAGES: English, Samoan, Russian.
BRANCH: United States Navy Sea, Air, and Land (SEAL) Teams.(Honorably Discharged.)
RANK: Special Warfare Officer 1st Class (E-6).
PROFESSION: Military Operator/Contractor and Investor for Shadow Company.
TRAINING: Direct action, Counter-terrorism, Amphibious reconnaissance, Unconventional warfare, Hostage rescue, Underwater demolition.
Training Scores
PFT: 298
Rifle Qual: 290
CQB: 22.8s
Disciplinary Record: Clean.
Notes: - 1 domestic decoration (Purple Heart) awarded by the American government for a wound sustained while in active duty, as a result of an act of a hostile foreign force. (2018)
Past Medical History
Height: 6ft3in / 191cm
Current Weight: 260lbs / 117kg
Blood Type: A-
Extensive physical injuries.
1x 3rd Degree Burns (from prolonged exposure to flames) and lacerations after an explosion. Extensive injuries to the skin and soft tissue of the upper left side of his body, including his face. Surgical intervention performed successfully.
15+ Stab Wounds with various degrees of gravity to the torso and upper extremities. 2 instances of antibiotics to stave off infection.
10x GSW. 3x in upper and lower extremities. 4x in upper torso. 3x in lower abdomen.
3x Concussion.
2x Pneumonia. 2 rounds of antibiotics for treatment.
3x Hypoxemia and respiratory distress from smoke/toxic gas inhalation. 3 rounds of oxygen therapy.
6x Food Poisoning.
Evaluated for hearing loss. Result: minimal.
Evaluated for visual acuity. Result: 20/20.
Family History
███████ [REDACTED] ███████
Note: Family medical history shows a tendency for heart disease, strokes/blood clots, and high blood pressure/cholesterol. Continue to monitor.
Social History
Smoking? Not anymore. Quit 10 years ago.
Drinking? Yes, socially. Never binging.
Physically Active? Yes. Swims 2+ hrs, 5 times a week. Boxing, 3 times a week. Cardio, everyday.
Sexually Active? Yes. Clear of STDs and STIs.
Psychological Treatment? No.
Religion? Christian. Non-Practicing.
Associations? N/A.
Medication List + Indications
Lidocaine – Issued for 3rd degree burns, 5 years ago, discontinued use.
Allergies
N/A
Notes
N/A
9 notes
·
View notes
Text

Attorney Lonna Romaine Hooks (1959) is an attorney and the first Black secretary of state for New Jersey. She was born and raised in Nashville. Her father was head of the art department at Fisk University, and the Hooks family lived on campus. While attending her local high school in Nashville, she took a public affairs course and worked at a local TV station, writing about “hot topics.”
She attended Howard University, earning her BA and her JD from Howard University School of Law. She first worked as a clerk for the District of Columbia Court of Appeals, before becoming a lawyer for Schering-Plough, a pharmaceutical company located in Kenilworth, New Jersey. She was in a car accident that left her with extensive injuries that required months of physical therapy. After that, she relocated to Montclair, New Jersey, and started a home-based private practice law firm.
She was president of the New Jersey State Board of Public Utilities when she met Hooks and hired her as her legal assistant. She worked as chief of staff during Whitman’s run for governor of New Jersey and was chosen as the 19th Secretary of State in 1993, the first African American to hold the position. As secretary of state, she, a Republican, was in charge of the New Jersey Historical Commission, the Martin Luther King Jr. Commission, the New Jersey Division of Elections, and the New Jersey State Museum. She served as Whitman’s business ombudsman and remained in the position until her resignation in 1998. She worked at Bloomfield College as the executive director of their new Global Leadership Institute, and next as executive director of the American Public Welfare Association. #africanhistory365 #africanexcellence
3 notes
·
View notes
Text


By: Leor Sapir
Published: Apr 4, 2024
Across the United States, thousands of parents have consented to having their children’s puberty stopped with a class of drugs called gonadotropin-releasing hormone agonists. Known colloquially as “puberty blockers,” these drugs overstimulate the pituitary gland to the point of preventing it from sending signals to the ovaries or testes to start producing the hormones responsible for puberty.
Parents who have consented to these drugs for their children love their kids dearly, but they’ve consented under entirely false pretenses. The doctors who’ve advised them say that puberty blockers are known to improve mental health — that they are even life-saving — and that they are fully reversible and just give kids “time to think.” None of this is true.
Major American medical associations say that “gender-affirming care” for kids is “medically necessary” and “life-saving.” Health authorities Finland, Sweden, Norway, Denmark and the U.K. disagree. Last month, the National Health Service of England decommissioned puberty blockers as a treatment of adolescent gender dysphoria. “We have concluded that there is not enough evidence to support the safety or clinical effectiveness of [puberty blockers] to make the treatment routinely available at this time,” the NHSE explained.
Imagine if American doctors told parents the following truths. The mental health benefits of puberty blockers are highly uncertain, according to multiple systematic reviews of the evidence, the bedrock of evidence-based medicine. The World Health Organization says the evidence is “limited and variable.” There is no research into long-term harms, but some evidence suggests decreased IQ and brittle bones. Permanent sterility is guaranteed for minors who go through full hormonal “transition.” Sexual dysfunction appears to be extremely common as well. Over 93 percent of kids who take these drugs go on to cross-sex hormones, which lead to permanent physical changes including excruciating genital growth, vaginal atrophy and tearing and much higher risk for cancer and cardiovascular disease.
There is no credible evidence that puberty blockers function as suicide-prevention measures. Finland’s top gender clinician has called the suicide narrative “purposeful disinformation” and “dangerous.” For all these reasons, health authorities in a growing number of countries, including some of the most LGBT-friendly, are now prioritizing talk therapy.
How many parents would consent to puberty blockers under these circumstances? Very few, if any.
It is common for drugs to enter pediatric use after evidence of their success in adult medicine. The opposite happened in gender medicine. It was the failure of “sex reassignment” in adult men to achieve satisfactory cosmetic outcomes and improve life functioning that led a group of clinicians in the Netherlands to propose starting the “reassignment” process in childhood.
Their hypothesis was as technologically appealing as it was ethically dubious: since males could not reverse the effects of testosterone-fueled puberty to pass as women, it would be beneficial to these men to have their puberty bypassed altogether.
The Dutch recognized the dilemma but thought they found a way around it. Relying on their experience using puberty blockers to treat a condition known as central precocious puberty (CPP), they argued that blockers were fully reversible and thus part of the diagnostic process. If it turned out that the kid wasn’t “truly trans,” the drugs would be discontinued and puberty allowed to resume.
Their argument was dubious from the get-go. First, CPP has an objective diagnosis, based on a blood sample, whereas gender transition is based on the adolescent’s feelings and experiences, which are subject to change. In a political climate such as ours, in which mere exploration of the reasons for rejecting one’s body can be labeled “conversion therapy,” differential diagnosis becomes impossible.
As Dr. Jason Rafferty, author of the American Academy of Pediatrics’ current policy statement on “gender-affirming care,” has put it, “the child’s sense of reality and feeling of who they are is the navigational beacon to sort of orient treatment around.” The AAP statement has been witheringly critiqued, and Rafferty and the AAP are now defendants in lawsuits by former patients.
Second, in CPP puberty suppression is by definition temporary; the goal is to delay puberty to its appropriate developmental window. In gender dysphoria, a “successful” prescription is where puberty is bypassed altogether. The assumption about reversibility, never tested and highly questionable form the start, proved to be the ethical foundation for the entire Dutch experiment, and it quickly crumbled. Over 93 percent of adolescents who are put on puberty blockers for gender issues continue down the medical pathway to cross-sex hormones. Some go on to surgeries.
Gender clinicians do not see this suspiciously high figure as a reason to rethink their approach. They see no possibility of iatrogenesis — a medical intervention that unintentionally induces harm, in this case by causing gender distress or confusion to persist artificially. On the contrary, they regard the high persistence rate as proof of their own remarkable diagnostic abilities.
More modest and scientifically-minded clinicians and researchers see things very differently. “Blocking puberty,” writes Sallie Baxendale, a professor of neuropsychology and author of an important new study on puberty blockers, “prevents the critical rewiring in the brain that underpins the ability make complex decisions. Puberty blockers may give children time to think but they simultaneously rob them of their developing capacity to do so.”
What is likely happening is that an ongoing youth mental health crisis whose origins predate and have little to do with gender is being misdiagnosed and mistreated with harmful and experimental drugs. Puberty blockers are the definition of a “quick fix” solution.
Researchers incorrectly refer to what the Dutch did as an experiment. In an experiment, falsifiable hypotheses are proposed, alternative interventions are tested, outcomes are monitored and competing explanations for observed results are thoughtfully ruled out.
The Dutch did nothing of the sort, according to a comprehensive scholarly examination of their study. Further, the only attempt to replicate that study, which was done in the U.K., failed. The researchers had to be forced to disclose their disappointing findings. Any scientific-minded person willing to put in the effort and read the literature will come to the same conclusion: Pediatric gender medicine is an industry built on fraud.
During the 2000s and 2010s, the Dutch pseudo-experiment with puberty blockers “escaped the lab” and became entangled in a fast-growing international social movement for transgender recognition. In the U.S., the drugs are being prescribed at numbers far exceeding anything the Dutch could possibly have imagined. Most adolescents referred to pediatric gender clinics are teen girls who have no history of dysphoria in childhood but who do have other mental health challenges that predate their distress with their bodies.
American medicine is no stranger to scandal — lobotomy, “recovered memory” and OxyContin are just a few examples. What makes pediatric gender transition unique is that it has been framed as a nonnegotiable civil right and defended by powerful civil rights groups, the Democratic Party and their ideological allies in the mainstream media.
A key reason for the divergence between U.S. and European medical authorities, as I’ve explained in a previous essay, is the latter’s greater willingness to follow principles of evidence-based medicine, including reliance on systematic reviews. Jack Turban, a prominent American gender clinician, revealed in a deposition that he seems not to know what a systematic review of evidence is.
Another reason is that in the U.S., doctors who practice child “transition” demand and often receive deference as the experts on the evidence for their practices; abroad, such clinicians are seen as having conflicts of interest. When the National Health Service of England appointed the highly respected Dr. Hilary Cass to lead its review of its youth gender service, it did so precisely because she was “a senior clinician with no prior involvement or fixed views in this area.” Sweden and Finland delegated the evaluation of evidence to experts with no personal involvement or stake in pediatric gender medicine.
Parents should never have been put in the position of having to decide whether to “allow” their kids to go through puberty. Those who would put the onus on parents are letting charlatans in the medical profession off the hook. Puberty is difficult for all teens, and it is not a disease. Puberty blockers offer teens in distress — especially girls with history of sexual abuse, autistic kids and gay kids — false hope by casting puberty as optional.
Puberty is a rite of passage from childhood into adulthood, responsible for the development of the body’s major organs and systems and not just its external sexual features. Puberty blockers rob children of their right to an open future.
#Leor Sapir#puberty blockers#medical malpractice#medical scandal#puberty#gender pseudoscience#medical experimentation#gender lobotomy#gender thalidomide#medical corruption#religion is a mental illness
24 notes
·
View notes
Text
We have seen that in the West, the European witchcraze signaled the arrival of a new age of gynocidal processions. During that era the personifications of the Second Divine Person—the sons of god representing the Son of God— appeared on stage, forming the professional and corporate mystical mergers that required the massacre of "indigestible" women. In nineteenth-and twentieth-century America (and in other nations following American leadership) a further phase has been reached. This is the Age of the Holy Ghost and his ghostly representatives. The multiple holy ghosts of the Age of Gynecology (body-gynecologists and mind-gynecologists) follow the mythic model of the "Third Divine Person." We have seen in the First Passage that the original christian holy ghost was a mythic male mother, the spirtual single parent who impregnated Mary, the Totaled Woman. The latter was a reversal of the parthenogenetic goddess, who was thus reduced to a brainwashed receptacle/ rape victim.
In studying the sado-rituals of the gynecological holy ghosts, it is useful to recall some of the theological lore associated with their christian theological archetype. The holy ghost, the feminine member of the divine trinity, was known as "the Spirit"— the one who inspires, or breathes into the souls of the chosen. In the ideal transsexual world of christian myth, "he" manages not only to impregnate Mary physically, producing the "Incarnate Word," but also to fecundate the souls/ minds of the faithful, engendering "supernatural life" and inspiring them with "divine" ideas and images. It is important to realize the interconnection between these two aspects of the myth, for they are reflected in the emergence of the two classes of specialists "devoted" to women, that is, the body-gynecologists and the mind-gynecologists.
The various types of psychotherapists are the theologians of gynecology. These theologians and the specialized "ministering" physicians whom they legitimate represent the two complementary functions of the holy ghost. Both function to keep women supine, objectified, and degraded a condition ritually symbolized by the gynecologists stirrups and the psychiatrist’s couch. By their combined efforts, these specialists keep many women in the state of perpetual patients whose bodies and minds are constantly invaded by foreign objects—knives, needles, speculums, carcinogenic hormone injections and pills, sickening self-images, festering fixations, debilitating dogmas.*
It is significant that certain male-defined feminine qualities are attributed to the holy ghost of christian theology. Thus he is called Helper and Healer—which makes him an appropriate paradigm for the "helping professions." He is also known by the name Gift. The deceptiveness of such appellations is apparent to victims of theological/psychiatric/ gynecological "help," who have learned the truth of the slogan: There is no such thing as a free lunch.
* As we have seen, it is no coincidence that the establishment of gynecology was followed chronologically by the creation and spread of Freudian ideology and its offspring. The medical establishment soon found that its colonization of women's bodies required the concomitant conquest of their minds/spirits. The new theology of therapy has fulfilled this role, extending its tentacles into the privacy of minds and hearts.
-Mary Daly, Gyn/Ecology
#mary daly#female oppression#western civilization#patriarchal religion#therapy is a scam to keep women docile
7 notes
·
View notes
Text
Dogs Help Improve Mental and Emotional Health

Dogs are man’s best friend. They make excellent pets and benefit humans' mental and emotional health.
Several studies have linked having dogs as pets with reduced symptoms of depression, increased comfort, and a higher sense of self-confidence. Some believe that petting them helps uplift a person's mood. In addition, spending time with pets can alleviate loneliness, stress, and anxiety, giving people hope and purpose.
Spending time with dogs has therapeutic effects for several reasons. It triggers the release of feel-good hormones such as serotonin and oxytocin. When a person arrives home from work and their dog runs to them, wagging their tail, the happiness they feel stems from oxytocin. The hormone regulates stress and anxiety while increasing relaxation.
Next, dogs help individuals manage their autonomic nervous system (ANS). The ANS is the network of nerves coordinating unconscious body systems, like breathing and digesting food. It helps activate fight-of-flight processes when individuals sense danger and de-activate them when they feel relaxed.
Emotional dysregulation, or the inability to control emotions, causes an imbalance in ANS. Hence, some events will make a person panic or feel overwhelmed. They may also cause deep sadness or anger. However, individuals with balanced ANS have greater control of their emotional states.
Moreover, dogs offer a calming, nonjudgmental presence for owners. Some dogs can sense mood shifts in the owners and respond by nudging or moving close to them. This unconditional love promotes acceptance and safety, moving people from heightened ANS activity to a more balanced state with better emotional regulation. Therefore, some psychotherapists recommend therapy dogs for people who experience post-traumatic stress disorder. The dogs make them feel safe and secure, reducing symptoms of PTSD.
Individuals interested in engaging dogs to improve their mental and emotional states can follow a few steps. Start with physical contact, such as petting, holding, or hugging a dog to improve mood. Letting a dog snuggle on a person's lap is enough physical contact.
Active individuals benefit from playing with dogs. Running and walking together or playing fetch in the yard helps reduce stress and anxiety. Since each activity is also a form of exercise, individuals and dogs reap more benefits, such as lowering their heart rate, blood pressure, and cholesterol levels. The American Heart Association lists having dogs as a way to reduce the likelihood of developing cardiovascular disease.
Next, going outside with dogs has social benefits. Dogs help start conversations with others. Dog owners who see each other while walking their canines, even though they do not know each other, will likely chat about their pets. A study of 800 people over 50 found that those who walked their dogs four times a week had more social interactions than those who did not own dogs.
Another study showed that people in wheelchairs who walked their dogs regularly received more smiles and had friendlier conversations with neighbors than those who did not. Such social interactions make people feel more connected with their communities, limiting loneliness.
Lastly, away from playful interactions with dogs, their presence boosts mental well-being. In addition, dogs require consistent care, such as regular feedings and cleaning. These daily tasks create structure in a person’s life, giving them a sense of purpose. Further, because dogs depend on them for survival, they develop a higher sense of self-worth, which increases their self-esteem.
2 notes
·
View notes