#sub-clavicular
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The “We are the 99%” Tumblr blog became the slogan for the Occupy Wall Street movement.
Text
Sub-Clavicular Hibernoma: A Rare Diagnosis of Lipomatous Tumor by Zaïd Boughaleb in Journal of Clinical and Medical Images, Case Reports

Abstract
Lipomatous tumors are the most common soft tissue tumors, including a large variety of benign and malignant lesions. Hibernoma is a benign lipomatous tumor originating from the brown adipose tissue inherited from the fetus. The diagnosis is often incidental, since the large majority are asymptomatic or very slow growing. Differential diagnosis with other lipomatous tumors is often challenging. Hence the diagnostic work-up is large and must be multidisciplinary. Biopsy and large resection with sane margins are the standard of care. We describe a 48-year-old male patient with a history of a painless, mobile, slow growing right sub-clavicular mass apparently evolving for eleven years. This patient underwent ultrasound, mammography, MRI, CT Scan and ultrasound guided large core biopsy at different points in time. We describe this case of a well-documented hibernoma of the sub-clavicular region in line with the current literature.
Keywords: CT scan; hibernoma; lipomatous tumor; MRI; ultrasound.
Introduction
Lipomatous tumors including a large variety of benign and malignant lesions are the most common soft tissue tumors, their prevalence increasing with age [1]. Sometimes, overlapping imaging features can be misleading in diagnosis [2]. Since the distinction between benign and malignant lipomatous tumor is challenging, especially when based on clinical and superficial work-up, the differential diagnosis of lipomatous tumors includes hibernoma [3]. Hibernoma is a rare, heterogeneous, slow growing fatty tumor of good prognosis [1], arising from brown fat precursors, representing approximatively 1% of all tumors derived from lipomatous tissues [1]. Usually, no symptoms are associated except when the enlarging mass impinges on local tissues4. To date a few thousand cases worldwide have been described [1].
Case Presentation
A 48-year-old male patient was referred to our mammography unit with a history of a painless, mobile, slow growing right sub-clavicular mass apparently evolving for eleven years. No skin redness, fever or signs of nerve or vascular compression were related. Previous ultrasound examinations reported a fatty mass with a diagnosis of lipoma (well-differentiated fatty tumor without suspicious radiological signs of malignancy [3]). Mammography showed a radiolucent mass consistent with a lipomatous origin on a targeted modified medio-lateral oblique view [5]. Ultrasound revealed a hyperechoic, homogeneous mass compared to the subcutaneous fatty tissue, measuring 11,5 x 3,6 x 10 cm, with vascular hyperemia on color-doppler ultrasound (Figure 1). MRI examination was performed to assess the precise extent and possible invasion of the underlying tissues. MRI described a mass measuring 10 x 3,9 x 9 cm with hypersignal on T2 sequence (but slightly lower than the subcutaneous fat signal [3]), hyposignal on T1 sequence compared to muscle structure (but slightly higher than subcutaneous fat signal [3]), very low signal on a fat suppression sequence and moderate enhancement on the post-contrast T1 sequence. No invasion of the adjacent soft tissues, muscles or bones was described (Figure 2). A CT scan without contrast media injection recently performed for other reasons showed a pre-pectoral low attenuation mass without involvement of the underlying tissues. In our case, density of the lesion was slightly higher than subcutaneous fat [5]. Eventually, diagnostic large core needle biopsies under ultrasound control were performed yielding the histological diagnosis of adipocytes with a microvacuolar and eosinophilic cytoplasm without signs of mitosis or necrosis. The diagnosis of hibernoma was raised. For aesthetic reasons, this patient was referred to our oncologic plastic surgeon; preoperative laboratory testing reported no evidence of metabolic disorder or infectious component [6]. Surgery showed a mass alongside the pectoral fascia, without muscle or vessel invasion. Histology confirmed the diagnosis of hibernoma.
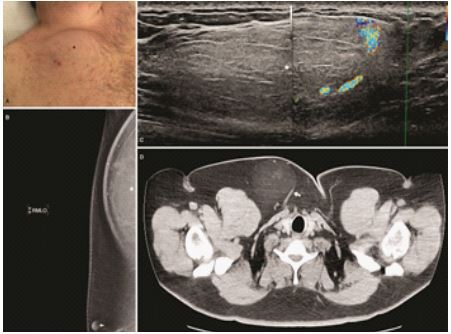
Figure 1: (A) Subclavicular swelling due to the clinical mass (black star). (B) Mediolateral modified oblique mammographic view showing a radiolucent mass (white star), nipple (with arrow). (C) Ultrasound: hyperechoic mass with peripheral vessels on color ultrasound (white star). (D) Axial non-enhanced CT scan showing the mass (white arrow).

Figure 2: (A) T2-weighted axial MRI image revealing a slightly hypointense mass compared to subcutaneous fatty tissue (black star). (B) Axial T1-weighted non-enhanced MRI image with fat suppression: hibernoma undistinguishable from adjacent fatty tissue. (C) Gross macroscopic specimen showing a lipomatous mass. (D) Axial T1-weighted MRI image with fat-suppression post Gadolinium injection demonstrating a slight enhancement of the mass (white arrow).
Discussion
Huge progress has been made since the descriptions by Merkel in 1906 and Gery in 1914 [7, 8]. Brown fat is a particular form of fat found in the hibernating and non-hibernating animals [9]. Representing approximatively 1,6% of all benign lipomatous tumors, hibernomas are very slow growing tumors usually occurring between the age of 20 and 50 years [11, 12]. Average age at diagnosis is 38 years and various gender predominance have been described in the literature. Intraosseous hibernomas are found in older patient [13]. The most common location, as the majority of fat tumors, are neck, shoulder and periscapular regions which are areas with possible remaining brown fat tissue [14]. However, hibernomas can occur anywhere in the body [15]. The clinical manifestations are rare, but might occur as a painless soft tissue mass, with a locoregional irritation or neurovascular compression [16]. Conventional radiography demonstrates a radiolucent mass with no adjacent osseous abnormalities or mineralization [17]. Ultrasound describes a rather uniformly hyperechoic mass [5], with increased vascular flow [17] generally unspecific, like other soft tissue tumors. In our case, the diagnosis of a typical lipoma [5] was ruled out due to vascular hyperemia on color doppler ultrasound. On CT scan, hibernoma presents as a homogenous low-density mass of lipidic composition between the attenuation of subcutaneous fat and skeletal muscle [5]. Contrast enhanced CT scan usually shows variable degree of enhancement [16] and intra-tumoral septas [10]. Diagnosis of hibernoma cannot be excluded based on the lack of intra-tumoral vessels [10]. On MRI, the imaging modality of choice [3], hibernoma shows an hypoT1 and hyperT2 signal because of the fatty component alike our case but differs slightly from the fat signal. On a fat-suppressed sequence, attenuation is similar to fatty tissue. After Gadolinium contrast media injection, enhancement is variable but predominantly present and rather heterogeneous [5]; a common sign are large flow voids indicating fast flowing flood in intratumoral vessels. Internal septation, one of the features of hibernoma [3], was absent in our case. High level of FDG uptake has been described in brown adipose tissue [16], sometimes even higher than liposarcoma [10] but overlapping results [2] prevent clear distinction between both tumors. Four types of hibernomas have been described, based on a histological classification [15]: the typical variant, the most common one like our case, the “myxoid” variant, the “lipoma-like” variant and the “spindle-cell” variant. Differences in imaging characteristics among these different histological subtypes of hibernomas are due to the variable amounts of water and fat content. One study distinguished between “lipoma-like” and “non lipoma-like” hibernoma [18]. Non-lipomatous hibernomas are probably indistinguishable from other liposarcomas [17]. Differential diagnosis of hibernoma is very large and may include benign tumors (lipoma, angiolipoma, hemangioma, hemangiopericytoma, hemangioblastoma, xanthoma, granular cell tumor, adult rhabdomyoma, lipoblastoma…) [16, 19] and malignant tumors (liposarcoma, clear cell sarcoma,…) 5, 10, 16. Clinical and imaging features as previously described may guide the diagnosis, but the histological examination gives the final diagnostic. In the absence of treatment, hibernoma continues to grow and leads to functional or cosmetic consequences 2. Tumor regrowth has been reported with incomplete excision of hibernoma 19. The standard of care of hibernoma is surgical removal with clear margins. Surgical excision is advised to rule out a possible malignant lesion with hibernoma-like differentiation which could be missed by core needle biopsy 1. No risk factor has been described [1]. Multiple lesions in a single patient are possible 21. After resection, the tumor generally does not recur. Since no malignant transformation or metastatic (22) spread have been described in the current literature, hibernoma can be considered as a benign tumor 1 for patients is 20.
In conclusion, the diagnosis of fatty tumors, often challenging especially with rare tumors like hibernomas, should comprise ultrasound, MRI and large core needle biopsies. Since hibernomas are benign tumors with no tendency to recur or metastasize, surgical resection with clear margins is recommended 17.
Declarations
Funding
This work did not benefit from any financial support
Conflict of interest
All authors declare no conflict of interest.
Ethical approval statement
The study has been approved by the Ethical Committee of the institution (76/2021).
Patient consent statement
A written permission to publish has been obtained from the patient.
For more details : https://jcmimagescasereports.org/author-guidelines/
#CT scan#hibernoma#lipomatous tumor#MRI#ultrasound#asymptomatic#sub-clavicular#hyposignal#Subclavicular#mammographic#Zaïd Boughaleb#JCMICR
0 notes
Note
dom erik fics? strangely every time i try read a dom erik he is a sub because of some kind of plot twist
Here are some excellent dom!Erik fics, Anon; hope you enjoy!!!
What You've Really Been Chasing by helens78
Charles has been chasing after something for years, but he's never found it. Erik steps in to show him what he's been missing.
Put me in the backseat, and they took me for a ride by tahariel (series)
When Erik enters the bedroom, pausing on the threshold just to look, near shivering with excitement, his new sub is waiting for him, laid out on top of the bedclothes like a present. He’s draped with a length of rich black silk, which clings to his naked body and hides nothing, accentuates everything.
Erik’s mouth runs dry.
Counting the Beat by clavicular
Written for this prompt on 1stclass_kink: Erik uses a metal sex toy (dildo, butt plug, nipple clamps, handcuffs, or maybe he just molds something) on Charles with his powers so he can watch from afar while fucking Charles senseless. Belts, buttons, and zippers are metal too, so I imagine Erik just sitting back in a chair smugly while he uses the metal on Charles' clothes/body to force Charles around and take his clothes off and such. Maybe there's a bit of power play going on where Charles tries to get in Erik's head and make him squirm and Erik disciplines him for it...
Twenty-One Guns by luninosity (series)
Sometimes Charles needs to not be in control for a while. Erik offers to help. First times, some confessions, porn with plot…
Alive With Open Eyes by Cesare, helens78
"I'd rather stay, though," Charles smirked, all too pleased with himself, "if you'll have me."
"No," Erik told him flatly. "Not like this. If you start this, you take it seriously. You're mine until I'm through with you."
Purple is for Emperors by Fullmetalcarer
Erik sat on the edge of the bed, slowly stroking his cock.
Charles knelt on the floor in front of him, naked and bound with purple cords.
Can Erik and Charles find happiness in a world where they don't fit in?
Finding North by ClarkeStetler, Goosenik (series)
Charles and Erik are (loosely) friends with benefits. They don't share personal details, last names, or anything concrete about their lives. This is ruined rather spectacularly when Charles gets recruited by the Mutant Apprehension Division of the FBI. Surprised is a bit of an understatement for their reaction to finding themselves partnered up and sent out on cases with the team.
Bit of a detective fic? Really just an excuse for us to play around with MAD (Mutant Apprehension Division) that we created in Playing House.
you burn me by warraw
Erik didn’t allow him a blanket or any other cover, so he is curled up on his side, hugging himself. From where Erik is standing he cannot see the sweet curve of his ass, just his front. But it is enough to enjoy the view.
Gifts by spuffyduds
Erik is generous. Charles is distracted.
No more fear by adern (series)
Erik was a Dominant himself, but he wouldn't ever threatened a submissive of punishement just because they had put the cutlery in the wrong order.
put me down by ninemoons42
Charles is normally happy to follow Erik's orders in and out of bed, but it's been a very bad day, and he's been caught entirely off guard by what he overhears.
Into His Arms by a_q
Written for the meme prompt: A human dominant over a mutant sub is almost unheard of. No one expected a human Erik Lehnsherr to be the dom of a Omega-level telepath. Erik is convinced it's a mistake, Charles is convinced it's perfect.
Moira tries to support her husbands new found connection, and Raven tries to protect Charles and keep him from giving too much of himself.
Open You Up by Magnetism_bind
I want smutty sex against the wall, on the table, wherever exciting, and I want submissive!Charles. And maybe some filthy oral sex...
59 notes
·
View notes
Photo

TENS Elastic Nail - Length 40cm are intended for Diaphyseal and certain Metaphyseal fractures of long bones, Sub capital Humerus, Metatarsal, and Metacarpal fractures, and complex Clavicular fractures in ...
https://www.orthopaedic-implants.com/nails-wires-pins/nails/tens-nail.php#tens-nails
6 notes
·
View notes
Text
Supta Kurmasana Goes Pop!
Some time ago I intimidated to compose a post regarding discomfort showing up in the joint that attaches the collarbone to the breastbone. I have had a couple of more current demands to discuss this prospective issue in supta kurmasana. As always I attempt to check out the composition, its function, observations about the yoga stance itself as well as maybe some manner ins which info might notify the means we operate in the posture or change it.
I'm gon na obtain technical on ya for half a second if for no various other factor than to educate you my algebraic (not actually) equation for generating the trade name of any type of joint in the body.
The equation is bone + O + bone = Joint Name
The breastbone is practically called the sternum, the collarbone the clavicle. Include them with each other, make a number of modifications to the endings of every one, and also you have the stern-o-clavicular joint. And it's the sternoclavicular joint that can go "pop" while doing a supta kurmasana.
The ask for details about reasons for discomfort in supta kurmasana, since late, have regrettably appeared of injury throughout modifications in this pose. Injury to this joint does not only come during an adjustment. We can easily do it to ourselves if we're not careful, and to be reasonable, even if we are being careful.
It appears odd to discuss bewaring when speaking regarding placing our legs behind our head and afterwards binding our arms behind our back while face down. It can periodically leave one to ask yourself why on planet we would ever before do something to ourselves? I believe that inquiry could be better left for a different article some day in the future.

Joint Structure and Movements
The joint itself is fairly special. OK ... I'm gon na get anatomical on ya once more. Joints are identified by their form and/or function. Some joints live beyond the typical classifications that have been developed. This is among them. This joint is usually identified as a saddle joint, picture 2 steed saddles, turn one inverted, turn it ninety levels as well as the curves onward as well as back satisfy up with one an additional as if the saddles relocate along each other in 2 directions.

The sternoclavicular joint is shaped virtually exactly similar to this except its contours are not fairly so deep as a steed saddle. In the instance of this joint, it moves ahead and also back in what we call protraction and also retraction. It goes up and down in what we call elevation as well as anxiety. This fits well with the design of a saddle joint.
However, there is one added function that lies outside the typical saddle form. This joint additionally has the capacity to revolve. It remains in this feature that the injury in supta kurmasana probably occurs.
It's not that this is the only place that we use the rotation at this joint. The majority of bindings behind our back such as marichyasana A, B, C, D, and prasarita padottanasana C with hands intertwined behind the back are various other instances. What happens right here in supta kurmasana is that we need to blend the turning of the clavicle with retraction. Retraction is when the side or outer end of the clavicle is relocating back in area. In this case, it happens by merit of us reaching our arms behind our back. Blending the two together raises the quantity of pressure in the joint.
In a supta kurmasana you occur to be doing this mix of activities while walking around your thighs. Because of this "obstacle" being in the way it forces us to get to better, and also develop even more basic tension through the sternoclavicular joint when we bind.
All of this makes adjustments a little bit perilous depending on the student and also their private aspects. Do they have brief arms? Tight shoulders? Wider thighs? Wider torso? There could be a variety of extra variables that might be seen as possible limitations in the binding element of a posture such as this. I talk extra regarding what is required from the body to move safely in and out of supta kurmasana on pages 258-260 (1st ed.) of my book Functional Anatomy of Yoga.
I would suggest that we consider our capacity or at our pupils' capability to bind in postures such as parsvottanasana, prasarita padottanasana C (2nd most typical place for injury at this joint with hands dealing with out behind the back), and the marichyasanas.
Adjusting the Pose
I don't wish to obtain unfathomable into exactly how one must change this yoga stance. The instructor needs to fit the modification to the pupil obviously. Not to mention I'm not going to tackle just how to change the legs below. All of it with each other is a whole other write-up as well as perhaps even a book!
It prevails to bind the arms initially in this pose and afterwards put the legs behind the head. In lots of positions the binding comes before the rest of the position takes place totally, for instance, in those marichyasanas I mentioned earlier. We would normally bind our arms first and afterwards fold onward or spin fully.
This stance might be an exemption to that guideline. Thinking that some of you out there put yourself right into a full raja supta kurmasana where your legs are totally behind your head. Do you do this with your hands bound first? No, you do not. You sit up, put your legs behind your head and after that lower yourself to the flooring utilizing those hands as well as arms as well as then after your forehead is on the flooring, you bind your arms.
I'm uncertain why this very same order of procedures should not apply to placing somebody else into the pose if you're assisting them. I understand for me personally, if I bind my hands initially and also then a person tries to place my legs behind my head, it isn't mosting likely to take place easily for them or for me. It isn't going to be very comfortable for me either.
Other individuals are different. Someone with thinner legs as well as longer arms could not have a trouble in either case they are adjusted. Think of it, does binding the legs to the side of the body allow those legs to relocate a lot more quickly or less easily?
Trying to change somebody's legs after binding their arms may also make them tighten up. Why? Because they're trying to hold onto the binding in between their fingers or hands. This is a place where that pop can happen.
The other place where the joint has a tendency to obtain wounded in this stance is when the arms are being readjusted much more deeply behind the back. Commonly the arm joints are squeezed with each other from behind. If it's you attempting to bind your very own shoulder, or you trying to change an arm deeper, don't forget to help the shoulder obtain better forward.
The shoulder ought to move down toward the flooring prior to the arm tries to reach back and rotate. Relocate down toward the flooring first tends to minimize pressure at the sternoclavicular joint as well as make more room for the rotation to happen around the leg if it's currently behind the head.
What To Do If You Have An Injury Here?
The more than likely culprit in an injury here is a ripped ligament (there are always various other possibilities). Prior to you flip out over the word tear, let's specify what that indicates to a ligament. Tear implies that the fibers in the tendon have actually been extended past a point where they can return to their original shape/position. It's like your old slinky. As soon as you stretched it out, as we all did at some point in its life, it never went back with each other similarly. There would be a little larger spaces in between the coils than when it was new.

A better method to describe it is to state it was over-stretched. What do we do about this? Ice it. Lower swelling, and swelling if there occurs to be any type of and maintain relocating the joint around. Remember that mark cells is going to begin creating whenever there is an injury to soft cells in the body. If you not do anything, it obtains tighter and also even more restricted.
If you wish to find out a process for collaborating with injuries you need to absolutely check out the on the internet injury workshop. It teaches you a process of just how to examine, customize, and also collaborate with injuries.
Don' t always move the joint around to the level that tore it, but keep relocate. Just maintain in mind that at a joint such as this, you may swiftly recognize just how interrelated things remain in your body. Your clavicle relocates with each breath you take. Muscle mass that connect to it likewise attach to your head and neck. It's feasible that wounding the sternoclavicular joint may trigger a variety of settlements to take place around your neck.
The sternocleidomastoid connects very near to the sternoclavicular joint and afterwards just behind the ear on the head. Your trapezius muscle mass is connected to completion of your clavicle and also scapula (which both move together). It's other end affixes to the rear of your head and also neck. The subclavius muscle mass that rest under (sub) the clavicle (clavius) also affix to the clavicle. All of these muscles apply their forces on the clavicle itself and the joint. If they are in balance, after that the clavicle remains in equilibrium. If some of them tighten in action to injury, which can take place, after that the balance is shaken off. If the balance is off, the effects can be neck as well as shoulder discomfort as an outcome of the preliminary injury to the joint. It can be a lot more extensive than we could initially think.
1 note
·
View note
Text
Rec: The most inclusive form of redemption (this side of black holes)

the most inclusive form of redemption (this side of black holes) (30003 words) by clavicular Rating: Explicit Warnings: Underage Relationships: Derek Hale/Scott McCall Characters: Scott McCall, Derek Hale Additional Tags: Alternate Canon, Season 3a, BDSM, Kink Negotiation, discussions of consent, Dom!Scott, sub!derek, Trust Issues, POV Scott McCall Summary: After all the tension and lies between them, Scott and Derek struggle to trust each other. They have no reason to even try letting the other in. Even so, they find themselves drawn to each other - find themselves fitting together in new and uncertain ways. Maybe it's what they both need, but neither of them knows how to deal with it.
Or: The one where Scott and Derek work out their problems with kinky sex.
5 notes
·
View notes
Text
300+ TOP ORTHOPAEDICS Objective Questions and Answers
ORTHOPAEDICS Multiple Choice Questions :-
1.Which is not a principle of compound fracture treatment? a) No tendon repair b) Aggressive Antibiotic cover c) Wound debridement d) Immediate Wound closure Ans:d 2.Medial meniscus is more vulnerable to injury because of? a) Its fixity to tibial collateral ligament b) its semicircular shape c) action of adductor magnus d) its attachment to fibrous capsule Ans:a 3.Injury to the popliteal artery in fracture lower end of femur is often due to? a) Distal fragment pressing the artery b) Proximal fragment pressing the artery c) Tight plaster d) Hematoma Ans:a 4.In transverse fracture of the patella, the treatment is a) Excision of small fragment b) Wire fixation c) Plaster cylinder d) Patellectomy Ans:b 5.monster type of dislocation of the hip is a) Anterior b) Posterior c) Central d) Dislocation with fracture of the shaft Ans:b 6. March fracture affects a) Neck of 2nd metatarsal c) Neck of 1 st metatarsal b) Body of 2nd Metatarsal c) Neck of 1 st metatarsal d) Fracture of lower end of tibia Ans:a 7.Commonest complication of extracapsular fracture of neck of femur is a) Non Union b) iscnemic necrosis c) Maiunion d) aTPuTmonary complications Ans:c 9.Blood coagulation profile in pregnancy is a) Increase in fibrinogen level of 10-25 % b) Decrease in factor X, XI, XII c) Decrease in plasminogen activity d) Increase in platelet count Ans:a 10.In classical caesarean section more chances of rupture of uterus is in a) upper uterine segment b) lower uterine segment c) utero cervical junction d) posterior uterine segment. Ans:a

ORTHOPAEDICS MCQs 11.Only indication for Internal version nowadays is a) Brow presentation b) Face presentation c) Second fetus of twins d) Breech Ans:c 12.Internal fixation is done in all fracture Except a) Compound b) Multiple c) Elderly person Ans:a 13.Myositis ossificans is commonly seen at tlie joint d) Hip a) Knee b) Elbow c) Shoulder d) Hip Ans:b 14.The most important factor in fracture healing is a) Good alignment b) Organization of blood clot c) Accurate reduction and 100% apposition of fractured fragments d) Immobilization e) Adequate calcium intake Ans:d 15.The most preferred treatment of fracture of neck of femur in a young person is a) Hemiarthroplasty b) Total hip treatment c) conservative treatment d) closed reduction & internal fixation Ans:d 16.Lisfranc dislocation is a) Tarsometatarsal dislocation b) Lunate dislocation c) Scaphoid dislocation d) Posterior dislocation of elbow Ans:a 17.Position of immobilization in fracture both bones of forearm in an adult male will be a) Prone b) Mid prone c) Supine d) 10° Supine Ans:c 18.Carpal bone which fractures commonly a) Scaphoid b) Lunate C) Hamate d) Pisiform Ans: a 19.True about clavicular fracture is a) Most common at medial 1/3 & 2/3 b) comminuted fracture common c) malunion occurs d) usually due to fall on elbow Ans:c 20.Commonest site of fracture scaphoid a) Waist b) Proximal third c) Distal third d) Tuberculosis Ans:a 21.Excision of fractured fragment is practised in all fractures except a) Patella b) Olecranon c) head of radius d) lateral condyle humerus Ans:b 22.The complication not common in colle's fracture is a) malunion b) non union c) sudeck's atrophy d) stiffness of wrist Ans:b 23.In 65 year old male with history of fracture neck of femur 6 weeks old, treatment of choice a) SP nailing b) Mc Murray's osteotomy c) hemiarthroplasty d) none. Ans:c 24.In Colles fracture not seen in a) Proximal impaction b) lateral rotation c) dorsal angulation d) medial rotation Ans:d 25.In fracture medial epicondyle of humerus,which of the following can be affected a) Flexion of fingers b) Adduction of fingers c) Abduction of fingers d) Flexion of thumb Ans:a 26.Most common cause of pathological fracture in a child is a) malignancy b) bone cyst c) fibrous dysplasia d) paget's disease Ans:b 27.A lady presents with a history of fracture radius, which was put on plaster of paris casts for 4 weeks. After that she developed swelling of hands with shiny skin. What is the most likely diagnosis. a) Rupture of extensor pollicis longus tendon b) Myositis ossificans c) Reflex sympathetic dystrophy d) Malunion. Ans:c 28.AH are components of Rotator cuff except a) Supraspinatus b) Infraspinatus c) Subscapularis d) Teres major Ans:d 29.Complication of fracture scaphoid is a) Injury to radial artery b) avascular necrosis of proximal part c) avascular necrosis of distal part d) injury to radial nerve Ans:b 30.Which fracture neck of femur has a poor prognosis a) Intra capsular b) Extracapsular c) Both d) None. Ans:a 31.Fracture blisters commonly appear on how many days ? a) 1- 3 days b) 3- 5 days c) 5-7 days d) 5-9 days Ans:b 32.If the greater tuberosity of the humerus is lost, which of the following movements will be affected a) Adduction and flexion b) Abduction and lateral rotation c) Medial rotation and adduction d) Flexion and medial rotation Ans:b 33. The most common cause of a sprained ankle is injury of a) Deltoid ligament b) lateral ligament c) Inferior tibiofibular ligament d) Anterior Talofibular ligament. Ans:d 34.In the case of 65 year old person with fracture neck offemur the treatment of choice is a) close reduction b) close reduction with internal fixation c) open reduction d) replacement of head and neck of the femur with a prosthesis Ans:d 35. Tardy ulnar nerve palsy is seen in : a) Cubitus valgus c) Fracture scaphoid b) Dislocation of elbow c) Fracture scaphoid d) Supracondylar fracture of humerus Ans:a 36.Common injury to baby is a) Fracture humerus b) Fracture clavicle c) Fracture radius-ulna d) Fracture femur Ans:b 37.Young man with # tibia of left side 2 months ago, is having popliteal cast, Now needs mobilization with single crutch. Which will be the preferred site ? a) Left sided crutch b) Right sided c) Any side d) Both sides Ans:a 38.Bryant's triangle is useful in diagnosis of following except a) Supratrochanteric shortening b) Infratrochanteric shortening c) anterior dislocation hip d) posterior dislocation hip Ans:b 39.Line joining Ant Sup. iliac spine to tip of gluteal tuberosity, should normally touch the Greater trochanter, this is a) Shoemakers line b) Nelaton's line c) Von-rossen d) Perkins Ans:b 40.Which of the following is least common in supracondylar fracture a) Non union b) Median nerVe injury c) volkmanns ischemic contracture d) cubitus varus Ans:a 41.Earliest symptom of Volkmann's ischemia is a) Pain in flexor muscles b) Absence of pulse c) Pain on passive extension d) Cyanosis of limb Ans:a 42.A patient develops compartment syndrome (swelling, pain and numbness) following manipulation and plaster for fracture of both bones of leg. What is the best treatment? a)Split the plaster b)Infusion of law molecular weight dextran c)Elevate the leg after splitting the plaster d)Do operative decompression of fascial compartment Ans:d 43.Anterior dislocation of shoulder causes all except a) Circumflex artery injury b) Avascular necrosis head of humerus c) Brachial plexus injury d) Chip fracture scapula Ans:d 44.In Colles# following is most common complication a) Non union b) Malunion c) Sudeck's dystrophy d) Volkmann's ischemic contracture Ans:b 45. Patient with supracondylar fracture following reduction presented with claw hand. The likely diagnosis is a) Volkmann's ischaemic contracture b) median nerve injury c) Ulnar nerve injury d) Dupuytrens contracture Ans:a 46.Pivot test for a) anterior cruciate ligament b) posterior cruciate ligament c) medial meniscus injury d) lateral meniscus injury Ans:a 47.Triangular relation of Elbow is maintained in a) Fracture ulna b) Anterior dislocation of Elbow c) Posterior dislocation of Elbow d) Supracondylar fracture Ans:d 48.Fracture which most often requires open reduction & internal fixation a) Lateral condyle of humerus b) Femoral condyle c) Distal tibial epiphyseal separation d) Fracture both bones forearm Ans:a 49. A patient had injury to the upper limb 3 yrs earlier, now he presents with paresthesia over the medial border of the hand and anaesthesia over medial two finger. The injuryis likely to have been a) supracondylar fracture b) lateral condyle fracture humerus c) medial condyle fracture humerus b) lateral condyle fracture humerus Ans:b 50.Commonest type of lesion causing recurrent shoulder dislocation is a) Shallow glenoid labrum b) Bankarts lesion c) Weakness of subscapularis muscie d) Injury to humeral head Ans:b ORTHOPAEDICS Objective Questions with Answers 51.Menisci calcification is a feature of a) Gout b) Hyperparathyroidism c) pseudogout d) ankylosing spondylosis Ans:c 52.A young adult presenting with oblique, displaced fracture olecranon treatment of choice a) Plaster cast b) Percutaneous wiring c) Tension band wiring d) Removal of displaced piece with triceps repair Ans:c 53.Volkmann's ischemic contracture mostly involves a) Flexor digitorum superficialis b) Pronator teres c) Flexor digitorum profundus . d) Flexor carpi radialis longus Ans:c 54.Avascular necrosis is commonest in one of the following fractures a) Gorden 1 & 2 fracture of femoral neck b) Gorden 3 & 4 fracture of femoral neck c) Sub-trochanteric fracture of femoral neck d) Baso-trochanteric fracture Ans:b 55.On measurement, the base of Bryant's triangle on the left side is found to be short by 2 cms as compared to the right side. This indicates a) Fracture of the neck of the femur b) Fracture of the shaft of the femur c) Osteoarthritis of hip joint d) Rheumatoid arthritis of the hip joint Ans:a 56.All the following requires open reduction & internal fixation almost always except a) Lateral condyle of humerus b) Olecranon c) Patella d) Volar Barton's fracture Ans:d 57.Pathognomic sign of traumatic fracture a) Swelling b) Tenderness c) Redness d) Crepitus Ans:d 58. A football player, while playing, twists his knees over the ankle. He still continues to play. a) Medial meniscus tear b) Anterior cruciate ligament tear c) Medial collateral ligament injury d) Posterior cruciate ligament injury. Ans:a 59.K-wire is used in a) Circlage b) fixing forearm bones c) prior to plating d) All of the above. Ans:d 60.Treatment of Acute myositis Ossificans is a) Active mobilization b) Passive mobilization c) Infra Red therapy d) Immobilization Ans:d 61. The treatment of choice for non-union of extracapsular fracture neck femur a) Hip spica b) Intramedullary nailing c) Internal fixation d) Compression plating Ans:c 62.Duga's test is helpful in a) Dislocation of hip b) Scaphoid fracture c) Fracture neck of femur d) Anterior dislocation of shoulder Ans:d 63.Open reduction in children is done for a) Supracondylar fracture b) forearm both bone fracture c) femoral condyle fracture d) lateral condyle of humerus fracture Ans:d 64.Avascular necrosis of the head of femur is not seen in a) Subcapital Fracture b) Intertrochanteric fracture c) Transcervical fracture d) Central dislocation of hip Ans:b 65.Stiffness in knee is maximum when traction is at a) Skin b) lower end femur c) upper end tibia d) calcaneum Ans:b 66. Intramedullary fixation is ideal in a case of fracture of shaft of femur when there is a) A transverse fracture b) A compound fracture c) Soft tissue interposition between the fractured ends d) Such a fracture in a child Ans:a 67.Meyer's operation is done for a) Recurrent dislocation of patella b) Dislocation of shoulder joint c) Dislocation of hip joint d) Scaphoid Ans:b 68.Treatment of choice for old non-united fracture of shaft of femur a) compression plating b) bone grafting c) nailing d) compression plating with bone grafting. Ans:d 69.The last step in the healing of a fracture is a) Hematoma formation b) Consolidation c) Remodelling d) Callus formation e) Demineralization of bones. Ans:c 70.A Bennet's fracture is difficult to maintain in reduced position because of the pull of a) Extensor pollicis longus b) Extensor pollicis brevis c) Abductor pollicis longus d) Abductor pollicis brevis Ans:d 71.Inter trochanteric fracture has trendelenberg sign negative because of the action of a) Gluteus medius b) Gluteus minimus c) G.maximus d) Tensor fascia lata Ans:a 72.A segmental compound fracture tibia with 1cm skin wound is classified as a) Type I b) Type II c) Type ILIA d) TypeIIIB Ans:a 73.Steinman pin is used for all except a) fracture of upper end of tibia b) fracture through lower end of tibia c) fracture through lower end of femur d) skull traction Ans:d 74.Treatment after removal of plaster for supracondylar fracture of humerus is a) active mobilization at elbow joint b) massage c) no treatment d) passive movements at elbow Ans:a 75. Lateral condyle can cause a) Genu valgum b) Genu varus c) Genu recarvatum d) Dislocation of ankle Ans:a 76. Muscles involved in Volkmann's ischemic contracture a) Flexor pollicis longus b) Flexor profundus c) Flexor sublimis d) All Ans:d 77. Medial meniscus tear is more common than lateral meniscus because of its decreased a) Nerve supply b) Vascularity c) Mobility d) Fibroelasticity Ans:c 78.Volkmann's ischaemic contracture is due to a) Arterial injury b) Venous injury c) Nerve injury d) Increase of compartment pressure in the limb Ans:d 79.Attitude of the limb in anterior dislocation of hip a) Flexion, abduction, external rotation b) Flexion, adduction, external rotation c) Flexion, Abduction, internal rotation d) Flexion, adduction, internal rotation Ans:a 80.Treatment of fracture clavicle in an infant is best treated by a) Cuff and sling b) Figure of 8 bandage c) Open reduction d) Shoulder cast Ans:b 81.Dislocation of hip joint palpable on per rectal examination a) Cogenital dislocation of hip b) Posterior dislocation of hip c) Fracture neck of femur d) Anterior dislocation of hip Ans:a 82.Fractures common in elderly women are all except a) Clavicular b) Colles c) Intertrochanteric d) neck of femur Ans:c 83.Late complication of Acetabular fracture a) Avascular necrosis of head of femur b) Avascular necrosis of iliac crest c) Fixed deformity of the hip joint d) secondary osteoarthritis of hip joint Ans:a 84.Treatment of anterior dislocation of shoulder is by a) Kocher's manoeuvre b) Dennis browne splint c) Barlows manoeuvre d) Surgery Ans:a 85.Patient comes with fracture of femur in an acute accident, the first thing to do is a) Secure airway and treat the shock b) Splinting c) Physical examination d) X-Rays Ans:a 86.Multiple bone fractures in a new born is seen in a) Scurvy b) Syphilis c) Osteogenesis imperfecta d) Morquio's syndrome Ans:c 87. Most common bone to fracture in body is a) Radius b) Clavicle c) femur d) vertebra e) Pelvis Ans:b 88.Cock up splint is used in management of a) Ulnar nerve palsy b) brachial plexus palsy c) radial nerve palsy d) combined ulnar & median nerve palsy Ans:c 89.The type of displacement of fractured fragment in which bone is not remodelled a) Anterior angulation b) Posterior angulation c) Lateral angulation d) Rotation Ans:b 90.Carrying angle is decreased in a) Cubitus varus b) Cubitus valgus c) Genu valgum d) Genu varum Ans:a 91. Transverse fracture of medial malleolus is caused by a) Abduction b) Adduction c) Rotation of foot Ans:a 92.Bennet's fracture is fracture dislocation of base of matacarpal a) 4th b) 3rd c) 2nd d) 1st Ans:d 93. Most common type of supracondylar fracture is a) extension type b) flexion type c) abduction type Ans:a 94.Intramedullary nailing is contraindicated in fracture shaft femur if a) The fracture is compound b) The fracture is near the knee joint c) The epiphysis have not fused d) Any of the above is present e) None of the above is present Ans:d 95.A man was diagnosed to have myositis ossificans progressiva at the age of 20 yrs. He died 5 yrs later. What is the most probable cause of death ? a) Starvation and chest infection b) Myocarditis c) Hypercalcemia d) Hyperphosphatemia Ans:a 96. The commonest elbow injury in children is a) Extension type of supracondylar fracture of humerus b) Di slocation of elbow c) Fracture lateral condyle of humerus d) Fracture medial epicondyle of humerus Ans:a 97. Ideal treatment with fracture neck of humerus in a lady will be a) Triangular sling b) Hemiarthroplasty c) Chest arm bandage d) Internal fixation Ans:a 98. In Intertrochanteric #has most common complication of a) Non union b) Malunion c) Avascular necrosis d) Nerve Injury Ans:b 99. Luxatio erecta a) tear of the glenoidal labrum b) inferior dislocation of shoulder c) anterior dislocation of shoulder d) defect in the humeral head Ans:b 100. McMurray's osteotomy operation is based on the following principle a) Mechanical b) Biological c) Bio-mechanical d) None Ans:c ORTHOPAEDICS Questions and Answers pdf Download Read the full article
0 notes
Text
Chemotherapy – All you wanted to know
Chemotherapy, by and large utilized for the treatment for disease, means drugs that keep malignant growth cells from isolating and developing. This is principally accomplished by murdering the objective cells which can possibly duplicate unusually. A wide assortment of medications are utilized to accomplish these goals. The viability of Chemotherapy depends, somewhat, on the phase of disease that is being dealt with.
While there are unfavorable reactions, the advantages of chemotherapy for the most part exceed the danger of any unfriendly impact.
Click Here If you are looking for the best oncologist In India .
What is Chemotherapy?
Chemotherapy is the utilization of medications to pulverize malignant growth cells; these are here and there called cytotoxic medications.
Chemotherapy medicines vary, comprising of only one medication (some of the time) or a wide range of medications that might be regulated over a couple of days or weeks. The treatment will for the most part involve numerous chemotherapy courses, and the routine a patient is given relies upon the kind of malignant growth to be dealt with.

How is chemotherapy given?
Chemotherapy might be given utilizing various courses, contingent upon the kind of malignant growth and treatment got.
Most regularly it is given by infusion into a vein (intravenously). It can likewise be given by mouth (orally), by infusion into a muscle (intramuscularly) or under the skin (subcutaneously).
In a couple of cases, chemotherapy will be infused into the liquid around the spinal string (intrathecally). However the medications are given, they are consumed into the circulatory system and bore the body with the goal that they can achieve the malignancy cells.
If you are looking at the best doctor near by you:
Best Oncologist in Hyderabad | Best Oncologist in Chennai| Best Oncologist in Delhi | Best Oncologist in Bangalore
Intravenous Chemotherapy
Intravenous (IV) chemotherapy can here and there be given by means of a 'dribble' into a vein in your arm. For this situation, a fine cylinder (a cannula) will be embedded into the vein by a specialist or medical attendant. This will be expelled before you return home.
On the off chance that the veins are hard to discover, it might be important for the patient to have a Peripherally Inserted Central Venous Catheter (PICC). This is an exceptionally fine cylinder, which is put into a vein in the criminal of your arm. Once set up, it is verified and can stay in the vein for a long time.
On the other hand, it might be important for certain patients to get chemotherapy by means of a focal line. The line is 'burrowed' with the goal that it keeps running underneath the skin and finishes in one of the huge veins that lead to your heart. Some prevalent locales for position of Central line are ' Pectoral district' adopting the sub-clavicular strategy or 'Neck area' approach for situation in Internal Jugular Vein.
A focal line is embedded while the patient is delicately calmed or under neighborhood anesthesia and can stay set up for a long time all through the treatment.
Click here to find the Doctors near me .
0 notes
Video
instagram
#tricepsdips Functional anatomy The triceps (primarily the lateral and medial heads), sternal and clavicular heads of the pectoralis major, anterior deltoid, scapulothoracic, and core musculature, all work in accord during the movement. The scapulothoracic muscles collectively stabilize the scapulae during the movement, especially as the descent is commenced. The core resists any movement, specifically lateral sway, which occurs right off the bat in lesser experienced lifters and weaker individuals or late in the set when fatigue begins to set in. The pectoralis and anterior deltoids provide the initial push at the bottom while the triceps, along with the aconeus, take over the movement when the elbow approaches 90 degrees of flexion, helping to lock the elbows out to complete the movement. parallel dips have been demonised, arguing that they destroy the shoulder and elbow joints. While there’s some validity to the argument because parallel dips aren’t advised for individuals such as throwing athletes, those with anterior shoulder instability, and pre-existing elbow pain. However, they shouldn’t be entirely steered clear of, especially by healthy lifters and athletes. Type of Movement : Unsupported Compound Sub Type : Bilateral Joint Action : Elbow Extension Muscles recruited : Target * Triceps Brachii Synergists * Deltoid, Anterior Stabilizers * Trapezius, Lower @manishmehta003 With 72kgs body weight performing the exercise with added resistance of 35lbs. Always follow principle of #progressiveoverload #tricepsworkout #tricepstraining #tricepworkout #hypertrophy #injuryprevention #bodybuilders #bodybuildermotivation #bodybuilderlifestyle #bodybuilder #bodybuilding #bodybuilding_and_fitness #bodybuildingtips #bodybuildingaddict #bodybuildingtraining #correctform #integrativehealth #integrativefitness #personaltrainer #integrativehealthcoach #k11 #k11academyoffitnesssciences #k11certifiedpersonaltrainer #yogabyaakaash #pune https://www.instagram.com/p/BvUW4Rhn64V/?utm_source=ig_tumblr_share&igshid=1qki2xz474b3u
#tricepsdips#progressiveoverload#tricepsworkout#tricepstraining#tricepworkout#hypertrophy#injuryprevention#bodybuilders#bodybuildermotivation#bodybuilderlifestyle#bodybuilder#bodybuilding#bodybuilding_and_fitness#bodybuildingtips#bodybuildingaddict#bodybuildingtraining#correctform#integrativehealth#integrativefitness#personaltrainer#integrativehealthcoach#k11#k11academyoffitnesssciences#k11certifiedpersonaltrainer#yogabyaakaash#pune
0 notes
Link
How to get a bigger chest
1) Bench press
(10 reps 3-4 sets comfort 2min)
Hold your wrist straight above your elbow in the bottom position. Take back your shoulders, move your feet into the ground, squeeze the bar and bind your lamps. Un-rack then reduces the bar in your chest control. Explosive drive back up
"The problem with bench press is that most men are focused instead on how much weight they are stimulating their chest," says physiologist Tom MacCormick. "It can promote your ego, but it will not increase your pecs.
Instead of focusing on external focus, look inside. When you press, focus on the amount of stress you put on top. Feel as low as muscle strain Focus on doing this, below, make sure you are using your chest to gain weight. You may have to lose weight first - but it increases your peak.
bigger chest
2) close-grip benches
(8 reps 3-4 sets the rest of 90sec)
Hold a shoulder width on the bar. Take back the blade of your shoulder contract your bead to bind your torso and gradually lose weight on your chest. Take back the weight position explosively.
"Since most people begin their chest training with the bench press, they end up developing their lower chest unevenly."
"Studies show that the sternocostal head [lower chest] is activated with broad grip in the widely flat or dotted bench press. The clavicular head [upper chest] is more active using the inclination between 30-60 degrees, While some studies show that a compressed grip increases this activation.
bigger chest
3) cable fly
(10 reps 3-4 sets the rest of 60sec)
Lie on a bench set to two-cave pulleys with a 15-degree incline with the rope attachment. Understand the ropes and turn slightly in your elbow, as long as you do not feel the strain in your chest, reduce your arms to the sides in a wide arc. Begin the steps by contracting your pecs.
"Most people fly exercises with dumbbells using a neutral grip," says McCormick. "It is sub-optimal for two reasons. First of all, the category in which the muscle is in tension with the dumbbell is small because gravity is not directly working on the load for the second part of the movement.
It is best to separate the peak or not to be the best, and the cable machine is a better option for flying with the bottom hold with the palms. Provides Chun and constant stress. You can add the external rotation of the arm at the beginning of the movement to increase to more strain and activation.
bigger chest
4) Smith Machine Incline Press
(8 reps 2-3 sets the rest of 60sec
Set the adjustable bench to 30 degree - 45-degree incline, and rotate it in the center of the Smith machine rack Understand the bar with an overhand, shoulder-width grip. Unlock the bar, reduce it to the upper part of your chest, and press directly.
5) Incline Dumbbell Fly
(10 reps 2-3 sets the rest of 60sec)
Set an adjustable bench at 30 degrees -45 degrees, and lie on it with one dumbbell in each hand. Turn your wrist so that your palms face each other.
Push weight directly on your chest, then, lean slightly in your elbow, open your arms as if you were going for a big bear's throat. Reduce your arms until you feel stretched in your peak, then bring the weight together on your chest.
6) flat Dumbbell fly
(8 reps 2-3 sets the rest of 60sec)
Lay back on a flat bench with a dumbbell in each hand. Keep a little turn in your elbows and widen your arms, reduce the weight until they are even from your chest.
Pick your pecs flex and weight back in the initial position.
bigger chest
7) Lower chest cable
(8 reps 2-3 sets the rest of 60sec)
Stand between two face cable stations and attach a D-handle to each of the low pulleys.
With each hand, a handle and elbows slightly inclined, raise your arms out of the waist height in front of your chest, flake your peak because you bring them together.
8) Plate chest press out
(8 reps 2-3 sets the rest of 60sec)
Put a pair of lightweight plates together between your palms in front of your chest, on the smooth side.
Squeeze the plates together, focus on your chest, and press your front until your arms are stretched.
Throw your lbs and pull the weight back onto your chest. Complete your representative and then, on the second set, press the weight down with your chest at 45-degree angle.
On the third set, press them at a 45-degree angle upwards.
bigger chest
Also, read -
Do BCAAs have calories
Can low testosterone cause hair loss
Creatine and its use
How to gain muscle
0 notes
Photo

HOW THE CHEST IS FORMED.🍑 . In order to know how to properly work your chest and choose the exercises for your chest routine, it is important to understand how you chest is formed. - Lets take a look at the different parts of the chest. - PECTORALIS MAJOR: This is the largest muscle of the chest. It is formed of three sub heads: sternal head, clavicular head and abdominal head. - STERNAL HEAD: Located near middle oft he chest. Runs from the sternum, across chest and inserts at the humerus. - CLAVICULAR HEAD: Located at the top of the chest. Runs from your clavicle down and across the chest. It is a difficult area to train for many. - ABDOMINAL HEAD: Muscle that runs along the bottom part of your chest. Connecting abdominal muscles to the chest muscles. - PECTORALIS MINOR: Found beneath the pectoralis major. Mainly helps you breathe easier. - SERRATUS ANTERIOR: Found at the sides and wraps around connecting to the front of the ribcages. Usually underdevelopped. - Here are a list of effective chest exercises: barbell press, dumbbell press, incline barbell press, decline barbell press, cable crossovers, dumbbell flies, etc. - Make sure that when you are working out your chest, you squeeze the chest on every repetition. Focus your mind on the muscle, chest. - What are your thoughts on chest developpement? - Chest training advice? - COMMENT BELOW! . TAG SOMEONE who needs help with building their chest! - Follow me @mathi.r.t for insane transformation plan, contest prep, gym related doubts and more inspiration! . #health #fitness #fit #tflers #fitnessmodel #fitnessaddict #fitspo #workout #bodybuilding #cardio #gym #train #training #photooftheday #health #healthy #instahealth #healthychoices #active #strong #motivation #instastyle #determination #lifestyle #weekend #fun #adventure #wbff #ifbb . @mathi.r.t 🔥 @mathi.r.t 🔥 @mathi.r.t 🔥.
#lifestyle#health#gym#fitspo#ifbb#instastyle#weekend#healthy#bodybuilding#fitnessmodel#determination#photooftheday#fit#instahealth#healthychoices#train#fitnessaddict#motivation#workout#fun#cardio#adventure#wbff#training#active#strong#fitness#tflers
0 notes
Photo

Metaphyseal fractures of long bones, Sub capital Humerus, Metatarsal, and Metacarpal fractures, and complex Clavicular fractures in Children ....
https://www.orthopaedic-implants.com/nails-wires-pins/nails/tens-nail.php
5 notes
·
View notes
Text
Rec: Sleepwalk back to the battle site

sleepwalk back to the battle site (1306 words) by clavicular Rating: Explicit Warnings: Creator Chose Not To Use Archive Warnings Relationships: Peter Hale/Scott McCall Characters: Peter Hale, Scott McCall Additional Tags: Alternate Universe, Codependency, Fairy Tale Elements, References to parallel universes, references to murder and abusive behaviours, Consensual Kink, Bondage, Dom/sub, Dirty Talk, Dark Romance Summary:"We begin the way all good fairy tales do. With an innocent youth lost in the woods... and a monster."
This isn't the story you think you know. But maybe all paths lead to the same place, in the end.
5 notes
·
View notes