#require a diagnostic either way)
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
"don't waste your money getting a diagnosis for the car if nothing is wrong" hey, just because it ran fine on a small drive doesn't mean there isn't problems, and while you claim to know exactly what wrong with it you never disclose that information to the person who drives it every day. Weird, huh? Believe it or not, I want to be able to fix problems, not just ignore them until the thing is completely unusable.
#neon moments#this is the same person who pushes everyone away because he is a terrible person and then say#“They left me with no explanation”#“They clearly never cared”#“I did so much for them”#We leave because you fail to recognise a problem as a problem until its irreparable#But its not like you'll ever figure that out#because youre stuck in this world where no matter how plain people make it#you'll never believe it#because youre a narcissist#one last side note#but this is also the person who just yesterday said I need to get the car fixed because of a separate issue#which I guess it's totally fine with bringing a car in (when it's not definitive what is causing this issue either and will most definitly#require a diagnostic either way)#but no#lets be pissy jsut to be pissy because I want to do something you don't agree with#(ONE MORE SIDE NOTE but this person also just yesterday siad “don't get so upset” over something that I slightly opposed him on)#but again#why would those rules every apply to you?#crazy how this world works#Neon rant
3 notes
·
View notes
Text
Some fact checks about plurality
The "Bible of psychiatry" is the DSM. In 1994, the DSM changed the name of Multiple Personality Disorder (MPD) to Dissociative Identity Disorder (DID). This was in response to a moral panic where critics claimed that the condition was fake.
The original and current diagnostic criteria do not require trauma for DID (or MPD) (DSM-III, p. 259; DSM-III-R, p. 272; DSM-5-TR, p. 331).
The international counterpart of the DSM is the ICD-11. Its essential features for DID do not require trauma, either.
Both books say that not all cases of multiple personalities are a disorder or a severe impairment. Psychiatry recognizes that medicalizing them is not always appropriate.
Plurality (or multiplicity) is a community umbrella term for many ways of being more than one person in a body. Psychiatrists who know enough about DID are aware of it. Plurality includes but is not the same as DID.
The community has always included plurals who formed for reasons other than trauma. Dividing the community by excluding non-traumagenic plurals and calling them fake is new. That only started in August 2014 on Tumblr, unheard of elsewhere.
When that started, a trauma-caused DID system created the word "endogenic." This means plurals who formed naturally rather than from trauma. The Lunastus Collective coined it in solidarity with them.
(Similarly, the coiner of another umbrella term, "alterhuman," is a member of a traumagenic OSDD system who supports endogenic plurals. The purpose of that word is for plural systems to unite with other sorts who differ from usual definitions of human individual, valuing what we do and do not have in common, instead of in-fighting about who is more legitimate.)
Community historian LB Lee gives several good reasons why-- as trauma-surviving plurals-- they choose not to call themselves "traumagenic" or divide the community by origins. If I may briefly paraphrase a couple of these: If you see suffering as your whole foundation of who you are, then you have a more difficult time envisioning a better situation. If you want others to respect you, a losing strategy is to put down people who are seen as similar to you.
Neither psychiatry nor the greater community of plurals see trauma history as an important distinction in determining whether someone is plural.
#plurality#PluralGang#DID OSDD#sysblr#endogenic#traumagenic#plural community#endo safe#traumagenic safe#alterhuman#SysCourse#plural#OSDD#DID#dissociative identity disorder#multiplicity#rated G#screen reader friendly#psychiatry#trauma#about words#I've been meaning to make this post for months; it is not a response to whatever the latest plural quarrel is.#if you don't want to see posts like this from me i always tag thoroughly so you can just blacklist a selection of the tags in your settings
797 notes
·
View notes
Text
One thing that I keep seeing whenever I make posts that are critical of macs is folks in the notes going "they make great computers for the money if you just buy used/refurbs - everyone knows not to buy new" and A) no they don't know that, most people go looking for a new computer unless they have already exhausted the new options in their budget and B) no they don't make great computers for the money, and being used doesn't do anything to make them easier to work on or repair or upgrade.
Here's a breakdown of the anti-consumer, anti-repair features recently introduced in macbooks. If you don't want to watch the video, here's how it's summed up:
In the end the Macbook Pro is a laptop with a soldered-on SSD and RAM, a battery secured with glue, not screws, a keyboard held in with rivets, a display and lid angle sensor no third party can replace without apple. But it has modular ports so I guess that’s something. But I don’t think it’s worthy of IFixIt’s four out of ten reparability score because if it breaks you have to face apple’s repair cost; with no repair competition they can charge whatever they like. You either front the cost, or toss the laptop, leaving me wondering “who really owns this computer?”
Apple doesn't make great computers for the money because they are doing everything possible to make sure that you don't actually own your computer, you just lease the hardware from apple and they determine how long it is allowed to function.
The lid angle sensor discussed in this video replaces a much simpler sensor that has been used in laptops for twenty years AND calibrating the sensor after a repair requires access to proprietary apple software that isn't accessible to either users or third party repair shops. There's no reason for this software not to be included as a diagnostic tool on your computer except that Apple doesn't want users working on apple computers. If your screen breaks, or if the fragile cable that is part of the sensor wears down, your only option to fix this computer is to pay apple.
How long does apple plan to support this hardware? What if you pay $3k for a computer today and it breaks in 7 years - will they still calibrate the replacement screen for you or will they tell you it's time for new hardware EVEN THOUGH YOU COULD HAVE ATTAINED FUNCTIONAL HARDWARE THAT WILL WORK IF APPLE'S SOFTWARE TELLS IT TO?
Look at this article talking about "how long" apple supports various types of hardware. It coos over the fact that a 2013 MacBook Air could be getting updates to this day. That's the longest example in this article, and that's *hardware* support, not the life cycle of the operating system. That is dogshit. That is straight-up dogshit.
Apple computers are DRM locked in a way that windows machines only wish they could pull off, and the apple-only chips are a part of that. They want an entirely walled garden so they can entirely control your interactions with the computer that they own and you're just renting.
Even if they made the best hardware in the world that would last a thousand years and gave you flowers on your birthday it wouldn't matter because modern apple computers don't ever actually belong to apple customers, at the end of the day they belong to apple, and that's on purpose.
This is hardware as a service. This is John Deere. This is subscription access to the things you buy, and if it isn't exactly that right at this moment, that is where things have been heading ever since they realized it was possible to exert a control that granular over their users.
With all sympathy to people who are forced to use them, Fuck Apple I Hope That They Fall Into The Ocean And Are Hidden Away From The Honest Light Of The Sun For Their Crimes.
2K notes
·
View notes
Text
There isn't a whole lot of content on Tumblr about schizoid personality disorder so I thought I would make a little informational post. SZPD is a cluster A personality disorder, of the odd/eccentric cluster alongside schizotypal and paranoid. It is on the schizophrenia spectrum, and comprises the negative rather than positive symptoms of schizophrenia.
This primarily means we have avolition, catatonia, flat/blunted affect (demeanor), limited interoception (emotional sensations), lack of bonds to others including primary family members, and indifference to the opinions of others.
Whilst this isn't a diagnostic criteria, many of us are also asexual and aromantic, meaning we don't want to have sex with other humans (but usually do masturbate) and have no interest in romantic companionship.
My most disabling symptom is avolition, because I have comorbid ADHD. This means when I don't have my medication (dextromethorphan 120mg) I just sit there and zone out and can't even hold a conversation or move my body, nor even do things like feed myself. It is genuinely crippling and I am unemployed because of this, even though my meds help, they don't cure me and I need a lot of time alone.
Schizoid is something of an "anti-human" disorder, because we fail to form basic social bonds with others including primary caregivers. As a child I got diagnosed with inhibited RAD because I could not tolerate human contact. This differs from autism because autistic people generally want to socialize, they just lack the skills. I don't want to socialize and it takes tremendous effort for me to do so.
To even make this post I had to wait for my meds to click in as I was just sitting there mindlessly beforehand. While we have low internal sensations of emotions like caring, love, happiness, trust, sadness, etc. we aren't typically antisocial/dissocial and don't have a pattern of exploiting others or dishonesty. This requires too much effort.
There is a schizoid version of narcissism but it is separate to narcissistic personality disorder. NPD is characterized by a very fragile ego. You can't contradict or disagree with NPD because they are unable to regulate the emotions caused by conflict. Conversely, SZPD does not care about the opinions of others at all and places little value on them.
Our sense of superiority is legitimate, meaning we just do genuinely believe we are smarter than other people. So your mileage may vary on how insufferable you find that. I recognize this trait in myself and work to actively challenge it since it is illogical for me to think I am more special than anyone else. But, my ego is very stable, so criticism doesn't bother me the way it would in NPD.
Interoception means the sensations you feel inside your body. We lack this, so even stuff like hunger and tiredness don't impact us until we are very hungry or extremely exhausted. I don't have the feeling you would to look at a family member and get a sense of love or trust. I have a logical sense of obligation that I developed through choosing what I value based on reason. I describe this as care, and I place importance on my friendships, but there is no emotional component to this, it is all cognitive.
Tangentially: I'm somewhat of an optimistic nihilist, believing that there is no grand purpose to existence. Yes, even as a religious person. I don't think G-d ultimately has a purpose either, as an agent of the universe. (I don't believe G-d created the universe.) We have a human nervous system, so we base our rubric for morality on suffering and decide what is meaningful both collectively and individually.
I don't believe in true freedom of will (but I do believe we have agency), because we know that Bereitschaftspotential or reaction potentials occur in the brain up to two seconds before we become conscious of a volitional desire. Our consciousness occurs because of quantum synchronicity in the brain, so our free will is in a bit of an in-between state rather than fully determined or fully free.
So, we are not born deciding "I'm going to be an abuser," that happens because of brain abnormalities. It's no different than the forces of creation and destruction at work like a virus infecting a host cell. I don't place much importance on concepts of self-hood, I view myself as the electrical and chemical processes that occur in my brain, which happen without my choosing, that I can influence and impact through my own agency.
Anyway, these are just some basic schizoid meanderings for you all and I hope that this was informative or interesting in some way. Peace.
#cluster a#schizoid pd#actually szpd#szpd#reactive attachment disorder#weemie#nihilism#neurology#quantum physics#schizospec#schizoid#dxm#dextromethorphan#auvelity
150 notes
·
View notes
Note
What was the purpose of the panels of blinking lights on those big mid-century computers? Were they showing calculations in progress?
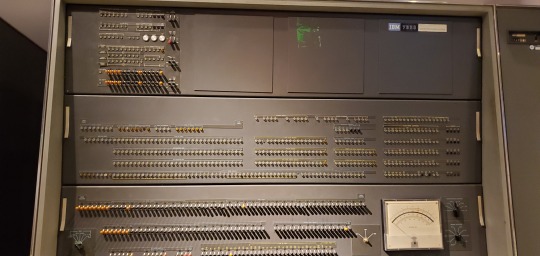
Excellent question, this is one of my favorite subjects! Blinkenlights serve a number of functions. Hollywood tended to use just the lights to make it look like a computer was busy doing something, but real computers had more than just lights on their front panel. Let's walk through a few examples of use cases with photos of computers I've seen over the years at museums and vintage computer festivals:



Some front panels were built to be used for diagnostics. Computers like these were primitive enough that they required constant care and debugging to do their jobs, especially the early vacuum tube machines (everything pictured here is transistorized). You could tell what peripherals were being used, but also check the status of registers, carry flags, status flags, data, various buses, etc. It was also a way to see if a program had "gone off into the weeds" and started doing things that were irregular, possibly due to a software bug, or a problem with the hardware.

On many of these machines, you can enter programs directly into the main memory using the front panel, but it's an incredibly tedious process -- something to be avoided if possible. Consider it a last fallback.

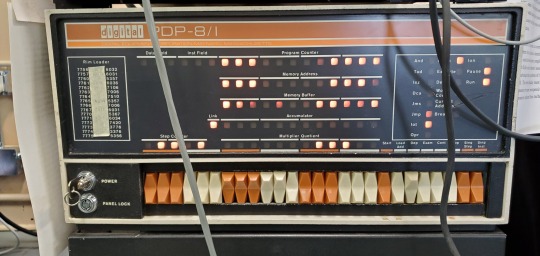
Other times, it's a starting point, which we call "bootstrapping" (this eventually evolved into the term "booting"). You aren't likely to program everything on such a limited interface, but you are more likely to enter in a small program that can tell the computer how to run a more complex peripheral, like a paper tape or punch card reader, or maybe some type of magnetic storage device. Once you can get a program loading off of a larger permanent storage device, you can load up software to interface with a terminal of some kind which is much easier.

Eventually, the microprocessor made home computers a possibility, but many were only equipped with a front panel out of the box. You would have to add in a serial card, more RAM, possibly some ROMs, and either a teletype or glass terminal in order to get a more sophisticated and intuitive interface from the computer, capable of programming in a higher level language. Some were considered more like trainers, or hobbyist devices, and simply lacked that ability, meaning all you got was a front panel with switches and lights.


I made my own front panel to see what the experience was all about:

Then everything changed in 1977, with the introduction of these three machines: the TRS-80 Model I, the Commodore PET 2001, and the Apple II. They were what you might call "appliance computers" and they had no need for a front panel.

Hopefully that answered your question!
727 notes
·
View notes
Note
Hi!
I'd like to request something with Mori Ougai (bsd) being head over heals for someone in the port mafia (who has the same status as Chuuya, but I can't remember what it's called, sorry...). Preferably ending with smut.
I couldn't find of you were open for requests or not, so sorry if this comes at the wrong time, and also okey if you decide to not Wright this, thank you either way
Doctor Knows Best (Mori Ougai x Reader)
𝗔/𝗡: 𝗱𝗶𝗱𝗻'𝘁 𝗮𝗰𝘁𝘂𝗮𝗹𝗹𝘆 𝗴𝗲𝘁 𝗶𝗻𝘁𝗼 𝗮 𝘀𝗺𝘂𝘁 𝗯𝘂𝘁 𝘀𝘁𝗿𝗼𝗻𝗴𝗹𝘆 𝗵𝗶𝗻𝘁𝘀 𝗮𝘁 𝗶𝘁 𝗶𝗻 𝘁𝗵𝗲 𝗲𝗻𝗱 𝗹𝗺𝗮𝗼. 𝘀𝗼𝗿𝗿𝘆, 𝗶 𝗰𝗼𝘂𝗹𝗱𝗻'𝘁 𝗵𝗲𝗹𝗽 𝗺𝘆𝘀𝗲𝗹𝗳- 𝘁𝗵𝗲 𝗯𝘂𝗶𝗹𝘁-𝘂𝗽 𝗶𝘀 𝘁𝗼𝗼 𝗺𝘂𝗰𝗵 𝗳𝘂𝗻. 𝗮𝗻𝘆𝘄𝗮𝘆𝘀 𝗶 𝗵𝗼𝗽𝗲 𝘆𝗼𝘂 𝗹𝗶𝗸𝗲 𝘁𝗵𝗲 𝗱𝗶𝗿𝗲𝗰𝘁𝗶𝗼𝗻 𝗶 𝘄𝗲𝗻𝘁 𝘄𝗶𝘁𝗵 𝘁𝗵𝗶𝘀 𝗿𝗲𝗾𝘂𝗲𝘀𝘁! 𝗲𝗻𝗷𝗼𝘆 :)
𝙒𝙖𝙣𝙩 𝙩𝙤 𝙧𝙚𝙖𝙙 𝙢𝙤𝙧𝙚? ⇒ 𝙈𝙖𝙨𝙩𝙚𝙧𝙡𝙞𝙨𝙩
𝙟𝙤𝙞𝙣 𝙢𝙮 𝙙𝙞𝙨𝙘𝙤𝙧𝙙 𝙨𝙚𝙧𝙫𝙚𝙧?
𝙗���𝙮 𝙢𝙚 𝙖 𝙘𝙤𝙛𝙛𝙚𝙚?
If you’re being honest, you’re more surprised that he hasn’t pulled you from your position yet.
It’s been a while since you’ve had a real command from him. One that really required your status as an executive of the Port Mafia, anyway. If it wasn’t dealing with paperwork or handling intelligence or giving orders from the safety of a nice cushy, building, it was just simply lying around. Waiting for something to do. Waiting for a reason to be here. Of course, you know you still have use here. Your status as a senior member and your special ability is what got you to rise in the ranks so quickly when you were much younger. But you’re not getting any younger like this. You’re not being very helpful like this. As helpful as you know you could be, at least. However…
“Breathe in for me, my lovely.”
You’re positive Mori is too into the idea of you being helpful right now. At least, not after the incident.
That’s really the only plausible explanation for your situation right now. That’s the only way you can explain how you ended up in his old doctor’s office in the Port Mafia’s base in just a nightgown after he heard you coughing over breakfast in your room. He even made sure to give you a personal escort and everything. That is to say, he took you by the hand and fussed over you every second of the way - even in front of your subordinates.
Now, if it were up to you, you would have chosen to be anywhere beside his examination table with all the top bottoms of your dress undone and the fabric settling dangerously around your shoulders as he goes through his usual routine of diagnostics. You would have chosen to be absolutely anywhere- except this close to him. And at the moment? You’re more than exasperated enough to make it known to him.
“Mori, I’m fine!” You insist with a frustrated huff. However, you do end up giving in very quickly and giving him a deep breath in and out as he presses the cool metal of the stethoscope against your skin. You keep your eyes adverted, not at all willing to give into his overly concerned self. But your compliance ends up putting a small smile on his face that you’re able to spot just out of the corner of your eye- something that warms your cheeks and flusters you greatly. Still, you’re not willing to go down without a fight. Even if the man you’re duking it out against just so happens to be your very, very smug boss. “The other doctor said I’d be good to get back in the field three weeks ago! You can’t keep doing this.”
At your protest, Mori just lets out an absent hum. Almost as if he doesn’t have a care in the world as to what you have to say or think or do. But you know deep down inside that’s a line. After all, he wouldn’t be showing this much concern over your health after the explosion you were in a couple months ago if he didn’t care about you. He wouldn’t be ditching the fancy black suit in favor of a measly little doctor’s coat and old purple button-up if you were someone else. Because you know he hasn’t done it to anyone- not even the other executives.
And that’s what makes you so upset. That’s what makes you so frustrated. That’s what makes things so unfair.
“A second opinion is common practice in the medical field, my dear.” He responds to you easily as a look of concentration passes over his face while he takes your readings. And it just makes you want to scream with just how quickly he’s able to brush you off. Though it looks like the anger had crept onto your face a little more than you were anticipating. Because all too soon, he’s taking the hand he put on your shoulder to keep you still and cupping at your chin to turn your head to meet his red eyes directly, a tight smile on his face. “And it’s Dr. Ougai, sweetheart. Remember who you’re talking to.”
You swallow a little nervously at his gaze, but in reality, you know you have nothing to fear. He’s been tough on you before. He’s been tough on you and your fellow executives plenty of times before. Yet one measly explosion and a moderate concussion later, you’re just now allowed to have unsupervised time in front of a computer. And that thought now only serves to annoy you further. Way, way, way further.
“I know exactly who I’m talking to.” You bite out, half a snarl curling at your lips. Mori only raises an eyebrow at you- expression amused and a little too playful for your liking. But you don’t give him the time of day to suck the joy out of your rebellion. You’ve just about had it with his coddling. You’ve just about had it with his constant nagging and the way he looks at you. Like you need to be protected. Like walking out of that explosion wasn’t a possibility that came with your job. Like you couldn’t handle the lifestyle you’ve signed up for yourself. You’ve just about had it. “I’m talking to my boss. The one who refuses to give me orders and let me do my job. The one who keeps calling me weak by never telling me what to-”
And unfortunately right now…
“You want orders?”
…he’s listening loud and clear.
For the first time in a while, Mori addresses you with a sharp tone. One that reminds you of what it means to be in the Mafia. To be skating on thin ice. But it’s what you wanted. That’s what you asked for. So that’s what you get. You made your bed. It’s only right that you’d sleep in it too.
“Yes.” You answer quietly, keeping your voice nice and even to avoid showing any emotion.
“Yes, what?” He shoots back almost immediately. The amused expression that was once on his face is gone- replaced by lips set in a straight line and half-lidded eyes that present all the seriousness that you would expect from a mafioso. And maybe it’s because you’ve been out of the game for a while than you’d like to be. Maybe it’s because of all this coddling and hand-holding that he’s been doing with you. Maybe it’s all that and a combination of more that made you feel so soft. So weak. Whatever it is, you have no doubt that it’s the very thing that caused you to let out another nervous swallow despite your best efforts to hide it. One that he notices easily. One that he addresses just as easily too. “Say it.”
“Yessir.” You tell him, nearly slurring over your words in order to get them out in time. Back straight and tall. Eyes forward. Body stiff. Like a good soldier should. Like a good soldier should. But that’s the thing. That’s the thing about him that you didn’t get. It’s the fact that he didn’t want a soldier.
“Good girl.”
He just wanted you.
You were slow to understand that until the final second. But the second you heard the purr of his compliment, you can’t help but feel it. You couldn’t help but feel like you had melted. Softened up a little bit. In a way that you’d like. In a way that Mori appreciated.
And of course, as seconds passed by, things became more and more clear to you. After all, you think there’s very little that needs to be explained when your doctor and your boss all but tear the stethoscope from his ears and toss it elsewhere in favor of surging forward and wrapping his arms around you. And you know there’s even less to be explained when those warning arms start creeping up the back of your nightgown and settling a little dangerously on your hip. And even less than that his deep, velvety voice is no longer spouting compliments. Instead- they’re pressing themselves against your neck and your collarbone and your shoulders and the valley between your breasts as he makes quick work of tugging down your already scandalously low-hanging dress even lower. In between the kisses he presses to your lips, of course.
And by the time your mind catches up with your body, you swear everything about you is overheating. The mere sensation of rough fingertips brushing over your bare skin- taking extra care to trace your new scars and your faded wounds- it’s enough to send you whining. And the mere sensation of his lips against your body- the little nibbles and the softness of his lips spreading here and there- it’s enough to send you squirming. Breaking you down and building you back into his image. Almost as if every time insisted you see a doctor or you take a break or you hold off going back to work was all in preparation for this one moment.
“You want orders, princess?” He asks you finally, and you are not sure you have enough fire in your belly left to answer like the mafioso you’re supposed to be. Not that he cares. Not that he wanted that anyway. Because he wouldn’t have gone through all the trouble of making you soft and pliable and desperate for his approval and his commands if that’s what he wanted for you, now would he. “You want to be my good girl?”
As if that switch that was flipped on inside of you is now up and at full force, you start nodding your head like a mad woman. Like this was what you made for me. For following his orders. For following his lead. Whether it’s killing in his name. Whether it’s moaning his name. As long as he tells you to do it. As long as he commands you to do it. Then’s enough for you. In fact, it’s more than enough for you.
“Then lay back and open your legs for me, darling.”
After all…
“You can do that for your Doctor, right sweetheart?”
…Dr. Ougai knows best.
#mori ougai x reader#mori ougai#mori ogai#mori ogai x reader#bungou stray dogs fanfiction#bungou stray dogs x reader#bungou stray dogs fanfic#bungou stray dogs#bungo stray dogs#bungo stray dogs x reader#bungo stray dogs fanfic#bungo stray dogs fanfiction#bsd#bsd x reader#bsd fanfic#bsd fanfiction#x reader#xreader#fanfic#fanfiction
345 notes
·
View notes
Note
You’ve dealt with your share of Evangelical Christians on this website, and you tend to be right about things, so can you give me your thoughts on a pet hypothesis I have on Christians (particularly Evangelicals) and lack of empathy?
My theory is like this: Christians believe that anyone who accepts Jesus Christ as their Savior and Lord (anyone who is a Christian) goes to Heaven, and everyone else goes to Hell. This means that good non-Christians, including people they interact with every day, will be tortured forever in the afterlife. This is distressing for most people, because they naturally empathize with non-Christian people who they have positive interactions with. Most people can extrapolate these good interactions to the billions of strangers in the world who aren’t Christians. If they have empathy for these people, they can put themselves in their shoes, and the pain of their eventual torture in the afterlife weighs on them.
This pain that is caused by empathy can be resolved in two ways: either the Christian dedicates the rest of their life to evangelism to save as many souls from the fires of Hell as possible, or they just cut off empathy to non-Christians so they can stop feeling this pain. Most Christians aren’t missionaries, so they just stop caring about other people. This doesn’t mean that they necessarily become cruel or impolite to other people, they just stop putting themselves in other people’s shoes/imagining life from another perspective, because that would be painful.
Once you’ve cut of empathy to a group of people for one reason (religious differences), it’s easier to cut off empathy for other reasons, or even to become bad at empathy through lack of practice.
Anyway, that’s just my hypothesis from being raised Evangelical. And I want to emphasize that this hypothesis is about empathy, not compassion, though they are related.
This all follows logically, and may apply to some individuals, but I don't think it can be relied upon in a diagnostic sense, if you get me?
The 'why' of what's going on in any given person's head doesn't matter to me unless that person is a close and personal part of my life, someone confiding in me because they want to better understand themselves and/or want to change and grow. I don't really feel motivated, personally, to explain the motivations and rationale of another person's bad behavior - I care about making the behavior stop and preventing it from happening again.
The only value in understanding why someone arrives at a place of diminished humanity (because that's what Evangelical Christianity does, really) is in either helping them regain it (applicable only in close personal relationships) or if it in some way guides a policy that prevents their diminished humanity from hurting others.
"You told Sally she's going to hell; we do not do that here. If you do that again, you will not be welcome here. Sally is not required to associate with you or accept an apology even if you want to give one."
is more important to me than
"You told Sally she's going to hell; why did you do that?"
The above is useful in understanding, as a person who's been hurt, why those people hurt you. It's a self-healing technique and entirely valid for that.
It's not useful for fixing the problem of evangelicals who think this way or preventing them from doing harm.
22 notes
·
View notes
Text
some ways that congenital hypotonia affects me personally in my everyday life
disclaimer: this is a "i want to see hypotonia talked about more"/vent-post adjacent thing rather than something that should be used as some kind of diagnostic reference. hypotonia is more of a symptom than a condition on its own & is associated with a wide variety of diagnoses, i personally don't have a label or explanation for what i experience other than "congenital hypotonia" (and my case is not "self-diagnosed," this was identified when i was still a child.)
generalized hypermobility and painful joint instability either caused by hypotonia or at least contributed to by it if not; no frequent dislocations but joints still tracking badly (especially my knees) and causing pain, ankle instability once gave me an injury
related to above, knees have occasionally buckled/threatened to give out, usually when i'm tired or when i've stood from a sitting position in a chair
unfixable bad posture putting unnecessary strain on a lot of things (reason why my hamstring muscles are so tight)
sitting or standing up easily causing fatigue and pain unless something else is adquately supporting my body (normal chairs usually don't suffice because that still requires adequate posture)
related to above, persistent need to lean on things for support; this is the primary reason why i own a cane
staying in bed a lot due to the above because it's the only time my body doesn't have to support itself
tendency to drool, usually when laying down
dysphagia (things feel "stuck" in my throat a lot, swallowing capsules is becoming more and more uncomfortable), aspirating food/water, acid reflux making these issues worse
may or may not be part of the reason i'm a bit of a loud breather
sometimes chewing hurts or is tiring (or talking)
related to above, mild speech issues mainly affecting articulation (e.g. mouth making a "v" sound rather than "th" sometimes), makes speech physically feel weird or forced, or something even painful; sometimes "talking out of the side of my mouth"
poor grip = poor handwriting, also often makes writing or gripping things painful, including holding/typing on my phone
related to above, makes drawing hard because i don't have proper grip/as much control over my hands as i should
doesn't happen too often but almost randomly losing my balance; i'll just be standing minding my own business and then i'll start tipping over
related to above, can't just stand still and be still, i start tipping in different directions and i think i've subconsciously learned to counteract this when i'n required to stand in place
walking/moving slowly because it feels like my muscles don't have the capacity to move any faster, even if i'm not really "tired" per-se (decreased state of readiness for movement)
have a very hard time holding my head up spine even remotely straight when i am actually tired/worn out
legs/arms start shaking if i hold them out against gravity
also, legs shake if i sit on the floor/a flat surface with my knees bent upward, or arms quickly start to give out if i lay on my stomach and prop myself up on my elbows
walking feels awkward/uncomfortable and wrong most of the time; anything wrong with my gait is probably only recognizable to a PT or someone else who knows what they're looking for, but things just feel too loose/floppy when i walk; probably the reason why i'm prone to tripping and accidentally kicking stuff (POTS-induced ataxia - or w/e it is - makes this much worse)
also probably contributes to constipation and maybe other digestive problems
there's probably more but that's all i can think of for now. this is not universal hypotonia experience as hypotonia is a symptom that varies in its severity and my case seems fairly mild, but i thought i'd talk a little bit about what it's like since it's an under-discussed thing (especially pertaining to disabled adulthood.)
this is okay to reblog.
88 notes
·
View notes
Text
whenever i see people talking about the purpose of mental health diagnoses, three reasons usually come up:
to encourage self-understanding
to concisely describe treatment options to professionals
to gain access to resources and accomodations
but it's hard for me to agree with any of these. given the harm associated with diagnosis, especially diagnosis of a personality disorder, i'm finding it increasingly difficult to justify diagnosing any mental disorder at all. below the cut is a breakdown of each of these three reasons, and why i believe that none of them hold up to criticism.
(1) to encourage self-understanding.
diagnostic criteria are so rigid that they discourage self-understanding. they fragment the human experience, categorizing it into easily digestible groups of "symptoms" rather than understanding a person's struggles holistically. this is why we have a phenomenon of people thinking, "well, my anxiety tells me this, but my depression tells me that" and "i'm having an intrusive thought but can't tell if it's coming from my ocd, ptsd, or bpd." diagnosis misleads patients into believing that, much like one might cough due to either pollen in the lungs or a respiratory illness, one might feel anxious due to either their generalized anxiety disorder diagnosis or their post-traumatic stress disorder diagnosis. a more accurate understanding of the human mind would necessarily involve doing away with the pathology of gad versus ptsd, and instead being able to understand that the anxiety might simply result from a combination of previous negative experiences, a naturally sensitive personality, and underdeveloped emotion regulation skills. a diagnosis is a description of a pattern of thoughts and behaviours; nothing more. my mental health conditions don't cause me to think or behave a certain way. rather, my thoughts and behaviours are similar to the thoughts and behaviours of other people who have also been deemed mentally sick. this makes it possible for doctors to use a certain diagnosis as a shorthand to describe my personality and skills (i refuse to call such things "symptoms") to other doctors. it does not mean that i have a sickness that causes me to think and act in certain way.
why would i want to understand myself through the lens of a psychiatrist, anyways? psychiatry is a deeply individual solution to systemic problems. we're living in a world that evolution could not prepare us for, yet we are told that there's something wrong with our brains if we're unable to adapt to these unprecedented living conditions. i refuse to believe that my brain is sick unless somebody has looked at my brain and can tell me where the sickness is. we must not forget that we're dealing with the discipline that understood homosexuality and hysteria as mental illnesses, and that initially understood autism to be a form of schizophrenia.
(2) to concisely describe treatment options to professionals
imagine, if you will, someone with post-traumatic stress disorder. all you know about them is that they have ptsd. now, recommend a treatment method for them!
nobody can give a good treatment recommendation based on that diagnosis alone. more information is needed: is the patient dealing with persistent general anxiety, sudden panic attacks, or a phobia? does the patient have compulsions? is the patient aggressive, anxious, or depressive? depending on the answers, the ideal treatment plan will be quite different.
now let's consider borderline personality disorder. there are 4 types of bpd and there are 256 possible ways to combine the 5 symptoms required for diagnosis (there are 9 symptoms in total). the personalities, cognitive abilities, and struggles of people diagnosed with bpd are quite diverse, and they will all require varying types and degrees of professional intervention. that being said, bpd is almost always treated with dbt and a few medication options including antidepressants, antipsychotics, mood stabilizers, and anticonvulsants. there are so many other disorders that are treated with dbt and the same drugs. so why make bpd, bipolar, ptsd, cptsd, and depression their own diagnoses? what reason is there, other than to fragment our struggles and generate stigma?
my wish for the future of psychiatry is that, instead of being diagnosed with a disorder that is simultaneously very specific yet inexplicably vague, patients will be told "your struggles are related to trauma and emotional dysregulation. i recommend that you take an antidepressant and attend dialectical behavioural therapy sessions," or "your struggles are related to catastrophization and unhelpful behaviours, i recommend that you engage in cognitive behavioural therapy."
(3) to gain access to resources and accommodations
there are better ways to do this. i don't think anyone should be turned away from the accommodations that they need. however, if resources are scarce and must be gatekept, then a simple interview or quotient test will be sufficient in determining the level of need.
#this took me 90 mins to write. pls enjoy it...#tags for reach ->#anti psychiatry#bpd#actually bpd#mad liberation#mental health#psychology#therapy#pop psychology#ableism#accessibility#therapy speak#leftism#radblr#anti capitalism#antifascist#late diagnosed autistic#late diagnosed adhd#actually mentally ill#actually autistic#neurodivergent#neurodiversity
44 notes
·
View notes
Text
started reading the cass review because i'm apparently just Like That and i want everybody crowing about how this proves sooooo much about how terfs are right and trans people are wrong to like. take a scientific literacy class or something. or even just read the occasional study besides the one you're currently trying to prove a point with. not even necessarily pro-trans studies just learn how to know what studies actually found as opposed to what people trying to spoonfeed you an agenda claim they found.
to use just one infuriating example:
Several studies from that period (Green et al., 1987; Zucker, 1985) suggested that in a minority (approximately 15%) of pre-pubertal children presenting with gender incongruence, this persisted into adulthood. The majority of these children became same-sex attracted, cisgender adults. These early studies were criticised on the basis that not all the children had a formal diagnosis of gender incongruence or gender dysphoria, but a review of the literature (Ristori & Steensma, 2016) noted that later studies (Drummond et al., 2008; Steensma & Cohen-Kettenis, 2015; Wallien et al., 2008) also found persistence rates of 10-33% in cohorts who had met formal diagnostic criteria at initial assessment, and had longer follow-up periods.
if you recognize the names Zucker and Steensma you are probably already going feral but tldr:
There are… many problems with Zucker's studies, "not all children had a formal diagnosis" is so far down the list this is literally the first i've heard of it. The closest i usually hear is the old DSM criteria for gender identity disorder was totally different from the current DSM criteria for gender dysphoria and/or how most people currently define "transgender"; notably it did not require the patient to identify as a different gender and overall better fits what we currently call "gender-non-comforming". Whether the kids had a formal diagnosis of "maybe trans, maybe just has different hobbies than expected, but either way their parents want them back in their neat little societal boxes" is absolutely not the main issue. This would be a problem even if Zucker was pro-trans (spoiler: He Is Not, and people who are immediately suspicious of pro-trans studies because "they're probably funded by big pharma or someone else who profits from transitioning" should apply at least a little of that suspicion to the guy who made a living running a conversion clinic); sometimes "formal" criteria change as we learn more about what's common, what's uncommon, what's uncommon but irrelevant, etc, and when the criteria changes drastically enough it doesn't make sense to pretend the old studies perfectly apply to the new criteria. If you found a study defining "sex" specifically and exclusively as penetration with a dick which says gay men have as much sex as straight men but lesbians don't, it's not necessarily wrong as far as it goes but if THAT'S your prime citation for "gay men have more sex than lesbians", especially if you keep trying to apply it in contexts which obviously use a broader definition, there are gonna be a lot of people disagreeing with you and it won't be because they're stubbornly unscientific.
Also Zucker is pro conversion therapy. Yes, pro converting trans people to cis people, but also pro converting gay people to straight people. That doesn't necessarily affect his results, i just find it funny how many people enthusiastically support his findings as evidence transitioning is… basically anti-gay conversion therapy? (even though plenty of trans people transition to gay? including T4T people so even the "that's actually just how straight people try to get with gay people" rationale for gay trans people is incredibly weak? and also HRT has a relatively low but non-zero chance of changing sexual orientation so it wouldn't even be reliable as a means of "becoming straight"? but a guy who couldn't reliably tell the difference between a tomboy and a trans boy figured out the former is more common than the latter + in one whole country where being trans is legal but being gay is not, sometimes cis gay people transition, so OBVIOUSLY that means sexism and homophobia are the driving factors even in countries with significant transphobia. or something.) anyway i hope zucker knows and hates how many gay people and allies are using his own study to trash-talk any attempts to be Less Gay. ideally nobody would take his nonsense seriously at all but it doesn't seem we'll be spared from that any time soon so i will take my schadenfreude where i can.
Steensma's studies have the exact same problem re: irrelevant criteria so "well someone ELSE had the same results!" is not exactly convincing. This is not "oh trans people are refusing to pay attention to these studies because they disagree with them regardless of scientific rigor", it's "one biased guy using outdated criteria found exactly the numbers everyone would expect based on that criteria, i can't imagine why trans people are treating those numbers as relevant to the past criteria but not present definitions, let's find a SECOND guy using outdated criteria. Why do people keep saying the outdated criteria is not relevant to the current state of trans healthcare. Don't we all know it's quantity over quality with scientific studies. (Please don't ask what the quantity of studies disagreeing with me is.)"
Steensma also counted patients as 'not persisting as transgender' if they ghosted him on follow-up which counted for a third of his study's "detransitioners" and a fifth of the total subjects and. look. i'm not saying none of them detransitioned, or assuming they all didn't would be notably more accurate, but i think we can safely treat twenty percent of subjects as a bit high for making a default assumption, especially when some of them might have simply not been interested in a study on whether or not they still know who they are. Fuck knows i've seen pro-trans studies which didn't make assumptions about the people who didn't respond still get prodded by anti-trans people insisting "the number of people claiming they don't regret transitioning can't possibly be so high, some of the people who responded must have been lying. (Scientific rigor means thinking studies which disagree with me are wrong even if the only explanation is the subjects lying and studies which agree with me are right even if we need to make assumptions about a lot of subjects to get there.)"
and this is not new information. not the issues with zucker, not the issues with steensma, not any of the issues because this is not a new study, it's a review of older studies, which in itself doesn't mean "bad" or "useless" -- sometimes that allows connecting some previously-unconnected dots -- but the idea this is going to absolutely blow apart the Woke Media, vindicate Rowling and Lineham, and "save" ""gay"" children from """being forcibly transed""" is bullshit. At most it'll get dragged around and eagerly cited by all the people looking for anything vaguely scientific-sounding to justify their beliefs, and maybe even people who only read headlines and sound bites will buy it, but the people who really believe it will be people who already agreed with all its "findings" and have already been dragging around the existing studies and are just excited to have a shiny new citation for it.
the response from people who've been really reading research on transgender people all along is going to be more along the lines of "……yeah. yeah, i already knew about that. do you need a three-page essay on why i don't think it means what you think it means? because i don't have time for that homework right now but maybe i can pencil it in for next semester if you haven't learned how to check your own sources by then."
#cass review#lgbt#transgender#transphobia#science#'tldr': *writes three-page essay* 'but i don't have time for a three-page essay rn'#also: holy run-on sentences#but seriously this is not going to change the mind of a single person who would be influenced by reading scientific studies#the studies already existed and have BEEN being used by terfs who think ZUCKER of aLL PEOPLE#is a good gotcha against anyone saying 'reputable studies indicate detransitioning is pretty uncommon actually'#but the responses i find truly fascinating are the ones along the lines of#'ohohoho i bet all those people who criticized jkr will be reeeaal quiet now' w. why.#if past studies didn't convince them the Special Collector's Edition of past studies won't#y'all don't have a monopoly on Scientific Knowledge just because y'all think your Fisher-Price level Gender Definition is the best#sometimes. other scientific information exists. and trans people and allies can even read that scientific information.#i know a weird number of y'all think we run on vibes and liberal propaganda but i promise a ton of us are absolute DORKS
35 notes
·
View notes
Text
Do you need trauma to be diagnosed with DID?
This blog post is not psychiatric advice. For that, you must ask your psychiatrist.
The DSM is the book that psychiatrists use to diagnose DID. The DSM's current diagnostic criteria for DID don't require trauma (DSM-5-TR, p. 331).
Is that new? No. No version of the DSM has ever required trauma for DID. That goes all the way back to when the DSM first had an entry for MPD, before they renamed the disorder (DSM-III, p. 259).
Do some psychiatrists use a different book for diagnosing DID? Yes, the ICD-11. Its essential features for DID don't require trauma, either.
#DID#endogenic#endo safe#dissociative identity disorder#sysblr#pro endo#pro endogenic#SysCourse#endogenic safe#plurality#plural#plural community#if you don't want to see posts like this from me i always tag thoroughly so you can blacklist some tags in your settings#psychiatry#trauma#rated G#screen reader friendly
91 notes
·
View notes
Text
Far Out
Chapter 12: Reunion
Once I had eaten, I began to feel a bit better, but I still couldn’t shake the feeling of loneliness. Despite how nervous the idea of going back into the Frontier public made me, I wanted to see Benni, and being around people could at least be a nice distraction. Now that I could walk, I would be able to assess how bad the damage to the ship really was. CDrive malfunctions were nasty, and a lot of systems were down, according to Benni. I would likely be able to fix most of them, but I had to see diagnostics first. Taking a look at the ship’s black box wouldn’t hurt either.
After taking a tablet out of one of the desk drawers, I made my way back up into the public rings of Brock Station. Back into the crowds. The stress of dealing with an unfamiliar space was ameliorated somewhat by the fact that it was in a familiar shape. If I had been from a planet, I would have definitely been freaking out right now. Luckily, I had been moved from station to station a lot. Figuring out another one wouldn’t be too difficult.
Even if Brock Station was more complicated than Ulthea’s stations, Helga was right about the station maps. They were at every junction, and well made. It really was impossible to get lost here. I took a moment to read the first one I saw, looking specifically for the docks. Unfortunately, they were literally everywhere around the station, attached to the outside rings. Five public rings, thirty docks per ring. This was a big station. There had been a number on the door to the dock where the Benevolence had been placed, and I knew it was on the same level as the medbay, but I had still been kind of out of it at the time. According to the map, the Docking Authority office wasn’t too far. They would definitely know where it was.
Far it was not, but as usual, the walk to the office was more tiring than I anticipated. How did mechanical assistance take more effort? I was an engineer, not a physiologist, so I didn’t have a lot of insight into why that might be the case, but I was definitely focusing on each step a lot more than I would with my own legs. Hopefully this would get easier with practice.
The Docking Authority office was about the size of Helga’s, but there were plenty more people inside. Some people were sat in chairs along the walls, messing with personal tablets as they waited to be called. A few people were standing in a line for one of the two kiosks at the end of the room. I got in behind them and tried to be as unnoticeable as a woman with mechanical legs, an eyepatch, and a bounty on her head could be.
It turns out, someone like that is pretty noticeable. The person ahead of me turned around as soon as I got in line behind them. We stared at each other for a moment. Well, I stared into a dark hood, and I assumed that they were staring at me. The hood was pointed in my direction, attached to a long neck, covered in fabric. Flowing robes covered their body, and they wore a toolbelt around what I assumed was their waist. They were about half a foot shorter than me.
Colors pulsed underneath the hood, and to my shock, I began to hear words, despite the fact that they didn’t say anything. “You’re that Ulthean girl, aren’t you?”
Was that their language? Dr. Skisk had mentioned something like this, but I never expected how strange it would feel. I was almost too stunned to respond, but I rallied and said, “Uh, yes. Jessie. Hi.”
The hood looked me up and down. “You look like you barely made it,” they pulsed.
I rubbed at one of my horns awkwardly. How was I supposed to respond to that? Did they mean I still looked terrible or were they just commenting on my unfortunately required accessories? Deciding to take the comment at face value, I said, “I, um. Yeah, I almost didn’t.”
“Hmm,” they mused, tilting their hood from side to side. “And you’re working for Urthstripe. I’ve got some routine maintenance on my ship coming up. You think you could calibrate my CDrive?”
“Oh,” I said. Maybe the uniform was a bit too recognizable as well. At least I knew how repair bays worked. “Sorry, I’m not a flux specialist. I also haven’t started yet, so it might be someone else on the schedule when you bring your ship in.”
Their hood stayed dark for a moment as they stared at me. Then, they turned away, but not before I heard them say “So much for Ulthean superiority…”
My face flushed immediately at that, and I straightened up in a combination of shame and knee-jerk anger. There was nothing I felt I could say in response. What in the name of the Blessed was that? Was I just supposed to say ‘oh sure, what dock are you in, I’ll go take a look’? That's not how any business worked!
I took a deep breath. Just relax. I had met plenty of rude customers in my time, it was fine. So much for Ulthean superiority. Silently, I seethed there until it was my turn to approach the desk. The person working there was a Felid with dark grey fur, with a nametag that said ‘Moietta’. Her eyebrows raised upon seeing my face, but they lowered once she saw my jumpsuit. I had a feeling that I just avoided a question I didn’t want to answer.
Moietta took a quick look at her terminal. “Let’s see… Jessie Black. How can I help you?” she asked, looking up again.
“I have a ship in one of the docks on ring three, but I don’t know which,” I replied. “The UAN Benevolence?”
The eyebrows went back up. “You don’t know… Oh, right, yes. Just a moment.”
After a minute, she had found the dock number and handed me a sticky note with the dock code so I could access it. I thanked her, and five minutes later, I was standing in dock 313. The Benevolence sat just the same way she had a couple of weeks ago, broken and still. I made my way carefully up the cargo ramp and entered the bay.
“Benni?” I called.
After a minute, there was still no response, and I sighed. It was more than likely that the batteries had been damaged when the CDrive malfunctioned, along with other backup power sources. Walking up to the door that connected the cargo bay to the rest of the ship, I punched a few of the buttons, trying to elicit some sort of reaction. Nothing. The cargo bay was starting to feel more like a tomb. Getting into a dead ship wouldn't be too difficult, and Benni itself would be fine, but…
“Benni!” I shouted. I don’t know why. It’s not like it would have heard me better. It was just so quiet, I had to fill the space with something.
A flicker, from one of the overhead lights. Then another. I gasped. As the buttons next to me lit up, I heard a familiar phrase spoken through the ship's PA system.
“Hello, Captain.”
“Oh, thank the Blessed,” I said, resting my forehead against the door. “I’m so glad you turned on.”
“It’s Good To Hear From You As Well.”
The door to the ship opened automatically, and I stepped inside, looking around. Emergency lights cast a dim red glow over everything. Even in the poor lighting, I could see a month’s layer of dust coating every surface. I winced, and headed towards the utility closet. “I'm sorry it took me so long to visit again. I was hurt pretty bad.”
“No Need To Apologize, Captain. I Set Myself To Wake Every Hour In Order To Scan For Your Lifesigns, Which Only Takes Thirteen Nanoseconds. My Cumulative Time Spent Actively Waiting Was Less Than One Minute.”
Carefully stepping over a pile of what seemed to be ceiling material, judging by the hole in it, I let out an amused snort. “You really did that? Why?”
“I Wished To Make Certain Of Your Proximity.”
I paused mid-step for just a moment as I processed what it was saying. “You were seeing if I was nearby?” I asked, unsure what it meant by proximity.
“Ensuring You Were Still On Station.”
My eye nervously swiveled up towards the ceiling, as if Benni was up there, and almost tripped on a loose drawer. I understood what Benni was implying. As safe as I apparently was, I still thought about it myself.
Finding the utility closet, I opened it and rummaged for cleaning supplies. On a shelf, I found a flashlight and clicked it on. “Someone told you I have a bounty, huh?”
“No, Captain, My Net System Is Offline, So I Was Unaware. That Information Has Now Been Logged. Thank you. I Was Referring To A Past Incident Of Crew Kidnapping In My Service History.”
I froze in the middle of pulling out a large box, flashlight held between my teeth. “Ohg. I’hm sorry, Ghenni.”
“Thank You, But There Is Nothing To Apologize For.”
I spat the flashlight out, and it clattered on the ground, shadows dancing across the walls. “Was it a long time ago? I’d be upset if I lost a crewmember like that, I was just offering my condolences.” I set the box down and sat on it, looking back up at the ceiling.
“It Occured Approximately Three Years Ago. Upset Is Like Gratitude. I Would Need Time To Process It, But Right Now I Would Rather Speak To You.”
That gave me a slightly warm feeling in my chest. You and me both, buddy. “Well, sure,” I said. “I’d like to get some things done on the Benevolence, and you can keep me company. So much has happened in just the past few days, I’m not gonna have time to tell you everything.”
Standing, I removed the lid of the box. Inside was a PalBrand AutoFlux-Sweepr™, ‘Military Grade’. It was a dull grey metal sphere, about a foot across, with a hole on one side, and a switch on the other. The switch made a satisfying click as I pressed it, and I stood back. The sphere rose out of the box, hovered for a moment, then flew off towards the cargo bay. That would take care of the dust and smaller debris.
“Captain, I Have Prepared A Set Of Diagnostic Logs For You. They Are Located In The AI Core Terminal.”
“Thanks, Benni,” I said. “Can you get a dump of your black box as well? I want to get a better feel for what happened when we made that last jump.”
“I Cannot. That System Has Been Compromised. However, The Black Box Itself Should Not Be, And I Am Able To Tell You How To Access It.”
I waved a hand dismissively, then realized Benni probably couldn’t see it right now. “No, it’s okay, I’ve pulled plenty in my time.”
“Of Course, Captain. Please Be Careful In The Cockpit. It Was Most Heavily Damaged When We Were Attacked, So There May Be A Lot Of Loose And Sharp Debris.”
“I will, don’t worry,” I said. Picking up the flashlight, I ventured deeper into the ship. With no windows to the outside, the visibility just continued to get worse.
As I got closer to the front of the Benevolence, a feeling of dread began to wash over me. I did my best to ignore the feeling and press on. The door of the cockpit stood ajar at an angle, clearly damaged. Even the emergency lights inside were off. Well, add it to the list. I took another step. The door loomed. My hands wouldn’t keep still. All I could see were ghostly outlines, thanks to the refraction of the light off the walls, but I couldn’t bring myself to point the shaking beam of light through the door. Okay, just breathe. Deep breath, then–
“Captain, Your Heartrate–”
Never in my life had I screamed as loud as I did just then. The mechanical braces, unable to keep up with the wild jerking signals my spine was sending them, toppled me to the floor.
“Captain, Are You Alright?”
After a moment of spread eagled hyperventillating, I struggled into a seated position. “I’m… Fine. You just scared me.”
“I Apologize, That Was Not My Intention. My Biosensors Were Indicating That Your Heartrate Was Exceeding Safe Levels.”
I placed a hand on my chest. My heart was still beating incredibly fast. Deep breath… and out. Staring into the pitch blackness through the door, I said, “Okay. Let’s save the black box for later. I’m going to go look at your diagnostics.”
“Very Well, Captain.”
< Previous Chapter | Start | Next Chapter >
5 notes
·
View notes
Text
Compromise in Bloom
Synopsis: Now that Charlie and Ethan are back together, Ethan must face Bloom and reach a compromise before Bloom destroys their new future.
Chapter 42 of the “with and without” series
Previous Series: “a weekend with dr. ramsey”
Pairing: Dr. Ethan Ramsey x MC (Charlotte “Charlie” Greene)
Words: 2.6k
Rating: Teen (language)
Also available on AO3 & Wattpad (link in Masterlist)

Ethan felt weightless as he floated down the Edenbrook halls. The whispered gossip and interested stares couldn’t touch him when he felt like this. The rumors of his reunion with Charlie hadn’t reached the whole staff, but soon, it would – and miraculously, not even the impending scandal bothered Ethan.
Because, really, none of it mattered.
For the first time in Ethan’s life, he saw the world with perfect clarity. The only thing he really cared about was Charlie. He’d conquered his career, made his name in academia, and succeeded at nearly everything he’d intended to do. He didn’t need to chase glory, nor did he need to sacrifice himself for his loyalty to this hospital.
Ethan had spent his entire career thinking he must be a martyr to his grand ambition. Nothing – and no one – could stand in the way of his achievement. He’d designed a life where he’d be remembered by textbooks but not by anyone who loved him.
And now he had a chance at something different. He’d felt the crushing loss of Charlie’s absence and was blessed with a second chance. He wouldn’t ruin it again.
Ethan was positively cocky as he walked through Edenbrook – even smiling at an intern who was obviously gossiping in the corner. In a few minutes, he’d be untouchable. For now, the crowd could be satisfied with the strange mystery of Dr. Ramsey’s surprise “vacation” and his unusually happy mood. They’d forget about all of it when they learned that Dr. Ramsey and Dr. Greene had professed their love in the parking lot. And Ethan would make no efforts to hide it either.
He’d promised to be obnoxious about how much he loved Charlie, and it was a promise he intended to keep – as soon as he resolved the danger lurking in the administrative wing.
This part of the hospital used to be an afterthought. It was tidy and well-maintained but never ostentatious. But of course, Bloom’s ego touched every part of Edenbrook, especially the administrative suite. When renovations began, Ethan insisted it was a ridiculous waste of resources that should have been extended to patient care instead. This was only the first of many disagreements.
Ethan wasn’t sure when his disagreements with Blooms had transformed into something more. They started small – fights over which cases should be assigned to the Diagnostics Team and Bloom’s level of involvement in their work. What began as a series of passive-aggressive digs escalated into a war.
Bloom drew the first blood when he leveraged Charlie’s career as blackmail on Ethan. His relationship with Charlie was the first casualty, but despite caving to Bloom’s demands, Ethan ensured it wasn’t the only blood on the field. He’d fought Bloom at every opportunity – blocking unethical treatments, refusing Bloom’s intended patients, and relegating research projects.
Ethan didn’t remember why he did it now. He wasn’t sure if it really was for the patients or if he was acting out on his anger and despair – and he hated himself for not knowing.
None of this was what Ethan wanted. They’d both gone too far.
Ethan didn’t want to fight anymore. He wanted to lay down his weapons and be with the woman he loved, which required compromising with his enemy.
Admittedly, he didn’t really want to do it. The idea of compromising on anything with Bloom made Ethan feel nauseous. There was only one reason he walked into that office – and her name was Charlie.
As soon as Ethan entered the room, Bloom’s assistant slumped into her desk. Meetings between Ethan and Bloom were increasingly frequent and famously antagonistic. Seeing Dr. Ramsey meant that her day was about to get a lot worse.
“He’s asked to not be disturbed,” the assistant glared at Ethan in silent warning. Please do not ruin my perfectly enjoyable afternoon, she quietly begged.
“He’ll want to speak with me,” Ethan insisted, smiling politely to sooth her ire. It didn’t work.
The assistant highly doubted that Mr. Bloom would actually want to speak with Dr. Ramsey, but she sensed that Dr. Ramsey wouldn’t give up without a fight. So, she lifted her phone and dialed Bloom’s direct line. Just as Ethan predicted, Bloom instructed her to invite Ethan in as soon as the assistant said Ethan’s name. Grimacing, Bloom’s assistant ushered him inside the CEO’s lavish office and firmly closed the door behind her, hoping they’d invested in sufficient soundproofing during renovations.
Leland Bloom didn’t stand to greet Ethan. Instead, he watched Ethan like a predator watched his favorite prey. Normally, this blatant intimidation tactic would have incensed Ethan, but today, he merely frowned.
Now this is intriguing, Bloom thought to himself.
Feuding with Ethan Ramsey had become a bit of a hobby for the ruthless billionaire. By now, it was more than just business. Bloom genuinely despised Dr. Ramsey, but that didn’t stop him from being perpetually curious about the medical genius. Seeing him break his normal routine was enough to enthrall Bloom.
“I thought you were supposed to be halfway across the country by now,” Bloom quipped.
Ethan hadn’t told Bloom about his plans to resign and move to San Diego, but his failure to inform Bloom hardly meant that the plan was a secret – nor would the change be unwelcome. As interesting and brilliant as Dr. Ramsey was, he’d become a roadblock, and Bloom didn’t tolerate roadblocks. Ethan would need to comply, or he would need to leave. Having Ethan resign eased the process.
“Change of plans,” Ethan’s face tightened.
“Later flight?”
“No flight.”
Bloom’s eyebrows shot to the top of his temples. Still, he tried to hide his surprise by teasing, “Staycation then.”
Ethan eyed his opponent, trying to mask his disdain. Ethan hated many things about Bloom, but perhaps most of all, he hated the games he played. Feigning ignorance was exhausting and pointless. What was the point of making a veiled threat when they both knew the truth?
They didn’t need to perform for anyone, especially each other.
“We don’t have to pretend, Leland.”
Bloom’s smile twitched at the use of his first name. He preferred more honorific titles just to remind Ethan of their power imbalance.
“Fine,” Bloom snarled, wiping a small piece of lint off his jacket, “But you should know that threatening to quit on such short notice violates your employment contract and does nothing to change my opinion of you. You won’t scare me into backing down, Dr. Ramsey. Nor will you save Dr. Greene from becoming collateral damage. Breaking up with her won’t change the fact you carried on an affair with your prize student, nor will it save her career if it all comes out.”
This got under Ethan’s skin – just as Bloom knew it would.
You had to admire a man who was so easily swayed by love. Once Bloom discovered this weakness, it was so easy to exploit. If Bloom had been a better man, he would have found a more challenging target to keep the odds fair. But no one would ever accuse Bloom of being a better man.
Rage built in Ethan’s chest, accompanied by the uncomfortable prickling of fear on his skin. Ethan promised Charlie he would stay, even though his presence could ruin her career. Making the promise didn’t soothe his terror, nor did their romantic reunion mean that Bloom would call off the attack – especially when it meant that Ethan was more eager than ever to protect Charlie.
Nothing was worth this feeling of dread – not the hospital, not the Diagnostics Team, not even Ethan’s career and reputation. Ethan would gladly give it all up for Charlie to be safe. That’s what almost drove him to California, and that’s why he was here in this office. He wasn’t out of grand gestures yet.
“Isn’t it time we called a truce?” Ethan exuded confidence as he spoke, but Bloom saw his lurking fear.
“A truce?” Bloom scoffed, “Truces are for people prepared to lose. I think you forget the stakes, Dr. Ramsey. Until the day my wife is cured, there is no loss I am willing to accept.”
“I never said you had to lose.”
Bloom wanted to lecture Ethan on the nature of their little war. This was a zero-sum game– one winner, one loser. Any result that didn’t promptly cure his wife and allow them to be reunited would be regarded as a loss. Ethan would be foolish to think anything else.
But Bloom was curious.
So, instead of informing Ethan of his unbearable naivete, Bloom motioned for Ethan to take a seat across from him. Ethan complied, doing his best to maintain his confidence and courage. Neither man was fooled by it.
“This is unsustainable, Leland,” Ethan used his first name, just to put Bloom back on edge, “I’m here to offer a compromise. You want the Diagnostics Team and my research. I want you to leave Charlotte out of this.”
Bloom stared with disinterest, “Go on.”
“I’m prepared to go on sabbatical – one year away from Edenbrook to work on my long-neglected research. I’ll leave the team to Dr. Carrick, who you know will be more amenable to your plans. There will be no scandal, no harm to the institution or yourself. I’ll return to my lab, where I’ll reinstate myself as an influential academic. I’ll publish in all the right journals and speak at all the right conferences. I’ll tell everyone that I was able to dedicate myself to academia because of your wisdom and generosity. My research will still be my own, but we both know it will benefit your wife’s case.
“You came here because of my research,” Ethan continued. For too long, Ethan had let their power dynamic remain imbalanced. It was time to correct that. “You wanted my prestige and my connections. You wanted my work. The only reason you want me gone is that I’m too difficult to manipulate. You’ll still get my research – you’ll have everything you wanted.”
“Everything?” Bloom sneered, “If you wanted to give me everything, you should have complied months ago.”
“You get this, or I leave – and you get nothing.”
The threat echoed in the room.
“What’s in it for you?”
“If I’m not working here, nothing is stopping me from being with Charlie.”
“You think a new job title will protect you from the scandal?” Bloom titled his head, offering insincere sympathy, “Ethan, you had an affair with your student for over a year. You can’t go back in time to hide that.”
“I’m not trying to hide the past. There will be no need. You’re not going to bring it up.”
“Oh, Ethan,” Bloom leaned back in his chair, genuinely amused by Ethan’s confidence. Bloom wasn’t a man of honor – what would ever stop him?
“If you make so much as a comment that harms her reputation or career, the deal is off. It took me less than a day to find another hospital begging for my expertise – I’m never out of options, Leland.”
“I could take away all of your options, Ramsey,” Bloom snarled. He was always prepared to bury Ethan if needed. He’d already tracked down a patient willing to sue and jeopardize Ethan’s medical license. Ethan wasn’t nearly as powerful as he thought.
“You could scare off every employer in the country. I wouldn’t care,” Ethan said honestly, “I’ve had a record-breaking career. I could retire tomorrow. I will retire tomorrow if need be.”
Normally, neither man would have believed this. Ethan was a slave to his career, and a life full of empty days and disgraced legacies would haunt him.
But there was something about Ethan’s voice when he said it – true sincerity. He was really willing to leave it all behind for Charlie.
That was the double-edged sword to manipulating a man so devoted.
“Leland, you told me that you were only interested in winning. Dragging my name through scandal and forfeiting my research hardly seems like a win,” Ethan challenged, “This feud isn’t healing your wife. We’re on the edge of personal and professional ruin, and the person who will suffer the most is the only person you claim to care about.”
Bloom winced. A low blow but deserved, nonetheless.
He came here for his wife. Ethan was nothing compared to that.
“Fine,” Bloom acquiesced, “I accept. You’ll be on a research sabbatical for the rest of Dr. Greene’s residency in exchange for no scandal or harm to her career. But when she finishes her residency, I’ll still expect your work. You’ll return to the team and follow my commands, or you’ll stay in your lab. I won’t accept your insolence any longer.”
Ethan’s stoic veneer cracked, and streams of relief and joy peaked through. The terms were less than ideal, and undoubtedly, Ethan would renegotiate his future after Charlotte graduated. But by then, they could both leave if they needed to, and Charlie would be able to enter the field without the mark of his scandal.
And tonight – and every night thereafter – Ethan could come home to Charlie without fear.
Despite everything, Ethan’s visible delight pleased Bloom. Perhaps compromise was better than destruction.
“You know, I always liked Charlie,” Bloom said candidly, “I never intended to harm her. She was an innocent victim in a holy war for the woman I loved.”
This excuse wasn’t enough for Ethan. It didn’t forgive months of cruelty and threats. It didn’t change the fact that Bloom’s actions had harmed multiple patients, nor did it erase the damage to Ethan’s relationship with Charlie. But despite all its deficiencies, this excuse was something Ethan could understand.
This ‘holy war’ was familiar. He’d fought a similar one months ago, when he’d sat behind glass and watched Charlie fade. He’d held her frail body and wished he could take off his protective gear and die with her, just so he’d be spared the horrible reality of life without her. He knew what it meant to watch a love fade from behind glass.
And Ethan knew that his personal victory was an affront to Bloom. Ethan cured Charlie and revived the promise of a lifetime with the woman he loved. He held her every night and indulged in the steady rate of her heartbeat.
But Ethan didn’t extend the same courtesy to Bloom. He hadn’t cured his wife. He hadn’t reunited them. Instead, he’d screamed about medical ethics while Bloom attempted to bend all the rules to save his true love.
Ethan didn’t blame Bloom for hating him. If he had been in the same position, he would have burned the city down just to have a few more minutes with Charlie.
“I always wanted a cure for your wife,” Ethan confessed, “I know what it means to be separated from the love of your life while they suffer. That’s a fate I wouldn’t wish on anyone, even you.”
The two men stared at each other for a moment – realizing the unique connection they’d often tried to forget. They were looking at the only other man who had experienced this kind of loss, and even if that was the ultimate cause of their animosity, it inspired a sense of kinship. Bloom would abide by the deal – if not out of honor but out of respect for a pair of lovers who had escaped his cruel fate.
Bloom stood, offering his hand to seal the deal. Ethan accepted.
“Dr. Ramsey, congratulations. You are officially on sabbatical.”
“Thank you, Mr. Bloom.”
As of this moment, Ethan Ramsey no longer worked at Edenbrook – which meant he never had to hide Charlie again.
27 notes
·
View notes
Text
An Explanation of the Diagnostic Criteria of Antisocial Personality Disorder (ASPD)
In order to be diagnosed with antisocial personality disorder (ASPD), one must meet three or more of the seven criteria listed in the DSM-V. Symptoms must be pervasive (present in a variety of contexts) and clinically distressing. Additionally, ASPD is the only personality disorder that cannot be diagnosed under 18 (minors would be diagnosed with conduct disorder or a similar behavioral disorder), and there must be evidence of conduct disorder with onset before 15 years.
The term "sociopath" is an outdated way to refer to ASPD and is used to increase the already ever-present stigma against the disorder (psychopathy is a separate distinction but is considered to be a subtype of ASPD).
1. Failure to conform to social norms with respect to lawful behaviors, as indicated by repeatedly performing acts that are grounds for arrest.
Examples include destroying property, harassing others, stealing, stalking, or pursuing illegal occupations such as prostitution or drug dealing.
Committing acts that are grounds for arrest counts whether they have been arrested or not.
2. Deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure.
May be a pathological or compulsive liar.
May be frequently manipulative and deceitful in order to gain personal profit or pleasure (e.g. to obtain money, sex, or power - although in reality, quite a few people with ASPD that I know do this because they're bored).
May be (mis)diagnosed with factitious disorder.
3. Impulsivity or failure to plan ahead.
Decisions are made on the spur of the moment, without forethought and without consideration for the consequences to self and others - often leading to sudden changes of jobs, residences, or relationships.
May binge drink or engage in risky sexual behavior.
4. Irritability and aggressiveness, as indicated by repeated physical fights or assaults.
May often seem irritable or lash out in verbal or physical ways.
In order for this criterion to be counted, irritability and aggressiveness must be physical.
Aggressive acts that are required to defend oneself or someone else do not fall under this criterion.
5. Reckless disregard for the safety of self or others.
Participating in things that could get them or another person seriously hurt or even killed (e.g., extreme food challenges, tide pod challenges, speeding/swerving a car, drunk driving, extreme sports [especially with little to no protection]).
May be evidenced in their driving behavior (e.g., recurrent speeding, drunk driving, multiple accidents).
May engage in sexual behavior or substance abuse that has a high risk for harmful consequences.
May neglect or fail to care for a child in a way that puts the child in danger.
6. Consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations.
May have significant periods of unemployment despite available job opportunities.
May abandon a job without a realistic plan for getting another job.
May be a pattern of repeated absences from work that are not explained by illness either in themself or their family.
Financial irresponsibility, as indicated by acts such as defaulting on debts, failing to provide child support, and failing to support other dependents on a regular basis.
7. Lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another.
Rationalizations may include "Life's unfair" or "Losers deserve to lose."
May blame the victim for being foolish, helpless, or deserving of their fate (e.g., "They had it coming anyway.")
May minimize the harmful consequences of their actions or indicate complete indifference.
May fail to compensate or make amends for their behaviors.
May believe that everyone is out to help themselves and should stop at nothing to avoid being pushed around.
SOURCES:
https://www.helpguide.org/articles/personality-disorders/antisocial-personality-disorder-aspd.htm
https://www.reddit.com/r/aspd/comments/qen3yx/what_are_some_of_your_examples_of_reckless_or/
88 notes
·
View notes
Text
speaking of psychosis- i wasn't speaking of it here but i was speaking of it- i've been trying to figure out what was up with the great psychotic episode of freshman year, because i had assumed it was a trauma-induced psychosis type of deal, but it occurred to me that i was definitely having sort of thought broadcasting types of beliefs, probably some other stuff but i can't remember atm and don't feel like digging thru my old vent account lol. (ramble continues under the cut this got VERY long)
(line with text so tumblr doesn't eat the image. idk if it still does that but better safe than sorry)
(the months with "2" are split into first and second half of the month bc it was relevant, couldnt figure out how else to signify that succinctly)
i cut out the labels of each belief for safety + in case that's triggering to ppl but each row is a different belief i had that in retrospect was probably some sort of delusion? top two are very similar but different enough i tracked them differently. bottom two might have just been anxiety+ptsd but i do really think they're connected to this
it was definitely at its worst mid nov-end of jan, but started in september and didn't really let up til like june
anyway like i said i had assumed it was a combination of trauma and being off my meds and isolation that made the perfect situation for me to go fucking crazy, but i hadn't really thought about it that hard . but now that i Am thinking about it, again, i was definitely having these kinds of beliefs before The Trauma
and in my past self's defense. one thing about my thought broadcasting beliefs specifically was that i was straight up being essentially cyberstalked at the time and didn't know, so i was completely right that certain people knew more about me than i had told them, but i was wrong about the reason why
anyway i was reading up on schizospec disorders for class (kind of. also just for fun) -- also important context schizophrenia does run in my family i think on both sides? but my parents are weird about talking about it. so that's part of this also.
but i noticed that of the three labels i was looking at- brief psychotic disorder, schizophreniform, and schizophrenia- (i didn't look into schizoaffective bc i dont think i have many bipolar symptoms, and didn't look into stpd bc i don't think it counts as a personality disorder if it lasts like 10 months lol, and delusional disorder because i do think i had some negative*&cognitive symptoms (*psych term meaning absence of things present in nonschizospec people, not literally just bad symptoms lol)-- though to be fair, that may have just been a combination of situational aspects & autism?)-- either way, it's not on this beautiful and awesome diagram in mspaint i made so i could illustrate the timeline aspect of the diagnostic criteria:
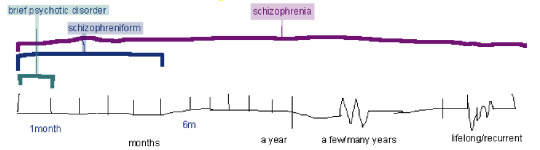
bc a diagnosis of brief psychotic disorder requires symptoms to only last a month, and schizophreniform for 1-6 months, whereas schizophrenia is lifelong .
basically the problem is- while the worst part of my psychotic(?) symptoms lasted ~4months, they were definitely there in some form for around 10 months, which is too long for a diagnosis of schizophreniform, but i don't feel comfortable just, assuming it's schizophrenia lol, especially when most of the symptoms i experienced dont affect my life anymore? it does make me nervous though that this happened right around the typical age of onset.
this might just be a problem with diagnoses being too specific to cover the entire spectrum of human experience, and i might just be outside of any area where a specific label could be applied . also, i know it's been written about but not become an actual diagnostic label- but there are places where ocd and psychosis can over lap, and schizo-obsessive disorder has been suggested as a diagnostic label, but not officially used anywhere afaik..
i think my main concern at this point is just, whether or not i should be concerned about it coming back. like, is it possible to be in various stages of active psychosis(?? it still feels very strange to refer to it that way but i guess that's what it was, so) for ~4-10 months, and then just be chilling after. or should i be worried. was this a one-time thing starting because i was off my meds and being worsened by isolation and trauma or is there a possibility of this happening again. and i think that's a question that can't be answered with any certainty, probably
9 notes
·
View notes
Text
Ranpo Edogawa (Bungo Stray Dogs) & Narcissistic Personality Disorder / NPD
*this is from a document i created that is still in progress*
Introduction:
Narcissistic Personality Disorder is a hard disorder to characterize. It is a cluster B personality disorder formed by a combination of trauma and genetics. There are different types, including grandiose, grandiose-vulnerable, and vulnerable/covert. Each of these types have different symptoms, and not all are represented by the current DSM diagnostic criteria. There are many NPD traits that are not brought up in the DSM, especially those present in vulnerable narcissism.
This document is made by someone with NPD. Everything mentioned here is either labeled as narcissistic traits is either part of the diagnostic criteria or it is frequently experienced by those with diagnosed or medically recognized NPD.
Before we get into Ranpo’s traits of NPD, I just want to make it clear that he does indeed have trauma. He was all on his own after his parents died, both of which are traumatic things. He was raised in a way that made him not understand himself. He was kicked out of institution after institution and was essentially homeless for a while.
Diagnostic criteria:
In order to have the disorder, a person must have at least 5 of the following:
Has a grandiose sense of self-importance (e.g., exaggerates achievements, expects to be recognized as superior without actually completing the achievements)
Is preoccupied with fantasies of success, power, brilliance, beauty, or perfect love.
Believes that they are "special" and can only be understood by or should only associate with other special people (or institutions).
Requires excessive admiration.
Has a sense of entitlement, such as an unreasonable expectation of favorable treatment or compliance with his or her expectations).
Is exploitative and takes advantage of others to achieve their own ends.
Lacks empathy and is unwilling to identify with the needs of others.
Is often envious of others or believes that others are envious of them.
Shows arrogant, haughty behaviors and attitudes
Grandiose sense of self importance:
There is no doubt that Ranpo is incredibly important to the Armed Detective Agency. This is the objective truth. After all, he is a genius and extraordinary detective. Despite this, he does indeed have a grandiose sense of self importance. He often states that his special ability is the best in the whole country, despite not knowing everyone’s abilities (or really caring, for that matter). He sees himself as far above others when it comes to his abilities, and even goes as far as to say that police and other detectives cannot solve a single case without him.
“The police are always so desperate for my help. They can’t capture a single criminal without me. The fact is, my Ultra Deduction is the best ability in this agency. I’m sure it’s the best power in the whole country. It’s no surprise that everyone depends on it.”
Obviously, Ranpo is not needed for every case, and the police can in fact catch criminals without his help. Ranpo goes for extremes and seems to see situations like these in black and white, which is a trait very commonly found in those with NPD.
Ranpo is incredibly confident in his abilities while also not believing that others could ever do the same. When Minoura is doubting Ranpo’s detective abilities, Ranpo decides to put Sukimoto (the police officer that accidentally killed his girlfriend) to the test. He asks the cop to solve the case in 60 seconds, and Sukimoto obviously is stressed and freaks out. Ranpo is confident and sure that the cop will not be able to solve the crime as quickly as he could. While it’s true that most do not have Ranpo’s power of deduction, he is 100% sure that Sukimoto does not have this ability despite not knowing them. He believes his ability is the best in the country, so how could anyone ever compare? Ranpo also seems to enjoy the fact that Sukimoto freaked out, smiling and bringing the timer close to him.
“Nice try, Sergeant. Too bad, you’ve got a ways to go before your case solving skills match mine. But don’t feel bad, you’ve been useful! You’ve helped us prove that Minoura’s best detectives are inferior to me.”
Ranpo makes it clear to others that he is better than them and has absolutely no shame in doing so. This is a VERY common trait in those with grandiose type NPD.
Believes that they are special:
This symptom ties right into the grandiosity. Obviously, Ranpo IS special, but he believes it to an extreme extent. For one, he has a hard time accepting that he is not actually gifted, despite being told by Fukuzawa soon after he originally told him he was. Once it was put into his brain that he had a special ability, there was no going back. Later on he does end up accepting that he does not have an ability (as seen in Dead Apple), but it takes him a little bit to get there. After being in Poe’s novel and Yosano praises him for finally figuring out that he’s not gifted, Ranpo is quick to tell her that he does indeed have a gift, or else he wouldn’t have been able to figure the crime out.
Requires excessive admiration:
Ranpo requires admiration or else he seems to get frustrated. For many narcissists, they need acknowledgment and praise for their achievements or else they get angry/annoyed/frustrated.
In season 1 after the Black Lizard attack at the ADA, several agency members praise Ranpo for his abilities. While he does not specifically seek this out, it is obvious that it feels natural and needed for him.
Has a sense of entitlement:
I would say that the sense of entitlement really ties into the previous symptoms. Ranpo feels entitled and deserving of others’ praise and often seeks for it, especially from Fukuzawa. Another example of Ranpo’s sense of entitlement is shown after the agency is attacked by the Black Lizard in season 1. While everyone else is cleaning up and fixing the agency, Ranpo is just sitting around drinking his soda.
Lacks empathy:
In my humble but very correct opinion, I’d say that Ranpo is entirely lacking in affective empathy. This is made very clear to me through his sense of entitlement and how he often treats others. He definitely does not do it out of malice, but his needs and wants come first.
His motto quite literally is “All’s well that’s well for me”, also translated as “As long as I’m fine, everything’s fine”.
In season 1 when Atsushi is kidnapped, Ranpo does not appear to care in the slightest. He doesn’t believe that the agency should go help, and he is even hesitant to tell others where Atsushi is, despite very much having the ability to figure it out. He believes that it is Atsushi’s problem and not theirs, therefore none of the other agency members including himself should have to help.
And while silly, this is also made clear in the scene where he asks Mushitaro for a piggyback ride. Ranpo sees it as him getting what he needs instead of understanding that’s not really something that you should ask of somebody else, especially not somebody you just met.
Fragile ego:
While this symptom is not present specifically in the DSM diagnostic criteria, it is very common for those with NPD. While people with NPD are often grandiose, those thoughts can easily switch to self judgment and even hatred when something goes wrong.
When Ranpo and Yosano are in Poe’s novel, Ranpo is distraught that he does not have his glasses to activate his ability. He is very agitated and even raises his voice at Yosano. The fact that he thinks he does not have his Ultra Deduction makes him want to do nothing but sit around. He acts as if he can do nothing because of it. This makes it clear that a lot of his energy comes from his confidence in his ability.
Conclusion:
This should be more than enough to convince one that Ranpo fits the criteria for Narcissistic Personality Disorder (and therefore has it).
It is important to note that while Ranpo is entirely lacking in affective empathy, he is able to experience cognitive empathy, though maybe not as often as the average person. There are examples of him experiencing and expressing cognitive empathy in the series, such as when he is talking to young Yosano about joining him and Fukuzawa at the Armed Detective Agency. It is also important to recognize that no form of empathy is required to be a good person. People are defined by their actions, not their feelings (or lack thereof).
While less important, there is still something to say about Ranpo having an equal person. With NPD, there is something called an “equal person” where the narcissist has someone that they see as equal to them – it’s exactly how it sounds. A lot of Ranpo’s grandiosity revolves around his skills as a detective, yet he still had said that Poe’s detective skills blew him away and that he was the only one to have ever done that. While maybe this might not seem like enough to confirm that Poe is his equal person, it certainly sets a basis for it.
#ranpo edogawa#bungo stray dogs#ranpo bsd#npd#npd safe#actually narcissistic#narcissistic personality disorder#edogawa ranpo#bsd ranpo
20 notes
·
View notes