#pathogen identification
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
The food pathogen testing market size is predicted to grow at a CAGR of 8.4% between 2023 and 2028, reaching a value of $22.7 billion by 2028 from a projection of $15.1 billion in 2023.
#Food Pathogen Testing Market#Food Pathogen Testing Market Report#Food Pathogen Testing Market Forecast#Food Pathogen Testing Market Trends#Food Pathogen Testing Market Size#Food Pathogen Testing Industry#Pathogen Detection Services#Microbial Hazard Assessment#Food Safety Verification#Pathogen Outbreak Prevention#Contaminant Testing Solutions#Food Safety Assurance#Pathogen Identification#Microbial Threat Detection#Pathogen Testing Protocols#Food Safety Compliance
0 notes
Text
How does one develop vaccines for emerging infectious diseases?
Emerging infectious diseases pose significant threats to global public health. Rapid and effective development of vaccines is crucial in mitigating the impact of these diseases. This article explores the process of developing vaccines for emerging infectious diseases, highlighting the key steps involved and the challenges faced. Understanding the development process is essential to appreciate the…

View On WordPress
#clinical trials#community immunity#disease outbreak control#Emerging infectious diseases#Equitable access#global health security#multidisciplinary approach#pathogen identification#preclinical studies#preparedness and response#public health collaboration#rapid response#regulatory approval#research and development#safety and efficacy#target antigen selection#vaccine design#vaccine development#Vaccine distribution#vaccine production
1 note
·
View note
Text
"When bloodstream infections set in, fast treatment is crucial — but it can take several days to identify the bacteria responsible. A new, rapid-diagnosis sepsis test could cut down on the wait, reducing testing time from as much as a few days to about 13 hours by cutting out a lengthy blood culturing step, researchers report July 24 [2024] in Nature.
“They are pushing the limits of rapid diagnostics for bloodstream infections,” says Pak Kin Wong, a biomedical engineer at Penn State who was not involved in the research. “They are driving toward a direction that will dramatically improve the clinical management of bloodstream infections and sepsis.”
Sepsis — an immune system overreaction to an infection — is a life-threatening condition that strikes nearly 2 million people per year in the United States, killing more than 250,000 (SN: 5/18/08). The condition can also progress to septic shock, a steep drop in blood pressure that damages the kidneys, lungs, liver and other organs. It can be caused by a broad range of different bacteria, making species identification key for personalized treatment of each patient.
In conventional sepsis testing, the blood collected from the patient must first go through a daylong blood culturing step to grow more bacteria for detection. The sample then goes through a second culture for purification before undergoing testing to find the best treatment. During the two to three days required for testing, patients are placed on broad-spectrum antibiotics — a blunt tool designed to stave off a mystery infection that’s better treated by targeted antibiotics after figuring out the specific bacteria causing the infection.
Nanoengineer Tae Hyun Kim and colleagues found a way around the initial 24-hour blood culture.
The workaround starts by injecting a blood sample with nanoparticles decorated with a peptide designed to bind to a wide range of blood-borne pathogens. Magnets then pull out the nanoparticles, and the bound pathogens come with them. Those bacteria are sent directly to the pure culture. Thanks to this binding and sorting process, the bacteria can grow faster without extraneous components in the sample, like blood cells and the previously given broad-spectrum antibiotics, says Kim, of Seoul National University in South Korea.
Cutting out the initial blood culturing step also relies on a new imaging algorithm, Kim says. To test bacteria’s susceptibility to antibiotics, both are placed in the same environment, and scientists observe if and how the antibiotics stunt the bacteria’s growth or kill them. The team’s image detection algorithm can detect subtler changes than the human eye can. So it can identify the species and antibiotic susceptibility with far fewer bacteria cells than the conventional method, thereby reducing the need for long culture times to produce larger colonies.
Though the new method shows promise, Wong says, any new test carries a risk of false negatives, missing bacteria that are actually present in the bloodstream. That in turn can lead to not treating an active infection, and “undertreatment of bloodstream infection can be fatal,” he says. “While the classical blood culture technique is extremely slow, it is very effective in avoiding false negatives.”
Following their laboratory-based experiments, Kim and colleagues tested their new method clinically, running it in parallel with conventional sepsis testing on 190 hospital patients with suspected infections. The testing obtained a 100 percent match on correct bacterial species identification, the team reports. Though more clinical tests are needed, these accuracy results are encouraging so far, Kim says.
The team is continuing to refine their design in hopes of developing a fully automated sepsis blood test that can quickly produce results, even when hospital laboratories are closed overnight. “We really wanted to commercialize this and really make it happen so that we could make impacts to the patients,” Kim says."
-via Science News, July 24, 2024
#sepsis#medical news#medical testing#south korea#blood test#bacteria#antibiotics#infections#good news#hope#nanotechnology
2K notes
·
View notes
Text

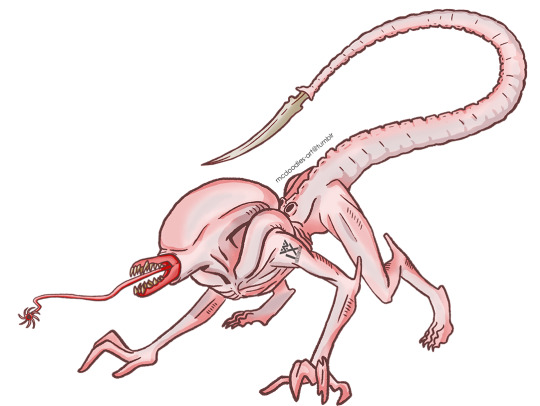
so i redesigned my mutant xenomorph oc after seeing romulus
pls dont repost my art or remove my captions. reblogs help more than likes. <3
large version of the infographic under the cut, with text ID included!
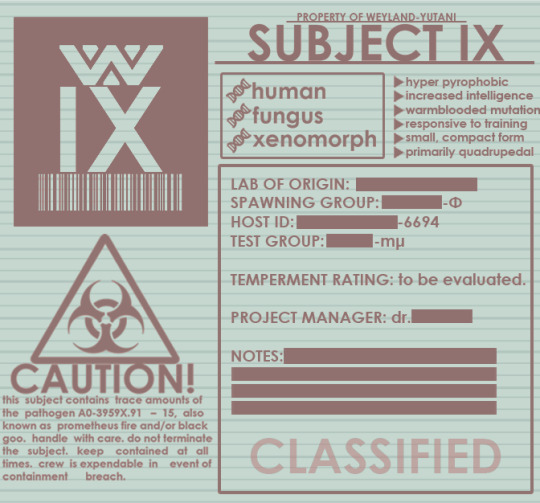
[text ID: Displayed is a series of graphics and data which convey some sense of lore about the oc. From right to left, top to bottom: first, there is the creature's shoulder tattoo design, replete with a Weyland-Yutani corporate logo and an identification barcode. Next, we see the text PROPERTY OF WEYLAND-YUTANI, SUBJECT IX, followed by two lists of traits. The first list is as follows, with a series of bulletpoints represented with DNA strands, to denote the creature's genetics: human, fungus, xenomorph. The second list is represented with generic, triangular bulletpoints and is as follows, hyper pyrophobic, increased intelligence, warblooded mutation, responsive to training, small/compact form, primarily quadrupedal. The next portion of the graphic is below a large biohazard symbol, and reads: CAUTION! this subject contains trace amounts of the pathogen S0-3959X.91-15, aka prometheus fire and/or 'black goo'. handle with care. do not terminate the subject. keep contained at all times. crew is expendable in event of containment breach. the following is a series of generic lab information, most of which is redacted. the artist admits to needing to fill space to make the graphic look nice. rip.]
#xenomorph#alien#alien vs predator#avp#alien romulus#romulus#covenant#prometheus#alien covenant#artists of tumblr#xenomorph oc#xenomorph art
39 notes
·
View notes
Text

Hostile Power Takeover? Learnings on Urban & Domestic Warfare , “PANDEMICS: How We are Spreading Diseases”:
Want to Stop Pandemics?
We Need to Address How Our Systems Contribute to Disease Spread & How It Is Making Pathogens Stronger
1: Understaffing & too much workload
- When it comes to the greatest factor that influences every other issue in preventing the spread of infectious disease in healthcare settings it is workload vs amount of staffing. Overburdening staff results in more medical errors, more issues missed, less time with patients, less time able to be spent per patient, often limited ability to customize treatment plans, less diseases screened for, less infectious control practices used like hand washing, more grouping of sick people in close proximity, using unsafer practices to save time, attempting tasks distracted, & many other sources of both harm & pathogen spread. This issue is inseparable from safety.
2: Need for Universal safety practices in hospital culture
-Often times many hospitals throughout different regions have different training programs with some similar content & some very different content included in their training. There are some safety-related practices that are not taught universally. I think the lack of standardization across the world has really negatively impacted us. As healthcare, healthcare staff, our healthcare buildings change & evolve, these safety practices can get lost along the way.
For example: Pathogens all spread in a certain & defined way based off their characteristics. Some of the more common disease spread through making physical contact with the pathogen (for instance touching something contaminated), touching & inhaling pathogens in droplets, and by breathing in airborne pathogens. BUT, it is important to remember that we often forget that most of the pathogens that make us sick are autonomous & tangible things. They take up space & they move. It is very easy to not see something & not feel it & for it then to be on the bottom list of priorities. Two major examples of often unknown risk are in 2 common practices:
>New Toilets
- A lot of hospitals got rid of toilet lids. Flushing bodily fluids results in those infectious particles going into the air. Disease that weren’t originally airborne would then be airborne. These pathogens can possibly be breathed in. Even if toilets are moved to a different room to protect patients, staff will possibly breathe in these particles.
>Venipuncture?
- You DO NOT need to get a needle stick injury to get a blood borne illness from someone. Drawing blood (specifically winged butterfly sets)produces blood splatter at a significant rate. This means if you were following the disease precautions that we do for everything else, you should be required to wear protective equipment: goggles, disposable gown, & gloves when drawing blood. This is not a standard that is enforced in the culture & many forget or are not aware. (1)
3: Lack of infectious disease teams
- Staff should be dedicated to prevention, control, & monitoring for success in these topics in each hospital. For obvious safety reasons.
4: Disease Screening & Pathogen identification
- Often times screenings are skipped due to patient’s lack of access to healthcare, understaffing, & lack of resources. But there are MANY practices I will continue to advocate for to get funding & to be done around the globe. I’m going to reiterate strongly that not all systems are perfect, but currently the risk for the world is far too high. I’m in favor of universal screening for blood borne disease with at least all inpatient hospital stays and likewise universal testing for respiratory illness is a good approach during “winter seasons”.
- I also think identification of pathogens & their characteristics inside places where healthcare is done is necessary. Reevaluation of cleaning practices is necessary. The level of antibiotic resistance we now see with MRSA or antibiotic resistant staph could happen to ANY other pathogen & we are not taking enough steps to prevent it.
6: Where “Knowledge” Becomes Deadly
- Unfortunately a large proportion of our knowledge comes from observing problems and then frantically attempting to solve them in the middle of a crisis. We have studies on diseases and then we learn & teach everyone based off the most up to date scientific knowledge we have available at that time. I think our understanding of a lot of disease processes & body processes are very incomplete. I also think that people have been steered in a very dangerous direction over the course of history despite ample warning. The specific directions medicine went into for standards of care over history is deeply disturbing & highly suggestive that someone trying to hurt people was attempting to influence the medical sphere by any means necessary including force. Without a full understanding of all the different functions organs do, the standard in medicine many, many years ago became to just start removing things. This became the “gold standard” of care or best practice for a very common problem that can be treated in other & less invasive ways. But since funding, research, & general direction hasn’t been focused on getting more info on specific important topics- these are practices we still do to this day. To reiterate something I said long ago, when someone has a tummy ache, no one actually suggests to take out the stomach. Despite nonstop pushing for more federal regulation, there are still few regulations on supplements. This is dangerous and it’s hard to recommend these type of needed supplements when they are not standardized across the board in regards to their safety. All your organs do multiple things. If you take any out or damage them you will need some type of “replacement therapy” to feel normal again. The issue is that primarily books & research inform healthcare worker education. But if no one will fund the research or investigate specific topics, the interventions & meds that help never get taught. It’s not that the interventions don’t work, it’s just that someone established the norm to be the most painful/hardest on your body type treatment. I reiterate, that seems HIGHLY suspect for something being wrong in multiple domains to get us to this point.
There are forces trying to take us down a dark path & I continually hope it isn’t too late to prevent harm in all domains of our lives. I debate with myself about including links with each post due to how cluttered it gets. But I think it’s incredibly uncomfortable topics like drawing people’s blood has a somewhat unknown & higher risk for pathogen exposure than people say that’s been demonstrated in research & people don’t make a bigger deal about it. It’s hard information to find on google & many hospital cultures do not emphasize its dangers in the same way even that we do towards MRSA. It’s incredibly uncomfortable reality to find ourselves in, but something’s got to change.
(1) https://www.sciencedirect.com/science/article/abs/pii/S0196655308005427
#disease#pathogen#doctor#nurse#registered nurse#nurse practitioner#nursing#nurselife#physician assistant#physician#md#rn#pa#meds#medication#medicare#medical#medicine#hospital#pain#chronic illness#chronic pain#chronically ill#chronic fatigue#pandemic
9 notes
·
View notes
Link
The introduction of Full Laboratory Automations has served to revolutionize the workflows of labs worldwide, helping with the automation of routine tasks and the capacity for digital analysis of the results. However, a significant limitation is the inability to identify and interpret bacterial cultures, a task that is considered essential in the field of microbiology and diagnostics. A group of researchers from the University of Brescia seeks to remedy this with the introduction of a new deep-learning model, “DeepColony,” that can help with culture interpretation and quantification.
Despite the introduction of several new techniques in microbiology labs all over the world, the practice of bacterial culture and interpretation is still the primary method for diagnosing the presence of infectious pathogens. There are many reasons for its popularity, simplicity, and cost efficiency being prime among them. However, despite all of the advantages it offers, the interpretation of cultures accurately still remains a challenging task, prone to human error and constrained by the availability of qualified and experienced staff. Though other tasks requiring visual interpretation, such as cytology and hematology, have since been automated through the use of machine learning algorithms, bacterial culture remains unchanged for the most part.
Considering this lack of resources, the creation and development of Full Laboratory Automation systems have allowed for the automation and digitization of various steps involved in culturing, such as processing, streaking, and incubation, at the end of which images are uploaded for analysis. This has helped with the reduction of turn-around times, better efficiency and quality, as well as lower costs. However, the interpretation of these images still remains a significant challenge. While prior image analysis tools have been created for certain specific scenarios, these aren’t as helpful for other circumstances. The need for a generalized image analysis tool capable of consistent interpretations is great.
Continue Reading
26 notes
·
View notes
Text
The T Cell Landscape
T cells, a critical component of the adaptive immune system, stand as the body's elite force in combatting infections and diseases. These specialized lymphocytes boast remarkable diversity, each type playing a distinct role in orchestrating a targeted and effective immune response.
T cells, like all blood cells, originate from hematopoietic stem cells residing in the bone marrow. However, their training ground lies within the thymus, a specialized organ located in the chest. Here, they undergo a rigorous selection process known as thymocyte education. During this process, immature T cells, called thymocytes, are presented with self-antigens (molecules unique to the body) by special cells. Thymocytes that bind too strongly to these self-antigens are eliminated, preventing them from attacking healthy tissues later. Only thymocytes that demonstrate the ability to recognize foreign invaders while exhibiting tolerance to self are released into the bloodstream as mature T cells.
Following this rigorous training, mature T cells exit the thymus and embark on their patrol, circulating throughout the bloodstream and lymphatic system. They remain vigilant, constantly scanning for their specific targets – antigens. Antigens are foreign molecules, such as fragments of viruses, bacteria, or even cancerous cells, that trigger the immune response.
The hallmark of a T cell is its T cell receptor (TCR), a highly specialized protein complex embedded on its surface. This receptor acts like a lock, uniquely shaped to fit a specific antigen, the "key." Each T cell develops a unique TCR capable of recognizing only a single antigen, enabling a highly specific immune response.
But how do T cells encounter these hidden antigens lurking within infected or cancerous cells? This critical role is played by antigen-presenting cells (APCs). APCs, such as macrophages and dendritic cells, engulf pathogens or abnormal cells, break them down into smaller fragments (peptides), and present them on their surface complexed with major histocompatibility complex (MHC) molecules. MHC molecules act as identification tags, allowing T cells to distinguish between "self" and "non-self." When a T cell's TCR encounters its specific antigen bound to an MHC molecule on an APC, a dance of activation begins. The T cell becomes stimulated, and a cascade of signaling events is triggered. This leads to the T cell's proliferation, producing an army of clones specifically tailored to combat the recognized threat.
T cells are not a single, monolithic entity. They comprise a diverse population, each type with a specialized function:
Helper T Cells (Th Cells):
Helper T cells, often abbreviated as Th cells, play a central role in coordinating immune responses. They express the CD4 surface marker and can recognize antigens presented by major histocompatibility complex class II (MHC-II) molecules. Subtypes of helper T cells include Th1, Th2, Th17, and regulatory T cells (Tregs), each with distinct functions and cytokine profiles.
Th1 cells mediate cellular immunity by activating macrophages and cytotoxic T cells, crucial for defense against intracellular pathogens.
Th2 cells are involved in humoral immunity, promoting B cell activation and antibody production, thus aiding in defense against extracellular parasites.
Th17 cells contribute to the immune response against extracellular bacteria and fungi, producing pro-inflammatory cytokines. Regulatory T cells (Tregs) maintain immune tolerance and prevent autoimmunity by suppressing excessive immune responses.
Cytotoxic T Cells (Tc Cells):
Cytotoxic T cells, also known as Tc cells or CD8+ T cells, are effector cells responsible for directly killing infected or aberrant cells. They recognize antigens presented by MHC class I molecules on the surface of target cells. Upon activation, cytotoxic T cells release perforin and granzymes, inducing apoptosis in target cells and eliminating the threat.
Memory T Cells:
Memory T cells are a long-lived subset of T cells that persist after the clearance of an infection. They provide rapid and enhanced immune responses upon re-exposure to the same antigen, conferring immunological memory. Memory T cells can be either central memory T cells (TCM), residing in lymphoid organs, or effector memory T cells (TEM), circulating in peripheral tissues.
γδ T Cells:
Unlike conventional αβ T cells, γδ T cells express a distinct T cell receptor (TCR) composed of γ and δ chains. They recognize non-peptide antigens, such as lipids and metabolites, and are involved in immune surveillance at epithelial barriers and responses to stress signals.
Beyond the Battlefield: The Expanding Roles of T Cells: The remarkable capabilities of T cells have opened doors for several groundbreaking applications in medicine:
Vaccines: By presenting weakened or inactivated forms of pathogens, vaccines "train" the immune system to generate memory T cells. This prepares the body to recognize and rapidly eliminate the real pathogen upon future exposure, preventing disease.
Cancer immunotherapy: CAR T-cell therapy, a revolutionary approach, genetically engineers a patient's own T cells to express chimeric antigen receptors (CARs) that recognize and target specific cancer cells. These "supercharged" T cells are then reintroduced into the patient, unleashing a potent attack against the tumor.
Autoimmune disease treatment: Researchers are exploring ways to manipulate T cells to suppress harmful immune responses that underlie autoimmune diseases like rheumatoid arthritis and multiple sclerosis.
The diverse array of T cells underscores the immune system's complexity and adaptability in mounting tailored responses against a myriad of threats. From orchestrating immune reactions to maintaining tolerance and establishing long-term immunity, T cells play multifaceted roles in safeguarding the body's health. Understanding the intricacies of T cell biology not only sheds light on immune-mediated diseases but also paves the way for developing novel therapeutic strategies harnessing the power of the immune system.
T cells represent a fascinating aspect of immunology, with their diversity and specificity driving the complexity of immune responses. As research advances, further insights into T cell biology promise to revolutionize immunotherapy and enhance our ability to combat diseases ranging from infections to cancer. By understanding and harnessing their power, we can unlock new avenues for protecting and improving human health.
#science sculpt#life science#science#molecular biology#biology#biotechnology#artists on tumblr#t cells#T helper cells#autoimmune#autoimmunity#helathcare#immunology#immunotherapy#medical care#cancer#human health#research#scientific research#the glass scientists#scientific illustration#research scientist
11 notes
·
View notes
Text
Gram-Stained Sputum: Abundant Pus Cells & Gram-Negative Diplococci

This Gram-stained smear of sputum shows plenty of pus cells alongside Gram-negative diplococci, a key indicator in diagnosing bacterial respiratory infections such as pneumonia. The presence of abundant pus cells suggests an active immune response, while the identification of Gram-negative diplococci points towards specific pathogens like Neisseria or Moraxella species. Understanding these characteristics in Gram staining is crucial for accurate diagnosis and treatment.
#LabScience #Microbiology #GramStain #PusCells #GramNegative #Diplococci #MedicalLab #ClinicalDiagnostics #RespiratoryInfections #LabNotes
"Plenty of pus cells and Gram negative diplococci in Gram stained smear of sputum" by Ajay Kumar Chaurasiya is licensed under CC BY-SA 4.0.
#medical laboratory science#science#microbiology#bacteria#bacteriology#biology#med student#medicine#medical students#lungs#respiratoryhealth
3 notes
·
View notes
Text
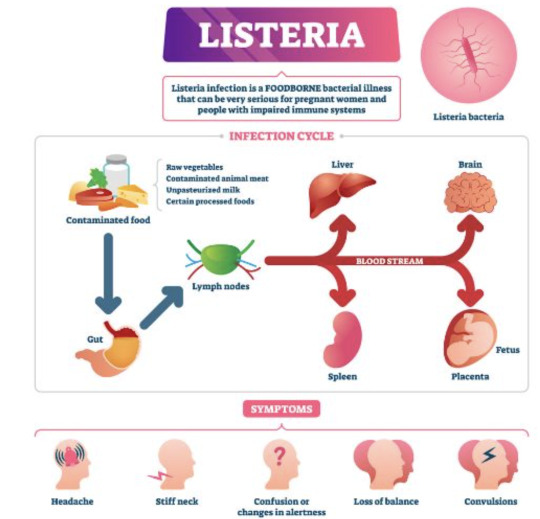
Listeria
For whatever reason it reminds me of Desperate Housewives and Wisteria lane. Or just Wisteria in general.

It's unfortunately it's anything but wistful or romantic.
This is inspired by the netflix series Poisoned. I hate that title but it's a great watch. I learned a lot from it. I highly recommend it particularly for medical students and residents etc.
So, listeria are gram positive rods (most bacilli are negative) making this relatively easier to remember (purple rods). Also catalase positive. IT's also a facultative anaerobe - so both cultures may be positive (aerobic and anaerobic bottles).

the species that is the culprit for major human pathogens is Listeria monocytogenes.
At increased risk groups (more likely to die of Listeriosis) - the immunocompromised and extremes of life, including the elderly, pregnant women and neonates. Immunocompromised: HIV, anyone on long term highish doses of steroids, leukaemia/oncology patients etc. Worryingly, incubation time is 3-90 days in these groups, so it's difficult to really trace or keep track of. Pregnant women are at 20x higher risk of acquiring the severe form.
Source: CDC

Hence why during pregnancy you're advised not to consume raw salads, fruits, cold cuts, soft cheeses, sprouts and smoked salmon or sushi, no mayo and no raw egg (definitely no raw milk) etc. Similarly, common recommendation is you serve none of these to children under the age of 1. It naturally lives in soil (hence avoidance of raw sprouts) and can live in animals. So it can frequently contaminate food.
Image Source: SA Health

As with COVID (I can't believe I'm using COVID as a measure of things), it can cause mild food borne illness (nausea, vomiting diarrhoea, myalgias, even fevers) to invasive disease causing sepsis and even meningitis or encephalitis. Incubation time is a few days in the mild form.
IMage source:
Death by Listeria when you have the severe form (Listeriosis) is 20%, astonishingly high given you have a 1% chance of dying from Salmonella.
It's a small risk but the issue is that complications and fatality if you do acquire is high. It's also highly preventable, but the challenge is food safety and avoiding certain foods as a consumer.
i.e. in pregnancy, most will have diarrhoeal illness that's mild. But in the subset that get invasive disease and really unwell, there's a 20% risk of miscarriage, risk of premature labour and risk of still birth at 3% in the US. In the states, pregnant women are also 10x more likely to get Listeria infection. That is, illness after exposure.
On the final note of prevention, also always properly refridgerate food to 4 degrees celsius and cook meat to 165 fahrenheit or 73 degrees celsius. As I've learned from the Poisoned documentary, you can ask restaurants to do this, ask them to use an internal thermometer to measure - as rare/medium rare etc have no meaning as it pertains to food safety. If they can't, order something else.

With meningoencephalitis, we just presume that Listeria is a possibility and treat empirically while awaiting investigations.
Investigations: - CSF (lumbar puncture) in event of signs of meningism or encephalitis (classic headache/fever/stiff neck/rash and/or acute confusion or seizure AND fevers) --> expect the classic features of bacterial meningiits and gram stain positive for purple rods - PCR - stool cultures have no value - blood cultures--> look for gram positive rods in the preliminary findings, expect a call from the lab Empirical therapy: - none in asymptomatic or mild disease. just monitoring until symptoms resolve and supportive care (fluids etc.) - Listeria is a notifiable disease to the health department in most Western countries that keep track of outbreaks. - in the US, standard treatment is ampicillin. - in Australia at least, standard therapy is IV benzylpenicillin, 2.4 g 4 hrly in meningitis or encephalitis and everyone is just started on this until bug identification/gram staining and sensitivities return. - in hypersensitivity, bactrim is used. - cephalosporins have no activity against them (or "inherently resistant), hence you can see IV ceftriaxone and benzylpen in the drug regimen for empirical therapy of meningitis - cef covers gram negatives, strep pneumo (most common cause of meningitis) and neisseria meningitidis - duration of therapy in severe disease: 3 weeks, 6 weeks if immunosuppressed
Really great summary here.
Random historical trivia
listeria is named for Dr. Joseph Lister, a British surgeon who introduced sterilisation of equipment and antiseptics to surgery, improve post op care and observed that microbes are the cause of cases of poor wound healing or post op infections. he also began to look at them under the microscope as an early pioneer of bacteriology.

Lister's father by the way, made compound microscopes for a living, so lister became proficient at using this and started publishing articles during medical school
this also led to a lot more research on inflammation and coagulation
weirder trivia: in his med school days, surgeons commonly did not wash hands between patients and some didn't even change gowns, glorifying how busy they where by how many stains were on it by the end of the day
so unsurprisingly his early battles to pioneer antiseptics and aseptic techqniues to prevent the transmission of infection in surgical patients were pretty uphill
Resources CDC guidelines WHO guidelines FDA Statpearls --> great at covering basic physiology and pathology etc. in a short form. Australian therapeutic guidelines - unfortunately not free.. so won't bother to link. If you work at any large-ish Australian hospital you'll have 'free' access. Wikipaedia US list of outbreaks CDC recommendations on foods to avoid vs okay to eat to avoid Listeria
7 notes
·
View notes
Text
Phytosanitary Sciences
In the field of plant health, there are several specialized sub-disciplines that focus on different aspects of plant well-being. Each of these areas has a specific focus and employs distinct techniques and knowledge to address issues related to plant diseases, pests, and other conditions affecting plants. Here are some of the key sub-disciplines:

Phytopathology
Definition: Phytopathology is the study of plant diseases caused by pathogens, including fungi, bacteria, viruses, and nematodes. Focus: Identification and characterization of pathogens, mechanisms of infection, disease epidemiology, and control strategies. Activities: Disease diagnosis, development of control methods (chemical, biological, and cultural), and development of resistant plant varieties.
Nematology
Definition: Nematology is the study of nematodes, small cylindrical worms that can parasitize plants and cause significant damage. Focus: Identification of nematode species, effects on plants, and development of control methods. Activities: Diagnosis of infestations, control of nematodes through physical, chemical, and biological methods, and research on plant resistance.
Agricultural Entomology
Definition: Agricultural entomology is the study of insects that affect plants, both as pests and in their interactions with crops. Focus: Identification of insect pests, their biology and behavior, and development of control methods. Activities: Monitoring insect populations, integrated pest management (IPM), and development of sustainable management strategies.
Plant Virology
Definition: Plant virology is the study of viruses that infect plants. Focus: Identification and characterization of viruses, their life cycles, and infection mechanisms. Activities: Diagnosis of viral infections, development of vaccines and control methods, and research on viral resistance.
Plant Bacteriology
Definition: Plant bacteriology is the study of bacteria that cause diseases in plants. Focus: Identification of pathogenic bacteria, understanding infection mechanisms, and development of control strategies. Activities: Diagnosis of bacterial diseases, chemical and biological control, and development of management practices.
Agricultural Mycology
Definition: Agricultural mycology is the study of fungi that affect plants. Focus: Identification and characterization of pathogenic fungi, infection mechanisms, and control. Activities: Diagnosis of fungal diseases, development of fungicides and cultural practices for control, and research on resistance to fungi
Phytosociology
Definition: Phytosociology studies the structure and dynamics of plant communities in relation to environmental conditions and biotic factors. Focus: Analysis of interactions between different plant species and their environments. Activities: Study of plant community diversity and composition, and their responses to environmental changes and management
Agroecology
Definition: Agroecology applies ecological principles to agriculture to promote sustainable farming systems. Focus: Integration of agricultural practices with environmental conservation and promoting sustainability. Activities: Development of sustainable management techniques and study of interactions between agricultural systems and the environment.
Plant Genetics and Breeding
Definition: Plant breeding involves selecting and creating plant varieties with desirable traits, such as disease and pest resistance. Focus: Development of cultivars with genetic resistance to pathogens and pests. Activities: Research and development of new varieties, and application of biotechnological techniques to improve plant resistance.
These areas are interdependent and often overlap, with many collaborating to address complex issues related to plant health and sustainable agricultural production.
#agriculture#plant health#Phytosanitary#pest control#plant science#agriculturalsolutions#pathology#Nematology#entomology#agroecology#botany#plants#mycology#Sustainable#agronomia#agro#agronomist#agronomy
3 notes
·
View notes
Text
Higurashi: Festival Accompanying Chapter 14
Wind is a recurring word this chapter. It's even part of the chapter title "A New Wind". More specifically, wind is being used as a metaphor for change. For the village, the changing winds blowing away the stagnant air is a good thing, but for Takano, the winds of change are only cruel.
In Eye-Opening chapter 8, Mion said she confronted Oryou over Satoshi's disappearance and now we got to see the effects of that. Oryou has built a reputation as a cruel and unyielding woman and much of the Sonozaki reputation comes from their leaders being feared as ruthless.
But here, just like in Massacre, we get a glimpse at her kinder side that she doesn't let anyone see. She was probably moved by how her actions upset Mion so much. And I wouldn't be surprised if she's just as upset for Shion as well.
But since Oryou can't just change, she needs to bring in someone new who can be the catalyst for change.

We have the moment where Ichiro Maebara decided to move to Hinamizawa. The wildest thing is he was so close to deciding against moving to the village because there is nothing there only to see children laughing and playing in the field.
There's something kinda mystical to me about this one panel:

Notice that Rika and Hanyu's bodies aren't in the panel itself. It's not uncommon to draw various people or objects extending beyond the border of a panel, but this perspective makes it look like Rika and Hanyu aren't part of the panel at all. It feels less like they're playing in the grass and more like they're playing on the page itself.
As beings who have been able to exist outside time and space, it feels appropriate that they could potentially escape the scene and be in a space that is a little closer to us than to the people in the story.
I kind of like to imagine that's what's happening here. Hanyu has never interacted with any of the previous worlds but here she is laughing, smiling, playing, and interacting with others. I like to imagine she brought herself and Rika into this very moment so they could talk to Ichiro and convince him to move to Hinamizawa. And this moment was so powerful that it echoed into every other timeline that Keiichi moved into Hinamizawa. After all, Ichiro mentioned this moment to Keiichi in Atonement chapter 12.
Ichiro is looking for a place to start over. He feels he's failed as a parent because he never noticed how much pressure he was putting on his son. And Rika has given him the assurance that this village is both a place where Keiichi can start over, be happy, and where his family can provide something new to the village. But more importantly, Keiichi can find friends here.

Imagine if Ichiro realized Rika knew his name without asking and decided to not move in cause that moment freaked him out.
As the winds of change blow in Rika's favor, they also blow against Takano. The progress of her research takes a sudden turn with Koizumi's death.
With his death came a great factional dispute and political upheaval within Tokyo and the direction of Takano's research is greatly changed. Tokyo has decided to immediately end the research into the military use of Hinamizawa Syndrome while giving them three years to conclude their research into the cure and eradication of the disease.
Honestly, this is a good thing. This is what disease and parasite research should be about. Them being given three years to conclude their research is proof that the heads at Tokyo acknowledge Hinamizawa Syndrome is a general, though not critical, health concern and they're providing the means to investigate and cure it.
The Irie Institute has already accomplished some of the most important tasks: pathogen identification, symptom identification, and early clinical trials. At this point, all that's left to do is further refine the cure which would might include things like antibody research and vaccination.
Honestly, I think Koizumi was just a giant warmonger still salty over losing WWII. The only reason Hinamizawa Syndrome research gained such traction was because he was an influential figure who both appealed to similarly salty warmongers and he probably knew how to rile up a colossal tall tale while keeping any detractors from having a voice.
With him dead, the people who either didn't fall for his words or understood the dangers of biological warfare were able to take the reigns. I can't exactly say if the new heads of Tokyo are more peace-seeking than the Tokyo Koizumi influenced, but they are at least more reasonable with respect to what Hinamizawa Syndrome is.
Of course, the problem is that Takano won't settle for anything less than reshaping the world in (what she thinks is) her grandfather's image. I'm sure any research group would be devastated to learn the work they've spent years on is going to be thrown out, but Takano's problem is she won't settle for a humble godhood where she saved a village from a horrible disease. She wants to be a god who reshaped the very nature of humanity.
back
2 notes
·
View notes
Text
Pneumonia In Children And Adults

Introduction
Pneumonia stands as a prevalent respiratory infection, exerting a significant burden on global public health. Its impact extends beyond mere morbidity, contributing to substantial healthcare costs and socioeconomic consequences. This discussion aims to elucidate the general nature of pneumonia, encompassing its pathophysiology, clinical presentation, diagnostic modalities, treatment strategies, complications, and preventive measures. By indulging into these factors, we aim to provide a better understanding of pneumonia’s complexity and underscore the importance of timely recognition and management.
Pathophysiology

Pneumonia ensues from the infiltration of infectious agents, including bacteria, viruses, fungi, and less commonly, parasites, into the lower respiratory tract. Upon inhalation or aspiration of these pathogens, they gain access to the alveoli, where they incite an inflammatory response. This inflammatory cascade triggers the release of pro-inflammatory cytokines and chemokines, recruiting immune cells to the site of infection. Neutrophils, macrophages, and lymphocytes converge to eradicate the invading pathogens, leading to the characteristic consolidation and exudate formation within the affected lung tissue. As the infection progresses, alveolar edema, impaired gas exchange, and parenchymal damage ensue, culminating in the clinical manifestations of pneumonia.
Clinical Presentation

The clinical presentation of pneumonia encompasses a spectrum of symptoms, ranging from mild respiratory complaints to life-threatening respiratory failure. Common symptoms include cough, productive sputum production, fever, chills, pleuritic chest pain, dyspnea, tachypnea, and systemic manifestations such as malaise and fatigue. The severity of symptoms varies depending on factors such as the underlying pathogen, the extent of lung involvement, the host’s immune status, and comorbidities. In pediatric populations, pneumonia may present with nonspecific symptoms such as feeding difficulties, lethargy, and irritability, posing diagnostic challenges. Conversely, elderly individuals may exhibit atypical presentations characterized by confusion, hypothermia, and exacerbations of underlying chronic conditions.
Diagnostic Modalities

The diagnosis of pneumonia hinges on a comprehensive clinical assessment, augmented by various diagnostic modalities to confirm the presence of pulmonary infection and reveal its etiology. A thorough history and physical examination provide invaluable insights into the patient’s symptomatology, risk factors, and clinical trajectory. Symptomatic findings such as crackles, wheezes, and diminished breath sounds may aid in localizing the site of infection and assessing disease severity. Radiographic imaging, notably chest X-rays and computed tomography (CT) scans, serves as the cornerstone of pneumonia diagnosis, revealing characteristic radiographic findings such as airspace opacities, lobar consolidation, and interstitial infiltrates. Laboratory investigations, including complete blood count (CBC), C-reactive protein (CRP), and procalcitonin levels, may corroborate the clinical suspicion of pneumonia and guide therapeutic decisions. Additionally, microbiological testing of respiratory specimens through techniques such as sputum culture, blood cultures, and polymerase chain reaction (PCR) assays facilitates pathogen identification and antimicrobial susceptibility testing, thereby informing targeted therapy.
Treatment Strategies

The management of pneumonia hinges on prompt initiation of empiric antimicrobial therapy tailored to the likely causative pathogen(s) and disease severity. Antibiotics represent the mainstay of treatment for bacterial pneumonia, with the choice of agent dictated by factors such as local antimicrobial resistance patterns, patient age, comorbidities, and recent antibiotic exposure. Commonly prescribed antibiotics include beta-lactam agents (e.g., penicillins, cephalosporins), macrolides, fluoroquinolones, and combination regimens for severe or healthcare-associated infections. Conversely, viral pneumonia necessitates supportive care measures, given the limited efficacy of antiviral agents in most cases. Influenza-associated pneumonia may benefit from neuraminidase inhibitors such as oseltamivir, while respiratory syncytial virus (RSV) pneumonia may warrant ribavirin therapy in select cases. Adjunctive therapies such as oxygen supplementation, bronchodilators, and corticosteroids may mitigate respiratory distress and improve clinical outcomes, particularly in severe or hypoxemic patients. The duration of antimicrobial therapy varies depending on factors such as the causative pathogen, clinical response, radiographic resolution, and the presence of complications. Close monitoring of clinical parameters and serial imaging studies guide the decision-making process, enabling clinicians to tailor therapy to individual patient needs.
Complications

Pneumonia harbors the potential for various complications, ranging from mild to life-threatening sequelae, necessitating vigilant monitoring and timely intervention. Common complications include pleural effusion, empyema, lung abscess, respiratory failure, septic shock, and acute respiratory distress syndrome (ARDS). Pleural effusion denotes the accumulation of fluid within the pleural space, secondary to inflammation or impaired lymphatic drainage, manifesting as dyspnea, pleuritic chest pain, and dullness to percussion on physical examination. Empyema represents a purulent collection within the pleural cavity, often complicating bacterial pneumonia and necessitating drainage via thoracentesis or chest tube placement. Lung abscesses manifest as circumscribed cavities containing necrotic debris and pus within the lung parenchyma, triggered by persistent fever, productive cough, and hemoptysis. Respiratory failure ensues from impaired gas exchange and alveolar hypoventilation, caused by worsening hypoxemia, hypercapnia, and respiratory acidosis, necessitating mechanical ventilation and intensive care support. Septic shock represents a life-threatening complication of severe pneumonia, characterized by systemic inflammatory response syndrome (SIRS) and end-organ dysfunction, requiring aggressive fluid resuscitation, vasopressor therapy, and broad-spectrum antibiotics. ARDS denotes a severe form of acute lung injury, characterized by diffuse alveolar damage, refractory hypoxemia, and bilateral infiltrates on chest imaging, necessitating lung-protective ventilation and supportive care in the intensive care unit (ICU). The occurrence of complications portends a poor prognosis and underscores the need for early recognition and intervention to mitigate adverse outcomes.
Preventive Measures

Preventing pneumonia entails a broad approach encompassing vaccination, infection control measures, and health promotion strategies aimed at reducing the risk of respiratory infections and their sequelae. Vaccination stands as a cornerstone of pneumonia prevention, targeting common bacterial and viral pathogens implicated in pneumonia pathogenesis. Vaccines such as the pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23) confer protection against Streptococcus pneumoniae, the leading bacterial cause of pneumonia, particularly in high-risk populations such as young children, older adults, and immunocompromised individuals. Influenza vaccination remains paramount in mitigating influenza-associated pneumonia and reducing disease transmission, underscoring the importance of annual vaccination campaigns targeting vulnerable populations. Additionally, adherence to infection control measures, including hand hygiene, respiratory etiquette, and environmental sanitation, plays a pivotal role in reducing the spread of respiratory pathogens in healthcare settings and the community at large. Health promotion efforts aimed at smoking cessation, optimizing nutrition, and addressing underlying comorbidities such as chronic obstructive pulmonary disease (COPD), asthma, and immunodeficiency bolster immune resilience and mitigate pneumonia risk. Furthermore, early identification and management of predisposing factors such as malnutrition, homelessness, and overcrowded living conditions attenuate pneumonia susceptibility and enhance overall health outcomes.
Conclusion
In conclusion, pneumonia emerges as a formidable respiratory infection, posing significant challenges to global public health. Its diverse etiology, clinical manifestations, diagnostic modalities, treatment modalities, complications, and preventive measures underscore the nature of pneumonia management. Timely recognition and intervention are imperative in mitigating the morbidity and mortality associated with pneumonia, necessitating a collaborative approach among healthcare providers, public health authorities, and policymakers. By fostering a comprehensive understanding of pneumonia’s manifest and implementing evidence-based strategies, we can strive towards reducing its burden and improving patient outcomes. Through ongoing research, education, and advocacy efforts, we can envision a future where pneumonia-related morbidity and mortality are substantially diminished, paving the way for enhanced respiratory health and well-being worldwide.
In managing pneumonia, compassion, empathy, and a holistic approach are essential alongside clinical expertise. Striving for excellence in knowledge and practice allows us to enhance respiratory medicine and patient outcomes.
As we address pneumonia and broader cardiovascular health complexities, let’s remain committed to optimal patient care. Together, we can impact lives positively and foster a healthier future.
Medical students encounter significant academic challenges during their studies, balancing coursework, clinical rotations, research, and personal commitments. Expert Academic Assignment Help offers tailored assistance to meet their needs, providing study materials, tutoring, assignment help, and exam preparation. Beyond academics, it fosters a supportive environment for mentorship and guidance. In essence, Expert Academic Assignment Help is a valuable resource for medical students, empowering them to excel academically and develop into competent healthcare professionals. Contact us at [email protected] for professional assistance
#assignment help#medical students#healthcare#nursing school#nursing student#medicine#medical help#academic assignments#university student#medical university#university life#university#student#student life#study blog#study inspiration#studyblr community#studyblr#study motivation#medication#medical student#medical school#medicare#writing#writers on tumblr#writerscommunity#writeblr#online writing#academic writing
2 notes
·
View notes
Text
I’ve been losing motivation in school lately and thinking a lot about why I want to go into biology research anyway. I’ve come to this conclusion before and I’m sure I’ll have to come to it again, but for me it’s ultimately a matter of being able to appreciate living things. I may gain and lose interest in specific subjects, but life will always matter to me. I could say it’s because we’re all alive together in this confusing, dangerous world, and for all we hurt and exploit each other, we all share a common history and a common goal, and all life deserves respect and appreciation, and that would be a nice sentiment, but it’s not the reason I like life. If it were, then it would be dependent on a single perspective, a single model of the world. But the models are what we build to explain and communicate our experiences. They do crosstalk with and influence our perceptions of those experiences, and they are instrumental in our ability to do anything productive with them, but they can only justify action in and of themselves so long as they are believed unquestioningly—and I think no belief should be beyond questioning. The reason I get invested in learning about life is the same reason I get invested in anyone or anything—because, in one way or another, I can relate to it. I can share the calm contentedness of a purring cat. I can wonder at what it would be like to be a bee, or an ant, or a wasp. I can take comfort in the steady, patient presence of a tree. I can be inspired by my own immune system’s ability to adapt and remember, and to strike a dynamic balance between self-defense and tolerance, while warily admiring the strategies which pathogens have developed to subvert it. And I can look at any living organism and know that, for all our differences, we share the same fundamental building blocks; we share a common ancestor and were shaped by common patterns and processes. And this is why I want to study biology—because primarily, I love life. And I don’t have to go into research, even if it is what I’ve decided to pursue and what I’ve been working towards since high school. Because life is always there, and I have always found ways to appreciate it. And I have set myself on this path, and given myself the chance to pursue a career in microbiology research, and I only got this far because, for better or worse, I did build myself a scaffold of unwavering belief—but I could not have maintained it if it did not rest on a foundation of fundamental identification with and appreciation for life. I don’t really know whether research is the best path for me anymore. I have a lot of respect for science as a tool for understanding the world, and I’d like to believe I could contribute to that work. I know it won’t be easy. I hope it could be worth it, and for now, I’ll do what I can to maintain that hope and work towards realizing it. But no matter what I decide to do, I want to be able to keep learning about and appreciating life, in whatever form that may end up taking.
#personal stuff#school#life#biology#self reflection#this is what reading burke and sartre and touching grass does to an overwhelmed bio major#homeostasister’s journey of self discovery
3 notes
·
View notes
Note
Hello! I was wondering if you could you talk a little about types of careers that have to do with botany, ecology, ethnobotany, etc? I do native plant landscaping and love it but I don't think it's a long-term option because it's hard on the body. I'm wondering what I can do next but my undergrad isn't related to any of this. What are some examples of jobs and what experience/degrees do they require? Are there options outside of academia? Thank you!
This is a tough question - both of us took the academic track in botany initially, and one of us is still a botanist! A lot of ecology/biology/botany jobs do want some sort of degree, although for some positions a general biology B.S. or even an associate's degree will work.
However, you have some experience with native plants from your current job, so it's possible you might be able to find something related to native plant ecology. You might potentially look into wetland delineation or a similar industry job that involves knowledge of native plants. There are a number of other ecology jobs related to botany in industry that you might be able to pursue with your experience, although they might be fairly entry-level. Friends of mine without a deep background in academia have gone into pathogen identification at plant nurseries and seed identification for independent laboratories that test nursery stock.
If you have experience with GIS programs, such as QGIS and ArcGIS, you may be able to find a GIS-related role at a university or botanical garden, too.
Volunteering can be a good way to network, although in our opinion, a lot of the best volunteer opportunities will be through academia. Botany labs and herbaria often have trouble finding volunteers, because quite simply, there are a lot of "sexier" volunteer opportunities offered by large carnivore research teams! Who doesn't want to collar grey wolves, after all?! University volunteer programs frequently email job listings to volunteer mailing lists, and if you participate in group activities, other volunteers, professors, and herbarium curators might have some job opportunity tips as well.
We also won't discount the option to go back into academia and get a master's degree or doctorate, too. We'd suggest volunteering in tandem, because this can be a great way to get really powerful references if you don't have any in the field already. If you do this, be sure to tour the universities and meet one-on-one with the advisor and program members you'd be working with. Unfortunately, if you're in the United States, studying for the Graduate Record Exam (GRE) can be rather tedious, the test itself is expensive, and academic job simply do not way well, so we understand why someone would avoid this route.
We would advise staying away from bushcraft and herbalism. There's a lot of pseudoscience and overexploitation of plants occurring in these practices right now.
14 notes
·
View notes
Text
Unveiling the Microscopic World: Exploring B.Sc Medical Microbiology in Dehradun
Microbiology, the study of microscopic organisms, is a field that holds the key to solving mysteries at the cellular level. The pursuit of knowledge in this domain becomes all the more captivating in the picturesque city of Dehradun, which is well-known for its educational institutions. This article explores the field of B.Sc. Medical Microbiology, highlighting the offerings of the top colleges in Dehradun and providing information on the course details, eligibility requirements, and the invaluable contributions of the college forum.
B.Sc Medical Microbiology: A Glimpse into the Microbial World:
Understanding Microorganisms: The B.Sc Medical Microbiology program is designed to provide students with a comprehensive understanding of bacteria, viruses, fungi, and other microorganisms. It forms the foundation for exploring their roles in health, disease, and the environment.
Clinical Applications: Medical Microbiology goes beyond laboratory studies; it extends into clinical applications, involving the identification, prevention, and control of infectious diseases. Students delve into the practical aspects of diagnostic procedures and microbiological techniques.
Immunology and Public Health: The curriculum often includes in-depth modules on immunology, emphasizing the body's defense mechanisms against pathogens. Additionally, students gain insights into public health aspects, learning how microbiology plays a pivotal role in disease prevention and control.
Eligibility Criteria for B.Sc Medical Microbiology:
To embark on the journey of unraveling the microbial world through B.Sc Medical Microbiology in Dehradun, prospective students must fulfill the following eligibility criteria:
Educational Qualifications: Typically, candidates should have completed their 10+2 education in the science stream with a focus on biology. Meeting specific percentage requirements in relevant subjects is often a prerequisite.
Entrance Examinations: Some colleges in Dehradun may require students to appear for entrance examinations to assess their aptitude for the program. These tests aim to ensure that candidates possess the foundational knowledge needed for successful engagement with the curriculum.
Course Description and Specializations: The three-year, six-semester B.Sc. Medical Microbiology program covers a wide range of topics, such as Microbial Physiology, Virology, Mycology, Immunology, and Medical Parasitology. Internships, fieldwork, and practical sessions are essential components that give students practical experience in laboratory techniques and diagnostic procedures.
The Best B.Sc Medical Microbiology Colleges in Dehradun:
Dehradun stands proud as a hub for quality education, and the best B.Sc Medical Microbiology colleges in the city contribute significantly to this reputation. The college forum serves as a valuable resource for aspiring students, offering insights into the top institutions, their faculty, infrastructure, and placement opportunities. Through the forum, students can make informed decisions about their educational journey, ensuring they enroll in institutions that align with their academic and career goals.
Conclusion:
Starting a B.Sc. Medical Microbiology Course in Dehradun is not only a quest for knowledge but also an investigation of the invisible world that has a significant impact on human health. The requirements for eligibility, the specifics of the courses, and the abundance of information offered by the college forum are important factors that direct prospective students to the top B.Sc. Medical Microbiology programs in Dehradun. As the microscopic world reveals itself, students are furnished with the abilities and information necessary to make a significant contribution to the field of medical microbiology.
2 notes
·
View notes
Text
Brazil to have USD 40 million to fight bird flu
The Ministry of Agriculture and Livestock of Brazil has received the amount for actions against the avian influenza. The country has 24 cases in wild birds, but there are no records in commercial production.

A provisional measure published Tuesday (6) on Brazil’s Official Gazette opened an extraordinary line of credit of BRL 200 million (USD 40 million) for the Brazilian Ministry of Agriculture and Livestock for actions against the highly pathogenic avian influenza (H5N1).
The publication is signed by president Luiz Inácio Lula da Silva and Planning and Budget minister Simone Tebet.
The Ministry of Agriculture issued a statement saying that due to the animal health emergency in force in the country and the confirmation of cases in wild birds in at least four states, the control and containment actions will be intensified.
The credit, according to the ministry, will be applied in the Unified System of Attention to Agricultural Health (SUASA). Planned actions include rapid identification, testing, and health case of the suspicious cases.
Continue reading.
#brazil#politics#economy#farming#bird flu#brazilian politics#mod nise da silveira#image description in alt
3 notes
·
View notes