#mri memes
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was named as a finalist in Lead411’s New York City Hot 125 in Aug 2010.
Text

#mri#chronic illness#chronically ill#chronic illness memes#chronic illness humor#mri humor#mri memes#medical memes#medical humor#doctor memes#doctor humor
17 notes
·
View notes
Text

thought too hard about MRI machines today and had this come to me in a vision
#MRI machine#memes#thought too hard about the giant magnet machine that is an eldritch horror and my brain spat this nonsense out#to the cadence of 'this is not a place of honor'
43K notes
·
View notes
Text


They did a CT scan on a fish
#forbidden taco#memes#meme#cute#funny#fish memes#cute animals#fish meme#wholesome#funny memes#lol#dank#fish#what is the copay for this fish#dank meme#dank memes#mri#medical meme#medical memes
14K notes
·
View notes
Text
Happy Telchin Tuesday I have a MRI today for my knee
#rae's random thoughts that would go on quotev#fable smp#fablesmp#days of the week#fable smp days of the week#fable smp memes#fsmp#fsmpblr#mri#mri scan
8 notes
·
View notes
Text
This image of Aki does things to me………


I literally cannot look away whenever this specific picture is on any screen
#he’s just so AgirBxirjeiq3729/)18;$jIriahen#*freaks out like the venom mri scan meme*#crimsonkenjii rambles
8 notes
·
View notes
Text
Vampire MRI
So, I (the older of the two idiots running this blog) have been having some health issues and had to have several MRIs done for them. Now, obviously laying in a big magnetic tube for 3 hours in total isn't exactly exciting. So what do you do? You let your mind wander.
Anyway, to the point:
If a vampire was to get an MRI done, what would we see, or what wouldn't we see? Like imagine dear Edward going into that tube, would he just look solid on the images? Would he maybe not be visible at all? Maybe he's magnetic and stuck until Carlisle has to explain in some mind boggling way why the machine has to be turned off, even though they never do that.
#twilight saga#the twilight saga#twilight#twilight renaissance#twilight renessaince#twilight meme#carlisle cullen#edward cullen#health#mri scan#mri#questions#smeyer#stephenie meyer#are vampires glorified living rocks?
31 notes
·
View notes
Text
#meme#did I make a meme for this yes#Like doctor I just want to know what's wrong with me#this was three different doctors mind you#Tbh with how Manny people in my family have already been medical study's it ant suprosing tho#one of these days will figure it out#This isn't counting the doctors who didnt know what was wrong but had no further notes#4 years in 3 specialists and all MRI and other test come back normal (there's been other doctors not just the specialists)
4 notes
·
View notes

Text

in honor of me getting an mri done i made this
0 notes
Note
If youre still doing hilson requests...
Can you do one about them examining Castiel (spn) and have it be a funny mix between the two?
Idea that i have is house just assuming dean/cas are together and dean assuming house/wilson are together and it just becomes the spiderman meme akskaksjjk
the file on house’s desk detailed a man who was near death - ribs shattered, punctured lung, lacerated spleen, bloodwork that indicated DIC. but that wasn’t why the file was on house’s desk. the case was shunted to house because, after performing CTs, MRIs, and x-rays, there was no abnormalities seen. the man had been wheeled into surgery, and when chase had excised into the abdomen, the spleen was perfectly intact. the thorax showed no sign of a punctured lung, and the ribs were completely normal with no signs of any breakages.
“i’m telling you, this man came into the ER a few hours ago and he was minutes from death. and now… he’s completely healed. its as if nothing happened in the first place,” cameron said. “people barely heal from all those injuries to begin with, let alone being perfectly healed in 3 hours.”
house dropped his cane down onto the floor and marched out of his office. “only reason i’m going to the ICU right now is to prove you wrong,” house said. “clearly your skills have slipped since you left the team.”
cameron rolled her eyes. “my medical skills are perfectly fine. i’m telling you, this was some kind of miracle from God.”
“no such thing,” house grumbled.
pushing into the ICU, house glanced at the apparent patient cameron and chase had been working on. the man seemed perfectly normal, standing and tugging on a long brown trenchcoat. another man was perched on the end of the bed, quickly handing some silver object to the man in the trenchcoat. the man in the trenchcoat brushed his fingers against the other man’s and he offered him the softest look as he uttered his thanks.
veering off to the side, house spied wilson sitting at the nurses station. moving to perch himself on the edge of the desk where wilson was hunched over, house bumped wilson’s shoulder with his leg. “get a load of the guy in bay 5. apparently he came in a few hours ago looking like he’d fucked a meat grinder, and now he’s up and walking like he’s danced through a healing portal.”
wilson glanced up, leaning his forearm against house’s left thigh as he twisted around house’s body to glance at the man in bay 5. “who knows, maybe he’s blessed with magic healing from a deity?”
“asshole,” house muttered, shoving wilson’s arm off his leg and grinning when wilson half fell out of his chair from the unexpected movement.
without another word, house bent down, snagged wilson’s sandwich and took a bite. “be back once i’ve interrogated handsome man and his leather-jacket boyfriend.”
“don’t talk with your mouth full,” wilson grumbled, snatching the sandwich back from house and taking a bite just to prove a point.
“yeah yeah,” house muttered, snagging his cane and thumping over to the men in bay 5.
“let’s get out of here before anyone notices-” the leather jacket wearing man started to say.
house thumped his cane down in front of the trenchcoat man. “too late for that.”
leather jacket man pushed himself off the bed and smoothly stepped in front of trenchcoat man. “you’ve got the wrong guy. cas just had a mild concussion. he’s fine.”
house dragged his eyes up and down leather jacket man’s body. “not from what the file says. your boyfriend should be dead. and yet, handsome over there is walking out of here as if nothing ever happened.”
“nothing happened,” the trenchcoat man - cas - said.
the other man cleared his throat, dropping his eyes to the floor as he muttered, “he’s not my boyfriend.” house watched, analyzing, as the other man half leaned back into cas’ space and his hand settled onto cas’ lower back. “we’ll be leaving now.”
house took a half-step back, pretending to let them pass, but at the last second he flicked his cane out in an attempt to trip cas. the man moved quickly, almost in the blink of an eye, shifting out of the way of the cane as his hand reached out to wrap around the other man’s bicep to steady him from the rapid movement.
house raised his eyebrows. “doesn’t seem like you have a concussion at all, do you, handsome?”
“back off,” the other man snarled.
“dean,” cas said, squeezing dean’s arm once. cas and dean’s eyes locked and they clearly had some silent conversation before dean stepped back in silent submission.
house smirked. “not your boyfriend, hm?”
dean glared and his gaze darted across the room, lighting up when he saw the man at the nurse’s station watching them closely. “I don’t think your boyfriend appreciates you hitting on cas.”
“i don’t have a boyfriend,” house snapped.
“oh really?” dean asked, stepping closer into house’s space and nodding his head towards wilson. “looked like you were sitting in that man’s lap. seemed pretty cozy to me, sharing food and touching.”
house glanced over at wilson and snorted out a laugh. “wilson isn’t my boyfriend. he’s my best friend. i just happen to steal his food just because i can.”
dean let out a derisive laugh. “looked like he couldn’t keep his hands off of you. seemed pretty boyfriend-y to me.”
“you can’t keep your hands off handsome man,” house pointed out.
“cas is my best friend.”
house glared at dean. dean glared at house. a recognition passed between them, a hint of panic. they both tore their eyes away from each other.
“c’mon cas, let’s go,” dean said, snagging cas’ wrist and pulling him towards the door. house let them go.
“what was that about?” house could hear cas asking as they left the ER, but he couldn’t catch the rest of the conversation.
moving back to the nurse’s station, house leaned against the desk by wilson; his eyes still on the place where dean and cas were.
“you just let them go? what happened?” wilson asked.
house didn’t reply, his gaze on the two men as they climbed into an impala. house caught the way dean watched cas get in first, something tender in the way his shoulders tensed and then relaxed as he watched cas settle into the car before dean climbed in himself. a moment later, they were gone.
waving a hand in front of house’s face, wilson called out, “earth to house. what’s going on?”
clearing his throat, house shook his head. “nothing. must’ve been a patient mix-up.”
wilson followed where house was gazing, but there was nothing outside the doors of the ER. shaking his head, wilson patted house’s knee and held out his sandwich for house again in a silent offer to share his food.
house took the sandwich without a word, suppressing a shudder as his fingers brushed against wilson’s as he took the sandwich.
#asked and answered#anon#house md#gregory house#greg house#james wilson#hilson#hate crimes md#malpractice md#hilsonvignettes#destiel#dean winchester#castiel#spn#supernatural#deancas#dcsnapshots
94 notes
·
View notes
Text
By popular (???) request, based on the outcome of this poll.
A WARNING: you guys really did pick the most complex one. This is loooooong. A DISCLAIMER. This is a silly little lesson aimed at folks who know sod-all about MRI. There are memes. There is (arguably) overuse of the term ‘big chungus’. If you are looking to delve deeper into the mysteries of K-Space, this is not the Tumblr post for you.
So, without further ado...
Today I am introducing you to my one true love. The legend. The icon.
Ferromagnetic material loves him. Claustrophobic people fear him.
Yeah, that’s right – we’re talking about the big boom-boom sexyboy magnet machine, hereby known as Big Chungus.

Aka...
MAGNETIC RESONANCE IMAGING
First off, though? Let’s start small.
Very, very small.
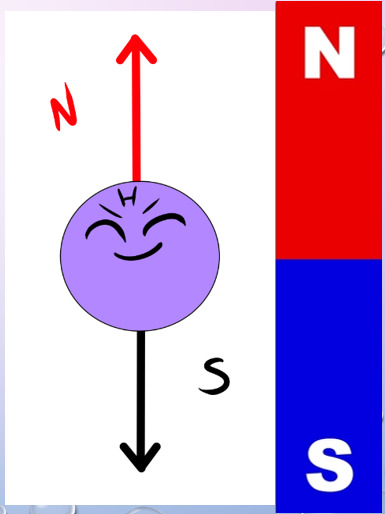
Meet HYDROGEN.

The nucleus of this element is made up of a single proton, which has a magnetic dipole – i.e., it acts like a tiny bar magnet.
Hydrogen is also a component of water. As we all know, we’re basically walking sacks of goop – meaning that Hydrogen is abundant throughout our bodies.
Therefore, when we stick you in a strong magnetic field… say, within our friend Big Chungus… we can manipulate all those tiny Hydrogen atoms in a variety of fun ways.

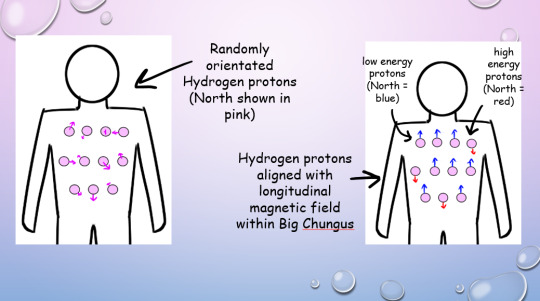
Under normal conditions, all your Hydrogen protons are pointing every-which-way.
But in Big Chungus, there is a strong longitudinal magnetic field that travels along the Z-axis of the machine. So, all your teeny tiny Hydrogen protons swivel to align with that field!
If a proton’s energy is LOWER than that of the longitudinal magnetic field (a majority), they will align PARALLEL with the field. If their energy is HIGHER (a minority) they will align ANTI-PARALLEL.
As most of the protons align with the longitudinal magnetic field, the net magnetisation vector within the human body is also longitudinal! This is called the thermodynamic equilibrium – the resting state for all those li’l protons when your body is within Big Chungus.
(You won’t feel any different, btw! We’re flipping a bunch of teeny-tiny bits inside you, but you won’t feel a thing!) (You might do later, when we activate the Gradient coils. We’ll….. get to that)
But, while all of this is very cool, it gives us no actual information. We gotta play some more with your protons - which brings us to arguably the most important concept in MRI. I mean, it’s literally in the name!

Let’s go back to our Hydrogen protons.

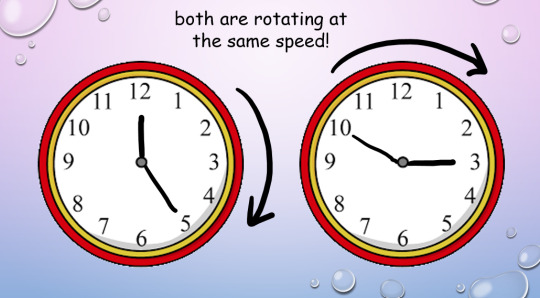
We’ve established that they’re all pointing in different directions. But they’re not just sitting still. They’re spinning and wobbling all over the shop.
We call this rotational wobbly movement precession.
In their natural state, these protons all precess at different speeds. When we subject them to Big Chungus, as well as all lining up neatly with the magnetic field, they all start to precess at the same speed.
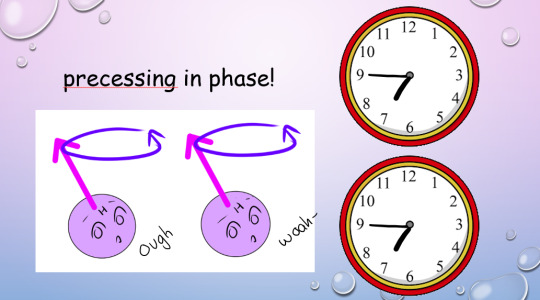
However, their magnetic North will be pointing to different points at any given moment. Imagine two clocks, both of which are ticking at the same rate, but which have been set to read different times.
This is where magnetic resonance comes in.
In addition to the homogenous longitudinal magnetic field provided by Big Chungus, we also create an oscillating magnetic field in the transverse plane by using a radiofrequency (RF) pulse. We can tune that oscillation to the ‘resonant frequency’ of Hydrogen atoms.
Every molecule capable of resonance has its own specific frequency. We use a funky equation called the Larmor Equation to work this out, or, as I like to call it, W, BOY!!!
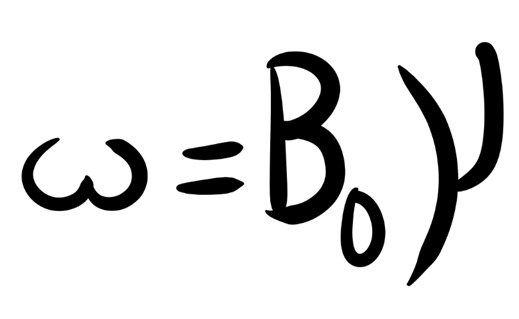
(The weird ‘w’ is the resonance frequency; the weird ‘Bo’ is the magnetic field strength, and the weird ‘Y’ is the gyromagnetic ratio of each particular element.)
So, we know exactly at what frequency to apply that RF pulse to your protons, to achieve resonance!
But what is resonance?

In acoustics, a ‘resonant frequency’ is the frequency an external wave needs to be applied at in order to create the maximum amplitude of vibrations within the object. Like when opera singers shatter glass with their voice! They’re singing at the resonant frequency of the glass, which makes it vibrate to the point where it compromises its structural integrity.
A similar concept applies in magnetic precession, with, uh, less destructive results. We’re not exploding anything inside of you, don’t worry!
(We do explode your innards accidentally in Ultrasound sometimes, via a different mechanism. But you’ll have to ask me more about that later. >:3)
To put it simply, magnetic resonance is the final step in getting those protons to BEHAVE. Now, the clocks have been corrected so their hands move at exactly the same time, in the same position. The protons are precessing ‘in phase’. Yay!
This creates transverse magnetisation, as the magnetic vectors of all those protons (which, remember, act as bar magnets) will swing around to point in one direction at the same time.
But the cool thing about resonance? It also allows the protons to absorb energy from the RF pulse.
(Do NOT ask me how. Do NOT. I will cry.)
And remember how the higher-energy protons flip anti-parallel to the longitudinal magnetic vector of Big Chungus, while the lower-energy protons are aligned parallel? And because we have more low-energy protons than high-energy protons, our body gains a longitudinal magnetic vector to match Big Chungus?
Zapping those protons at their resonant frequency gives 'em energy (a process known as ‘excitation’, which I love, because I get to imagine them putting little party hats on and having a rave).
So, loads of them flip anti-parallel! Enough to cancel out the net longitudinal magnetic vector of our bodies – despite the best efforts of good ol’ Chungus!
(Keep trying, Chungus. We love you.)

Our protons are as far from our happy equilibrium as they can possibly be. We’ve lost longitudinal magnetisation, and gained transverse magnetisation. Oh noooo however can we fix this ohhhh noooooo
Simple. We turn off the RF pulse.
Everything returns to that sweet, sweet thermodynamic equilibrium.
Longitudinal magnetisation is regained. I.e., the protons realign with Big Chungus’s longitudinal magnetic field, with the majority aligned parallel rather than anti-parallel.
This is called SPIN-LATTICE RELAXATION.
‘T1 time’ is the point by which 63% of longitudinal magnetisation has been regained after application of the RF pulse. A T1-weighted image shows the difference between T1 relaxation times of different tissues.
And, without that oscillating RF pulse, we lose resonance – the protons fall out of phase randomly, due to the delightful unpredictable nature of entropy, and Transverse magnetisation reduces.
This is called SPIN-SPIN RELAXATION.
Or, if we’re feeling dramatic…

‘T2 time’ is the point by which 37% of the transverse magnetisation has been lost. A T2-weighted image shows the difference between T2 relaxation times of different tissues.
(Spin-spin is objectively a hilarious phrase to say in full seriousness when surrounded by important physics-y people. However, a word to the wise: do not make a moon-moon joke. They are not on Tumblr (present company excluded). They will not understand. You will get strange looks.)
But remember how resonance lets our protons shlorp up that sweet, sweet energy from the RF pulse? Well, in order to get back to thermodynamic equilibrium and line up with Big Chungus again, they have to splort that energy back out.
This is why we stick a cage over the body part we’re imaging. That cage isn’t a magnet, or a way of keeping you still – it’s a receiver coil.
It picks up the RF signal that’s given off by your innards as they relax from the intense work-out we just put them through. How cool is that??

The amount of time we wait between applying the RF pulse and measuring the ‘echo’ from within your body is called the ‘ECHO TIME’, or ‘TE’ (because we didn’t want to call it ET).
(yes, we’re cowards. Sorry.)
We also have ‘REPETITION TIME’ or ‘TR’ – the amount of time we leave between RF pulses! This determines how much longitudinal magnetisation can recover between each pulse.

By manipulating TE and TR, we can alter the contrast (i.e., the blacks and whites) on our image.
Areas of high received signal (hyperintense) are shown as white, while areas of low received signal (hypointense) are shown as black. Different sorts of tissue will have different ratios of Hydrogen-to-other-shit, and different densities of Hydrogen-and-other-shit – ergo, some tissue blasts out all of its stored energy SUPER QUICK. Others give it off slower.
A T1-weighted image has a short TR and TE time.
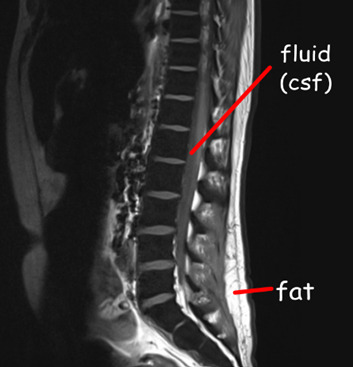
Fat realigns its longitudinal magnetisation with Big Chungus SUPER QUICK. This means, on a T1-weighted image, it looks hyperintense. However, water realigns its longitudinal magnetisation with Big Chungus slooooowly. Therefore, on a T1-weighted image, fluid looks hypointense! Ya see?
A T2-weighted image has a long TR and TE time.
The precession of protons in fat decays relatively slow, so it will look quite bright on a T2-scan. But water decays slower, and therefore, by the time we take the T2 image, fluids within the body will be giving off comparatively ‘more’ signal than fat – meaning they’ll appear more hyperintense!
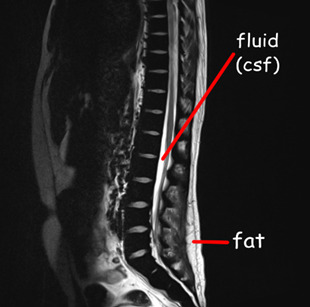
If we have a substance with intrinsically long T1 and T2 values, it will appear dark on a T1-weighted image and bright on a T2-weighted image, and the same in reverse. If a substance has a short T1 value and a long T2 value, it will appear relatively ‘bright’ on both T1 and T2-weighted images – i.e., fat and intervertebral discs.
As every tissue has its own distinct T1 and T2 property… we can work out precisely what sort of tissue we’re looking at.
When we build in all our additional sequences, this becomes even clearer! This is why your MRI scan takes sooooo long – we’re running SO MANY sequences, manipulating TR and TE to determine the exact T1 and T2 properties of various tissues within your bod.


There is, however, a problem.
The RF signal given off by each proton doesn’t shoot out in a handy-dandy straight line. Meaning, we have no idea where the signal is coming from within your body.
Enter our lord and saviour:
THE GRADIENT COILS.
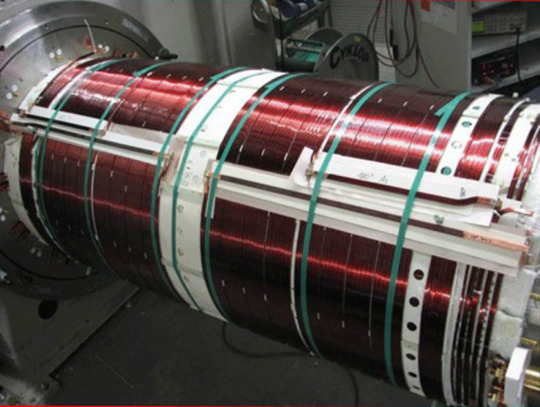
(Shim coils are also very important – they maintain field homogeneity across the whole of Big Chungus. While Big Chungus wouldn’t need them in a perfect theoretical scenario… reality ain’t that. Big Chungus’s magnetic field is all wibbly-wobbly, so we use Shims to keep everything smooth! That’s all you need to know about them. BACK TO THE GRADIENTS.)
There are three of them, wrapping around each of the three planes of your body. When these activate, they cause those epicly eerie booming noises, characteristic of a Big Chungus ExperienceTM.
youtube
The Gradient coils are also what causes those weird tingling sensations you get in an MRI machine – which, don’t worry, aren’t permanent! Your nerves just go ‘WOAHG. THASSALOT OF MAGNET SHIT. HM. DON’T LIKE THAT.’ But they’ll calm down again once you’re freed from Big Chungus.
The gradient coils cause constant fluctuations in the magnetic field across all three dimensions. They activate sequentially, isolating one chunk of your body after the next.
As these fluctuations cause variation within the signal received, we can look at how much THAT particular signal, received at THAT particular number of milliseconds after an RF pulse, varied when THAT particular gradient was activated, in comparison to when THAT OTHER gradient was activated.
For every single bit of signal output.
That gives us A WHOLE LOTTA DATA.

^ imagine this, but the cupboard contents is just. data.
Way too much data, in fact, for our puny human brains to comprehend – so obviously, we feed it to an algorithm.
K-space is a funky computational matrix where all this info gets compiled during data acquisition. Once we’ve finished the scan sequence and have all that yummy raw data, it can be mathematically processed to create a final image!
Just like that. Simple, right?

TL;DR
You are full of Hydrogen.
Hydrogen nuclei (protons) are basically tiny magnets
These tiny magnets are orientated completely randomly, with ‘North’ pointing in all directions
We stick billions of these tiny magnets (i.e., you) into a mahoosive magnet (i.e., Big Chungus)
All the tiny magnets flip around to align with the longitudinal magnetic field of Big Chungus
High energy protons = antiparallel Low energy protons = parallel
As you have more low energy protons than high energy protons in your body, the net magnetic vector of your body is longitudinal – just like Big Chungus!
All your protons are spinning and wobbling (precessing) at random rates
We use an RF pulse, tuned to the Resonance Frequency of Hydrogen, to make ‘em precess in phase (wobble at the same time, all pointing in the same direction at once). This creates a Transverse magnetic vector.
This in-phase precession is ‘Magnetic Resonance’
Magnetic Resonance means the protons can absorb energy from the RF pulse
Now there are more high energy protons within your body! They flip antiparallel, and the net longitudinal magnetic vector of your body decreases.
We measure the time it takes for the high-energy protons to release that energy and return to alignment with the net magnetic vector of Big Chungus (Spin-Lattice Relaxation / T1 recovery)
And the time it takes for the precessing-in-phase protons to Quit That Nonsense and all start wobbling in random directions again (Spin-Spin Decay / T2 recovery)
Each tissue within your body has a different composition & density of Hydrogen atoms – which means each tissue within your body has a unique T1 & T2 recovery time
By measuring the signal at different times (TE) and by varying the frequency with which we apply RF pulses (TR), we ‘take pictures’ that show variations in the amount of signal these tissues are giving off. The signal is caught by the large radiofrequency receiver coils we put over you when you enter the machine.
Because the signal given off during recovery/decay blasts out in all directions, we don’t know exactly where it originated within your body.
Gradient coils are arranged across X, Y, and Z axes throughout the gantry of Big Chungus. They cause tiny fluctuations in the magnetic field, in sequential chunks throughout space. This is the booming noise you hear when you’re in the machine.
These tiny fluctuations cause variations in the signal we receive, depending on how close the signal is to the activated gradient coil. All this data is compiled in a magical computational matrix called K-space. A funky algorithm then decodes those variations and couples them up with the strength of the signal to give us 1) How much signal is being blasted out at that particular moment 2) Where exactly that signal comes from within your body, according to the 3D map produced by the gradient coils
It then represents these values with a pretty picture!
Tl;dr tl;dr:

71 notes
·
View notes
Text
I am once again making memes to cope with chronic health issues.
At the sangha meeting I was chatting with this lady about how I've had a headache basically for a year and a migraine since April and the eye doctor said there's pressure on my optic nerves from my brain and that I have an MRI scheduled for 3 weeks from now and I'll have a spinal tap after that and she was like "oh, so you might have hydrocephalic migraines. I have those. But the pressure was just low enough that I don't qualify for surgery." And I was like "what, so you just have to suffer?" And she was like "yeah..." and my reaction to that was
Anyway my MRI is on the 23rd so send me "tests actually show the problem" vibes that day if you can.
21 notes
·
View notes
Text
DIAGNOSTIC OLYMPICS, SEASON 1, EPISODES 5-15
part one
Hi! I was curious about who on House (besides House) gets the most diagnoses right. Other folks have already run a tally (it's Chase), but I was curious how other factors would influence the tally — whose ideas get run with, who manages treatment, who screws up… So I thought I'd keep score.
1 point for getting the answer. This is almost always going to be House.
.5 points for Valuable Contribution — stuff that isn't the final answer, but either is thought to be the final answer or is valuable to the solving of the case. Stuff like "noticing something on the MRI" doesn't count; things like "figuring out how to treat" does.
-.5 to -1 for Mistakes — stuff that delays or prevents diagnoses, injuring or killing patients, etc.
FIDELITY
DIAGNOSES: African Sleeping Sickness
+1 House: Figures it out very early, the trick is proving it, which takes significantly longer. +.5 Foreman: When at first it looks like sleeping sickness is impossible, he comes up with a strong secondary theory and gets House Praise GO-GETTER AWARD: This is the third time Cameron has brought House a case, and in just a couple episodes she'll bump that up to four. PROBABLY A COINCIDENCE AWARD: Chase immediately guesses parasites based on the idea that "maybe she was lying about never leaving the US." This is the second time in three episodes his first offhand guess ends up being right.
POISON
DIAGNOSES: Pesticide Poisoning
+1 Team: This is another episode where they basically know what's happening immediately, the trick is proving it/figuring out how to treat it. +.5 Cameron: Successfully bullies the mother after she shoots down everyone else. House and Chase had to trick her in the end anyway, but credit where it's due. -5 COOL POINTS: When the patient is seizing, the subtitles have Chase saying "stay calm." The words that actually come out of his mouth are "stay cool, mate."
DNR
DIAGNOSES: Bad Arteries
+1 Team: Another episode where no one person has a big breakthrough; they only catch the cause of the patient's paralysis on a scan. +.5 House: His determination that something is wrong and should be addressed leads to the patient not only being able to walk, but still being alive. Legally shady, medically good. +.5 Cameron: Suggests a stroke early on, and a scan does find a clot. It doesn't end up being the problem, just a symptom, but good call. +0 Foreman: His first time running a case and it really doesn't go well. He keeps following House's orders and doubting himself, lies about treatment, and is generally wishy-washy. He didn't make any mistakes (because he didn't make any calls), but not a good showing.
HISTORIES
DIAGNOSES: Rabies
+1 House: Figures out the patient has rabies. -.5 Foreman: Makes a number of mistakes, from refusing to take any of the patient's symptoms seriously to wanting to discharge her to almost giving her an MRI with a metal pin in her arm. I was going to give him a full point demerit, but he does accurately guess she gave herself the insulin OD intentionally, and once he gets over himself and realizes he fucked up he works really hard to help the patient.
DETOX
DIAGNOSES: Termite poisoning
+1 House: Figures it out while actively suffering drug withdrawal. +.5 Chase: The patient's eye gets a clot and goes blind, but he's on blood thinners and they can't operate. House is willing to just let the eye be blinded, but Chase figures out a creative way to remove the clot and save the eye. +0 Cameron: Suggests lupus and gets really, really stuck on it, but still goes along with all of House's ideas. They do eventually treat for lupus when House runs out of other ideas, but he's clear he doesn't think it's a good one. +5 MEME AWARD: First time lupus comes up on the show!
SPORTS MEDICINE
DIAGNOSES: Cadmium poisoning
+1 House: Takes him a while, because at first they dismissed environmental causes, but when the patient's wife shows a symptom he figures it out in three seconds. +.5 Chase: Initially suggests Addison's, which House likes and the team runs with. Later, is the first of the team to realize House thinks cadmium poisoning, and figures out the source. +10 FRIENDSHIP POINTS: The first time in the series the fellows hang out outside work, we see them getting drinks at one point and dinner with a drug rep at another.
CURSED
DIAGNOSES: Anthrax and Leprosy
+1 House: He figures out that the patient and his father both have leprosy. He also figures out Rowan Chase has cancer, but we're not grading on that case. +.5 Cameron: The first to realize anthrax after House notices something wrong with the sample. +.5 Chase: He has like three merits and three demerits for this one. His early guess of mold causing pneumonia is a good one, and leads them to anthrax. He also bonds with the patient and gets a truer history from him. However, once his dad shows up, Chase spends the rest of the episode just trying to prove him wrong: first that the patient doesn't have sarcoidosis, then testing for every single auto-immune disease known to man because daddy thinks it is one. On the other hand, he also sticks to his guns on anthrax and is proven correct even after the team and House (and dad) dismiss it as a possibility. -1 Rowan Chase: Being a bad father aside, his guesses are plausible but all wrong. As Baby Chase points out, Daddy Chase is just guessing rheumatoid diseases because that's what he knows. THE REMY HADLEY AWARD: Chase manages to be so opaque and so resistant to House's manipulation attempts that House gives up entirely and just tries to have an honest conversation with him. 13 would be proud.
CONTROL
DIAGNOSES: Ipecac poisoning
+1 House: Figures it out, and advocates hard for his patient to have a heart transplant once he realizes she's sick because she's self harming. Ethically shaky, medically good. +.5 Cameron: Reads a self-help book and manages to get the guys to agree with all her ideas and run her tests. She continues to have good ideas through the case, even if she quickly gets on all their nerves. +0 Chase: hot take alert! He loses points for his fuck up early in the episode: he's too busy flirting to realize he scanned the wrong leg. Luckily for him, it had no bearing on the case, but it could have gone very badly. On the other hand: Going off a vague clue (that House was acting oddly), he also manages to figure out the ipecac poisoning and that the patient's illness was self inflicted. He then runs to Vogler (+50 Rat Points). Shitty move ethically, good diagnosing. I wouldn't give him the credit if he hadn't also been careful to wait to tattle after the transplant was done.
MOB RULES
DIAGNOSES: Beef allergy
+1 House: The episode is really much more about Vogler and Chase's ratting than the case. The patient has an unrelated symptom (high estrogen) that throws everyone off for a while, but once House finds the cause it's pretty quick and obvious.
RUNNING TALLY:
HOUSE: 11.5 TEAM: 3 FOREMAN: 1 CHASE: 2.5 CAMERON: 2.5
Cameron has the biggest jump, going from .5 to 2.5: she isn't making any big leaps, but unlike Chase and Foreman, she's consistently solid and not making any big mistakes either. Good for her!
#diagnostic olympics#house md#hate crimes md#i am open to arguments and debates about my grading#i'm trying to explain my reasoning and keep things fair but a lot of this is sort of subjective#malpractice posting
16 notes
·
View notes
Text

[ID: the “wait, it’s all [blank]” meme of one astronaut pointing a gun at the other, edited to read “wait, it’s all celiac?” / “always has been.” with the word celiac in a groovy pink font. end ID]
happy celiac awareness month 💓🖤💓 folks expressed interest in my #Controversial Opinion, so here we go:
as someone who “has” non-celiac gluten intolerance, i don’t believe it exists.
this, as with all of my diagnostic opinions, is built from both health research & sociology, specifically the genealogy of (my) disabilities – how the labels we use & the divides we create between diagnoses are socially constructed. conditions don’t announce themselves as discrete entities; instead, labels are given based on, at best, current medical understandings of symptoms + clinical visualization measures (imaging, bloodwork, genetic testing, etc). conditions that were once considered two separate things may eventually be restructured under the same diagnostic label, & what was once considered one singular disease may be divided into separate categories, in response to new information or the new recognition / respect of existing information.
the issue with this system, though – with access to healthcare which is predicated upon diagnosis, which is itself predicated on checklists of symptoms & clinical visibility – is that we don’t know shit. our bodies are not required to present symptoms in accordance with the ICD 10, & chronic illnesses are very much an “ask four doctors, get five answers” situation.
for example: without any of my symptoms, imaging, or bloodwork changing, i’ve been diagnosed with active ankylosing spondylitis, ankylosing spondylitis that is in remission, fibromyalgia, & spondyloarthropathy. the only difference is the doctors: their belief or lack thereof in my symptoms, their familiarity with current research, & the diagnostic systems they abide by. under the NHS, it was definitionally impossible for me to have ankylosing spondylitis that was not visible on an MRI, therefore i must have been in remission, even as my symptoms were just as debilitating as before & treatable by immunosuppressants.
how this pertains to celiac: as with all chronic illnesses, symptoms of celiac disease are a broad spectrum. some people have severe growth impairment from a young age; others may only have minor skin manifestations. other common symptoms are vague & potentially attributable to any chronic illness, such as fatigue, depression, & gastrointestinal issues. crucially, though, damage to the small intestine is still occurring even in people with celiac who do not flare after consuming gluten.
following this,
the diagnosis of non-celiac gluten intolerance has nothing to do with symptom presentation or severity. it doesn’t even mean there is no clinically visible damage to the small intestine. rather, it just means you didn’t pass the test:
in my case, not only was the (notoriously unreliable) antibody blood test negative, but so were subsequent tests for the genetic markers associated with celiac.
two people with the same exact experiences can get put into two different boxes, solely based on bloodwork – but that’s not how genetics works. it’s pretty much impossible that only those two markers dictate whether or not someone has celiac, or any given disease, because genetics are infinitely more complex than that; equally, plenty of autoimmune disorders can have a genetic component but are not exclusively found in people with that particular marker (ankylosing spondylitis & HLA-B27, for example).
therefore, i firmly believe non-celiac gluten intolerance is celiac disease, just influenced by other genetic factors and/or antibodies we haven’t yet identified.
there are a whole host of issues created by the false divide of celiac vs non-celiac gluten intolerance, certainly including things i’ve never considered, but here are a few examples of what i refer to as diagnostic violence, the physical & social consequences of these forms of categorization:
celiac disease increases people’s risk for small bowel cancer. but if it’s been determined by the medical establishment that according to their criteria, you don’t have celiac disease, then you won’t receive cancer screening.
since a food intolerance is not considered an autoimmune disease, there is no medical evidence of an underlying cause of arthritis, for example, making it that much harder for people to receive diagnosis & treatment for autoimmune symptoms.
diagnostic paperwork & a letter from a doctor is almost always required to receive accommodations, & food-related accommodations are notoriously difficult to obtain at universities which require the purchase of a meal plan without sufficient gluten-free options, for example.
as a response to the dangerous ableism permeating societal attitudes toward gluten-free food, many people (diagnosed) with celiac fall back on communicating the seriousness of their needs at the expense of their undiagnosable peers. “it’s not just an intolerance!” i read over & over – never mind that gluten made me so sick i lost a significant amount of weight, my hair fell out, i had signs of multiple vitamin deficiencies, & i could only keep down liquids.
this is honestly the most blatant example i’ve come across of the complete arbitrariness of diagnostic categories, but it’s far from the only one, & i’d love to hear other folks’ controversial opinions – what physical disabilities do you tell people you have without a diagnosis? do you consider yourself to have that condition, or is this just for expediency of communication? how does your undiagnosability affect your interactions with community formed around that diagnosis?
your experiences are real, your symptoms are serious, & it is not your fault that white supremacy demands a categorizability which all bodies inherently fail. join the club – we’ve got plenty of gluten-free snacks. 💓🖤💓
#celiac#celiac disease#dietary restrictions#gluten intolerance#gluten free#sociology#disability studies#diagnosis is a form of violence#abolish the clinic#mac.txt#image described
85 notes
·
View notes
Note
*insert vaguely coherent british yelling*
somehow I missed it off my low-key ESSAY of a rambling comment on ao3 but I am so proud of what you’ve achieved with FaC and I hope you are too!! Creating something of that length and depth and just absolute QUALITY, in general but also whilst studying a PHYSICS PHD?? insane achievement >>>
you have my complete respect and admiration and honestly have permanently altered my brain chemistry in ways I want to study under a microscope and maybe an MRI machine (I’m a neuroscientist-in-training, for context :D)

⬆️⬆️ in the absence of a true meme…this is what finding FaC felt like :D
wishing you all the best with your studies!! and undoubtedly I will continue to (politely) yell in your comment section 🫡
*returns British yelling*
Hello!!!
You are way too nice ahhh! I am really proud of it, thank you :)))
Insane is definitely how the PhD makes me feel on a regular basis but I did fully do this to myself so I blame past me for all mistakes (also I just like complaining and when my brain is working properly, I do actually really enjoy it lol)
Good luck fellow STEM human! Can't wait to be politely yelled at from time to time :p
6 notes
·
View notes
Text
Hey y'all fun fact in in the hospital rn
Not dying or anything but my left leg/hip are absolutely FUCKED and I can barely walk, doctors say it's bad sciatica and some herniated disks in my spine, waiting on getting an MRI but it might be a while cause this hospital doesn't have an MRI scanner so they need to see if they can get me in at the hospital a few towns over. They also said something about maybe having to see a spine surgeon but that's up to me and my family doctor to decide
Anyway, send me pictures of your pets and tell me about them!! Especially if they're uncommon pets, I love insects 🪲🐞🐜🐌🪳🦋🐛🪱🕷️🦂
If you don't have any pictures of pets, memes and well wishes would be incredibly appreciated as well ❤️
7 notes
·
View notes