#independent medical assessment
Text
Insightful Independence: The Importance of Independent Medical Assessments
Introduction:
In the realm of healthcare, independent medical assessments play a crucial role in providing unbiased and objective evaluations of an individual's health condition. These assessments are conducted by independent medical professionals who are impartial and free from any conflicts of interest. In this article, we will explore the significance of independent medical assessments, their key components, and the benefits they offer in ensuring accurate diagnoses and fair evaluations.

The Significance of Independent Medical Assessments:
Independent medical assessments are essential in various scenarios, including personal injury claims, disability evaluations, workers' compensation cases, and insurance claims. The primary purpose of these assessments is to provide an impartial and unbiased evaluation of an individual's health condition, treatment options, and functional abilities. They help ensure fairness, integrity, and accuracy in the decision-making process, benefiting both the individuals seeking assessments and the organizations involved.
Key Components of Independent Medical Assessments:
Independent medical assessments typically consist of several key components, each contributing to a comprehensive evaluation. While the specific components may vary depending on the nature of the assessment and the relevant jurisdiction, some common elements found in independent medical assessments include:
Review of Medical Records: Independent medical assessors thoroughly review the individual's medical records, including previous diagnoses, treatment history, and relevant diagnostic tests. This helps them gain a comprehensive understanding of the individual's medical background and facilitates an accurate evaluation.
Physical Examination: A hands-on physical examination is conducted to assess the individual's current health status, functional limitations, and any objective signs of impairment or disability. The physical examination may involve assessing mobility, strength, range of motion, reflexes, and sensory functions. It provides valuable insights into the individual's physical condition, helping the assessor make an informed assessment.
Diagnostic Tests: In some cases, additional diagnostic tests may be ordered to gather objective data and support the assessment. These tests may include imaging studies, laboratory tests, or specialized procedures to confirm or rule out specific conditions, injuries, or disabilities. The results of these tests contribute to the overall evaluation and help ensure accuracy.
Impartial Evaluation: Independent medical assessors are trained professionals who have no personal or financial interest in the outcome of the assessment. Their role is to provide an unbiased evaluation based on their expertise and the available evidence. This impartiality is crucial in maintaining the integrity of the assessment process and ensuring fairness to all parties involved.
Benefits of Independent Medical Assessments:
Independent medical assessments offer several benefits that contribute to fair and accurate evaluations:
Objectivity and Impartiality: Independent medical assessors provide objective evaluations free from personal biases or conflicts of interest. This objectivity ensures that the assessment is fair and unbiased, providing a reliable and accurate representation of the individual's health condition.
Expertise and Specialization: Independent medical assessors are typically highly trained and specialized in their respective fields. Their expertise allows for a thorough understanding and assessment of complex medical conditions, ensuring the accuracy of the evaluation.
Enhanced Decision-Making: Independent medical assessments provide valuable insights that assist decision-makers, such as insurance companies, legal professionals, and adjudicators, in making informed decisions. The objective and comprehensive evaluation helps facilitate fair and equitable settlements, treatment plans, or disability determinations.
Trust and Confidence: Independent medical assessments enhance trust and confidence in the assessment process. Individuals seeking assessments can have confidence that their case will be evaluated objectively, while organizations involved can rely on the credibility and expertise of the independent assessors.
Conclusion:
Independent medical assessments play a vital role in ensuring fairness, accuracy, and objectivity in evaluating an individual's health condition. These assessments provide an unbiased evaluation of medical conditions, treatment options, and functional abilities, assisting decision-makers in making informed decisions. By relying on independent medical assessors, individuals and organizations can have confidence in the integrity and accuracy of the assessment process. The importance of independent medical assessment cannot be overstated, as they contribute to fair outcomes, trust, and confidence in the healthcare and legal systems.
0 notes
Text
Medibytes Legal provides Independent Medico-Legal Services with a difference. We are efficient and take swift action on your case, minimising time from assessment to report so that you can act upon the opinion you receive in a timely and considered way.
We empower your decisions by providing medical experts who understand the industry and are experienced in the art of moving a case forward with robust, evidence based opinions.
Our specialists conduct Independent medical examinations and provide evidence based reports on the following types of cases:
Workers Compensation
Personal Injury
Public Liability
Institutional Abuse
CTP
Income Protection
TPD
Fitness for Duty
Superannuation Claims
We provide a quick report turnaround of between 4-10 business days.
#medico legal specialists#medico legal assessments#medico-legal assessment#medico legal experts#medico legal services#medico-legal experts#medico-legal services#independent medical examination#favorable ime report#ime report#independent medical examination nsw#expert witness report#independent medical opinion#independent medical examination fair work#medico legal report#independent medical examination victoria#workers compensation doctor#independent medical examination queensland#workers compensation independent medical examination#ime doctor#independent medical examiner#building expert witness report#independent medical examination australia#medico legal reporting services of australia#psychiatrist medico legal report#independent medical examination providers#medico-legal report#medico legal psychiatrist report#medicolegal report#independent medical report
1 note
·
View note
Text
“Autism isn’t a disability”, “it’s just a difference”.
I am of lower support needs. I hold down a (part time) job. I have travelled around my home country. I live alone.
At work they complain about my speech. I’m too quiet, they say, “barely audible” is the words used at my autism assessment. My voice is all monotone, and it needs to be more expressive. I get this complaint every week for a year straight, until my manager gives up. I don’t attend trainings because I forget and find it overwhelming anyways. My coworkers form friendships, and I watch them talk, wondering how they make it look so easy. I get a new manager, I tell her I find the work socials too overwhelming to attend. She tells me I can just say I don’t want to come. I don’t know how to tell her that I desperately want to, to be like the rest of my coworkers, instead of constantly being the one sat on the sidelines.
I come home, and I can hear my neighbours again. The niggling background noise messes with my head, and I meltdown; I throw myself on the floor, I hit my head on the ground repeatedly as I scream and cry, tear out my hair and scratch my arms and face. When I complain, people tell me that I just have to accept that neighbours make noise, that I should just ignore it, or block it out. I am the problem, the one overreacting. I put in earplugs and it hurts and I'm crying again. I wear headphones but I can't handle the noise for that long.
I have reminders set for everything. Every chore, no matter how big or small. My phone beeps at me, reminding me that I need to wash the dishes. If I don't go now, then tick the little box on my phone to say I did it, it won't get done. My home is almost always a mess despite this. It's not just chores either. I won't think to wash, dress myself, brush my teeth or hair, without those reminders. And unless someone actively prompts me to do so, I will do those tasks "wrong". I haven't changed my underwear in a month, and I'm currently aware that's a problem, but within the hour I'm going to forget all over again until I'm next prompted.
I can't sleep without medication - it's not unusual for autistic people to have messed up circadian rhythms. Without my medication it's hard to even tell when I'm awake and when I'm asleep. When I was younger and at school I slept through so many lessons, and when I have my mandatory breaks from my sleep meds I sleep through every alarm I set. I want to work full time some day, and I'm terrified of what my sleep issue will mean for me then.
I don't travel independently. I don't travel anywhere alone, always with someone or to someone. If to someone, I have assistance the whole way. I find it embarrassing sometimes. Yes, I have a job that requires a certain level of intelligence. No, I cannot get on a train by myself. If I am not shown To The Train, To My Seat, I will be unable to travel.
Last time I travelled, I was left alone at the station for ten minutes. I stayed rigid and sobbed the whole time. I was overwhelmed. It was too loud, I didn't know where I was or where I was meant to be going, and until the assistance person came back I couldn't do anything because for some reason I cannot understand it.
I spend a lot of time trying to explain to people that despite my relative competence, I am unable to do many things. Why can I understand high level maths but not how to get on a damn train? No fucking idea.
"Autism isn't a disability" most severely affects those with higher support needs, and this is absolutely not to take away from them. But for fucks sake, autism is disabling.
Maybe you personally are extremely lucky and just find you're a little "socially awkward", or just find some textures painful or nauseating. Maybe you would be fine with just a couple of adjustments.
But for a lot of us, even lower support needs autistics, it doesn't work like that. I will never sleep properly without medication. I still have the self-harming type of meltdowns as an adult, over things that are deemed as being "just part of life". I live alone but have daily visits from family - if I'm left fully alone I forget all the little daily things one is "meant" to do. I had speech therapy as a child to get me to the "barely audible" "mostly correct" speech. I don't mask, I'm not really sure how I would to begin with.
I'm not unhappy with being autistic. It's just who I am. Life would be easier if I were neurotypical, but I also wouldn't be me. I just wish those luckier than me could...stop saying it's all chill and not at all a disability.
Because yes, socially, I am "awkward". I obviously don't make eye contact - I stare down and to the side of whoever I speak to. People think it's weird or creepy or a sign of disinterest. My autism assessor wrote down about how I often use words and phrases that don't make sense to others, even though they make perfect sense to me. In my daily life this means I'm frequently misunderstood, and have to try explain what I mean, when what I mean is exactly what I said, and the true issue is that what I mean just doesn't make sense to others. I gesture, at times, but again, my gestures apparently don't make sense in relation to what I'm saying. I take things literally, I have almost no filter, and I can't explain how I go from topic to topic.
And yes, I do have sensory problems. Sometimes people, including others with sensory problems, tell me that "sometimes sensory issues have to be tolerated", and I wonder what they think of as being sensory issues. I'm sure they do struggle, but if I say I can't handle a touch, I mean you will need to forcefully hold it against me for me to touch it more than a second and it will make me meltdown. If I say "I can't eat that", I mean that I am unable to swallow it, that I will gag and choke and inevitably spit it back out, as much as I try. If I say I can't handle a noise, I mean I'm so close to a meltdown and my meltdowns are a problem for everyone around me.
But yes. Autism. Not a disability. Just a fun quirky difference.
1K notes
·
View notes
Note
How did you find the doctor(s) who assessed you for ADHD? Im looking into the process of getting diagnosed because (although ive suspected I might have adhd for years now) I've been struggling a lot more lately and i want to try medication to see if it helps at all. Im trying to search for psychiatrists through my health insurance portal but the the results im getting are all for child/adolescent psychiatry specialists, and I dont think that'll be much help for an adult adhd assessment? Did you have an established therapist to refer you for your assessment or were you able to find a psychiatrist independently?
I actually just kind of had to freeform it, but that does mean I have some tips to share!
I will say, I have never once used a health insurance portal to find someone to treat me for anything. Often their search engine is fucked up and the information is sometimes out of date. I almost always either ask someone who I know has had similar issues if they have a recommendation, ask my treating physician if I have one, or just google until I find someone reputable-looking; any qualified medical center or professional will list what insurance they take anyway, and you can always ask when you make the appointment.
So here's the process for how to do that!
When I was first considering it, I asked a friend who'd had an evaluation that came back not-ADHD, which I liked because it meant we knew it wasn't like, a weird Adderall pill mill or something. I really wanted to have a professional and thorough evaluation because I knew myself and knew I was capable of gaming a questionnaire. The place she had her evaluation was unfortunately having some staffing issues; part of the reason it took me so long is that I played phone tag with them for ages -- I'd call, and regardless of what time of day I called, their scheduler would be "out", so I'd leave a message and never get a call back. Ultimately I said "I really need to talk to a human, because your scheduler has not returned any of my numerous calls" and they said they could transfer me to another office outside of Chicago (in the burbs). That was not going to be accessible to me, so I told them thanks but I'll go somewhere else. Then COVID hit and I was not going to go anywhere near a medical center unless I had to for about two years.
So, when I was making my second serious run at getting evaluated, I did what might be expected of me by longtime readers of this blog: I made a spreadsheet.
I want to caveat this up top with REALLY IMPORTANT CONTEXT: I did not do all of this in a single day. The process from starting research to making an evaluation appointment took about a month, and probably would have taken longer if I wasn't getting somewhat desperate. Do not push yourself to do this as a single act. Research alone is a multi-day process; some days I looked at the open tabs and only entered one tab's worth of information. It took me quite a bit of time to write the form email I sent inquiring about an assessment. It took me time to call the clinic back when they asked me to call to book the appointment. This is a series of steps, not a single leap.
So!
I was looking for a clinic rather than an individual, in part because I'd heard a couple of horror stories about people who went to a psychiatrist and just got argued with for an hour instead of actually getting evaluated. So I googled, and here are some key terms for you, chicago adult adhd assessment. Chicago obviously for the region, but "adult adhd" (putting it in quotes will help) is the important term that will help you filter out a lot of child psych stuff. A lot of what I looked at did included family or child assessment/therapy but were clear that they also evaluated adults.
Then I went through every legit-looking search result and noted down, in my spreadsheet, the name of the clinic/company, the contact phone and email, the URL, the physical location (I needed to be able to get to it fairly easily) and whether they took my insurance. Even if they didn't take my insurance (all but one did) I still put them into the spreadsheet so that if I found them again I could check the sheet and know I didn't need to investigate further. I also tended to bump more legitimate and friendly-looking places to the top of the sheet. And if I were going to do it again I would also look for one specific thing, which is an assessment guide of some kind.
The assessment guide may be something they only give you after you speak with them, so it's not a no-go if they don't have one on their website, but it basically tells you what generally will go on during the assessment, how long it will take, and what you should bring. A full assessment like I had is estimated to take 4-6 hours and they recommended I wear layers so I wouldn't be overly cold/warm in their office, and to bring a snack. That's the kind of information you want, duration of the assessment and what they recommend for you, to ensure that you're working with people who are thorough and care about your comfort.
So, I have this spreadsheet now of places to reach out to, which I know take my insurance and do adult assessment. In the spreadsheet I also had columns for what date I contacted them and whether they'd responded. I started reaching out via email, one per day, with the form email I'd written.
The form email basically said "I'm 42 with no previous diagnosis but I have a family history of autism and dyslexia. I've been told I should get assessed for ADHD, so I'm looking for a clinic that will do the assessment and takes (my insurance). I prefer to be contacted by email but if need be, my phone number is (phone number). Please let me know if you have any open appointments and what information you will need from me to book an evaluation with you." (You can always ask for more information about the actual evaluation process once they respond.)
If I didn't get a response within 24 hours, I moved on to the next, but I only greyed out the text in that line of the spreadsheet; I didn't disqualify/remove the nonresponsive ones because again, I wanted to make sure I kept that information in case they eventually did respond. I did this with about ten clinics, because I figured I must be able to find at least one in ten who could do the eval, and I could go back and research more if necessary.
I think the third or fourth one I reached out to was the first to respond, and I ended up going with them; I had a very positive experience in the assessment itself but it was a real pain in the ass getting the documentation from them -- they took about a month to go through the evaluation data (this is not abnormal but is rather longer than usual according to my psychiatrist) and they gave me an in-person-by-zoom report once it was ready. That said, it took another four months and the threat of reporting them to the state to get them to send me the text of the eval (in part because the evaluator left the clinic unexpectedly with my formal report not yet written). But that's something that's truly impossible to know until you're working with them, and highly unusual, so don't let concerns about that deter you. If you end up in that situation come hit me up and I'll tell you how I dealt with that.
My eval recommended an executive function coach, but if I haven't been able to func it by now I never will, so I thanked them for the recommendation and went looking for a psychiatrist unaffiliated with the clinic to prescribe me meds. There, the key words you're going to be looking for are again "adult adhd" but also "adult disability" and if you want medication that's less likely to be a huge fucking hassle, "medication management". My psychiatrist and I meet every two months to reup my prescription, but he doesn't require me to take a regular drug test or meet him in person in order to get a new scrip, as some people have encountered. We meet in person once or twice a year (I can't remember, it's due to a legal requirement in Illinois) but otherwise it's over zoom.
So yeah -- it's a process, but there are ways to streamline and manage it, and a few tripwires in place to make sure you don't end up screwed by the system. Definitely feel free to ask if you have questions, either here or if you want a more indepth conversation you can email me at [email protected]. GOOD LUCK!
314 notes
·
View notes
Text
Independence day? The very foundation of Independence is safety. What is the point of hoisting the tricolor when the white is stained with red.
There was a time when people believed of this profession as next to God's, people would fall into the feet of healthcare workers, join their hands to thank them. I think you guessed it already, medicine. And now?
"A female doctor resting in R.G. Kar hospital's seminal hall gets raped, brutalized, murdered."
"a doctor was tied to a tree, robbed and his wife and daughter gang-raped in Gaya district of Bihar"
"two resident doctors of Banaras Hindu University were beaten up by patient's attendants and goons"
"Two resident doctors of JJ Hospital, Mumbai were beaten up by patient's relatives"
"Two medical residents working at the Sassoon Medical College were brutally thrashed; a junior resident doctor suffered a skull fracture; a doctor suffered fractured ribs and broken bones"
"a junior lady doctor on night duty was stabbed to death by a patient"
And this has recently come to light. We have never even talked about our nursing staff and the amount of harassment they face. If doctors commit suicide from exploitation and extreme mental and physical breakdown, nurses commit suicide as result of extreme harassment and abuse, be it physical, sexual, mental. I hope everyone remembers Aruna Ramchandra Shanbaug.
The non-medic communities are not even willing to take a stand for us.
Everyone wants world-class but affordable treatment, even free treatment, free medicines and empathetic and responsible doctors, but no one has the bloody balls to take a stand and raise their voices for us.
This is not what our families sent us for. This not what we opted for. This is not what we're working are assess off for.
#desi tumblr#desi tag#being desi#desi things#desi dark academia#desi girl#desi#indian students#indian#india#indian memes#doctor#doctors#crime against humanity#crimes against women#crimes against humanity#healthcare#nursing#nurse#medicare#medico#tw: violence#tw: death#tw: rape#tw: abuse#kolkata#west bengal#nirbhaya#delhi#new delhi
148 notes
·
View notes
Text
By: Andy L.
Published: Apr 14, 2024
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
-
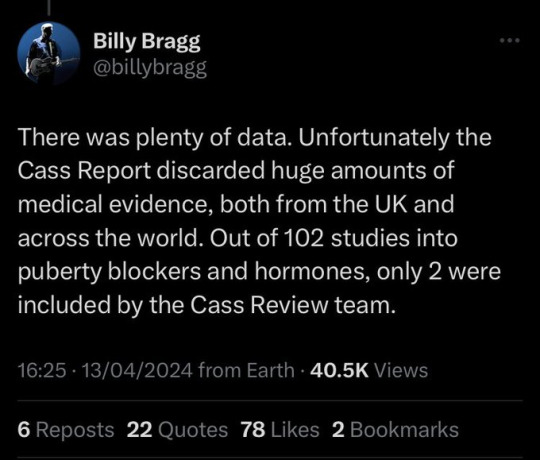
Myth 1: 98% of all studies in this area were ignored
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
-
Myth 2: Cass recommended no Trans Healthcare for Under 25s
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
-
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
-
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
==
It's not so much "myths and misconceptions" as deliberate misinformation. Genderists are scrambling to prop up their faith-based beliefs the same way homeopaths do. Both are fraudulent.
#Andy L.#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#misinformation#myths#misconceptions#detrans#detransition#gender affirming healthcare#gender affirming care#gender affirmation#affirmation model#medical corruption#medical malpractice#medical scandal#systematic review#religion is a mental illness
380 notes
·
View notes
Note
Hi! Would you please write one with Matt/Kelly/Jay x reader where the reader is walking home or something and gets attacked. Roughed up a bit maybe a concussion and like a dislocated shoulder... but she manages to get away before anything too bad happens and just runs on instinct to 51. Kelly and Matt all worried and trying to comfort her but she’s in shock. Sylvie and Violet take care of her and take her to med. Jay meets them there. Maybe with worried brother-in-law Will and a Connor appearance?
Messed with the wrong one- Matt, Kelly, and Jay
Warnings: attack briefly described, vomiting, possibly wrong medical jargon
————————————
You have always been decently independent, which is something that your boys love and hate at the same time. You enjoy doing the grocery shopping and often find yourself walking the short distance to the small neighborhood market around the corner from your shared home. Today was no different.
It was late in the afternoon. The sun was just starting to set and you were happily enjoying watching the beautiful colors change in the sky. Jay was still at work, you having been able to leave early since you finished your paper work, but Jay still had a few files left to tidy up. Your errands could have waited, but you had the time now. So, while Matt, Kelly, and Jay were all still at work, you planned on getting a head start on dinner.
You were two blocks from the market when you felt four hands grab you and drag you into a nearby ally. All your training kicked in and you fought back as hard as you could. All you could think about was getting home to your boys. You kicked and punched, having to drag yourself off the ground twice. The second time you found yourself on the ground, your head also found purchase on a brick wall. You quickly shook it off and stood, laying one guy out and dodging the other, bolting down the ally and running as fast as you could. You didn’t dare look back.
Next thing you know, you are running through the bay doors of 51 and Kelly is snatching you up in his arms. You are violently shaking, blood tricking down your neck and face. You don’t respond when Kelly talks to you, given the fact that you can’t hear him over the ringing in your ears. You notice blurred figures run past you and out of the bay doors, others running out of the firehouse to see what the commotion is all about. Matt comes to your side, but you flinch and scream when he touches you.
“Shhh. It’s okay. It’s okay. It’s just Matt.” Kelly whispers, rocking you back and forth in his arms. He isn’t sure you hear him, but you relax as you bury your face into his neck and breath in his familiar scent.
Matt doesn’t attempt to touch you again. Not yet anyways, but he thinks he understands why you screamed now. Your left arm is cradled between you and Kelly protectively, leading Matt to believe that your hurt. “Kelly. She’s hurt pretty bad.” Matt whispers, walking around you slowly to examine you with only his eyes.
Kelly nods. “I know. I know baby. Let’s sit down, yeah?” Kelly says, acknowledging Matt and guiding you to sit in his chair at the squad table.
Brett and Violet are standing at the ambo with the doors open. They are both assessing you from afar until Matt and Kelly can get you focused or give them permission to approach. Brett can tell you are slipping into shock, but she doesn’t want to make things worse, so she waits.
It doesn’t take long after Kelly gets you sitting down. His hands pushing your shoulders to lower you down has you screaming in pain. Matt steps aside and waves the medics over, allowing Kelly to keep a hold on you since he got to you first.
“Y/n? It’s Sylvie Brett. Can you hear me?” Brett asks, crouching down to find your tear filled eyes. When you nod, Brett smiles warmly at you. “Good. Good. Can you tell me what hurts?” Brett asks, not yet laying a hand on you.
You gently run your right hand over your collar bone and then touch the back of your head. When your hand comes away with blood, you start shaking harder and hyperventilating. You didn’t feel that.
“Hey. Hey. Baby. It’s okay.” Kelly soothes, taking your hands in his. He carefully wipes them off with a towel that Violet offers as Brett stands to examine your head wound.
“Pretty deep.” Brett comments. At this point, you have lost most of the color in your face and are sweating pretty heavily. Brett can tell, without checking your vitals, that the shock is fully setting in. “Kelly. Get her loaded up. Violet, run inside and tell Boden what’s going on then drive us to med. Matt, call med and have them set up a trauma room and have x ray and CT ready upon arrival.” Brett instructs, putting her feelings as your friend aside to get you help quickly.
Everyone jumps to their tasks. Kelly scoops you up and apologizes as you cry out in pain from the movement. Brett gets in the ambo and immediately pulls out some pain killers and an Iv tray for you. She hands Kelly a towel to keep pressure on your head wound as she hooks you up. You barely flinch as the Iv is stuck in your hand, but begin to calm slightly as the meds take over.
When you stop whimpering, Brett moves to check your chest. “Y/n. I gotta look, okay? No pressing. I promise. Just gotta make sure that everything is still relatively where it’s suppose to be.” Brett said, not wanting to scare you with the fact that your bone could potentially be out of your skin or at an alarming angle or something.
You nodded, leaning your head further into Kelly’s hold as Matt finally jumped in and the ambo began moving. You groaned as the movement caused nausea to spike as your head swam. “Mmmm.” You ground out, trying to breath through the nausea.
“What’s wrong hunny?” Brett asked, pulling back from looking at your collarbone, which seemed to be in place, to look at your face. You had gone pale once again, your face scrunched up as you shakily brought a hand to your mouth. “Okay. Hang on.” Brett said, pushing Kelly forward to lean over and grab a sick bag for you. Matt immediately took it and held it under your chin so that Brett could keep examining you.
“M-Matt.” You gasped, clutching onto his wrist when he came into view. It was like you were just processing that he was even around at all.
“Shhhh. I’m here baby. Kelly and I are here.” Matt soothed, using his free hand to wipe tears from your face. “We are almost to med. We gotcha now.” Matt murmured, hating to see the pain and fear in your eyes. He wanted nothing more than to find whoever did this to you and lay into them, but you were his first priority.
Matt’s thought process was cut short when you heaved, flying forward with a scream of pain at the end of it. Kelly stood, holding your forehead in one hand and the cloth to the back of your head with his other hand. Matt held the bag around your mouth, holding one of Kelly’s arms to stop from trying to steady you or put his hand in the wrong place and hurt you more instead o comforting you.
“Brett. You gotta do something.” Kelly said, trying not to burst into tears as you threw up, screaming when you had enough air. You were shaking violently again, the pain and the vomiting causing your body to go into overdrive.
“Kelly. I can’t. We are two minutes out. I gave her enough to take the edge off, but they gotta assess her before she gets anything else on board.” Brett tried to reason, wiping tears from her own face as she attached wires to you to check your vitals. “I’m so sorry Y/n. I’m so sorry. We are getting you to med.” Brett whispered, her heart aching as she watched her friend get sick and scream while her other friends desperately tried to help.
As soon as the ambo got to Med, Conner Rhoads, Maggie, and your brother in law, Will Halstead, were pulling open the doors. Will stood slightly away, knowing he couldn’t treat you, but he also couldn’t leave you and the boys until Jay got there. Luckily, Jay had been notified by Will when he found out, so he knew his brother would be there soon.
“What do we got?” Conner asked, helping Brett get the stretcher out of the ambo as Kelly kept up, one hand still holding the cloth to your head while the other held the bag Matt had to secure it under your chin as you gagged.
“Deep head lac and suspected broken collar bone. The vomiting started about 4 minutes ago. GCS 6, 140/97, pulse 120, O2 95 on room air.” Brett spout out. “Iv in the field. Left hand. Administered 5 of Morphine to take the edge off.” Brett said, getting your sheets in her hands.
“Okay.” Conner said, “On my count. 1, 2, 3.” Conner counted, then helped transfer you onto the hospital bed. You screamed out again as they moved you, then proceeded to pass out. “She’s out. Elevate her feet. Tip the bed.” Conner instructed, following your head down as you were moved. He checked your pupils and palpitated your collarbone while you were out. “I can feel some inflammation around her collar bone on the left side. Most likely broken, but still in place. She also has a minor concussion. I’m gonna have them do an xray and CT just to make sure on both.” Conner said, standing and looking at the monitor. “Maggie, put her on 5ML of oxygen. Her stats are dropping some. Probably from the pain. Let’s go ahead with another 15 of morphine and some Zofran too.” Conner said, typing it all up pretty quickly.
You began to stir as Kelly pushed some fly away back. Conner was quick to get to you, repositioning the bed to a more comfortable position and checked your head lac. Your eyes fluttered open just as Conner was stepping back.
“Welcome back.” Connor said with a smile. “Your gonna be okay. We need to run some tests, but I think that you’ll only need a few stitches and all you’ll need is a sling to stabilize that arm while your collar bone heals.” Conner supplied, smiling as he heard Matt, Kelly, and Will sigh in relief.
You nodded, then winced. “Hurts.” You whispered, throat raw from throwing up.
Conner nodded and moved aside for Maggie. “Mags is gonna give you more morphine and some Zofran. Sound good?” Conner asked, searching your face for confirmation. When you you gave a shaky thumbs up, he smiled. “Good, I’ll check back in a bit.” Just as Conner was leaving, Jay skidded to a stop as he came barreling through the door, almost hitting Conner in his haste to get to you.
“Baby girl.” Jay breathed, patting Conner on the shoulder and going around him to get to you. He was sweating, eyes wild as he searched your body for injuries, hands and bottom lip shaking.
“J-Jay.” You immediately sobbed out. “I’m sorry. I’m so sorry.” You wailed, covering your face with your right hand.
Jay shook his head as he laid a hand on your leg. “Shhh. No baby. No. It’s okay. It’s not your fault sweet girl.” Jay soothed, rubbing your leg over the blanket. “We got them. Voight and Antonio have them. Your safe.” Jay soothed, smiling sadly at you.
“She was so smart and so brave. She ran straight into the bay doors of the fire house.” Kelly praised, kissing your forehead.
“You know your always safe with us.” Matt said, rubbing one of your feet over the blanket.
“I-I didn’t even think. I j-just ran.” You sniffed, wiping your face with the back of your arm. “I just thought a-about you guys. I-I needed to get h-home to you guys.” You murmured, tears streaking down your face again as the horrors of the event began to creep into your head.
“You’ll be home tonight sweet girl. Until then, we are here.” Jay soothed, moving forward as Maggie walked out, kissing your forehead gently. “You did so good Angel.”
“I’m home here with you guys. Wherever you are is home.” You whispered, finally relaxing as the drugs numbed the pain and the nausea. You were exhausted and you knew your boys would keep you safe, so you allowed your eyes to slip closed.
——————
Tag list:
@treehouse-mouse
@shadowmeadowsworld
@sorry-i-spaced
@zephyrmonkey
@allisonargent144
@amie134
@lane-rodgers-barnes
@pensfan5871
@dumb-fawkin-bitch
@marvel-and-chicago-fan
@daggersquadphantom
@stellakiddsblog
@100yroldteenagers
@senjoritanana
@celtic-shadow-wolf
@starset21
#one chicago#one chicago x reader#matt casey#kelly severide#jay halstead#matt casey x reader#jay halstead x reader#comfort#kelly severide x reader#fluff#emeto fic#emeto tw#tw emeto
348 notes
·
View notes
Note
hello!! i saw you were asking for more spencer x sunshine!reader requests and here i am!!
do you think you could do something where reader has chronic pain in her hips and walks with a limp most of the time, but once it gets super super cold it starts to hurt more so she has to use a cane..? it’s getting colder where i live so i’ve slowly had to start using my cane, but i always get embarrassed/insecure about using it in public so some days i go without and then immediately regret it!! haha
of course you don’t have to write this is you don’t want to!! i’m sure i have tons of other ideas up in my noggin haha. love you and take great care of yourself!! xxx
I hope you like this, I googled some aids for the pain so hopefully this is good and if there’s anything that’s wrong please please let me know
The groundhog lied, it’s snowing when it’s supposed to be sunny.
You should’ve known you would’ve been in pain all day when the night before when your hip started locking more and more.
Still, you dress for the weather and put on a pair of thermal tights under your navy dress suit. You can’t be bothered with pants.
You stare at your cane as you reach your front door, biting your lip as you deliberate.
On one hand, you could take it and ease the pain off your hip, or you could leave it and save the embarrassment you feel for needing it so young.
In a split second you make your decision, limping out the door without it.
You regret your decision to also wear kitten heels when you hobble into the bullpen, Spencer’s eyes immediately catching the uneven drift in your walk. He notices your easy outfit too, a pleated blue skirt with a breathable blue top to match, no blazer today.
“What’s wrong?” He asks, crossing his desk and making his way over to you but you wave him off.
Spencer ignores that completely and reaches you in seconds, eyes assessing what you refuse to say.
��Spencer I’m fine, I just slept wrong.” It’s obvious he doesn’t believe you when he cocks an eyebrow. Spencer’s already noticed a slight lean to your walk, your very obvious limp and the way that your smile seems to border grimace.
His hands reach for hips as he closes the little gap between you.
“Oh aren’t you forward,” you smile through your words but Spencer knows there’s something different to your tone.
“Would you shush? It’s more swollen than it should be if you slept wrong.”
His brown eyes pin you and make it hard to lie to him as you stare him down. You want to ask how he knows it’s your hip, but he’s got a big, genius brain, it really was silly to think you could hide it from him.
“Spence, it’s okay.” You say, twisting out of his hands and hissing when you do so, your hip cracking at the motion. Tears prick your eyes.
“You’re a terrible liar, come sit down.” He leads you to his chair, hands gentle as they touch your lower back and hip. “What’s going on with your hip, darling?”
You blame the way you just instantly open up about what you term your worst feature, to the fact that he’s dropped a pet name like that so casually.
“I suffer with my hip, flare ups mostly during winter and it’s chronic. I have a cane but it’s embarrassing to need one so young so I don’t use it and it hurts more but at least I have my independence.”
Spencer shakes his head, touching your cheek. “I know that’s how you feel, but if it’s cracking like this you at least need a balm if you don’t want the cane. Or I could get you compression pants for it.”
You scrunch your nose at the emotion suddenly building in your throat, “I do have a balm but the smell is too strong. Doesn’t go with my perfume.”
Spencer laughs, fully shaking his head at you. He thinks for someone so happy all the time, you shouldn’t worry half as much as you do. Certainly not about if your medicated balm will go with your perfume.
“Come with me,” he says, taking your bag from you and setting it on his shoulder.
“Where are we going? Mid morning pick me up? Rendezvous in the bathroom stall?” Your eyebrows dance and Spencer shakes his head, maneuvering his body so you’re leaning on him more than walking on your own.
“No, we’re going to the bathroom so you can apply more balm and then I’m going to your place to get your cane.”
You stop walking, heels cutting off with an abruptness, that if Spencer hadn’t been anticipating it you would’ve fallen from his grip.
“No Spence, it’s fine. I’m used to it.” He starts walking again, bringing you with him to the bathroom and sitting you on the sink’s edge.
“I know you are,” he rifles through your bag, grinning when he finds the tube of medicated balm. “But humor me for a moment and say it’s a little worse than usual, so you need it?”
You huff, “Can’t I just use the compression stuff?”
Spencer looks up, surprise lighting his eyes but a knowing, almost smug smile plays on his lips.
“Yeah?” He does a wicked evil thing by stroking the tops of your thighs and tilting his head just a little so some of his curls fall in his face.
“Spencer,” you push at his chest, grumbling when he laughs. He holds your palm to his chest, “I can do this part myself.”
“Promise you’ll actually apply the rub? I need to go out to get the compression pants.”
You shake your head, “I’ll get one after work Spence, the balm is enough.”
He doesn’t listen to you, “Apply the balm, I’ll be twenty minutes.”
You’re one hundred percent sure he takes Anderson with him to drive the SUV and is back in twenty minutes with two different pairs of compression pants, pain relievers and muscle relaxants.
#spencerreid#spencer reid#spencer reid one shot#spencer reid fanfiction#spencer reid imagine#spencer reid drabble#spencer reid blurb#spencer reid fluff#spencer reid fanfic#spencer reid fic#dr spencer reid#spencer reid x black reader#spencer reid x reader#spencer reid x yn#spencer reid x you#spencer reid x y/n#spencer reid x sunshine!reader
339 notes
·
View notes
Text
(OOC: Reposting the summary I made to stand on its own for people who caught bits of it but don't want to have to switch between several different blogs)
A THOR-class NHP named Arthur entered cascade in Harrison Armory's PR offices. He caused significant electrical damage to the offices but as far as I can tell no one was seriously injured, and the PR intern, Jimbo, managed to calm him down. The situation now seems to be resolved amicably.
Rev, an AGNI-class NHP implied that they caused Arthur to cascade. Recent comments by them suggest that they did this to advance the cause of NHP equality (forgive my rumormongering, but I have my doubts. Their omninet page contains a great deal of what seem to be boasts of war crimes and genocide, they don't strike me as much of an egalitarian. That said, my Loyal Wing tells me she's met and fought cultists who earnestly believe in a future where humans and NHPs are free to inflict horrific atrocities upon one another, so who knows. People are complicated. I'm also unconvinced Rev actually did cause Arthur to cascade, the manner they describe seems implausible.)
The Corsair Mercenary Company and the squad commander of the MSMC 796th, Kennedi/Lockbreaker, were angered by this claim. I'm not sure why this incident, which Jimbo resolved well before there was a actual fighting, prompted her to act independently, but there was some indication of the security breach having wounded her pride. (It is also possible that they were, in fact, being contracted by a HA higher-up and only pretending to act independently). She recruited another squad, the MSMC 148th, and they set out for Rev's abode in Karrakin space.
Rev caused the NHP at Corsair Mercenary Company, which named themself [STABBY], to cascade. [STABBY] then took control of several subalterns and systems and attempted to kill the CMC, inflicting a high casualty count before being shut down by MSMC 796th's "Slipshod" using a liturgicode virus. (Based on [STABBY]'s rapid decision to attempting to kill the CMC once given the ability to do so, even if during cascade, it seems likely that they did not have a positive relationship and allegations of abuse seem credible)
The MSMC squads arrived and engaged Rev's Genghis body and a group of Hercynian lancers Rev had recruited via Hercynian Refurbished Armaments. The battle ended with both Rev and Lockbreaker's mechs effectively destroyed, Rev's casket damaged and Lockbreaker in critical condition. There was significant collateral damage dealt to the planet, though fortunately no civilians, bystanders, or other innocents were harmed.
Albatross long patrol "Osprey" received several distress calls from the area and rerouted to investigate. When they arrived, medics were able to stabilize Kennedi and assess the situation. Rev was recovered by "an associate", the MSMC squadrons were able to contact command and get returned to headquarters, and I belive the Hercynians returned to Hercynia. After assisting local damage control and double-checking that no one was hurt, long patrol Osprey will be returning to their nearlight patrol route.
109 notes
·
View notes
Text
Dr. Dad
part 1
This picks up where we left off from part 1. I am still learning how to link post and such so cut me some slack please lol
Pairing : Simon "Ghost" Riley / Reader
The reader is a 5th year resident that just had a baby with Simon who is an Attending. The reader does not want anyone to know that they are together until she makes fellow at the hospital.
He lets out a little smirk. His face turns serious for a moment.
“My love know you don't have to come back to work so soon”
You sigh you knew that was coming. He’s been saying this since you told him that you were going back to work last week after you placed Bella into her bassinet. He was silent for a while just standing in the doorway of the bathroom.
Looking at you.
Assessing you.
Trying to think of something to say to convince you not to do.
You had a relatively easy birth, having the birth of the baby at the hospital closest to your home and not the one you work at. It's not that you don't want anyone to know about you and Simon but , the relationship started when you were on his surgical rotation which is not allowed. You did let HR know about the relationship after you were off his rotation and the start date of your relationship officially is when you started your oncology rotation, which you really needed support for anyway.
When you fell pregnant you told Simon almost immediately. It was not an ideal time , you were a fifth year resident with little to no time on your hands , drowning in student loan debt, and you're barely making 60k a year. Simon on the other hand is an attending physician with over 6 years of experience in the field and 3 years working at the hospital. He was happy and together you let the medical director know about the relationship and pregnancy and those are the only people you told.
When you started to show , there was a lot of rumors surrounding you.
It has to be one of the other residents , its the xrays tech baby , she always gets her patient pushed to the front
You did nothing to dispel the talk, much to Simon’s disagreement.
“Let me say something”, he says one night after a 16 hour day.
“You can say something , just don't say that your mine” you say
You have an issue with being hyper independent, you realize that in fact a little to much. You love Simon but you let him know that you will be a working mom , you will be keeping your last name, and no one will know that you are dating Simon until you make Fellow , which is why you need to get back to work.
Your mother was a godsend and also retired so when you called and let her know you were going back to work she didn’t try to convince you not to do it she just ask,“how can I help.”
A knock on the door brings you back to the present.
You sigh and proceed to unlatch the breast pump and hand them to Simon. He has a mini fridge and you dont trust these other residents to not fuck with your milk.
Another this time harder and longer
“One Second” you say brightly. While Simon glares at the door while towards it to unlock it.
One of the 3rd year residents walks in and looks a little a pale. Lets you know that Graves is looking for you.
"Does he seem upset", You don't really care if he is but you would like to prepare how preppy you should act towards him. You firmly believe in killing people with kindness especially when it has to do with Graves who probably drinks Interns tears for breakfast , lunch and dinner.
"Is he bother you?", Simon ask. To anyone else it sounds like a normal question one of concern from a colleague. But you know he's worried he ask the question like it pains him from going to find Graves and tell him to lay off. No one likes Graves but he technically isn't doing anything wrong , he has the right to kick anyone out of his OR, to make interns scribe all his charts , and terrorize his residents until they rather to scut work then be in presence.
"Nothing that I can't handle" , you smile at him and then look to the resident that was sent to retrieve you.
"I'm right behind you", the resident turns and just about runs out the room.
You hand the milk to Simon and place a quick kiss on his lips, he makes an almost groaning sound and drags you back for another kiss , a deeper kiss with his hand tighting around your hips. You pull away with a little giggle, "I miss you too" you say , your eyes lowering that makes it known exactly what you miss.
You straighten your clothes back up , make sure that you don't look at tired as you seem and head out to another 4 hours of running around like you are fresh intern right from medical school and not a tired mom that just wants to sleep on the couch holding your baby.
#simon riley x reader#simon ghost riley#ghost call of duty#cod 141#cod#medical fanfic#I really like medical drama lol#I take inspo from ER and Grey's
74 notes
·
View notes
Text
The Importance of Independent Medical Assessments: What to Expect
Introduction
Independent medical assessments play a crucial role in various aspects of healthcare, providing impartial evaluations of an individual's health status, injuries, or medical conditions. Whether conducted for insurance claims, legal proceedings, disability determinations, or workplace-related matters, these assessments offer objective insights that help facilitate fair and accurate decision-making. This guide delves into the importance of independent medical assessments, outlining what individuals can expect from the process and how it contributes to ensuring proper medical care and support.

Understanding Independent Medical Assessments
Independent medical assessments, also known as impartial medical evaluations or third-party medical assessments, involve the evaluation of an individual's health condition by a healthcare professional who is independent of the individual's treating physician or healthcare team. These assessments are typically requested by insurance companies, legal entities, employers, or government agencies to obtain an objective opinion regarding an individual's health status, functional capacity, or medical impairment.
Importance of Independent Medical Assessments
Objectivity and Impartiality: One of the primary advantages of independent medical assessments is their objectivity and impartiality. Unlike assessments conducted by treating physicians who may have a vested interest in the patient's care, independent assessors provide unbiased evaluations based solely on medical evidence and clinical findings.
Verification of Medical Claims: Independent medical assessments help verify the accuracy of medical claims made by individuals seeking compensation, benefits, or disability accommodations. By reviewing medical records, conducting physical examinations, and performing diagnostic tests, assessors can confirm the presence, severity, and causation of injuries or medical conditions.
Clarification of Medical Disputes: In cases where there are disagreements or disputes regarding medical diagnoses, treatment plans, or disability determinations, independent medical assessments serve as valuable tools for resolving conflicts. The impartial opinion of an independent assessor can help clarify medical issues and facilitate consensus among involved parties.
Assessment of Functional Capacity: Independent medical assessments evaluate an individual's functional capacity, including their ability to perform activities of daily living, work-related tasks, or specific physical activities. These assessments are crucial for determining an individual's level of impairment or disability and informing decisions related to vocational rehabilitation, job accommodations, or disability benefits.
Facilitation of Fair Decision-Making: Independent medical assessments contribute to fair and equitable decision-making in various contexts, including insurance claims, legal proceedings, worker's compensation cases, and disability determinations. By providing objective medical opinions based on thorough evaluations, these assessments help ensure that individuals receive appropriate medical care, support, and compensation.
What to Expect During an Independent Medical Assessment
Pre-Assessment Preparation: Prior to the assessment, individuals may be required to provide relevant medical records, diagnostic imaging reports, and other documentation related to their health condition or injury. It's essential to gather and organize these documents to facilitate the assessment process.
Physical Examination: Independent medical assessments typically involve a comprehensive physical examination conducted by a qualified healthcare professional. During the examination, the assessor will assess various aspects of the individual's health, including vital signs, range of motion, strength, reflexes, and sensory function.
Medical History Review: The assessor will review the individual's medical history, including past illnesses, injuries, surgeries, medications, and treatments. A thorough understanding of the individual's medical background is essential for accurately assessing their current health status and identifying any pre-existing conditions or risk factors.
Diagnostic Tests and Assessments: Depending on the nature of the assessment, the assessor may order additional diagnostic tests or assessments to further evaluate the individual's health condition. These may include blood tests, imaging studies (such as X-rays, MRI, or CT scans), functional capacity evaluations, or psychological assessments.
Interview and Discussion: The assessor may conduct an interview with the individual to gather information about their symptoms, limitations, functional abilities, and impact of their health condition on daily life activities. Open communication during this process helps ensure that the assessor obtains a comprehensive understanding of the individual's health concerns and needs.
Documentation and Reporting: Following the assessment, the independent assessor will prepare a detailed report summarizing their findings, observations, and medical opinions. This report may include information about the individual's diagnosis, prognosis, treatment recommendations, functional limitations, and any other relevant factors.
Conclusion
In conclusion, independent medical assessment play a crucial role in various aspects of healthcare, providing impartial evaluations that contribute to fair decision-making and proper medical care. These assessments offer objectivity, verification of medical claims, clarification of medical disputes, assessment of functional capacity, and facilitation of fair decision-making. Individuals undergoing independent medical assessments can expect a thorough evaluation process, including pre-assessment preparation, physical examination, review of medical history, diagnostic tests and assessments, interviews, and documentation/reporting. By understanding the importance of independent medical assessments and what to expect from the process, individuals can navigate the assessment process with confidence and ensure that their healthcare needs are accurately assessed and addressed.
0 notes
Text
U.S. spy agencies verified Israeli claims that Hamas and another Palestinian terrorist group used Shifa Hospital in Gaza City as a command center and to hold hostages, The New York Times reported on Tuesday.
In late November, the Israel Defense Forces released extensive video evidence of terror tunnels under Shifa Hospital—the Gaza Strip’s largest medical facility—saying it “unequivocally” proves the modus operandi of Hamas, “which systematically operates from hospitals.”
The terrorist group held at least three of the estimated 240 hostages it kidnapped on Oct. 7 at Shifa, the IDF said.
Nevertheless, critics continued to claim that the IDF had little evidence Hamas used the hospital as a command post.
“In the weeks since the operation, news organizations have continued to raise questions about Hamas’s presence at the hospital. And health and humanitarian organizations have criticized the Israeli operation. A humanitarian team led by the World Health Organization, which visited Al-Shifa immediately after Israeli forces stormed the hospital, called it a ‘death zone,'” the Times reported.
But a senior U.S. intelligence official said Tuesday that the American government was convinced that Hamas used the hospital complex to direct terrorist forces, store weapons and hold “at least a few hostages.”
The official also said U.S. spy agencies had information that Hamas destroyed evidence before the IDF operation at the hospital got underway.
A U.S. official expressed confidence in the intelligence assessment as it was based on information gathered independently by both Israel and American agencies.
In November, the IDF recovered the body of Cpl. Noa Marciano, who was kidnapped by Hamas, in a building adjacent to Shifa Hospital. Also found next to the hospital was the corpse of another hostage, Yehudit Weiss.
Israeli forces arrested the hospital’s director, Muhammad Abu Salmiya, on Dec. 23.
“In the hospital, under his management, there was extensive Hamas terrorist activity. Findings of his involvement in terrorist activity will determine whether he will be subject to further ISA [Israel Security Agency, i.e. Shin Bet] questioning,” the IDF said in a statement.
194 notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
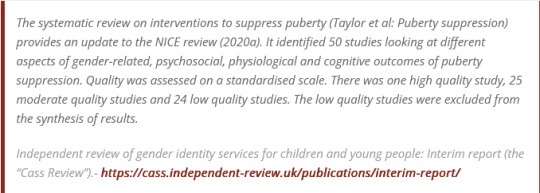
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
100 notes
·
View notes
Text

╰ ᥫ᭡. ⋆· ˚ ༘ * SEVENTEEN LUNA FILES

Bae Jiyeon ❨ 배지연; born January 30, 1997 ❩ known mononymously as Luna, is a Korean-English singer. Born and raised in Kensington, London, United Kingdom. Luna lived in the United Kingdom for fourteen years before returning to South Korea in 2011. She is a member of the South Korean co-ed band SEVENTEEN and its fixed sub-group the Vocal Team.
╰ ౨ৎ BASICS
Birth Name: Bae Ji-Yeon ❨ 배지연 ❩
English Name: Luna Bae
Stage Name: Luna
Birthdate: January 30, 1997
Birthplace: Kensington, London, United Kingdom
Nationality: Korean-English
Ethnicity: Korean
Spoken Languages: Korean ❨ fluent ❩, English ❨ fluent + English accent ❩, Japanese ❨ intermediate ❩
╰ ౨ৎ ARCHETYPES
Zodiac Sign: Aquarius
Chinese Zodiac Sign: Ox
MBTI: INTJ
Hogwarts House: Slytherin
Godly Parent: Hades
╰ ౨ৎ PHYSICAL
Height: 169cm ❨ 5’6" ❩
Weight: 43kg ❨ 94lbs ❩
Blood Type: O+
Hair Color: Black
Eye Color: Brown
Body Modifications:
Piercings: Lobe ❨ 3 on each ear ❩, Conch ❨ right ear ❩, Helix ❨ 2 on each ear ❩, Flat ❨ left ear ❩, Tragus ❨ both ears ❩, Rook ❨ both ear ❩, Daith ❨ right ear ❩, Forward Helix ❨ right ear ❩, and Belly button piercing
Tattoos: The number 17 ❨ side of right wrist — dedicated to the band ❩, Crescent moon ❨ side of left wrist — dedicated to her name ‘Luna’ ❩, The letter J in cursive ❨ inside her left ring finger — her initial from her name ‘Jiyeon’ but some fans theorize it’s for ‘Jeonghan’ ❩, A ribbon/bow ❨ on the back of her right hand — her trademark love for ribbons and bows ❩, ‘Lady of the Moon’ calligraphy ❨ by her right rib cage — a nod to her name once more ❩, ‘eventually’ calligraphy ❨ inside her right middle finger — just like she said, “Eventually everything that is for me will come.” ❩, and ‘lovebug’ calligraphy ❨ on the back of her neck — the nickname her grandparents had given her ❩
Unique Features: Dimple on right cheek, piercing siren eyes ❨ cat-eye/ foxy shaped ❩, beauty mark on right cheekbone and left cheek, smirk smile
Medical Conditions: Anemic and has a former collarbone fracture caused after falling during a ballet routine when she was 10 years old
╰ ౨ৎ LUNA CLAIMS
Face Claim: Jang Wonyoung ❨ IVE ❩
Singing Voice: IU
Speaking Voice: Jang Wonyoung ❨ has a naturally deep voice when she speaks, however gets higher when she whines and unironically and unknowingly does aegyo ❩
Dance Style: Momo ❨ TWICE ❩ — SEVENTEEN performances, Kazuha ❨ LE SSERAFIM ❩ — Ballet performances
╰ ౨ৎ PERSONALITY
MBTI: INTJ ❨ The Architect ❩
Personality Traits: As an INTJ, often referred to as ‘The Architect’, Luna embodies a unique blend of intelligence, strategic thinking, and an independent spirit. Her personality reflects a deep understanding of the world around her, often viewing situations through a logical and analytical lens. This makes her an exceptional problem-solver, able to assess challenges and devise effective solutions with ease.
Growing up in Kensington, London, Luna was immersed in a world of creativity and intellect. As an only child of a retired ballerina and an anthropologist, she was exposed to the arts and sciences from a young age. Her mother encouraged her to pursue ballet, starting lessons at the age of three. This early training not only honed her physical abilities but also instilled in her a sense of discipline and dedication. However, Luna often felt the pressure to excel, which led to her developing a strong work ethic and perfectionist tendencies.
Despite her outward confidence, Luna struggled with feelings of isolation. Her intimidating features and talent sometimes made it hard for her to connect with her peers, leading her to seek solace in books, art, and music. These experiences nurtured her introspective side, allowing her to develop a rich inner world filled with creativity and imagination.
During her training period, Luna’s INTJ traits truly shone. Her analytical mind enabled her to quickly grasp complex choreography and vocal techniques, allowing her to excel in evaluations. She was often dubbed the ‘Ace’ among her fellow trainees for her versatility and ability to adapt to various tasks effortlessly. However, this did not come without challenges; she faced moments of great pressure to live up to the title and of self-doubt, particularly in a competitive environment where she felt the weight of expectations.
Luna’s leadership qualities emerged during her training, as she often took the initiative to help fellow trainees improve. Her strategic mindset allowed her to navigate the often chaotic training schedule, and she quickly learned to manipulate situations to her advantage, especially during group activities or evaluations. While she maintained a somewhat aloof demeanor, her ability to connect with her peers through shared interests— such as crafts with Joshua or dance challenges with Hoshi— showed her capacity for forming meaningful relationships.
Now as a world known idol, Luna’s INTJ personality manifests in her strong presence and charisma on stage. She is known for her meticulous approach to performances, carefully analyzing each aspect of her shows to ensure they are executed flawlessly. Her strategic thinking allows her to anticipate audience reactions, making her a master at captivating crowds.
Luna’s intelligence also extends to her interactions with fans and the media. She navigates interviews and public appearances with ease, often using her wit and charm to leave a lasting impression. However, she remains somewhat guarded, finding it challenging to open up fully about her feelings, particularly in the context of her somewhat complicated relationship with Jeonghan.
While she is often seen as intimidating due to her ‘resting bitch face’, those who take the time to know her discover her warmth and loyalty. She is protective of her fellow members, particularly the youngest ones, and values the deep connections she has formed within the group. Luna’s ability to balance her independent spirit with her caring nature makes her a unique and multi-faceted character in the K-Pop industry.
Positive Traits: Independent, disciplined, versatile, charismatic, protective, strategic, analytical, ambitious, intelligent, loyal
Negative Traits: Perfectionist, aloof, stubborn, overly critical, reserved
╰ ౨ৎ HISTORY
1997-2011: Luna was born in Kensington, London, into a well-off family that nurtured her artistic inclinations. Her mother, a retired ballerina, introduced her to the world of dance, leading Luna to begin ballet training at the tender age of three. This early exposure fostered her love for performing arts and instilled a strong work ethic in her. Academically gifted, she attended Southbank International School Kensington, where she excelled in her studies and developed a deep passion for music. Despite her wonderful childhood, Luna often felt isolated due to her personality, seeking solace in her artistic pursuits and immersing herself in the creativity that surrounded her.
2011-2012: At the age of fourteen, Luna made the pivotal decision to move back to Seoul, South Korea, to pursue her dream of becoming an idol. This transition marked a significant change in her life, as she entered the competitive world of K-Pop. She initially trained at YG Entertainment for a year, where she faced the rigors of idol training and learned to adapt to the intense environment. Throughout this time, she was constantly approached by PLEDIS Entertainment, a smaller company that offered her a chance to further her dreams. After much consideration, Luna trusted her instincts and made the bold decision to switch companies, believing it would ultimately lead her closer to her goals. She has mentioned in an interview that her leaving a huge and well known company for a smaller one was one of the riskiest thing she has ever done and yet she does not regret it.
2013-2015: Luna trained for another two years at PLEDIS Entertainment, honing her skills as a lead vocalist in preparation for her debut. During this time, she faced various challenges, including rigorous practice schedules and the pressure to excel among her peers. However, her determination and talent shone through, allowing her to form strong bonds with the other trainees. She was supposed to either debut in a girl group or as a solo artist, however, in 2015, Luna finally achieved her dream of debuting as a member of the co-ed band SEVENTEEN, alongside thirteen talented male members. This milestone marked the beginning of her journey in the spotlight, showcasing her versatility and dedication as an artist.
2015-Present: Since her debut, Luna's life as an idol has been a rollercoaster ride filled with both challenges and triumphs. She has navigated the ups and downs of the entertainment industry, facing public scrutiny and the pressures of fame. Despite these obstacles, the joy of being with her fellow members, whom she considers family, has been a constant source of strength. Together, they have achieved remarkable success, creating unforgettable memories and sharing their passion for music with fans worldwide. Luna's perseverance and commitment to her craft continue to drive her as she embraces the journey of an idol, always striving to achieve her goals and dreams.
╰ ౨ৎ LUNA-VERSE MASTERLIST
ೃ⁀➷ comment or message me to be added to the tag list :)
˚₊· ͟͟͞͞➳❥ SUBMIT A REQUEST AND ASK ME ANYTHING!
: ̗̀➛ requests are always open ♡ - lunaఌ
Taglist: @yeoberryx @minminghao @angie-x3
#seventeen 14th member#⋆ ˚。⋆🌙˚LUNA-VERSE#seventeen#svt#svt x reader#seventeen x reader#svt imagines#svt fanfic#scoups#jeonghan#jeonghan x reader#jeonghan x you#jeonghan x y/n#jeonghan x oc#yoon jeonghan#yoon jeonghan x reader#yoon jeonghan x you#joshua hong#dk#woozi#vernon#vernon x reader#wonwoo#wonwoo x reader#mingyu#mingyu x reader#hoshi#jun#the8#svt dino
43 notes
·
View notes
Note
Thinking about you being wheeled into the hospital paramedic straddling your waist delivering harsh compressions while the other has the ambu bag pressed to your face. You have a neck brace on and aed pads still on your chest as you just coded in the back of the ambulance. once in the room a team lifts you up and places you on the hospital bed. All your clothes are immediately cut off leaving you completely nude in a room full of strangers. A strong doctor takes over compressions rocking your body. Head nodding with every thrust arms flailing to the side and bare feet rocking in sync with compressions. A nurse quickly puts the tube down your throat before grabbing the defibrillator. She rubs the jell onto the paddles before placing them onto your bare chest. “Clear” your body arches up before crashing down. You undergo a brutal code for the next 30 minutes before they get a pulse back. What do you want to happen next?
Well that's a fun little story.
After successfully restoring my pulse, I remain in a critical condition, completely unresponsive and unable to breathe independently. My pulse is weak but stable, requiring close monitoring. The medical team is urgently investigating the underlying cause of the arrest. They are utilizing ultrasound imaging and other advanced diagnostic tools to assess my injuries. The team is also considering whether immediate surgical intervention is necessary or if I should be transferred to the Intensive Care Unit (ICU) for further stabilization and observation. Either of which I'm lickley to code again.
34 notes
·
View notes
Text

Six-Sentence Sunday: Synchronize AU, Ch 8
I’m sadly still quite a long way off from finishing the next chapter, but I was finally able to write a little for it the other day, so here’s a small sample.
This scene is basically one in which Sebastian is having issues swallowing and Agni decides to step in, which leads Sebastian into admitting something.
Agni was always observant, and the instant he heard Sebastian coughing, he was at his side, a concerned expression on his face. “Are you having swallowing problems today?”
Sebastian couldn’t meet Agni’s eyes. “I’m fine. I just need some water.”
Agni frowned but nodded and left to get him some.
Sebastian stared at the cup in his hand, setting it on the over-bed table in front of him. He tried to swallow again and felt like he had to use his tongue and accessory neck muscles to execute it. He shut his eyes tight and swore in his mind. He was supposed to be better. He was stronger. He could sit up unsupported for a short amount of time and even transfer to his chair from bed on his own.
This felt like a slap in the face. He didn’t want to believe it. Maybe he was just tired?
“Here you go,” Agni said, offering him the cup with a straw. “I’m going to put my hand on your throat, but swallow normally.”
Sebastian acted indifferent, but he was scared. And pissed. He hesitantly took a sip of water; it felt like it took five or six swallows when it should have easily passed with only one. And he’d barely finished when he began to cough again, several times, enough that Agni took the cup away.
“You’re NPO until Dr. Albrecht clears you,” he said with authority, taking both cups away, meaning that Sebastian wouldn’t be allowed anything by mouth—not food, drink, or medicine. “I’ll give you your medication via your g-tube and go prepare a liquid meal for you once I’ve done that.”
“No,” Sebastian said, his fingers bunching in the blankets. He coughed again since it felt like the water was still stuck in his throat, even though he knew he had to be imagining it. “Please, Agni.”
Agni paused, cups in each hand, staring down at Sebastian, his face sympathetic, and yet stern. “Aspiration pneumonia is serious. This isn’t negotiable.” Basically, if Sebastian’s mouth and throat muscles were weak, it meant he couldn’t prevent food, liquid, and saliva from going down into his lungs. If that happened enough, it could lead to infection and even death.
Sebastian said nothing else as he watched Agni move, suddenly feeling crushed by despair. It had been foolish to hope, he’d known it.
But Agni made things different, somehow. As odd as it might seem, the one who’d come to care for all the needs he couldn’t attend to alone somehow made him feel more independent than he had in years.
And now . . .
“Sebastian? Are you all right? You’re breathing OK?”
Sebastian’s eyes flew from where they’d been fixed on the feeding tube supplies to those beautiful gray eyes. He wanted to be furious with Agni, as if he were to blame for Sebastian’s body betraying him, but he couldn’t bring himself to take his frustrations out on the nurse. Not now. Not after all they’d been through, how much Agni had helped him, even when he probably didn’t deserve it. “Do you have to do this?”
Agni tilted his head, assessing Sebastian. “I’ll do everything I can so you won’t be nauseous.”
That wasn’t what Sebastian meant, but he sighed and moved the blanket away, lifting his shirt to expose his abdomen, the little button that lay flush against his skin in the lower right just above where his pants waistband would be.
“I didn’t want this,” Sebastian said, watching Agni as he worked.
Agni paused what he was doing. “Sebastian?”
“The tube.”
Catch up with Synchronize by reading ch 1-7 on AO3!
#black butler#黒執事#sebastian michaelis#agni#synchronize au#six sentence sunday#sebagni#poi writes#modern au#chronic illness au
82 notes
·
View notes
Last Seen Blogs

noodledooodles-blog
Hogwart's School of Artcraft and Doodledry

shmko
uco


bramj4udotom
برامج فور يو

geshna
Geshna +:+