#how much does a clinical research associate make
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
Natural Breeding Clinic - Prologue
warnings: MDNI, breeding kinks, general sex, mention of infertility and insemination methods
a/n: It's here. Finally.

Teaser - Prologue - Patient 1
You take a deep breath and sit down in front of the laptop, waiting for the other person to join the call. Never in your life had you heard about such a unique reproductive center but lately, you’d been feeling the pull to start your own family. You’d discussed this with relevant people in your life. Everyone had said if you really wanted a child, then you should go with the options you thought were right for you.
You’d done the research, looking into different doctors and fertility clinics, but this one just stood out. There were testimonials from several happy families, saying their methods, though unconventional, were effective, and the doctors showcased on the website were all incredibly striking, each one handsome in their own way. But it was the success rate that caught your eye. A 98% guaranteed rate that you would be pregnant, and that pregnancy would be healthy. The site didn’t go into too much detail on their method, but the wording caught your eye.
“A natural breeding clinic” they’d called themselves. You’d finally bitten the bullet and called, requesting an information session. The screen suddenly lightens and you focus your attention as an attractive woman with shoulder-length brown hair comes into view. She smiles in a welcoming way before speaking.
“Hello. Am I speaking with Mrs. L/n?” You nod and smile back, trying not to look awkward or uncomfortable.
“Perfect! My name is Shoko Ieiri, I’m the main coordinating nurse here at Jujutsu Fertility. Thank you for scheduling an information session with us.”
“Yes, of course. I just needed more details before I booked an appointment.”
“Indeed.” Shoko claps her hands together before continuing. “Let me start by telling you a little bit about ourselves. We’ve been around for almost 6 years now. What sets us apart is that we focus more on women��s comfort than most other clinics. And we are sought out by people who are willing to use a sperm donor. We do not perform insemination services with sperm that are not from our own stock.”
“Your own stock? Are you associated with a sperm bank? And screen all the donors yourself?”
“Not a sperm bank in the conventional sense. We have 5 doctors who keep excellent health and their sperm is regularly screened to ensure quality. They are the only stock we allow for insemination.”
You blink to make sure you haven’t misheard. “The…doctors? Are you saying the fertility doctor I’d be meeting with will also be my sperm donor?”
“That is correct.” Shoko nods her head to confirm. “You will be meeting with the doctor of your choosing for at least 5 sessions. They will need to be at least once a week. Some women take the week off and come in 5 days straight.”
“5…sessions?” you ask, confused by the wording.
“Yes. It’s to ensure the insemination process has occurred an optimal number of times.”
“Wait…so…I’m going to be inseminated multiple times? How much downtime do I need in between each insemination?”
“Hardly any. Our method isn’t like a typical clinic. Most women leave feeling very normal and a lot more satisfied than when they came in.”
“Not like a typical clinic? So…you don’t use the catheter method?”
“We use minimal medical equipment in our inseminations.”
“Minimal…so what does the procedure entail?”
Shoko clears her throat and continues. “So it begins with you choosing one of our doctors. We highly recommend spending some time on this part. It’s essential that you feel attraction towards your doctor. Once you make a choice, they will reach out to discuss how your insemination experience can be optimized for you. You will receive a biodata on their sexual profile, their preferred methods of arousal, and other relevant details.”
“I’m sorry, but what?” You are at the edge of your seat wondering if you’ve entered an alternate dimension. Surely, this was all being made up? “Arousal, sexual profile- why would I need all these details? I thought sperm donors only gave information like height, weight, medical history and stuff like that.”
“Why wouldn’t they? You’re choosing to be bred by them. They would have to make sure their patient is satisfied with the experience.”
“Bred?” You bleat the word stupidly.
“Yes. We are a natural breeding clinic. We use the method nature has provided to us to ensure a pregnancy.”
The gears in your brain start turning and something finally clicks.
“Are-are you saying…I would be having sex with my doctor?”
“That is correct.” Shoko smiles gently at you, pleased that you have finally caught on.
“The human body doesn’t necessarily enjoy having medical equipment inserted into it. All that cold plastic, and the mechanical methods of insertion. It puts the body in a state of stress. Not good for implantation. So our doctors will inseminate you through the process of intercourse.”
Her words fall like a fog around you. You can feel your heart racing, a flush creeping into your cheeks. It was…insane. The doctor of your choosing was essentially going to fuck a baby into you. As your mind starts pulling up the images of their doctors, each one impossibly handsome and striking, you feel a familiar throb starting between your legs. Wetting your lips, you try to talk to continue with the information session.
“I see. And…there are benefits to this?”
“Yes. Intercourse allows the body to relax, releasing happy hormones. In this stress-free state, in addition to the knowledge that your doctor is someone you’re attracted to and trust, the chance of an implantation doubles.”
You gape at Shoko, your mind reeling from all the information.
“And…when you say the insemination process will be optimized for my best experience…?”
“The doctor you choose will ask you extensive questions about your preferences. What turns you on, positions, dislikes, toys. It’s to determine if they will satisfy your breeding experience. If they feel they might not be a good fit, they’ll recommend another one of our doctors.”
You swallow, your mouth going dry. “I see. And…what else do I need to know?”
“We will start by collecting your medical history and run some blood work to make sure your body is ready for an insemination process. Women who have a domestic partner will need to get both a waiver and a consent form signed by their partner that they have been informed what happens for the insemination.”
“Of course. Makes sense.”
“You will be assigned an emotional support companion during this process. It will either be myself or Mr. Ijichi Kiyotaka. We are there to help ease your nerves and ensure you enjoy the process. And all patients must think of a unique safeword to use during the insemination process.”
“Safeword?” you parrot back, still processing.
“Yes. At any point during the process, should you feel uncomfortable, your safeword ensures all actions cease and your doctor will give you some space to breathe and reassess the situation.”
All you can do is nod along. Shoko gives you a look of reassurance. “I can guarantee that most women are pleased with the results. And our doctors are quite skilled in what they do. It’s natural to feel a little shy and embarrassed but at the end of the day, we all share a common goal- a healthy baby.”
Despite your initial shock, you feel some of your trepidation fade away. Shoko continues.
“If you are ok with all of this, I can send you the forms to get the process started. Once those are filled, you can take some time to decide on your doctor. Then we’ll set up a call with them.”
“Thank you.” You make a split-second decision. “Please go ahead and send the forms.”
“Excellent. I’ll send them to the email you put in your inquiry. Was there anything else?”
You shake your head no. “I think I have all I need.”
“Great! I look forward to assisting you again.” Shoko ends the call and you immediately go the the website again to look at the doctors, one of which will end up fathering your child. Such a hard decision. How will you ever make the choice?

@thesunxwentblack @kentocalls @actuallysaiyan
@belle-oftheball34 @jesssicapaniagua
@figmentforms

© nanamiscocksleeve original work | no copying, plagiarizing or translating
#jjk smut#nanami kento#gojo satoru smut#suguru geto smut#hiromi higuruma smut#choso kamo smut#shoko ieiri#ijichi kiyotaka#natural breeding clinic#nanami kento smut#gojo satoru#geto suguru smut#geto suguru#choso kamo#higuruma hiromi#jujutsu kaisen#jjk x reader#jujutsu kaisen smut#nanami kento x reader#nanami kento x reader smut#gojo satoru x reader#gojo satoru x reader smut#geto suguru x reader#geto suguru x reader smut#higuruma hiromi x reader#higuruma hiromi x reader smut#choso kamo x reader#choso kamo x reader smut#ncs#ncs scribbles
1K notes
·
View notes
Text
Dealing With More Anti-Endos Invading Endogenic Spaces! This Time With a Dash of r/Systemscringe
This is just a straight-up lie.
While @thelunastusco did identify as endogenic at one point, that was a VERY long time ago.
I won't go into too much detail about this. You can see their response here:

Wait... are endogenic systems faking or not? 🤔
You seem like you're having a really hard time deciding.
If endogenic systems don't say they have a disorder, they literally can't be faking it.
If endogenic systems do think they have a disorder, then how would they be groomed into thinking they don't?
In the future, try your best to make a rationally coherent point.
Because you've clearly failed here.
Also, not what grooming is. Anti-endos, stop comparing endogenic systems to abusers.
Now, normally, I would go into the whole spiel of how actually endogenic systems are recognized by the majority of psychiatrists who have researched the subjects, by the World Health Organization, etc. But @cambriancrew already tried that, pointing to studies that have been done, and this was how @problematicpooch responded:

So essentially, don't trust the many, many professionals telling you endogenic plurality is real because some studies are wrong! 🙄
And WHAT RESEARCH HAVE YOU DONE?
Have you managed to find even one paper by a psychiatrist or psychologist anywhere stating it's impossible to be plural without trauma? Anywhere?
Because I think it's safe to say that our research is more valid than yours. Ours comes from respected doctors in the field. Yours comes from r/systemscringe. (Don't worry. I'm getting there.)
By the way, the Crew didn't say all studies need to be true if they're published. They said a book specifically peer reviewed and published by the American Psychiatric Association wouldn't have been published if the reviewers felt it contained untrue information.

Why are anti-endos always wanting to traumatize a bunch of children?
Why not just try testing alternative hypotheses for the formation of plurality?

Does anyone else get the feeling that anti-endos attack research into endogenic systems because they're scared?
"Research into endogenic systems is taking away from research into DID" is a pretty silly argument. A lot of research into DID and OSDD has been conducted by trauma specialists. Very little of the research into endogenic systems have been. Doctors who have traditionally focused on traumagenic plurality still are focused on that.
There's zero merit to the idea that this is taking away from research into DID in any way.
And again, the ICD-11, written by World Health Organization, is clear that you can experience multiple distinct identity states without a disorder.
The Hearing Voices Network has been fighting for the 80s to normalize that voice hearing isn't inherently pathological.
Just because someone has experiences similar to a mental illness doesn't mean they have a mental illness. Especially if the don't meet criteria for distress or impairment.

Okay... you know what... I AM going to whip out the ICD-11 here because I want to zero in on another part of this. In the criteria, for DID, you need to experience impairment in areas of functioning due to the disorder.

The DSM-5 has a similar criterion, worded as a requirement of "clinically significant distress or impairment" in important areas of functioning.
The ICD-11 contrasts this with non-aversive distinct personality states that aren't associated with impairment.

No, it's not ableist to say that DID is harmfull.
And the criterion I mentioned in the DSM is literally called the harm criterion, and establishes that a disorder can't be a disorder if it doesn't harm the person in some way.
Referring to dissociative disorders as being harmful isn't ableism. If they weren't harmful, they wouldn't be disorders. That's how disorders work!
Having other people in your head isn't inherently a disorder if it doesn't come with distress or impairment.
This doesn't mean that people with dissociative disorders are monsters. It just means they have a disorder that causes some for of distress or impairment.
Though maybe you, specifically, are.
r/systemscringe
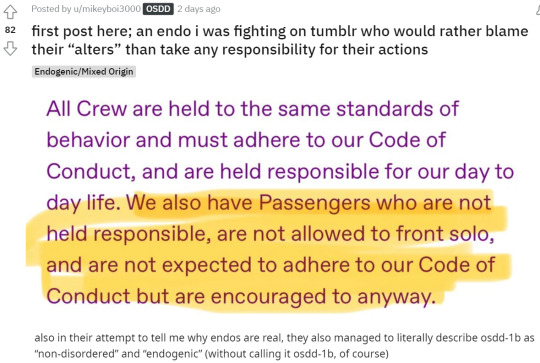
After being torn apart, Problematicpooch ran to r/systemscringe where xe goes by u/Mikeyboi3000
Now, xe tried pulling this in the discussion with Cambrian too, who addressed it here:
Obviously, no correction from u/mikeyboi3000.
That would require a shred of intellectual honesty xe doesn't possess.
Anyway, while we're here, let's take a deeper look at the comments.

Casually accusing someone you don't of being an abuser while you have THAT as your flair is absolutely wild!
Also, they described symptoms the OP says are OSDD-1. At no point did the Crew actually claim OSDD isn't a disorder.

I think most people should have a general code of conduct for themselves. At least basic moral principles.
I would think it's weird that this person doesn't, but then I remembered that this is on r/systemscringe. Of course they wouldn't have any moral principles.

I don't think I've ever seen the Crew use that word for themselves. u/Mikeyboi3000 just stuck that in quotations for some reason.
By the way, if anyone's forgotten who u/sleep-bread-dough is, I debunked their r/systemscringe posts last week.
This is the user who makes system-friendly-sonas to pretend to be supportive of their system friends, and doesn't think DID systems should be allowed to work.

The problem isn't about consciousnesses.
While it may not be fair, if you're unable to hold a single member of the system accountable, then society's laws quickly break down.
Imagine if ghosts were real and could permanently possess someone. Ghosts start possessing people, and permanently are locked into those bodies. The ghosts then commit crimes. If you say, "well, we can't hold this person accountable because they're possessed," then they can commit more crimes without penalty.
If punishing a group is the only way to hold an individual accountable, then the whole group needs to be held accountable.
For example, if anti-endos routinely invade endogenic tags, crosstagging into our spaces, and they refuse to change and stay in their own corners when they're asked, then I have no choice but to crosstag my responses into their tags with the hope the rest of the anti-endo community can rein them in, punishing the entire group for the actions of an individual.
Maybe it doesn't seem fair, but sometimes things that seem unfair are necessary for maintaining order.
I think system responsibility is one of those things, where even if a system were made up of completely 100% separate people, all would need to be held accountable for the actions of one or nobody would be held accountable.
This wasn't the only post u/Mikeyboi300 made either after Tumblr arguments in the past few days. Xe also did one after being corrected by LunastusCo on their origins.
To anyone who may engage with this user, please be warned that doing so may result in them posting you to r/systemscringe in retaliation.
If you're worried about being posted on r/systemscringe, the best thing you can do is to block @problematicpooch.
#syscourse#pro endo#pro endogenic#anti endo#anti endogenic#sysblr#psychology#psychiatry#multiplicity#systemscringe#r/systemscringe#reddit#system stuff#systems#system discourse#actually plural#actually a system
63 notes
·
View notes
Text
I did a bit of research and scraped together memories from a few semesters of psychology, hoping I haven’t fundamentally gotten anything wrong. I attempted a small (clinical) psychological analysis of Sharp in which, of course, some things had to be shortened, trying to determine how the events in Scarborough might have affected him.
TW: Mention of PTSD, trauma, personality disorders
Does Sharp suffer from PTSD?
What is PTSD?
• Trigger: uncontrollable, unpredictable event
• Stress reaction where people suffer from the persistent re-experiencing of the traumatic event (flashbacks, nightmares)
-> Guilt for surviving
-> In addition to chronic stressors, everyday stressors also influence the course of the illness and mental state (noise, stressful events (I’m looking at you, Garreth), job stress)
• There are several stages to diagnose PTSD:
1. Trauma
In psychiatric classification systems, trauma (in relation to PTSD) is defined as follows: (only) exceptional, (potentially) life-threatening events or events associated with severe injuries; applies to Scarborough, but:
-> not every trauma leads to PTSD; while an estimated 60% have had a traumatic experience, only about 8% of the male population develop PTSD (for women, it's 20%); the likelihood increases if the trauma was inflicted intentionally, which applies to Scarborough.
2. Flashbacks, nightmares (explanations follow below)
3. Avoidance behavior
-> Avoidance of stimuli related to the trauma:
So, we have this: Sharp claims that fear played no role in his decision to leave the Ministry:
-> there is a study (Lanius et al. 2003) that compared traumatized individuals with and without PTSD: those with PTSD showed lower brain activity when experiencing emotional memories (people with PTSD thus suffer from a disorder in emotion processing)
-> What does this mean? Either the emotion is present, but Sharp's brain can not process it, or maybe he simply doesn’t want to discuss his emotions with a student
-> Repression might also play a role in this statement, as well as the fear of making himself vulnerable (if someone uses my fears against me, I have to relive them)
4. Overstimulation
-> constant state of alertness
-> sleep disturbances, irritability
5. Duration > 1 month
6. Psychosocial impairments
Problem: We don’t see much: Does he have nightmares, flashbacks, concentration issues? Does he relive the trauma? Does the experience restrict him?
Between the lines, it can be seen that he feels guilt, but there is hardly any indication of the extent of it (if he didn’t feel guilt, to be honest, that would worry me too).
Counterarguments / Ambivalences:
• He speaks relatively openly about what he experienced
• He admits his mistake: this could be a sign that he has come to terms with it or that he blames himself for it
• He actively seeks a cure and even takes a new job for it, which argues against avoidance behaviour.
7. Differential diagnosis
-> Reactions to trauma can cause disorders of varying severity
-> Trauma can also bring other psychological disorders, including adjustment disorders, or:
• a persistent personality change after extreme stress:
Aesop mentions that success can make one complacent. From this, it can be concluded that the trauma has profoundly changed his personality:
• in the above-mentioned disorder, the personality change includes:
-> among other things, a hostile and distrustful attitude (thinking of the first encounter with MC, see this post),
-> social withdrawal (new job)
-> as well as constant internal tension and restlessness out of fear of being threatened (his extreme perceptiveness could be a sign of this; when MC talks to Garreth, Sharp knows exactly what they discussed afterward)
-> all this therefore applies to Sharp
However, this disorder tends to occur with persistent stress that can begin in childhood, which either indicates that Scarborough, though a one-time event, still burdens him, or that his personality changes cannot be classified as a disorder.
Conclusion: Sharp probably does not have PTSD, but Scarborough caused severe trauma. We can assume that the event has profoundly shaped his personality. Whether it can be called a personality disorder, I can not judge. However, I do wonder what the "old" Sharp was like. But that’s a question for another post.
#hogwarts legacy#professor sharp#aesop sharp#professor aesop sharp#hogwarts legacy headcanons#hogwarts legacy theory
21 notes
·
View notes
Note
Hey!! Do y'all know where we can find any resources/symptom lists/etc specific to osdd-1b?? We've been questioning whether or not that might be a thing we have going on, but when we try to look into it, most of what we're finding groups DID and OSDD together and emphasizes memory gaps, which we dont really have.
Hey, we’re not a clinician or expert, but from what we know about DID and OSDD:
- there’s really not a huge amount of difference between these two disorders. The differences may be minor or arbitrary, and honestly the difference in diagnosis may vary vastly from clinician to clinician.
- that being said, there’s likely even less of a difference between OSDD-1a and OSDD-1b. We’re not a clinician and we have trouble sometimes understanding clinical language, so researching the differences between these subcategories (without turning to community-created content) has been difficult for us. Vaguely, we understand OSDD-1a to mean a dissociative disorder with amnesia but no parts/alters, and OSDD-1b to mean a dissociative disorder with parts/alters but no amnesia.
These things being said, we’ll include the information we could find. Please don’t disregard resources that have information on OSDD along with DID! Like we said, these disorders are closely linked, so it makes sense that they’re often grouped together.
Trying to find accurate, reliable info on OSDD-1b if anything reminded us how horribly under researched dissociative disorders are. We couldn’t find much that isn’t unsourced in a wiki or written on a personal blog.
^ this is an ask we answered in the past. A lovely system reblogged it with their thoughts and info regarding OSDD 1a and 1b
youtube
^ we really love the CTAD clinic! This video may be useful, though the clinician speaking here does advise against self-diagnosis and proposes renaming OSDD as “minor DID” which we don’t entirely agree with.
Please use critical thinking and your best judgement when exploring these links. You know yourself better than anyone else!
We’re sorry we couldn’t find more up-to-date, reliable, and accurate information for you. This might be something best brought up in therapy or with a qualified professional. Still, we hope something in this list of resources might help you.
💫 Parker and 🐢 Kip
27 notes
·
View notes
Text
More thoughts on Baizhu's story quest #2 - Baizhu's lack of self
↓ ↓ Spoilers below ↓ ↓
The dynamic between Baizhu and Changsheng is interesting in the sense of how Baizhu has both negated and asserted himself in the relationship. When we think of 'selfless' behaviour, it has come to mean putting other people first. But a more literal meaning is being without self. Baizhu's behaviour is quite paradoxical in that the two states exist at once.
In choosing to undertake the art of healing (before he ever made his contract) he had taken an oath under his master to practice his art for the benefit of all, regardless of wealth or status. In essence, this ethical duty requires the medic to put personal feelings aside and administer their art in a fair way without prejudice or reasonable refusal. This is the first denial of self and is common to other professions such as lawyers. You also cannot allow emotions to cloud your clinical judgment and sometimes must make difficult decisions in the best interests of the patient, no matter how they offend you morally or emotionally.
The demands and rigours of such a job are such that you never have a day off. Yes, a clinic may have opening hours, but an emergency can present itself at any time or place. The doctor's duty requires that they must assist. It becomes a way of life and long working hours end up dictating how you spend your leisure time or who you meet. It permanently alters how you think; your brain is constantly viewing the world through the lens of your profession. For example, a simple walk in the mountain will turn into 'Oh, I wonder if that flower might have a medicinal benefit?' when most people will simply stop to look at the pretty flower. In this way, Baizhu further loses his definition of self.
It is also common to vocational professions to lose one's sense of self in that your identity becomes wrapped up in your job. People forever associate the name Baizhu with him being a doctor. Not Baizhu the human being. If one were to remove his medical inclination, what would be left of him? His voicelines are all based in some way around his profession - even his hobby is research. He doesn't even commit to a favourite food in favour of dispensing some health advice about having a balanced diet. Who actually is Baizhu as a person? What are his own preferences and desires? Is there anything of him apart from his dedication to his art? Once again, he has suppressed his sense of self. Or conceals it from the people around him in a guarded way. He deliberately makes himself two-dimensional in his presentation, but it plays as being mysterious and enigmatic. He uses a mischievous sense of humour to dodge and deflect questions he doesn't want to answer. For whatever reason, he does not want others to penetrate the external layer.
In this way, and on account of his pure heart and altruistic nature, taking the contract became a self-fulfilling prophecy, as much as he wants to deny the existence of fate. Changsheng refers to him as her mannequin. But it's probably more accurate to say that Baizhu has made himself a vessel or conduit for her power for the purpose of healing. A further denial of self.
He wears a smile so as not to cause worry to the people around him and encourage his patients despite the huge suffering he experiences daily. He has invalidated his own pain for the convenience of others (something which many sick or disabled people do). Again, denial of self.
But on the other hand, according to Jiangli, Baizhu's senior apprentice, he most likely would have been able to formulate a remedy for Jialiang on his own steam had he not reverse-engineered and adapted her version. She says that his intellect is exceptional in its own right.
In other words, Baizhu is more than a vessel; he has his own knowledge and skillset and likely would have been an exceptional physician even without the contract. Changsheng's arts merely serve to amplify it or make the process of his research more meaningful and elevate his talents to miraculous. His inquisitiveness and analytical nature were always his alone. He uses her abilities as research tools to develop cures and better understand how diseases and toxins work, thus expediting the research and development process.
In spite of his ostensible modesty (he refers to himself as 'delusional' and 'troublesome' and uses humble language) Baizhu seems to be aware of his ability and I wonder if this is the reason why he is so confident - arrogant? stubborn? - that he will defy the demise suffered by his predecessors to Changsheng's contract. In this way, he asserts self. And he does so either oblivious to the love that other people hold for him, or in spite of it.
Either, through denial of self, he cannot imagine himself worthy of love. I think this is unlikely - he is aware of his brilliance and his aesthetics suggest he is equally aware he is attractive. I suspect that he simply weighs up the grief of his loved ones against the benefits that could be brought to countless more unnamed people in the future through his ability to heal them. In this way he asserts self in the strongest and most painful way possible; he will not be deterred from walking his path as a healer. The only suffering he wilfully refuses to alleviate through his single-minded actions is that of those who cherish him most.
But then, he is confident that such a possibility will never arise because he is convinced of his future success. Maybe he is even inspired by it and becomes all the more determined to succeed in his endeavours, precisely to protect them. This sort of hubris is never destined to end well.
I would hope he uses their pain to temper any temptation to be reckless, but I fear the lure of testing his limits would always win. I think he will either end up dead, or cursed to immortal agony, because he cannot find cures for all of the ailments he's accumulated and some will do permanent damage even if they are cured later. After all, Changsheng's power is eroding and she cannot balance his Qi forever.
I wonder if, with either outcome, he would regret his decision or not.
31 notes
·
View notes
Text
Does “food as medicine” make a big dent in diabetes?
New Post has been published on https://thedigitalinsider.com/does-food-as-medicine-make-a-big-dent-in-diabetes/
Does “food as medicine” make a big dent in diabetes?

How much can healthy eating improve a case of diabetes? A new health care program attempting to treat diabetes by means of improved nutrition shows a very modest impact, according to the first fully randomized clinical trial on the subject.
The study, co-authored by MIT health care economist Joseph Doyle of the MIT Sloan School of Management, tracks participants in an innovative program that provides healthy meals in order to address diabetes and food insecurity at the same time. The experiment focused on Type 2 diabetes, the most common form.
The program involved people with high blood sugar levels, in this case an HbA1c hemoglobin level of 8.0 or more. Participants in the clinical trial who were given food to make 10 nutritious meals per week saw their hemoglobin A1c levels fall by 1.5 percentage points over six months. However, trial participants who were not given any food had their HbA1c levels fall by 1.3 percentage points over the same time. This suggests the program’s relative effects were limited and that providers need to keep refining such interventions.
“We found that when people gained access to [got food from] the program, their blood sugar did fall, but the control group had an almost identical drop,” says Doyle, the Erwin H. Schell Professor of Management at MIT Sloan.
Given that these kinds of efforts have barely been studied through clinical trials, Doyle adds, he does not want one study to be the last word, and hopes it spurs more research to find methods that will have a large impact. Additionally, programs like this also help people who lack access to healthy food in the first place by dealing with their food insecurity.
“We do know that food insecurity is problematic for people, so addressing that by itself has its own benefits, but we still need to figure out how best to improve health at the same time if it is going to be addressed through the health care system,” Doyle adds.
The paper, “The Effect of an Intensive Food-as-Medicine Program on Health and Health Care Use: A Randomized Clinical Trial,” is published today in JAMA Internal Medicine.
The authors are Doyle; Marcella Alsan, a professor of public policy at Harvard Kennedy School; Nicholas Skelley, a predoctoral research associate at MIT Sloan Health Systems Initiative; Yutong Lu, a predoctoral technical associate at MIT Sloan Health Systems Initiative; and John Cawley, a professor in the Department of Economics and the Department of Policy Analysis and Management at Cornell University and co-director of Cornell’s Institute on Health Economics, Health Behaviors and Disparities.
To conduct the study, the researchers partnered with a large health care provider in the Mid-Atlantic region of the U.S., which has developed food-as-medicine programs. Such programs have become increasingly popular in health care, and could apply to treating diabetes, which involves elevated blood sugar levels and can create serious or even fatal complications. Diabetes affects about 10 percent of the adult population.
The study consisted of a randomized clinical trial of 465 adults with Type 2 diabetes, centered in two locations within the network of the health care provider. One location was part of an urban area, and the other was rural. The study took place from 2019 through 2022, with a year of follow-up testing beyond that. People in the study’s treatment group were given food for 10 healthy meals per week for their families over a six-month period, and had opportunities to consult with a nutritionist and nurses as well. Participants from both the treatment and control groups underwent periodic blood testing.
Adherence to the program was very high. Ultimately, however, the reduction in blood sugar levels experienced by people in the treatment group was only marginally bigger than that of people in the control group.
Those results leave Doyle and his co-authors seeking to explain why the food intervention didn’t have a bigger relative impact. In the first place, he notes, there could be some basic reversion to the mean in play — some people in the control group with high blood sugar levels were likely to improve that even without being enrolled in the program.
“If you examine people on a bad health trajectory, many will naturally improve as they take steps to move away from this danger zone, such as moderate changes in diet and exercise,” Doyle says.
Moreover, because the healthy eating program was developed by a health care provider staying engaged with all the participants, people in the control group may have still benefitted from medical engagement and thus fared better than a control group without such health care access.
It is also possible the Covid-19 pandemic, unfolding during the experiment’s time frame, affected the outcomes in some way, although results were similar when they examined outcomes prior to the pandemic. Or it could be that the intervention’s effects might appear over a still-longer time frame.
And while the program provided food, it left it to participants to prepare meals, which might be a hurdle for program compliance. Potentially, premade meals might have a bigger impact.
“Experimenting with providing those premade meals seems like a natural next step,” says Doyle, who emphasizes that he would like to see more research about food-as-medicine programs aiming at diabetes, especially if such programs evolve and try to some different formats and features.
“When you find a particular intervention doesn’t improve blood sugar, we don’t just say, we shouldn’t try at all,” Doyle says. “Our study definitely raises questions, and gives us some new answers we haven’t seen before.”
Support for the study came from the Robert Wood Johnson Foundation; the Abdul Latif Jameel Poverty Action Lab (J-PAL); and the MIT Sloan Health Systems Initiative. Outside the submitted work, Cawley has reported receiving personal fees from Novo Nordisk, Inc, a pharmaceutical company that manufactures diabetes medication and other treatments.
#2022#Abdul Latif Jameel Poverty Action Lab (J-PAL)#Analysis#blood#blood sugar#compliance#covid#diabetes#diet#Disease#Economics#effects#Exercise#Experienced#Faculty#Features#Food#form#Foundation#Health#Health care#how#it#management#Medicine#mit#MIT Sloan School of Management#natural#network#notes
2 notes
·
View notes
Text
Known COVID-19 Health Complications
Last Updated September 8, 2023
Repeat Infections
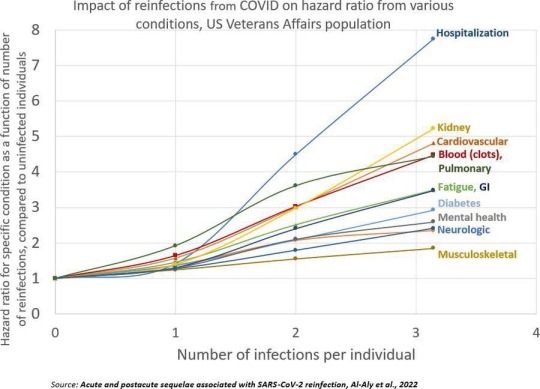
Summary: Repeat infections, even if mild during the acute phase, cause cumulative damage to the body and increase your risk of developing health complications or Long COVID. You should aim to limit the number of times you are infected as much as possible, even if you are not currently high risk (Note: Health complications post-COVID-19 infection can make you high risk) and have been vaccinated.
Published Research
Acute and postacute sequelae associated with SARS-CoV-2 reinfection | Nature Medicine Bowe, B., Xie, Y, & Al-Aly, Z. (2022).
Articles & Reports
Repeat COVID-19 infections increase risk of organ failure, death – Washington University School of Medicine in St. Louis (wustl.edu) Sauerwein, K. (2022).
Why Getting COVID-19 Multiple Times Is Risky For Your Health | Time Park, A. (2022).
Heart & Cardiovascular Damage
Summary: COVID-19 increases your risk of heart failure, heart attacks, strokes, pulmonary embolism, palpitations, arrhythmia, myocarditis, blood clots (thrombosis), etc. post-infection. Inflammation during the acute phase of a COVID-19 infection can damage the heart and blood vessels.
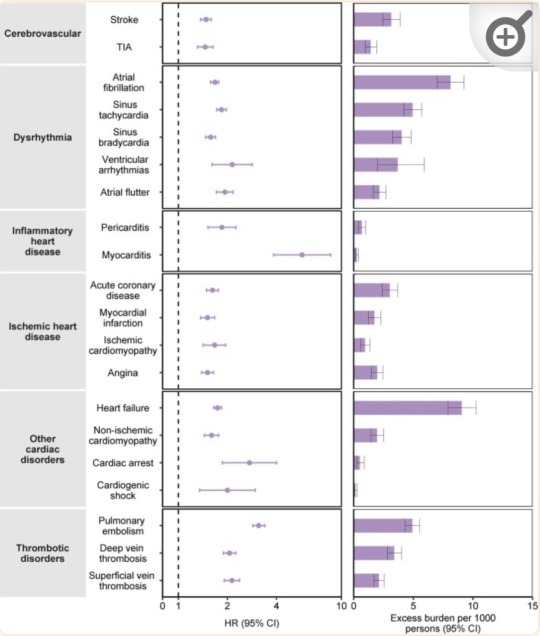
“Risks and 12-month burdens of incident post-acute COVID-19 cardiovascular outcomes in participants without any history of cardiovascular outcomes prior to COVID-19 exposure compared to the contemporary control cohort.” (Xie et al., 2022)
Published Research
Core mitochondrial genes are down-regulated during SARS-CoV-2 infection of rodent and human hosts | Science Translational Medicine Guarnieri, J. W., Dybas, J. M., ... Wallace, D. C. (2023).
Long-term cardiovascular outcomes of COVID-19 - PMC (nih.gov) Xie, Y., Xu, E., Bowe, B., & Al-Aly, Z. (2022).
Articles & Reports
Blood Clotting Proteins Might Help Predict Long COVID Brain Fog - Scientific American Reardon, S. (2023, September 1).
SARS-CoV-2 can damage mitochondrion in heart, other organs, study finds | CIDRAP (umn.edu) Van Beusekom, M. (2023, August 9).
Your vascular system and COVID | Heart and Stroke Foundation Heart and Stroke Foundation. (2023).
COVID, heart disease and stroke | Heart and Stroke Foundation Heart and Stroke Foundation. (2023, April 17).
How does coronavirus affect your heart? - BHF British Heart Foundation. (2023, March 21).
COVID-19 and Heart Damage: What You Should Know (clevelandclinic.org) Cleveland Clinic. (2022, May 10).
Heart Problems after COVID-19 | Johns Hopkins Medicine Post, W. S., & Gilotra, N. A. (2022).
COVID and the Heart: It Spares No One | Johns Hopkins | Bloomberg School of Public Health (jhu.edu) Desmon, S., & Al-Aly, Z. (2022, March 14).
COVID-19 takes serious toll on heart health—a full year after recovery | Science | AAAS Wadman, M. (2022, February 9).
Brain & Neurological Damage
Summary: COVID-19 infection increases your risk of developing cognitive impairments, mental health issues, poor memory, early onset dementia, and permanent loss of smell due to brain damage and the atrophy of brain matter. "Brain fog" and problems concentrating are common complaints post-infection that have also been linked to brain damage. Damage to blood vessels due to inflammation during the infection may be responsible for this by restricting oxygen flow to the brain. COVID-19 may also directly infect the brain.
Published Research
Biology | Free Full-Text | Vascular Dysfunctions Contribute to the Long-Term Cognitive Deficits Following COVID-19 (mdpi.com) Shabani, Z., Liu, J., & Su, H. (2023).
Frontiers | COVCOG 2: Cognitive and Memory Deficits in Long COVID: A Second Publication From the COVID and Cognition Study (frontiersin.org) Guo, P., Ballesteros, B. A., Yeung, S. P., Liu, R., Saha, A., Curtis, L., Kaser, M., Haggard, M. P., & Cheke, L. G. (2022).
COVID-19 and cognitive impairment: neuroinvasive and blood‒brain barrier dysfunction - PMC (nih.gov) Chen, Y., Yang, W., Chen, F., & Cui, L. (2022).
Comparison of post-COVID depression and major depressive disorder | medRxiv Perlis, R. H., Santillana, M., Ognyanova, K., Green, J., Druckman, J., Lazer, D., & Baum, M. A. (2021).
Articles & Reports
Long COVID May Impair Memory, Cognition for Months (healthline.com) Rossiaky, D. (2022).
COVID Variants Can Affect the Brain in Different Ways - Neuroscience News (2023).
The hidden long-term cognitive effects of COVID-19 - Harvard Health Budson, A. E. (2021). Harvard Medical School.
Long Covid: Even mild Covid is linked to damage to the brain months after infection (nbcnews.com) Ryan, B. (2022). NBC News.
COVID-19 Can Affect the Brain Even Long After an Infection | Time Ducharme, J. (2023). Time.
Lung Damage
Summary: COVID-19 infections can cause lung damage or scarring, and can trigger pneumonia, bronchitis, ARDS, and sepsis. Additionally, some people experience shortness of breath (dyspnea) and difficulty exercising as a post-acute sequela after infection, or multiple infections.
Published Research
At a crossroads: COVID-19 recovery and the risk of pulmonary vascular disease - PMC (nih.gov) Cascino, T. M., Desai, A. A., & Kanthi, Y. (2021).
[Pulmonary manifestations in long COVID] - PubMed (nih.gov) Sommer, N., & Schmeck, B. (2022).
Residual Lung Abnormalities after COVID-19 Hospitalization: Interim Analysis of the UKILD Post-COVID-19 Study - PubMed (nih.gov) Stewart, I., Jacob, J., George, P. M., Molyneaux, P. L., Porter, J. C., Allen, R. J., Aslani, S., Baillie, J. K., Barratt, S. L., Beirne, P., Bianchi, S. M., Blaikley, J. F., ...Jenkins, G. R. (2023).
Articles & Reports
Even mild cases of COVID-19 may cause long-term lung damage - UPI.com HealthDay News. (2022). United Press International.
COVID-19 Lung Damage | Johns Hopkins Medicine Galiatsatos, P. (2022).
Immune System & Autoimmune Diseases
Summary: COVID-19 infection can impair the functioning of your immune system. This means that those who have previously been infected are potentially immunocompromised (higher risk). For some people, the way COVID-19 impairs their immune system results in the onset of autoimmune diseases.
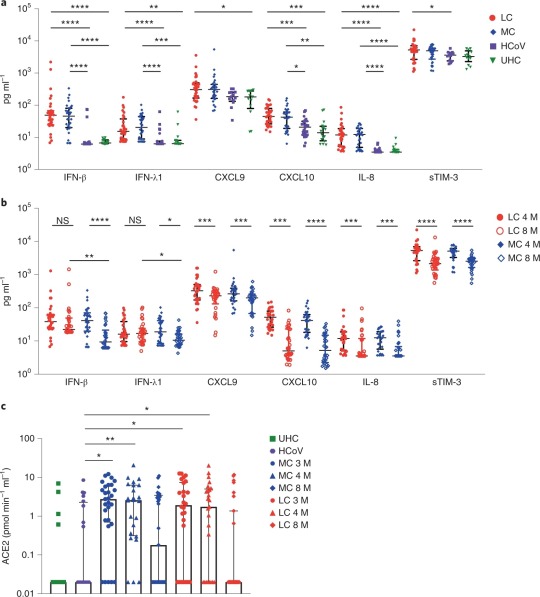
“Elevated levels of proinflammatory cytokines that persist more than 8 months following convalescence.” (Phetsouphanh et al., 2022)
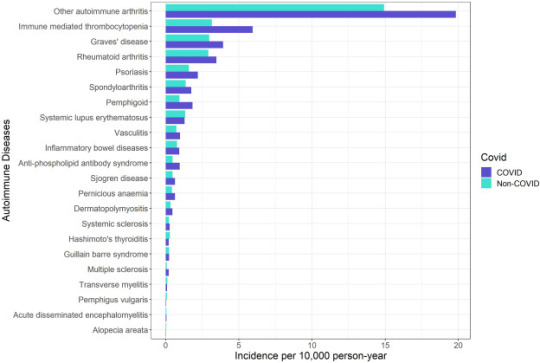
“Crude incidence of each autoimmune disease by COVID-19 and non-COVID groups.” (Peng et al., 2023)
Published Research
Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection | Nature Immunology Phetsouphanh, C., Darley, D. R., Wilson, D. B., Howe, A., Munier, M. L., Patel, S. K., Juno, J. A., Burrell, L. M., Kent, S. J., Dore, G. J., ... & Matthews, G. V. (2022).
Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection | BMC Medicine | Full Text (biomedcentral.com) Ryan, F. J., Hope, C. M., Masavuli, M. G., Lynn, M. A., Mekonnen, Z. A., Yeow, A. E. L., Garcia-Valtanen, P., Al-Delfi, Z., Gummow, J., Furguson, C., ... Lynn, D. J. (2022).
Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study - eClinicalMedicine (thelancet.com) Peng, K., Li, X., Yang, D., Chan, S. C. W., Zhou, J., & Wan, E. Y. F. (2023).
Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection | BMC Medicine | Full Text (biomedcentral.com) Winheim, E., Rinke, L., Lutz, K., Reischer, A., Leutbecher, A., Wolfram, L., Rausch, L., Kranich, J., Wratil, P. R., Huber, J. E., Baumjohann, D., ... Krug, A. B. (2021).
Articles & Reports
How COVID-19 Changes the Immune System | Time Park, A. (2023, August 18).
How COVID-19 alters the immune system -- ScienceDaily ScienceDaily. (2021, October 28).
Impacts of COVID on the immune system (medicalxpress.com) Herrero, L. (2022, September 19).
COVID-19's impact on the immune system, and how this may affect subsequent infections - ABC News Smith, B. (2022, December 1).
COVID-19 can derange immune system; survivors have autoimmune diseases (usatoday.com) Szabo, L. (2021, March 2).
Long COVID & PASC
Summary: Long COVID is an umbrella term that refers to the onset of disabling symptoms/conditions resulting from any of the previously mentioned organ, immune system, and vascular damage sustained during infection. These conditions are also referred to as "post-acute sequelae of COVID-19" (PASC). Vaccination can reduce the damage experienced by decreasing inflammation during an infection, but Long COVID/PASC can affect anyone. This is especially true in the case of multiple infections. Your risk of developing Long COVID, or worse/new symptoms, increases with each additional infection.
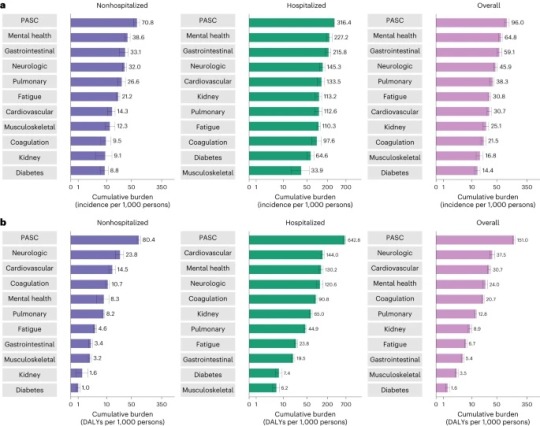
“Cumulative incidence and DALYs of postacute sequelae overall and by organ system at 2 years after infection.” (Bowe et al., 2023)
Published Research
T cell apoptosis characterizes severe Covid-19 disease - PubMed (nih.gov) André, S., Picard, M., Cezar, R., Roux-Dalvai, F., Alleaume-Butaux, A., Soundaramourty, C., Cruz, A. S., Mendes-Frias, A., Gotti, C., … Estaquier, J. (2022).
SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC) | Nature Immunology Proal, A. D., VanElzakker, M. B., Aleman, S., Bach, K., Boribong, B. P., Buggert, M., Cherry, S., Chertow, D. S., Davies, H. E., Dupont, C. L., ... Wherry, E. J. (2023).
The immunology of long COVID | Nature Reviews Immunology Altmann, D. M., Whettlock, E. M., Liu, S., Arachchillage, D. J., & Boyton, R. J. (2023).
Long COVID: major findings, mechanisms and recommendations | Nature Reviews Microbiology Davis, H. E., McCorkell, L., Vogel, J. M., & Topol, E. J. (2023).
Long COVID prevalence and impact on quality of life 2 years after acute COVID-19 | Scientific Reports (nature.com) Kim, Y., Bae, S., Chang, H., & Kim, S. (2023).
Postacute sequelae of COVID-19 at 2 years | Nature Medicine Bowe, B., Xie, Y., & Al-Aly, Z. (2023).
Articles & Reports
Long COVID | NIH COVID-19 Research National Institutes of Health. (2023, June 8).
Long COVID or Post-COVID Conditions | CDC Centers for Disease Control and Prevention. (2023, July 20).
The Most Important Question About Long COVID | Harvard Medical School Pesheva, K. (2023, August 9).
Nearly One in Five American Adults Who Have Had COVID-19 Still Have "Long COVID" (cdc.gov) Centers for Disease Control and Prevention. (2022, June 22).
2 notes
·
View notes
Text
• the batshit lack of scientific literacy which leads people to not comprehend basic true things like:
biology (trans people are real, gender & sex are a spectrum in every species, this is biological fact). AMA American Medical Association supports this. gender norms are social depending on time period & culture
vaccines (viruses & bacteria exist and we know how to treat them). one of the safest & most effective forms of medicine that exists.
masks work (see above) because they protect against against certain sizes of particles or droplets which can transmit disease
climate - if you dump hot sewage into a lake it becomes polluted & the temp increases. pretend the sky is a big lake and everyone's CO2 is sewage.
antibiotics - stop taking them bc you have the sniffles, you are increasing antibiotic resistance & that is dangerous for the whole community/world. if you have a fever or purulent discharge ANYWHERE, that is the time to go to the clinic for eval. antibiotics DO NOT WORK against VIRUSES or ALLERGIES. Anti-biotic means anti-bacteria. second, you cannot take ANY rando antibiotic for a UTI. every UTI is different and can be caused by a diff bacteria, meaning you will make it worse if you take the wrong antibiotic/increase your resistance to that antibiotic. you HAVE to take your antibiotic in the time it says on the label AND the full course, this is rigorously designed to decrease antibiotic resistance by making sure the bacteria does not replicate in your body enough to overcome the antibiotic in the time it takes for that SPECIFIC ANTIBIOTIC to be metabolized (it involves MATH based on TYPE OF BACTERIA treated - gram pos or gram neg)
essential oils - many essential oils and natural medicinals do work (in context and to a degree)! stop shitting on people who use them you just alienate them from medicine. there is a time for natural cures and a time for acute cures (antibiotics, broken bones, vaccines, cancer treatment or surgery, preventative med scans etc). there are LOTS of schools of medicine - allopathic (Western), TCM, Ayurveda, Quantum medicine, energetic medicine, herbal medicine. All of these have credible research supporting them. Integrative medicine (combining them all) is the future
flouride - it is not poisoning you and it's good for you if you live in a country where it is highly regulated (FDA does regulate, ADA approved and endorses)
the weather - it is not possible with our current technology to control the weather to the degree of hurricanes, blizzards, floods. if it was, someone would have done it and we'd all be dead. cloud seeding is an example of a weather tech that does exist & it's an example of this bc it causes increased respiratory illness where it is done.
clean energy - the only reason we dont have it or highspeed worldwiderail or a highspeed universal translator is... obvious. because those are very much attainable with current tech. we also have buildings with rooftops and free sunlight. free. sunlight. free. energy.
AI - it needs regulation & laws on image/text/audio recording, artistic theft, and data gathering. Right now all it does is steal data & give misinformation. It COULD be used for good (medical imaging assistance) but overwhelmingly is not right now.
things we need to address:
gen z men getting pulled into alt-right pipelines through andrew tate, joe rogan, elon musk, jordan peterson etc
the gullibility and stupidity of half the country voting against our collective best interests
the broad effect social media has on public and common good
lazy minds and lack of empathy
outside-country interference (trump and elon’s connections to russia and the amount of bots from other countries spreading misinformation)
the long-term effects of AI and rampant disinformation
57K notes
·
View notes
Text
Opening Your Earnings: How Much Do Phlebotomists Make and Pay for Services?
# Unlocking Your Earnings: How Much Do Phlebotomists Make and Pay for Services?
**Meta Title:** phlebotomist Salaries: Earnings and Service Costs Explained **Meta Description:** Discover how much phlebotomists earn and the costs associated wiht their services. Learn about salaries, benefits, and tips for entering this rewarding career.
—
## Introduction
Are you considering a career in phlebotomy or simply curious about the earnings in this field? Phlebotomists play a crucial role in the healthcare industry,drawing blood for tests,donations,or research. But how much do they make, and what do you need to know about the costs involved in their services? In this article, we’ll explore phlebotomist salaries, the expenses they incur, and additional insights that can guide you through this rewarding career.
## Understanding Phlebotomy
### what is Phlebotomy?
phlebotomy is the practice of drawing blood from patients for various medical purposes. Phlebotomists are trained professionals who ensure the process is carried out efficiently and safely. This field is essential for diagnostics, blood donations, and medical research.
### The Path to Becoming a Phlebotomist
To become a phlebotomist, individuals typically need to:
– **Complete a Phlebotomy Training program**: These programs can take as little as a few weeks to several months. – **Obtain Certification**: While certification is not always mandatory, it can greatly enhance job prospects. – **Gain Practical Experience**: Many programs include hands-on clinical experience.
## How Much Do Phlebotomists Make?
### Phlebotomist Salaries Overview
Salaries for phlebotomists can vary widely depending on factors such as location, experience, and workplace setting. According to the U.S. Bureau of Labor Statistics (BLS), the median annual wage for phlebotomists in the United States was approximately **$37,000** in 2022. Below is a breakdown of approximate earnings based on experience level:
| Experience Level | Average Annual Salary | |——————|———————-| | Entry-Level | $30,000 – $35,000 | | Mid-Level | $36,000 – $42,000 | | Experienced | $43,000 – $55,000 | | Specialized | $56,000 – $70,000 |
### Geographic Impact on Salaries
Location plays a significant role in determining phlebotomist salaries. Phlebotomists in metropolitan areas or states with higher living costs tend to earn more. Here are the top-paying states for phlebotomists:
– **California**: $47,000 – **Washington**: $45,000 – **New york**: $44,000 – **Massachusetts**: $43,000 – **Virginia**: $41,000
### Benefits of Working as a Phlebotomist
Aside from a competitive salary, phlebotomists may enjoy other benefits, such as:
– **Health Insurance**: Many employers offer health benefits. – **Flexible Hours**: Part-time and full-time positions are widely available. – **Opportunities for Advancement**: With experience and additional training,phlebotomists can move into roles such as laboratory technicians or managers. – **Job security**: The demand for healthcare professionals continues to grow.
## The Costs incurred by Phlebotomists
### Training and certification Costs
While pursuing a career in phlebotomy offers great potential for earnings, it does come with initial costs:
– **Training Program Fees**: These can range from $1,000 to $3,000. - **Certification Fees**: Fees vary but typically range from $100 to $200 per exam. - **Continuing Education**: Many phlebotomists need to complete periodic continuing education, costing around $50+ per credit hour.
### Equipment and Supplies
Phlebotomists may also incur costs related to specialized equipment,such as:
– **Needles and Lab Supplies**: These often need to be replenished and can be costly. – **Uniforms/Scrubs**: Some employers may require specific attire. – **Travel Costs**: For those who travel between locations or work in home health settings.
## Practical Tips for Aspiring Phlebotomists
If you’re looking to transition into this rewarding profession, here are some practical tips:
– **Research Training Programs**: Look for accredited institutions and compare tuition costs. – **Consider Certification**: Obtaining certification from recognized organizations like the National Phlebotomy Association (NPA) can improve job prospects. – **Network in the Industry**: Join local healthcare groups or online forums to connect with experienced professionals. – **gain Volunteer Experience**: Offering your services at blood drives or clinics can provide valuable hands-on experience.
## Case Study: A Day in the Life of a Phlebotomist
### Meet Sara
Sara is a phlebotomist working in a busy urban hospital. She loves her job because of the direct impact she has on patient care. Here’s how a typical day unfolds:
1. **Morning Start**: Arrives at work and prepares equipment. 2. **Patient Interactions**: Draws blood from patients, ensuring a amiable atmosphere to ease anxiety. 3.**Documentation**: Logs blood samples and maintains meticulous records. 4.**Collaboration**: Works with nurses and lab technicians to ensure sample accuracy. 5. **Continual Learning**: Attends a weekly seminar on new phlebotomy techniques and patient safety.
## Conclusion
Phlebotomy is a rewarding career choice for those interested in the medical field, offering competitive salaries and benefits. Understanding how much phlebotomists make and the costs they incur for services is essential for anyone considering this path. By completing the necessary training and gaining practical experience, aspiring phlebotomists can unlock their earnings potential while making valuable contributions to patient care. Whether it’s drawing blood for tests or donations, phlebotomists serve an essential role in the healthcare ecosystem.
**Are you ready to take the next step in your career? Dive into the world of phlebotomy and start your journey today!**
—
This article is structured to provide readers with thorough facts about phlebotomist salaries and the costs associated with their services, while maintaining SEO best practices for improved online visibility.
youtube
https://phlebotomytechnicianschools.org/opening-your-earnings-how-much-do-phlebotomists-make-and-pay-for-services/
0 notes
Text
Opening Opportunities: What Phlebotomy Technicians Earn and How to Boost Your Pay in 2024
Unlocking Opportunities: What Phlebotomy Technicians Earn and How to Boost Your Pay in 2024
Phlebotomy is a crucial role in the healthcare industry, responsible for drawing blood samples from patients for medical testing. As the demand for skilled healthcare professionals rises, so does the interest in earning potential and career advancement within this field. In this article, we’ll explore what phlebotomy technicians earn in 2024 and share effective strategies to boost your pay.
Understanding Phlebotomy Technician Salaries in 2024
According to recent statistics,phlebotomy technicians can expect varied salaries based on several factors,including experience,location,and workplace setting. Here’s a breakdown of what you can typically expect:
Experience Level
Average Annual Salary
Entry-Level (0-1 years)
$30,000 - $35,000
Mid-Level (2-5 years)
$36,000 – $45,000
Experienced (5+ years)
$46,000 – $55,000
Specialized Roles
$56,000+
The figures above represent national averages and can vary significantly based on regional factors and job responsibilities.
Factors Affecting Phlebotomy Salaries
several key factors influence how much phlebotomy technicians earn:
Geographic Location: Salaries may vary significantly from one state to another, or even within regions of a state.
Type of Employer: Hospitals, private clinics, and laboratories often offer different pay scales.
Certification: Certified phlebotomy technicians often earn higher salaries than their non-certified counterparts.
Experience and Skills: More experienced technicians and those with specialized skills typically command higher wages.
How to Boost Your Pay as a Phlebotomy technician
If you’re looking to maximize your earnings as a phlebotomy technician, consider implementing the following strategies:
1. Acquire Additional Certifications
Obtaining certifications from trusted professional organizations can significantly enhance your qualifications. Consider certifications such as:
American Society for Clinical Pathology (ASCP)
National Phlebotomy Association (NPA)
American Medical Technologists (AMT)
2. Gain Experience in Specialized Areas
Specializing in areas like pediatric or geriatric phlebotomy can enhance your value. The more complex the procedures you can perform, the higher your earning potential.
3.Seek Advancement Opportunities
Consider career advancement into roles like a phlebotomy supervisor or training specialist. Leadership positions often offer a higher salary and additional benefits.
4. Networking and Professional Development
Engage in professional networks and organizations. Attend workshops and conferences to stay updated on industry trends and to meet othre professionals who may offer higher-paying opportunities.
5. Negotiate Your Salary
When starting a new job or during performance reviews, don’t hesitate to negotiate your salary. Research the average pay for your role in your area to make a compelling case.
Benefits of Becoming a Phlebotomy Technician
The role of a phlebotomy technician not only offers competitive salaries but also comes with several attractive benefits:
Job Stability: The demand for phlebotomy professionals continues to grow,ensuring job security.
Flexible Hours: Many phlebotomy jobs offer flexible working hours, making this career ideal for those seeking work-life balance.
Personal Fulfillment: Working in healthcare allows you to make a significant impact on patients’ lives.
First-Hand Experiences: what It’s Really Like to Be a��� Phlebotomy Technician
while statistics and factors provide a general overview,hearing from those in the field can offer valuable insights. Here are experiences shared by actual phlebotomy technicians:
“Every day is different! I love being able to connect with patients and help them through a sometimes stressful experience.” – Emily, 3 years in phlebotomy.
“The training can be intense, but it’s worth it when you see how critically important your work is to patient care.” – John, 5 years in phlebotomy.
Conclusion
the earning potential of phlebotomy technicians in 2024 is promising, particularly for those willing to pursue further education, gain experience, and take initiative in their professional development. By understanding the factors impacting salaries and implementing strategies to elevate your career, you can effectively unlock opportunities for a rewarding phlebotomy career. Whether you’re just starting or considering advancements, the future looks radiant for phlebotomy technicians willing to invest in their professional growth.
youtube
https://phlebotomytechnicianschools.net/opening-opportunities-what-phlebotomy-technicians-earn-and-how-to-boost-your-pay-in-2024/
0 notes
Text
Revealing the Costs: How Much Does a Phlebotomy Course Really Cost?
Unveiling the Costs: How Much Does a Phlebotomy Course Really Cost?
Are you considering a career in healthcare? If you’ve found yourself asking, “How much does a phlebotomy course really cost?” you’re in the right place! Phlebotomy is a vital role in any medical facility, making it a sought-after position. In this article, we will delve into the average costs involved in pursuing a phlebotomy course, the benefits of the profession, and some practical tips to help you embark on this rewarding journey.
Understanding Phlebotomy
Phlebotomy involves drawing blood for tests, transfusions, research, or blood donations. It’s a specialized skill that requires training and certification. Being a phlebotomist can be both rewarding and financially stable, which is why many are pursuing this path. But before you enroll in a course, it’s important to have a clear understanding of the associated costs.
Breakdown of Phlebotomy Course Costs
Phlebotomy course costs can vary widely depending on several factors, including location, type of institution, and additional fees. Here’s a detailed breakdown of the potential expenses:
Expense Type
Average Cost ($)
Tuition Fee
1,500 – 3,000
Books and Supplies
200 – 500
Certification Exam Fee
100 – 200
CPR Certification Course
80 - 120
Uniforms and Personal Supplies
50 – 150
Background Check/Fingerprinting
50 – 100
Total Estimated Costs: When combined, the total estimated cost of a phlebotomy course can range from $2,030 to $4,120.
Factors Influencing Course Costs
Several factors can affect the cost of your phlebotomy training:
Institution Type: Community colleges often offer more affordable options compared to private trade schools.
Location: Living in high-cost areas may increase tuition fees.
Course Length: Longer courses may come with higher costs due to extra class hours and materials.
Certification Requirements: Some programs include additional certifications in the cost, while others charge separately.
The Benefits of Taking a Phlebotomy Course
Investing in a phlebotomy course not only prepares you for a successful career but also offers numerous benefits:
Job Demand: There’s a growing need for trained phlebotomists in hospitals, clinics, and labs.
Flexibility: Many courses offer part-time and online options, accommodating your schedule.
Short Training Period: Most phlebotomy programs can be completed in a few months, allowing you to enter the workforce quickly.
Good Earning Potential: The average salary for a phlebotomist can range from $30,000 to $40,000 annually.
Practical Tips for Aspiring Phlebotomists
Here are some helpful tips to ensure you maximize your phlebotomy training experience:
Research Programs: Look for accredited institutions that offer robust training programs and consider their reputation in the job market.
Compare Costs: Don’t settle for the first option; compare multiple programs to find one that fits your budget.
Consider Online Courses: If you’re short on time, look for online or hybrid programs that allow theoretical learning from home.
Network: Connect with current phlebotomists or instructors to gain insights and tips for succeeding in your education and career.
Case Studies: Real Experiences from Phlebotomy Students
Here are a couple of first-hand experiences from recent phlebotomy students:
Student A: Community College Success
“I enrolled in a community college phlebotomy program that cost me about $2,500. I found the costs manageable due to financial aid options, and I completed my training in just four months. The hands-on training and externship paved the way for my job in a local clinic.”
Student B: Private School Experience
“I took a phlebotomy course at a private trade school. Although the tuition was higher at $3,500, the small class sizes and personalized instruction made a huge difference. I was well-prepared for my certification exam, and within weeks of graduating, I landed a job in a hospital.”
Conclusion: Making an Informed Decision
Understanding the costs associated with phlebotomy training is crucial for those considering this career path. With tuition ranging from $1,500 to $3,000 and additional expenses, it’s essential to budget wisely and explore funding options such as financial aid and scholarships.
By investing in a phlebotomy course, you’re embarking on a fulfilling career path with a growing job market and the opportunity to make a significant impact in the healthcare field. Make sure to research thoroughly, connect with professionals, and choose a program that fits your financial and educational needs. Good luck on your journey to becoming a certified phlebotomist!
youtube
https://phlebotomycertificationcourse.net/revealing-the-costs-how-much-does-a-phlebotomy-course-really-cost/
0 notes
Text
For how long Is the Phlebotomy Program? Your Complete Guide to Training Duration and Career Path
How Long Is the Phlebotomy Program? Your Complete Guide to Training Duration and Career Path
How Long Is the Phlebotomy Program? Your Complete Guide to Training Duration and Career Path
Are you considering a career in the healthcare field? Phlebotomy could be a rewarding path for you, offering the chance to work directly with patients and play a crucial role in diagnostic processes. But how long is the phlebotomy program, and what does it entail? This comprehensive guide will break down everything you need to know about the training duration, career paths, and the benefits of becoming a certified phlebotomist.
Understanding Phlebotomy
Phlebotomy is the practice of drawing blood from patients for testing, transfusions, or donations. A trained phlebotomist must understand various blood-drawing techniques, patient anatomy, and laboratory safety standards. With the increasing demand for healthcare professionals, the need for skilled phlebotomists is higher than ever.
How Long Does the Phlebotomy Program Last?
The duration of phlebotomy training programs can vary significantly based on educational methods and institutions. Here’s a quick overview:
Program Type
Duration
Typical Courses
Certificate Program
4-8 Months
Introduction to Phlebotomy, Safety Protocols, Anatomy
Diploma Program
9-12 Months
Advanced Phlebotomy Techniques, Patient Care, Lab Procedures
Associate Degree
2 Years
Phlebotomy Practices, Medical Ethics, Clinical Laboratory Science
1. Certificate Programs
Most straightforward and the most common route to enter the field, certificate programs typically last between 4 to 8 months. They focus primarily on the essentials of blood collection and may include a clinical externship component for hands-on experience.
2. Diploma Programs
A diploma program extends training to about 9-12 months and often includes more in-depth courses. These programs may also provide more comprehensive clinical experience, making graduates highly skilled and employable.
3. Associate Degrees
For those looking for a more in-depth education, an associate degree in phlebotomy generally takes about 2 years. This degree option not only covers phlebotomy practices but also includes general education classes, giving a broader background in medical and health sciences.
Career Paths in Phlebotomy
Phlebotomists can work in various settings, including:
Hospitals
Laboratories
Clinics
Blood donation centers
Home health services
Additionally, experienced phlebotomists can advance their careers by taking on supervisory roles, specializing in certain procedures, or pursuing further education in related fields, such as nursing or laboratory technology.
Benefits of Choosing a Phlebotomy Career
Short Training Time: Compared to many other medical careers, phlebotomy programs take much less time.
High Demand: With a growing healthcare sector, the demand for phlebotomists continues to rise.
Hands-on Work: If you enjoy working directly with people and providing valuable medical services, this career may be ideal.
Flexible Hours: Many institutions offer part-time shifts, allowing for a better work-life balance.
Practical Tips for Aspiring Phlebotomists
If you’re interested in enrolling in a phlebotomy program, consider the following tips:
Research accredited programs to ensure quality education.
Look for programs that offer hands-on clinical experience.
Check job placement services provided by the school.
Consider financial aid options if needed.
Personal Experience from the Field
To better understand the day-to-day experiences, we spoke with Jane Doe, a certified phlebotomist with over 5 years of experience:
“The training was intense but incredibly rewarding. I loved being able to help patients feel at ease during a potentially stressful procedure. The skills I learned in my program helped me become confident in my abilities, and I’ve built meaningful connections with my patients over the years.”
Conclusion
becoming a phlebotomist can be a swift and rewarding career path with training programs lasting from 4 months to 2 years, depending on the educational route chosen. With the healthcare industry continually expanding, a certified phlebotomist possesses valuable skills that are in high demand. By choosing a program that suits your goals and interests, you can kickstart a fulfilling career in a thriving field. Whether you aim for a certificate, diploma, or degree, the journey into phlebotomy promises both professional growth and personal satisfaction.
youtube
https://phlebotomyschoolsonline.org/for-how-long-is-the-phlebotomy-program-your-complete-guide-to-training-duration-and-career-path/
0 notes
Text
Assignment: Community and Health PSA
Navigating My First Few Weeks at HCC: What I’ve Learned So Far
Transitioning into life as a college student feels a bit like being thrown into the deep end-often, there's just so much to learn. I took my Intro to HCC class for a few weeks, and already I know about what I've learned about myself, my goals, and how to maneuver through navigating life in college. A couple of the things I have learned about the first few modules:
Module 1: Personal Purpose Statement & Academic Goals
It was building a personal purpose statement as well as setting academic goals in the first module. I did not realize the importance of knowing the reason why I pursue a college education. Purpose statements led me to think about my long-term goals and how they relate to the pursuit of psychology
Moreover, we were introduced to the various educational avenues through which one can traverse at HCC, such as the Associate in Arts (AA) and Associate in Science (AS) degrees. That is, the AA perfectly serves students intending to transfer to a 4-year university, whereas the AS degree serves primarily for rapid on-the-job workforce entry. Here, I learned that I can structure my educational pathway.
Module 2: Meeting Your Advisor
Module 2 came with an activity where we were to meet with our academic advisor to create the Education Plan. I was a bit anxious on the day of the meeting, but it was worth it as my advisor literally helped me decide on the classes that I should take and gave me tips on transferring to a university after my AA. The takeaway? You got it: staying organized and meeting deadlines keeps everything on track.
Module 3: Career Exploration
Module 3 has been completely devoted towards career exploration. Career research and Career Presentation are their main aspects. I chose Clinical Psychology because it is my field of interest. In this module, I found out learning the educational path to earn a degree in psychology like applying for graduate studies after acquiring a bachelor's degree. This module has helped me connect my educational goals with my career ambitions and made me realize the importance of staying focused on both.
Module 4: Financial Capability
Module 4 also talked about the tuition fee and how to financially prepare oneself for pursuing higher education. There were topics covered such as size and types of scholarship, financial aid and benefits it considers over time for attaining a degree. It was one of those real eye-openers comparing what a degree makes in future dividends compared to what someone would earn without one, as it brought to bear a clearer understanding of the importance of investing in my education.
Module 5: College Support Systems Directory
This module propelled me into exploring the various available support services under HCC-tutoring, career counseling, and mental health resources, among others. It opened my eyes to the reality that college life does not have to be endured alone. There kind of a support available, and that will make a world of difference to my success.
Module 6: Academic Advising Part 2
Module 6 was all about talking with my advisor about finalizing my Education Plan and seeing if I'm on the right track. After reviewing it, I felt much more confident about my next steps in education. My advisor helped me pin down the classes to prepare me for my psychology career and gave me a quick transfer to a four-year university. It was a good reminder that academic advising isn't something you do once, and it's important to check back every so often to see that I'm continuing to make the best choices.
Module 7: Community Engagement
The last area that I have taken, Module 7, is about community engagement; it relates pretty much to my career area of interest, which works to assist others. Another thing we are doing is working on a Public Service Announcement (PSA) project that will raise awareness about some issue we will comprise within the important ones. By that, I will get to combine everything that I learn at college and preserve touch with the real world. Whether it is about mental health, education, or any other cause, this will definitely inspire me to think about how I can apply my teachings to impact the community.
So far, it is organizing my time, learning how to set clear goals, and exploring the resources around me. Most importantly, I am getting more confident about my future, given that there is a sound plan in that direction now. College is not just about classes but also setting up a future for oneself and moving forward with it, rich and real!
1 note
·
View note
Text
Phlebotomy Pay Scale: How Much Does a Phlebotomist Make?
**Title: Phlebotomy Pay Scale: How Much Does a Phlebotomist Make?**
**Introduction:** If you’re considering a career in phlebotomy, one of the key factors you may be interested in knowing is the pay scale for phlebotomists. Phlebotomists play a crucial role in the healthcare industry by drawing blood for medical tests, donations, and research purposes. In this article, we will explore the average salary range for phlebotomists, factors that can influence pay, and tips for maximizing your earning potential in this rewarding career.
**Average Salary Range for Phlebotomists:** According to the Bureau of Labor Statistics, the median annual wage for phlebotomists in the United States was $36,480 as of May 2020. The lowest 10 percent earned less than $26,000, while the highest 10 percent earned over $50,000. However, it’s essential to note that pay can vary depending on factors such as location, experience, education, and employer.
**Factors Influencing Phlebotomy Pay:** Several factors can impact a phlebotomist’s salary, including:
1. **Location:** Phlebotomists working in metropolitan areas or in states with higher costs of living tend to earn higher salaries. 2. **Experience:** More experienced phlebotomists may command higher pay rates than those who are just starting. 3. **Education:** Phlebotomists with additional certifications or degrees may qualify for higher-paying positions. 4. **Employer:** Working for a hospital or healthcare facility can often result in higher salaries compared to working for a smaller clinic or laboratory.
**Ways to Maximize Your Earning Potential:** If you’re looking to increase your salary as a phlebotomist, consider the following tips:
1. **Obtain certification:** Getting certified by a reputable organization like the National Healthcareer Association (NHA) can make you more competitive in the job market and lead to higher pay. 2. **Pursue additional education:** Consider pursuing further education or training in the field of phlebotomy to increase your skills and qualifications. 3. **Gain experience:** As you gain more experience in the field, you may become eligible for promotions and higher-paying positions. 4. **Negotiate your salary:** When applying for a new job or during performance reviews, don’t be afraid to negotiate your salary to ensure you’re being fairly compensated for your skills and experience.
**Conclusion:** the pay scale for phlebotomists can vary depending on location, experience, education, and employer. While the median salary for phlebotomists is around $36,480 per year, there are ways to increase your earning potential in this field. By obtaining certification, pursuing additional education, gaining experience, and negotiating your salary, you can set yourself up for a successful and financially rewarding career as a phlebotomist.
youtube
https://phlebotomycareertraining.net/phlebotomy-pay-scale-how-much-does-a-phlebotomist-make/
0 notes
Text
3 questions: Leveraging insights to enable clinical outcomes
New Post has been published on https://thedigitalinsider.com/3-questions-leveraging-insights-to-enable-clinical-outcomes/
3 questions: Leveraging insights to enable clinical outcomes

Associate Professor Thomas Heldt joined the MIT faculty in 2013 as a core member of the Institute for Medical Engineering and Science (IMES) and the Department of Electrical Engineering and Computer Science. Additionally, Heldt is a principal investigator with MIT’s Research Laboratory of Electronics (RLE), and he directs the Integrative Neuromonitoring and Critical Care Informatics Group in IMES and RLE. He was recently named an associate director of IMES, where he will focus on internal affairs, among other duties.
Heldt received his Medical Engineering and Medical Physics (MEMP) PhD from the Harvard-MIT Program in Health Sciences and Technology (HST) in 2004. Heldt’s research interests include signal processing, estimation and identification of physiological systems, mathematical modeling, model identification to support real-time clinical decision making, monitoring of disease progression, and titration of therapy, primarily in neurocritical and neonatal critical care. Here, Heldt describes how he collaborates closely with MIT colleagues and others at Boston-area hospitals, and how his research uses and analyzes physiologic data to aid clinical action.
Q: How does your research apply to solving clinical needs?
A: We look at current clinical environments and observe the volumes of multimodal physiologic waveform data that are collected on patients in critical care, peri-operative care, or even emergency care. Much of this data is typically visually reviewed by the clinicians and subsequently discarded after a holding period of just a few days. We thus lose the opportunity for more systematic analyses and for deriving patient-specific insights. Critical to such analyses of these data streams is a deep understanding of the relevant physiology at the time scales of interest. We leverage insights from physiology, formulated as reduced order mathematical models capturing the essential mechanisms that enable clinical action. We have applied this approach successfully to estimate intracranial pressure noninvasively, to make diagnostic decisions based on the analysis of the shape of the capnogram, and, are currently using ultrasound-based approaches to detect embolic events in patients on life support, such as ventricular assist devices or extracorporeal membrane oxygenation.
Q: You work closely with colleagues across MIT, and with clinicians at Boston-area hospitals, including Boston Children’s Hospital (where you hold a courtesy research appointment in neurology), Boston Medical Center (neurosurgery), and Massachusetts General Hospital (emergency medicine). What has been the fruit of some of these collaborations — what is the impact on your research?
A: Boston is a fantastic place to conduct translational research that crosses from our laboratories at MIT into the clinical environments for validation in the actual target patient population! The collaborative disposition and forward-thinking mindset of our clinician colleagues have really been fundamentally enabling for our research and have provided amazing mentoring to our students, postdocs, and me. We have collected validation data in brain-injured patients in the ICUs [intensive care units] at Boston Medical Center, Boston Children’s Hospital (BCH), and Beth Israel Deaconess Medical Center (BIDMC); we have collected pilot and validation data for our capnography work in the emergency departments at BCH and BIDMC; we have collected data for our emboli work in the operating rooms and ICUs at BCH, and have analyzed the medical records of the neonatal ICU at BIDMC and the emergency department at Massachusetts General Hospital.
Our work with the neonatologist at BIDMC was focused on analyzing the monitoring alarm patterns in the neonatal ICU. We counted a staggering 177 alarms/baby/day, or one alarm every eight minutes on average, per baby. And this is a 54-bed neonatal ICU operating close to capacity every day! Such volumes of alarms contribute to noise pollution in an environment that should ideally be very calm. Additionally, since most of the alarms are nuisance alarms or do not require any clinical intervention, the clinical staff becomes desensitized to the alarm load and might end up ignoring truly important events. We analyzed the alarm patterns and alarm thresholds for a particular type of heart rate alarms and recommended a change in thresholds. This resulted in a 50 percent reduction in heart rate alarms per patient per day. Initially, the clinical staff had to file weekly reports to make sure the reduction in the alarm rate did not result in missed or adverse events. After about three months without a single reportable event, the hospital safety committee approved the change.
With colleagues from the MGH Department of Emergency Medicine, we developed and tested a triage rule to identify patients at risk of septic shock. At the time, the MGH ED [emergency department] saw more than 120,000 patients/year, and around 75 percent of patients ending up in the ICU with severe sepsis and septic shock came through the emergency department. Hence, ED triage was the first point of patient contact and the first opportunity to flag patients for possible sepsis and septic shock and initiation of early goal-directed therapy. One result of our work was a significant reduction in the time to appropriate antibiotic administration in the emergency department. The work was subsequently validated in other Partners hospitals and implemented in the electronic medical record system of Partners-affiliated hospitals.
Q: Can you talk a bit about your background, and about how you became interested in systems-physiology and biomedicine? What are your goals for your research, and for your career?
A: That is a longer story! In short, I started out studying physics back in Germany. After a while, I got interested in applying concepts I learned in physics to physiology and medicine, so I designed my own MD/PhD program by picking up medicine as a second major. Through some fortuitous events, I ended up attending surgeries for congenital heart defects for about a term. This was a very formative experience, and almost pushed me toward dropping physics and going all-out on becoming a surgeon. However, I had also always wanted to spend part of my education abroad and had applied to various universities in the U.S. I ended up getting admitted to the graduate physics program at Yale and spent a couple of years doing nonlinear optics. While I loved the work at Yale and had a fantastic mentor, I missed the clinical exposure and application of my work to medicine. I had heard about the HST program and decided to send in an application. I joined the MEMP program in 1997 and have been at MIT ever since.
In our current research, we are very interested in providing better monitoring modalities for patients with brain injuries. We are developing novel algorithmic and device approaches so we can replace the current invasive monitoring modalities with entirely noninvasive ones and provide additional clinically actionable information that gives insights on the physiology of the injured brain and can help guide treatment decision. I want to see some of these technologies through to routine deployment at the bedside.
The great thing about being in IMES and MIT is that we everybody is very collaborative. What I am looking forward to is much of the same, working with colleagues in IMES on important problems that none of us is be able to tackle alone, but that together we have a real chance of tackling — and having fun along the way!
#000#Administration#amazing#analyses#Analysis#antibiotic#approach#baby#background#Beth Israel Deaconess Medical Center#biomedicine#Brain#brain injuries#career#change#Children#clinical#Collaboration#collaborative#computer#Computer Science#data#Data Streams#decision making#deployment#devices#Disease#education#Electrical engineering and computer science (EECS)#electronic
0 notes
Text
Understanding Laser Skin Whitening Treatment Price: What You Need to Know
Laser skin whitening treatments have gained popularity as a quick and effective way to achieve a brighter and more even skin tone. However, many individuals interested in this procedure often find themselves asking, "How much does it cost?" In this blog, we will explore the various factors that influence the price of laser skin whitening treatments and what you can expect in terms of costs.
What is Laser Skin Whitening?
Laser skin whitening is a non-invasive procedure that utilizes laser technology to reduce melanin production in the skin, leading to a lighter and more uniform complexion. The treatment targets areas of hyperpigmentation, sunspots, and uneven skin tone, making it a popular choice for those seeking a more radiant appearance.
Factors Influencing the Cost of Laser Skin Whitening
Clinic Reputation and Location
The reputation of the clinic and its location play a significant role in pricing. Established clinics in metropolitan areas may charge more due to their advanced technology, skilled professionals, and higher operational costs.
Type of Laser Used
Different types of lasers (such as Q-switched lasers, fractional lasers, or CO2 lasers) have varying costs associated with their use. More advanced technologies may offer better results but can also come with a higher price tag.
Treatment Area
The size and area being treated can affect the overall cost. Treating a small area, such as the face, may be less expensive than a full-body treatment.
Number of Sessions Required
Most patients require multiple sessions to achieve optimal results. The total cost will depend on the number of sessions recommended by your dermatologist or skincare professional.
Consultation Fees
Initial consultations with dermatologists or skincare specialists may incur additional fees. It’s essential to consider these when budgeting for your treatment.
Average Costs of Laser Skin Whitening Treatments
The price for laser skin whitening treatments can vary widely based on the factors mentioned above. On average, you can expect to pay:
Per Session: INR 5,000 to INR 20,000, depending on the clinic and technology used.
Total Treatment: For a complete treatment course (usually 3 to 6 sessions), the total cost may range from INR 15,000 to INR 1,20,000.
Additional Costs to Consider
Post-Treatment Care: Some clinics may recommend specific skincare products or treatments to enhance results and maintain your skin’s health. These can add to the overall expense.
Follow-Up Appointments: Regular check-ups to monitor progress and any necessary touch-ups may also contribute to the total cost.
Is It Worth the Investment?
While laser skin whitening treatments can be a bit pricey, many individuals find the results worth the investment. Achieving a brighter and more even skin tone can boost confidence and enhance your overall appearance. However, it’s crucial to do your research, choose a reputable clinic, and consult with a qualified dermatologist before undergoing any treatment.
Conclusion
Understanding the price of laser skin whitening treatments involves considering various factors, including the clinic’s reputation, the type of laser used, and the number of sessions required. While the costs can vary, it’s essential to weigh the benefits against the investment. With the right approach, you can achieve the glowing skin you desire.
If you’re considering laser skin whitening treatment, ensure you consult with a qualified professional to discuss your options and get a personalized quote.
0 notes