#antiretroviral therapy
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has a 66 index score for customer satisfaction in the US.
Text
Immunomodulators' Power: Widening Applications and Medical Impact
Immunomodulators have emerged as crucial components in the field of medicine, gaining increasing attention for their ability to regulate and modify the immune system’s responses. These agents play a pivotal role in treating a diverse range of conditions, from autoimmune diseases and cancer to infectious diseases and organ transplants. By modulating immune responses, immunomodulators offer…

View On WordPress
#Allergies#Anti-Inflammatory Medications#Antiretroviral Therapy#Autoimmune Diseases#Cancer Treatment#Cytokinesis#Immunomodulators#Immunomodulators Applications#Immunomodulators Market#Infectious Diseases#Organ Transplants#Rheumatoid Arthritis#Vaccines
1 note
·
View note
Text
youtube
#HBV#HIV-1#hepatic flare#antiretroviral therapy#HBsAg seroclearance#HBV/HIV co-infection#immune reconstitution#liver enzymes#viral clearance#chronic hepatitis B#HIV treatment outcomes#liver health#ART-induced immune response#infectious diseases#hepatology#co-infection management#liver function monitoring#viral hepatitis#immune response dynamics#public health.#Youtube
1 note
·
View note
Text
#The ART Of Life After HIV: HIV & Antiretroviral Therapy (ART)#Antiretroviral Therapy#Antiretroviral Therapy For HIV#Antiretroviral Therapy HIV Treatment
1 note
·
View note
Text
Omg and people two cubes down from you have no idea what your abbreviations and acronyms and special jargon are and sometimes you'll be talking with another professional in the field and *think* you're both using the same acronym but you're NOT.
No one tells you when you get a Big Serious Job™ how many fucking abbreviations you’ll be forced to learn.
#this is enough of a problem that at the big national conference i went to for work this year the us dshs had clearly instructed all the#presenters to say the full goddamn name and not just use the acronym. department of state health services (dshs said dishes)#health resources and services administration (hrsa said hersa)#and that's not even for the really particular acronyms & abbreviations lol#but it did have to be intelligible to people at all levels of expertise so. like i get it#but it didn't stop presenters from throwing AZT around! me mentally updating them: ZDV XD which is still not the full modern name#anyway azidothymidine (azt) aka zidovudine (zdv) brand name Retrovir was the first and for way too long only effective ART antiretroviral#therapy and is still used today especially to prevent mother-to-child HIV human immunodeficiency virus transmission but also in other uses#and my silly brain took quite a while to stop seeing azithromycin and calling it azt. yes the letters are there. no the antibiotic isn't ART#and DEFINITELY ABSOLUTELY do not put such notes as “pt was administered AZT” when it was in fact azithromycin. oh but the abbreviation is#just sitting right there...so easy...NO. NOMENCLATURE CLARITY IN NOTES TO BE READ BY OTHERS. it is important.#meanwhile my team's dshs consultant be like argh yet another event note with random abbreviations#it's uh...it's hard not to use them...
42K notes
·
View notes
Text
HIV/AIDs Research and Treatment Breakthroughs
Explore the latest breakthroughs in HIV/AIDS research and treatment, that have the potential to reshape the landscape of HIV/AIDS management.
#"HIV/AIDS Research and Treatment#HIV Care#HIV Cure Research#Antiretroviral therapies#current research on HIV/AIDS#CME Programs#CME Conferences#CME Medical courses#CME credits#doctor conferences#medical CME#Primary Care Conference#Medical CME Online#Emergency Medicine Online CME#Medical Conference Website#Physician Conferences#Medical CME Courses#Doctors CME Conferences#CME training for Physicians#Medical Event Organizer#Organizing Medical Events#Medical Conferences#Medical Speakers#Healthcare Marketplace
1 note
·
View note
Note
wait, can you actually have hpv and still have sex? i kinda always thought hpv was like The End until you could get it undetectable or something and that that would take like three years and if you don't get treated you die
hi anon,
I believe that you're thinking HIV, not HPV.
however, HIV also doesn't have to be the end of a person's sex life. when managed properly with antiretroviral therapy a person can become "undetectable," meaning that there is no longer enough of the virus in their body to be detected by an HIV test. a person can become undetectable in as little as 1-6 months, and as long as they continue taking their medication and maintain their undetectable status afterward they will not be at risk of transmitting HIV to sexual partners or, if they are capable of giving birth, transmitting to their children.
people with HIV, like people with any STI, deserve and are capable of healthy and fulfilling sexual relationships and regularly live long, happy lives with their infections.
196 notes
·
View notes
Text
It was the mid-1980s when Paul Toh came of age as a gay man, decades before smartphones and dating apps made sex a lot more accessible right at your fingertips. Toh has been diagnosed with HIV since 1989.
Now semi-retired with his own business distributing antiretroviral therapy medication and HIV pre-exposure prophylaxis (PrEP), the 59-year-old said that in those days, cruising in public parks, toilets, and back alleys of dirty shophouses along pre-cleanup Singapore River for sex was par for the course.
Unsurprisingly, cruising in public made gay men easy targets for police officers. “They started going to these cruising grounds undercover, with the explicit intention of entrapping and arresting gay men,” Toh added.
Police raids in nightlife establishments with gay clientele also became common, with prominent gay discotheque Niche having its liquor license withdrawn by the police in 1989 and the Rascals incident of 30 May 1993, in which multiple patrons were arrested for not having their NRICs on them. This came to be remembered by veteran activists as Singapore’s Stonewall.
Fear about the spread of AIDS was part of the reason why police intensified their clamp down on queer spaces. In April 1987, Singapore experienced its first AIDS-related death. And one year later, the Director of Public Affairs of the Singapore Police Department said in a Straits Times article that “homosexual activities have been strongly linked to the dreaded AIDS disease,” making it an “added reason in the public interest for police to disallow homosexuals to convert places licensed for entertainment into places where they can congregate.”
Iris’ Work of Fighting Stigma
76-year-old health advisor Iris Verghese was among the first health workers to rise to the occasion when Singapore reported its first HIV/AIDS cases.
“I knew just as little about HIV/AIDS as everyone else,” said the retired nurse, who first joined Middle Road Hospital, a now-defunct treatment centre for sexually transmitted diseases, in 1974. As part of her job, Verghese was tasked with contact tracing people who had sexually transmitted infections.
The job brought Verghese to brothels and nightclubs in Geylang’s red-light district, which meant she was no stranger to serving society’s Others with kindness.
“A lot of it has to do with my faith.”
“I thought about my role models like Jesus and Mother Teresa—they didn’t care what illness you had. If they could hang out with people with leprosy, then who am I to refuse to care for those with HIV/AIDS?”
Verghese’s work is well-documented, and everyone has given her the accolades she deserves—from President Halimah Yacob to the Roman Catholic Archdiocese of Singapore to the Straits Times, which named her an everyday hero in 2019.
Plague, a 15-minute short film by Singaporean filmmaker Boo Junfeng, captures the emotional gravity of the care work performed by Verghese and health workers like herself.
The emotionally-stirring film is inspired by Verghese’s work with HIV/AIDS patients in the ’80s and offers a look into the life of Jamie, a patient who stopped coming to the clinic for treatment and counselling.
In the film’s climax, set in the patient’s HDB flat, Verghese tries to dissuade Jamie from inflicting internalised stigma. Jamie insists on using disposable plastic cups and utensils and cleaning every surface he touches for fear of passing the virus to his loved ones.
Wanting to prove that HIV/AIDS is not transmissible through saliva, Verghese takes Jamie’s plastic cup and drinks from it. She then hands him a regular glass, beckoning for him to drink from it, only for him to swipe it away, breaking the glass and cutting himself in the process.
Thus comes the true test of Verghese’s dedication to her profession as she steels herself to the drastically heightened risk. Now that her patient is bleeding, she is dealing no longer just with saliva, but with blood carrying the virus.
In our interview, Verghese recalled many incidents like these. One that stuck with me was her counselling session with Singapore’s first HIV patient, a young gay professional, in 1985. “As I listened to him and gave him a hug, he broke down and cried,” she said. “He said he felt so good afterwards.”
Safe Sex Outreach in the 80s
“Things were very different in the ’80s and ’90s,” said Professor Roy Chan, Founding President of Action for AIDS Singapore (AfA). AfA is a non-government organisation founded in 1988 to fight HIV/AIDS infection in Singapore.
“There was no internet then. When we set up AfA, we had to rely on word of mouth, phone calls, faxes, pagers, and so on. Mobilisation was not as easy then, but we overcame the obstacles we faced. It was very much more hands-on in those days,” Chan recalled.
Chan set up AfA as a non-governmental organisation in 1988 to respond to the needs of people living with HIV/AIDS, regardless of their sexual orientation or gender identity, as well as to advocate for greater action and awareness around HIV/AIDS.
AfA was also one of the first community groups in Singapore that served the needs of LGBTQ+ individuals—namely men who have sex with men—disproportionately affected by HIV/AIDS.
“Back then, people didn’t have as much access to the internet as we do today, meaning that accurate information on HIV/AIDS was much harder to come by, making education efforts vital,” Chan recalled. “On the flip side, no internet meant the gay nightlife scene was more vibrant than what it is today.”
Since the gay community in the 1980s and 1990s did not have the internet and mobile phone apps to meet other people online, they had to go to physical spaces to fulfil their need for connection, whether it was nightlife establishments or cruising grounds.
Gay clubs were hence crucial in AfA’s outreach programs on safe sex practices back in the ’80s—even if it meant risking the possibility of police raids.
Back then, there were very few places in Singapore where gay men felt safe enough to gather in abundance, making gay clubs a viable hub for outreach and education.
AfA’s outreach efforts endure today in the form of the Mobile Testing Van initiative on weekends. The van, parked outside popular gay nightlife spots in Singapore, aims to bring HIV testing closer to the public, bridging the fear and stigma of walking into a stand-alone clinic to get tested.
The Consequence of Outreach
The people brave enough to put themselves out there to serve a larger cause were but a small minority, especially given the cultural milieu of the time.
“There was so much that was unknown about HIV/AIDS even among the medical community, much less the general public,” said Verghese.
“Even at Middle Road Hospital, two doctors resigned, and twenty-five nurses asked to be transferred out.”
AfA’s awareness campaigns and fundraiser drives drew a lot of publicity—and no doubt some backlash.
Still, beneath all the headlines and the star power lent by high-profile celebrity allies was the silence surrounding individual HIV/AIDS cases.
“It was all very hush-hush. People didn’t want to talk about it. No one wanted to know who died of AIDS,” Verghese shared when I asked if the atmosphere in the 90s was similar to that depicted in films and drama series such as The Normal Heart and Pose.
The shows portrayed the HIV/AIDS crisis in the disease’s epicentre in New York as being a time of deaths and countless funerals attended by surviving gay men.
One exception to this veil of silence was Paddy Chew, the first Singaporean person to come out publicly as being a person living with HIV/AIDS.
Chew—well-known for his one-man autobiographical play Completely With/Out Character—told Verghese and her husband that he wanted no crying at his funeral.
“He asked me to arrange his funeral such that his ashes will be thrown into the sea from a Singapore Armed Forces boat,” said Verghese. She and Chew’s close friends were instructed to be dressed in their party best, with helium balloons that were to be released out at sea.
“There was one helium balloon that drifted away from the other balloons. To me, that felt like it was Paddy’s soul saying goodbye to us one last time.”
A Tale of Two HIV Diagnoses
Perhaps by coincidence—or not, since Verghese was one of the very few nurses dedicated to caring for HIV/AIDS patients at the time—Toh’s then-partner was also one of Verghese’s patients.
“My then-partner Freddie and I handled our HIV diagnoses very differently, but of course, we also came from very different backgrounds and life experiences,” said Toh.
“I found out about my status because an ex-lover of mine had come down with pneumocystis pneumonia (PCP). I flew to Sydney for a diagnosis so that I wouldn’t be registered in the local system here if I was found to be positive.”
On the other hand, Freddie found out about his HIV-positive status because he was a regular blood donor. Not only was his diagnosis inevitably recorded in the national registry, but Freddie also ran into legal trouble. He was charged in court for false disclosure of his sexual activity.
“Because of how the entire trial turned out, Freddie was sentenced to imprisonment for twice the expected duration. It affected his entire outlook in life, feeling like he was being framed by a bigger power with an agenda, with the whole world against him,” said Toh, who cared for Freddie until he passed in 2008.
Toh, on the other hand, took his diagnosis as an opportunity to re-evaluate his life and make the most of the eight years that the doctor told him back in 1989 he had left to live.
“When I received my diagnosis, the only thing in my mind was this: it is the quality of life that matters, not the quantity.” And so, the two spent the next few years of their lives travelling the world, making their remaining years as meaningful as they could be.
Anything for a Chance at Life
Maximising his remaining years did not stop at travel for Toh. Having managed to get his hands on antiretroviral therapy in Sydney in the form of azidothymidine (AZT), he went on to look for more effective forms of medication while the technology was being developed in real-time. Toh wanted to help other HIV patients like himself.
In 1994, Toh joined the Asia Pacific Network of People with HIV/AIDS (APN+), a regional network advocating for the improvement of the lives of people with HIV/AIDS in the Asia-Pacific region, later becoming a Board member and secretariat.
“North America and Europe were progressing swiftly in their battle against HIV/AIDS thanks to the work of activists there putting pressure on their governments and the medical community to channel funding towards the research and development of suitable treatment for HIV/AIDS,” said Toh.
“In Asia, however, it’s a different story. We had to be street smart in our advocacy while also looking elsewhere for allies.”
This meant looking to donors in the West who could be persuaded to recognise the importance of HIV/AIDS advocacy in Asia.
“I was very lucky to have the opportunity to be one of the first few Asians who had access to HAART, said Toh.
HAART (Highly active antiretroviral therapy) is a triple-combination of antiretroviral drugs discovered in 1996 by Professor David Ho. Toh had been invited to attend the 11th International Conference on AIDS in Vancouver, Canada, where the discovery of this triple cocktail was announced.
Within three months of beginning HAART treatment in 1996, Toh saw his health improving tremendously, with his CD4 count—a measure for the immune system of PLHIV—increasing exponentially and his viral load becoming undetectable within the fourth month.
Although Toh already had a supply of free antiretroviral medication from his healthcare provider in Sydney, he continued to look elsewhere for alternative sources for patients who were unable to afford the patented medication.
“Unlike Taiwan, Hong Kong, and South Korea, where medication for HIV/AIDS was provided to patients for free, Singapore was the only Asian Tiger which did not do so,” said Toh.
“Meanwhile, pharmaceutical companies in developing countries like Brazil, India, and Thailand were manufacturing their own generic antiretroviral medication in spite of patent laws, making it more affordable.”
While still not free, MOH announced in 2020 that HIV medication would become subsidised.
Singapore’s Very Own ‘Buyers Club’
With patented HIV/AIDS medication in the ’80s continuing to be inaccessible to many who needed it, buyers clubs—similar to the one featured in the 2013 film Dallas Buyers Club—would soon emerge worldwide, including Singapore.
“The funny thing was that Australia had easy access to HIV/AIDS medication, so there was a lot of stock available in Sydney,” said Verghese. A family vacation down under in 1987 turned into an informal research trip for her to network and gather the information that she needed to perform her job optimally.
During her trip, she met HIV researcher Dr David Cooper, who brought her to Albion Street Centre (now known as The Albion Centre), which specialises in HIV/AIDS management.
Through her newfound contacts, Verghese managed to get her hands on some of the unused stocks of medication in Sydney back to Singapore for her support group.
“We even got the help of the Singapore Airlines flight attendants to pool together their unused baggage allowance to bring this medication back,” she recounted with a laugh.
Antiretroviral medication was not the only asset that Verghese brought back. She learned a lot about the virus from the professionals she met in Sydney, allowing her to move faster than the national response and gather the information needed to tend to her patients.
A Ground Up Initiative
“George Yeo was actually very impressed with what we were doing,” recounted Verghese. “He wanted to meet with the community to learn more about our efforts and arranged a closed-door meeting with us.”
The meeting was the culmination of months of sending letters to Yeo, the Minister of Health at the time. The dialogue session was held to discuss the government’s rule that mandated the bodies of AIDS sufferers to be buried or cremated within twenty-four hours of dying.
This rule was finally lifted in December 2000, after four years of advocacy by AfA.
They argued that the policy was outdated, having been implemented in the mid-1980s when hardly anything was known about HIV/AIDS.
“I think we’ve certainly had to prove ourselves as an organisation over the years,” Chan said. “There might have been concerns among some who thought of us as a gay rights organisation, or misconceptions that AfA worked solely on issues that concern gay people.”
“But we’ve proven ourselves over the years to be a serious and effective organisation tackling HIV/AIDS and sexual health with clear metrics of success, and the results and continued support from the government speak for themselves,” added Prof Chan.
Toh, who served as AfA’s Executive Director from 2007-2009, concurs.
“Actually, not many people know this, but MOH has been quite supportive of AfA over the years. Even during my term, they would hold closed-door discussions with us, intently wanting to work with us on eliminating HIV/AIDS,” said Toh. He reckoned that MOH did not want to be publicly seen as supporting something considered by society as ‘morally corrupt’ no matter how beneficial it is to wider society.
The Fruits of Our Predecessors’ Labour Are Not Handed on a Silver Plate
The history of HIV/AIDS and its role in fomenting community-building among the LGBTQ+ community has always been a topic of fascination for me.
I can only imagine what it must have been like to see everyone in your social circles and communities succumbing, one by one, to an unknown disease.
Covid-19 provided the closest representation of the tumultuous and uncertain time in the ’80s.
In the midst of writing this, however, the comparison became a much closer one. Monkeypox is now affecting men who have sex with men more than the rest of the general population.
“It’s not the same thing,” Chan said, cautioning against making blanket comparisons between monkeypox and HIV/AIDS.
“For starters,” he intoned, “monkeypox is not an unknown disease. We’ve known about monkeypox for decades, so it is nothing close to HIV back in the ’80s.”
Admittedly, life is easier for a gay man like me, who came of age at a time when HIV/AIDS is no longer considered a significant threat.
With common knowledge of medication as well as preventative measures like safer sex and pre and post-exposure prophylaxis (PrEP and PEP), it is easy for me and my peers to take for granted the freedoms that we now enjoy, thanks to decades of advocacy and destigmatisation.
But as Prof Chan said, “It is important not to be complacent. The freedoms and advancements we have today were not handed on a silver platter. Earlier generations had to fight very hard for all of these things.”
172 notes
·
View notes
Text
One thing I want to add to this is that to "get around" paying for coverage, HDHP plans are becoming more prevalent. They won't cover a lot of Medical costs until you hit your deductible regardless if you have a copay. And even a small (under 5K) deductible can be difficult for a family or individual to afford/meet. What they want you to do is get a HSA (those are fine but have rules) or an FSA (these have some *extra* shenanigans) to pay for your healthcare until you hit that deductible. So, y'know, yes you have coverage and can't be denied/kicked off your plan for existing but it's can be a bitch and a half to get health insurance to actually pay for shit.
That said: the ACA was the right move. We need it. We need it expanded. We need the same kind of health coverage as places like Norway and Sweden.
One thing the analysts back in 2012 were right about is that they’d stop calling it “Obamacare” the second it started working and lo and behold anytime it was actually threatened under Trump it became The ACA and now Leftists who were in Kindergarten when the ACA was passed think Democrats have added nothing to this country.
#The ACA also now has mandatory coverage for HIV/AIDS antiretroviral therapy (ART - the maintenance drugs you may have heard about!)#Remember when these were price gouged bc they were 'high demand'? ACA swiftly made coverage mandatory after that snafu#But in all honesty a lot of this mandatory coverage is the result of years of behind the scenes tireless work!#ACA also covers cancer care! SO much cancer care that I am a necessary expert for my analyst team to teach cancer etiology + coding#ACA is also a generally 'zero sum game'#Meaning insurers can't use this as a profit center. There are multiple audits a year to confirm patient population 'sickness'#we need single payer healthcare
18K notes
·
View notes
Text
Also preserved in our archive
HIV/AIDS & COVID-19, particularly long COVID, share several significant similarities, especially in terms of viral persistence, T cell damage, immune system dysfunction, & activation of other pathogens. These parallels are important for understanding the long-term effects of both infections and their impact on the immune system.
1. Viral Persistence
Both HIV & SARS-CoV-2 can persist in the body, leading to chronic symptoms & immune system complications. In HIV, the virus establishes reservoirs in various tissues, allowing it to evade immune detection and antiretroviral therapy (ART), leading to lifelong infection. Similarly, recent studies at Brigham and Women’s Hospital suggest that a subset of people with long COVID may harbor persistent SARS-CoV-2 proteins in their blood, potentially explaining ongoing symptoms months after the acute infection has resolved[4][10]. This viral persistence is thought to drive chronic inflammation and immune dysfunction in both.
In long COVID, viral reservoirs have been identified in multiple organs, including the gut, blood, & nervous system[12]. This mirrors HIV's ability to persist in tissue reservoirs such as lymphoid tissues. For both viruses, this persistence can lead to prolonged immune activation & may contribute to ongoing symptoms like fatigue, cognitive issues, & cardiovascular problems.
2. T Cell Damage & Exhaustion
Both HIV and SARS-CoV-2 cause significant damage to T cells, particularly CD4+ T cells. In HIV infection, CD4+ T cells are directly targeted by the virus, leading to their depletion over time and resulting in severe immunodeficiency if untreated. Similarly, severe COVID-19 has been associated with a reduction in CD4+ T cells due to excessive immune activation and exhaustion[1][2]. In both, CD8+ T cells also become dysfunctional due to chronic exposure to viral antigens.
T cell exhaustion is a common feature in both infections. In HIV, chronic infection leads to high levels of inhibitory receptors like PD-1 on T cells, contributing to their reduced functionality[2]. In severe COVID-19 cases, similar markers of T cell exhaustion (e.g., PD-1 and TIM-3) are observed[1]. This exhaustion impairs the body's ability to clear the virus effectively and contributes to prolonged illness.
3. Immune System Dysfunction
Both HIV/AIDS & long COVID can lead to profound immune system dysfunction. In HIV infection, even with effective ART, individuals often experience chronic immune activation and systemic inflammation due to incomplete immune recovery[6][9]. This persistent immune activation is linked to increased susceptibility to other infections and long-term health complications.
Similarly, long COVID is believed to involve ongoing immune dysregulation even after the acute phase of SARS-CoV-2 infection has passed. Some studies suggest that persistent viral proteins may continue stimulating the immune system, leading to chronic inflammation[4][12]. This ongoing immune activation may explain why some individuals experience prolonged symptoms such as fatigue, brain fog, or cardiovascular issues even after clearing the virus from most tissues.
4. Activation of Other Pathogens
Both HIV/AIDS and long COVID are associated with the reactivation of latent pathogens due to weakened immune surveillance. In people living with HIV (PLWH), co-infections with viruses like Epstein-Barr virus (EBV) or cytomegalovirus (CMV) are common due to compromised immunity[7]. Similarly, studies have shown that reactivation of latent viruses such as EBV may contribute to long COVID symptoms[7]
In both conditions, the weakened immune system's inability to control these latent infections can exacerbate symptoms and complicate recovery. For example, EBV reactivation has been linked with neurocognitive symptoms in long COVID patients[7], while opportunistic infections such as Pneumocystis jirovecii pneumonia are common in advanced HIV/AIDS patients[3]
So, HIV/AIDS and long COVID share several key similarities regarding viral persistence, T cell damage, immune system dysfunction, and the reactivation of other pathogens. These shared features highlight the importance of understanding how chronic viral infections can lead to long-term health consequences through mechanisms like persistent viral reservoirs and ongoing immune activation. Insights from HIV research may help inform treatment strategies for long COVID, especially in targeting viral persistence with antiviral therapies or addressing chronic immune dysfunction.
Sources
[1] SARS-CoV-2 and HIV-1: So Different yet so Alike. Immune ... pmc.ncbi.nlm.nih.gov/articles/PMC9608044/
[2] Sharing CD4+ T Cell Loss: When COVID-19 and HIV Collide on ... www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2020.596631/full
[3] Overview of SARS-CoV-2 infection in adults living with HIV www.thelancet.com/journals/lanhiv/article/PIIS2352-3018(21)00070-9/fulltext
[4] Study Finds Persistent Infection Could Explain Long COVID in Some ... www.massgeneralbrigham.org/en/about/newsroom/press-releases/study-finds-persistent-infection-could-explain-long-covid-in-some-people
[5] New COVID studies show varied viral clearance time in patients with ... www.cidrap.umn.edu/covid-19/new-covid-studies-show-varied-viral-clearance-time-patients-lower-immunity
[6] Immunologic Interplay Between HIV/AIDS and COVID-19 link.springer.com/article/10.1007/s11904-023-00647-z
[7] Long COVID in people living with HIV - PMC - PubMed Central pmc.ncbi.nlm.nih.gov/articles/PMC10167544/
[8] Persistence and Evolution of SARS-CoV-2 in an ... - NCBI www.ncbi.nlm.nih.gov/pmc/articles/PMC7673303/
[9] The immune response to SARS-CoV-2 in people with HIV - Nature www.nature.com/articles/s41423-023-01087-w
[10] Persistent infection could explain long COVID in some people, study ... www.sciencedaily.com/releases/2024/10/241009122346.htm
[11] Plasma-based antigen persistence in the post-acute phase of ... www.thelancet.com/journals/laninf/article/PIIS1473-3099(24)00211-1/fulltext
[12] Long Covid trials aim to clear lingering virus—and help patients in ... www.science.org/content/article/long-covid-trials-aim-clear-lingering-virus-help-patients-need
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#hiv/aids#HIV#Aids#aids crisis#long covid#covidー19#covid conscious#covid is airborne#covid isn't over#covid pandemic#covid19#get vaccinated
108 notes
·
View notes
Text
Love in the big city and HIV
So, I have recently watched one of the best dramas of the year, “Love in the big city”, in which HIV is a major theme.
The show portrays really well the stigmatized scenario around HIV: as a person living with the virus, Go Young feels exactly as if he's carrying some kind of curse. He can't accept it, but who can blame him for that, if "Kylie", as he calls the virus, is always around like an inconvenient person? In his sex life, while applying to a job, and even while hanging out with friends.
Society doesn't make it easy for a person living with HIV to accept the condition and that's essential when it comes to healthcare, which is what I want to address today.
First, let me introduce myself: my name is Nico and I'm a Medicine student in Brazil. Here, we have probably one of the biggest public health system in the world, the Unified Health System (a.k.a. SUS). In this essay, I intend to share some general information about HIV, its treatment and prevention, by using some parts of “Love in the big city” to discuss this theme, because although the show did an amazing job when it comes to talking about it, there are some points I found needed some better explanation.
HIV is a sexually transmitted infection (STI) that can also be transmitted by the contact with infected blood (e.g: incompatible blood transfusion; use of shared needles) or from the mother to a child inside the womb or during labor. The virus uses a specific type of immune cell to multiply. Explaining it in a very simple way, he gets inside the cell, uses its components to produce new viral copies and then ruptures the cell membrane to release these new copies in the blood, killing the cell by doing so. For this reason, untreated HIV is very dangerous, since it can cause immunodeficiency (failure of the immune system), making the person susceptible to acquire opportunistic infections, which are diseases that usually don’t occur in people with regular immune systems. When someone has immunodeficiency caused by HIV, this person is diagnosed with Acquired ImmunoDeficiency Syndrome (AIDS). That being said, AIDS and HIV are not the same. There are many people living with HIV that don’t have AIDS, thanks to appropriate treatment.
There are multiple ways a person can discover about having HIV: you can be notified because the person you have had relations with discovered the infection, or by taking blood tests for blood donation, or in the worst case scenario, when you are already suffering from an opportunistic infection. Go Young, for example, discovered it because of the blood tests results while he was in the army. One thing I found very outrageous was that the physician instantly inferred that Go Young was gay because of that, but this is impossible, since anyone can get the virus, regardless of their sexual orientation. This appointment was like a death sentence: the unempathetic doctor as a ruthless judge, blaming the patient and not offering a single word of comfort. (Quite the opposite: he even asked that very intimate question about sex positions. Seriously, I wanted to punch this doctor so hard.)


Nonetheless, even if it was made in a very inappropriate way, diagnosis is still very important, because that is the only way one can have access to treatment. Each patient must be evaluated separately, since treatment may vary due to the different genetic subtypes of the virus and the person’s own body response. Medication can also be adjusted until satisfactory results are accomplished. Overall, all patients are submitted to a lifetime antiretroviral therapy in order to stop the virus from multiplying and to keep immune cells at a higher level. In the series, we can see Go Young asking for any antiretroviral in a pharmacy, but in real life, he would be very specific about the drugs.

If done properly, treatment can provide quality of life and long life expectancy (very similar to people who don’t have HIV), prevent opportunistic infections and, most importantly, transmission! Yes, that is exactly what you read: treatment can result in really low levels of HIV in the blood, which is called “undetectable viral load” if it happens for at least six months. There is even a saying which goes “Undetectable = untransmittable”. In this scenario the patient can even have sex without a condom with their partner, which is what happened with Go Young and Gyu Ho in the series. However, it is important to mention that this only applies to HIV: one can still get other STIs while having unprotected sex.


In addition to condoms and proper treatment, there are other ways of preventing HIV infection. Susceptible people can use the pre-exposure prophylaxis (PREp) medication, which highly reduces the risk of getting HIV from intercourse (and also from blood contact in a less effective way). There is also the post-exposure prophylaxis (PEP), which can prevent infection if taken within 72 hours after possible exposure. Treating other STIs, not sharing needles, using lubricant (less chance of injury during intercourse) and avoiding sex while in use of alcohol or drugs are some other habits we can do ourselves to minimize the risk of acquiring HIV.
Nevertheless, individual actions can help only until a certain point, given that the best prevention is the “combination prevention”, which includes not only behavioral and biomedical approaches, but also structural interventions. Every country should have their own public policies to assist people living with HIV and to prevent transmission. I’m proud to say that, in Brazil, thanks to our public health system, everyone has access to condoms, lubricants, tests, treatment, PREp and PEP - all free of charge. The system also has policies of damage control, providing all of these strategies to the population of risk, such as sex workers and people with a substance use disorder, including kits with individual needles to prevent sharing and, consequently, blood transmission. No wonder we are an international reference for HIV/AIDS treatment and prevention.
To conclude, I also need to remind you that you can actively help in this cause by simply showing support. As we all watched in “Love in the big city”, a person living with HIV faces all kinds of prejudice in society. Go Young carried a heavy burden for years, not being able to share it with anyone until Gyu Ho embraced him. Sometimes, patients have these prejudices themselves and it can deeply hinder treatment. I have seen this myself: a patient that denied the diagnosis and returned to the hospital sometime later with a severe health condition.
You can be the person that will accept and embrace this other person, who is only living with a chronic condition, such as many people who live with hypertension or diabetes, for example. You can be the person that will call out on others for their preconceived opinions. You can be the person who will share high-quality information to your friends, family, fellow workers or students (There are links in the last paragraph with reliable information for those who want to do some further research).
Finally, I can’t stress enough how much I loved “Love in the big city” for addressing so many types of love and so many sensitive topics, including this one, in such a beautiful way. It has been a long time since I had felt so connected to a story, to a character so human like Go Young.
I hope this essay provided a little bit of information to you. I mostly used the knowledge I have learned in college and sites of well-recognized organizations, such as the UNAIDS, the World Health Organization (WHO) and, for the Portuguese speakers, the Brazilian Ministry of Health (Ministério da Saúde). Thank you for reading, and please, feel free to send me any questions you might have, I’ll do my best to answer them. Also, if you notice any English mistakes, please let me know so I can correct them.
#love in the big city#HIV#aids#health and wellness#healthcare#medicine#SUS#Unified health system#Sistema único de saúde#Viva o SUS#Proteja o SUS#go young#gyu ho
80 notes
·
View notes
Text
"Five people have gone into remission thanks to advancements in medicine — and a sixth patient may also now be free of HIV.
One of the biggest breakthroughs in HIV/AIDS prevention in recent years is the widespread use of PrEP (pre-exposure prophylaxis).
This drug therapy, approved by the Federal Drug Administration in 2012, has been a key player in preventing HIV transmission through sex or injection drug use. Antiretroviral drugs, such as PrEP, also slow the replication of the virus and prevent it from progressing to AIDS.
Although PrEP has become a more accessible treatment for the virus, scientists have been hurriedly working towards cures for HIV for decades — and we’re finally seeing some results.
In February of this year, scientists in Germany confirmed a fifth-ever patient had been cured of HIV after receiving stem cell transplants that include genetic mutations that carry a resistance to HIV.
But it looks like a sixth patient may soon be able to join this very exclusive club.
The man, referred to as the “Geneva patient,” underwent a stem cell transplant after cancer treatment, though these cells did not include the HIV-resistant genetic mutation.
Still, he went off antiretroviral therapy for HIV in November 2021, and his viral load remains undetectable.
Instead, doctors are researching whether a drug called ruxolitinib may be partially responsible for his recovery.
Ruxolitinib decreases inflammation associated with HIV by blocking two proteins, JAK1 and JAK2. This helps kill off “reservoir cells” that lay dormant in the body and have a potential to cause rebounds in patients with HIV.
Experts say the AIDS crisis can end by 2030 across the globe — as long as leaders prioritize this goal.
A new report from UNAIDS shows a clear, optimistic path to ending the AIDS crisis. (This looks like a 90% reduction in cases by 2030.)
The organization’s report includes data and case studies that show that ending AIDS is a political and financial choice — and that governments that have prioritized a path towards progress are seeing extraordinary results.
By following the data, science, and evidence; tackling inequality; and ensuring sufficient and sustainable funding across communities, the global community could wipe out the AIDS pandemic by the end of the decade.
The report demonstrates that progress has been strongest in the countries and regions that have the most financial investments, like eastern and southern Africa, where new HIV infections have been reduced by 57% since 2010.
Investments in treatments, education, and access to care have also led to a 58% reduction in new HIV infections among children from 2010 to 2022 — the lowest number since the 1980’s.
Plus, the number of people on antiretroviral treatment around the globe has risen from 7.7 million in 2010 to 29.8 million in 2022.
The moral of the story? This goal can be achieved, if world leaders put their minds — and wallets — to it.
A region in Australia might be the first place in the world to reach the United Nations targets for ending HIV transmission.
Researchers believe that the central district of Sydney, Australia is close to becoming the first locality in the world to reach the UN’s target for ending transmission of HIV.
Specifically, new infections among gay men have fallen by 88% between 2010 and 2022. In fact, there were only 11 new HIV cases recorded in central Sydney last year, and almost all HIV-positive Australians are on antiretroviral drugs.
... "These numbers show us that virtual elimination of HIV transmissions is possible. Now, we need to look closely at what has worked in Sydney, and adapt it for other cities and regions across Australia.”
Namibia is ahead of schedule in UN targets to end HIV/AIDS.
Although the virus is still the leading cause of death in Namibia, the country is well on track to hit 95-95-95 UNAIDS targets before its 2030 deadline.
In Namibia, 92% of people know their HIV status, 99% of people living with HIV are on treatment, and 94% of people living with HIV who are on treatment are virally suppressed.
In addition to these exciting statistics, new infections have plummeted. The estimated rate of new HIV infections in Namibia is five times lower than it was in 2002, according to the Centers for Disease Control & Prevention.
These encouraging numbers are thanks to the investment and strategic response of PEPFAR, but also to the willingness of local governmental agencies and organizations to adhere to the UN’s Fast-Track approach.
Breakthroughs are being made in HIV vaccine therapies.
Long before we were all asking each other “Pfizer or Moderna?” about our COVID-19 vaccines, scientists have been researching the potential of mRNA vaccines in treating some of the world’s deadliest diseases — like HIV.
And with the success of our mainstream mRNA vaccines, an HIV inoculation remains a goal for researchers across the globe.
Last year, the National Institutes of Health launched a clinical trial of three mRNA vaccines for HIV, and similar studies are being conducted in Rwanda and South Africa, as well.
CAR T-cell clinical trials are underway to potentially cure HIV.
This spring, UC Davis Health researchers have dosed the second participant in their clinical trial, which poses the use of CAR T-cell therapy as a potential cure for HIV.
The study involves taking a participant’s own white blood cells (called T-cells), and modifying them so they can identify and target HIV cells, ultimately controlling the virus without medication.
The first participant in the study was dosed with anti-HIV T-cells last August, and the trial is the first of its kind to utilize this technology to potentially treat HIV.
Of course, the trials have a long way to go, and the lab is still preparing to dose a third participant for the study, but CAR T-cell treatments have been successful for lupus and forms of cancer in the past...
“So far, there have been no adverse events observed that were related to the treatment, and the two participants are doing fine.”
Guidance on how to reduce stigma and discrimination due to HIV/AIDS is reaching people around the globe.
While the stigma surrounding HIV and AIDS has significantly decreased — especially towards the LGBTQ+ community — with advancements in treatment and prevention, discrimination is certainly not gone.
While most people now understand HIV/AIDS better than they did decades ago, those most impacted by the virus (like gay men and low-income women and children) still face ongoing barriers to care and economic security.
It is vital to maintain awareness and education interventions.
After all, experts suggest that eliminating discrimination and stigma are key factors in reducing disease. And not eliminating stigma impedes HIV services, argues UNAIDS, “limiting access to and acceptance of prevention services, engagement in care, and adherence to antiretroviral therapy.”
Luckily, UNAIDS provides guidance on how to reduce stigma and discrimination in the community, workplace, education, health care, justice, and emergency settings.
The goal is to, of course, decrease stigma in order to decrease disease, but also to provide folks with the culturally significant support they need to live safe, integrated lives — with or without disease.
For instance, a 2022 study conducted in Northern Uganda showed that local cultural knowledge passed through Elders was a successful intervention in reducing HIV-related stigma among young people.
“Research in school settings has shown that the use of local cultural stories, songs, myths, riddles, and proverbs increases resilient coping responses among students and strengthens positive and socially accepted morals and values,” the study’s discussion reads.
So, while an uptick in acceptance gives us hope, it also gives us a directive: Keep telling the accurate, full, and human stories behind HIV/AIDS, and we’ll all be better for it. "
-via GoodGoodGood, August 3, 2023
#hiv#hiv/aids#aids crisis#public health#medical research#vaccines#australia#namibia#united nations#queer issues#trans issues#lgbtq issues#lgbtq community#infection prevention#good news#hope
273 notes
·
View notes
Text
in relation to the last reblog, some things about HIV. (it's not really a proper educational post (tm) just some facts and misconceptions that i wanna bring so please do your own research if you're able).
HIV is transmitted through blood and sex.
HIV is NOT transmitted through air, saliva, common dishes, household items, etc.
PrEP = pre-exposure prophylaxis. treatment that you get if you regularly participate in risky activities to prevent getting HIV. if you regularly participate in risky activities (share syringes with someone, have unprotected sex), you may consider using PrEP. YOU NEED TO BE HIV- TO USE PrEP!! usage of PrEP if you've already got HIV is dangerous! HIV may develop resistance to the anti-retroviral drug you intake for PrEP, and it can make treatment more difficult!
PEP = post-exposure prophylaxis. treatment that you get as an emergency if you get at risk suddenly (had unprotected sex with someone whose status you don't know, were sexually assaulted, don't remember whether you used condoms or not, condom slipped/teared, shared syringe with someone, etc). it is an EMERGENCY MEASURE that couldn't be used on a regular basis. if you're exposed at risk on a regular basis, consider using PrEP.
PEP needs to be started NO LATER THAN IN 72 HOURS after exposure. the earlier you start, the higher the effectiveness is.
what does it mean: after exposure, you'll have HOURS to contact with medical provider/center/place where you can get PEP and start treatment. so it's better to research opportunities beforehand. maybe get a supply, if it's legal. but at least you need to find a place where to go in emergency case.
the most risky activities are: usage of same syringe for injections, unprotected sex with contact of genitalia and anal, sexual assault (PEP is recommended). consencual oral sex has very very very low risks (PEP is not recommended). anyways, if you think you have been exposed at risk, you should contact your medical provider or centers that specialize in HIV prophylaxis and treatment. it's better to contact in any doubts.
idk how it works in other countries, but where i live we have (some) HIV/AIDS centers where people can get tested, get PrEP, PEP, and help with access to antiretroviral treatment. places that you can research: HIV/AIDS centers, planned parenthood, reproductive clinics, queer-specialized places, etc.
HIV IS NOT ADDICTS-ONLY DISEASE. HIV IS NOT QUEER-ONLY DISEASE. HIV IS NOT MARGINALIZED PEOPLE-ONLY DISEASE. marginalized groups have their risks because of stigma, ostracization, medical neglect, etc. BUT no one is immune to HIV. A LOT OF, and i mean it, generally privileged people get and transmit HIV because they're sure they will never get it.
there are MORE THAN ONE HIV STRAIN. and you can get more than one HIV strain. so if you're living with HIV and going to have risky activity with someone living with HIV and you've not gotten it one from another, YOU STILL NEED PROTECTION. (if you both don't have undetectable viral load).
UNDETECTABLE = UNTRANSMITTABLE. if someone lives with HIV and has undetectable viral load, they can't transmit HIV to someone else. which means you can have unprotected sex with them (if you all don't have other STDs), they can give birth and don't transmit HIV to the children, etc.
HIV IS NOT THE ONLY STD. there are others, and their transmission differs from HIV transmission. for example, oral sex is risky for gonorrhea. so DON'T NEGLECT CONDOMS!
HIV and STDs are not the worst things in the world. most STDs are either curable or controllable, and you can live fine with them. and anyways, no disease should be stigmatized.
HIV and STDs aren't dirty. thinking that "only dirty shameless people can get HIV/STD" is a) discriminatory; b) factually incorrect - everyone can get STDs; c) prevents people from getting tests and treatment; d) promotes the spread and evolution of STDs.
anti-retroviral therapy may be expensive/inaccessible in lots of places. research the situation where you live and your opportunities in case you'll need HIV-associated treatment (PrEP, PEP, anti-retroviral treatment).
people who know that they have HIV are not the "dangerous" ones. the "dangerous" ones are people who have never gotten tested, who are sure that HIV is not something that they can get, and who ask you to have a sex without a condom.
i'm sorry if i say obvious things here, but i'm not sure about public awareness around HIV and thought that if someone can be surprised that person living with HIV can have children without HIV, then these things should be articulated.
10 notes
·
View notes
Text


World AIDs Day - December 1st.
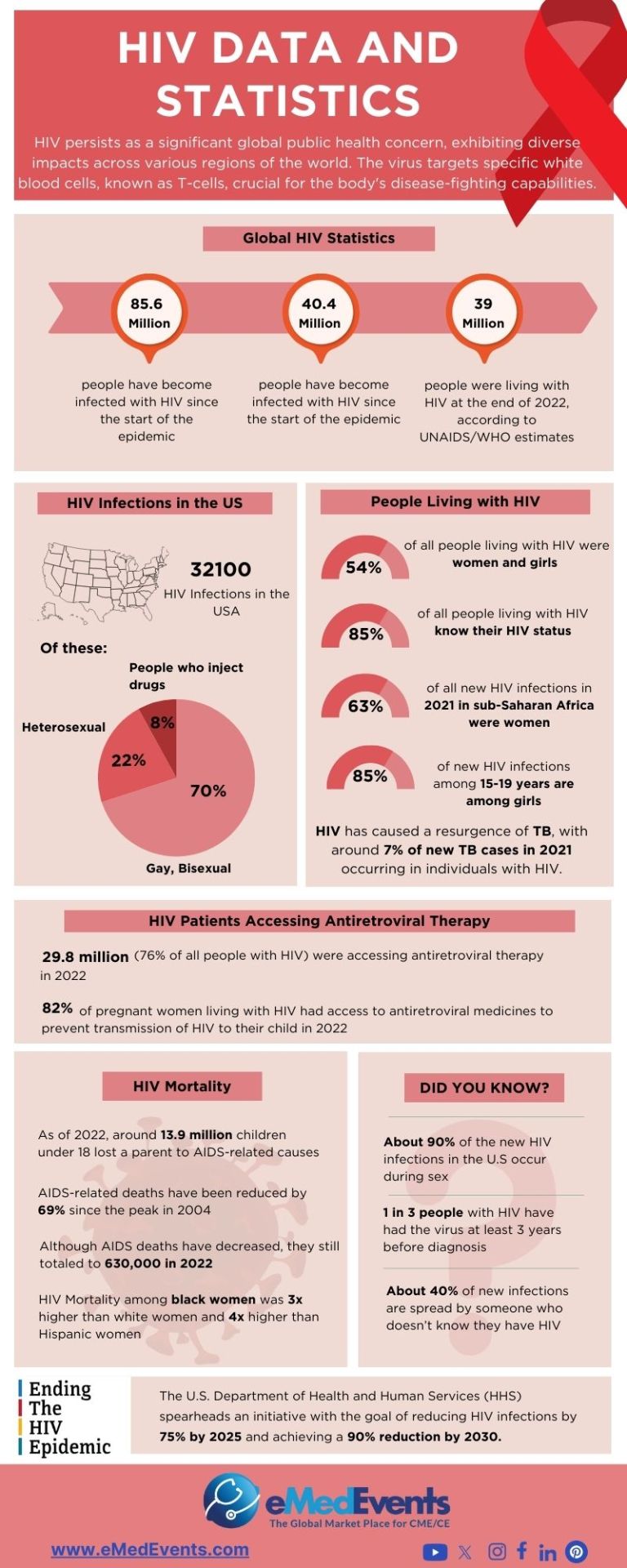
Global HIV statistics
🎀 38.4 million [33.9 million–43.8 million] people globally were living with HIV in 2021.
🎀 1.5 million [1.1 million–2.0 million] people became newly infected with HIV in 2021.
🎀 650 000 [510 000–860 000] people died from AIDS-related illnesses in 2021.
🎀 28.7 million people were accessing antiretroviral therapy in 2021.
🎀 84.2 million [64.0 million–113.0 million] people have become infected with HIV since the start of the epidemic.
🎀 40.1 million [33.6 million–48.6million] people have died from AIDS-related illnesses since the start of the epidemic.
╔═.✵.══════════╗
🄼🅈 🄻🄸🄽🄺🅂
╚══════════.✵.═╝
56 notes
·
View notes
Text

A sombre shot of Sam Reid and John Leary as Dale Jennings and Murray Gallagher from No More Lies, as well as some others ❤️
.
.


Next Thursday, it will have been three years since No More Lies first went to air on the ABC. It’s a funny feeling, seeing all these Season One episodes reach their third year anniversaries, as I have such strong vivid memories of watching this show as it first aired, whilst we were in lockdown. It truly doesn’t feel like that long ago, but according to time and mathematics, it is.


No More Lies really did strike a nerve. It’s brilliantly brave and searing storytelling around the plight of HIV and AIDS affected people and how the media represented - or rather, misrepresented - their stories and circumstances. This is why I love The Newsreader so dearly. It hasn’t portrayed the 1980s through rose-coloured glasses, and has sought to elevate the stories and perspectives that were either misrepresented or not represented at all during the time. It also demonstrates how easy it is to fall for misinformation, and I genuinely believe that this episode is a great lesson in media literacy. The whole show itself, but in particular this episode, should be used in schools and universities.


A part of my paternal family history is my Dad’s younger brother, who was a young gay man who contracted HIV during the 1990s. This was the decade in which medical treatment and antiretroviral therapies became available to significantly prolong the progression of the virus to AIDS in HIV-affected patients. He was thankfully able to benefit from these therapies and medications, which bought him two decades of life, longer than our Russ and Caroline would have lived for.


We sadly lost my paternal uncle Christmas 2012, when he was only forty years old. Through watching this episode with my Dad, it gave me the courage and the instigator for a discussion about my uncle’s condition, how people responded to it, and how it impacted his life. I’ll forever be grateful to No More Lies, and especially to Michael Lucas and Kim Ho, for giving me the opportunity to have this discussion with my Dad, which I had been hesitant to have for at that point nine years. Never underestimate the power of good media and the conversations and connections it can bring about. 💖🌟
#dale jennings#sam reid#murray gallagher#john leary#helen norville#anna torv#noelene kim#michelle lim davidson#adam lindell#tim draxl#russ the newsreader#geoff walters#robert taylor#rob rickards#stephen peacocke#caroline gibson#alexandra schepisi#the newsreader#nas1986 s1 story a day
12 notes
·
View notes
Text
Brazil sees rise in HIV cases, but lowest mortality since 2013

In 2023, Brazil recorded a 4.5 percent growth in the number of HIV cases compared to 2022. In the same time frame, however, the mortality rate fell to 3.9 deaths, the lowest in the last ten years, as per official data released Thursday (Dec. 12).
A total of 38 thousand cases of the disease were recorded last year. The majority were registered among men—around 27 thousand. In terms of age, the most cases were registered among people aged from 25 to 29. AIDS-related deaths totaled 10,338 in 2023, the lowest since 2013.
The increase in the number of registered cases, the Ministry of Health reported, is related to the expansion of the supply of pre-exposure prophylaxis (PrEP), since testing is required for anyone interested in taking it. As a result, more people infected with HIV were detected and immediately included in antiretroviral therapy.
“The challenge now is to re-engage people who stopped treatment or were neglected—many of them during the last government—as well as to make treatment available to all newly diagnosed people, so they can have a higher quality of life,” the ministry says in a statement.
Continue reading.
#brazil#brazilian politics#politics#hiv aids#healthcare#epidemiology#image description in alt#mod nise da silveira
2 notes
·
View notes
Text
The Immunology In Africa Podcast: Science in The Pursuit Of Health

Podcasting has long tendrils that can wrap itself around topics, events, issues, and questions that evade other format -- TV, film, radio, even books -- because the target audience either large enough or considered significant to cover.
How about immunology on the African continent?
Welath Okrete has taken on that challenge. The Immunology in Africa Podcast focuses on science communication in immunology & related research — spotlighting Africa & amplifying African stories.
By amplifying the stories, struggles, and successes of Africans researching the immune system, ImmunoAfrica creates a platform for scientists, up-and-coming researchers, and members of the public to explore the immune system collectively.
In a recent article on Medium, Okrete wrote: "I embraced the idea to launch a podcast in 2021 out of sheer curiosity. I wanted to learn about African immunology — about local African scientists and their contributions to the rapidly evolving global field of immunology. However, I didn’t want to do so by just reading long, complex journal articles. While I felt it’d be super cool to directly hear these scientists talk about their work, I couldn’t find any audio platform to tune in to. Podcasting had become a thing then, so I thought it wouldn’t be a bad idea to start one — but I wasn’t particularly excited about doing so. Here’s why."
Wealth Okrete has a bachelor's degree in Biochemistry from the University of Benin, Nigeria, where, he shares, "my interest in immunology, infectious diseases, and vaccines first ignited."
Okrete continues: "I got into science communication as a writer, mainly because I considered writing a convenient route to expressing my ideas. Podcasting, however, was inconvenient — it would entail forcing myself out of my little, cozy shell into a larger, unfamiliar sphere. The challenge it presented was also different — I didn’t think I had what it would take to host an immunology podcast. So, I reached out to Julius Wesche to learn the ropes — and a few weeks later, on January 28, 2022, he would school me on the tools, dos, and don’ts of podcasting."
As of August 1, 2024, the podcast is two years old.

Okrete comments: "Over this time frame, I have been awed by the invaluable contributions of African immunologists to making the continent and the world a healthier place. I have spoken with professors, postdocs, and PhD students, exploring topics from how HIV/ART (antiretroviral therapy) disrupts immune function in infants born to women living with HIV to why Africans tend to generate weaker immune responses to routine vaccines. Guests on the podcast have shared insights into a wide range of diseases, including neurocysticercosis, tuberculosis, cancer, Lassa fever, and alpha-gal allergy. And with their help and our team of volunteers, ImmunoAfrica has spread ‘the gospel of African immunology’ across more than 50 countries, in just 2 years.
I started an immunology podcast because I had a keen interest in the field," says Okrete. "That interest, alongside the science communication experience I had gained overtime, became my comfort zone. Even if you don’t fully agree with my idea of a comfort zone, my point is to always think of how the skills, experiences, or networks within your reach can facilitate your flight into new terrains."
For aspirational podcasters, Okrete advises: "Think of how the skills, experiences, or networks within your reach can facilitate your flight into new terrains. Plan and stay organized."
Admittedly, the episodes are scientific in nature, but educational about the efforts made in Africa to combat disease.
For example, in the July 8th show, Dr. Ousmane Traoré is an immunology and parasitology researcher currently working as Laboratory Manager at the Clinical Research Unit of Nanoro (CRUN / URCN) in Burkina Faso. He was a key figure in several malaria vaccine trials, including the phase II and III trials for R21/Matrix-M and the phase II trial for RH5/Matrix-M.
On the December 2023 episode, Kumba Seddu, who started her PhD journey at Johns Hopkins University, investigates male and female immune differences to viral vaccines and infections. Her research added to the growing evidence that vaccinated females have greater antibody responses than males. This increased vaccine-induced antibody response in females is due to hormonal (estrogen) effects and sex chromosome (XX) effects.
I also recommend listening to Tony Doe's superb Into The Podverse about podcasting in Africa, and the opportunities and challenges on the continent. Tony is a podcasting veteran who is definitely ear worthy for people on all continents.
Get a taste of the podcast via the trailer. As a host, Wealth Okrete is articulate, passionate, and knowledgeable about his topic.
Check out The Immunology in Africa podcast. I know the science may be arcane to many, but the narrative about the Herculean efforts by scientists and others to improve the health of millions of African citizens is a story too positive to pass up.
This review is part of an ongoing series of reviews, recommendations, and essays about Indie podcasters -- their craft, their challenges, and the critical role they play in podcasting. These entrepreneurs display skills as disparate as hosting, sound production, graphic design, scriptwriting, interviewing, marketing genius, and financial watchdog. They are the heart and soul of podcasting.
2 notes
·
View notes