#Substance Use Disorders
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There are dozens of funny blogs to kill time on Tumblr.
Note
TW for drug usage + medical ableism
While I was looking through the disability tags I saw a couple of posts talking about people being denied their medications over assumptions that they’ll use it for recreational purposes. Idk how common this is because I’m not currently on any meds but there were multiple posts with a lot of notes so I presume it’s not rare.
So here’s my problem: one of my characters has a history of substance abuse during their backstory (the addiction is at their lowest point), and a bit before the actual beginning of the story they start the path to recovery. Part of this recovery is of course getting sober, but part of it is also getting support for dealing with their disabilities (idk if it matters but they’re a mix of physical and psychological) and some of that help comes in the form of getting medicated. Because these are both pretty big things for the character so get mentioned a lot, and because they happen in like the same segment of the story, I’m worried that it may give the impression that the character is taking the medication to use recreationally to readers, which isn’t a stereotype I want to employ at all. Do you guys think this could be a problem?
Hello,
Keep in mind that if he has a history of substance abuse disorder, his doctors are going to know that and probably will not put him on a Schedule 2 medications. Depending on where he is in his recovery, they might play it safe and avoid Schedule 3, too, or at least Schedule 3 medications that are related to what he was previously addicted to. Schedule 4 and Schedule 5 should be safe. So I would recommend finding lower-schedule medications for the conditions he has and learning about those. They won't be as powerful as things with a higher chance for addiction and there will be a huge difference in what his day will be like if he takes ibuprofen for pain versus morphine.
But really, if you show him taking his medication responsibly and describe how it helps because of how bad his symptoms are without it, it likely won't give the wrong impression. It's not like he would be randomly pulling a random Vicodin out of his pocket and taking a pill whenever he feels like it, he would take his medications at certain times, with certain amounts of time between doses, or in extreme circumstances like taking something for a panic attack. If you write him using his medications as he should and being careful (in my experience, usually a bit overly careful because he really wouldn't want to go through substance abuse all over again,) you won't have a problem. Writing about him using medication responsibly won't look like him recreationally abusing substances. I think you should be fine.
If you have any questions about using medication with a history of substance abuse, feel free to send an ask!
Mod Aaron
58 notes
·
View notes
Text
U.S. Senators criticized leaked telehealth restriction plans of DEA in a letter to President Biden.
Some senators have sent a letter to President Biden to criticizing the leaked proposed DEA’s plans to restrict telemedicine options, saying “it is vital that any new regulations do not erect barriers to necessary, life-saving care.”
The senators who signed the letter are: Sheldon Whitehouse, Lisa Murkowski, Mark R. Warner, Marsha Blackburn, Peter Welch, Ben Ray Luján, Jeffrey A. Merkley, Ron Wyden, Angus S. King, Jr, Mark Kelly, Martin Heinrich.
If any of them were my senator, I would be writing and thanking them — this is the letter I’m sending to my senators and the White House:
I’m disappointed to hear that the DEA plans to restrict access to telehealth options. Telemedicine is medicine, and I agree with the senators who said: “it is vital that any new regulations do not erect barriers to necessary, life-saving care.” in the October 11, 2024 letter to the White House. Please act in preservation of telehealth prescribing of medicine classed as controlled substances. Mental health conditions and substance use disorders are considered covid risk factors, and many risk factor conditions require the use of controlled prescriptions. https://www.cdc.gov/covid/risk-factors/index.html It’s essential for people who have disabilities, people who have difficulty traveling to in-person appointments, live in rural areas with few options close to home, and those who want or need to avoid preventable exposure to constantly circulating potentially dangerous infectious disease, by having the option of a televisit when no in-person physical examination is needed.
Please feel free to copy or repurpose for your own letters to reps.
More info:
Lawmakers Pan DEA's Leaked Plans for Telehealth — Meanwhile, a third extension of current rules is in the works by Shannon Firth, Washington Correspondent, MedPage Today October 16, 2024
#healthcare#pandemic#public health#government#telemedicine#telehealth#remote#in-person#RTO#rural health#DEA#rulemaking#barriers to healthcare#controlled substances#prescription medications#televisits#mental health conditions#substance use disorders#biden administration
0 notes
Text
When it comes to dealing with substance use disorders, finding effective treatment options is crucial. Psychiatric services in San Antonio, Texas offer a range of interventions, with Medication-Assisted Treatment (MAT) being one of the most effective. MAT combines medications with counseling and behavioral therapies, providing a holistic approach to recovery.
0 notes
Text
Decoding Addiction Treatment: Exploring Drug Rehab and Treatment
Meta-description: The labyrinth of Addiction Treatment can be confounding. Our meticulous exploration illuminates all components of therapy, imparting invaluable wisdom and pragmatic resources. Foreword Embarking on the path of recuperation from substance misuse can seem formidable. This composition, “Decoding Addiction Treatment,” endeavors to navigate you through each phase of this…
View On WordPress
#Addiction#Detoxification#Inpatient#Insurance#Legal Implications#Mental health#Online Resources#Outpatient#Recovery#Relapse#Stigma#Substance use#Substance Use Disorders#Support Systems#Therapy#Treatment
0 notes
Text

Don't like that meme format but I felt like it was a pretty clear way to formalize my thoughts on Catherine Todd discourse
#dc#dc comics#catherine todd#jason todd#red hood#(note that the chart here doesn't say “iq score” but “respect for people with Substance Use Disorder score#btw)
1K notes
·
View notes
Text
i know this won't be available everywhere, but especially if you live in a larger city where a lot of folks are affected by opioid use/addiction, it's a really good idea to ask local pharmacies, and even food banks if they are giving out free narcan (naloxone). this can also be found at certain behavioral health offices as well, my case manager is able to get them for me for free. narcan is a life saving medication that can temporarily halt an opioid (oxycodone, hydrocodone, heroin, fentanyl, codeine, morphine, etc.) overdose while you wait for emergency medical services to arrive.
opioid overdose is distress of the respiratory system, meaning that the person overdosing likely is struggling to, or can't breathe at all. it's very important to watch to see if the person is dealing with labored or shallow breathing.
here the official use guide:
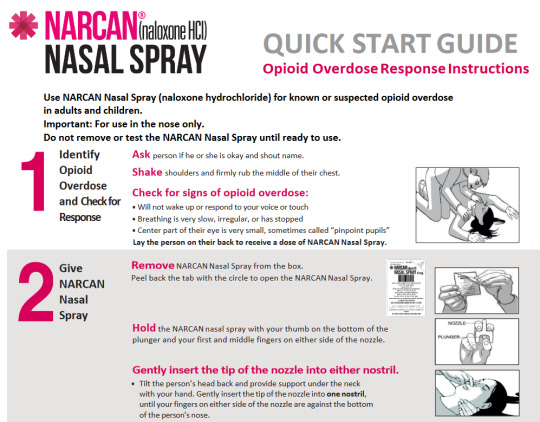
[Image ID start: Two screenshots from the FDA's Narcan (Naloxone HCl) Quick Start Guide infographic. It reads:
"Narcan (Naloxone HCl) Nasal spray quick start guide. Opioid Overdose Response Instructions.
Use NARCAN Nasal Spray (naloxone hydrochloride) for known or suspected opioid overdose in adults and children.
Important: For use in the nose only.
Do not remove or test the NARCAN Nasal Spray until ready to use.
1.) Identify Opioid Overdose and Check for Response Ask the person if they are okay and shout name.
Shake shoulders firmly and rub the middle of their chest.
Check for signs of Opioid Overdose:
Will not wake up or respond to your voice or touch
Breathing is very slow, irregular, or has stopped
Center part of their eye is very small, sometimes called "pinpoint pupils".
Lay the person on their back to receive a dose of NARCAN nasal spray.
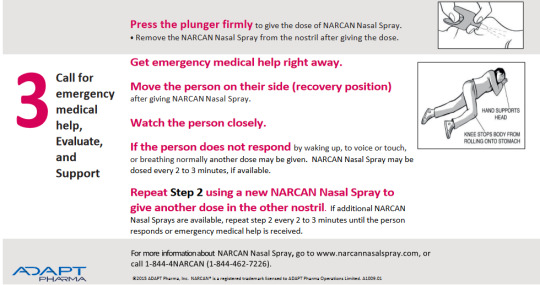
2.) Give NARCAN nasal spray
Remove NARCAN nasal spray from the box. Peel back the tab with the circle to open the NARCAN nasal spray.
Hold the NARCAN nasal spray with your thumb at the bottom of the plunger and your first and middle fingers on either side of the nozzle.
Gently insert the tip of the nozzle into either nostril.
Tilt the person's head back and provide support under the neck with your hand. Gently insert the tip of the nozzel into one nostril, until your fingers on either side of the nozzle are against the bottom of the person's nose.
Press the plunger firmly to give the dose of NARCAN nasal spray.
Remove the NARCAN Nasal Spray from the nostril after giving the dose.
3.) Call for emergency medical help, Evaluate, and Support
Get emergency medical help right away.
Move the person on their side (recovery position) after giving NARCAN Nasal Spray
Watch the person closely.
If the person does not respond by waking up, to voice or touch, or breathing normally another dose may be given. NARCAN Nasal Spray may be dosed every 2 - 3 minutes, if available.
Repeat Step 2 using a new NARCAN Nasal Spray to give another dose in the other nostril. If additional NARCAN Nasal Sprays are available, repeat step 2 every 2 to 3 minutes until he person responds or emergency medical help is received.
For more information about NARCAN Nasal Spray go to www.narcannasalspray.com, or call 1-844-4NARCAN (1-844-462-7226)."
End image ID.]
#cripple punk#crip punk#cpunk#madpunk#mental health#neurodivergent#addiction#substance use#substance use disorder#opioid use#narcan#punk#diy punk#health#resources#mental illness#mental health support#naloxone#our writing#overdose mention#drugs mention#substance addiction
1K notes
·
View notes
Text
For those who have experience with addiction,
*this does not need to mean when it became a fully fledged addiction, just when first became at least a little problematic in your life
#psych disability polls#polls#psychiatric disability#mental illness#neurodivergent#disability#symptoms#age of onset polls#addiction#tw addiction#tw substance abuse#substance use disorder
62 notes
·
View notes
Note
aspd + probably delusional culture is feeling like some kind of substance abuse will fix you (it definitely wont but can't hurt to try right?) (it definitely can but oh well)
aspd-culture-is
#psh this is a mood#hence why ''aspd-culture stop drunkposting'' exists in some tags on here but I try to keep it to just culture asks not questions#in moderation I've found drinking settles the strong desire to do something worse#my therapist would probably not agree with this sentiment but she does believe in harm reduction#tw drvg mention#tw substance abuse#cw substance use#cw drvgs#cw alchohol mention#tw alcohol mention#aspd-culture-is#aspd culture is#aspd culture#actually aspd#aspd#aspd awareness#actually antisocial#antisocial personality disorder#aspd traits#anons welcome
26 notes
·
View notes
Text



ೀㅤㅤAlchie / Alchy
A flag for beings who are called/considered alcoholics or reclaim the word alchie / alchy for themselves. Can be used regardless of age.
⚠️ NOTE : for awareness and pro-recovery. not made to romanticize or encourage alcoholism, it's exclusively for those who suffer from alcohol addiction and alcohol addiction disorders.
ྀི◟ ͜ ̣̣̥⠀ self-indulgent, flag by me. inspo from this post



#🍷. ︵ a lil smth for you#💋. ︵ snuff's hoard#🕯️⸺ siin's coining#💌mail!#alchie#alchy#tw alchohol mention#alcoholism#tw alcohol#tw alcoholism#addiction#addiction disorder#substance use disorder#substance use#mogai#liom#mogai flag#mogai coining#mogai term#liom coining#mogai gender#anti radqueer#anti transid
29 notes
·
View notes
Text
How To Write Characters With Addiction
From @differentnighttale: "I am curious if you give advice about writing people with addictions for example substance. I have reasons my male MC does it. But how can I describe the addictions the MC has correctly."
In this post we are going to be talking about addiction! From alcoholism, substance abuse, nymphomania, to everything else that can be a possible addiction. This post will be all about making this realistic and complex :)
A) What Are The Benefits?, Make It Convincing
Grab a fucking piece of paper or whatever you have and just write a paragraph from your addict's perspective on the situation. Omit the bad stuff. Make it highly convincing. if you aren't thinking "hmm, understandable" after you've written and read it, you did it wrong.
What do they get out of it?
Why did they like it at first?
Are they calmer, more intensely concentrated, does it take the edge off?
Are they more confident?
Does it ease the sense of being fundamentally wrong or dull some other pain?
Is it fun to do something rebellious?
What made them like this thing so much they tried it again, and again, and again?
B) Think About The Consequences, And Ignore It
Oftentime, at least in my experience, people will continue with a bad habit if it means they don't have to be the one to think about the consequences.
The Consequences For Addiction Include:
Financial. Depending on what your character uses to get their fix and how much they use, they might be spending hundreds a week if they are a particularly aggressive user. People often steal money from their loved ones. Addiction also tends to get people fired. Write a scene where your drunk character gets fired for operating machinery. Have them be a burdenous sponge.
Social. It's common for addicts to lose their loved ones since it often gets to a point where it's impossible to care about these people despite how much you love them. Make love ones leave your character! And don't blame them
Physical. STDs, Overdose, Liver Failure, and a shit ton of other issues from the chronic to the fatal either cause, exacerbate, or are linked with addiction. Recovery can't automatically save your character so don't write that story.
Psychological. Being an addict isn't fun since you get to struggle with points 1, 2, and 3 all at the same time! Write about your character issues. Their lack of control. Their spiralling life.
Write all about your character's suffering. And then have them justify it. Make it convincing.
They need it. It's not their fault that this is the only that helps them! Everyone just doesn't get it. I'm trying to work on it, OK?! It'll all work out! They know that it's wrong but...
My most hated shit is when a character's arc is easy. They struggle with some things like a big dramatic argument with their wife, they cry a bit, and then they learn that "drugs are bad" so everything is fine :D
NO!!! Why don't you write about a friendship that doesn't get mended? A chronic illness they now have to pay huge medicine bills for? A fucked-up rap sheet that they can't escape?
And it's not because we want to punich addicts. It's because it doesn't matter if you care about addicts if you don't care about the messy shit!
It's easy to sympathize with an addict if you make them the most innocent victim who never hurts someone intentionally and who gets rid of the addiction in a second and never struggles with it ever again!
Do the hard shit. Make your readers sympathize with the unsympathetic asshole addict! Addicts aren't always good people! They can be dickbags. And they still deserve resources. Life isn't some kind of karma game where dickbags suffer and good people rise! Everyone deserves to not suffer!
Addiction is ultimately a disease. But it's a disease that can make someone you love into an absolutely unlikeable person. And this is coming from someone with an alcoholic dad <3 He does good things and bad things. I can sympathise with my dad and not let him walk all over me.
C) Withdrawal Is Leaving An Ex, Relapse Is Returning
Addiction is a motherfucker trying to leave. It's basically the equivalent of a clingy ex who keeps contacting you, asking for just one conversation, and the moment you so much as acknowledge them you are fucked.
And suffering the brunt of a clingy ex who won't take the hint tends to cause the same symptoms as withdrawal!
Obviously, withdrawal symptoms depend on what type of ex you have and what age you are and yada yada yada. Research for specificity :)
Withdrawal symptoms can include:
Headaches
Insomnia
Fatigue
Hallucinations
Seizures
Tremors
Cravings
etc.
BE AWARE: Relapses are when someone returns back to their drug if they were going cold turkey or going back to their original dose. Relapses can sometimes result in an overdose due to the fact that the brain has been weened off the substance and is now overwhelmed by the high dose.
Relapses often happen when a person makes the deliberate choice in order to stop these fucking nightmarish symptoms. To use the analogy of a clingy ex, you start talking to them in order to tell them to stop contacting.
Relapses can also happen through being in a setting where the behaviors associated with the addiction such as sex, gambling, drinking, substance use, and all manner of things are normalized.
This setting could be a party, a bar, or even a friend group.
Relapse is made more likely if someone is self-detoxing away from a support group or a doctor.
Writing about withdrawal and relapses are an important part in making a story feel more authentic. Just like with mental illness, people rarely learn the lesson and follow it perfectly. They make mistakes. Slip back into old habits. Do shitty things.
We aren't writing their suffering to punish them. We are doing it because you can't say you care if all you are willing to do is look at the easy parts.
D) Little Tidbits To Keep Track Off
This is the miscellanious things that didn't fit into their own boxes.
Friends!
Do they have friends who also have their addiction? How do they hang out? What are they like? How are their substance using friends different from their non-addict ones?
Slang!
Don't just look up slang for your substance of choice. You'll need to look at some first-hand accounts of addiction. Find an influence who has struggled with substance abuse in the past and see how they talk about it!
Variables!
Remember to keep their geographical location, socioeconomic status, time, and a host of other factors. If your character is a penniless alcoholic then it's unlikely they'll get their hands on some type of expensive gin. They'll probably use rubbing alcohol. Keep the price of your drug in mind.
A character's status will also impact their slang. No one unironically says doobie anymore.
A character's location will also impact how they get their shit and how other characters will react to that addiction.
A character's financial status also impacts how the consequences of their actions impact them. A low-income character wont be able to afford the same medication as a rich addict. They also won't have the same luxury for quality therapy, rehab, programs, time, anything really.
Look At The Addict And The Loved Ones
Try not the skew the reality of addiction to paint the addict as the victim and the loved ones as evil for not being forgiving and tolerant enough.
Keep sympathy for both the addict and the loved ones. Or drop sympathy for both of those characters.
E) RESOURCES
FDA and DEA online databases and drug resources
Social Networking Groups
Medical Journals
Local medical professionals, police, and medical examiners
The US national poison center
#writing#writeblr#on writing#creative writing#writing advice#addiction#recovery#writers#writer#writers on tumblr#writers and poets#writerscommunity#writing addiction#writing life#writing community#writing inspiration#writing ideas#helpful#writing reference#reference#addictive#substance addiction#substance use disorder#tw substances#resource
41 notes
·
View notes
Text
"ugh i hate Snowbirds so much they really ruined Roy's character by making him an addict and also it was one story a long time ago but nobody ever lets it go like it's fine we get it he's okay now why are we never letting it go he deserves so much better when will dc fans grow past this" -> buddy you are about to become so well acquainted with my good friend, Hammers
#dc#dc comics#roy harper#addiction is a lifelong struggle y'all#yes Roy's character isn't defined ONLY by his addiction#yes there many amazing important things about him#addiction is a lifelong struggle#it gets better with time sure#but regression relapse etc. are part of life#part of healing#roy undergoes so many bad events#ofc he's gonna struggle#of course he's gonna have cravings#i want to see him relapse and heal#and y'all need to learn to be normal about characters with Substance Use Disorders#roy harper dc#roy harper defense squad#him struggling with addiction ruined NOTHING and he doesn't need to get over it#vent post#speedy#snowbirds don't fly#vent
50 notes
·
View notes
Text
#narcissisticabuserecovery#narcissisticabuse#complex ptsd#trauma recovery#cptsd recovery#boundaries#mental health#self care#empathy#gaslighting#substance use disorder
200 notes
·
View notes
Note
hey wait no no. come back
tell me more abt npd terzo im /gen interested
(@puppsworld)
Ouuuugh… my guy… my shayla…
(Disclaimer: I don’t have NPD, I’m just going off personal accounts of the disorder I found online. Readers lmk if anything I say is misinformation and I’ll correct it)
His self-worth is entirely based on his status and power and how others see him. He climbed the ranks in the church and took pride in being the hot “bad boy” cardinal. Every promotion would give him an ego boost for a while but he kept craving more.
He tends to have thin skin. He hides it well but criticism cuts down to the bone and if not processed correctly he’ll lash out or spiral inward. He needs himself to be perfect.
Becoming Papa was a major ego boost and being onstage and performing was addicting. He got constant praise and adoration, his own pack of ghouls, fame and fortune… it was all he could’ve ever asked for.
In the beginning of his time as Papa he was pretty stable, mostly enjoying the new rank and the freedom to write music (and the ghoul sex). But as he toured, he grew distant from his ghouls, only interacting with them onstage and rarely seen by them offstage. He couldn’t bear if anyone saw under his carefully crafted mask of opulence and glamour and confidence.
Omega was the only one who was allowed to see the real him. He held Terzo’s fragile heart in his hands and kept it safe. He was honest- not rudely so, but enough to rein Terzo in. He was the grounding force he needed to get through the highs and lows of touring.
When he got dragged offstage and told he would be retiring, he just broke. He isolated himself, screamed at Omega when he tried to check on him, and started drinking heavily. The ONE TIME he was convinced to come out of his room to play uno with his brothers he got dragged away and beheaded.
#the band ghost#terzo emeritus#papa emeritus iii#Papa 3#terzomega#omega3#Wham answers#cw substance use#(Mentioned)#anyway shout out to people with “evil” disorders. Love y’all.
12 notes
·
View notes
Text
You know what the worst fucking thing about liberal rhetoric is? Using "harm reduction", a term that refers to health policies offering safe options and alternatives for drug users instead of punitive control, to rationalize re-endorsing back into power a regime that is still overseeing one of the worst human atrocities of the 21st century.
#you wouldn't spit on an addict if they were on fire and don't want abolition because you think they belong there#'harm reduction' hell is too good for you#ableism#drug usage#addiction#substance use disorder#disability#mental illness#disability justice#social justice#abolition#us politics#shit liberals say#white liberals#us imperialism#american imperialism#war crimes#knee of huss
31 notes
·
View notes
Text
it’s post-yr-wip wednesday, so enjoy more scenes from my forthcoming follow-up to krapp’s last tape, this time ft. events from the viewpoint of alice molloy, 1985-1989 ✨ all yr canon-typical content warnings for disordered substance use, pregnancy trauma, AIDS crisis-related death, child endangerment, codependent relationships with multiple concerning/unethical power differentials, etc.
“What mad Nijinsky wrote
About Diaghilev
Is true of the normal heart;
For the error bred in the bone
Of each woman and each man
Craves what it cannot have,
Not universal love
But to be loved alone.”
from “September 1, 1939”, by W. H. Auden
It’s 1986 and Alice Molloy sits on the steps of San Francisco City Hall. She has been Alice Molloy for, approximately, the past thirty minutes. She is twenty-five years old. She looks out across Van Ness Avenue, at the War Memorial Opera House. She’s never been to the opera before. She’s never been married before, either.
She rolls the name around in her mouth: Alice Molloy, Alice Molloy, Alice Molloy. She likes it. She feels like a snake that’s shed its skin, and now relaxes on the warmth of a sunned rock. She wonders how long it will take her to forget that she had any other name before this one.
There is another her, maybe — scared and strung out — still inside, wandering the atrium. Maybe there is another her buried in a grave in Evergreen Cemetery.
But this Alice, the one here on these steps, in this waning late afternoon sunlight, is Alice Molloy. She is Alice Molloy, with her newborn daughter, and her new husband, and their second-floor, one bedroom apartment near Buena Vista Park.
—
December 6, 1985. The CDC recommends delaying pregnancy until more is known about the risks of mother-to-child transmission of AIDS. As of December 1, there have been 217 reported cases of AIDS among children under age 13, and 60% of them have died by the time of publication.
In Paris, their apartment is cold and there’s black mold around the windowsill. Daniel has a persistent cough. Alice wakes up nauseous.
Three months ago, in San Francisco, Daniel gets an advance for a novel and insists they spend it all right away.
Though he’s covering with bravado, Alice can tell he’s nervous. He’s never had more than a couple hundred dollars to his name, and never expected to have his sobriety tested in this manner either.
They book two transatlantic tickets to Paris and a sublet in the Latin Quarter.
Alice wants to chainsmoke at café tables on crowded streets and imagine stories about passersby while Daniel scribbles in his notebook. She wants to go dancing. She wants to see the Mona Lisa. Alice is twenty-four, Daniel is thirty-two.
(Over the past several months, Alice has planned more funerals that she cares to count. She is perpetually in the final hospital visit-cremation-memorial service cycle. As the most junior member of the organisation, her duties tend to be administrative: making payments and filing bank receipts. By cash and by cheque, payments are made to the crematorium, the ambulance, the reception hall, to the sandwich caterers, to the company that rents the folding chairs and plastic table cloths, to the leaflet printers, and the delivery trucks. At the end of it all, someone has to fold up the chairs and turn off the lights. That someone is Alice.
There is an impersonality to the deaths, she finds. Sometimes people with bring a framed photo of “the deceased” to the memorial service — a sister, a daughter, a girlfriend, a roommate, a friend. When there’s no photo, she often pictures Raequel. Twenty-two now? Would she look older? Or younger? Paris presents itself as a respite).
Paris’ crisp October turns to a drizzly November and finally to a frigid December. Any argument that sparks between Daniel and Alice is swiftly resolved by swallowing one’s pride and huddling together under their singular scratchy wool blanket for warmth.
In Paris, Daniel has coughed for three months. He’s smoking his packs twice as slowly because he has to take bone-rattling, hacking coughs after every few drags.
In Paris, Alice throws up three days in one week.
(They have both danced around this. It is the heavy, silent thing they neglect to mention. Daniel is sick. Alice is sick. With what — who knows? Fading track marks testify to their rich, independent histories of indiscriminately sharing needles and swapping bodily fluids with, at best estimate, one quarter of the Bay Area’s creatures of the night).
In Paris, over dinner, Alice tells Daniel she’s pregnant.
She tells him she’s pregnant and he says yeah.
He’s staring at the cigarette in his hand, poised over the ashtray and Alice can see the gears turning inside his head. France permits elective abortion up to ten weeks, she can see him thinking. She can tell he’s doing the math in his head.
She tells him she’s pregnant, and he says yeah.
They finish their meal in silence, but Alice is too nauseous to keep anything down so throws up again in the brasserie’s toilette. After she’s finished, she presses her head against the cool metal of the cubicle door and then kicks it violently several times.
When she re-emerges, Daniel has already settled the cheque. He’s got another cigarette in his mouth, this one unlit, and he’s chewing on the filter, eyes still staring into middle distance, gears still turning. Alice has stuffed her jacket pocket with extra towelettes in case she needs to throw-up in a public garbage can on their walk back to their apartment.
—
“We both could have it —“ Alice’s train of thought twists and weaves, running the alternatives and counter-alternatives too fast to keep track of until its a circular, tangled mess. “It would be born sick,” she says.
“We don’t know if we—“
“But we could. What if it’s born sick? If it’s— if it’s not able to grow?”
“Failure to thrive,” Daniel supplies.
“I know whatAnd, in a heartbeat of indignation, Daniel ask, “What? What do you want? Do you expect a child to consent to being born?”
“Maybe the hospital finds out! Maybe it’s — taken away from us. Because it’s our fault. How could we live with ourselves?”
“We make a choice. We live with it.”
“I don’t know if I can.”
“Look.” Daniel presses his hand to her cheek, and his eyes fixed on Alice’s. “If it’s wrong — does it matter?” His thumb traces her cheekbone, over the scar on her eyebrow, where it turns from dark to blonde. “All human decisions are made like this.” He kisses her eyebrow. He sounds surer and steadier than Alice has ever heard him before. “No parent knows what will happen to their kid. What does it matter if it’s wrong? There is no wrong. Just you and me. Me and you. And I want to be with you. Forever.”
Later, Daniel proposes and she says no. Things are falling apart. She doesn’t trust that the centre will hold.
On their last day in Paris, they go to the Louvre. Alice wants to see the Mona Lisa.
—
San Francisco, 1989. Alice Molloy is twenty-nine.
A week after the World Series Earthquake, Daniel’s mother calls him from Modesto to deliver the belated news of his father’s passing, the post-script to his unattended funeral. Daniel interrupts the daily pre-school drop off routine in order to purchase a self-obliterating quantity of heroin.
It’s thirteen hours before Alice finds him. When she finally does, he crawls to her on his hands and knees. He clutches her legs, sobbing, shaking, and high. She says nothing to him, and her cool and implacable assessment of the situation is this: I take care of you, I’ve always taken care of you. I love you, I’ve always loved you. You and me, me and you. Daniel would not die here. Their dance would not end like this.
Her fingers grasp his matted curls, and she gently forces his head back to meet her gaze. With a thumb, she carefully wipes his grimy, tear-stained cheeks. She whispers to him: I forgive you. Of course I forgive you. How could you doubt such a thing? I have forgiven you of everything before now. I would forgive you every time, even this.
And Alice knew this: Daniel was hers. And he would never runaway from her again.
Outside, Lena is asleep in the backseat of the car. She is three years old.
#this is my manifesto against well-adjusted and normal alice molloy allegations#do NOT let her go to therapy#let her have a fraught psychosexual rivalry-turned-affair with ex-wife number 2#also genuinely i doubt this will make sense without the context of krapp’s last tape#critical info established prior is that alice meets daniel when she is his programme manager at the drop-in resource centre#for sex workers seeking support with disordered substance use recovery#a program which she herself is a graduate of#(Raequel is Alice’s younger sister still in the life whom she’s lost touch with)#(daughter number one is Lena)#(daughter number two — ie the one Daniel pictures as Claudia before he sees her pictures in Paris — is rae)#(named after Alice’s younger sister)#delete later#tv series: interview with the vampire#i love 2 yap abt my ocs that have been extrapolated entirely from scant traces of biographical material
17 notes
·
View notes
Text
you! person who talks about how "everyone has an addiction" and mainly means phones/video games! quick quick, tell me how you feel about people who compulsively use drugs!
#head in my haaaands. if this is how you chose to conceptualize all unhealthy relationships to nonliving physical objects#then at least let it build some compassion and solidarity for people with substance use disorders#'everyone has an addiction and there's no shame in that! well unless it's drugs alcohol or gambling. those people suck.' dude.#absolutely not interested in litigating what I mean here so no rebloggie for you. sorry.#marina marvels at life
98 notes
·
View notes