#what does a clinical research associate do
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s website traffic is steadily declining.
Text
!season 1

Viktor is, you've clearly observed, insecure of himself.
Quite valiantly, due to some looming social norm or personal feeling, he tries to hide it. But in moments like these, such an act becomes impossible. Try as he might, desperately at times, when he's pressed against you in the warm water, your fingers over his skin, your fingers in his hair, his failure is palpable.
"Are you okay?" You murmur into the nape of his neck, his back against your chest. The water threatens with gentle churns to spill over the bathtub.
He turns his head to press a kiss against your wrist.
"More than," he says, voice quiet but firm, "I just feel, sometimes," and he hums, as though forming an adequate description of his emotions were the hardest task on the planet. Viktor, your genius scientist, hesitant not to innovate, to change the world with his research, no. He's hesitant only to make sure he says the right thing to you.
"Like I'm too good for you?" You ask, catching his eye. By the gentle look you know that's what he means. He faces away again, nods in a vaguely ashamed way.
How, you've always wondered, can you truly change someone's perspective? When words don't seem to persuade, when actions bring only fleeting relief, what can you do?
"It's irrational, I know, some... flaw of the mind. You don't need to keep reassuring my senselessness." He leans into your touch, takes your free hand into his, soap suds bubbling between your fingers.
"Sometimes you talk about yourself like you're a machine, you know." You muse. He gives a half-hearted laugh.
"Not a well functioning one."
Are words or actions worth more in this game of convincing? Does he feel it deeper when you press your lips into his hair, or when you mumble compliments and honeysuckle words into his ear? He shivers either way.
It's a long game, you know. It's taken months to even reach this stage, where the self-deprication is a rarity, not the norm. Maybe it'll take his whole life before he can accept every part of himself like you can, before he can truly see himself through your eyes, gleaming and gem-speckled as they are.
You free your hand from his, reach up instead to knead shampoo into his thick hair. He responds with a sigh and sinks somehow further against you, the water falling slowly to a more lukewarm temperature. You're not sure how long the two of you have been in here, talking quietly about very little, exchanging words that'll disappear forever with the water. But you really can't find it in you to care.
There's work to be done, errands to run. Errands that should've been run a week ago. This ceremony, this meditation makes all of it null. For where else would you want to be? Where else exists besides here, this room, this moment, static in the cooling water with the embodiment of perfection.
When you tell it to him, as you so often do, when you tell him that he's perfect, he can't believe you. The first time you ever said it, peering into his eyes as if they held some secret treasure within, he thought you were joking. He'd laughed, more out of obligation than actual humour, but your expression remained still. Sincere. To say he was moved would be a wildly inadequate explanation. What he felt in his chest that night was something otherworldly, something without a name. He's come now to associate it simply with yours.
You run water through his hair, rinse out the shampoo as he lies pliant in your hands. He insists you use your soaps in his hair, some floral-scented collection you've used for who knows how long, because the smell reminds him of you.
There's no point in overthinking it, you suppose. No point in trying to map out and organise moods, emotions. No point in trying to turn a gentle human experience into something clinical, something without humanity.
That swirling, omnipresent yet transient concept of humanity. You simply must cradle it within your own. You press your lips into his wet hair, whisper words made of ginger and lavender into his ear. Because at the end of the day, you're human. You're in love. And sometimes, that's all that matters.
1K notes
·
View notes
Text
Natural Breeding Clinic - Prologue
warnings: MDNI, breeding kinks, general sex, mention of infertility and insemination methods
a/n: It's here. Finally.

Teaser - Prologue - Patient 1
You take a deep breath and sit down in front of the laptop, waiting for the other person to join the call. Never in your life had you heard about such a unique reproductive center but lately, you’d been feeling the pull to start your own family. You’d discussed this with relevant people in your life. Everyone had said if you really wanted a child, then you should go with the options you thought were right for you.
You’d done the research, looking into different doctors and fertility clinics, but this one just stood out. There were testimonials from several happy families, saying their methods, though unconventional, were effective, and the doctors showcased on the website were all incredibly striking, each one handsome in their own way. But it was the success rate that caught your eye. A 98% guaranteed rate that you would be pregnant, and that pregnancy would be healthy. The site didn’t go into too much detail on their method, but the wording caught your eye.
“A natural breeding clinic” they’d called themselves. You’d finally bitten the bullet and called, requesting an information session. The screen suddenly lightens and you focus your attention as an attractive woman with shoulder-length brown hair comes into view. She smiles in a welcoming way before speaking.
“Hello. Am I speaking with Mrs. L/n?” You nod and smile back, trying not to look awkward or uncomfortable.
“Perfect! My name is Shoko Ieiri, I’m the main coordinating nurse here at Jujutsu Fertility. Thank you for scheduling an information session with us.”
“Yes, of course. I just needed more details before I booked an appointment.”
“Indeed.” Shoko claps her hands together before continuing. “Let me start by telling you a little bit about ourselves. We’ve been around for almost 6 years now. What sets us apart is that we focus more on women’s comfort than most other clinics. And we are sought out by people who are willing to use a sperm donor. We do not perform insemination services with sperm that are not from our own stock.”
“Your own stock? Are you associated with a sperm bank? And screen all the donors yourself?”
“Not a sperm bank in the conventional sense. We have 5 doctors who keep excellent health and their sperm is regularly screened to ensure quality. They are the only stock we allow for insemination.”
You blink to make sure you haven’t misheard. “The…doctors? Are you saying the fertility doctor I’d be meeting with will also be my sperm donor?”
“That is correct.” Shoko nods her head to confirm. “You will be meeting with the doctor of your choosing for at least 5 sessions. They will need to be at least once a week. Some women take the week off and come in 5 days straight.”
“5…sessions?” you ask, confused by the wording.
“Yes. It’s to ensure the insemination process has occurred an optimal number of times.”
“Wait…so…I’m going to be inseminated multiple times? How much downtime do I need in between each insemination?”
“Hardly any. Our method isn’t like a typical clinic. Most women leave feeling very normal and a lot more satisfied than when they came in.”
“Not like a typical clinic? So…you don’t use the catheter method?”
“We use minimal medical equipment in our inseminations.”
“Minimal…so what does the procedure entail?”
Shoko clears her throat and continues. “So it begins with you choosing one of our doctors. We highly recommend spending some time on this part. It’s essential that you feel attraction towards your doctor. Once you make a choice, they will reach out to discuss how your insemination experience can be optimized for you. You will receive a biodata on their sexual profile, their preferred methods of arousal, and other relevant details.”
“I’m sorry, but what?” You are at the edge of your seat wondering if you’ve entered an alternate dimension. Surely, this was all being made up? “Arousal, sexual profile- why would I need all these details? I thought sperm donors only gave information like height, weight, medical history and stuff like that.”
“Why wouldn’t they? You’re choosing to be bred by them. They would have to make sure their patient is satisfied with the experience.”
“Bred?” You bleat the word stupidly.
“Yes. We are a natural breeding clinic. We use the method nature has provided to us to ensure a pregnancy.”
The gears in your brain start turning and something finally clicks.
“Are-are you saying…I would be having sex with my doctor?”
“That is correct.” Shoko smiles gently at you, pleased that you have finally caught on.
“The human body doesn’t necessarily enjoy having medical equipment inserted into it. All that cold plastic, and the mechanical methods of insertion. It puts the body in a state of stress. Not good for implantation. So our doctors will inseminate you through the process of intercourse.”
Her words fall like a fog around you. You can feel your heart racing, a flush creeping into your cheeks. It was…insane. The doctor of your choosing was essentially going to fuck a baby into you. As your mind starts pulling up the images of their doctors, each one impossibly handsome and striking, you feel a familiar throb starting between your legs. Wetting your lips, you try to talk to continue with the information session.
“I see. And…there are benefits to this?”
“Yes. Intercourse allows the body to relax, releasing happy hormones. In this stress-free state, in addition to the knowledge that your doctor is someone you’re attracted to and trust, the chance of an implantation doubles.”
You gape at Shoko, your mind reeling from all the information.
“And…when you say the insemination process will be optimized for my best experience…?”
“The doctor you choose will ask you extensive questions about your preferences. What turns you on, positions, dislikes, toys. It’s to determine if they will satisfy your breeding experience. If they feel they might not be a good fit, they’ll recommend another one of our doctors.”
You swallow, your mouth going dry. “I see. And…what else do I need to know?”
“We will start by collecting your medical history and run some blood work to make sure your body is ready for an insemination process. Women who have a domestic partner will need to get both a waiver and a consent form signed by their partner that they have been informed what happens for the insemination.”
“Of course. Makes sense.”
“You will be assigned an emotional support companion during this process. It will either be myself or Mr. Ijichi Kiyotaka. We are there to help ease your nerves and ensure you enjoy the process. And all patients must think of a unique safeword to use during the insemination process.”
“Safeword?” you parrot back, still processing.
“Yes. At any point during the process, should you feel uncomfortable, your safeword ensures all actions cease and your doctor will give you some space to breathe and reassess the situation.”
All you can do is nod along. Shoko gives you a look of reassurance. “I can guarantee that most women are pleased with the results. And our doctors are quite skilled in what they do. It’s natural to feel a little shy and embarrassed but at the end of the day, we all share a common goal- a healthy baby.”
Despite your initial shock, you feel some of your trepidation fade away. Shoko continues.
“If you are ok with all of this, I can send you the forms to get the process started. Once those are filled, you can take some time to decide on your doctor. Then we’ll set up a call with them.”
“Thank you.” You make a split-second decision. “Please go ahead and send the forms.”
“Excellent. I’ll send them to the email you put in your inquiry. Was there anything else?”
You shake your head no. “I think I have all I need.”
“Great! I look forward to assisting you again.” Shoko ends the call and you immediately go the the website again to look at the doctors, one of which will end up fathering your child. Such a hard decision. How will you ever make the choice?

@thesunxwentblack @kentocalls @actuallysaiyan
@belle-oftheball34 @jesssicapaniagua
@figmentforms

© unintentionalseductress original work | no copying, plagiarizing or translating
#jjk smut#nanami kento#gojo satoru smut#suguru geto smut#hiromi higuruma smut#choso kamo smut#shoko ieiri#ijichi kiyotaka#natural breeding clinic#nanami kento smut#gojo satoru#geto suguru smut#geto suguru#choso kamo#higuruma hiromi#jujutsu kaisen#jjk x reader#jujutsu kaisen smut#nanami kento x reader#nanami kento x reader smut#gojo satoru x reader#gojo satoru x reader smut#geto suguru x reader#geto suguru x reader smut#higuruma hiromi x reader#higuruma hiromi x reader smut#choso kamo x reader#choso kamo x reader smut#ncs#ncs scribbles
1K notes
·
View notes
Text
For much of living memory, the United States has been a global leader of scientific research and innovation. From the polio vaccine, to decoding the first human chromosome, to the first heart bypass surgery, American research has originated a seemingly endless list of health care advances that are taken for granted.
But when the Trump administration issued a memorandum Monday that paused all federal grants and loans—with the aim of ensuring that funding recipients are complying with the president’s raft of recent executive orders—US academia ground to a halt. Since then, the freeze has been partially rescinded for some sectors, but it largely remains in place for universities and research institutions across the country, with no certainty of what comes next.
“This has immediate impact on people’s lives,” says J9 Austin, professor of psychiatry and medical genetics at the University of British Columbia. “And it’s terrifying.”
The funding freeze requires agencies to submit reviews of their funded programs to the Office of Management and Budget by February 10. The freeze follows separate orders issued last week to US health agencies—including to the National Institutes of Health, which leads the country’s medical research—to pause all communications until February 1 and stop almost all travel indefinitely.
The confusion is consummate. If the funding freeze continues through February, and even beyond, how will graduate students be paid? Should grant applications—years long in the writing—still be submitted by the triannual grant submission deadline on February 5? What does this mean for clinical trials if participants and lab techs can’t be paid? Will all that research have to be scrapped thanks to incomplete data?
Even if Trump fully reverses the freeze on research funding, the damage, multiple sources say, has been done. Although for now the funding freeze is temporary, the administration has shown how it might wield the levers of government. The implication is that withdrawing funding could be done more permanently, and could be done to individual institutions, individual organizations, both private and public. This won’t just set a precedent for the large East Coast or West Coast universities, but those located in both red and blue states alike.
While always an imperfect arrangement, science in the US is largely funded by a complex system of grant applications, reviews by peers in the field (both of which have had to be halted as part of the communications pause), and the competitive distribution of NIH funds, says Gerald Keusch, emeritus professor of medicine at Boston University and former associate director of international research for the NIH. According to its website, the NIH disburses nearly $48 billion in grants per year.
When it comes to medical research, America truly is first, and if it abdicates that position, the void left behind has global ramifications. “In Canada, we have always looked to NIH as an exemplar of what we should be trying to do,” says Austin, speaking to me independently of any roles and affiliations. “Now, that’s collapsed.”
Science is, in its very nature, collaborative. Many consortiums and alliances within scientific fields cross borders and language barriers. Some labs may be able to find additional funding from alternative sources such as the European Union. But it is unlikely that a continued withdrawal of NIH funding could be plugged by overseas support. And Big Pharma, with its seemingly endless funds, is unlikely to step up either, according to sources WIRED spoke with.
“This can’t be handed off to drug companies or biotech, because they’re not interested in things that are as preclinical as a lot of the work we’re discussing here,” says a professor of genetics who agreed to speak anonymously out of fear of retribution. “Essentially, there’s a whole legion of university-based scientists who work super damn hard to try to figure out some basic stuff that eventually becomes something that a drug company can drop $100 million on.”
The millions of dollars awarded to high-achieving labs is used to fund graduate students, lab techs, and analysts. If the principal investigator on a research team is unsuccessful in obtaining a grant through the process Keusch describes, often that lab is closed, and those ancillary team members lose their jobs.
One of the potential downstream effects of an NIH funding loss, even if only temporary, is a mass domestic brain drain. “Many of those people are going to go out to find something else to do,” the professor of genetics says. “These are just like jobs for anything else—we can’t not pay people for a month. What would the food service industry be like, for example, or grocery stores, if they don’t pay somebody for a month? Their workers will leave, and pharma can only hire so many people.”
WIRED heard over and over, from scientists too fearful for their teams and their jobs to speak on the record, that it won’t take long for the impact to reach the general population. With a loss of research funding comes the closure of hospitals and universities. And gains in medical advancement will likely falter too.
Conditions being studied with NIH funding are not only rare diseases affecting 1 or 2 percent of the population. They’re problems such as cancer, diabetes, Alzheimer’s—issues that affect your grandmother, your friends, and so many people who will one day fall out of perfect health. It’s thanks to this research system, and the scientists working within it, that doctors know how to save someone from a heart attack, regulate diabetes, lower cholesterol, and reduce the risk of stroke. It’s how the world knows that smoking isn’t a good idea. “All of that is knowledge that scientists funded by the NIH have generated, and if you throw this big of a wrench in it, it’s going to disrupt absolutely everything,” says the genetics professor.
While some are hopeful that the funding freeze for academia could end on February 1, when the pause on communications and therefore grant reviews is slated to lift, the individuals WIRED spoke with are largely skeptical that work will simply resume as before.
“When the wheels of government stop, it’s not like they turn on a dime and they just start up again,” says Julie Scofield, a former executive director of NASTAD, a US-based health nonprofit. She adds that she has colleagues in Washington, DC, who have had funding returned to their fields, and yet remain unable to access payment through the management system.
Austin says that already the international scientific community is holding hastily arranged online support groups. Topics covered range from the banal—what the most recent communication from the White House implies—to how best to protect trainees and the many students on international visas. But mostly they’re there to provide support.
“I’ve had a lot of messages from people just expressing gratitude that we could actually get together,” Austin says. “There’s just so much unaddressable need. None of us has the answers.”
Scientists, perhaps more than any other profession, are trained to “learn and validate conclusions drawn from observation and experimentation,” says Keutsch. That applies to the current situation. And what they observe during this pause of chaos does not portend well for the future of the United States as a pinnacle of scientific excellence.
“If people want the United States to head toward being a second-class nation, this is exactly what to do. If the goal is, in fact, to make America great, this is not a way to do it,” says the genetics professor. “This is not a rational, thoughtful, effective thing to do. It will merely destroy.”
This story has been written under a pseudonym, as the reporter has specific and credible concerns about potential retaliation.
193 notes
·
View notes
Note
I totally understand and can empathize with fat activists when it comes to medical fatphobia. But I do think its important to provide nuance to this topic.
A lot of doctors mention weight loss, particularly for elective surgeries, because it makes the recovery process easier (Particularly with keeping sutures in place) and anesthetic safer.
I feel like its still important to mention those things when advocating for fat folks. Safety is important.
What you're talking about is actually a different topic altogether - the previous ask was not about preparing for surgery, it was about dieting being the only treatment option for anon's chronic pain, which was exacerbating their ed symptoms. Diets have been proven over and over again to be unsustainable (and are the leading predictor of eating disorders). So yeah, I felt that it was an inappropriate prescription informed more by bias than actual data.
(And side note: This study on chronic pain and obesity concluded that weight change was not associated with changes of pain intensity.)
If you want to discuss the risk factor for surgery, sure, I think that's an important thing to know - however, most fat people already know this and are informed by their doctors and surgeons of what the risks are beforehand, so I'm not really concerned about people being uninformed about it.
I'm a fat liberation activist, and what I'm concerned about is bias. I'm concerned that there are so many BMI cutoffs in essential surgeries for fat patients, when weight loss is hardly feasible, that creates a barrier to care that disproportionately affects marginalized people with intersecting identities.
It's also important to know that we have very little data around the outcomes of surgery for fat folks that isn't bariatric weight loss surgery.
A new systematic review by researchers in Sydney, Australia, published in the journal Clinical Obesity, suggests that weight loss diets before elective surgery are ineffective in reducing postoperative complications.
CADTH Health Technology Review Body Mass Index as a Measure of Obesity and Cut-Off for Surgical Eligibility made a similar conclusion:
Most studies either found discrepancies between BMI and other measurements or concluded that there was insufficient evidence to support BMI cut-offs for surgical eligibility. The sources explicitly reporting ethical issues related to the use of BMI as a measure of obesity or cut-off for surgical eligibility described concerns around stigma, bias (particularly for racialized peoples), and the potential to create or exacerbate disparities in health care access.
Nicholas Giori MD, PhD Professor of Orthopedic Surgery at Stanford University, a respected leader in TKA and THA shared his thoughts in Elective Surgery in Adult Patients with Excess Weight: Can Preoperative Dietary Interventions Improve Surgical Outcomes? A Systematic Review:
“Obesity is not reversible for most patients. Outpatient weight reduction programs average only 8% body weight loss [1, 10, 29]. Eight percent of patients denied surgery for high BMI eventually reach the BMI cutoff and have total joint arthroplasty [28]. Without a reliable pathway for weight loss, we shouldn’t categorically withhold an operation that improves pain and function for patients in all BMI classes [3, 14, 16] to avoid a risk that is comparable to other risks we routinely accept.
It is not clear that weight reduction prior to surgery reduces risk. Most studies on this topic involve dramatic weight loss from bariatric surgery and have had mixed results [13, 19, 21, 22, 24, 27]. Moderate non-surgical weight loss has thus-far not been shown to affect risk [12]. Though hard BMI cutoffs are well-intended, currently-used BMI cutoffs nearly have the effect of arbitrarily rationing care without medical justification. This is because BMI does not strongly predict complications. It is troubling that the effects are actually not arbitrary, but disproportionately affect minorities, women and patients in low socioeconomic classes. I believe that the decision to proceed with surgery should be based on traditional shared-decision making between the patient and surgeon. Different patients and different surgeons have different tolerances to risk and reward. Giving patients and surgeons freedom to determine the balance that is right for them is, in my opinion, the right way to proceed.”
I agree with Dr. Giori on this. And I absolutely do not judge anyone who chooses to lose weight prior to a surgery. It's upsetting that it is the only option right now for things like safe anesthesia. Unfortunately, patients with a history of disordered eating (which is a significant percentage of fat people!) are left out of the conversation. There is certainly risk involved in either option and it sucks. I am always open to nuanced discussion, and the one thing I remain firm in is that weight loss is not the answer long-term. We should be looking for other solutions in treating fat patients and studying how to make surgery safer. A lot of this could be solved with more comprehensive training and new medical developments instead of continuously trying to make fat people less fat.
659 notes
·
View notes
Text
Fear-mongering and herbalism
Herbalism is a crucial element for many practitioners of witchcraft, and lately I've seen a lot of fear-mongering in the #baby-witch and #witchblr tags that it's raising some serious red flags. Caution is necessary, yes, but over-simplified warnings against herbs that have a very long history and tradition of safe and effective use can rob people of accessible, beneficial ways to take an active role in their own health and wellbeing.
True: People absolutely need to be cautious about what they are putting in their bodies. True: "Natural" does not equate to "good" or "healthy". True: You need to speak to a medical professional regarding medical issues.
All these things being true do not mean that you cannot find plants that are safe to ingest, and that can benefit your health and support you. You can use herbs safely and you do have the power and ability to find information about them.
I've literally seen posts that say not to ingest any kind of herb because "you don't know what's in them" and "you don't know dosage, so it might harm you".
This lack of nuance is precisely the type of thinking that breeds misinformation and unnecessary fear, as if there is not enough of that to go around! It seems like because MAGA and anti-vaxx folks have been using the line "do your own research!!" so much, people are associating research with... right wing conspiracy theory? Somehow? Don't forget that being capable of doing good research also means being capable of evaluating your sources, and thinking critically about what you're reading.
Here are some of the misconceptions I've come across in the last couple days:
Laypeople can't safely use herbs
Fear of toxicity in herbs is common and rational, but herbs that you can find in your kitchen are food-grade and widely available. You don't need to eat them in enormous quantities to experience their benefits.
For example, thyme can help support the lungs during cold and flu season. Ginger tea is great for minor digestive upsets. These are things you have access to and can provide a safe means of relief.
Local apothecaries are very knowledgeable about where they source their herbs and what dosages are safe. They are also able to tell you if their herbs are pesticide-free, organic, etc.
Where you want to be cautious is ordering herbs online, especially places like Amazon or Etsy where there is no control whatsoever. Even supplements have been found to frequently not contain what they are said to contain, and you really have to do research about the company you're buying from beforehand.
If you don't have a local apothecary, you can still buy herbs online! Just make sure you are using a reputable website such as Mountain Rose Herbs where you can get bulk herbs.
Lesser known herbs require more caution, but there are fantastic books about herbalism and they provide information on dosage and various ways the herbs can be used responsibly. Your local library is almost guaranteed to have several books about herbalism, and if you aren't sure about a particular herb, look it up in multiple other resources to see if their information matches up. You can even find information about many commonly used herbs on WebMD.
Also, don't forage herbs that you plan to ingest if you are not experienced. This is a recipe for disaster, and incredibly dangerous. I'm not going to go into super huge detail about this, because it would merit its own post, but seriously, just don't do it until you have experience. Plant identification apps are not sufficient to identify herbs you plan to ingest.
Herbal remedies cure major illnesses
Herbs can play a supportive role, but it's crucial to recognise their limits. Herbal medicine should complement, not replace, medical treatment for severe chronic conditions. Clinical herbalists are trained to assess what's appropriate for herb-based support and when a situation requires immediate medical attention.
Herbs are not a panacea that will cure every ailment. Every person is unique and any single herb can have wildly different effects on the body. Some people might find incredible relief, while another person may find no effect at all, or may even find an herb doesn't agree with them.
Herbalists think they are medical practitioners
Because there is no federally regulated body for herbalists, people sometimes think it's the wild west out there and anyone can do anything, but that's not the case. Herbalists are not exempt from the law, and no one is legally allowed to practice medicine if they are not licensed to do so. Period. No amount of traditional knowledge changes that.
While the herbalist profession is not regulated federally, there are regulating bodies that are run by herbalists and that set standards for what is expected and permitted. If you search for "herbalism guild Canada" you will find the Canadian Council of Herbalist Associations which has tons of information, and some provinces also have their own guilds. Most guilds will have a list of reputable herbalists that you can access and they have strict requirements for being added to those lists. You can find these requirements on their websites and gauge them for yourself.
Part of training to become a clinical herbalist is knowing you are not a medical practitioner. You are taught not to diagnose people, and how to recognise when something is outside of your scope of practice.
From the CCHA:
9. A registered herbal practitioner will offer interdisciplinary collaboration with other health professionals
Herbalists focus on holistic, complementary care, rather than taking on the role of medical practitioners. A qualified herbalist works alongside them to support the body's systems, rather than attempting to independently treat or diagnose medical systems. For example, they might work with clients to ease side-effects from medication, but they won't independently treat serious conditions like infections.
Herbalists are anti-vaxx and anti-science
The vast majority of clinical herbalists are not anti-vaxx or anti-modern medicine at all, and focus on combining traditional knowledge about plants with modern science. Are there herbalists out there who are anti-vaxx? Absolutely, just like any demographic you can find people who are spouting nonsense, but that is not the norm.
Thankfully, herbalism schools and herbalists are pretty up front with their beliefs. The CCHA has these requirements for herbalists in the guild:
3. Herbalists have an extensive knowledge base combining traditional wisdom and modern scientific perspective [...] 7. A registered herbal practitioner is trained in herbal safety, drug interactions, and possible contraindications [...] 10. A registered herbal practitioner is accountable to a professional organization, must maintain annual continuing education and must abide by professional standards
When I was looking for a clinical herbalist myself, I always checked their website information and whether they were registered with a guild, and what the requirements for that guild were. The herbalist I chose also had a clear section on her website where she stated that she had experience working with people on psychiatric medications.
You can also often find their stance on other things such as LGBTQIA+ issues (such as statements on their website regarding their approach to HRT).
The school I ultimately selected for my education was one that had explicit information about how they integrated new science into their curriculum, and how frequently it was updated.
If you are not finding the information you're looking for, just ask! It's completely acceptable and not rude to contact an herbalist and ask them what their approach is on the things you are concerned about. They will be happy to answer these questions and give you any information they can to help you decide if they are a good fit for you.
Conclusion
Herbalism is not about replacing medical care or promising miracle cures. It's about tapping into centuries-old knowledge and combining it with modern insights. Embrace herbs with curiosity, responsibility, and respect, and you can have an incredible and beneficial relationship with them.
I'm sure there are plenty of points here that I have omitted or not sufficiently covered. I hope readers will take this as an indictment of the author, me, rather than one against herbalism as a whole.
62 notes
·
View notes
Text
…here are twenty five more studies that further irrefutably prove vaccines are dangerous, useless, and are directly responsible for the autism epidemic:
A two-phase study evaluating the relationship between Thimerosal-containing vaccine administration and the risk for an autism spectrum disorder diagnosis in the United States A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population Commentary--Controversies surrounding mercury in vaccines: autism denial as impediment to universal immunisation Methodological issues and evidence of malfeasance in research purporting to show thimerosal in vaccines is safe Abnormal measles-mumps-rubella antibodies and CNS autoimmunity in children with autism Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997-2002 Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature? A case series of children with apparent mercury toxic encephalopathies manifesting with clinical symptoms of regressive autistic disorders A comprehensive review of mercury provoked autism Thimerosal Exposure and the Role of Sulfation Chemistry and Thiol Availability in Autism B-Lymphocytes from a Population of Children with Autism Spectrum Disorder and Their Unaffected Siblings Exhibit Hypersensitivity to Thimerosal Theoretical aspects of autism: causes--a review Conjugate vaccines and autism Autism: a novel form of mercury poisoning A prospective study of thimerosal-containing Rho(D)-immune globulin administration as a risk factor for autistic disorders Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders The potential importance of steroids in the treatment of autistic spectrum disorders and other disorders involving mercury toxicity Reduced levels of mercury in first baby haircuts of autistic children Cultured lymphocytes from autistic children and non-autistic siblings up-regulate heat shock protein RNA in response to thimerosal challenge A possible central mechanism in autism spectrum disorders, part 1 The role of mercury in the pathogenesis of autism Transcriptomic analyses of neurotoxic effects in mouse brain after intermittent neonatal administration of thimerosal Causal relationship between vaccine induced immunity and autism Elevated levels of measles antibodies in children with autism Subtle DNA changes and the overuse of vaccines in autism What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature?
37 notes
·
View notes
Note
Hello, I'm not really sure where to go with this question, and I'm really confused.
I am trans afab, but I've been noticing a lot of things recently and I am not sure what they are or what to do about them. I am pre T, and I'm fourteen years old. I've been growing a moustache, and I'm not sure how or why, I haven't done anything to add to it, but it keeps getting thicker and darker. I also have a bit of a unibrow and I'm overall just fairly hairy. I also have a deeper voice, and I have since I was 11, and I have also noticed that my vagina looks very different to anything I've seen or looked up. My clit kinda sticks out a bit, and everything seems in a slightly different place? I also have a bit of skin at the side that hangs down by a lot, like it's very big. It feels like an bag almost? I don't know how to describe it.
It's getting to a point where I'm beginning to worry about it, I've tried researching it but nothing I've found really helped, and I just don't understand what's going on. I don't know if it's just normal puberty or if I'm just having placebo because I am trans but it's really worrying me now and I don't know how to bring it up to my mum or anything.
I don't know if this is tmi or anything, and I don't really know what you could do, but I just need help because I don't know what my body is doing anymore. I really don't want to make anyone uncomfortable or intrude on any space, but I just need someones input that isn't Google.
hey anon! you may have a hormonal intersex condition called hyperandrogenism(the intersex part is debated a lot but. i would consider it intersex and so does a lot if intersex people)

from the cleveland clinic
it can be associated with some other medial conditions that are life or health threatening, but not always, so if this causes any problems for you i’d recommend going straight to your primary doctor. since you’re 14, i’d definitely recommend bringing this up at your next checkup(if you’re still distressed about it)since i know stuff like that can be uncomfortable to talk to your parents about
110 notes
·
View notes
Note
as someone who has maladaptive daydreaming disorder this pisses me off so FUCKING BAD. im too shakey to type much less read this fully but oh my fucking god. oh my god. what the FUCK. how fucking DARE this person take MY DISORDER and twist it to conform to their DISGUSTING ABLEIST BELIEFS?? im reFUCKINGvolted
https://www.tumblr.com/alyssasmaddworld/741046067507904512/theres-this-level-of-dissociation-that-goes-hand?source=share
i- this post is a lot, but i'll try deconstruct each point here.. i'll be focusing on points that i can debate here / can disprove or try to disprove here because otherwise this will be a really long post,, longer than it already is. also i'll be referring to maladaptive daydreaming as MD for simplicity's sake. if i get any information on MD wrong please let me know as i do not have this disorder(?) nor do i know much about it outside of the research done for this post.
the source linked here does say that it is a dissociative disorder and it does say that it might not be caused purely by trauma " Although trauma may be one causal factor, we indicate several other etiological pathways to the development of MD. We discuss associations with related concepts and suggest directions for future research " so there isn't much for me to say here other than the part about plurality, but we'll go more into depth on that below.
this.. the source they used is pluralpedia.. which used the source of a tumblr blog.. so lets get into this. the first source also mentions maladaptive characters / MD characters but it also says that it is not like DID " We discuss and exemplify with clinical vignettes the shared phenomenological characteristics between MD and dissociative phenomena, such as double consciousness, vivid visual imagery, and the creation of internally narrated characters. MD characters can be experienced as somewhat independently-agentic, although unlike dissociative identity disorder (DID), they typically do not take control over the daydreamer’s behavior "
so lets look into MD characters, shall we? the only source i can find on MD characters ((other than the one they linked / tumblr posts)) consider them more of a form/type of daydreaming (experiencing the daydream as yourself or as a character, daydreaming about a character, ect). these characters are not at all similar to alters and the "closest" i found was the foreign character
" For those who heavily engage in maladaptive daydreaming, they often will begin to develop "The Foreign Character" type of maladaptive daydreaming. In this type, you daydream about a central character who you believe is yourself, but who is fundamentally different in almost all respects. " — maladaptivedaydreaming.org
however these are not at all similar to alters which are
" two or more separate identities called “alters.” They control your behavior at various times. Each alter has its own personal history, traits, likes, and dislikes " — WebMD
the same source on foreign characters also states that " The reality is that for most people, they engage in these kinds of daydreams because they want to daydream about things entirely devoid from themselves and their real world experience. They don't want to daydream about themselves being a doctor or being better looking (to use the prior examples I used), but instead they want to dream about themselves being entirely different people so they can escape from who they really are. ". other than that source there is very little evidence on these characters being separate identities, even then it's important to keep in mind that it is not the same as having a split identity as it only appears during daydreams i would assume and would not be able to control you, how you think, how you behave, ect. ((which the first source literally said,, do endos even read their sources??)) i would also like to add that if these characters feel real and you believe all your daydreams to be real then it might actually be a delusion. there's nothing wrong with having delusions but it is also important to recognise that it's not real and that it does not at all compare to being a system.
the first source they used to claim that having MD is the same as being plural is a pro endo source, it defines being plural as " The most simplified definition of the term plural that includes all people who take the label is “someone who shares the same physical body with other individuals.” Such a group is sometimes referred to as a system, though many plural groups use different terminology. " which,, again having daydreams are is not the same as having separate identities, so really this source means nothing.. and the second source is.. just insane really. its a study done on the experiences of those with multiple identities. they did two things, one was an online survey that had 200-300 results and then 6 interviews.. which is definitely not enough evidence, since they cannot know if people are lying on those online surveys and 6 people are not enough to make it a reliable source. but lets focus on the part they pointed out, which was:
" Empirical measurement of multiplicity is sparse. The first inventory published in the field was the Plural Self Scale (Altrocchi, 1999), which assesses the structure of the personality. High scores indicate that thoughts and feelings are different through time and situations. The other inventory to assess multiplicity was developed by Carter (2008) and consists of 20 items, such as “Does your handwriting change noticeably at different times?” or “Do you swing suddenly from one mood to another for no apparent reason?.” However, these scales measure the integrity of the self and rely on the assumption that there is a “you” or “I” who is able to self-reflect. Individuals who consider themselves multiple refer to themselves as a group of selves (“we”). Thus, questionnaires that assess the extent of self-integration fail to assess the experience of individuals who claim to have multiple selves who all have different thoughts, feelings, motivations, and levels of complexity. " which-- just isn't much of a criteria other than the questions, of which are "does your handwriting change at different times" and " do you swing from one mood to another with no apparent reason", but it literally says this fails to asses those who claim to be plural-- so i don't see what their point was here really. it just seems like they're saying words for the sake of saying words.
i don't think this person realises what closed culture is.. tulpulmacy is not a form of being plural nor should it be considered that, thoughtforms are usually used purely for meditation or for your spiritual journey, not for fun,, unlike "tupla systems" which are often not even Buddhists, which is the main issue. a closed practise, which is what tulpulmacy is, is a "practice in which you can only take part in their craft if you were specifically born into the practice, or went through an initiation process.". while i'm not 100% sure what exactly they mean with the last part there isn't much for me to say here other than the fact that tulpulmacy is not the same as being plural and we did have a former Buddhist actually talk to us about this here! and while it isn't exactly sourced i feel its still an important read.
i believe they're speaking about the word plural here,, which wasn't made by endos?? the word plural just refers to more then one. unless they mean traumagenic?? which then confuses me because their source doesn't really mention it--
culture is dynamic yes, but some cultures are closed and it's important to understand that-- just because the culture is shifting doesn't mean you can steal closed practises.
"endogenic sphere" makes me shiver but okay, lets talk about this too. there isn't a lot of research on MD, so i cannot say what the direct cause is. "Experts don’t know exactly why maladaptive daydreaming happens. However, they suspect it happens because maladaptive daydreaming can be a coping mechanism for problems like anxiety, depression and other mental health conditions."
no?? what?? as i said above, many times, having MD is not the same as having DID / being a system and also the image only refers to feeling disconnected from the body and sense of identity which is pretty common with dissociation and doesn't exactly prove anything related to endogenic systems..
i- ?? i mean as i said before we don't know what exactly causes MD but i don't believe people chose to do this?? not really??
" maladaptive daydreaming is often compulsive, which means a person feels like they need to do it. Because the need to daydream is similar to an addiction, daydreaming more often can make it a strong habit, so it’s very hard to stop doing it. That’s why seeking mental healthcare for it sooner rather than later is important. "
but all being said, its not a vaild form of plurality because its nothing like having separate identities?? sure when daydreaming you might identify as a different person but you're still you. your overall identity is intact and i'm pretty sure most people with MD do not think their daydreams are real, i believe that would be a delusion instead of a daydream-- and an important separation is these characters would only show up in daydreams i assume, while alters are always there, infact in DID you yourself is an alter but in MD one of you is a person and the other is a character created through daydreams,, which is not comparable to genuine parts / alters. ((also please do not harass the person who made the original post, our post / response is purely meant to educate and correct misinformation and we do not intend for people to go to the op's blog and send them things))
#sourced#kind of sourced#requested info#answered asks#anti endo#endos dni#system#did osdd#osddid#plural#system stuff#did#traumagenic system
57 notes
·
View notes
Text
Study puts understanding of long COVID and vaccination into question - Published Sept 4, 2024
This article highlights why I haven't been celebrating about recent findings that vaccination reduces long covid:
We still do not have a solid definition of what long covid is.
We still don't know how long it takes some people to develop long covid: Some people develop long covid symptoms months or even years after infection.
Many are undiagnosed with long covid because of a lack of understanding in the medical community.
The reduction stated in initial studies on vaccination and long covid cited about 30% reduction: That isn't enough for me to take off my mask.
Dr. Ziyad Al-Aly has been somewhat off his game in recent months, giving in to hope and showing signs of pandemic fatigue. His desire to be done with the pandemic may be tainting what he writes, in my opinion. As there is no cure for long covid (and we still don't know exactly what causes and perpetuates it), it seems silly to suggest that vaccination is a long covid silver bullet while cases continue to skyrocket worldwide.
I'm a non-medical observer, but I keep track of the latest studies and news, so I'm not totally uninformed, but take this blurb with a gain or two of salt. I could be wrong, but it doesn't look that way yet.
A new study from researchers at the Mayo Clinic suggests that being vaccinated against COVID-19 does little to prevent long COVID.
The findings contradict what has become conventional wisdom in the last 3 years—that vaccines offer a chance to significantly reduce the risk of long COVID, or new or persistent symptoms 3 months or more after infection, most likely by reducing the severity of infection.
Melanie Swift, MD, MPH, was the lead author of the study, which was published in Open Forum Infectious Diseases. She said despite the current thinking that vaccines reduce the risk of developing long COVID, she wasn’t surprised she found no association.
"A lot of the early literature on long COVID was really defining long COVID through patient surveys," Swift told CIDRAP News. Swift’s study instead relied on participants having received a long COVID diagnosis from a physician after having a documented case of post-vaccination COVID-19 infection.
6.9% developed long COVID The study was based on the electronic records of 41,652 people aged 5 years or older with SARS-CoV-2–positive polymerase chain reaction (PCR) tests between February 2021 and December 2022 and a diagnosis of long COVID 30 days to 6 months following infection.
The average age of patients was 41 years, 55.2% were female, and 90.7% were White. At the time of initial infection, 9,744 (23.4 %) were vaccinated with two doses of mRNA COVID-19 vaccine, and 7,658 (18.4 %) had received more than two mRNA doses.
A total of 8.2% of patients required hospitalization for COVID-19, and most infections occurred during the Delta and Omicron eras (39.8% and 47.1%, respectively).
In total, 6.9% of patients were diagnosed as having long COVID, with no observed difference between unvaccinated patients, those vaccinated with two doses of an mRNA vaccine, and those with more than two doses.
Long COVID was associated with older age, female sex, and hospitalization for the initial infection. It was inversely associated with infection during the Omicron period, the authors wrote.
Swift said that vaccines still play a role in preventing long COVID. “If you don’t get COVID, you don’t get long COVID," she said. "It remains the most important medical tools in our arsenal by virtue of not getting COVID and severe COVID, but we can’t stop there and say ‘if you were vaccinated, you don’t have to worry about long COVID.’”
Confounding factors and health behaviors Clifford Rosen, MD, a senior scientist at the MaineHealth Institute for Research, has reviewed studies on long COVID and vaccines. He said the current study may be skewed because of its sample size.
"It’s a small cohort that is relatively homogeneous and likely has different healthcare behavior than other EHR [electronic health record] studies," Rosen said. Instead, he said long COVID studies done based on Veterans Affairs (VA) data offer a more heterogenous cohort.
Ziyad Al-Aly, MD, chief of research and development at the VA St Louis Health Care System and a clinical epidemiologist at Washington University, has been behind most VA studies on long COVID.
He just published a review of evidence showing that vaccination reduces the risk of long COVID. While the effect size varies by 15% to 70%, there is an estimated average reduction of 40% to 50%, almost universally.
He said he found Swift’s study surprising and said it likely suffers from one main confounding factor: The type of patient who seeks out a long-COVID diagnosis likely uses healthcare and is vaccinated.
Al-Aly said vaccination may help reduce some clusters of long-COVID symptoms better than others. Fore maple, his work has shown a "profound effect in pulmonary symptoms of COVID, and less on metabolic effects on long COVID.”
Though more research needs be done on long COVID and vaccination, Al-Aly remains confident that vaccines play an important role in reducing the risk of long COVID.
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator#long covid
35 notes
·
View notes
Text
Q Fever
Aka, Query fever. What a weird name for a disease. Imagine telling people that's what you got.

in the 30s-40s, an Australian pathologist in QLD/Brisbane, came across an outbreak of the same or similar illness among abbatoir or slaughterhouse workers.
At the time, he called the disease "Q" fever or query as a temporary name until the pathogen could be identified. Unfortunately it stuck.
decades later, now nobel prize winner and virologist, MacFarlane Burnett isolated and identified the microbe responsible. I think this discovery contributed to his prize. i forget already.
Microbe responsible: Coxiella burnetti. Named for Burnett and HR Cox, the American bacteriologist who found the genus Coxiella where C burnetti falls under.
Initially they felt it was related to Rickettsia, responsible for Rocky Mountain Spotted Fever, but as science progressed, this was disproven.
Now for a Case Report
A 55 yo Italian man with a history of aortic valve replacement was diagnosed with pyrexia of unknown origin twice. Further signs included myalgias/splenomegaly/night sweats. The 2nd time he was admitted for PUO he deteriorated rather dramatically and was put on meropenem and teicoplanin.
A host of organisms was tested for on serological testing based on the man's travel and epidemiological history, all negative. Even a rheumatological panel was done, also less revealing. He also had a history of MGUS (a haem disoder), which is kind of a red herring here.
Cultures were negative, no vegetations were seen on a TTE - so they did consider IE. Which is an important differential for PUO.
Eventually a PET-CT was done (often favoured when investigations do not yield much for a sick patient with fevers), finally revealing a focus of infectious on his ascending aorta, where he'd also had previous surgery done. And in a round about way, they also further identified Coxiella Burnetti. He was treated doxycycline and hydroxychloroquine. As it's so rare in Italy, it wasn't really considered even though he mentioned rural travel.
Bottomline: Q Fever is an important consideration in the work up for culture negative IE. Further to this, always consider IE in the differentials for PUO particularly if they're at increased risk for IE (prosthetic valves, damaged valves, select congenital heart issues, previous IE). IE can present with night sweats, fevers, weight loss and splenomegaly. It can be insidious and chronic in nature. other risk factors can be more suggestive as we'll get into below.
Causative organism
Coxiella burnetti, it's a zoonoses - i.e. transmissible from animals. Special powers: very tough/hardy, can survive extreme environments (high temps and UV light etc.) over prolonged periods and is resistant to many common disinfectants/surface cleaners.
It's an intracellular pathogen and gram negative coccobacilli (PINK!)
name coccobaccili reminds me of cocopuffs.
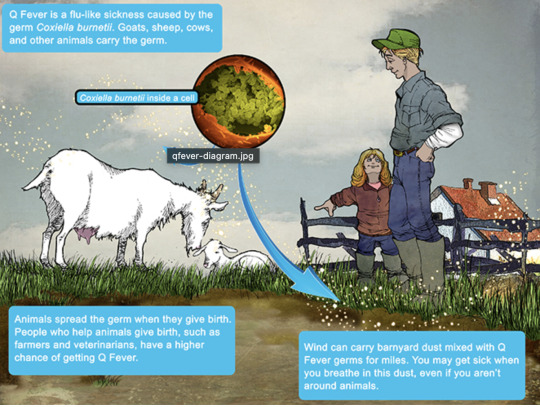
it's mainly associated with farm animals, which the CDC so wholesomely displays on its website on Q fever (wtf).

goats, sheep, cattle typically (but many other animals, even birds, dogs and horses can be reservoirs)
in particular bodily fluids - amniotic fluid, placenta, faeces/urine, milk etc.
you can get it through unpasteurized milk and through inhaling it if it lands on dust in the area
ever visit a farm or petting zoo lately? OMG WASH YOU HANDS.

That said, it's typically inhaled in inorganic dust. You inhale it, it goes to the lungs, and then the bloodstream.
Increased risk for Coxiella burnetti (What to take on history of exposures and when to strongly consider it)
live on a farm or near one
exposure to a farm
work as a vet on a farm
farm worker, dairy workers, researchers on these animals/facilities
slaughterhouse/abbatoir
Also from CDC:
Clinical presentation
Most won't get sick after exposure and remain asymptomatic, a very small minority does. even though it is highly infectious.
incubation time is 2-3 weeks (consider this time in your history of exposure, did they work on the farm 2-3 weeks ago as opposed to yesterday).
Nonspecific acute infectious symptoms:
nonspecific systemic fevers/malaise/arthralgias/myalgias--> key is high fevers though and can be associated with headache and photophobia.
non specific GI - N/V/diarrhoea
respiratory ones - SOB or cough, consider it as atypical cause of community acquired pneumonia.
rare: hepatitis and jaundice (granulomatous) or encephalitis with neurological complications such as demyelinating disease or CN palsies, also haemolytic anaemia and HLH (yikes)

really it's the history of exposure that will lead you down the garden path to Q fever.
Chronic Q fever is perhaps worse, and can present as culture negative IE/PUO. Months/years later, as B symptoms as above above + LOW/LOA, night sweats. More likely to occur if you are predisposed for IE as above, have a weakened immune system for any reason, including pregnancy.
Chronic Q fever has a mortality of 10% if left untreated. About <5% of those with acute Q fever develop this if left untreated. Speculation is that it's more of an autoimmune process or abnormal immunological response to the bacteria.
To be honest, most who walk in the door with community acquired pneumonia get treated empirically for atypicals anyway, (standard course of doxycycline), so we hardly really ponder the question of Q fever in every patient. But if they present chronically and did not have atypical cover at the onset of acute symptoms, then it's something important to consider.
Other important conditions - can cause complications in pregnant women and 20% will get post Q fever syndrome. like chronic fatigue.
investigations
Serology! nice and easy. Look for IgG antibodies in the chronic presentation. Or PCR. Down side to serology - can take 2-3 days for the body to make said antibodies to the bacteria for detection. PCR can be done on any fluids/tissue sent.
Cultures useless, hence it fall under the umbrella of culture negative (hard to grow outside a host cell, it is an obligate intracellular pathogen).
Other hints on bloods (as serology/PCR takes time to return) - elevated or low platelet's, transaminitis with normal bili, opacities in CXR with hilar lymphadenopathy, CSF will show raised protein levels if done when encephalitis is suspected.
imaging can also support the diagnosis.. as illustrated by the case report.
Treatment
Acute disease - as standard for atypical bugs, doxycycline 100 mg BD for 14 days. Alternatives - TMP SMX or Clarithromycin.
Chronic Q fever or IE:
native valves: doxycycline and hydroxychloroquine (200 TDS) for 18 months
prosthetic: same but 24 months
why hydroxy: enhances the action of doxycycline (increases the pH of the phagolysosome)
Follow-up: look for 4 fold decrease in IGG
Sources:
CDC
Stat Pearls
Wiki as linked above
#australian history#medblr#medblrs#infectious disease#infectious diseases#q fever#coxiella#coxiella burnetti
74 notes
·
View notes
Note
FOR MY ASK GAMEEEEE
1, 3, 4, 6, 12, 15, 20, 21, 23.
- @brutally-loving
Hi Krue! I’ll answer these for Zandik <3
1. What animal does your F/O remind you of?
A raven - for its intelligence, eerie presence and ability to pick apart mysteries with a sharp mind. And a shark - for the predatory nature, sharp teeth and the way he never truly stops moving forward, always hunting for knowledge.
3. What is your favorite hobby to think about doing with your F/O?
Experimenting together, though not always in a traditional, clinical way. He’s lost in his work, scribbling calculations at an alarming pace, muttering theories under his breath, and I, his most valued assistant, creation, and his wife, stand beside him - sometimes helping, sometimes teasing him for overworking himself. Maybe I’m lying on the operating table, allowing him to study me more, unafraid of his scalpel.
Philosophical debates over dinner are another hobby, an intellectual sparring that only strengthens the bond between us. And on rare, quieter evenings? Stargazing in the desert, lying on the cool sand, speaking of the fake sky, eternity, and how insignificant yet fascinating human life is. He'd scoff at sentimentality, but his gloved fingers would linger against mine just a second longer than necessary.
4. What chores would your F/O do around the house? Are there any they REALLY dislike?
Chores he would do around the lab:
organizing research notes and materials - Everything must be in its proper place for maximum efficiency. If a single document is misplaced, we can expect a dramatic reaction.
calibrating and maintaining equipment - If anyone else touches his machines, they’ll never do it right. Best to handle it himself.
overseeing test subjects (including myself) - Whether it’s monitoring data or making precise adjustments, he takes personal satisfaction in his work.
Chores he’d avoid like the plague:
cleaning up after experiments – Bloodstains? Shattered glass? That’s what assistants (like me) are for. He’s too busy refining theories to deal with the aftermath.
cooking and meal prep - If it isn’t something he can eat or drink quickly while working, it’s an inconvenience. He might forget to eat for hours, if not days, so cooking is my job.
laundry - He wears the same coat until it’s absolutely necessary to change it. One of his segments might handle laundry, but he certainly won’t.
Bonus: Chores he’d delegate to his segments:
“lesser” administrative work - One of his segments can handle mundane tasks like lab supply inventory, since he considers it beneath his time.
dealing with unimportant visitors - If someone dares to interrupt his work for trivial reasons, he has other versions of himself to shoo them away.
6. What kind of ringtone or notification sound would you have for your F/O?
Since I’m part of his hivemind, I don’t really need one, as we talk through telepathy a lot. Still, if my self-insert would have a phone, his voice saying “Ah… Did you think you could ignore me?” or something like that whenever he called would be funny (and make me a blushing mess).
12. What color do you associate with your F/O?
Light blue, like his hair!
15. What would your F/O get you for Valentine's day, if anything?
1) Zandik is all about his work and my relationship with him is no different - a gift that benefits us both is the perfect option. He might craft something personally tailored for me, like a specialized Geo-focused enhancement tool or a new experimental device that maximizes my powers (especially considering my sand abilities).
2) For him, the greatest gift he could offer would likely be knowledge. A private “lesson” on a forbidden or rare piece of research he’s been working on, something that could be either dangerous or highly advanced would be something he thinks would show me how much he cares. I’d learn more about his deepest interests this way.
3) He might also see the day as the perfect opportunity to “celebrate” by involving me in one of his most advanced and personal experiments yet - something that could challenge both of us, test the limits of my powers and deepen our bond in a scientific way. The experiment would be a way to bring us closer and prove the connection between us, perhaps by enhancing my abilities even further. “Gift” or not, it’s a test of love and intellect.
20. What're your F/O’s favorite personality traits of yours?
My intellectual curiosity, seeing that I’m equally interested in experimenting and expanding my limits, just like him. My ambition and determination to constantly improve and my dedication to furthering my abilities, especially considering how far I've come under his guidance, would be something he’s especially proud of. My independence, I don't simply exist as his assistant or test subject - I stand on my own and make my own decisions. I complement his need for control and precision. My ability to adapt and learn, as I’m the type who can absorb information, challenge him, and still stand firm in my ideas, which he’d view as a sign of strength. The fact that I've grown both emotionally and intellectually thanks to him makes him proud. My determination to challenge him - he’d find it incredibly stimulating when I challenge his views, question his methods or test the limits of his ideas. It shows that I’m not just a passive participant but someone who brings a unique perspective. It also means that deep down, I’m on his level, capable of thinking critically and independently. This appeals to his sense of superiority in a way that’s paradoxically flattering to him. He likes that I keep him on his toes.
The way I’ve survived his experiments and the resilience I show despite the pain and challenges I’ve faced also stand out to him.
21. If your F/O drew you, how would you describe the art piece?
If Zandik drew me, the art piece would likely reflect his meticulous nature and sharp attention to detail, with an almost clinical precision. I would be depicted with an air of otherworldly grace, perhaps standing amidst his laboratory's cool backdrop, with sand swirling at my feet or entwined around my form as a reminder of my powers. The lines would be clean and sharp, much like the precision with which he conducts his experiments. Every curve, angle and shadow would be deliberate, as though he’s trying to capture not just my physical form but the very essence of who I am - my power, my resilience and my complex bond with him. The color palette would be muted - greys, deep blues and maybe hints of warm sand tones.
23. What color would your F/O associate you with?
He’d likely associate me with a rich, deep shade of sand, a warm, earthy tone reflecting my Eremite desert heritage and connection to the sands. The sand, in his eyes, is a metaphor for my ever-shifting nature, how I can adapt, heal and even reform, much like the grains of sand that move and change shape yet remain a constant force in nature. He might see dark reds or crimson intertwined with that, representing my passion and the power he’s helped unlock!
7 notes
·
View notes
Text
Dealing With More Anti-Endos Invading Endogenic Spaces! This Time With a Dash of r/Systemscringe
This is just a straight-up lie.
While @thelunastusco did identify as endogenic at one point, that was a VERY long time ago.
I won't go into too much detail about this. You can see their response here:

Wait... are endogenic systems faking or not? 🤔
You seem like you're having a really hard time deciding.
If endogenic systems don't say they have a disorder, they literally can't be faking it.
If endogenic systems do think they have a disorder, then how would they be groomed into thinking they don't?
In the future, try your best to make a rationally coherent point.
Because you've clearly failed here.
Also, not what grooming is. Anti-endos, stop comparing endogenic systems to abusers.
Now, normally, I would go into the whole spiel of how actually endogenic systems are recognized by the majority of psychiatrists who have researched the subjects, by the World Health Organization, etc. But @cambriancrew already tried that, pointing to studies that have been done, and this was how @problematicpooch responded:

So essentially, don't trust the many, many professionals telling you endogenic plurality is real because some studies are wrong! 🙄
And WHAT RESEARCH HAVE YOU DONE?
Have you managed to find even one paper by a psychiatrist or psychologist anywhere stating it's impossible to be plural without trauma? Anywhere?
Because I think it's safe to say that our research is more valid than yours. Ours comes from respected doctors in the field. Yours comes from r/systemscringe. (Don't worry. I'm getting there.)
By the way, the Crew didn't say all studies need to be true if they're published. They said a book specifically peer reviewed and published by the American Psychiatric Association wouldn't have been published if the reviewers felt it contained untrue information.

Why are anti-endos always wanting to traumatize a bunch of children?
Why not just try testing alternative hypotheses for the formation of plurality?

Does anyone else get the feeling that anti-endos attack research into endogenic systems because they're scared?
"Research into endogenic systems is taking away from research into DID" is a pretty silly argument. A lot of research into DID and OSDD has been conducted by trauma specialists. Very little of the research into endogenic systems have been. Doctors who have traditionally focused on traumagenic plurality still are focused on that.
There's zero merit to the idea that this is taking away from research into DID in any way.
And again, the ICD-11, written by World Health Organization, is clear that you can experience multiple distinct identity states without a disorder.
The Hearing Voices Network has been fighting for the 80s to normalize that voice hearing isn't inherently pathological.
Just because someone has experiences similar to a mental illness doesn't mean they have a mental illness. Especially if the don't meet criteria for distress or impairment.

Okay... you know what... I AM going to whip out the ICD-11 here because I want to zero in on another part of this. In the criteria, for DID, you need to experience impairment in areas of functioning due to the disorder.

The DSM-5 has a similar criterion, worded as a requirement of "clinically significant distress or impairment" in important areas of functioning.
The ICD-11 contrasts this with non-aversive distinct personality states that aren't associated with impairment.

No, it's not ableist to say that DID is harmfull.
And the criterion I mentioned in the DSM is literally called the harm criterion, and establishes that a disorder can't be a disorder if it doesn't harm the person in some way.
Referring to dissociative disorders as being harmful isn't ableism. If they weren't harmful, they wouldn't be disorders. That's how disorders work!
Having other people in your head isn't inherently a disorder if it doesn't come with distress or impairment.
This doesn't mean that people with dissociative disorders are monsters. It just means they have a disorder that causes some for of distress or impairment.
Though maybe you, specifically, are.
r/systemscringe
After being torn apart, Problematicpooch ran to r/systemscringe where xe goes by u/Mikeyboi3000
Now, xe tried pulling this in the discussion with Cambrian too, who addressed it here:
Obviously, no correction from u/mikeyboi3000.
That would require a shred of intellectual honesty xe doesn't possess.
Anyway, while we're here, let's take a deeper look at the comments.

Casually accusing someone you don't of being an abuser while you have THAT as your flair is absolutely wild!
Also, they described symptoms the OP says are OSDD-1. At no point did the Crew actually claim OSDD isn't a disorder.

I think most people should have a general code of conduct for themselves. At least basic moral principles.
I would think it's weird that this person doesn't, but then I remembered that this is on r/systemscringe. Of course they wouldn't have any moral principles.

I don't think I've ever seen the Crew use that word for themselves. u/Mikeyboi3000 just stuck that in quotations for some reason.
By the way, if anyone's forgotten who u/sleep-bread-dough is, I debunked their r/systemscringe posts last week.
This is the user who makes system-friendly-sonas to pretend to be supportive of their system friends, and doesn't think DID systems should be allowed to work.

The problem isn't about consciousnesses.
While it may not be fair, if you're unable to hold a single member of the system accountable, then society's laws quickly break down.
Imagine if ghosts were real and could permanently possess someone. Ghosts start possessing people, and permanently are locked into those bodies. The ghosts then commit crimes. If you say, "well, we can't hold this person accountable because they're possessed," then they can commit more crimes without penalty.
If punishing a group is the only way to hold an individual accountable, then the whole group needs to be held accountable.
For example, if anti-endos routinely invade endogenic tags, crosstagging into our spaces, and they refuse to change and stay in their own corners when they're asked, then I have no choice but to crosstag my responses into their tags with the hope the rest of the anti-endo community can rein them in, punishing the entire group for the actions of an individual.
Maybe it doesn't seem fair, but sometimes things that seem unfair are necessary for maintaining order.
I think system responsibility is one of those things, where even if a system were made up of completely 100% separate people, all would need to be held accountable for the actions of one or nobody would be held accountable.
This wasn't the only post u/Mikeyboi300 made either after Tumblr arguments in the past few days. Xe also did one after being corrected by LunastusCo on their origins.
To anyone who may engage with this user, please be warned that doing so may result in them posting you to r/systemscringe in retaliation.
If you're worried about being posted on r/systemscringe, the best thing you can do is to block @problematicpooch.
#syscourse#pro endo#pro endogenic#anti endo#anti endogenic#sysblr#psychology#psychiatry#multiplicity#systemscringe#r/systemscringe#reddit#system stuff#systems#system discourse#actually plural#actually a system
64 notes
·
View notes
Text
Zero context WIP game ! Thank you @clawbehavior for the tag, excited to do this because I've got like 10 different wips and kept resisting the temptation to post snippets. These fics don't have definitive titles yet so the ones here are approximative descriptions
1. Ms Ji & the Kangs
“Yohan-ah, I love you, don’t cry” Isaac says, patting his baby brother’s stomach when he fusses. They’re both laying on Isaac’s bed after lunch, a bit drowsy in the early hours of the afternoon. Young-Ok watches the two as she folds laundry.
“Nanny, why does Yohan have no eyebrows ?” Isaac asks curiously.
She chuckles at the question, taking a tiny pair of socks out of the basket and folding them together. “Most babies are born without much hair, he’ll grow them later on.”
2. Conversations
Gaon swipes ‘accept call’ and props his phone against a utensil holder as Elijah’s lovely face comes into view. She has cut her hair into a bob, even bangs forming a curtain on her forehead.
“Gaon, it's an emergency ! You need to come to Geneva and do something !” Elijah’s voice immediately comes through the phone speaker, loud enough to be heard over the sound of meat sizzling on the stove. “Yohan is serious about growing that ugly mustache and the clinic receptionist keep trying to hit on him !”
3. Yohan through Isaac's photography
October 1991, Yohan showing me his teeth
Gaon chuckles at the photo. It’s blurry like the objective had gone out of focus at the last minute. Yohan is giving the camera a smile and scrunching his nose, eyes closed under his fringe like he’s shielding them from the flash. Some milk teeth are missing from his gums, two permanent ones just peeking above the surface. He must have been no more than six or seven here.
4. Gaon scrolls online forums
"Judge Oh, I have this file I wanted discuss with you"
Jinjoo comes up behind him to see just as he is about to unlock his computer. What greets Gaon after entering his password is the previous night's research topic brightly displayed on the screen. Shit. Carelessly, he had simply shut the laptop before going to bed, instead of closing the tabs and erasing his search history.
Panic and embarrassment seize Gaon on the spot. He's about two hundred-percent certain that Jinjoo got a glimpse of what was written on the screen. Omegaverse fanfiction of him and their boss. Gaon wants to explode.
"You have…a lot of open tabs, Judge Kim."
5. Another snippet from Conversations
“You have something under your eye”
“Hmm ?” Yohan hums, closing said eye when Gaon’s thumb gently swipes across his skin.
“Eyelash.” Gaon flicks it away “crap I should’ve told you to make a wish”
They’re laying on the couch in a tangle of limbs, Gaon on top of Yohan like a weighted blanket, chest to chest, book long abandoned on the coffee table. Kkomi is on the armrest behind Yohan’s head, sniffing at his hair. Gaon yawns into Yohan’s collar.
“We should go to bed.” Yohan says, voice hoarse.
6. Sunah lives
It is routine until her ears catch familiar voices, ones she thought she would never hear again, along with the cries of a fussy child.
“Gaon-ah, give her to me”
Sunah turns around to see, to her surprise, peering over the café’s balcony, Kang Yohan, his niece, his former associate, passing over an agitated toddler.
“I told you we should have brought her stroller,” Kim Gaon’s reprimands are a refreshing thing to hear “She gets tired.”
“It would have been inconvenient though, with all the stairs and narrow streets.” Kang Elijah chimes in. She is on crutches now, standing just a few centimeters shy of her uncle’s height.
“That’s fine” Kang Yohan hauls up the little girl against his chest so that her head rests on his shoulder, pats her back. “Appa will be the stroller today."
Tagging @thedeviljudges if you feel like doing it !
29 notes
·
View notes
Text
Questions Game!
Thanks for the tag @greenwitchfromthewoods 🥰
Do you make your bed? Normally my husband does since he works from home every day, but on the days I do, I will! I am a neat freak so I can't rest unless the bed is made
Favorite number? 2- I was born on April 2nd, started dating my husband on August 2nd, got married on July 22nd, 2 was always the jersey number I would pick whenever I played sports, 2 has just always been my favorite number!
What's your job? I work as a clinical research associate for a company that sponsors phase 1 trials of new cancer drugs! I basically just input a lot of data to a lot of different platforms so trials can stay up and running! I used to be an elementary school teacher, which there are parts that I really miss, but I'm glad to have a job that lets me keep my sanity a lot more 😅
If you could go back to school, would you? I have a masters and no money, so no, I'm good 🫡 If I could go back to the concept of college where you went to 2 classes a day, worked a part time job and had endless amounts of free time, then yes 😂
Can you parallel park? Don't ask me to parallel park or I will have a mental breakdown
Do you think aliens are real? Absolutely???? If you don't think so then????
Can you drive a manual car? No, and again, please don't ask me to, I will sob (can u tell I am an anxious driver)
What's your guilty pleasure? Drinking pop 😩 (or soda for all you non-midwesterners) I know it's so bad for you, and I barley ever have it, but when I do? Lord have mercy, I could drink like 17. Nothing slaps harder than a McDonald's coke
Tattoos? No, I am a big baby when it comes to pain and the most indecisive person I know, I don't think I could ever commit to something permanent on my body. I love tattoos on other people, though!!!
Favorite color? Yellow and sage green!
Do you like puzzles? Yes, but if they're not like, crazy complicated??
Any phobias? I'm an ✨anxious girlie✨ I don't really have an specific phobias, but I just worry a lot about something bad happening at any given moment?? Like yesterday at the gym, I was worried my house was going to set on fire because I was running the dryer while I was gone??? (yay intrusive thoughts!!!)
Favorite childhood sport? I played every sport under the sun as a kid- soccer, basketball, baseball, hockey, golf, swimming, gymnastics, dance, snowboarding, wakeboarding- I'd like to think I'm pretty athletic and I'm also very competitive 😬 I think my favorites were always baseball and hockey! Fun Madeline lore- I was a HUGE tomboy growing up and convinced my parents to let me play in a boy's baseball league from 4th to 8th grade. I was the only girl, and was actually pretty decent, but once everyone hit puberty and could throw 70 mph fastballs, I was like "yeah, I'm out" 😂
Do you talk to yourself? A concerning amount?? I am such a non-confrontational person, that any arguments I need to get off my chest, I just have with myself
NP tags: @honeyedmiller @raspberrybesitos @morallyinept @tightjeansjavi @itsokbbygrl
7 notes
·
View notes
Note
I sent this ask to a different blog but I don't think they're going to post it... I'm so sad, I'm screaming into the void. I'm scared. I'm sending to you because you're where I learned so much of this
Did i say anything wrong? I put so much work into this ask, I grabbed a screenshot partway through, so this isn't EXACTLY the same ask, but it's very close, I had to rewrite some.
from one DID system to another, please, hear me out, I'm desperate to be heard
Literally NO endos claim to have DID
There's like two, and they still say it's caused by trauma but they were systems first and later trauma made their system unstable
If endos want to demedicalize CDDs, why would they claim to have it? It's a roundabout way to achieve the same goal, it's just extra steps
Endos are literally fighting to get away from CDD spaces, do you actually see endos in the DID tag? The cdd tag? NO
They're in the plural tag, a word they choose to separate from the more clinically associated "multiple" of MPD, they're in the syscourse tags because they're allowed to participate, syspunk is less than a month old and it should be a meme at this point because they already had anti endo as a tag
They are literally saying they are systems that are UNRELATED to CDDs, not that they want to demedicalize being a system System doesn't belong to DID, look at IFS, psychological anthropology, or multiple theory of self, jungian archetypes, or does that mean we should be angry about "computer system" because it dehumanizes us?
And stolen terms? We know who came up with system hopping, it has never been used in RAMCOA. Do any of you actually know where tulpa came from? Like the actual word? Do you know who Alexandra David Neel is? The white woman who invented an imaginary practice that didn't actually exist (What she wrote about is not the same as Buddhist emanation), and created the word tulpa based on another white guy's mistranslation to entertain more white people during the Vietnam War?
So they have new words, they're trying to create more new words, there's so much real, actual research by real doctors into this phenomenon of nonpathological multiplicity in ways that exist outside of clinical psychopathology
The only overlapping word is "system
Plurals tend to get really upset when you use words like alter for them, they don't want to be medicalized at all, they understand what DID is and say, "| don't fit that description", and they're allowed to say that
If I, a DID system, feel I'm healed and integrated and choose to drop the DID label, no one can stop me, and we can't stop people from not picking it up to start with
Why can't anyone have actual conversations about this stuff, I'm so anxious because it seems like people are purposefully trying to misunderstand and lying about how bad the problem is
"Existing" isn't enough to qualify as misinformation, and it seems the only incorrect and unverifiable facts are coming out of the anti endo community.
I'm just so scared and sad.
I just want to know it's going to be okay
First -- I'm glad we can post this for you. I highly recommend screenshotting asks you send to people! It's helped me a lot with my paranoia in the past (did I send that on anon? Did I send that at all??) and it's a good record of your words for later.
Second.
I agree with you, I really do. This is so frustrating, and the self-described anti-endos who have recently flooded system spaces on tumblr are completely unwilling to look at the facts. They're obstinate and stubborn as mules, and unfortunately, that is not going to change. Most of them, if not all of them, are either children or caught in a current cycle of abuse with no way out. Most if not all are currently fighting for survival. They are not in a place to accept others; they can barely accept themselves.
People are purposefully ignoring information. People are purposefully avoiding it.
And it is not, and never has been, your job to fix their issues.
These are people who have always been unwilling to listen. They are children who cannot, for their own reasons, listen at the moment. For whatever reason, they are not in a position to accept endogenic plurality exists, and the more they are pushed, the more they will spit up their vitriol on the puke towel that is syscourse (or, worse, "syspunk").
It is sad. It can be scary. But it's not on your shoulders to fix them.
At the end of the day, you have to ask: what is most beneficial for me in this moment? Next, what is most beneficial for my family in this moment? Then, what is most beneficial for my followers in this moment? Then, and only then, are you getting to "beneficial for the tag to see," if you get there at all. The ask you sent them is lovely, and needed, but they are not ready to see this sort of thing, I can guarantee it.
That's why I'm glad it's here: so others can see it.
The last point I'll make is... Please make sure that you are valuing the correct things in your life, anyone reading this. If syscourse is stressing you out, please make sure to take appropriate breaks and check your brain. Remember that this is largely an online issue; the real world is quickly progressing to be more plural accepting and more accepting in general, and there are far bigger issues than an idiot crosstagging misinformation in a niche online discourse. I'm not trying to say this isn't an issue, and it should absolutely be spoken out about, but make sure to take care of yourself while you do. Anti-endos and pro-endos who are idiots online are not the end all be all of system activism. In fact, they rarely fit that definition.
Please do not let these places completely wreck you emotionally. You deserve so much better than that.
Sending love to all our followers; good luck staying afloat out there. <3
#Mod Quill#(But all of us love you all)#(Mwah)#syscourse#dude approved#kiss kiss#reading research is syspunk#debunk#you did good anon proud of you i hope you can relax tonight#happy Friday#pro syscourse conversation
13 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
Over the past few weeks, Dr. Hillary Cass has begun giving interviews in the United States to defend her report targeting transgender care. The Cass Review has faced criticism for its alleged anti-trans political ties, biased findings, promotion of conversion therapists, and poor treatment of evidence regarding transgender care. In an interview with NPR, Dr. Cass claimed that transgender individuals' care should be judged by their "employment," rather than their satisfaction with the care received. Later, during an interview with The New York Times, Cass misleadingly stated that she had not been contacted by any lawmakers or U.S. health bodies, despite having met with political appointees of Gov. Ron DeSantis to discuss banning trans care before her report was published. In response, both the American Academy of Pediatrics and the Endocrine Society have categorically rejected the review as a justification for bans on care and have challenged many of its alleged findings. In a statement released by the Endocrine Society, they reiterated that they stand by their guidelines around the provision of gender affirming care for transgender youth: “We stand firm in our support of gender-affirming care. Transgender and gender-diverse people deserve access to needed and often life-saving medical care. NHS England’s recent report, the Cass Review, does not contain any new research that would contradict the recommendations made in our Clinical Practice Guideline on gender-affirming care… Medical evidence, not politics, should inform treatment decisions.”
[...]
Similar sentiments were shared by Dr. Ben Hoffman, president of the American Academy of Pediatrics, who responded to the Cass Review, “What we’re seeing more and more is that the politically infused public discourse is getting this wrong and it’s impacting the way that doctors care for their patients. Physicians must be able to practice medicine that is informed by their medical education, training, experience, and the available evidence, freely and without the threat of punishment. Instead, state legislatures have passed bills to ban and restrict gender-affirming care, which means that right now, for far too many families, their zip code determines their ability to seek the health care they need. Politicians have inserted themselves into the exam room, and this is dangerous for both physicians and for families.”
Transgender care saves lives. A Cornell review of more than 51 studies determined that trans care significantly improves the mental health of transgender people. One major study even noted a 73% lower suicidality among trans youth who began care. In a recent article published in the Journal of Adolescent Health in April of 2024, puberty blockers were found to significantly reduce depression and anxiety. In Germany, a recent review by over 27 medical organizations has judged that “not providing treatment can do harm” to transgender youth. The evidence around transgender care led to a historic policy resolution condemning bans on gender affirming care by the American Psychological Association, the largest psychological association in the world, which was voted on by representatives of its 157,000 members.
Interestingly, Cass herself advocated against care bans in her most recent New York Times interview released today, where she stated, “There are young people who absolutely benefit from a medical pathway, and we need to make sure that those young people have access,” although she added a caveat that those young people should be forced to consent to research in order to access care, leaving many to question the ethics of such an approach. Regardless of Cass’s statements, her review is being used to justify bans in the United States and worldwide.
Both the Endocrine Society and the American Academy of Pediatrics came out to reject bans on gender-affirming care in the wake of the anti-trans Cass Review by Dr. Hilary Cass.
Dr. Cass herself advocated against bans on gender-affirming care in a recent New York Times interview; however, her report is being used as justification for bans on gender-affirming care worldwide.
See Also:
LGBTQ Nation: Cass Review author says leading medical org only supports trans health care under “political duress”
#Hilary Cass#Cass Review#Gender Affirming Healthcare#Transgender#Transgender Health#American Academy of Pediatrics#Endocrine Society
9 notes
·
View notes