#symptoms of vaccine injury
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text

#vaccine injury table#vaccine injury news#vaccine injury compensation in canada#vaccine injury uk#vaccine injury compensation data#vaccine injury shoulder#vaccine injury lawyers near me#symptoms of vaccine injury#canada vaccine injury support program#dtap vaccine injury#hpv vaccine injury#national childhood vaccine injury act#vaccine shoulder injury#vaccine related shoulder injury
0 notes
Text
its actually nuts how missing a single vaccination has shaped my entire fucking life. like not only would I not be deaf if I had gotten it on time but I probs wouldn't have adhd either 🫣
#like yeah I have a family history of adhd but im pretty sure the current model suggests u can be genetically *predisposed* but the actual-#development of adhd is thought to be closely linked to environmental 'triggers' like childhood stress or head injuries lol#or in my case brain trauma. fun fact: a suspected 62% of kids who survive hib meningitis later develop adhd symptoms#vs. 5% incidence in the general population.....#when I first heard that I was still in denial bc i thought of adhd as a 'natural' condition like ur just born that way#so if meningitis survivors displayed symptoms that didnt mean they were ACTUALLY adhd. except literally all adhd is-#is a collection of symptoms its not some tangible 'switch' thats flipped in some ppl and not others. maybe thats a rly obvious statement-#but I found it kinda hard to get my head around. i guess just bc of how a lot of psychology is viewed by the public innit#anyway being deaf + nd kinda fucking sucks yall better be jabbing ur babies with every vaccination possible or im coming for ur knees#its funny bc it sounds like im saying watch out !! vaccination may PREVENT neurodivergence NOT cause it !!#*andrew wakefield voice* u wouldnt want a child with autism#but thats not what i meaaaannn obvs ur kid not getting xyz disease that could kill them is the number 1 most important thing#its so cringe actually bc hib b incidence has been down to abt 2 in every 100 000 babies since the vax was introduced in 1985#so I was one of like. probably less than 10 babies to get it in the fucking country and they misdiagnosed me a bunch of times#bc it was so uncommon + I had some rarer symptoms plus the only way to actually CHECK is to test spinal fluid which is a faff#if theyd realised earlier then i also wouldnt be deaf bc it wouldnt have been as severe. just a series of unfortunate events i guess#anyway. immunology is so fascinating i wish id focused on it more in my degree tbh#over and OUT#.diaries
6 notes
·
View notes
Text
Anybody else have an instance where their shoulder was bent weird while doing something and it felt like it was out of place but you could still use it and popped it right back but now it does that same thing every once in awhile and you’re starting to wonder if you dislocated it and healed it wrong?
#emma posts#is this a super specific instance or do I share this experience with someone?#also should I see my doctor about it?#it’s been like a year so idk what she could do even if it was dislocated back then#it might have happened even earlier but I just remember it really fucking up while I was building a chair#I was holding something in place at a weird angle and pop! but then I put it right back#and I never lost the use of it during that whole thing and it only took two days to feel totally normal again#but it’s happening a lot more since that day. just not often enough for me to know what does it#I keep doing these things that it’s like ‘should I see a doctor? should I tell the nurse that looks at me once a week?’#and then I forget about it until something goes wrong again#my body just has a habit of fucking itself up and then going right back to normal again within a day or two#some stuff is extreme enough for me to go to the er or something like that kidney stone#but a lot of other weird injuries or symptoms that go away right afterwards I just feel like#what could my doctor even do about it? and then I have to schedule an appointment and get a ride and all that. ugh’#I do need to get an iud and vaccines soon though#I’m pretty sure I’m up to date on most vaccines but I’m not sure about the flu#I did go in last year and get two or three at a time to catch up with anything I missed or needed updated#it was mostly updating stuff like tetanus#I don’t know if there’s been a more recent covid booster from the last one I got I think a few months ago#but when I get an iud I need to schedule an appointment with my neurologist and that’s also annoying and takes time and finding a ride#and getting a ride there isn’t even going to somewhere in the same town! my general doctor is in this town#but apparently estrogen levels can effect one of my seizure medications so I would need a dose adjustment
0 notes
Text
(Original Idea)
@smokess

It’s been a few weeks since you first arrived in the Devildom. You’ve already made your way through a few of the rougher patches: learning the magic laws, getting used to demon food, and navigating the maze that is the House of Lamentation. But there are still moments when things catch you completely off guard, and today happens to be one of them.
You’ve just been called to the dining room for breakfast, but as you walk in, your thoughts are still buzzing from yesterday’s events. You’re trying to put together how you ended up in this bizarre world full of demons with their own customs, traditions, and... strange ways of doing things.
As you sit down, the brothers—Lucifer, Mammon, Leviathan, Satan, Asmo, and Beel—are already seated, along with Diavolo and Barbatos, who were visiting from the palace. The atmosphere is relaxed, almost too relaxed. They’re chatting, mostly about the latest human technology (Mammon is in a heated debate with Levi over the newest video game release) and general happenings in the Devildom.
But then, as you reach for your plate, your body betrays you.
You start sneezing, repeatedly. It’s not that unusual for you—back on Earth, you’ve had bad allergies before, especially in the spring. But here? You didn’t realize that it was possible for pollen from another dimension to mess with your system.
"Huh, bless you, I suppose." Lucifer comments, his tone a bit dry. He raises an eyebrow as you snatch a napkin and try to muffle another series of sneezes.
"Are you okay?" Beel asks, his voice sincere, though it’s impossible to ignore that he's already eyeing the plate of food in front of you, the steam rising from it. He’s always hungry, always concerned about food, and while you’re trying to focus on the allergy attack, his concern doesn’t help.
"I-I think it’s just my allergies," you manage to choke out between sneezes, your hand scrambling to find something to wipe your nose with.
Barbatos, ever the composed butler, immediately gets up and makes his way over to you with a tray of what looks like...some kind of odd, green liquid in a cup.
"Please drink this, MC. It should help soothe your reaction. We have a lot of unique flora in the Devildom, and they can affect humans in different ways."
You eye the drink with a mixture of suspicion and gratitude. At this point, you don’t really have any other choice.
“What... what’s in this?” you ask, sniffing it carefully.
“It’s a blend of herbs from the underworld,” Barbatos says with a calm smile. “Completely harmless. It should help with your symptoms. But you might want to avoid consuming anything too exotic until your body gets used to the local flora.”
You take a cautious sip. Surprisingly, the liquid doesn’t taste too bad, and within moments, your sneezing fits subside.
"Thanks, Barbatos," you say, giving him a grateful smile, but you're still mentally processing the fact that you might have to get used to demon herbs now.
“So, MC,” Diavolo begins, his voice loud and friendly as always, his large frame leaning toward you with genuine interest, “I wanted to ask, what kind of... ‘treatments’ do humans undergo back home?”
The question catches you off guard. You look around, noticing the brothers are now all paying attention—Diavolo's curiosity seems to have sparked a sudden group interest.
“Treatments?” you ask, hoping you understand the question right.
“You know, for things like... well, if you get sick, or need vaccinations?” Diavolo gestures, his enthusiasm barely contained. “It’s always interesting to hear how humans take care of themselves!”
You blink, processing the concept of vaccines. You realize that in the Devildom, none of these demons are likely familiar with things like flu shots or allergy medication... or even common human ailments like cold and flu. It’s a foreign concept here.
“Uh, well, humans get vaccinated—shots, you know, to prevent diseases? We also go to the doctor for stuff like fevers or injuries.” you say slowly, unsure if they understand what you're saying.
The room goes quiet. Then, unexpectedly, Mammon snickers.
"Wait, so ya all just get stuck with needles?" he asks, looking at you with wide, alarmed eyes. "Why would ya let someone do that to ya? Sounds like torture!"
You let out a small laugh, trying to explain it in a way they'd understand. "It’s for our protection. Without vaccines, we could get really sick from things we can easily avoid."
The demons all exchange looks of utter confusion. Satan looks thoughtful, though, his hand resting under his chin. “That’s... fascinating. So you just... accept being injected with something? No magical potions or healing spells?”
“Nope,” you answer, shaking your head. “Just medicine and stuff we get from the Earth. No magic involved.”
Diavolo claps his hands together in an amused gesture. “How strange! I wonder if that would work in the Devildom... Barbatos, what do you think?”
Barbatos, ever the pragmatic butler, raises an eyebrow. “I’m not entirely sure, My Lord. But I believe it would require a rather significant amount of effort. Perhaps we should stick to what we know works.”
You chuckle nervously, trying not to feel too alien. It’s weird being the only one who understands what vaccines even are, let alone periods, or allergies...
The conversation shifts after a while to other aspects of human life, which you’re not exactly prepared for. After some time, the talk turns to... well, other human customs—especially biological ones.
"So... do humans have... um... I don't know how to say this," Asmo starts, clearly not sure how to word it delicately. "Do humans, uh, have... ‘monthly’... discomforts?”
You freeze mid-bite, the word monthly hanging in the air like an uncomfortable weight. You’ve always been pretty private about your cycle, especially now that you’re in a room full of demons who probably know nothing about it.
“I, uh... it’s called a period,” you mutter, hoping the subject won’t get too awkward.
"A period?" Satan asks, leaning forward, eyes wide with curiosity. "Like... punctuation?"
“No!” you exclaim, mortified. "I mean... it’s a human thing. A... biological process." You sigh, trying to explain without sounding too embarrassed. "It’s a monthly occurrence where... my body, um, prepares for something it doesn’t need. So, it... uh... sheds the lining in the uterus."
The demons stare at you blankly. Even Lucifer, usually composed, looks momentarily baffled.
“And that... happens to you... every month?” Levi asks, horrified. “How do you... I mean, that sounds awful!”
You nod. "It can be uncomfortable. It’s like a... natural part of being human."
Barbatos, ever the tactful one, steps in smoothly, his voice calm. “It seems humans have a great deal to manage in their biology. Fascinating.”
“Right? And we’re just expected to deal with it,” you add, still feeling embarrassed but relieved that they’re not asking too many more questions.
Later, the conversation veers into a discussion about where you came from, your homeland, and your nationality. It’s a tricky subject, especially since most of these demons have never even heard of your country, let alone your hometown.
“So, you’re from Earth, right?” Lucifer asks, tapping his fingers on the table, as if contemplating the situation. “But Earth is so vast. How do you classify your people?”
You pause, unsure how to approach it. “Well, there are countries, and people belong to different nations. I come from a country called...”
The name of your country seems to hang in the air, but as you mention it, the demons exchange confused looks. They’ve never heard of it.
“Wait, so what’s that country like?” Mammon asks, genuinely curious. “What’s ya... currency? What’s the most popular food?”
You try your best to explain, but each question leads to another, and soon you realize how very, very different Earth is from the Devildom.
But as weird and overwhelming as this all is, you realize that these moments of confusion and surprise are part of what makes your time here so unique. The demons may not understand everything about you, but they're clearly invested in learning—whether it’s how to handle your allergies or what a "period" is.
And really, at the end of the day, it's that curiosity and willingness to understand each other that makes the Devildom feel a little more like home every day.
#x reader#obey me x gender neutral reader#obey me leviathan#obey me satan#obey me mammon#obey me lucifer#obey me asmodeus#beelzebub obey me#obey me diavolo#obey me barbatos#platonic#obey me lucifer x mc#obey me luci x mc#obey me luci x reader#obey me lucifer x reader#obey me lucifer x you#obey me mc#obey me brothers#obey me shall we date#obey me swd#obey me satan x reader#obey me x reader#obey me asmo x reader#obey me asmo x mc#obey me mammon x you#obey me mammon x reader#obey me mammon x mc#obey me beelzebub x reader#obey me beelzebub x mc#obey me levi x reader
499 notes
·
View notes
Text
Biology of Inkfish - Health
Notably, neocephalopods only possess an innate immune system and completely lack an adaptive immune system as seen in most fish - their immune systems are “non-learning”. This means that cephalings do not form immunities to diseases, nor do their immune systems protect them from diseases they have endured before. In comparison to organisms with an adaptive immune system, vaccines are redundant to cephalings, but on the positive side, allergies do not occur.
Common symptoms of disease in inkfish include headaches, changes in ink consistency, ink droughts, duller tentacle colors, muscle weakness, dizziness, wobbly movements and loss of appetite. Excessive ink bleed, low body temperatures, dry skin, fatigue, loss of coordination and general tiredness are also common symptoms of various infections. Sick individuals usually naturally seek out warm or even hot environments, and may spend excessive time in hot showers, underneath heated blankets or even the oven in ill-advised lapses of judgment. Raising the body temperature helps combat infection and beat illness faster, but can exacerbate symptoms of dehydration and be potentially dangerous to the brain and organs if not controlled.
Infections are easily transmitted through fresh ink or skin contact with other inkfish. As a result, infected inkfish are strictly banned from ink sports, as one Turf War with one infected player will almost certainly infect every player coming in contact with the ink.
Cephalings also encounter many conditions that aren’t necessarily caused by bacteria, such as cancers, muscle tears, beak chipping and growth abnormalities. Growth abnormalities may include quickly manifesting issues such as deep-sea gigantism or splitting or malformation of limbs. Abnormalities in limb growth most often occur when a limb is regenerating, but typically pose no risks.
An inkfish in poor health, mental or physical, will often have thin or droopy tentacles, reduced ink production and dull coloring. Some very common causes for these symptoms can be stress, poor mental health, very poor nutrition or disease.
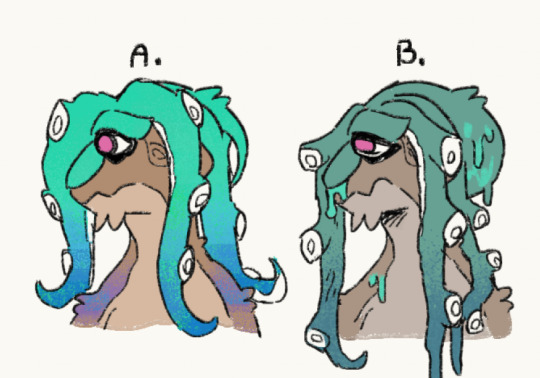
[The same inkfish when healthy (A) and when sick (B) exhibiting some common symptoms of illness. The most prominent symptom of any illness is desaturation of the skin.]
Regenerative Abilities
Cephalings are somewhat famous for their regenerative abilities and overall hardiness. Their bodies are incredibly flexible, and they have no bones - making them very impact-resistant. While they often sustain scratches and wounds thanks to their relatively thin skin, their regenerative abilities make up for many of their shortcomings.
In nature, neocephalopods would often lose limbs, from tips of the limbs to entire arms ripped off. This is a type of injury they are well adapted to, to the point that crown tentacles are even routinely cut off and minced for fashion purposes in the modern day. Wounds on the limbs bleed for a short time until the regenerative process begins; in inkfish, this window is even smaller due to ink bleeding out and helping to block the site of injury. Depending on whether the cephaling is healthy and gets proper sustenance, the limb often grows back in less than a year; in smaller species, it may grow back in even just a few months. Although cephalings can regrow their limbs as many times as they have to, it is quite common for mutations to occur, and the arm may split or grow in a strange shape.
Cephalings can regenerate a lot more than their arms - they can also regenerate parts of their organs, brains, and eyes to a lesser degree. Eyes can regenerate fully from shallow wounds, and partially from deeper wounds, to the point that an almost fully demolished eye can regenerate enough tissue to regain the ability to sense light. Minor brain- and heart injuries can also be regenerated, although with a higher margin of error with larger injuries that are still survivable. Damage to a branchial heart* is typically survivable, and the organs usually heal completely over time.
(* The branchial hearts are paired and are responsible for supplying blood to one gill each. Losing one entirely and surviving on just one gill is generally possible, although the reduced respiration poses some challenges.) Large injuries can still be lethal for cephalings. While losing one or more limbs isn’t particularly dangerous, situations where this happens as an effect of a predator attack often leave the cephaling unable to flee and thus cause them to get eaten. Injury to the systemic heart or the brain is also usually lethal within a short period of time. While they can regenerate limbs and organs, they are vulnerable to damage to the torso and mantle and are likely to perish from wounds that involve chunks being ripped off.
Common Ailments
Various ink infections. There are MANY kinds of infections that are caused when bacteria that really shouldn’t be in there get inside the ink sac. This typically causes atypical ink production and consistency, dizziness, possible body pains and ink droughts. Most ink infections are easily identified and are treated with antibiotics or gel that absorbs into the ink veins.
Ink bleed. A state in which ink bleeds out of the ink sac and the body involuntarily. It’s typically caused by the ink ducts being open involuntarily and abnormally, the body producing too much ink, the ink produced being too runny or a combination of several factors. It is usually a symptom of illness or abnormality of the ink sac.
Ink drought. The opposite of ink bleed. An ink drought is a condition where the ink sac produces much less ink than normal, or even none. It usually leads to issues with the muscles and upright posture due to low ink pressure, and usually leads to problems of the ink vein system and dry skin if left untreated.
Poisoning or Envenomation. The most common cases of poisoning are from contact with poisonous creatures, skin contact with chemicals, or from toxin accumulation in seafood. Symptoms of poisoning vary VERY widely based on the toxin, affected species and the amount of toxin absorbed, ranging from mild discomfort and lightheadedness to paralysis and rapid death.
Hypothermia. Low body temperatures are a very common problem within cephalings, especially during colder months. They can be caused by being in environments that are much too cold or consuming too much cold food or drink. Symptoms include drowsiness, shivering, weakness and lethargy. The treatment is simple and consists of warming up the patient, although this should be done gradually.
Malnutrition. Malnutrition is a bigger issue among cephalings than one would assume, and is often caused by either too little food altogether, or not enough meat being consumed. As a lot of modern street food is mostly carbohydrates and is vegetable-based, the overall consumption of meat can dip very low for some cephalings despite their carnivorous nature. Common symptoms include loss of muscle, tiredness and irritation, lightheadedness, consistent hunger, decreased ink production and stunted growth (typically in juveniles).
Muscle weakness. Issues stemming from muscle weakness are very common in cephalings, especially inkfish, which derive a lot of their stability from ink flow. Since cephalings lack real bones, any excessive weakening of the muscles can result in rapid loss of walking and standing ability. Significant loss of muscle function may result from general long-term inactivity, illness, malnutrition, low ink pressure or low ink levels and is quite common. Even slightly extended periods of inactivity or illness sometimes require people to depend on external mobility aids afterwards, and canes especially are a widely used option for countering muscle weakness both short- and long term. Some inkfish counter significant muscle weakness by abandoning bipedalism altogether and turning to spending most of their time in swim form. Some forms of muscle weakness prevent switching between forms altogether, though this occurs mainly in people who stop switching forms for an extended amount of time.
Ink pressure issues. An inkfish’s ink system pulses ink around at a somewhat consistent rate, keeping up the natural flow. An absence or overabundance of ink, ink infections, illness, stress and anxiety as well as a myriad of other things may cause ink pressure to be higher or lower than normal. High ink pressure typically causes restlessness, stiffness and ink bleed, whereas low ink pressure causes wobbliness and unstable movement, lethargy, muscle pain and reduced stamina.
Beak issues. Cephaling beaks grow slowly but indefinitely and need to routinely be filed down if not naturally worn down. If the beak isn't used enough to naturally even out from use, one may run into beak overgrowth. For most people, mild beak overgrowth isn't an issue, and parts of the beak sticking out of the mouth is generally considered inconsequential. More advanced beak overgrowth can become problematic by digging into parts of the buccal mass and causing infections and making eating difficult. This typically occurs with individuals who have fear regarding beak procedures or healthcare. Other common issues with the beak include beak misalignment and brittleness of the beak.
Radular decay. Radular decay occurs when bits of food are stuck between or under the radular teeth, causing infection, and is more common with plant-based food sources. It is prevented by regular cleaning or brushing of the radula. Mild forms may be limited to radular pain and occasional bleeding, but severe radular decay may require the radula to be removed, which significantly limits a cephaling's diet. For perhaps obvious reasons, radular decay is not of significance for species that have no radula.
Sucker infections. Infections of the suction cups are most prevalent in squid, which have chitinous sucker rings which can trap muck, grime and other particles between the ring and fleshy tissue. Alternatively, hooks or rings can grow incorrectly or overgrow if not maintained and dig into the flesh, causing infection. They occur more commonly in people who regularly use their suckers and get them in contact with different things, but often fly under the radar for people who use their suckers for touch-based things less and thus assume that sucker care is irrelevant. Infections of the sucker usually cause pain, bleeding, dryness and potential shriveling up of the infected suckers, where severe infections can cause individual sucker necrosis and spread to the whole limb. Crown tentacle infections are particularly dangerous in that the infection can easily spread to the brain. In situations where a sucker is badly infected, it is typically precautionary to remove the sucker, a part of the limb or the whole limb, as it is often safer and more convenient to replace an inflamed sucker than it is to wait for infection to subside.
Conditions and Mutations
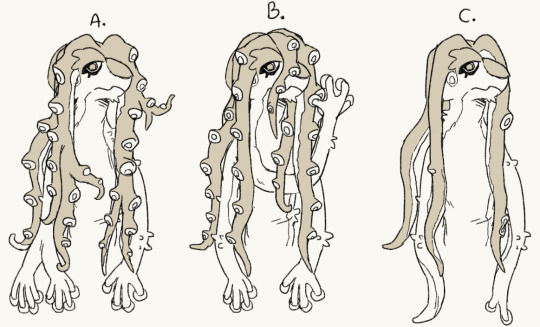
[Three common limb mutations, the most common types of significant mutation among cephalings. Limb mutations can occur as part of a genetic condition or by chance during regeneration of a limb. With the modern prevalence of tentacle cutting, it is said that up to 40% of limb regenerations involve some form of mutation. Pictured are A. branching, B. anemonism and C. blanking.]
White Beak. The color of the inkfish beak especially varies greatly in its ratio of black and white. While the base of the beak is always pale, ancestral squid and octopus beaks were mostly dark in the exposed area. In modern inkfish, a common mutation makes the beaks almost entirely pale, which also has the effect of them being softer in comparison. In the current day, predominantly white beaks are more common than black beaks are, although the majority of people will have some form of gradient in beak color and hardness. In a big part of the population, this comes with a larger risk factor for beak chipping and limitations for food hardness, though it also reduces the risk of beak overgrowth in comparison to black beaks. Brittle beaks are usually treated primarily with a threshold for maximum food hardness and beak polish to protect the surface of the beak, whereas beak chipping is usually handled by attaching artificial parts to the beak to shield it during regrowth or filing the rest of the beak to be level with the chipped segment. Cracks in a beak can be filled in with a hardening filler substance that conceals the crack and strengthens the beak.
Color Lock. Some cephalings are born without some of their ink sac chemicals, which limits the colors of ink they can mix - some extreme cases are limited to just one color. Aside from the inconvenience of having limited ink colors, the mutation is harmless. In some cases, people may choose to treat color lock by ingesting dyes to color their ink to whatever the situation calls for. Sometimes, color lock can be caused temporarily by a disease or underlying health condition, but permanent color lock is only genetic.
Ink Wither. A condition in which the ink sac produces very little ink, and may stop producing ink completely. It causes permanent ink drought, though ink drought on its own is usually a temporary symptom caused by a myriad of things. Although ink wither usually exists from birth due to unusual development of the ink sac or other related complications, it is sometimes caused when an ink drought caused by other triggers, such as disease, dehydration, bacterial infections or malnutrition, is prolonged and becomes chronic. It is treated mostly through artificial ink refills, ink soak therapy* and external mobility aids due to low ink levels often causing complications with stability.
(*Ink soak therapy is a treatment in which an inkfish bathes in a shallow tub or dish of ink. Prolonged contact with large amounts of ink has been proven to stimulate the body's own ink production, so it is an effective remedy for some instances of ink drought and also helps absorb ink into the system.)
Ink Boom. An opposing condition to ink wither in which the ink sac produces excessive amounts of ink and continues to do so even when full. It usually co-occurs with chronic ink bleed. The severity of the condition determines difficulty of the treatment; in cases of slightly above-average ink production, attention to hydration and sufficient purging of ink throughout the day may be enough to manage the condition, whereas high-producing cases may require constant monitoring and frequent hospital stays. In most affected people, the severity of the condition varies on environmental or other factors and may come in episodes. Ink boom is a condition often developed by long-term ink battlers due to frequent usage of large amounts of ink, but may develop throughout childhood or in adulthood, where it most often develops from substance use or stress. Typical symptoms include comorbid chronic ink bleed, stiffness, swelling under the skin, dehydration, malnutrition and restlessness. Treatments include purging of excess ink to avoid buildup, monitoring hydration and nutrition levels, medications to relax the ink sac or, in extreme cases, removal of the ink sac, which imposes dependence on externally sourced ink but eliminates the root cause. Ink boom sometimes occurs temporarily as a comorbidity to various health complications, and is sometimes a precursor for progressing into ink wither later in life.
Branching. Branching is a state where the limbs split and branch at the ends to form new ones continuously. Branching can be developed at birth, upon which it is typically permanent. A person with branching will typically have their limbs split into two or more growths upon the tip being cut off, or a new branch may start growing out of a non-injured limb arbitrarily. It can affect all the limbs or just some of the limbs, but an inkfish with genetic branching will always develop branches on a limb, even if cut off and regrown, although the size and position of the branching may change and vary. In individuals where only some limbs are affected, cutting off an unaffected limb will typically spread branching to that limb upon regrowth. Consequently, there are many people that are unaware of having the condition due to having no external traits until a limb is first regenerated. Some people may develop temporary branching as a result of stress, or randomly while regenerating a limb. Branches can be removed by cutting off branches and burning the root tissue to prevent regeneration, although this is done primarily for cosmetic reasons due to branching of the limbs being generally inconsequential health-wise.
Anemonism. A common genetic mutation that causes more than the usual amount of limbs to form. In most cases, it manifests in the form of additional crown tentacles, but there are sometimes extra arms or legs. The rarity goes up with the amount of extra limbs present; it is quite common for inkfish to have one or two extra crown tentacles, for example. It differs from branching in that the new limbs originate straight from the body with complete or partially complete muscle groups, rather than branching off from an existing limb. New limbs do not grow in later in life, although the onset depends on the type of anemonism; additional locomotive limbs are present from birth, whereas additional crown tentacles will grow in with the rest of the tentacle crown. Conditions where one or more of the limbs or crown tentacles are absent are considered a subset of anemonism, usually referred to as reverse anemonism.
Blanking. A somewhat rare condition which causes less or no suction cups to form, resulting in greatly reduced amounts of suckers and a signature “blank tentacles” look. It is usually present from birth, although similar effects may occur in regenerated limbs for people without the condition. It affects both the crown tentacles and the graspers; some people may only have a few suckers, some people may have none at all, and it may affect different limbs disproportionately or only affect some of the limbs. It is most noticeable in octolings, although it occurs in all sucker-bearing cephalings. In decapods, it often causes the tentacular clubs to form in unusual shapes or not form at all, and commonly results in oddly shaped or missing sucker rings. People with the condition often have comorbidities affecting the suckers, such as splitting, asymmetry, stunted development of the sucker or dulled chemoreception. For people with blanking, cutting off and regenerating limbs still produces reduced suction cup numbers, and developing other regenerative limb abnormalities is quite common. It is a condition that doesn’t require medical treatment, although people for whom it affects the graspers may benefit from specialized equipment for fingerless species.
General Limb Abnormalities. Extra limbs, missing limbs, extra suckers or missing suckers, limbs with no hand or multiple hands per limb - the list goes on. There is a plethora of limb abnormalities within neocephalopods, and they are not actually that uncommon; roughly one in 5 inkfish has something of the sort at some point of their life. Oftentimes, extra limbs, suckers or arms are at least partially or even fully functional. Many limb abnormalities are permanent and present from birth, while the most common ones can develop at any time, usually resulting from damage to a limb. People with one type of genetic limb abnormality are also likely to have other coexisting conditions; for example, anemonism and blanking often co-occur.
Kraken Syndrome. Kraken Syndrome is a psychological condition where the Kraken response* triggers dangerously easily. This condition occurs when the body is conditioned to frequent Kraken transformations to the point where the brain becomes exponentially more receptive to triggers for Krakening and thus dramatically lowers the threshold for natural Kraken episodes to occur. When this threshold is low enough, the Kraken is triggered abnormally easily and Kraken Syndrome is diagnosed. It is treated mainly with exposure therapy, mood stabilizing medication, depressants and sedatives, and specific medications that induce fatigue or physically weaken the body enough to prevent physical Krakening. It is highly comorbid with anxiety disorders, which also often function as triggers. Kraken Syndrome became widely documented in the late 2010’s, almost uniquely among frequent users of the Kraken special weapon. It is not to be confused with the rare condition where the Kraken form is able to be triggered at will with no psychological effects; this is not a type of Kraken Syndrome as it involves a voluntary transformation as opposed to a lowered threshold for involuntary uncontrolled transformations.
(* The Kraken response occurs with the fight-of-flight response of inkfish and correlates with a threshold of emotional distress that triggers the transformation. During a Kraken transformation, the inkfish becomes aggressive and disoriented, ink production is drastically increased, ink builds in the muscles and tissues increasing the individual's size, and a deimatic display is forced, often creating a high-contrast pattern. It isn't a panic reaction in itself and not all panic reactions inherently lead to a Kraken episode, but some degree of extremely high anxiety and desperation or anger are mandatory for a Kraken to trigger. The threshold that a Kraken triggers tends to vary based on person, but it generally requires an extremely high-stress situation with imminent threat. In general circumstances, the average inkfish will probably Kraken zero to three times in their life.)

[An image detailing the differences between typical emotional agitation required to trigger the Kraken response between unaffected individuals and those with Kraken syndrome. The special charge state is considered the basic state of agitation when special weapons become usable due to increased metabolic rates and high ink production. The Kraken response is typically far above the average person's typical agitation levels and triggers only in extremely dire situations. Usage of the Kraken drug for Turf Wars artificially lowers that threshold for the transformation itself to roughly the same threshold as the special charge state. Frequent transformations under the influence of the drug do not trigger the psychological disorientation and other effects of the Kraken, but they are still generally detected by the body and brain as an emergency situation, which lowers the natural threshold for natural Krakening over a long period of transformations to compensate for frequent threats. This causes an effect where even minor agitation may trigger the brain into a full-blown Kraken transformation in response to a nonexistent threat and is the case for people with Kraken syndrome. High-strung Kraken syndrome is diagnosed when the threshold for Krakening is so low that it co-occurs with the natural special charge state of the individual or even before that emotional threshold.]
Deep-Sea Gigantism. Shortened often to DSG, deep-sea gigantism is a sudden growth spurt caused by high long-term stress levels. It is a defensive response to unfamiliar or threatening life situations, mostly fueled by hormonal changes in the body in the long term. DSG gets its common name due to its prevalence in people moving in or out of the Deepsea, in which case it is often triggered by extreme change in pressure levels, disorientation through change in environment and general stress of moving, which captures a lot of common triggers for the condition. The name isn’t to say that the underground or -water are the only conditions where it occurs; it may occur as a response to any type of long-term stress, anxiety, frequent threatening situations or even some medications. The main symptom of deep-sea gigantism is unnatural, accelerated growth that might be dismissed in the short term and only becomes apparent within the span of months where it becomes clear that the pace is abnormal, and it is common to outgrow the typical size estimates for one’s species under long-term DSG. Other symptoms include increased hunger and appetite, fatigue, rapid muscle gain, headaches and general disorientation. The condition may be self-fueling due to the body directing most of the energy into growth and thus causing potential deficiencies elsewhere. Long-term instances of DSG with significant growth may also cause issues and comorbid conditions to develop due to the growth of the body and the growth of the organs and ink sac often being disproportionate. Deep-sea gigantism differs from regular gigantism in that it is a temporary (albeit often long-lasting) condition that has external triggers as opposed to a permanent condition. It is typically treated with anti-stress medication, eliminating underlying root causes, and limiting energy intake. Short periods of DSG often go entirely unnoticed, but longer periods are highly problematic due to the increase in body size not being reversible.
Hyperchromatophorism. Casually referred to as hi-chrom, it is a type of hyperpigmentation that causes chromatophore amounts in excess and causes the skin to be abnormally brightly colored in adult individuals where chromatophores are typically sparse. It is different from late onset of mature chromatophore sparsening due to the density of chromatophores being drastically higher to begin with. Usually, hyperchromatophorism is present from birth and affects either the whole body or large areas of the body, causing vivid colors and patterns to display across the whole body or areas of the body rather than just the crown tentacles. The intensity of these colors depends on the individual, and the condition may be light and only cause slightly increased saturation in parts of the body, or it can cause the entire body to be a solid color. It is mirrored by hypochromatophorism, which is a partial or complete lack of chromatophores in an area, and is about as common as the former but less noticeable due to mainly being visible in the crown tentacles. Either condition can occur in people without the conditions in areas where skin regenerates, and is quite common with large wounds.
Chronic Ink Bleed. Chronic ink bleed is a condition where excessive amounts of ink seep through the skin and the ink ducts are permanently, or predominantly, open. It is a consistently repeating or constant presence of the ink bleed condition which varies in severity based on whether the ink ducts are permanently open or only frequently open. Chronic ink bleed almost always co-occurs with chronic dehydration, low ink levels, malfunctions of the ink sac and ink system and mobility issues stemming from ink loss. It is usually managed with means that prevent or lessen ink evaporation; absorbent body wear, lotions that clog ink ducts around the skin or other medications that force the ink ducts to close, or alternatively frequent ink refills often administered by portable machines intravenously. Inkfish with chronic ink bleed often fare poorly in areas with dry air. Significant and long-lasting ink bleed is often a symptom of illness, and it may turn chronic after severe episodes of sickness. Chronic ink bleed can be a birth condition or it may develop later in life; late onset is often seen in professional Turf War players. It may also develop as a side effect of medication, unrelated illness, high stress or anxiety levels or hormonal imbalance, although in these cases it is typically reversible.
Color dysfunction. Color dysfunction is a condition where the color-changing skin cells aren’t under conscious control, and cycle colors randomly. It doesn’t apply to dead or inactive chromatophores as the affected cells are alive and active, but the ability to control them is absent, limited, or leads to inaccurate displays. Cephalings with the condition have highly variable skin patterns, from constantly cycling colors in no particular order, spontaneous deactivation or activation of the skin cells, or colors that somewhat correlate with emotion or activity but still have no conscious control. People with color dysfunction may have it across the entire skin, or it may be isolated to specific patches of the body while other areas have controllable pigment cells. It may also develop in areas where skin regenerates for people that do not have it as a pre-existing condition. It is most often present from birth, but sometimes develops later in life in response to stress, brain damage or psychological conditions, where it may be permanent or subside with time. Symptoms also often arise temporarily as a response to drugs, medications or high stress situations. Color dysfunction has a high occurrence rate alongside different psychological conditions and is presumed to be a mismatch of electrical signals in the brain to what is actually displayed on the skin, or overall dysfunction of the center that dictates color change.
Color stasis. Color stasis is a subtype of color dysfunction where the color-changing cells are alive but permanently deactivated involuntarily. It differs from chromatophore atrophy or chromatophore death in that cells are not dead, but deactivated. It is caused by inactivity of the brain center in charge of color change, whether that is due to an absence, partial inactivity or nerve damage to parts of the body or brain. It can be present from birth or develop later, typically due to brain damage or substance abuse. It may also extend to all skin or only be present in select areas or patches of skin. People without the pre-existing condition sometimes develop individual patches of color stasis in areas where skin regenerates.
194 notes
·
View notes
Text
PROOF THAT COVID VACCINES DAMAGE COGNITION
We Now Have Proof That The COVID “Vaccines” Damage Cognition
Countless people have observed their loved ones becoming “more compliant” and “broken” after the shots.
This was deemed a “conspiracy theory,” but now we have the data to back it up.
A new study from South Korea analyzed the electronic health records of 2.2 million and later 4.3 million individuals in Seoul. What researchers found was alarming.
By comparing the rates of various new medical conditions in vaccinated versus unvaccinated groups over three months, the study revealed that the vaccinated experienced:
A 68% rise in depression
A 44% surge in anxiety and related disorders
A 93.4% increase in sleep disorders
A staggering 138% jump in mild cognitive impairment
A 23% rise in Alzheimer's disease
Dr. Pierre Kory writes:
“In my practice of treating vaccine injuries, one of the three most common symptoms I see is brain fog. So many of my patients had been in the prime of their lives, can now barely function, have significant cognitive impairment and need a lot of help from our nurses to carry out their treatment plans. I never imagined I would see any of this in people far younger than me and instead I see it every day. I bear witness to an immense amount of suffering on a daily basis that is hard to put into words.”
-----------------------------------------
As I have stayed in several of my previous posts, I believed that the government had our best interests at heart and I received all 4 of the 1st round of COVID vaccines. Besides heart issues that suddenly appeared (AFib, flutter), I agree that there has been more brain fog and a cognitive as well as a physical decline since I received those vaccines. It is a sad day when we can no longer trust what our government tells us. Remember, knowledge is power and we need to question EVERYTHING they tell us!
#the great awakening#wef#world economic forum#government corruption#fjb#democrats#joe biden#illegal immigration#bill gates#donald trump#covid vaccine#question everything
532 notes
·
View notes
Text
COVID-19's long-term effects on the body: an incomplete list
COVID’s effect on the immune system, specifically on lymphocytes:
NYT article from 2020 (Studies cited: https://www.biorxiv.org/content/10.1101/2020.05.18.101717v1, https://www.biorxiv.org/content/10.1101/2020.05.20.106401v1, https://www.unboundmedicine.com/medline/citation/32405080/Decreased_T_cell_populations_contribute_to_the_increased_severity_of_COVID_19_, https://www.medrxiv.org/content/10.1101/2020.06.08.20125112v1)
https://www.biorxiv.org/content/10.1101/2022.01.10.475725v1
https://www.science.org/doi/10.1126/science.abc8511 (Published in Science)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9057012/
https://www.forbes.com/sites/williamhaseltine/2022/04/14/sars-cov-2-actively-infects-and-kills-lymphoid-cells/
https://www.cleveland.com/news/2022/10/in-cleveland-and-beyond-researchers-begin-to-unravel-the-mystery-of-long-covid-19.html
SARS-CoV-2 infection weakens immune-cell response to vaccination: NIH-funded study suggests need to boost CD8+ T cell response after infection
https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/lymphocytopenia
https://thetyee.ca/Analysis/2022/11/07/COVID-Reinfections-And-Immunity/
Dendritic cell deficiencies persist seven months after SARS-CoV-2 infection
https://www.frontiersin.org/articles/10.3389/fimmu.2022.1034159/full
https://www.n-tv.de/politik/Lauterbach-warnt-vor-unheilbarer-Immunschwaeche-durch-Corona-article23860527.html (German Minister of Health)
Anecdotal evidence of COVID’s effects on white blood cells:
https://twitter.com/DrJohnHhess/status/1661837956875956224
https://x.com/TristanVeness/status/1661565201345564673
https://twitter.com/TristanVeness/status/1689996298408312832
Much more if you speak to Long Covid patients directly!
Related information of interest:
China approves Genuine Biotech's HIV drug for COVID patients
COVID as a “mass disabling event” and impact on the economy:
https://www.ctvnews.ca/health/report-says-long-covid-could-impact-economy-and-be-mass-disabling-event-in-canada-1.6306608
https://x.com/inkblue01/status/1742183209809453456?s=20
COVID’s impact on the heart:
https://www.dailystar.co.uk/news/world-news/deadly-virus-could-lead-heart-31751263 (Research from: Japan's Riken research institute)
https://www.brisbanetimes.com.au/national/queensland/unlike-flu-covid-19-attacks-dna-in-the-heart-new-research-20220929-p5bm10.html
https://www.mdpi.com/2077-0383/12/1/186
https://medicalxpress.com/news/2023-04-mild-covid-effects-cardiovascular-health.html
https://publichealth.jhu.edu/2022/covid-and-the-heart-it-spares-no-one
https://www.bhf.org.uk/informationsupport/heart-matters-magazine/news/coronavirus-and-your-health/is-coronavirus-a-disease-of-the-blood-vessels (British Heart Foundation)
COVID’s effect on the brain and cognitive function:
https://www.openaccessgovernment.org/article/brain-infection-by-sars-cov-2-lifelong-consequences/171391/
https://www.cidrap.umn.edu/covid-19/study-shows-covid-leaves-brain-injury-markers-blood
https://www.theguardian.com/world/2020/jul/08/warning-of-serious-brain-disorders-in-people-with-mild-covid-symptoms
Cognitive post-acute sequelae of SARS-CoV-2 (PASC) can occur after mild COVID-19
Neurologic Effects of SARS-CoV-2 Transmitted among Dogs
https://journals.lww.com/nsan/fulltext/2022/39030/neurological_manifestations_and_mortality_in.4.aspx
https://www.salon.com/2023/06/17/new-evidence-suggests-alters-the-brain--but-the-extent-of-changes-is-unclear/
https://www.scientificamerican.com/article/covid-virus-may-tunnel-through-nanotubes-from-nose-to-brain/
https://neurosciencenews.com/post-covid-brain-21904/
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(22)00260-7/fulltext
https://medicalxpress.com/news/2022-08-covid-infection-crucial-brain-regions.html
https://news.ecu.edu/2022/08/04/covid-parkinsons-link/
Covid as a vascular/blood vessel disease:
https://www.salon.com/2020/06/01/coronavirus-is-a-blood-vessel-disease-study-says-and-its-mysteries-finally-make-sense/
https://www.salon.com/2023/12/27/brain-damage-caused-by-19-may-not-show-up-on-routine-tests-study-finds/
https://www.nih.gov/news-events/news-releases/sars-cov-2-infects-coronary-arteries-increases-plaque-inflammation
https://www.mdpi.com/2077-0383/12/6/2123
https://www.sciencedaily.com/releases/2021/10/211004104134.htm (microclots)
Long Covid:
Post-COVID-19 Condition in Canada: What we know, what we don’t know, and a framework for action
https://www.ctvnews.ca/health/coronavirus/more-than-two-years-of-long-covid-research-hasn-t-yielded-many-answers-scientific-review-1.6235227
https://www.cbc.ca/news/canada/london/cause-of-long-covid-symptoms-revealed-by-lung-imaging-research-at-western-university-1.6504318
https://www.cbc.ca/news/canada/montreal/long-covid-study-montreal-1.6521131
https://news.yale.edu/2023/12/19/study-helps-explain-post-covid-exercise-intolerance
Other:
- Viruses and mutation: https://typingmonkeys.substack.com/p/monkeys-on-typewriters
Measures taken by the rich and world leaders
Heightened risk of diabetes
https://jamanetwork.com/journals/jama/fullarticle/2805461
https://www.nature.com/articles/d41586-022-00912-y
Liver damage:
https://timesofindia.indiatimes.com/city/mumbai/46-of-covid-patients-have-liver-damage-study/articleshow/97809200.cms?from=mdr
tl;dr: covid is a vascular disease, not a respiratory illness. it can affect your blood and every organ in your body. every time you're reinfected, your chances of getting long covid increase.
avoid being infected. reduce the amount of viral load you're exposed to.
the gap between what the scientific community knows and ordinary people know is massive. collective action is needed.
#putting this somewhere at least as reference for... somebody hopefully#covid#disability#y'all. it is bleak out there but some very good people are doing their best to help#we need as many people aware and helping as possible
464 notes
·
View notes
Text
Quick aside: The people claiming they have Long Covid because of covid vaccination need to prove it. The scientists studying the phenomenon need to prove it. You know who never give us the specific antibody titers of these supposed vaccine injuries? The people who claim they've "never had covid" based on .... vibes(?) and the scientists studying them. Weird how they have near-identical symptoms and biomarkers to people who get Long Covid from an infection! It couldn't be that they're lying or had an asymptomatic infection and never knew they were sick! Nope! It's the jab! Make sure to hesitate about your next vaccination!
138 notes
·
View notes
Text
Writing Notes: Bites & Stings

References (Dog Bites; Cat; Human; Spider; Bee & Wasp; Snake; Jellyfish)
Bites and stings - puncture injuries inflicted by an animal that penetrate the skin.
DOGS
A typical dog bite results in a laceration, tear, puncture, or crush injury.
Bites from large, powerful dogs may cause fractures and dangerous internal injuries. Dogs trained to attack may bite repeatedly during a single episode.
Infected bites usually cause pain, cellulitis (inflammation of the connective tissues), and a pus-filled discharge at the wound site within 8–24 hours.
Many infections are confined to the wound site, but some of the microorganisms in the mouths of dogs can cause systemic and possibly life-threatening infections.
Rabies is rare among pet dogs in the United States, most of which have been vaccinated against the disease. Tetanus is also rare but can be transmitted by a dog bite if the victim is not immunized.
CATS
The mouths of cats and dogs contain many of the same microorganisms.
Cat scratches and bites are also capable of transmitting the Bartonella henselae bacterium, which can lead to cat-scratch disease, an unpleasant but usually not life-threatening illness.
Cat bites are mostly found on the arms and hands.
Sharp cat teeth typically leave behind a deep puncture wound that can reach muscles, tendons, and bones, which are vulnerable to infection because of their comparatively poor blood supply.
This is why cat bites are much more likely to become infected than dog bites.
Also, people are less inclined to view cat bites as dangerous and requiring immediate attention; the risk that infection has set in by the time a medical professional is consulted is thus greater.
HUMANS
Humans bites result from fights, sexual activity, medical and dental treatment, and seizures. Bites raise the possibility of spousal or child abuse.
Children often bite other children, but those bites are hardly ever severe.
Human bites are capable of transmitting a wide range of dangerous diseases, including hepatitis B, syphilis, and tuberculosis.
Human bites fall into two categories:
Occlusional (true) bites present a lower risk of infection.
Clenched-fist injuries, which are very infectious and can permanently damage the hand, usually result from a fist hitting teeth during a fight.
People often wait before seeking treatment for a clenched-fist injury, with the result that about half of such injuries are infected by the time they are seen by a medical professional.
SPIDERS
As a rule, people rarely see a black widow bite, nor do they feel the bite as it occurs. The first (and possibly only) evidence that a person has been bitten may be a mild swelling of the injured area and two red puncture marks.
Within a short time, some victims begin to experience severe muscle cramps and rigidity of the abdominal muscles. Other possible symptoms include excessive sweating, nausea, vomiting, headaches, and vertigo, as well as breathing, vision, and speech problems.
A brown spider’s bite can lead to necrotic arachnidism, in which the tissue in an area of up to several inches around the bite becomes necrotic (dies), producing an open sore that can take months or years to disappear.
In most cases, the bite simply produces a hard, painful, itchy, and discolored area that heals without treatment in 2–3 days.
The bite may be accompanied by a fever, chills, edema (an accumulation of excess tissue fluid), nausea and vomiting, dizziness, muscle and joint pain, and a rash.
BEES & WASPS
The familiar symptoms of bee and wasp stings include pain, redness, swelling, and itchiness in the area of the sting.
Multiple stings can have much more severe consequences, such as anaphylaxis, a life-threatening allergic reaction that occurs in hypersensitive persons.
SNAKES
Venomous pit viper bites usually begin to swell within 10 minutes and sometimes are painful.
Other symptoms include skin blisters and discoloration, weakness, sweating, nausea, faintness, dizziness, bruising, and tender lymph nodes.
Severe poisoning can lead to tingling in the scalp, fingers, and toes; muscle contractions; an elevated heart rate; rapid breathing; large drops in body temperature and blood pressure; vomiting of blood; and coma.
Many pit viper and coral snake bites (20–60%) fail to poison (envenomate) their victim, or introduce only a small amount of venom into the victim’s body.
The wounds, however, can still become infected by the harmful microorganisms that snakes carry in their mouths.
Coral snake bites are painful but may be hard to see.
One to seven hours after the bite, a bitten person begins to experience the effects of the venom, which include tingling at the wound site, weakness, nausea, vomiting, excessive salivation, and irrational behavior.
Major nerves of the body can become paralyzed for 6–14 days, causing double vision, difficulty swallowing and speaking, respiratory failure, and other problems.
Six to eight weeks may be needed before normal muscular strength is regained.
JELLYFISH
Jellyfish venom is delivered by barbs called nematocysts, which are located on the creature’s tentacles and penetrate the skin of people who brush up against them. Instantly, painful and itchy red lesions usually result.
The pain can continue up to 48 hours.
Severe cases may lead to skin necrosis, muscle spasms and cramps, vomiting, nausea, diarrhea, headaches, excessive sweating, and other symptoms.
In rare instances, cardiorespiratory failure may occur.
Source ⚜ More: Writing Notes & References More: Writing Realistic Injuries ⚜ On Anatomy ⚜ Poison ⚜ Fight Scenes Part 1 2
#writing notes#animals#writeblr#dark academia#spilled ink#literature#writers on tumblr#writing reference#writing prompt#medicine#poets on tumblr#poetry#words#writing inspiration#creative writing#fiction#dogs#writing ideas#thomas gainsborough#writing resources
125 notes
·
View notes
Text
Why the Spleen Sucks
The spleen is a really shittily placed organ, making it prone to injury. This injury is usually severe and can lead to death if not properly managed. We're going to look at the function of the spleen, what happens when it is damaged, and how to write about.
Where is the spleen? It's in the upper left quadrant of the abdominal cavity, nestled right against the ribs (typically 9-11) at the midaxillary line. It's behind the stomach and is considered intraperitoneal. The main thing is that the spleen is very vulnerable. It is literally right up against the ribs without much protecting it. It's shaped like a little bean and is purple in humans. It is fed by the splenic artery, which comes off of the celiac trunk (which sticks off of the abdominal aorta).
What does the spleen do? Its main job is to filter out old and malformed red blood cells. It also holds immune cells. Certain diseases can cause the spleen to enlarge, including cirrhosis of the liver (it's connected to the hepatic portal system), sickle cell anemia (RBCs are stuck in it), and autoimmune disorders. The spleen also holds about 250 mL of RBCs in reserve in case you need them.
What happens when it is injured? The spleen can be ruptured and lacerated kinda easily. Blunt trauma to the ribs can cause it to rupture, and this is seen in contact sports and car accidents mostly. Because of those giant gaps between the ribs, it's also prone to injury from knife attacks. Gunshot wounds are another common cause, as well as broken ribs penetrating it (broken ribs are very sharp, like way sharper than you imagine). Rupture is more likely when someone has splenomegaly.
When the spleen is damaged, you're going to get a lot of intraperitoneal hemorrhaging. The spleen filters a lot of blood and has blood in it, so there's going to be a lot of blood in the abdomen (obviously). This will lead to distention, guarding (abs are tense), and hypovolemia. The left upper quadrant will be painful, and there can also be referred pain to the left shoulder (Kehr's sign).
If the patient has a small laceration, the symptoms aren't always as dramatic. Sometimes they'll just have low hemoglobin (which is on RBCs), maybe some thrombocytopenia (lots of platelets in the blood).
How do you fix this? If the injury is small and the patient is hemodynamically stable, they can usually be given a blood transfusion and the spleen can heal itself. Sometimes surgery is also performed to clamp a vessel or repair the outer layer of the spleen.
If the injury is major, then surgery will be performed. If the patient is less critical, they may go in and try to fix the problem. If it can't be fixed, they may do a splenectomy (remove the spleen). In a critical patient, they might forgo the nice pretty incision on the left side, and instead just split the patient down the middle. In these situations (in my experience), there isn't a lot of time to waste. One thing that we aren't going to waste time on is anesthesia, for example. This is with a lot of very critical surgeries, at least from what I have seen. Like the surgeon will start cutting as they are working on knocking out the patient, but usually they are in so much pain that they don't even register it.
If you remove the spleen, the patient is more at risk for infections, but with modern medicine and vaccinations, it's not as much of a big deal as it used to be. The patient will probably be fine.
Writing tips: (new section idea, hope you guys like it, lol) As with any injury, you have to make sure that you are giving them an acceptable mechanism of injury. With the spleen, this is either blunt trauma or penetration/laceration. Getting tackled, getting stabbed, getting shot, all great MOIs.
Second thing, present the appropriate signs and symptoms. A sign would be like bruising, hypotension, tachycardia, etc. A symptom would be LUQ pain, Kehr's sign, etc.
Next, figure out what you're going to do and where you're going to do it. In the field, there probably isn't much you can do. The most would probably be a laparotomy and clamping the splenic artery, but I mean, when I was an EMT, we were not doing this. There's a lot of stuff you can theoretically do, but never gets done. But I mean you can write it. If the patient makes it to the hospital, I think it would be more fun to do emergency surgery and just split them right down the middle. There's going to be a lot of blood in the greater omentum, very high stakes and exciting.
Anyways, hope you guys liked this, please let me know if I got anything wrong. I wrote this off of my personal experience and a few good textbooks, but there can always been mistakes in things.
#medicine#med student#medical school#biology#med school#med studyblr#whump writing#anatomy#spleen#hospital whump#surgery#emergency medicine#medical writing#writing reference#injury
74 notes
·
View notes
Text
As of October 15, 2024, CDC has released more than half of the anticipated 7.8 million entries of V-safe free-text entries. ICAN’s analysis of the entries released so far reveals almost 12,000 reports of kidney pain, kidney stones, or kidney infections.
As many of you already know, V-safe was developed by CDC for individuals to report symptoms after COVID-19 vaccination. This month, we decided to look at V-safe reports of kidney issues.
We know from other vaccines that vaccination can negatively affect kidney function, causing harm far from the injection site. Sadly, it doesn’t occur to most people that an injection in their arm can harm a distant system of their body. But as ICAN has reported again and again, all body systems can be impacted by vaccination.
A 2024 study found a “strong causal relationship” between COVID-19 vaccination and kidney diseases such as acute interstitial nephritis (inflammation of kidneys) and podocytopathy (injury to special cells in the kidney). A 2022 study found a correlation between acute kidney injury (AKI) and COVID-19 vaccination and that “AKI following the COVID-19 vaccines led to poor prognosis, with 19.78% death in the Pfizer-BNT group, 17.78% in MODERNA, and 12.36% in JANSSEN.”
The V-safe app entries—most made in just the first few days and weeks following vaccination—reveal many reports of kidney pain, the abrupt development of kidney stones, and hospitalization for kidney infections. Here are a few examples:
“Infection of Kidneys and UTI. Blood in urine and kidney stone on left kidney.”
“I’m in the hospital right now Because I’m still peeing blood they think it’s kidney stones.”
“Kidney stone requiring emergency surgery, ureteral stent placement and subsequent removal; UTI.”
“Intermittent stabbing, pulsing pain around left kidney.”
“Severe flank pain (I think it’s a kidney stone) I’m in the ER”
“Diagnosis with new onset kidney stone”
“Severe kidney infection back pain fever”
Readers will not be surprised to learn CDC doesn’t recognize kidney issues as adverse events related to COVID-19 vaccination, despite CDC’s access to this same V-safe data in real time as the vaccines were rolled out. ICAN will continue to do CDC’s job for it and bring attention to these dangerous and sometimes life-threatening conditions.
28 notes
·
View notes
Text
Here is a video that talks about the reality of living with Long COVID. This is another reminder that this virus is still prevalent and just as deadly, if not more. COVID has killed nearly seven million (documented cases) people worldwide. You are not immune, you are not invincible, and this is something you should still be taking seriously. It’s not in the past, it is still spreading and mutating and harming and disabling and killing.
Wear your masks, get the vaccines if you can.
Video Length: 1m 16s
Transcription:
"Hi, my name is Hannah, and COVID took my life from me. I was 23 when I got sick in August of 2020, and I'm turning 27 this month. I was an athlete for 10 years, and I had straight A's all through high school. I graduated with honors, multiple scholarships, and I was years in the school for my PsyD. I loved going on adventures, traveling, reading, painting, drawing, I even loved having a job. I even had a healthy immune system, and that was all until I got COVID." - "I've been diagnosed with epilepsy, and the back to back seizures have caused brain damage; it has caused dementia type symptoms, spelling problems, mood changes, POTS, which haused caused me to be hospitalized multiple times with concussions and injuries. I'm on IV infusions and medications for that." - "I have to use a wheelchair, I can no longer legally drive; diabetes, an autoimmune disease, chronic and debilitating fatigue, vision deterioration, had to have my thyroid removed, lost half my hair. I still have a hard time breathing and have low oxygen at points-- chronic pain, muscle aches, tooth decay, increased mental health issues and ideations. I had to quit my job, withdraw from school, and I never see anyone but my family and doctors I can longer draw, travel, and I really struggle with reading, which is my favorite thing." - "My loved ones are terrified to leave me home alone, and I'm scared to even sleep at night because I'm afraid that I won't wake up. I spend my days alone in bed because life has to go on without me. This is the reality of it [long covid]. And 1 in 5 infections cause long COVID. I promise you, you are not invincible."
#you are not invincible#long covid#covid#covid 19#autoimmune#immunocompromised#get vaccinated#chronic illness#chronically ill#disabled#physically disabled#hypothyroidism
131 notes
·
View notes
Text

In numbers… The government media office documents important facts about the reality of Gaza’s children under the aggression:
🔻 15,694 children killed by the occupation.
🔻 About 34,000 children were injured.
🔻 3,600 children are missing under the rubble.
🔻 About 1,500 children lost limbs or eyes or were permanently disabled due to injury.
🔻 At least 200 children were kidnapped by the occupation.
🔻 17,000 children became orphans, 3% of whom lost both parents.
🔻 More than 700,000 children were forcibly displaced from their places of residence.
🔻 About 650,000 children lost their homes after they were destroyed by the occupation.
🔻 625,000 children were forced by the aggression to drop out of school and lose the academic year.
🔻 98% of Gaza’s children do not find safe drinking water, and depend on less than 3 liters of water per day.
🔻 3,500 children with chronic diseases are at risk of death due to malnutrition and lack of necessary medical care.
🔻 60,000 fetuses in their mothers’ wombs, exposed to miscarriage, death, or birth defects due to the effects of bombs and explosives.
🔻 About 40,000 infants did not receive the necessary immunizations and vaccinations on a regular basis.
🔻 82,000 children showed symptoms of malnutrition, 35% of whom suffered severe symptoms.
🔻 33 children lost their lives due to famine and malnutrition.
🔻 450,000 children are at risk of developing chest cancer and respiratory diseases, due to reliance on burning rubble waste to prepare food.
🔻 All children in Gaza are vulnerable to epidemics and infectious diseases, due to the lack of personal hygiene and overcrowding in areas of displacement and shelter.
🔻 All children in Gaza suffer from psychological trauma and behavioral problems such as fear, anxiety, and depression due to the aggression.
Government Media Office Gaza, Palestine June 14, 2024 AD
52 notes
·
View notes
Text
i'm just going to say it
the covid vaccine ruined my life
i already had some minor health issues before i got it, and i knew there was a warning of increased risks for side effects if you live with chronic conditions, especially inflammatory conditions—not just for that vaccine, but for literally any vaccine
but i was looking for a job at the time, and i thought it would increase my chances to have both of my doses
i have not had a moment of good health since that vaccine
not a single moment in 3 years
immediately post-vaccination, i was completely bedbound for 6 months. absolutely debilitated. i am usually able to function better these days, but i feel like i'm playing ping pong, getting bounced between "barely functioning" all the way back to "bedbound"
i don't talk about it because:
-you get labeled as crazy
-people don't take you seriously
-people think you're exaggerating/misremembering/otherwise misrepresenting
-nefarious little conspiracy theorist anti-vaccine weirdos use the stories of people with vaccine reactions to push their idiotic agenda
i'm not an anti-vaccine person. i wouldn't have even got my covid vaccines if i had any doubts in their efficacy
i just happen to be a small, miniscule percentage of people that had long-lasting side effects that ended up mimicking the condition of long-covid, which manifests in symptoms closely related to me/cfs
and yeah, i'm probably going to live with it for the rest of my life
in no way would i use my experience to push an anti-vaccine agenda. and to have people using me as a sideshow specimen for their anti-vaccine rhetoric is so, so dehumanizing. i left all the vaccine side-effect and injury support forums because it kept getting infiltrated by physically healthy anti-vaccine people telling us 'you're all going to die early', among other vaccine fear-mongering
i feel kinship and comfort with long-covid forums and me/cfs forums, and i would instead go over to those, but even they think people with vaccine reactions are exaggeratory liars
i'm so, so tired
there is no place for me
nowhere
10 notes
·
View notes
Text
hi friends,
i want to talk to y'all for a minute about Long COVID. I'm not usually open and vulnerable about my life on here but it seems important.
Some of you know that I caught COVID on the way home from a trip in August of 2023 and have been dealing with Post-acute COVID symptoms since.
My initial infection wasn't so bad, it triggered the worst migraine of my life so far but with Paxlovid I felt okay through most of it. It probably would have been much worse if we weren't up to date on our vaccinations.
I have a fairly moderate case of Long COVID, here's a list of what I've experienced:
On Rosh Hashanah I developed a migraine and I haven't had a migraine free day since.
My vision and astigmatism are both worse.
There are several foods I can no longer digest.
My PMS/PMDD symptoms are more severe.
Every old injury I have is inflamed constantly, my bad knee is so swollen and sore walking and sitting are challenging.
I have periods of brain fog and mental exertion increases my migraine.
Sometimes exercise or even showering leaves me short of breath with hear plapitations. I can't predict if/when this will happen.
I've experienced an intensification of some sensory sensitivities and other autistic traits.
This is what I have observed in myself and doesn't touch what I cannot.
It sucks. I'm more depressed and anxious. I had to abandon my dreams of becoming a psych nurse. I'm grieving lost capacity and may never be able to go back to the theatre work I love. Sometimes I don't know who I am anymore.
I say all this because the winter surge is coming soon. COVID isn't over. Wear a mask. Get your shots. Protect the people in your community. We don't understand this virus well enough to be cavalier about it.
I love you, please be safe.
15 notes
·
View notes
Text
So, I have another crazy story about the clinic where I used to work; this time as a patient instead of an employee. Under a cut because it's very long.
So back when I first got really sick, I was in the hospital a few times primarily for really high heart rate. I work out a lot and my normal resting heart rate is in the 60s; back in February I suddenly started getting palpitations, and my heart rate was going up to like 140 bpm just standing at my bathroom sink washing my face. I wore a seven day monitor at one point and my highest recorded heart rate on that was 157 bpm--just shuffling like a zombie around the house. I was also super weak and just felt overall like death.
Hospital runs a bunch of labs and imaging tests and can't find anything that would explain it. The last doc I saw said there was a bright spot on my echocardiogram monitor that could just be flashback from the monitor, but taken with some of my symptoms, he felt OK with a presumptive diagnosis of pericarditis (inflammation of the sac around your heart), especially as the treatment is just high dose ibuprofen for a week, nothing invasive or drastic. I need to follow up with a cardiologist, but I don't have a primary care physician who can refer me to the heart clinic. I had just turned in new patient paperwork at a local clinic so I contacted them to see if I could get in, but they said it would likely be a month before I could be scheduled with anyone.
In the meantime, the ibuprofen isn't working and my condition is getting worse. I have my next period, and after a couple of heavy days, I get even weaker, my heart rate goes even higher, and I get really dizzy all the time. I also am now short of breath just rolling over in bed. I legit feel like I'm dying. Because my symptoms get worse after blood loss, it suddenly pops into my head that about 17 years ago after a blood donation I got really sick, and all my symptoms that I can remember having at the time are the same, especially the cardiac issues. I took iron back then and that resolved it. I started wondering if my iron was low, did a bunch of research into iron deficiency without anemia, and realized every single symptom, including ones I had been having for a while prior to the heart issues (terrible fatigue, brain fog, headaches, sleep disruptions, restless legs at night) could be from low iron.
So I need to get labs done, and also I do still need a referral to make sure my heart is ok. I can't get in with anyone, so out of desperation, I go back to my old clinic because I know they'll get me in quickly. They schedule me an appointment for the next day with a doc who is going to turn out to be batshit crazy.
I go to my appointment with my presumptive diagnosis of pericarditis, and the doctor asks if I had the Covid shot. I tell him yes, but my last booster was in 2021, so not relevant here.
Well boy howdy was I wrong. He launches into a whole-ass rant about how bad the shots are, how many people have been injured by them, tells me I, a formerly very healthy, athletic woman, now have heart issues due to the shot, etc. etc. I say, 'Ok, but would the shot really randomly cause me issues three years later when I was perfectly fine after I got it?' (The answer is no.) Doc stays the course in blaming the shot. I have paperwork I need filled out for medical leave from my job, and he PUTS ON MY PAPERWORK THAT I HAVE TO TURN IN that my cardiac issues came on and progressed after the shot (three YEARS after, you DUMBASS) and that his impression is post vaccine injury. I feel too badly to do much more than sway on the exam table and occasionally interject that I had the shot three years ago and I don't think that's the problem. The majority of my appointment is him ranting about the shots. Whatever, I'm desperate, give me my fucking referral to the cardiologist and order my iron panel.
I get labs done and sure enough, my iron is low. I start supplementing and shortly afterwards get a call from the cardiac clinic; I lucked out and got in just a few days after my referral was sent to them because someone canceled their appointment last minute. I see an ARNP at my first visit and she says the echo I had done at the hospital looks fine to her, but they'll do a seven day monitor, a repeat echocardiogram, and have me follow up with the cardiologist just to make sure they don't miss anything.
So they do this, and in the meantime, after a couple of weeks on iron supplements, I start slowly but steadily feeling a bit better. My fatigue and brain fog that I was having every day improve significantly after only a week on supplements. My dizziness goes away. I feel a tiny bit stronger every day and now can sit up longer and start holding conversations with people. It's slow but steady progress for about three weeks: and then I get my period again. It doesn't knock me back to square one, but I definitely take a couple of steps back in my recovery. It's a little lighter this time, though, which is a good sign.
I follow up with the cardiologist. He says actually my heart is in really good shape; no signs of pericarditis or anything wrong with it; my high heart rate isn't due to a cardiac issue. Cool. I didn't think so at this point, but good to hear I don't have heart issues.
So I go back to follow up with my doc and plan to ask to really focus on the iron issue since the cardiologist confirmed my heart is fine. I have come a long ways but am still mostly bedridden; it is very slow to get your levels up on iron supplementation, and every time I get my period, it sets me back a little. Maybe some low dose iron infusions would help boost my levels so my recovery doesn't go backwards on account of me bleeding for a week every few weeks.
Doc comes in the room. He is clearly Not Happy cardiology did not confirm his conspiracy theories about the shot injuring me. I tell him about the symptoms I have seen improve and even resolve after about six weeks on iron supplements, and how I think most if not all of my problems are from low iron. He pretty much completely ignores this. He asks me if my fatigue and brain fog have improved. I say, yes, they were some of the first symptoms to improve after I started taking iron. He does not even acknowledge I have spoken. He tells me he thinks I have a combination of chronic fatigue syndrome and POTS (postural orthostatic tachycardia syndrome) caused by the shot. I remind him I just told him my fatigue had improved a lot since starting iron. And my heart rate is coming down too and not spiking as much, my issue is that every period after I've been improving, I suddenly get a little worse again. He ignores this. He tells me he is going to refer me to the neurologist to check for chronic fatigue and POTS. Ok, whatever, I'm pretty sure I don't have those things, but fine, have another specialist tell you you're wrong.
After about eight weeks on supplements, I really feel like I'm starting to turn a corner. I don't feel normal, but my heart rate has come down quite a bit, I can stand and walk around a lot longer without feeling like I'm going to pass out, and I feel the closest to normal that I have been in months.
And then I get my period again and my heart rate goes back up. I'm super frustrated at this point because I was So Close to being a functioning human again, so I decide to push for a low dose iron infusion. I just want to boost my levels high enough to get me over this hump so every period doesn't set me back right as I feel like I'm coming back to life. I've read lots of papers on iron deficiency without anemia (meaning your hemoglobin is normal) and decide to make an appointment armed with one paper in particular which was written by a doctor who has been treating iron deficiency for decades, and which lays out really comprehensively the numbers at which patients should be considered deficient based on their labs and symptoms, what numbers you should shoot for when treating the iron deficiency (I am higher now but still quite a ways away from the goal), and also lists a bunch of symptoms women in particular have reported that have resolved with iron treatment. I highlight all the symptoms on the list that I have had, as well as other sections particularly relevant to my specific case. (Spoiler alert: I did not even give him the paper.)
So I go to my appointment and he asks if I've heard from the neurologist yet. I say no, I'm sure it will be a while (there's only one in town, and I'm sure it takes a long time to get in). In the meantime, I really want to focus on getting my iron levels up. I lay everything out: all the improvements I've seen, how my period keeps setting me back, and how I want to try just a low 100mg infusion to boost me up so I don't take two steps back every time I get my period. He tells me I have chronic fatigue and POTS as a result of the Evil Shot. I tell him, once again, that my fatigue has greatly improved on iron supplements. He does not even acknowledge I have spoken. He tells me a local doctor is being PERSECUTED and PROSECUTED for prescribing Ivermectin for Covid. Ok, that doesn't relate to my personal medical issues that we are here to discuss, and also, Ivermectin is not approved for the treatment of Covid. I ask him again if I can get a low dose infusion. I understand insurance probably won't cover it, that's fine, I can pay out of pocket, I just need him to order it. He tells me he personally takes Ivermectin. Good for you. Again, not related to my medical issues that I am here to dicuss.
I mention that I have had restless legs at night for a long time, because I know this at least is commonly associated with low iron, maybe that will get his attention; nope. He totally ignores me again. I even try blaming the shot for low iron (sorry, Covid vaccine, sometimes you have to take one for the team). I say I have read Covid and maybe even the shot can deplete your iron; maybe the shot did this to my iron. No dice. (Mr. Jenn did applaud me for trying when I told him about it, though.)
He starts in about my POTS again. I say, ok, but POTS is a postural issue, right? He says, yes! I say, ok, then if I have an issue where my nervous system doesn't regulate my blood flow properly when I change from sitting to standing, why is my resting heart rate way higher than normal when I'm just lying in bed doing nothing, and why has my heart rate been coming down and is not spiking like it was after several weeks on iron supplements until I get my period? I'm not sure that fits with POTS.
He again does not even acknowledge I've spoken.
I ask again for an infusion to help boost me up so I'm not set back every period. He says as long as I'm menstruating it will set me back. Yes, I am aware I will lose more iron on my period, what I am asking is that while I am in ACTIVE CLINICAL IRON DEFICIENCY can we please do something to speed up getting my levels high enough so every time I bleed it doesn't knock me down again. He asks if I have considered a hysterectomy or uterine ablation for the bleeding (you know, invasive surgeries, instead of talking about birth control pills, which he didn't even mention). I said that was kind of extreme and I didn't want to consider that right now. I ask him about the infusion again. He says it's not a concern. I say, yeah, it is, I am having debilitating symptoms that have left me bedridden for three months. I need to get back to my life and my job. He tells me Congress is investigating the shots and it will come out how bad they are, but a lot of people won't believe it. I say, well, that's Congress' business, can I please have an infusion. He tells me insurance won't cover it. I say I know, I already mentioned that earlier (while you were ignoring me in favor of ranting about a vaccine I had three years ago), I have a health savings account, I can pay out of pocket. He tells me he's pretty sure I have chronic fatigue and POTS but we'll see what the neurologist says. I need to call and see if I can get in more quickly with the neurologist. I say, ok, in the meantime, since realistically it could take months for me to get in with the neurologist, can I PLEASE HAVE A FUCKING INFUSION. He tells me if I want one I will have to badger another doctor into it. (I can't remember the exact word he used, but the way he worded it made it sound like I was trying to bully him. No, you jackass, I am asking for an extremely common, low risk medical treatment for issues that have left me unable to work or leave my house for anything other than doctor's appointments for THREE MONTHS.)
So I left incredibly frustrated, needless to say.
Next day Mr. Jenn goes to his appointment at the clinic I initially tried to get into to follow up on labs he had done for an annual physical, and his doctor tells him his cholesterol is slightly high, but not enough to be concerned, he just needs to watch his saturated fats and red meat intake. Mr. Jenn tells him we've actually temporarily increased our red meat intake because of my health issues. He then mentions all of the issues I've been having, my lab results, and how I've improved a lot on supplements, but keep getting set back by my period. His doctors goes, 'Have you guys looked into infusions for her? You should try that.'
I DID BUT MY DOCTOR IS CRAZY.
Mr. Jenn explains that I had asked for an infusion and my doctor refused. His doctor gives him a weird look and wants to know why. Mr. Jenn explains it's because he's super set on it being chronic fatigue and POTS and won't consider anything else even though my 'chronic fatigue' and 'POTS' symptoms have both improved on iron supplements. The doctor again gives him a weird look and asks why he's stuck on those diagnoses and won't consider iron deficiency.
Because he's crazy, good sir.
Mr. Jenn's doctor then suggests we see if I can self-refer for an infusion and just pay out of pocket, but you need a doctor's order even if you're not going through insurance, so the next day when the clinic opens, I call, explain I tried to establish care there earlier so they have my new patient paperwork, but that I needed an urgent referral, and had to go somewhere else because they were a month out, but I really (REALLY) want to change doctors, is <Mr. Jenn's doc> taking new patients? He is not, but they'll put in a note with one of the ARNPs accepting new patients to see if they're willing to schedule me.
However, I know the new manager of the clinic (actually an old coworker from the crazy clinic that I'm friendly with), so the other day I texted her, briefly explained the situation, and she asked which doctor I wanted to see and said she'll talk to him when he's back from the long holiday weekend and see if he would be willing to see me. She will let me know later this week (he's not back in till Wednesday). So fingers crossed I can get in with a non-lunatic soon.
24 notes
·
View notes