#medication is good
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There are dozens of funny blogs to kill time on Tumblr.
Text

#stop demonizing adhd drugs#congratulations to drugs for winning the war on drugs#cannabis is medicine#being high is not a bad thing#better living through modern chemistry#fibromyalgia and dopamine depletion#adhd and dopamine regulation#adhd and caffeine#we can't all be neurotypical karen#don't make me tap the sign#if you can't make your own neurotransmitters store bought is fine#new age bullshit for the next generation#we know better now#drugs are good#medication is good#don't tell me what to do#gen x annoyed with all the rest of you t shirt
32 notes
·
View notes
Text

faded blue house portrait hanging on the wall at the local urgentcare
#medical assistant: yeah i never saw that show but i heard it was popular in the 90s?#me: (takes lethal psychic damage)#house md#good post good post
115K notes
·
View notes
Text




sorry danny, sam will never think you’re cool
#danny phantom#danny fenton#sam manson#theres some ocs#college au#sam’s goth book club#i feel like she’d make a lot of good friends at a college#the trio has a highly rehearsed excuse for danny being weird#nobody has any idea what ecto-contamination is bc it doesn’t exist#ghosts are common-ish knowledge by now and amity is the known epicenter#stranger: holy shit your hand just went through that wall#danny: yeah it’s a medical condition :(#fentonworks is in on it too#for credibility#too bad the goths wanted vampires#moving to a new city did wonders for dannys popularity though#he’s got a lot he’s hiding so he can’t really take advantage#he probably knows more people number wise#but has less friends than sam#Tucker has a thriving social media life#but doesn’t get out much#hence that technus comic#can’t believe I finished this#lit took a whole ass week#hahahaha
24K notes
·
View notes
Text

My personal understanding of the situation
#tf2#team fortress 2#tf2 medic#tf2 miss pauling#tf2 pauling#i wish i was home and could draw this digitally or at least well#i found out medics name at 2 am and couldn't go back to sleep from hysterics. funniest choice of a name for him istg#and i realized we were given miss Paulings name in the comic 5 minutes before drawing this#i love both their names. i will forever mourn Joseph Ludwig#but#this is so funny its so worth it#and flo..... Florence Pauling.... okay lesbian omg......... i#good for her#i hope she's happily married to the loveliest woman who loves her sm#and i hope medic doesn't cry himself to sleep after heavy laughs at his name for 3 hours
8K notes
·
View notes
Text
It's been a while since you've seen a doctor, and you're nervous as you follow the nurse back to my office. What's there to be nervous about, this is just a little checkup, right? You notice the nurse's manicured burgundy nails as she knocks sharply on the door. She turns to you, smiling prettily, and says, "the doctor will see you now."
You push open the door and enter quite a large room. The nurse follows, closing the door behind you. In the center is the examination table, off to the right is a small crowd of young adults, appearing to be made up of men and women, and on the left is me, seated at my desk. "Welcome," I say, standing and extending one hand. My voice is deep, warm, and smooth, and you fumble for a moment, blushing a little, before you remember to shake my hand. Your hand is dwarfed in mine, my strong fingers encircling you, and a thought flashes unbidden through your mind - what would those fingers feel like inside you? - but, come on now, that's really not appropriate...
"I have a few students with me, as you can see. Is that alright?"
"Well, yes, of course!" Why shouldn't it be?
"Excellent. Now, I'm pioneering this new full-body examination method - it's really quite extraordinary, the maladies I can detect this way - but be warned, it is, shall we say, unorthodox. Is that alright?"
Just for a moment, you see something in my eyes, something behind the genial smile and gentle, reassuring tone. Just for a moment, you feel like some specimen, some piece of meat, pinned down under the lights with nowhere to go... but just for a moment. Surely, nothing bad can happen, and I'm a doctor, aren't I? You can trust me. So you swallow your fear, and you acquiesce.
"Excellent! Let's have a seat on the table, if you don't mind, and we'll make a start. Nurse V, if you would..."
As you sit on the table, the clinical, sterile seating a little cold against your skin, the pretty nurse steps behind the table, facing you, waiting for something. From your right, I approach, and you feel again just how much larger than you I am as my broad shoulders block out one of the ceiling lights. With all these people watching you, it takes all you have not to squeeze your legs together, just a little bit.
We begin with a quick examination of your face - "you have beautiful eyes, you know," I purr into one ear. I place one hand on the side of your neck and tilt your head; god, you've been reading too much, haven't you, the way you want these strong, expert fingers to close around your throat.
"Now, open your mouth for me, please." You oblige, and I cup your chin and slide my thumb into your mouth, pressing down on your tongue. Your eyebrows jump in surprise, and you look at me questioningly.
I smile again, still inside you. "Unorthodox, remember? Now, close your mouth and try to swallow." From behind, the nurse strokes your cheek with the back of one hand, and you feel a sudden ache between your legs. You close your lips around my thumb and swallow. It tastes... clean, mostly, as one might expect from a doctor, but you can taste the sweat underneath.
"Very good, one more time for me."
You swallow again, and you feel me slide my thumb over the surface of your tongue, pressing down, swirling in circles.
"And, one more time... yes, that's it, good job, very good job."
The praise for this degrading task is more than you can bear, and you squeeze your thighs together. Fuck, it's humiliating, everyone just saw you do that... All these eyes on you, the beautiful nurse behind you, this big, strong doctor with these big, strong hands and that big fucking bulge... but no, this is just a checkup, nothing is going to happen, right?
While you were thinking, I dried my hand off and had begun speaking.
"I'm - I'm sorry?"
"No worries. I was saying, can you remove your top, please? We need to examine your heart and your breathing."
You stare at me. "Remove my - "
"Yes, remove your top. The fewer barriers between me and you, the less interference with my examination." My face is quite serious, almost bored - this really must be routine. You look back at the nurse, and she smiles slightly and nods. So you undress, your nipples betraying you, standing at attention. You blush as the crowd of students looks at you intently. The nurse lays one warm hand on your shoulder, slender fingers gripping you reassuringly, and your eyes are drawn once more to those burgundy nails.
I step in close, and you feel my breath warm on your chest. "Now, observe the stiffness in the patient's nipples - this is to be expected, given the cool air, and it's certainly nothing to be ashamed of," I say, smiling. I press my stethoscope up over your heart, the metal cold on your skin, and your mind is betrayed by the pounding of your heart. My eyes flick up to meet yours, and I grin, predatorily, and once again you feel like a piece of meat beneath the lights.
I examine your breasts, starting with your left. Enclosed in my big, strong hands, I squeeze and push, prod and pull, ostensibly feeling for any abnormalities, but the way my fingers brush over your nipples, the intensity with which I sink them into your soft breasts, heaving now as your breath comes faster... My practiced tongue rasps over one nipple and a tiny moan escapes your lips as you try desperately to hide how much you're enjoying this; try desperately, and fail.
Abruptly, I pull back. "Excellent! All seems well here." I rest one hand on your other shoulder and turn to the students. "Note the pleasure response during this section of the examination, and I hope you were paying attention to the oral technique."
I turn back to you, my eyes dancing as they meet yours. "Fully undress, if you would. The inspection must continue."
Your hands tremble as you slide your clothes down off your waist, and the nurse aids you, her lovely hands stroking along your thighs and calves as she does.
"And spread for us, please."
Obediently, your thighs open, exposing your cunt, your needy, aching wetness, to all.
"Note the beauty of the patient's sex, here. The shape of the folds," I murmur, tracing one finger along your sensitive lips, "the balanced ratio of the clitoris to the vulva overall," sliding two fingers on either side of your clit, squeezing gently between them, "the appropriate pleasure response in - "
You lose what I say as I plunge two fingers inside you, powerful and dextrous, knuckles slipping past your tightness easily. It feels so fucking good to finally have something inside you, after all this aching and teasing, and god, so many people are watching, they're all watching your pussy spread and toyed with by this big, strong, handsome older man, and now the nurse's slender fingers are across your throat and her lips are on your forehead, and she tells you that you're doing so well for me, you've been so good...
My fingers press up inside you, finding your g spot, and with my thumb rubbing on your clit, I start melting you. Waves of pleasure course through your body, you gasp, moan, whimper, and with your eyes closed you can't tell whose lips are so soft on yours, but it feels so fucking good, and all those people are watching and it makes you want it more, your back arching, chest heaving, melting under the attention, and finally, mercifully, you cum, contracting around my fingers, squeezing your thighs together, trembling, shaking, gasping for air. You hear me say something, but you're so overwhelmed with pleasure that all you can make out from my speech is "very, very good".
The hand withdraws from your throat, and I gently, gently, extricate my fingers, and settle my hand atop one thigh, fingers slick with your desire.
The nurse whispers affirmation in your ear as I address the class. "Stimulation in this manner, of the two most sensitive sex stimuli, brings the most consistent and powerful orgasms to those possessing these organs." I stroke the inside of your thigh reassuringly, before turning to you.
"The final part of this examination is seeing how well you handle penetration. I'm going to need your unequivocal verbal consent before proceeding."
The nurse leans in and whispers into your ear, "might I suggest 'please, sir, will you fuck me?'" You'd blush harder if you could.
You swallow, nervously, and there's a twisting in your gut as you say it. "Please," you begin, voice cracking. "Please, sir, will you fuck me?"
"Yes, that is sufficient. I must say, though," I warn, unzipping my jeans, "that I am quite large." I slap my cock down on your tummy, and the sheer weight of it shocks you. You've seen size like this in porn, sure, but fuck, you've never touched something like this. When you tear your gaze away from my cock, I'm grinning down at you, predatory again. "You can back out at any time, you know." My voice is low, teasing, challenging. "Should we continue?"
You nod shakily, and spread your legs a little wider.
One hand on your raised knee, one hand guiding my cock, I push against you. For a moment you realize the exam had to be done in this order; if you weren't so fucking wet, there's no chance you'd be able to take me. But all thoughts are blasted out of your mind as I push harder and slide in.
It's so fucking thick that you can't help but groan. You've never felt so full, so strained inside, being pushed in every direction; you're not built for this, maybe there's just too much, your body is rejecting me - and then I push again, another few inches, and you slam your head back against the padded table, a long, drawn-out "fuuuuuck" wrenched from your lips. You feel my strong hands brace at your hips, and with a final thrust, slamming your cervix up into your guts, moving your entire body, the ridges of my cock sliding deeper and deeper, sliding painfully, pleasurably past your walls, I'm inside you.
The nurse rests her hands on you again, and purrs in your ear, "you're doing so well for him, I know it's hard, it's so hard, but you're doing such a good job, pretty girl..."
Glacially, I pull out, allowing you a moment to rest, before thrusting in again, hands still at your waist. You sob once, loudly, and then you sink into it as I pick up a rhythm, deep, deep strokes inside you. You hear me grunting, whispering something, and I grow more frantic, impaling you a little harder, and through the wall of pleasure you hear me rumble, "nurse V, begin the overstimulation procedure."
"Certainly, doctor." She leans over you, lips fiercely meeting yours, and one of those slender hands reaches down to abuse your clit. An image of those burgundy nails on your cunt flashes through your mind as I continue pounding you, forcing you to spread for me, adjust to me, even as the nurse plays your clit like an instrument, and fuck, she's a virtuoso.
You sing a song of moans and voiceless curses under our combined mastery, knowing your audience is entranced, filled with a blazing, lusty pride. The deep bass of my voice, resonant in your skull, is saying something, but you cannot hear me; you're moaning, groaning, pleading, "yes, yes, oh my god yes" over and over...
The song swells to a crescendo and with two sudden strikes, two powerful thrusts into you, it ends with a thick, hot, sticky white wave of my approval inside you. You feel it pulse deep, deep inside, filling you, load after load delivered straight past your bruised, abused cervix.
You come back to reality with my cum spilling from between your legs, trailing thickly down onto the exam table. I zip up my jeans while the nurse helps dry you off, from all the sweat and saliva. She dabs caringly at your mouth, and you notice that the cloth is dyed the same shade as her lipstick.
"Now," I address the class, "I hope you were paying attention." I rest one hand on your aching, trembling thigh. How many times did you cum with me inside you? How long were all these people watching you writhe beneath me, begging, losing yourself in the pleasure? You have no fucking clue. "This patient has bravely volunteered for each of you to examine her, here and now, while she's available to us."
Your jaw drops. When did you agree to that? You would never - but you were begging, "yes, yes, yes" earlier, weren't you, while I was talking. You agreed. Everyone heard you say it.
"One at a time, please. And," I say to you, grinning wolfishly, "don't worry. I'll be watching the entire time."
#size difference#size k!nk#fr33use#mine#cnc k!nk#free use kink#free use slvt#medical play#cnc free use#rough cnc#rapedoll#rapekink#rapetoy#rough kink#r4pepl4y#r4p3 fantasy#r4ape kink#r4p3 kink#bimboification#dumb slvt#dumbification#needy wh0re#dumb wh0re#good slvt#fr33use slvt#size matters
21K notes
·
View notes
Text
"The first modern attempt at transferring a uterus from one human to another occurred at the turn of the millennium. But surgeons had to remove the organ, which had become necrotic, 99 days later. The first successful transplant was performed in 2011 — but even then, the recipient wasn’t immediately able to get pregnant and deliver a baby. It took three more years for the first person in the world with a transplanted uterus to give birth.
More than 70 such babies have been born globally in the decade since. “It’s a complete new world,” said Giuliano Testa, chief of abdominal transplant at Baylor University Medical Center.
Almost a third of those babies — 22 and counting — have been born in Dallas at Baylor. On Thursday, Testa and his team published a major cohort study in JAMA analyzing the results from the program’s first 20 patients. All women were of reproductive age and had no uterus (most having been born without one), but had at least one functioning ovary. Most of the uteri came from living donors, but two came from deceased donors.
Fourteen women had successful transplants, all of whom were able to have at least one baby.
“That success rate is extraordinary, and I want that to get out there,” said Liza Johannesson, the medical director of uterus transplants at Baylor, who works with Testa and co-authored the study. “We want this to be an option for all women out there that need it.”
Six patients had transplant failures, all within two weeks of the procedure. Part of the problem may have been a learning curve: The study initially included only 10 patients, and five of the six with failed transplants were in that first group. These were “technical” failures, Testa said, involving aspects of the surgery such as how surgeons connected the organ’s blood vessels, what material was used for sutures, and selecting a uterus that would work well in a transplant.
The team saw only one transplant fail in the second group of 10 people, the researchers said. All 20 transplants took place between September 2016 and August 2019.
Only one other cohort study has previously been published on uterus transplants, in 2022. A Swedish team, which included Johannesson before she moved to Baylor, performed seven successful transplants out of nine attempts. Six women, including the first transplant recipient to ever deliver a baby back in 2014, gave birth.
“It’s hard to extract data from that, because they were the first ones that did it,” Johannesson said. “This is the first time we can actually see the safety and efficacy of this procedure properly.”
So far, the signs are good: High success rates for transplants and live births, safe and healthy children so far, and early signs that immunosuppressants — typically given to transplant recipients so their bodies don’t reject the new organ — may not cause long-term harm, the researchers said. (The uterine transplants are removed after recipients no longer need them to deliver children.) And the Baylor team has figured out how to identify the right uterus for transfer: It should be from a donor who has had a baby before, is premenopausal, and, of course, who matches the blood type of the recipient, Testa said...
“They’ve really embraced the idea of practicing improvement as you go along, to understand how to make this safer or more effective. And that’s reflected in the results,” said Jessica Walter, an assistant professor of reproductive endocrinology and infertility at Northwestern University Feinberg School of Medicine, who co-authored an editorial on the research in JAMA...
Walter was a skeptic herself when she first learned about uterine transplants. The procedure seemed invasive and complicated. But she did her fellowship training at Penn Medicine, home to one of just four programs in the U.S. doing uterine transplants.
“The firsts — the first time the patient received a transplant, the first time she got her period after the transplant, the positive pregnancy test,” Walter said. “Immersing myself in the science, the patients, the practitioners, and researchers — it really changed my opinion that this is science, and this is an innovation like anything else.” ...
Many transgender women are hopeful that uterine transplants might someday be available for them, but it’s likely a far-off possibility. Scientists need to rewind and do animal studies on how a uterus might fare in a different “hormonal milieu” before doing any clinical trials of the procedure with trans people, Wagner said.
Among cisgender women, more long-term research is still needed on the donors, recipients, and the children they have, experts said.
“We want other centers to start up,” Johannesson said. “Our main goal is to publish all of our data, as much as we can.”"
-via Stat, August 16, 2024
#infertility#uterus#organ transplant#reproductive health#public health#medical news#childbirth#good news#hope#pregnancy#cw pregnancy
15K notes
·
View notes
Text


Saw the soldier I was pocketing hanging around my body yelling medic on the death cam, though it was cute.
#my art#tw blood#tf2#tf2 medic#tf2 soldier#we hung out all of an infinite 2fort match it was actually really fun it was my first time playing medic and he was a good first impression#this game is about making friends with strangers and then never seeing each other again
4K notes
·
View notes
Note
That's good to hear!!
all it took was falling asleep at 4pm and eating a huge breakfast....
0 notes
Text
I found an extremely dope disability survival guide for those who are homebound, bedbound, in need of disability accommodations, or would otherwise like resources for how to manage your life as a disabled person. (Link is safe)
It has some great articles and resources and while written by people with ME/CFS, it keeps all disabilities in mind. A lot of it is specific to the USA but even if you're from somewhere else, there are many guides that can still help you. Some really good ones are:
How to live a great disabled life- A guide full of resources to make your life easier and probably the best place to start (including links to some of the below resources). Everything from applying for good quality affordable housing to getting free transportation, affordable medication, how to get enough food stamps, how to get a free phone that doesn't suck, how to find housemates and caregivers, how to be homebound, support groups and Facebook pages (including for specific illnesses), how to help with social change from home, and so many more.
Turning a "no" into a "yes"- A guide on what to say when denied for disability aid/accommodations of many types, particularly over the phone. "Never take no for an answer over the phone. If you have not been turned down in writing, you have not been turned down. Period."
How to be poor in America- A very expansive and helpful guide including things from a directory to find your nearest food bank to resources for getting free home modifications, how to get cheap or free eye and dental care, extremely cheap internet, and financial assistance with vet bills
How to be homebound- This is pretty helpful even if you're not homebound. It includes guides on how to save spoons, getting free and low cost transportation, disability resources in your area, home meals, how to have fun/keep busy while in bed, and a severe bedbound activity master list which includes a link to an audio version of the list on Soundcloud
Master List of Disability Accommodation Letters For Housing- Guides on how to request accommodations and housing as well as your rights, laws, and prewritten sample letters to help you get whatever you need. Includes information on how to request additional bedrooms, stop evictions, request meetings via phone, mail, and email if you can't in person, what you can do if a request is denied, and many other helpful guides
Special Laws to Help Domestic Violence Survivors (Vouchers & Low Income Housing)- Protections, laws, and housing rights for survivors of DV (any gender), and how to get support and protection under the VAWA laws to help you and/or loved ones receive housing and assistance
Dealing With Debt & Disability- Information to assist with debt including student loans, medical debt, how to deal with debt collectors as well as an article with a step by step guide that helped the author cut her overwhelming medical bills by 80%!
There are so many more articles, guides, and tools here that have helped a lot of people. And there are a lot of rights, resources, and protections that people don't know they have and guides that can help you manage your life as a disabled person regardless of income, energy levels, and other factors.
Please boost!
#signal boost#please reblog#I'm so so glad this has gotten the traction that it has!#chronic pain#chronic illness#disability#fibromyalgia#cfs#chronic fаtiguе ѕуndrоmе#actually disabled#spoonie#me/cfs#cfs/me#long covid#important#invisible disability#ehlers danlos syndrome#lyme disease#chronically ill#cpunk#cripplepunk#it's a bummer that it's so US centric but if you're outside of the US you can look into similar programs#I hope that other countries have options like these#the US seems so behind when it comes to medical care and disability resources. and i mean it is#but it's good to know all of your rights as a disabled person or if you ever become disabled
21K notes
·
View notes
Text


regular dogs
#tf2 dogs live in my tablet and they will not leave. someone call animal control#1 am on a sunday and i wish you all a good night#tf2#tf2 medic#tf2 sniper#tf2 scout#tf2 spy#tf2 demoman#tf2 fanart#fanart#lasagoofs
3K notes
·
View notes
Text
hey STEB NATION (me and 5 other fish enthusiasts) how are we feeling
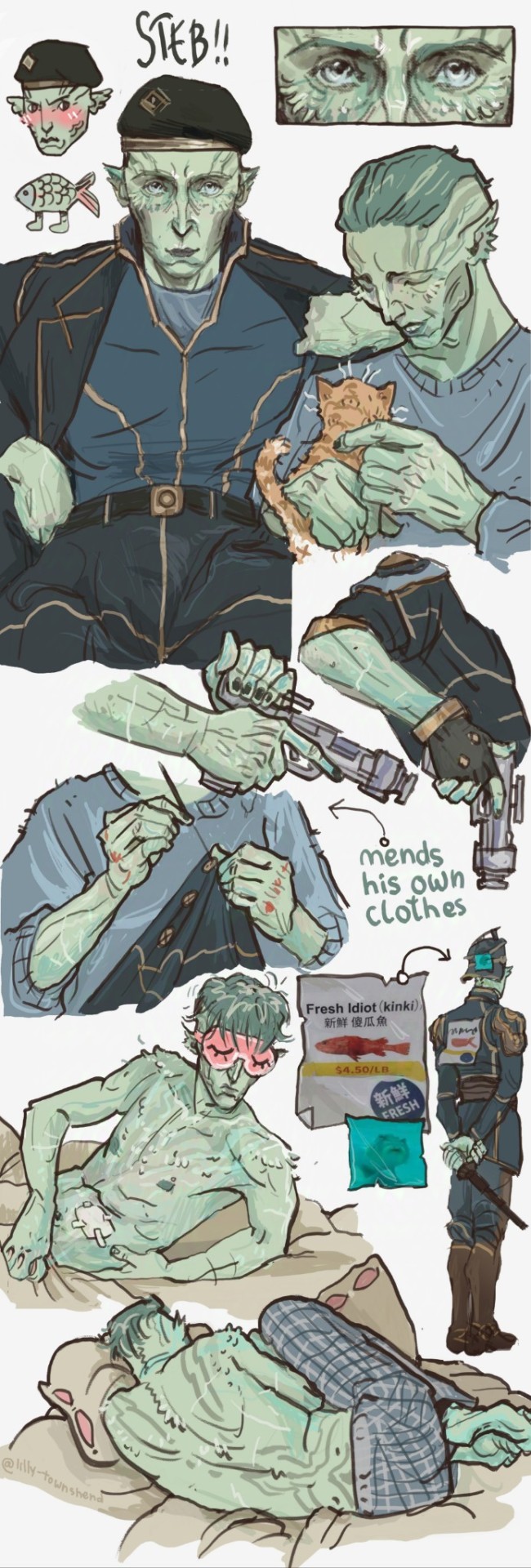
#do we think he needs sleep masks because his eyes are sensitive to light#do we think he's good at sewing things bc he's a medic#do we think he sleeps curled up bc idk bc my heart tells me so#we definitely do think he's selectively mute#arcane#steb arcane#arcane art#steb my love#steb x reader#viktor arcane#silco#jinx#steb#viktor x reader#monster fuqqer#hear me out#arcane fanart
6K notes
·
View notes
Text
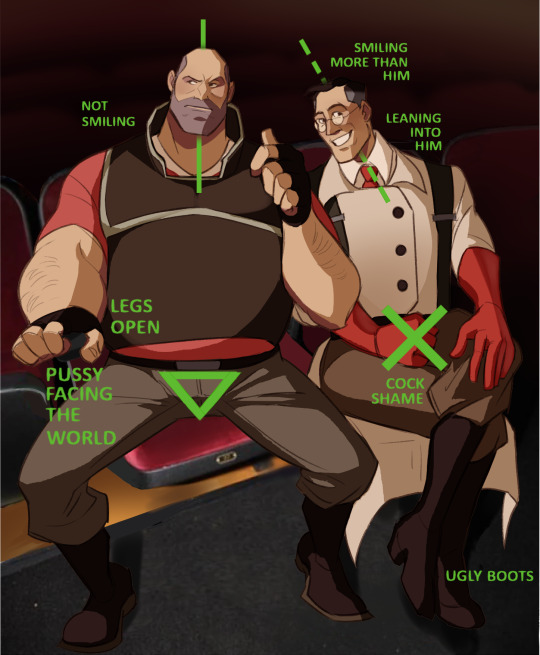

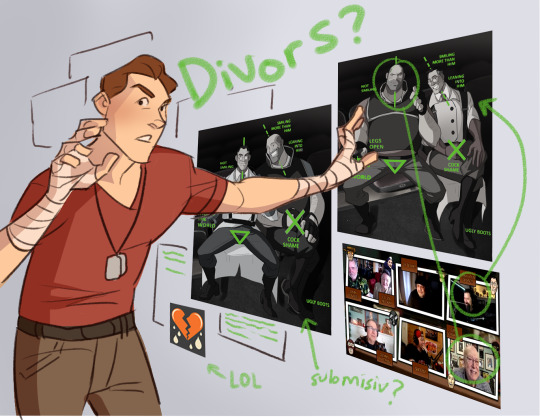
Desperately needed to do another shitpost and that Will Smith cock shame meme came to mind - I couldnt decide who fit who as you can see so now theres just a red and blu version lol which maybe indicates they dont quite fit the meme but shh Also kinda looks like a conspiracy board
I dunno why Scout would care so much about whether or not they stay together (they're the teams rock😩)
Cut below is me playing around with the images lol

I just thought it was funny
#tf2#team fortress 2#heavymedic#tf2 medic#tf2 heavy#red oktoberfest#scout: if we dont make sure they stay together the whole friend group is over#i think its so funny how many divorce arcs they go through lol#this actually wasnt a good art day at all i was really struggling#and took me forever sigh#its how it is at least it shall post
3K notes
·
View notes
Text
listen. listen to me so carefully right now. (if you're in the eclipse path/planning on viewing). please don't stare directly at the sun tomorrow. i am begging you - do not stare at it. if you got eclipse glasses off of amazon/other, please put them on in your house and make sure you can't see anything; if you can still see like regular sun glasses, they are not safe for eclipse viewing, you will burn your retinas, and we cannot fix that. eclipse glasses should be iso/ce certified, and aas (american astronomical society) approved. please make smart choices and protect your eyes. please.
#psa from your friendly neighborhood eye care provider#the office is already fielding so many calls about this make good life choices#very important#eclipse#solar eclipse#eye health#not medical advice#just me screaming to please protect your eyes#ive seen exactly one case of solar retinopathy in my career so far please don't give me another one
14K notes
·
View notes
Text
i think everyone who's ever had migraines should be financially compensated forever btw
#camera talks#disability stuff#this is for my chronic migraine girlies (gn) <3#i think we should all get 1 million million dollars everyday actually#this is the worst fucking night of my life (everytime i have migraines) (specifically rn tho)#chronic pain#chronic migraine#migraines#chronically ill#disabled#disclaimer because idk I’ve got a lot of notes on this#I have diagnosed chronic migraines. I used to have them 5-6 times a week#now with medication on a good week I’ll only be affected 2-3 days#on bad weeks it’s much worse#anyways don’t doubt my condition I know what I’m talking about thx
40K notes
·
View notes
Text
you're in the habit of denying yourself things.
if someone asked you directly, you would say that you love a little treat. you like iced coffee and getting the cookie. you drink juice out of a fancy cup sometimes, and often do use your candles until they gutter out helplessly.
but you hesitate about buying the 20 dollar hand mixer because, like. you could just use your arms. you weren't raised rich. you don't get to just spend the 20 dollars (remember when that could cover lunch?), at least - you don't spend that without agonizing over it first, trying to figure out the cost-benefits like you are defending yourself in front of a jury. yes, this rice cooker could seriously help you. but you do know how to make stovetop rice and it really isn't that hard. how many pies or brownies would you actually make, in order to make that hand mixer worthwhile?
what's wild is that if the money was for a friend, it would already be spent. you'd fork over 40 without blinking an eye, just to make them happy. the difference is that it's for you, so you need to justify it.
and it sneaks in. you ration yourself without meaning to - you don't finish the pint of ice cream, even though you want to. the next time you go to the store, you say ah, i really shouldn't, and then you walk away. you save little bits of your precious things - just in case. sometimes you even go so far as putting that one thing in your shopping cart. and then just leaving it there, because maybe-one-day, but not right now, there's other stuff going on.
you do self-care, of course. but you don't do it more than like, 3 days in a row. after that it just feels a little bit over-the-edge. like. you can't live in decadence, the economy is so bad right now, kid.
so you don't buy the rice cooker. you can-and-will spend the time over the stove. you can withstand the little sorrows. denial and discipline are practically synonyms. and you're not spoiled.
it's just - it's not always a rice cooker. sometimes it is a person or a job or a hug. sometimes it is asking for help. sometimes it is the summer and your college degree. sometimes it is looking down at scabbed knees and feeling a strange kind of falling, like you can't even recognize the girl you used to be. sometimes it is your handprint looking unsteady.
sometimes it is tuesday, and you didn't get fired, and you want to celebrate. but what is it you like, even? you search around your little heart and come up empty. you're so used to denying that all your desires draw a blank.
oh fuck. see, this is the perfect opportunity. if you had a mixer, you'd make a cake.
#warm up#this isn't good#writeblr#this is complicated by the fact i can't stand up too long or i fuckken pass out and <3 hit my damn head <3#but i did take a deep breath and buy myself the stupid rice cooker#and!!! a very cheap sushi kit!!! i have been wanting to try making sushi for literally YEARS#the kit was only like 15 dollars!!!! and i haven't purchased it bc?!!??!?!?!?!!?#..... i didn't get the mixer tho that felt. like a lot. like too much.#on my list is a kitchenaid. one day when i get a check and i have paid off my student debt#and medical debt#i will put that first little bit of cash#into a kitchenaid 5qt stand mixer (with attachments)#i really do just go into their refurbished section and stare lustily at each option#but yeah i feel guilty about the rice cooker even tho i know for a fact this damn thing is gonna be a lifesaver#oh shit also fuck i forgot to mention . poached eggs
31K notes
·
View notes
Text
"A medical technology company in Australia is aiming for a world-first: it wants to launch a blood test for endometriosis (sometimes called 'endo' for short) within the first half of this year [2025].
In a recent peer-reviewed trial, its novel test proved 99.7 percent accurate at distinguishing severe cases of endometriosis from patients without the disease but with similar symptoms.
Even in the early stages of the disease, when blood markers may be harder to pick out, the test's accuracy remained over 85 percent.
The company behind the patent, Proteomics International, says it is currently adapting the method "for use in a clinical environment," with a target launch date in Australia for the second quarter of this year [2025].
The test is called PromarkerEndo.
"This advancement marks a significant step toward non-invasive, personalized care for a condition that has long been underserved by current medical approaches," managing director of Proteomics International Richard Lipscombe said in a press release from December 30.
Endometriosis is a common inflammatory disease that occurs when tissue similar to the lining of the uterus grows in other parts of the body, forming lesions. The disease can be very painful, and yet the average patient often suffers debilitating symptoms for up to seven years before they are properly diagnosed.
While there are numerous reasons for such a long delay, symptoms of endometriosis are often highly variable, unpredictable, difficult to measure or describe, and dismissed or overlooked by doctors.
Today, the only definitive way to diagnose endometriosis is via keyhole surgery called a laparoscopy, which is expensive, invasive, and carries risks.
Proteomics International is hoping to change that.
In collaboration with researchers at the University of Melbourne and the Royal Women's Hospital, the company compared the bloodwork data from 749 participants of mostly European descent.
Some had endometriosis and others had symptoms that were similar to endo but without the lesions. All participants had a laparoscopy to confirm the presence or absence of the disease.
Sifting through the bloodwork, researchers ran several different algorithms to figure out which proteins in the blood were best at predicting endometriosis of varying stages.
Building on previous research, a panel of 10 proteins showed a "clear association" with endometriosis.
For years now, scientists have investigated possible blood biomarkers of endometriosis to see if they could differentiate between those who have endo and those who do not. Similar to cancerous tumors, endo lesions can establish their own blood supply, and if cervical cancer can be diagnosed via a blood test, it seemed possible that endometriosis could be, too...
Proteomics International claims patents for PromarkerEndo are "pending in all major jurisdictions," starting first in Australia.
It remains to be seen if the company's blood test lives up to the hype and is approved by the Australian Therapeutic Goods Administration (TGA). But that's not outside the realm of possibility.
In November of 2023, some researchers predicted that a "reliable non-invasive biomarker for endometriosis is highly likely in the coming years."
Perhaps this is the year."
-via ScienceAlert, January 9, 2025
--
Note: As someone with endometriosis, let me say that this is a HUGE deal. The condition is incredibly common, incredibly understudied, and incredibly often dismissed. Massive sexism at work here.
I got very lucky and got diagnosed after about 6 months of chronic pain (and extra extra lucky, because my pain went away with medication). But as the article says, the average time to diagnosis is seven years.
Being able to confirm endometriosis diagnoses/rates without invasive surgery will also lead to huge progress in studying/creating treatments for endo.
And fyi: If you have a period that is so painful that you can't stand up, or have to go home from school/work, or vomit, or anything else debilitating (or if any of those things apply if you forget to take pain meds), that is NOT NORMAL, and you should talk to a competent gynecologist asap.
#endometriosis#periods#menstrual cycle#menstruation#chronic pain#period pain#period problems#period cramps#medical news#medical sexism#australia#good news#hope
2K notes
·
View notes