#insight medical publishing
Text

By: Christina Buttons
Published: Apr 4, 2024
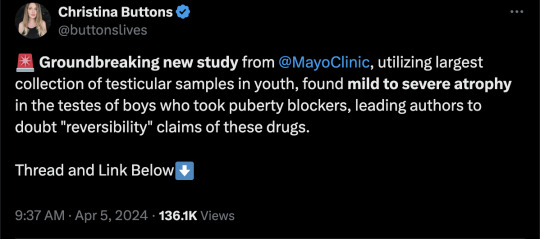
[ Figure 2: Representative images of Hematoxylin and Eosin-stained sections of testicular tissue biopsied from the testis from GD patients (A) with and (B) without PB exposure. ]
In a groundbreaking study from the Mayo Clinic, a globally recognized leader in medical research and patient care, researchers examined the effects of puberty blockers on testicular development in gender dysphoric male children. Their investigation revealed evidence of mild to severe atrophy in the sex glands of these children, leading the authors to express doubt in the claims of “reversibility” often made about puberty blockers.
The authors assert, “We provide unprecedented histological evidence revealing detrimental pediatric testicular sex gland responses to [puberty blockers].”
This preprint study, not yet peer-reviewed, presents evidence that puberty blockers induce significant cellular changes, impacting testicular development and sperm production in ways that are not fully reversible, with potentially permanent effects on testicular function and fertility. It challenges the longstanding view of puberty blockers as a reversible "pause button" on puberty.
As noted by the researchers of this study, no long-term studies exist for the use of puberty blockers in the context of stopping puberty for gender dysphoric children, and many potential health consequences remain unknown. In particular, the long-term impact on reproductive health is uncertain, making this study critical for filling this knowledge gap.
To address these unknowns, the Mayo Clinic has established the largest collection of testicular samples for patients aged 0-17 years, including those with gender dysphoria who have and have not yet received puberty blocker treatment, creating a database of over 130,000 individual cells for analysis.
Using a novel approach, the research team meticulously analyzed testicular tissue samples from youths undergoing puberty blocker treatment, with those not on puberty blocker treatment serving as controls. This comparison provides important insights into the potential cellular and molecular changes induced by these drugs.
Key Findings
The study utilized the Mayo Clinic's Pediatric Testicular Biobank for Fertility Preservation, which has been recruiting patients primarily from pediatric urology departments since 2015. Researchers analyzed testicular specimens from 87 young individuals (ages 0-17) undergoing fertility preservation surgery for various health reasons. Among these, 16 were gender dysphoric boys between the ages of 10 and 16, all of whom began identifying as transgender girls between the ages of 2 and 15. At the time of surgery, 9 patients (56%) were already on puberty blockers, with exposure ranging from 3 to 52 months. The authors noted that 100% of the 16 children would eventually go on to take them, highlighting “the widespread nature of PB intervention in this demographic.”
Among nine patients treated with puberty blockers, two exhibited unusual features in their testicles upon physical examination. One patient had abnormalities in both testicles, including incomplete development of the tunica albuginea, which is a protective covering around the testicles. The other patient had a right testicle that was difficult to detect.
In one part of the tissue-level analysis, over 400 testicular biopsy samples were analyzed and stained to examine the differences between those treated with puberty blockers and those who were not. Comparisons showed that testicular development in those treated with puberty blockers was abnormal compared to non-treated individuals. There was variability in how individuals responded to puberty blockers, leading to different outcomes in testicular development, including the degeneration of testicular tissues.
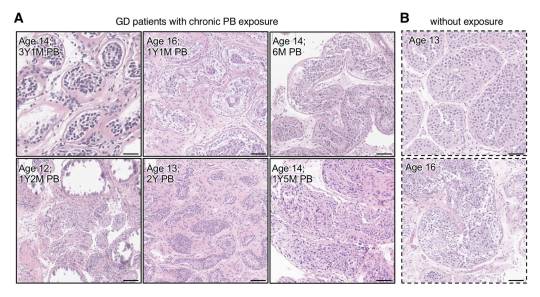
The study authors presented a case of a 12-year-old patient who underwent treatment with puberty blockers for 14 months. In this individual, 59% of the sex glands showed complete atrophy, along with the presence of microlithiasis—a condition where small clusters of calcium form in the testicles. This insight suggests that puberty blockers could lead to lasting structural changes. Additionally, research has shown a link between testicular microlithiasis and testicular cancer.

[ D) Representative images of normal (top) and fully atrophied sex gland (bottom). ]
This study also utilized single-cell analysis to investigate the effects of puberty blockers and aging on testicular cell composition. It took a very detailed look at individual cells from the testicles of a 14-year-old who had been on puberty blockers for over 4 years. The study analyzed a total of 130,100 cells, including 11,199 cells from the juvenile puberty blocker-treated patient.
The study observed that over 90% of the cells responsible for sperm production in this patient were stunted at an early developmental stage, unable to progress further. Additionally, it found "pathologically" higher and lower levels of two types of support cells (Sertoli cells) necessary for healthy sperm development. These findings suggest that puberty blockers can disrupt the normal maturation process of cells critical for sperm production.
In another part of the analysis, the authors found distinct cell-specific changes, including altered expression patterns of puberty-associated genes in endothelial cells, due to puberty blocker treatment. The authors believe that these drugs might induce juvenile testicular atrophy in part by disrupting the normal function of testicular endothelial cells.
Another aspect of the study focused on examining the effects of puberty blockers on the genetic activity of early-stage sperm cells, revealing significant changes that could potentially influence their development and fertility. By analyzing the activity of specific genes within these cells, the researchers found that puberty blockers may have caused alterations in gene expression, affecting processes crucial for the normal growth and function of these cells. This analysis suggests that the use of puberty blockers in gender dysphoric youth could have lasting implications for their reproductive health, particularly by impacting the ability of these early-stage sperm cells to mature properly.
Study Impact
Puberty blockers are increasingly used as a treatment for gender dysphoric youth to halt the development of secondary sex characteristics, such as breast development and widening of hips in females, or the growth of facial hair and deepening of the voice in males. Thousands of children in the United States are placed on this medical pathway as part of the gender-affirming model of care, under the presumption that these drugs are safe and fully reversible.
However, many aspects of the long-term consequences of puberty blockers, which have been administered to children off-label in an experimental manner, remain unknown. This study contributes valuable insights into the potential irreversible harm these treatments can cause to bodily and reproductive functions.
Arguably, the most critical finding is the evidence of mild to severe sex gland atrophy in children treated with puberty blockers. This atrophy signifies potential damage or impairment to the structures essential for sperm production, raising serious concerns about the long-term fertility impacts of these drugs for these individuals.
Given the Mayo Clinic's esteemed reputation in the medical and research communities, should the study pass peer review without any issues, its findings will carry significant weight.
Broader Implications
Puberty blockers belong to a group of synthetic gonadotropin-releasing hormone (GnRH) analogues. These drugs act on the pituitary gland to hinder the release of chemical signals that typically trigger the production of estrogen and testosterone. Historically GnRH analogues were used to treat conditions such as prostate cancer, fibroids, and endometriosis and, in some cases, as a measure to chemically castrate sex offenders.
In children, puberty blockers prevent the natural changes of puberty driven by sex hormones and have been used to treat central precocious puberty, a condition where a child begins to sexually mature much earlier than usual. In gender dysphoria, puberty blockers are administered experimentally, lacking long-term testing.
Notably, the U.S. Food and Drug Administration (FDA) has not approved puberty blockers and sex hormones for use in pediatric gender care. No clinical trials have substantiated the safety of these drugs for such non-approved applications and manufacturers of puberty blockers have repeatedly declined to conduct safety trials for their use on this cohort.
While puberty-blocking drugs are often promoted as “safe,” "reversible" and a "pause button" on puberty, these characterizations seem to stem from their approved use for treating central precocious puberty in younger children, not their burgeoning off-label use for managing gender dysphoria in adolescents.
Past studies have indicated possible negative effects on bone density and brain health. There is also a concern that these drugs might solidify gender dysphoria in adolescents, potentially leading them down a lifelong road of biomedical interventions. Following reports in 2016 of suicidal ideation in children administered puberty blockers, the FDA instructed drug manufacturers to include a warning about potential psychiatric issues on the drugs' labels.
Puberty blockers are increasingly administered to adolescents at Tanner Stage 2, the first signs of puberty. Research shows administering puberty blockers at this stage, followed by cross-sex hormones, may result in infertility, sterility, and sexual dysfunction. Furthermore, they inhibit the development of mature male genitalia, making it difficult to create a pseudovagina in the event of a later vaginoplasty due to a lack of sufficient tissue.
The National Health Service England recently announced it would no longer prescribe puberty blockers to youth outside of research settings and closed down its only national clinical service for pediatric gender medicine, following a review that deemed the service "not safe.”
Several European countries, including Sweden, Finland, the UK, Denmark, and Norway have updated their guidelines for youth transition to align with systematic evidence reviews, the gold standard in evidence-based medicine. These reviews concluded that the risks associated with youth transition outweigh any purported benefits. Consequently, these countries have implemented restrictions on medical interventions, prioritizing psychotherapy as a first-line response for minors experiencing gender-related distress.
==
They're sterilizing boys and giving them cancer. When "god" does it, we call him evil. When humans do it, we call it "gender affirming care."
#Christina Buttons#puberty blockers#atrophy#medical scandal#medical malpractice#medical corruption#sterilization#fertility#irreversible#gender affirming care#gender affirming healthcare#gender affirmation#queer theory#gender ideology#gender identity ideology#intersectional feminism#religion is a mental illness
231 notes
·
View notes
Text
The book "The Long Covid Survival Guide" might be something magz audience would find useful.
The Long COVID Survival Guide:
How to Take Care of Yourself and What Comes Next
Stories and Advice from Twenty Long-Haulers and Expertsby Fiona Lowenstein
The first patient-to-patient guide for people living with Long COVID—with expert advice on getting diagnosed, dealing with symptoms, accessing resources and accommodations, and more
“The Long COVID Survival Guide aims to give people struggling with long COVID practical solutions and emotional support to manage their illness.”—NPR, It’s Been a Minute
For people living with Long COVID, navigating the uncharted territory of this new chronic illness can be challenging. With over two hundred unique symptoms, and with doctors continuing to work toward a cure, people experiencing Long COVID are often left with more questions than answers.
A support group in book form, The Long COVID Survival Guide is here to help. Twenty contributors—from award-winning journalists, neuroscientists, and patient-researchers to corporate strategists, activists, and artists—share their stories and insight on topics including:
getting diagnosed
finding a caregiver
confronting medical racism and gaslighting
navigating employment issues
dealing with fatigue and brain fog
caring for your mental health, and more.
This vital resource provides the answers and reassurance you need, to take care of yourself and prepare for what comes next.
Contributors: Karyn Bishof, JD Davids, Pato Hebert, Heather Hogan, Monique Jackson, Naina Khanna, Lisa McCorkell, Karla Monterroso, Dona Kim Murphey, Padma Priya, David Putrino, Yochai Re’em, Rachel Robles, Alison Sbrana, Chimére L. Smith, Letícia Soares, Morgan Stephens, and Terri L. Wilder
The link has more information and more places to buy it. It is available as Physical book and E-book. It was published on November 8, 2022.
The price averages $18.95 U.S. & $24 Canadian.
Quick Links though.
Where to buy: Amazon. Bookshop. Better World Books. Books-A-Milion
Free E-Book File Download
(for those who can't viably access, have it delivered to where live, or pay)
1K notes
·
View notes
Note
I don’t know if you already wrote about this so forgive me if this is a repeat question but, what do you think about Leona’s depression? I feel it’s pretty obvious in game and yet it’s always glossed over as him being ‘lazy’ idk but I don’t find many talking about his really shitty mental health with any seriousness.

Surprisingly I haven't addressed this (at least not in detail)! So thank you for bringing this to my attention; I definitely feel like I've heard people (especially Leona fans) discuss this quite frequently. If you look in the right places, you’re sure to find insightful commentary on the subject! I know I certainly have, but I've yet to say my own piece on it yet.
Now, before I actually get to actually rambling, I want to preface this post with a few points so we can walk in knowing the perspective I'm coming from. Analysis isn't a "one size fits all"! My experiences and background will color the lenses through which I view Leona’s mental health.
First and foremost, I usually don't go out of my way to claim, "this character has X condition" beyond what is outright stated or implied in canon. That does NOT mean that I disapprove of fans who may have their headcanons that say otherwise or project onto or relate to characters' mental health. You can consume the media you like however you want! I am just saying that I don't have this preference so I feel somewhat uncomfortable speaking on this matter.
Secondly, I am trying to approach this situation from a very clinical viewpoint (as I do have knowledge in this area). This means that when I look for “implications” or read between the lines, I am doing so as objectively as I can. It’s how I choose to process and understand characters from a health angle. This does not mean that my opinion is certain; you could very well find someone else in this area that gives you the opposite opinion. As always, I warn you that my response is for fun, it is NOT meant to be taken as medical advice.
Lastly, PLEASE READ THE ENTIRE POST before you comment or share your own thoughts. I'm up for having a discussion, but I ask that you not do so without getting the full context of my thoughts. It’s a lot of information, and I did my best to break it down in a way that (I hope!!) is easy to understand.
CONTENT WARNING: due to the nature of the question at hand, I will be discussing or mentioning potentially triggering topics such as ***depression, suicidal ideation, dieting, homophobia, and substance abuse.*** Please look away if you are not in the right headspace to read about such topics.
Okay, let's rip the band-aid off now: I don't think Leona is clinically depressed.
Pause. Rewind. Take note of my careful wording there: clinically depressed. I don't think Leona is clinically depressed. What does that mean, and how does that relate to "being depressed"?
I think when people describe Leona as "depressed", they commonly mean that he "has depression", not that he is just feeling sad or has low self-esteem. By "having depression", I'm going to assume they are referring to "major depressive disorder", which is the technical term for the condition.
"It's just an abbreviation of the longer term. What's the issue with using 'depression'?” you're probably wondering. “You understand that we mean major depressive disorder.” Well, equating the two does NOT a diagnosis make.
Mental conditions such as major depressive disorder are documented in a handbook known as the DSM (or the Diagnostic and Statistical Manual of Mental Disorders). The latest version, the DSM-5-TR (5th edition with text revisions), was published in 2022. The DSM is a manual that sets forth criteria for each diagnosis in its pages. Of course, this includes major depressive disorder—and it may surprise you to learn that Leona does not meet its diagnostic criteria.
A diagnosis of "depression" (the term I will henceforth be using as shorthand for the disorder) is much more than having persistent feelings of sadness or hopelessness, being unmotivated/lazy, and wanting to sleep often. (I bring up these three things specifically because they are the ones I see being pointed at most frequently to “prove” the diagnosis.)
In order to be formally diagnosed, an individual must be experiencing at least 5 or more of the following symptoms during the same 2-week period:
Depressed mood most of the day, nearly every day.
Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day.
A slowing down of thought and a reduction of physical movement (observable by others, not merely subjective feelings of restlessness or being slowed down).
Fatigue or loss of energy nearly every day.
Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
Diminished ability to think or concentrate, or indecisiveness, nearly every day.
Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
At least one of the symptoms should be either 1) depressed mood or 2) loss of interest or pleasure in activities they previously found enjoyable. Furthermore, the symptoms must cause what is known as "clinically significant distress", which is defined by impairment in important areas of functioning. This includes, but is not limited to, socialization, occupation, and/or education. The symptoms must also not be the result of substance abuse or another medical condition, and the individual must ever have experienced mania or hypomania.
Let’s briefly go through each criterion + additional documents and see what evidence there is or isn’t to support it:
We do not have his medical records to cross reference, so for the sake of convenience let’s assume no underlying or additional medical conditions.
We must consider additional context about family, lifestyle, etc. which can confound his symptoms. For example, as a prince, Leona has grown up having most things done for him by servants. This is what he is used to. So when we observe Leona not doing basic things for himself (getting food, doing laundry, making his bed), how much of this can we truly attribute to an underlying condition and how much of this can we attribute to Leona being accustomed to a certain kind of lifestyle?
Leona (at least from what we know of) does not experience mania, nor is he depicted as taking mind or behavior altering substances.
Of the first two criteria, Leona must fit into one: either 1) depressed mood most of the day, nearly every day, or 2) markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day. These depend on how you interpret his actions and behaviors. Personally, I don’t think Leona strongly fits into 2 because he still has an interest in his hobbies like Magift/Spelldrive and playing chess (though his involvement in it varies depending on the context). I will concede that there is stronger evidence for 1 over 2, as Leona has definitely expressed sadness and despair regarding himself and his future prospects. It is these thoughts that drive him away from home and keep contact with his family at a minimum. It is these thoughts that prevent him from seeing himself as worthy or even capable of change—a sentiment he shares in book 6, when he encourages Jamil but does not grant himself the same kindness or optimism. For this reason, we will go with the first criterion.
He has not experienced notable weight loss nor gain, nor a notable increase or decrease in appetite. Regarding his general diet, Leona has expressed a preference for meat and rejects vegetables. This by itself does not really provide any useful information in of itself; many people have this preference.
Leona does not experience a slowing down of thought. He is still very sharp and quick-witted in responding to his surroundings, especially in potentially dangerous ones, and coming up with an appropriate plan to counter. It can be argued that Leona has had a reduction in physical movement, as many characters often make remarks about how they perceive him as lazy or not doing much. However, this criterion actually refers to the speed at which one completes an activity and as far as I know, Leona is not said to be moving sluggishly, he only conducts himself in a manner that can be described as "lazily elegant". Even if we stretched the definition to encompass long-term goals he is putting off (like graduation), this criteria is still not counted for Leona since the wording used in the DSM-5-TR states “slowing down of thought AND reduction in physical movement” must be present. In other words, both must be true, not just one of them.
Leona does seem to experience some level of fatigue or loss of energy. This could be one way of interpreting his desire to sleep excessively instead of tending to more meaningful matters (like class). Fatigue, in this case, can also refer to emotional or mental fatigue. The sleep, then, can serve as a means of escape from reality for Leona, but it does not indicate actual physical tiredness. Rather, the tiredness can be intangible. This is also a potential explanation for his lack of motivation when it comes to some activities, especially those that demand him to take charge.
Leona does appear to experience feelings of worthlessness, though perhaps not excessive or inappropriate guilt. In fact, I would wager Leona does not demonstrate the latter, although this could be attributed to the fact that we are not in his head and he does not open up to others about his feelings. For example, we still don't know what his feelings are on almost killing Ruggie in a fit of rage. This does not discredit this criterion though, as the wording in the DSM is “feelings of worthlessness OR […] guilt” meaning one or the other suffices. It is no secret that Leona seeks recognition for his skills—something he was denied as a child and even put down for. While he is aware of his strengths, he has moments when he doubts himself (stating that he can’t change, or giving up when he realizes his plans won’t work so what’s the point in trying?), the contributions he can make (even when his older brother reassures him he can help their country), and encouragement from others (Jack telling him his play inspired him).
As I've said before, Leona does not have a diminished ability to think or concentrate. It has been shown to us time and time again that he doesn't do schoolwork not for lack of trying or lack of understanding, but because he thinks of himself as above it. Leona has already been tutored by the finest teachers royal money can buy, so he believes there is not much else for him to learn. He is also not shown to be indecisive--he can make decisions very quickly and can guide others or at least convince them to go along with him.
Leona does not have suicidal ideation or have recurring thoughts of committing suicide/death. While it's true that this is a game rated for ages 4+ (and therefore has restrictions on what content is and is not allowed in it), TWST has demonstrated to us that there are ways to imply suicidal ideation and other dark themes without explicitly saying it. (One notable example is Idia in late book 6, where he drops lines like "I'll go with you" and expresses dissatisfaction with "this world" to Ortho, who is known to be dead. To this, Ortho reassures him and encourages him to keep living. In fact, I could go on a whole tangent about how Idia better fits the criteria for major depressive disorder, but we're not going to get into that here.) The fact that TWST does not really imply this about Leona makes me think this is not true of him.
It can be said that the symptoms Leona does have are clinically significant, as his behavior is shown to have significant impact on his studies to the point where he was held back a grade. This was not because he did not know the material, but because he failed to find the motivation to attend class and to do his assignments. It also appears that Leona didn't really make an effort to work toward his future until book 7, when he actually talks his internship plans and about wanting to graduate.
We may guess that the symptoms persisted for two weeks or more (given Leona’s history and involvement in the main story), but the frequency of the symptoms is unclear since the game controls what we see of Leona and what we don’t.
Taking all of that into consideration, Leona does in fact exhibit depressive symptoms, but only 3 at most (I say “at most” because we have no idea about the true frequency at which some behaviors occur; we aren’t with Leona 24/7, nor has he reported it to us) out of the 8 total criteria. That’s 2 short of a diagnosis.
“But wait, there’s a lot of information missing here! We don’t have medical records, his weight and appetite changes, etc.” That’s true—but see, the main issue I take with diagnosing fictional characters in the first place is that we oftentimes do not know a character in detail enough to understand the full scope of their lives and symptoms. Noticing a few details is one thing and valid to an extent, but to evaluate an individual is not purely observational. This is particularly true for TWST characters, as even though there is plenty of content to refer back to for behavior, there is still a lack of really going into daily activities or deep feelings (beyond the one post-OB flashback for the OB boys). We cannot observe their behavior extensively. Because of this, tons of key criteria may not be visible to us from the audience’s perspective, let alone a medical history or other data to consider for assessment. We will almost always have an incomplete profile of a fictional character. Health is holistic and not entirely based on what we as individuals see or on all anecdotal evidence.
Just as health considers all parts of the individual, we, too, must consider individual cases of depression. It is possible for depression to exist without a diagnosis—many people (especially older adults), unfortunately, go undiagnosed for their condition. At the same time, it is possible for Leona to have depression which manifests in an atypical way. Each person with depression presents differently than the last, so I so not intend to make any blanket statements about the general population with this condition. The only statement I am making here is that based on my own interpretation of the current lore TWST has granted is, Leona Kingscholar does not satisfy the criteria for a formal clinical diagnosis, at least not for major depressive disorder as is defined by the DSM-5-TR.
Interestingly, Leona does fit the diagnostic criteria for a subclinical form of depression in a 1994 version of the DSM (IV). Minor depression or minor depressive disorder, colloquially known as “everyday depression”, is defined as having 2–4 depressive symptoms persisting for more than 2 weeks. One of these symptoms must be either depressed mood or loss of interest. It should be noted that this terminology is no longer recognized, as new information is added and dropped from the manual all the time. The information is flexible based on the consensus of a panel of hundreds of experts. Older versions of the DSM can be horribly outdated and it is not advised to reference them over newer ones. (As an example, "homosexuality" was legitimately listed as a mental illness in the very first version of the DSM. Yikes. Thankfully, this was dropped from the DSM-II. Other conditions like "multiple personality disorder" are granted new names like "dissociative identity disorder" or reworked altogether as our studies and understanding of mental health and science improve. It is important to keep up with the research coming out and update our approaches accordingly.)
We do not currently have a label for Leona’s situation aside from perhaps experiencing depressive episodes (periods of notable sadness lasting under 2 weeks) and exhibiting some depressive symptoms. I must stress that just because we lack a full-blown diagnosis, it doesn’t mean that it doesn’t impact his life. Leona is shown to very clearly be struggling with his mental health. He spends a lot of time in bed, typically cannot be motivated to attend class or do complete assignments, and has moments where he thinks very lowly of himself in spite of the confidence he exudes to others. What's more is that because Leona does not speak to others about what he's going through, it comes off as laziness or arrogance to his peers. Think of it this way: if you have a bad day and snap at a stranger or an acquaintance, the stranger/acquaintance is far less likely to grant you grace or forgiveness for your behavior compared to, say, a friend. They are not as familiar with you, so they will have less patience and are less likely to consider what you may be going through on a personal level. This also applies on a fandom level; if a fan is not actively reading between the lines, they, like Leona's peers, may miss the depressive symptoms he is displaying because they aren't looking for it.
How many people can we say are close friends with Leona for him to open up to them about his circumstances? I would say Leona barely even lets his own dorm members be intimate enough with him to let them know about this part of himself. He has Savanaclaw backing him, but he probably does not talk to the mobs extensively. Ruggie is his errand boy, but I doubt Leona pours his heart out to him. And Jack is the newbie who did technically betray their dorm, so Leona might not trust him. Forget about people beyond his dorm. Even his family is not much better off; we've seen that Leona tends to brush off his brother's friendliness and attempts to make amends. There is no strong support system in place for him, which is tricky because Leona perpetuates it by keeping others at bay. In the light novel adaptation of book 2, Leona has an inner monologue about how he is afraid of letting others give him hope because it will encourage him to try again, only to fail another time. I imagine similar logic applies here; he is afraid of showing his vulnerable side because it might give him hope for change when he as late as book 6 expresses that he has given up on himself. I think that this is the detail about Leona most look to when they consider his mental health. The hallmark of depression is, after all, the feeling of perpetual sadness and despair itself. Most do not realize that other factors are considered.
From a clinical lens, it is not “obvious" that Leona is depressed. However, I understand why the prevailing sentiment tends to skew in the opposite direction. For the layman, it may be difficult to distinguish what is and is not clinically significant enough to warrant an actual diagnosis. Again, most will cite the same three pieces of information to support the depression reading: Leona's irritability, his unwillingness to participate, and the rejection he experienced as a child (which has now manifested as self-doubt and low self-esteem). Characters are often judged based on fans' own experiences, and this naturally comes with biases and subjectivity. Thus, some fans may project their own understanding or preconceived notions of what the "typical" depressed person acts like in their head onto Leona. This is normal human empathy at play.
I believe that other fans see depression in Leona either because they experience it themselves or are familiar with someone in the same shoes. It can be difficult, and at times we can find solace and solidarity in fiction, especially if we find a character that “speaks to us” and seems relatable. That character may be Leona for some people. If you see do see him in this light or relate to his situation, I’m not invalidating your feelings. On the contrary, I'm happy that you were able to find comfort in him and that a piece of media you love can serve as a coping mechanism. You keep on doing you!
It is at this point that I will reiterate what I said at the start with a little extra nuance: I do not think Leona clinically depressed BUT I do believe he has depressive symptoms and poor mental health as the result of his cumulative circumstances. It is possible for him to have major depressive disorder, but we cannot determine this for certain with the information available to us right now. We are still missing several key components that would typically be considered in the evaluation process.
I think it's important to step back from focusing on labels and instead focus on the individual experience, and how you can still grow as a person and not let a perceived label define you. Leona is definitely working on himself! Changing, particularly changing a deeply ingrained mindset, takes much time and effort. We may not see the progress since Leona tends to hide it and/or we have limited intractions with him. We may not always see giant strides because the process is difficult. Even so, Leona is trying to jump over those mental and emotional hurdles. He's putting his all back into Magift/Spelldrive training. He's attending classes and doing the assignments. He's going home for the holidays. He has an internship planned. He wants to graduate.
I've enjoyed following Leona's journey of growth and self-development and seeing all the intense discussion surrounding that. It all comes from a place of love and wanting to support the characters we care about, no matter how we may individually view him.
#twst#twisted wonderland#Leona Kingscholar#disney twisted wonderland#disney twst#twst character analysis#twisted wonderland character analysis#notes from the writing raven#question#tw//depression#tw//suicidal ideation#tw//suicide#twst analysis#twisted wonderland analysis#Cheka Kingscholar#Falena Kingscholar#Farena Kingscholar#tw//substance abuse#tw//dieting#Jamil Viper#Idia Shroud#Ruggie Bucchi#Jack Howl#Savanaclaw#tw//homophobia
280 notes
·
View notes
Text
Interlude: Dumbstruck

You face up to a very adult problem in Javi’s absence that leaves you questioning your future forever.
Rating: 18+
Warnings: Angst, Discussion of Pregnancy, Pregnancy Loss, Miscarriage, Medical Setting.
A/N: Major trigger warning for this one. If you don't want to read this post, you will not lose anything from the story. There are no major plot developments or changes in their relationship. You can skip it out, or if you'd like a summary I will happily send you one. Further discussion under the cut.
Major confession that I've had this sat in the drafts for... years now due to the above, and not yet having anything lighter ready to publish to follow up... But today is the day. And happier things soon after!!
I've kept descriptors to a minimum for obvious reasons, as well as the fact that this is obviously only one experience based on personal anecdote- please don't take this as gospel, nor a universal experience.
This was originally planned to be a whole chapter but I was struggling with the heavy themes and aware that it's not everyone's cup of tea. However, I still felt like it added some important insight so wanted to keep it in some capacity so have decided to post it anyway. Keeping it as an 'interlude' also felt quite representative of the experience, in the sense that often it's an event that happens unbeknownst to people on the outside, but is a weight you carry with you. Reader/ Bug will carry on with the knowledge of that experience with her, but others will continue to move on around her none the wiser, and you can choose to do the same if it's a post you don't wish to read.
New York, Spring, Age 30: Dumbstruck
The dial tone lasts for an eternity, you’re sure. You try to focus on the way your heartbeat thrums between the beeps, double time nearly, thud, thud, thud, like a bird throwing itself against a glass pane. The skin at the edge of your fingernail is worn clean, blood starting to pool in the cuticle.
You hear the scrape of the receiver being lifted and a voice finally calls, the raspy accent filling the line.
“This is Murphy.”
“Hey Steve, can I speak to Javi, please? Now. I need to speak to him now.”
“Bug? Are you alright? You sound like you've seen a ghost. If that were possible.”
Your interactions with Steve Murphey so far had been limited.
By that, you meant you had spoken to him on the phone maybe twice, and on both occasions, you were trying to get through to Javier. The fact he’s able to recognise you immediately in spite of that is intriguing to you, and at any other moment, you’d take the time to consider the tone of affection he takes with you in just one sentence.
You try to keep your tone light but it’s impossible, the panic rising up in you like a tidal wave. You must sound worse than you think because he’s onto it in a second.
Fuck, fuck, fuck, you mumble to yourself and reach out to steady your frame against the wall in the hallway of your new apartment.
“Now,” you seethe, losing your guard completely, the tears starting to bubble at your eyelids as you lean your head back in frustration to rest on the setting plaster.
You hear the phone ripped from Murphy’s hand in a muffled frenzy and Javi’s there, breathing down the line.
“Javi-”
“What is it? Are you hurt?”
You sob then, immediately, hearing his voice, the weight of the situation finally hitting you with full force.
“I’m- I think I’m having a miscarriage,” you breathe, deadpan, utterly in shock as you hear the words pass your lips for the first time since you’d started to process.
“I can’t be sure, but…” your voice trails off quietly, giving up the guise.
It had taken you long enough to get your head around, already stunting the phone call by at least ten minutes as it was. In reality, there was no ‘think’ about it. You knew. It was impossible not to know.
Silence from the other end of the line. You hear something smash to the ground, Murphy’s indistinct words, the slow, rattling intake of Javi’s controlled breath.
“You’re pregnant?” he asks slowly, quietly, as though the words are arriving before the thoughts that spur them.
“No, I’m fucking not,” you yell between clenched teeth, trying to contain the overwhelming rage that’s bubbling up inside you. “Not now I’m not.”
Another devastating pause, and you feel the way your fingers instinctively grip the cord of the phone a little tighter, awaiting his response.
“Is it-?”
“Please, don’t,” you cut sorely, “don’t ask me that fucking stupid question right now. Javi, I’m so scared.”
You clap your hand to your mouth as the sobs start to pour out, giving in completely. The emotion is overwhelming, fear, shock, and surprise moving over you in relentless, intersecting waves, with no time to differentiate one from the next.
“Okay,” he replies firmly, taking the wheel in the only way he knows how. “Okay, it’s going to be okay.”
His tone is strong and soothing, and you can’t help but lean into its gentle familiarity. You wanted to give it up, to give over to him entirely and let him make it all okay.
“It must have been the couch,” he can’t help but shoot down the line, more to himself than to you.
“Javier.”
In the complex swell of your emotions, above all else you’re seething, unable to even fathom the possibilities surrounding what's happening right now.
You carrying his child. His baby. A life together, as forced as it may have been, suddenly wilting away without even a chance to romanticise the prospect. It was gone in the blink of an eye before you even knew you had it.
You’re furious. Like everything else, it wasn’t fair.
“I need to go home,” you sigh, trying to brush away the tears with a shaking hand as you draw together some kind of plan in your head.
You were already compartmentalising, packing away the thoughts you couldn't give yourself even a moment to dwell on.
“You need to go to the hospital. That’s the only place you need to be right now. I’ll call you straight back and I’ll be there as soon as I can but you need to get some help right now, baby. I need you to call someone who can help you out until I arrive.”
‘Baby’. In the heat of the moment, it was always ‘Baby’. Like it was a slip of the tongue reserved for special occasions; weddings that weren’t even yours. Anniversaries. Children.
But in your temperamental state, it knocks you sideways anyway, pushing you off kilter and bringing the tears to the brink again.
“Javi, please,” you keen, unsure of what you're even asking for.
You’re scared, achingly so, more so than you’d ever felt even when you were a child. This was something else, something new. You needed something stable and solid to hold on to, and he was a thousand miles away.
“I know, baby, I know. But you need to do this, for me. Just be brave and I’ll be back on the line in just a tick. Just make the call.”
You slam your fist against the phone cradle in frustration, resetting the dial tone without another word, and thumb in the number without even looking at the keys. As always, it rings once.
“Rosie?” Rasps Jack, ready and waiting, business smart except for the nickname, his favourite turn of phrase.
“Emergency,” you eke out, sinking to the floor now as you feel the sensation start to sink in, heartbreak rather than consternation hitting for the first time.
“Are you at home?” He’s deadly serious, the professional front fitting into place like a reflex.
“Yes. Medical, call Ginger. I need an ETA of 10 or less. Hospital transfer, the car will do.”
“Are you safe? Are they still in the apartment?”
“No external risk. Code O0-,” you hold your breath for the final digit, finally making it a complete reality, “3. Potentially 3.3, I’m not sure right now, I can’t remember the ICD codes.”
He hears your crying now. He understands. His heart breaks for you.
“Rosie,” he breathes.
“Please Jack, just deal with it. I’m failing every one of my training protocols right now, I know, but I just cannot handle what is happening right now. I can't do this.”
“I’m on it. Stay put. Just stay by the phone. Breathe.”
You can hear his pager going off, the shuffling of the papers moving across his desk as he stands to leave.
“And whatever you do,” he adds staunchly, “don’t look.”
“‘Don’t look’?” you repeat, but when you lift your hand from the plasterwork where you’d been steadying yourself, you see it, the way the harsh red seeps into the porous craftsmanship.
“How do you-”
“Just trust me, Darlin’. I’ll be there soon.” And the line rings dead.
Left alone, truly alone, you slump to the ground and ruminate in comfortless solitude. In the quiet stagnation of your apartment, you can only defer so far. It's fruitless to fight it. For just a moment, you let yourself sit, and think, and wait.

Jack had barely left your side in the ER, vigilant and dutiful.
His straightforward attitude was soothing and efficient, and allowed for a rare moment of surrender as he handled the overwhelming process of the inpatient clinic. Sitting by his side, you took a quiet comfort in the way his personal concern occasionally bled into his unrelenting professionalism, appreciating every squeeze of your hand, each cup of cold coffee, and every form you didn't have to read and sign.
When night came, Javi took his place, arriving on the first non-stop flight to Newark Liberty. He didn't even bring a backpack, just an unread paperback and his keys.
You try to picture the two men crossing paths in the hallway, shaking hands, nodding heads.
They’d never met. What absurd circumstances to finally come face-to-face, each an urban legend in their own right.
When he climbs up next to you to hold you close to him in the hospital bed, jacket, shoes and badge still in place, you break, the sobs wrenching from your chest like nothing you’ve ever known. There was nothing to hide, nothing to lose.
“Was it ours?” he eventually asks, his forehead never leaving your own, his voice a quiet whisper in the cavernous space of the dim room.
“Of course it was ours,” you sigh, bone-weary, drained and devastated.
“Why didn’t you say anything?”
“I didn’t know,” you say, frankly, the candour obvious in your upfront sentiment. “I wasn’t due for a medical until next month.”
“You didn’t suspect?”
“I’ve been busy. I didn’t really think, work has been a lot.”
“Would you have kept it?” he asks, more tentative still, aware of how precariously close everything feels as he reels off his pressing questions.
You hesistate, but not for long.
“Yes, probably. I’m in love with the idea of it more than anything. It’s irrelevant now, but-”
“It’s not irrelevant," he interrupts quickly. "Don’t say that. How can something we made be irrelevant?”
His fervour takes you back, even in its hushed whisper.
“Made by accident,” you huff back frustratedlym “it’s not like we knew-”
“Well, so what? We’d have been just fine. I know that. It wouldn't have mattered. We-"
“Mr. Peña," you hear from the open doorway, the tone firm but kind. "We don’t allow visitors overnight I’m afraid, only family.”
He doesn’t turn to the attendant before he replies, simply gripping you tighter, pressing his legs into yours as he holds your taut frame against his own.
“I am family.”
“Alright then,” she replies without complaint, clearly not seeing the merit in pushing it. “I’ll see you both in the morning.”
You’d been alone for less than ten minutes before he came skulking back into the room, black coffee and another round of toast in hand.
He was reluctant to be away from you for longer than a minute at a time, you could tell. He used to get like this when you were sick, or when you’d be sent home to bed from gym with bad cramps.
They’d said the tub was the best place for you at home. The heat would help, the chaos contained. He kneels down on the floor next to you, resting his arm on the enamel and laying his chin on top.
"How are you feeling?" he asks again, and you caress his cheek with a wet hand.
"Not great, but better. The peanut butter is helping."
You crack a feeble smile, but you can see the look in his eye is heavy.
“Querida, I don’t want to waste any more time.”
You bring yourself closer through the water so that your head is resting next to his, close enough for your noses to touch. He brings a hand up to tuck a strand of wet hair behind your ear, and rubs his thumb across your cheekbone.
“What do you mean?” you ask, but you know what he's saying, what he's asking. The impossible situation.
His face says as much.
“Javi, please,” you sigh, but you laugh quietly as you say it, “you know it’s not as simple as that. If anything this has proved it.”
“I don’t care,” he replies candidly, but the frustration in his voice is the overriding detail. “I don’t want to care. It shouldn’t matter. Not after things like this.”
“Javi, you just moved. You’re fighting the war on drugs for goodness sake. You really think now is the time to have a baby? To be a father?”
“I don’t care. Whatever happens with us, whenever, is the right time. You’ve always said that. I should have been here. It could have been different.”
“Don’t talk like that. Not right now. Just tell me everything’s going to be alright. We’ll get it together one day. We’re young”
“Not as young as we were,” he scoffs.
“Twenty-eight! That’s certainly not old, Javier.”
“Why can’t you just… give in? I’d have left. If you asked. I will leave. If you ask.”
“No, actually, I don't think you would," you ponder, shaking your head slightly, "and I wouldn’t ask you to. Not even now.”
Your blunt words appear to stump him, and whatever the next line of his argument was is lost and replaced with a tender kiss to your bare shoulder, his bottom lip sliding along your damp skin.
“I’m sad, Ladybug."
“So am I, Javi,” you sigh, and when you feel his quiet tears on your shoulder, you let your own follow suit.

You shift in his arms, rolling onto your back to stare at the clear night through the skylight. It was a familiar reminder of home, one you were enjoying today.
“When are you off?” you finally ask, the question becoming the second most unavoidable topic in the room.
“First thing. I shouldn’t even really be here.”
“I’m glad you are. I hope you’re not in too much trouble.”
“If I am, I am. It's a hard one for them to argue with, really."
He curls himself around you and cradles your stomach, quietly mourning the loss of something that never really was. Another future together, gone before you even had the chance to consider it.
You fall asleep wrapped in one another, just like always. But before you drift off, for one night, you talk about a future that you’ll never have.
“We couldn’t call her that,” you scold indignantly.
“Why not?" he retorts, smirking innocuously. "We never call you it. It’s a nice name.”
“It’s my mother’s name. That’s exactly why you never call me that. What kind of narcissist names their child after them?”
“Most people. My Mother’s name, then. That makes more sense, surely. Everyone loved her.”
“Pa would weep,” you sigh, lovingly.
“In a good way.”
“Would you want it to be a girl?”
He smirks, rubbing his nose against your shoulder.
“Maybe. I wouldn’t care. I’d be too excited about seeing you big and fat. Carrying my brood.”
“Why do you make that sound so filthy?” you scold.
“I’m just trying to put a positive spin on the prospect of another shotgun wedding.”
You elbow him sharply in the ribs, and he laughs.
“I could be your little harlot. We could live out of wedlock. Social exile.”
“Not a chance," he scolds, feigning shock. "I’m a man of God. We don’t actually want to kill Pa."
You snuggle into him closer, turning in his arms to come and face him.
“Do you think our family has any idea, at all?”
The look on his face is passive, but you can see the words settling somewhere. You don't know if it's the talk of home, or of something bigger; the idea that your summer fling surmounts to so much more when you give it the space to exist.
“I don't know. I wonder sometimes if Pa knows, deep down. I feel like he’s asked me before, in more ways than one. I think he asked when I told him about Lorraine. Like it was a loaded question, you know?"
"They always are with him."
“Do you think they know?” he asks.
“I don’t think they’d be surprised, necessarily. Like it’s an inevitable thing, almost.”
He holds your face between his hands then, drawing it away from his so he can look at you clearly, pulling the damp strands of hair away with broad strokes of his thumbs.
“Do you think it is? Inevitable?”
“Yes," you whisper, a clean answer, cutting through the mirth.
He kisses your upturned lips, tracing them over with the pad of his thumb before finally letting you go.
“I hope you’re right.”
“You know I always am.”
A/N: I know I mentioned dates before but I’ve actually broken my own timeline here since technically Murphy wouldn’t be in Colombia until they were at least 30, but I figured for the sake of continuity it made sense here.
Also please let me know if I've missed anyone from the tag list! I has been such a very long time 🌚
Playlist Recommendation
Taglist
@furious-rogue-stuff
@athalien
@sara-alonso
@vanemando15
@chronic-nosebleed
@mashomasho
@hnt-escape
@angelofsmalldeath-codeine
@hylasposts
#Spotify#changes#jose pedro balmaceda pascal#pedrito#narcos#narcos fanfiction#pedro pascal characters#reader insert#pedro pascal#pedrostories#javier peña x you#javi peña#javier peña#javi x bug#javi#narcos fan fiction#narcos fanfic#changes fan fiction#javier pena x you#javier pena x reader#narcos fic#bug x javi#javi x bug fanclub#javier pena#javi pena#javier peña supremacy#javier peña x reader#pedro pascal x reader
38 notes
·
View notes
Text
Arthritis medications could reverse COVID lung damage - Published Sept 6, 2024
Arthritis drugs already available for prescription have the potential to halt lingering lung problems that can last months or years after COVID-19 infections, new research from the University of Virginia School of Medicine and Cedars-Sinai suggests.
By examining damaged human lungs and developing an innovative new lab model, the scientists identified faulty immune processes responsible for the ongoing lung issues that plague an increasing number of people after they've otherwise recovered from COVID-19. These lasting harms of COVID infection, known as "post-infection lung fibrosis," have no good treatments. The new research, however, suggests that existing drugs such as baricitinib and anakinra can disrupt the malfunctioning immune response and finally allow damaged lungs to heal.
"Using advanced technologies like spatial transcriptomics and sophisticated microscopy, we compared lung tissues from patients and animal models we developed in the lab. We found that malfunctioning immune cells disrupt the proper healing process in the lungs after viral damage. Importantly, we also identified the molecules responsible for this issue and potential therapeutic options for patients with ongoing lung damage."
"'Spatial-omics' are state-of-the-arts technologies that can measure the molecular features with spatial location information within a sample," explained researcher Chongzhi Zang, PhD, of UVA's Department of Genome Sciences. "This work demonstrates the power of spatial transcriptomics combined with data science approaches in unraveling the molecular etiology of long COVID."
The researchers note that the findings could prove beneficial not just for lung scarring from COVID but for lung fibrosis stemming from other sources as well.
"This study shows that treatments used for the acute COVID-19 disease may also reduce the development of chronic sequelae, including lung scarring," said Peter Chen, MD, the Medallion Chair in Molecular Medicine and interim chair of the Department of Medicine at Cedars-Sinai. "Our work will be foundational in developing therapies for lung fibrosis caused by viruses or other conditions."
Understanding COVID-19 lung damage
The researchers – led by Sun, Chen and Zang – wanted to better understand the cellular and molecular causes of the lingering lung problems that can follow COVID infections. These problems can include ongoing lung damage and harmful inflammation that persists well after the COVID-19 virus has been cleared from the body.
The researchers began by examining severely damaged lungs from transplant patients at both UVA and Cedars-Sinai. None of the patients had a lung disease that would have required a transplant prior to contracting COVID-19, so the scientists were hopeful that the lungs would provide vital clues as to why the patients suffered such severe lung damage and persistent fibrosis. Using the insights they obtained, the scientists then developed a new mouse model to understand how normally beneficial immune responses were going awry.
The researchers found that immune cells known as CD8+ T cells were having faulty interactions with another type of immune cell, macrophages. These interactions were causing the macrophages to drive damaging inflammation even after the initial COVID-19 infection had resolved, when the immune system would normally stand down.
The scientists remain uncertain about the underlying trigger for the immune malfunction – the immune system may be responding to lingering remnants of the COVID-19 virus, for example, or there could be some other cause, they say.
The new research suggests that this harmful cycle of inflammation, injury and fibrosis can be broken using drugs such as baricitinib and anakinra, both of which have already been approved by the federal Food and Drug Administration to treat the harmful inflammation seen in rheumatoid arthritis and alopecia, a form of hair loss.
While more study is needed to verify the drugs' effectiveness for this new purpose, the researchers hope their findings will eventually offer patients with persistent post-COVID lung problems much-needed treatment options.
"Tens of millions of people around the world are dealing with complications from long COVID or other post-infection syndromes," Sun said. "We are just beginning to understand the long-term health effects caused by acute infections. There is a strong need for more basic, translational and clinical research, along with multi-disciplinary collaborations, to address these unmet needs of patients.
Journal reference:
Narasimhan, H., et al. (2024). An aberrant immune–epithelial progenitor niche drives viral lung sequelae. Nature. doi.org/10.1038/s41586-024-07926-8
www.nature.com/articles/s41586-024-07926-8
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator
19 notes
·
View notes
Text
Medical astrology
This article draws inspiration and is based on information found in two notable books: "Complete Practical Astrology" by Edward Lyndoe, published in 1938, and "Complete Herbal" by Nicholas Culpeper, dating back to 1652. It's not uncommon for individuals with a stellium in a specific zodiac sign to experience health issues associated with that sign more prominently compared to those with just one planet in that sign. The concentration of planetary energy in one sign can intensify the characteristics and tendencies associated with it, including health-related aspects.
The history behind it
In early-modern Europe, people held a deep fascination with the connection between celestial bodies and our well-being. This belief traced back to ancient notions of the Four Elements and the Four Humors, forming the basis of humoral theory in medicine. Originating with Hippocrates and evolving through Galen, this theory centered on balancing bodily fluids: blood, phlegm, black bile, and yellow bile. Men were seen as hot and dry, while women were considered cold and wet. Dietary choices and flavors were believed to influence humor balance.
These ancient ideas were intricately linked to Zodiac signs, seasons, cardinal directions, qualities, temperaments, and life stages. People believed that our health relied on maintaining a delicate equilibrium among these factors, shaping a complex system that demanded precise language to explain.
As interest in astrology grew in the 16th century, printed books, such as "Planetary Books" and "Folk Calendars," became popular sources of knowledge. These texts provided valuable insights, bridging the gap between celestial and earthly realms. They aimed to empower readers with wisdom about their place in the universe.
Aries: rules over the head, face, eyes, and the brain's cognitive functions, influencing the distribution of both mental and physical energy. This sign is associated with health concerns like headaches, fevers, neuralgia, eye issues, skin eruptions, inflammations, wounds, and accidents. Individuals born under Aries may have an abundance of energy, often exceeding their mental and emotional balance. Many health issues can be traced back to factors such as excessive physical exertion or bouts of intense anger. It's advisable for Aries individuals to prioritize maintaining a sense of balance and inner poise to promote their overall well-being.
Taurus: you should know that your sign is linked to certain areas of your body like the neck, ears, throat, larynx, and tonsils. These body parts might need a little extra care. Your sign is also associated with your ability to recover from health issues. However, it's important to be mindful of diseases that can specifically affect your throat. One thing to keep in mind is that Taurus individuals often have a love for indulgence and comfort, which can sometimes lead to health challenges. Additionally, your tendency to dwell on problems might make you more sensitive to minor health issues. So, remember to strike a balance and take good care of your well-being.
Gemini: For those born under the sign of Gemini, certain areas of the body require attention. Gemini influences the arms, shoulders, muscles, and bones, as well as the respiratory system, including the trachea and bronchi, and even the hands. People with this sign may be more prone to health issues like bronchial complaints, lung conditions such as pneumonia and pleurisy, nerve-related diseases, asthma, and anemia. These health challenges can often be traced back to nervous reactions and restlessness, which are characteristic of Gemini individuals.
Cancer: you have an influence on various parts of the body, including the stomach, breasts, solar plexus, diaphragm, and the upper portion of the liver. These areas are closely tied to matters of nutrition and digestion. Health issues that commonly afflict those born under Cancer often originate from emotional factors, triggered by mental irritants. These emotional disturbances can lead to nervous reactions and a general decrease in vitality. Interestingly, it's been suggested that more often than not, the health of a Cancerian is affected by external factors and the actions of others rather than self-inflicted harm. So, it's important for Cancer individuals to prioritize their emotional well-being and maintain a harmonious environment to support their overall health.
Leo: you have a special connection with the heart, spine, and vital forces carried by the blood. This makes you particularly susceptible to issues like heart troubles and poor circulation. Remember, many of these health challenges can be linked to overexertion or pushing yourself too hard. So, take good care of your energy levels and avoid unnecessary strain to keep your health in top shape.
Virgo: you have a unique connection with your own digestive system, which encompasses your intestines, alimentary canal, and the lower part of your liver. However, it's essential to recognize that individuals born under this sign might also be more prone to experiencing digestive issues and complaints, especially concerning the intestines. For you, these digestive troubles could occasionally stem from nervous causes, potentially leading to discomforts like acidity and other digestive challenges. It's a part of your unique astrological makeup, emphasizing the importance of taking extra care of your digestive well-being and managing any stress or anxiety that might contribute to these issues.
Libra: you are associated with specific areas of the body, including the kidneys, loins, appendix, lumbar vertebrae, and the skin. These are related to the body's liquid processes. Health challenges that often affect Virgos include kidney problems and issues related to the spine. These troubles are frequently linked to nervous exhaustion. To maintain your well-being, it's crucial for Virgos to manage stress and avoid situations that lead to nervous strain.
Scorpio: your zodiac sign governs several vital areas of the body, including the organs of reproduction, bladder, gallbladder, colon, and rectum. These parts are closely tied to procreation and reproduction. Health issues frequently associated with Scorpios involve the organs mentioned earlier. Problems may arise due to excessive worrying and the influence of others on the individual, which can break down resistance. To maintain good health, it's important for Scorpios to find ways to manage stress and emotional pressures effectively.
Sagittarius: you have a connection to certain body areas like the hips, thighs, and sciatic nerves. These parts are linked to your senses and how you perceive illnesses through your nerves. Health issues that Sagittarians often face include conditions like gout, rheumatism, and sciatica, as well as accidents. Restlessness can be a contributing factor to these problems, and individuals under this sign may have a propensity for accidents and injuries. Therefore, it's essential for Sagittarians to cultivate a sense of caution and mindfulness to prevent such mishaps and maintain their well-being.
Capricorn: you have an influence on the knees, joints, and hair. These are connected to processes related to preservation and conserving energy. Health issues commonly associated with Capricorns include skin complaints and diseases affecting the parts of the body influenced by this sign. Such ailments often have their origins in inhibitions. Therefore, it's important for Capricorns to focus on finding a balance between preserving energy and addressing any emotional or mental inhibitions that may impact their well-being.
Aquarius: your influence goes to the lower legs (calves and ankles), teeth, and blood circulation. These areas are interconnected with the body's circulation and eliminative processes. Health issues often associated with Aquarians include accidents affecting the ankles, as well as complaints related to this part of the body. Conditions such as varicose veins, blood poisoning, and certain nervous diseases may also be relevant. Many of these health challenges may have nervous causes, often tied to the highly sensitive nature of those born under the Aquarius sign. Therefore, maintaining emotional balance and managing stress is crucial for overall well-being.
Pisces your zodiac sign influences specific areas of the body, including the feet and toes. These are related to perspiration and the lymphatic processes within the body. Health challenges often associated with Pisceans include conditions like influenza, colds, and diseases accompanied by mucous discharges. Many of these complaints may have their origins in an overactive or overheated mind, possibly with perceived injuries from others. Additionally, individuals born under the Pisces sign tend to exhibit a high level of physical and mental sensitivity, which can contribute to various health issues. Therefore, it's important for Pisceans to manage stress, maintain emotional balance, and address any perceived injuries to promote overall well-being.
#astro observations#astro community#astro placements#astrology#all signs#astro notes#asteroid#astrologer#for you#zodiac placements#medical astrology
83 notes
·
View notes
Text


The First World War for many German artists was a catalytic experience that changed their work forever. Although Max Beckmann “only” volunteered as medical orderly and unlike e.g. Otto Dix didn’t sit tight in the trenches, the experience initiated a drastic shift in his work: where before Beckmann had dealt with historical topics in a late impressionist idiom that channeled influences from Rembrandt, Goya and early Cézanne, from 1915 onwards his style developed into what he himself coined „transcendental objectivity“, an amalgamation of Expressionism, Cubism and late medieval art. It was a direct reaction to the horrors he was confronted with as medical orderly and followed a nervous breakdown in the same year: biblical scenes, crammed into tight spaces and painted in a flat instead of spatial manner from now on are the new direction in Beckmann’s oeuvre. In brutal, almost nightmarish tableaus classical scenes like „Descent from the Cross“ and „Christ and the Sinner“ Beckmann processed the turmoils of war and the societal upheaval it triggered way beyond the end of the war.
Late last year the Neue Galerie in New York dedicated a comprehensive exhibition to Max Beckmann’s formative years between 1915 and 1925 which was accompanied by the eponymous catalogue published by Prestel. In crisp reproductions it features the paintings, drawings and lithographs presented in the exhibition but also features insightful essays by curator Olaf Peters and others. The former provides an excellent analysis of the artists’ dramatic stylistic changes and his reaction to postwar Germany with a particular focus on the disabled veterans. In the lithographic portfolio „Hell“ from 1919 he depicts the traumatized survivors and takes a biting satirical look on postwar society that also represents a link to his later Circus-themed works.
What both exhibition and catalogue quite plainly show is the incredible urgency contained in Beckmann’s works between 1915 and 1925 and with what radicality he reacted to the fault lines in postwar society. At the same time this period forms the basis for all the later works, one of the many reasons for me to warmly recommended the catalogue!
#max beckmann#art book#expressionism#modern art#new objectivity#art history#exhibition catalogue#prestel
27 notes
·
View notes
Note
Crime writer Tony actual assassin bucky,
I am so bad at crime rest in pieces Tony lmao.
Tony sort of... falls into writing accidentally. Rhodey joins a book club in college and Tony joins with him because he's codependent and after the first three books, they read a frankly abysmal adaption of the Black Dahlia murder. Unfortunately, Tony is the best at working out of spite, so as soon as 'man, even I could write a better and more respectful novel than this,' it just sort of... happens. Rhodey is the first person he shows, nervous and antsy. Rhodey has the best poker face Tony's ever seen, even better than Howard and Obie's. He had no idea what Rhodey thinks of it.
Finally, Rhodey looks up at him, and he says, "This was really good, but it could be better. I'm giving it to the book club." Tony wails in dismay because he's a perfectionist when it comes to showing things off, but Rhodey drags him to book club kicking and screaming, because they're mostly English majors and they'll have more insight than he does. The book club rips it to shreds, but they tell him exactly why, and his second draft barely has any red marks on it at all when they read it.
While Tony's in college, he publishes his novels under a pen name, and his book club are his editors. Once he graduates, he starts publishing under his own name, with part of the proceeds going into two non-profits--a book club and a writers workshop for underprivileged youth.
Bucky's descent into serial killing is not an accident at all. One of his sisters is beaten almost to death by her boyfriend, and when the guy only gets a slap on the wrist by the courts because it's his first offense, Bucky makes him disappear. The only other person who knows is Steve, mostly because they're so close he would have found out anyway. Luckily, the most Steve ever says about it is, "Don't tell me anything. I'm a bad liar."
He figures part of it is because Steve had been with him when they'd found his sister bleeding and unconscious on her apartment floor. He'd seen Steve's jaw clench at the hearing when the guy was let off on probation. His rage that the system was failing someone who had almost been murdered by an intimate partner. Steve had decided to throw himself into getting laws changed, harsher sentences. It was slow going. It was probably the only reason he turned a blind eye when Bucky decided to take a more... hands on approach.
Tony and Bucky, miraculously, meet when Bucky sneaks into his apartment. Or, well, "meet." Tiberius had just been let off assault charges simply because he was rich, and Tony hadn't gotten a chance to change the locks because he was in the hospital recovering from being strangled. Bucky had meant to sneak in and kill Tiberius while Tony was still at the hospital, so he'd have an alibi.
But apparently Tony had signed out of the hospital against medical advice to avoid the press, and Bucky had snuck into his apartment to find Tiberius backhanding him to the ground. So he simply stepped further into the apartment and snapped Tiberius's neck. Clean. Efficient. Fast enough that Tony, dazed and bleeding from a head wound again, wouldn't realize it.
"Let's get you cleaned up," Bucky says gently, helping Tony to his feet.
"But Tiberius--" Tony starts, lip bleeding as well.
"He's sleeping," Bucky assures him, and helps Tony to the bathroom to clean him up. Calls a friend to come sit with him because he's adamant he's not going to the hospital. Gets him tucked onto the couch with a milkshake and an old sci-fi movie in the background. Grabs Tiberius by the scruff to drag him out.
"So dinner? Tomorrow? With me?" Tony slurs, blinking doe eyes at him.
"Sure," Bucky agrees, good-natured, and expects to never see him again.
"So," Tony says, tablet and stylus in hand. "What's the easiest way to kill somebody."
"We are at my job," Bucky complains immediately, grabbing him by the arm to drag him over to the antique book section. "How did you find me?"
"I'm Tony Stark," Tony says, and then, "Also I follow Steve on Instagram and there are pictures of you with him. I asked where you worked and he's a bad liar."
"He really isn't, he just panics," Bucky says. He sighs, crossing his arms over his chest, and does not mention that the way Tony is checking out his biceps are not subtle. "Why do you follow Steve?"
"I like the work he's doing to get more stringent laws for domestic violence," Tony tells him seriously, and Bucky throws his hands up in frustration. "Anyway. Do you wanna go get lunch?"
"You watched me k--" Bucky begins, outraged, then swallows it back and takes a deep breath. He glances around to make sure they're still alone, then whispers, "You watched me kill your ex-boyfriend."
"He was going to kill me," Tony says, shrugging. "The bar is on the floor."
"Jesus Christ," Bucky moans, dragging his hands down his face.
Tony has the self-preservation of a gnat and keeps inviting Bucky out. Bucky is absolutely appalled. He's dangerous. Tony has seen him kill somebody. And he still wants to have dinner?
"And raunchy sex that makes me blush when I remember it maybe," Tony offers, shrugging. "Tiberius didn't usually even get me to come."
Somehow Bucky is not surprised and yet still incredibly offended on Tony's behalf. "Well, I'm pretty good in bed," he says mulishly, because it's not fair that Tony hasn't had a partner that cared about his pleasure in bed recently. And then somehow he gets locked down into a long-term relationship. He is absolutely stunned.
"Tony's like that," Steve tells him, and then, "Actually I'm surprised this didn't happen sooner. Please tell Tony to stop telling me how good you are in bed."
"You tell Tony to stop asking me to show him how to kill people for his books," Bucky retorts, and then they both stare at each other, stone faced, as they realize oh. So this is just what Tony's like then.
Bonus: Tony goes back to his old pen name so he can write self-published raunchy romance novels of a writer and his serial killer boyfriend. Bucky is mortified but also aroused. Tony coyly asks him what he'd do in the killer character's position in the bedroom and Bucky is FURIOUS that it gets him horny. It doesn't stop him from showing Tony, though.
#aurumacadicus answers#ask meme#5 headcanons meme#winteriron#tw: domestic violence#tw: domestic abuse#not between tony and bucky tho
135 notes
·
View notes
Text
The V. Vale Value-Pak
*Who reads the bizarre, out-there maunderings of this eccentric San Francisco punk publisher known to the world as "V. Vale," well, obviously Rudy Rucker and Bruce Sterling both do.
*******************************************************
I started reading at age four and early on began memorizing “aphorisms”, although I didn’t learn that word till much later.
My earliest books that were really mine were some volumes of The Book of Knowledge, which introduced me to extreme history and anthropology (the gladiator conflicts in the Roman Coliseum games; an article on New Guinea natives, etc).
I had an illustrated paperback on “world’s weirdest animals” (not the real title; can’t remember that) which introduced me to genre-crossing life forms like the platypus, the Komodo dragon, the Bower Bird, etc.
The real eye-opener was a hardback medical textbook which contained a close-up B&W photograph of the genitals of a hermaphrodite (!). So when I found myself hanging out in libraries, did I restrict myself to children’s books? No; I looked at every book in the library, regardless of “category”.
Recently RE/SEARCH published a book (thanks to a brilliant assistant editor) called Quotes by Vale. I just turned at random to a quote on page 102:
“CORPORATE MEDIA: Whatever the OFFICIAL NARRATIVE, the Real Truth is Always The Opposite”.
And that in a nutshell is my driving motivation to publish. That’s it!
We’re about to enter 2024 — that year will mark my 47th year as a publisher (since the first issue of Search & Destroy).
And that’s when the idea of a V. VALE VALUE-PAK hit me! So obvious I never thought of it before!
I’ve spent my whole life promoting OTHER PEOPLE, so now maybe I can at least TRY to induce people to read my own writing and thoughts.
Well, they actually appear in all RE/Search books, although less obviously.
So, why not?
The V. Vale Valu-Pak contains...
My most recent books:
1.UNDERGROUND LIVING: V. Vale Photos (color and B&W, with an insightful introduction by author Rudy Rucker)
2. MESSAGE FROM YOUR EDITOR (essays from the past 20 years, with a brilliant introduction by author Bruce Sterling)
3. VALE QUOTES (my aphorisms)
My two zines:
4. HOW TO READ (includes HOW TO WRITE, a 1-page zine)
5. TERMINAL PUNK (my attempt to write the “best” “philosophy of punk” publication)
The 4 zines that cartoonist extraordinaire Krusty Wheatfield did on V. Vale:
6. SEARCH FOR WEIRD #0
7. SEARCH FOR WEIRD #1+2
8. SEARCH FOR WEIRD #3
9. HOW TO STAY TOGETHER FOREVER
I hope that at least a few readers of this newsletter will take a chance and order the V. VALE VALU-PAK, aided and abetted by a big discount.
Total retail value is usually $135… but we offer a 20% off New Year special price: $105!
And in the US you’ll only pay $5 shipping.
But the offer expires on Friday night (Jan 5, 2024).
I’m still having trouble sleeping (uh, thanks for all your suggestions) so maybe THAT'S why my brain thought of this (hare-brained) “idea”?!?
Here’s the link with all the details:
Thanks for reading this far,
Your Editor,
V. Vale
V. Vale New Year's ValuPak
Three books and 6 zines featuring V. Vale “front and center”! Get all of the V. Vale items at an OVER 20% discount: $135 value for $105. New Year’s Special through Friday night Jan 5, 2024.
$105.00Shop
RE/Search Publications
20 Romolo #B
San Francisco, CA, 94133
US
Unsubscribe
40 notes
·
View notes
Text
By: Eric W. Dolan
Published: Sept 20, 2024
A new study published in Proceedings of the National Academy of Sciences suggests that specific networks in the brain, when damaged, may influence the likelihood of developing religious fundamentalism. By analyzing patients with focal brain lesions, researchers found that damage to a particular network of brain regions—mainly in the right hemisphere—was associated with higher levels of fundamentalist beliefs. This finding provides new insight into the potential neural basis of religious fundamentalism, which has long been studied in psychology but less so in neuroscience.
Religious fundamentalism is a way of thinking and behaving characterized by a rigid adherence to religious doctrines that are seen as absolute and inerrant. It’s been linked to various cognitive traits such as authoritarianism, resistance to doubt, and a lower complexity of thought. While much of the research on religious fundamentalism has focused on social and environmental factors like family upbringing and cultural influence, there has been growing interest in the role of biology. Some studies have suggested that genetic factors or brain function may influence religiosity, but until now, very little research has looked at specific brain networks that could underlie fundamentalist thinking.
The researchers behind this study wanted to address a critical gap in understanding how brain lesions might affect religious beliefs, particularly fundamentalism. Prior research suggested that damage to the prefrontal cortex could increase fundamentalist attitudes, but this work was limited to small sample sizes and focused only on one part of the brain. The authors of the study hypothesized that instead of a single brain region being responsible, religious fundamentalism might arise from damage to a distributed network of connected brain regions.
“My primary interest is and has been mystical experience. But in the process researching the cognitive neuroscience of mystical experience, I came across brain network associations with religious fundamentalism,” study corresponding author Michael Ferguson, an instructor in neurology at Harvard Medical School and director of Neurospirituality Research at the Center for Brain Circuit Therapeutics.
To explore whether damage to specific brain networks could influence the likelihood of holding religious fundamentalist beliefs, the researchers used a method called lesion network mapping, which helps identify how different regions of the brain are connected and how damage to one area might disrupt related brain functions. The study involved two large groups of patients with focal brain damage, giving the researchers a unique opportunity to analyze how different types of brain lesions might be linked to religious beliefs.
The first group consisted of 106 male Vietnam War veterans who had sustained traumatic brain injuries during combat. These men, aged between 53 and 75 at the time of brain imaging, were part of a long-term study conducted at the National Institutes of Health. The second group included 84 patients from rural Iowa who had experienced brain injuries from various causes, such as strokes, surgical resections, or traumatic head injuries. This second group was more diverse in terms of gender and had a broader range of injury causes.
Both groups completed a scale designed to measure religious fundamentalism, which asked participants to respond to statements reflecting rigid and inerrant religious beliefs, such as the view that there is only one true religion or that certain religious teachings are absolutely correct and unchangeable.
For each participant, the researchers mapped the precise locations of their brain lesions using advanced imaging techniques like computerized tomography (CT) and magnetic resonance imaging (MRI). These scans were then analyzed using lesion network mapping to see how damage to certain brain areas was connected to changes in religious fundamentalism scores. The researchers also compared the brain lesion data to a larger database of lesions associated with various neuropsychiatric and behavioral conditions, which helped them understand how the brain regions linked to religious fundamentalism overlap with those involved in other psychological traits.
The researchers found that damage to certain areas of the brain, particularly in the right hemisphere, was associated with higher scores on the religious fundamentalism scale. Specifically, lesions affecting the right superior orbital frontal cortex, right middle frontal gyrus, right inferior parietal lobe, and the left cerebellum were linked to increased religious fundamentalism. In contrast, damage to regions such as the left paracentral lobule and the right cerebellum was associated with lower scores on the fundamentalism scale.
“The strength and reproducibility of the signal between psychological self-report measures of religious fundamentalism and the functional networks we identified in the brain surprised me,” Ferguson told PsyPost. “It increases confidence in the results.”
Interestingly, the researchers noted that the brain regions identified in this study are part of a broader network connected to cognitive functions like reasoning, belief formation, and moral decision-making. These areas are also associated with conditions like pathological confabulation—a disorder where individuals create false memories or beliefs without the intent to deceive. Confabulation is often linked to cognitive rigidity and difficulty in revising beliefs, characteristics that are also found in individuals with high levels of religious fundamentalism.
The researchers also found a spatial overlap between brain lesions associated with criminal behavior and this fundamentalism network, which aligns with previous research suggesting that extreme religious beliefs may be linked to hostility and aggression toward outgroups.
“It’s sobering, but one of the takeaway findings is the shared neuroanatomy between religious fundamentalism, confabulations, and criminal behavior,” Ferguson said. “It refocuses important questions about how and why these aspects of human behavior may be observed to relate to each other.”
The researchers emphasize that damage to this brain network does not guarantee that a person will develop fundamentalist beliefs, nor does it imply that individuals with strong religious convictions have brain damage. Instead, the findings point to the possibility that certain brain networks influence how people process beliefs and how flexible or rigid their thinking becomes, especially in the context of religion.
“A major caveat is that these results do not indicate that people with strong religious beliefs confabulate or that individuals high in religious fundamentalism commit crimes,” Ferguson explained. “Rather, our data may help us understand the style of cognitive or emotional processing that increase or decrease the probability of holding fundamentalism attitudes.”
The authors suggest that future research should explore how this brain network influences religious fundamentalism in more diverse populations, including people from non-Christian religious traditions or from different cultural backgrounds. It would also be valuable to study patients both before and after brain injuries to better understand how changes in the brain might affect religious beliefs over time. Additionally, research could investigate how this brain network relates to other types of belief systems, such as political ideologies or moral convictions, to see if similar patterns of cognitive rigidity or reduced skepticism emerge in these contexts.
“The personal beliefs of the authors span a broad continuum from adherents of religious faiths through agnosticism to atheism,” Ferguson noted. “We approach the weighty subject matter of this research as earnest seekers of scientific data and encourage readers to receive our results in the spirit of open-minded empirical inquiry driven by scientific curiosity and without prejudice or malice to any group or faith.”
The study, “A neural network for religious fundamentalism derived from patients with brain lesions,” was authored by Michael A. Ferguson, Erik W. Asp, Isaiah Kletenik , Daniel Tranel, Aaron D. Boes, Jenae M. Nelson, Frederic L. W. V. J. Schaper, Shan Siddiqi, Joseph I. Turner, J. Seth Anderson, Jared A. Nielsen, James R. Bateman, Jordan Grafman, and Michael D. Fox.
--
Significance
Religious fundamentalism is a global and enduring phenomenon. Measuring religious fundamentalism following focal brain damage may lend insight into its neural basis. We use lesion network mapping, a technique that uses connectivity data to identify functional brain networks, to analyze two large, independent datasets of brain lesion patients. We found a network of brain regions that, when damaged, are linked to higher religious fundamentalism. This functional network was lateralized to the right hemisphere and overlaps with the locations of brain lesions associated with specific neuropsychiatric and behavioral conditions. Our findings shed light on neuroanatomy that may influence the emergence of religious fundamentalism, offering implications for understanding the relationship between brain networks and fundamentalist behavior.
Abstract
Religious fundamentalism, characterized by rigid adherence to a set of beliefs putatively revealing inerrant truths, is ubiquitous across cultures and has a global impact on society. Understanding the psychological and neurobiological processes producing religious fundamentalism may inform a variety of scientific, sociological, and cultural questions. Research indicates that brain damage can alter religious fundamentalism. However, the precise brain regions involved with these changes remain unknown. Here, we analyzed brain lesions associated with varying levels of religious fundamentalism in two large datasets from independent laboratories. Lesions associated with greater fundamentalism were connected to a specific brain network with nodes in the right orbitofrontal, dorsolateral prefrontal, and inferior parietal lobe. This fundamentalism network was strongly right hemisphere lateralized and highly reproducible across the independent datasets (r = 0.82) with cross-validations between datasets. To explore the relationship of this network to lesions previously studied by our group, we tested for similarities to twenty-one lesion-associated conditions. Lesions associated with confabulation and criminal behavior showed a similar connectivity pattern as lesions associated with greater fundamentalism. Moreover, lesions associated with poststroke pain showed a similar connectivity pattern as lesions associated with lower fundamentalism. These findings are consistent with the current understanding of hemispheric specializations for reasoning and lend insight into previously observed epidemiological associations with fundamentalism, such as cognitive rigidity and outgroup hostility.
==
Two of the authors of the above paper also published the following:
Abstract
Background
Over 80% of the global population consider themselves religious, with even more identifying as spiritual, but the neural substrates of spirituality and religiosity remain unresolved.
Methods
In two independent brain lesion datasets (N1 = 88; N2 = 105), we applied lesion network mapping to test whether lesion locations associated with spiritual and religious belief map to a specific human brain circuit.
Results
We found that brain lesions associated with self-reported spirituality map to a brain circuit centered on the periaqueductal gray. Intersection of lesion locations with this same circuit aligned with self-reported religiosity in an independent dataset and previous reports of lesions associated with hyper-religiosity. Lesion locations causing delusions and alien limb syndrome also intersected this circuit.
Conclusions
These findings suggest that spirituality and religiosity map to a common brain circuit centered on the periaqueductal gray, a brainstem region previously implicated in fear conditioning, pain modulation, and altruistic behavior.
--
For reference, I previously posted about a similar study from 2017:
Abstract
Beliefs profoundly affect people's lives, but their cognitive and neural pathways are poorly understood. Although previous research has identified the ventromedial prefrontal cortex (vmPFC) as critical to representing religious beliefs, the means by which vmPFC enables religious belief is uncertain. We hypothesized that the vmPFC represents diverse religious beliefs and that a vmPFC lesion would be associated with religious fundamentalism, or the narrowing of religious beliefs. To test this prediction, we assessed religious adherence with a widely-used religious fundamentalism scale in a large sample of 119 patients with penetrating traumatic brain injury (pTBI). If the vmPFC is crucial to modulating diverse personal religious beliefs, we predicted that pTBI patients with lesions to the vmPFC would exhibit greater fundamentalism, and that this would be modulated by cognitive flexibility and trait openness. Instead, we found that participants with dorsolateral prefrontal cortex (dlPFC) lesions have fundamentalist beliefs similar to patients with vmPFC lesions and that the effect of a dlPFC lesion on fundamentalism was significantly mediated by decreased cognitive flexibility and openness. These findings indicate that cognitive flexibility and openness are necessary for flexible and adaptive religious commitment, and that such diversity of religious thought is dependent on dlPFC functionality.
--
It should be noted that fundamentalism is not exclusive to (traditional) religions.
“… fundamentalism, properly understood, is not about religion. It is about the inability to seriously entertain the possibility that one might be wrong. In individuals such fundamentalism is natural and, within reason, desirable. But when it becomes the foundation for an intellectual system, it is inherently a threat to freedom of thought.”
-- Jonathan Rauch, “Kindly Inquisitors: The New Attacks on Free Thought”
Flat Earth, anti-vax and wokery (modern feminism, "anti-racism," "gender identity" ideology, fat activism, etc) are all fundamentalist in nature. There is no evidence you can present to disabuse them of the tenets of their faith.
This phenomenon creates a problem for society in dealing with fundamentalist and false beliefs, especially when they have attained cultural dominance and institutional power. And particularly when they're held to be inerrant and absolute, and those who hold them regard dissent as heretics, and those who follow available evidence as evil. A good test for this is to look at the reaction when the belief is questioned; is the questioner regarded as factually wrong or morally suspect?
#fundamentalism#religious fundamentalism#false beliefs#inerrancy#unfalsifiable#religion#religion is a mental illness
14 notes
·
View notes
Text

How Prions Proceed
Insight into the mechanisms of prion protein replication, spread and aggregation in neuronal cells
Read the published research article here
Image from work by Juan Manuel Ribes and Mitali P. Patel and colleagues
Medical Research Council Prion Unit at UCL, Institute of Prion Diseases, University College London, London, UK
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Nature Communications, December 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#biology#neuroscience#prions#cjd#bse#mad cow disease#immunofluorescence#neurons#brain
33 notes
·
View notes
Note
sorry if you've been asked this before but have you gone to college or are you interested? a lot of my fav writers went to pretty prestigious places and have masters or phds etc and i was the type of person who never thought i'd be able to go to school for writing (or anything really) but i'm gonna try this upcoming school year. would love any insight you have if any <3
my feelings on further education for writing are complicated, but to put it out there at the top: i did not go to college & do not consider it necessary to be published
i did not apply to college in high school, which was highly controversial according to teachers, who insisted i need to at least look. i had some poor grades (almost failed creative writing, almost failed sophomore english) & did not attend many after school programs. i skipped class, had a suspension on record for fighting, & i was deeply deeply clinically depressed. i was in therapy, on medication, & could not see that another few years of school would suit me, especially because i was trying to come out as trans in a small school & that exhausted & despaired me. i did not have savings, scholarship offers, & my parents had told me since childhood that any secondary education would be my responsibility
i would like to go to college now i think, or at least attend more workshops & small classes for poetry & fiction, but i still feel it is very unlikely. education costs are too high for me to consider it an agreeable sacrifice for those experiences & connections. if i had the chance to go somewhere for writing, it would have to be within a financial margin that seemingly does not exist for current college costs & i refuse to take out loans, especially when i would rather work a day job & further my transition
i think it is very possible to educate yourself. there are lots of online resources available that can provide you with lessons, prompts, readings, & "homework". one key element, that ive discussed with other published friends, is that doing it alone... means you are that: alone. there is a lot of value in being taught by someone or someones who can answer your questions & give you a uniquely human perspective. i have taught myself a lot privately, but it does come with a sometimes crushing distance that can feel downright alienating, if not discouraging. there is a thrill in discussing poetry in a group that cannot be replicated in solitude
on the other hand, i think experiences cannot be taught in a classroom. to write, you must live first. you have to have material & it is difficult to craft material when you are entirely occupied with study. heartbreak, loss, love, wonder, can all happen during college, & even college is its own experience, but i do think there is a lot of overlooked value in people who just do... people things without wondering if it'll make a good poem
when i went to a writing retreat last year, i was the only man to attend (or ever apply!) & the only person in the group to not have gone to, or actively be in, college. i was torn between thinking i was an outsider, because everyone around me was "better educated" & feeling like id accomplished something all on my own
so... at the end of the day, i think it is entirely personal whether someone goes to college for writing. i know people who have gone & loved it & others who did not find it useful. i think these depend upon yourself, the school, your style, what you're hoping to achieve, etc. i think most of all it's deeply important to learn with other people when you can, to talk to people about poetry, to go to readings & subscribe to journals & visit libraries & take notes. how that is done is up to you
144 notes
·
View notes
Text
BFRB Resources for Struggles Like Ours
These resources vary from reliable sites and blogs to published journal articles, professional papers, books, and more. If you have any recommendations for me, feel free to Submit something.
A separate post for tips, tricks, and non-affiliate product recommendations will be linked here as soon as I've posted it.
Now then, some of you may be wondering...
What is a BFRB?
Body-focused repetitive behaviors are among the most poorly understood, underdiagnosed, and untreated group of mental health disorders.
According to the TLC Foundation for BFRBs:
"Body-focused repetitive behaviors (BFRBs) include any repetitive self-grooming behavior that involves biting, pulling, picking, or scraping one’s own hair, skin, lips, cheeks, or nails that can lead to physical damage to the body and have been met with multiple attempts to stop or decrease the behavior."
(From the TLC Foundation's webpage, "What is a BFRB?")
The PickingMe Foundation says:
"BFRB's are self-grooming behaviors in which individuals pull, pick, scrape, or bite their own hair, skin, or nails, resulting in damage to the body. Many people are more familiar with its sister disorder, Trichotillomania - Hair Pulling Disorder."
(From the PickingMe Foundation's webpage, "What is Dermatillomania?")
The Recovery Village describes BFRBs as:
"Body-focused repetitive behaviors (BFRBs) are a group of mental health conditions that cause people to bite, pick, pull or scrape their skin, hair or nails compulsively. While some people with BFRBs have awareness and insight into their behaviors, others do them automatically. BFRBs are often linked with disorders like anxiety or substance abuse. Treatment is essential for people with BFRBs, but many often hide evidence of these harmful actions and have trouble asking for help."
(From The Recovery Village's webpage, "Body-Focused Repetitive Behaviors")
According to Angela Hartlin's skin-picking support website:
Body- Focused Repetitive Behaviours (BFRB’s) “is an umbrella term for any chronic behavior that causes a person to consistently cause physical damage to oneself unintentionally through a compulsive act in order to relieve anxiety.” The key difference between BFRB and other compulsive behaviours that cause harm to the body is that BFRBs are characterised by direct body-to-body contact. The website goes on to list other BFRBs such as: hair-pulling disorder (trichotillomania), hair eating disorder (trichophagia), skin biting disorder (dermatophagia), nail biting disorder (onychophagia), and nose picking disorder (rhinotillexomania).
Getting BFRBs officially classified as disorders has been a long, slow process that only hurts those of us who struggle with them daily, as treatments and available resources relating to BFRBs can be very difficult to find. That's the reason why I'm composing this. I'll keep updating this post to the best of my abilities, both for myself and for anyone else it might help.
The good news is that while progress may be slow, there is still progress. Dermatillomania was finally added to the DSM-V-TR under the same OCD-Related Disorders umbrella as Trichotillomania, which has been a big step in the right direction. The more awareness brought to BFRBs, the sooner more can be recognized for what they are so the people suffering from them can receive proper medical and psychiatric help where necessary.
Are BFRBs a type of self-harm?
No.
While the two are not mutually exclusive, the general consensus seems to be that where self-harm is voluntary, BFRBs are grooming behaviors that have gone awry to the point that they are categorized as "OCD-Related Behaviors" in the DSM-V-TR due to their compulsory nature. These behaviors may or may not be driven or worsened by anxiety.
In the case of BFRBs, even though these behaviors cause varying degrees of bodily harm, they're ultimately driven by impulses and urges that cannot easily be controlled. Quite often the triggering event is discovering a physical imperfection in any way for any reason and attempting to "fix" it, despite the behavior being counterintuitive to the goal. The resulting behavior can occur actively or passively, with severe active episodes usually likened to being held hostage in your own body.
There is no desire to harm and very little ability to stop, and then all of it is followed by distressing feelings such as shame, guilt, or embarrassment. We try so hard to "break the habit" that we ultimately beat ourselves up mentally for "failing" yet again. Even though many of us might know we can't control it, it's too easy to blame ourselves for something we feel is somehow our fault.
[Please be advised the purple paragraphs below are personal examples with a few details that may be triggering for some.]
For example, the only way I can come out of bad episodes is when my bodily literally cannot continue. This may look like my back giving out from leaning on the counter in the bathroom, or my legs going completely numb from sitting for too long, or (much more commonly) my fingers or nailbeds hurt too much for me to keep using them, regardless of how much I may or may not have bled.
This is always followed up by what I call the "walk of shame" phase as I clean up every injury, apply Neosporin or other balms/salves, and bandage what I can. I've burst into tears before when I had to use Neosporin like it was lotion in order to cover everything, because I had too many wounds on my arms to be able to safely apply bandages/plasters.
No part of that process, from the trigger response to the cleanup, is something I want to do. If I had a say in it, I'd never pick or bite ever again, and my skin would finally be able to heal.
Self-harm, on the other hand, is a term reserved for bodily harm that is deliberately inflicted on oneself, usually as a way of dealing with difficult emotions, memories, situations, or experiences. Instead of acting on an uncontrollable compulsion, this type of harm stems from a different set of triggers, many of which relate to trauma or other disorders. This makes the behavior more of an unhealthy coping mechanism for people in pain who are desperate for release from those feelings.
Note: If you are unsure if your behaviors are a result of a BFRB or self-harm, Crisis Text Line is a good resource:
"Self-harm is serious. And, while the intention behind self-harm usually is not death, it can still be dangerous—both physically and emotionally. Talking to someone who can help you find alternatives is incredibly important. Of course, you can start by texting us. Also, consider telling someone you know who can help you connect with a professional."
General BFRB Resources:
Sites:
The TLC Foundation - "The TLC Foundation for Body-Focused Repetitive Behaviors helps end isolation and shame for people experiencing hair pulling, skin picking, nail biting, cheek biting, and associated behaviors." They feature a robust website full of information on all BFRBs, including "Medications for BFRBs" and "Evidence-based Therapeutic Treatment for BFRBs."
The Recovery Village - "The Recovery Village aims to improve the quality of life for people struggling with substance use or mental health disorder with fact-based content about the nature of behavioral health conditions, treatment options and their related outcomes. We publish material that is researched, cited, edited and reviewed by licensed medical professionals." (BFRB-specific information can be found here.)
SkinPick.Com - While this site is centered around skin picking/excoriation disorder/dermatillomania, they have excellent resources for other BFRBs as well, including their Glossary page, "Complete List of BFRBs," and the blog section for "Related Disorders." I have also listed their site in the Dermatillomania section below.
Articles:
Online Journal: International Journal of Environmental Research and Public Health, Special Issue: "Body-Focused Repetitive Behaviours (BFRBs). Risk Factors, Prevention, Treatment"
The Recovery Village’s article, "7 Myths About Body-Focused Repetitive Behaviors"
The Recovery Village’s article, "8 Little Known Facts About Body-Focused Repetitive Behaviors"
Outreach:
"Health Education & Community Programs" (the TLC Foundation)
Communities & Support:
PickingMe Foundation's Online Support Group.
TLC Foundation's Support Group Directory for peer-led support groups.
SkinPick's online Forum.
Self-Help:
Nathan Peterson's ComB Model for BFRB Treatment, Part 1 and Part 2 on YouTube. Peterson is a licensed OCD specialist who helps people with OCD, anxiety, and BFRBs in person, through his OCD & Anxiety YouTube channel, and through his site, OCD-Anxiety.Com. (His BFRB specific course can be found on his site here.)
SkinPick's free self-guided program to stop skin-picking.
PickingMe Foundation's Derma Resource Packets "...are our campaign to spread Dermatillomania awareness to skin care providers (Dermatologists, Estheticians, Nail Salons, Clinicians), mental health professionals, and anyone who wants more info! We provide them with tools and the opportunity to point Skin Picking Disorder sufferers in the right direction."
PickingMe Foundation's Management Tips page, a "growing list of tips and management strategies!"
Mobile Apps:
SkinPick App – "A free tool to monitor your skin picking behaviors."
Specific BFRB Resources:
Onychophagia:
Not every instance of nail-biting is considered onychophagia. Most nail-biting behavior dissipates over time. It’s when it doesn’t that the behavior requires a closer look. Chronic nail-biting is categorized as an obsessive-compulsive related disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR).
SkinPick's blog post, "Onychophagia: More Than a Nervous Habit"
"Art of Prevention: The importance of tackling the nail biting habit," authored by Mohsen Baghchechi BS, Janice L. Pelletier MD, FAAP, Sharon E. Jacob MD, FAAD, FAAP. Published in the International Journal of Women's Dermatology, Volume 7, Issue 3, June 2021, Pages 309-313.
"Update on Diagnosis and Management of Onychophagia and Onychotillomania," authored by Debra K. Lee and Shari R. Lipner. Published in the International Journal of Environmental Research and Public Health, 2022, 19, no. 6: 3392.
Dermatophagia:
Formerly referred to as "wolf-biting," dermatophagia has yet to be recognized as a diagnosable disorder.
SkinPick's blog post, "Do you eat your own skin after picking? There's a name for that."
SkinPick's blog post, "Dermatophagia - What is it?"
Dermatillomania:
Dermatillomania means “Skin Pulling Madness,” and has only been diagnosable since 2013. It is currently classified as an “Obsessive-Compulsive and related disorder” in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), where it is listed as Excoriation Disorder. However, it is known by many names, such as: Skin Picking Disorder, Compulsive Skin Picking, Acne Excoriée, Pathological Excoriation, Neurotic Excoriation, Pathological Skin Picking, and Psychogenic Excoriation. The many names for this disorder cause interference with its understanding and awareness.
Dermatillomania is often confused with other conditions. Common misdiagnoses result because the picking behavior is a result of a medical condition, confused with OCD, Body Dysmorphic Disorder (BDD) and in some cases, Non-suicidal Self-Injury (NSSI).
PickingMe Foundation - "Picking Me Foundation NFP is the only donor-supported non-profit dedicated to advocating for Dermatillomania (Skin Picking Disorder) sufferers, supporters, and educational communities alike, encouraging individuals to choose themselves over the mental illness that chose them by #PickingMe over Skin-Picking."
Angela Hartlin's Skin Picking Support website. Hartlin is the author of, "FOREVER MARKED: A Dermatillomania Diary" and the creator of the documentary, "Scars of Shame," which you can watch for free here with the password, "Scars1" (Thanks, Angela!)
SkinPick.Com - "SkinPick is the #1 platform to treat excoriation disorder (dermatillomania). Get one-on-one support from a therapist specializing in treating compulsive skin-picking through evidence-based techniques."
SkinPick's "Do I Have Dermatillomania?" Test
SkinPick's blog post. "Skin Picking and Body-Focussed Repetitive Behaviours (BFRB)"
Stuff That Works’ page, “Excoriation (Skin-Picking) Disorder”
Trichotillomania:
Probably the most famous BFRB, Trich has the most resources available thanks to being the first diagnosable BFRB. The resources below are more general as a result:
TrichStop - "TrichStop is the world’s leading platform for Trichotillomania treatment. Get one-on-one support from a therapist specializing in treating compulsive hair pulling through evidence-based techniques." From the same support team behind SkinPick.Com.
TrichStop's "Do I Have Trichotillomania?" Test
TrichStop's blog post, "Trich and Comorbid Disorders: What We Are Learning"
The TLC Foundation's Trichotillomania page.
"Trichotillomania," authored by Aubree D. Pereyra; Abdolreza Saadabadi. Published in StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. (Ongoing)
More to come.
There are more BFRBs than this out there, but I don't have the resources gathered for them yet. Hopefully the General resources help! I'll update this as I have time. In the meantime, I wish you all luck on your BFRB journeys.
-> Anxious? Try This:
#bfrb#bfrb awareness#resources#bfrb resources#dermatillomania#dermatophagia#onychophagia#trichotillomania#mental heath support#mental health#signal boost#awareness#mental health resources#compulsion#obsessive compulsive disorder#anxiety#skin biting#skin picking#nail biting#self help#bfrb research#psychology#psychology research#abnormal psychology#bfrb studies
64 notes
·
View notes
Text
Embracing the Unexpected: 40 Surprising Events That Could Happen to Anyone
Have you ever had one of those moments when you suddenly realized that life is full of possibilities you hadn’t even considered? Sometimes, we get so caught up in our routines and expectations that we forget how wildly unpredictable and extraordinary our lives can be. It’s in those moments of surprise and wonder that we truly grasp the vast array of experiences life has in store for us.
Here’s a list of 40 unexpected events that could happen to anyone, each one a reminder of the limitless potential for change and excitement in our lives.
Winning a Major Lottery: Finding yourself with a life-changing sum of money overnight.
Reuniting with a Long-Lost Sibling: Discovering and reconnecting with a family member you never knew existed.
Being Featured in a Viral Video: Suddenly becoming a sensation on social media or the news.
Encountering a UFO: Witnessing something in the sky that challenges your understanding of the world.
Receiving an Unexpected Inheritance: Gaining a significant amount of wealth from an unknown relative or estate.
Meeting A Celebrity: Having a chance encounter with someone you’ve admired for years.
Participating in a Groundbreaking Scientific Study: Being selected for a cutting-edge research project or clinical trial.
Surviving a Major Natural Disaster: Experiencing a catastrophic event and coming through it.
Discovering Hidden Family Secrets: Uncovering intriguing or shocking details about your family’s history.
Finding a Rare and Valuable Artifact: Stumbling upon something precious or historically significant.
Becoming an Overnight Internet Star: Gaining widespread recognition from an unexpected online phenomenon.
Witnessing a Rare Celestial Event: Seeing a once-in-a-lifetime astronomical occurrence.
Experiencing a Major Career Shift: Transitioning into a completely different profession or industry.
Participating in a Cultural Festival Abroad: Immersing yourself in an unusual and vibrant cultural celebration.
Encountering a Mythical Creature: Observing something that seems out of the ordinary or legendary.
Being Part of a High-Stakes Reality Show: Competing or participating in a popular reality TV program.
Receiving a Personal Message from a Historical Figure: Feeling a deep connection to someone from history through an unexpected experience.
Living Through a Historic Event: Being present during a momentous occasion that shapes history.
Having a Profound Spiritual Awakening: Experiencing a transformative spiritual realization or insight.
Discovering a Hidden Talent: Finding out you have an extraordinary skill or ability you never knew you had.
Becoming a Published Author: Seeing your writing or creative work in print and gaining public attention.
Joining an Exclusive Club or Organization: Becoming part of a prestigious or secretive group.
Finding a Significant Treasure: Discovering a hidden or buried object of great value.
Experiencing a Miraculous Recovery: Overcoming a severe illness or injury in a way that defies medical expectations.
Participating in an Experimental Art Project: Engaging in a unique and avant-garde artistic endeavor.
Winning a Major Competition: Securing victory in a high-profile contest or event.
Facing an Unexpected Heroic Moment: Stepping up to help others in a critical situation.
Embarking on a Spontaneous Adventure: Going on an unplanned trip or journey that changes your perspective.
Experiencing an Unexpected Romantic Connection: Meeting someone who profoundly impacts your love life.
Receiving a Unique Award or Honor: Being recognized in an unconventional or surprising way.
Witnessing a Historic Scientific Discovery: Observing or being involved in a groundbreaking scientific breakthrough.
Encountering an Unsolved Mystery: Coming across a puzzle or enigma that captivates your curiosity.
Becoming a Community Leader: Unexpectedly stepping into a role of influence or leadership in your local area.
Living Through an Unusual Weather Phenomenon: Experiencing rare or extreme weather conditions firsthand.
Joining a Revolutionary Movement: Becoming involved in a transformative social or political cause.
Discovering a Hidden Gem: Finding a secret or overlooked place that becomes special to you.
Experiencing a Unique Cultural Exchange: Engaging deeply with a different culture in a meaningful way.
Becoming a Subject of a Documentary: Having your life or experiences captured and shared in a film.
Participating in a Space Mission: Being involved in an exploratory or research mission beyond Earth.
Encountering a Profound Life-Changing Event: Experiencing something so impactful that it reshapes your entire outlook on life.
Each of these events serves as a reminder that life is full of surprises and opportunities. Embrace the unknown, stay open to new experiences, and remember that anything truly can happen.

7 notes
·
View notes
Text
Natural and socio-environmental factors in the transmission of COVID-19: a comprehensive analysis of epidemiology and mechanisms - Published Aug 13, 2024
Abstract
Purpose of review
There are significant differences in the transmission rate and mortality rate of COVID-19 under environmental conditions such as seasons and climates. However, the impact of environmental factors on the role of the COVID-19 pandemic and the transmission mechanism of the SARS-CoV-2 is unclear. Therefore, a comprehensive understanding of the impact of environmental factors on COVID-19 can provide innovative insights for global epidemic prevention and control policies and COVID-19 related research. This review summarizes the evidence of the impact of different natural and social environmental factors on the transmission of COVID-19 through a comprehensive analysis of epidemiology and mechanism research. This will provide innovative inspiration for global epidemic prevention and control policies and provide reference for similar infectious diseases that may emerge in the future.
Recent findings
Evidence reveals mechanisms by which natural environmental factors influence the transmission of COVID-19, including (i) virus survival and transport, (ii) immune system damage, (iii) inflammation, oxidative stress, and cell death, and (iiii) increasing risk of complications. All of these measures appear to be effective in controlling the spread or mortality of COVID-19: (1) reducing air pollution levels, (2) rational use of ozone disinfection and medical ozone therapy, (3) rational exposure to sunlight, (4) scientific ventilation and maintenance of indoor temperature and humidity, (5) control of population density, and (6) control of population movement. Our review indicates that with the continuous mutation of SARS-CoV-2, high temperature, high humidity, low air pollution levels, and low population density more likely to slow down the spread of the virus.
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#still coviding#public health#wear a respirator
13 notes
·
View notes
Text
When the US Supreme Court published its decision in Dobbs vs Jackson Women’s Health Center in June 2022, pro-choice advocates’ misinformation about pregnant women’s access to emergency care spread quickly, uncritically, and widely in the media.
We heard shocking stories of women suffering from complications and being wrongly denied care out of confusion about ethics and state law. So I launched a project called Pro-Life Professional Insight to collect and publish stories from pro-life medical professionals, who illustrate how they save women’s lives without elective abortion.
One of the first stories in the project reminded me that if I were going to think deeply about the problem of abortion, I should also listen to the stories of women who have had them.
6 notes
·
View notes
Last Seen Blogs

crimesoughtarchive
C R I M I N A L.

crying-elf-lass
Untitled

caldanielas
Diaper Under Clothes

tabi-niwa
旅好き

awesomefreak15
World of Wonder