#including asymptomatic cases
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In Q3 of 2020, 31% of US users access the Tumblr app daily.
Text
Meanwhile, in Ontario the government not only ended our safety measures, they are actively underfunding healthcare by billions of dollars
(Which are instead going to a highway no one wants, or just sitting in a “surplus”)
To the extent that emergency rooms are being permanently closed and half of them can’t afford an MRI machine
Nothing can possibly go wrong
does anyone else think it’s crazy how we just casually reference “the pandemic” now. i catch someone in conversation saying “during the first quarantine…” and as comfortable as it feels to hear and say now, there’s still a twinge of like…. i cannot believe we’re using these words in real life in reference to real events. this isn’t a scifi movie this isn’t a young adult post apocalyptic novel we’re literally casually discussing a global pandemic that ravaged the entire world and it was REAL ?
#health#covid#long covid#about 30% of infections resulted in long covid in the 2021 studies#including asymptomatic cases#i know someone who didn’t know they’d even had covid til they got tested for antibodies trying to work out what their symptoms were#it was long covid#they never even knew they were sick
25K notes
·
View notes
Text








A very interesting cloud formation!
#I don't think I had ever really seen clouds like this before? it looks like a cool painting or something :0#Pulling just a few images from my cloud and sky photos folder which has like 650 pictures in it becvause I'm obsessed with the sky lol#I will usually spare everyone the cloudposting but... in some exceptions when it's really cool I must Share#(upcoming covid mention in tags for those avoiding the topic)#I WANT TO BE ON AN AIRPLANE SO SO BAD I am going to start casting evil spells to explode all these 'back to normal' bastards who are out#spreading virus and shit HHHHHH... Covid is NOT over actually contrary to popular beielf especially for people with health conditions#that make them more vulnerable or would have worse consequences if they were to catch it etc. etc. wearing a mask in public is#in MOSt cases not THAt much of a horrific terrible evil inconvenience and it helps keep everyone around you safer including these#vulnerable populations!!!! Even if I didn't have any problems myself I would STILL be masking because it's a small gesture that can make a#big difference in people around me being comfortable. It's not like people with health issues just never have to go out or go to the stor#or whatever. There are still people out there who could be helped by extra precautions that are being overlooked. grrrrr...#Like at this point since I'm vaccinated and everything I would MAYBE consider flying on an airplane IF everyone else around me#was masking and being just as careful as me. But at this point it's just the wild west and I would literally be the only one who gives#a shit or who gets tested freqeuntly before after and during traveling and wears the proper type of mask well fitting and not half off my f#ce and blah blah blah. And precautions work best when EVEYRONE is participating. There's only so much you can protext yourself if everyone#around you is doing nothing. So.. alas.. I still do not feel safe traveling. And probably won't for years until more progress is made in#terms of like understanding and treating certain long covid issues and etc. Since I think it's inevitable that if I start going out again#I would get covid. Me and my household bubble are some of the only people I know who haven't had it yet (or at least not knowingly so - if#so it was one of the asymptomatic cases etc.). So if I was GOING to get it anyway I'd at least like the assurance that whatever long term#issues I inevtabley suffer because of it will be more easily treatable at that point instead of entirely disabling even further than I'm#already disabled. etc. AAANYWAY!! all that to say. I JSUT REALLY WANT TO be on an airplane!!! I dont even like traveling and going places I#hate vacations and would rather be at home working on my projects I'm fixated on lol HOWEVER I love the view from airplane windows#like the very few times in my life Ive actually been on a plane and the window is so COLD when you lay your forehead on it and sometimes yo#even see little ice crystals and it's like you're just in a landscape of clouds with a sea of clouds above and below and aaaAAAAAA#Literally I want to get on a plane just to go up in the air and then land and fly back. I don't even want to go on a real trip. I just NEED#to see the sky I need to be IN the sky I need to have that VIEW and the cold and everything!!!! gRGGHGgg... And I will do that the entire#time. I think my longest plane ride was 7 hours and I do not watch movies. I dont text or play games. I literally do nothing to entertain#myself except stare straight out the window for 7 hours (with a few eating and bathroom breaks). not even joking lmao. It's like a trance#I LOVE the sky and clouds so much and the view you get from an airplane is like incomparable!! also I love airports with the big windows an#people watching. but mostly I just long for the sky view again. GRRR.. sobbing and yearning >:T
44 notes
·
View notes
Text
What I Want You To Know About Long COVID
Well lads, I've been suffering from Long COVID for over a year now. My life is at a complete standstill. I'm 25 years old and I'm too sick to go back to school, I can't work, I had to move back in with my parents and I'm still stuck here.
Here are just a few things I wish people knew about Long COVID, including things I didn't know myself until I got it.
COVID destroys your immune system. Yes, even if you don't have Long COVID. Are you getting sick more often now? When you get sick, does it last longer? There are many studies showing that COVID causes t cell depletion, even in mild COVID cases! T cells are how your body remembers how to fight off infections you've had before so losing those cells? Bad news.
Your initial infection can be mild and you can still get Long COVID. Right from Yale Medicine, "Most people with Long COVID had mild acute COVID." (This is also a good link for a basic Long COVID overview).
There can be a gap of time between when you "get better" from the initial COVID infection to the onset of Long COVID symptoms. Some people get sick with an initial COVID infection and never get better. Some get better and then weeks or months later start developing Long COVID symptoms. Long COVID symptoms can even fluctuate over time, can go away for months and then suddenly come back.
So many people have Long COVID and don't realize it. Do you feel more tired lately but no matter how much you sleep, nothing helps? Is it harder to concentrate at work or school? Can you just not think like you used to? You could have Long COVID and not even know it. Even mild post-COVID symptoms are still Long COVID.
COVID can do anything to your body. Long COVID has over 200 recognized symptoms and can affect basically any part or system of your body. There is no one mechanism or cause of Long COVID which unfortunately also means there's no one cure either.
The effects of COVID are cumulative. Each COVID reinfection increases your chances of developing Long COVID. COVID is also affecting your body in other ways, yes, even if you're otherwise young and healthy! "Repeat COVID-19 infections increase risk of organ failure, death".
Once you have Long COVID, repeat COVID infections will make your symptoms worse. "80% [of Long COVID patients] saw their symptoms worsen [from reinfection]. In 60% of people who were in recovery or remission from Long COVID, reinfection caused a recurrence of Long COVID."
There is a lot more I want to say about Long COVID but I want to keep this post at least somewhat manageable to read. Like how when COVID is contracted during pregnancy, those COVID-exposed fetuses have a 6.3-fold increased risk of motor developmental delays, or that another study found 50% of babies exposed to COVID in utero had developmental delays.
You need to keep caring about COVID, for others around you and also for yourself even if you're "healthy". Everyone is at risk. And don't forget 40-60% of COVID infections are asymptomatic, which is why masking even if you feel fine is crucial. The only way right now to not get Long COVID is to not get COVID in the first place. It's not too late, if you've stopped masking it's never too late to start again! I know it's easy to get distracted by things in your life that seem more real than the possibility of getting sick some time in the future, and the peer pressure to not mask can be intense. But it only feels less real or less important until your entire life is having Long COVID. Trust me.
I know this is a complicated issue, many people can't afford to stay home when sick even if they want to because of their jobs, there are disgusting policies trying to ban wearing masks, but please if you can. Keep masking. Masking works, masking saves lives.
This post got a bit longer than I wanted so below the cut is a non-exhaustive list of my Long COVID symptoms and some of my experiences as one of the "healthy young people" who got "unlucky". cw brief mention of suicidal ideation.
Welcome to the Thunderdome that is my body with Long COVID. Keep in mind these are just my experiences and symptoms, Long COVID can cause any range of symptoms at varying severities.
Dysautonomia: Exercise intolerance, Post-Exertional Malaise (PEM), fatigue, and heat intolerance. What do those things mean? Here's some specific examples. Absolutely terrible circulation I am so cold all the time but also, if I get a little too warm I will pass out. Eating hot food makes my heart rate spike, I sweat, my body feels heavy. Blood pooling and pins and needles in my feet when I walk. Don't even think about exercising past walking, it's impossible. I used to work out an hour a day 4 times a week and now walking up one flight of stairs makes my heart pound and I can't breathe. Can't take even just warm showers anymore or I will pass out. Heat rashes from being in the sun for 10 minutes.
Digestive issues: Honestly too many to name but: constant bloating, extreme nausea, constipation, slow motility, lack of appetite, just so much cramping and pain. I lost 18 pounds from Long COVID, as someone who was already considered underweight their entire life, and almost had to get a shunt put into my chest to deliver nutrients because I was nearly completely unable to eat. For the first 6 months of Long COVID, if I could manage 600 calories a day, that was a good day.
Histamine intolerance: Oh boy. My worst symptoms, I don't even know where to start with it. If you know Mast Cell Activation Syndrome (MCAS) it's very similar. I can only eat 19 foods. If i eat a single bite of something not on that list, it's 48 hours of absolute hell. Coughing, migraines, itchy eyes, such extreme nausea I cannot even describe it, panic/feeling of doom, racing heart rate, derealization, rash, uncontrollable muscle tremors. I only learned about histamine intolerance 5 months into having Long COVID so before that, I was experiencing these symptoms nearly every single day. Terrifying isn't even a strong enough word to describe how it felt to experience all this and have no idea what it was, how to stop it, or if it would ever stop. Really dark times.
Neurological issues: More of that derealization. Inability to concentrate. Anxiety. OCD-like symptoms such as thoughts getting "stuck" in my head, repeating 24/7 completely unable to stop them, genuinely felt like my brain had cracked open and I had lost my mind. Constant dizziness like I'm on a boat.
Sleep issues: I sleep like garbage. I have insomnia, I wake up dozens of times every night and every single time I sleep I have intensely vivid dreams. I can't sleep longer than 7 hours total no matter how exhausted I am. It is exhausting. I'm exhausted, I'm so so tired.
And finally. Just. Really intense suicidal ideation. My body, my health, my entire life has been stolen from me because someone else decided my life was worth less to them than wearing a mask or staying home if they feel sick. Before I got Long COVID, I was preparing to go to South Korea to teach English, then on to a PhD in neurolinguistics, I was supposed to meet my long distance partner and had already booked plane tickets when I got sick. All of that has been destroyed.
Most of us with Long COVID are stuck in a cycle of being extremely sick, then if you're lucky you'll slowly get better over months, just to get reinfected and go right back where you started or worse. Honestly, I'm not scared of dying from COVID. I'm scared of living for a long time, suffering from Long COVID the entire time. This isn't living.
I don't know how to end this now. I'm still fighting, I'm trying experimental treatments, I'm not giving up yet. I hope everyone reading this stays healthy and well.
9K notes
·
View notes
Note
How is William's reason of not going to the olympics acceptable when he was literally mingling with other people through his work and privately? I mean the walkabouts, attending footballs games, attending concert.
Does it mean every person he meets particularly on walkabouts is medically assessed before going?
Because attending an international event on a different continent that his team has no control over and which 9.5 million other people from around the world also attended at the height of the summer Covid surge is not the same thing as attending local events that his team has full control over.
The private football games? William sits in the back row so there was no one breathing on him from behind. The people he goes to the games probably aren’t screened, but those guys definitely know not to be around him if they’ve got the sniffles.
The Euro football games? William sits in the royal box and there’s definitely a protocol for who sits there. Maybe they’re not getting swabbed and temperature-checked, but the people with access to that box and all the dignitaries who sit there know better than to be sick and go to an event. Additionally, William usually (but not always) sits in the front row when he’s on duty at a football game, so there’s less people breathing on him there.
That concert? He was in a private box with a very restricted number of people around him.
Those walkabouts? I’m only aware of 2 and those were tens of people, not the usual hundreds that pack in to small spaces that see him.
At the Olympics, he’d have been around thousands of people. He’d have been sitting smack in the middle of a crowd, no priority seating next to controlled open spaces for him. And considering that there were 40 Olympians confirmed to have COVID during the games (including some of the Australian team), that means there were far higher numbers of unreported cases, undisclosed symptoms, and asymptomatic cases. Then consider how quickly the virus spreads, how you can be asymptomatic but quite contagious, and the risk increases exponentially. All it takes is one person.
And, I’ll bet you didn’t know this, but the Tour de France actually implemented COVID restrictions after a number of athletes tested positive. If the Tour de France is implementing COVID restrictions 2 weeks before the Olympics are kicking off, then yes, Olympic organizers and global health experts were absolutely concerned about the Olympics turning into a superspreader event for the COVID summer surge.
And yes, everyone William meets - planned or on an impromptu walkabout - does undergo a health screening to meet him. No, they’re not getting swabbed and tested and temperature-checked, but there’s definitely an aide around who’s asking the people likely to meet William “hey, have you had any symptoms in the last couple of weeks?” If there’s an aide who goes around collecting people’s consent to be photographed by the media, there’s an aide doing health screenings. It’s not a foolproof system and yes, people can lie if they really want to meet or see William, but the point is that his team is controlling everything to the best of their abilities to help him help Kate’s health because they were and are in charge of planning and coordinating the events. They wouldn’t have been able to do that in Paris at the Olympics because they weren’t the ones organizing the events and managing the crowds.
It was smart that William chose not to go to the Olympics to keep his immunocompromised wife as healthy as possible because he and his team didn’t have the same control in Paris that they do over appearances and events in Britain. That alone is all the justification anyone needs.
I’ll close with this soapbox: William is smart enough to conduct his own risk analyses of where he goes and what he does. Why can’t we trust his judgement that an international sporting event in another country that the whole globe attends was much too risky for him to attend than a local event in his own city? You don’t need my analysis breaking it all down; you just need to trust that William knows what’s best for himself and his family. After all, he’s the one with all the information and data about Kate’s health, her treatments, her recovery, etc., since all we know is that Kate had abdominal surgery, she was in the hospital for 2 or 3 weeks, there was cancer present, she underwent chemotherapy, and sometimes she has good days and sometimes she has bad days. We don’t know how bad the bad days are. We don’t know what her medications are or what side effects she may be experiencing. We don’t even know if William is undertaking additional medical precautions - for instance, is he changing clothes and washing up in the mud room before he goes into the house to see Kate? How often is he washing his hands? Does he self-isolate for a day or so at KP after he goes to these events to avoid bringing something home to Kate?
We just don’t know. But William knows. All we can do is trust his judgment, and he decided that it was far too risky and medically unsafe to go to an international event with millions of other people in another country than to go to sports at a local arena.
If you don’t trust William’s judgment, then that’s fine. But this isn’t the incident to accuse him of covid hypocrisy. Just call him out for not working. (But note that if anyone does say that to me, my response is going to be “then why aren’t you upset that Queen Camilla didn’t go to the Olympics?“)
93 notes
·
View notes
Text
Anthony Fauci: A Mosquito in My Backyard Made Me the Sickest I’ve Ever Been. (New York Times)
Excerpt from this New York Times Op-Ed by Anthony Fauci:
There is no treatment for West Nile virus disease, and I was left to deal with its toll on my body. It was terrifying. I could not swing my legs over the side of the bed to sit up without help from my wife and three daughters. I could not stand up without assistance and certainly could not walk. A very scary part of the ordeal was the effect on my cognition. I was disoriented, unable to remember certain words, asking questions of my family that I should have known the answers to. I was afraid that I would never recover and return to normal.
Fortunately, over a period of a few weeks slow improvement began. I was able to walk with a walker and then without any assistance. Now I can walk a few miles per day with only minimal fatigue, and my cognitive issues have completely resolved. I am on my way to a total recovery, but it has been a harrowing experience.
I tell my story because West Nile virus is a disease that, for many people, can have devastating and permanent consequences. At my age of 83, I was at risk of permanent neurological impairment and even death. Yet the public may be unaware of the danger of this disease and that it continues to spread across the United States; it has been identified in 46 states this year. Unfortunately, very little is being done about it from scientific and public awareness perspectives.
West Nile virus belongs to the family of flaviviruses that also includes yellow fever and dengue viruses. It was first detected in the United States in the New York City area in 1999, most likely introduced from the Middle East or parts of Africa where it is prevalent. Mosquitoes get the virus from infected birds, and then pass the virus on to humans by a bite. West Nile virus infection is by far the most common mosquito-borne disease in the United States: Since 1999, about 60,000 cases have been reported. The actual number of infections is surely higher, no doubt in the millions, since many cases are not reported because infections are often asymptomatic or are confused with other common maladies such as flu. Among the reported cases in the United States, more than 30,000 have had neurological symptoms like mine, resulting in about 23,000 hospitalizations and close to 3,000 deaths.
As climate change makes it easier for mosquitoes to proliferate in many places, West Nile virus disease as well as other mosquito-borne illnesses are emerging as greater threats in this country and elsewhere. Yet, efforts to develop a vaccine or treatment for this illness are modest compared with those for other diseases of public health importance.
So, how do we address this emerging public health threat? Vaccine development must go forward; however, to be successful, clinical trials must be international and include countries with a consistent and large number of cases each year. The pathway to a vaccine cannot be in the United States alone. Global public-private partnerships between the N.I.H. and the drug industry have historically proved successful in the development of a number of important vaccines such as those against hepatitis B and Covid. There is no reason this shouldn’t also be the case for a West Nile virus vaccine.
The same holds true for the development of antiviral drugs. There is no insurmountable scientific obstacle to developing safe and effective antiviral drugs for West Nile virus infection. The pharmaceutical industry in collaboration with the N.I.H. and other partners had remarkable success in developing effective drugs for other emerging viral infections. Examples include lifesaving drugs for H.I.V. infection, therapies for hepatitis C infection and useful drugs for Covid-19 and influenza. With international research partnerships and political will spurred by an engaged activist community such as we have seen with H.I.V. and now long Covid, West Nile virus treatments and prevention tools should be within our grasp.
49 notes
·
View notes
Text
It is very likely that polio has infected people in the Gaza Strip, in what would be a setback for global efforts to eradicate the disease, a World Health Organisation spokesperson said on Tuesday, Reuters reports.
Gaza’s Health Ministry declared a polio epidemic across the Palestinian enclave late on Monday after samples of the virus were found in sewage. It has not announced any human cases.
According to the WHO, polio is now endemic only in Pakistan and Afghanistan, but more than 30 countries are still listed as subject to outbreaks, including Gaza’s neighbours, Egypt and Israel. Any country risks a return of polio if outbreaks are not contained with mass vaccinations.
The WHO’s Christian Lindmeier told a UN press briefing that people had probably already been infected in Gaza but that detecting cases can be difficult since most cases of the potentially deadly viral disease are asymptomatic.
“Having vaccine-derived polio virus in the sewage very likely means that it’s out there somewhere in people,” he said. “So the risk of (it) … spreading further is there and it would be a setback definitely (for global efforts).”
34 notes
·
View notes
Text
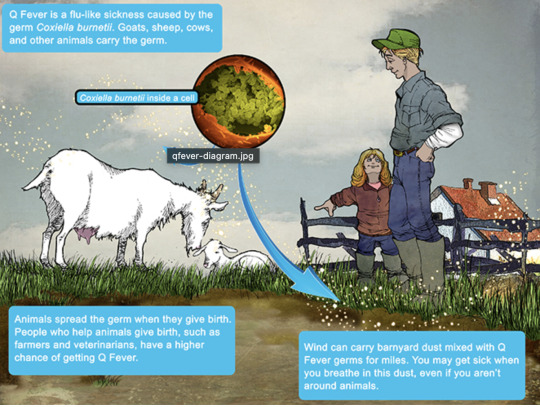
Q Fever
Aka, Query fever. What a weird name for a disease. Imagine telling people that's what you got.

in the 30s-40s, an Australian pathologist in QLD/Brisbane, came across an outbreak of the same or similar illness among abbatoir or slaughterhouse workers.
At the time, he called the disease "Q" fever or query as a temporary name until the pathogen could be identified. Unfortunately it stuck.
decades later, now nobel prize winner and virologist, MacFarlane Burnett isolated and identified the microbe responsible. I think this discovery contributed to his prize. i forget already.
Microbe responsible: Coxiella burnetti. Named for Burnett and HR Cox, the American bacteriologist who found the genus Coxiella where C burnetti falls under.
Initially they felt it was related to Rickettsia, responsible for Rocky Mountain Spotted Fever, but as science progressed, this was disproven.
Now for a Case Report
A 55 yo Italian man with a history of aortic valve replacement was diagnosed with pyrexia of unknown origin twice. Further signs included myalgias/splenomegaly/night sweats. The 2nd time he was admitted for PUO he deteriorated rather dramatically and was put on meropenem and teicoplanin.
A host of organisms was tested for on serological testing based on the man's travel and epidemiological history, all negative. Even a rheumatological panel was done, also less revealing. He also had a history of MGUS (a haem disoder), which is kind of a red herring here.
Cultures were negative, no vegetations were seen on a TTE - so they did consider IE. Which is an important differential for PUO.
Eventually a PET-CT was done (often favoured when investigations do not yield much for a sick patient with fevers), finally revealing a focus of infectious on his ascending aorta, where he'd also had previous surgery done. And in a round about way, they also further identified Coxiella Burnetti. He was treated doxycycline and hydroxychloroquine. As it's so rare in Italy, it wasn't really considered even though he mentioned rural travel.
Bottomline: Q Fever is an important consideration in the work up for culture negative IE. Further to this, always consider IE in the differentials for PUO particularly if they're at increased risk for IE (prosthetic valves, damaged valves, select congenital heart issues, previous IE). IE can present with night sweats, fevers, weight loss and splenomegaly. It can be insidious and chronic in nature. other risk factors can be more suggestive as we'll get into below.
Causative organism
Coxiella burnetti, it's a zoonoses - i.e. transmissible from animals. Special powers: very tough/hardy, can survive extreme environments (high temps and UV light etc.) over prolonged periods and is resistant to many common disinfectants/surface cleaners.
It's an intracellular pathogen and gram negative coccobacilli (PINK!)
name coccobaccili reminds me of cocopuffs.
it's mainly associated with farm animals, which the CDC so wholesomely displays on its website on Q fever (wtf).

goats, sheep, cattle typically (but many other animals, even birds, dogs and horses can be reservoirs)
in particular bodily fluids - amniotic fluid, placenta, faeces/urine, milk etc.
you can get it through unpasteurized milk and through inhaling it if it lands on dust in the area
ever visit a farm or petting zoo lately? OMG WASH YOU HANDS.

That said, it's typically inhaled in inorganic dust. You inhale it, it goes to the lungs, and then the bloodstream.
Increased risk for Coxiella burnetti (What to take on history of exposures and when to strongly consider it)
live on a farm or near one
exposure to a farm
work as a vet on a farm
farm worker, dairy workers, researchers on these animals/facilities
slaughterhouse/abbatoir
Also from CDC:
Clinical presentation
Most won't get sick after exposure and remain asymptomatic, a very small minority does. even though it is highly infectious.
incubation time is 2-3 weeks (consider this time in your history of exposure, did they work on the farm 2-3 weeks ago as opposed to yesterday).
Nonspecific acute infectious symptoms:
nonspecific systemic fevers/malaise/arthralgias/myalgias--> key is high fevers though and can be associated with headache and photophobia.
non specific GI - N/V/diarrhoea
respiratory ones - SOB or cough, consider it as atypical cause of community acquired pneumonia.
rare: hepatitis and jaundice (granulomatous) or encephalitis with neurological complications such as demyelinating disease or CN palsies, also haemolytic anaemia and HLH (yikes)

really it's the history of exposure that will lead you down the garden path to Q fever.
Chronic Q fever is perhaps worse, and can present as culture negative IE/PUO. Months/years later, as B symptoms as above above + LOW/LOA, night sweats. More likely to occur if you are predisposed for IE as above, have a weakened immune system for any reason, including pregnancy.
Chronic Q fever has a mortality of 10% if left untreated. About <5% of those with acute Q fever develop this if left untreated. Speculation is that it's more of an autoimmune process or abnormal immunological response to the bacteria.
To be honest, most who walk in the door with community acquired pneumonia get treated empirically for atypicals anyway, (standard course of doxycycline), so we hardly really ponder the question of Q fever in every patient. But if they present chronically and did not have atypical cover at the onset of acute symptoms, then it's something important to consider.
Other important conditions - can cause complications in pregnant women and 20% will get post Q fever syndrome. like chronic fatigue.
investigations
Serology! nice and easy. Look for IgG antibodies in the chronic presentation. Or PCR. Down side to serology - can take 2-3 days for the body to make said antibodies to the bacteria for detection. PCR can be done on any fluids/tissue sent.
Cultures useless, hence it fall under the umbrella of culture negative (hard to grow outside a host cell, it is an obligate intracellular pathogen).
Other hints on bloods (as serology/PCR takes time to return) - elevated or low platelet's, transaminitis with normal bili, opacities in CXR with hilar lymphadenopathy, CSF will show raised protein levels if done when encephalitis is suspected.
imaging can also support the diagnosis.. as illustrated by the case report.
Treatment
Acute disease - as standard for atypical bugs, doxycycline 100 mg BD for 14 days. Alternatives - TMP SMX or Clarithromycin.
Chronic Q fever or IE:
native valves: doxycycline and hydroxychloroquine (200 TDS) for 18 months
prosthetic: same but 24 months
why hydroxy: enhances the action of doxycycline (increases the pH of the phagolysosome)
Follow-up: look for 4 fold decrease in IGG
Sources:
CDC
Stat Pearls
Wiki as linked above
#australian history#medblr#medblrs#infectious disease#infectious diseases#q fever#coxiella#coxiella burnetti
74 notes
·
View notes
Text
H5N1: What to know before fear spreads
What is H5N1?
H5N1 is a 1996 strain of the Spanish or Avian Flu first detected in Chinese birds before spreading globally across various avian species. H5N1 is similar to H1N1, but spreads slower and has a much higher mortality rate.
H5N1 may also be referred to as Influenza A. The American Association of Bovine Practitioners has seen fit to rename H5N1 to Bovine Influenza A Virus, or BIAV, and are encouraging others to use the same terminology.
I would not be surprised if the colloquial name among the public becomes Bovine Flu or American Flu in the coming months, and may be referred to as the Chinese Flu by the same folks who took the spark of the SARS-CoV-2 (COVID-19) pandemic as an excuse to be publicly racist to East Asian people without social repercussions.
BIAV is a virus, meaning that it is a (probably) non-living packet of self-replicating infectious material with a high rate of mutation. BIAV is structured similarly to SARS-CoV-2, having a packet of infectious material encased in a spherical shell with a corona, or crown, of proteins that can latch to living cells to inject RNA.
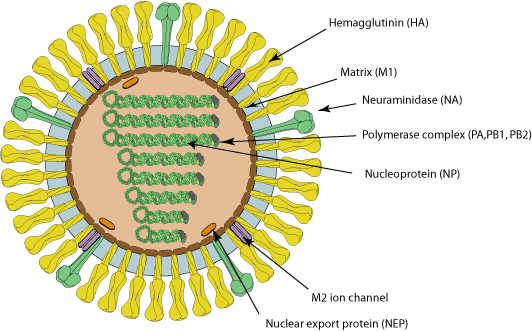
Image source with interactive model: ViralZone - H5N1 subtype
What is the history of BIAV?
In 1996 and 1997, an outbreak of BIAV occurred among poultry and infected 18 people in Hong Kong, 6 of which died. This seemingly isolated incident then infected ~860 people with a >50% death rate.
At the time, BIAV was known as Highly Pathogenic Avian Influenza, or HPAI, and killed nearly 100% of chickens within a 48 hour period.
From 2003 to 2005, continual outbreaks occurred in China and other East Asian countries, before spreading to Cambodia, the Netherlands, Thailand, and Vietnam.
From 2014 to 2016, it began being detected in American fowl, as well as mutating the H5N6 (lethal in birds, no human to human transmission) and H5N8 (largely spread through turkeys, ducks had immunity) viruses.
BIAV has since evolved into a clade known as 2.3.4.4b, and was first detected in 2021 in wild American birds. This then caused outbreaks in 2022 among wild and domesticated birds (such as chickens) alike, but was largely being overshadowed by the pressing SARS-CoV-2 pandemic at the time.
From 2022 to 2023, it was observed to be spreading among various mammals, including humans. Now, in 2024, we're having the most concerning rapid outbreak of BIAV since 2003.
BIAV is known to spread from mammal to mammal, particularly between cows and humans. BIAV may also be spread from cow to cow (highly likely, but not confirmed - this is likely the reason the virus has spread to Idaho from Texan cattle), and is known to be lethal to domestic cats and birds within 48 hours.
How does BIAV spread?
BIAV spreads through fomites - direct contact with infected animals or infected surfaces and then touching parts of your face or other orifices - as well as through airborne particulates, which may be inhaled and enter the sinuses and lungs.
BIAV is known to spread through:
Asymptomatic Ducks, geese, swans, various shorebirds
Symptomatic, may be lethal Foxes, bears, seals, sea lions, polar bears, domestic cats, dogs, minks, goats, cows, (potentially human to human, but unconfirmed - there have only been 8 potential human to human cases in 2024).
How can I protect against BIAV?
As BIAV is a type of Influenza A, existing protocols should do fine.
Current recommendations are to wash your hands vigorously after interacting with birds (I would also recommend doing this with mammals), avoid touching your face or other open orifices, and wear N95 masks.
Avoid sick or dead animals entirely - I would also recommend reporting them to your local Animal Control or veterinary centre and warning them about the infection risk. People who work with animals are recommended to also wear full PPE such as N95 masks, eye protection, gloves, and partake in vigorous hand washing.
If you suspect you've caught BIAV, seek medical attention immediately. Existing medications such as oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil can reduce BIAV's ability to replicate.
Standard flu shots will not protect against BIAV. Remember - symptoms of BIAV may not manifest for between 2 to 8 days, and potentially infected people should be monitored for at least 10 days.
How far has BIAV spread?
BIAV is currently a global virus, though the current infection location of note is the United States.
Image Key: Dark red - Countries with humans, poultry and wild birds killed by H5N1 Deep red - Countries with poultry or wild birds killed by H5N1 and has reported human cases of H5N1 Light red - Countries with poultry or wild birds killed by H5N1
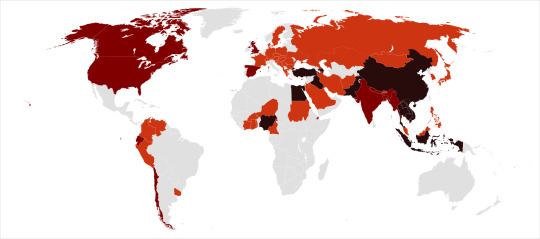
Image source: Wikipedia - Influenza A virus subtype H5N1 - File: Global spread of H5N1 map
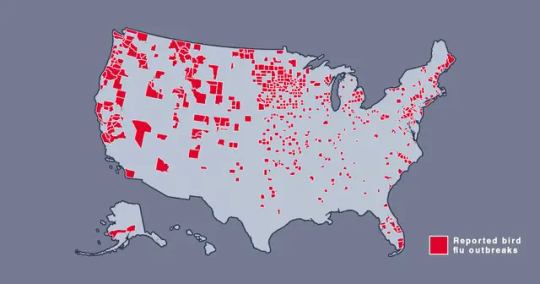
Image source: Metro.co.uk - Map shows where bird flu is spreading in US amid new warning - File: The Centers for Disease Control and Prevention’s H5N1 bird flu detections map across the United States
Should I be afraid?
You needn't be afraid, just prepared. BIAV has a concerningly high lethality, but this ironically culls its spread somewhat.
In the event human to human transmission of BIAV is confirmed, this will likely mainly affect marginalized communities, poor people, and homeless people, who are likely to have less access to medical care, and a higher likelihood of working in jobs that require frequent close human contact, such as fast food or retail jobs.
Given the response to SARS-CoV-2, corporations - and probably the government - may shove a proper response under the rug and refuse to participate in a full quarantine, which may leave people forced to go to work in dangerous conditions.
If this does spread into an epidemic or pandemic, given our extensive knowledge about Influenza, and the US having a backup vaccine for a prior strain of H5N1, a vaccine should be able to be developed relatively quickly and would hopefully be deployed freely without charge - we won't have to worry about a situation like The Stand.
Wash your hands, keep clean, avoid large social gatherings where possible, wear an N95 mask if you can afford them (Remember: Cloth masks are the least protective, but are better than nothing. If you can't afford N95 masks, I recommend wearing a well-fitted cloth mask with a disposable face mask over it to prevent pneumonia from moisture buildup in the disposable mask), support the disabled, poor, and homeless, and stay educated.
We can do better this time.
Further things to check out:
YouTube: MedCram - H5N1 Cattle Outbreak: Background and Currently Known Facts (ft. Roger Seheult, M.D.)
Wikipedia - Influenza A virus subtype H5N1
Maine.gov - Avian Influenza and People
CDC.gov - Technical Report: Highly Pathogenic Avian Influenza A(H5N1) Viruses
Wikipedia - H5N1 genetic structure
realagriculture - Influenza infection in cattle gets new name: Bovine Influenza A Virus (BIAV)
#H5N1#bird flu#avian flu#bovine flu#BIAV#pandemic#epidemic#COVID 19#coronavirus#spanish flu#long post#text post#no id#undescribed#news#politics#us news#us politics#american news#american politics#world news#global news#global politics#world politics#lgbt#lgbtq#queer#trans#communist#socialist
49 notes
·
View notes
Text
Leptospirosis: What it is, what it does, and how you can protect yourself and your pets.
People always have questions about leptospirosis (lepto) when they come into the clinic, especially in regards to the vaccine. This post will hopefully clear up those questions or any confusion regarding lepto and its vaccine, and why it's so serious. The information in this post comes from my formal education as a LVT, as well as other sources including the CDC, PAHO, and AVMA. If I missed anything or you see something that's incorrect, please let me know!
First and foremost: What is leptospirosis?
Leptospirosis is a bacterial disease that effects human and non-human animals. It's caused by bacteria in the genus Leptospira. In humans, it can cause a wide range of symptoms that can be very general. This leads to misdiagnoses. Animals such as dogs, livestock, and certain wildlife are all susceptible to infection.
How is leptospirosis spread?
Lepto is most often spread through contact with the urine of an infected animal. This is especially the case (but not the only case) with wild rodents. Infected dogs can seem healthy, but still pass the bacteria on in their urine. In urine-soaked soil, the bacteria can survive for weeks to months.
Dogs typically become infected when their mucous membranes or open wounds come into contact with urine or urine contaminated surfaces (like soil or water). Infection can also be spread through urine-contaminated bedding or food, or the tissues from the carcass of an infected animal. There have been rare instances where lepto has been transmitted by bite or breeding. A pregnant dog who is infected may pass the bacteria to her puppies through the placenta.
Humans contract lepto pretty much the same way: through contact with urine from an infected animal or urine-contaminated surfaces.
What are the signs and symptoms?
In humans:
High fever
Headache and muscle aches
Chills
Jaundice
Vomiting and diarrhea
Redness of the eyes
Abdominal pain
Rash
Humans can also be asymptomatic, which is particularly concerning. It usually takes anywhere from 2 days to 4 weeks post-exposure to the infection source before any symptoms are displayed. The illness begins abruptly and it may occur in 2 phases. The first phase is where you will see a lot of the general symptoms listed above. The person infected may recover for a period of time, but become ill again. The second phase is more severe, leading to kidney or liver failure, and possible meningitis. The illness can last a few days to 3 weeks or longer.
Without treatment, recovery can take several months.
In dogs:
Signs and symptoms may vary slightly depending on the strain of the infected bacteria. The signs are also very general in dogs, but the most common ones include:
Loss of appetite
Vomiting and diarrhea
Lethargy
Abdominal pain
Jaundice
Dehydration
Increased thirst and urination
Weight loss
Stiffness or muscle pain
The disease can also progress to kidney and liver failure in dogs, with damage to other organ systems also noted in the literature. Lepto can also cause bleeding disorders, which can lead to blood in urine, vomit, feces, or saliva, and petechiae on the mucous membranes or light colored skin.
Who is most at risk?
For humans, those who are most at risk include those who work with animals or outdoors where you come into contact with wildlife. The Pan American Health Organization (PAHO) also mentions that sewer workers and military personnel are at-risk populations. Farmers (and generally people who work with livestock) also make the list, as do veterinarians, veterinary technicians, and veterinary assistants.
For dogs, it's all of them. "All dogs are at risk of leptospirosis, regardless of age, breed, lifestyle, geographic location, time of year, and other factors." (source: AVMA)
Situations that can increase the risk of your dog contracting leptospirosis are listed below:
Exposure to drinking from slow-moving or stagnant water sources (this includes puddles)
Roaming on rural property
Exposure to wild animals or farm animals, even if it's only in the yard
Contact with other dogs (such as in urban areas, dog parks, boarding, or training facilities.
How is leptospirosis treated and diagnosed?
Disclaimer: I am NOT a medical doctor or DVM, but I am an LVT. If you think you're experiencing these symptoms, PLEASE go see your doctor. If you think your dog or any of your other animals are experiencing these symptoms, PLEASE take them to your vet.
Diagnosis in non-human animals:
Unfortunately, routine blood tests alone cannot diagnose leptospirosis. That's why it's important for your vet to use all information available to them (i.e. diagnostics, signs and symptoms, lifestyle, etc). There WILL be abnormal results for blood work, most likely high liver and/or kidney values and high white blood cell count. There are specific tests available for diagnosing lepto, such as the DNA-PCR and MAT tests. Both may be needed to reach or confirm a diagnosis. False negatives are possible, so your pet may be treated as if they have leptospirosis, even if the test results are negative. False positives are exceedingly rare.
Diagnosis in humans:
Leptospirosis is diagnosed in a similar fashion in humans. A physical exam, blood work, and urinalysis will likely be run. The same style of tests are used: DNA-PCR and MAT.
Treatment in non-human animals:
Leptospirosis is treated with antibiotics and supportive care. Doxycycline is most commonly used, and will likely be prescribed for 2 weeks or more. Supportive care includes hospitalization with IV fluids and management of electrolyte levels. Additional medications and procedures may be necessary.
Treatment in humans:
The treatment is similar in humans, with antibiotics (usually doxycycline). Your doctor may also suggest to take ibuprofen and monitor yourself at home for less severe cases. If the case is severe, then you'll likely spend time in the hospital. Additional medications or procedures may also be necessary.
Outcomes:
In non-human animals:
Leptospirosis is responsive to treatment with antibiotics. Complete recovery is possible, but some animals that survive may be left with chronic kidney and liver disease. Some animals may not survive if the infection has gotten to the point where it causes severe organ damage or the ability of blood to form clots.
In humans:
You can survive leptospirosis. Most cases have either very mild symptoms that go away on their own, or none at all. Without treatment, leptospirosis can cause kidney damage, meningitis, liver failure, trouble breathing, and even death. PLEASE go see a doctor if you think you're experiencing any of these symptoms, especially together.
Prevention
How can you prevent infection and protect your pets?
For dogs, there's the leptospirosis vaccine. This is an annual vaccine that vaccinates against multiple strains of Leptospira. If you're worried about your dog having a vaccine reaction, let your vet know and they can administer an injection of diphenhydramine (generic benadryl) beforehand, OR you can ask them what the appropriate dose is for your dog and give them the respective amount at home (in tablets or liquid). Vaccine reactions are uncommon, but if they do happen, it's usually immediately after exposure to the vaccine. You can ask to stick around in the lobby/waiting area of your vet clinic for a few extra minutes if you're still concerned.
Limit your dog's access to standing water. Don't let them drink from it. Prevent rodent problems where you can by properly storing food items in appropriate containers, securing your garbage, and patching up any access points into your house if you see them. Try to avoid contact with wildlife, when possible.
For humans, the recommendations remain similar. Don't wade or swim in stagnant water, ESPECIALLY if you have open wounds. Avoid contact with wildlife. WASH YOUR HANDS, often and appropriately. USE PPE if you work in a veterinary setting and properly clean and disinfect surfaces and equipment. Make sure you know or research the area that you're in if you like swimming and boating. Check to see if there have been any recent lepto infections. Cover your scrapes and wounds with waterproof bandages and wear water shoes if possible.
I hope this post answered a lot of your questions! Thanks for reading.
Sources under the cut.
Sources:
#animals#pets#dogs#leptospirosis#zoonotic diseases#infectious diseases#vet med#vetblr#petblr#dogblr#my posts
47 notes
·
View notes
Text
Bird Flu Updates Nov 19th 2024
A bunch of updates and info got released today and I saw a lot of people catastrophizing about them on twitter so I figured I'd make a post compiling it all with links. I suggest you read all of these articles yourself rather than trusting me, but I will include what I consider to be the main takeaways from each. (You can use this site to get around any paywalls.)
The preliminary genetic sequence from the very specific version of H5N1 the teenage patient in BC is sick with shows a couple of mutations that could help it bind to the cells in the respiratory tract and thus make it easier for it to infect humans and/or potentially spread between us.
While that sounds really bad, the article makes it clear this is just two mutations we think will make humans more susceptible to it, we do not know for sure what the real-world implications of this are, and as of right now we continue to lack any proof that the virus has truly gone H2H.
It is entirely possible that these mutations took place over the course of the teenager's illness, and were not present before. This is concerning because it ofc reminds us how easily this virus can mutate and evolve, but also a bit of a blessing because no one else has become sick so these mutations clearly are not enough for H2H spread, and also that means it's very likely that with the right precautions this version will die out once the teenager recovers. And even if other people become infected as long as they isolate we can still corner and kill off this version of the virus.
However, it mutating in this way once proves it can absolutely happen again, and surveillance and sequencing are important to make sure we know as soon as possible if these or other mutations occur.
D1.1 is the clade of H5N1 that is spreading in the wild bird population in Canada, and also is the one 11 farm workers in Washington were infected with while euthanizing infected poultry. However, these versions do not show the concerning mutations, leading credence to the theory that they occurred in the teenage patient's body and only there.
Currently no one else in the area, including people who've had direct contact with the teenage patient, have tested positive for H5N1. Serology testing of the patient's direct contacts is underway to confirm or deny if another person did catch it but had a mild or asymptomatic infection, the results should be in later this week.
Professionals interviewed repeatedly stress that surveillance is key, and also that the US is currently doing a piss poor job of handling this situation.
More info on the same subject can be found in this STAT article.
Update on the Hawaii outbreak, "H5N1 Avian Influenza linked to Mililani Pet Fair"
The outbreak has been confirmed in a backyard flock in Central Oahu.
Several birds from this flock were present at the Mililani Pet Fair which took place on November 2nd, and while the birds did not develop symptoms until after, it's entirely possible they were contagious but asymptomatic at the fair and thus could have spread the virus to humans and other animals present.
Direct Quote: "However, out of caution, the DOH is urging attendees who handled the affected birds to watch for symptoms such as fever, cough, sore throat, and pink eye, which typically appear within two to five days of exposure, though in some cases symptoms may take up to 10 days to develop."
The article goes on to say that while they believe the risk of it spreading from these birds to any other animals or humans is low, basically anyone who touched a duck or goose while there and becomes ill needs to seek medical attention.
"Those affected are also encouraged to contact their primary care provider for evaluation and to notify the DOH Disease Reporting Line at 808-586-4586, available 24/7."
"For those wishing to report unusual illnesses in birds or animals, the HDOA’s Animal Industry Division is available at 808-483-7102 during business hours or 808-837-8092 after hours and on holidays"
(Sorry posting a lot of that as quotes because it's important.)
A child in California tested positive for H5N1 despite having no known contact with infected animals.
While the test did come back positive at the hospital, it was a very low viral load and they also tested positive for other respiratory viruses that could have caused the symptoms, so as of right now this is being treated as a possible infection, not a confirmed one. We won't know for sure until samples taken reach the CDC who has the ability to do more in-depth and accurate tests.
Because it was a low viral load it is highly unlikely that the child was contagious. They also only have mild symptoms and are recovering at home.
Close family has all been tested and none came back positive for H5N1, though a couple did have the same non-H5N1 respiratory illness the child did.
The child did attend daycare while symptomatic, and as a precautionary measure the California Department of Public Health is reaching out to everyone who was potentially exposed and their families to offer tests and preventative care.
This statement reiterates that the risk to the general population is still considered low, there is no evidence of H2H spread, all infections in the state have been mild and none required hospitalization, pasteurized milk is safe to drink, and that farm workers are urged to get the current seasonal flu shot.
Six new human infections, and one presumptive positive that is awaiting confirmation. (However this article is from yesterday, I believe one new case and one presumptive positive have been added in California today, Nov 19th. You can keep up with the numbers here.)
All mild, the California cases were all dairy workers, the Oregon one worked with poultry.
This is the first human case in Oregon.
Still no evidence of H2H spread.
21 of 28 monitored wastewater treatment plants have tested positive for H5N1, but experts believe that could be from unpasteurized milk, bird droppings, or contaminated animal products that were thrown out.
Risk to the public is still considered low.
Still no idea how the teenager in BC caught it, but apparently their family dog was dealing with a number of health issues and was euthanized around the same time the investigation began, and while the first test on the dog did not come back as positive for H5N1 they are going to perform a more detailed autopsy to make sure the dog wasn't the source.
Worth noting that this teenager lives in Fraser Valley, which, according to this article, has very high amounts of H5N1 in the environment.
Other Info:
This Newsweek article claims to have gained access to emails sent by Michigan health officials who theorize indoor cats are getting H5N1 from their humans, but not from the humans getting sick, just from them unknowingly picking up some of the virus on their clothes or shoes while outside and dragging it in with them, where their cats can be exposed.
This study using ferrets has interesting results on how previous infections with other, similar flu viruses might either offer more or possibly less protection from H5N1.
This article explains what mutations we would have to see in H5N1 for it to become transmissible between humans.
My Thoughts:
I still fully believe the experts when they say we do not have any proof of H2H spread of H5N1 at this time. The fact that we have yet to see contacts with sick people become sick themselves shows that we're still safe.
I think right now the best thing we can do is continue to minimize the chance that we ourselves become the mixing vessel that gives H5N1 those mutations. That means:
Avoiding interacting with wild animals and birds, especially ones that seem sick. Don't pet stray cats or dogs, don't play wildlife rehab in your backyard with a sick animal you found at the park, now is not the time for careless contact with something that could get you seriously sick. I would also avoid going to farms, fairs, or just interacting with any poultry or livestock if you aren't 100% sure the animal isn't sick, and if you do interact wear a mask at the very least. A farmer's market is probably fine, but I'd still wear a mask if I were you.
I would avoid cleaning up dead animals, especially birds, on your own unless you have absolutely no other choice. Look up if your local gov has a number to call for this sort of thing, and if they don't and you're on your own wear proper PPE(gloves, N95, long sleeves and pants, ect.) and wash up thoroughly afterwards.
Teach your kids to stay away from sick or dead animals, especially birds. Also don't let your pets near them, watch your dogs if they're in the yard or on walks, and I would seriously suggest keeping your cats indoors. (There have been 53 cases of H5N1 in domestic cats in the US, and only two of them were indoor only, the rest were either outdoor only or indoor/outdoor. Keeping them inside clearly drastically reduces the risk of your cat getting sick, and as far as I've seen H5N1 is almost 100% fatal in cats.)
Wearing a mask, any mask, when you go out. It's clear people are catching this from the environment, and on top of that we are going in to cold and flu season and I've heard reports of ERs being swamped by people sick with various respiratory viruses, so masking up is probably the best thing you can do to protect yourself and others.
On that same note, get your flu shot, covid booster, and if you qualify for them your RSV and pneumonia vaccine. Getting sick at all is not great atm, but if you do catch H5N1 you want to REALLY make sure you don't get something else at the same time, because that would give the virus everything it needs to mutate into something extremely dangerous.
Learn the symptoms of H5N1 and be on the look out for them. If you get sick with respiratory symptoms AND pink eye, especially if you did have contact with a bird or other wild animal, contact a doctor to get tested and treated, and isolate as best you can.
Continue to avoid raw milk. Drinking raw milk is the stupidest thing you could possibly do atm fr do not drink raw milk. I still think eggs and beef are safe, but if you want to be extra mega safe cook both all the way through to ensure any bits of virus are dead. Also wash your hands after handling eggs, even just in the shell. The outside of eggs can get pretty dirty.
Consider stocking up on masks and buying an air purifier, as well as maybe some cleaning supplies if you're concerned about dragging it into your house. Don't panic buy, but if you've been putting off buying any of this stuff I would go ahead and start doing so now.
If you have a mice problem and the means to do something about it, especially if you have a cat, now is the time to do something about it.
And of course, there are people being hella dramatic on twitter about this, so remember that it has not gone H2H and it is almost 100% certain that should that happen the Case Fatality Rate will NOT be 50%. As I said in my other post CFR is a constantly fluctuating variable based on how many people have already died, it is not the odds that any given person who gets it will die, and we are clearly missing cases that are so mild people don't even realize they're sick, so the CFR is absolutely lower than 50%. You should try to ignore people who make sweeping claims without sources, they're just trying to exploit your fear to farm for engagement. The best thing you can do is protect yourself so you do not become the mixing vessel this virus takes off in, which means masking and other common-sense precautions. Things aren't great atm, worry is warranted, but the world is not ending and panic is not helpful.
Stay safe out there o/
15 notes
·
View notes
Text
Heads up folks, we might be in for Covid 2.0, in a manner of speaking. H5N1 is no joke. It's decimating entire herds of cows, killing tons of cats, and we're seeing mutations similar to what happened with the Spanish Flu. All on the heels of Covid, which has quietly ravaged a lot of our immune systems, not to mention a lot of our mental faculties. The following was copypasta'd from Facebook, from a tipoff from a biologist friend.
>
Sharon Astyk
rdotSonespc6gcf0ft8113iuia07750ig86a281141h8t43h8a4l0l7ah941 ·
The media has finally picked up the fact that we face an near-term bird flu pandemic, and is getting worried. And overwhelmingly, the narrative from popular medical folk on tv (most of whom are long term covid minimizers and got their roles for taking the Biden administration's "covid is nbd" position) and media outlets is "This pandemic will be much worse, it will make covid look like nothing."
And I understand why they are saying this, and I don't want to pick too hard on these folks, even though a lot them deserve it for their enthusiastic encouragement of mass infection and mass disability from a severe vascular pathogen. But they aren't wrong that H5N1 will almost certainly cause a much higher mortality, and that its larger range of animal transmission routes and fomites will create some challenges. But they are fundamentally and deeply wrong that this is really a fully separate, second pandemic. Pandemic two is actually part two or maybe five (depending on how you think about it) of the covid pandemic. And it is yet again covid running the show.
What do I mean? I mean H5N1 has been around for 30+ years, and has been a major concern on the global pandemic landscape forever, right? How could this be a continuation of covid. Well, let me count the ways. There are a lot of them - covid and H5N1 are working together in really important ways.
1. The first one, and one of the most important is something I warned you all about this summer - covid is providing enormous cover for cases of H5N1 to pass undetected in the general population.
This summer I was very (rightly, I fear) worried about the ways in which a massive summer wave, combined with emergent bird flu in farmworkers, and potential community spread might conceal H5N1 and allow it to mutate. When everyone has covid, respiratory and eye symptoms (which covid also causes) can pass undetected.
Moreover, when excess deaths are high, well above the expected rate, small clusters of even deaths are likely to pass undetected, attributed to covid, or other causes exacerbated by the pandemic. The rise in excess deaths from covid related causes, including strokes, heart attacks, brain bleeds, etc... and the chronic over extension of health care systems that often don't test means that we are missing a lot more Flu A cases that might have been bird flu.
How many did we miss? No clue. Remember, we cancelled all the covid reporting, and only have wastewater data right now, so there isn't even a good way to estimate what would be expected FROM COVID in the absence of public health interventions, and establish was was excess. I expect some good data on this in 2026 or 2027, but for now, we are flying blind.
This is really important because the CDC explicitly says that what they are looking for is unusual ER use and clusters of respiratory illness - but in an unchecked respiratory pandemic, that's very hard to identify. Remember, most cases of H5N1 are almost certainly going undetected both among farmworkers (we know there were clusters of farmworker and farmworker family illness that were never tested) and in the community.
2. Covid is an immune damaging illness. Almost everyone in the world has now had covid at least once, and a majority of people in most of the world have had it multiple times (we know this from immune assays, and most people who think they've never had covid are wrong - remember, 40% of infections are asymptomatic, and that's not a good thing, because often asymptomatic infections are a sign your immune system isn't responding appropriately and will not clear the virus.)
We have known since 2020 when China reported immune damaging properties from covid that covid damages Tcell response, and lowers CD8 counts. Eventually, your immune system does seem to recover in many people (not all) after 6-8 months without reinfection. However, most people who are not masking will not have six to eight months without reinfection, and we know that some of the damage is cumulative from multiple infections. Most people who get long covid don't seem to have the same recovery of immune properties.
So yes, covid is why you get sick all the time now. It makes you more vulnerable to other pathogens. And we also have evidence from animal studies that it does cause immune damage in some other species. Do you see where I'm heading with this?
One of the things that immunologists and virologists keep saying is that historically speaking, H5N1 is behaving in ways it has not in the past. For example, the virus has mutated in both wild and domestic cats and several other mammal species to infect mostly the brain, not the respiratory tract - it is now a neurotropic virus. Cats are having seizures, difficulty walking, blindness and death.
Remember, this is a virus that has been around for 30+ years and has infected a number of species before, but has mostly been a problem in industrial agriculture. It has now entered more than 50 mammal species populations, and a much wider range of birds than ever before (small songbirds for example, were previously rarely infected, as were corvids.)
There are birds falling out of the sky dead, seal populations losing more than 90% of their offspring, and we are vaccinating endangered birds so we don't lose them entirely (one of the things that I don't understand is how relaxed everyone was about mass extinction from bird flu - even if it never affected humans.)
Now I am not a virologist or an immunologist, and this is speculation on my part, but the timing matches, and my suspicion is that I'll be shown to be right later, sadly. It was in the autumn of 2021 that we really began to see H5N1 moving into animal populations it had not been in, and showing major changes in its effects in seals, mink, additional speciese of wild birds, and mammals.
What happened in 2020 and 2021 - well, we know that in 2020 and 2021, besides mass infection of HUMANS with the SARS2 virus, we also had widespread infection of wild animal populations. We know it was found in deer, in big cats in zoos, and in many species. And we know that it has immune suppressing and damaging qualities.
So when we ask, "Why is this virus behaving differently, particularly in mammals" we need to recognize that covid, unchecked, spreading through animal reservoirs, may well have affected its impact on those populations, and enabled the virus to spread into mammalian hosts and pick up some of the adaptations needed to infect mammals (btw, we are mammals) widely.
3. Another way this is an extension of our covid pandemic is our social response. The general public believes that we OVER-REACTED to covid. And they don't believe that by accident. That was a concrete, clear and intended message from a wide range of political actors from both parties.
The Republicans pretty consistently believe that we over-reacted to covid PERIOD - that it was an unserious disease that mostly infected people they thought deserved it, and that vaccination, social distancing, masking, etc... was always used for political power grabs.
But the Democrats believe similarly ridiculous things - despite the fact that we've known that long covid is a possible outcome from the very beginning, and that covid is vascular, neurotropic, raises your risk of cardiac and neurological problems, diabetes, autoimmune disease, cancer, cognitive decline, alzheimers, parkinsons, brain damage, kidney failure, hearing loss, eye problems, bone and hip joint problems and is immune damaging like HIV etc... etc... with each infection, they endorsed a "let it rip" position and removed masking in health care, on public transport, while telling people the disease was mild (coined for the omicron variant which was the MOST deadly one we had, look it up.)
By implying that school children were invulnerable because they were short (I'm not kidding) and that kids wouldn't transmit, rather than make schools safer by cleaning air and reducing class sizes, they engaged in a mass infection policy that is deeply damaging to the health of billions. Particularly horrific was the claim that the disease was inevitably mild in children, just because the acute phase was - leading to gaslighting families who couldn't understand why their children weren't the same, and also to reduced vaccination rates in kids, because why vaccinate for a mild illness?
Hospital acquired covid infections have a very high mortality rate, and yet, we removed masking in health care. Imagine saying "everyone should get the HIV virus, to build up immunity to HIV" - and that's pretty much what happened.
In order to explain why people were dying of heart attacks and strokes at younger ages, why cancer was striking younger and more severely, why diabetes rates were spiking, both parties came up with several implausible answers. The first was to leverage anti-vaccine sentiment and blame the vaccine. In order to do so, they had to create some really interesting new ideas, including the idea that you could "shed" the spike protein on to others.
The Democrats ALSO leaned heavily on anti-vaccine sentiment as I've written before - yes, they promoted the covid vaccine, and made ridiculous claims for it, calling those who died a "pandemic of the unvaccinated" even though vaccinated patients made up a majority of all deaths as early as 2021 (and yes, I know more people were vaccinated, but that doesn't change the claim.)
They allowed the anti-vax movement to carry a lot of water in explaining the even though we knew perfectly well that the things they were noticing were caused mostly by covid, they never acknowledged that, implicitly giving credence to the anti-vax movement.
They also came up with immunity debt, whereupon people who stayed home for six months in 2020 had to get really, really sick a lot, even though that doesn't happen to astronauts on space stations or Antarctic researchers because reasons. Immunity debt has been debunked many times, it is not a real concept, and did not exist before we needed an explanation for why covid was not the thing making you sick. I won't bother with it here.
They also claimed educational debt from the period where schools were online (not closed) was the cause of an increasing level of behavioral, health and intellectual problems CAUSED by a neurotropic, brain damaging virus.
Moreover, because they did not want to continue pandemic economic supports (which were good for people - half of American kids came out of poverty, premature births plummeted, an entire variety of flu went extinct, suicides among kids and teens dropped dramatically, wages rose, discretionary income rose, housing access was vastly improved, etc....) we were told over and over that covid was the worst time in our lives until we believed it, and that staying home had been a horror show. Now that does not make 2020 fun, and the casting of social supports back on families was a high cost, but this lie didn't serve families, it served people who wanted to make money.
The problem is that the general public who didn't have time for deep dives because life, BELIEVES all these things, because propaganda works. Which is why vaccination rates overall have tanked, because the anti-vaccine movement is still carrying a ton of the weight of explanation for covid (even though we long since disproved any additional risk), and immunity debt. Which is why people are still blaming the "lockdowns" for the fact their kids are struggling in school, and for food price inflation linked to bird flu and global warming.
SO YOU NOW HAVE A GENERAL AMERICAN PUBLIC WHO BELIEVES THE BEST WAY TO DEAL WITH ILLNESS IS TO GET SICK AS MUCH AS POSSIBLE AND THAT VACCINES ARE DEADLY. They also believe that masks are unnecessary, that public health measures do more harm than good, and were an over reaction. They believe that patriotism and good citizenship consists of going out to brunch and concerts and sporting events unmasked. They believe that teenagers were killing themselves because they couldn't go to school (I truly cannot believe anyone believes that last sentence who has met a teenager.) They believe controlling infection is not only unnecessary but harmful, and that social controls of disease are evil and bad.
So what do you think is going to happen when a high mortality flu pandemic hits the US, and public officials try and tell people that they need to isolate, stay home, reduce exposure, wear masks, take a vaccine and close schools and public venues?
The Democrats and Republicans who promulgated all these insane lies for their own and their rich benefactor's benefit are going to try and overturn them, but the problem is that it isn't as easy to UNTEACH things as it is to teach them. And since they STILL have a huge investment in denying that those things were necessary for covid, they are going to be selling a dual message - covid is cool, but bird flu is bad so mask and vaccinate and stay home for one but not the other - and most people can't tell them apart, because one of the central messages was covid is the same as flu.
Folks, flus, like covid, mutate far too fast to provide a sterilizing vaccine. A sterilizing vaccine is one like measles where you can basically stop the disease entirely by vaccinating enough people (no vaccine is 100% sterilizing so this is a functional category, rather than a precise one.) BTW, we ALWAYS knew that coronaviruses and flus don't provide sterilizing immunity, which is why you sometimes get flu even if you get the flu vaccine. That will not change with an H5N1 vaccine.
Even ignoring the fact that flu vaccines are mostly made in eggs, and that's going to be an issue too - so even if we have a vaccine made rapidly that applies to the strain that is circulating, it will do what the covid vaccine does - reduce severe illness and death in many people. It will NOT prevent you from being infected, and its protection will gradually wane as the virus mutates and changes its structure. And some people will still get severe illness and still die.
Antivirals, too, have limited use and at least one of the mutations that is already showing up in H5N1 reduces its sensitivity to some of the most common ones. So while anti-virals will help, they will not solve the problem or save everyone - even if they are available, and we are likely to have a severe shortage.
Which means that what will be needed are NPIs - Non-Pharmaceutical Interventions like handwashing, surface cleaning, masking, air cleaning, closing crowded venues like schools and theaters, reduced exposure. And those are things we just spent four years demonizing as unnecessary.
4. At the beginning of 2024, H5N1 still needed three mutations in order to be fully human to human transmissible. Two of them showed up during the cow flu segment in both birds and mammals. A third one, one of the things that made the 1918 "Spanish" flu so deadly, E190D, has shown up twice in humans - in both the teen in British Columbia who had severe illness lasting months, and the LA patient who had severe illness as well.
In both cases, the birds they likely contracted it from (in the BC teen, possibly through a pet mammal intermediary) the birds didn't have this mutation, suggesting it emerged in situ in the patients. That's a really concerning thing - twice now, H5N1 has developed the main mutation needed to make it transmissible to humans in a human patient, both with severe illness.
This is a HUGE jump. And an important one. Which makes my point #1 really critical - because we have no idea how many human cases of bird flu there have been/are currently. We know it is extremely hard to get your flu typed, that local labs still can't do it, although Labcorp is reportedly working on it, and that there are certainly undetected cases. IT ONLY TAKES ONE PERSON OR ONE ANIMAL MIXING VESSEL and flus are extremely good at mixing (which is why it is also a concern that several nations seem to be having an extremely severe and atypical flu season, because the severe elements of H5N1 or other potential pandemic flus including H3N3 and various H9s can also recombine with a seasonal flu already adapted to humans and make it more severe and dangerous.)
But what does that have to do with covid? Well, if I'm right about point #2, that the immune damaging factors of covid spreading through wild animal populations may have encouraged H5N1's mutations and mammal host adaptation (and again, I'm only speculating), it is also the case that a huge population of immune damaged HUMANS is now being regularly exposed (we know from wastewater that bird flu is showing up in urban populations with no farms) and that immune damaged people have a hard time fighting off viruses (that's why you get sick all the time again.)
And if your body is slow at clearing a virus, because your immune system isn't working particularly well, you are very likely to find yourself in a situation where you might have more than one virus at the same time (one of the characteristics of the covid era is coinfection with multiple viruses, much more than previously seen), including multiple flu viruses. And your body might allow mutations to occur more easily, because you can't fight it off.
We only know about 60-odd human infections this year, the majority of them in the US among farmworkers. The fact that TWO of them had the E190D mutation, out of 60something is really pretty stunning, since both patients formed it spontaneously. That suggests that something really is going on with human immune systems, and as happens, we know what that is.
The logical conclusion, which I cannot prove, but feel comfortable speculating about here - is that both mammalian mutations and human mutations are made more likely by covid infection related immune damage. That is, the likely reason we are about to have an H5N1 pandemic, and the reason it is going to be really unpleasant, much more than if we hadn't already convinced ourselves that the normal things humans do to stop diseases are all bad, is that we had a covid pandemic - or rather we HAVE a covid pandemic.
That is, we have a single pandemic with multiple sources, about to hit us with its second, much more severe wave. And it is going to be a doozy. If we had chosen to control covid, we might be in a very different place.
14 notes
·
View notes
Text
Also preserved in our archive (Daily updates!)
by Dr. Monica M. Bertagnolli
In 2021, NIH launched the Researching COVID to Enhance Recovery (RECOVER) Initiative , a nationwide research program, to fully understand, diagnose, and treat Long COVID. We continue to learn more about this condition, in which some people experience a variety of symptoms for weeks, months, or even years after infection with SARS-CoV-2, the virus that causes COVID-19. But we’re still working to understand the underlying reasons why people develop Long COVID, who is most likely to get it, and how best to treat or prevent it.
Studies have shown that for some people, SARS-CoV-2 doesn’t completely clear out after acute infection. Scientists have observed signs that the virus may persist in various parts of the body, and many suspect that this lingering virus, or remnants consisting of SARS-CoV-2 protein, may be causing Long COVID symptoms in some individuals. Now, in a new study supported by RECOVER, scientists found that people with Long COVID were twice as likely to have these viral remnants in their blood as people with no lingering symptoms. The findings, reported in Clinical Microbiology and Infection , add to evidence that Long COVID may sometimes stem from persistent infection or SARS-CoV-2 protein remnants.
The study team, led by David Walt and Zoe Swank at Brigham and Women’s Hospital in Boston, had earlier found preliminary evidence in a small pilot study that a SARS-CoV-2 protein could often be detected in the bloodstreams of people with Long COVID up to a year after the initial infection. In the new study, they wanted to better quantify this in a much larger group of people with Long COVID. The researchers developed a highly sensitive test to look for whole and partial proteins from the SARS-CoV-2 virus. They analyzed 1,569 blood samples collected from 706 people at various times after SARS-CoV-2 infection.
Overall, 21% of those in the study had detectable levels of a SARS-CoV-2 protein between 4 and 7 months after infection. In total, 82% of the study’s participants (578 people) had at least one symptom of Long COVID more than a month after their infections. Commonly reported symptoms included fatigue, brain fog, muscle pain, joint pain, back pain, headache, sleep disturbance, loss of smell or taste, and gastrointestinal symptoms. More than half of participants in this group (378 people) reported experiencing ongoing cardiopulmonary, musculoskeletal, or neurologic symptoms, and among those participants, 43% (165 people) had detectable virus protein. Also of note, of the asymptomatic people, about 20% had detectable virus protein.
While the researchers can’t definitively show that persistent infections are the cause of some Long COVID symptoms, the findings add to growing evidence that low levels of viral protein being present may explain some but not all cases of Long COVID. The authors and many other researchers suspect that Long COVID likely has multiple underlying causes. For instance, it’s possible that the virus may lead to harmful changes in the immune system that play a role in some cases of Long COVID.
Scientists also want to see if there is a subset of people with Long COVID or persistent symptoms who may benefit from antiviral treatment. To this end, RECOVER is supporting a clinical trial evaluating whether the antiviral drug Paxlovid (a combination of nirmatrelvir and ritonavir), which is used to treat COVID-19, could also be used to improve Long COVID symptoms. The trial is using the SARS-CoV-2 blood test developed by the Brigham and Women’s study team to evaluate whether Paxlovid can eliminate viral proteins from participants’ blood.
More study is needed to understand the causes of Long COVID symptoms in people who test negative for persistent infection, the researchers note. They are conducting follow-up studies in even more people with Long COVID, including those with compromised immune systems. They hope to learn more about what causes some people to be at higher risk for retaining some SARS-CoV-2 protein remnants and Long COVID.
Reference:
Swank Z, et al; RECOVER consortium authors. Measurement of circulating viral antigens post-SARS-CoV-2 infection in a multicohort study. Clinical Microbiology and Infection. DOI: 10.1016/j.cmi.2024.09.001 (2024).
Study Link: www.sciencedirect.com/science/article/abs/pii/S1198743X24004324?via%3Dihub (PAYWALLED)
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#long covid#covid is airborne
39 notes
·
View notes
Text
September is Chiari Malformation Awareness Month!
Hi yes hello! Since many people probably aren't aware of it, I wanted to bring attention to something we ourselves have called chairi malformation at the start of its awareness month! Its recognized with a purple ribbon usually with a zipper on it (for the zipper scars of those who've had Chiari surgery)
What is Chiari Malformation?
Chiari (key-arr-ee) Malformation is a brain malformation in which the brain is too large, skull is too small, or some combination on the both, causing the cerebellar tonsils (and in some instances the brain stem) to slip through the skull and into the spinal chord.
Chiari is most typically a congenital effect. There are two main types (though they aren't the only ones). The most common of the two us Chiari 1, in which only the cerebellar tonsils are descended through the skull. The second most common, Chiari 2 (also known as Arnold-Chiari malformation) has more tissue herniation in the cerebellar tonsils and even the cerebellum, as well as brain stem herniation as well.
(See Below, the Cerebellar tonsils are marked in red while the brainstem is marked in green and yellow. This is considered a normal MRI)
Chiari malformation is likely to occur in 1 in 1,000 people, making it uncommon but not rare. The statistics are likely to be slightly higher than that for Chiari 1, as many people don't present symptomatically (and many incidents are only found in cases where the person was receiving radiological imaging for other instances such as head injury, so many people are unaware they had Chiari to begin with).
The only way to diagnose Chiari is through radiological imaging (many arguing upright MRI specifically is the only proper way to view the real level pf herniation). Herniation is measured down from the McRae line to the lowest point on the cerebellar tonsils. Depending on the accuracy of the machine (and which imaging tool is used) herniation can appear at different levels at different times. (See below, my first MRI looks markedly less in comparison to my second MRI, which features a roughly drawn on McRae line. In the second image I was noted to have a 7-8mm herniation.)

Symptoms
Chiari is marked by a number of symptoms and commorbidities, even moreso depending on the type you have. Symptoms can occur at any level of herniation. Some people with Chiari can have a 3mm descent and have debilitating symptoms, while some may have a 15 mm descent and be completely asymptomatic. The most common of these is occipital headaches & migraines, ranging from mild to severe, but many more are possible. These range from...
Balance Issues
Dizziness & Vertigo
Neck & Shoulder Pain
Difficulty Swallowing
Sore Throat
Sleep Apnea
Nausea & Vomitting
Tinnitus & Hearing Loss
Blurred Vision, Visual Snow, & Vision Loss
Muscle Weakness
Numbness or Pins & Needles (Caused by Nerve Damage)
Poor Motor Skills
Fatigue
Cognitive Difficulties (including but not limited to Brain Fog, Memory Problems, Confusion, & Difficulty Speaking)
Insomnia
Photophobia/Light Sensitivity
Syncope, Fainting, & Drop Attacks
Seizures
Dysautonomia
Since the cerebellar tonsils block the opening to the base of the skull, Chiari can halt the proper flow of CSF (Cerebral Spinal Fluid) between the brain and the spinal chord. Because of this, Syringomylia (cysts filled with CSF formed on the spine called Syrinxs) is considered common with Chiari. Other common disorders with Chiari are Scoliosis, EDS & Cervicocranial Instability, POTS, Tethered Spinal Chord Syndrome, Spina bifida, & Hydrocephalus.
So What's the Solution?
Well, the only known solution for Chiari as of right now is surgery. This surgery is called posterior fossa decompression-- in which a small portion of the base of the skull is removed from the Chiari patient to relieve pressure and give more room for the brain. The surgeon can then do for sone patients a duraplasty, in which the dura (or opening of the brain) is cut open and a patch of tissue is sewed into the incision to make the dura bigger and give even more room for the brain. Surgery can also be done as a preventative measure against syrinxes for those without them. In the case the patient also has a syrinx, more surgical procedure can be done to drain the cyst. In patients with EDS, special procedures must be made to avoid surgical complications and making things worse.
Surgery is not guaranteed to completely alleviate symptoms, but typically helps with some. However, due to large misunderstanding and disagreement on proper diagnostic traits of Chiari from doctors (most typically neurologists and neurosurgeons) many may be denied surgery for a number of years, and Chiari Diagnosis can take on an average of 4 years to officially receive.
Some go years experiencing symptoms and having "low lying cerebellar tonsils" (or similar language, such as incidental tonsillar ectopia) noted on their radiology reports without doctors officially recognizing it as Chiari. In this time many are misdiagnosed with other disorders such as chronic headaches, multiple sclerosis, fibromyalgia, and more before finally finding a doctor who will listen. Many will brush off the radiological findings as just a difference in your brain being formed at birth before admitting the symptoms can be due to Chiari. It can take years of your own patient advocacy before someone finally listens.
This is why awareness to it is so important, in hopes of reaching other people and doctors and forming a stronger understanding of the condition from information found by experts on it and those with Chiari themselves. With more awareness comes more accessibility to treatment and surgery so those who are symptomatic can hopefully find some relief. So this month send a little love & luck to those with Chiari!

#chiari#chiari malformation#chiari awareness#neurological disability#disabled#disability#disability awareness
37 notes
·
View notes
Text
Toward the end of last year, US health authorities got a tip-off about an upcoming wave of respiratory syncytial virus, a seasonal virus that kills 160,000 people globally every year. Before hospitals reported an uptick in patients, they could see that RSV was more acute in the northeast of the country, with concentrations of the virus ultimately reaching levels more than five times greater than in the western United States. Their early warning system? Wastewater.
By regularly testing virus levels in public wastewater, health institutions are able to target treatments and interventions to the worst-affected areas before doctors on the ground realize something’s going on. “If you can get the information to hospitals or clinics weeks earlier, that gives the opportunity to start thinking about what treatments they might need,” says Marisa Donnelly, senior principal epidemiologist at Biobot Analytics, which helped develop a wastewater surveillance system for the US Centers for Disease Control.
RSV is very common: Every year, 64 million people worldwide get an RSV infection, according to the US National Institute for Allergy and Infectious Diseases—but it’s particularly problematic for the very old and very young. Preventative measures are available, including vaccines and monoclonal antibodies. But often, by the time a community recognizes it has an RSV outbreak, it’s too late to mount the most effective response. Getting hold of enough drugs can also be tricky. “Wastewater analysis gives you better situational awareness of what’s going on and how much it’s fluctuating over time, because we have [historically] very much underdetected RSV cases,” says Bill Hanage, associate director of the Center for Communicable Disease Dynamics at the Harvard T.H. Chan School of Public Health.
The concept of tracking a virus through wastewater came to prominence in the early days of the Covid-19 pandemic in 2020, says Tyson Graber, associate scientist at the Children's Hospital of Eastern Ontario Research Institute, who worked on wastewater analysis as part of Ontario’s Covid response. Initially, researchers weren’t too hopeful. “Nobody thought that you could actually detect bits and pieces of material from a respiratory virus,” says Graber. Yet it proved possible: The scientists were able to detect the presence of SARS-CoV-2, the virus behind Covid-19.
This near-real-time analysis of the virus’s spread helped improve responses to the pandemic not just in Ontario, but worldwide. In the US, the CDC launched its National Wastewater Surveillance System in September 2020.
While each pathogen has its own “predilections and eccentricities,” says Graber, it was possible to adapt the process to look for RSV. Regular RSV testing in wastewater now takes place in the US, Canada, Finland, and Switzerland.
A study of the Ontario experiment in RSV wastewater tracking found that it gives more than a month’s notice in identifying when RSV season begins, and nearly two weeks’ warning of a surge, compared to waiting for people to turn up sick. “We definitely see increases in [RSV in] wastewater starting before we see those same increases in clinical data like hospitalizations,” says Donnelly.
Jasmine Reed, a CDC spokesperson, says that wastewater analysis complements other surveillance systems. “It can capture asymptomatic cases and other cases independent from medical systems, and provides a broader population-level perspective on disease spread,” she says.
The CDC’s program is set up so that, if RSV levels are high in a particular community, local health departments can prioritize interventions, including testing, infection control, and vaccination efforts.
Donnelly envisions wastewater surveillance becoming like a public health “weather app” where communities can check virus activity in their area and make informed decisions on behaviors like masking or vaccination. “We want this system to be expanded across the United States so that everybody has access to wastewater information and add additional tools to keep themselves healthy,” she says. Hanage foresees wastewater analysis being used to track other communicable viruses, like mpox.
While there’s plenty of excitement about the technique, others are more cautious. “It’s one of those sciences that has got a lot of people really excited,” says Paul Hunter, a virologist and professor in medicine at the University of East Anglia. “You either think it’s brilliant or you think it’s pointless, and there’s very little in between.”
Hunter recognizes that wastewater analysis can pick up the spread of disease—and points to evidence that it did so in the Covid-19 pandemic—but questions whether the extra cost is worth the extra insights it provides. “Certainly in Covid, we didn’t think it was [necessary] in the UK, and I think that was the correct judgment,” he says.
But proponents say it’s worth it for RSV—especially given some of the challenges around drug shortages. Last year’s RSV season proved particularly vexing to the US health system, as shortages of nirsevimab, an antibody injection given to infants, were reported across the country.
There’s hope that things will be different when RSV season begins again in the coming weeks. “If you can get the information to hospitals or clinics weeks earlier, that gives the opportunity to start thinking about what treatments they might need,” says Donnelly.
3 notes
·
View notes
Text

A/N: I wanted a road trip fic, and considering this idea has been gathering dust for about a month now I figured I could give it life. I love Carol Danvers-She’s my wife (Diana Prince is DC wife) and I’ve honestly lost track of how many times I’ve seen Captain Marvel. Not to mention the poster (I had, it got torn -_-), the keychain, THE HAT (Like in the photo! I have one!), the little lego figure, the lunchbox…. Yeah, she’s my wife. Also kind of a slowburnish fic for the first part. I am considering making this into a small series.
Pairing: Carol Danvers x F! Reader
Warnings: Language, talk about COVID in USA. Dissing the USA’s government.
Words: About 1.5k
Tagging: @tyler-t0t
Summary: After being cooped up in the tower for months during quarantine, you need to get out and get moving. You’re restless, and can barely fall asleep because of it. Then, Carol Danvers makes you an offer: A two-week road trip to see her friend and her god daughter. It’s two weeks straight in a car, with minor detours depending. With nothing better to do and the fact that you might rip your hair out if you have to stay inside for another fucking week-you accept.
~~
“I need to get the hell out of this tower.” I grumbled as I paced by the bay windows. Natasha watched in interest as my rapid steps thundered throughout the room.
“Well they’re still trying to find a cure for the virus. We can go out, but we need to distance ourselves and wear masks.” She replied, lazily picking at her nails.
“Yeah, but I need to get out of this city. As much as I love the bustle of New York, I need to get out - take a break from the noise, the smells, the city itself. I need to get out into the country again.” I said as I walked towards the kitchen.
Despite quarantine making almost everyone gain some weight, I had stretched and done nearly everything I could indoors. It included working out, and I was happy with the results of that hobby. Arts and crafts were burned out, as well as movies and tv shows. Actually, the only thing I really did anymore was swim and read. Everything else I’d done to the point of mental exhaustion.
I opened the fridge and pulled out a beer, ignoring the fact that it wasn’t even four in the afternoon yet.
“Well, you could go on a road trip.” She said, her torso leaned back over the arm of the couch as she stared at me. Stretching like a lazy cat, she got up and silently padded to the kitchen. I handed her a beer and lifted myself up to sit on the island counter.
She nodded in thanks and took a sip from it. “I’ve got nowhere and no one to go to, Nat. Not even Clint’s family, because if I have the virus I don’t want to give it to them.” I replied.
She nodded, remembering what we’d agreed on.

“We can’t do anything to help. I’d actually look bad if we went out and did anything. The best thing is to stay here, and only if we’re absolutely needed, then we leave.” Steve said as he flipped through the folder on the table. We’d finally gotten the official word from S.H.I.E.L.D. about what we were supposed to do. Or rather, what would look good to the press.
Cases were rising and it seemed everyday they doubled, or tripled, in some states. I wasn’t worried for anyone in the tower, save Tony because even though the man had a metal heart, I doubted he washed his hands often.
“And in the meantime?” Sam asked him, flipping through his folder. Steve started listing off ideas and I tuned out, starting to look through my own folder.
Inside were some lists and things we could do, put together by the ever-loving government. Most ‘Ideas’ included making our social media presence known and trying to encourage people to stay home, followed by training when we didn’t have anything better to do.
“I’m not going back home, not with travel restricted and asymptomatic people.” Clint spoke, his hands resting on the back of his chair as he stared blankly at the table.
“It’s going to be okay, Clint. As soon as we’re cleared and the lockdown ends, we’ll be off. Until then, no one gets to visit your family. It’s for their safety.” Natasha said, soothingly rubbing a hand on his back.
First thing on my list was sleeping, because I’d barely gotten back from a six week mission when this shitstorm started. Staying home for a while sounded nice.
“(Y/N), what’s the first thing you’re going to do?” Bruce’s voice ripped me out of my thoughts. I gave him a small, sleepy smile and replied that I was probably going to sleep for a week or so. The doctor chucked and patted my shoulder as he left the room, the others slowly draining out.
I sighed as I flipped through the folder some more, rereading the paper until it was memorized. I headed out of the conference room and to my floor, only stopping to get some food from the kitchen. We might have a small kitchen on our floors, but the best food was kept in the main kitchen.
I yawned as I set the basket and the folder down on the kitchen island, and headed to my room. I kicked my shoes off and practically collapsed on the bed. I was out before my head hit the pillow.
“I know that Clint isn’t even going to them. It’s horrible, I have no idea why we’re still not on lockdown.” I said as I absentmindedly read the label on the bottle.
Natasha sighed as she drained her beer, and tossed in the garbage. “Because our government is filled with horrible people who value their own wealth over the lives of others. Greed is what America has become.” She said over her shoulder as she headed to the elevators.
Where she was off to wasn't my business and I had a feeling she’d rather shoot me than have me find out about it. I stayed in the kitchen while I finished my beer, going through my ‘inspirational’ Instagram feed of people doing their routines and workouts from home. I grew tired of it rather quickly, and tossed my empty bottle in the trash. Maybe I should just delete social media in general.
I walked out of the kitchen, busy enough deleting Snapchat and Instagram that I didn’t notice I was about to bump into someone until we collided.
“I am so sorry!” Immediately came out of my mouth as I stepped back, looking at the figure who was….
Carol freaking Danvers.
I had no idea she was staying here, let alone that she was on this planet.
“Hey, it’s no big deal. I was actually looking for you.” She said as she straightened her jacket. Her blonde hair was growing long, just barely running past her shoulders. Dressed in a pair of workout pants and her windbreaker with a white pair of sneakers - and the fact that she had her bluetooth headphones around her neck, it seemed like she just got back from a run outside.
“Me?” I questioned, raising an eyebrow. She grinned and I swore my heart shuddered at the sight. It wasn’t known that I had a moderate-to-severe crush on her, and as far as I was publicly concerned, only Natasha and Wanda knew about it. The latter had told the former. Damn mind readers.
“Natasha said you were about to go insane from being cooped up in here.” She replied, heading past me and into the kitchen. I turned and watched her start to make a protein shake.
“I’m taking a road trip to see my friend. It’s a two week drive, because she lives in the middle of nowhere. I was looking for someone to come along with me.” She said as she prepared her drink.
My jaw opened and closed like a rusty gate before my brain finally registered the words and formed an answer to them.
“Yeah, sure. When do we leave?” I asked. I finished deleting all the social media, save Pinterest, Tumblr, and Youtube off my phone. Bye-Bye snap streaks.
“Tomorrow. I was figuring we’d stop and get some snacks before we headed out on the road. You’re not allergic to cats, are you?” She asked me, sipping her drink.
I shook my head. A two week road trip with my crush? Holy shit…
She nodded at me. My phone buzzed, and with a glance I knew that Natasha had set me up for this.

Wow. Sometimes you love your red headed assassin friends.
“Okay then. Guess I’ll go pack.” I said as I turned, headed for the elevator.
Holy shit.
#miscfandomwrites#avengers x reader#marvel#marvel x reader#Carol danvers#carol danvers x reader#captain marvel#captain marvel x reader
7 notes
·
View notes
Text
Americans with well-treated HIV can no longer be barred from enlisting in the U.S. military, a federal judge ruled Tuesday, striking down the Pentagon’s last remaining policy limiting the service of those with the virus. “Defendants’ policies prohibiting the accession of asymptomatic HIV-positive individuals with undetectable viral loads into the military are irrational, arbitrary, and capricious. Even worse, they contribute to the ongoing stigma surrounding HIV-positive individuals while actively hampering the military’s own recruitment goals,” wrote Judge Leonie Brinkema of the U.S. District Court for the Eastern District of Virginia. In her ruling, Brinkema mentioned her landmark 2022 decision that ended the Defense Department’s long-standing policy of forbidding service members who were diagnosed with HIV after enlisting from deploying in active duty outside the continental U.S. and being commissioned as officers. “Modern science has transformed the treatment of HIV, and this Court has already ruled that asymptomatic HIV-positive service members with undetectable viral loads who maintain treatment are capable of performing all of their military duties, including worldwide deployment. Now, defendants must allow similarly situated civilians seeking accession into the United States military to demonstrate the same and permit their enlistment, appointment, and induction,” she wrote. Research has shown that people with HIV who have an undetectable viral load thanks to antiretroviral treatment, as is the case for the vast majority of people on HIV treatment, cannot transmit the virus to others through sex. Advances in care and treatment of the virus have extended the lifespan of people with the virus to near normal. People with well-treated HIV are effectively healthy. However, they are still at higher risk of various health conditions related to aging, including heart disease and various cancers.
3 notes
·
View notes