#in combination the symptoms can look really similar to bpd
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, Tumblr had 29.4 million users in the US.
Text
the borderline symptoms in early to mid-teens to npd sublimation cope pipeline
#this post is about me specifically hi#I spent a decent chunk of my teenage years flipping back and forth on whether or not I had bpd#then a bunch of shit happened (including me getting my hormones in order) and I realized that no#it’s actually grandiose npd and aspd/antisocial tendencies#+ bipolar 2#in combination the symptoms can look really similar to bpd#or at least in my case. this isn’t advice I don’t know you#faustian.txt
2 notes
·
View notes
Note
hey!!! if its ok i’d like you’re thoughts on something ig and to sorta ask you something
so im bodily 15 atm, and i have cptsd. when i look at posts regarding certain cluster b experiences (possibly some cluster c aswell) i relate a LOT (obviously im not saying that bc i relate that i have these disorders, i just kinda have a feeling that *something* is going on). its tricky bc i keep looking into things and i cant really find an answer. i also dont know if im too young and that its just because im a teenager.
i wont get into like what “symptoms” i experience rn bc i feel like thats a whole other conversation but yeah.
i hope i dont sound like one of those people that are like “i must have x bc i related to a silly video i saw” im just really confused and i feel like something aint right
i know you’re probably not professionals so feel free to delete or ignore this if its too much, but if not, what do you think?
So, here's the thing (and we will attempt to avoid being patronizing): It is absolutely correct that your age and emotional/psychological development can affect things, and that the process of development can cause things that look like mild symptoms. It's also correct that that combined with c-ptsd (and any other disorders you may have; you'd be surprised how many symptoms and comorbidities autism, ADHD, NPD, and BPD all share) can make it extremely hard to determine where your symptoms are coming from and whether there might be something more.
(You're also correct that we are not professionals; this is all coming from our own research and personal experiences, so as with everything, take this with a grain of salt.)
However. I would argue that it would be far more harmful to deny any possibility of having a personality disorder until you reach some arbitrary age threshold than it would be to say that you do have a PD. Especially if looking at your life experiences through the lens of having a PD is helpful, and if resources for pw/[x]PDs are helpful to you. Even if you don't end up having a PD, that doesn't mean you were just a hormonal stupid teenager refusing to listen to the Adults™ or whatever the fuck--it means that you looked at your experiences, found something that seemed similar, and it turned out that you were wrong; but hopefully, along the way, you found things that were helpful.
Under the assumption that you have done a lot of research, I would personally recommend saying that you have traits of a particular disorder as opposed to saying you have the full disorder, and that is to two ends: one, a lot of adults with PDs (especially in ASPD spaces, if that's one of the disorders you're looking at) will kick your shit to hell and back if you even insinuate that you think you may have the full disorder (which I think is extremely counterintuitive if we want teenagers to understand their experiences and, yknow, not develop a full-blown personality disorder, regardless of whether you think teenagers can have a full personality disorder); and two, it might help you target the specific symptoms that you're experiencing without saddling you with the belief[/knowledge] that you have an incredibly stigmatized and lifelong disorder.
A lot of this stuff depends on a few things: (A) what your symptoms are (and if they can be better explained by other things, especially other things you know you have); (B) how severe your symptoms are (like the difference between being generally grouchy versus being actively hostile); and (C) how long your symptoms have lasted (if they only started popping up in the past few months or the past year versus if you've had them for years and years).
If you end up not having a personality disorder, anon, I think it will still be better for you in the long run to explore the possibility instead of shrugging it off under the excuse that you're "too young". It could turn out that you never had the disorder and it really was something else, it could turn out that you have traits but not the full disorder, or, hell, it could turn out that, by using resources and support you found by being part of communities surrounding PDs, you ended up not developing the full PD (even if you may still have a few traits)--because, at this age, you are still developing, and you are changing a lot, and very little is set in stone when it comes to these types of things--and you should absolutely take advantage of that! And even then, speaking from a more selfish perspective, it will never be a bad thing for more people to understand what it may be like to have a personality disorder.
For a bit of actionable advice on determining whether or not you may have one, though:
(1) Do your research. Obviously it's great that you're getting information from people with the disorders themselves by looking at PD communities; however, not everything having to do with the disorder will be talked about, and quite honestly, Tumblr is a terrible place to find definitive information on the PDs. Life experience? Yes. Actual information looking at how the disorders work and what they can entail in full? Ehhh, not quite. Look at a variety of academic sources, but in the same vein, keep your wits about you--professionals aren't immune to ableism, and may often perpetuate it with glee. Some of it may be obvious, some of it might not be.
(2) Keep an eye on your symptoms--make a manual check against the actual criteria every once in a while (but keep in mind that the DSM is also deeply flawed and biased); @shitborderlinesdo has a ton of checklists based on the DSM and individual testimony that can help. We first started questioning ASPD when we were 14, and we'd do those kinds of manual checks once every several months or once a year or so. It both helps you understand what your symptoms are, and helps you keep track of how you're doing over time. Don't use online quizzes for this; quite honestly, they're not really good for anything except validation if you know you'll get a high score.
(3) Look at stuff other than personality disorders, too, and try to figure out why your interest skews towards specific disorders. For a long ass time, we believed we had StPD and did our absolute best to ignore any information to the contrary, because (due to our symptoms) if it wasn't StPD, the only thing it could be otherwise was schizophrenia, and we were scared shitless of the idea; at first because we were scared of the idea that our symptoms might've been so severe, but eventually because we were afraid to admit that we were wrong. (As I've said before, no shame in being wrong--do as I say, not as I do.)
Ultimately, I can't stop you from doing anything, and I can't force you to do anything either. I'm just a mentally ill guy with an internet connection. My life experiences have led me to this conclusion, and others may disagree with it--that's perfectly fine. Again, I am not a professional. You know yourself and your experiences the best, and I think by this point, you have enough understanding of yourself and the world to be able to figure out what'll be best for you and your health, given that you have the proper resources to do so. You are a being with life experience, even if it's less than others may have; you aren't a rock, and you aren't a three year old who still hasn't realized that touching the lit stove will equal a burned finger. I personally think that the way a lot of folks go about talking to and about teenagers who think they may have personality disorders is, frankly, infantilizing and invalidating, and it just ends up with traumatized and unsupported teenagers turning into traumatized and unsupported adults, with the added bonus of an extra helping of imposter syndrome to top it all off.
I hope you're doing well anon, and I hope you see this (sorry for responding so late lmao). Off into the world ye may go, hopefully with a bit more knowledge and idea of what to do next than you had before.
35 notes
·
View notes
Note
(?) i keep self triggering nonstop i cant help it. i purposely search for nasty things related to my trauma just so i can feel bad. how do i stop it i cant stop i hate it
We have some information you might find helpful, because my friend you can stop harming yourself, you can heal. You are a person worthy of health and healing.
Triggering oneself is a form of self-harm it can help to look at it that way when breaking down what you are trying to get out of it on the level of dysregulation and seeking to deal with it on a somatic level as well as bringing judgment from the situation.
Coping Skills: Combating Self-Harm Urges
Self-harm urges can be so strong and are very hard to deal with, but we can work against them to better-coping skills.
Self-harm, self-mutilation or self-injury comes in multiple forms not just cutting that is normally discussed. Examples include compulsive masturbation, burning, hitting yourself against things, excessive scratching to the point of drawing blood, punching self or objects, infecting oneself, inserting objects into body openings, drinking something harmful and breaking bones purposefully.
These skills also work for self-triggering behaviours doing actions that cause yourself severe emotional distress like flashbacks or panic attacks.
Here is some advice to start finding safer coping skills:
The first step is to look at what is pushing you to self-harm.
Look at:
What things tend to happen before you do the behaviour? Are their common external triggers?
what emotional state are you in before you trigger yourself? For example are you angry, empty, keyed up, anxious? Do you feel like you need a realise? Are you experiencing intrusive thoughts?
What physical sensation are you experiencing beforehand? Are you holding tension anywhere particular? Are you in physical pain? Are you already experiencing body memories?
What emotions are you feeling afterwards? Do you feel less empty? After the panic subsides are you actually calmer?
What physical sensation do you have afterwards?
Okay, now you can look for replacement actions that can handle the feelings without triggering yourself.
knowing outside triggers can help you avoid them if possible, and prepare for them ahead of time if that’s not possible.
If you recognize the emotional state the persists the actions you can try and work on bringing yourself down from this state first. Learn about coping skills to handle this feeling. (Coping skill suggestions: Anger, anxiety/stress 1 and 2, intrusive thoughts)
If you are feeling specific body sensations beforehand look at ways to help that. For muscle stress this might help, heating pads or light stretching might help. If you have a headache ice pack might help. If you are already having body memories this or this might help.
Now sometimes the emotion you are getting after the triggering is just as important as the emotion that was before. Now here you can look for a replacement action that brings you a similar emotional feeling that isn’t as harmful. This post gives some examples of replacement skills for self-harm. If something you find is you are looking to break an emotional blank, or you feel more “real” afterwards I could suggest finding emotional things (music, movies, books) that can still bring strong emotions.
If you have physical sensations you are seeking again it is good to find a replacement action. Sensory aids might help info about that here.
Three important things to consider for long-term recovery
Deeper things are always at play. Underlying mental health conditions (Like BPD, PTSD or Depression) and trauma. Working through these problems, often a professional can be helpful reaching out to them is important.
Reaching out to friends and family can be really helpful in keeping yourself safe. Which is of the utmost importance.
If you find yourself harming yourself greatly please look at our crisis resources.
[WordPress Link]
Intrusive thoughts are often present here and dealing with them can combat the urges you have to self-harm as it can help mitigate the severity of the urges and thought spirals involved.
Coping Skills: Dealing with Intrusive Thoughts
Intrusive thoughts are unwanted thoughts that intrude into the thoughts process of those who deal with them. They are commonly associated with OCD, PTSD, eating disorders, addiction and self-harm.
Intrusive thoughts are not just thoughts that seem random or unskilled (that called thinking), and they aren’t always accompanied by the urge do something (compulsions). They can extremely distressing thoughts, violent, sexual or panic-inducing ideas and images are really common manifestations.
We dealing with intrusive thoughts an important first step is to understand while these thoughts are in your brain they don’t represent desires for the thoughts to happen or that it’s your real secret morality. It’s a function of what you are struggling with (mental illness, trauma and stress) not you being a bad person. Reminding yourself of that combats shame and paralyzation of feeling helpless to act.
next is letting them be. Intrusive thoughts happen, rumination, berating yourself for having them, or aggressively trying to push them away are all not helpful. Learning to just let them come into your brain and leave without a huge shift in behaviour and mood is important. Doing this robs them of their emotional power and lessens the pain. It’s okay to have them, It’s okay that they hurt you, letting these thoughts go is fine and healthy.
You don’t owe it all of your energy to trying to work them out, make thoughts stop happening, or repressing the emotions till it hurts more.
This just takes practice when experiencing them letting yourself know its just a thought, not real or something you must act on. When you feel the emotions and stress from the thought take a deep calm breath. Do your best to steady your emotional/physical response. When you can’t distract or not panic that’s fine, don’t get angry just try again next time.
Another important thing to remember is to not modify your whole life around intrusive thoughts. Avoidance is, of course, something people with PTSD and anxiety suffer with in general, but it’s key to start working your life around what you want and not avoiding intrusive thoughts. Starting with small things that might be ignored because of the thoughts not linked to large trauma, This is an important step to remove the power of the thoughts.
If your thoughts are often based on catastrophizing logic talk might actually help. Intrusive thoughts about say natural disasters thinking about how unlikely something is to happen so not number one priority might help, remind your self “it is valid to worry but maybe not so much right this second.”
Distraction isn’t always bad, many intrusive thoughts can be let go but patterns sometimes do need to be addressed. If you have trauma-based intrusive thoughts healing from trauma is often key to making them better.
Be Blessed all
~Admin 2
[WordPress link]
So if it’s online porn you could turn of safe-search and block the sites. This can combat the easy patterns we get stuck into. It can have a withdrawal effect and don’t hate yourself for slipping up. When you feel the need try and chose another act. Distracting yourself with things that require a lot of brain space is often a good step.
If you need some kind of stimulation you could try using written erotica that doesn’t have the same possible damage on the people involved in the production. Because of the biological aspects of addiction sometimes if you cut “cold turkey” as it were can push to worse behaviour.
Another tool for compulsive actions is to put it off, don’t judge yourself to just stop any and all behaviour but extend the time as long as you can combine with replacement behaviours.
Due to the nature of sexual trauma, it can be really useful to breakdown the relationship to sex and how that is affecting you. Doing so can help work through triggers. Coping Skills: Healing A Relationship With Sex After Sexual Abuse
Our Coping Skills Masterpost might be useful in finding ways that help you deal with your trauma symptoms over time and reduce the regulation you automatically fall into.
It’s important to disconnect from behaviours that harm you, and depending on what you are engaging with harm others. Participating in these don’t make you inherently a bad person, it just means you are in a place of struggle and need to work towards healing.
Be Blessed,
-Admin 2
18 notes
·
View notes
Text
BPD
Borderline Personality Disorder
Now getting into the lesser known disorders we start with Bpd A.K.A Borderline Personality Disorder.
Who gets BPD?
A personality disorder such as BPD will show up by late adolescence or early adulthood. It remains relatively stable throughout adult life, and can gradually improve with increasing age. This is in contrast to other mental health conditions, which come and go over time, with periods of illness interspersed with periods of wellness.
The risk of suicide in people who experience a personality disorder is significant.
It is important that if you are having any suicidal thoughts you seek help immediately.
People who have a diagnosis of BPD may develop other mental health conditions, particularly if stressed. These include eating disorders, social phobia, bipolar disease, post traumatic stress disorder, depression and drug and alcohol abuse. It is important for people with personality disorders to learn ways of coping with stress, and to seek help early should any of these other conditions arise.
It is most important to get diagnosis and treatment as early as possible. With the best possible treatment over a period of time there is evidence to show that people with BPD can improve considerably.
If you think you have a personality disorder, or you are worried about a loved one, it’s important to talk to your doctor or counselor, or someone else you can trust, as a first step to getting the important help you or they need.
What causes a personality disorder such as BPD? There has been considerable debate in the past regarding whether personality is determined by nature (genes) or nurture (upbringing). There is now good evidence that personality development occurs as a result of both genetic and upbringing influences.
People with a personality disorder often believe they developed it because things have gone wrong in their lives – it could be abandonment, sexual or physical abuse, traumatic experiences, being in an unhappy family/whānau, feeling alienated from people and society or not living up to people's expectations.
Other people with personality disorders cannot so easily identify things that have gone wrong in their lives. They may agree with the view that their disorder is genetic in origin. A lot of people with mental health problems believe it is a combination of these things. Sometimes people think their mental health problem is a punishment for their moral or spiritual failure.
It's important to remember that it is not your fault you experience a mental health problem.
Signs to look for (symptoms)
People with BPD experience some or all of the following:
Frantic efforts to avoid real or imagined abandonment A pattern of unstable and intense interpersonal relationships Impulsiveness (potentially self-damaging) Intense anger, that does not fit with the situation, or difficulty controlling anger Recurrent suicidal behavior or self-harm Ongoing feelings of emptiness Experiencing minor problems as major crises ‘Black and white’ thinking which often means switching between love and hate in personal relationships How the doctor determines if you have BPD (diagnosis) People with personality disorders such as BPD, in general, do not often seek out treatment until the disorder starts to significantly impact their life.
In addition, because people with BPD often experience other mental health conditions which may be very similar to symptoms of BPD, it can be difficult to diagnose.
Once you have spent some time talking to your GP, they will refer you to a mental health professional qualified to diagnose and treat people with this condition. A diagnosis of BPD is made after talking with you about what you have been experiencing, especially around your level of personal functioning and personality traits that may suggest a particular personality disorder. For this reason, it’s important the mental health professional gets a full picture of the difficulties you have had, both from you and your family/whānau or others who know you well.
To be diagnosed as having a personality disorder, your pattern of behavior will be causing you significant distress or difficulty in personal, social, and/or work situations.
Therapy, such as
Talking therapies These therapies involve a trained professional who uses clinically researched techniques to assess and help people to make positive changes in their lives. They may involve the use of specific therapies such as Dialectical Behavior Therapy (DBT), which has been found to be effective; and, cognitive behavioral therapy (CBT), which largely focuses on overcoming unhelpful beliefs and learning new strategies.
Counselling may include some techniques referred to above, but is mainly based on supportive listening, practical problem solving and information giving.
DBT and CBT approaches are the most effective, but must be continued over a significant period of time, often for a year or more.
Problem solving/skill training
This is often part of an overall approach, but can also be learnt in skills training groups. They aim to help you learn more effective ways of dealing with problem situations.
All types of therapy/counselling should be provided to you and your family/whānau in a manner that is respectful of you, and with which you feel comfortable and free to ask questions. It should be consistent with and incorporate your cultural beliefs and practices.
Medication
Medication is generally used for treating any other mental health condition that you may be experiencing, e.g. Depression. It may also be useful as a short-term strategy to help with coping in times of extreme stress or distress. If you are prescribed medication you are entitled to know:
The names of the medicines What symptoms they are supposed to treat How long it will be before they take effect How long you will have to take them for and what their side effects (short and long-term) are. If you are breast feeding no medication is entirely safe. Before making any decisions about taking medication at this time you should talk with your doctor about the potential benefits and problems.
Complementary therapies
The term complementary therapy is generally used to indicate therapies and treatments that differ from conventional western medicine and that may be used to complement and support it.
Certain complementary therapies may enhance your life and help you to maintain wellbeing. In general, mindfulness, hypnotherapy, yoga, exercise, relaxation, massage, mirimiri and aromatherapy have all been shown to have some effect in alleviating mental distress.
Physical health
It's really important to look after your physical well being. Make sure you get an annual checkup with your doctor. Being in good physical health will also help your mental health.
Other strategies to help yourself
Talk to your doctor about treatment options and stick with treatment Try to maintain a stable schedule of meals and sleep times Engage in mild activity or exercise to help reduce stress Set realistic goals for yourself Break up large tasks into small ones, set some priorities, and do what you can, as you can Try to spend time with other people and confide in a trusted friend or family member Tell others about events or situations that may trigger symptoms Expect your symptoms to improve gradually, not immediately Identify and seek out comforting situations, places, and people Continue to educate yourself about this disorder. Important strategies to support someone’s recovery Family, whānau and friends of someone with a personality disorder such as BPD have found the following strategies important and useful.
Remember that people with these conditions tend to easily take words and actions the wrong way. It’s important to be clear in what you say, and to be willing to clarify your meaning or intention if you get a bad reaction. It’s also important not to take these reactions personally, but see them as a result of the person misinterpreting you. Learn what you can about the condition, its treatment, and what you can do to assist the person. Take the opportunity, if possible, to contact a family or whānau support, advocacy group or culturally appropriate organizations. For many, this is one of the best ways to learn about how to support the person, deal with difficulties, and access services when needed. Encourage the person to continue treatment and avoid alcohol and drug abuse. Find ways of getting time out for yourself and feeling okay about this. It’s important to maintain your own wellbeing
1 note
·
View note
Note
I'd love to hear more of your thoughts on Ben having BPD
ok WHEW you just opened a fucking can of worms this about to be the longest post i’ve ever made i hope you have your seatbelt on
let me just preface this by saying nearly everything i talk abt in this post will be based off of my personal experiences w bpd. some people experience it differently, some people might not agree w some of the things i say, but i can only talk abt my own pov. therefore, this just my own personal opinions on ben having bpd. so yh lmao
and disclaimer!! i’m not a doctor!! don’t take anything i say in this post as diagnostic criteria! i’m not an expert or mental health professional!! when it comes to your own mental health or the mental health of ppl in your life, do not consider me a source to reference like ‘oh well lauren sunsetsover said xyz’ like pls just don’t do that. do your own research. and most importantly consult a doctor!!!!!! i am not one!!!!!!!!!
also there are very few sources in this post bc most of this is just shit i’ve absorbed over the years from doctors and doing my own research lmao
now that’s out of the way let’s go! (this became part character study, part informational masterpost on bpd. also it got really fuckin long, hence the read more, so be warned lmao)
warning for potentially triggering content (abuse/mentions of suicide and self harm - nothin too bad but i do touch on ben’s behaviour and history, and this is a p serious mental health issue we’re talking abt here so! take care of yourselves!!)
ok so! some things to keep in mind before we even get to ben:
i believe (at least in the uk) borderline personality disorder is considered to be an outdated name, and one that essentially isn’t appropriate or fit for purpose anymore, so in my experience, a lot of the time now it’s referred to as eupd (emotionally unstable personality disorder) in medical settings. which is way more apt name imo, and tells you more abt what bpd actually is (but i still call it bpd bc it’s easier and ppl know what that is lmao). so like. emotionally unstable personality disorder. i bet that conjures up a way more vivid idea in ur head than borderline personality disorder does.
no one 100% knows what causes bpd, though it’s thought to be a combination of genetic and environmental factors, like most things. but the general consensus is that bpd develops when something (usually traumatic, but not always in an extreme sense. ppl w bpd have often been victims of some type of abuse in their childhood, but that’s not necessarily always the case) happens in your childhood that impacts the development of your personality. kind of a bizarre metaphor but hopefully it will help u understand: u know how in finding nemo, the egg nemo was in got damaged by the shark? and even tho the damage looked minor, it actually meant that one of his fins was permanently damaged - it was malformed, it didn’t grow right, he couldn’t use it properly? well imagine the fin = the personality; that’s what happens to a person w bpd’s personality. smth happens to us in our childhood that permanently damages our personality, and so it doesn’t grow and develop properly as the rest of us does, making it less functional than an average person’s. u can imagine how that can lead to all sorts of problem (we’ll get to them later)
but bc it’s a mental disorder that affects the personality, you can’t be diagnosed w bpd until you’re 18, when your personality is basically developed fully (i believe it can be diagnosed slightly younger, but those are rare and extreme cases). however, symptoms can start to present themselves earlier, as ur personality begins to develop and mature. (mine started presenting in my early teens)
bpd doesn’t really go away, and treatment with medication generally isn’t effective for long periods of time. however symptoms can be treated with continued therapy, and symptoms sometimes can start to ease as you get older!!
bpd also gets misdiagnosed a lot bc a lot of the symptoms are similar to that of other mental health problems. the biggest one it gets misdiagnosed as seems to be bipolar disorder, which i get tbh. i’ve always considered bpd very similar to bipolar, just like… quicker cycles. there are even memes about it. also bpd has a tendency to coexist w other mental health issues, which makes it harder to recognise and diagnose.
so now lets look at this from a diagnostic perspective
in order to be diagnosed w bpd you basically have to deemed, by a medical professional, to be meet certain criteria, and to have been meeting these certain criteria for a significant amount of time. there are some variations to this criteria, and proposed subtypes and basically different flavours of borderlines but i’m not even gonna go there. i’m just gonna talk abt what i’m most familiar w and how i think that applies to ben.
i’m copying and pasting the diagnostic criteria part from here bc as far as i’m aware this is the criteria doctors use for diagnosis. there are 9 different ‘indicators’/’criteria’, and you have to display or meet at least 5 of them in order to be considered for a bpd diagnosis:
1. Frantic efforts to avoid real or imagined abandonment
this is one of, if not the biggest part of bpd. that trauma i mentioned earlier? often stems from or is related to abandonment, or perceived abandonment, in childhood, be it physical or emotional. for example, a child that’s being abused by one parent might feel abandoned by the other parent if they don’t do anything about it, even if the second parent has no idea the abuse is going on. sound familiar? a similar thing happened to ben, with stella. phil not doing anything about the abuse ben was facing at the hands of stella - even though he didn’t know it was happening, even though phil did do something once he found out - was an abandonment to ben. and that’s just the tip of the abandonment iceberg for ben - kathy faking her death and leaving him was an abandonment (even when he thought she was actually dead), phil’s own abuse was an abandonment, as was his reaction when ben came out, and so on. and abandonment like that skews your thinking so you believe that everyone is going to abandon you, sooner or later, that they must be abandoning you for a reason, you must be a terrible person, you must be unworthy of people’s effort/time/love etc etc.
even when paul died, that was an abandonment to ben! like logically we know - and ben probably knows too - that paul didn’t want to die, he didn’t want to leave ben, he didn’t deliberately leave ben. but that doesn’t matter. mental illness is illogical, bpd is illogical, esp when it comes to abandonment. e.g. my therapist had to cancel a few of our appointments once bc she was ill, and it felt like an abandonment. like it was personal somehow, like she wasn’t coming into work bc of me, bc i was too much work, too hard to handle. ofc that wasn’t true, but that’s how it felt. it’s illogical. so ofc my solution was to just not go to my appointments even when she came back, bc like what other response is there lmao. it’s just that everything a person does feels personal, like it’s because of/about you, even when it isn’t. even when it has nothing to do w you. that’s probably why ben can come across at selfish at times, like he’s making everything about him. because it is all about him, in his mind. everything is because of him, is his doing, his fault etc. his way of thinking is skewed into thinking like that, bc shit keeps happening to him and ppl keep leaving him, so it must be his fault.
and!! ‘frantic efforts’ isn’t necessarily what u think it is!! it can be desperate begging ‘i’ll do anything to keep you in my life’ type actions, but it just as equally can be lashing out and abandoning someone in order to prevent them from abandoning u first - a ‘get them before they get me’ mentality (the whole scene where phil was in the hospital comes to mind - the ‘why doesn’t he love me back?’ was the more desperate part of him, tho it wasn’t necessarily an ‘effort’ per se, but then him trying to kill his dad basically in order to have the abandonment be at least on his own terms? that’s lashing out, and def qualifies as a ‘frantic effort’ lmao). and how often do we see that in ben? lashing out at jay in the hospital because he knew he was mad at him, and he’d rather hurt jay physically before he could hurt him emotionally? ben trying to support callum and showing him kindness, only to turn around and threaten to out him when he finds out callum asked stuart to sort him out? everything that happened w his dad, trying to fuck him over before his dad can get there first, trying to get rid of keanu so he can’t be abandoned in favour of him (although that didn’t really work, but it rarely does work the way u want it to lmao). and the biggest one to me, though probably one that people have already forgotten, is him breaking up w that guy he was seeing in newcastle even tho they were into each other bc he ‘had to, otherwise [he] would have ruined his life’. even tho we don’t really get details, that says it all to me. it’s v much a pattern that’s present in ben.
2. A pattern of unstable and intense interpersonal relationships characterized by extremes between idealization and devaluation (also known as “splitting”)
i feel like this one doesn’t need much explaining lmao
here is a definition of splitting from here (which is a very good article on splitting imo if u wanna read more abt it): ‘Splitting is a term used in psychiatry to describe the inability to hold opposing thoughts, feelings, or beliefs. Some might say that a person who splits sees the world in terms of black or white, all or nothing. It’s a distorted way of thinking in which the positive or negative attributes of a person or event are neither weighed nor cohesive.’
a little explanation of it from me: ppl w bpd can sometimes have very simplistic, all or nothing views on things. and splitting is basically when ur opinion on something or someone changes very quickly (sometimes instantly), often to an extreme (e.g. going from loving and idolizing someone, to absolutely fucking hating them, or from having a neutral opinion on something to suddenly becoming extremely angry abt it) sometimes without even having an identifiable trigger. it links into black and white thinking, which u may have heard of before - u either love someone and they can do no wrong, or u hate them and they disgust you. either something is amazing or it’s terrible. there is no grey area, no in between. it goes back into the whole ‘not being able to regulate ur emotions properly’ thing lmao there’s rarely nuances to our emotions or feelings, we’re all or nothing a lot of the time. so splitting is when ur opinion rapidly changes to one of these extremes. sometimes u can even go back and forth, splitting over and over on the same person/thing which is super fun.
ben splits on his dad all the time. all the fucking time. he doesn’t care about phil at all and wants to ruin him, then he wants phil’s approval and to be welcomed back into the family fold and the business. then ben hates him and wants him dead, then 5 minutes later he wants his love, wants to be a good son again. that’s splitting. u can also see it w jay, too, but no where near as extreme as w his dad. and i’ve seen it a couple of times w callum too, but again, it’s way more subtle. u probably wouldn’t notice it if u weren’t looking for it, whereas w phil it’s obvious.
but like i don’t need to explain ‘unstable and intense interpersonal relationships’, do i? just look at the relationships w phil, w jay, w lola, w callum, even w paul - they were unstable back when they first got together, and were arguably kind of intense too. (he settled a bit w paul, but his death/perceived abandonment fucked him up a lot beyond the expected ways). he’s always arguing w the ppl he loves. he tried to get poor billy killed, and yet since then he’s had no problem w him!! none of his relationships - apart from maybe his mum and ian (i don’t include lexi bc she’s a child) - are stable. and i would definitely describe his relationships as intense lmao
3. Identity disturbance: Markedly or persistently unstable self-image or sense of self
u can see this most - as most things - in his relationship w his dad. he fluctuates between seeming to know his worth (and demanding other people know it too), knowing he deserves his dad’s love and approval (why else would he be so mad abt the fact hes not getting it, if not bc he knows he’s worthy of it? if he didn’t think so, he wouldn’t be so angry abt not getting it - he’d be accepting/understanding, wouldn’t he?) and being desperate to do anything to get his dad’s love/approval, even things that are below him, turning into a child, begging to know why his dad doesn’t love him, why he’s never been enough. that scene where phil had found out abt ben trying to frame keanu and leaving him for dead is the epitome of this. u can see ben fluctuate between a hurt, traumatized little boy, begging his dad for some answers, some explanation as to why he’s not enough, begging him not to start drinking again, and a man who is angry, angry at his dad, angry at himself for crumbling like this, bc he should be stronger than this. u see him change multiple times in that one single scene. go watch it again. you’ll see it too.
some more examples: his absolute certainty that he is better and more qualified than the likes of shirley and keanu for working with his dad, and then being like ‘my dad was right, i’m good for no one’ - they don’t line up. does he have self esteem and know his worth or not? also his entire relationship w callum is an example of this - all those changes in his attitude towards cal and their situation? he often treats callum like they’re equals who understand each other, yet sometimes it seems like he thinks he’s superior to callum (e.g. the scene outside the cafe), and others he behaves (keyword) as though he thinks he’s not good enough for callum (why else would he just take all that shit from whitney and not say anything in retaliation? why, if not because he deems it more important that callum has an easier time of it than he does; that he regards cal’s comfort more important than his own? and why would he do that, if he held himself in such high regards? i mean he certainly acts like it sometimes, so why not then?)
also like……. who is ben? is he the bastard who cares about no one but himself, who’s always causing trouble not only for himself but for the people he cares about? is he the guy who just completely folds when people he knows hurtle abuse at him, accepting it lying down, who thinks he’s no good for anyone? the guy who goes out all night and drinks himself silly and purposefully gets himself into fights? the guy who shows callum so much empathy even tho it brings him nothing but pain, who loves jay unconditionally, who tried so hard to help bobby when he came back from prison? which one is he? which one does he want to be? does he even know?
(and you could argue that people are just multi-dimensional, but there’s just such a vast gap between these different facets of ben’s character and he can flip through them so fast it’s jarring, which is why i think it’s more like he straight up doesn’t have a consistent sense of self. which is a big part of bpd)
4. Impulsive behavior in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating)
again, does this need explaining?
doing illegal shit, excessively drinking, becoming unnecessarily violent, fucking up his relationships, just generally doing reckless things regardless of the consequences - this has always been a part of ben’s character.
(his constant hook ups could be another one, but the jury’s still out on that one. if anything it’s less the sex that worries me and more the flippant attitude he has when meeting up w ppl - they could be anyone and do all sorts, at the end of the day)
it became most obvious recently around the anniversary of paul’s death - drinking himself sick, gambling all his money away, deliberately starting fights. but even before that and since then it’s been there.
it’s basically just a way to self sabotage.
i feel like this one isn’t a consistent part of ben’s behaviour like the others are, but it is undeniably there, so.
5. Recurrent suicidal behavior, gestures, or threats, or self-harming behavior
although ben (to my knowledge) hasn’t displayed any suicidal behaviour, he has at times spoken in ways that could kind of sway that way. (i’m no good for anyone, i’m not worth it, why do you care etc)
also self harming!!! just because he doesn’t hurt himself in a direct way doesn’t mean he doesn’t deliberately put himself in situations where he’ll get hurt, and that is self harm!! letting stuart beat him at pride was self harm!! picking that fight w those homophobes at e20 was self harm!!! drinking to excess is a form of self harm!!! putting himself in harm’s way, even if he doesn’t get hurt, is self harm!!!! just bc he might not be self harming in the traditional sense doesn’t mean he’s not hurting himself!!! this one has been on my mind for so long!!!! oh my god!!!!! he absolutely has a pattern of self harming/self destructive behaviours, and just a general disregard for his own safety and well being!!!! the fact that it doesn’t worry more ppl in his life is so upsetting to me!!!!!!
6. Emotional instability in reaction to day-to-day events (e.g., intense episodic sadness, irritability, or anxiety usually lasting a few hours and only rarely more than a few days)
aka the biggest part of bpd: pt 2
i feel like this definition doesn’t really do justice to this aspect of bpd. this is basically you literally having no control of your emotions. ‘day-to-day events’ have fuck all to do with it half the time. u could be sitting there minding ur business and all of a sudden you wanna smash up the entire room, for seemingly no reason. one time i was crying - like uncontrollably sobbing, a complete mess - and had been for maybe half an hour? and then all of a sudden, literally mid sob, it stopped. like it just stopped. i was done, i wasn’t sad anymore. i went from inconsolably crying to perfectly fine in a split second. can you even imagine that? it’s fucking crazy. that’s what having bpd is like. it’s like mood swings x1000 (that’s why i describe it like bipolar on a smaller scale - their mood swings last days/weeks/months, ours last minutes/hours, sometimes days but not often). you can be fine, then all of a sudden you’re not. or you can be not fine, and then all of a sudden you are. you can be ecstatic, then all of a sudden all the joy gets sucked out of ur body n u wanna die. then 5 mins later ur fine again. u can cycle thru every single human emotion in the space of a few hours with no warning whatsoever. u can go from feeling so many emotions u don’t know which one to focus on to feeling none at all. it’s exhausting. so yes ‘day-to-day events’ (this can be as minor as the way someone speaks to you, or not enjoying ur food as much as u thought u would, and it can make u terrifyingly sad or spark uncontrollable rage in u) can trigger it, but it’s like… at least that’s kind of justifiable. most of the time u just cannot regulate, control or predict ur emotions whatsoever. and often the emotions u do feel are not appropriate for the situation at hand lmao
on top of that, ppl w bpd have massive problems processing their emotions. while most ppl have the capacity to identify what they’re feeling and why, ppl w bpd often can’t. and bc they can’t identify it properly, they don’t know how to process it. that’s why emotions and feelings are so often black and white - we might develop the ability to recognise Big Emotions, like love and hate, happiness and sadness etc, but we can’t figure out the smaller, nuanced emotions. it becomes or, not and.
this is also why our emotions feel so big and all encompassing!! we can’t ignore our emotions!! they are our focus in a lot of ways. when ur sad, it feels like the world is ending, every single time. when ur happy, ur euphoric and nothing else matters, and so on. every emotion has the volume turned up to 100. that’s why our emotions sometimes come out in extreme or unhealthy ways - our emotions often feel so big we have such a hard time handling them. so we go to drastic lengths, whatever they may be, to cope.
(also bc most ppl w bpd are victims of abuse, we’re often hyperaware of other people’s moods, which can impact ours. someone can be annoyed for some innocuous, innocent reason, and yet bc we can sense it, we become scared or defensive and may lash out.)
and ben… little old ben, have u ever seen him have a rational reaction to anything in his life? how often have we seen him have an appropriate response to smth? my dad is shit, so i have to destroy him. failing that, i have to kill him. oh, my brother isn’t gonna let kill him? time to punch him in the face. my daughter ate all my cereal? it’s Overreaction Time. (this one in particular is Very Me like yes lexi is a child and he was unfair but my 7 year old cousin once drank all my j2os and i almost had a breakdown so i Get It) i’m feeling like shit? time to antagonise these homophobes until they beat me in the middle of the street. i sleep with this man once? time to get overly involved. he shows me a little bit of love and kindness? time to develop feelings for him despite him insisting he’s straight, the fact that he’s with a woman and i have been harassed and beaten by his homophobic family multiple times. but it isn’t going the way i wanted it to? time to impulsively hit him for not knowing what he wants, then immediately regret it.
and like. he went from crying his eyes out in his dad’s kitchen to threatening kat slater within the span of what, 10 minutes? he went from trying to kill his dad, to falling tf apart w jay, to trying to manipulate his dad - who had just woken up from a coma - for his own gain again, in the span of maybe an hour. if that doesn’t say rapid cycling, inconsistent emotions idk what does.
like idk enough about the old bens to say if this is a consistent characteristic of his or not (although based on the fact he killed a woman bc he was angry w his dad, i’d say it’s fairly safe to assume lmao) but ever since he came back his reactions and emotions have been pretty much never once been rational, stable or consistent.
(and like i wanna say i am saying all of this from the perspective of the bad days. so if you’re thinking ‘well, ben isn’t like that all the time’ ur right. neither am i. some days i’m fine, some days it’s not that bad, sometimes i can cope. but i still have bpd, even on those days. and imo, so does ben.)
7. Chronic feelings of emptiness
this is one i don’t really see in ben. we maybe see moments of emptiness, but certainly not enough to call it ‘chronic’.
also a lot of the moments we do see emptiness in ben, i feel like it’s forced emptiness, more for his own benefit or for the benefit of others rather than actual genuine emptiness. it’s not that he’s not feeling anything, it’s that what he is feeling he’s not showing. that’s very different from actually feeling empty.
8. Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights)
this! is! such! a! massive! part! of! having! bpd! and it’s a part that no one ever fucking talks about either!!!
and again, does this one need explaining?
ben is anger. he’s a ball of it, and he has been for a very, very long time. he’s angry at his dad, at the world, at himself. for all sorts of reasons, both complex and simple. if i sat here and tried to get into all of it this post would be twice as long as it already is. and i don’t think i really need to, anyway. it’s not as if any of us need to dig very deep to see it, is it?
‘frequent displays of temper, constant anger, recurrent physical fights’ like i really don’t need to elaborate do i? bc what does ben do when he’s angry? his temper flairs up, he gets physical, lashes out, makes threats.
and he’s so often angry in response to emotional pain, which is the saddest (and for me, most relatable) part. just look at paul’s anniversary, how angry he was just in general, to everyone - even his mum, who is like the only exception to his anger since he’s been back - when he was just hurting and sad. how angry he got when he found out keanu had replaced him in phil’s will, when really he was just hurt. he gets angry and violent so people don’t see him as weak bc he’s hurting. he has been conditioned to get angry instead of getting sad. it’s not healthy at all.
there is so much more but i feel like it’s unnecessary for me to get into it. bc u know. ben’s not exactly subtle in his anger is he lmao
9. Transient, stress-related paranoid ideation or severe dissociative symptoms
this is the only other one that i don’t see in ben at all, and it’s one that i don’t really experience myself either so i don’t even have any insight to offer lmao
so!! more or less 7/9!! that’s a passing grade for diagnosis!!! welcome to the club, mr mitchell!!!!
all of this, of course, has been purely from a medical, diagnostic standpoint (w some of my personal experiences sprinkled in lmao). there’s so much more to say from like a ‘living w bpd day to day’ standpoint but like, this post is already way too fuckin long so i’m just gonna hit on a few that i feel are important in regards to ben, and ones i have’t spoken abt yet
most ppl w bpd have a ‘fp’ or ‘favourite person’ (tho it can be multiple people), which sounds nice but it’s kind of a really complicated and difficult thing tbqh. here’s the best definition i could find: ‘When someone with BPD uses the term “favorite person” to describe someone else, they are typically insinuating that this is a person they cannot survive without. For BPD sufferers, the favorite person is the person who is a source of emotional support and dependence. This individual has the ability to truly impact the BPD sufferer’s day in either a positive or negative manner. The favorite person to someone with BPD holds a critical role in their lives by holding the power to ‘make or break’ the successful navigation of daily tasks and struggles.’ it’s a difficult thing to explain/understand (so please feel free to google ‘favourite person bpd’ to get a better understanding), and is not always as dramatic as it sounds, but it’s like… even if they aren’t a source of ‘emotion support’, ur mental wellbeing can hang on this person’s every move. (which is not healthy, i know, but it’s just a thing that happens w bpd!) and phil is absolutely ben’s fp. ben hates phil, and yet is still so desperate to be in his good graces, in his life no matter what that costs him… and ben’s self esteem, his actions, his moods are so dependant on phil. it just?? makes so much sense to me. i realize it may not make much sense to someone who doesn’t have any understanding of what a fp is, but like if u do, i’m sure u see what i see.
i think maybe jay was another fp of ben for a while in the past. i don’t think he is as much since ben has come back, but in the past?? maybe. like less in the ‘my happiness is dependant on u’ way and more in like a ‘i’m very very attached to u and need u in my life and would maybe go crazy if anything or anyone got in the way of that’ way.
and i think callum might be sneaking into territory now too tbqh. it would explain why callum’s actions and words have such an impact on ben’s moods despite not much really happening between them. and like i wanna say: someone becoming ur fp is not a choice. it just happens. it’s not like ben is going ‘oh im going to get overly attached to u just for a laugh’, no. this would be completely out of his control. and when it happens, it fucking SUCKS. so if that is what’s happening, it’s going to have a massive impact on ben - and it seems like it already is.
and like taking the whole fp thing out of it (bc i know it’s complicated and hard to grasp) bpd would explain why ben seems to be so attached to callum even tho very little has actually happened between them!!! like bpd will have u falling in love w someone who just shows you basic human kindness and decency, and i mean that very literally!!! bc like i said when you have bpd, you struggle to navigate and handle basic emotions, so all the nuances of romance and love? jesus christ. it goes back into black and white thinking - i either love this person or i hate this person, there is no in between. so callum, showing ben kindness? showing him support with what’s going on w louise and what happened w phil? not hating him and thinking he’s despicable and evil and all those things people say about him? and ben, having bpd? he probably wouldn’t be able to comprehend that maybe cal’s just being friendly, esp not after they slept together. so ofc he would latch tf on to that. i would latch tf on to that. his behaviour towards callum just seems very on brand for having bpd to me, genuinely.
and !! all those things whitney said the other night !! people complained about him not arguing back, but like… she’s almost saying what ben wants to hear, when it comes to callum. bc i touched on it before but like the thing is when, you have bpd ur thought process is like ‘i care about this person, they are good, i don’t deserve them, i am bad, i am going to ruin them, i’m probably manipulating them into spending time with me and caring about me, but i can’t let them go, i need them, i bet they don’t even like me, i don’t deserve them, i don’t want them to get hurt, i don’t want to hurt them, i am going to hurt them, in the end.’ (and eventually it spirals into ‘actually they’re probably going to hurt me first bc everyone always does so let me completely destroy this relationship so it’s unrecoverable and hurt them now so they can’t hurt me later’ but that’s another story) and whitney more or less confirms that for him!!! in essence, what she says to him is ‘you’re bad, he didn’t want anything to do with you but you manipulated him into it. you don’t deserve him, you’ve hurt him, you’ve hurt me, how could you do this?’ so like… ofc he’s not gonna argue w her. he’s already had a shit day, all of the fight is gone from him, and he agrees w her!! i’m sure he was thinking that he deserved what whit was throwing at him - not necessarily for what he’d done to her, but because he is Bad and callum is Good and he needs to stay away from him, otherwise he’ll ruin him. bc that’s just what bpd brain tells u, even when u’ve got no basis to believe it. (unless ur splitting or experiencing a big emotional high, but again, that’s a different story)
and that kind of makes sense as to why he’d go to the wedding. going back to the anger instead of sadness thing - he’s hurting, so he’s going to get angry and vengeful. he has been hurt, so now he is going to hurt in return. esp considering both callum and whitney have seen him in such a vulnerable state. it’s probably a pride thing, too.
also just to expand a little more on the ‘unstable sense of self’ thing - ppl w bpd (and also victims of abuse, but sometimes that particular venn diagram is a circle) tend to change the personality based on who they’re with. which is what most people do, yes, but i mean the Extreme version. it’s a trauma response thing - u’ll reflect parts of a person’s personality back at them, or even take bits from personalities of ppl u know they like in the hopes that they’ll like u more like that, as opposed to ur real personality (if u even know what that is). and sometimes those parts stick (esp when you idolize the person u stole them from/they’re your fp), and it’s like u all of a sudden realize ur entire personality is built of parts of other ppls personalities that you’ve stolen. so it makes sense to me that ben seems to have so many differing personalities/sides to his personality, bc he’s learned which parts to show to who, and in what situations - in response to his abuse as a kid, if nothing else.
(and before anyone can even go there: that is not an act of manipulation. it’s a trauma response. it’s something that happens without us consciously having any say in it, as a way of self-preservation. it’s like if i make myself likeable and appealing to u, you’re less likely to hurt me, physically or emotionally. and yes ben has a habit of manipulation, but this is not a part of it. none of ben’s manipulation is directly bc of his hypothetical bpd, it’s bc that’s just who he is. i don’t ever want to see the two equated, or see anyone say any shit like ‘ben must have bpd bc he’s manipulative’, ever.)
just for the hell of it, here are some spicy bpd memes, bc that’s how we communicate on the internet. (here are two in particular seem quite relevant to ben rn lmao + bonus one for phil!!)
so! there we are!!! i’m sure there’s some important stuff i overlooked and that this is not what u expected when u sent me this question, but there are so many misconceptions and stigmas out there surrounding bpd that i wouldn’t have felt right half assing it. and i hope, if nothing else, u learned something abt bpd that u didn’t know before :-)
if u read this far ur a trooper lmao but if anyone has any questions, be they abt ben having bpd or bpd in general please feel free to ask!! i’ll do my best to answer them to the best of my ability 💖💖
#ben mitchell#ballum#eastenders#petty as hell but it was really bugging me that this wasnt showing up in tags so i'm posting it again lmao#sorry if u already liked/replied to it :-(#bpd#anon#question
25 notes
·
View notes
Text
Mental Health Awareness Week: My Story
Hi to anyone who’s reading this!
My name is Lauren and this is my first personal post on my Tumblr (which I’m using because I am a granny who can’t be arsed to work out the basics of Wordpress). My intention in making this blog was ultimately to talk about mental health and fashion and things that interest me and I suppose I knew that ultimately I was going to make a post like this but I just didn’t realise it would be so soon. But then Theresa May lit up Downing Street and it was Mental Health Awareness week and Borderline Personality Disorder Awareness month and I realised, best to just get this out of the way before I can start making excuses to put it off until the end of time. It’s a hard post to make because I don’t exactly know who the audience will be; I’m writing it for the mental health community and anybody who’s interested in what Borderline Personality Disorder is/looks like but I’m also conscious of the fact that one day my family and friends and even potential employers could be reading this. How much detail am I supposed to go into? A lot of people still feel uncomfortable discussing topics like this; they start seeing you a different way when they know you suffer from a mental illness, even though you’re the same person you’ve always been. It’s also hard to know where to start when I’m talking about my mental health. I feel like other posts of a similar nature tend to have a clear start, beginning, and end. A clear cause or inciting incident, one self-explanatory, well-understood diagnosis, and a clear pathway to recovery. I don’t have a single, defining trauma I can pinpoint anything to, and I don’t think I have complex PTSD (which is often conflated with BPD but as I understand it, not always the same thing). I have a family history of mental illness and a series of less significant events that in hindsight might have affected me more than I originally thought, but until I became able to think about concepts such as “mental health” and self-image and relationships in the abstract, I believed that I generally had a pretty happy childhood. My family did their very best and they loved me and we always had a roof over our heads and food on our plates. When I did start to conceptualise my mental health, I kind of thought of it as a wave of depression and insecurities and anxieties that hit me when I was in my early teens. I think this is the same for a lot of people. Only when I got a diagnosis of Borderline Personality Disorder (which I will shorten to BPD for the purpose of making this easier to read, lol!) in October 2018 did I question that.
I’ve done a lot of questioning since I got the diagnosis, the same kind of questions that make this post hard to write. Am I really that ill? Am I not just being dramatic? Do I have any right to feel like this given the privilege I have? When in reality, this deep-rooted gut instinct to doubt who you are and what you have a right to feel is an intrinsic part of BPD.
There are 9 key symptoms involved in the disorder, 5 of which must be experienced to a degree that is severe enough to affect your day to day functioning in order to receive a diagnosis. My formal assessment which took place during my stay at an inpatient psychiatric ward in October 2018 revealed I was just on the cusp of receiving a diagnosis; in 5 of the 9 categories I scored highly enough that the symptom was impairing my ability to function, thus I only just qualified (lucky me!). That’s what mental illness is really, a collection of ingrained and/or inherited behaviours that are inhibiting one’s day to day life. With regards to BPD, these 9 behaviours or symptoms are as follows:
1. Fear of abandonment (check).
2. Unstable relationships.
3. Unclear or shifting self-image (check).
4. Impulsive, self-destructive behaviours (check).
5. Self-harm (check).
6. Extreme emotional swings (check).
7. Explosive anger.
8. Dissociative experiences (check).
9. Chronic feelings of emptiness (check, check, CHECK).
See, when the diagnosis was first suggested to me informally by a community mental health nurse in June of 2018, I was a bit like…what?! That can’t be me! I don’t have outbursts (it’s okay if you do and you’re working on it)! I don’t scream and throw things (again, okay if you do and are working on it)! And I’m definitely not manipulative (any person can be manipulative so I don’t even know where this one comes from)! That was, like, all I knew about BPD. Stereotypes. Think Glenn Close in Fatal Attraction type bullshit, we’re talking the woman that coined the phrase bunny boiler. I didn’t know that BPD can present in a million different ways, based on the person who’s suffering with it, because I thought BPD was the person. The widespread consensus on BPD isn’t the most humanising. So I hope me explaining how it’s affected my life and the way its presented itself over the years helps in turning the tide, which so many amazing people have already begun to do by sharing their stories. My aim is to do the same.
I’ve had a lot of time to think about the areas in which BPD has affected my life since my formal assessment, in which I felt I learnt a lot more about the disorder. In particular, the idea that I was always this happy child that got hit by a wave of inexplicable, crippling depression once I hit my teenage years. I remember during the assessment, the doctor asking me to talk about my early relationships and it kind of struck me at that moment that I’d been going through this pattern of switching between extreme attachment towards versus extreme devaluation of my relationships with the closest people in my life for as long as I could remember. My first real best friend of several years basically stopped speaking to me (and in hindsight, I do not blame her, lmao!) when we were about 12 because I can only imagine she was sick of me either picking a fight or desperately seeking her reassurance every time she dared to hang out with another friend. I remembered how it felt when she did choose to spend time with somebody else rather than me: “oh my god, she likes them more, she finds me boring, she hates me and she doesn’t want to be friends with me anymore! Everything’s over! I’ll never find anyone who loves me like she does because why would they? I can’t go on with my life until I know that she isn’t going to leave me!”. I think at that age, everyone has that shrill inner voice that doesn’t exactly consider logic or react in the most sensible way, but instead of my shrill inner voice going away, it just faded to more of a constantly niggling monotone that continued to affect the way I behaved around other people for years to come. This was just one of the signs that things weren’t as they should be from an early age. I think I was around 13 when the Child Adolescent Mental Health Services (otherwise known as the dreaded CAMHS), whom my parents had initially got me referred to for sleeping problems, diagnosed me with generalised anxiety and social phobia. Social phobia, despite this being its DSM name, is more commonly known as social anxiety. This came about after I had undergone successful CBT for said sleeping problems and thought I’d just drop it in, as you do, that basically, every social interaction felt like I was putting on a desperate show to keep the few remaining people left in the theatre from walking out. I told them that school was emotionally exhausting me. Whilst after the first couple of rocky years of transitioning from primary to secondary school I had developed a close group of friends, I still felt like aside from the closet few of them, absolutely nobody liked me. That was definitely true of some people, but likely not to the extent I envisioned it. I had come to feel, I suspect due to a combination of genes and a few environmental factors, like I was inherently unloveable and annoying, and even though I’m in a good place right now, these are things I continue to struggle with. When you’ve believed these things for so long, to act according to them is second nature.
The thing about BPD is that it’s hard to determine what is a co-morbidity and what is part of The Disorder™. I’m still not quite sure whether my social anxiety was in and of its own issue or if it was driven by the borderline symptom of fearing abandonment. Even recently, during a period of relative stability, I went back to my GP about dysmorphic thoughts concerning my body and appearance as I believe they go beyond the threshold of what is to be expected as part the unstable self-image facet of BPD. Whilst I can accept, for example, that the self-harming and binge eating I began indulging in around the same time I received my anxiety diagnoses were my way of coping with the mood swings and chronic feelings of emptiness I was also experiencing (get me working in the checklist of symptoms here, I imagine this is how film writers feel when they namedrop the movie in the characters’ dialogue), I have a feeling the image issues I have would exist regardless of the influence of the unstable self-image part of BPD. I mean, would perfectionism alone take me to the extremes of punishing myself for missing out on all A*s by an A or two at GCSE and A-level, forcing myself to do a degree I had no particular interest in just because the university was in the single digits in the international league tables, or at one point eating only apples for 10 days until I could barely stand up because I wanted to look like those girls on 2013 emo black and white Tumblr? Probably not. But you don’t need to have an unstable self-image to latch onto the idea that only the very best will do in today’s world, lol (typed with a totally straight face)! Yeah, if the niche that is socialist twitter has taught me anything it’s that, that’s like, late-stage capitalism for you. It’s hard to look at myself and know what is a good quality, or just a character trait, and what is disordered. I think when you call a mental illness a personality disorder, the people who are labelled with it are inevitably going to have that problem.
Surprising absolutely no-one, trying to fit into these ideals I had created and emotionally detaching myself from my friends and family didn’t do any good for my wellbeing. I gave into self-destructive impulses with increased frequency and as I went into sixth form and drifted even further away from the few people I did feel close to, I began to experience derealisation (not depersonalisation, though this is something a lot of people with BPD do experience). This would come under the dissociative experiences symptom of the BPD. It was like my eyes were glass windows and I was just watching life unfold in front of me from the other side. It’s not as if I didn’t have control of my actions, I did, I threw myself into revision, but it all just felt slightly unreal, like I was going through the motions, almost robotically, detached from everyone around me. Everything was muted. Generally, I find that my mood swings between 5 different states: lethargic depression, extreme distress, anxious irritability, an almost mania like sense of confidence and purpose, and a more pleasant calmness. The best way to explain how I experience this switch is that I can almost physically feel the gear of my brain shift, with this change of energy then flowing down to the rest of my body. My thoughts take on a different tone of voice, my body feels heavier, or if I’m going up, it’s like I can feel electricity running and crackling through me. It can happen in a split second, and it can be random, though often it’s triggered by something as small as a phone call or how much I’ve eaten. If multiple plans fall apart at the same time, it can be enough to make me angry at the world and distrustful of everyone in my life, closed off and weighed down. However, back when I was experiencing this derealisation, I remember only really switching back and forth between feeling numb and feeling passively suicidal; I feel like I lost my teenage years to this big, grey cloud of meh-ness that fogged up my brain and obfuscated my ability to regularly feel any positive emotion. To use a cliche, there was this void inside of me that nothing would fill and I had learnt that trying to use relationships to do this was dangerous for me because without sounding melodramatic, it hurt too much when I felt they weren’t reciprocating my love (what a John Green line, lmao).
My fear that people didn’t like me morphed into paranoia that even the people I was supposed to be friends with were ridiculing me the second I left the room; please don’t laugh when I say my greatest pleasure during this time was to go home at lunchtime to avoid having to spend an hour sat with them so I could eat Dairy Milk Oreo, nap and listen to The Neighbourhood (careful, don’t cut yourself on that edge!). I put on a lot of weight due to binge eating, would often leave sixth form early or skip it altogether, and saw my GP, who reestablished my anxiety diagnoses now with an exotic side order of depression. When it comes to NHS services where I live, I’ve kind of won the postcode lottery. There’s a large, conservative elderly population which I’m assuming is the reason our area receives a lot more funding than other, debatably more deserving other areas, and this meant that along with prescribing me the first of many SSRIs I was to try, I was also referred back to CAMHS. I’d been discharged from them about 2 years prior, and what had back then been about a 1 or 2-month waiting list to be seen had doubled in longevity since. I say I won the postcode lottery because, in a lot of places, it’s not uncommon for people to still be waiting to be seen by their local mental health team over a year after they’re first referred. Even so, the help I was offered was very minimal; I met a counsellor once every couple of months that didn’t really specialise in any particular kind of therapy and would kind of just talk at me for the hour I saw her. This was in spite of me expressing suicidal feelings and regularly self-harming.
That being said, by the time I left sixth form, I had finally found an SSRI that worked to blunt the intensity of my social anxiety. I was attending my “perfect” university with my “perfect” grades and (prepare yourself for the twist of the century) I finally managed to get my lazy arse to the gym, and get to that “perfect” weight. I was forming emotional connections with people for the first time in years. On a shallow level, in my first year of uni, things were finally beginning to look up, and yet I was experiencing worse mood swings than ever, becoming more dependent on drugs and alcohol to function through these, and throwing myself into intense friendships where anything less than utmost enthusiasm on the other end of the relationship would send me back into that “oh my god, I’ll never make another friend in my life, I’ll always be alone, I can’t deal with this, the only way to deal with this pain is to end it!” mode. I don’t know why things got so drastic so suddenly. Maybe it was being away from my parents, or maybe it’s just that late teens/early twenties are a time when negative emotions do tend to get more serious after being repressed for years and consequently accumulating. The whole having to be the smartest person in the room to maintain a sense of self shtick was also taking a bit of a hit because university is bloody hard and everyone’s bloody smart and bloody passionate and here I was not even understanding what the assigned reading was trying to say let alone having any brilliant ideas about it to contribute; I was so quiet in one of my seminar groups the lecturer forgot I existed in a class with a grand total of 9 students. Big fish in a little pond to little fish in a big pond syndrome or maybe just more simply put, imposter syndrome, is a real thing and when you struggle with your identity anyway, it’s enough to throw you off completely. I finished that year with a first but I told myself it probably wouldn’t happen again. A couple of days later, feeling shit and overwhelmed, I did what I’d taken to doing to manage my emotions, and got high. The delusional episode ended me up in A&E for self-harm, and when they let me go the next day, I travelled back to my family home and pretended nothing was wrong.
The whole “act like everything’s fine” approach doesn’t work in the long term. 10/10 would not recommend. Without my parents around, when I went back to uni in September, everything fell apart again. I was using drugs every day, either not eating at all or binge eating, self-harming, binge drinking regularly, skipping all my lectures. Honestly, when I think back to that time it’s like I’m watching myself from outside my body. I was feeling very done with the dumpster fire (how very American of me) that was my brain. I was done with the constant 100mph up and down internal monologue. I was done with trying to cope and to hold myself together. I intentionally overdosed multiple times and after one sent me to A&E, my dad brought me home from university. It was a horrible shock for my parents: they knew I was a worrier that could be a little closed off and miserable sometimes, and they were the ones who’d first taken me to CAMHS when I was younger, but they’d struggled with that, and so from then on I’d tried to keep my issues to myself. To be honest, I don’t blame them at all for not realising anything was drastically wrong. I did a pretty good job of hiding my problems; everyone had their own things to deal with and so I became quite adept at internalising my feelings and acting “inwards” rather than outwards. It was also definitely a case of things escalating whilst I was away. With all this in mind, the overdose kind of came out of nowhere for them, but I was so detached from reality I didn’t even consider this at the time. Thankfully, I can’t really remember how they actually reacted either. Benzodiazepines do that to you, a little tidbit of information that all these teen rappers and social media personalities hyping up Xanax fail to mention. I think my dad made the decision to bring me home rather than have me stay in hospital in London, as was offered, because he thought that would be better for me. However, a few days later, after numerous, distressing visits from the crisis team (another name that will be regrettably familiar to anyone who has experienced severe mental health problems before), where I can only assume a lack of time and recourses on their part forced me to repeat what had happened over and over again to the revolving door of staff members, I took another overdose. I had become paranoid that they were out to get me and falsely believed that I was too much of a burden on my family, who were having to take time off work to look after me. This time from A&E, I went on to stay in a psychiatric ward where I was given the formal diagnosis of Borderline Personality Disorder I mentioned earlier. And it’s here that my life changed forever, I believe for the better.
It changed my life for many reasons. Firstly, it was incredibly validating. To learn that I didn’t have a plethora of different problems but rather one problem, the different facets of which can present themselves in many different ways and affect multiple areas of your life, was so, so reassuring. It not only gave me a clear treatment path but helped me to understand that there was a reason all this was happening. Additionally, the events forced me to open up to my parents and for them to grasp the severity of the situation. After all these years, I finally felt like I had a support system. My parents had always been there before but I had emotionally distanced myself from everyone, and being a “typical teenager” I believed they didn’t understand me (get that angst). I think in retrospect they didn’t understand me because I wasn’t using the right words. I didn’t want to sound dramatic so whenever I spoke to either of my parents about how I felt, I downplayed it a lot. My mum, who works so incredibly hard and has a lot on her plate herself, had a tough upbringing so her approach to me being miserable was pretty much telling me to be grateful for what I had. Had she known what I was really getting at, I know that she wouldn’t have reacted like this to what I was saying. The minute I got my diagnosis, she went out and bought every (mildly offensively titled) book on how to support someone with BPD out there and I learnt today has even been trying to bring an emphasis on mental health into her workplace! She is a wonderful person.
With all this being said, my main piece of advice for other people who are newly diagnosed with BPD or just suffering from any kind of mental health condition is to be brutally honest with the trusted people around you about what you’re dealing with. It will be uncomfortable but I can promise it’ll be worth it. With something like BPD, having a support system who know exactly what you’re dealing with, minus the vagueness and the bullshit, is so, so important. I say this because, despite Theresa’s green lights, neither she nor her party are doing much in the way of providing the funding for professional help. When I first came out of hospital, I had a lot of nights where I felt incredibly depressed, almost as depressed as I did before I went in. Prior to my family knowing about my BPD diagnosis, I would have dealt with these feelings in unhealthy ways but this time, I could go to my mum and stay with her and just cry it out until the feeling passed. That is also a useful sentiment to remember, that the feelings will pass. It’s in the nature of BPD to swing around, when I’m not experiencing a period of depression, and that’s something I find it helpful to remember. I personally really like the Youper app to track my moods because when I do get suicidal, feel anxious or wired, I have something to look at objectively to remind myself that I did feel like this before, in fact, I felt like this yesterday, but a few hours later I told the app I felt okay again. It also helps you to dissect your irrational thought processes and identify “thinking traps”. Meditation, ASMR and CBD are big parts of my life and stability, though I would recommend doing some research into the latter before trying it yourself.
On a less subjective, more physiological level, I notice that my medication really aids my emotional stability; when I have been off it, my mood swings are a lot more intense. So whilst medication isn’t for everyone, it can be something to consider talking to your GP about to see if it could be beneficial for you. Another help is the DBT skills course I completed in March, DBT being the abbreviation of dialectical behavioural therapy, the treatment specifically developed for BPD by Marsha Linehan. If you have time, she’s a great person to do some research into. She herself was diagnosed with what doctors called an “incurable” case of BPD yet she’s gone on to do the most incredible things and help so many people also suffering from the disorder. Not only did DBT provide me with a skill set of more functional coping mechanisms for both interpersonal insecurities and individual struggles, but I liked the fact that once a week I got to be with a group of people who really understood what I’m dealing with and didn’t judge. Even if you can’t find a DBT group, it’s worth checking to see if there are any mental health peer support groups in your area for this reason. I found that being around people who are dealing with similar issues helped me to see my own struggles more objectively; it reminds you that what you’re experiencing is not about you personally and that whilst you may feel isolated, you’re not. The world hasn’t got it out for you. It’s a condition that many people experience. In terms of the feelings of emptiness BPD causes, I have found that since my diagnosis, I’ve actually had more of a sense of purpose in life. On a practical level, having therapy along with a year out of uni and the presence of a constant support system has had me time to get back into writing properly. What I’ve found to be even more rewarding, however, is my participation in the online mental health community.
Something I wasn’t made aware of prior to my diagnosis was the amount of stigma there is still towards mental health issues, Borderline Personality Disorder especially. It really is one of the most demonised mental health issues in and outside of the healthcare system and that’s a hard fact to learn, because it’s a difficult enough condition to learn to manage already without knowing that there are people out there who think you’re a monster for it and are going to judge everything you do through a certain lens. Whilst we are a lot more accepting as a society of conditions like depression and anxiety, conditions such as bipolar, schizophrenia and personality disorders are still greatly misunderstood by wider society who have largely taken their understandings of these illnesses from ill-informed media portrayals and shallow, surface-level observations of a sufferer’s behaviour. I doubt the name “personality disorder” helps matters; it’s hardly the most flattering description of what we’re dealing with I’ve ever heard. I’ve found that even mental health professionals and other mental illness sufferers have a negative bias towards BPD. There’s a widespread view that we are dangerous, manipulative individuals who choose to be difficult and act erratically, that our behaviour is not “organic” like that produced by other mental health problems. I have no idea where the latter assumption comes from. Most experts on the condition tend to agree that the mood swings, impulsive, destructive behaviour, and irrational thinking originate in the hypothalamus and come from a faulty fight-flight response or other atypical brain structures; in other words, BPD has a biological basis. Whilst I agree that we can learn to change our coping mechanisms, the idea that they are as a result of anything other than pure desperation and mental anguish is incredibly puzzling and dehumanising. Simply looking the causes of the condition up online or doing a small amount of research from a credible source debunks all the common BPD stereotypes, yet people like to speak about it as if they know everything about the condition just because they’ve heard a few horror stories. There are nasty people in the world. Some of them have BPD, but that doesn’t mean everyone with BPD is a nasty person, and the bottom line is that most people suffering from Borderline Personality Disorder will hurt themselves before they hurt anyone else. We are so hypersensitive to any changes in our relationships in the first place that the last thing we want to do is damage them. When we say something feels like the end of the world, that’s because the emotional dysregulation part of BPD really makes it feel like it is. We’re not being dramatic or trying to get your attention. In fact, I can say for certain that despite feeling this way on a daily basis for about 7 years, I rarely actually voiced the sentiment. I still don’t. But I should be able to. To give the example of one person suffering from physical illness and one suffering from a mental illness, where both publicly talk about the pain they’re experiencing, why is only the latter of the two called an attention seeker? If the former tweeted about how much pain they were in, nobody would bat an eyelid. Why is this? When so many people experience mental health problems? When the gender who are typically expected by society to repress their feelings accounted for over 70% of suicide victims in the UK last year? It’s clear that keeping our feelings to ourselves and suffering in silence doesn’t do us any good, so why are so many so eager for us to continue doing so? I think being open about mental health simply needs to be normalised, and that once it is, hopefully, this sentiment will die out. I find that by being open about my mental health on social media (still quite selectively, I must admit! I can’t see myself making a post about BPD on Facebook any time soon!) has given me a sense of purpose because I do feel like I’m helping to normalise this kind of honesty. With regards to the stigma that surrounds BPD specifically, I feel that my presence online and my support of others helps to show that we’re just human beings who are struggling, not the awful mythos that surrounds us.
To finish, one of my main goals in my recovery is to be more compassionate to myself. BPD is a hard enough diagnosis to have without constantly internally doubting and questioning it. I find that as the months go by, I am feeling more and more stable, and this leads me to question if I was ever sick, especially since I only displayed 5/9 of the borderline traits in the first place, which meant that I only just met the diagnostic criteria. I don’t have psychotic rage or complete blackouts and tend to act inwards rather than outwards. I am what is considered within the mental health community to be a “quiet” borderline. I know theoretically that this doesn’t make my condition any less valid, but for this reason, part of me fears moving towards being “well”. Because if I’m well, then I feel like I’ve lost part of an already fragile identity. Of course, I’d rather not have BPD. But because I’ve been expressing symptoms for so long, I worry what’s left of me without it. At the same time, I fear going back to a place where my BPD is so severe that I have to go back to hospital. So really, it’s like you’re stuck between a rock and a hard place. It’s a double-edged sword. Is that enough cliches? The thing that I wish more people could understand is that mental illness in itself is traumatic and that even when you’ve moved on, what you experienced will always be a part of you. You still need that support. I’m not going to lie, resisting the urge to indulge in old coping mechanisms and habits is hard, and whilst the sense of pride I feel every time I don’t, or every time I use responsibly something I’m used to abusing is rewarding, there are days where waiting for the need to use them to pass is very long and very hard. I need to stop telling myself that just because I am feeling better than I did, I don’t deserve that support anymore. I do. I still deserve compassion. I still deserve a safety net. I still deserve a sense of understanding from the people around me. I deserve all of it, as does everyone else. I also deserve to be proud of how far I’ve come already instead of berating myself for not having come far enough. As I write this I haven’t self-harmed in 169 days, have been at my current job for coming up to 6 months, have an interview for a psychology course at the uni I came to love in a week’s time. I’m finally somewhat healthily managing my weight for the first time in years! I have also decided that once I do return to university, my reason for being there is not contingent on me maintaining firsts; my mental health, and what I do with the degree is much more important. I would ultimately like to go into clinical psychology and do as much as I can in that area to help people going through similar issues. With the current state of the mental health (and healthcare, in general) system in the UK, it’s definitely easy to get disheartened that the services it provides will never be adequate due to funding issues. However, in the meantime, I think the more of us with lived experience that can get into mental health care, the better the service that eventually is provided can be. Every week I’m thinking of new things I’d like to research once I have the footing, epigenetic and intergenerational trauma and the use of psychedelics and the benefit of peer support groups. There’s always a way to turn the negative into a positive, even if it takes time to learn how to do so and I think after all these years, I’m finally getting the hang of it. If my brain has been a “dumpster fire” for the last however many years, then I don’t want to let the ashes go to waste. I’m going to make them into some really morbid confetti! As I sit here writing this, I can firmly say I am happier than I’ve ever been. Game of Thrones is pissing me off (might do a post how identity and attachment issues lead to a correlation between BPD and obsessive character fixations at some point because BOY has that been driven home to me this week!) but tomorrow I’m going to an ABBA party with uni friends, Yvie Oddly is smashing drag race, and my cat is lying next to me purring. It gets better. The hard days become less frequent and they get easier to cope with too; you can learn to ride the waves and find reasons to continue doing so, regardless of how tiring it might be sometimes.
My pipe dream for this time next year is that we have people in government who really care about the invisibly ill of this country. That Downing Street can do more than turn green. I hope that we get to see more realistic and sympathetic portrayals of BPD in the media that draw attention to the issue without glamourising or romanticising it and that we get more portrayals of queer, disabled and POC experiences of mental illness too as it’s not just skinny caucasian girls that deal with this shit! Most importantly, I also hope that I continue to flourish, and wish the same for everyone struggling with mental illness/any kind of turmoil. Anybody who reads this ’til the end, wow! Thank you! It was a bit of an essay but what do you expect coming from an ex-history student and wannabe author, lol! Please let me know if there is something you’d like to see me post about on this Tumblr, such as any specific BPD symptoms and how they might present, how I deal with social anxiety and body image, or even anything completed unrelated to mental health! God knows I love the sound of my own…prose? Is that the right word to use?
I hope you enjoyed reading!
Lauren x
#mentalhealthawareness#mentalhealth#borderline personality disorder#borderlne#bpd#bpdrecovery#social anxiety#socialphobia#bpdprobz#body dysmorphia#recovery#addiction
9 notes
·
View notes
Note
Is it ordinary with BPD to not really care much about your relationships with anyone except your fp? Maybe it's because she's my very best friend, but little things she does that make me feel like shit wouldn't affect me if they were done by anyone else. Also, I've seen on a lot of sites that people with BPD make “frantic efforts to avoid abandonment” but if I feel my fp prefers someone else to me, I'll completely push her away and start hating her. Then decide I'm in love with her 2 days later.
Hi darling,
These are good questions to ask, and I can definitely imagine that you’ve been wondering about this. When struggling with BPD, it’s really common to experience black and white thinking. This can result in what you’re experiencing where you’ll completely push your best friend away and even start hating her (the black thinking) and then a couple days later you’ll be in love with her (the white thinking). When dealing with black and white thinking, small things can affect you more, as something really small can flip your opinion from someone over from white to black (or the other way around)
It’s also possible that when you push her away, this is also some way to avoid abandonment. When you feel like she prefers someone else, you push her away so that she can’t be the one to leave you anymore. So in a way, you’re avoiding the abandonment, although the outcome is similar. Does that make sense? I don’t know for sure if that’s why you push her away at times, but it might be good to look into it.
Something that is good to keep in mind is that there isn’t a textbook version of BPD. To be diagnosed with it, you need to experience at least 5 out of 9 symptoms. Some people will experience 5 symptoms, others will experience 9, or anything in between. This means that there are 256 different combinations of symptoms. So really, everyone’s experience with it is different! Even if your experience might seem to be less common, that doesn’t mean your struggles aren’t valid!
Are you currently receiving any treatment for your BPD lovely? DBT (Dialectical Behavioural Therapy) is a therapy that’s been proven to be very helpful for those struggling with BPD! We have a page on the different DBT skills here. Another therapy that can be really helpful is MBT (Mentalisation-Based Treatment). Here you learn to manage your feelings better and to stop them from affecting you as much. I think it can be really good to look into these, if you aren’t already receiving help. If you’re currently seeing a therapist but aren’t enrolled in either of these therapies, it might be an option to discuss with your therapist.
I hope this helped at least a little bit lovely! I wish you all the luck in dealing with all of this. It can get easier!
Sometimes what seems impossible, is just hard.
Keep fighting beautiful ❤
Love Pauline
#mental health#advice#advice blog#BPD#borderline personality disorder#fear of abandonment#abandonment#friends#best friend#fp#favourite person#DBT#dialectical behavioural therapy#mhapauline#Anonymous
6 notes
·
View notes
Note
I know you've already answered something similar, but I sometimes think that I might be on the spectrum. I've become more aware of my stimming/need to stim. But I feel like I'm faking it. That I only think that I see the symptoms because I want to be in with the in crowd (my friends, most of them are) or whatever. And I feel like I would've been diagnosed earlier. Idk I'm just really afraid of bringing this up with my therapist.
It’s okay to be afraid of bringing this up, anon. Bringing anything up with a therapist or psychologist is scary, and this is a big thing to bring up. Especially if you have any reason to feel as though you’ll be ignored or dismissed, and given the ableist ideas many professionals have about autism and how it presents, there is a chance of having to endure the pain of this. It’s a very real, very valid thing to fear, and I think we’ve all felt it at some point.
It’s also okay to feel like you’re faking it. But, honestly, I can’t imagine anyone wanting to be autistic that doesn’t have a connection or similarity of experience that draws us to the label. Being openly autistic means opening yourself up to an awful lot of ableism. It’s hard, scary and sometimes incredibly dangerous. I’ll be honest and say that this word is one of the better things that has ever happened to me, in that it has given me a label, a connection, a community, a way to conceptualise all that is strange in me - and it has opened the door for me to conceptualise other identities (being aro and grey-ace, things I consider connected to autism in me, like my lack of gender). Being able to go back and look at my characters through the lens of I am autistic and accidentally writing characters who are also autistic was a delight I find hard to put into words. But … it is dangerous to be autistic. It means not being understood by so many medical professionals; it means being dismissed. It means having your stims questioned on the street by strangers. For me, it meant having to quit a job because “not being able to control my facial expressions because I’m autistic” wasn’t good enough when a customer got angry at me. It means people having a label to put to your difference and that label used against you.
What I mean is this: on the off chance anyone is actually faking autism to be popular or part of a crowd, they’re opening themselves up to an awful lot of awfulness. That’s an incredibly high price to pay for connection. (I know we autistics are awesome people, but I don’t think many allistics are willing to endure the social consequences of being autistic in return for that awesomeness.) The reality is that most of us are trying to fake allism (consciously or unconsciously) to be popular or part of a crowd, not the reverse.
If you think you might be autistic, please explore it. Please. Follow autistic blogs, track the #actuallyautistic tag here on Tumblr, ask questions of autistic people. The worst that can happen is that you find out you’re not autistic, but you come away having learnt more about us. That harms nobody.
I can tell you, from the very depths of my heart, that time and age has nothing to do with the validity of your diagnosis. Nothing. It has everything to do with the fact that parents, doctors and teachers are awful at recognising autism, especially if you aren’t a cis white boy. Even then, if your autism presents a little atypically, you can still fall through the cracks. It’s only relatively recently that SPD symptoms were even included as part of an autism diagnosis, meaning people with communication skills good enough to muddle through (people like me) were overlooked entirely. It didn’t matter that I had few friendships growing up; it didn’t matter that I lacked a lot in interpersonal skills; it didn’t matter that I had no small talk skills, or any meaningful conversation skills, unless it happened to be a special interest of mine. I could rattle off a script for buying items (after many years of trying to figure this out) and I didn’t stim too much (largely because it had been abused out of me) so I was just shy and quiet, and my parents never mentioned the screaming matches we had about their stealing my pillow (to replace it with a “better” one) to our family doctor.
Anon, I was diagnosed last year. I’m thirty. (I’m a bit older than most people here. I don’t usually give my age out online other than “adult” because, as a writer, so much of my personal details are already readily accessible. But I think, today, this is something you need to know.) True, I’d been told at seventeen by an autistic friend that she and her mother thought me autistic. True, I’d been told at twenty-eight that my psychologist, parent of an autistic son, thought me very similar to him. True, I’d been told at twenty-nine that an autistic friend thought a character I wrote was based on her … when it was actually an exploration of my own SPD symptoms. True, I’d self-dx’d as having SPD for a couple of years. So when I underwent a BPD assessment only to have them tell me that they suspected I was autistic and assessed me for that … well, the evidence was there, but as I’ve said before, I was still shocked. And then I was angry, so angry.
The evidence was there, and two strangers saw it after a couple of one-hour sessions, but so many people who’d known me all my life (the people with the power to improve it) didn’t see it or refused to say the word. How could they have not have seen it? How did they all make me go so long before a professional finally said the word? How was it that I had to spend so many years feeling different, feeling alienated from all the things people don’t struggle with, until finally someone professional told me I’m autistic?
(Of course, now I know more about professionals, I don’t consider their words very important. Reading autistic people’s posts here on Tumblr affirmed my autism. Seeing how similar their challenges and feelings and experiences are to mine affirmed my autism. We are not identical - very autistic is different - but we have enough in common that autism is right for all of us.)
Yet, when I came online, I discovered that this is normal. So normal. That there are women and NB people who are being diagnosed in their thirties, forties, fifties and older. That so many people are only now getting the word that makes sense of their lives. That ableism, racism and misogyny all combine together to routinely deny many people a diagnosis that gives us understanding, identity and community.
As a late-diagnosed autistic, I swear to you that there’s many reasons why you might not have been diagnosed earlier, and none of them invalidate your autism.
My advice is the same as in this post, if you decide you want to bring this up with your therapist. But please know that you can take your time. Do it at a pace that is comfortable for you, if you want to. And if you don’t want to, don’t! If you choose to self-diagnose, the vast majority of the autistic community considers it good enough (as we should) because we know how many of us are missed by professionals. We know the professionals are awful at recognising autism and we’re not going to let their biased viewpoint keep our own from connecting with us and sharing the resources we have.
It’s natural to feel the way you’re feeling, anon, but I don’t believe you’re faking or doing this to be popular. I believe you’re discovering similarities in your own experience, those similarities drawing you to connect with other autistics. ND folk (even unknowing ND folk) tend to folk together - other ND folk make better sense to us, after all!
It’s hard for me to message with people because of my chronic hand pain, so I tend to be quite erratic in this (and if it’s been a high ask day I might not get to them at all that day, so expect that, too) but if you need to talk to me about this, the message box on my personal blog is always open, okay?
Best of luck, anon.
- Mod K.A.
#actuallyautistic#autism focus#autism discussion#discussion post#not a toy#ask#anon#text#personal#long post#very long post#mod K.A.#reassurance post
10 notes
·
View notes
Text
High and Low Project Review
For this project I was tasked with creating 15 A1 or larger drawings or collages. I started the project and after an initial brainstorm I decided to focus on high and low moods. As I suffer with Borderline Personality Disorder, unstable moods are something I am well acquainted with.
After a supply trip to Home Base I found the wallpaper and had the idea to create my first piece, Rainbows Unicorns And Things I can’t Escape. I really enjoyed creating the piece and loved the reactions from my peers in the studio who all commented on the contrast between bright colors and dark messages. I was still experimenting with the ideas of bringing text and image together and was unsure of the next step within my project. I still had a newspaper from our day visiting London galleries. I thought the found images used were striking, dark and Gothic. Which seemed perfect for my low mood ideas.
This lead me to create I think I Will Be Like This Forever, I wanted to play with different materials and texture. The images from the newspaper were interesting but very flat, I used thick acrylic paint, oil pastels and spray paint to give the work body. I then created messages and images that either corresponded with the newspaper or suited the aesthetic of the piece. The piece has a very rough and raw finish, I was pleased with what I had created but I knew that my next step would be to refine it. I did this when I started working on Distant Lover, I chose to keep a monochrome colour scheme and to make the messages flow more. The piece became something that felt melancholy, gothic horror, almost romanticising death. Both of these pieces really reflect my feelings during a depressive episode because often I lose touch with reality and see death as a viable option instead of something to fear. The works are honest and that’s what I like the most about them.

Moving on within the project I knew I wanted to do something different I wanted to create work that was more minimalistic, to continue to play with different media and ways of expressing messages without text. That is when I created the two paintings I Am Closest To Heaven By Your Side and By Your Side I Am Alone. Painting is a medium I haven’t used within my practice often. The pieces reflect manic highs and lows. The rainbow piece represents feeling deeply in love, a symptom of BPD is unstable relationships which often flip between idiolisation and unwavering devotion and extreme isolation and self sabotage. I enjoyed the challenge of trying to convey what i wanted to say without words, relying solely on image. Although I think that combining image and text is something I am reluctant to give up as it feels like an integral part of my practice as an artist. Image and text felt to me that there were endless possibilities and I wanted to keep experimenting within this project.

I decided I wanted to create my own illustrations and combine text and image that way, adapting my use of bright colors and dark messages into something aesthetically sleeker and refined. I created my first drawing TV Head, this piece focuses on dissociation and how at times I am devoid of all emotion and am unsure of my existence. I felt very pleased with the piece and wanted to create more illustrations that matched my messages. I wanted to create work that had an array of messages representing low mood with images related to the text. So I created Colorful Thoughts. Once again I used multiple bright colors. I feel that this work was my most successful out of all of my pieces so far.


After researching various artists such as Betsy Usher and listening to them talk about BPD I decided I wanted to make art that described some tangible aspect of my condition in a way that was understandable to those who don’t have BPD. So I wrote Stop Flicking The Switch, which is a poem that describes my rapid mood cycle as if it were as simple as flicking a switch, a switch I have no control over. I accompanied the text with simple line drawings of light switches to act as visual metaphors between light and dark moods. I was pleased with this work as it was the first time I had made art describing my condition in a tangible way.

However even with the praise from peers and tutors, I felt there was something missing, that I still wasn’t ready to commit to this type of work. I felt that to stop experimenting with media would only stifle the progress I was making. Within this short time I had created such a varied body of work, I wanted to keep pushing myself. I reflected upon my past work, mostly the paintings, I felt that I needed to take a step back from text and see if I could make work without it, I had gotten into my own head, my work was stagnating. I needed to try something new.
I decided to go back researching artists and found inspiration in Samuel Beckett’s not I, I was interested in the way the film felt ominous and apologetic and only showed a mouth, separate from any other facial features. I wanted to study individual parts of the body, look at their texture and how by being forced to see individual parts of the body it changes how they’re interpreted. Instead of seeing something usual you see the unusual texture and colours of the body. I started by using digital cameras to focus on capturing high quality detail. I then decided to take polaroids to further obscure the image, to make it disconnect from what we know of the body even further. I then experimented with altering the photos more my photocopying them and changing from colour to black and white. I felt this series of works was really interesting and I loved working with photography.

I had also completed a plaster workshop in this time and still thinking about Beckett’s Not I, I chose to cast my mouth, encasing it in a block. This was a metaphor linking back to my earlier mental health works. It represented being trapped and not being able to do anything about your feelings but try to explain what you feel. These mouths will be two of my final pieces as I felt incredibly proud of them because of their wordless message
I still felt that my experimenting wasn't over yet. I started to think of materials I hadn’t used in my work so far, I looked at my blog to refresh myself on the artists I had researched, I found Jordan McKenzie Spent 2008 & Spent (Litmus) 2010 and I thought the colours were interesting and I wanted to create something similar. I decided to use bleach over parker ink instead to create similar blots. I then combined this with text. I felt this was work I hadn’t ever made before, it was new and I was excited by the unpredictability of the bleach and how no two pieces ever looked the same. I decided to choose 3 of these as my high pieces because they will be displayed high and the colours reflect that of a starry night sky, which is the highest point I can see, which felt poetic to me.



I think this project was a very important for me to develop my practice. I think my experimentation was successful, I produced such a varied body of work, like never before. I really feel I have begun to understand what it means to be an artist and what my practice could be. I think that letting my doubts get to me really slowed down my work and caused me to fall behind my schedule, so in my next project I will work on time management and try to stick with realistic goals so that I don’t feel overwhelmed within my project. I know that mental health is something else I will study again in the future as it is such a big part of my life and my identity.
0 notes
Text
Dissociative Disorders 101
In this post, I'm going to give an outline of Dissociative identity disorder (DID) and Other Specified Dissociative disorder (OSDD).
These two disorders are terribly misunderstood due to horrible representation in media, a lack of education on the topic. Many people still refer DID as Multiple Personality Disorder (MPD) an outdated term from when DID was classified as a personality disorder, we now know the disorder is better seen as a dissociative disorder. I hope this post will help clear up misunderstandings about these topics.
[CW: Mentions of abuse, medical trauma, war, human tracking, suicide, self-harm, and addiction. All of these are briefly mention and not discussed in detail. Ableism is the only cw discussed in detail]
[Note: This post is not to be used as a diagnostic tool.]
DID & OSDD Glossary:
Alter: Shorthand for alternate personality or alternate identity. The most common language to refer to the multiple identities in the system. You may also see the terms "parts" & "headmates".
Alter jobs: also called “Alter types” or “Alter Roles”. This refers to the common occurrence of certain alters taking on specific roles. This often happens because to some extent DID & OSDD acts as extreme involuntary coping skills. Examples of this are protectors who deal with danger, caretakers who help keep the alters in the system comforted, or trauma holders who retain memories of trauma.
Co-Consciousness: often shortened to co-con. When two or more alter are aware of the outside together. Thoughts of both alters can often blend together. Even at times alters may have split control of the body.
Depersonalization and Derealization: Often shortened to DR/DP. DR/DP disorder is its own diagnosis but those with other dissociative disorders experience it as well. Depersonalization the feeling of oneself is not real or is heavily disconnected from the body. This can even result in one of feeling in control of limbs at all. Derealization is the feeling of the outside world not being real, or a simulation.
Fronting: The act of being the alter conscious at the time and ability to interact with the outside world.
Host: Either the person believed to be the “first” personality (sometimes called the core or original) or the latter who fronts the most.
Splitting: In this case, it refers to when new alters form.
System: A word used to reference all of the alters as a whole. Used like "I am an alter in a system" or sometimes “ I am a system”. Rather someone uses this term is a matter of personal preference, and if they see themselves as part of a system or collectively are a system.
What is Dissociation?
Dissociation refers to the mechanism our brain has to disconnect us from our surroundings sometimes as a benign reaction but severe dissociation is associated with trauma and other mental illnesses.
Every Person has the capacity for dissociation and many experiences some degree of the skill like when you drive home but don’t remember it. However daydreaming in class, spacing out every now again is healthy, there is a huge difference between those experiences and those of people with dissociative disorders.
Dissociation is primarily associated with DID but can also be a symptom of C-PTSD, Borderline Personality Disorder (BPD) and some forms of psychosis. There are also physiological conditions that cause and/or mimic dissociation. Like seizures and migraines.
What are the symptoms of DID & OSDD?
[Disclaimer: I’m aware that the DSM is a flawed way to look at mental health, but it is the best way we have to ensure all parties are working with the same definition of terms]
DID:
DID diagnostic criteria are as follows:
1)Two distinct identity states are present. They have to be separate and able to act autonomy. It isn’t “feeling” like another person.
2)Amnesia must occur, defined as gaps in the recall of everyday events, important personal information and/or traumatic events
3)The person must be distressed by the disorder or have trouble functioning in one or more major life areas because of the disorder. This criterion is common among all serious mental illness diagnoses as a diagnosis is not appropriate where the symptoms do not create distress and/or trouble functioning.
4)The disturbance is not part of normal cultural or religious practices.
This DID criterion is to eliminate diagnosis in cultures or situations where multiplicity is appropriate. An example of this is in children where an imaginary friend is not necessarily indicative of mental illness.
5) The symptoms are not due to the direct physiological effects of a substance
So what does that mean? It means that those who have the disorder have at least one alter the hallmark of DID. Alter come in all kinds of varied types and versions. The amnesia criterion does refer to forgetting traumatic events, but also incidents in normal life.
Alters themselves are a complex they aren’t "alter egos or" made up people. Alters can be almost anything, children (younger than the body) adult alters (older than the body), alters based on fiction called Fictional introjects (fictives for short), alters who are angels or spirits, ghost alters, animal alters, alters of varying race and sexualities. This is because alters form to ensure the survival of the child, this includes alters to comfort, protect, soothe and hold trauma away from the wider consciousness. This means that anything that can fill that role can be put into an alter. There is no control over alters, they are not imaginary friends or malleable they are the best way the mind had to survive.
In day to day life DID might look like having missing time, experience dissociation even when in control, a sense of not having an identity, hearing voices within their heads (not auditory hallucinations), meeting people you feel like you should know, having actions you took but have no recollection of, overlapping emotions and trouble focusing.
People with DID have high rates of self-harm, suicidal behaviour, addiction, disordered eating and other behaviours that cause damage to oneself. This is often even more distressing as one might hurt themselves and not remember it because an alter did it.
Those with DID will also often have what is referred to as “Inner worlds” or “headspace” this refers to in the mind of the person there is a mental world within. This is a place where alters have a form, body and voice within the mind. It is often a combination of a coping skill used as a kid to escape and a way to be able to interact with others alters. Headspaces often are where alters feel they are when not fronting. It also provides a way of seeing where alters who are not in communication with others are, and can sometimes serve as a visual connection to understanding the others in the system and understand trauma.
Somatic symptoms are really common, Including: Headaches, nausea and vomiting, Non-epileptic seizure/psychogenic seizures, blurred vision, muscle aches, nerve dysfunction (like dysautonomia), fatigue, other feelings of illness. This is sometimes part of conversion disorder.
People with DID & OSDD almost always also have (C-)PTSD. So symptoms like hypervigilance, nightmares, and flashbacks. As they have DID & OSDD and have experienced trauma they likely have symptoms from that other than dissociation, even if they do not meet PTSD criteria.
BPD has high comorbidity with DID, many people with DID or OSDD are misdiagnosed with BPD. Other common comorbid conditions include Anxiety Disorders, Depression, Eating Disorders, and Conversion Disorder.
OSDD:
So the thing about OSDD is a category of conditions that don’t fit another diagnosis. With this post, we are mostly concerned with OSDD-1a and OSDD-1b because those disorders are most similar to DID and form systems.
The DSM Description is as follows:
This category applies to presentations in which symptoms characteristic of a dissociative disorder that cause clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet the full criteria for any of the disorders in the dissociative disorders diagnostic class. The other specified dissociative disorder category is used in situations in which the clinician chooses to specify the reason that the presentation does not meet the criteria for any specific dissociative disorder. This is done by recording "other specified dissociative disorder" followed by the specific reason (e.g., "dissociative trance"). Example presentations that can be specified using the "other specified" designation include the following:
1. Chronic and recurrent syndromes of mixed dissociative symptoms. This category includes identity disturbance associated with less than marked discontinuities in sense of self and agency, or alterations of identity or episodes of possession in an individual who reports no dissociative amnesia.
2. Identity disturbance due to prolonged and intense coercive persuasion: Individuals who have been subjected to intense coercive persuasion (e.g., brainwashing, thought reform, indoctrination while captive, torture, long-term political imprisonment, recruitment by sects/cults or by terror organizations) may present with prolonged changes in, or conscious questions of, their identity.
3. Acute dissociative reactions to stressful events: This category is for acute, transient conditions that typically last less than 1 month, and sometimes only a few hours or days. These conditions are characterized by constriction of consciousness; depersonalization; derealization; perceptual disturbances (e.g., time slowing, macropsia); micro-amnesias; transient stupor; and/or alterations in sensory-motor functioning (e.g., analgesia, paralysis).
4. Dissociative trance: This condition is characterized by an acute narrowing or complete loss of awareness of immediate surroundings that manifest as profound unresponsiveness or insensitivity to environmental stimuli. May be accompanied by minor stereotyped behaviours of which the individual is unaware and/or that he or she cannot control, as well as transient paralysis or loss of consciousness. The dissociative trance is not a normal part of a broadly accepted collective cultural or religious practice.
Those with OSDD-1a&b meet most but not all of DID criterion. They are considered Complex Dissociative Disorders along with DID.
OSDD-1a is either identity disturbance with less distinct alters than DID (they cannot physically take executive control over the person's body, but strongly influence the person's thoughts and actions with this type there is amnesia.
OSDD-1b does have distinct alter do exist and can take executive control with the type there is no amnesia.
How does DID or OSDD Develop?
DID & OSDD comes from long term childhood trauma. When a child is exposed to long term trauma and the identity of the child cannot properly integrate. This means your brain put up amnesic barriers to memories and perception forming the separate identity states.
DID is highly correlated with sexual abuse, physical abuse, medical trauma, living in a war zone, child trafficking, and Ritual abuse. Another key factor in a child developing these disorder is the lack of healthy attachment (more info here) You can not develop this disorder after age 9, you can't develop it from a single trauma.
The most current theory used to understand how these disorders works are Structural Dissociation. It refers to the way our brain changes the usual structure to compensate for traumatic experiences. It also posits that a child is not born with an integrated personality, to begin with, and this what allows the extreme dissociative symptoms of DID to manifest.
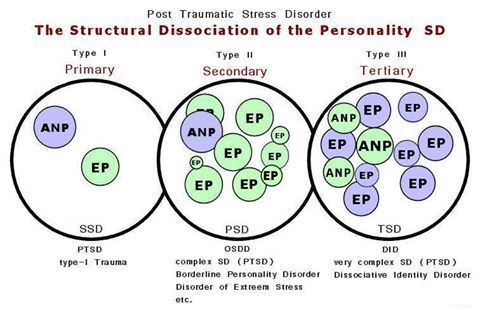
(Image Source)
ANP refers to “Apparently Normal Part” (someone who takes care of daily life)
EP refers to “Emotional part” (someone who holds trauma memories, reactions, and/or sensations).
Primary SD: is found among those with PTSD. The EP holds all trauma associated things such as fight or flight, feelings, sensations, etc, and is not a fully differentiated being (such as alters are/can be in DID and OSDD-1)
Secondary SD is OSDD, complex PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Secondary SD is OSDD, PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Tertiary SD refers to DID. There are multiple ANP and multiple EP. They are more developed than the ANP and the EPs in Secondary structural dissociation (though DID parts can have the same degree of development as OSDD-1 parts and vice versa). EPs can be “small”, as in less developed and would be considered fragments, as they hold limited trauma material such as a single feeling or one or two of the senses in a few trauma memories (or just one or two of the senses in one trauma memory). EPs can also be a fully developed part, such as an ANP would be, but hold trauma material. Multiple ANPs exist and can have various jobs associated with daily life such as a school part, a work part, a caretaker part, etc.
This theory is one of the most widely accepted concepts of how alters form and best matches most people's experience. It does contradict the idea that alters are split pieces of one cohesive identity being split the old model.
Another thing to keep in mind about this theory is it shows the structure and function of the brain are altered from a young age. Brains conditioned to dissociate during stress and trauma will continue to split during stress. This means alters can continue to form in those with DID & OSDD past age 9.
This Video explains further how this relates to alters splitting
Treatment:
DID & OSDD can be treated and worked on so the person is no longer experiencing the adverse effects or usually lessen them. Treating DID works mostly the same way as any other trauma survivor. Most kinds of trauma therapy can be used, EMDR being the exception. Certain kinds of meditation and visualisation also prove to be not as effective.
Medication can be used to treat comorbid disorders like depression or anxiety but there are no pharmacological treatments for DID on its own.
What is unique about DID is there is the aspect of how the alters affect you. With DID & OSDD time spent with, alters is crucial. Helping alters who are struggling with trauma becomes deeply important in healing.
The two main options with alters are integration or communication.
Integration refers to a process of when two identity states fuse together. This means you have less altered consciousness states, it also relates to them both being able to handle their trauma. The goal here is to end up with the patient having a singular integrated identity.
The other treatment focuses on forming functional working relationships with the altar and helping them process trauma individually, integration might still happen but a singular identity is not the end goal.
Mythbusting:
“People with DID are just psychotic or delusional” False, psychosis is not a feature of DID or OSDD and has been shown to act completely differently for the person and in the brain than psychosis. This is also offensive as it denigrates people with psychosis.
“DID is fake/made up by a therapist/ social contagion/the person only believes they have alters” False: DID has been observed in multiple studies and social contagion, malingering and therapist coercion are no longer prime theories. People saying this often bring up the false memory scare and Sybil. Both of those have been proven to be wildly overstated and are not the only evidence we have. There are cases dating back to the 1500s with the first psychiatric observations in the 1800s.
“Aren’t they dangerous?” or “they're so scary and crazy!” or “Don’t they need to be locked up” False, The real facts are people with dissociative disorders don’t commit violence at a higher rate than anyone else. They are much more likely to be the victims of violence. Starting with the fact they faced violence as a child to even have the disorder.
“Isn't that possession?” or any other spiritual concepts. False, There is nothing supernatural reasons for DID. Some people have spiritual or religious beliefs that change how they personally perceive their condition, but there is nothing supernatural about DID or OSDD.
“It’s super rare” Not actually the estimate for DID is about 1% of the population. Might sound small but with the number of people in the US alone who have, it means you're likely to meet someone with it.
“I would know if you had it” Not likely. Most people with DID present with covert DID. These people do not have alters who act wildly different from the host. Generally alters will attempt to not show obvious signs as well as being n the same mind with similar physiological aspects and upbringing influence things like mannerisms. Only 5-6% of people with DID have an overt presentation. Even these people are unlikely to be able to wildly change the way they dress and the like as it’s impractical.
“Bad alters/evil alters/violent alters/murder alters” False. There are often alters who might feel aggressive or be persecutors who hurt the other alters. But they are not going to commit murder or rape. They are usually more dangerous to the person with the disorder than anyone outside. And this anger usually stems from trauma.
“You can’t have the disorder you wouldn’t know” and other variations on “Crazy people don't know their cray”. False usually people with DID reach out to help themselves they don’t get forced into it. Because the symptoms of DID disrupt life and the usual comorbid PTSD or other mental health conditions. People with DID are also often aware to some extent of their alters. Rather this is voices, time gaps, or passive influence. And people who have known about the disorder and are in treatment often have good communication between alters in the mind, they are definitely aware of their health.
I Hope this is helpful for those with and without the disorder to better understand these conditions. My personal experience with DID does mean I’m particularly passionate about education on this topic even more as it intersects with education about trauma in general. I hope this didn’t come off as adversarial and helps people learn.
-Admin 1
{Resources: Structural Dissociation Explained, OSDD Diagnostic Material, The Fantasy Theory of DID, New Models of DID, DID Literature Review, DID Research.org, DSM Library, Webermann, A. R. & Brand, B. L. (2017). Mental illness and violent behaviour: The role of dissociation. Borderline Personality Disorder and Emotion Dysregulation}
#blog post#mental illness#mental health resources#mental health education#mental illness education#dissociative identity disorder#did#other specified dissociative disorder#osdd#osdd1#multiple personality disorder#mpd#dissociative disorder#dissociatvie disorders#dissociation#childhood trauma#structural dissociation#bpd#cptsd#ptsd#disordered eating#long post
39 notes
·
View notes