#bottom surgery resource
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
28.6 is the average number of monthly visits per US mobile user.
Text
Phalloplasty Procedure Full Outline Offical (Radical Free Flap Procedure)
What is phalloplasty/ phallo?
Phalloplasty - "includes several surgical procedures that aim to construct male genitalia that looks as natural as possible. The surgery is divided into several steps that may vary from patient to patient. Generally, they are the three following steps" (Source1) . We aren't going to count if the prerequisite of hysterectomy. Since my surgical procedure, they have removed the requisite of an oophorectomy, that procedure is now optional thanks to the always advancing technology.
The first step:
a surgery that consists of creating a penis from a skin flap from a specific area of your body (most common areas are forearm and lower back) of the body that you would chat about with the surgeon(s) and that specific skin will be grafted to the genital area.
The second step:
Here, surgeons construct the urethra that will llow urination. This is known as Urethra Lengthening (often referred to UL) (Urethra Lengthening Procedure Post)
The third step:
At this stage, you will receive testicular and erectile implants that will allow for penetrative sex. Note: this is not the only type of phalloplasty sugerical options.
The first surgical step consists of:
the creation of a penis or phallus from a skin flap and fatty tissue of the donorn site involving the removal of blood vessels (to create a blood supply) and nerves (this is where nerves are disconnected and reconnected, which can take some time to gain full tactile function or feeling. This skin will be grafted to the genital area where a penis would naturally sit on your body. The next part of the procedure is:
"the burial of the clitoris at the base of the phallus;
the creation of the penile urethra within the phallus;
the lengthening of the biological urethra;
the creation of the glans;
the creation of the scrotum;
the closing of the vaginal cavity; and
the removal of a layer of skin from the thigh to compensate for tissue loss
on the donor arm." - (Source1) Some of these things are not the same for every surgeon, be sure to ask about if your clitoris could be not buried for example, or different pumping systems, varying styles in surgerical procedures from clinic to clinic, even surgeon to surgeon.
The second step consists of the construction of the urethra:
This procedure connects the penile urethra so the part of the urethra inside the phallus itself to your biological urethra that was elongated in the first step of the phalloplasty surgical procedure. The connection of the urethra is made by creating a tube from the skin of the scrotum between the openings of both parts of the urethra.
Note that the anatomical makeup of the phallus is composed of only skin, fatty tissue, blood vessels, and nerves.
It does not contain any muscles or a sphincter (a muscle that opens and closes like your butt does aka "the breakwall"), which means that after the second step, you may have to empty your urine either temporarily or permanently manually from the portion of the phallus by applying pressure to the phallus. (UL Article)
A minimum of a six month waiting period is necessary between this and the next stage planning.
Permanent hair removal from the area that will be used to construct the urethra is also required to avoid complications (unless during the consult the doctor states otherwise). Note that it is impossible to determine in advance which area will be depilated since it must be evaluated after Step one. It is at this time that you will receive information about hair removal,
The third step:
Involves insertion of implants (erectile device and testicular implants).
This procedure will allow you to be able to get an erection in your penis (phallus) and now you have the ability of penetrative sex. Erectile Devcies Post
You will have to wait a minimum of three to six months after the second step (healing and surgeon(s) pending) and have no urinary problems before planning the third step. If complications do come up, they will have to be completely treated and healed before the implant surgery can be performed.
"Depending on the surgeon's assessment, the second and third steps may be reversed." (Source1)
Everyone has to decide whether to undergo one, two, or all three steps. Meaning you can stop after any phase/step of the three)
This choice is super personal and must be made according to what you need, your expectations of the outcome, and the impact it has on your daily life.
There are a few factors that may influence your decisions, such as wanting to urinate while standing, the desire to have penetrative sex, having more masculine genitalia, etc.
The estimated time to complete all three stages of phalloplasty can vary from two to three years, including the waiting I'm between surgeries.
These results may vary according to the age, weight, quality, and elasticity of the skin at the donor site, the scarring process, lifestyle habits and the overall health of the patients, healing, how well you take care of yourself, etc. The radial forearm free-flap technique is shown to produce the best results from bottom masculinizing surgery options.
Mandatory Prerequisites for Phalloplasty:
Hysterectomy with removal of the cervix done minimum six months before the phalloplasty procedure. *There are two options for this: removing the uterus only (called "total hysterectomy"), or option two removing the uterus, fallopian tubes, and the ovaries, also called "total hysterectomy with salpingo-oophorectomy"*
Permanent hair removal (second step when recommended to start). The recommended options are laser hair removal or electrolysis, which may be more beneficial for results. from the area of the phallus donor site to prevent complications with hair growth (fistuals), which can cause issues such as infection and even surgerical intervention to fix the issue area(s). Surgeons typically like to see the graft site not have any hair growth for a minimum of three months.
Talk to your primary physician and/or gynecologist to help you make an informed decision about your choice on the type of hysterectomy you get.
And talk to your surgeon and your primary doctor about which option of hair removal is better suited if one is not insisted on you using it.
A vaginectomy can be removed since only 2 cm will be used for the phallus.
Body Mass Index (BMI)
Before phalloplasty can be performed, it is important to know that you must have a healthy weight or have a BMI under 30, and you can not have excessive fat accumulation in your abdominal area.
"Being overweight and abdominal fat can compromise the connection of blood vessels during the procedure and lead to significant surgical complications.
If your BMI is 31 or higher you be most likely required to lose weight before the surgeon will perform the procedure.
Patients with a high BMI also have a decreased potential for healing and decreased satisfaction with surgical results." - (Source1)
Source List:
Source1 -GRS Montreal,Quebec, Canada - downloadable PDF -used as the direct quotes and most of the information
John Hopkins Hospital - used for an information source. -https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/phalloplasty-for-gender-affirmation
Cleveland Clinic -an information source (I barely used this)- https://my.clevelandclinic.org/health/treatments/21585-phalloplasty
Article- Self written on Urethra Lengthening Procedure
Article- Self Written - Erectile Devices Available
#transgender resources#ftm trans resources#female to male affirmation surgery blog#educational blog#phalloplasty resources#phalloplasty procedure layout#phalloplasty procedure#transgender#trans ftm#ftm transition#transman#ask me things#phalloplasty#ftm phalloplasty#lgbtq#phalloplasty blog#phallo education#bottom surgery resource#ftm bottom surgery resources#ftm trans ed
29 notes
·
View notes
Text
More info on Radial Forearm "Flap" Phalloplasty which some ppl were curious about in the notes of the other post.
You're welcome.
The OP is Emmett Preciado (he/him), you can go watch this & the first phallo info video on his IG below:
instagram
instagram
#Instagram#videos#bottom surgery#phalloplasty#radial forearm phalloplasty#trans masc#ftm#trans man#trans men#trans resources#gender transition#transblr
7K notes
·
View notes
Text
please don't forget to check out our queer resources page if you are in need of help
sometimes you don't want to send an ask or look through tags and that's totally cool! we've compiled a queer resources page on our blog where you can easily look for what you need. please feel free to use the find in page option in your browser to find what you're looking for
we will continue to add resources as time goes on!
#resources#lgbtqia#lgbtq#lgbt#queer#gay#lesbian#bisexual#pansexual#trans#transgender#transmasc#transfem#transfemme#transmasculine#trans man#trans woman#trans women#hrt#hormone replacement therapy#top surgery#bottom surgery#butch lesbian#dyke#our writing
416 notes
·
View notes
Note
Can you tell me about bottom surgery (ftm)? Cause I was trying to research it and apparently it makes it so they can't like ejaculate? I'm probably misremembering something I misread but I'm now worried because I was hoping that getting bottom surgery would help me be more comfortable in my body and that maybe it turns out I'm not asexual (not like i think it's wrong, I just find the idea of not being able to imagine myself like that very annoying since I do want to have sex eventually I think)
Well, it really depends on what type of bottom surgery we're talking about. There are quite a few different options, like metoidioplasty, phalloplasty and different options within both of those.
That said, you generally can ejaculate after bottom surgery. You just don't ejaculate semen. You can also orgasm. Depending on the type of surgery, some people can also penetrate others during sex-It just depends on the type and your recovery.
This is a good article with a lot of information on bottom surgery and this one goes a bit more into depth on the sexual side of things, if you're interested!
Hope this helps, lemme know if you have any other questions. <3
#sex education#asks#sex tips#anatomy education#trans education#bottom surgery#phalloplasty#transmasc education#transmasc resources
70 notes
·
View notes
Text
Hey so with the barbie movie coming out mod is once again seeing comments like “I’m nonbinary and wish I could just have flat genitalia like a doll, it would take away my dysphoria”. Mod got a dysphoric culture ask about it like 2 years ago actually and now there are more so:
This is possible.
If your transition goal is to have a complete removal of all your internal and external genitalia, there is a real surgery that people get to do that. It’s called genital nullification.
It’s also called nullectomy or nullo.
It’s not a very new or super complicated surgery. Everything is taken out/taken off and you’re left with just a hole for your urethra (where you urinate out of). The urethra may be moved as part of surgery. If you research the procedure you’ll also probably hear them talk about urethral shortening, because nullification is mostly done on cis men/transfems/nonbinary patients who require a penectomy as part of the surgery.
Now don’t get this for an aesthetic or because you like how dolls look. It takes 6-8 weeks of recovery and is as serious a decision as any other bottom surgery. More info is here and here. This website has some info and pictures (graphic warning) of nullification along with phallus-preserving vaginoplasty, another nonbinary surgery.
Hopefully this helps someone!
#not dysphoric culture#resources#mod talks#nonbinary#gender affirming surgery#trans resources#nonbinary resources#bottom surgery#bottom dysphoria#genitalia tw#tw genitalia mention#transfem#amab nonbinary#lgbtq+
787 notes
·
View notes
Text
pro neopussy people money where your mouth is cuz neocunt costs a fucking house and requires the work of a full time job to actually get and if you appreciate it you should appreciate more being in the world
#basically i need help getting bottom surgery and idk how to ask cuz it's not entirely money#i just genuinely can't find the right resources that won't gaslight me and tell me i'll never get surgery
33 notes
·
View notes
Text
Please Reblog this Post Trans Community and Allies.
I am Zestual (some know me as Shadow), and I run a blog for female to male transition and have for almost four years now.
A little about me I am a retired social worker and addictions counsellor. I have completed all surgeries (last one was just over a decade ago). I've had chest surgery, I've had phalloplasy. I actually enjoy sleuthing the internet for proper information to inform the community that phalloplasty is not bad, and not nearly as risky as many say. As long as you take care of yourself pre and post op you will have a phallis that you've dreamed of.
This includes hormone treatments, top surgeries, metoidioplasty, phalloplasty, and much much more.
If you are looking for a resource that only uses reputable sources and is a source of unbiased information on transition.
Here is the blog directory:
https://www.tumblr.com/answersfromzestual/748974533324800000/improved-blog-directory-find-what-you-need?source=share
Feel free to ask question, send in concerns or questions. I welcome all blog related questions, comments, and concerns.
-Zestual
#Transgender#trans positivity#transman resource blog#Resource blog#ftm gender affirming surgery blog#Transgender educational blog#Ftm trans information#Ftm trans education#transgender ftm#phalloplasty#ask me things#ftm transition#transman#phalloplasty blog#lgbtq#Phalloplasty educational blog#Top surgery educational blog#Bottom surgery educational blog#Ftm trans educational blog#Ftm resources#transitioning#Tansmasc#Transfer#trans nonbinary#ftm phalloplasty#Ftm education#Unbiased gender affirmation informational blog
53 notes
·
View notes
Text
Bottom surgery questions part 3!
Part 1, Part 2 Bonus Info on RFF Phallo
Source: Emmett Preciado IG
He cut his hair but apparently he donated it so he's forgiven
instagram
#Instagram#bottom surgery#phalloplasty#trans#transgender#ftm#trans masc#trans man#trans men#transblr#transitioning#radial forearm phalloplasty#trans resources
1K notes
·
View notes
Text
Certified Sex Ed Post!
we should hype up bottom surgery more i think. both twitter transphobes and chronically online trans people really like to be disgusted at phalloplasty, vaginoplasty, ext. and i really think we should treat them as cool and sexy and neutral like top surgery scars or whatever
#sex education#gender transition#trans education#trans resources#Bottom surgery#vaginoplasty#transfem resources
86K notes
·
View notes
Text
does anyone have good resources for locating bottom surgery doctors? im specifically looking for docs who do metoidioplasty
48 notes
·
View notes
Note
Hello. I feel I want to know about how sex feels like post-bottom-surgery but I'm too embarrassed / don't want to make other trans women feel uncomfortable... to actually ask anyone I know? Is this something you can advise upon?
Hi! That makes sense. It can be very hard to find information on bottom surgery, sex aside. Now, I don't have personal experience but these are some trans women's accounts of it here, here and here.
Also asking on "r/MTF" on Reddit, or "r/askatransgender" could be helpful! That way, you're not approaching any other trans women directly and if they're not interested in answering, they can just scroll away. And there might also be others with resources I don't have. [Anyone who has any resources/info, feel free to add on!]
Hope this helps! Lemme know, especially if you have anymore questions. <3
#sex education#asks#anatomy education#anatomy resources#bottom surgery education#transfem education#transfem resources#trans education#trans resources
63 notes
·
View notes
Text
I find it interesting how people don't seem to know about or expect trans men to get bottom surgery or other masculinizing surgery and treat top surgery as *the* surgery. Like, I saw my anthropology mentor today and I hadn't seen her since before I had surgery, and she said something along the lines of like "it must be such a relief to get *the* big surgery over with", as if top surgery would be the only major surgery I could feasibly get over the course of my transition. And you see this a lot with people equating trans men with having a vulva, using terms like "boypussy" (a personal ick) when referring to sexual experiences involving trans men, as if trans men couldn't possibly have other genitalia. And of course facial masculinization surgery is also a thing many trans men opt for, but it is never talked about as even a potential resource for trans men, despite it being a valid option.
Personally, I think top surgery is it for me. I would love to be able to get bottom surgery, but unfortunately I have genitourinary disorders and I don't think it's a good idea to mess with anything down there. But if I didn't have those disorders, bottom surgery would not be off the table. And getting a hysterectomy or something similar certainly is *not* off the table, I would like to get some sort of sterilization procedure at some point.
I don't know if this is part of people thinking trans men somehow have an easier time "passing" than other trans people without significant intervention (we don't) or people being uncomfortable with the idea of trans men "ruining" our femalehood, or maybe it's a combination of both ideas and others, but it's just such a frustrating phenomena.
3K notes
·
View notes
Text

This is a take I've seen fairly often- that trans men & mascs only think they experience transandrophobia because they refuse to accept that what they're experiencing is misogyny.
It's also a completely ridiculous take. The fact that trans men/mascs are targeted by misogyny is a fundamental part of transandrophobia theory. Trans men/mascs, and others who regularly discuss transandrophobia, emphasize over and over again the ways in which trans men/mascs experience misogyny. For example, the idea that they are women and therefore are too stupid and brainwashed to be trusted about their genders, or the sense of entitlement to trans men/mascs' bodies (how dare you ruin your perfect breasts, how dare you transition in a way that makes you unable to carry children, how dare you not be the beautiful woman i want you to be).
In fact, the people who deny that trans men/mascs experience misogyny tend to be the same people who argue against the concept of transandrophobia. They insist that trans men receive male privilege, and in fact actually benefit from misogyny rather than suffer from it.
When trans men/mascs point the ways that they are affected by misogyny, they are accused of spreading TERF rhetoric (as though acknowledging the ways in which people who were assigned female at birth are oppressed automatically means you believe in "sex consciousness" and "afab unity" against anyone assigned male at birth"), or accused of implying that trans women aren't affected by misogyny (they absolutely are, the belief that trans men and women can't both be affected by misogyny stems from oppositional sexism)
All this to say: The people who talk about transandrophobia are well aware that trans men/mascs suffer from misogyny, and aren't denying this out of dysphoria or internalized misogyny- they aren't denying this at all. The people who deny that trans men/mascs suffer from misogyny are the people who believe transandrophobia doesn't exist.
And, transandrophobia isn't "just misogyny." Misogyny is a crucial component of transandrophobia- again, no one who talkes about transandrophobia is denying this- but not the only component.
Trans men/mascs being denied access to gynecological healthcare (that cis women are able to access) because they appear to be men, or have their gender legally changed to male isn't "just misogyny."
Trans men/mascs to losing their friends, support, and abuse and mental health resources when they come out and transition, or reach a point of being "too masculine," isn't "just misogyny".
The belief that going on testosterone will make trans men/mascs dangerous and violent, and the negative rhetoric about bottom surgery, isn't "just misogyny."
Being called a gender traitor and accused siding with the enemy and only transitioning to gain male privilege isn't "just misogyny."
Trans men/mascs being impregnated specifically as a method of forcing them to detransition isn't "just misogyny."
Choosing to use a women's bathroom (either due to safety concerns or transphobic laws) and being kicked out or assaulted for looking male isn't "just misogyny."
Trans men/mascs getting violently attacked because "if you want to be a man so bad, I'll beat you up like one" isn't "just misogyny."
People who talk about transandrophobia very much recognize that trans men/mascs experience misogyny (and are trying to get people who deny transandrophobia to recognize this as well), and there are aspects of transandrophobia that go beyond "just misogyny." Neither of these things contradict each other. In conclusion, "'transandrophobia' is just misogyny but transmascs don't want to admit it" is completely false all around, so I wish it wasn't such a commonly held belief.
#transandrophobia#anti-transmasculinity#looking for sources just ended up taking a toll on my mental health so i decided not to link 'proof' for the examples of transandrophobia#if you're curious about a specific one and ask in good faith i might provide something though#anyway. you ever see such a garbage take you have to write an entire tumblr post about it
637 notes
·
View notes
Note
what does a tdick like... actually look like? or how they behave post-testoterone and pre-surgery? I haven't really been able to find like anything educational about how they work- what the look like, how they differ from other genitalia during sex and/or arousal, any of that stuff. I'd really appreciate it if you could explain it?
Bottom Growth or T-Dick Info:
For educational purposes only
I will be calling a "T-dick" a "T-phallus" in this answer.
I highly suggest all read through my second source, it is very informative about growth, sensations, and also has some good general knowledge as well.
Clitoral hypertrophy: the clitoris growing in length and width while taking testosterone.
So a t-phallus very much looks like the head of a penis, the shape, the contours, it just doesn't have a hole for urination like a penis or a shaft especially when you are aroused. A t-phallus gets erect when you are aroused just like a penis. It is considered the pleasure organ.
During arousal (turned on), it actually swells up and fills with blood, becoming erect and more stiff (hard)
While your t-phallus gets bigger on testosterone many people describe their changes in their orgasms and pleasurable feeling. For example you may like a different kind of touch now because that feels more pleasurable. "Some people describe feeling a more erection-like sensation when aroused." - source 2
Typical bottom growth on testosterone therapy is typically 1 to 4 cm, sometimes even more, this growth varies. One small study¹ about bottom surgery reported the average length of bottom growth measured from 2.5 cm to 4 cm in the study participants who eventually underwent surgery. Another study² found that at the one year mark, the average growth was 4.6 cm.
During sexual intercourse with someone with female genitalia: will require you to use a dental dam as protection (dental dam information), this is just basically a sheet of latex or another kind of plastic (like male condoms), to prevent direct contact. You don't not just need to use one during oral sex but if you are rubbing your genitals together it may be a good idea. If you are sharing toys make sure to clean them thoroughly between using it on the opposite person. (Making sure sex toys are clean is always a good idea).
If you are having sexual intercourse with cis males/ male genitalia: you should be requiring that person to wear a condom, even if they are trans themselves, any bodily fluid contact can spread a STI. Or you can use female condoms.
Here are some articles on sexual health.
Sexual health article 1
Sexual health article 2
Below are example images of a t-phallus and growth:

Source²

Source²
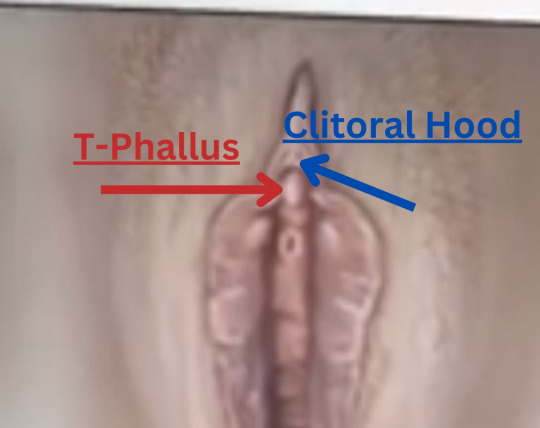
- a more realistic view.
You can see that there is a tip that gets slightly thinner with the connective tissues. So you have a head of a penis to put it very generally and your 'shaft' is almost buried in the connective tissue/ hood (which I used to call my 'foreskin', it made me feel more comfortable.
Sources, Images, and Studies
Source 1
Source 2
Medical Study¹ -PDF
Medical Study²
Fun facts: We all are actually considered to have female genitalia in the womb until about the second trimester of pregnancy, then your body gets a flood of either estrogen (X) or testosterone (Y), which is what tells your body to form the genitals. This is actually interesting because it shows that the clitoris is actually a tiny penis in a way, since it actually does become a penis as a fetus develops. - I learned this in my child development class.
#anon ask#ask#ask zestual#ask Answersfromzestual#Answersfromzestual#transgender#trans ftm#ftm transition#transman#ask me things#bottom growth information#pre phalloplasty penis#pre phalloplasty t dick growth#t dick info#t penis info#pre bottom surgery growth#testerone and t dick growth#testosterone and ftm bottom growth#ftm bottom growth#lgbtq#ftm resources#ftm education blog#educational post#educational use only
38 notes
·
View notes
Text
Bottom surgery questions part 2!
Part 1 + Bonus Info on RFF Phallo
Source: Emmett Preciado IG
instagram
#Instagram#bottom surgery#phalloplasty#trans#transgender#ftm#trans masc#trans man#trans men#transblr#transitioning#radial forearm phalloplasty#trans resources
474 notes
·
View notes
Text
Hello there!
I run a ftm transition blog that mainly focuses on phalloplasty, but I do have several articles on other types of surgeries and procedures as well.
Please check out my blog directory, I also take questions, comments, and concerns.
i wish ppl didnt shit so hard on (transmasc) bottom surgery man. i feel like i wouldve looked into a metoidioplasty a lot sooner if i hadnt seen all of the negativity and stigma surrounding phallo and metoidioplasties. but as soon as i actually looked into it i realized it was something i want! extremely bad! and i feel like a lot of other transmascs would want bottom surgery if they actually knew more about different types and results
#ebby echoes#trans tag#bottom surgery#transmasc#trans#metoidioplasty#phallo#phalloplasty#Phalloplasty resources#metoidioplasty resources#transgender ftm#Transgender ftm#Transgender reaources#Phalloplasy educational blog#Ftm Bottom surgery resources#Transmasc resources#Trans non binary resources#Sorry to hijack your post but I'm trying to get more information out to the public#Thank you
2K notes
·
View notes