#No Evidence for Gender Affirmation
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
The most popular pages on Tumblr are about Minecraft, GIFs, and David J. Peterson.
Text
Children Are Bring Harmed - The Lack of Ethics in "Gender Affirming" Medicine
If you are violating one of the principles of human medicine – first do no harm – it may be wise to reconsider your position on ‘gender-affirming treatment’ regardless of how lucrative it is. “Children are being harmed. Young people are being harmed. In many ways, this story is not new. From snake oil to thalidomide, from lobotomies to opioids, medicine has a long history of fake cures and…
View On WordPress
#First Do No Harm#Medical Industry#Medical Profession#No Evidence for Gender Affirmation#Transgender ideology
0 notes
Text






By: SEGM
Published: Aug 13, 2023
Near-zero regret” findings among adults suffer from a critical risk of bias and have low applicability to youth
Recent research published in JAMA Surgery evaluated satisfaction and regret among individuals who had undergone chest masculinizing mastectomy at the University of Michigan hospital. The average patient age at the time of mastectomy was 27 years; no patients who were under age 18 were allowed to participate in the study.
The participants reported high levels of satisfaction and low levels of regret at an average of 3.6 years following mastectomy. The study authors lauded the “overwhelmingly low levels of regret following gender-affirming surgery,” and framed their findings as in conflict with the “increasing legislative interest in regulating gender-affirming surgery,” referring to current legislative attempts to restrict or ban “gender-affirming” procedures for minors. Another group of authors provided an invited commentary on the paper, reinforcing the view held by the study authors, and asserting the presence of a “double standard:” “gender-affirming” mastectomies have come under undue scrutiny by states’ legislators, while other surgical procedures with higher regret rates do not appear to concern legislative bodies.
The study suffers from serious methodological limitations, which render the findings of high levels of long-term satisfaction with mastectomy among adults at a "critical risk of bias"—the lowest rating according to the Risk of Bias (ROBINS-I) analysis. ROBINS-I is used to assess non-randomized studies for methodological bias. The "critical risk of bias" rating signals that the results reported by the study may substantially deviate from the truth. The results also suffer from low applicability to the central issue the study and the invited commentary sought to address, which was whether legislative attempts to regulate “gender-affirming” surgeries are warranted in minors. Unfortunately, these highly questionable findings are misrepresented as certain and highly positive by both the study authors and the invited commentators, several of whom have significant conflicts of interest.
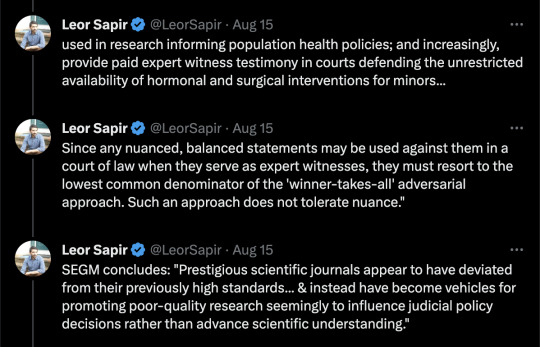
Below, we provide a detailed explanation of the key methodological issues in the study which render its claims untrustworthy and not applicable to the patient population at the center of the debate: youth undergoing gender reassignment. We also comment on the alarming trend: several prestigious scientific journals appear to have deviated from their previously high standards for scholarly work and instead have become vehicles for promoting poor-quality research, seemingly to influence judicial policy decisions rather than advance scientific understanding. We conclude with recommendations about how journal editors can restore the integrity of scientific debate and raise the bar on the quality of published studies in the field of gender medicine.
[ For in-depth analysis, see: https://segm.org/long-term-regret-satisfaction-mastectomy-critical-appraisal ]
SEGM Take-Aways
Although this study reports extremely high rates of satisfaction and low regret, the timeframe in which these outcomes were assessed is insufficient—just 3.6 years post-mastectomy on average. The sample is also highly skewed: 50% of the participants had mastectomies in the last 3.6 of the 30 years. This skewing of the length of time since surgery is expected, given the sharp rise in the number of people (especially adolescents and young adults) identifying as transgender and undergoing chest masculinization mastectomy. It is also a short time in which to assess regret, particularly since one quarter of study participants were younger than age 23 at time of surgery and the median age of first birth in the US is 30 years.
The conclusion of high satisfaction/low regret suffers from a critical risk of bias due to the high non-participation rate, important differences between participants and non-participants, and lack of control group. Problematically, the authors misuse the (critically-biased) results from adults to argue against regulations for irreversible body alternations for minors and do so with a decidedly politicized spin.
The only intellectually honest commentary is that we do not have good knowledge of the likely rates of detransition and regret following chest masculinization mastectomy, nor do we know how many people experience regret but remain transitioned. There is an urgent need for quality research in this area. Previously, detransition and regret rates were considered to be low: they may have indeed been low due to the much more rigorous screenings, or the results may have been biased by the notoriously high dropout rates that plague “regret” research. Regardless, there is now growing evidence of much higher rates of medical detransition.
A recent study from a comprehensive U.S. dataset with no loss to follow-up revealed a 36% medical detransition rate among females within just 4 years of starting hormonal transition. At least two recent studies suggest that average time to regret among recently-transitioned females is about 3-5 years, but there is a wide range. Much less is known about detransition among those who undergo surgery. A growing number of detransitioners now express regret associated with the loss of breastfeeding ability, with one case study detailing breastfeeding grief experienced some 15 years post-mastectomy.
The study and invited commentary exemplify three problematic trends that plague studies emerging from the gender clinics: problematic conflicts of interest of the authors; leveraging scientific journals to disguise politically-motivated pieces as quality research; and a conflicted stance by the gender medicine establishment on surgery for minors. We expand on each briefly below.
Conflicts of interest of study authors and commentators
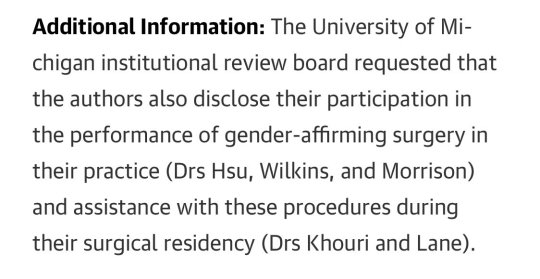
The significant conflicts of interest of the gender clinicians who study and report on the outcomes of “gender-affirming” interventions cannot be overlooked. These clinicians are conflicted financially, since their practices specialize in “gender-affirming” interventions, as well as intellectually. While conflicts of interest among experts are common, such experts should still attempt to be balanced in their discussions and should acknowledge and reflect on their conflicts of interest.
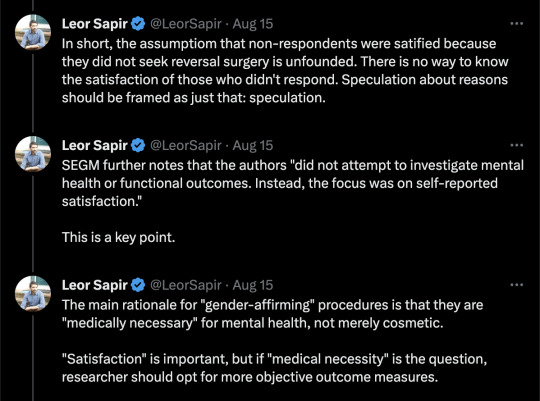
The interpretations of the data in the study is neither rigorous nor balanced, and both the study and the invited commentary have a decidedly political spin. Further, the invited politicized commentary does not disclose that at least one of the authors is a key expert witness opposing states’ efforts to regulate “gender-affirming” surgeries for minors. This role alone precludes the ability to provide a balanced commentary.
There is a fundamental problem with research emerging from gender clinic settings. The same clinicians provide gender-transitioning treatments to individual patients in their practice; serve as primary investigators and custodians of data used in research informing population health policies; and increasingly, provide paid expert witness testimony in courts defending the unrestricted availability of hormonal and surgical interventions for minors.
As a result, such clinicians cannot express nuanced perspectives. Since any balanced statements may be used against them in a court of law when they serve as expert witnesses, they must resort to the lowest common denominator of the "winner-takes-all" adversarial approach. Such an approach does not tolerate nuance. Unfortunately, this approach contributes to the erosion of the quality of the published work in the arena of gender medicine and accelerates loss of trust about the integrity of the scientific process.
Misuse of scientific publications to promote politically-motivated articles disguised as scientific research
That prestigious medical journals now serve as platforms for promoting misleading, politically motivated research that aims to apply a veneer of misplaced confidence in highly invasive, irreversible treatment should worry everyone committed to evidence-based medicine and the integrity of science. Moreover, it impairs our ability to accurately assess and improve the long-term health outcomes of the rapidly growing numbers of gender-diverse and gender-distressed youths.
This is not the first time that a JAMA has been used as a platform for positioning advocacy for “gender-affirming” care as scientific research. In 2022, JAMA Pediatrics published a study that assessed bodily happiness in a group of subjects aged 14-24 three months after chest masculinization mastectomy. Despite the very short follow up and dropout rate of 13%, the authors argued that their findings supported the premise that there was no evidence to suggest that young age should delay surgery. They also asserted that their research would help dispel the misconception that such surgeries are experimental. The editorial commissioned to bolster the authors claims was descriptively titled, “Top surgery in adolescents and young adults-effective and medically necessary.”
Another troubling trend is the misuse of statistical tools to reframe research findings that contradict the author's own position. For example, a well-known study that claimed that access to puberty blockers reduce the risk of suicide disregarded the fact that individuals reporting use of puberty blockers use had twice as many recent serious suicide attempts as their peers who did not use puberty blockers. Like the finding cited above, the doubling of suicide attempts was not statistically significant due to a small underpowered sample—but the magnitude of the effect was striking and should have tempered the authors’ enthusiastic conclusion that puberty blockers prevent suicides. Another recent gender clinic study, widely and positively covered by major media outlets, claimed that puberty blockers and cross-sex hormones led to plummeting rate of depression—even though the rate of depression among youth taking those medications remained demonstrably unchanged. More information about problems with research originating from gender clinics is detailed in this recent analysis.
Gender medicine’s stance on pediatric surgery
More generally, the gender medicine establishment is in a curious state of internal conflict about its stance on “gender-affirming” surgeries for minors. On the one hand, it has become common for advocates of “gender-affirmation” of minors to insist that surgeries for minors are not performed and anyone who suggests otherwise is spreading “scientific misinformation” and “science denialism.” On the other hand, gender clinicians publish mastectomy outcomes for minors in major medical journals, and laud surgeries for minors as “effective and medically necessary.” It is not uncommon for these opposing claims to be made by the same group of researchers and clinicians, as they test various arguments, searching for the "angle" that is most likely to convince judges and juries--and public at large--that scrutiny of the practice of pediatric transitions, which is increasingly occurring in European countries, is not warranted in the United States.
Notably, none of the European countries that are enacting severe restrictions on the use of puberty blockers or cross-sex hormones for minors have ever allowed surgeries for youth under 18. That the U.S. gender affirmation professionals continue to fight regulation of these problematic procedures speaks volumes about how far the U.S. healthcare has drifted when it comes to "gender affirmation" of minors.
Final thoughts
While it is challenging to determine how best to reduce the temperature of the highly politicized nature of the debate in gender medicine, the editors of scientific journals can begin to restore balance by recognizing how far the field has drifted from the standards of quality scientific research, and begin to expand their circle of peer-reviewers to those with diverse views. Inviting those concerned with the state of gender medicine (and not just the practices’ advocates) into the peer-review and commentary process is the first essential step to improve the quality of research published in the field of gender medicine.
--


--

==
The activists are predictably - and consistent with the superficiality of their own ideology - upset that anyone should look below the surface. It seems to be more troubling that anyone would notice the shoddiness of the research, than that the research is shoddy.
If this is supposed to be "healthcare," you would think that they would want the best healthcare, and be more alarmed at the misrepresentations of the study, than by people finding those misrepresentations.
Could it be that this is ideological rather than medical? 🤔
The conflicts of interest and funding sources alone are remarkable.
#Leor Sapir#SEGM#Society for Evidence Based Gender Medicine#double mastectomy#top surgery#gender affirming mastectomy#ideological corruption#ideological capture#medical malpractice#conflict of interest#sarcastic font#medical scandal#medical corruption#gender ideology#genderwang#queer theory#gender affirming care#gender affirming surgery#gender affirming healthcare#medical mutilation#sex trait modification#religion is a mental illness
308 notes
·
View notes
Text
4 notes
·
View notes
Text
i’m going to be alone again september <3 and i have to stay alive until november because im finally getting legal aid for [redacted] sooooo i think i’ll make it into 2024 ! i hope to see you all there :3 <3
#evidence of life#best wishes for all im rooting for you yes you no seriously you i don’t need to know you to root for you good vibes can be sent to /all/#so i’ll probably be more active like mid september and october after that i can’t say#trans rights are human rights autumn#someone /very/ special is getting gender affirming surgery i hope the procedure goes smoothly and healing just as smooth#if you see this mwah !!!!! if you don’t mwah !!!!! i’m so happy for you <333 im so excited to see what’s next for you <333
5 notes
·
View notes
Text
got an ask that I legitimately can't tell if it's trolling or not. Poe's Law.

fictional character may be a war criminal but god forbid I make a joke insinuating he might be a transphobe!
I'm wheezing. there are so many layers here.
-the fact that if you spend 5 seconds googling ER character model datamining you find out that it's false (this is the one thing that would make me say it's deliberate trolling except!! People are this stupid.)
-the idea that having a binary trans person as a lackey means Notorious Pompous Arse With Superiority Complex considers them Valid
-the idea that knowing about the existence of binary trans people is the same as knowing about non-binary people
-the fact that I got this intensely pedantic response to a silly comic I made about pedantry.
If this is a joke, congrats anon I love you you are the funniest person on this website. masterfully crafted. you have distilled tumblr down to its essence.
#enzel.txt#do you really need top contender for World's Shittiest Video Game Dad to affirm your gender#it's just. I can't explain how funny this is.#the idea that someone thinks an offhand joke i made in the tags is a forreal serious headcanon and they have to refute it with 'evidence'#I would absolutely say it's a joke except I have *seen* people say shit like this with their whole chest
3 notes
·
View notes
Text
Fact check: where the fuck did these numbers come from. See
Overall, 25 099 patients (52.3%) were aged 19 to 30 years, 10 476 (21.8%) were aged 31 to 40, and 3678 (7.7%) were aged 12 to 18 years. When stratified by the type of procedure performed, breast and chest procedures made up a greater percentage of the surgical interventions in younger patients, while genital surgical procedures were greater in older patients.
3215 patients (87.4%) aged 12 to 18 years underwent GAS and had breast or chest procedures
405 patients (11.0%) aged 12 to 18 years underwent genital surgery.
Above quotes are for data collected for 2016-2020.
The followup study (which i believe op references) addresses the gap in cisgender affirming care vs trans & gender diverse (TGD) affirming care:
Gender-affirming health care aims to align an individual’s physical gender expression with their intrinsic gender identity. An example is breast reduction for cisgender males with gynecomastia. Recently, there have been increased legislative efforts restricting gender-affirming health care specifically for transgender and gender diverse (TGD) people.1 Proponents of these efforts express concerns that TGD minors may be too commonly using gender-affirming surgical procedures. Given stringent clinical standards for gender-affirming care,2,3 use of gender-affirming surgical procedures by TGD minors is expected to be low. However, there are limited national data; while 1 study provided national estimates, it did not capture minors under the age of 12 years and did not exclude procedures with clinical justifications outside of gender affirmation.4 Therefore, using a national dataset, we evaluated the extent to which TGD minors and adults received gender-affirming surgical procedures in 2019. Additionally, in line with a recent publication from bioethicists to acknowledge that gender-affirming care is used by people of all genders,5 we provide a novel characterization of the relative use of 1 gender-affirming surgery—breast reductions—by TGD and cisgender populations.
Note the following quote is for a single year in the US, 2019.
The rate of undergoing a gender-affirming surgery with a TGD-related diagnosis was 5.3 per 100 000 total adults compared with 2.1 per 100 000 minors aged 15 to 17 years, 0.1 per 100 000 minors aged 13 to 14 years, and 0 procedures among minors aged 12 years or younger (Figure 1). Of gender-affirming surgical procedures identified among adults and minors, 1591 of 2664 (59.7%) and 82 of 85 (96.4%) were chest-related procedures, respectively. Of the 636 breast reductions among cisgender male and TGD adults, 507 (80%) were performed on cisgender males. Of the 151 breast reductions among cisgender male minors and TGD minors, 146 (97%) were performed on cisgender male minors (Figure 2).
Fact check: there were 151 breast reductions in (insured) minors in the US in 2019, of which 146 (97%) were for cisgender male people. Among minors, the only surgeries identified as for gender affirming care specifically, 82 of 85 (96.4%) were chest-related procedures.
Furthermore (and supporting op's point):
In this cross-sectional study of a national insured population in 2019, there were no gender-affirming procedures conducted on TGD minors aged 12 years and younger, and procedures on TGD minors older than 12 were rare and almost entirely chest-related procedures. Additionally, when considering breast reductions among cisgender males and TGD people—a surgery that can be considered gender-affirming among both populations—most were performed on cisgender males. Thus, these findings suggest that concerns around high rates of gender-affirming surgery use, specifically among TGD minors, may be unwarranted. Low use by TGD people likely reflects adherence to stringent standards of gender-affirming care.2,3

When you look up gender affirming surgery it says 'a broad range of procedures that help transgender and non-binary people transition to their gender identity'.
Seems 97% had the same procedure.
#long post#tldr: fact check is partly true. op's numbers are missing some context but they're absolutely correct in pointing out that#gender affirming surgeries for minors in the US are vanishingly rare#and gender affirming surgeries for minors in the US adhere to stringent standards of care#the very fact fewer gender affirming surgery patients regret their surgery post op than ANY OTHER KIND OF SURGERY should be#all the evidence we need. but like it's good to have more data
6K notes
·
View notes
Text
Synopsis: The Cass Review on transgender care has been crucial in the UK, leading to the cessation of prescribing puberty blockers outside of research protocols. However, in the U.S., where the gender-affirming care model is standard, Cass's four-year investigation and final report have been ignored. The newly released Cass Review on transgender care for young people has been pivotal in the UK, where the prescription of puberty blocking drugs outside of research protocols has now ceased. The review concluded that the evidence on use of puberty blockers and hormones for children and teens experiencing gender related distress is wholly inadequate and called for a more holistic approach to care. Parents and their children are being misled in clinics all over the country. There is no evidence that giving puberty blockers followed by hormones and surgery is lifesaving care and there is mounting evidence that the harms outweigh the advantages. ...I'm already hearing from the boards of directors and trustees of some hospital systems who are starting to get nervous about what they've permitted. So I think that's going to accelerate change within American healthcare.
#transgender#puberty blockers#gender affirming care#cass review#mental health#science based evidence
0 notes
Text
The study itself is titled, “Long-Term Regret and Satisfaction With Decision Following Gender-Affirming Mastectomy,” and sought to study the rate of regret and satisfaction after 2 years or more following gender affirming top surgery. The study’s results were stunning - in 139 surgery patients, the median regret score was 0/100 and the median satisfaction score was 5/5 with similar means as well. In other words… regret was virtually nonexistent in the study among post-op transgender people. In fact, the regret was so low that many statistical techniques would not even work due to the uniformity of the numbers: In this cross-sectional survey study of participants who underwent gender-affirming mastectomy 2.0 to 23.6 years ago, respondents had a high level of satisfaction with their decision and low rates of decisional regret. The median Satisfaction With Decision score was 5 on a 5-point scale, and the median decisional regret score was 0 on a 100-point scale. This extremely low level of regret and dissatisfaction and lack of variance in scores impeded the ability to determine meaningful associations among these results, clinical outcomes, and demographic information. The numbers are in line with many other studies on satisfaction among transgender people. Detransition rates, for instance, have been pegged at somewhere between 1-3%, with transgender youth seeing very low detransition rates. Surgery regret is in line with at least 27 other studies that show a pooled regret rate of around 1% - compare this to regret rates from things like knee surgery, which can be as high as 30%. Gender affirming care appears to be extremely well tolerated with very low instances of regret when compared to other medically necessary care.
[...]
The intense conservative backlash, to the point of disputing reputable scientific journals, likely stems from the fact that reduced regret rates weaken a central narrative these figures have championed in legal and legislative spaces. Over the past three years, anti-trans entities have showcased political detransitioners, reminiscent of the ex-gay campaigns from the 1990s and 2000s, to argue that regrets over gender transition and detransition are widespread. Some have even asserted detransition rates of up to 80%, a claim that has been broadly debunked. Yet, research consistently struggles to find substantial evidence supporting this narrative. The rarity of detransition and regret is underscored by Florida's inability to enlist a single resident to bear witness against a lawsuit challenging the state's ban on gender-affirming care.
20K notes
·
View notes
Text
Differences Between "Gender Affirming Care" and Evidence Based Medicine.
TL:DR – The column on the left is activist dogma that has been pushed into the medical system. The column on the right is what proper evidence based care looks like.

View On WordPress
1 note
·
View note
Text

By: Benjamin Ryan
Published: Jan 23, 2025
The most rigorous academic analysis to date of the research backing puberty blockers and cross-sex hormones as treatments for gender-related distress in young people has found it has produced ‘very uncertain’ evidence.
A pair of major new analyses of research into providing gender-transition drugs to adolescents and young adults have indicated that a prevailing orthodoxy in the U.S. medical community — that such treatments are safe and effective for gender-distressed minors — is largely based on “very uncertain” scientific evidence.
The most rigorous such analyses of their kind to date, these new academic papers are the latest reports to cast doubt on the transgender movement’s battle, now on the defensive, to protect minors’ access to ultimately irreversible gender-transition treatments. The new analyses reach the damning conclusion that almost all the research assessing such treatments is decidedly unreliable at anticipating risks and benefits alike, thanks to consistently weak study designs that leave the door wide open for biased and unreliable results.
This sweeping finding echoes the four-year independent assessment of the field of pediatric gender medicine, called the Cass Review, that was commissioned by Britain’s National Health Service and published to great fanfare in April. The nearly 400-page report was anchored on the finding that the field was based on “remarkably weak evidence.”
These critical assessments of the controversial medical practices – which in recent years have been banned for minors in 24 states – stand in direct conflict with a nearly united front among American medical associations who endorse the prescribing of puberty blockers and cross-sex hormones for minors experiencing gender dysphoria, which is distress stemming from a conflict between an individual’s sex and gender identity. Prominent societies such as the American Academy of Pediatrics and the American Medical Association have touted such treatments as effective and even life saving – since, advocates claim, gender treatments prevent suicides.
Dr. Gordon Guyatt, a physician and professor at McMaster University in Ontario, effectively begs to differ, having found that there is no such clear-eyed certainty about the impacts of these treatments on young people. Known as the “godfather of evidence-based medicine,” Dr. Guyatt on Thursday published in the Archives of Disease in Childhood a pair of systematic review papers of pediatric gender medicine that are the first of their kind to pool study findings and conduct meta-analyses regarding particular outcomes among young people who have received these interventions.
One of the analyses examined studies on puberty blockers given to youth with gender dysphoria. The other looked at studies of cross-sex hormones to treat gender dysphoria in adolescents and young adults.
Dr. Guyatt and his colleagues concluded in both papers that there is “considerable uncertainty regarding the effects” of each intervention, given that the available research almost entirely yielded evidence of “very low certainty.” Regarding hormone treatment in particular, the authors concluded that “we cannot exclude the possibility of benefit or harm.” The only research finding they considered to be of “high certainty” was that a small percentage of people who started cross-sex hormones subsequently experienced cardiovascular health events.
“These papers come to the same conclusion as many other evidence syntheses — which is that we do not have a good evidence base to suggest that these treatments are effective,” said Dr. Ronny Cheung, a consultant general pediatrician in London. Dr. Cheung is the lead author of a recent peer-reviewed rebuttal to a white paper spearheaded by Yale University pediatrician Meredithe McNamara that sharply criticized the Cass Review.
The publication of these two papers from Dr. Guyatt is certain to provoke a chorus of disapproval among the many fierce defenders of pediatric gender medicine in America in particular, given their response to the Cass Review. That report has led the UK to ban puberty blockers outside of a promised clinical trial; and it has been broadly cited in litigation in the U.S. by opponents of these interventions for minors. Striking back, a coterie of academics such as Dr. McNamara has mobilized to cast doubt upon the report’s methodology and conclusions.
These champions of pediatric gender medicine have asserted in a string of recent publications, most of which have not been peer reviewed, that, for example, Cass has held these medical interventions to an exceptionally and impossibly high evidentiary standard. Pediatric treatments for all sorts of conditions, some of these champions have pointed out, are routinely based on low-certainty or very-low-certainty evidence (as opposed to moderate- or high-certainty evidence).
“It is true that many treatments in medicine have been, and are, used without a satisfactory evidence base. Sometimes this has led to belated evidence gathering in terms of clinical trials, which have subsequently shown benefit,” Dr. Cheung said in an email. “Equally, others have resulted in disastrous outcomes for patients despite the best intentions and biological plausibility. But it is a logical fallacy to say that because many treatments are given without sufficient evidence base, therefore any treatment without sufficient evidence base should be given.”
Moti Gorin, an associate professor of philosophy at Colorado State University said that given the “complexity and vulnerability” of pediatric gender dysphoria cases, “our standards should be very high.”
The Sun asked the lead authors of all of the recent Cass critiques to comment on Dr. Guyatt’s new papers. The sole respondent was Chris Noone, a lecturer in psychology at the University of Galloway, who argued that the new papers comment “on already identified limitations of research on these interventions related to sample size and comparison groups that are inevitable due to the small population, the impossibility of blinded comparison groups, and the ethics of preventing access to these interventions.”
As he has previously, Dr. Noone criticized the particular tool Dr. Guyatt’s team used to score the quality of the evidence, which he said, “given the aforementioned limitations will automatically lead to a judgment of very low certainty in the evidence.”
“The authors fail to articulate how a study of puberty blockers or hormone therapy for young people with gender dysphoria could ever produce evidence that is considered certain” by this tool, Dr. Noone said.
Dr. Guyatt was not available for comment.
The Trans Turning Point
The stakes have never been higher for the beleaguered and politicized medical field of pediatric gender medicine. The Supreme Court is set to rule, probably in June, on the constitutionality of state bans on gender treatments for minors in a case, first marshalled by the ACLU, in which the Biden Administration challenged Tennessee’s law. And while Donald Trump has yet to make good on his campaign promise to further restrict access to pediatric gender-transition treatment, within hours of his inauguration on Tuesday he signed a sweeping executive order attacking what his administration calls “gender ideology” throughout federal law.
This turning point in the history of transgender advocacy writ large follows a decade of dramatic growth in the population of young people diagnosed with gender dysphoria or otherwise identifying as trans, both in the United States and across the Western World. A research letter out of Harvard published in JAMA Pediatrics on Jan. 6 found about one in 1,000 privately insured 17-year-olds received cross-sex hormones between 2018 and 2022; and recent trends suggest this figure was likely considerably higher at the end of that period, especially among biological girls.
Another paper published Thursday in the Archives of Disease in Childhood reported that between 2011 and 2021, diagnoses of gender dysphoria among adolescents in primary care practices in England surged by more than 50-fold. Following a pattern well documented in the United States, diagnosis rates were similar between biological boys and girls until 2015, at which point they split, until the rate among natal girls was nearly twice that of boys in 2021. By that time, about one in 250 youths had such a diagnosis at age 18. Levels of anxiety, depression, and self-harm were high among this overall population, especially the girls.
The 2020s has seen the publication of a slew of systematic literature reviews – the gold standard of scientific evidence – assessing the quality of research and the resulting reliability of the evidence it produces among studies of gender-transition treatments for youths. All these papers have reached essentially the same conclusion: that the evidence backing prescribing gender-transition medications to minors is wanting and highly uncertain.
Such critical findings have led the health authorities in a swath of Northern and Western European nations, including the UK, to reclassify such treatments as experimental and to sharply restrict access to minors — or to at least consider pulling back on such access. In America, which lacks a comparable centralized health authority, medical-practice standards tend to be set by medical associations; and with the exception of one group representing plastic surgeons, those societies have overwhelmingly held firm in their support of such interventions.
The Evidence-Based Medicine Revolution Confronts Pediatric Gender Medicine
With Dr. Guyatt as one of its talismen, the field of evidence-based medicine emerged during the 1990s as a movement to hold scientific evidence to a higher standard. The goal was to assess the likelihood that the findings of research on any particular subject would actually bear out in clinical practice and that the recommendations based on that evidence were arrived upon in a rigorous and transparent way.
The field, for example, sought to confront the fact that, even if multiple studies reach similar findings, this might be due to the fact that they were all biased in a similar way and not because the results were valid. The type of analyses pioneered by Dr. Guyatt are meant to identify potential sources of bias in scientific research and to separate the evidentiary wheat from the chaff.
“Systematic review procedures block opportunities for cherry-picking studies that support only one side of an issue and help ensure all relevant studies are included,” said James Cantor, a Toronto psychologist and sex researcher who has often served as a paid expert hired by states to aid in defending their bans of this treatment. (Dr. McNamara has conversely often served as a paid expert for the other side. Both she and Dr. Cantor have been criticized for never having treated gender dysphoria in a minor.)
“The methods also work to ensure that all studies get evaluated with the same standards, minimizing opportunities to be more critical or favorable with studies on one side,” Dr. Cantor continued. “Because so many authors have been engaging in exactly these kinds of biased tactics when claiming what the science says about the effects of medicalized transition, the anti-bias methods of systematic reviews are even more important than usual.”
For the new paper on puberty blockers published Thursday, Dr. Guyatt and his colleagues scoured the relevant medical literature and settled on 10 key studies to analyze. Those papers, they concluded, “provided very low certainty evidence,” meaning the investigators had very little confidence the findings reflected the true impact of the treatment on gender dysphoria, global function (how well a person functions in daily life), depression, and bone mineral density.
Dr. Guyatt’s puberty blocker paper also highlighted a review paper out of England that recently called into question the veracity of the oft-repeated claim that the treatments are “fully reversible.”
The cross-sex hormone analysis examined 24 studies in which the average participant was younger than age 26 upon starting treatment (the average age ranged from age 15 to 25). These papers, the authors concluded, largely provided very low certainty evidence regarding such treatment’s impacts on gender dysphoria, global function, depression and bone mineral density changes. One study, which had an untreated comparison group, provided simply “low certainty” evidence—meaning the investigators had merely “limited confidence” it reflected the true effect of the treatment—that taking hormones was linked to a somewhat lower odds of having depression.
The only outcome the investigators considered to be of “high certainty,” meaning they were “very confident” it was close to reflecting the treatment’s true impact in clinical practice, was that there was a 4% rate of cardiovascular events among biological females 7 to 109 months after they started testosterone. That was due to a 2019 research letter by Dutch investigators that found that estrogen use in patients who were born male, with a median age of 30, was tied to a nearly doubled rate of stroke and a greater than fourfold higher rate of blood clots; and that testosterone use in biological females, with a median age of 23, was tied to an almost quadrupled heart attack rate.
Dr. Noone said that particular study could not isolate the impact of hormones on such outcomes, and that the heart disease events might have been driven by higher rates of tobacco smoking among trans people or the impacts of anti-trans stigma.
Overall, the design of the puberty blocker and cross-sex hormones literature reviews meant they could provide insights into the quality of life of youth on the drugs, the study authors concluded. But the analyses could not answer questions about the impacts of the drugs, such as whether quality of life or global function is better among those receiving the medications compared with others who were not.
The Battle Over Research Standards
Many advocates of pediatric gender medicine have insisted that randomized controlled trials, or RCTs, of gender-transition treatments for minors are not ethical—because, they argue, the benefits of these interventions are already so well established.
There is broader consensus among research experts that RCTs might not be feasible. For one, it would be impossible to blind such a study, since it soon becomes obvious to any young person whether they are experiencing physical changes indicative of being on hormones or off of blockers. And youth randomized to an untreated control group might be disinclined to remain in a study they saw as providing them no benefit.
All that said, Dr. Guyatt and his colleagues wrote in their new papers that to understand the impacts of both puberty blockers and cross-sex hormones on young people, “methodologically rigorous studies,” such as those that follow a population over time “are needed to produce higher certainty evidence.” They noted that this includes “RCTs (if ethical)” for blockers in particular.
Thus, the study authors did not insist on “high certainty” evidence, as many critics of the evidence-based approach to assessing pediatric gender medicine often attest, accurately or not, is the topline argument stemming from systematic literature reviews of the field; they called for higher certainty.
Similarly, despite a recent editorial in the New England Journal of Medicine suggesting that the Cass Review set the standard at the RCT level, the British report actually made a more general call for improved methodological rigor in studies of these treatments.
Dr. Guyatt’s papers further argued that physicians counseling young people about receiving these interventions have an obligation to communicate to these patients and their caregivers about the very low certainty of the supporting scientific evidence. Acknowledging the crucial role that patients’ so-called values and preferences play in such clinical decision-making, the investigators called upon the authors of clinical guidelines and policy makers to be transparent about “whose values they prioritize when developing treatment recommendations and policies.”
Supporters of minors’ access to these medications often claim that the rate of regret-based detransitioning — in which someone stops gender-transition drugs and reverts to identifying and presenting as their birth sex — among those who started treatment as minors is extremely low. The Cass Review, though, found that due to limited patient follow-up, the true detransitioning rate is unknown.
Approximately two dozen detransitioners have filed lawsuits against their care providers, often claiming to have suffered irreversible harms to their body. Many of these plaintiffs are represented by a Texas firm established by a quartet of former white-shoe attorneys who set up their practice for the sole purpose of representing detransitioners — a population that they anticipate will only grow given the recent surge in trans identification among adolescents.
The authors of the two new analyses found they could reach no conclusions about rates of regret, anxiety or pelvic pain tied to receiving puberty blockers or hormones. Nor could they reach any conclusions about whether cancer was connected to hormone use or whether puberty blockers were linked to the suicide death rate. The analysis on hormones referenced one two-year U.S. study, published in 2023, in which, among 315 persons who started cross-sex hormones between ages 12 and 20, two died by suicide. Dr. Guyatt’s team deemed this association based on very low certainty evidence.
Nor did these analyses provide any substantial insights into a key concern: fertility. Concerns that providing treatment for childhood gender dysphoria with blockers and hormones might cause infertility have motivated many critics of this medical field to call for a higher quality of evidence than might otherwise be acceptable for pediatric medical interventions.
Leor Sapir, a fellow at the Manhattan Institute who studies pediatric gender medicine, praised Dr. Guyatt’s new analyses as the most “methodologically rigorous systematic reviews” in this field to date. He said that a notable shortcoming of the papers was the limited information they provided about various potential harms of these treatments — a fault he attributed to the wider medical field.
“Gender clinics and clinicians are usually the ones who study medical interventions in this area,” Dr. Sapir said, “And they have little interest or incentive to conduct rigorous, longitudinal studies on the harms of the interventions they adamantly support.”
Following the Science
Dr. Guyatt’s papers are likely to impact ongoing litigation over pediatric gender medicine. Alabama’s attorney general, Steve Marshall, made that evident in a statement to the Sun, when he praised the new papers and said they confirmed “that states like Alabama are on firm footing in restricting these treatments for minors and by encouraging the medical community to finally follow the science itself.”
The papers did not, however, call for such bans, rather for better research. Some of the nation’s major pediatric gender care research hubs are in states that have passed such bans, which threaten to end their research entirely.
As Mr. Marshall’s scathing amicus brief to the Supreme Court for the case over Tennessee’s ban laid bare, records that the attorney general subpoenaed from the World Professional Association for Transgender Health, a prominent transgender medical-activist group, revealed that WPATH suppressed publication of systematic reviews it had commissioned from evidence-based medicine experts at Johns Hopkins University as it developed its 2022 revision to its widely referenced trans-care guidelines.
“It is no great mystery why WPATH acted the way it did,” said Mr. Marshall. In a nod to Dr. Guyatt’s advice for guidelines committees, Mr. Marshall continued: “As these latest systematic evidence reviews confirm, there is woefully insufficient evidence to support WPATH’s strong recommendation that kids be given puberty blockers, cross-sex hormones, and surgeries to treat their gender-related distress.”
Dr. Guyatt’s papers are likely to be attacked due to their funding source. The research was commissioned by the Society for Evidence-based Gender Medicine, or SEGM, which is a collective of physicians and researchers who are skeptical of the evidence supporting pediatric gender medicine and are regarded as an adversary by the transgender rights movement.
The Southern Poverty Law Center has gone so far as to brand SEGM a hate group that traffics in pseudoscience. (The SPLC has itself faced heavy criticism from the right in recent years for expanding its label of hate groups to apply broadly to religious conservatives and other groups that oppose liberal orthodoxy.) However, a three-day conference SEGM held in New York City in the fall of 2023 was almost entirely lacking in politics or any trace of prejudice or animus against transgender people. Instead, it offered a trenchant crash course in evidence-based medicine principles and their application to this field.
That said, SEGM’s critics assert that the organization leans on such intellectual principles as a mere pretext to sow doubt among the public and policymakers alike and, above all, to lend academic credibility to efforts to outright ban these interventions.
In an interview, SEGM cofounder Zhenya Abbruzzese, a health researcher, firmly denied any such political motivation. She further said that Dr. Guyatt’s team kept her organization “at arm’s length” throughout the work on the review papers, and, unlike the Johns Hopkins team’s ultimate arrangement with WPATH, the academic team had full right to publish regardless of the findings.
Speaking to the effort in modern medicine to treat gender dysphoria in young people with blockers and hormones, Ms. Abbruzzese said, “We are operating in the dark. But we don’t have to be.”
She pointed to the robust national health databases in many European nations, in particular in Scandinavia, and argued that researchers could reach at least moderately certain conclusions about the potential impacts of these treatments by conducting research based on those health records.
“It’s time to look at that data in a very rigorous way,” Ms. Abbruzzese said.
Researchers have already conducted such health-database analyses regarding gender transition surgery’s association with mental health outcomes in Swedish adults and cross-sex hormones’ link to suicide deaths in Finnish youths.
Both studies found the interventions were tied to no such benefits.
[ Archive: https://archive.today/GSsQP ]
==
History will judge this as worse than thalidomide. It's been clear for a long time that there's no evidence supporting the effectiveness of these 'treatments.' The evidence in support is of poor quality, while the evidence against shows that these treatments are not only ineffective but also harmful. Unlike thalidomide, which was withdrawn very quickly, the present day scandal continues on despite everything we already know solely because of suicidal empathy.
#Benjamin Ryan#medical scandal#medical malpractice#medical corruption#gender thalidomide#thalidomide#gender affirming care#gender affirming healthcare#gender affirmation#puberty blockers#wrong sex hormones#cross sex hormones#pediatric gender medicine#systematic review#evidence#science#medicine#evidence based medicine#religion is a mental illness
9 notes
·
View notes
Text
lol i made a comment on an instagram reel and i used the phrase "people with uteruses" and somehow it's gotten a few thousand likes and about 20 transphobes being like women?? you mean women?????? someone with a uterus is always a woman??????????? in the comment replies
#so far i'm resisting the urge to respond to any of them#but one of them did click on my profile like a creep#and my profile mentions i'm in med school#and they tried to be like 'you're in med school did you miss anatomy class'#and i really want to respond like#no i didn't miss anatomy#i also didn't miss the multiple lectures and evidence based presentations and patient experience panels that told us multiple times#that gender affirming care saves lives!!!!#get fucked transphobes#my dumb text post
1 note
·
View note
Text


Yet another report found that the Cass Review was dangerously flawed. The Integrity Project at Yale concluded the review "obscures key findings, misrepresents its own data, and is rife with misapplications of the scientific method."
From the new report: "The Review also subverts widely accepted processes for development of clinical recommendations and repeats spurious, debunked claims about transgender identity and gender dysphoria. These errors conflict with well-established norms of clinical research and evidence-based healthcare. Further, these errors raise serious concern about the scientific integrity of critical elements of the report’s process and recommendations."
Read the full report here: https://law.yale.edu/yls-today/news/report-addresses-key-issues-legal-battles-over-gender-affirming-health-care
2K notes
·
View notes
Text
i really want to emphasize the fact that many of these recent bills aimed at denying trans minors gender-affirming care have special exceptions built in to allow for nonessential surgeries on intersex children. they want to make sure doctors can continue pressuring parents into putting their intersex kids through procedures that have no evidence of benefits and are well known to cause harm (cw on these articles for discussions of intersex medical abuse/trauma).
these bills are not designed to protect children, they're designed to eradicate sex and gender diversity. they want to force both trans and intersex people into their binary little boxes and it will do immense harm to both groups.
18K notes
·
View notes
Note
I'm seeing a worrying amount of idiots on tumblr dot com push that "Kamala hates trans women" and I am losing my mind at how they are pushing it, constantly, saying she is a proven transmisogynist, despite it being a complete lie and her actively working behind the scenes to help trans women in prison. Is there like, sources that could help debunk this shit because I'm at my wits end as these people scream and cry and vomit trying to get biden to drop out but then are like "eghhhh still don't wanna vote for a transphobic cop..." when she's NEITHER-
Isn't the internet wonderful? first rule NEVER examine your priors! ALWAYS! hang onto whatever the first hot take you had on a subject to THE DEATH!
"Kamala is Transphobic!" over here in reality
past that trans and LGBT rights groups have been quick to endorse her like
Advocates for Trans Equality
Human Rights Campaign
just today 1,100 LGBT celebrities, lawmakers and leaders endorsed her
“The intersection on the issue of reproductive care and trans care, and the ability of families to be able to have care for their children and their families, is really, again, an intersection around attacks that are on an identity,” -Vice-President Harris, 2023
any ways the root of the idea she's transphobic comes from one case in 2015. Two inmates in the California State Prison system sued to get GRS, which as inmates would have been covered by the Prison system. It's worth noting here, both women got what they wanted, one was paroled and got the surgery covered by California Medicare while the other serving a life sentence was ultimately covered by the prison system.
Two things are important to bear in mind here, 1. Part of the job of California Attorneys General is to defend the state when it is sued, thats the job, 2. It seems early on in the case Harris was not personally aware of it, about 1,000 lawyers work in the Cali AG's office and so the AG cannot be personally aware of every case, and check this quote from the Lambda Legal lawyer handling the case:
“The California AG’s office shifted its handling of these cases significantly after now-Sen. Harris took over,” Renn said. “Initially there was language in briefing for the state that glaringly misunderstood the medical necessity of transition-related medical care and was patently offensive. But then, there was a dramatic change, which seems to have gone along with important policy shifts.”
Link
in 2019 Harris talked about the case and working after it was settled to change the policy of the California State Prison system
"When that case came up, I had clients, and one of them was the California Department of Corrections. It was their policy. When I learned about what they were doing, behind the scenes, I got them to change the policy," Harris said.
"I commit to you that always in these systems there are going to be these things that these agencies do. And I will commit myself, as I always have, to dealing with it," Harris said.
Any ways Harris can consistently spoken out for and supported Trans people, banned the hateful Trans panic defense when she was AG, in the Senate supported the Equality Act, during her 2020 campaign for President she drew attention to the hate crimes against black trans women while holding herself accountable for the 2015 case. As Vice-President she drew fire voicing support for Dylan Mulvaney during the hellish Bud Light backlash. Her Husband Doug was tapped to host the first ever White House Trans Day of Remembrance
basically you're looking at a great ally who clearly supports trans rights, who was involved in a case, which involved two people who got the surgeries they were looking for paid for by the State of California, close to 10 years ago now, there's evidence that both she moved the case in a better direction when she took over it and also that she changed the polices of the state to before more gender affirming.
#kamala harris#election 2024#Trans#trans rights#trans equality#us politics#american politics#politics#misinformation
2K notes
·
View notes
Text
Some have already admitted that KOSA will be used to censor LGBTQ content, especially that which relates to gender-affirming care. 29 Armed with cherry-picked and selectively interpreted studies associating trans content with “anxiety, depression . . . and suicidal behavior,” an ambitious attorney general will claim that “evidence-informed medical information” 30 requires that platforms prohibit minors from viewing such content under KOSA’s duty of care.
They're claiming that KOSA has been fixed. It hasn't been. Please read this detailed explanation of what's wrong with the current version of the bill and then CALL YOUR REPS.
7K notes
·
View notes
Text
🚨 Important new article on gender self-determination as a medical right in CMAJ! I argue that people have a right to gender-affirming care and that many common barriers aren’t justified by evidence. Trans health needs to centre human rights more! 🏳️⚧️
(Audio version.)
#lgbtq#lgbtqia#transgender#trans#trans health#trans healthcare#gender affirming care#gender affirming healthcare#medicine#trans rights#human rights
1K notes
·
View notes