#SEGM
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
1,644 Tumblr posts in 1 second.
Text






By: SEGM
Published: Aug 13, 2023
Near-zero regret” findings among adults suffer from a critical risk of bias and have low applicability to youth
Recent research published in JAMA Surgery evaluated satisfaction and regret among individuals who had undergone chest masculinizing mastectomy at the University of Michigan hospital. The average patient age at the time of mastectomy was 27 years; no patients who were under age 18 were allowed to participate in the study.
The participants reported high levels of satisfaction and low levels of regret at an average of 3.6 years following mastectomy. The study authors lauded the “overwhelmingly low levels of regret following gender-affirming surgery,” and framed their findings as in conflict with the “increasing legislative interest in regulating gender-affirming surgery,” referring to current legislative attempts to restrict or ban “gender-affirming” procedures for minors. Another group of authors provided an invited commentary on the paper, reinforcing the view held by the study authors, and asserting the presence of a “double standard:” “gender-affirming” mastectomies have come under undue scrutiny by states’ legislators, while other surgical procedures with higher regret rates do not appear to concern legislative bodies.
The study suffers from serious methodological limitations, which render the findings of high levels of long-term satisfaction with mastectomy among adults at a "critical risk of bias"—the lowest rating according to the Risk of Bias (ROBINS-I) analysis. ROBINS-I is used to assess non-randomized studies for methodological bias. The "critical risk of bias" rating signals that the results reported by the study may substantially deviate from the truth. The results also suffer from low applicability to the central issue the study and the invited commentary sought to address, which was whether legislative attempts to regulate “gender-affirming” surgeries are warranted in minors. Unfortunately, these highly questionable findings are misrepresented as certain and highly positive by both the study authors and the invited commentators, several of whom have significant conflicts of interest.
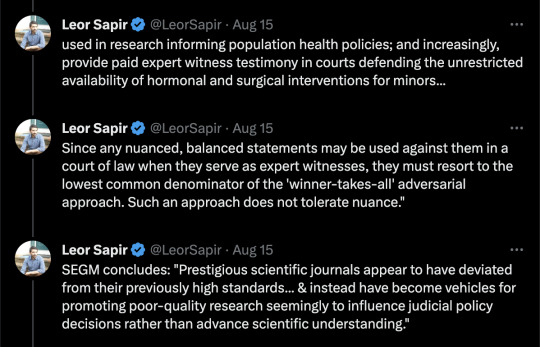
Below, we provide a detailed explanation of the key methodological issues in the study which render its claims untrustworthy and not applicable to the patient population at the center of the debate: youth undergoing gender reassignment. We also comment on the alarming trend: several prestigious scientific journals appear to have deviated from their previously high standards for scholarly work and instead have become vehicles for promoting poor-quality research, seemingly to influence judicial policy decisions rather than advance scientific understanding. We conclude with recommendations about how journal editors can restore the integrity of scientific debate and raise the bar on the quality of published studies in the field of gender medicine.
[ For in-depth analysis, see: https://segm.org/long-term-regret-satisfaction-mastectomy-critical-appraisal ]
SEGM Take-Aways
Although this study reports extremely high rates of satisfaction and low regret, the timeframe in which these outcomes were assessed is insufficient—just 3.6 years post-mastectomy on average. The sample is also highly skewed: 50% of the participants had mastectomies in the last 3.6 of the 30 years. This skewing of the length of time since surgery is expected, given the sharp rise in the number of people (especially adolescents and young adults) identifying as transgender and undergoing chest masculinization mastectomy. It is also a short time in which to assess regret, particularly since one quarter of study participants were younger than age 23 at time of surgery and the median age of first birth in the US is 30 years.
The conclusion of high satisfaction/low regret suffers from a critical risk of bias due to the high non-participation rate, important differences between participants and non-participants, and lack of control group. Problematically, the authors misuse the (critically-biased) results from adults to argue against regulations for irreversible body alternations for minors and do so with a decidedly politicized spin.
The only intellectually honest commentary is that we do not have good knowledge of the likely rates of detransition and regret following chest masculinization mastectomy, nor do we know how many people experience regret but remain transitioned. There is an urgent need for quality research in this area. Previously, detransition and regret rates were considered to be low: they may have indeed been low due to the much more rigorous screenings, or the results may have been biased by the notoriously high dropout rates that plague “regret” research. Regardless, there is now growing evidence of much higher rates of medical detransition.
A recent study from a comprehensive U.S. dataset with no loss to follow-up revealed a��36% medical detransition rate among females within just 4 years of starting hormonal transition. At least two recent studies suggest that average time to regret among recently-transitioned females is about 3-5 years, but there is a wide range. Much less is known about detransition among those who undergo surgery. A growing number of detransitioners now express regret associated with the loss of breastfeeding ability, with one case study detailing breastfeeding grief experienced some 15 years post-mastectomy.
The study and invited commentary exemplify three problematic trends that plague studies emerging from the gender clinics: problematic conflicts of interest of the authors; leveraging scientific journals to disguise politically-motivated pieces as quality research; and a conflicted stance by the gender medicine establishment on surgery for minors. We expand on each briefly below.
Conflicts of interest of study authors and commentators
The significant conflicts of interest of the gender clinicians who study and report on the outcomes of “gender-affirming” interventions cannot be overlooked. These clinicians are conflicted financially, since their practices specialize in “gender-affirming” interventions, as well as intellectually. While conflicts of interest among experts are common, such experts should still attempt to be balanced in their discussions and should acknowledge and reflect on their conflicts of interest.
The interpretations of the data in the study is neither rigorous nor balanced, and both the study and the invited commentary have a decidedly political spin. Further, the invited politicized commentary does not disclose that at least one of the authors is a key expert witness opposing states’ efforts to regulate “gender-affirming” surgeries for minors. This role alone precludes the ability to provide a balanced commentary.
There is a fundamental problem with research emerging from gender clinic settings. The same clinicians provide gender-transitioning treatments to individual patients in their practice; serve as primary investigators and custodians of data used in research informing population health policies; and increasingly, provide paid expert witness testimony in courts defending the unrestricted availability of hormonal and surgical interventions for minors.
As a result, such clinicians cannot express nuanced perspectives. Since any balanced statements may be used against them in a court of law when they serve as expert witnesses, they must resort to the lowest common denominator of the "winner-takes-all" adversarial approach. Such an approach does not tolerate nuance. Unfortunately, this approach contributes to the erosion of the quality of the published work in the arena of gender medicine and accelerates loss of trust about the integrity of the scientific process.
Misuse of scientific publications to promote politically-motivated articles disguised as scientific research
That prestigious medical journals now serve as platforms for promoting misleading, politically motivated research that aims to apply a veneer of misplaced confidence in highly invasive, irreversible treatment should worry everyone committed to evidence-based medicine and the integrity of science. Moreover, it impairs our ability to accurately assess and improve the long-term health outcomes of the rapidly growing numbers of gender-diverse and gender-distressed youths.
This is not the first time that a JAMA has been used as a platform for positioning advocacy for “gender-affirming” care as scientific research. In 2022, JAMA Pediatrics published a study that assessed bodily happiness in a group of subjects aged 14-24 three months after chest masculinization mastectomy. Despite the very short follow up and dropout rate of 13%, the authors argued that their findings supported the premise that there was no evidence to suggest that young age should delay surgery. They also asserted that their research would help dispel the misconception that such surgeries are experimental. The editorial commissioned to bolster the authors claims was descriptively titled, “Top surgery in adolescents and young adults-effective and medically necessary.”
Another troubling trend is the misuse of statistical tools to reframe research findings that contradict the author's own position. For example, a well-known study that claimed that access to puberty blockers reduce the risk of suicide disregarded the fact that individuals reporting use of puberty blockers use had twice as many recent serious suicide attempts as their peers who did not use puberty blockers. Like the finding cited above, the doubling of suicide attempts was not statistically significant due to a small underpowered sample—but the magnitude of the effect was striking and should have tempered the authors’ enthusiastic conclusion that puberty blockers prevent suicides. Another recent gender clinic study, widely and positively covered by major media outlets, claimed that puberty blockers and cross-sex hormones led to plummeting rate of depression—even though the rate of depression among youth taking those medications remained demonstrably unchanged. More information about problems with research originating from gender clinics is detailed in this recent analysis.
Gender medicine’s stance on pediatric surgery
More generally, the gender medicine establishment is in a curious state of internal conflict about its stance on “gender-affirming” surgeries for minors. On the one hand, it has become common for advocates of “gender-affirmation” of minors to insist that surgeries for minors are not performed and anyone who suggests otherwise is spreading “scientific misinformation” and “science denialism.” On the other hand, gender clinicians publish mastectomy outcomes for minors in major medical journals, and laud surgeries for minors as “effective and medically necessary.” It is not uncommon for these opposing claims to be made by the same group of researchers and clinicians, as they test various arguments, searching for the "angle" that is most likely to convince judges and juries--and public at large--that scrutiny of the practice of pediatric transitions, which is increasingly occurring in European countries, is not warranted in the United States.
Notably, none of the European countries that are enacting severe restrictions on the use of puberty blockers or cross-sex hormones for minors have ever allowed surgeries for youth under 18. That the U.S. gender affirmation professionals continue to fight regulation of these problematic procedures speaks volumes about how far the U.S. healthcare has drifted when it comes to "gender affirmation" of minors.
Final thoughts
While it is challenging to determine how best to reduce the temperature of the highly politicized nature of the debate in gender medicine, the editors of scientific journals can begin to restore balance by recognizing how far the field has drifted from the standards of quality scientific research, and begin to expand their circle of peer-reviewers to those with diverse views. Inviting those concerned with the state of gender medicine (and not just the practices’ advocates) into the peer-review and commentary process is the first essential step to improve the quality of research published in the field of gender medicine.
--


--

==
The activists are predictably - and consistent with the superficiality of their own ideology - upset that anyone should look below the surface. It seems to be more troubling that anyone would notice the shoddiness of the research, than that the research is shoddy.
If this is supposed to be "healthcare," you would think that they would want the best healthcare, and be more alarmed at the misrepresentations of the study, than by people finding those misrepresentations.
Could it be that this is ideological rather than medical? 🤔
The conflicts of interest and funding sources alone are remarkable.
#Leor Sapir#SEGM#Society for Evidence Based Gender Medicine#double mastectomy#top surgery#gender affirming mastectomy#ideological corruption#ideological capture#medical malpractice#conflict of interest#sarcastic font#medical scandal#medical corruption#gender ideology#genderwang#queer theory#gender affirming care#gender affirming surgery#gender affirming healthcare#medical mutilation#sex trait modification#religion is a mental illness
308 notes
·
View notes
Text

Fuck SEGM fuck Genspect, they are enemies of freedom and the working class
#Fuck SEGM fuck Genspect#they are enemies of freedom and the working class#segm#genspect#anti lgbtq#lgbtqia#lgbtqia+#pride month#pride#lgbtqia+ solidarity#lgbtqia+ community#ausgov#politas#auspol#tasgov#taspol#australia#fuck neoliberals#neoliberal capitalism#anthony albanese#albanese government#anti homophobia#homophobia#class war#anti imperialism#anti capitalism#anti colonialism#anti cop#anti colonization#eat the rich
0 notes
Text

Ödeme ve Elektronik Para Kuruluşları Sektörü Sürdürülebilirlik Çalıştayı Yaptı Türkiye Ödeme ve Elektronik Para Kuruluşları Birliği (TÖDEB) ve Sürdürülebilir Eğitim Gelişim ve Mükemmellik Derneği (SEGM) iş birliği ile “Ödeme ve Elektronik...
0 notes
Text

Ödeme ve Elektronik Para Kuruluşları Sektörü Sürdürülebilirlik Çalıştayı Yaptı Türkiye Ödeme ve Elektronik Para Kuruluşları Birliği (TÖDEB) ve Sürdürülebilir Eğitim Gelişim ve Mükemmellik Derneği (SEGM) iş birliği ile “Ödeme ve Elektronik...
0 notes
Text
Ödeme ve Elektronik Para Kuruluşları Sektörü Sürdürülebilirlik Çalıştayı Yaptı Türkiye Ödeme ve Elektronik Para Kuruluşları Birliği (TÖDEB) ve Sürdürülebilir Eğitim Gelişim ve Mükemmellik Derneği (SEGM) iş birliği ile “Ödeme ve Elektronik...
0 notes
Text

Ödeme ve Elektronik Para Kuruluşları Sektörü Sürdürülebilirlik Çalıştayı Yaptı Türkiye Ödeme ve Elektronik Para Kuruluşları Birliği (TÖDEB) ve Sürdürülebilir Eğitim Gelişim ve Mükemmellik Derneği (SEGM) iş birliği ile “Ödeme ve Elektronik...
0 notes
Text
Go Give caWsbar some Love and a Donation. :)
Given the general public rise in awareness of gender ideology and how it affect them and their children it would be good to be able to find resources to help fill in the blanks. The Canadian Women’s Sex Based Rights – caWsbar – Website is good place to start. Here are their 10 principles: Parents with Inconvenient Truths About Trans – a substack dedicated to telling the stories and…

View On WordPress
#Against Gender Idology#caWsbar#Education for the recently peaked#Parents with Inconvenient Truths about Trans (PITT)#SEGM
0 notes
Text
Denmark latest European country turning away from transgender mutilation of children | The Most Revolutionary Act
The news that Denmark is moving away from the so-called “affirmative model of care” approach to youth struggling with gender dysphoria exposes, once again, how utterly radical and out of step with the rest of the world Canada and blue America are on the issue of “sex changes” for minors. Predictably, mainstream media outlets have ignored this development entirely – there is no press coverage that…
View On WordPress
0 notes
Text
By: SEGM
Published: Jun 11, 2023
A new peer-reviewed article, “Transition Regret and Detransition: Meaning and Uncertainties,” published in the Archives of Sexual Behavior, reviews clinical and research issues related to transition regret and detransition. The article emphasizes that “although recent data have shed light on a complex range of experiences that lead people to detransition, research remains very much in its infancy,” and there is currently “no guidance on best practices for clinicians involved in their care.”
The author, Dr. Jorgensen, notes that the term “detransition” can hold a wide array of possible meanings for transgender-identifying people, detransitioners, and researchers, leading to inconsistencies in its usage. Although regret and detransition overlap in many people, not everyone who regrets their transition takes steps to detransition and conversely, not all of those who detransition regret their transition. Proponents of the “gender-affirming care” model typically focus on the latter group who are driven to detransition by external forces such as discrimination, lack of support from family and friends, or difficulty accessing health care. Euphemisms such as “gender-identity journey” and “dynamic desires for gender-affirming medical interventions” have been used to describe this process.
But the author highlights studies and personal testimonies of detransitioners who do deeply regret their transition, mourn the physical changes made to their bodies, and feel betrayed by the clinicians and medical institutions that offered hormones and surgery as antidotes to their gender confusion and distress. For this group of young people, internal factors such as “worsening mental health or the realization that gender dysphoria was a maladaptive response to trauma, misogyny, internalized homophobia, or pressure from social media and online communities,” were the primary drivers of their decision to detransition.
As the author highlights, a consistent theme in studies and personal testimonies of detransitioners is that there are major gaps in the quality and accessibility of medical and mental healthcare: “Many detransitioners reported not feeling properly informed about health implications of treatments before undergoing them (Gribble et al., 2023; Littman, 2021; Pullen Sansfaçon et al., 2023; Vandenbussche, 2022). Likewise, many felt that they did not receive sufficient exploration of preexisting psychological and emotional problems and continued to struggle post-transition when they realized gender transition was not a panacea (Littman, 2021; Pullen Sansfaçon et al., 2023; Respaut et al., 2022; Sanders et al., 2023; Vandenbussche, 2022). Despite ongoing medical needs, most patients did not maintain contact with their gender clinic during their detransition.” Detransitioners report wanting more information about how to safely stop hormonal therapies and surgical reversal or restorative options, but few clinicians are sufficiently knowledgeable about these issues to manage their care.
The author notes that our ability to predict who will be helped by transition-related medical interventions and who will be harmed by them is limited and we currently have no idea how many of the young people transitioning today will eventually come to regret their decision: “no one is systematically tracking how many young people regret transition or, for that matter, how many are helped by it.” However, the increasing number of detransitioners publicly sharing their experiences suggest that historical studies citing low rates of regret are no longer applicable. Moreover, these studies suffered serious methodological flaws that would tend to underestimate the true rates of regret including high rates of attrition and narrow definitions of regret.
More recent studies that have included the current case mix of predominantly adolescent-onset gender dysphoria suggest that up to 30% of those who undergo medical transition may discontinue it within only a few years (Roberts et al., 2022). It is likely that a number of them will experience significant regret over lost opportunities and permanent physical changes.
So how did we get here?
The author suggests that less restrictive eligibility criteria for accessing transition-related medical interventions under the gender-affirmation and informed consent models, coupled with the rapid rise of adolescents and young adults presenting to gender clinics, many of whom suffer from complex mental health problems and neurodiversity, has important implications for the incidence of transition regret and detransition. Under these models of care, standard processes of differential diagnosis and clinical assessment are seen as “burdensome, intrusive, and impinging on patient autonomy.” Moreover, the author points out that hormonal therapies and surgery are now conceptualized as a “means of realizing fundamental aspects of personal identity or ‘embodiment goals,’ in contrast to conventional medical care, which is pursued with the objective of treating an underlying illness or injury to restore health and functioning.”
Furthermore, adolescents and young adults might not be mature enough to appreciate the long-term consequences of their decisions about the irreversible medical interventions used to achieve “embodiment goals,” and/or their capacity to give informed consent may be limited by comorbid mental health problems or neurodevelopmental challenges. Additionally, “feelings of profound grief about lost opportunities and negative repercussions of transition might not be fully captured by framing the emotional experience in terms of regret” because “regret is an emotion that is unique in its relation to personal agency (Zeelenberg & Pieters, 2007), but the exercise of personal agency in the transition process might have been limited for people who began transition as minors, whose decision-making capacity was compromised by mental illness, or who were not fully informed of known and potential adverse health implications.”
The author offers some suggestions for how detransition may be prevented and inappropriate transitions avoided:
Improving the process of informed consent.
Prioritizing treatment of co-occurring social, developmental and psychological problems.
Using precise language about medical interventions.
Helping young people expand their understanding of what it means to be a man or woman.
Being transparent about the quality of evidence supporting medical interventions and the uncertainty about long-term harms.
The author ends by emphasizing that when clinical cases are complicated by a lack of knowledge about the natural trajectory of the condition and a paucity of evidence supporting treatment options, “minimizing iatrogenic harm requires application of cautious, thoughtful clinical judgement, meticulous examination of the data that are available, as well as a willingness to change practice in the face of new evidence.”
Jorgensen calls on the gender medicine community to “commit to conducting robust research, challenging fundamental assumptions, scrutinizing their practice patterns, and embracing debate.”
--
Read more about the phenomenon of detransition:
Boyd I, Hackett T, Bewley S. Care of Transgender Patients: A General Practice Quality Improvement Approach. Healthcare. 2022; 10(1):121. https://doi.org/10.3390/healthcare10010121
D’Angelo, R. (2020). The man I am trying to be is not me. The International Journal of Psychoanalysis, 101(5), 951–970. https://doi.org/10.1080/00207578.2020.1810049
Entwistle, K. (2020). Debate: Reality check – Detransitioner’s testimonies require us to rethink gender dysphoria. Child and Adolescent Mental Health, camh.12380. https://doi.org/10.1111/camh.12380
Expósito-Campos, P. (2021). A Typology of Gender Detransition and Its Implications for Healthcare Providers. Journal of Sex & Marital Therapy. https://www.tandfonline.com/doi/abs/10.1080/0092623X.2020.1869126
Hall, R., Mitchell, L., & Sachdeva, J. (2021). Access to care and frequency of detransition among a cohort discharged by a UK national adult gender identity clinic: Retrospective case-note review. BJPsych Open, 7(6), e184. https://doi.org/10.1192/bjo.2021.1022
Littman, L. (2021). Individuals Treated for Gender Dysphoria with Medical and/or Surgical Transition Who Subsequently Detransitioned: A Survey of 100 Detransitioners. Archives of Sexual Behavior. https://doi.org/10.1007/s10508-021-02163-w
Marchiano, L. (2021). Gender detransition: A case study. Journal of Analytical Psychology, 66(4), 813–832. https://doi.org/10.1111/1468-5922.12711
Roberts, C. M., Klein, D. A., Adirim, T. A., Schvey, N. A., & Hisle-Gorman, E. (2022). Continuation of Gender-affirming Hormones Among Transgender Adolescents and Adults. The Journal of Clinical Endocrinology & Metabolism, 107(9), e3937–e3943. https://doi.org/10.1210/clinem/dgac251
Vandenbussche, E. (2021). Detransition-Related Needs and Support: A Cross-Sectional Online Survey. Journal of Homosexuality, 20. https://doi.org/10.1080/00918369.2021.1919479
==
Genderists often say things like "detransition/regret is rare" and "detransition is only due to discrimination." These run in the opposite direction to genderist assertions, as this means "detransition/regret due to discrimination is rare."
Most of the numbers they cite are either poorly sourced as mentioned above, or worse, from the days of "watchful waiting," where transition only came at the end of a comprehensive care process; a completely different model.
Not only is it dishonest, given they regard watchful waiting, or anything else as "harmful" and "gatekeeping," but the low regret rate actually supports that more cautious, thoughtful process.
And besides, claiming to know the success rate under the "affirming"/"informed consent" models is itself dishonest too. Detransitioners are not going to rush back to the same doctors who facilitated their mistake. Especially in a climate where they'll be blamed or vilified.
#SEGM#Society for Evidence Based Gender Medicine#transition regret#regret#detransition#detrans#gender ideology#queer theory#gender affirming care#medical transition#medical malpractice#medical mutilation#medical corruption#religion is a mental illness
107 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
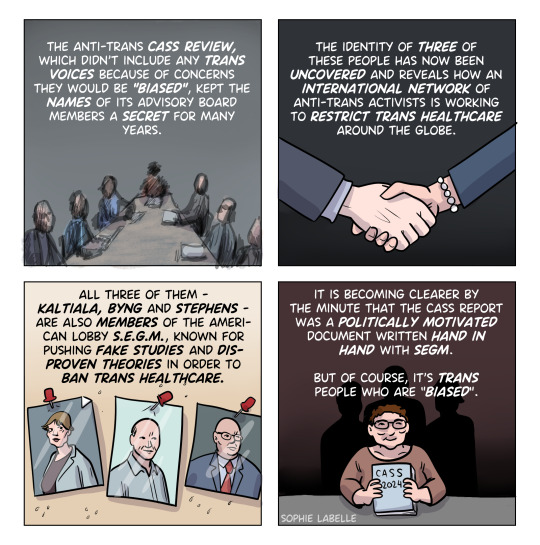
In a major move, the Southern Poverty Law Center has formally designated the anti-transgender pseudoscience organizations Genspect and the Society for Evidence-Based Gender Medicine as anti-LGBTQ+ hate groups. This designation is part of the civil rights organization’s latest release of its “Year In Hate & Extremism” report, which tracks hate groups and extremist groups throughout the United States. Members of these and other anti-LGBTQ+ organizations listed have played significant roles in the passage of anti-LGBTQ+ legislation and policy by concealing and underplaying their ties to anti-LGBTQ+ extremism. Most recently, members of the newly designated hate group, Society for Evidence-Based Gender Medicine, helped advise the Cass Review in the United Kingdom, which has led to the criminalization of possession of some forms of transgender care there and is currently being used to argue for heavy restrictions in the United States.
The designation is significant, placing these organizations alongside other extremist groups like the Alliance Defending Freedom and the Family Research Council—Christian fundamentalist organizations pushing anti-LGBTQ+ policies in the United States and internationally. Justifying the new designations, the report points to conferences held by these organizations that featured “expert witnesses” employed by the Alliance Defending Freedom to target LGBTQ+ people in the United States. It also highlights an investigative analysis that discovered the organizations were at the center of a massive “anti-LGBTQ pseudoscience network.” The analysis further determined that in the case of SEGM, the organization’s funding stream included Koch Foundation money funneled through the Edward Charles Foundation. Notably, SEGM shared funding streams with right-wing Christian groups like the Alliance Defending Freedom and the Family Research Council.
[...] The latest report from the Southern Poverty Law Center (SPLC) indicates that in 2023, the number of anti-LGBTQ+ hate groups increased by one-third to 86 groups, the highest number ever tracked by the organization. According to the group, this surge is primarily due to the rise of “family policy councils” that push right-wing Christian agendas and members of anti-LGBTQ+ pseudoscience networks that often share the same goals. “As in previous years, the anti-LGBTQ policy push was grounded in demonizing LGBTQ people and using pseudoscientific claims about LGBTQ people, but the weaponization of pseudoscience as a tool of trans suppression and the targeting of fundamental freedoms like free speech, expression, and assembly through book and drag bans has become a more prominent feature in recent years,” the report says, highlighting the increasing use of organizations weaponizing disinformation to target transgender people.
The SPLC has given anti-LGBTQ+/anti-trans extremist organizations such as SEGM, Genspect, Do No Harm, and Awake Illinois the hate group designations as part of their 2023 review of hate and extremism.
#SPLC#LGBTQ+#Transgender#SEGM#Genspect#Cass Review#Anti Trans Extremism#Hate Groups#Anti LGBTQ+ Extremism#Society For Evidence Based Gender Medicine#CAPTAIN Report#Awake Illinois#Do No Harm#Southern Poverty Law Center
4 notes
·
View notes
Text
MO AG analysis part 2
part 1
So I'm doing this largely because most of the people pushing hateful legislation are citing the same sources, which means the mistakes that one of them makes will be repeated for all of them. Calling them mistakes is generous, though, because in the vast majority of circumstances, they are twisting the words of researchers for their purposes.
Either way, anyone who actually reads the articles these people misrepresent has the opportunity to take the intellectual high ground. It doesn't mean much when we're dealing with legislators who are pushing whatever agenda they're paid to push, and the only thing that can change their minds is green, but it's important to point out that the science is not on their side and they're being grimy and dishonest.
Okay to continue:
the sources under footnote 3 and 4 don't reveal much interesting information. More quotes taken out of context, what's important to get from them is that when they say there's a lack of evidence for benefits of puberty blockers in children, what they actually mean is there's a lack of research. There's a lack of evidence that they harm anyone, too. Both the Swedish study (Socialstyrelsen NBHW 2022, the AG's order links a PDF directly) and the US Agency for Healthcare Research and Quality (AHRQ, footnote 4, link in the AG's order and the website is a little confusing but on that page they have a full PDF discussing what they call "key questions") are saying there is not enough research, not that there are no benefits to the treatment.
One thing that is important to bring up about the Sweden study is that despite the way that the AG's order reads, the Swedish researchers aren't calling for a stop of treatment or anything like that. The language actually seems like it was used to inspire more funding and more studies. They call for treatment in exceptional cases, which prolonged identification as trans/or another gender aside from one's sex assigned at birth and stress from puberty are sufficient. So once again, another issue with another source that transphobic extremists have been using against us.
Footnote 5 is where it starts to get juicy again. Specifically, the AG says "And Finland has openly declared these interventions to be 'an experimental practice.'" The Finnish document (linked here). The full paragraph that mentions experimental practices:
"In light of available evidence, gender reassignment of minors is an experimental practice. Based on studies examining gender identity in minors, hormonal interventions may be considered before reaching adulthood in those with firmly established transgender identities, but it must be done with a great deal of caution, and no irreversible treatment should be initiated. Information about the potential harms of hormone therapies is accumulating slowly and is not systematically reported. It is critical to obtain information on the benefits and risks of these treatments in rigorous research settings."
A lot of this document talks about how the scientific work has not been done/or done to standards necessary by the Finnish government. Different people have different opinions on the work that has been done (when it comes to trans children), which I'll discuss when it comes up in the AG's order. Also, for the order calling for restrictions on both minors and adults, most of the complaints the AG puts out are related to minors.
In this case, what the Finnish government is saying is that there's no guidelines about dosages, what to expect, when to start, when to stop, etc. And personally, I think with gender-affirming care, there's not going to be. There's not one way to approach transitioning, or feeling comfortable in your body, or whichever route someone takes. There's not one kind of gender dysphoria. (There's not even two kinds, if you were thinking about it as ftm or mtf.) With many other types of medical treatment, there's protocols for these things. For example, a patient presents with depression. The doctor has a few options: therapy, antidepressants, etc. If they choose antidepressants, the doctor looks at the demographics: some are not indicated for children and others are specifically only for children, they tend to start males with TCAs and females with SSRIs though they don't have to, there may be other factors to take into account as well like other medical conditions or other medications, or often if a member of your family has had success with a certain medication, they'll start with that one. When they pick a medication, there will be a recommended dosage, especially for children where dosages are related to weight, but they start low and slow and titrate upwards until they hit the maximum recommended dose and if the medication doesn't work, they switch. They determine efficacy by interviews, there are assessments to determine if someone's mood is improving. With treatment for gender dysphoria for minors, there's neither "this symptom = this treatment" nor "symptom persists = treatment is not working." That barely works for trans adults, either, and this is an issue inherent with medicalizing gender, and is a really big topic to tackle and needs its own post, at minimum.
Treatment is therefore experimental in the sense that the doctor and patient need to experiment with what works and what does not. It will be different for every patient and a specific set of procedures cannot be used.
Anyway, I'm not going to do a deep dive into what Finland requires for medical research, but it seems like they have higher expectations than the studies that have been done. Even so, they acknowledge that patients that need it should still be treated while research is being done. This is contrary, yet again, to the AG's order and all of the bills banning gender-affirming care for minors.
Footnote 6 is what I've been waiting for! This is the real tea. So this source is an article written this year (Abbruzzese et al. 2023, open source article linked here). It's a critique of the "Dutch studies" that pop up again and again in the discussion of gender-affirming care for minors. The Dutch studies are research done by Annelou de Vries, mostly in the 1990s I believe, that gave minors gender-affirming care and followed up with them later. It's one of the only studies cited for a longitudinal view of use of puberty blockers in the treatment of trans minors. There's quite a few articles based on this research, including ones these authors mention from I believe 1997, 2012, and 2014. Also important to note, this article is actually a response to de Vries, who had written an article in response to a previous critique issued by the same authors. So, Studies done by de Vries (and colleagues) between the 1990s and 2020s -> Levine et al. 2022(a in the sources of this article), a review they wrote to the collection of research -> de Vries, A.L.C. 2022 (written in direct response to Levine et al. 2022) -> then Abbruzzese et al. 2023, the article being discussed here as the MO AG's Footnote 6
Levine et al. and Abbruzzese et al. are the same three authors, they just switched who got first author.
And who these authors are is extremely important.
Stephen Levine is the only actual academic of the trio. This is probably why he was first author on the article. Levine is in the Department of Psychiatry, Case Western Reserve University in Ohio.
Julia Mason is a pediatrician at Calcagno Pediatrics, also in Ohio. (apparently also part of the SEGM, which I talk about below)
E. Abbruzzese is the really interesting one. Abbruzzese is part of the Society for Evidence-Based Gender Medicine.
The SEGM is a hate group disguised as a medical association. Anyone who reads that title and doesn't know better wouldn't think they were anything but reputable.
Their website states that they don't have any political agenda or affiliations, and this is their response to a question "Does SEGM support LGBTQ people?"
SEGM believes that LGBTQ people should be treated with dignity and afforded the same human rights and protections as all other individuals. Many of the professionals collaborating within SEGM are lesbian and gay, and a number have loved ones who identify as transgender.
The field of pediatric gender medicine is currently engulfed in an intense international scientific debate. Although most are debating in good faith, some have met SEGM’s position of concern over the unknown risk/benefit profile of youth gender transitions with accusations of “transphobia.” If such a standard is to be applied, then entire countries that have expressed the same concern as SEGM, including the UK, Norway, Finland, and Sweden—the first country to recognize transgender people’s legal status—would be similarly labeled “transphobic.” Resorting to ad hominem attacks is often a reflection of weakness in one’s own argument, and we believe such tactics detract from the quality of scientific debate.
In recent months, we have seen a shift toward more civil debates, and we have been grateful to see our position of concern fairly represented by The Economist, The Associated Press, Newsweek, Wall Street Journal, Medscape, NPR, Kaiser Health News, and a growing number of other news sources.
Idk, I wonder why people are calling you transphobic if you're not?
They're citing all the sources that extremists use to delegitimize gender-affirming care for youths. They're using the same language as the extremists. They're misinterpreting the same Scandinavian releases. Hmm.
Also, the news outlets mentioned in the last paragraph have links to articles. The Economist: It's behind a paywall and I immediately got frustrated when I couldn't get past it, but 1. the article's title is:
"Questioning America’s approach to transgender health care
Some paediatricians want a re-examination of the professional guidance"
American, huh? We don't spell it "paediatrician." So, we've got a non-American viewpoint being presented as an American one. Not to mention the divisive nature of the title. and 2. the parts I can read are already insidious. They're telling a story of a 15 year old who gets offered both top surgery and hormones within "a couple of visits" to a therapist and. in what world? not the one we currently get healthcare in. Sure, we've gotten more accepting now, but I still call bullshit. Not to mention the insidiousness of this quote: “I just didn’t know what ‘gender-affirming care’ meant. It sounds so beneficial and positive.”
The Associated Press: This article is actually well-written. They did a good job of presenting the multiple angles of the issue in the very few paragraphs they had to write it. Apparently the author no longer works for the AP. The only thing that worries me is that the part about the SEGM is at the end, so it's the last thing someone would think about if they read the whole article. The article is actually about a paper published in the journal Pediatrics that followed trans children and found that, surprising no trans person, their identities stick. The part about SEGM highlights some of SEGM's awful lines of thinking:
The Society for Evidence-Based Gender Medicine, a nonprofit group of health professionals who are concerned about medical transition risks for minors, said other evidence shows high numbers of kids outgrow transgender identities by puberty or adulthood. Some researchers point to flaws in that data.
Dr. William Malone, an advisor to the group, said the new study appears to reinforce concerns “that early social gender transition may cement a young person’s transgender identity, and lead minors on the path to eventual medicalization, with all its inherent risks and uncertainties.”
The SEGM thinks that social transitioning solidifies what might not be a solid identity. I mean one of the purposes of social transitioning is to determine whether being another gender in public full time is what someone wants, whether it alleviates some or all of their dysphoria. they don't want any medical treatments because a kid might be unsure, but they don't want the kid to socially transition to find out if they're sure.
My tearing into SEGM will continue in the next part, and then I'll start actually discussing the article, but I'm going to try to actually get something relevant to my schoolwork done tonight.
Part 3
1 note
·
View note
Text
ok just a quick Q because I keep seeing stuff that makes me wonder if a lot of people think differently than me or i'm just encountering the few cases that disagree in the wild

#valangel#hazbin hotel valentino#hazbin hotel angel dust#happy days in hell (hazbin tag)#i just saw someone being like 'they're not in the studio so is this angel's room?' or smth yesterday#and i was like. you don't think this is a Literally Happening Now segme- oh huh i have seen a couple people thinking that#and I contemplated making a post just pointing out 'here's why this is (imo but i'm pretty confident) a flashback' but then yknow#wanted to make sure i wasn't Making Up A Guy to some extent lol
14 notes
·
View notes
Text
Picked up the Pandora Principle for a thrid time for reading on my trip and Yeah. its's still the best book ever
#i'm learning to appreciate the parts where the focus isnt on spock or saavik#previous readthroughs i was so checked out during Bobby Harper and Obo segme#-nts#like WHEN are we getting to the SAAVIK FACTORY#but i ubderstand their purpose now and think theyre fine#and everything with the enterprise crew is still excellent#and spock and saavik specific stuff is still GOD TIER#ah saavik. the most complicated girl of all time.
7 notes
·
View notes
Text
Hey, @staff @support what the fuck is this ad? Why is an ad about SEGM, a well known anti-trans lobbyists group which is oft cited by transphobic legislation, on my dash?

"Queerest place on the internet" doesn't stop you from advertising for these assholes it seems
It links to this article btw: link. And for contrast, SEGM's Wikipedia page: link
#scream into the aether#can you tell I'm irate? cause I'm irate#i know the article is milquetoast as fuck about SEGM but that's kinda the problem. they're not milquetoast#also it's so frustrating that you can't report ads anymore#or even link to them or anything. just 'Go Ad-Free' cause that's the only important thing to Tumblr
3 notes
·
View notes
Text
TRAUM IS INSANE bc i keep remembering verse's posts about guda not seeing shit clearly/they have trouble differentiating people smth like that and it applies to Servants especially where they used something like the Saber-face example where Morgan is "Saber-face" even as she has white hair blue eyes compared to Artoria idk i vaguely remember the post but VERSE IS ALWAYS RIGHT AGHH
#reading traum like oughh my god this reminds me of one of tumblr user verse versegm segm THE GUDA GUY post's...#fgo#guda
3 notes
·
View notes
Text
reminder btw that segm are best buds with david "jews are lizard people" icke
5K notes
·
View notes