
Statistics
We looked inside some of the posts by sunflorable and here's what we found interesting.
Average Info
Notes Per Post
155K
Likes Per Post
100K
Reblog Per Post
55K
Reply Per Post
91
Time Between Posts
1 month
Number of Posts By Type
Text
11
Photo
6
Last Seen Tumblr Blogs





Fun Fact
Kazakhstan’s Minister of Communications and Informatics has blocked the Tumblr site because it contained 60 sites of terrorism, extremism, and pornography in 2015.











Text
I say this wholeheartedly and without ironic intent. I hope supernatural continues to have drama for the next 10 years at least. I hope that in 2033 i can once again text my best friend saying "something is happening in supernatural" for the 5 millionth time.
33K notes
·
View notes
Text

You're conducting an absorbing research.
Remember to go to sleep.
25K notes
·
View notes
Text
Analyzing Missouri Attorney General's Order Restricting Gender-Affirming Care, Part 3
Part 2
Continuing where I left off...
Overnight, I decided that analyzing all the SEGM media coverage is a little excessive and I think I proved my point that they're not what they claim to be. There's one more set of journalistic articles in the list SEGM lauds that I want to briefly touch on: the Kaiser Health News article and Undark article, and there are others on the same topic. But these articles are discussing an anti-Biden political ad that ran saying that the Biden admin is pushing for kids to transition, you know, the whole right wing attack saying that kids are trans because adults are pressuring them. SEGM is mentioned in these articles because they chose to weigh in on political issues. In the Kaiser article, they're cited as saying what the ad is pushing is not correct (but the writer describes them as being "wholly skeptical of the acceleration in gender-affirming care"). In the Undark article they're discussed for a few reasons. First, this quote:
In an email to Undark, SEGM cited research stating that the proportion of gender dysphoric youth who later desist could be much higher than other estimates suggest.
The research (link in quote) they're citing is their own. It's the Levine et al. (2022) article mentioned in Part 2, research that once again, was funded by and written by members of the SEGM. Additionally:
The authors wish to thank SEGM staff for their grant and bibliographic support.
Not only did SEGM fund the study, they curated the sources used in the study. Imagine being told to do a research paper on a subject but someone gives you the sources. You're going to produce results that the funding organization wants you to produce, not a true scientific study.
With this study (or I should say, review of previous studies) that SEGM has funded and designed to have biased results, SEGM then sends this article to journalists, politicians, and others saying "look, these scientific researchers say the same thing as us!" and if you're not familiar with academia and/or don't pay close attention, you miss the fact that this article is so incredibly fucked up it shouldn't have been published.
Second, this Undark article, and many others, interview Michael Biggs for his opinions. They describe him thus:
Michael Biggs, a sociologist at Oxford University, says that many trans-identified youth could actually be gay and lesbian children struggling to come out. To those who say it’s cruel to restrict access to gender medicine, Biggs said, “You can also reverse that and say you’re taking gays and lesbians” who aren’t in need of medication and “putting them on this terrible route” that could damage their fertility and sexuality.
Two paragraphs later, they mention that he's also an academic advisor for the SEGM. So, an academic advisor for this organization is speaking out on political topics to journalists....and perpetuating the terribly myth that trans people are actually confused gays and lesbians. He's disguising it by saying that they're kids, and that's why they're confused, but that's the underlying assumption.
Besides, if we take into account that these are kids exploring their gender, whether that's identity or expression, why is he making the leap to sexuality?
It's playing into the stereotype that gay men are inherently feminine and lesbians are inherently masculine. Not to mention, it's sexualizing children. Are they thinking about the concept of gender only in terms of who each gender can have sex with?
I can go on and on, but how many of us as trans adults were asked if we were just confused homosexuals? Even if we're not attracted to people of the sex we were assigned at birth? I've had to explain numerous times that I'm bi, but mostly into men, and the therapist I saw at the beginning of my transition couldn't make sense of that and it came up over and over. I think when she finally understood it, it wasn't in a "wow this is a fucked up way of thinking" way and instead was more like "well I guess that means you're definitely actually trans, and not a confused lesbian because you're not a lesbian!"
Back on topic: we have this supposedly apolitical organization at the heart of the debate for gender-affirming care for children time and again, and they're spouting harmful views, but they keep hiding behind the data they produced, being like "this is what the science says!" but the science itself is their science, and it's being repeatedly used to persecute trans people.
If your research is being used to harm people, and you do not accept responsibility and you continue to produce more research in exactly the same way, you are complicit in harming those people.
PSA over, but I needed to introduce this information before I could explain the issues with the AG's Footnote 6, linked in part 2.
As a reminder, at least 2 out of 3 of the authors of this article are affiliated with SEGM. The first author explicitly lists it as their organization, while the third author does not. Only one of the three is actually involved in academia.
Noticeably, the journal article does not have a disclosure statement. For those not familiar with academic journals, many articles these days will have a little section at the end that says whether or not the authors have affiliations or funding sources (etc) that may bias the article. For example, I've seen an article that deals with human genetics and the disclosure statement was like "one of the authors [author name] owns stock in 23&me". For 99% of articles with these statements, it says something like "the authors claim no affiliations." The fact that this article does not have one when at least two of the authors are associated with an organization deeply entrenched in political issues. Even if they claim they're apolitical, they can't ignore the fact that their organization is involved in so many of these arguments.
Then, there's the article's acknowledgment section: "The Society for Evidence-Based Gender Medicine (SEGM) paid for this publication to have Open Access."
Mentioned in Part 2, this article (Abbruzzese et al. 2023) is a response to one written by de Vries who is the author of most of the research they're slamming, which in turn was a response to Levine et al. (2022) mentioned above.
Levine et al. 2022 is a critical review of research done by de Vries back in the 1990s (published about multiple times between then and now). de Vries' research is what many in the discussion of gender-affirming care for youth refer to as "the Dutch studies" and resulted in what's known as "the Dutch protocol." Because it's so widely cited and plays a role in the guidance that exists for giving minors puberty blockers, it makes sense to critically analyze it. It also makes sense, if you're transphobic, to attack it relentlessly.
There's no funding for Abbruzzese et al. (2023) because it's a response and no additional resources were needed, but the initial article Levine et al. (2022) was funded by SEGM, and the bibliography was provided by SEGM. So, this is a continuation of SEGM-funded and SEGM-manufactured research.
Next, I want to discuss their making this article open access.
Open access academic articles are generally seen as a good thing. In principle, the idea that science (or any type of academic study or discussion) is not being gatekept from people who are not affiliated with a university or who do not have the money to subscribe to an academic journal on their own is valiant. Ensuring that people are able to access important information that may concern them is generally a positive. Generally. I support this, generally. In my own research, I discuss the importance of collaborating with Indigenous communities and allowing them access to research about their own ancestral pasts and about the land on which they reside. So I'm generally very pro-open source. Please don't take this as me disparaging open access research.
However, SEGM is paying the fee to make this article open access.
For those unfamiliar with the process, there are journals that are completely open access, and simply publishing in those makes your article open access. There are also journals that are behind paywalls, but offer the option of making your article publicly available. That usually comes with a price tag. Presumably, to cover what they "lose" in article purchases. However, this is usually extremely expensive.
Taylor & Francis, the publisher of this particular journal, which is The Journal of Sex and Marital Therapy (strange journal to put an article about children's healthcare, right?) touts the increased visibility of open access articles (Open Select is the service they use to make things open access) like this:
Articles published Open Select with Taylor & Francis typically receive 95% more citations* and over 7 times as many downloads** compared to those that are not published Open Select.
Additionally, T&F has a calculator for the cost of making an article open access. For a review article in the Journal of Sex and Marital Therapy from an organization in the USA, this is $3175.
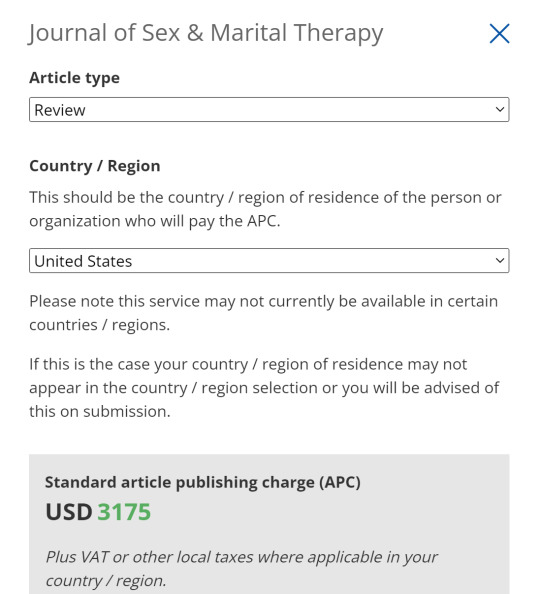
Which, frankly, isn't as expensive as I expected. But still, three thousand dollars for increased visibility...for a response to a response of a review article. It's not important to them how many people cite this because, as mentioned, 2/3 of the authors are not academics, and the one that is was not first author on this article, so it doesn't matter as much to his metrics, tenure, or any of that. Additionally, as mentioned, it's a response to a response of a review. It's not the research itself anyway.
So what do they gain by increased visibility?
People, like you, like doctors, like parents, who would not normally have access to many journals, now have access to it. This is particularly useful when publishing in a journal that's not really related to your topic. Pediatricians probably sub to a few journals, but they're not going to be this one. Probably the one they get with being a member of the American Academy of Pediatrics, maybe a couple of others specifically relating to medicine and children. Journal subscriptions are expensive, so if you're not directly affiliated with a university or something that gives you access to databases, you're probably only using a few that relate to your professional practice. Especially if you're not publishing articles, but using them as guidance on a topic you're not too familiar with.
For example, I literally watched my doctor google "sertraline and bupropion," look at the first few results, nod, and then prescribe me bupropion on top of my sertraline when I was having decreasing effects from my antidepressant. I'm pretty sure he already knew they were often used together in this way, and I personally already knew that, so I'm sure he was just confirming his knowledge before he misspoke (which he had done before about medications, doctors only have to take ONE pharmacology class). But if a pediatrician had a trans kid come in and they don't know what to do, they're going to read some journal articles, look at recent developments in research. If the results in the few journals they have access to are limited, they'll turn to google scholar and try to find an open access article.
Like this one.
This was done to influence how doctors practice medicine for trans kids.
Additionally, and this part is hypothetical because I don't know if they have access or not. If politicians don't have access to academic journals, this could have been done to influence their perceptions about gender-affirming care for youth. That one of the most widely cited studies has criticisms. This is useful for people unable or unwilling to do the mental work of analyzing the research themselves. For example, if they don't have access to the original articles (I didn't check if the original Dutch research is open access or not, since I am affiliated with a university I didn't think of it because I didn't know this was going to later come up), they can read someone's analysis of it. And they won't think too deeply about who that person is or why that may matter in their analysis, because they're not academics, and they're not used to approaching articles the same way academics are.
Often, a politician may just look for articles that confirm their viewpoints, too, instead of doing honest research. This is an easy to grab article, extract some quotes from it, and call it a day. Now you can say your policy/bill/emergency order is backed by science, and most people won't spend multiple hours doing a deep dive into all the research you've cited....and the person who does is writing thousands of words on posts getting zero notes so it doesn't matter anyway.
ANYWAY, there's a lot more I can add to a debate about downsides of open access articles, which is unfortunate, because in an ideal world, everyone should have access to research, but that's as much as pertains to this particular case.
This is a common practice of the SEGM, too. From their website:
SEGM provides grants to individual researchers and research organizations, and we pay open access fees for publications in scientific peer-reviewed journals to ensure widespread access to quality data and clinical practice guidance.
So that's part 3. It's short, sorry, and I'm still on the same source, but I've got things to do and I'll probably make part 4 later today anyway.
1 note
·
View note
Text
MO AG analysis part 2
part 1
So I'm doing this largely because most of the people pushing hateful legislation are citing the same sources, which means the mistakes that one of them makes will be repeated for all of them. Calling them mistakes is generous, though, because in the vast majority of circumstances, they are twisting the words of researchers for their purposes.
Either way, anyone who actually reads the articles these people misrepresent has the opportunity to take the intellectual high ground. It doesn't mean much when we're dealing with legislators who are pushing whatever agenda they're paid to push, and the only thing that can change their minds is green, but it's important to point out that the science is not on their side and they're being grimy and dishonest.
Okay to continue:
the sources under footnote 3 and 4 don't reveal much interesting information. More quotes taken out of context, what's important to get from them is that when they say there's a lack of evidence for benefits of puberty blockers in children, what they actually mean is there's a lack of research. There's a lack of evidence that they harm anyone, too. Both the Swedish study (Socialstyrelsen NBHW 2022, the AG's order links a PDF directly) and the US Agency for Healthcare Research and Quality (AHRQ, footnote 4, link in the AG's order and the website is a little confusing but on that page they have a full PDF discussing what they call "key questions") are saying there is not enough research, not that there are no benefits to the treatment.
One thing that is important to bring up about the Sweden study is that despite the way that the AG's order reads, the Swedish researchers aren't calling for a stop of treatment or anything like that. The language actually seems like it was used to inspire more funding and more studies. They call for treatment in exceptional cases, which prolonged identification as trans/or another gender aside from one's sex assigned at birth and stress from puberty are sufficient. So once again, another issue with another source that transphobic extremists have been using against us.
Footnote 5 is where it starts to get juicy again. Specifically, the AG says "And Finland has openly declared these interventions to be 'an experimental practice.'" The Finnish document (linked here). The full paragraph that mentions experimental practices:
"In light of available evidence, gender reassignment of minors is an experimental practice. Based on studies examining gender identity in minors, hormonal interventions may be considered before reaching adulthood in those with firmly established transgender identities, but it must be done with a great deal of caution, and no irreversible treatment should be initiated. Information about the potential harms of hormone therapies is accumulating slowly and is not systematically reported. It is critical to obtain information on the benefits and risks of these treatments in rigorous research settings."
A lot of this document talks about how the scientific work has not been done/or done to standards necessary by the Finnish government. Different people have different opinions on the work that has been done (when it comes to trans children), which I'll discuss when it comes up in the AG's order. Also, for the order calling for restrictions on both minors and adults, most of the complaints the AG puts out are related to minors.
In this case, what the Finnish government is saying is that there's no guidelines about dosages, what to expect, when to start, when to stop, etc. And personally, I think with gender-affirming care, there's not going to be. There's not one way to approach transitioning, or feeling comfortable in your body, or whichever route someone takes. There's not one kind of gender dysphoria. (There's not even two kinds, if you were thinking about it as ftm or mtf.) With many other types of medical treatment, there's protocols for these things. For example, a patient presents with depression. The doctor has a few options: therapy, antidepressants, etc. If they choose antidepressants, the doctor looks at the demographics: some are not indicated for children and others are specifically only for children, they tend to start males with TCAs and females with SSRIs though they don't have to, there may be other factors to take into account as well like other medical conditions or other medications, or often if a member of your family has had success with a certain medication, they'll start with that one. When they pick a medication, there will be a recommended dosage, especially for children where dosages are related to weight, but they start low and slow and titrate upwards until they hit the maximum recommended dose and if the medication doesn't work, they switch. They determine efficacy by interviews, there are assessments to determine if someone's mood is improving. With treatment for gender dysphoria for minors, there's neither "this symptom = this treatment" nor "symptom persists = treatment is not working." That barely works for trans adults, either, and this is an issue inherent with medicalizing gender, and is a really big topic to tackle and needs its own post, at minimum.
Treatment is therefore experimental in the sense that the doctor and patient need to experiment with what works and what does not. It will be different for every patient and a specific set of procedures cannot be used.
Anyway, I'm not going to do a deep dive into what Finland requires for medical research, but it seems like they have higher expectations than the studies that have been done. Even so, they acknowledge that patients that need it should still be treated while research is being done. This is contrary, yet again, to the AG's order and all of the bills banning gender-affirming care for minors.
Footnote 6 is what I've been waiting for! This is the real tea. So this source is an article written this year (Abbruzzese et al. 2023, open source article linked here). It's a critique of the "Dutch studies" that pop up again and again in the discussion of gender-affirming care for minors. The Dutch studies are research done by Annelou de Vries, mostly in the 1990s I believe, that gave minors gender-affirming care and followed up with them later. It's one of the only studies cited for a longitudinal view of use of puberty blockers in the treatment of trans minors. There's quite a few articles based on this research, including ones these authors mention from I believe 1997, 2012, and 2014. Also important to note, this article is actually a response to de Vries, who had written an article in response to a previous critique issued by the same authors. So, Studies done by de Vries (and colleagues) between the 1990s and 2020s -> Levine et al. 2022(a in the sources of this article), a review they wrote to the collection of research -> de Vries, A.L.C. 2022 (written in direct response to Levine et al. 2022) -> then Abbruzzese et al. 2023, the article being discussed here as the MO AG's Footnote 6
Levine et al. and Abbruzzese et al. are the same three authors, they just switched who got first author.
And who these authors are is extremely important.
Stephen Levine is the only actual academic of the trio. This is probably why he was first author on the article. Levine is in the Department of Psychiatry, Case Western Reserve University in Ohio.
Julia Mason is a pediatrician at Calcagno Pediatrics, also in Ohio. (apparently also part of the SEGM, which I talk about below)
E. Abbruzzese is the really interesting one. Abbruzzese is part of the Society for Evidence-Based Gender Medicine.
The SEGM is a hate group disguised as a medical association. Anyone who reads that title and doesn't know better wouldn't think they were anything but reputable.
Their website states that they don't have any political agenda or affiliations, and this is their response to a question "Does SEGM support LGBTQ people?"
SEGM believes that LGBTQ people should be treated with dignity and afforded the same human rights and protections as all other individuals. Many of the professionals collaborating within SEGM are lesbian and gay, and a number have loved ones who identify as transgender.
The field of pediatric gender medicine is currently engulfed in an intense international scientific debate. Although most are debating in good faith, some have met SEGM’s position of concern over the unknown risk/benefit profile of youth gender transitions with accusations of “transphobia.” If such a standard is to be applied, then entire countries that have expressed the same concern as SEGM, including the UK, Norway, Finland, and Sweden—the first country to recognize transgender people’s legal status—would be similarly labeled “transphobic.” Resorting to ad hominem attacks is often a reflection of weakness in one’s own argument, and we believe such tactics detract from the quality of scientific debate.
In recent months, we have seen a shift toward more civil debates, and we have been grateful to see our position of concern fairly represented by The Economist, The Associated Press, Newsweek, Wall Street Journal, Medscape, NPR, Kaiser Health News, and a growing number of other news sources.
Idk, I wonder why people are calling you transphobic if you're not?
They're citing all the sources that extremists use to delegitimize gender-affirming care for youths. They're using the same language as the extremists. They're misinterpreting the same Scandinavian releases. Hmm.
Also, the news outlets mentioned in the last paragraph have links to articles. The Economist: It's behind a paywall and I immediately got frustrated when I couldn't get past it, but 1. the article's title is:
"Questioning America’s approach to transgender health care
Some paediatricians want a re-examination of the professional guidance"
American, huh? We don't spell it "paediatrician." So, we've got a non-American viewpoint being presented as an American one. Not to mention the divisive nature of the title. and 2. the parts I can read are already insidious. They're telling a story of a 15 year old who gets offered both top surgery and hormones within "a couple of visits" to a therapist and. in what world? not the one we currently get healthcare in. Sure, we've gotten more accepting now, but I still call bullshit. Not to mention the insidiousness of this quote: “I just didn’t know what ‘gender-affirming care’ meant. It sounds so beneficial and positive.”
The Associated Press: This article is actually well-written. They did a good job of presenting the multiple angles of the issue in the very few paragraphs they had to write it. Apparently the author no longer works for the AP. The only thing that worries me is that the part about the SEGM is at the end, so it's the last thing someone would think about if they read the whole article. The article is actually about a paper published in the journal Pediatrics that followed trans children and found that, surprising no trans person, their identities stick. The part about SEGM highlights some of SEGM's awful lines of thinking:
The Society for Evidence-Based Gender Medicine, a nonprofit group of health professionals who are concerned about medical transition risks for minors, said other evidence shows high numbers of kids outgrow transgender identities by puberty or adulthood. Some researchers point to flaws in that data.
Dr. William Malone, an advisor to the group, said the new study appears to reinforce concerns “that early social gender transition may cement a young person’s transgender identity, and lead minors on the path to eventual medicalization, with all its inherent risks and uncertainties.”
The SEGM thinks that social transitioning solidifies what might not be a solid identity. I mean one of the purposes of social transitioning is to determine whether being another gender in public full time is what someone wants, whether it alleviates some or all of their dysphoria. they don't want any medical treatments because a kid might be unsure, but they don't want the kid to socially transition to find out if they're sure.
My tearing into SEGM will continue in the next part, and then I'll start actually discussing the article, but I'm going to try to actually get something relevant to my schoolwork done tonight.
Part 3
1 note
·
View note
Text
Missouri AG order
ANYWAY this is what I wanted to rant about.
As someone with the time, means, and interest to research the sources used in the Missouri AG's emergency order to stop gender-affirming care, I did that.
Well, I'm about halfway through, but it's a lot of repeating sources after this point, and I've been at this for hours now. Neglecting all the other things I was supposed to do today.
This is the first part of my analysis, which is going to be very long, because this hardly made a dent in my notes.
So, we know that in general these transphobic extremists use junk science and cherry pick their data, that's not new. But it's hard and rare to get them to give sources, and so many. So I jumped on the opportunity to look through these sources, and also the AG cited a lot of the figures I've been interested in finding out the origins of. So yeah. This might help some people, might not, but I did the research, so here I am.
First of all, the AG switches between the old and current WPATH (World Professional Association of Transgender Health) standards of care, whenever it suits him.
The old SOC, SOC 7, were published in 2011, probably the same ones I looked at early in my transition when I was figuring out what the hell to do. It's a 68 page document.
The SOC 8, by contrast, is 260 pages, published in 2022. Obviously, between 2011 and 2022 the healthcare profession and people in general learned a lot about trans people. The Missouri AG didn't like this, so continuously cites the SOC 7 when they say things like they don't know the long term effects of puberty blockers, etc. A lot of the unsure language that casts doubt on the legitimacy of trans people's identities and the benefits of transition disappeared between the 7 and 8...because we learned so much in that time.
He also writes about WPATH like they're begrudgingly admitting uncomfortable facts. He thinks any acknowledgement of not knowing something is some kind of gotcha moment.
As you could also imagine, the AG is misinterpreting a lot of the citations he makes. Seriously, if I didn't know it was intentional I'd think this person was just awful at research and reading comprehension. Things in quotes in the AG's order are actually not quotes from sources. Some are, but a lot of the WPATH ones that are supposed to be direct quotes are not. He misrepresents what the WPATH was trying to say (in the SOC 7) here:
"Often this care takes the form of psychotherapy, also known as talk therapy, rather than any chemical or surgical intervention. As the World Professional Association for Transgender Health has previously put it, this therapy often involves exploring the many influences on a person’s gender identity, including 'peer and other social relationships,' and ensuring that 'gender dysphoria is not secondary to, or better accounted for, by other diagnoses.'"
The page he is quoting from is not discussing psychotherapy, but rather an assessment as a precursor to receiving hormones and other medical treatments for gender dysphoria. He lifted the "peer and other social relationships" (not actually a direct quote, despite his quotations) part not from a request to explore "influences on a person's gender identity" but rather from a request to determine history of gender dysphoria, the impact of stigma against trans and gender nonconforming people, and the availability of peers, family, relationships as a support system.
The AG goes on to say that WPATH recommends doing talk therapy to ensure that gender dysphoria is not secondary to, or better accounted for, by other diagnoses. What WPATH (once again, the SOC 7, not the current one) actually says is that "the role of mental health professionals includes making reasonably sure that gender dysphoria is not secondary to, or better accounted for, by other diagnoses."
A recurring theme throughout this document is an insistence that any other mental health condition is an automatic exclusion of being eligible for gender-affirming care, and the AG tries to make it seem like the research supports this assumption. It does not, and it will emerge as a topic again and again with different sources.
As a source of comparison, the 2022 SOC 8 describes the same situation differently: "The role of the assessor is to assess for the presence of gender incongruence and identify any co-existing mental health concerns,..." Importantly, the SOC 8 says that the provider should be able to distinguish between gender dysphoria, incongruence, and diversity vs any of these coexisting conditions. It does not say that any conditions are grounds for excluding someone from care. WPATH even asks for the provider to ensure that any mental or physical health condition that could impact the outcome of gender-affirming treatment is assessed, and risks and benefits are discussed with the patient, before deciding to move forward.
And goes on, very importantly, to acknowledge the agency of both the trans patient and the health care provider and present a patient-provider relationship that is honestly so relieving to see. Chef's kiss.
"...the decision to move forward is shared between the TGD (transgender and gender diverse) person and the assessing HCP (healthcare provider), with both playing a key part in collaborative decision-making."
It goes on to mention that counseling and psychotherapy can be helpful for people who want it, but it is not a requirement. Which is huge. (but that's a different discussion, just mentioned here because obviously if you're trying to gatekeep gender-affirming care you'll refer to the old version that doesn't say that).
This is going to be much longer than I intended it to be, this is just a discussion of the first source. I'll bring more up later.
Part 2 Here
1 note
·
View note
Text
welcoming myself back hi
considering using my tumblr more, at least for the time being. also considering making a new account altogether for professional/archaeology/political stuff. In the meantime, I'm gonna use this blog to...idk vent my long-format frustrations.
I've largely been in a social media blackout/in only lurking mode on other sites while in grad school but now I'm getting deeply involved in political stuff and also just in general feeling more like I need to word vomit on some forum and...nothing quite hits like tumblr.
1 note
·
View note
Photo
crab doodle :>
my computer broke but i finally fixed it!
593 notes
·
View notes
Text

Happy 20th anniversary Kingdom Hearts 💖 I’ve only been with the series for a few years but it has been the most important video game series to me for bringing so much warmth and new friends into my life!
1K notes
·
View notes
Photo


More char post series living da life vignettes!
3) Krel picks up a job at Hex Tech, and gets his fill of tech magic under the tutelage of Zoe! I would love to see these two interacting, I feel like they would get along super well and be an amusing duo to watch.
4) The toe kiddos (+3 old kiddos) go to Disneyland cuz they deserve it!!! Archie, Douxie and Zoe would be the “chaperones” and Nari would be the chaperone who needs chaperoning. I would love to do some more vignettes of the wonderful chaos on this trip haha.
Enjoy y’all! HAPPY THOUGHTS HAPPY THOUGHTS!
3K notes
·
View notes
Photo


I’ll be doing a series of fan art of the toa kids post series enjoying life finally/ hangout vignettes (ignoring ROTT, assume Arcanes got defeated in some form of fanciful fashion or chose to pursue different life goals). CUZ THIS IS THE REALITY I CHOOSE THANK YOU OK HERE WE GO! FANON AWAY! 1) First off, big bro Douxie teaching Claire how to drive! 2) Steve confiding in his found fam after a rough day. I feel like after Wizards, there is more warmth between him and Douxie and I’d love to see the three of these kiddos ( 2 hella old kiddos) spending more time together and supporting each other!
4K notes
·
View notes
Photo



I planned to have this finished by the time the new #KH3 game came out but I finally finished this and the game #imdead #crytilidie
10K notes
·
View notes

