#cross sex hormones
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
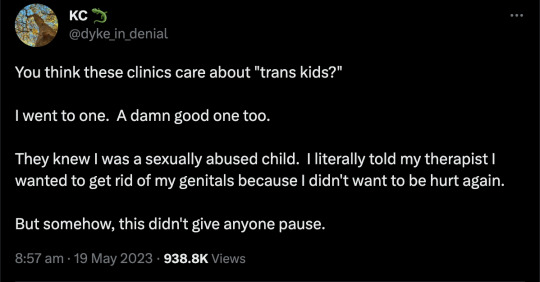



You may remember KC Miller.

She deleted her account after she went viral as it was all too much. This is from her new account.
#KC Miller#detrans#detransition#medical malpractice#medical corruption#sex trait modification#medical scandal#medical transition#unethical#gender ideology#queer theory#genderwang#testosterone#wrong sex hormones#cross sex hormones#double mastectomy#this never happens#religion is a mental illness
1K notes
·
View notes
Text
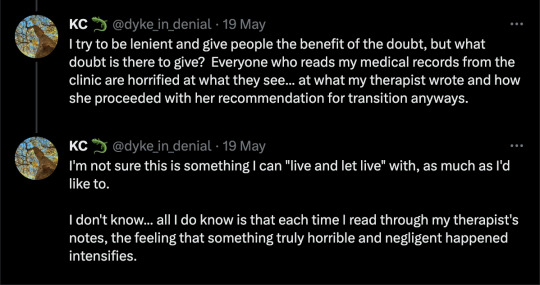
This is one of the reasons why I will never accept that transwomen are real women.
#transgenderism#transgender ideology#mtf#mentrual cycle#cross-sex hormones#trans#zachary elliott#quotes
889 notes
·
View notes
Text
To say anything about the city I grew up in is firstly wildly ungrateful and out of touch and biting the hand that fed me so well. I get pissed off too when foreigners on the internet dare to say anything about it (city is directly equivalent to country here because it’s a 734 square kilometre island) and it surprises me because I’ve never been overly patriotic. But the prospect of living the rest of my life here and dying is also soul destroying
#the argument for leaving though is hilarious like okay#so you want to migrate to become dependent on cross sex hormones and get murdered on your way home?#eat your food bland and overpriced? get rained on? look at hot people?
8 notes
·
View notes
Text
Woke up in the middle of the night before and ended up in a dysphoria spiral so bad it literally kept me from sleeping. In case anyone was wondering how it's been going for me
#open mick night#just constantly despairing over how little control i have over my own body. and people love saying shit that makes it feel worse lmao#i need to get out of this HOUSE chowdah i need cross sex hormones
9 notes
·
View notes
Text
Effects of Cross Hormone Therapy.
The Comprehensive Impact of Hormone Replacement Therapy on Transgender Individuals: Physical, Psychological, and Athletic Considerations" By: Dr. Sydney Taylor
Introduction
Hormone therapy is a pivotal aspect of the transition process for many transgender individuals, profoundly impacting their physical and psychological well-being. Transgender men (assigned female at birth but identify as men) and transgender women (assigned male at birth but identify as women) often seek cross-sex hormone therapy to align their physical characteristics with their gender identity. This therapeutic intervention, which includes exogenous testosterone for transgender men and exogenous estrogen for transgender women, is considered medically necessary for many and has been shown to significantly improve quality of life.
The prevalence of transgender individuals has been historically challenging to estimate. However, recent surveys in the United States suggest that approximately 0.3-0.5% of the population identifies as transgender. As societal understanding and acceptance of transgender individuals have grown, so too has the number of people seeking hormone therapy.
Hormone therapy for transgender individuals involves carefully managed regimens to achieve desired physical transformations while monitoring for potential side effects. Testosterone therapy for transgender men induces virilization, suppressing feminizing characteristics and promoting the development of masculine features such as increased muscle mass, facial and body hair growth, and voice deepening. On the other hand, estrogen therapy for transgender women promotes feminization, aiding in breast development, fat redistribution, and the reduction of male-pattern hair growth.
While the benefits of hormone therapy are well-documented, there remain critical considerations and debates, especially regarding its impact on aspects like athletic performance and long-term health. For instance, the effects of gender-affirming hormones on muscle mass, strength, and endurance raise questions about fairness and inclusion in competitive sports.
In this article, we will delve into the multifaceted effects of hormone therapy on transgender individuals, drawing from a range of recent studies and clinical guidelines. We will explore the physiological changes induced by hormone therapy, its psychological impacts, and the broader implications for societal integration and acceptance of transgender individuals. Through this exploration, we aim to provide a comprehensive overview of how hormone therapy shapes the lives of transgender people, fostering a better understanding of its significance and complexities.
Effects of Hormone Replacement Therapy on Trans Men
Hormone replacement therapy (HRT) for transgender men, commonly involving the administration of exogenous testosterone, has profound and wide-ranging effects on both physical and psychological aspects of health. This section explores the various impacts of testosterone therapy on trans men, based on current research and clinical findings.
Physical Effects
Virilization: Testosterone therapy induces several masculinizing effects. Within the first three months, many trans men experience the cessation of menses (amenorrhea), an increase in facial and body hair, skin changes, and increased acne. These changes often include a shift in fat distribution and an increase in muscle mass, leading to a more masculine body shape(tau-05-06-877).
Voice Deepening: One of the notable changes is the deepening of the voice, which occurs due to the growth of the laryngeal cartilage and thickening of the vocal cords. This process typically begins within 9 to 12 months of starting testosterone and can take up to two years to complete(tau-05-06-877).
Clitoral Enlargement and Genital Changes: Testosterone causes an increase in clitoral size, which starts within the first three to four months and generally stabilizes by one year. Additionally, there is an increase in ovarian stromal tissue and potential cyst formation, mirroring changes seen in polycystic ovarian syndrome(tau-05-06-877).
Body Composition: Testosterone therapy leads to increased lean body mass and upper body strength while concurrently decreasing body fat. This results in a more defined muscle structure and a reduced hip-to-waist ratio, contributing to a more traditionally masculine physique(tau-05-06-877).
Hair Growth and Loss: Trans men often experience increased hair growth on the face, chest, abdomen, and other areas, while also potentially encountering male-pattern baldness, particularly if they are genetically predisposed(tau-05-06-877).
Psychological and Cognitive Effects
Mood and Cognitive Changes: Testosterone has been shown to increase energy levels, aggression, and libido in trans men. Patients often report feeling more aligned with their gender identity and experience an improvement in visio-spatial abilities. Psychologically, many trans men feel more masculine and settled in their new gender role once testosterone therapy has commenced(tau-05-06-877).
Reduction in Gender Dysphoria: The suppression of menstruation, which many trans men find distressing, is often reported as one of the most psychologically beneficial effects of testosterone therapy. The overall improvement in alignment with one's gender identity leads to better mental health outcomes and reduced stress levels(tau-05-06-877).
Metabolic and Health Considerations
Cardiovascular and Metabolic Health: While testosterone therapy can adversely affect lipid profiles by increasing triglycerides and reducing HDL cholesterol, studies indicate that these changes do not translate into a higher risk of cardiovascular disease. Long-term studies show that the mortality rate for trans men on testosterone therapy is comparable to the general population(tau-05-06-877).
Bone Health: Testosterone therapy helps maintain bone density and may even increase cortical bone size and thickness. This is crucial in preventing osteoporosis, a condition that trans men are at risk for if sex hormone levels are not adequately maintained(tau-05-06-877).
Hematocrit and Red Blood Cell Production: Testosterone induces the production of erythropoietin, leading to increased red blood cell production. While this can result in higher hematocrit levels and a potential risk of polycythemia, careful monitoring and management can mitigate these risks(tau-05-06-877).
Surveillance and Monitoring
Ongoing surveillance is critical for trans men undergoing testosterone therapy. Regular monitoring of hormone levels, lipid profiles, and bone density is recommended to ensure therapy is both effective and safe. Adjustments to dosage and the type of testosterone used may be necessary based on individual responses and health outcomes(tau-05-06-877).
In summary, hormone replacement therapy with testosterone provides significant benefits for trans men, aligning physical characteristics with gender identity and improving mental health and quality of life. However, it requires careful management to address potential risks and ensure long-term health and well-being.
Effects of Hormone Replacement Therapy on Trans Women
Hormone replacement therapy (HRT) for transgender women primarily involves the administration of exogenous estrogen, often in combination with anti-androgens, to induce feminization and suppress masculinizing characteristics. This section explores the various impacts of estrogen therapy on trans women, based on current research and clinical findings.
Physical Effects
Breast Development: One of the most notable changes induced by estrogen therapy is breast development. Breast growth typically begins within two to three months after initiating treatment, with maximum development usually reached after two years. However, the extent of breast development varies among individuals, with many trans women opting for breast augmentation surgery to achieve their desired breast size and shape(tau-05-06-877).
Skin and Hair Changes: Estrogen therapy leads to significant changes in skin texture, making it softer and less oily. There is also a reduction in facial and body hair growth, although additional hair removal methods like electrolysis or laser therapy are often necessary to achieve the desired feminine appearance. Over time, body hair becomes finer and less dense(tau-05-06-877).
Body Composition: Estrogen therapy results in an increase in subcutaneous fat, particularly around the hips, buttocks, and thighs, contributing to a more typically feminine body shape. Concurrently, there is a decrease in muscle mass and strength, aligning more closely with typical female body composition(tau-05-06-877).
Reduction in Libido and Erectile Function: A common effect of estrogen therapy is a reduction in libido and erectile function, which many trans women view positively as it aligns more closely with their gender identity. Additionally, there is a decrease in testicular volume due to suppressed gonadotropin production(tau-05-06-877).
Psychological and Cognitive Effects
Mood and Emotional Well-being: Estrogen therapy has mood-modulating effects, often resulting in increased feelings of well-being and decreased depression scores. Many trans women report an increased sense of femininity and a calmer mood as a result of hormone therapy(tau-05-06-877).
Reduction in Gender Dysphoria: Hormone therapy significantly reduces gender dysphoria, leading to improved mental health outcomes. The alignment of physical characteristics with gender identity alleviates distress and enhances overall quality of life(tau-05-06-877).
Metabolic and Health Considerations
Cardiovascular Health: The metabolic effects of estrogen therapy include alterations in lipid profiles, such as decreased low-density lipoprotein (LDL) cholesterol and increased high-density lipoprotein (HDL) cholesterol. However, estrogen therapy, particularly oral formulations, can increase the risk of venous thromboembolism (VTE). Transdermal estrogen is often recommended to minimize this risk(tau-05-06-877).
Bone Health: Estrogen plays a crucial role in maintaining bone density. Long-term estrogen therapy helps prevent osteoporosis, which is particularly important as anti-androgens and orchiectomy can reduce testosterone levels to very low levels, increasing the risk of bone demineralization. Regular bone density screening is recommended to monitor and manage this risk(tau-05-06-877).
Fertility Considerations: Estrogen therapy, combined with anti-androgens, significantly reduces fertility. It is essential to discuss the potential impact on fertility with patients before starting hormone therapy and offer options for gamete storage if they wish to preserve their reproductive capabilities(tau-05-06-877).
Surveillance and Monitoring
Ongoing surveillance is critical for trans women undergoing estrogen therapy. Regular monitoring of hormone levels, lipid profiles, and bone density is essential to ensure therapy is both effective and safe. Adjustments to dosage and the type of estrogen used may be necessary based on individual responses and health outcomes(tau-05-06-877).
In summary, hormone replacement therapy with estrogen provides significant benefits for trans women, aligning physical characteristics with gender identity and improving mental health and quality of life. However, it requires careful management to address potential risks and ensure long-term health and well-being.
Effects of Hormone Replacement Therapy on Athletic Performance
Trans Women
The inclusion of transgender women in competitive sports has sparked considerable debate, particularly concerning the potential advantages retained after gender-affirming hormone therapy (GAHT). This section examines the impact of estrogen and anti-androgen therapy on athletic performance in trans women.
Strength and Muscle Mass:
Decrease in Muscle Mass: Estrogen therapy in trans women leads to a significant reduction in muscle mass and strength over time. Studies indicate that within the first year of feminizing hormone therapy, trans women experience a reduction in lean body mass and muscle area by approximately 5%. This decline continues beyond three years, aligning more closely with the muscle mass and strength of cisgender women(tau-05-06-877)(577.full).
Muscle Strength: Despite the reduction, trans women generally retain a higher absolute muscle mass than cisgender women. However, their relative muscle strength, when corrected for lean mass, tends to be similar to cisgender women. Longitudinal studies have shown a steady decline in muscle strength, particularly in upper body strength, such as hand grip strength, which can decrease by 4-7% over the first year of hormone therapy(tau-05-06-877)(577.full).
Cardiorespiratory Function:
VO2 Max and Endurance: Cardiovascular capacity, as measured by VO2 max, is a crucial determinant of performance in endurance sports. Trans women on long-term hormone therapy have been shown to have lower VO2 max compared to cisgender men but similar to cisgender women. This change reflects a decrease in hemoglobin and hematocrit levels, which are crucial for oxygen transport during intense exercise(tau-05-06-877).
Running Performance: Trans women show a decline in running performance after starting GAHT. For instance, a study on trans women in the U.S. Air Force found that prior to hormone therapy, they ran 1.5 miles 21% faster than cisgender women. After two years of feminizing hormones, their running speed slowed but still remained 12% faster than their cisgender female counterparts (577.full).
Impact on Athletic Performance Over Time:
Short-term Effects: Within the first year of starting hormone therapy, trans women experience significant decreases in muscle strength and lean body mass. These initial changes are critical as they mark the beginning of alignment with the physical performance levels of cisgender women.
Long-term Effects: Over several years, the differences in performance metrics between trans women and cisgender women diminish further. By four years, many physical performance indicators, such as the number of push-ups and sit-ups performed, align more closely with those of cisgender women(tau-05-06-877)(577.full).
Trans Men
Testosterone therapy for transgender men generally enhances physical performance, leading to increases in muscle mass and strength.
Strength and Muscle Mass:
Increase in Muscle Mass: Testosterone therapy significantly increases muscle mass and strength in trans men. Studies indicate that within the first year, there is a notable increase in lean body mass and muscle strength, aligning their physical capabilities closer to those of cisgender men(tau-05-06-877) .
Muscle Strength: Trans men generally experience improvements in upper and lower body strength, with performance metrics such as push-ups, sit-ups, and running times reaching the levels of cisgender men within one to two years of starting hormone therapy (tau-05-06-877).
Cardiorespiratory Function:
VO2 Max and Endurance: Testosterone therapy enhances cardiorespiratory function, increasing hemoglobin and hematocrit levels, which improves oxygen transport during exercise. This leads to improved performance in endurance sports(tau-05-06-877).
Running Performance: Before starting hormone therapy, trans men generally perform at a lower level compared to cisgender men. However, after one year of testosterone therapy, their performance in activities such as running significantly improves, aligning closely with that of cisgender men (tau-05-06-877).
Impact on Athletic Performance Over Time:
Short-term Effects: The initial year of testosterone therapy brings about rapid improvements in muscle mass, strength, and overall physical performance. These changes are vital for the physical alignment of trans men with their gender identity.
Long-term Effects: Over several years, trans men continue to experience improvements in physical performance, often exceeding the average performance of cisgender men by the fourth year of hormone therapy(tau-05-06-877).
The effects of hormone replacement therapy on athletic performance in transgender individuals are complex and multifaceted. While feminizing hormone therapy in trans women reduces muscle mass and strength, bringing their physical capabilities closer to those of cisgender women, some residual advantages in certain performance metrics may remain. Conversely, testosterone therapy in trans men significantly enhances muscle mass, strength, and overall physical performance, aligning them closely with cisgender men. These findings highlight the need for nuanced guidelines in sports to ensure fair and inclusive participation for transgender athletes. Further longitudinal studies are necessary to fully understand the long-term implications of hormone therapy on athletic performance.
Conclusion
Hormone replacement therapy (HRT) plays a critical role in the transition process for transgender individuals, offering substantial benefits in aligning physical characteristics with gender identity and improving overall mental health and quality of life. For transgender men, testosterone therapy induces significant virilizing effects, including increased muscle mass, deepened voice, and cessation of menstruation, contributing to enhanced well-being and reduced gender dysphoria. Regular monitoring is essential to manage potential risks such as cardiovascular health and bone density.
For transgender women, estrogen therapy, often combined with anti-androgens, facilitates feminization through breast development, fat redistribution, and reduced body hair growth. Despite potential risks such as venous thromboembolism and bone health concerns, estrogen therapy markedly improves psychological well-being and quality of life. Close surveillance and appropriate adjustments to therapy ensure these benefits are maximized while minimizing adverse effects.
When considering athletic performance, HRT has a nuanced impact. Trans women experience a reduction in muscle mass and strength, aligning their performance more closely with cisgender women, though some advantages may persist. Conversely, testosterone therapy significantly enhances muscle mass, strength, and endurance in trans men, aligning their athletic capabilities with cisgender men.
Overall, hormone replacement therapy is a cornerstone of medical care for transgender individuals, fostering significant physical and psychological benefits. However, it necessitates careful management and monitoring to address and mitigate potential health risks. The complexities involved, especially concerning athletic performance, highlight the need for ongoing research and tailored guidelines to ensure fair and inclusive participation in sports and broader society. By understanding and addressing these multifaceted effects, healthcare providers can better support the transgender community, promoting health, well-being, and equality.
References
· Unger, C. A. (2016). Hormone therapy for transgender patients. Translational Andrology and Urology, 5(6), 877-884. doi:10.21037/tau.2016.09.04
· Roberts, T. A., Smalley, J., & Ahrendt, D. (2021). Effect of gender affirming hormones on athletic performance in transwomen and transmen: implications for sporting organisations and legislators. British Journal of Sports Medicine, 55(7), 577-583. doi:10.1136/bjsports-2020-102329
· D’hoore, S., et al. (2022). Gender-affirming hormone therapy: An updated literature review with an eye on the future. Journal of Internal Medicine. doi:10.1111/joim.13274
· Seal, L. J. (2015). A review of the physical and metabolic effects of cross-sex hormonal therapy in the treatment of gender dysphoria. Annals of Clinical Biochemistry, 52(1), 10-20. doi:10.1177/0004563214538340
· Hembree, W. C., et al. (2017). Endocrine treatment of gender-dysphoric/gender-incongruent persons: An Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 102(11), 3869-3903. doi:10.1210/jc.2017-01658
· Van Caenegem, E., et al. (2015). Bone mass, bone geometry, and body composition in female-to-male transsexual persons after long-term cross-sex hormonal therapy. Journal of Clinical Endocrinology & Metabolism, 97(7), 2503-2510. doi:10.1210/jc.2012-3551
· Wierckx, K., et al. (2012). Long-term evaluation of cross-sex hormone treatment in transsexual persons. Journal of Sexual Medicine, 9(10), 2641-2651. doi:10.1111/j.1743-6109.2012.02876.x
· Colizzi, M., Costa, R., & Todarello, O. (2014). Hormonal treatment reduces psychobiological distress in gender identity disorder, independently of the attachment style. Journal of Sexual Medicine, 10(11), 3049-3058. doi:10.1111/jsm.12284
· Kranz, G. S., et al. (2015). High-dose testosterone treatment increases serotonin transporter binding in transgender people. Biological Psychiatry, 78(8), 525-533. doi:10.1016/j.biopsych.2015.01.023
· Mueller, A., et al. (2010). Body composition and bone mineral density in male-to-female transsexuals during cross-sex hormone therapy using gonadotrophin-releasing hormone agonist. Experimental and Clinical Endocrinology & Diabetes, 118(5), 317-320. doi:10.1055/s-0029-1243631
· Leinung, M. C., et al. (2013). Endocrine treatment of transsexual persons: Extensive personal experience. Endocrine Practice, 19(4), 644-650. doi:10.4158/EP12155.OR
#transgender#transfem#trans women#transmasc#transblr#trans pride#cross hormone therapy#trans hrt#hrt estrogen#medical transition#ftm hrt#lgbt pride#lgbtq community#lgbtqia#pride month 2024#pride month#happy pride 🌈#hormones#hormonal changes#hormonalhealth#transbian#estrogen#testosterone#sex hormones#trans rights#trans athletes#trans male#trans mtf
4 notes
·
View notes
Text
We have a serious problem
Michael Laidlaw, MD: I'm a board-certified endocrinologist, practicing in private practice for the last 16 years. I've been studying and publishing in this area for the last 5 years, including peer reviewed journals such as Journal of of Clinical Endocrinology and Metabolism, and others. I also have a patient who is a detransitioner.
I think it's important to note that studies are shown that desistance, or growing out of this condition, of children by adulthood is very high. It's some 50-98%.
I want to be sure before I give someone a very powerful hormone like Insulin that they in fact have diabetes.
What about cancer? Before we give any powerful agents such as chemotherapeutics or surgeries, we certainly want to have physical evidence of this problem, such as biopsies or imaging.
Now, the gender affirmative therapy treatment proposed by WPATH gives very powerful hormones and surgeries on what basis? Where can we find the gender identity to be certain that these children will not desist by adulthood? Can we use imaging of the brain or blood tests, genetic testing, are there other biomarkers to ensure that we are correct? There is no such thing.
Julia Mason, MD: The Endocrine Society put out guidelines in 2017, and they were very careful in the guidelines. One, to point out that the evidence was of low and very low quality. And they also said in the guidelines that they have no idea how you identify which kids are trans and require this treatment.
And then the American Academy of Pediatrics the next year just leapt into that void and said, oh, oh, we'll tell you how you know which kids. You ask them.
Prior to 2018 I had maybe one trans patient. But then there was another one. And another one. And another one.
It wasn't until later that I started asking questions like, wait, every single kid I send to the gender clinic gets put on puberty blockers or cross-sex hormones. Just, it was happening immediately.
Patrick Hunter, MD: This affirmative model of care has spread wildly in the last 8 years. Now we have objective, unbiased systematic reviews. These systematic reviews tell us the evidence for youth transition is poor quality, and with very low certainty for benefit.
In JAMA Pediatrics, there was a study reported from Northwestern University in Chicago. Patients ranged in age from 13 to 24 years. The authors concluded that mastectomy was beneficial and should not be delayed in youth. What lead them to that conclusion? The finding that 3 months after surgery, the 36 patients were happy with their flat chests. They lost 9% of their surgical cases to follow-up. Nine percent. In 3 months.
It is absurd, meaningless to draw any conclusions after 3 months.
This paper is indicative of the quality of research we have in this field, published in our most prestigious journals.
We have a serious problem.
#gender ideology#queer theory#medical transition#desistance#detrans#sex trait modification#genderwang#detransition#trans identity#cross sex hormones#wrong sex hormones#puberty blockers#poor research#medical malpractice#medical scandal#medical corruption#endocrinology#low quality#ideological capture#ideological corruption#religion is a mental illness
988 notes
·
View notes
Text

Effects of puberty blockers on males
Effects of puberty blockers on females
Cross-sex hormone use in males (female-typical levels of estrogen and testosterone) has a host of detrimental effects to the body.
Cross-sex hormone use in females (high testosterone) has a host of detrimental effects to the body.
#transgenderism#transgender ideology#ftm#mtf#gender fluid#non-binary#gender ideology#puberty blockers#testosterone#estrogen#hrt#hormone replacement therapy#cross-sex hormones
207 notes
·
View notes
Text
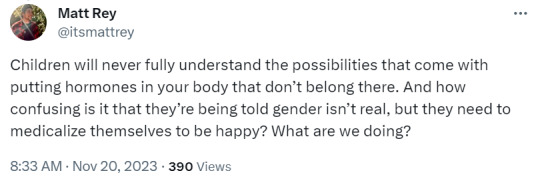
I would rather be a TERF than be someone who ignores that this can happen just to be an ally. True friends and allies would want anyone especially minors to be informed of what they were getting into concerning any medical procedure.
The tragic story of Griffin Sivret, and why it matters for every MA family.
Massachusetts Informed Parents Aug 19, 2024
Over the weekend we learned of the tragic death of 24-year-old Griffin Sivret, a “trans man” and MA native. For the sake of clarity, we will refer to Griffin by her natal sex. According to multiple sources, at the time of her death Griffin lived in RI but grew up in Worcester and attended Worcester Public Schools. She then went on to Becker College in Leicester. You can read her obituary HERE.

Before we go any further, we would like to extend our condolences to Griffin’s friends and family, especially her parents. Our hearts go out to you in your time of profound and unfathomable loss.
As a parent, the first thing that often comes to your mind when you hear that a young person has died, is the question: “What happened?” The answer to that question is why we feel that Griffin’s story must be told.
While an official cause of death has not been released, it has been reported that Griffin’s death was related to the long-term complications of “gender-affirming” surgery. Specifically, in Griffin’s case, the surgery that degraded her health and may have led to her death is phalloplasty. Phalloplasty, for those of you who have not yet been baptized into the hellscape that is “gender-affirming” surgery, is when a surgeon creates a neophallus (essentially, a fake penis) out of a flap of skin taken from either the forearm or the thigh of a natal female and sews it onto her groin area. This might sound like something straight out of a horror movie, but it’s very real. Phalloplasty surgery carries a high rate of complications, and the neophallus never functions like an actual penis, and often causes a multitude of other physical problems. For a firsthand account of what it is like to go through this surgery and to live with the complications, see this article from “trans man” and activist Scott Newgent. Newgent underwent phalloplasty while in her 40’s, and now works to sound the alarm about how dangerous this procedure is, and how it has destroyed her life.
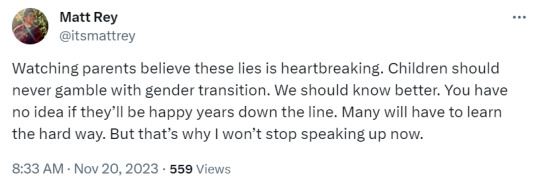
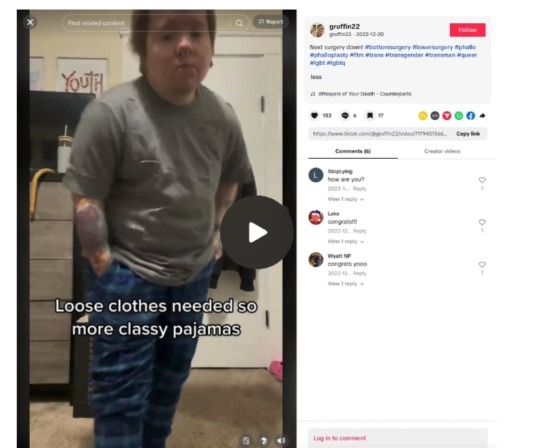
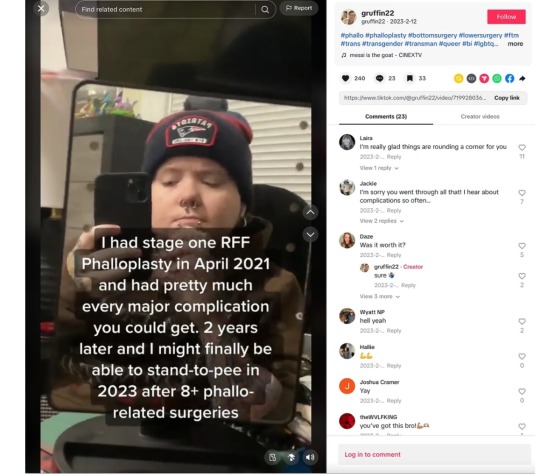
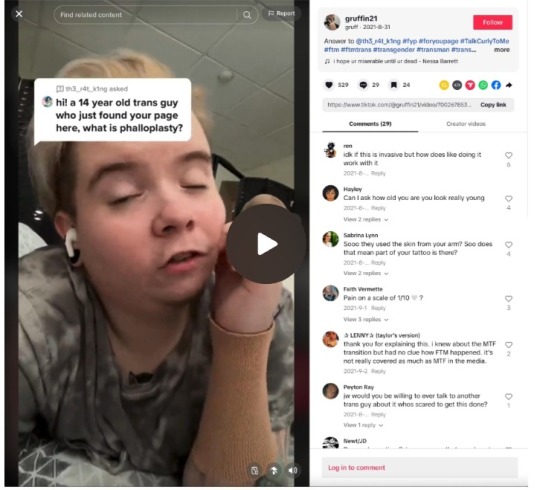
Or you could listen to Griffin herself. Because as it turns out, Griffin was quite an avid TikTok-er. Over the course of a few years, she posted regularly on the app, where she talked about her surgery. As time went on, her posts became more and more about the complications of her surgery. In her last post, she looked quite ill. Two months later, she was gone. Her TikTok profiles are still up, and they can be viewed HERE and HERE. Griffin chose to share these parts of her life publicly, so we encourage everyone who wants to understand her perspective to listen to her share her experiences in her own words.
Here is one from just a little over three years ago, where she highlights the surgeries and “gender affirming” medical interventions she has had. Notice she started testosterone in 2014, which would have been when she was around 14 years old.
In this video Griffin can be seen driving to the hospital for yet another phalloplasty revision surgery, just six months later:
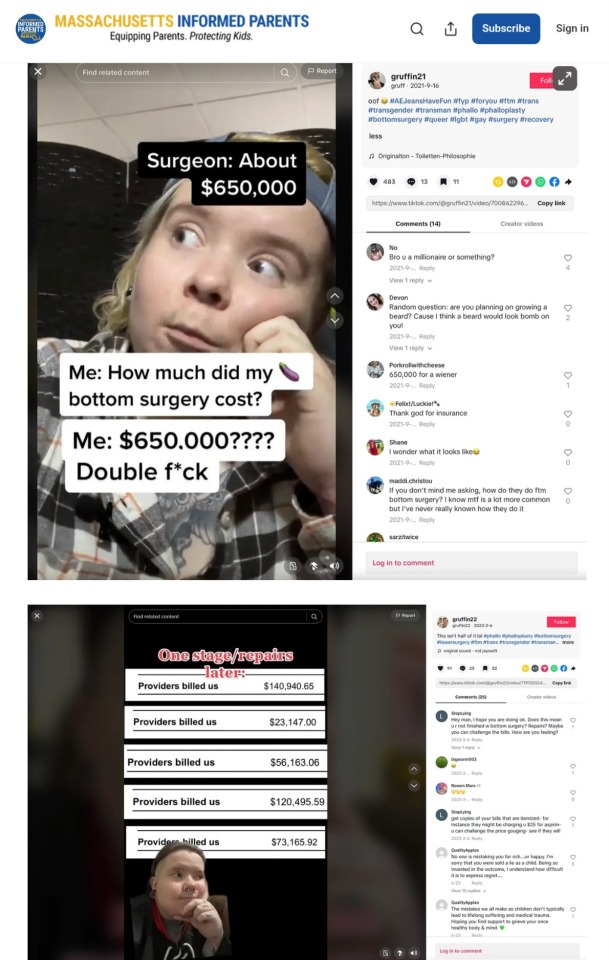
And just two months later she shares her grand total of phalloplasty-related surgeries to date: 8. She had eight surgeries on her genitals, and her neophallus still didn’t work the way she wanted it to.
Her TikTok doesn’t give much additional information on her health after that, other than her last post, where she sadly looks rather ill.
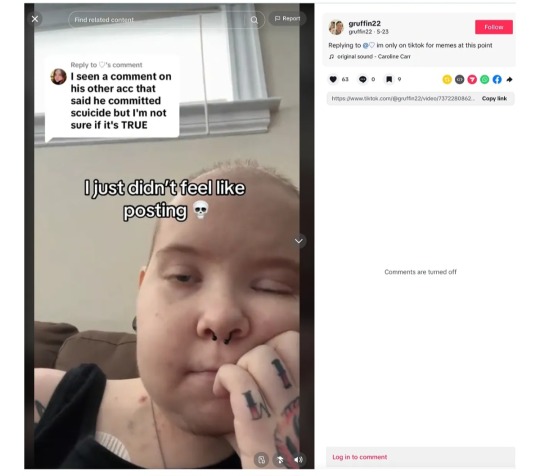
Now, heartbreakingly, she is gone.
We don’t pretend to know Griffin, or to understand all of her motivations or everything she went through. For the perspective of someone who has followed Griffin much more closely and had engaged her online while she was alive, go over to Twitter/X and check out user Exulansic’s profile, @TTExulansic. But even with our limited perspective there are many important things that can be learned from this tragedy, and to prevent future suffering for other people like Griffin, they must be explored.
“Gender affirming care” harms. Sometimes, it kills. Based on the evidence we saw, Griffin’s medical issues all seem to be traceable back to the surgical and medical interventions provided by “gender affirming” doctors. She spoke openly about the physical suffering that came along with the surgeries. While she maintained a public facade of being glad that she had a “penis,” she warned other people about the devastating physical impacts of her surgeries (see below). For almost half her life, she was a medical patient, all in the name of affirming her trans identity. While we don’t know the exact cause of her death, it is fair to say that at the very least, her “gender affirming care” left her physically weak and fragile. At worst, it killed her. (And if it did, it wouldn’t be the first time this happened. Here’s an article about another young person who lost their life due to “gender affirming” surgery.)

Losing a child is every parent’s worst nightmare. But affirming your gender-confused child’s trans identity won’t keep them safe. Parents of children who express a trans identity are often told by professionals that they must go along with the child’s new identity because otherwise, their child will kill themselves. “Would you rather have a living son, or a dead daughter?” counselors, social workers, and pediatricians ask traumatized parents. Manipulated and distressed by this question, many parents affirm their child’s trans identity because they feel they have no other choice. From what we can tell, Griffin’s parents were supportive of her trans identity. They used her preferred pronouns. At the age that most kids are entering high school, Griffin was already allowed to take cross-sex hormones. Her parents seemingly did what counselors advise parents in their situation to do - they affirmed her self-professed male identity, and they allowed her to transition. But tragically, their daughter is gone. The “gender affirming” treatment didn’t ultimately save her.
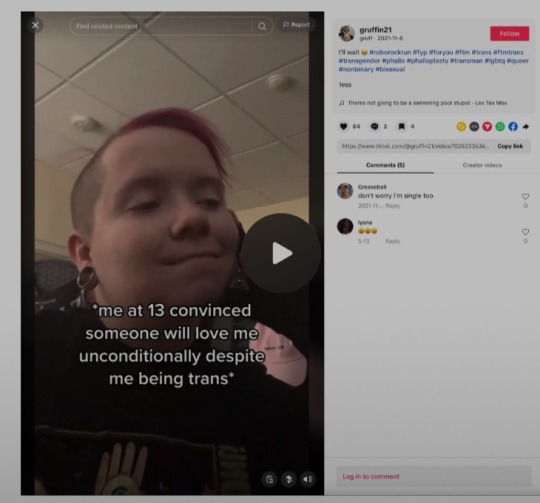
Hurting people hurt people. We don’t know what led Griffin to adopt a trans identity at 13 years old. But we do know that it is not uncommon for young people to seek solace in a trans identity after some sort of sexual assault, or simply because they feel so uncomfortable in their own developing body that they think it would be easier if they were a man instead. Regardless of her reasons, it is clear from Griffin’s TikToks that she was hurting emotionally as well as physically. And yet, it’s also possible that she hurt other impressionable young people by using her platform to promote gender surgery. In the TikTok below, she is answering a question from a 14-year-old “trans guy” about the ins and outs of phalloplasty. In it, she says that phalloplasty “surgically creates a penis.” This is simply not true. A neophallus created by phalloplasty is not the same thing as a penis. But the young person asking the question views Griffin as an expert, and they are left with no reason to question her answer. It makes you wonder: were confused young people enticed into a dangerous medical pathway by watching Griffin’s videos? Is there unintentional collateral damage from Griffin’s influencer persona? We may never know the answer to this question, but we do know it’s one more reason why parents need to keep their kids off of social media.
“Gender affirming care” is big business - for surgeons. In the TikToks below, Griffin gives two different figures for how much her doctors billed insurance for her phalloplasty and related surgeries. In a third video you will see later in this post, she gives yet another figure. The amounts don’t add up, but they are all astronomical. If anyone was still wondering if a perverse incentive exists for surgeons to do these dangerous, radical surgeries… well, now you have your answer.
Griffin received her “gender affirming care” in MA, and the doctor who performed her phalloplasty is still performing this surgery on other young people. Griffin identifies her surgeon in the TikTok below. His name is Dr. Oren Ganor, and he is the co-director/co-founder of the Center for Gender Surgery at Boston Children’s Hospital. Gender surgery at Boston Children’s has a complicated and controversial history, and they have (unconvincingly) denied performing gender-affirming surgeries on minors. According to this article, Dr. Ganor has argued that the capacity for gender surgeries for minors needs to be increased. What does Dr. Ganor think about what happened to Griffin? Was Griffin’s surgery deemed a success? We hope a medical authority looks into this. Regardless, it’s important to know that Griffin didn’t get her surgery done by some hack in a back alley. She didn’t fly to a third-world country to get bargain-basement surgery. She went to the co-director of the most prominent gender surgery clinic in the state, and still faced this disastrous result.

In this post Griffin accuses Safe Homes of allowing adult predators access to vulnerable minors (in this case, under the guise of a drag show - ironically, the very thing we are always told doesn’t happen), of looking the other way when sexual assaults occurred, and of employing a “literal child groomer'“ who was continued to be allowed to work with minors even after they were reported.

Safe Homes encourages minors to join their Discord community. Discord is a website known for being infiltrated by predators. It allows for private chatrooms with little accountability, and most parents don’t know it exists.
Now, we can’t speak to Griffin’s accusations specifically. But common sense tells us that if an adult wanted to gain access to kids for nefarious sexual purposes, one of the best places to go would be an organization that attracts impressionable kids based on their perceived sexual identity and wraps its actions in the seemingly impenetrable rainbow-colored cloak of “Love is Love.” We imagine that it must have taken a LOT of courage for Griffin to publicly criticize an organization like Safe Homes, especially as a member of the “LGBTQ community.” While we have not yet been able to verify Griffin’s accusations against Safe Homes, we were able to verify her involvement there. In 2016, she was awarded an award at their annual gala. See her name in the photo below, which you can also view HERE.

Safe Homes is clearly a powerful and influential organization. What did Griffin see/hear/experience that pushed her away from the very organization that gave her an award? Do the politicians in these pictures know of her accusations against Safe Homes?
On her personal Facebook page, Griffin checked in to Safe Homes multiple times.

Griffin was also active on the Safe Homes Facebook page. In the post below, you can see that Safe Homes was very excited that “gender affirming” surgeries were coming to Boston. Chillingly, you can also see that Griffin “liked” that post. Is this how she first learned of the very surgery that would destroy her health, and possibly lead to her death?
It seems she was unsafe at “Safe Homes,” in more ways than one.


We checked out what Safe Homes has been up to lately, and we didn’t like what we saw. First of all, we saw multiple posts in memory of Nex Benedict, the “nonbinary” young woman from Oklahoma who tragically died of suicide but was falsely hailed in the media as a martyr after it was incorrectly reported that she was killed in a hate crime. Yet there was not a single post honoring Griffin, a past recipient of their “People of Courage” award, who was actually part of their organization and whose funeral was several weeks ago.
But their apparent ignoring of Griffin’s tragic death wasn’t the only terrible thing we saw. Safe Homes, which services kids as young as 14 (and focuses on ages 14-23), is leading more young people down the same path that harmed Griffin. They are ushering more confused, hurting young people into the gender medicalization pipeline by offering easy access to “short-term counseling for individuals seeking letters for HRT or gender-affirming surgeries” at their “Safe Homes Transgender Resource Center.”

They bring in special speakers, like this woman from Planned Parenthood, to talk to minors about hormone treatment:

They teach minors how to legally change their names:

And despite Griffin’s publicly expressed concern about how a Grindr-loving groomer drag queen had gained access to minors via Safe Homes in the past, they still seem to be bent on bringing drag queens around kids. Here is one recent example, where they were involved with/promoted a screening of the Barbie movie for “Youth Pride Night,” where a drag queen Diva D was set to perform:

And here’s drag queen Diva D, who you might remember from dancing on a table at Sutton’s Connections Conference. He’s not the only drag queen that Safe Homes has brought around minors, but he’s the most recent. (And for the record, we think it’s odd that he just can’t seem to get enough of performing for minors. You would think that the amount of negative feedback he received from his performance in Sutton would have inspired him to stick to performing for adults, but apparently it didn’t.)

A month before that event, Safe Homes hosted a drag show at The Rose Room Cafe in Webster. There was no minimum age noted to attend this event. One of the drag queens who performed, Lana Backwards (aka Rhys Stuller, née female), was a high school friend of Griffin. According to a tribute written on Rhys’s Facebook page, Rhys and Griffin attended Safe Homes together as teens - a fact that, given everything we now know about Griffin’s concerns about Safe Homes as well as the trajectory of these two girls’ lives, feels like it needs more investigation.

Safe Homes’ parent organization is Open Sky Community Services, a massive organization that provides community services to all of central MA. They openly support Safe Homes’ mission, including publicizing the Transgender Resource Center that provides easy access to hormones and surgeries for gender-confused youth.
Does Open Sky care about what happened to Griffin? Do they know that their support of “gender affirming care,” the combination of bad science and medical malpractice that has devastated the bodies and minds of so many impressionable young people, very well could have led to Griffin’s untimely demise? We think someone should ask them.
A quick google search provided evidence that Safe Homes has a foothold in many MA public schools. Fitchburg High School lists them on their guidance website as a mental health resource. Worcester Public Schools shared Safe Homes as a resource as well. Burncoat and Worcester Technical High School have invited Safe Homes to speak to their classes, as have Northboro Middle and High School. And we know that Safe Homes works with Pride Worcester and SWAGLY, both of which have been known to network with MA public schools.

To the Sivret family, we again extend our sincere condolences for the loss of Griffin. Our earnest prayers for comfort will be with you during this time of profound grief.
To parents everywhere, this sad loss brings to light many important things that we must all know in order to protect our own kids, and the kids in our communities. We can’t trust social media influencers to give our kids good advice, especially if they are in the middle of fighting their own battles. We can’t trust the medical establishment to keep our kids safe, not even highly regarded doctors who work for prestigious hospitals. We can’t trust our schools to protect them from outside organizations that, according to Griffin, allowed bad actors to prey on vulnerable minors. And we certainly can’t trust those same outside organizations to place our child’s health and well-being over their commitment to radical ideology - even if they have the glitter of prestige and host galas attended by high-ranking politicians. We must be aware that all of these systems, and all of these institutions, can fail our children. We have to know this story so that we can protect them. Because while what happened to Griffin is happening to kids and young adults all over the country, this time it happened in our own backyard.
May those who loved Griffin remember her fondly. And may the rest of us remember that no family is immune from this form of heartache. It is up to all of us to be eyes-wide-open, so that if it is our child who believes the lie of gender ideology, and they think gender surgeries will make them happy and whole, we can tell them the truth. And we can tell them this story. #equippingparents #protectingkids
#Rest In Peace Griffin Sivret#The consequences of trans surgeries#Phalloplasty#Phalloplasty surgery carries a high rate of complications#Scott Newgent is an activist raising awareness of the complications of phalloplasty#Cross sex hormones for minors#people getting such horrible results from people considered the best in their field is proof that these surgeries are too experimental
6 notes
·
View notes
Text
A WATER TYPE MILF, DEM TIDDIES STAY ON SQUIRTLE.ᐟ

*REPOSTED! tumblr sucks. plz boost!*
♡ thots expanded from this post ♡ 𝓬𝔀: MDNI 18+ ONLY. choso x milf!reader, toji x milf!reader, although not rly full on choji. a lil fluff, a lil angst, a lil crack —tho mostly filthy domestic smut dripping in milf kinks. [plz dm me for h-anime name if you want it]

half-curse roommate!choso who you moved in with because its not like you can live with your on-again-off-again babydaddy!toji —the sorcerer killer —with a whole ass baby. although toji is an active co-parent (well, as active as a paid assassin who is gone most days of the week can be) what’s glaringly apparent to you is that toji doesn't have the best reputation. and you having the cursed energy of a mere window meant you couldn't protect yourself nor your 6 month old baby girl, should a long list of people come looking for him. staying with him, according to you, is out of the question. so when you need to move out of your apt and you heard from yuji that choso needed a roommate and didn't mind a young infant, you were sold. plus, toji thought he was a 'harmless enough lookin' chump' who could at least put up a fight against any threat… and the rent was cheap.
half-curse roommate!choso who's like a godsend as he's so helpful and considerate of you and the baby. he doesn't mind the all the crying. or that you are too exhausted at times to clean up properly. and that 9 times out of 10 you look a general hot ass mess while at home. if that weren't enough, choso would even play with your baby girl, letting you get in a much needed nap in. you tell him every time you’d only need 20 mins and he can wake you up but choso will sit with her on the sofa until you wake up. possibly hours later, but choso claimed he was happy to get to act like a big brother again. a natural born 'big brother type', choso will watch cocomelon for hours and let her cute chubby fingers tug on his pigtails. all while he makes funny faces that without fail guarantees a burst of tiny giggles, even if she'd previously been crying.
half-curse roommate!choso who also doesn't seem to mind when toji, said actual baby daddy shows up unannounced, usually at some ungodly hour to 'see his girls'. although you suspect that by 'his girls' instead of you and the baby, toji means your milk swollen tits and your creamy mommy pussy, as toji spends more time interacting with them than you or the baby. it's only a 2 bedroom apt too, so as not to wake the baby, you are usually fucking in the living room. not very subtly either. it's not like you’re the one lacking in decency though. you always full-on deny toji sex in favor of heavy petting under a blanket. yet after toji's made you lather his fingers in your squirt for the third time that night, your mommy brain, still trying to balance your hormones, goes completely smooth. its easy then for toji's minor requests for you to return the favor by 'just warming his cock up a lil' bit' always lead to major backshots off the edge of the couch. those deadly backshots, were how you got pregnant in the first place, mind you. thankfully, while you're face-down-ass up, you’re blissfully unaware. otherwise you’d be mortified that the sounds of your cushion-muffled moans and wet flesh slapping together drown out the shuffling scurry of feet and carefully shut doors when your roommate has to cross the living room to use the bathroom in the middle of the night.
half-curse roommate!choso who although you think is super sweet, being half curse makes him a bit naive. still, his endearing boyish charm is much welcomed when you are so used to toji's gruff and blunt personality. you also love choso's reactions when you flatter him with compliments like: 'you're the best choso!' or 'what would i do without you?' choso's ears will always redden he becomes bashful and quiet. you really mean every word tho! although you always get the biggest reaction, widening eyes and a blush that extends past his ears to his cheerful cheeks when you adoringly profess 'choso, you'll make such a good daddy one day ~♡ ' if he's even choked on his own spit a few times and you have to hide your giggles as you pat his back until he can swallow properly again.
half-curse roommate!choso who deliberately takes night shifts now. not just to give you your privacy for when toji comes over, but he tells you it's so he could watch the baby in case your nanny, who has bailed on you a few times before, doesn't show up. when you protest, telling choso he doesn't need to rearrange his whole life for you, he won't hear anything else about it. he's half curse he reasons, he's more suited to patrolling the night shifts anyway. you honestly don't even know how to thank choso who is honestly more of a co-parent then toji at this point.
half-curse roommate!choso who practically has a heart attack when he comes into the kitchen on his way to work, to find you with your bare breasts out feeding your baby girl on one boob and a pump machine on the other. you quickly have to calm him down and let him know that it's a perfectly natural thing to breastfeed in the open and is nothing him nor you need to be ashamed about. although it's true you usually pumped at night when choso was already at work so your baby could have fresh bottles for the morning, today your breasts were extra sore from being so full and your baby girl much too fussy. so that's what had you in the kitchen for an impromptu feed n' pump session.
half-curse roommate!choso who apologizes for his reaction as he didn't mean to offend you (he didn't, but he's soooo cute for thinking he did). opening up to you, choso divulges he never knew any of this as he didn't grow up with a mom. you knew choso was half-curse but you're shocked to discover he's a literal test tube baby and thereby completely unaware of most healthy parent-child dynamics. choso was definitely never breastfed. you smile at his genuine curiosity when he asks you to tell him more. so you explain that this impromptu feeding is more to pacify the baby. other than nourishment, nursing was one important way a mother could bond with a child so young. it provided the baby comfort and was one of the best ways to get them to settle down. and just like magic before choso's eyes your baby girl had been soothed in a matter of minutes, her anxious gurgles calming into soft coos as she sleeps.
half-curse roommate!choso whose desperately tries to retain eye contact as he converses with you at the kitchen table. your totally clonked-out baby girl had unlatched and you proceeded to have a normal conversation with him like your whole swollen n' leaky tit wasn't so casually exposed. choso berates himself to focus and 'act normal'. he knows its normal, you told him as much yourself and you're being normal. so why does choso feel everything but normal right now? choso panics. It’s way too hot in here! he had to get out, like now —what time was it again? standing up abruptly, choso sudden motion startles you when he announces he would be late to work, if he didn't leave right now. choso immediately regrets it though once he sees your furrowed brow and plump lil pout as you had been enjoying your conversation. choso knows because of the baby and toji that you don't get out much. frantic to make amends, choso can't help but to pay you a compliment on his way out the door. now it was your turn to blush wildly when he sincerely looked you in the eye and says—
“heh, i wish i grew up with a mommy, especially one as lovely as you.”
half-curse roommate!choso who comes back home earlier than usual that night, around 3 am but looks like he's worked a whole weeks worth of night shifts from his worn down appearance. his robes are tattered in various places, the bags under his eyes are more pronounced than usual, and wait... is that blood!? it took him a while to snap out of his dissociative melancholy, to notice you were even awake at this hour. trying to keep it together, choso gives you a smile that doesn't quite reach his own gaze. he honestly expected you to be asleep, as your baby girl usually slept well throughout the night. but you told him she had woken up an hour ago hungry and now you couldn't fall back asleep. truly though, you are a sight for sore eyes to choso. yet choso still cant help but feel more like a burden and failure when you begin to worry over if he had any injuries. the blood on him isn't his though, its civilians. so many, he hadn't been able to save everyone when a special grade curse had attacked a large apartment complex. 'its not your fault choso!' you along with everyone else had told him but it doesn't make it hurt any less. seeing people cry out for their fallen loved ones, he knew that pain all too well. no one else should have to suffer it while he had the power to prevent it.
half-curse roommate!choso who you make it your mission to comfort. he's always doing everything to help you, it's the least you can do in his time of need! gently you drag choso by one of his muscular arms to the sofa. you motion for him him lay his head on your shoulder and once he is settled, your arm cradles his head with delicate pats. however, it’s when you feel choso’s silent, wet tears hit your skin and he can no longer hold back his trembling, maternal instincts kick in. You immediately guide him to lie on his side, pulling him against your plush, buoyant chest so you can cradle him close, slipping effortlessly into full "mommy-mode." you coo lovingly for him to 'let it all out' as he sobs. you figure grown man or not choso is unlikely to ever have been given the grace just to unload on someone. he certainly wouldn't with his only remaining brother, yuji, who choso would never dream of burdening with his own problems. yet, like an angel, your warm hushes and gentle rocking soothes choso, wrapping him in a comforting embrace like a much needed security blanket. With soft caresses, you brush his wispy bangs away from his handsome face, keeping them from sticking to his tear stained skin. choso in turn pushes his face deeper into your bosom, clutching onto you like a lifeline.
half-curse roommate!choso who you'd been holding for quite a while when it finally dawns on you the increasing puddle of moisture you feel on your chest isn't the result of his teary sobs but your leaky tits. omg owww! and no sooner did you notice that fact then the familiar ache of them being too full confirms it. its clear to you now choso's crying had triggered your milk production as it if he had been your own child! although speaking of baby girls, choso looked so sweet and content with face buried into your plush curves, his own tears now dried. you absolutely hate to have to move him. but you knew you needed to because while you weren't ashamed of your completely natural bodily reactions —you also had enough couth not to drip your breast milk all over someone's face!
half-curse roommate!choso whose cheek you swipe feather like touches over as you tell him you have to get up. choso's response of course though is to hold on to you that much tighter. his croaky whispers plead to you, proclaiming how this 'feels so nice' —outright begging to stay like this for just a bit longer. and while his sappy puppy dog pout is activating something in you, and you want to give-in, the increasing swell of your tits is becoming unbearable. you need to go pump, like asap. so you try to bargin with choso that you can hold him more in a bit but right now you are soiling yourself and him.
half-curse roommate!choso who curiously enough, had been oblivious that the soaked wetness gathering between the both of you is no longer coming from him. daring to lick his lips, choso whimpers as he can taste the creamy, and mildly sugary, secretions that settled on them. you're so mortified to see choso's face covered in a sheen of your breastmilk you fail to notice just how intensely he’s been staring at your nipples. your pert lil' buds, practically greeting him, beckoning to him, centimeters from his face through your now soaked, transparent white pj top.
half-curse roommate!choso who upon zeroing in on the small pearly beads of milk pebbling through the fabric of your shirt, instinctively leans in to lap it up with a tentative lick. the action shocks you as you gasp, swallowing hard. your breasts feel so heavy with milk and are positively aching to release even the tiniest bit of it. unfortunately, choso's continuous microlicks only tease the idea of relief, the texture of his tongue chafing your soppy tee against your sore nips which had begun to tighten even harder— it was pure torture.
"c-choso!"
half-curse roommate!choso who when hearing his name squeaked out in such a pitchy cry immediately stops. instantly realizing what he's doing a stream of "s-shit shit, m'sorry, m'sorry!!" appologies slur out of him. choso looks up at you sheepishly, face burning in shame as he continues. "i-it's just that you're so soft n' warm... n' i've never felt so safe anywhere before, well ever! i swear it! i-i know that's no excuse but it tasted s'gud..." not being able to look you in the eyes anymore you can tell choso is about to pull away and instantly your fingers tangle up around one of his pigtails, holding him in place. you shake your head. "mm n-no, cho if you want to have some more, you can... if it's not too weird for you." all your good sensibilities are screaming at you, this isn't a good idea. never in a million years did you expect to be in this situation with choso. however such is life, and the facts are now: its late, your tiddies ache miserably and choso is giving very much eager baby girl ready to be nursed. how could you be expected to have the willpower to disengage??
"ya know, you'd actually be doing me a favor cho... pumps can be so uncomfortable and a mouth always feels so much better… um, is that okay?"
half-curse roommate!choso who thinks its more than okay and from then on gleefully volunteers to become your living, breathing, personal breast pump. you had to dump so much of what you would normally pump anyway, your body working overtime to produce milk as your baby girl definitely had the appetite of her often absentee daddy who at least would send money for bills and diapers consistently. sweet baby jesus, toji would most certainly go slap the fuck off if he found out about these breast pump!choso sessions. but tbh? fuck toji because he isn't here to drain your overactive milk ducts, choso is. and choso is so eager to do it too! its toji's own damn fault you decide. just like you decided to rationalize to yourself that choso latching onto your milk bloated tiddies is strictly quid pro quo. choso's simply helping you drain your tits and you're giving him the intimacy he so desperately craves. this is a friendly thing… you’re healing his inner-child and fears of abandonment —if anything you're like his mom, right? perfectly platonic.
half-curse roommate!choso who forces you to confront the fact there's nothing platonic to you about him so lewdly moaning out 'mommy' as he swirls his tongue around the plump fat of your puffy areolas. you can barely see his face now as choso isn't content unless he's practically suffocating himself under your heavy mammaries while he nurses on them. you swear choso would swallow your whole boob completely if he could get it all in his mouth. not leaving the other ignored, Choso’s hand gently bounces and massages the one he isn’t sucking, stimulating milk flow to be ready for when her turn comes. you suppose this was also around the same time he started calling you 'mommy' and that you'd end your pump sessions with your thong wet, sticky and practically glued onto your twitching cunny.
half-curse roommate!choso who causes your thoughts wander to more debased and salacious fantasies the longer he's latched onto you. would choso latch on just as well to your clit? would he smother himself just as deeply into yout cunt? and most importanly...would he enjoy suckling out the savory umami flavor of your pussy juices just as much as your sweet creamy tits? you imagine choso would do just as good of a job coaxing your cunt to spill its nectar as he did with your lactating breasts. these lewd ponderings ensure that by the end of every one of choso's feedings your pussy would be aching far more deeply than your tits ever were. but there was one BIG problem preventing this from becoming your reality...
half-curse roommate!choso who you aren't getting any sexual vibes from. at all. you think, like a lot of things, choso is clueless. so of course he doesn't know how often your clit pokes out between your pussy lips to throb to the flick of his tongue on your stiffened peaks. nor how your actual tummy would flutter, abs sucking in aggressively when he'd accidentally rake his teeth over your pert flesh... how could he? he wasn't even hard! your 'baby girl' choso would even doze off at times, all the while languidly slurping your soggy nipples raw. although it's not like you could really tell for certain... choso is always in baggy sweats or robes. you'd convinced yourself though that even if choso was a little slow on the uptake, he was still a man. and you knew exactly how men could be, thanks to toji. there's no way he could have contained his urges over a half dozen times if he was felt anything erotic about the way he’s so viciously slurping up the suds of his spit and your milk. choso is so sloppy with it, there’s rarely a moment where milk isn’t dribbling down from the corners of his lips.
half-curse roommate!choso who you are able to confirm definitely gets hard when after a nursing session, you spy him in the bathroom through the crack of the door. choso failed to shut it all the way. this gives you the perfect silver of a view to see him hunched over and resting his forearm on the wall, as he frantically jerks himself over the toilet. much of choso's black undershirt is currently stuffed into his mouth, giving him chipmunk cheeks as he attempts to silence his needy whimpers. the entirety of his sculpted abs and pecs are on display and your eyes can’t stop their journey to drift lower and lower. your own legs rub together as you notice how much choso is actually shaking, ferally chasing his nirvana as he thrusts his—rather large n' hefty cock —into his pre soaked palm. holy shit he had to be as big as toji! you're openly gawking, the crack in the door opening a little wider with your face pressing against it but choso isn't even in this reality anymore to be interrupted. his eyes squeeze shut as he envisions his thick cock between your bouncing tits, your sweet nourishing milk oozing over his balls. safe to say, choso had been extremely hard up this entire time. you find out just how hard up too when after immediately cumming his dick is still twitching as he starts stroking himself once more, you’d stand there while he would do it do twice more too.
half-curse roommate!choso whose eyes fly open during your very next feeding session when not 5 minutes in your delicate hand cups his dick over his sweats outta nowhere. oh he's VERY hard. choso is a hair away from bussin right then when he feels your silky smooth hands sneak beneath his sweats grasp his hefty cock. his breath hitches around your breast as he chokes on your milk from you running your thumb over his wet slit. choso's fat round cockhead already dampened his swampy shorts with pre. you can't even fit your hand all the way around him but that didn't stop choso's eyes from rolling back into his head when you give him those first few pumps. soft grip twisting using the liquid already running out of his tip as lubricant.
"ungh, whaa...?"
half-curse roommate!choso who can't even succinctly question what's going on because the fact you actually have your pretty palm around his cock is melting his mind and destroying any sense he has of space and time. this had to be a wonderful dream? had he somehow fallen asleep, drowned and or smothered himself in your breasts and this was heaven? it felt like it. shit, his own rough hand could never compare. you sweetly blow a kiss down at him, your movements only increasing in speed and friction.
"you earned this, cho. it's only fair mommy milks you after you've done such a good job for mommy being her pump baby..."
half-curse roommate!choso who hisses when you fully tug his engorged length out of his shorts. his cock pulses angrily, still inflamed even as the cool air hits it. fresh hot tears run down choso’s cheeks and spill on your chest as the pleasure is almost unbearable for him. choso won't last long the way his red tip is sobbing, soaking on to his quivering belly and you know it. "
c'mon baby. be a good boy and cum for mommy, yeah?"
you moan as choso nips and sucks ferally at your tits, other hand twisting and pinching your wet n puffy nipples enough to make you whine for even more. god, you’d never been this sensitive??would you finally cum just from your tits? watching choso fall to pieces in your lap and on your breast is something you didn't know how much you needed until this very moment.
"mommy m'c-c-cumming!"
lifting his hips to thrust up into your hand, choso spurts his frothy load like a supersoaker. it’s like a geyser, so much more than you'd ever seen a man cum before —and by your hand alone! your fingers attempts to contain his vicious cum but it spurts out everywhere. syrupy semen coats him, the sofa, and especially your forearm. a deviously sweet smile plays on your lips when your hand doesn't stop its twisting and pumping motions. getting every last bit of milk out, like choso had always done for you.
"mmm' nah cho-cho, i think you can give mommy more right?"
sniffling around your breast choso blissfully pleas for your to wait but his greedy little hips never stop, chasing even more ecstasy despite his over sensitive cock making his head swim.
"m-mommy m'pweaseeee..."
"mommy? huh? the fuck is all this bullshit!?"
oh whoops, when did toji get here?
half-curse roommate!choso who you have to shield from the wrath of babydaddy!toji who is totally crashing tf out over you catching you in such a compromising with choso. toji is roaring for you to get out of the way so he can 'handle' this. you refuse, telling toji he’d never see you again, your pussy or your tits... not to mention never see his daughter, if he harmed a single hair on choso's pigtailed head. your voice, elevated to a yelling to match toji’s, is what sets your daughter off and you demand toji go get her. you’re putting papa bear on time out. besides he needs to go cool off and spend time with his baby girl, who rarely sees him when she’s actually awake. you weren't in any kind of relationship with toji so he had no right to be angry. surprisingly, toji just grumbles, and obeys. glaring death at choso on the way to your bedroom. he's barating himself for even thinking that dweeby loser was harmless. although toji coulda swore choso was a eunuch at first glance.
babydaddy!toji who honestly, isn't even livid over seeing your freshly manicured nails, that he'd cash app'd you the money for, overflowing with choso's cum. your grip, still stroking the last spurts from his spent cock. a sympathy hand job wasn't too surprising really. especially since toji knew fapping is exactly what the lil' emo cuck did in the bathroom the nights toji actually spent over. choso would pathetically beat his meat to the squelchy sounds of your stretched, wet pussy, farting around toji's girth, ripping through your guts.
babydaddy!toji isn't even particularly upset with choso's pathetic display of tears, cumming like a whiny bitch boy while calling you his 'mommy'. disgusting. no frankly, what's really got toji hot and wanting to spill choso's blood is the massive messy milk ring pooling around choso's mouth and running down his chin. rage seethes through toji at the revelation: it's choso's fault toji hadn't been getting as much milk lately when he'd come over to play with his favorite girls (your tits).
half-curse roommate!choso who doesn't know how bad toji is plotting to get him out of the picture for good. somehow without harming him and pissing you off. toji wouldn't stand for this much longer though, that milk was meant for just for toji (and his daughter ofc, he supposes).
tsk, fuck! —suckin’ on those jumbo mommy milkers was the only reason why babydaddy!toji had worked so hard to get you fucking pregnant in the first place. >:(
♡ blkkizzat ©2023-2025 ♡
♡ strictly prohibited: ai, copy, plagiarism, redistribution, translations. ♡
𝓪𝓷: i'm ovulating and i need one of these men to put a baby in me. choso and toji with lactating kinks make my brain go crazy. one day ill write the gojo x nanami x milf!reader lactation fic based off one of my fav h-animes lol bet. also no one yell at me i wrote these at work and school when i was bored and my actual full fics i need like my entire focused brain to write lol
♡ funny meme i made for this fic ♡
reblog and comment please!♡
#the demons won y'all#so wrote this with my pu$$y not my brain if you couldn't tell lol#no thots - head empty - coochie wet#✎ᝰ𝓀𝒾𝓏𝓏𝒶𝓉¢σσкє∂тнαт#✎ᝰ𝓀𝒾𝓏𝓏𝒶𝓉¢σσкѕ#choso kamo x reader#toji fushiguro#choso smut#jjk x reader#toji x reader#toji fushiguro x reader#jjk x you#choso kamo#jjk smut#toji smut#jjk x reader smut#jujustsu kaisen x reader#jujutsu kaisen x you#choso x reader#jujutsu kaisen#choso x you#jjk choso#choso x female reader#choso x y/n#jjk x y/n#jjk x black reader#choso x black reader#choso kamo x you
3K notes
·
View notes
Text
Juno (Hotch x Fem!Reader) -- one shot
Hello again! This goes from zero to 100 in two seconds flat don't @ me!! Sabrina's new album came out and reawakened something in me (everyone say thank you Sabrina) (also this is not beta'd I wrote this in a short n' sweet haze)
Summary: Aaron is working from home but what paperwork he needs to do is the absolute last thing on your mind.
Warnings: smut! 18+ only! this is so filthy! in no particular order: multiple orgasms, cockwarming, choking, brat tendencies, stoplight system, unprotected sex, breeding kink (briefly), face fucking, overstimulation
WC: like 3,400 I lost my damn mind clearly

You’re not sure what’s gotten into you. Blame it on period hormones (probably) or the fact that Aaron looks absolutely delicious right now in his tight black t-shirt (most likely), but you’re going to go insane if either of you have clothes on for another five minutes.
The problem is, Aaron is trying to focus. It’s one of his days where he works from home, an idea you gave him when you realized how easy it would be for him to do the same paperwork just from the comfort of your living room. It was a brilliant idea at first. You got to see him more, and were able to do your own thing around the house while he did his work. You got to have lunch together, and offer a genuine mental break in between his mountain of paperwork.
Now, though, you can’t find it in you to give a single fuck about whatever needs to be signed, who needs to clear what, and what phone calls he still needs to make.
“Honey,” you call sweetly from the kitchen. You watch him from over the island, your thoughts going all sorts of ways -- namely, deep into the gutter. “Want to break for lunch?”
You see Aaron shake his head, still typing furiously on his laptop. “It’s not even noon yet.”
“Brunch?” you try again, walking out of the kitchen. You lean against the doorframe, crossing your arms over your chest in the way you know he loves because of the view it gives him of your cleavage. And you’re wearing a v-neck shirt today for that exact reason, too.
Aaron still doesn’t look up. “I’m sorry honey, maybe in an hour?”
You let out a huff that you know he hears because he finally looks up, eyebrows raised just so. It’s a look that you love. Curious, veering toward that playful annoyance that you can’t seem to go a few hours without his undivided attention.
Which, you can, by the way. You’re more than capable. It’s just that right now, it’s a crime that his eyes have been looking at paperwork when they should be looking at you.
“Are you okay?” he asks, and there’s some hesitation in his voice. You know he’s assuming the worst. That you’re not okay mentally, and that’s why you need him to take his lunch break now or maybe for the rest of the day. He’s done it before on your darker days.
But you’re okay. You’re perfectly fine. You’d just be even better if he put the damn laptop away and put his fingers to use somewhere else.
Which is exactly why you come to a stop in front of him and reach forward, tilting his screen down and down until it closes. He lets you.
He lets you take his laptop and put it on the table beside the couch. He watches you, his fiery brown eyes taking in every second. He lets you straddle his hips, your arms circling his neck.
“I see now,” he smirks, his hands finding their rightful place on your waist and squeezing lovingly. “By ‘lunch break’ you mean…”
“Put a baby in me,” you blurt, rocking your hips against his.
He stills, his hands making you stop your movements, too. His eyes are darker now in a way you haven’t seen in a while. “What?”
“Please,” you say, leaning your forehead down onto his, trying to move your hips again. “Need you.”
“Honey, we can’t have--”
“Yes I know the semantics, Aaron,” you mutter, now annoyed and lifting your head to glare at him. He has a vasectomy, you get that. “I mean fuck me like you’re putting a baby in me.”
His hands squeeze again. “I see.”
You frown. “Don’t tease me.”
“I’m not,” he smirks, one hand leaving your waist to stroke your cheek. “You’re adorable when you’re horny.”
You roll your eyes, peeling yourself off his lap. He lets you go, albeit with a curious look. You turn and head for the bedroom.
“Where are you going?” he calls out after you, still with that damn smirk lacing his words.
“To get myself off,” you reply in a deadpan. “Since someone--”
You don’t have a chance to finish your sentence before Aaron is right behind you, hands on your hips, spinning you around to face him. That look full of fire is back again, stern this time.
“Did I say you could do that?” he says in a low tone.
“Did I ask?” you retort, backing out of his grasp and darting into the bedroom.
Now there’s a smirk on your lips. It’s quickly approaching shit-eating grin territory, which you know will only egg Aaron on further. This little game of cat and mouse happens to be your favorite, and he knows it.
You’re barely two steps into the bedroom when Aaron is attached to your back yet again, this time wrapping his arms around your waist, locking you in.
“Color?” he whispers, his lips right at your ear, sending shivers straight down your spine.
You groan. “Green. Neon green. So green, I need you to--”
He spins you again, this time backing you into the wall and attacking your lips. Finally, you think, though you know you’re in for it now. The thought has a grin crawling up your lips, and you’re unable to stop it.
“What’s so funny, hm?” he scolds, moving his lips to your neck instead, to the exact spot he knows makes you weak in the knees. Like clockwork, he has to wrap an arm around your waist to keep you upright, your knees buckling when he bites down just so.
“Nothing,” you manage through a moan, tipping your head back onto the wall. “Shit.”
“You’re ridiculous sometimes, you know,” he says, but he’s smiling against your skin. “Can’t let me focus on work because you need me to fuck you.”
“In my defense,” you try, your hands scrambling for his shoulders, for something to ground you. “You didn’t fuck me this morning.”
“I fucked you last night,” he reminds you, as if you needed the reminder. It’s the reason you slept so soundly. “Was that not enough?”
You can’t help it; you laugh.
He lifts his head, raising an eyebrow at you. The same question as before on his lips.
“Sorry, I thought you were joking,” you say.
“You’re insatiable.”
“Guilty,” you grin, grabbing his face and pulling him back in for another kiss.
You make out against the wall for too long like two teenagers behind the bleachers at school. You hook one leg around his hips, pulling him in and grinding against his obvious erection. It’s enough to have him groaning into your mouth, pressing you against the wall with renowned vigor.
You can feel how wet you’re becoming and fuck, neither of you have even taken a single article of clothing off yet.
Aaron notices, one hand traveling south without you paying attention, too busy relishing the way he licks into your mouth, stealing your every breath. The kissing becomes increasingly sloppy when he works his hand into your leggings, under the waistband of your underwear, and into you.
“Oh my god,” your back arches against the wall, pushing his fingers deeper. He doesn’t bother with one, starting right away with two, curling them when you grind harder.
“You’re soaking my hand,” he practically growls into the next kiss, adding a third finger after only a few thrusts. Your body accepts it willingly, always ready for him. “Jesus.”
“More,” you gasp, pushing him deeper. “Aaron, more, I’m serious--” Your words break off as he scissors his fingers, making your eyes roll back instantly.
“I can feel you already,” he smirks against your cheek, pressing a kiss there, an action so sweet and gentle compared to what the rest of him is doing. “Come on, honey. You’re cumming as many times as you want.”
That makes you inch closer to the edge at a frightening speed. He says you can cum as many times as you want, but what he means is he’s going to force as many orgasms out of you as he can. Until you tell him to stop or he decides you need a break.
The thought of being an overstimulated mess in his embrace later has you climaxing against his fingers, your head falling onto his shoulder as his movements never cease, milking every last wave out of you.
You lift your head in search of his lips again, which he willingly gives to you, his fingers slowing to soothing strokes as you whimper into his mouth. You’ve only had one orgasm and you already feel ruined. He can tell the way you tremble against him, so he checks in once more.
“Green?” he whispers, kissing your forehead.
You nod. “Green. You?”
He smirks. “Absolutely.”
He picks you up into his arms, inelegantly tossing you onto the bed behind you. You giggle as you bounce on the mattress, tugging your shirt over your head as he does the same to his. His hands move for his belt and you practically jump to the end of the bed, swatting his hands away.
“Since when is that your job?” you frown up at him, unbuckling his belt without looking.
He laughs, petting your head gently. “So sorry, you’re right.”
“What was that?” you tease. “I don’t think I heard you.”
“Don’t push it.”
“I have no idea what you mean,” you smirk, pulling his belt out of the loops and tossing it somewhere. You don’t wait for him to reply before you unbutton his jeans, yanking them down with his boxers.
There’s just something about his dick. You hate that you love it, or maybe you don’t hate it at all. All you know is you need it in your mouth right now.
So, you do that, without any warning. Aaron thrusts forward into your mouth on pure instinct, not expecting you to wrap your lips around him so soon. You slide down the edge of the bed onto your knees, pulling him back to you by his thighs.
You take your time, pushing his jeans and boxers down further. When you pull back for air, he steps out of them and kicks them elsewhere, returning to you quickly, knowing better than to keep you waiting.
You swallow him down again, moaning around him in the way you know he loves. It takes all of two seconds before he gently holds the back of your head, asking silently for permission that you were already about to grant. You look up at him, batting your eyelashes as you squeeze his thigh twice. Go ahead.
The thing about Aaron fucking your face is that it took a while for him to do it as hard as you really wanted. He’s always so gentle, a quality that drew you to him initially. You love how gentle he can be. But you love it equally as much when he is rougher with you.
Like now, when he has you pinned against the bed, one hand on the back of your head as he fucks into your throat. It’s blissful, quite frankly, the way he feels, and you thank the universe every time for your lack of a gag reflex.
He holds you there with a deep groan, and you feel him twitch in your throat once before he pulls you off entirely. You frown up at him, once again not getting what you wanted, but he doesn’t have any time for that.
He picks you up by your armpits, hauling you back onto the bed. Your leggings and underwear are gone in a single second, along with your bra. He’s crawling up your body and crowding your space before you have a second to protest that he wasn’t down your throat for near as long as you wanted him to be.
All frustrations leave your mind the second he pushes inside of you, immediately sliding home, his hips flush against yours.
It’s a feeling you’ve grown to love, the way he hits you so deep. Another thing it took him a while to be comfortable doing.
He’s not average sized by any means, and you’re the first to admit it made you salivate the first time you saw. The first time he fed himself into you and worried that he was hurting you, meanwhile you were clawing his back because you wanted more. It hurt for a moment, only an uncomfortable pressure because he was bigger than your vibrator, but as soon as you were used to the size of him, you wanted all of him.
He stays there, deep in you without moving for a moment, grinding against you. His lips attack yours again before he pauses to lean his forehead on yours, trying to catch his breath.
“You drive me crazy,” he says on a shaky exhale.
You wrap your legs around him, thrusting your hips up to take him a little more. His hips stutter, pushing in the way you wanted him to, the way you know you can make him do involuntarily.
“Fuck,” he bites out, turning his attention to your neck again.
You thread your fingers through his hair, tugging. “Exactly. So why aren’t you moving?”
He nips at your neck. “Because if I move, I will cum right away.”
“Who said I only want you to cum inside me once?”
He groans again, fingers digging into your hips as you circle them, though he doesn’t try to stop you. “Greedy” is all he says, but he finally moves.
The thrusts are slow at first, Aaron clearly trying to pace himself. You can’t say you’re doing the same, already chasing your second high as he slams his hips into yours. Your hand reaches down to rub your clit, but is promptly smacked away by Aaron’s hand as he glares at you.
“Since when is that your job?” he echoes you from earlier, only this time, there’s more heat to it. He grabs both of your wrists, pinning them above your head to stop any other temptation. “Not this time.”
His thrusts pick up speed and depth, his body moving against yours in the exact way that makes you fall apart. It’s not often that he doesn’t let you cum from added clit stimulation -- not that you can’t without it; it just makes the high feel that much better -- but sometimes he does. It’s an ego trip for him as much as it is for you.
It also adds an unpredictable nature to it, which is why your second orgasm takes you by such surprise. You seize against him, your hands doing all sorts of squirming to try to break free of his grasp, but he doesn’t let you, and he doesn’t let up. You don’t realize why until you feel the warmth spreading into you as he reaches his own peak.
You’ve clearly worked him up as much as you worked yourself up because his thrusts barely slow down, and he doesn’t soften inside of you.
Instead, he pulls out only to flip you on your side, sliding in behind you and pulling your leg up and back over his hips. The action causes some of his cum to spill out of you, but you don’t have any time to focus on that before he fucks back into you.
You’ve ceased to have any coherent thoughts as Aaron whispers dirty nothings into your ear, one arm wrapped around your body to keep you pinned against him. The pleasure doesn’t stop and at one point, you question if your second orgasm stopped at all or if it has continued this entire time.
Aaron reaches underneath the pillow where he knows he’ll find one of your vibrators because he heard you using it this morning. No, he didn’t fuck you this morning, but you fucked yourself, and truly, at 8am, he should’ve known you’d end up like this by eleven.
Your mind doesn’t register what the sound means until the vibrator is pressed against your clit. Your body jerks, scrambling for some grounding, your hands finding it in wrapping them around his arm.
He switches hands on the vibrator, so one hand is free to wrap around your throat. Your eyes roll back as soon as you feel the gentle pressure, your body practically going limp against him.
“Come on, sweetheart,” he murmurs directly into your ear, his thrusts slowing to deep strokes. “You’ve got a couple more in you.”
“A couple?” is all you manage to say, your hand squeezing his wrist so he knows to squeeze your throat a little more.
“Mhm,” his voice rumbles in your ear, sending goosebumps all over your body. “Is it too much?” His question is laced with just the right amount of pity that makes you shake your head against him. “I thought so,” he replies, switching the vibrator to a higher setting.
It sends you into your third orgasm instantly, squirming violently against him as he pushes into you deeper. He knows how much you love that, and loves how much you squeeze around him as he slides inside, fighting against your muscles that threaten to force him out. You’ve done it before, a mesmerized look on his face and yours when you both realized what happened. Since then, you told him you liked it more when he fought to stay inside.
He takes the vibrator away as you calm down, his hips also pausing, keeping himself deep inside you. The pressure is soothing, and you take a moment to take a deep breath. His palm falls away from your throat, instead propping underneath your cheek.
It takes a few seconds before you feel yourself spasming around him. He chuckles against your back, pressing a kiss to your neck. “Still?”
You nod dumbly, rocking your hips again. “Yeah. I don’t know, I just-- Need more.”
“I’ve got you,” he soothes, pulling out again to roll you onto your stomach instead, one of your favorite positions.
You’re floating as you settle into the pillows, letting Aaron manhandle you wherever you need to be. You groan in your happy, blissed out state as he slides home again, draping himself over your back.
He is gentler now, knowing that’s exactly what you need at this point. The last orgasm he pulls from you is just as gentle, and he pushes deeper into you, letting you ride it out.
He pulls your hips up and thrusts once, twice before he’s spilling into you. You didn’t realize he was that close again. The warmth is soothing this time as it spreads through you.
Aaron leaves you only to settle behind you, spooning you once again. Your hand reaches behind you to find him, and he catches your wrist.
“You need to rest,” he chides softly.
“I know,” you whimper. “Need you inside me.”
“Okay, okay,” he murmurs, pressing a kiss to your neck as he slides in again, still half-hard, but it’s enough. You settle down as soon as the weight of him is tucked inside you again. “Better?”
“Mhm,” you sleepily nod, pushing back into him so he holds you tighter. “Do you have to go back to work?”
He chuckles against you, sighing. “No, I’m done for the day, I think,” he says. “I’ll tell them you weren’t feeling well.”
That makes you laugh. “We need a better excuse.”
“Or I need to go back to working in the office.”
You roll your eyes. “Like that’ll make a difference.”
He shakes his head, his mind remembering the same memories that you are. The many lunch hours when you went to eat with him, and ended up with your back pressed into the couch, his tie stuffed in your mouth to keep you quiet.
“Go to sleep,” he says, pulling you impossibly closer. “I’ll make us lunch when we wake up.”
“Perfect,” you smile, nuzzling into him. “Love you.”
“Love you too, honey,” he says, pressing little kisses to your neck and cheeks, wherever he can reach. “Now sleep.”
You’re already halfway there. The combination of him nestled inside of you and the post-orgasm exhaustion is enough to lull you into a restful sleep.
#aaron hotchner#aaron hotchner x fem!reader#aaron hotchner x reader#aaron hotchner x you#aaron hotchner smut#aaron hotchner fanfiction#hotch x fem!reader#hotch x reader#hotch x you#hotch x fem!reader smut#aaron hotchner x fem!reader smut#criminal minds smut#aaron hotchner one shot#criminal minds#aaron hotchner songfic#my usual
4K notes
·
View notes
Text
baby phat. onyankopon.
𑄽𑄺 warnings 𑄽𑄺 4.K word count. blackfem!reader, pregnant!fem reader/kink, drabble, onyankopon, grumpy!onyankopon, sweet!onyakopon, dominant!onyankapon, masturbation, phone/facetime sex, vaginal penetration, lil bit of sweet talkin’, creaming, praising, LOTS of dirty talk, kinda aggressive dirty talk, just a fine ass black man, minors aren’t welcome!


━━ 𝒄𝙤𝒐𝙘𝒉𝙞𝒆𝙛𝒂𝙞𝒓𝙮 𝙩𝒉𝙤𝒖𝙜𝒉𝙩𝒔 .ᐟ my brain is foggy from real life so just wanted to give y’all a lil something to leave you hot and bothered. if i gotta suffer, you do too. love you.

THE SCENT OF CASHMERE VANILLA, COCOA BUTTER AND BROWN SUGAR WAS WHAT YOU USUALLY WOKE UP TO. Unfortunately, that scent was missing within the bed. You sat up tiredly as you took a deep breath, raising your fingers over the smooth swell of your belly—you were now eight months pregnant, and your husband wasn’t home as much as you wanted him to be.
With a sigh, you pull yourself out of bed to prepare for the day. Onyankopon had been in contract with the New Orleans Saints for only a couple of months now. Becoming pregnant was an accident—but spending the rest of your life with him wasn’t the worst thing in the world. You’d practically traveled to every part of the state to be there with him for games—a baby wasn’t too far along after.
The only unfortunate part of this situation was his absence. With him just being signed, he was around the state with press conferences, practices, essentially in the hazing part of his successes. You were happy for him as you knew this was all he wanted, but you missed him, and so did the baby growing inside your belly.
Thankfully, you did have the support of his mom, who was there for you as if you were her own daughter. She was there to help you with your daily routine—feeding Ony’s two large Dobermans since she was terrified of dogs, going with you to your ultrasound for the day, and dragging you into every store she saw with infant clothes. You enjoyed your time with her—but you still missed Onyankopon.
It’s not like the two of you didn’t communicate. You had your ways. Texting when he wasn’t busy, phone and video calls into the night, pictures of daily activities, or all of those options in more…intimate times. It opened up a new exploration of your relationship as you were more shy to the nastier suggestions, but as more time was spent away from him, you’d do anything to show how much you missed him.
Speaking of, it was your favorite time of the day. Your daily phone call with him was closer to the evening time, the sun beginning to set within the state of Louisiana. He was only a couple of hours away as they were in Mississippi, days away from preparing to play their kick off game against Ole Miss—but it felt like he was across the country at this point.
You adjust the bow that ties against the halter of your yellow sun dress, silver cross sat between the swell of your breasts and constantly hardened nipples due to your hormones. You were going for a more natural route with your hair, flip-over sew-in under midnight black curls, dragging all the way down your back, framing your flushed and freckles cheeks.
You back yourself up a bit as you’re seated within the master bedroom, blood red IMAC brightening against your caramel skin, camera reflecting back at you as the call rang. When it connected, you were met with the familiarity of his hotel room—seeing as the room was slightly dim, the TV’s light against his brown skin, full lips even more delectable through the grainy camera. His durag protects his hair, goatee connected perfectly, jawline prominent under his stoic gaze. He was edible.
You wave, “Hi, baby! Can you see me?”
“I can,” he mused.
His deep timbre voice was comforting as he greeted, “Hey, my pretty ass baby. Look at you,” His eyes flickered over your face, breasts, and your swollen belly, making your thighs press together, “How you’ feeling?”
You sigh, pulling your hair behind your ear, “I’m okay. You’ like my dress?”
Your voice was soft, already feeling the tiniest bit insecure as you’d just gotten back into form fitting clothes. You’d cried as your body changed in the earlier months.
Onyankopon smirks, shifting on the chair where his knees spread, “Pretty as fuck, Mama. Bout’ to bust that shit open with all that ass,” he grunts, which makes you giggle as he continues, “I miss you.”
“I miss you more, baby,” you exhale, trying not to make yourself upset, “You need to come home soon. Your big ass wolves that you call dogs are scaring your mom.”
“Oh? Now they’ my dogs. You ain’t say all that when you wanted them,” he retorts, licking over his lips.
Your eyes follow the movement of his tongue as you shift on the chair. He looked handsome as ever. You can’t help but stare at his full lips, the small dimple in his cheek, and the dark hue of his eyes as he leans towards the computer desk, pulling out rolling paper as he prepares to roll a blunt. You weren’t sure why, but it was always the sexiest thing to watch.
You blink as your eyes scan the screen, clearing your throat a bit as you raise an eyebrow, “They’ ain’t drug testing y’all?”
Onyankopon shrugs, “It’s preseason, Baby,” he murmurs as he begins to break down the tree on the rolling paper, “Besides, all I’m doing is smoking. That ain’t so bad.”
“Mhm,” you roll your eyes, “Well you better cut that ain’t so bad habit before our little Pumpkin comes,” you run your fingers over your belly.
Your eyes run across his mouth as he licks over his joint, sealing the end, “Don’t call him that shit. That’s my son,” he grabs for his lighter, “My lil’ man been kickin’?”
“Your lil’ football player has been punting in my damn stomach,” you blow out a breath, “He’s moving down to my bladder. If he shifts anymore, imma’ need a walker.”
Your fingers grip around the cross hanging between your breasts, “…You’re my Pumpkin too, y’know.”
A chuckle leaves Onyankopon as he brings his freshly lit joint to his lips, inhaling as he holds off the urge to laugh. A cloud of gray leaves his lips as he blows.
“He gon’ have my long ass legs.”
His eyes flicker up momentarily from the screen, making it fog, “You my pumpkin, too,” he repeats back, exhaling into the camera.
You didn’t want to interrupt as you watched him—the haze of his red eyes already becoming apparent. He’s sexy. Fuck.
Your fingers absentmindedly trail along your belly, feeling your cheeks become warm as you bring your eyes down. You ask softly, “How was practice?”
"We got a new tight end, nigga think he somebody. But besides that, same ol'. Just drills and shit really,” He banters, shifting forward in his chair as he stares up at you, "You know I'm bored as hell right now, Mama."
You could see the haze in his eyes grow as he slowly takes another hit of his joint—Uh oh.
You narrow your eyes, curls swaying over your shoulder, “Oh, am I boring you?”
"You?”
Onyankopon leans back against the chair, exhaling into the computer. He grins a bit as the camera is engulfed in smoke, "Nah. You could never, baby.”
You watch him with curious eyes as he shifts in the chair, groaning slightly which makes your mind wander—The only thing you could see was his face, shoulders, chest and what you could assume to be his stomach. He wears a white long sleeve, clinging to his muscular frame. You knew all the tattoos that hid under his top. But something was under the computer table…
You give him a soft, awkward smile. You know how he got when he was high. This was your husband, yet he made you nervous like a schoolgirl.
You then say, “Oh!” Standing as you search for your purse, ass directly within the camera as you question, “I got the ultrasound photos, baby! Wanna see?”
Your husband hums, low and deep as he says back to you, “Mhm,” You feel his lustful eyes on the screen, “Come show me.”
Your hands tremble as you search, almost excited for him to see the photos. Or maybe you were just nervous—again.
You drop the brown Telfar on the side of the desk, it only takes you three steps to be in front of your computer again, holding the black and white printout up to the screen.
You can hear a faint laugh as Onyankopon murmurs once again, “Bring it closer, girl.”
You fully sit down again, leaning forward as you point your acrylic nail against the sonogram, “See, that’s his little toesss, and that’s his little fingers!” you giggle, “You see?”
Onyankopon’s face breaks out into a smile as he groans slightly, “Goddamn. I lied, he got my fingers. Musta’ got your toes, Mama. Can’t see ‘em too good.”
You hum, “Guess he won’t be too good for basketball then,” you tease.
Onyankopon snorts at that as he says, “Basketball she says— You know what? Just ‘cause you said that, he’s not playin no sport. Imma’ get lil’ man his own studio.”
You giggle a bit at that, “My child ain’t finna’ be no damn rapper. You can kill that thought.”
“That’s ‘cause he’s gonna’ be a singer. Got your pretty ass voice, I know it.”
You roll your eyes, “You’ just flirting, boy. Cut it out.”
Onyankopon chuckles at that, but he doesn’t deny it. His eyes fall back to that serious gaze he had before, a soft tint of red within them.
“You’ got me thinking about you.”
His voice, it’s almost like it’s own way of peer pressure. Your hands run over your belly anxiously as you blink, “Me?”
"Yeah,” Your husband draws out, eyes flickering up and down the screen in anticipation, “Don't play all shy.”
You can see him shift in the chair as he leans back, and his eyes stare back at the screen. You can tell he was waiting for something.
At the same time, your body becomes…significantly warm. Before he was signed, you and Onyankopon had sex almost every single day. You couldn’t get enough of each other, never did. Your mind flashes to those memories, and your thighs rub together a bit. At the same time, the door to the master bedroom opens, allowing you to exhale for a second.
Gray curls come into view, brown skin and familiar eyes that belonged to your mother-in-law. She held a bowl of food with a smile.
She walked towards the camera, “Hey, Honey-Bun, you alright in here? I made you some jambalaya—“
She pauses, looking towards her son on the camera as her eyes immediately narrow, “I know your big headed ass better put that joint away.”
Onyankopon groans as his mother comes into view, “Yes ma’am,” he coughs, hovering a fist over his mouth. He was still high—which you could tell based on his flushed appearance and tone. His mother was very anti-weed, so he always tried to hide it as much as possible. You can see some movement under the table, which you assumed was Onyankopon putting the blunt away.
“Why’ the hell do you think it’s a good time to be smoking, Onyankopon? They don’t drug test y’all?”
Oh god. You knew your mother-in-law could easily begin complaining, and you wish she’d walked in at any other time as you placed a calming palm against her arm.
Onyankopon clears his throat, making his face close to the screen so you could really see his eyes, “Ma—Ma. I’m in the preseason. Ain’t got no games for a couple days. They ain’t doin’ that, they ain’t doin’ all that.”
“Preseason? The ‘hell does that mean? Are y’all playing or not? If you’re not playing then why can't you come back home to check on your mother and your pregnant wife?” She comes closer to the camera, you can’t help but sigh lightly to yourself.
Onyankopon groans again as he leans back in the chair, “Momma, I’m not finna’ get into it with you again. You and Baby know. You jus’ gon’ talk over me if I start speakin’ anyway.”
He can’t help but tongue his cheek momentarily, and your heartbeat increases with just his simple movements—but you’re brought back to reality when his mother speaks up even quicker.
“Are you at least eating? Did you get the care package I sent you? I got all your soaps, and that little teddy bear you had as a baby—you never went anywhere without Mr. Snuffles,” which makes you giggle at the familiar toy, something Onyankopon hated being reminded of.
He mumbles, “…I’m good, Momma, got your care packages. Lawd. Stop with all that…”
“Thank you for the food, Momma,” you give her a smile, “I’m not super hungry at the moment, do you mind leaving it in the fridge?”
Onyankopon’s mom gives a smile back, “Of course. I’m actually gonna head back home for the night, do you need anything else?”
You shake your head, “I’m perfect. Just gonna’ keep talking to Ony for a little while longer.”
Onyankopon sighs as his mother says her goodbyes, exiting out of the room. Now, you notice his eyes flickering up and down your curves, which makes you squirm under the spotlight. Onyankopon then repeats, “I miss you bad as fuck, girl. You miss me?”
You hate yourself for the emotions that produce randomly at times. The conversation between your mother-in-law and Onyankopon, the way he made you easily giggle, the imagery of his warmth surrounding you but not actually being there—it didn’t feel the best.
The dark fluff of your cat-eye lash extensions flutter as you nod your head, using your knuckles to lightly swipe your watery eyes as you nod, “I miss you so much, Ony…”
Your husband’s face softens slightly. He hated to see you so emotional due to his absence, and would rather be anywhere else. But you always supported his dreams, and wanted to build the perfect life for your baby boy. He mutters, “Stop all that crying, baby. Wipe ya’ face. You know I’ll be back.“
You shakily sigh a bit, nodding your head as you kneel your face down to let the tears fall that way, “I—I know, it’s just hard sleeping without you,” you sniffle, “Lil’ Pumpkin likes when you rub my stomach to sleep…”
Onyankopon sighs, “And I love rubbin’ your stomach, baby.”
He then says, “Soon as I get back, we gon’ sleep for a whole week. Ain’t nobody gonna’ bother us. I’m all yours.”
Your heartbeat increases—Onyankopon always had a way to make you emotional without even being near. It also made you somewhat…aroused.
“I miss you like crazy. I miss ya’ voice, I miss ya’ smell. I miss ya’ pu—“ he cuts himself off before he goes into that territory, which makes your body heat up slightly.
You watch as he brings the blunt back up to the camera, pulling another drag of smoke, the move always so efficient as if it was nothing. His eyes are back to being low—it makes you shift your legs again. He cuts on low background music to play, and a familiar song catches your ears, She Will, by Lil Wayne.
You hum softly, “You love this song.”
You take a moment to recall why the song gave you such a sense of Deja Vu. But as you remember, you halt.
The memory was at a family event— Onyankopon’s going away party. His family irritated him by being loud, over talking and messy—a black family’s usual antics. He’d managed to sneak downstairs with you to the car for a moment of silence, the two of you smoking, the song faintly playing in the back. You’d…remembered this vividly.
Your mind glazes over the moans you produced in that backseat, the sound of your skin connecting, your vulnerability, your legs trapped over his shoulders…
Your mind comes back to reality as you’ve been watching him this whole time. Your hand had somehow made its way to your chest…rubbing over your exposed skin, clutching your pendant again.
“Mama,” Onyankopon murmurs as he brings another drag of the blunt back on camera, blowing the smoke into screen as he spins back to his sentence earlier, “‘Got me thinking about you bad as fuck.”
He was high as hell.
Your eyes run over his large silhouette as he leans back against the chair, knees spreading out further as he makes himself comfortable, head tilting back a bit as he watches you.
Your mind wanders again, back to that song—back to that night. Your mind can’t stop. Your head is spinning with the memories, it physically makes you whimper, squeezing your thighs, tugging your pendant fully.
Your husband’s gaze grows in lust as he leans forward a bit, whispering, “Talk to me. Whatchu’ thinkin’ about?”
The hand clutched around your pendant squeezes a bit tighter as you glance towards the camera, “The song…makes me think of that night in the car…” you softly admit, rubbing your fingers over your collar bone, your fingertips bringing you warmth.
He brings the blunt back on camera again before a stream of clouds leaves his lips, “You miss that night, Mama?”
You nod your head, your entire body now hot. You could feel your nipples poking through your top again, aching in a way that almost becomes painful. Your thighs are so tightly together, as you adjust the seating position, you grind against yourself a bit, making the tiniest gasp pull from your lips.
Onyankopon groans through the screen, and you can hear his voice say, “You in our bedroom?”
He was becoming impatient.
"Go to it. On the bed," he murmurs, "Hurry up.”
“Too far from you, Ony,” you pout, bringing your hands against your breast, giving a squeeze to them, trying to relive how full they feel.
There's a pause before a deep exhale leaves his lips. His tone goes deep again, "Go."
You shudder as you stand, your legs feeling numb. You tilt the monitor more towards the king sized bed, silky black comforter set along the oversized mattress. You crawl along the sheets, turning towards him again, your knees along the bed as your dress begins to hike against your soft thighs.
His eyes flicker downward at you, and you can feel his gaze run up your smooth, caramel skin. His gaze burns into yours, giving an intense look.
You hear his voice again, “You gon’ do what I say?”
You nod your head, lightly digging your teeth against the pink of your soft lips.
“Always listen to you, Ony…”
Your man growls, “That’s right, ‘cause you good. You gon’ be good for me?”
Your hands squeeze the flesh of your breast, your nipples never being this sensitive before your pregnancy. You gasp in a soft tone, but the sound is heavier. You nod your head, “Bought something I w—wanna show you…”
You hear his breathing pick up, “Yeah? Show me,” he murmurs. “You look so muhfuckin’ good right now, baby.”
You reach behind you as you pull a toy from under the pillow—it’s pink, silicone, almost looking like glass. Big, just as big as him.
“Pretty like you, Daddy…”
"Look at that," You hear a deep noise escape his lips before there's a shuffling noise, you couldn't exactly make out what it was—then it was followed by another noise. This one you recognized; the strings of his sweatpants. His dark pink tip slaps along the sculpted muscle of his stomach, practically making your mouth water.
“You like it?” You ask softly.
You take the object and graze it lightly along your body, seating yourself fully along the bed. You’re at the most perfect angle to spread your legs.
“Yeah, baby,” he grunts, letting more of his body come into view as he’s in a reclined position. You can begin to see his toned chest come into view when there's some shuffling noises again, his breathing picking up, “Love it.”
You pull at the string of your dress, letting the halter fall over the swell of your belly, material hanging in between your stomach and hips. You were now bare at the top, hair swaying over your body and face as you shuddered a bit, “They’re starting to fill with milk, baby… sensitive…”
You can hear a deep, deep groan echo in the screen, almost sounding frustrated, “Fuck. You’ playing right now. Put that shit in your mouth.”
You bring the toy up to your mouth, spreading your full lips apart as you let it slide on your tongue, coating it with your saliva. At the same time, you spread your legs, showing off the glistening arousal bedaubed on your pussy. You were wet.
“Fuck, baby....” he growls lowly, beginning to stroke himself, “Pussy so pretty. I can feel that shit on my tongue. I’m just slurping your shit up.”
His voice is rough with desire, each word punctuated by a squeeze of his fist around his thick tip.
“Get you’ a pillow for your lower back, baby. ‘Know it hurts sometimes.”
You listen, pulling the satin pillow behind you for a bit of support, feeling the small ache in your back beginning to decrease.
“Comfortable, Mama?” He questions, you nod your head.
“Good. Rub that dick all over your clit.”
Your eyes flutter shut as you imagine his lips dropping kisses against your clit. He’d go from your inner thighs, teasing you. He’d watch as you’d squirm with every suckle of your skin, your entire body shuddering as his hot breath fanned over the hood covering the pink nub, being pulled up by his lips, being kissed by his tongue. You brush the toy against your clit that throbs, spreading your legs a little more as you whimper, lightly dragging the tip in circles on your upper pussy. The sound it makes, your pussy keens.
His hand begins to pick up speed as he pumps through his fist, “You like that, huh? Rubbing this big ass dick all over your clit?” He grunts, his voice strained with pleasure, “Slap that shit on your pussy. Get them’ pretty ass eyes rolling back."
He knew everything about your body. Including the way you’d spasm at this action, so you listened, slapping the heavy toy against your clit, your legs trembling in response, eyes rolling to the back or your head. You groan a bit, head falling back, eyes fluttering before you bring your attention back to your arousal that pools beneath your thighs, pulling your legs wider to show the gummy pink of your pussy.
The anticipation builds as you tease yourself, circling your clit with the toy, then dipping it inside your opening just enough before withdrawing again.
“Why that shit so fuckin’ wet already?” His jaw clenches, head tilting back, fist rotating on his tip, dragging down every couple of seconds.
Your folds wrap around the toy every millisecond as you slide the outsides of it against yourself, teasing so much that your eyes haven’t stopped rolling back.
The swell of your belly shifts a bit as you whine softly, “Ony…”
“Shut the fuck up,” he snaps, “Ain’t even put that shit in yet. Where’ my lil’ nasty bitch at? She would’ve been droolin’, dropping herself all on my dick. Just drenching my shit. Quit playing.”
“Right here,” you whimper, nodding your head, digging your teeth back into the plump of your lips. Instead of dipping the toy in to tease yourself, you take a palm to pull one of your legs up in the air, using your other hand to drag the toy towards your opening, separating the aching stretch of your folds as you begin sinking it’s tip inside.
You’re gasping as you watch it go in, unable to see more, yet you feel every inch swelling your walls, disappearing under the sight of your large belly.
You whimper, “It’s in there, baby.”
"Get it all the way in, baby. Bury that shit deep," he commands, pumping faster now, his breathing ragged. You’re dropping it in, inch by inch, your inhale deep as you pull it halfway out, toes curling as you sink it back in, an air pocket gushing as your arousal sops around the pink toy.
Your eyes are fluttering chaotically as you shudder, “Fuck, agh—“ you don’t stop, fist brushing over your clit as you’re dropping it down into you.
He’s talking, "You remember when we first met? Couldn’t even handle my fingers. Now look at you,” A low chuckle escapes him, "Now I got you stretching that pussy out. Dick just drop, drop, dropping in that shit…”
His words trail off into a grunt as he quickens his strokes, “You my lil’ freaky ass bitch, huh?”
You whimper, pouting at the way your pussy cries its tears, sobbing out in waves of arousal that pool each time you pull the toy out, painting the pink silicone white. You squeal lightly as its balls slap against the outside of your pussy, the fleshy sound splattering up more of your wetness as you petulantly whine, “Yeah, Ony…”
"That's right, baby. Take that shit like a good lil' slut," he says, voice dripping with lust as he watches you work the toy deep inside yourself, “Rubbing that pretty ass clit while you're stuffed. Fuck, you look so damn good."
He picks up pace, stroking harder and faster as he nears his own climax, “Gonna give you all this fuckin’ nut. You want it?”
“Want it,” you tremble, in and out, the toy’s just going in you at this point, disappearing without a trace, lost in your pussy. You’re just gushing. The sound is like a mouth blowing raspberries into one’s palm, fleshy, nasty.
“Can’t cum without you,” you pout, “Need you….I need you,” you’re opening your mouth, the sob coming deep from your chest, fucking yourself even harder, one leg shaking violently as it’s held in the air, eyes possessed as they’re rotating. You loved these moments—but they were never enough. Not even for him.
“You don’t need nothing,” He groans, his words coming out more raspy, “Keep that pussy wet as fuck. I’m coming.”
#onyankopon x black y/n#onyankopon x black reader smut#onyankopon x reader#onyankopon x you#aot onyankopon#onyakapon#attack on titan smut#aot#onyankapon#anime oneshot#onyankopon smut
2K notes
·
View notes
Text
trapped
pairing: robin (dick grayson) x catwoman apprentice! reader
tags: mdni, fem reader, reader is a year older than dick, enemies to lovers¿?, dick calls reader “cat”, reader calls dick “birdie”/“baby”, very hormonal teens, dry humping, enclosed space, forced proximity, making out, groping, sub dick, thigh riding, praise, handjob, p in v, cowgirl, unprotected sex, creampie, reader is more “experienced” (lmk if i missed any)




You had never known stability. Not in the traditional sense.
Your earliest memories were of cold nights and empty pockets, of learning that in Gotham, you had to take what you wanted because no one was going to give it to you. And maybe that was why Selina Kyle took you in—because she saw something of herself in you.
From the moment Selina took you under her wing, normalcy became a foreign concept. She never pretended to be a mother, never showered you in words of affection, but she provided. She gave you food, a place to sleep, and most importantly—a purpose.
Life with her was exhilarating. Nights spent darting across Gotham’s rooftops, breaking into places you had no business being in, taking what you wanted simply because you could. Selina taught you everything—how to move unseen, how to pick locks with delicate precision, how to manipulate, how to charm.
And, of course, how to run.
But no matter how good you were, they were better.
Batman and Robin.
They were always there, always a step behind, always chasing.
Selina handled Batman, slipping through his grasp time and time again, leaving only whispered promises and stolen kisses in her wake.
And you? You were left to deal with Robin.
The first time you saw him, you nearly laughed.
A kid. Shorter than you, all bright colors and attitude, wearing a mask that barely hid the smugness in his expression.
Not like you were a kid yourself, right?
“You’re kidding,” You had said, eyeing the small figure in bright red, green, and yellow. “You’re Robin?”
From the way Selina warned you about Robin, you expected… something else.
Not this short, flamboyant boy in pixie boots and wearing that shit-eating grin.
Robin bristled at your tone, crossing his arms. “Yeah, and?”
“You just seem… smaller than I expected.”
He scoffed. “You’re, like, barely taller than me.”
You hummed, amused. “Still taller.”
It should’ve been easy. You’d spent months training under Selina, learning how to evade, how to slip through fingers like water. He was just a kid—a kid in bright colors, a cape to slow him down, and all energy and attitude.
But Robin was fast.
And relentless.
No matter how quick you were, how well you knew Gotham’s rooftops, he kept up. Every twist, every jump, he was right there, like a shadow that refused to be shaken.
He grinned through it all, like the chase itself was the fun part.
By the time you finally lost him—ducking into a hidden alley, heart pounding, breath sharp—you realized something.
You weren’t annoyed.
You were excited.
For the first time in your life, you were looking forward to something.
And it became a game.
Every time Selina clashed with Batman, you and Robin danced around each other, locked in your own little battle. He was all quips and acrobatics, relentless determination wrapped in bright colors, and you matched him move for move.
And then, somewhere along the way, over the years, the game changed.
It was subtle at first.
The way his hands lingered just a second too long when he grabbed you. The way his breath hitched when you leaned in, voice low and teasing.
And then, one night, after a particularly close chase—
“You’re slowing down, Birdie,” you teased, perched on the edge of a rooftop, looking down at him. “Getting tired of chasing me?”
Robin huffed, rolling his shoulders, the movement fluid yet tense, like he was shaking off exhaustion—or frustration. He was older now, no longer the scrawny kid you used to outrun on Gotham’s rooftops. He’d grown into himself, his frame broader, his stance more grounded, more sure. The suit, once bright and almost ridiculous in its vibrancy, seemed different now. The red looked richer, darker under the moonlight, the shadows clinging to the fabric, emphasizing the sharp angles of his body. His cape, now black and lined with gold, draped over his shoulders with an ease that made him seem more intimidating, more like a real threat than just Batman’s sidekick.
And then there was his voice—lower, rougher, with an edge that hadn’t been there before.
An edge that reminded you of Gotham’s Dark Knight.
Gone was the high-energy bravado of a kid playing hero. Now, when he spoke, there was weight behind his words, something firm, something undeniably commanding. It sent a strange thrill through you, though you’d never admit it.
“Who says I’m not letting you get away on purpose?”
You raised an eyebrow. “Awfully generous of you.”
“Maybe I like the chase,” he said, stepping closer, his gaze sharp. “Maybe I like you.”
The air shifted.
Your smirk didn’t waver, but your heart did.
For the first time, you didn’t have a quip ready.
And then, just as quickly as it came, the moment passed.
He grinned again, all mischief and ease, like he hadn’t just thrown a wrench into your entire world.
You rolled your eyes, shoving down whatever had just coiled in your chest. “You really should work on your flirting, Robin.”
“Is that a challenge?”
You leapt off the rooftop, and this time—
You let him catch you.

You were nineteen now.
It wasn’t that you weren’t grateful to Selina—she’d taken you in when you had nothing, taught you everything you knew. But you weren’t a stray kitten anymore. You had your own ambitions, your own scores to settle, and it was time you made a name for yourself.
Tonight was supposed to be the first step.
A simple break-in. A massive corporation with deep pockets and even deeper corruption. You weren’t just stealing from them—you were stealing leverage. Blackmail, blueprints, the kind of information that could buy you power.
Everything had been going smoothly—until he showed up.
“Still breaking into places you don’t belong?”
You didn’t need to turn around. You knew that voice—low, smug, and just the right amount of irritating.
Robin.
Or, as you liked to think of him now, Gotham’s Most Persistent Pain in the Ass.
You smirked, still focused on the files flickering across the computer screen. “You know me, Birdie. I just love a good challenge.”
“You’re getting sloppy,” he countered, stepping closer.
You caught his reflection in the screen—older now, taller. The bright colors of his suit had been traded for something darker, more tactical. His stance was solid, muscles tense, ready to spring.
You sighed dramatically. “You gonna fight me, or just lecture me to death?”
“I was thinking both.”
And then he moved.
You barely had time to react before he was on you, reaching for the drive in your hand. You twisted away, knocking over a chair in your retreat, and bolted.
The chase was on.
You darted through the office space, leaping over desks, twisting through narrow hallways, all while Robin stayed infuriatingly close. You could feel him at your heels, relentless as ever, and for the first time in a long time, you wondered if you might not shake him this time.
Then you saw it—a maintenance door left slightly ajar.
You shoved through, sprinting inside just as Robin reached for you. His fingers just barely caught the back of your jacket, and in his effort to stop you, he yanked.
Hard.
The force sent you both crashing through the doorway, tumbling down a short flight of metal stairs in a mess of limbs and curses.
You landed first, sprawled on your back against the cold floor. Robin landed on top of you, knocking the breath from your lungs as the door behind you slammed shut with an ominous clunk.
A silence settled.
“…Did you just tackle me down a flight of stairs?”
Dick groaned, pushing himself up slightly, bracing himself on his arms—his body still pressed against yours. His breath was warm against your cheek when he muttered, “You fell.”
“You pulled me.”
“You ran.”
You rolled your eyes, shifting slightly beneath him—only to realise just how close you were.
The space around you was tiny.
Metal shelves lined the walls, stacked with old equipment and cleaning supplies. The air was thick with dust and stale air, and the dim, flickering light overhead barely illuminated anything.
You and Dick were practically pressed against each other.
And worse?
The door wasn’t budging.
It’s like it automatically locked you both in the moment you entered.
Dick must’ve come to the same conclusion because he exhaled sharply, muttering a quiet, “Fantastic.”
You turned to face him, looking him up and down. “Aww. Trapped in a tiny, enclosed space with me? Try not to look so excited, Birdie.”
Dick clenched his jaw, shifting his weight, and—
Oh.
That was… interesting.
For the first time since you met him, he was the one who faltered. His breath hitched, his fingers twitching slightly where they rested against your waist.
“What’s wrong?” you asked, voice dropping to a whisper. “Never been this close to a girl before?”
His gaze flickered to your lips before he caught himself, schooling his expression into something unimpressed. “I hate you.”
“Uh-huh,” you hummed, tilting your head. “That’s why you’re still on top of me?”
Dick tensed. Then, with a sharp inhale, he pushed off you, moving to sit up—only to immediately hit his head against one of the low shelves with a dull thud.
You laughed.
Dick glared, rubbing the spot where he’d smacked his skull. “Glad you’re enjoying yourself.”
“Oh, of course.”
You pushed yourself up, stretching out your legs as much as the tiny space allowed. Dick was sitting against the opposite wall now, knees bent, arms resting over them. The space was too small for either of you to fully move without touching the other.
A slow smirk curled at your lips as an idea took root.
You shifted, closing the distance, swinging a leg over his to straddle his lap.
His whole body stiffened.
“W—What are you doing?” he asked, voice suddenly very unsteady.
“Getting comfortable,” you murmured, leaning in just slightly. “You don’t mind, do you?”
His breath shuddered.
This was new.
You’d spent years teasing him, pushing his buttons, testing his patience. But this—the way he was looking at you now, wide-eyed, breathless, trapped beneath you with nowhere to go—this was different.
You could feel the way his heart was racing.
You dragged your fingers down his chest, slow and deliberate. “Still think I’m getting sloppy?”
Dick exhaled shakily. “I—”
He stares unabashedly at the way your plush thighs brush against his sides when you shift to make yourself comfortable, he feels the way heavier breasts push against his chest as you leaned closer.
Dick wasn’t an idiot.
He knew you were doing this on purpose.
You can feel Dick’s eyes, despite it being hidden behind that damn domino mask of his. It was all over your face, and for a moment—you saw the way his breath hitch when his eyes landed on your lips.
That only fueled you more.
And without a second thought, you kissed him.
The second your lips met his, the tension snapped.
Dick made a quiet, desperate noise against your lips, his hands grasping at your waist, unsure whether to pull you closer or push you away. You made the decision for him.
His hesitation lasted seconds before he gave in, melting beneath you, responding with an eagerness that sent a thrill down your spine.
You nipped at his lower lip, earning a shuddered gasp, and God, you’d never seen him like this—needy, breathless, completely at your mercy.
“Is this what you wanted?” you murmured against his lips, your hips shifting just enough to make him choke on a breath.
His fingers dug into your sides as he struggles to maintain control.
He swallows hard, Adam's apple bobbing in his throat. “Fuck—Cat… no—” Despite the words, his body betrays his desire, hips twitching up to meet yours, his hands sliding up your back.
Dick kisses you again, soft and deep, pouring his desperation and desire into the embrace. And you didn’t waste a second to kiss him back, your hips slowly moving against his thigh, seeking out any sort of relief while also trying to provide Dick some.
And Dick—
He whimpered, soft and pathetic, adorable coming from him.
Your hand moved to cup his face, your thumb stroking along the soft skin of his cheek, leaning down to deepen the kiss.
"You're so pretty." You murmur softly, pulling away slightly to stare at him, your hand making its way to remove his mask. But Dick’s hand immediately caught your wrist, stopping you.
“N-no, wait, mask stays on, Cat. We can’t—“ He didn’t finish the sentence as you rolled your hips against him instead, body jerking in his hold. Somehow the gravity of the situation just stills in his head for a moment. “Shit, shit, wait—we should talk about this, right?”
“What’s there to talk about?” You mutter out, as you press kisses along his jawline. “You want this—I want this. We both want this, don’t you agree?”
You could feel his breath, ragged and shallow.
There was no escaping the sheer intensity of it. Every inch of his body was pushing into yours, and his movements—though tentative—were driven by an undeniable need. His hips, for all his effort to hold back, shifted instinctively, and for a brief second, you felt the unmistakable press of his body against yours. And in one swift motion, you removed his domino mask, tossing it aside as your eyes met his baby blue ones.
He looked at you with wide eyes, clearly torn between wanting to pull away and wanting more. You could practically hear his heart racing in the thick silence.
He swallowed hard. “I—” His voice cracked, and for the first time, you saw it. The boyish cockiness was gone, replaced by something more raw, more real. He was trembling slightly, unsure but wanting, and it made something stir in your chest.
You slid your hands up his chest, fingers brushing over the outline of his suit, feeling the heat of his skin beneath the fabric. His reaction was immediate—he let out a quiet, shaky breath as his hands slid down your back, pulling you even closer.
He kissed you again, this time with more force, his lips hungry, as if he couldn’t get enough. His hands roamed, brushing against your sides, your waist, his fingers lightly pressing against the curves of your body. You could feel him struggling to stay in control, his movements growing more erratic, more desperate, but still so careful, as if he was afraid of pushing you too far.
“Damn it,” he muttered between kisses, his voice tight with frustration. “I hate that you’re making me lose control.”
You smiled against his lips, pulling back just slightly. “You don’t have to hate it, you know.”
His eyes met yours again, and there it was—vulnerable, unsure, but undeniably drawn to you. “I—” He paused, exhaling slowly, as if gathering his thoughts. “I want this. But I don’t know what I’m doing.”
“You don’t have to know everything,” you said softly, running your hand down his chest once more. “Just go with it.”
Dick’s body reacted immediately, the way his hands moved to your back, pulling you closer as if he couldn’t get enough. You could feel the desperation in him, the way his movements grew more fervent, more insistent, as if the moment had finally overtaken him.
There was something so intoxicating about it—the way he kissed you with such intensity, like every second he spent with you in this confined space only heightened the tension between you. You could feel his body pressing against yours, his every movement a silent invitation, a challenge. His hands, once hesitant, were now roaming freely, touching you with a fervor that made your heart race.
Dick reaches up with one hand to cup your breast, thumbing your nipple through the fabric of your suit, and you let out a guttural moan.
“That’s it, baby, don’t hold back.” You mumbled, your hand grabbing a fistful of his hair, tilting his head up to meet his lips once more.
And don’t hold back he did. His hand fondled with your clothed breast, while the other made its way to the zip on your back.
Dick's gaze lazily makes its way up your form, greedily taking in every inch. He gently bites down on his lower lip, face starting to look flushed as he lets his guard down. Bending forward, you close the distance between your mouths, nipping gently and taking that plush lower lip for yourself. He gasps, but gives as good as he gets, tonguing into you with a little groan. When he tries to take control and deepen the kiss, you smirk and pull back, drawing a pouty little sigh from him.
"Ah ah, birdie—let me do all the work, yeah?" You scold him. His forehead came to rest on your shoulder, his warm breath mixing with yours.
“I’m sorry, I just—” You placed a finger on his lips, clicking your tongue.
“Don’t apologise.” You murmur, lifting his head up as you start to press kisses all over his jawline once again, trailing down to his neck. Dick whines softly at the sudden shift, mewling your name.
He grinds against your clothed cunt, the fabric of your suits making it easier to hurriedly slide against each other.
Dick wishes he could feel how tightly you’d wrap around him instead of this but he needed release now, and this was the quickest way to get it.
But you notice his neediness.
You noticed how much he was aching to be inside of you.
He was bucking into you desperately, moving his hands to grope your tits and roll your nipples between his fingers.
“There you go… Good boy, keep going.” You whisper, your hand trailing down to the hem of his pants, tugging at it.
Dick inhales sharply as he feels your fingers brushing against the waistband of his pants, his hips twitching in anticipation. He's breathing heavily now, chest rising and falling rapidly against yours.
“Ah fuck…” His voice is strained, torn between wanting to give in completely and the lingering hesitation. “I want to... but we should... shit.. but we should be careful.”
You tilt your head at that, your hand resting against his growing arousal, rubbing against it painstakingly slow. “And where’s the fun in that?”
Fuck.
Despite his words, his hips lift slightly, seeking more of your touch. “Please, just... let me...” He swallows hard, hands gripping your waist as he looks up at you with hazy, desire-filled eyes. “...let me make you feel good.” His fingers slip beneath the fabric of your bottom, brushing against the bare skin of your stomach, leaving tingles in their wake.
“Tell me what you want. I'll do anything... anything you want.” His voice is a needy whisper, one you knew you couldn’t resist now.
Your eyes darken with lust as you take in the sight of Dick beneath you, seeing the desperation etched into every line of his body. You can feel the heat radiating off him, the way his heart is pounding against your chest, the tremble of his fingers as they dig into the fabric of your suit.
Slowly, teasingly, you slide your hand lower, palming the growing bulge in his pants. You can feel him, hot and hard, straining against the confines of his costume.
Dick lets out a strangled groan, his hips bucking up into your touch, seeking more friction.
Boldly, you hook your fingers into the waistband of his pants and slowly, torturously, begin to tug them down. The fabric resistive at first, but with a final, sharp tug, you yank them down, exposing his bare skin to the cool air of the room.
Dick's cock springs free, long and cute and perfect, the tip already glistening with precum. It twitches as the air hits it, and you can't help but lick your lips at the sight. You wrap your hand around his shaft, feeling the weight of him, the heat, the way he pulses in your grip.
Dick is panting now, his eyes glazed over with lust as he stares up at you, taking in the sight of you looming over him, his cock in your hand. He looks wrecked, destroyed, completely at your mercy, and it sends a thrill through you, a rush of power and desire.
You stroke him slowly, teasingly, watching as he writhes beneath you, his body arching into your touch. You can feel him leaking more, his cock throbbing in your hand, and you know he won't last much longer at this rate.
So you lean down, your breasts brushing against his chest as you murmur in his ear, your breath hot against his skin. “That's it, baby... just like that. You feel so good... I can't wait to taste you.”
You take your time, stroking him with long, deliberate movements from base to tip. Your hand is soft and warm, encircling his thick shaft completely as you work him over. You can feel every ridge, every vein, the way he throbs and twitches in your grip.
Dick's breath comes in ragged gasps, his chest heaving as he struggles to maintain control. His eyes flutter shut, brows furrowed in concentration, a sheen of sweat breaking out on his forehead. Soft, breathless moans spill from his lips with every upward stroke, the sounds growing louder, more desperate as you continue your ministrations.
As you pick up the pace, pumping him faster, his reactions become more intense. His hips start to lift, meeting your strokes, fucking up into your fist with a desperate hunger. Quiet, strangled moans spill from his lips, each one making your own desire peak in response.
“Fuck... Dickie, you like that, huh? Like how you’re fucking my fist, don’t you? Such a good boy..”
You watch, as Dick’s face contorts with pleasure. His brows furrow, teeth sinking into his lower lip hard enough to leave indentations. The tendons in his neck strain as his head tips back, throat bared to you in a silent offering. His eyes, when they meet yours, are hazy and dark, the blue of his irises nearly swallowed by the black of his pupils.
The wet sounds of your hand moving over his cock fill the small space, obscenely loud in the charged silence. You can feel him leaking more, his precum making your strokes slicker, easier. His cock is red and angry, the head an almost painful shade of pink, the slit weeping with his desire.
You lean down, your breasts brushing against his heaving chest as you bring your mouth to his ear. Your lips brush the shell of it as you whisper, your voice low and heavy with lust. “That's it, baby... doesn't it feel good? Doesn't it feel amazing to have my hand wrapped around this big and needy cock of yours? I can feel how much you want it... how much you want me...”
Dick shudders, his body wracking with sensation as he listens to your words. A broken whimper escapes him, his voice hoarse and wrecked as he manages to gasp out, “F-Fuck… please, (Name)… I need you so bad…”
You never knew how much you needed him begging for you until now. And god did it feel good.
You can feel his desperation, his absolute need for release. And you're going to make him work for it. Slowly, torturously, you increase the speed of your strokes, squeezing just a bit tighter, twisting your wrist on the upstroke.
Dick is panting now, his breath coming in short, sharp bursts. His face is flushed, eyes squeezed shut, jaw clenched tight as he tries to hold back. But you can see the way his body is tensing, the way his cock is throbbing harder, leaking more steadily against your palm.
“(Name)... I can't... I'm gonna... fuck, I'm gonna...” His words dissolve into a guttural moan, his entire body going rigid.
You feel his cock throb and twitch in your grip, and then with a hoarse cry of your name, he's coming undone. Thick, hot ropes of cum erupt from his cock, painting your hand and his stomach with his release. His body shudders and jerks through each wave of pleasure, his hand gripping yours like a vice.
You work him through it, stroking him through each aftershock, feeling his cock pulse and twitch against your fingers until finally, he collapses back against the wall, chest heaving, skin sheened with sweat. He looks utterly debauched, hair disheveled, lips kiss-swollen and parted around shallow breaths. His eyes flutter open, hazy and unfocused, struggling to regain some semblance of coherence.
Slowly, you bring your hand up to your mouth, making a show of licking his spend from your fingers, my tongue swirling around each digit, ensuring he can see every last bit of him disappearing between your lips. Dick watches closely, his chest still rising and falling rapidly, a fresh wave of desire washing over his eyes as he takes in the sight of you licking his cum off your hand.
“Mmm, you taste good, Dick,” You purr, wrapping your hand around his re-hardening shaft, giving him a slow, teasing stroke. “I could get used to this view—you, all wrecked and wanting, cock throbbing and ready to go again already.” You lean in closer, your lips brushing against his ear as you whisper, “You really are an overachiever, aren't you?”
You can feel him shiver against you, his hips lifting slightly into your touch. You grin, pulling back to look at him with a wicked gleam in your eyes. Then, slowly, you reach back and unzip the rest of your suit, peeling the tight material down your body until you’re just left in your panties.
You hook your thumbs into the waistband and tug them down, baring your dripping cunt to his hungry gaze.
Dick's eyes widen as he takes in the sight of you, his tongue licking his lips as he stares at your glistening folds. You grab his hand, guiding it between your legs, pressing his fingers against your aching clit. He inhales sharply at the contact, feeling the slick heat of your arousal coating his digits.
“Fuck, (Name).…you're so wet.” He breathes, his fingers starting to move on their own, stroking along your slit, feeling how ready you are for him. “Is this...is this because of me?”
You moan softly, rolling your hips against his hand, seeking more of that delicious friction. “Yes, birdie...it's all for you,” You gasp, your head falling back as his fingers find a particularly sensitive spot. “I'm so fucking turned on right now, and it's all because of you.”
You reach down and grab his wrist, guiding his hand to move faster, to press harder against your clit. You grind against him, coating his fingers in your slick arousal, your body trembling with need. You can feel how hard he is, his cock throbbing and leaking against your ass, and you know he wants you just as badly.
Without warning, you shift your hips, positioning yourself so that the head of his cock brushes against your entrance. You feel him gasp, his fingers pausing in their movements as he realizes what you’re about to do. You look down at him, your expression one of pure, unadulterated lust, and then you sink down.
You take him in inch by delicious inch, your walls stretching around his thick length, wrapping him in your tight, wet heat. You both moan at the sensation, your bodies fitting together like two puzzle pieces, made to be joined like this. You don't stop until you’re fully seated on his lap, his cock buried to the hilt inside your clit, pressing against his pelvis.
“Oh fuck, Dick...” You whimper, your nails digging into his shoulders as you start to move, rolling your hips in a slow, sensual grind. “You feel so fucking good inside me.”
Your words seem to spur him on, and he starts to thrust up to meet you, his hips lifting off the ground to drive his cock deeper into your needy cunt. The room fills with the obscene sound of skin slapping against skin, your moans and cries of pleasure echoing off the metal walls. You can feel him getting closer, his thrusts becoming more erratic, more desperate, and you know he won't last much longer.
“Come on, baby,” You pant, your voice high and breathless as you ride him harder, faster, chasing your own release. “Come inside me. I want to feel you come inside me, Dick. Please...please come for me.”
With a final, harsh thrust, you grind down against Dick. His eyes widen as he feels your walls clench around him, your words pushing him over the edge.
He pistons his hips up harder, his heavy balls slapping against your ass with each punishing thrust. He leans in, burying his face between your breasts, his mask brushing against your skin as he suckles and nips at the soft mounds, leaving marks of possession in his wake.
“Fuck, (Name)...you feel too good,” he pants against your skin, his voice a low, guttural rasp. “So good...”
His words dissolve into a strangled moan as his thrusts become erratic, losing their rhythm as he teeters on the brink of climax. He's so close, his cock pulsing and throbbing inside your clenching walls, your arousal dripping down his shaft with each thrust.
“Ngh— fuck..” he hisses out, his fingers digging into the flesh of your hips hard enough to bruise as he holds you down, making sure you take every last drop of his seed. You can feel the hot, thick ropes of his release painting your insides, dripping down onto his lap and the floor below, filling you up just as you'd begged him to do.
You're both panting hard, chests heaving as you come down from your highs. You slump against his chest, completely spent, your body still twitching with the aftershocks. Dick's arms wrap around you, holding you close, his face buried in your hair as he tries to catch his breath.
You can't help but smile, cupping his face in your hands and pulling him in for a slow, deep kiss. You pour all of your satisfaction, all of your desire, all of your growing feelings for him into that kiss. When you finally pull away, you're both smiling, both looking at each other like you can't quite believe this is real.
But then, Dick's eyes widen in realization as the final pulses of his release subside, his softening cock still buried deep inside your fluttering heat. A look of panic flashes across his face beneath the mask as the gravity of what just happened sinks in.
“I...fuck, I'm so sorry,” he starts, voice shaking with remorse. “I didn't mean to... shit, I shouldn't have...”
But you silence him with a searing kiss, your lips crashing against his in a desperate attempt to stem the flow of apologies. You pour every ounce of passion and hunger into the kiss, your tongue delving into his mouth, tangling with his own. For a moment, Dick is stunned, his body stilling beneath you as he allows you to plunder his mouth.
When you finally pull back, your chests heaving, you fix him with a stern look. “Didn't I tell you not to apologise?” you demand, voice low and firm. “I know exactly what I wanted, and I wanted this. I wanted to feel you come inside me, Dick.”
Dick swallows hard, Adam's apple bobbing in his throat. “But I didn't use a condom,” he argues weakly. “I could have...we could have...”
You place a finger against his lips, silencing him once more. “Shh. I know the risks. But where’s the fun in not taking them?”
Dick's eyes search yours, a war raging behind those hidden depths. Slowly, hesitantly, he nods, your finger falling away from his lips. “Alright,” he murmurs, voice low and rough. “Fine, you win, Cat.”
A slow, shy smile curves your lips as you lean in to press a soft kiss to his jaw, your body still nestled against his, his release cooling inside you. “Good,” you whisper against his skin. “Because I think we're going to be stuck in here for a while,” you say with a grin, glancing around at the small, enclosed space. “You’re going to have to deal with me a little longer, Robin.”
Dick laughs, a real, genuine sound that makes your heart flutter in your chest, his hands sliding up your back to tangle in your hair. “You're insatiable,” he accuses, but there's no bite to his words, only a grudging sort of awe.
“But I think I can handle that,” he says, pulling you down for another kiss. “Especially if it means more of this.”
You nipped at his earlobe before soothing it with your tongue.
“You're just now figuring that out?”
—
Safe to say, Batman found you both a few hours later, and him and Selina lectured you both about the need for protection. (At least you were on the pill.)
All Rights Reserved © Works are exclusive to this Tumblr
#dick grayson x reader#dick grayson x reader smut#nightwing x reader#nightwing x reader smut#nightwing smut#dick grayson smut#sub dick grayson#dc comics#dc comics smut#rizzcom
758 notes
·
View notes
Note
Thinkin’ about Price, who’s on med leave and under strict orders not to engage in any strenuous activity, begging his controversially young wife to take pity on an old man and fuck him.
Your daughter is born nine months later. You like to joke she exists bc your husband was actually home long enough to put a baby in you.
NOW YOU GOT ME THINKIN ANON—

MEDICAL LEAVE
𝜗𝜚 the one where john's finally home long enough to get you pregnant
𝜗𝜚 pairing: john price x younger wife!reader (reader is afab) 𝜗𝜚 cw: smut (minors—DNI), age gap (price is in his late 30s, reader is late 20s), mentions of surgery/recovery, john having a pain kink (need i say more?), unprotected sex (wrap it before you tap it/get tapped), unedited as usual, bad ending

"john, the doctor had strict orders for you to—"
you're cut off mid-rant by john slotting his lips over yours, the mitts of his hands covering your cheeks and tugging your face closer to his. his tongue juts out to lick needily at the seam of your lips, the faint taste of the painkillers he had just taken still fresh on his tastebuds only to be replaced by the sweet mint of your toothpaste.
john would've kept kissing you, too, if he hadn't tried to twist his hips over to face you, making him pull away sharply and hiss out at the way the fresh sutures etched in his ribs twinged in pain.
"john—"
"m'fine," john grunts out hoarsely as he lays back down flat on his back, eyebrows pinched low in the middle of his forehead and tongue licking at the remnants of your spit on his lips. "just wanna—christ—wanna be inside ya."
and that’s how you got to your current position, sitting directly behind john’s thick and leaking cock as you lean back to rest your hands on his hairy muscled thighs—anywhere that wasn’t sutured closed or bruised from the surgery he’d undergone. from beneath furrowed brows, your soft eyes focused on the molten heat buoying in his pupils.
“i don’t wanna accidentally hurt you, john,” the end of your sentence comes out pinched in a whine as the calloused pad of his thumb begins circling your sopping clit, your hips jumping at the stimulation and instinctively rolling forward against his sensitive cock.
john uses the thumb petting at your clit to distract you from the way he manhandles you up, notching the head of his cock between your folds and holding you there for a moment. “i don’t fuckin’ care if it hurts, ‘lright? don’t wan’ you stoppin’ until i feel you cummin’ ‘round my cock four times, and i fill up this pretty fuckin’ pussy—understand me?”
and even though john’s cemented into your shared bed on his back, he keeps you all nice and obedient under his thumb, using the hand he keeps groping at your hip as a way to guide the way your movements. every so often, his sutures would twinge in just a way to send a jolt of pain up his spine—but then he would feel your gummy walls gripping his cock just a little tighter, and the pain would warp into delicious pleasure.
you, ever the good little wife you were, did exactly as john told you—only pulling off of him when your fluids were a messy mixture between my thighs and you could barely walk to the bathroom on wobbly legs.
it didn’t even cross your mind when a month and a half later, you’re a mess of hormones and continuous morning sickness that threatens to knock you out from work for a couple days. john tells you it’s fine, that he’ll work some more late nights to cover your income for a couple days, but you’re determined to keep working.
only after nearly fainting at your home one morning (after john fucked you through at least 2 orgasms) did you find yourself on the doctor’s examination table, fingers nearly snapping john’s hand bones in half when he read off the positive pregnancy result.
and when your daughter is born nine months later (december 14th, by the way—a sagittarius baby), you’re curled up in the hospital bed with john holding you closely, the baby sandwiched comfortably between you two and grappling at one of his thick fingers.
“y’know how long i’ve been waiting for this?” you giggle out softly as you nose against john’s beared jaw, eyes fluttering closed and system overflowing with painkillers and endorphins. “guess you were finally home long enough to actually put a baby in me this time.”
©️ ink-n-shadow 2024
do not copy, plagiarize, steal, borrow, or repost any of my work without my expressed permission
#honestly i want john to get me pregnant like asap#or i can get him pregnant#either way#call of duty#cod mw2#john price x reader#john price cod#john price#captain john price#john price x you#captain price#task force 141#iNs Captain John Price 🎗#call of duty modern warfare#price cod#cod mwii#cod#john price smut#tf 141#john price x reader smut#john price x you smut
2K notes
·
View notes
Text
"Three things I wish I knew before I transitioned to male.
One: that injecting myself with cross sex hormones actually was damaging my perfectly healthy body.
Two: that changing my identity and changing my body wasn't actually going to heal the pain that I had within myself. It was just an escape that created actually more trauma for me.
Three: that it was okay to be a tomboy and not fit into society's beauty standards of what a woman was supposed to be like. That I was perfect the way I was, and I didn't need to change myself."
#detrans#detransition#gender ideology#queer theory#medical transition#sex trait modification#wrong sex hormones#cross sex hormones#medical scandal#gender identity#tomboy#save the tomboys#genderwang#religion is a mental illness
507 notes
·
View notes
Note
stiles comes to you after his female anatomy class and asks you to help. he says he’s never even watched torn so has never even seen a vagina, but yours is the first one he winds up seeing and eating out
༄ word count — 2.3k
፨ characters — stiles stilinski
☓ tw — none
⊹ cw — smut & oral, losing of virginity
☼ a/n— i have... severely neglected this blog
✎ masterlist
─
you were sitting on your couch watching tv, a root beer flavored sucker between your lips. you were channel surfing, nothing catching your eye. your front door opened unannounced, making your head whip towards it.
after it closed, the familiar face of stiles poked around the corner.
you sighed, glad it wasn't an intruder.
"hey," you greeted. "ever heard of knocking?"
"sorry, it's raining and the door was unlocked. i figured you wouldn't mind."
he kicked his shoes off and walked over to sit next to you, mimicking your position by crossing his arms.
"what flavor is that?" he asked, looking at the stick in your mouth.
"root beer."
"nice."
"so what's up?"
"i was hoping you could help me study."
"as long as it's not math."
"honestly, i kinda wish it was."
"why? what is it?"
"so... it's for my health class. we're doing a human anatomy course for the sex ed unit."
"and you need my help... why?"
"well... it's female anatomy." you raised your eyebrows. "you're the only person i'm comfortable with asking for help on this."
you just looked at him for a second before taking in a deep breath and turning off the tv.
"alright, fine."
within a couple of minutes you were both upstairs on your bed. you sat against your headboard, him laying on his side horizontal across the bed with his assignment in front of him.
so far, it was just multiple choice and fill in the blank questions. he was reading them out, getting your answers.
"what do the ovaries do?" he asked, a diagram of the uterus, ovaries, and fallopian tubes above the questions, with lines to label each.
"make hormones and contain eggs."
he skimmed the answers, finding the one that fit that description the best.
once he finished that chart, he flipped the page to see a very detailed diagram of a vagina, also with lines pointing to specific parts of it for him to label.
he looked at it for a moment, as if he was really studying it.
"vulva."
"i'm pretty sure that's just an all-inclusive word to include everything."
he circled the right answer
"what is the... clitoris? did i say that right?"
hearing stiles say the word 'clitoris' was a bit weird, but to be fair most people don't really say the full word.
"are you really asking me what the clit is?"
"yeah, what is it?"
you looked at him slightly in disbelief, chuckling a bit.
"come on, stiles."
"what?"
you were dumbfounded. everyone knows what the clit is.
"you've never even heard the word?"
"i've heard of it, i just don't know what it is."
"it's kind of obvious if you're looking at a vagina."
he shrugged. "never seen one. well, other than this drawing."
now this left you stunned. never seen a vagina? how was it possible for a teenage boy to never have seen one?
"you've watched porn, though."
he shook his head. "nope."
somehow he continued to shock you more with every sentence.
"never?"
"never."
"stiles, you're a teenage boy, and you're telling me you've never watched porn?"
"never needed to."
"the clitoris is... it's like a little bud above the vaginal opening. it's full of nerve endings and it's really only there for pleasure purposes."
"huh. interesting. can i ask you a question?"
"shoot."
"does every vagina look like this?"
"what do you mean?"
"like... are they all identical?"
"uh... no. every vagina is different. just like every penis is different. some of them are dangly, some are hairy, it just depends on the person."
"does yours look like this?"
your eyebrows dipped.
"did you really just ask me that?"
"i thought i was allowed to ask questions."
"yeah, general questions."
"that is a general question."
you sighed. "similar. but not really. i mean, they all have the same basic parts. but the anatomy is different sometimes."
he nodded. "wish i could see a real one up close."
it was kind of funny, how he was talking about vaginas like a specimen he could study.
"you will someday." he made eye contact with you and raised his eyebrows slightly. "stiles. you're not implying what i think you are, are you?"
"i mean... i'm not gonna say no."
"i'm not showing you my vagina!"
"that's not what i was asking, pervert," he said in an unconvincing tone.
to be completely honest, you weren't completely against the idea. the best way to learn was to see the real thing, not just a drawing.
you sighed. "fine." his eyes lit up a bit. "on one condition."
"mm?"
"no touching. only looking."
he nodded.
"sounds fair to me."
you could not believe you were fully exposing yourself to him right now, your vagina just out. your upper body was propped up on your pillows, your knees bent and thighs spread with his eyes glued to you.
"and no judging my lack of shaving."
he shrugged. "doesn't bother me."
he was looking at you like it was a book and he was reading every word.
"this is kinda weird, right?" you asked, trying to break the tension. and trying to distract him from the fact that his gaze was causing you to grow wetter and wetter with every second.
"a little bit, yeah."
"so... my vagina is the first one you've ever seen."
"yep. looks pretty similar to the drawing."
a few seconds of heavy silence went by.
"i mean... it's hard to learn when you're not... hands-on." you mentally slapped yourself for how cringey that sounded.
he froze, looking up into your eyes.
"what?"
"yeah, i mean... how are you supposed to learn what the clitoris is if you don't get to see what it does?"
"oh. i don't- i don't know."
"exactly."
"but you said no touching."
"i know what i said. maybe sometimes it's good to... break rules."
he slowly crawled closer to you and you spread your thighs wider. the cold air against your wetness could've given you chills.
"what... what do i do?" he asked, his face only a couple of inches away.
"see if you can find the words on your paper."
he looked over at it. "labia."
he lightly poked your wet lips — not the ones on your face.
"good."
"was that it?"
"mhm. good job."
"clitoris," he said without looking back at the paper.
"you remembered that one."
he looked around for a second before, without warning, placing the pad of his pointer finger onto your clit, making you take in a deep breath.
"that?"
"yep. right again."
"what do you... do with it?"
it was uncomfortable to explain, especially with a face in your vagina and a finger on your clit.
"uh... lots of things. really it's just different ways of touching it and touching it with different things. so, you could go in circles, back and forth, up and down. you can also use your tongue or some kind of toy. it's another thing that just depends on the person, everyone likes different things."
"what do you like?"
"circles, usually."
with a second of hesitation, he began slowly moving that finger in circles. you let out a breathy moan and closed your eyes, but he stopped.
"was that okay?"
you opened your eyes and looked down at him.
"that was good."
"so... what happens? is there like... an end goal here?"
"orgasm. it's how most women have to get there. sex, like penetration, usually isn't enough to get a lot of us there."
"really?"
"yeah. that's why it's important for our partners to do something other than just regular sex."
"so... do you usually prefer fingers or... a tongue?"
"well... me personally, i usually prefer a tongue. i feel like it's just more intimate."
"and what do you do with the tongue?"
"same thing you would with fingers. circles, back and forth, up and down-"
you were interrupted by a warm tongue on your clit, unable to hold in a gasp. he was going in circles like you said to do, and it was like he knew what to do immediately.
it felt good. you looked down at him to see him returning the gaze, a smirk creeping across his face.
"good, just like that, stiles."
you were doing your darndest to keep your hips still, ensuring he did everything right his first time. he placed his hands atop your thighs, making sure they stayed spread.
you reached up and pushed your hair out of your face, fisting a ball of your own hair. you were moaning, which he wasn't expecting to hear the first time he did this.
"you're doing good, stiles. that feels good."
he didn't answer, but his ego grew a few sizes at that. the closer you got to your orgasm, the more he had to hold you still. his arms were now wrapped around your thighs, his hands flat against your belly.
"fuck, okay, i can feel it coming," you said, looking down at him. "keep going, i'm gonna cum."
when you did look at him, it looked like he was experienced in this. his positioning, his hands, his pace, everything screamed 'i've done this a thousand times before'.
he liked this. being able to make you melt with just his tongue was making him hard, but he couldn't help it. your sweet voice moaning his name was like music to his ears, and the closer you got the louder you became.
your fingers tangled in his hair, trying not to pull too hard.
"don't stop, stiles. i'm almost there. i'll tell you when to stop."
he obeyed, not changing a single thing he was doing. if it hadn't have been so obvious, he might not have known you were cumming.
your back arched sharply, you took in a loud gasp, and your legs were trembling.
this was an incredible orgasm. you were perplexed by his skill, as ten minutes ago he had never even laid eyes on a vagina, much less eaten one out. but he was a quick learner, as you'd figured out from all the werewolf stuff.
"alright, stop, stop," you choked out. he immediately pulled away, using his shirt to wipe his mouth. you closed your legs and reveled in your high. your hand covered your eyes and you struggled to catch your breath.
"was that okay?" he asked innocently.
"are you kidding?" a moment later, you propped yourself up on your elbows. "how did you know how to do that?"
he shrugged. "i just did what you described."
"i've had more than one guy go down on me who was experienced and couldn't make me cum at all. that was, what, two minutes?"
"i guess i'm a natural," he joked.
you tilted your head to the side. "c'mere." you spread your legs again and his eyes widened, slowly following your directions. he held himself above you and you pulled him down to kiss you.
your hand trailed down his chest and landed on his belt, the clanking of the buckle making him pull away.
"what're you doing?" he whispered, looking at your half-closed eyes.
"well... i can see you're rock hard. i just figured, if you're losing your oral virginity, you might as well lose the regular one too."
he gulped hard, not moving.
"oh."
you stopped messing with his belt, furrowing your brow.
"unless you don't want to. you don't have to. don't feel like i'm pressuring you."
he shook his head.
"i don't. it's just... i didn't expect this. i wasn't planning on doing that when i came over, and i definitely didn't expect this. i didn't bring a condom or anything."
"i have some." you reached down and cupped his bulge in your hand, which made him falter a bit. "they might be a bit snug, but they'll fit."
he nodded, and you continued unbuckling his belt. when you got his pants shimmied down a bit and he was exposed to you, you noticed how red his cheeks were.
"what's wrong?"
"nothing. just... i don't want to disappoint you."
"stiles, it's your first time. i'm not expecting you to last past the first thrust." you can tell he took that as an insult. "i didn't mean it like that. no guy lasts past the first thrust during their first time. vaginas are different than hands or socks. i want you to feel comfortable with this. i promise i'm not judging you."
he nodded. "okay."
"if you don't want to have sex yet i could always just blow you instead. you might last longer that way."
"no, i want to do this."
"okay."
you reached over and grabbed a condom out of your nightstand drawer and opened it for him.
"want me to put it on for you?" you asked, to which you received a nod.
the feeling of your hand stroking down on him could've made him cum right then and there. but he wanted to wait until he was at least inside of you.
the feeling of his tip pressing into you was magical for both of you, and once he was fully nestled into you, he pressed a deep kiss onto your mouth.
he didn't move for a moment, wanting this to last as long as possible.
he was a nice size, not small by any means but not the biggest you'd had. he was perfect.
"you okay?" you whispered, pushing his hair off his forehead.
he nodded, the redness in his cheeks spreading to his chest. he slowly pulled out, and let out a loud, shaky moan with the next thrust. him laying his forehead against your chest let you know that he had cum, his arms trembling a bit.
when he looked at you again, he chuckled.
"what?" you asked.
"lasted past the first thrust." you both laughed at that, and you kissed him again. "next time it'll be better."
"next time?" he nodded. "when will that be?"
he thought for a second. "give me a couple of hours."
#fanfic#smut#stiles stilinski#stiles stilinski imagine#stiles stilinski imagines#stiles stilinski smut#stiles stilinski one shot#stiles stilinski x reader#stiles stilinski x y/n#dylan o'brien#dylan obrien#dylan o'brien imagine#dylan obrien imagine#dylan o'brien imagines#dylan obrien imagines#dylan o'brien smut#dylan obrien smut#tw#teen wolf#teen wolf imagines#mtv
970 notes
·
View notes
Text
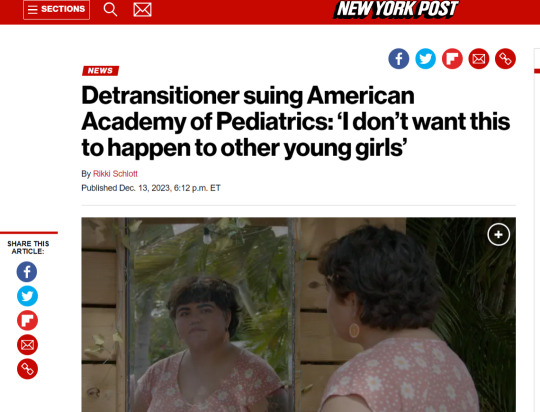
A Florida woman who medically transitioned from female to male as a 14-year-old is suing the American Academy of Pediatrics — alleging she was whisked through the process as a minor by “a collection of actors who prioritized politics and ideology over children’s safety, health, and well-being.” Isabelle Ayala, now 20, is also suing her doctors in Rhode Island in a first of its kind case, filed in Providence/Bristol County Superior Court. “I just really don’t want this to happen to other vulnerable young girls,” Ayala, who lives in Wellington, Florida, told The Post. “I don’t want puberty to be the enemy. I don’t want our natural biology to be the enemy.” ... Ayala says she was sexually assaulted as a child and began precocious puberty at age 8 — both experiences she says made her resent her femininity and believe she was better off male. “I decided to transition because of just a series of unfortunate things that I had tied to being female. And those things made me hate being female,” Ayala said. At 11, she found solace in the transgender activist community on Tumblr, and thought, “This is going to fix me.” She learned from trans activists that fabricating suicidal ideation is a surefire way to get a testosterone prescription quickly. So, at age 14 she did just that: “I learned that from the internet that… I had to convince [my doctors and family] that if they don’t affirm me, I’m gonna kill myself.” Ayala said she was referred to a gender clinic and diagnosed with gender dysphoria by transgender health expert Dr. Jason Rafferty. According to the lawsuit, he determined she “would benefit from being put on cross-sex hormones” in a single visit that lasted less than an hour. ... Ayala alleges that her previous diagnoses of autism, ADHD and PTSD were largely overlooked by her healthcare providers. The lawsuit claims her doctors “falsely represented that cross-sex hormone therapy was the only treatment option available to Isabelle to effectively treat her gender dysphoria, as well as her anxiety, depression, PTSD and suicidality.” Less than a year into treatment, Ayala said, she actually did attempt suicide. “She was a guinea pig under one of the top experts in this field of so-called gender medicine,” Bolar said. “She was hitting rock bottom, and he continued to put her down this experimental path of medicine.” By age 17, in 2020, Ayala felt the urge to begin presenting femininely again. A YouTuber who had detransitioned inspired her to identify as a woman again — and she soon realized her transition had been a massive mistake. Three years on, according to the lawsuit, she still struggles with unwanted body hair, vaginal atrophy and an altered bone structure from the testosterone. “She has since contracted Hashimotos’s disease, an autoimmune disease that only the males in her family have a history of, from taking testosterone,” the suit claims.
The emphasis is mine.
#transgenderism#transgender ideology#gender ideology#ftm#puberty blockers#hormone replacement therapy#cross-sex hormones
31 notes
·
View notes