#Medical Schools and Hospitals
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
US Tumblr user growth rate is estimated to slow down to 4.1%.
Text
How to Secure Competitive Rotations: A Guide for International Medical Students in the USA
Are you an international medical student dreaming of gaining valuable clinical experience in the United States? Securing competitive clinical rotations is a crucial step in your medical journey. In this comprehensive guide, we'll walk you through the process of obtaining clinical rotations in the USA, ensuring you're well-prepared for this exciting opportunity. Let's dive in!

Table of Contents
Understanding Clinical Rotations
What Are Clinical Rotations?
Why Are Clinical Rotations Important?
Eligibility and Requirements
Meeting Educational Prerequisites
Visa and Legal Requirements
Finding the Right Institutions
Researching Medical Schools and Hospitals
Utilizing Online Resources
Preparing a Strong Application
Crafting a Compelling Resume
Writing an Effective Personal Statement
Navigating Interviews and Evaluations
Acing the Interview
Excelling in Clinical Evaluations
Financial Planning
Estimating Costs
Exploring Scholarships and Financial Aid
Cultural Adaptation and Communication
Adapting to the US Healthcare System
Enhancing Communication Skills
Living Arrangements and Logistics
Housing Options
Transportation and Daily Logistics
Getting the Most Out of Your Rotation
Building Strong Relationships
Maximizing Learning Opportunities
Succeeding in the USMLE
Preparing for the USMLE Step 2 CK
Tips for Success
Understanding Clinical Rotations
What Are Clinical Rotations?
Clinical rotations, often referred to as clinical clerkships or simply rotations, are a fundamental component of medical education. During rotations, medical students have the opportunity to work alongside experienced healthcare professionals, gaining hands-on experience in various medical specialties.
These rotations typically last for several weeks and cover a range of disciplines, including internal medicine, surgery, pediatrics, and more. They provide students with a real-world understanding of medical practice, helping bridge the gap between theoretical knowledge and practical application.
Why Are Clinical Rotations Important?
In Prasad Medical Center, Clinical rotations serve several crucial purposes for medical students:
Skill Development: Rotations allow students to develop essential clinical skills, such as taking patient histories, performing physical examinations, and interpreting diagnostic tests.
Exposure to Specialties: They provide exposure to different medical specialties, helping students explore potential career paths.
Networking: Rotations offer opportunities to connect with practicing physicians and potential mentors in the field.
Residency Preparation: Successful completion of rotations is often a prerequisite for applying to residency programs in the United States.
Now that we've covered the basics, let's explore how international medical students can secure competitive rotations in the USA.
Eligibility and Requirements
Meeting Educational Prerequisites
Before embarking on your journey to secure clinical rotations for international medical students in USA, it's essential to ensure you meet the educational prerequisites. Most institutions require that you:
Have completed the core clinical clerkships in your home country.
Possess a strong academic record.
Demonstrate proficiency in English by passing exams like TOEFL or IELTS.
Visa and Legal Requirements
Securing the appropriate visa is a critical step in the process. International students typically apply for a J-1 visa, which is specifically designed for exchange visitors in programs such as clinical rotations. Be sure to:
Consult your institution's international student office for guidance on the visa application process.
Familiarize yourself with the legal requirements and restrictions associated with your visa.
Book Your Appointment online
Finding the Right Institutions
Researching Medical Schools and Hospitals
To secure competitive rotations, research is your best friend. Start by identifying medical schools and hospitals known for hosting international medical students. Look for institutions that:
Have established international student programs.
Offer a variety of clinical specialties.
Provide support and guidance for international students.
Utilizing Online Resources
The internet is a treasure trove of information. Explore online forums, social media groups, and websites dedicated to medical students. These platforms often contain valuable insights and firsthand experiences from fellow international students who have completed rotations in the USA.
In the next section, we'll delve into the nitty-gritty of preparing a strong application.
Preparing a Strong Application
Crafting a Compelling Resume
Your resume is your first impression on potential rotation sites. Ensure it highlights your:
Educational background, including your medical school and any honors or awards.
Clinical experience and relevant medical skills.
Extracurricular activities and leadership roles.
Read more: Clinical Rotations for International Medical Graduates in the USA - Prasad Medicals
Writing an Effective Personal Statement
Your personal statement should reflect your passion for medicine and your desire to learn and contribute during your rotations. Share your:
Motivation for pursuing clinical rotations in the USA.
Unique qualities and experiences that set you apart.
Long-term career goals and how rotations fit into your journey.
Navigating Interviews and Evaluations
Acing the Interview
Interviews are your opportunity to showcase your personality and dedication. Practice common interview questions and emphasize:
Your enthusiasm for the field and the institution.
Your ability to work effectively in a team.
Your commitment to providing quality patient care.
Excelling in Clinical Evaluations
During your rotations, clinical evaluations play a pivotal role in your success. Always strive for excellence by:
Being punctual and professional.
Seeking feedback and actively working on improvement.
Building strong relationships with residents and attending physicians.
Financial Planning
Estimating Costs
Understanding the financial aspects of your rotations is crucial. Consider expenses such as:
Tuition fees, if applicable.
Visa and application fees.
Living expenses, including accommodation and daily costs.
Exploring Scholarships and Financial Aid
Don't forget to explore scholarship opportunities and financial aid programs for international medical students. Many organizations offer assistance to help alleviate the financial burden.
Now that we've covered the essentials, let's discuss cultural adaptation and communication.
Cultural Adaptation and Communication
Adapting to the US Healthcare System
Adapting to a new healthcare system can be challenging. Here are some tips for a smooth transition:
Familiarize yourself with US healthcare policies and practices.
Be respectful of cultural differences in patient care.
Seek guidance from mentors and fellow students who have undergone a similar transition.
Enhancing Communication Skills
Effective communication is essential in healthcare. Work on your:
English language proficiency.
Listening skills.
Ability to convey information clearly and empathetically to patients.
Living Arrangements and Logistics
Housing Options
Your living arrangements can significantly impact your experience. Consider options like:
On-campus housing provided by the institution.
Off-campus apartments or shared housing with fellow students.
Transportation and Daily Logistics
Ensure you have reliable transportation to and from your rotation sites. Plan your daily logistics, including commuting time, meals, and study schedules, to make the most of your rotations.
Getting the Most Out of Your Rotation
Building Strong Relationships
Networking is key to your success. Build relationships with:
Residents and attending physicians who can provide guidance and recommendation letters.
Peers and colleagues for support and camaraderie.
Maximizing Learning Opportunities
Take every opportunity to learn and grow during your rotations. Be proactive in:
Observing procedures and patient interactions.
Asking questions and seeking mentorship.
Keeping a journal to track your progress and experiences.
Succeeding in the USMLE
Preparing for the USMLE Step 2 CK
As an international medical student, passing the USMLE Step 2 CK is essential for your career prospects. Prepare by:
Enrolling in a comprehensive review course.
Practicing with sample questions and mock exams.
Staying organized and focused on your study goals.
In conclusion, securing competitive clinical rotations for IMG in the USA as an international medical student is an achievable goal with careful planning and dedication. Remember to stay persistent, make the most of your opportunities, and always strive for excellence in your medical journey.
Frequently Asked Questions
1. How do I find hospitals that accept international medical students for rotations?
You can start by researching medical schools and hospitals known for hosting international students. Online forums and social media groups are also excellent resources for recommendations.
2. What is the best way to prepare for the clinical rotations interview?
Practice common interview questions, emphasize your passion for medicine, and showcase your ability to work effectively in a team.
3. Are there financial aid options available for international medical students pursuing rotations in the USA?
Yes, many organizations offer scholarships and financial aid to help international students with the costs of rotations.
4. How can I excel in my clinical evaluations during rotations?
Be punctual and professional, seek feedback, and build strong relationships with residents and attending physicians.
5. What are the key tips for succeeding in the USMLE Step 2 CK?
Enroll in a review course, practice with sample questions, and stay organized and focused on your study goals.
By following these guidelines and staying committed to your goals, you can secure competitive clinical rotations in the USA and make the most of this invaluable experience in your medical career.
Good luck!
Contact us for knowing more about the clinical rotations
Address: 894 Eastern Parkway, Brooklyn, NY 11213
Phone: +1 718-774-6060
Fax: +1 718-774-4426
#clinicalrotations#clinical rotations for IMG in the USA#Medical Schools and Hospitals#prasadmedicalcenter
0 notes
Text
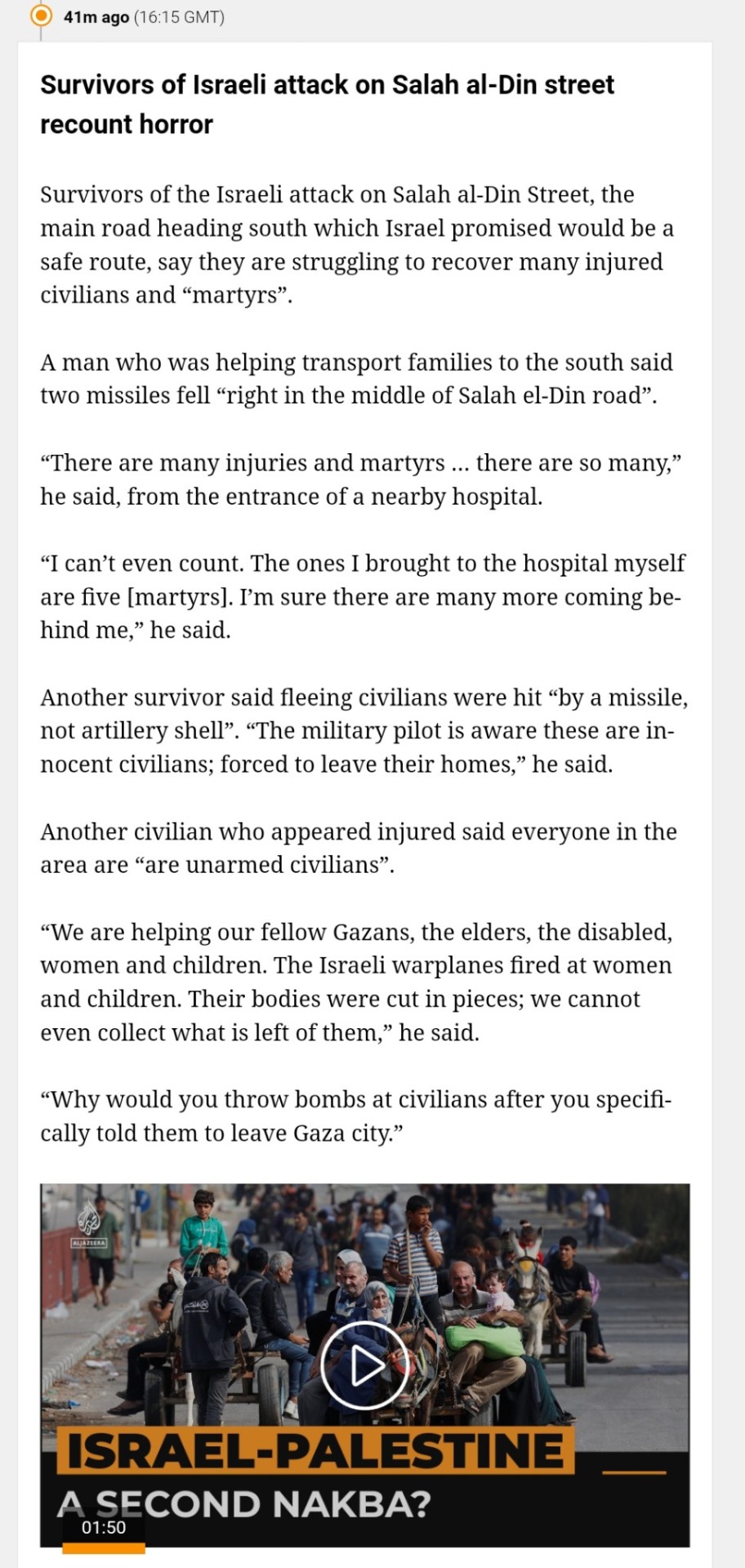


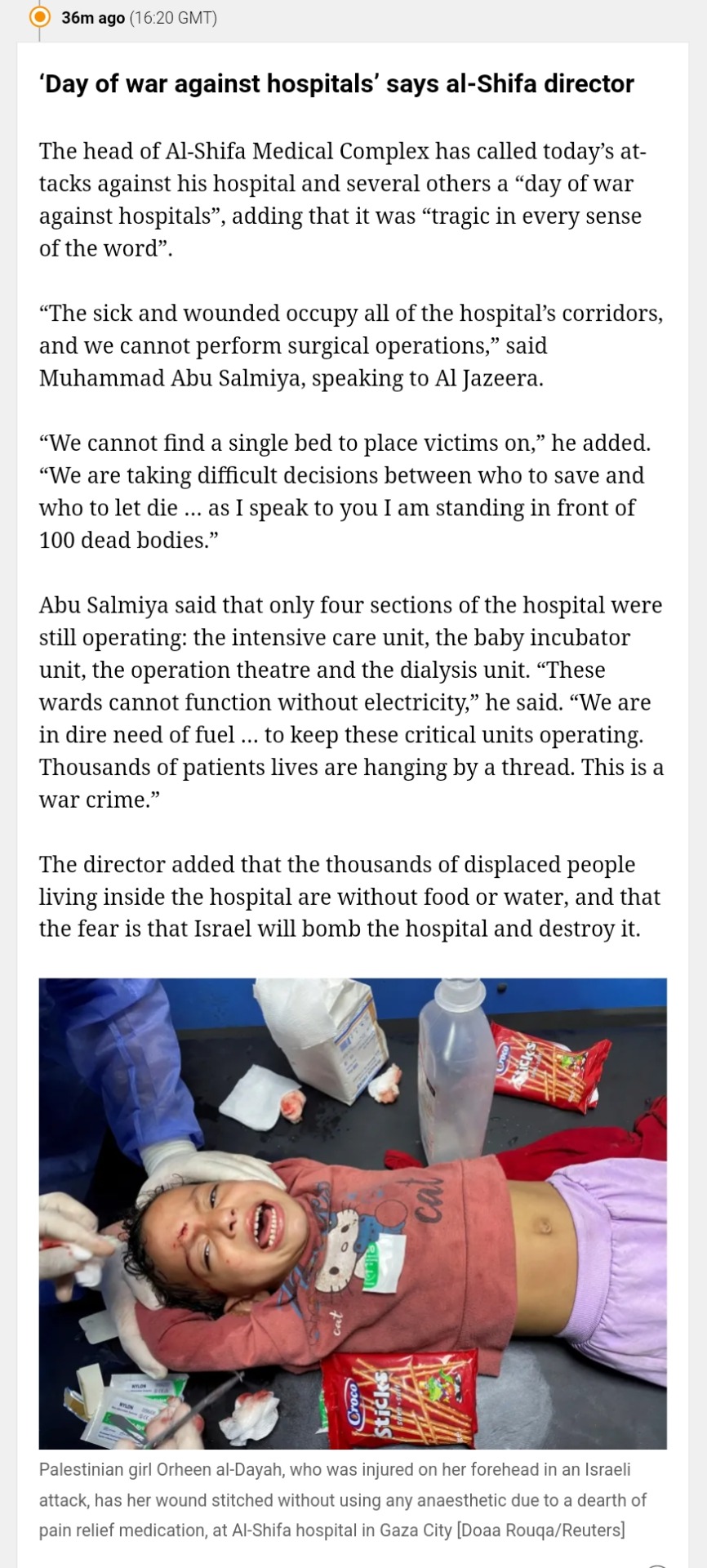
Here's an amalgamation of news from the last 2 hours
Schools, hospitals, the one road civilians are fleeing down, NOTHING IS FUCKING SAFE.
WERE YOU ANGRY ABOUT AL-AHLI? WELL HERE, THERE'S FUCKING MORE. BRING THAT RAGE BACK AND START MAKING NOISE.
#free gaza#free palestine#gaza strip#irish solidarity with palestine#palestine#gaza#news on gaza#al jazeera#boycott israel#israel#Netanyahu#antony blinken#USA#Medical Aid for Palestinians#Al-Quds Hospital#Melanie Ward#Mads Gilbert#al shifa hospital#Al-Buraq School#Mohammed Abu Salmiya#Chris Hedges#Analysis#Death toll#Salah Al-Din Street#Hamas#Amalgamation#News updates#Current events#Jerusalem#Colonialism
7K notes
·
View notes
Text

#black literature#black history#black tumblr#black excellence#black community#black history is american history#american history#civil rights#black girl magic#blackexcellence365#physician#doctor#medical student#medical school#medical doctor#justina ford#equal rights#hospital#medical field#black history month#black history facts
192 notes
·
View notes
Note
the blood donor Anakin au is so funny to me bc i can't donate blood but i would try constantly if there was a hot doctor there. if there was an obi wan lookalike there he would see me on a regular basis
i believe it was @huchamabacha that pointed out in her reblog tags that just wait until anakin learns that he could maybe man the table where donors check in or be the one that goes around handing out juice boxes to donors afterwards which i think is soooo incredibly valid and means that there is hope for you as well to meet a hot doctor at the blood drive lmao
i'm imagining obi-wan doesn't see anakin for a few months and he's starting to relax and then he shows up and anakin is sitting behind the check-in table wearing a 'volunteer' badge and the smarmiest but yet somehow sort of earnest smile obi-wan has ever seen
(after they get together there's at least one (1) halloween where anakin insists on dressing as sexy nurse - obi-wan isn't allowed to complain because anakin points out he could try to wear this get-up to the actual next blood-drive they work together, and suddenly obi-wan is counting his lucky stars)
#asks#obikin#funniest i think if anakin actually works in hospital administration#hadn't been able to complete medical school cause he dropped out when his mom died#but has a background in medical knowledge that means he knows damn well that he can't give blood#and also that while obi-wan is being chewed out by an exasperated mace windu#anakin is like a hallway away being a professional nuisance
52 notes
·
View notes
Text

Sir, what happened to your chin?
#opbackgrounds#one piece#ch523#character design#did he go to the same hospital as captain morgan?#which is to say#I don't believe that man's been to medical school
89 notes
·
View notes
Text
Why the Spleen Sucks
The spleen is a really shittily placed organ, making it prone to injury. This injury is usually severe and can lead to death if not properly managed. We're going to look at the function of the spleen, what happens when it is damaged, and how to write about.
Where is the spleen? It's in the upper left quadrant of the abdominal cavity, nestled right against the ribs (typically 9-11) at the midaxillary line. It's behind the stomach and is considered intraperitoneal. The main thing is that the spleen is very vulnerable. It is literally right up against the ribs without much protecting it. It's shaped like a little bean and is purple in humans. It is fed by the splenic artery, which comes off of the celiac trunk (which sticks off of the abdominal aorta).
What does the spleen do? Its main job is to filter out old and malformed red blood cells. It also holds immune cells. Certain diseases can cause the spleen to enlarge, including cirrhosis of the liver (it's connected to the hepatic portal system), sickle cell anemia (RBCs are stuck in it), and autoimmune disorders. The spleen also holds about 250 mL of RBCs in reserve in case you need them.
What happens when it is injured? The spleen can be ruptured and lacerated kinda easily. Blunt trauma to the ribs can cause it to rupture, and this is seen in contact sports and car accidents mostly. Because of those giant gaps between the ribs, it's also prone to injury from knife attacks. Gunshot wounds are another common cause, as well as broken ribs penetrating it (broken ribs are very sharp, like way sharper than you imagine). Rupture is more likely when someone has splenomegaly.
When the spleen is damaged, you're going to get a lot of intraperitoneal hemorrhaging. The spleen filters a lot of blood and has blood in it, so there's going to be a lot of blood in the abdomen (obviously). This will lead to distention, guarding (abs are tense), and hypovolemia. The left upper quadrant will be painful, and there can also be referred pain to the left shoulder (Kehr's sign).
If the patient has a small laceration, the symptoms aren't always as dramatic. Sometimes they'll just have low hemoglobin (which is on RBCs), maybe some thrombocytopenia (lots of platelets in the blood).
How do you fix this? If the injury is small and the patient is hemodynamically stable, they can usually be given a blood transfusion and the spleen can heal itself. Sometimes surgery is also performed to clamp a vessel or repair the outer layer of the spleen.
If the injury is major, then surgery will be performed. If the patient is less critical, they may go in and try to fix the problem. If it can't be fixed, they may do a splenectomy (remove the spleen). In a critical patient, they might forgo the nice pretty incision on the left side, and instead just split the patient down the middle. In these situations (in my experience), there isn't a lot of time to waste. One thing that we aren't going to waste time on is anesthesia, for example. This is with a lot of very critical surgeries, at least from what I have seen. Like the surgeon will start cutting as they are working on knocking out the patient, but usually they are in so much pain that they don't even register it.
If you remove the spleen, the patient is more at risk for infections, but with modern medicine and vaccinations, it's not as much of a big deal as it used to be. The patient will probably be fine.
Writing tips: (new section idea, hope you guys like it, lol) As with any injury, you have to make sure that you are giving them an acceptable mechanism of injury. With the spleen, this is either blunt trauma or penetration/laceration. Getting tackled, getting stabbed, getting shot, all great MOIs.
Second thing, present the appropriate signs and symptoms. A sign would be like bruising, hypotension, tachycardia, etc. A symptom would be LUQ pain, Kehr's sign, etc.
Next, figure out what you're going to do and where you're going to do it. In the field, there probably isn't much you can do. The most would probably be a laparotomy and clamping the splenic artery, but I mean, when I was an EMT, we were not doing this. There's a lot of stuff you can theoretically do, but never gets done. But I mean you can write it. If the patient makes it to the hospital, I think it would be more fun to do emergency surgery and just split them right down the middle. There's going to be a lot of blood in the greater omentum, very high stakes and exciting.
Anyways, hope you guys liked this, please let me know if I got anything wrong. I wrote this off of my personal experience and a few good textbooks, but there can always been mistakes in things.
#medicine#med student#medical school#biology#med school#med studyblr#whump writing#anatomy#spleen#hospital whump#surgery#emergency medicine#medical writing#writing reference#injury
77 notes
·
View notes
Text

i thought of this au this morning. i’ve written 10 pages of headcanons, research, and outlines already.
i had a polisci paper i needed to write today…
#hermitblr#hermitcraft#hc#life series#life series au#hermitcraft au#healing hermits au#medical au#hospital au#should be doing school work
23 notes
·
View notes
Text
Sekaiichi hatsukoi is so much fun bc the tyrannical boss who takes their job way too seriously and the new employee who doesn’t know a damn thing is such a relatable concept and you can plop the entire cast into whatever au you want and it would still work just as well
#sekaiichi hatsukoi#I spent my last shift trying to put the characters into a lab work au and it still worked#Ritsu as the son of a hospitals ceo who got a cushy day shift job in microbiology at his dads hospital fresh out of lab school#he loves it and he’s good at it but he overhears the nighshifters talking shit abt how good he has it and that he doesn’t have to work that#hard bc micro is slow-paced and honestly it’s usually the same species of bacteria so it isn’t that hard to identify the species#so he quits and gets a job at a rival hospital but he’s put into a 2nd shift blood bank position despite never having worked in it#takano is the lead tech who comes down hard on anyone who makes mistakes bc this is literal life or death#it’s not just streaking plates and doing fun little biochemistry tests then putting the sample into the crispr to verify#the most advanced technology they have in bb is the cell washer. convenient but not as helpful#his first few days there are just back to back massive transfusion protocols and he genuinely wants to crawl into a hole and die#things calm down after his first week but it’s a huge learning curve and no one has the patience or the time to properly train him#emerald can all be blood bank specialists. Yokozawa is the head of histology.#having trouble finding roles for everyone else#kirishima could be a pathologist and Yukina could be a receptionist at a medical office while he goes to phlebotomy school(?)#or nursing school. something like that
24 notes
·
View notes
Text


Between the OR and the ICU always finding some time for coffee 🤍
#studyblr#med life#medicine#studyspo#studystudystudy#studying#medical students#medblr#medical school#med#study motivation#medical studyblr#study hard#study aesthetics#motivation#hospital#clinical rotations#icucare#photography#dark academic#medecine university#uniblr#100 days of productivity#study inspo#linastudyblrsbog
126 notes
·
View notes
Text
Working on my robot au and i decided ichimatsu would be the brother that would be extremely popular bc hes marketed as a domestic companion. There'd be someone in a civil rights legal battle with the supreme court to actually allow ai-human marriages to be legally recognized, with an ichibot.
I say this for several reasons, but mostly bc i can see yall doing that.
Osomatsu would be the cheapest to buy secondhand bc he keeps accidentally gaining real sentience and uses it immediately to gamble, commit crimes, fuck around and over all do osomatsu related bullshit. But he can drive! Thats his special feature!
I have ideas ofc for the other ones but lol ive been thinking "and osomatsu can drive too please stop returning him you cab use him as a taxi driver and make money off of him you just have to be okay with the fact he might hit on your customers or crash your car, or steal your money to gamble pleeaaaseee we're trying to fix this in Series 4!"
#open_mouth.exe#see the issue is that oso should be a big brother unit and theyre robbing him of hos true purpose#suematsu would ofc be social units. they would be purely companions with jyushi specifically being therapeutic#he'd be frequently seen in hospitals as a form of durable medical equipment or youd find him in schools as a coach or chaperone#there would be a few professional leagues made of jyushi custom configurations in the same way you see robot fighting#and theyd be use for multiple sports including mma and wrestling. and baseball ofc and stuff. jyushi is a companion tho but his uses are#medical and sport. hes a team member.#todo for the most part multipurpose but he does best as a companion. he's typically be used for lonely people who want to chat. lgbts. and#customer facing jobs. he'd be use anywhere from client relations. call centers. some restaurant chains would have one as a gen manager#he's priced out for the most part from the average population bc he has the most complex scripts so finding one secondhand would be rare#bc like jes highly sought after. many people WANT to buy him as a life partner after interacting w him in a csr context#but see his literal 22.5k price tag new and go thats the price of a new car..#osomatsu on the otherhand theyre tryong to give away at the door. current gen 3 brand new osos are less than 3k. they desperately want to#keep him in circulation bc hes a literal scientific marvel like they finally made the first artificial deadbeat loser#he tends to get bought by ppl who want a boyfriend or a friend but typically ends up as a bad influence so ppl return him#i got stuff about kara and choro but i haven't thought about it too deeply. i feel like both of them would be used for unintended purposes#Karamatsu for instance feels like he would be designed for people with social anxiety or for creative fields#but i feel like people would end up having an entire mod scene specifically for sexing him up in various ways like ppl woild become#programmrrs to fuck him. Kara can also drive but its not important bc oso comes with an internal gps and he doesnt#choro feels like he'd be designed as an elderly caretaker and companion but would end up somewhere else. i think#people would use his predisposition for entertainment and idols as like a utau and would have him either produce or sing music#like choro units would end up in so many bands
10 notes
·
View notes
Text
HenRen/Buddie AU where they slightly swap stories and Buck and Eddie are the couple who are set up by friends/family who share custody of Eddie’s son (Shannon takes Chris to LA in this timeline and Eddie follows) and Hen is the hot single mom (Eva and Hen were together when she got pregnant with Denny but she leaves shortly after his birth) who is the bane of Karen’s existence after she’s brought in as a medical consultant for their new project until she learns not only is Hen charming and smart but her son might be the cutest kid in the world
#I like to think Hen still works at the 118 for a bit then actually pursues medical school where she meets nurse!Maddie and nurse!Eddie#Chimney is still a paramedic and visits Hen on his days off which is how he ends up falling for Maddie#Maddie came to LA sooner and her and Buck live together and she sets him up with Eddie after bonding with her now work bestie#Eddie instead of being a paramedic goes to school and studies nursing for a bit bc Shannon has custody of Chris and wants them to finally#be stable and have stable hours but after a couple months of separation they realize they work better as coparents than partners#and agree to get divorced and share joint custody of Chris#Hen serves as a doctor at the hospital where Maddie and Eddie work at but does a lot of medical trials and is brought on as a consultant bc#she loves to learn new things#Karen is still a rocket scientist bc that’s sick af and I literally don’t want her to have another job LMAO#anywayyyy#911 abc#buddie#eddie diaz#evan buck buckley#henren#Henrietta Wilson#Karen Wilson
14 notes
·
View notes
Text
Awful wretched horrible chronic illness decided to come out of remission whilst ap exams this is unfair I want to kms.
#probably went out of remission because of the stress + lowering of medication but igggghhhgg#I was doing so well too#6 months without a flare up and then I get this bro 😔#I just hope I don’t end up in the hospital again#chronic illness#uggggh so tired idk if I’ll be able to go to school tmr
5 notes
·
View notes
Text
Trigger warning: hospitals, blood 🏥🩸
I've started my fourth year of medicine and it's only been a week and a few days. I've had two intakes (intake is like the med student equivalent of being "on call" but obviously you are free labour (you're not actually free labour, you pay the university tuition so we're in a deficit here)) and oh boy. Hospital working hours are 08h00-16h00 usually, with intakes from 16h00-22h00. Running around dark, probably haunted, hospital corridors at night with nothing but the torchlight from your phone to light the way? The fourth elevator on the extreme right always opens twice and makes strange groaning noises. Once we heard something akin to a whisper ~ behind us in the elevator. My first block is on the 13th floor. The hospital I'm working at is built on the beachfront. When it rains, the sea mist is so thick and surrounds everything. You can see the harbor lights from the fogged up windows. The dark grey sea beckons you. Last night I was down in casualty. The doors were wide open, and I could see the parking lot, and then the beach, and then the ocean. The rain lashed down on the water. It looked so grey and dark but I felt oddly compelled to walk out the door and down to the water in the rain, until the cuffs of my pants tasted the salt water. To get to the new children's hospital, you have to walk past the abandoned, decrepit old wing of the children's hospital. It's a giant, hollow, shell of a building, mesh and wire twisting in the wind, the wind howling through it's empty corridors. Sometimes if you look into the broken windows you may see a pair of tiny, glowing eyes staring at you. Blink and all you see is darkness again and stained bricks. We always rush quickly past. Sometimes when you're on intake and exhausted and the 4 hours of sleep starts catching up to you, and it's late at night, past 10, you start seeing and hearing things. I helped take bloods today. When filling the blood collection tube, some splashed onto my exposed skin. I stood there, frozen for a few seconds, in shock. Paralyzed by the sight of it. My friend nudged me towards the sink. Mechanically washing my hands, the strong smell of the alcohol sanitizer lingering. It was so red. Sometimes, when we have a few minutes, we stand at the windows and watch the waves. We point at the surfers and laugh when they wipe out, the waves carrying them away. We talk about going down to the beach. On our way back to the ward, we see the cleaner lady wipe blood drops off the floor with a paper towel. The air smells like sanitizer, sickness, iron, and sea mist.
#medical school#med student#med studyblr#hospital#monsters#gothic#horror#haunted#writers on tumblr#artists on tumblr#poetry#short story#dear diary#look i know this is my art blog but i am also a medical student and i use this space as my personal diary sometimes okay#i like sharing stuff with you guys#i havent made much art recently but i do have lots of med school stories to offer#if that interests you perhaps#i am a 4th year so we have just started clinical years#which means hospital work#art#writing#writeblr#i fear i am a jack of all trades#for context i am not american lol#i am from a developing country#med school is 6 years where i am from
7 notes
·
View notes
Text
Blocking the Neuromuscular Junction
Neuromuscular blocking agents (NMBAs) stop transmission at the junction between nerves and muscles, which will cause partial or complete paralysis. Why do we want to do this? The main reason is to cause paralysis for starting endotracheal intubation (relax throat muscles), surgery (keep the patient still), and for putting people on ventilators (stop them from fighting against the machine).
You might also give someone an NMBA if they are coughing up blood, having a severe asthma attack, have high intracranial pressure, or are shivering with hypothermia.
There are two types of these drugs and they work two different ways, though they are all given intravenously.
Depolarizing NMBAs
So to initiate muscle contraction, our body uses a transmitter called ACh. When this binds to a receptor, some ions move around and the muscle contracts. This is called depolarization. After some time, the cell can repolarize as ACh is digested by the enzyme AChE.
The main depolarizing NMBA is Succinylcholine. This also binds to the same receptor, causing muscle contraction. However, it is not digested by AChE, so the cell cannot repolarize. The muscle will keep contracting until it runs out of calcium ions and relaxes. The muscle is paralyzed after that because the receptor is still blocked. Only when the serum enzyme BChE digests it can we reactivate the muscle.
Succinylcholine is mostly used for intubation. It only lasts for a few minutes, which is good because once you trach someone you don't need to paralyze their throat anymore.
The main risks of this drug are hyperkalemia (potassium exits the cell when the muscle is depolarized), muscle pain, hyperthermia, and increased intraocular pressure. Succinylcholine is contraindicated in burn patients.
Nondepolarizing NMBAs
These drugs also act on the ACh receptor, though they do not activate it. The most common ones are atracurium, cisatracurium, vecuronium, and rocuronium. I'll go through a few important notes on each one.
Atracurium (an isoquinoline) is metabolized into the active laudanosine, which has a stimulating effect on the central nervous system and can cause seizures. It also increases histamine, which can cause flushing. Cisatracurium is also an isoquinoline, but it does not cause an increase in histamine or break down into laudanosine. Both of these can be reversed using neostigmine to up the concentration of ACh and outcompete them at the receptor.
Rocuronium and vecuronium are both aminosteroids. Rocuronium has a quick onset and is great for rapid sequence intubation. It also does not require dosage adjustment for those with renal impairment. Vecuronium is slower, and needs to be adjusted for those with renal and liver impairment. These can both be reversed with sugammadex, which will form a complex that can be pissed out. The only thing with sugammadex is that it can cause bradycardia, decrease the effectiveness of contraceptives, and increase the risk of bleeding.
The adverse effects of all of the nondepolarizing NMBAs are apnea, hypotension, and electrolyte imbalance. You also need to increase the dose for those with burns and trauma. These drugs also interact with volatile anesthetics, increasing their effects. However, this is actually a favorable effect, as it lowers the dose of anesthetic required.
Using These Drugs
The main thing to remember here is that NMBAs do not cause sedation or amnesia. You must use them with things like propofol, midazolam, benzodiazepines, opioids, etc. I will repeat: DO NOT USE THESE DRUGS ALONE. The patient will be paralyzed but CONCIOUS and AWARE. For the love of medicine, please. The reason I say this is because I have seen paramedics give "problem patients" a paralytic without a sedative in some sick sort of revenge. Fuck them. I don't care what a patient did, that is not okay to do. Still makes me mad just thinking about it.
Anyways, so these are one part of the drugs required for surgery. If you just sedate someone, they'll still move around, and you don't want that while you are cutting on them.
Writing Tips
There isn't too much to say here, but I think it is important for people to know these drugs exist and only paralyze, not sedate. So shit, if you wanna write some crazy horror stuff happening, you can just have someone be paralyzed. Or also this is how people can be aware during surgery. I think there was a big case about this a few years ago. Sensation is still intact when these drugs are given alone, so go forth and torture people I guess (??) - IN FICTION
Anywho, that's all, thanks for reading. Maybe I will write soon about intubation, sedatives, and other stuff like that. Kinda neuro (which one the poll).
#medicine#medical writing#med studyblr#med school#med student#medical school#whump writing#medications#neurology#hospital whump#whump reference
23 notes
·
View notes
Text
I have an idea for a KHR hospital AU where all the acrobaleno are different kinds of doctors/work in different departments at the hospital but Skull is just a regular guy who’s always there because he gets injured so much
#khr#katekyo hitman reborn#khr skull#or maybe he’s a stunt devil or something#also only have some vague ideas of where the others work#since my knowledge of hospitals come from medical dramas#and the time in high school when I volunteered at one lol
65 notes
·
View notes
Text
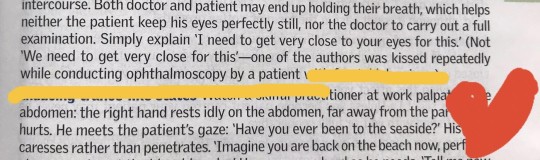
Oxford Handbooks are not only brilliant for quick revision before clinical internships,but they can also boost up your cry-baby mood from all day spent in hospital with pearls like this ❣️
(omg he was kissed REPEATEDLY!!)
#Shoul I re-consider my chosen specialty ?#Ophtalmology is so romantic?!#better mood after reading this#medical university#oxford handbook#clinical medicine#medical stuff#medical humor#medblr#medblr community#medical training#oxford books#med school#hospital#clinical pearls#studyspread#tmedic#studyblr#i wanted to cheer you up#boost mood#❤️#ophtalmology#clinicalstudy
20 notes
·
View notes