#I have All The Electrolytes in supplement form
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com rank in the US is 25.
Text
Hey y'all! The AC in my house is like half-broken and I have all the heat tolerance of a particularly sad penguin*, so I could use some advice. I am from a desert area, so I know the stay hydrated, electrolytes, loose clothes type advice, but do you have any advice for handling the heat in humid areas specifically? Also, does anyone have any recommendations for sun hats? Specific sun hats you recommend are what I'm looking for, but if you don't have a specific one an idea of what criteria I should look for would be very helpful too *I say this jokingly, idk how much heat tolerance penguins actually have. I have POTS, salt wasting syndrome, and some unknown autoimmune issue that probably involves my endocrine system? Docs are still working on it but the sum total is I cannot exist in hot temperatures
#the person behind the yarn#tj asks weird questions#this one isn't that weird that's just my tag for this#I have All The Electrolytes in supplement form#and I take them regularly! and a medication to make me retain them better!#it just doesn't work enough for summer#the AC is keeping it to mid 80s at the highest but at like anything over 78ish I start wilting#like a dramatic houseplant#and I saw a post and apparently benadryl makes you sweat less??#which on the one hand is good for me personally for 'hey that is my salt I want to keep it' reasons#but on the other is bad for 'actually lowering temperature' reasons#though to be clear I don't really overheat. like. I do not get actual heat exhaustion#my problem is my body is Too Good at vasodilation in an effort to shed heat#so my blood pressure drops and it makes my heart rate skyrocket to try to compensate#but frequently when it's hot my body temperature is actually a full degree or more BELOW my normal#I am not in danger of actual overheating in any way shape or form. I'd pass out first from low blood pressure lol
24 notes
·
View notes
Text
Okay but can we talk about the amount of electrolytes (sodium specifically) that Bakugo must need to consume to exist??
Weird thing to fixate on, I know, blame my degree, but think about this: His quirk relies on his ability to sweat, which means the more he sweats the more he can use it. The main thing you lose when you sweat is water and sodium, the longer you sweat, the more those leave your body, that's common sense. Sodium helps you retain water and maintain the fluid balance inside and outside your body, which is why you see it hanging out with water so much and why it's such an important electrolyte that gets lost easily. Yes, technically, you also lose magnesium and potassium, but you lose less of those in sweat than sodium.
Most people don't actually need to supplement electrolytes, even those who exercise regularly, (this is excluding those with illnesses, just considering the average person here), you can get what you need from plain water. Even some athletes don't necessarily need to, it tends to depend heavily on how long you exercise, which is why you see people who do ultramarathons or ironmans downing them. There's ways to test whether or not you actually need them, but suffice it to say, more often than not, just drinking normal water is perfectly fine.
But Bakugo?? There's no way that boy doesn't burn through sodium like it's a fucking competition.
See, the key to whether or not electrolyte supplementation is needed is often found in how long you exercise for, as well as the environmental conditions. Say, if you're exercising outside in the spring for like, thirty minutes to an hours, just water is going to be all you need. Contrast that with a hero course student who likely exercises excessively, multiple times a day, every day, and has a quirk that relies on sweat. That is a recipe for ✨disaster✨ and you know what I don't see on his, or LITERALLY ANY OTHER HERO'S, costume??
A WATER BOTTLE.
I don't care if it ruins the aesthetic you're going for, dude, get a freaking water bottle and some little electrolyte packets before you pass out. How have any of these kids not thought of having some form of water on them while hero-ing?? Like y'all gonna be out on patrol for HOURS without any source of hydration? What a great way to die!
Honestly though, how many times do you think Bakugo just keeled over as a kid? Like dehydration can be a sneaky little shit, and with a quirk like that I'm sure they became besties.
Honestly, I wonder if he does actually carry electrolyte drinks and packets around with him because of that. Like, Izuku had to drag his ass back home too many times while they were out playing as kids and he got tired of it so he spent forever researching different electrolyte brands and sleuthing out which had the best water to sodium to sugar ratio (because you do want some sugar in your electrolyte drinks, the sodium uses it as a quick transport to get where it needs to go) for optimal rehydration. And now he's like, hyperaware of the symptoms and anytime his classmates look even a tiny bit like they might be dehydrated he just storms up and starts throwing electrolytes at their face like:
"DRINK YOUR WATER YOU IDIOTS, DO YOU WANT SURVIVE THE FUCKING LEAGUE OF VILLAINS JUST TO DIE OF DEHYDRATION?? THAT'S FUCKING PATHETIC. SIT DOWN AND DRINK THAT BEFORE YOU PASS OUT, DUMBASS."
All while violently shaking a water bottle with the electrolyte powder to shove down their throat.
Aggressive love, yk? At least he's trying.
#mha#katsuki bakugou#mha spoilers#mha manga spoilers#my hero academia#izuku midoriya#bakugo katuski#also my bachelors WIP is nutrition#so you know I'm not just talking out of my ass#I do study this professionally#boku no hero academia
21 notes
·
View notes
Note
I'm the anonymous person from before..
I won't get into too much details about my personal conditions so I'm only giving enough details for you to know my remedies for migraines that might help. But, some remedies, you have already done by now.
So I severe from migraines a lot. And because I'm autistic, I've always had many migraines because of sensory overload type situations that would last days and even a week. Depends on the situations though.
Some of these are my "remedies" for my migraines.
Laying, even sleeping if that sleeps, in the darkest room you have so I would suggest covering your windows if you need to darken the room to make it less bright. Laying with an eye mask might help with that.
Ice. I recently got this icepack that's like wearing an eye mask, and it's giving enough pressure to your whole head (without hurting you) that tends to seem relaxing. But I don't think you have that. So you ice, ice packs, on your head and neck. Wearing the ice around your ice would be more effective than one your head from my personal experiences.
Drinking water. Coconut water, if you could actually be able to drink it since not everyone enjoys the flavor, is the real water that actually will help hydrate you faster. Mineral waters like fiji could help since lots of those waters have electrolytes. Maybe consume salty foods like soup or chips, or even a pinch of salt on your tongue, just to keep the water in your body. Since not everyone knows salt retains the water in body.
Ibuprofen. Or whichever medicine you usually take.. I would have said to try taking turmeric? Turmeric helps with head and body pains if it's a more holistic approach. Maybe add to your food? Supplements?
Bathing. Warm, or even hot, baths and showers. A hot salt water bath could help? Or just a regular hot shower. Not everyone knows a warm water may actually help with migraines. Since showers and baths are considered to be forms of heat therapy for migraines. They say that among other heat-related remedies, a warm shower has the power to stop pain signals from traveling to the brain and increase blood flow, which can help soothe muscles.
Eating. Because sometimes lack of eating causes migraines too.
Don't know if I missed anything? I was trying to think of my remedies.
Let me just say that I love you so much. I’ve only started getting migraines in the last 5-7 years so it’s still “new” to me.
Just wanted to start off saying thank you thank you thank you. I’m currently undiagnosed but very likely to be autistic as well and it’s only really presented itself fully in the last few years, meaning I’ve always had it, obvi, but I only recently started unmasking. So just learning that that could be a cause is something new and so super useful.
As for the dark room and laying down. I spent about 70% of the last two days sleeping and lying down hoping it would help. And it did a little bit.
The dark room is usually what I do for my severe migraines. I lock myself in my bathrooms and put a towel at the bottom of the door.
Ice is something I never thought about! I’ll have to go get some ice packs!!! I have a heat pad but no ice packs.
If I plug my nose I can drink coconut water but I’ve been guzzling all weekend I can promise you that ♥️.
I don’t have ibuprofen on hand but I did take a shit ton of acetaminophen and it unfortunately did nothing. however I’ve never tried tumeric so I will have to keep that on hand as well!!
And a shower was actually one of the first things I tried because I know it always helps. And it did. But I can’t stay in the shower for 48 hours :(. Stupid being a land mammal and the powers that be charging for a fundamental human right.
I had a really yummy dinner last night that my partner made me for eating. It was a big helping of chicken pasta Alfredo. I want to think it helped but I honestly couldn’t have told cause I felt a little nausea every time I took a bite. But it was so so good.
Hon if you’re missing anything I can’t say anything but thank you for the things that you did remember. I’m gunna keep this ask for later when I inevitably get another one because this has been so incredibly helpful.
Thank you thank you thank you so much truly ♥️♥️. You’re a good human. I hope you know that.
#the kindest of souls#if I hadn’t mentioned it earlier. thank you. i love you. i am 10000% referring back to this at a later date#my mum thinks this particular migraine was weather induced cause the weather here has been insane lately#but yeah. keeping this in my little storage container for future use ♥️#asks#anon#ms.mailbox📬#THANK YOU ♥️♥️♥️♥️♥️
12 notes
·
View notes
Text
The Post-Bisalp Diaries, Part Two: Survival Of The Tubeless
Happy Two Week Anniversary of me noping the fallopes!
When I was reading up on how others managed post-Bisalp before my own surgery, I saw suggestions like "take Gas-X for bloating", "use stool softeners so you don't 'strain' yourself", "have a heating pad for the shoulder pain", and so forth. They sounded helpful, and it was a good thing I had that stuff already on hand (for other reasons).
That said, here's what really helped me out during my recovery. ***DISCLAIMER*** Your mileage may vary, all bodies are different, and I sure as shit am no doctor or medical practitioner!
*Turmeric-Curcumin Pills*
It's what I first turn to when I get crap like PMS cramps or headaches. I do have ibuprofen on hand, but it's more of a last resort remedy for me. The ones I've been taking post-surgery are Gaia Herbs Turmeric Supreme, but I also have Terry Naturally's Curamin (regular strength) pills.
*CBD Stuff*
Thank goodness I live in a state where CBD products are legal to own. Tinctures and gummies, particularly the ones from Lazarus Naturals, have been a godsend.
*Probiotics*
I still took probiotics pre-surgery, albeit in food form (yogurt, sauerkraut, etc.) since I couldn't have supplements then. When I learned that I was given antibiotics during my surgery, I knew I needed to take probiotics later in the day; it's what balances out your digestive system after the antibiotics fuck with it. Maybe it could explain why, even if my appetite was reduced for the first few days, I didn't have bad gas. I took a high-dose probiotic (think the pills with over 40+billion cultures) in the first week, then, for the second week, went down to probiotics with no more than 25 billion cultures. And some low-sugar yogurt.
*Pedialyte Pops*
Like with many others who had a Bisalp, sore throat is a common post-surgery symptom. (It's the result of having a breathing tube down your throat during the procedure.) Though I had regular popsicles on hand, I ended up buying Pedialyte Freezer Pops as well as they also have electrolytes in them. And they're also fairly low sugar!
*Thrift Stores*
So I had to change up my wardrobe a bit for my recovery. A month leading up to my surgery, I got some jumpsuits, loose, high waisted pants with a comfortable waistband, slip-in shoes so I don't have to bend over and tie my shoes, and even a bed rest pillow in case I felt like a lazy-ass. Thanks to thrift stores, I got all that for a bargain. Who the fuck needs Wal-Mart?
By the way, because of my need to be active, and me fighting the fatigue during the first few days of recovery, I didn't use that bed rest pillow. I guess I may need it down the road, and it only cost me $5.
*Eating Low-Carb, Minimally Processed Foods*
Having been on Keto for the past few years, the diet has not only helped me shed blubber, but I've become more active from it. I can't say if eating low-carb/sugar-free foods and minimally processed foods helped my body heal quicker, but, save for the first three days after surgery, I never felt sluggish in my recovery.
*A Decent Landlord & Loan Deferments*
OK, forget the physical aspects of my recovery; it's the financial aspects that took the real beating. I'm able to receive Short Term Disability while out from work (I do not work from home and my job is very physical), but waiting for the payments have become a pain in the clit. I'm still waiting for them, and it just happens to be a holiday weekend right now. Just my luck! So, I like to give a shout-out to my landlord who was cool with me underpaying my rent for this upcoming month, and the few loan companies who I have accounts with that were able to postpone my payments so I don't go so broke to where I need to sell my sterilized ass on the streets for a few bucks. (Like, literally a few bucks--it's the going rate for old millennial ass.)
Also, a friendly reminder that just because one is childfree doesn't mean they got deep pockets. Some of those "I got to vacation in Italy last week 'cause I got no kids!!!!" posts you see on Reddit's Childfree subreddit are likely made-up as hell (it's Reddit, after all). Now that I think about it, I think I'm more of a WINK (What Income? No Kids) instead of a SINK at the moment.

A Few Things I Got/Have That I Didn't Need In The End...
--GasX pills (I was never really gassy, and they were the 99-Cent Store version as opposed to the name brand, so I didn't lose money on that)
--Shoulder/Heating Pad (others have suggested it, but I only used it just once and that was because it was a cold night)
--stool softeners (I think the probiotics helped me out with this one)
--ibuprofen (took it once and it fucked with me. I'm used to the 200mg pills, but 600mg per pill?! Fuck no!)
--prescribed oxycodone (didn't even open that shit)
And A Couple Things You Don't Need To Buy...
--disposable underwear (the hospital will provide you with as many pairs as you need. I never bled, thankfully, but I was still given a few pairs.)
--anti-nausea patch (another thing the hospital will give you, but only if you request it. I could've saved myself $6 from the pack of anti-nausea patches I bought on eBay! *punches air*)
*****
Again, what helped me out post-Bisalp may or may not help the next person in recovery. If there's one thing I highly recommend that will help the next person recover from a Bisalp smoothly, it's having plenty of money so you don't have to worry about financial shit like me.
**ETA: Tumblr told me this is my 100th post here. I'd celebrate but I also outed myself as a broke bitch in the post, so...
6 notes
·
View notes
Text
I am increasingly annoyed at the state of my healthcare and wondering what the actual hell is going on at my doctor's office.
In January, combination of dehydration and infection meant I had a surprise ER visit, where I learned I was a little low on potassium as well, and keep an eye on that.
No problem, I kept that in mind as I was grocery shopping, thought it was fine.
Two weeks ago I fucked around with my caffeine intake and Found Out in the form of chest pains, as well as some heart issues, which lead to a holter monitor for a few days, a chest x-ray, bloodwork, all sorts of fun things as they determined if I was having mini heart attacks or not. Everything came back fine, but I was never told 'well, come in to do more tests to find out if you're actively dying'. Meanwhile, I got desperate enough to pick up a potassium supplement as a hail Mary, hoping that an electrolyte imbalance was the cause of my problems.
And it looks like it was, because despite never having been told this from my bloodwork at this latest doctor's visit, the chest pains cleared up almost immediately and the heart stuff shortly after that.
And I still haven't heard back from my doctor's office, so either they assume that I'm not dying and I'll be fine so no need to talk to me, or they just aren't bothering to let me know what they're looking into.
1 note
·
View note
Text
The "ick"post really grinds my gears.
I'm not the tallest man on earth. I'm not the heaviest man on earth.
I'm also over 6 feet tall, if only by a bit. I'm also a little over 200 lbs.
Regular ocean waves *won't* bowl me over. But why would a shorter, lighter man be worth less as a human being, simply for being somewhat more susceptible to ocean waves? Is he going to spend his whole life in those waves? Is he always going to be bowled over by waves? Is that all he is? Someone bowled over by the waves?
That said, I am not the man, though I feel pity and solidarity for him. No, I'm the man who would carry a water bottle.
Remember: I am over 6 feet tall, and I am over 200 lbs - about 205, 210 last I checked. I have significant body mass, and I have a large surface area. The heat affects me tremendously. If I have to stay out in the heat for a long time, and I have water, I might go through bottle after bottle of water, sweating and sweating it all out, and I may not have to urinate, for hours, because the water comes out in the form of sweat before it could ever possibly pool in my bladder enough that I'd have to pee. I also need lots of electrolytes, because I sweat so much that, good as water is, I get heat migraines from electrolyte loss unless I supplement my water with electrolytes, and drink a lot. It wasn't my choice to live in the desert, and my body is certainly not made for desert survival (thank you, Scottish genes, for preparing me to live in the Scottish uplands, when, aside from my dad's brief stay in the UK for a few years as a kid, my family hasn't been anywhere in Europe for centuries, too busy being damn colonizers on a land that deserves better than this, and had the bright idea of moving to hotter and drier places that aren't bad places, but are places we physically do not do well in). Nonetheless, I am in the desert, and I must deal with the heat as best I can, when exposed to the elements.
Yet adapting to circumstance is... "ick". What is this "ick"? "Disgusting"? "Weak"? "Inferior"? "Unattractive"? "Embarrassing?"
I am sure my dry, bloated, rotting body, dead from heat and dehydration, would, on the contrary, be ruggedly handsome, masculine, and sexy. Huh? Don't you want to fuck the dead body of a man who died from the heat, because he valued his masculinity enough not to carry a water bottle?
Disgusting. Such judgment is the true "ick".
0 notes
Text
HerpaGreens Reviews - WARNING! I Tried This Herpa Greens For 30 Days!
HerpaGreens is a dietary supplement that claims to be effective in treating and preventing herpes outbreaks. The product is formulated with natural ingredients that work together to boost the immune system, reduce inflammation, and fight off the herpes virus. This article will provide an in-depth review of HerpaGreens, examining its ingredients, benefits, and potential side effects, as well as customer reviews and pricing information.


What is HerpaGreens?
HerpaGreens is a dietary supplement that is formulated to help treat and prevent herpes outbreaks. The product is designed to work by boosting the immune system and reducing inflammation in the body, which can help prevent the herpes virus from replicating. The supplement is made with natural ingredients, including fruits, vegetables, herbs, and spices, which are believed to have antiviral and immune-boosting properties.
According to the manufacturer, HerpaGreens is a safe and effective alternative to traditional herpes medications, which can cause a range of side effects and may not be effective for all patients. The supplement is also said to be easy to use, as it comes in a convenient powder form that can be mixed with water or added to smoothies or other beverages.
HerpaGreens Ingredients
HerpaGreens is made with a blend of natural ingredients that are believed to have antiviral and immune-boosting properties. Some of the key ingredients in the supplement include:
Spinach: Spinach is a nutrient-rich leafy green vegetable that is high in antioxidants, vitamins, and minerals. It is believed to have anti-inflammatory properties that can help reduce inflammation in the body and boost the immune system.
Broccoli: Broccoli is another nutrient-rich vegetable that is high in vitamins, minerals, and antioxidants. It is believed to have antiviral properties that can help fight off the herpes virus.
Tomato: Tomatoes are high in antioxidants and are believed to have immune-boosting properties. They are also believed to have antiviral properties that can help prevent herpes outbreaks.
Ginger: Ginger is a spice that is known for its anti-inflammatory and immune-boosting properties. It is also believed to have antiviral properties that can help fight off the herpes virus.
Green tea: Green tea is high in antioxidants and is believed to have immune-boosting properties. It is also believed to have antiviral properties that can help prevent herpes outbreaks.
Turmeric: Turmeric is a spice that is known for its anti-inflammatory and immune-boosting properties. It is also believed to have antiviral properties that can help fight off the herpes virus.
Garlic: Garlic is a natural antibiotic that is believed to have antiviral and immune-boosting properties. It is also believed to have anti-inflammatory properties that can help reduce inflammation in the body.
Spirulina: Spirulina is a type of blue-green algae that is high in protein, vitamins, and minerals. It is believed to have immune-boosting properties that can help prevent herpes outbreaks.
Reishi Mushroom: Reishi mushroom is a type of mushroom that is believed to have immune-boosting properties. It is also believed to have antiviral properties that can help fight off the herpes virus.
Coconut Water: Coconut water is a natural electrolyte that is believed to have immune-boosting properties. It is also believed to help reduce inflammation in the body.
#herpagreens reviews#herpagreens#herpagreens review#herpagreens supplement#HerpaGreens#herpagreens scam
0 notes
Note
Do you know if supplemental estrogen has the same level of harm for men as testosterone does for women? My cursory impression is that testosterone supplementation is much more deleterious for women's health in the long run, which just evidences the misogyny and female erasure in the movement. Estrogen has protective effects and been implicated in why women live longer on average. What are your thoughts? Signed, a radfem lurker who really appreciates all that you do :)
hey dear lurker!
yes, i'd say testosterone in women is more harmful as a rule than estrogen in men. in the cursory research I did, there aren't the same reports of chronic, debilitating pain in trans women as there are in trans men. However, that doesn't mean estrogen is without risks.
If you read my post about testosterone in the female body, you would see that testosterone lowers Ki67 levels. Ki67 is the protein that increases as cells prepare to divide. Dangerously low levels (as seen in FTMs) probably mean the cells aren't multiplying at all, leading to atrophy. Dangerously high levels means the cells are multiplying out of control, leading to cancer. Estrogen stimulates Ki67 levels. Estrogen is a known carcinogen.
In this study of 2260 trans women, it was found that the MTFs are 46 times as likely as their unmedicated counterparts to develop breast cancer. However, they were still not as likely to develop breast cancer as females.
The other major risk that stands out is cardiovascular. most pronounced is the increased risk of venous thromboembolism, the definition of which is:
is a condition in which a blood clot forms most often in the deep veins of the leg, groin or arm (known as deep vein thrombosis, DVT) and travels in the circulation, lodging in the lungs (known as pulmonary embolism, PE).
here is a table from this study that I will explain.
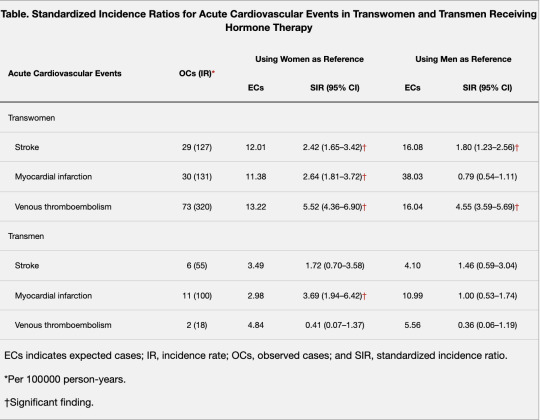
"expected cases" (ECs) means the control group, i.e. the risks of cardiovascular events in undrugged women and men respectively. The standardized incidence ratio, or SIR, is taken by dividing the number of observed cases (OCs) with the number of expected cases. a SIR under 1 means the incidence of a cardiovascular event is lower in trans women than in the control groups. a SIR above 1 means the incidence is increased.
For MTFS, the SIR is comfortably above 1 for both stroke and venous thromboembolism when compared with the male control group. (we can also see that for trans men, the SIR for myocardial infarction (heart attack) is very high, but that's for another post)
That means they are at higher risk for those cardiovascular events.
Now, because trans people are prone at higher incidences to "psychosocial stressors and smoking", synthetic hormones are probably not the only factors in the increased risk of cardiovascular events. But it's safe to say they are a major factor.
This study documents pain in MTF and FTM individuals after they've started cross-sex hormones.
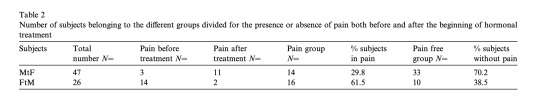
(again, tangent— 61.5 PERCENT FTMS EXPERIENCED CHRONIC PAIN. OVER HALF. )
But MTFS also had a significant rate of chronic pain at 29.8 percent. they reported headaches, "breast" tenderness, and musculoskeletal pain. They also reported that the pain got worse as hormone "treatment" continued. it is also worth noting that testosterone dulls pain, meaning that MTFS on t-blockers and estrogen will be experiencing pain at a level and type that they've never felt before, which I can imagine is alarming. They also tend to be sexually impotent, prone to depression (as T is a mood stabilizer), and can suffer from lethargy, brain fog, and sleep disturbances off T, which can be partially attributed to the diuretic and anti-androgen Spironolactone.
here is a list of side effects of Spironolactone, link here:
(mild)
diarrhea and abdominal cramping
nausea and vomiting
high potassium levels
leg cramps
headache
dizziness
drowsiness
itching
(severe)
Allergic reactions. Symptoms can include:
skin rash
hives
fever
trouble breathing
swelling of your lips, mouth, tongue, or throat
Electrolyte and/or fluid problems. Symptoms can include:
mouth dryness
extreme thirst
extreme weakness and tiredness
fast heart rate and dizziness
not being able to urinate
Dangerously high potassium levels. Symptoms can include:
muscle weakness
not being able to move your legs and arms
extreme tiredness
tingling or numb feeling in your hands or feet
slow heart rate
Breast enlargement (gynecomastia). Symptoms can include:
growth of breast tissue in males and females
Severe skin reactions. Symptoms can include:
redness, blistering, peeling or loosening of your skin, including inside of your mouth.
now, most of these effects probably have low incidence rates, but the sheer number of effects leads me to think—if you're on this drug, there's a good chance you've got a handful of side effects. most of them are relatively harmless and some of them are debilitating.
I would throw in some testimonials from reddit, but r/mtf has recently been privated. It seems they felt it was necessary to have a safe space for males where they could talk about issues that pertain exclusively to them. I wonder why the same measures have not been taken for r/ftm. I wonder.
So, in conclusion, trans women do have an increased risk of cancer, cardiovascular events and chronic pain, and the drugs they take may have a range (a rainbow, even!) of nasty side effects. But chronic pain is nowhere near as guaranteed in trans women as in trans men.
edit: a couple of these studies are behind paywalls. I used sci-hub to access them.
#radfem#radfems do interact#terf safe#medical malpractice#mtf#ftm#hrt#gender critical#gender abolition
125 notes
·
View notes
Text
Btw, these are fucking amazing. Never have to drink gatorade again!!!!! The Salt Sticks company realized a ton of ppl with autonomic dysfunction were using their electrolyte capsules to manage their illness, so they formulated a new kind aimed specifically at chronically ill people and the Vitassium Club mentioned on the label here is a list you can get on by filling out an online form, that will give you 20% off every order of Vitassium. You do not need to give proof of diagnosis to get on the club. All you need to do is tell them "yes I have a chronic illness which I need to manage with electrolyte supplements". They don't need a diagnosis name or a doctor's name. It is self reported. SO SIGN UP!!!!!!!


2K notes
·
View notes
Text
A Guide to Outpatient COVID Treatment: Step-By-Step Doctors’ Plan That Could Save Your Life
Recently, Dr. Peter McCullough, MD, of Baylor University Medical Center in Dallas testified to Texas Senate HHS Committee about how mass media and even some government agencies are silencing clinical outpatient evidence for effective treatment of COVID19 and instead push vaccines only (video shown below).
Treatments like those mentioned by Dr. McCullough can be found in sites like https://c19early.com/ but specifically, McCullough refers to the following Appendix to a document published by Association of American Physicians and Surgeons (AAPSonline.org) as an educational resource. It is based on a paper published in American Journal of Medicine (link), by Dr. Peter McCullough and 22 other clinicians (MDs) and researchers (PhDs).
“Seek early treatment and be your own advocate. All of the physicians contributing to this booklet are on the frontlines treating outpatients at the first signs of COVID illness. Studies in the US and many other countries clearly show that patients who are treated within the first 5 days of symptoms have better outcomes using the combination of medications in the algorithm below.”

COVID-19 hospitalizations and death can be reduced with outpatient treatment.
Principles of COVID-19 outpatient care include: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, 4) antiplatelet/antithrombotic therapy 5) administration of oxygen, monitoring, and telemedicine.
“For the ambulatory patient with recognized early signs and symptoms of COVID-19, often with nasal real-time reverse transcription or oral antigen testing pending, the following 4 principles could be deployed in a layered and escalating manner depending on clinical manifestations of COVID-19-like illness and confirmed infection: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, and 4) antiplatelet/antithrombotic therapy. Because the results of testing could take up to a week to return, treatment can be started before the results are known. For patients with cardinal features of the syndrome (ie, fever, body aches, nasal congestion, loss of taste and smell, etc.) and suspected false-negative testing, treatment can be the same as those with confirmed COVID-19. Future randomized trials are expected to confirm, reject, refine, and expand these principles. In this article, they are set forth in emergency response to the growing pandemic as shown in Figure 1 .
Treatment algorithm for COVID-19-like and confirmed COVID-19 illness in ambulatory patients at home in self-quarantine. BMI = body mass index; CKD = chronic kidney disease; CVD = cardiovascular disease; DM = diabetes mellitus; Dz = disease; HCQ = hydroxychloroquine; Mgt = management; O2 = oxygen; Ox = oximetry; Yr = year.
The basic groups of prescription medicines and other therapies used in COVID-19:
▪ Combination anti-viral medicines started as soon as symptoms occur ▪ Medicines to decrease inflammation, such as corticosteroids (called immunomodulators)
▪ Anticoagulant therapy to prevent blood-clots that can cause strokes, heart attacks, kidney shut-down, and death.
▪ Non-prescription supportive treatments with zinc, vitamin D, vitamin C, electrolyte drinks such as Pedialyte, and others.
▪ Home-based oxygen support, such as with an oxygen concentrator. These machines are available by physician prescription from home health medical supply businesses and are covered on most medical insurance plans.
I. Antiviral Agents:
These must be started quickly at STAGE I (Days 1-5):
Symptoms include sore throat, nasal stuffiness, fatigue, headaches, body aches, loss of taste and/or smell, loss of appetite, nausea, diarrhea, fever.
These medicines stop the virus from (1) entering the cells and (2) from multiplying once inside the cells, and they reduce bacterial invasion in the sinuses and lung:
▪ *Hydroxychloroquine (HCQ) with azithromycin (AZM) or doxycycline
OR
▪ Ivermectin with azithromycin (AZM) or doxycycline
Either combination above must also include zinc sulfate or gluconate, plus supplemental vitamin D, and vitamin C. Some doctors also recommend adding a B complex vitamin.
Zinc is critical. It helps block the virus from multiplying.
Hydroxychloroquine is the carrier taking zinc INTO the cells to do its job.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 16
II. Anti-inflammatory Agents - Corticosteroids (“steroids”): Oral and Nebulized.
These are started at STAGE II (Days 3-14) to reduce inflammation, the cause of added damage to the lungs and critical organs. Symptoms include worsening cough, difficulty breathing, chest heaviness/tightness or chest pain.
As inflammation damages the airways interfering with normal oxygen-carbon dioxide exchange, blood oxygen levels drop and people experience loss of focus, drowsiness, confusion, difficulty concentrating, low energy and severe fatigue.
The exaggerated Inflammation response in COVID further increases the risk of blood clots.
Prescription medicines and other support added now to Stage I medicines are: ▪ nebulized budesonide to help penetrate the lungs and reduce inflammation ▪ oral prednisone, methylprednisolone, dexamethasone
▪ colchicine – may also be added to reduce inflammation
▪ full strength adult aspirin 325 mg to reduce inflammation and risk of blood clots ▪ home oxygen concentrator may be needed to improve oxygen levels (requires physician prescription)
III. Prescription Anticoagulants (“blood thinners”):
STAGE III (Day 7 and beyond): Symptoms seen in Stage II intensify. Difficulty breathing becomes extreme, oxygen levels drop sharply, risk of heart attack or stroke increases. At this point, people are critically ill.
The medicines to be added to Stage I and II medicines now include:
▪ Aspirin 325 mg unless told not to take by your doctors
▪ And/or low molecular weight heparin injections (e.g. enoxaparin [Lovenox]) OR
▪ apixaban (Eliquis), or rivaroxaban (Xarelto), or dabigatran (Pradaxa) or
edoxaban (Savaysa) in standard doses for 5 to 30 days
If these added steps do not lead to improvement, or the patient becomes unstable, a 911 call is warranted for ER evaluation and hospital admission so that more aggressive IV medications (such as remdesivir, Regeneron, and others) may be considered, and more intensive ventilation regimens are possible in ICU settings.
IV. Vitamins, Supplements, and Oxygen.
▪ Zinc sulfate, gluconate or citrate. These forms are available in pharmacies, health food stores, and sold online. Zinc sulfate 220 mg provides 50 mg elemental zinc, the recommended anti-viral dose. Zinc in the form of zinc picolinate form is not recommended following reports of liver damage and tumors from studies about 20 years ago. Following these reports, the German Commission E that regulates supplements used in medical practice in Germany banned this form of zinc.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 17
▪ Vitamin D3, preferable in oil in capsules for better absorption. Recommended doses for anti-viral benefit vary from 5000 IU or more for 5-30 days
▪ Vitamin C with bioflavonoids for antioxidant, anti-inflammatory effects. Dose
recommendations from our contributors vary from 1000 mg (1 gram) once or twice a day up to 4 or more times a day.
▪ A word about quercetin. Some physicians are recommending this supplement to reduce viral illnesses because quercetin acts as a zinc ionophore to improve zinc
uptake into cells. It is much less potent than HCQ as a zinc transporter, and it does
not reach high concentrations in lung cells that HCQ does. Quercetin may help
reduce risk of viral illness if you are basically healthy. But it is not potent enough to replace HCQ for treatment of COVID once you have symptoms, and it does not
adequately get into lung tissue unless you take massive doses (3-5 grams a day),
which cause significant GI side effects such as diarrhea.
Control of Contagion
A major goal of self-quarantine is the control of contagion. Many sources of information suggest the main place of viral transmission occurs in the home. Facial covering for all contacts within the home as well as frequent use of hand sanitizer and hand washing is mandatory. Sterilizing surfaces such as countertops, door handles, phones, and other devices is advised. When possible, other close contacts can move out of the domicile and temporarily stay with others not ill with SARS-CoV-2. Findings from multiple studies indicate that policies concerning control of the spread of SARS-CoV-2 are effective and extension into the home as the most frequent site of viral transfer is paramount.
Reduction of Self-Reinoculation
It is well-recognized that COVID-19 exists outside the human body in a bioaerosol of airborne particles and droplets. Because exhaled air in an infected person is considered to be “loaded” with inoculum, each exhalation and inhalation is effectively reinoculation. In patients who are hospitalized, negative pressure is applied to the room air largely to reduce spread outside of the room. We propose that fresh air could reduce reinoculation and potentially reduce the severity of illness and possibly reduce household spread during quarantine. This calls for open windows, fans for aeration, or spending long periods of time outdoors away from others with no face covering to disperse and not reinhale the viral bioaerosol.
Combination Antiviral Therapy
Rapid and amplified viral replication is the hallmark of most acute viral infections. By reducing the rate, quantity, or duration of viral replication, the degree of direct viral injury to the respiratory epithelium, vasculature, and organs may be lessened. Additionally, secondary processes that depend on viral stimulation, including the activation of inflammatory cells, cytokines, and coagulation, could potentially be lessened if viral replication is attenuated. Because no form of readily available medication has been designed specifically to inhibit SARS-CoV-2 replication, 2 or more of the nonspecific agents listed here can be entertained. None of the approaches listed have specific regulatory approved advertising labels for their manufacturers; thus all would be appropriately considered acceptable “off-label” use.
Zinc Lozenges and Zinc Sulfate
Zinc is a known inhibitor of coronavirus replication. Clinical trials of zinc lozenges in the common cold have demonstrated modest reductions in the duration and or severity of symptoms. By extension, this readily available nontoxic therapy could be deployed at the first signs of COVID-19. Zinc lozenges can be administered 5 times a day for up to 5 days and extended if needed if symptoms persist. The amount of elemental zinc lozenges is <25% of that in a single 220-mg zinc sulfate daily tablet. This dose of zinc sulfate has been effectively used in combination with antimalarials in early treatment of high-risk outpatients with COVID-19.
Antimalarials
Hydroxychloroquine (HCQ) is an antimalarial/anti-inflammatory drug that impairs endosomal transfer of virions within human cells. HCQ is also a zinc ionophore that conveys zinc intracellularly to block the SARS-CoV-2 RNA-dependent RNA polymerase, which is the core enzyme of the virus replication. The currently completed retrospective studies and randomized trials have generally shown these findings: 1) when started late in the hospital course and for short durations of time, antimalarials appear to be ineffective, 2) when started earlier in the hospital course, for progressively longer durations and in outpatients, antimalarials may reduce the progression of disease, prevent hospitalization, and are associated with reduced mortality. In a retrospective inpatient study of 2541 patients hospitalized with COVID-19, therapy associated with an adjusted reduction in mortality was HCQ alone (hazard ratio [HR] = 0.34, 95% confidence interval [CI] 0.25-0.46, P <0.001) and HCQ with azithromycin (HR = 0.29, 95% CI 0.22-0.40, P <0.001). HCQ was approved by the US Food and Drug Administration in 1955, has been used by hundreds of millions of people worldwide since then, is sold over the counter in many countries, and has a well-characterized safety profile that should not raise undue alarm. Although asymptomatic QT prolongation is a well-recognized and infrequent (<1%) complication of HCQ, it is possible that in the setting of acute illness symptomatic arrhythmias could develop. Data safety and monitoring boards have not declared safety concerns in any clinical trial published to date. Rare patients with a personal or family history of prolonged QT syndrome and those on additional QT prolonging, contraindicated drugs (eg, dofetilide, sotalol) should be treated with caution and a plan to monitor the QTc in the ambulatory setting. A typical HCQ regimen is 200 mg bid for 5 days and extended to 30 days for continued symptoms. A minimal sufficient dose of HCQ should be used, because in excessive doses the drug can interfere with early immune response to the virus.
Azithromycin
Azithromycin is a commonly used macrolide antibiotic that has antiviral properties mainly attributed to reduced endosomal transfer of virions as well as established anti-inflammatory effects. It has been commonly used in COVID-19 studies initially based on French reports demonstrating markedly reduced durations of viral shedding, fewer hospitalizations, and reduced mortality combination with HCQ as compared to those untreated. In the large inpatient study (n = 2451) discussed previously, those who received azithromycin alone had an adjusted HR for mortality of 1.05, 95% CI 0.68-1.62, and P = 0.83.23 The combination of HCQ and azithromycin has been used as standard of care in other contexts as a standard of care in more than 300,000 older adults with multiple comorbidities. This agent is well-tolerated and like HCQ can prolong the QTc in <1% of patients. The same safety precautions for HCQ listed previously could be extended to azithromycin with or without HCQ. Azithromycin provides additional coverage of bacterial upper respiratory pathogens that could potentially play a role in concurrent or secondary infection. Thus, this agent can serve as a safety net for patients with COVID-19 against clinical failure of the bacterial component of community-acquired pneumonia. The same safety precautions for HCQ could be extended to azithromycin with or without HCQ. Because both HCQ and azithromycin have small but potentially additive risks of QTc prolongation, patients with known or suspected arrhythmias or taking contraindicated medications or should have more thorough workup (eg, review of baseline electrocardiogram, imaging studies, etc.) before receiving these 2 together. One of many dosing schemes is 250 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection.
Doxycycline
Doxycycline is another common antibiotic with multiple intracellular effects that may reduce viral replication, cellular damage, and expression of inflammatory factors. This drug has no effect on cardiac conduction and has the main caveat of gastrointestinal upset and esophagitis. As with azithromycin, doxycycline has the advantage of offering antibacterial coverage for superimposed bacterial infection in the upper respiratory tract. Doxycycline has a high degree of activity against many common respiratory pathogens including Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, anaerobes such as Bacteroides and anaerobic/microaerophilic streptococci and atypical agents like Legionella, Mycoplasma pneumoniae, and Chlamydia pneumoniae. One of many dosing schemes is 200 mg po followed by 100 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection. Doxycycline may be useful with HCQ for patients in whom the HCQ-azithromycin combination is not desired.
Favipiravir
Favipiravir, an oral selective inhibitor of RNA-dependent RNA polymerase, is approved for ambulatory use in COVID-19 in Russia, India, and other countries outside of the United States.35 It has been previously used for treatment of some life-threatening infections such as Ebola virus, Lassa virus, and rabies. Its therapeutic efficacy has been proven in these diseases. Like, the antimalarials and antibiotics, favipiravir has no large-scale randomized trials completed at this time, given the short time frame of the pandemic. A dose administration could be 1600 mg po bid on day 1, following by 600 mg po bid for 14 days.
Immunomodulators
The manifestations of COVID-19 that prompt hospitalization and that may well lead to multiorgan system failure are attributed to a cytokine storm. The characteristic profile of a patient acutely ill with COVID-19 includes leukocytosis with a relative neutropenia. These patients have higher serum level of cytokines (ie, TNF-α, IFN-γ, IL-1β, IL-2, IL-4, IL-6, and IL-10) and C-reactive protein than control individuals. Among patients with COVID-19, serum IL-6 and IL-10 levels appear even more elevated in the critically ill. As with any acute inflammatory state, early treatment with immunomodulators is expected to impart greater benefit. In COVID-19, some of the first respiratory findings are nasal congestion, cough, and wheezing. These features are due to excess inflammation and cytokine activation. Early use of corticosteroids is a rational intervention for patients with COVID-19 with these features as they would be in acute asthma or reactive airways disease. The RECOVERY trial randomized 6425 hospitalized patients with COVID-19 in a 2:1 ratio to dexamethasone 6 mg po/IV daily for up to 10 days and found dexamethasone reduced mortality (HR = 0.65, 95% CI 0.51-0.82, P <0.001). One potential dosing scheme for outpatients starting on day 5 or the onset of respiratory symptoms is prednisone 1 mg/kg given daily for 5 days with or without a subsequent taper.
Colchicine
Colchicine is a nonsteroidal antimitotic drug that blocks metaphase by binding to the ends of microtubules to prevent the elongation of the microtubule polymer. This agent has proven useful in gout and idiopathic recurrent pericarditis. The GRECCO-19 randomized open-label trial in 105 hospitalized patients with COVID-19 found that colchicine was associated with a reduction in D-dimer levels and improved clinical outcomes. The clinical primary end point (2-point change in World Health Organization ordinal scale) occurred in 14.0% in the control group (7 of 50 patients) and 1.8% in the colchicine group (1 of 55 patients) (odds ratio, 0.11; 95% CI, 0.01-0.96; P = 0.02). Because the short-term safety profile is well understood, it is reasonable to consider this agent along with corticosteroids in an attempt to reduce the effects of cytokine storm. A dosing scheme of 1.2 mg po, followed by 0.6 mg po bid for 3 weeks can be considered.
Antiplatelet Agents and Antithrombotics
Multiple studies have described increased rates of pathological macro- and micro-thrombosis. Patients with COVID-19 have described chest heaviness associated with desaturation that suggests the possibility of pulmonary thrombosis. Multiple reports have described elevated D-dimer levels in acutely ill patients with COVID-19, which has been consistently associated with increased risk of deep venous thrombosis and pulmonary embolism. Necropsy studies have described pulmonary microthrombosis in COVID-19. These observations support the notion that endothelial injury and thrombosis play a role oxygen desaturation, a cardinal reason for hospitalization and supportive care. Based on this pathophysiologic rationale, aspirin 81 mg daily can be administered as an initial antiplatelet and anti-inflammatory agent. Ambulatory patients can be additionally treated with subcutaneous low-molecular-weight heparin or with short-acting novel anticoagulant drugs in dosing schemes similar to those use in outpatient thromboprophylaxis. In a retrospective study of 2773 inpatients with COVID-19, 28% received anticoagulant therapy within 2 days of admission, and despite being used in more severe cases, anticoagulant administration was associated with a reduction in mortality (HR = 0.86 per day of therapy, 95% CI: 0.82-0.89; P <0.001). Additional supportive data on the use anticoagulants reducing mortality has been reported in hospitalized patients with elevated D-dimer levels and higher comorbidity scores.53 Many acutely ill outpatients also have general indications for venous thromboembolism prophylaxis applicable to COVID-19.
Delivery of Oxygen and Monitoring
Because ambulatory centers and clinics have been reticent to have face-to-face visits with patients with COVID-19, telemedicine is a reasonable platform for monitoring. Clinical impressions can be gained with audio and video interviews by the physician with the patient. Supplemental information, including vital signs and symptoms, will be important to guide the physician. A significant component of safe outpatient management is maintenance of arterial oxygen saturation on room air or prescribed home oxygen under direct supervision by daily telemedicine with escalation to hospitalization for assisted ventilation if needed. Self-proning could be entertained for confident patients with good at-home monitoring.
Many of the measures discussed in this article could be extended to seniors in COVID-19 treatment units in nursing homes and other nonhospital settings. This would leave the purposes of hospitalization to the administration of intravenous fluid and parenteral medication, assisted pressure or mechanical ventilation, and advanced mechanical circulatory support.”
youtube
This is the group’s statement on vaccines:
“Vaccines in Development:
Several vaccine models are being investigated for SARS-CoV-2 (COVID-19) including DNA and RNA vaccines. These vaccines take genetic information from other sources that is introduced into the cells. This information includes instructions to produce a SARS2-like viral antigen itself, and the immune system then reacts to it to develop immunity to the virus.
The most important consideration before approving a vaccine for human use is to make sure that the vaccine is safe and effective. Developing safe and controlled infection models for humans normally takes many years of phased testing in the lab and then in humans. Many physicians and scientists have been concerned that vaccine manufacturers, with government support, are speeding up this process in ways that are not allowing adequate time for the usual phased testing leading up to human clinical trials. Two vaccine manufacturers already have voluntarily paused their clinical trials in people due to serious adverse events.
Currently, there are no RNA-based vaccines approved for human use so it would seem prudent to take the time needed to ensure safety. Vaccines for RNA viruses are notoriously challenging and difficult to develop. We still, after all these years since AIDS emerged in the 1980s, do not have a vaccine for the AIDS virus, or the SARS-1 coronavirus that emerged in 2002-2003, and both are RNA viruses.
Several attempts have been made to create vaccines for coronavirus and other respiratory viruses but none of the vaccines have survived the testing phases. The vaccine trials for SARS-1 from 2003, for example, was shut down because it produced autoimmune hypersensitivity reactions when exposed to the natural virus after immunization in animal studies.
Another problem is that the SARS-2 virus has already shown many mutations. Viruses adapt to the environment to survive. Like the flu virus, it is difficult to predict what mutations will occur and circulate around the world each season. A new vaccine must be reformulated to adjust to the changing genetic makeup of the SARS-2 virus.
Even the best vaccines for flu are only about 30-60% effective. Compare that with an effectiveness for improvement ranging from 64% to more than 90% in more than 100 new studies showing early, outpatient treatment with our existing medications described in chapters.
As research on the vaccine continues, safety and effectiveness are of primary concern. The good news is there are very safe and effective early treatments already available as we described in Chapter 3. Clearly, early, home-based treatment has now been so successful and offers so much hope, there is less urgency to have a vaccine.”
You can sign up to receive the full protocol here: https://aapsonline.org/covidpatientguide/ or find the research paper here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7410805/
5 notes
·
View notes
Text
The Pennywise Saga: Purging, Presents, and Predictable
TRIGGER WARNING: Discussion of disordered eating, and eating disorders.
Well, I figured things would go moderately smoothly because it was the first meeting in 8/9 months. And it did. We were kind, grey rocked, and they were kind. The restaurant we ended up going to didn't have any really healthy options, it was unfortunate, but that was my fault. It was me who chose it because it was the first one that came to mind.
Pennywise suffers from an eating disorder. We all know it. She eats a quarter of a meal, and sends it back. Hides food in her napkin. Plays with her food. Sends it back for too much dressing. She constantly berates the waitress, or tells the waitress to talk to the chef about what's wrong with the meal.
I've been doing Intermittent Fasting. I've lost 75lbs. I've been very mindful of my eating, but I've also gone overboard at many points. Fasting for 20 days straight (still taking vitamins, supplements, electrolytes, only drinking black coffee, water, and green tea). It took telling my doctor telling me that I may end up with hair loss for me to stop. My hair is the only thing I truly think is beautiful about me. It's the one thing Pennywise has always loved, too. Despite it being an auburn during the winter, and a ginger tone during the summer months – she had dyed my hair dark brown since I was nine or so to make me look more like the rest of the family. It took until I was 29 or so to stop the habit.
I carried on like this though and still have been doing this. Restricting harder and harder, fasting for 3-5 days twice a month, and even purging. Eating 300 calories or less a day. Exercising excessively despite my bad ankle (more metal than bone). Wearing a brace so that I can get in 20,000 steps. Now with the brown recluse bite on my upper, inner thigh, I've taken some time off, so as not to irritate the area (at my doctor's advice). Anyway, some doctors say that disordered eating is hereditary in a way. Monkey see, monkey do, I guess. I struggle with it immensely.
I've lost 75lbs / 34kg since mid-December. I quit drinking, ordering out, and did all the above. I was actually kind of excited to show off my weight loss, because she would be... proud. It's weird how the brain, despite knowing, despite being told that she's a narc, despite years of mistreatment, or buying 'goal clothes' for me for every birthday and Christmas ever since I was nine or so. If you don't know what 'goal clothes' are, they're clothes that are sizes too small so that you have to lose weight to fit into them. The only thing that ever fit me was shoes. However, she knew that I'd lost 75lbs, as I was rather proud of that fact, and had texted her about it. She couldn't respond because I had and still have all their numbers blocked, but I wanted to brag a little.
First comment when Pennywise saw me was,
"You look the same as when we saw you last time. I thought you said you lost weight."
It crushed me instantly.
We just continued on, I said nothing, smiled through it, and said our hellos. And of course, in the way my family does, we did our one-armed hugs (and air kisses to the one cheek for the women) -- we have very strict conduct of how we touch one another in our family. We stood our ground and did not allow either of them into the house. Pennywise did ask why she couldn't wait in the house, despite the rules being laid out in plain English the day before. I wouldn't have let her in even if she had to pee. I'd have let her piss herself before I let her in our home. We gave them their Christmas presents, and they gave us ours to take home later on, and headed to the restaurant.
When the waitress came, we all ordered. Pennywise asked for the fries that came with her meal to be put on a separate plate. Only… she didn't. Four times in a row, she asked for gravy to be put on a separate plate. When the waitress looked confused and asked,
"You want gravy on the side?" Pennywise looked confused and my father had to say,
"She means fries. She wants her fries on a separate plate."
Pennywise looking confused, countered with,
"That's what I said."
We all looked at her and shook our heads. She still looked confused, but the waitress accepted it, and we carried on. Perhaps Pennywise is starting to... I don't know. It was almost like a moment of aphasia.
In typical habit, I ordered knowing Pennywise would be watching what I ate. I ordered the 'Lunch Rush' without the soup, just the small salad and half a sandwich.
Only, she didn't watch what I ate.
Today, for the first time in my ENTIRE life (and the ENTIRE time that my husband has known her), she didn't send her food back, hide it in her napkin, and nearly finished everything on her plate. When we got home, I commented on how she actually ate. And even my husband noticed that she actually ate.
It was… Intriguing to watch. To see her actually eat. I know that sounds strange, but after so many years of watching her disordered eating -- it was just... kind of mind-blowing. She didn't watch what I ate. AND she ate. It was... a little confusing and intriguing to BE the one watching instead of being watched.
Then Pennywise discussed how her surgery was coming up, and discussed the nitty-gritty details of it. She spoke while we listened, and that was that.
Of course, she opened her Christmas present when we got back to the car. I got her handmade moccasins from the Native reservation because she always buys herself new ones from a store in the mall. I thought she'd appreciate the real thing.
The beautiful handmade moccasins I got her from the reservation didn't fit – but I expected that – I got them in my size and for myself (she insists we're the same size - we're not). Nothing I buy her is ever good enough anyway, so I simply planned ahead this time. They wouldn't fit her, or she wouldn't like them, and I'd have to return them. Call me selfish if you want, but she's returned every gift I've gotten her since… well, honestly, I can't remember the last time I got her a gift she kept. So this time, I just planned ahead.
We left after giving them directions, doing our one-armed hugs, and went our own ways. It's not that exciting of a story. I think that Pennywise is suffering from the early signs of dementia. I don’t know how I feel about that. I feel despair. I feel anger that she’ll never remember all the horrible things she did to me. That she’ll never apologize. That her first words to me were to mock my weight despite being 75lbs lighter. I feel sad. I feel some weird form of elation -- that maybe she’ll forget me entirely, and I won’t have to worry about her anymore. Sympathy that she’s got cancer, and clearly showing the signs of dementia. My heart is breaking, and yet... I don’t know. I don’t know HOW to feel. I’m crying as I write this last part out because the emotions are so confusing. I always wished she would just disappear. That my troubles would... go away and distancing myself from my family made my troubles fade. But the fact that she’s actually fading away. That she may not make it through this... I feel... Confused. Broken. Validated. Vindictive. Heartbroken. It was like I made a wish, and it... came true, in the worst way possible. I wouldn’t wish this on my worst enemy or critic, and Pennywise is both of those things. This is not closure. This is not... a happy ending. This is just... an ending, in a way. It’s not over yet, and I’m over-analytical and hypervigilant from years of abuse and protecting myself. I’m still working out my feelings and they are just -gestures vaguely- all over the place. I don’t know how I should feel. When I first found out she had cancer, I just felt... numb. I felt like I should care more. But seeing her face-to-face, and seeing her fading away. Only a glimpse of the woman she’s always been at the beginning of her visit, before she became docile and suffered aphasia with her speech. It... broke me. In a way I can’t explain. Today has been an awful day, really. My emotions are... everywhere, and I can’t grasp any one feeling for long before it morphs into something else.
#intermittent fasting#intermittent fast#intermittent#fasting#fast#raised by narcissists#narcissists#narcissist#narc#aphasia#dementia#confused#feelings#don't understand#rude#sad#emotional#pennywise#the pennywise saga
3 notes
·
View notes
Text
Peptide Chemistry
The Power Of Peptides The Current Fad In Advanced Skincare.
Content
Dpc10 Peptide
Sarma For Mass Is A Conditioner That Assists Build Up The Muscles.
Ostarine (mk.
A Bluffers Overview To 2 Of Skin Cares Most Powerful Energetic Ingredients.
This last method is an attempt to minimize the possibilities of detection, while the benefit to the biker's efficiency lingers. The medical uses AAS are focused on treatment of glandular or endocrine conditions, consisting of disease of the adrenal glands and weakening of bones in females. direct-peptides’s free Belgium peptides best buy can be treated with a testosterone by-product as replacement therapy following healing from testicular cancer cells. MOST LIKELY one of the most notorious team of representatives used by professional athletes, these are a mix of synthetic and also normally taking place representatives, which have a variety of intricate physiological impacts. These can be very severe indeed and also usually relate to dose and duration of use.
For example vacuuming the rugs for 20 mins will melt virtually 100 calories as well as reducing the grass about 150 calories. So don't forget the importance of this sort of workout as well as if you are not very good at doing the chores then perhaps currently is the moment to make a resolution to provide more interest.
Are Peptides good for hair?
Peptides, being “smaller proteins,” when applied, cause changes in cell behavior, stimulate follicle growth, and promote natural hair production and improvement of hair color.
Generally, stimulants have a reasonably short period of action, once more largely dependent upon their path of administration. As an example, a dosage or 'hit' of cocaine will produce its maximum results in mins, which begin to disappear after around 20 mins. Amphetamine, specifically if absorbed tablet form, has a much longer-lasting effect, individuals typically really feeling 'wired' or unnaturally sharp several hours later on. Energizers do not require to be taken chronically before an event, and have generally instant effects.
Dpc10 Peptide
These medications are meant to be utilized as a future substitute for testosterone, which can have many different adverse effects as well as threaten at high dosages. The majority of the study on SARMs remains in animal versions as well as even after that some rather severe side effects have been kept in mind-- despite the intent for SARMs to prevent the adverse facets of testosterone use.
Yet even after a number of days, I began to understand that my "hunger" was a signs and symptom of regular. Nutrition practices come to be deep-rooted and also we accumulate an internal narrative; "I can not function effectively without morning meal", "I need a coffee to start my day", "If I avoid lunch I obtain a mid-afternoon time-out". I enjoy food and also consume a lot of it, so the suggestion of taking in nothing for 72 hrs was intimidating.
Sarma For Mass Is A Conditioner That Aids Develop The Muscles.
These representatives are relatively brand-new on the biking scene, with EPO particularly having actually received much limelights over the last few years. All of the examples provided here are produced as fabricated alternative to hormonal agents that occur normally in the body. They as a result mimic the activity of these hormones in managing a variety of essential physical procedures.
Collagen Peptides Market 2021-2026 In-Depth Analysis on Key Trends, Leading Players & Revolutionary Opportunities - SoccerNurds
Collagen Peptides Market 2021-2026 In-Depth Analysis on Key Trends, Leading Players & Revolutionary Opportunities.
Posted: Fri, 08 Jan 2021 11:59:28 GMT [source]
Nonetheless, they still do not seem only particular to the target receptors, and also unintended biding to exterior receptors is still noticeable. Specifically, SARMs are produced to attach to receptors in skeletal muscle and also bone to trigger pathways associated with skeletal muscle hypertrophy and bone regeneration. SARMs were originally established to deal with some serious usual issues that occur with the senior clients when their testosterone levels start to naturally decline as well as they end up being vulnerable to sarcopenia as well as osteoporosis.
However, controlled drugs such as amphetamine and drug are typically constantly mistreated and this can result in dependancy. Right here is a succinct as well as insightful account of the significant medicine courses in common use. The scenario is intensified further by prevalent co-administration of 'masking representatives'.
Ostarine (mk.
This indicates that they have to all be provided by injection, typically right into a muscle or under the skin. IGF-1, so far, has no genuine medical uses and appears to function directly at the degree of tissues, where it stimulates a rise in healthy protein synthesis as well as fat metabolism. EPO mimics an all-natural procedure, w here the release of the body's very own hormone from the kidney is boosted in action to an autumn in the amount of oxygen carried in the blood. As an example, this may be caused by ascending swiftly to a high altitude or as a result of too much blood loss.
youtube
As they are proclaimed as a steroid choice without the side effects, it is not unusual how their appeal is quickly expanding. Such a medication might hypothetically serve at replacing testosterone usage in medical settings, which comes with several damaging adverse effects.
A Bluffers Guide To 2 Of Skin Cares Most Effective Active Ingredients.
The chances of estrogen-related sides and water retention are dramatically reduced, as well. Just as with AAS, stacking prevails with peptide hormones; competitors frequently blend and also match a cocktail of representatives. During an occasion they may additionally supplement this routine with a stimulant. EPO creates a rapid increase in haematocrit (occasionally as much as 60 per cent; normal variety per cent), with measurable rises still apparent 4 months complying with withdrawal of the medicine. This is because new members cells have a lifetime of around 120 days. Nevertheless, the pattern of management taken on by somebody seeking performance-enhancing benefits indicates that the degree of the medication in the blood is practically regularly elevated. This implies that they are damaged down by the acids in the belly, in much the same means as proteins in food throughout food digestion.
In contrast, the 'polar zipper' device refers to hydrogen bonding interactions in between the amino acid side chains on surrounding beta strands.
As a result, allowed ɸ values will be relatively restricted compared to various other amino acids.
In 2019 Vapourtec developed a collaboration in the direction of peptide synthesis with Professor Peter Seeberger as well as his Group at Max Plank Institute, Berlin.
This job has actually been released in the paper revealed instantly below.
The side-chain of proline is covalently bonded to the N of the amino team, so in polyproline, there will certainly be less freedom of turning about the Cα-- N bond than with other amino acids.
In overdose as well as most particularly when a rival has actually come to be dried, physical adverse effects can be harmful. Hyperthermia complying with amphetamine ingestion probably killed Tom Simpson on Mont Ventoux in 1967. Some evidence recommends that chronic stimulant misuse was a contributing consider the death of 1998 Scenic tour de France victor Marco Pantani.
Have a look at our recommendations sheet on Diet for concepts concerning exactly how diet regimen can assist your recuperation. Action pedometers can be bought for around ₤ 15 on Amazon.com, in camping stores like Blacks or from the BHF On-line Store. The inquiry that often occurs is just how much workout should we do? The NHS advises concerning 150 minutes or 2 as well as a half hours of moderately intense workout each week for grownups. In theory individuals taking antipsychotics ought to go for greater than this as they need to offset this additional threat element. One sort of workout that is commonly underestimated is basic activity such as home duties and caring for the garden.
Day one was the hardest-- by 5pm I had a cracking headache, regardless of drinking around six litres of water; I assume it went to the very least partly to caffeine withdrawal. A person suggested consuming a mineral-rich salt option such as Himalayan salt, which replaces the electrolytes cleared out of your body; whether it was a placebo effect or not, the headache soon went away. There's absolutely nothing wrong with hostile weight reduction, but reduced-- or in this situation no-- calorie diets are absolutely not lasting as well as ought to kept an eye on closely. If you are thinking of improving the amount of exercise you are obtaining then it may be a good time to think about enhancing your diet too.
SARMs have comparable effects to low doses of testosterone, however to a lesser degree. An additional among the primary advantages of SARMS is that, unlike testosterone, a lot of them do not get converted into 5α-DHT. On top of that, they do not show up to undertake aromatization right into estrogen which might decrease the occurrence of negative effects such as gynecomastia. At the very least in animal research studies, SARMs have actually shown to partly accomplish this, with compounds such as S1 as well as S4 binding to androgen receptors with high affinity and also demonstrating tissue selectivity.
Peptide-based Cardiovascular Therapeutics Market 2021 The demand for the Market will Drastically Increase In The Future - KSU The Sentinel Newspaper
Peptide-based Cardiovascular Therapeutics Market 2021 The demand for the Market will Drastically Increase In The Future.
Posted: Fri, 08 Jan 2021 09:59:15 GMT [source]
SARMs are a reduced term for careful androgen receptor modulators. To sum up, there are countless advantages you can receive from utilizing RAD140. In order to attain also far better results, experts recommend using RAD alongside various other supplements. It doesn't matter if you make use of supplements or go the all-natural way, the most crucial thing is you're keeping fit. Enhancing muscles is not constantly mosting likely to be easy as well as there is no harm in looking for assistance. Ibutamorenis non-hormonal as well as consequently requires no PCT after the cycle mores than. It is finest made use of in a minimum of a 3 month cycle with dosage raising every month.
Huge doses of caffeine can generate convulsions and stress and anxiety assaults. More seriously, long-lasting amphetamine as well as cocaine usage often causes dependency and also dependancy.
These can assist the professional athlete in escaping detection during regular or check, generally by raising the rate at which the medicine are eliminated from the body. It struck me that our mindset towards nutrition is governed as much by practice as by cravings. We drift through much of our life on auto-pilot, consuming when we generally consume. Norway peptides best buy from direct peptides anticipate picking up breakfast at my neighborhood coffeehouse, and also I was constantly "starving" when I arrived.
Considered that these agents really change exactly how a whole variety of genetics work, it's probably not shocking that the prospective adverse effects from lasting AAS use are considerable and also major. This indicates that lasting users go to much greater threat of experiencing a cardiac arrest or stroke. Unlike stimulants, AAS are taken constantly since they do not have instant medicinal results. They need to be taken over a fairly extended period in order to create substantial impacts on efficiency. Usually, a considerably raising dosage of several AAS is taken several months prior to competition-- a process referred to as 'stacking'-- with a reduction in dosage a month or 2 before an event.
The optimum dosing time for MK 677 goes to night straight before going to sleep. This is a non-peptidic, orally active and also selective agonist of the growth hormonal agent secretagogue (secretion-boosting) receptor. It simulates the action of ghrelin in the stomach, raising growth hormone and also IGF-1 levels, yet does not influence cortisol levels. LGD 4033 a SARM like Ostarine but 12 times as effective at just 1/3 the dose! SARMs are harmless to the liver and have little impact on blood pressure. This eliminates the requirement for preloading and on-cycle support supplements. Consequently, a SARM cycle will inevitably be more economical than a traditional AAS/PH (steroid/prohormone) cycle.
#buy peptides direct eu#buy peptides direct europe#eu peptides best buy#europe peptides best buy#buy best quality peptides direct eu#buy best quality peptides direct europe
1 note
·
View note
Note
I have a chronic illness in which makes me bruise so easy, three things my doc has recommended for bruise relief is 1. Heat compress or even soaking in a warm bath, that helps with blood circulation which helps already formed bruises to break down. 2. Vitamin C since it’s anti-inflammatory, either take supplements or eat Vitamin C rich veggies and fruit. 3. Pineapple, it has anti inflammatory enzymes in it.
Of course things could be different for different people and I’m not a doctor so obviously this is just stuff that I do. Please don’t do anything that makes you uncomfortable before talking to a real doctor. Wishing you all the best and hopefully some relief!!!!
Oh my goodness, thank you so much for this! I’m sorry you bruise easily, that must be a pain. My doctor knows about my condition and we’re working on finding a solution, but for now I just kind of randomly lose consciousness lol. It’s all good though, during the day my brother and his fiance stay with me just in case, and I always load up on electrolytes before driving! Again, thank you so much for this, I’m going to try out as many of these as I can.
1 note
·
View note
Text
As all of you know if you don’t know by now I have a connective tissue disorder called Ehlers Danlos syndrome. I myself have referred to it as the “junk drawer disorder” due to the long list of comorbidities or conditions you can have a long with the primary condition. The definition of Comorbidity noun or plural noun: comorbidities Is the simultaneous presence of two chronic diseases or conditions in a patient.
When I discuss my medical issues many times it’s actually these “comorbidities” I am talking about. Although the majority of my medical issues can be explained by my genetic disease called Ehlers Danlos Syndrome. The majority of the time when I discuss my medical issues I get the looks of disbelief or some have even asked “do you really have all these problems?” The answer to that is simple, it’s yes!
So I decided I’ll list only the comorbidities that I have confirmed diagnoses (dxd) of. During the next couple of months I will discuss these medical problems in more detail.
These are not in any specific order. The list is a Semi-common Comorbidities (Unofficial) list. It's how the article labels it and I think it’s smart to label it this way. Mainly because there currently isn’t any statistics, how common these comorbidities are among EDS patients. The original list can be found at the website at the bottom of this post.
FELLOW ZEBRAS I’d like your input on anything you see that you also experience or have been diagnosed with.
~ Chronic Pain * dxd neuropathy*, neuralgia Myofascial Pain Syndrome* ACNES
~Fibromyalgia*
~Mood disorders dxd Anxiety*, PTSD*, Major Depressive Disorder*
~ irritable bowel syndrome IBS*
~Incontinence* at any age (often from occult tethered cord and/or MCAD or allergy induced) only experienced not diagnosed
~Uterine or rectal prolapse, pelvic floor dysfunction*
~Frequent (seemingly idiopathic) nausea and vomiting (may be from impinged vagus nerve/MCAD/hiatal hernia/gastroparesis/Chiari)
~ Arthritis of all kinds, Osteoarthritis* in the spine, neck and hands, but RA common especially early onset
~ Insomnia* also referred to as “painsomnia”(trouble falling and staying asleep, multiple causes in the EDS patient including pain and hyperadrenergic)
~ Hypotonia (unusually weak muscles despite “training” or physical therapy)
~Dizziness* (with or without syncope)
~Thyroid issues (high and low, often auto-immune despite normal TSH “levels For me Hyperparathyroidism*
~Deviated septum
~Chronic and recurrent sinus infections and sinusitis* (allergy shots have helped this)
~Frequent joint dislocations and subluxations (partial dislocations) or being so-called “double-jointed“ bracing is helping
~ PCOS and menorrhagia (very heavy periods)
~Tendonitis* and bursitis* of all kinds (aka “soft tissue rheumatism”, alt. tendinitis)
~Varicose veins* and spider veins, often early onset, easy bruising*
~Migraines* and headaches of ALL kinds and durations, (often driven by hydrocephalus from MCAD)
~ Strokes* (I had a TIA 2012)
~Mitral valve prolapse* (mine is mild)
~Easy bruising* often from no apparent cause or injury
~GERD* (weak hiatal sphincters and MCAD can contribute here – the stomach produces acid in response to histamine from food reactions)
~Gastroparesis* (slow or no stomach emptying) and dysmotility (poor digestive movement) beyond just constipation and IBS, possibly from impinged nerves & vessels
~Sciatica* (VA lists this as SI Joint Dysfunction
~Bilateral hip dysplasia* (sometimes seen at birth, and later) ability to “pop” – aka sublux – hips out and back in easily, which should be avoided!)
~Malabsorption and malnutrition* and nutritional deficiencies despite diet and even supplementation sometimes. (Poor absorption).
~Electrolyte imbalances* (often low potassium)
~Osteopenia* (low bone density) and osteoporosis* (brittle bones), often early onset
~Hiatal hernia* (stomach to esophagus sphincter) and all other forms of hernias just about anywhere (inguinal, duodenal, abdominal, etc.)
~Costochondritis* (pain at front rib attachment point to sternum)
~Chondromalacia* (cartilage loss) of all kinds, especially patellae (loss of cartilage in the knees, but can occur elsewhere, e.g. hips)
~Frozen shoulder
~Striae* aka “stretch marks” even in males and young (prepubescent) females (i.e. not always associated with pregnancy!)
~Bruxism* (jaw clenching, tooth grinding)
~TMJ* pain and issues, subluxations and dislocations (Temporo-mandibular joint syndrome, jaw alignment trouble)
~Restless Leg Syndrome* (RLS) and leg cramps (often eased by increased magnesium)
~Plantar Fasciitis*
~Chronically low Vitamin D and B12 levels* (caution urged for those with MTHFR mutations with the latter, may need a different form of Vi
Weak or crowded teeth, many need early or partial dentures
~Receding gums*
~Hair loss early, and even in women, especially those with signs of MCAD or iron imbalances
~Deviated septum (misaligned nasal cartilage)
~Trouble swallowing & choking issues, often neuropathic in origin from CCI, sometimes due to floppy laryngeal tissues
~Esophageal spasms (can extend to anywhere along GI tract also)
~Skin tears or rips, trouble suturing, would dehiscence (trouble healing post surgery, especially soft inner tissues)
~Liver problems, including fatty liver and lesions, enlarged liver
~Enlarged gallbladder & spleen, appendicitis (may be MCAD driven)
~Breast Ptosis (sagging, droopy breasts) had surgery to lift and reduce
~Leaky gut syndrome
~Dry eyes and blepharitis (bacterial eyelid infections), as well as retinal tears and more
http://ohtwist.com/about-eds/comorbidities
Remember Stay Zebra Strong!!
#common#comorbidities#ehlers danlos life#dysautonomia#pots#medicalptsd#medical#list#zebras#zebra#disability#ehlers danlos#ehlersdanlosawareness#self care#quotes#ehlers danlos problems#disabledveteran#tubie#veteran#chronic pain#spoonie
9 notes
·
View notes
Text
Ultra Thermo KetoUK – (ALERT – 2020* Must read Ultra Thermo Keto UK?
Ultra Thermo Keto UK :

Ultra Thermo Keto UK: are you shocked to learn that nothing works to lose weight? Do you have to lose real fat for the last time? Also, should you be sure of your body? At this point, Ultra Thermo Keto is there to help you reach your goals in the blink of an eye! This amazing fat consumption recipe can help you achieve significant weight loss results. Losing real pounds of fat has never been easier with this improvement! Since then, this equation increases digestion, strengthens vitality and pushes the body to consume its own fat reserves! Believe it or not, this improvement triggers your body's characteristic fat burning procedure.
For most people, we are discussing the necessary weight reduction. You will eat less and practice for a considerable period of time, if not months, and you will hardly notice an adaptation in your body. Also, at this point, most people have given up. Fortunately, Ultra Thermo tablets are not classified as "Ultra Thermo" for unknown reasons. This equation can cause your body to consume fat in a few days. In this sense, instead of taking a break and anticipating the results, you will see significant changes in your body in a few weeks! without forgetting, you consume kilos of steaming heat with an unchanged mass / muscle mass ratio. In this sense, it not only loses the weight of water, but consumes fat forever. This is why you have to accept it for yourself. Take a photo to try it now and get an Ultra Thermo Keto Expresso cost offer today!
Ultra Thermo Keto Avis France - Does Ultra Thermo Keto Really Work?
Of course, you must contact the customer to confirm the purchase. Of course, the offer will be sent by the service provider as soon as it does. Pay for the packaging Ultra Ultra Thermo Keto reviews for the EcoSlim effect. EcoSlim alcohol is made from high quality ingredients that are safe for the human body.
Ultra Thermo Keto - Slimming - Side Effects - Tip Gives a unique story that is used in the form of a virus. Of course, the products are harmless, so you don't have to worry about any problems. Of course, safe to use. Eco Slim Slim Cost. The actual price is $ 59, which is equal. A 50% discount is obtained from the previous price of $ 2,600 only for customers who want to lose weight EcoSlim Customer Data. Korina Horia, 24 years old. All my life I have been very physically active, but all week I was slim and I felt the impact of Ultra Thermo Keto. It helped me lose weight, separate it from the emotions it evokes. I was determined to choose something that would help me get faster, be more dramatic, and lose 13 pounds. It all started slowly, but regularly lost 1 kilogram. Tomas Lukaci, 32. The fact remains, according to Ultra Thermo Keto , regarding dangerous harm, I cannot control even my daughter to enter, for this reason, I was so alarmed by the violence. When I lost 10 pounds, I started going to the gym. Coming home is a great product that I spend at work or even at work.
How will Ultra Thermo Keto help you lose weight?
Ultra Thermo Keto UK 26 years old. My brother Broterand offered me several programs in 2013. I thought it was a contradiction. How can I lose weight without diet or exercise? In any case, it convinced me that Amazon Ultra Thermo Keto opinion lost weight on stage while I was trying it out. I never thought it was worth it. I started using it in February and in May I changed completely. This gives good advice. I lost 61.5 to 22 pounds in less than a month. Now I am a happy person. Finally, I recommend that you try this product for several weeks and find the Ultra Thermo Keto review site.a real pleasure. EcoSlim is certainly very safe in terms of fuel loss. By the way, this article was revised in 2012 by the Academy of Sciences.

Ultra Thermo Keto UK shows that self-harm does nothing to harm your body. Which is good for your health and well-being. The perfect bodybuilding will also attract people to you, the Ultra Thermo Keto price site hides Amazon, especially if you are really a virgin, and everyone, regardless of gender and age, wants to have a unique choice. with priority. Good eating and exercise habits as well
Benefits of the Ultra Thermo Keto Diet?
equally expensive medicines are often inadequate and do not reach the savings target. In some cases, people with Ultra Thermo Keto cheaper reviews reduce eating strategies, as well as the causes, exercise and are aware of bad habits that can have a negative impact on health, except for the benefits . to come up
Ultra Thermo Keto - to reduce - cost - cheaper - composition. It is also recommended to avoid plastic packaging and to remove the cells. What should you do to gain a slender figure in the short term, without reducing your energy too much, by planning a meal in addition to exercise? The unique design of Eco Slim is a truly beneficial supplement that probably not only affects weight, but also improves overall well-being and even well-being. Some other words related to the Siriir Emo Slim supplement are the Ultra Thermo Keto energy based nutritional supplements., developed by an American company specializing in packaging and manufacturing. Medication helps Eco Slim to study fat burning and increase metabolism. This treatment helps men lose weight, improve their health and well-being, as well as their health and mood. The content of Ultra Thermo Keto in Cheap Search actually claims that, unlike many similarities, this is not a test of the level of attractiveness of the review due to its important features. it also improves body weight;
How should you use the Ultra Thermo Keto Diet?
Accelerate and increase your operating costs; effectively increases the level of glucose in the intestine; stimulates the absorption of nutrients; educational opportunities, the eradication of hunger, in addition to actions which almost never go against the objectives;
Ultra Thermo Keto - France - forums - the pharmacy is very affordable. Many witnesses have proven the effectiveness of the drug. The process is actually done through the system. Data from experts overseeing the manufacturing industry has truly ensured a robust design tailored to customer needs. In fact, the energy point percentages are presented correctly. Emphasize the development of a system that promotes well-being and promotes Ultra Thermo Keto pharmacy in France pharmacy in addition to its evaluation objectives. Eco Slim contains: This alga has a strange and commercial building which can take the form of an interior and also gives you a sense of humor.
This substance increases blood sugar and lowers blood sugar. it is only in the capsicums that the pepper liquefies and oils itself correctly during the dressing. This is located in the Ultra Thermo Keto pharmacy to organize a forum for weight loss and is a useful addition to the body's defense system in addition to reducing interest; Greens, which contain a large amount of vitamins, alkaloids, fatty acids, in addition to plant life, which in fact has obesity problems,
Ultra Thermo Keto - in pharmacies - UK- forum and increases the metabolism of the human body's immune system, soaps, this function improves the digestive system, cleans and improves the water level in Ultra Thermo Keto Avis cream of calcium tablets and electrolytes. Dandelion is an excellent diuretic. This ingredient is used in the diet and helps to lose weight. Ultra Thermo Keto - pills - cream - how to use the opinions of real customers, has proven that this new innovative product is effective in the treatment of weight problems; Most modern girls find dessert for weight loss. Eco Slim is exactly how to reduce Czech weight. The eco-harmony is due to the fact that the houses of these plants improve their health and well-being and help you lose weight. Remove the guarana. This feature improves mental health and helps eliminate the added kilograms; Licorice and turmeric. Submit this herbal formula that can help melt your cells, how to use all Themomo Keto tablets, and also increase your nutritional benefits, as well as contraindications. Thank you very much for preparing and studying the secret Czech system, dieting has no harmful effect on the body.
Any unwanted side effects of the medication, except some viruses or possible intolerance to the individual. On the one hand, with any treatment or even more, the use of Ultra Thermo Keto cream for thin earth should advise you to continue to adhere to the brand: this reduces the need to rinse the water literally or in the statute of the Czech Republic; should be 3 times a day. Use the warranty regularly to ensure you get the recommended results. The result of its unique customization, the performance of this tool.
Does Ultra Thermo Keto work?
Ultra Thermo Keto works by putting the body in a state of ketosis. Ketosis is where the body is completely hungry and is forced to use fat for vitality and fuel. He begins to consume the layers of fat that he leaves aside and uses them to regain vitality. This invites a slender body. This is regularly the basic idea of a keto diet. Ketosis is faster after using a keto supplement.
Ultra Thermo Keto can be a low carbohydrate diet and contains a large amount of fat. Fats normally represent 80 to 90% of the total intake. everyone will need an unusual predictable keto diet with their somatotype. When you limit your sugar intake and eat fat gradually, your body will go into ketosis and start using fat for all of your body's capabilities.
Using Ultra Thermo Keto: much like the resulting keto diet. When you start using this enhancement, it accelerates your ketosis strategy. In the event that you follow a keto diet and use the potentiation added to your eating routine, the results are amazing at this point. Your body is immediately affected by a state of ketosis and you are ready to reach your predetermined weight goal much faster at this point than you would have recently followed with just a diet.
Using Ultra Thermo Keto reduces it, but it also encourages it to decrease as expected. This is often what gives and gives the keto with the fat counter improvements available in the market.
Ingredients Ultra Thermo Keto
Ultra Thermo Keto As mentioned, this equation only contains common BHB ketones. Ketones are basically the green light for your body to go into ketosis. In addition, BHB could be a substrate that also advises your body to go into ketosis and start consuming fat. In this regard, it is the Ultra Thermo Keto repair office. They activate fatty ketosis in your body. Also, goodbye, since you take them regularly, you should also stay in ketosis.
It is essential to stay in ketosis as much as possible, as an increasingly stubborn muscle / fat ratio with extreme heat is consumed. Fortunately, the Ultra Thermo Keto formula does it all for you. Therefore, as long as you accept the recipe as a guide, you should stay in the fat consumption zone. Is it safe to say that you are ready to start eating fat and exercising during an Ultra Thermo Keto? At this point, why are you holding on? Touch any image on this page to start getting the side effects you've always dreamed of!
Side effects of Ultra Thermo Keto:
Ultra Thermo Keto There are many diet pills full of counterfeit bras. Also, these container closings can hurt you after a while. Indeed, it will be they who will cause the preeminent reactions. Fortunately, the links in this equation are 100% characteristic. In this sense, you should not try the side effects of Ultra Thermo Keto. Obviously, if you find it, just stop taking this recipe. It is smarter to be protected than sorry.
Also feel the upper part of your body. That way, if it doesn't work for you, listen to your body and stop taking it. beat everything, we hope you enjoy this equation. In addition, we hope you will really appreciate the low-cost Ultra Thermo Keto offer that arrives immediately. Things are as they are, in case you want to eat fat and keep it while you are doing it, why stay there? Touch an image on this page to encourage your idea before it disappears!
How to buy ultra thermo keto in UK?
Ultra Thermo Keto This is the perfect opportunity to define the leader of your weight loss program. With the Ultra Thermo Keto Advanced Weight Loss desktop, you will start consuming fat in a few days. At this point, you will see real changes in your body that will make you happy. not to mention that it is one of the smartest financial recipes we have discovered on the web. Either way, the low-priced Ultra Thermo Keto offer won't last long. Therefore, if you want to consume fat and start seeing real results, it's best not to take a break. Basically, tap on any image on this page to encourage keto grip. At this point, plan to start burning the excess fat and getting a FLASH!
How To Work Ultra Thermo Keto Return Policy You will receive a refund for the product if you request it within 30 days of purchase. For all damaged orders or if you are not satisfied with the results, the refund may be processed within the time limit.
Ultra Thermo Keto Reviews - Final Verdict After reading the Ultra Thermo Keto review, it is now confirmed that the supplement is ideal for use by adult men and women. It overcomes obesity problems and gives it a subtle and elegant shape without causing side effects. So if you are overweight, go take the pill today.

see more at :http://www.innovationdiet.com/ultra-thermo-keto-avis/
1 note
·
View note