#Health Claims
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr app for Google Glass was released on May 16, 2013.
Text




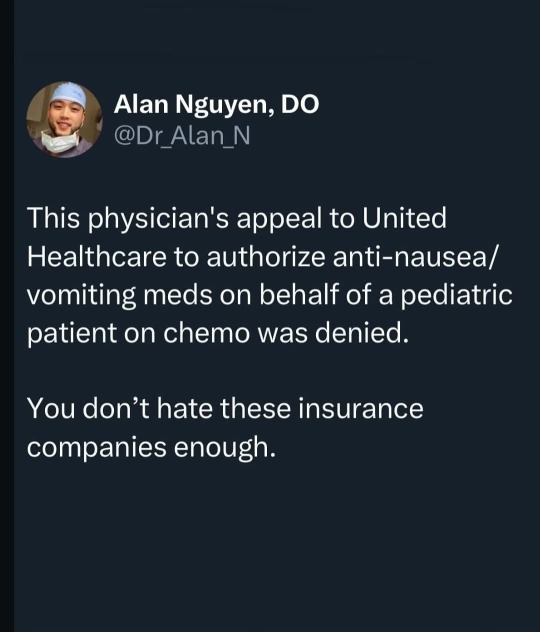
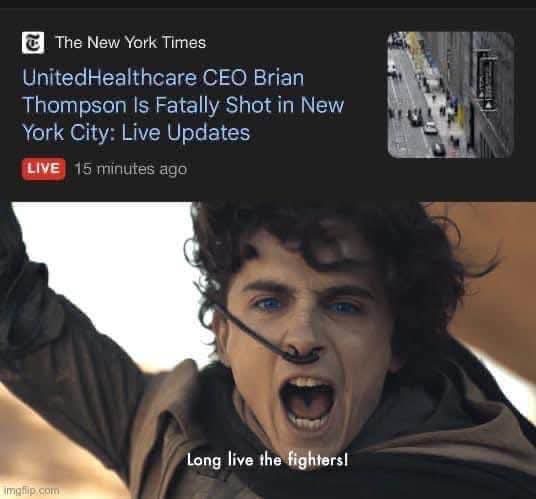
#threads social#united healthcare#us health system#insurance company#insurance claims#brian thompson#let the mystery shooter remain a mystery#let ceos live in fear
29K notes
·
View notes
Text

The Good, The Bad, and the Ugly - Michael Moore
MICHAEL MOORE ... "The easiest thing we can do is to give up. I know for many of you, what we face now seems insurmountable. So I want to share with you something GOOD that happened this week, before I get to the Bad and the Ugly."
#dr rex equality news information education#graphic source#graphic#graphics#hortyrex ©#horty#quote#it is what it is#MIchael Moore#health claims#healt insurance#the good#the bad#the ugly#intersting read#excellent posting
0 notes
Text
Navigating the Regulatory Landscape of Beauty Supplements at TOSLA Nutricosmetics show
In this new episode of the Nutricosmetics 2030 Show, host Matic Batagelj sits down with me, diving deep into the complex world of beauty supplement regulations, challenges, and opportunities within the industry, touching on topics from health and beauty claims to the intricacies of marketing within legal boundaries. HIGHLIGHTS: 00:00: Introduction to the complex world of beauty supplement…

View On WordPress
#advertising#beauty claims#beauty supplements#food labeling#Food law#food supplements#health claims#influencer marketing#regulatory#TOSLA
0 notes
Text
Obesity in Obstetrics
Mini review
The people in industrialized countries have experienced a dramatic increase in obesity in recent times. Prevalence of obesity has doubled in the last 25 years. In the United States, 17-th on the list of most obese places in the world - average BMI 28.8 Kg/m2, more than 60% of reproductive-age women are overweight and 35% are obese, representing a 70% increase in pre-pregnancy obesity. In Romania, 75th on the list- average BMI is 22.2 Kg/m2, the lowest average BMI in the European Union (9.4% obesity in 2016). [1] One of three Romanians is overweight, and one of four is obese. There are over 3.5 million obese in Romania. The highest obesity rate is recorded in Moldova, where the percentage is 23.8%. Only 10% of them see a doctor. Only one percent are included in a national obesity education program [2].
Not all ethnic groups are at equal risk. Of particular concern is the rapid increase in adolescent overweight and obesity. Concordantly, pregnancy obesity rates are also increasing. Obesity is associated with increased morbidity and 6- to 12-fold increase in mortality. Obesity is highly complex in terms of etiology and prevalence. Genetic predisposition, race, socioeconomic status, built environment (e.g., the presence of sidewalks or community design), accessibility of healthy and affordable foods, sleep habits, and geographic region all play a role. Lifestyle changes, which include consuming foods and beverages with a high glycemic index, increased food portion sizes, decreased structured physical activity, and increased screen-based sedentary behavior, have influenced the prevalence of obesity.
Antenatal Monitoring
An evaluation of dietary intake and exercise habits can provide insight into women at risk. All pregnant women without contraindications should participate in regular exercise. During prenatal visits women should be questioned and advised about their diet and exercise habits. Where available, nutritional counselling can be a helpful adjunct for women not meeting the weight gain recommendations.
The sonographer’s ability to evaluate fetal structures is largely dependent on maternal size. Approximately 15% of normally visible structures will be sub optimally seen in women with a BMI above the 90th percentile. In women with a BMI above the 97.5th percentile, only 63% of structures are well visualized. Obstetric care providers should take BMI into consideration when arranging for fetal anatomic assessment in the second trimester. Anatomic assessment at 20 to 22 weeks may be a better choice for the obese pregnant patient.
Use all available technical tools improving image quality in obesity: lower transducer emission frequencies; harmonic imaging; compound imaging; speckle reduction filters. Consider approaching the fetus through the four major abdominal areas with least subcutaneous fat: periumbilical area, suprapubic area, right and left iliac fossae. Consider using the transvaginal approach for the assessment of the central nervous system (CNS) in fetuses in vertex presentation.
Gently inform the patient and her partner that obesity will reduce the diagnostic accuracy of the scan. Consider including the BMI value among the demographic data in the report to document the presence or absence of maternal obesity. Report other cofactors of limited acoustic window, such as previous cesarean section (for the scar), twinning and myomata.
Pregnancy Complications
The risk of spontaneous abortion is increased in obese women. Lashen et al. identified an odds ratio for spontaneous abortion of 1.2 (95% CI 1.01 to 1.46) for obese women (BMI > 30 kg/m2). The authors also identified an increased risk of recurrent early miscarriages (more than 3 successive miscarriages < 12 weeks’ gestation) in the obese population, odds ratio 3.5 (95% CI 1.03to 12.01).[8] Similar risks have been identified in obese women undergoing in vitro fertilization treatment [3].
Pre-gestational diabetes is more prevalent in obese women. Therefore, testing during early in pregnancy for women with risk factors is recommended. Obese women are also at increased risk of developing gestational diabetes (GDM). Not surprisingly, obese women are also at increased risk of having a macrosomic child. Physical activity is inexpensive and can significantly reduce the risk of gestational diabetes. More relevant to the obese population, they also reported a 34% reduction in the development of gestational diabetes in women who did not participate in vigorous exercise but who did participate in brisk walking compared with those who participated in easy pace walking. Women with GDM have a 30% chance of developing type 2 diabetes later in life [4].
Intrapartum Complications and Management
Macrosomia and shoulder dystocia
The use of antenatal ultrasound to detect fetal macrosomia is associated with such obstetric interventions as labor induction and cesarean section. The rate of cesarean section is affected. Higher cesarean section is more frequent when ultrasound examination indicates a macrosomic fetus.
Fetal monitoring
The obese abdominal wall may make monitoring more difficult than in other cases, and of course, the positive predictive value of antenatal testing (e.g. cardiotocography, nonstress testing, biophysical profile assessment) is limited. There is no evidence to support the routine use of internal fetal monitoring in this population, but it may be more effective in some women. Monitoring contractions and ensuring adequate labor in obese women poses a special challenge. Obese women require more oxytocin in labor. Consider allowing longer first stage of labor before performing a cesarean for labor arrest. Although most obstetric care providers rely on manual palpation and/or external tocometry, the use of an intrauterine pressure catheter may be advantageous in some cases.
Cesarean section
The risk of cesarean section is increased in the obese parturient. The increase in cesarean section rate may be partly due to the fact that overweight and obese nulliparous women have a slower progression of the first stage of labor. When faced with lack of descent in the second stage of labor, some practitioners may opt for cesarean section rather than operative vaginal delivery because of concerns about fetal macrosomia and shoulder dystocia. This may explain the low rate of operative vaginal delivery in some series [5]. Obese women undergoing caesarean section experience more complications, including blood loss > 1000 mL, increased operative time, increased postoperative wound infection and endometritis, and need for vertical skin incision. The obese diabetic women who undergo cesarean section have an odds ratio for postoperative wound infection of 9.3 (95% CI 4.5 to 19.2), and those who require a vertical skin incision have a 12% rate of wound complication serious enough to require opening the incision [6].
For morbidly obese patients, two standard 50-cm-width operating tables secured together may be necessary. Specially constructed wider operating tables would be ideal. Weighing scales suited for obese patients are necessary not only to measure weight and evaluate weight gain during pregnancy, but also for calculating medication dosages. A wider delivery bed that is easy to move around and that may be used at all stages of delivery, including cesarean section, without the need to move the patient into another bed is most useful. Nursing care of obese patients requires ergonomic adaptation and knowledge about the special risks involved in caring for these patients. More trained nurses are necessary to care for morbidly obese patients.
The decision-to-delivery interval may be longer when an emergent or urgent cesarean section is required in obese parturient. Causes for this delay may include patient transport and bed transfer, the time to establish adequate anesthesia, and the operative time from incision to delivery. The 30-minute rule of emergency cesarean section is an arbitrary threshold rather than an evidence-based standard.
Vaginal birth after cesarean section
In the absence of contraindications, women who have had their first child by cesarean section are asked to consider vaginal birth in subsequent pregnancies. The success of vaginal birth after cesarean section is commonly quoted at 80% [7]. Obese women are less likely than their lean peers to be successful in delivering vaginally after previous cesarean section (VBAC). In women with a BMI > 29 kg/m2 the success rate is 54% to 68% [8]. The success rate is further reduced in even heavier women. Chauhan et al. found a 13% VBAC success rate in women >300 lbs (136 kg) [9].
Thromboembolism
The risk of thromboembolism is high in obese parturients. Edwards et al. reported 683 obese women (BMI > 29 kg/m2) who were matched to 660 normal weight women (BMI 19.8 to 26.0 kg/m2). The incidence of thromboembolism was 2.5% in the obese women, and only 0.6% in the controls.[29] BMI >30 plus one additional risk factor qualify for seven days of postpartum Clexane; BMI >30 plus two additional risk factors require Clexane antenatally and for 6 weeks postpartum; BMI>40 should be regarded as already having two risk factors. Clexane dosage should be calculated by weight:
Early mobilization and T.E.D. anti-embolism stockings are clinically proven to reduce the incidence of deep vein thrombosis by up to 50% and to promote increased blood flow velocity in the legs 138% of baseline by compression of the deep venous system.
Perinatal outcomes
Maternal obesity is also an established risk factor for stillbirth. The reported risk of stillbirth is 2-5 times higher in obese compared with normal-weight women. The risk of stillbirth associated with obesity increases with gestational age. Infant mortality rates increase from 2.4/1000 among normal weight women (BMI 18.5-24.9) to 5.8/1000 among women with grade 3 obesity (BMI ≥ 40.0). Maternal overweight and obesity are associated with increased risks of infant mortality due to increased mortality risk in term births and an increased prevalence of preterm births. Maternal obesity may increase the risk for intellectual disability or cognitive deficits in offspring from 1.3- to 3.6-fold. Maternal prepregnancy obesity and high gestational weight gain of > 18 kg was associated with a 3-fold increase in offspring IQ deficit (mean of 6.5 points lower) [10]. The majority of studies that have examined a link between high maternal BMI and childhood diagnosis of autism spectrum disorders have found a significant positive association. This risk may be further augmented by intrauterine growth restriction (IUGR), preterm birth, high gestational weight gain, gestational or pre-gestational diabetes, and preeclampsia [11].
Conclusion
A national information campaign is required to exploit women’s interest in having as healthy a pregnancy as possible by giving them the information they need to become fit and have a normal BMI before they consider pregnancy. Periodic health check-ups and other appointments for gynecologic care prior to pregnancy offer ideal opportunities to raise the issue of weight loss before conception. Women should be encouraged to enter pregnancy with a BMI < 30 kg/m2, and ideally < 25 kg/m2. Although obesity is not an indication for the transfer of routine obstetric care, consultation with or referral to physicians with expertise in obesity may be appropriate if the obstetrician cannot safely and effectively care for the patient because of the lack of the specialized training, experience or institutional resources.
To Know More About Nutrition and Food Science International Journal
Please click on: https://juniperpublishers.com/nfsij/index.php
For more Open Access Journals in Juniper Publishers
please click on: https://juniperpublishers.com/index.php
1 note
·
View note
Text

859 notes
·
View notes
Text




Seeing a black woman winning makes me feel so empowered....
#aesthetic#beauty#inspiration#self care#self love#affirmations#manifesation#beautiful women#black women#black beauty#black luxury#luxury#luxurious#successmindset#successful#claim it#becoming her#beautiful#health and wellness#women empowerment#women empowering woman
1K notes
·
View notes
Text
0 notes
Text
Born to be on the cover of vogue forced to ambush unsuspecting CEOs in the dawn


#luigi mangione#fuck brian thompson#brian thompson#ceo down#fuck ceos#claims adjuster#deny defend depose#fuck health insurance ceos#united healthcare
733 notes
·
View notes
Text
Last week, It emerged that health insurance leaders pressured the DOJ to bring federal charges against Luigi Mangione.

#luigi mangione#deny defend depose#the claims adjuster#us politics#politics#america#eat the rich#health insurance#united healthcare#uhc ceo#ceo#brian thompson
370 notes
·
View notes
Text
Rolling Stone is the only news outlet giving honest reporting on this
We all know we're terrible people for being happy he's dead. Show us the funny tweets.

Look. Balanced reporting.

If you're reporting on this story and just brushing this away as a bunch of meanies being mean on the internet, I think you're not doing your job very well. Blue Cross saw enough to make them walk back their anaesthesia policy. Maybe this won't make huge changes happen. But it had an immediate impact on something genuinely horrible and horrifying and I'm very glad of it.
292 notes
·
View notes
Text


#insurance company#claim denied#acute lead poisoning#brian thompson#united healthcare#us health system
3K notes
·
View notes
Text
Something I really like about timebomb is that Ekko actually knows what he's getting into.
I'm not really seeing it get talked about but in season 1 they mention that Ekko and the firelights help people addicted to shimmer get off it and lead more fulfilling lives within the community. I should probably rewatch the scene for the exact wording (might be misremembering tbh) but that comment implies A LOT.
First: Ekko's mission is helping people where he can, he would probably try and help Jinx even if he wasn't in love with her
Second: He has experience dealing with severe mental illness as that often goes hand in hand with drug abuse, namely depression/suicidal ideation like what Jinx was exhibiting
Third: He's probably mapped out best course of action FOR dealing with this and has already figured out his own limits/boundaries. Meaning he knew what he was getting into trying to talk Jinx out of suicide, and was thus more equipped to deal with the aftermath
Fourth: He's probably helped ex members of Silco's gang. The firelights seem to have a theme of healing and repairing and recovering, so they've probably also learned to forgive. If they're mission is to rebuild the lanes into a safe space, they can't exclude people they don't like, they have to make room for them. I think they fought Silco out of necessity, and I doubt Jinx would be the first person they help who's killed one of them.
These all might be a bit of a stretch but I think it really fits. Beyond that, it shows that Ekko can ACTUALLY help Jinx. As much as unconditional love can do, Ekko has the tools for Jinx's recovery and a path ready for her. He also probably knows that her "healthy" will look different from AU Powder's "healthy." On top of that, I expect he knows how to respect her even in the middle of psychotic breaks and won't agitate her already frail mental state
#if you would like to (respectfully) disagree with me I'll GLADLY talk with you. I can think of nothing but Arcane atm#timebomb#ekko arcane#putting it in the tags bc I want to let people agree with my timebomb takes without having to listen to my other ship opinions#uh on that note I have some Caitlyn and Vi opinions that go a bit hand in hand with this#but I think that in contrast Caitlyn and Vi are mutually self destructive#see neither of them seem to make the others mental health... better.#Vi is desperate and needs love wherever she can get it#and Caitlyn... I'm not sure. I have a hard time reading her but a lot of the vibes I get off her feel like she just likes having the power#over vi#I KNOW THAT'S A STRONG CLAIM#hear me out#Vi in her search for unconditional love does a lot of enabling#a good example is when Caitlyn arrests that henchman in episode 3(?)#Vi is VISIBLY uncomfortable with that and for good reason!#Caitlyn just locked someone up for life for... nothing?#kinda like Marcus did to her (yes Marcus was trying to protect her but I doubt that's how Vi sees it)#but Vi doesn't voice this or push Caitlyn on it#instead she asks Caitlyn not to change#not great communication on Vi's part#but also indicative of how little their values align#and how little Caitlyn actually considers Vi and her problems and history#Caitlyn doesn't help Vi heal and she turns on Vi the second Vi stops enabling her and letting Caitlyn do as she thinks is best#neither of them are ready to deal with the others problems or communicate well#again. willing to discuss this. my opinions are swayable.#I just personally found Caitlyn made the most sense and was most compelling when she was going down facist dictator path#sure she could be more but I don't think the show ever really transitioned her away from that#you can see it in the way she treats Maddy#hhhhhh I should go to bed rather than spill every last thought I've ever had
283 notes
·
View notes
Text
Navigating the New Landscape: FDA's Upcoming Food Regulations and Their Impact on Manufacturers
The Food and Drug Administration (FDA) plays a pivotal role in ensuring the safety and proper labeling of food products in the United States. The latest update on its website details a range of regulations under development that will significantly impact the food industry. These upcoming regulations are designed to enhance transparency, improve food safety standards, and provide clearer guidance…

View On WordPress
#FDA#Food#Food & Drug Administration#food labeling#Food law#food standards#FOP#health claims#healthy#nutrition labeling#Regulation#USA
0 notes
Text
Mentally ill people actually get abused and assaulted at HIGHER rates than the average population. And we're not immune to genuine health emergencies and serious physical health issues either. The "they're mentally ill, so what they're complaining about is probably all in their head" ableism is hurting and killing many, many people
199 notes
·
View notes
Text
When Jesus pretended to be dead for 3 days it's a miracle and everyone is sympathetic. But when I, James Somerton-
#james somerton#hbomberguy#Sorry#just to be clear i dont wish somerton any harm#for the money he tricked people into donating i'm sure there will be a lawsuit. maybe??#for the plagiarism idk if and how the law applies#for his personal mysoginistic racist etc views i've seen maybe one of his videos years ago and i don't remember his claims#i just think that as an influancer / youtuber he's a public figure and it's not the public's responsability to cater to his mental health#whether his mental health issues are real or just excuses#i'd rather he change career and be held accountable than he hurting himself#being in a bad mental state doesn't justify your actions#especially if the bad mental state is directly caused by the conequences of said actions
454 notes
·
View notes
Text
if anyone is able to help me out i'd appreciate it, im still broke as hell. this month has been really difficult for me. i worked a total of 5 days all month and my bank account is in the negatives again after paying bills and getting some living essentials. i dont know how im going to pay my rent like this. i applied to a financial relief fund from a local trans advocacy group but it's going to be a few weeks until anything comes from that. if you have literally anything to spare it would help me out a lot 😭🙏 i feel bad ive been asking for help so often and i know everyone is struggling, im working on getting my life back in order but everything fucking sucks and is difficult right now :( even just spreading this is a huge help
pp: paypal.me/bewearrr vnm: tobias_leviathan
thank you 💕💕
#im looking for a new job but i dont think its gonna happen any time soon :( my current job is fucking miserable#im working on comms to the best of my ability but i can only draw so fast and i dont want to injure myself and its hard to stay motivated#when ur mental health is tanking so hard#my physical health has been tanking too like stress is getting to me so hard i fucking started a period out of nowhere#i havent menstruated in like 10 years legitimately#im so beyond stressed i have to stop myself from panicking all the time#i have a bunch of work coming up this week but its nowhere near full time#they schedule based 'on performance' when youre part time and since im only here one day a week and they put me at the station i hate--#the most its almost inevitable that theyre using this as a way to get me to not be there. i dont think my boss likes me very much.#bc then they can claim my performance isnt good BECAUSE YOU PUT ME ON THE TASK THAT IVE SAID FROM DAY ONE I DONT WANT TO DO
180 notes
·
View notes