#Family History of High Cholesterol
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
69% of Tumblr users are millennials.
Text
#LDL Cholesterol (Low-Density Lipoprotein)#HDL Cholesterol (High-Density Lipoprotein)#Total Cholesterol#Triglycerides#Cholesterol Levels#Hyperlipidemia#Heart Disease Risk#Diet and Cholesterol#Statins#Lifestyle Changes#Blood Test for Cholesterol#Cholesterol Management#Family History of High Cholesterol#Symptoms of High Cholesterol#Cholesterol Guidelines#health & fitness#health and wellness
0 notes
Text
do not let western doctors make you scared of white rice!!!!
#the num 1 thing my doctor told me when she saw my family's history of high cholesterol was to stop eating white rice#but red meat is actually the num 1 thing associated with high ldl cholesterol and mortality rates#and rice -consumed with healthy portions of other vegetables/soy products/seaweed- is not as highly associated with it#dont let the west demonize a staple food of the east#u can still have ur white rice in modest proportions#its the red meat u gotta watch out for tho- eat more fish!!
3 notes
·
View notes
Text
I also found out I have pretty pretty high cholesterol. This wasn't something my doctor flagged for me just 4 years ago when I last had labs, meaning it's a pretty new issue. That checks out since I've always had good cholesterol.
In good news I'm not even in the ballpark of at risk for diabetes which is the one everyone's worried about for me constantly cuz im fat.
Made an appointment with a psych but I can't get in till May. But once I get my vitamin D under control and get on some kind of mental health pills/assistance and get some energy back it'll be a lot easier to exercise. Until then I'm just gonna focus on eating meat and dairy a little more discerningly and drinking more water cuz my labs came back dehydrated too >_>;
I really wish my doctor had given me some more specific instructions than just "go on a diet and exercise" without even asking me about my diet or activity levels but what can you do. Once you're over 300 pounds you're not really a person to a doctor until you've lost half that.
#diet tw#weight#nice to know I don't really need to worry about sugar#i keep getting tested for diabetes cuz everyone wrings their hands at me about it and its literally never been a concern according to tests#its not in my family which is like 80% of it or some crazy number#high cholesterol is in my family but heart attacks arent really#my mom's side is pretty healthy just riddled with addiction which is why i dont fuck around with substances besides a touch of the maryjane#dont know a lot about my bio fathers side except theyre very mentally ill and also very fat#my mom says i look just like my paternal grandmother but i never met her#kind of scary to only know about one side of family history but what can you do#anyway enough with the rambling i have to be up in like 6 hours...
5 notes
·
View notes
Text
I wish there was an app that let you track nutrient intake without showing you your calorie intake. I just want to track my fiber and protein to help manage my chronic illness without triggering my number obsession please
#OCD and anorexia are linked/frequently comorbid so I try to avoid doing things that could trigger anorexia like calorie counting#but I need to up my fiber intake to fix my high cholesterol since I have a family history of high cholesterol-related heart disease#diet tw
8 notes
·
View notes
Text
hate that the word 'diet' is such a weighted word, cuz you can tell someone 'oh yeah i'm altering my diet cuz my cholesterol is a little high' and they'll go oh so you're trying to lose weight? this is weight loss related right? diets mean weight loss. you're trying not to be one of those depraved fat people anymore are you? here's fifteen ways to totally ruin your whole body by depriving yourself, but at least you won't be a fatty fat anymore :)
#rhobi: the sitcom#i got my blood results back so it's on my mind rn#got a family history of high cholesterol so i'm not exactly surprised
3 notes
·
View notes
Text
I generally agree with OP, but I'd like to highlight a few points:
Most of the studies OP has linked are anywhere from a decade to almost 15 years old. Generally, this means that the data may not be super reliable for the general population in the present (2023), since methodology may have changed, new studies on the subject may be added, populations may change, etc. Basically-take the claims therein with a grain of salt.
The study looking at if exercise led to weight loss in Type II diabetics noted a significant decrease in visceral fat (the fat around your organs, feels hard like a drum) with exercise than without. Visceral fat, not subcutaneous fat (the softer fat closer to the skin) is what is more concerning medically, as it is associated with metabolic diseases like Type II diabetes. Whether visceral fat is the cause of these diseases or a symptom of it is currently up for debate, though. From what I have read so far on PubMed, inflammation within the fatty tissue is more indicative of problems than the actual fat itself.
The study looking at if exercise led to weight loss in non-alcoholic fatty liver disease (NAFLD) says that the data they found was so biased/sparse that most of the analyses they sought to do were essentially impossible, so we can't really say if exercise impacts weight at all in this group.
The study on computer interventions and weight loss in overweight/obese people was also extremely sparse on data, focused primarily on women, and found that in person interventions were generally more effective at weight loss than computer based ones. However, both are not going to lead to immense weight loss, at least not within a year or two. This is something that the other studies OP linked also found.
TL:DR Most of the claims OP made are verifiable, but take them with a grain of salt since the studies are old and many have unreliable data sources. Exercise may reduce visceral fat in Type II diabetics, but not necessarily overall body weight. We can't really say if exercise does anything to body weight in people with NAFLD.
If you're going to exercise, do it for general health reasons, not for weight loss.
Me: Exercise does not cause weight loss. This is a fact that has been demonstrated so robustly in research that even doctors, who hate and fear evidence, are grudgingly starting to admit this.
Someone reading that post: Cool, but have you considered that exercise leads to weight loss?
Me: I am going to eat you
#finally my graduate school experience is becoming useful#also yeah i agree with OP bc 1. every single person on my mom's side has belly fat no matter how skinny you are#(tho my family also have a history of type ii diabetes so maybe there is some truth to the visceral fat finding)#and 2. when i was depressed and underweight i STILL had noticeable belly fat#even now i regularly exercise and am mostly vegetarian and i still have it lol#btw i didn't even do those changes bc i wanted to lose weight#i did it bc my cholesterol is stupid high and i kept getting RSIs#fuck my family's genetics!!!
77K notes
·
View notes
Text
Folic acid and heart health
Folic acid is a B vitamin that is important for many bodily functions, including cell growth and repair. It is also important for heart health. How folic acid benefits heart health Folic acid helps to lower levels of homocysteine, an amino acid that can damage blood vessels. High levels of homocysteine are a risk factor for heart disease, stroke, and other cardiovascular problems. Folic acid…
View On WordPress
#blood vessel function#cardiovascular disease#diabetes#doctor&039;s advice#family history#folic acid#food sources#heart health#high blood pressure#high cholesterol#homocysteine#inflammation#medications#pregnant women#recommended daily intake#supplements
0 notes
Text
I want to talk a bit about the whole "fat trans men are denied top surgery" thing because it's true. Many surgeons have BMI requirements and will not operate on anyone classified as more than "overweight".
But I also want to discuss how testosterone often makes you gain weight, putting trans mascs in a fairly difficult position.
When I started testosterone, I weighed 178lbs. I rapidly shot up to 198lbs. At 5'10" I'm classified as just over a BMI of 30 according to my discharge papers, making me classified as obese. I also started having a bit of a cholesterol problem and being that A: I've also hit my 30s in that time and B: I have an extensive family history of high cholesterol in the men in my family, we tried changing my diet and exercise to see if it was lifestyle or if it was genetic.
In that timespan I dropped 3lbs (bringing me to 195lbs, just under that obese line) and my cholesterol continued to climb. It's been about 7 or 8 months with no other change.
When I tell people that I weigh roughly 200lbs, they don't normally believe me. To be clear I don't really care about any of these numbers, I care about my overall health irt stamina, strength, fatigue, etc and I care about my actual muscle mass and body condition. There are, admittedly, times where I look at my stomach and go :( aww I used to be skinnier. But then there's also times like two nights ago when I looked in the mirror after my shower and just saw A Guy standing there looking at me.
Anyway. My point is, testosterone (and age) made me gain a significant amount of weight, and nothing really I've done has gotten it off. Which is fine with me, because I feel better at this current condition and am stronger and have more stamina than I ever did at lower weights even when I was a competing athlete. Everyone I tell my weight and BMI to is shocked to learn that I am 200lbs and classified as obese. From complete disbelief until I stand on a scale, to the immediate "you wear it well" or "it's all muscle though", to the inevitable "okay but BMI is a load of shit anyway", clearly even though that's what the numbers say I am not exactly the poster child for what lawmakers and fat phobic doctors fear monger about when they discuss the "obesity epidemic".
I am lucky enough that while my surgeon is being very annoying in other ways, she at least has no BMI requirement. For 7 or so months I have been putting in a lot of effort to try and lose some weight to fix my cholesterol and I have pretty much nothing to show for it. If it's that hard for me, someone who visually doesn't really look fat, how difficult must it be for someone who is definitely not toeing the line like I am. How impossible for someone who is in the 400lb, 500lb, 600lb range.
Testosterone makes you gain weigh, and then surgeons won't operate if you gain too much. What a fucking joke.
1K notes
·
View notes
Text
A brief guide to Testosterone HRT
If you’d like the one for Estrogen HRT, ask in the comments and you shall receive.
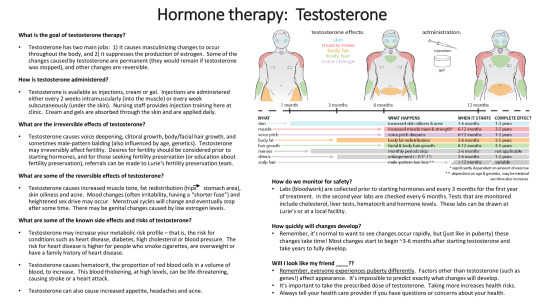
Image from the Transpeak Discord - unsure of actual source (a clinic?) (if anyone knows, please tell!)
Alternate text under the cut
Alt:
What is the goal of testosterone therapy?
Testosterone has two main jobs: It causes masculinizing changes to occur throughout the body, and it suppresses the production of estrogen. Some of the changes caused by testosterone are permanent (they would remain if testosterone was stopped), and other changes are reversible.
How is testosterone administered?
Testosterone is available as injections, cream, or gel. Injections are administered either every two weeks intramuscularly (into the muscle) or every week subcutaneously (under the skin). Nursing staff provides injection training here at clinic. Creams and gels are absorbed through the skin and applied daily.
What are the irreversible effects of testosterone?
Testosterone causes voice deepening, clitoral growth, body/facial hair growth, and sometimes male-pattern balding (also influenced by age and genetics). Testosterone may irreversibly affect fertility. Desires for fertility should be considered prior to starting hormones, and for those seeking fertility preservation (or education about fertility preservation), referrals can be made to Lurie’s fertility preservation team.
What are some of the reversible effects of testosterone?
Testosterone causes increased muscle tone, fat redistribution (hips to stomach area), skin oiliness and acne. Mood changes (often irritability, having a “shorter fuse”) and heightened sex drive may occur. Menstrual cycles will change and eventually stop after some time. There may be genital changes caused by low estrogen levels.
What are some of the known side effects and risks of testosterone?
Testosterone may increase your metabolic risk profile — that is, the risk for conditions such as heart disease, diabetes, high cholesterol or blood pressure. The risk for heart disease is higher for people who smoke cigarettes, are overweight or have a family history of heart disease.
Testosterone causes hematocrit, the proportion of red blood cells in a volume of blood, to increase. This blood thickening, at high levels, can be life-threatening, causing stroke or a heart attack.
Testosterone can also cause increased appetite, headaches, and acne.
A low-detail diagram of the upper half of three bodies is displayed. From left to right, the bodies represent having been on testosterone for little to no time (a month or less), a medium amount of time (six to eight months) and a greater amount of time (a year or more).
The diagram is a visual representation of testosterone effects on the body. Hip mass shifts to the stomach area, The adam’s apple grows. Muscle mass grows and shoulders become broader. Facial and body hair grows on the arms, face, and assumably the legs not displayed in the image. The skin gets oily and acne appears on the face.
Testosterone affects: skin, muscle mass, body fat, body hair, voice change.
Increased skin oiliness and acne starts within 1-6 months of testosterone. Its complete effect can be within 1-2 years.
Increased muscle mass and strength starts within 6-12 months of testosterone. Its complete effect can be within 2-5 years. This effect is highly dependent on the amount of exercise one does.
Voice pitch deepening starts within 6-12 months of testosterone. Its complete effect can be within 1-2 years.
Body fat redistribution starts within 3-6 months of testosterone. Its complete effect can be within 2-5 years.
Facial and body hair growth starts within 6-12 months of testosterone. Its complete effect can be within 3-5 years.
Monthly periods stop within 2-6 months of testosterone.
Clitoral enlargement of 0.5 inches to 1 inch begins within 3-6 months of testosterone. Its complete effect can be within 1-2 years.
Male pattern hair loss starts when you have been on testosterone for over a year. Its complete effect date is variable. It depends on age and genetics, and can be minimal.
Sex drive also increases.
How do we monitor for safety?
Labs (bloodwork) are collected prior to starting hormones and every three months for the first year of treatment. In the second year, labs are checked every six months. Tests that are monitored include cholesterol, liver tests, hematocrit, and hormone levels. These labs can be drawn at Lurie’s or a local facility.
How quickly will changes develop?
Remember, it’s normal to want to see changes occur rapidly, but (just like in puberty) these changes take time! Most changes start to begin around 3-6 months after starting testosterone and take years to fully develop.
Will I look like my friend _____?
Remember, everyone experiences puberty differently. Factors other than testosterone (such as genes!) affect appearance. It’s impossible to predict exactly what changes will develop.
It’s important to take the prescribed dose of testosterone. Taking more increases health risks.
Always tell your health care provider if you have questions or concerns about your health.
#mod cole#trans#transmasc#transgender#trans man#ftm#transmasculine#trans guy#testosterone gel#testosterone#testosterone hrt#ftm hrt#trans hrt#hrt#hormone replacement therapy#testosterone replacement therapy#trans boy#transsexual#trans ftm#trans men#trans male#trans pride#transblr#transsexuality#trans masc#ftm trans#trans resources#trans resource#resources#has this already been posted on this blog? we’re about to find out
299 notes
·
View notes
Text
141 and what their patient file looks like
┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊
summary: This is what I imagine everyone's favorite pharmacist as well as medics see when they look at 141's medical file.
Based on this pharmacist and 141 interactions
pairing: Task Force 141 x pharmacist!Reader
warnings: medical/pharmacy terminology, medical inaccuracies, swearing, depiction of wounds, mention of substance use disorder and abuse
Terms
PMH - Past medical history - the total sum of a patient's health status prior to the presenting problem
FH - Family history - contributing family history, generally parents and siblings
SH - Social history - contributing social behavior and routine
a/n: not canon at all! this is just a reference for me
┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊
Price
PMH
Height: 1.88 m (6' 2'')
Weight: 93 kg (205 lbs)
Blood type: O+
Extensive physical injuries
21+ stab wounds - 2 required antibiotics for recurrent infection
9x bullet wound - 5x in the extremities, 4x in the chest (no perforation of vital organs), healed without complication
5x abrasion collar - 1 near right eyebrow became infected following medical eval and stitches
3x diagnosed concussion
Aspirin-sensitivity
Previously evaluated for tinnitus and hearing loss
FH
Father - deceased at 76 from liver disease - 50 pack years, mycardial infarction (x2)
Mother - deceased at 84 due to chronic heart failure (CHF) -Glaucoma, asthma, CHF
Sister - Sports induced asthma, hypothyroidism
Negative family history of diabetes, hypertension, and cancer
SH
Smokes - 30 pack years
Drinks regularly - 4-5 hard liquor each weekend; 1 glass of whiskey occasionally
Physically active - Enjoys recreational activities such as hiking, swimming, and biking
Has 1 dog, currently under the care of pt's younger sister
History of monogynous long term relationships, currently single
Medication list + indications
Amoxicillin/Clavulanic acid 625mg - Infection
Morphine 15mg + Ketamine 3mg - IV - Pain
Paracetamol 750mg - Pain
Buproprion SR 150mg - Smoking cessation - not-taking est 2004
Allergies
Aspirin allergy - Reaction: hives and asthma - ONLY PRESCRIBE PARACETAMOL
No environmental, food, or animal allergies
Notes
Patient has denied smoking cessation options
Soap
PMH
Height: 1.88 m (6' 2'')
Weight: 91 kg (200 lbs)
Blood type: O+
7x stab wound - 6 required antibiotics for recurrent infection, 2 MRSA resistant
2x bullet wound - 2x in lower extremities, healed with no complication
6x abrasion collar
2x broken collar bone - healed, with no complication
Lactose sensitivity - Recurrent IBS if ingested
Chipped first left molar following opening a beer with teeth
FH
Father deceased at 68 due to heart failure - Type 2 Diabetes Mellitus, high cholesterol
Mother - Stage I HTN (hypertension)
Sister #1 - Postpartum depression, generalized anxiety disorder
Sister #2 - Elevated cholesterol/triglycerides
Brother - No known chronic health issues
Positive family history of diabetes and hypertension, but no cancer
SH
Drinks regularly and heavily - 8-12 beers and 2-3 glasses of hard liquor each weekend; 1 glass of scotch occasionally
Smokes socially - 5 pack years
Physically active
Close relationship with family, has 4 dogs at home under the care of pt's mothers
Avid fan of The Glasgow Football Club
Medication list + indications
Clindamycin 300mg with ciprofloxacin 400mg - Infection
Amoxicillin/Clauvanic acid 625mg - Infection
Vancomycin 18mg/kg - MRSA resistant infection
Paracetamol 500mg - Pain
Morphine 15mg IV - Pain
Doxycycline 100mg - Acne discontinued in 2004
Allergies
Insect stings - Observed anaphylaxis to childhood bee sting
Notes
Patient demonstrates medication non-adherence, counsel ESPECIALLY with antibiotics
Scored 6 on Alcohol use disorders identification test for consumption (AUDIT C)
Gaz
PMH
Height: 1.86 m (6' 1'')
Weight: 93 kg (205 lbs)
Blood type: B-
3x stab wound - healed, no complications
1x broken collar bone
2x broken femur
Diagnosed concussion - evaluated in Oct. '19
FH
Father - Type 1 Diabetes, high cholesterol
Mother - Vitiligo, Stage 3 breast cancer
Positive family history of maternal cancer and diabetes, but no hypertension
SH
Social drinker - 3-4 beers each weekend
Does not smoke
Physically active - Enjoys morning and evening runs
Enjoys spicy food and tries to introduce into diet
When on leave, enjoys attending concerts and music festivals
Medication list + indications
Piriteze 10mg - Allergic rhinitis
Fluticasone Propionate - 93 mcg/actuation - Allergic rhinitis
Paracetamol 500mg - Pain
Allergies
Seasonal - Pollen and pet dander
β-Lactam allergy - Reaction: anaphylaxis evaluated in '19
Notes
Organ donor
Ghost
PMH
Height: Weight: 1.93 m (6' 4'')
WeighT: 100 kg (220 lbs)
Blood type: AB-
Extensive cuts and scarring to entire body
4+ stab wounds - healed, no complications
Gun shot to lower abdomen - healed, no complications, evaluated in Nov. '22
13+ collar abrasion
2x broken nose
Childhood injury of broken tibia and large toe
Psych eval - History of depression and post traumatic stress disorder, childhood history indicates emotional and physical abuse
FH
Father - status unknown Diagnosed alcohol use disorder
Brother - deceased, cause of death non-contributory - Substance use disorder
Mother - deceased, cause of death non-contributory - Hypertension, thrombophilia (blood clotting disorder)
Positive family history of hypertension, but no diabetes or cancer
SH
Social drinker - 3-4 glasses of hard liquor each weekend
Smokes socially - 10 pack years
Physically active - Enjoys nightly walks
Psych eval - Other squad members act as his emotional support
Expressed interest in cats and tattoo art (FLAGGED: Further input and comments from other medical professionals would be appreciated)
Medication list + indications
Paracetamol 1000mg - Pain
Amoxicillin/Clavulanic acid 625mg - Infection
Morphine 20mg + Ketamine 4.5mg IV - Pain
Mafenide acetate 5% topical - Antimicrobial, burn wounds
Fluoxetine 20mg twice daily - Depression - not taking est 2001
Allergies
NKDA - No known drug allergies
No environmental, food, or animal allergies
Psych recommends evaluation of a pet, such as cat, for pt while on leave
┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊ ⋆ ┊ . ┊ ┊┊
#task force 141 x reader#task force 141#cod x reader#call of duty modern warfare#cod mwii#modern warfare 2#simon riley x reader#simon ghost riley#call of duty#john soap mactavish#kyle gaz garrick#gaz x reader#soap x reader#price x reader#kyle garrick x reader#john price x reader#Johnny mactavish x reader#mw2 imagine#madebyizzie#mw2#izzie is writing#pharmacist! series
1K notes
·
View notes
Text





As usual, gym OOTD is: “Hasn’t accepted that he needs to size up.” 🐷 skipping cardio and letting my shirt ride up in front of everyone when I do my lifts.
I’m really being a fat slut recently. I’ve just been crushing my protein goals after a lengthy period of being too depressed to build muscle. I am feeling so BIG and loving the growing strength. I’m just totally embracing my appetite and the jiggles.
Oh course, I’m sure that it’s only a matter of time before I start freaking out again about the new highs on the scale and make another pathetic attempt at losing some of it. I’m not worried though. I know where I’m eventually going to end up and it’s going to make me so happy.
Standing at the precipice of stepping off the cliff of the 150 lb range is as thrilling and euphoric as it is genuinely terrifying. I can see myself and my path to 165 lbs (which would be my ideal next pit stop on my way to my goal of obesity at 180 lbs) but dang, I’m gonna be ruined physically and mentally if I’m not careful. I think that so long as I keep in shape I can mostly convince myself that my weight isn’t /too/ bad but it’s such a tight line to walk to not get fat too fast to stay fit (for me at least) and it gets more and more tempting to be lazy with every extra pound.
I’ve also basically decided that I’m gonna seek medication related to diabetes prophylactically when I reach that point. Like, I can eat as plant based as possible and work out to support my cholesterol and blood pressure but with my family history and signs of insulin insensitivity already appearing at a certain weight I’m gonna need some sort of pancreatic support - to minimize the squeeze from visceral fat if nothing else (besides more subq would be sexyyyyyyy) I’ve made a ridiculous delusional plan that I could access something like that and it could actually really support my gain by preventing damage from my obesity instead of reacting to it and hopefully minimize the chances of being in a situation where I have to lose weight for my health.
“Piggy boy is such a fatass that he needs meds because he just can’t say no to ice cream, doc. That’s why his belly is spilling out of his shirt and he’s up 10 pounds year over year for the past 5 years. You better do something quick before he starts tipping past 200 lbs and the gains accelerate until he can barely waddle back into this office.”
183 notes
·
View notes
Note
My doctor, who knows I have Hypermobility and possible EDs, suggested I got to a chiropractor and I still haven't psychologically recovered. (I did not go)
My doctor, who treated my mom for hyperlipidemia and treated my sister for her high cholesterol, is the one who prescribed a Keto diet (contraindicated for people with a family history of high cholesterol).
As much as I do hate CAM (and i do!) it has to be said that doctors aren't much helping their case in terms of what is or is not science based.
It sucks because it all sucks! The medical industry sucks! The alternative medical industry sucks! GPs don't know what the hell is up with any zebras they come across and the zebra doctors are few and far between! Insurance pays for chiropractic sometimes when they won't pay for PT and the patient gets screwed!
People shouldn't have to know all of this shit to feel safe going to the doctor! People shouldn't have to do deep dives into every single thing their doctor brings up to figure out whether it's legit (not in the least because if you act like you know too much about something there's a good chance your doctor will act like you're faking or drug seeking!)
The medical system is catastrophically broken and that's awful because it's still better than everything else, which is a huge indictment of our society.
Bad! It's all extremely bad! And I hate it and i'm sorry that your doctor did that! (Though I'm very glad that you did not go).
230 notes
·
View notes
Note
Writing a suicidal protagonist, but not depressed.
I'm going through a bit of a rough patch at the moment so I'm trying to put it into my writing. Do you have any advice for writing this? I mean, I suppose I already have the experience, but writing tips are always welcomed.
(I really hope this doe)sn't come across as trauma dumpy, I'm not seeking any irl advice. I suppose I just see it as an objective reality of many that doesn't necessarily need to invoke things such as comfort or anything, y'know?)
I'm glad you're trying to put such personal experiences into your writing.
Since I don't know much about your specific protagonist, in addition to incorporating your own experiences, I'll provide you with some writing notes on suicidal behaviour that you can refer to in order to make your writing more realistic or true to life (and you're right, literature on such real and sensitive topics doesn't always need to invoke comfort, or provide a lesson of sorts to the reader. Because simply depicting the realities of many people is enough - or more than enough - and is very important, even if it makes people uncomfortable... because it IS not a comfortable topic). Needless to say, each person has varying experiences.
Attitudes toward suicide have varied throughout history and vary considerably among different cultures.
The ancient Greeks considered suicide an offense against the state, whereas the Romans believed that suicide could be a noble way to die.
The view of suicide as a sin prevailed in Western societies for hundreds of years.
Only since the later decades of the 20th century did suicide cease to be considered a criminal act.
Suicidal Behavior - term used for individuals who have engaged in potentially self-injurious behavior with at least some intent to die as a result of the act. Evidence of intent to end one’s life can be explicit or inferred from the behavior or circumstances. A suicide attempt may or may not result in actual self-injury.
Levels of Suicidal Behavior
completed suicide
suicide attempts that are potentially fatal
suicide gestures—behaviors that are not necessarily lethal but are a cry for help or attention, such as superficially cutting one’s wrists
suicide gambles—attempts in which people gamble that their lives will be saved through intervention, such as a fatal but slow-acting drug overdose
suicide equivalents—behaviors that invoke responses similar to those seen with suicide, such as a teenager running away from home as an indirect call for help
suicidal ideation or thinking about suicide, which can range from nonspecific thoughts that life is not worth living to specific suicide planning
Mental illness is a major risk factor for suicide.
More than 90% of Americans who commit suicide have been diagnosed with a psychiatric illness and/or have problems with substance abuse, especially alcohol, opiates, and cocaine.
Schizophrenia, bipolar disorder, and borderline and certain other personality disorders are risk factors.
People are at particularly high risk for suicide during the first week following discharge from a psychiatric facility.
Other suicide risk factors include individuals who:
are victimized by bullying
are isolated from other people and community
have a family history of suicide
have a history of attempted suicide
have a history of childhood abuse or family violence
have had traumatic experiences
have experienced stressful events, such as separation or divorce, job loss, or death of a spouse
have a chronic or progressively debilitating disease or condition; chronic, severe, or intractable pain; or loss of mobility or independence
have access to a firearm
are victims of alcohol or substance abuse, which weakens impulse control
have low total serum cholesterol
reside at a higher altitude, possibly due to altitude-related metabolic stress in individuals with mood disorders
are involved with the criminal justice system, or are incarcerated (especially during the first hours or week of imprisonment)
have sleep problems and disorders
are impulsive
have been exposed to suicidal behavior in others, including family members, peers, or friends (especially among adolescents) or celebrities, which is referred to as contagion
take certain medications
live in low-income households or in poverty
are unmarried
are lesbian/gay/bisexual/transgender (LGBT)
CAUSES. Suicide results from combinations of factors specific to each individual.
Studies have found a connection between genetic factors and suicide.
Some suicides appear to be impulsive acts, whereas others follow a major life event or crisis. However, the most common trigger is the pain and desperation of a mental illness, often unrecognized and untreated depression or bipolar disorder.
A complex of illnesses involving changes in the brain, depression is very common in the general population. People in recovery programs are often at particular risk.
Many people with depression develop anxiety disorders, which can further contribute to suicidal thoughts or behaviors.
Depression is particularly dangerous when the individual is emerging from the darkest depths of the disease and has the energy to act upon suicidal impulses.
Suicidal depression is not always obvious. For example, some depressed men appear irritable or angry rather than depressed. ‘‘IS PATH WARM?’’ is a mnemonic for signs of suicidal behavior:
I—ideation
S—substance abuse
P—purposelessness
A—anxiety
T—trapped
H—hopelessness
W—withdrawal
A—anger
R—restlessness
M—mood changes
Other signs of suicidal intentions are:
isolation or withdrawal
emotional distancing
lack of family or friends
distraction, seeming to be in one’s own world
lacking any sense of humor
dwelling on the past, especially losses and failures
feelings of hopelessness and helplessness
preoccupation with death
You can refer to a mental status review used by clinicians to guide you in describing your character. This includes:
appearance—the patient’s clothing, personal hygiene, and any physical evidence of self-harm
affect—expression, emotion, and intonation when describing plans for self-destructive behavior
thoughts—suicide command hallucinations (usually auditory); delusions about the benefits of suicide, such as thoughts that relatives will be better off after the person dies; and obsession with suicide
homicidal potential
judgment, insight, and intellect
orientation and memory, including signs of delirium or dementia
The need for suicide intervention is assessed by the following:
ideation—whether the patient has thoughts of self-harm
plans—the more specific the suicide plan, the greater the risk
purpose—what the patient believes will be achieved by suicide
potential for homicide
NOTE: The clinician will also evaluate risk factors as described above.
Most people give clear warnings of their suicidal thoughts; however, those around them may not recognize the significance or may not know how to respond. People who are concerned that a family member or friend is at risk for suicide should do the following:
educate themselves about warning signs and risk factors
identify healthcare professionals who know the person and can help
call 911 or the local emergency number if the person seems to be at immediate risk
Factors that lower the risk of adult suicide include:
a significant friendship network outside of the workplace
a stable marriage
a close-knit extended family
religious faith and practice, especially religions that value life and discourage suicide
a strong interest in or commitment to a project or cause that encourages social interaction and cohesion
One of the "Conditions for Further Study" in the DSM (Diagnostic and Statistical Manual of Mental Disorders) is Suicidal Behavior Disorder (SBD). This is NOT an official diagnosis yet, but research is ongoing. I'll include here a few proposed criteria and potential diagnostic features, just for reference purposes:
A suicide attempt is a self-initiated sequence of behaviors by an individual who, at the time of initiation, expected that the set of actions would lead to his or her own death. (The “time of initiation” is the time when a behavior took place that involved applying the method.)
Determining the degree of intent can be challenging. Individuals might not acknowledge intent, especially in situations where doing so could result in hospitalization or cause distress to loved ones.
Markers of risk include:
degree of planning, including selection of a time and place to minimize rescue or interruption;
the individual’s mental state at the time of the behavior, with acute agitation being especially concerning;
recent discharge from inpatient care; or
recent discontinuation of a mood stabilizer such as lithium or an antipsychotic such as clozapine in the case of schizophrenia.
Examples of environmental “triggers” include:
recently learning of a potentially fatal medical diagnosis such as cancer,
experiencing the sudden and unexpected loss of a close relative or partner,
loss of employment, or
displacement from housing.
Conversely, features such as talking to others about future events or preparedness to sign a contract for safety are less reliable indicators.
Again, the above excerpt is for a proposed criteria and potential diagnostic features for SBD (not yet an official diagnosis).
I'll include here a few interesting studies on SBD. Some researchers aren't for it. Most are discussing the current lack of data and research on it. 1 2 3 4
Also I think I misunderstood your request when I first read your message. I thought you wanted to write a suicidal protagonist but they're not depressed. But just in case, here are a couple of articles exploring suicidal ideation in non-depressed individuals. I would recommend looking into the qualitative findings as this could help writers if this is the topic you want to write about. 1 2
Lastly, since this is quite a sensitive topic, it is advisable for you to keep in mind conscious language, particularly when you're planning to share your writing with a wider audience and when publishing. Editors and publishers also frequently advise to get a sensitivity reader. Because while you might have the best of intentions, if you’re dealing with serious issues that real people deal with, it would be a good idea to do some research or get a sensitivity reader. Or both. Here's an excerpt from that previous post:
Words have power. Where and to what degree that power has an impact will inevitably depend on who the reader is. Words can drive a story forward and compel the reader to turn the page. Or they can disengage readers, even hurt them, and compel them to, at best, reject the novel; and at worst, review it negatively. Doing the awareness work prior to publication can help to prevent this while at the same time improving knowledge and craft.
Sources: 1 2
Hope this helps. And thank you for writing about such an important topic.
#anonymous#character development#character building#original character#writeblr#writers on tumblr#literature#poets on tumblr#writing prompt#spilled ink#dark academia#poetry#psychology#studyblr#light academia#fiction#creative writing#writing reference#writing tips#writing advice#writing resources
65 notes
·
View notes
Text
Welp, I talked with my doctor and we've decided that it's about time to admit my family's strong history of genetic cardiovascular disease is starting to catch up with me. I've known it was coming since I was a kid but I'd been hoping I could at least make it to 30 first!
I'm in my late 20s, and I know that sounds young for this kind of thing, and to clarify I'm absolutely 100% fine right now, but literally not a single man on my dad's side of the family has reached 40 without at least one heart attack. My grandpa had his first one at 26, a few years younger than I am. We've just got a very very strong genetic history of heart disease and I knew it would find me eventually. I get my blood work checked often because of this, especially knowing that being on testosterone would raise me to the risk levels of a cis guy, and we've finally decided my cholesterol is just too high.
It's just a little scary, to be on a statin to lower cholesterol at my age, and I can't help but wonder how long it's going to be until it gets more serious. My blood pressure is absolutely fine and my levels aren't even at the point where they'd usually start medicating for, they're just going ahead and doing it now given my family's history, so I'm not, like, at risk of imminent death or anything, but it's just really freaky.
#and before anyone tries to be a doctor at me: i promise i've been conscious about a heart-healthy diet and exercise my entire life#it's genuinely just genetic#personal
36 notes
·
View notes
Text
hey you scrollin there i have an important life tip
if you are still in contact with your parents, or you have access to your family's medical history, this is a good question to ask that you never really think of until something happens
"Does my family/Do we have a genetic history of anything I should keep an eye out for?"
Because the average tumblr user that stuck around before the twitter exodus is now reaching that 23-30 range, and that's when your body starts needing regular maintenance and if you don't- the 35-40 range is when issues start popping up.
I've known that my family has had a history of two types of cancers. Breast cancer from one side, thyroid cancer from both, so I've been wary of those and keeping an eye out in the back of my mind. RECENTLY I've also learned that my family has a history of high cholesterol and a few other things (my genetics are a fun smorgasbord of conditions and disorders :D.) I am glad I've found out about these things now so they don't end up being an expensive trip to the hospital later... or at least a less expensive trip.
BASICALLY, if you have the resources, ask about your family's genetic medical history before your body lets you know for you and consider any preventative habits you can start to prevent anything becoming a major problem later.
aighty you can go back to ur scrollin, thankee for readin 👋
476 notes
·
View notes
Text

Why so Many F*cking Lemons??
National Treasure is the kind of film that presents many mysteries and asks its viewers the hard questions. Questions like:
What if there was a treasure map on the back of the Declaration of Independence?
What if American history was a cool connected puzzle?
What there was a big ol' treasure?
But most importantly it asks us to consider:

4. Why does Patrick Gates have a whole fridge full of lemons???
Now the most obvious answer here is because the plot demands it. Ben and co need to cover the whole back of the Declaration in lemon juice, (although do they?) so they have to have enough lemons on hand.
The second most obvious reason is because the cinematography demands it. I mean this shot looks a lot better than, like, a single lemon. (Probably the same reason for Dakota Johnson's bowl of limes. It looks better.)
But neither of those answers are very fun, so let's dig deeper.
What is the plausible, in-story reason why Patrick Gates has a bowl of lemons?
Theory 1: Patrick Gates is a connoisseur of homemade lemonade
According to this hypothesis, Patrick loves homemade lemonade so much that he makes it for himself on the semi-regular. Yes, it's like October, but why should that stop him.
Does this check out?
When we meet him, Patrick is hanging out alone in his bathrobe late on a Friday night, having had pizza for dinner and something from a soda fountain to drink. That doesn't strike me as a foodie who wouldn't just buy lemonade if he wanted some.
Theory 2: Lemon Fish
In this version, Patrick is about to grill some fish. There's a way to do it (which is really tasty, and doesn't require a grill pan or rack) where you place bunch of slices of lemon directly on the grill grates and grill the fish on top of them. The fish doesn't stick and it imparts a delicious citrus flavor.
But again, we run into the same plausibility issues:
it's autumn
the Patrick Gates we meet here doesn't seem dedicated enough to the food he eats to do through the somewhat tedious process of grilling fish, especially not in not-summer
Theory 3: Cards with the Boys
What if Patrick is part of a weekly rotating card game? It's maybe a few masons he knows from his treasure hunting days and some of the guys from the insurance company (I don't know what I think that Patrick sells insurance, but I guess that's the most 'square' job I could come up with).
They rotate houses every week or month, and it's soon to be Patrick's turn to host. The drink of choice amongst the group is whisky sours, tom collins's or another straightforward drink that requires lemon juice.
This at least I think is more plausible with what we see of Patrick's lifestyle than an explanation with a more foodie-type bent. With Ben and his ex-wife both out of his life, Patrick must be a pretty lonely guy. I like the idea of him having a circle of friends.
Theory 4: Health Benefits
And here I think we have the most plausible answer: that Patrick might be interested in the health benefits associated with lemons and drinking lemon water.
Different compounds in lemons can have benefits regarding
lowering cholesterol
managing blood sugar
kidney health
and more, but those are the ones I suspect Patrick might be interested in. He's of a certain age, lives alone, and (unless we caught him on an off night) might not take the best care of himself as far as his diet. Perhaps he's been found to have high cholesterol, is pre-diabetic or has other blood sugar concerns, or has the decreased kidney function that can be associated with aging.
Perhaps he's had kidney stones or another health issue or scare in recent years and is attempting to take better care of himself.
Maybe that soda fountain cup is full of lemon water.
Conclusion
While all of these are plausible to various degrees, I find myself more interested in the last two. Patrick as an aging man without any family (or at least not any family who still speaks to him), living alone and becoming concerned with his health is heartbreaking, but I think adds a certain softness to the character, and extra layer to him and to his reconciliation with Ben.
And in any case, I also like the idea that he hasn't been completely alone since his falling out with Ben. While Patrick does behave in a way that suggests a fairly traditional 'breadwinner,' family man masculinity, we at the National Treasure Gazette will always stan platonic relationships and social supports. I'd like to believe that Patrick has his own squad of friends he can rely on.
I don't think I've ever thought about Patrick Gates this much, but now that I have, I find myself kind of wanting to give him a hug? He may not be the easiest character to love, but he has his own struggles.
What about you?
What are your theories regarding the lemon bowl?
I'd love to hear in a reblog, reply, tag, etc!
12 notes
·
View notes