#Eye genetic disorders
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
China blocked Tumblr because of pornography and censorship problems in 2013.
Text
The Role of Genetics in Glaucoma: Unraveling the Connection
Genetics plays a pivotal role in glaucoma, an eye genetic disorder. Inheriting certain genetic variations can increase susceptibility. Understanding these genetic factors helps tailor preventive measures and treatment strategies.
#Eye genetic disorders#genetic eye disease#is glaucoma hereditary#cause of blindness in India#Glaucoma genetic inheritance#Glaucoma genetic testing#How to prevent glaucoma#Glaucoma inheritance pattern#average age for glaucoma
0 notes
Text
Blindness Insight
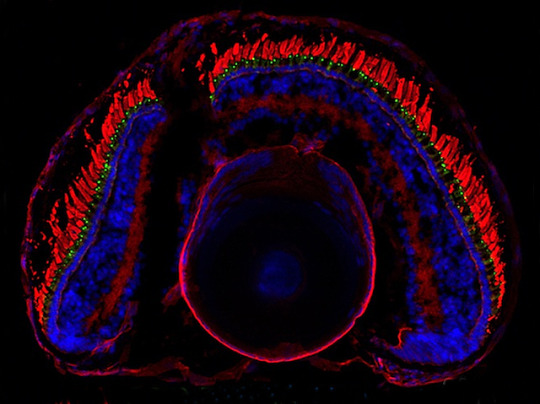
A study in the model organism the African clawed frog (Xenopus laevis) reveals the details of mechanisms underlying the human inherited retinal degenerative disease Leber congenital amaurosis.
Read the published research article here
Image from work by Theresa Fresquez and colleagues
Department of Ophthalmology and Visual Sciences, University of New Mexico, Albuquerque, NM, USA
Image contributed by the authors under a Creative Commons Attribution 4.0 International (CC BY 4.0) licence
Published in Journal of Cell Science, January 2025
You can also follow BPoD on Instagram, Twitter, Facebook and Bluesky
#science#biomedicine#immunofluorescence#biology#eyesight#eye disease#congenital disease#genetic disorders#frog
7 notes
·
View notes
Text
sometimes it pains me knowning that genetics is so vastly complex and heavily effects the way we live our individual lives but the primary people who care about this are eugenicists and not people who are just curious about the variety in human bodies
#my father is a couple inches shy of being diagnosed with dwarfism and i ended up being tall like my mom#but have the proportions of a short person#this has resulted in my skull being larger than 99.5% of the population's skulls#you can very clearly see the outline of my skull around my eyes and cheeks#and my brow and cheekbones are so prominent that it makes my eyes look sunken in#but i'll never know if this is just normal genetic expression in my family or if i have a growth disorder#because if it's not causing me to be incapable of participating in capitalism it's not considered worth knowing#and most of that side of the family is dead so i can't even talk to them to find out if other members of my family are like this
2 notes
·
View notes
Text
#except i watched queer eye yesterday#of an 18yr old who lost her entire family - siblings and parents - through the years to a genetic disorder#and the end of the ep ended with a memoriam bc she died herself a year after filming#and so that was a giant bummer and not the uplift i was looking for!!#queer eye#queer eye germany
50 notes
·
View notes
Text
The Science Diaries of S. Sunkavally, p 637.
#fimbria#genetic disorders#mental retardation#George Sacher#brain size#lifespan#foetal alcohol syndrome#alcohol#acetone#ginger#garlic#blood thinners#NADPH#myoglobin#obesity#xenon#krypton#argon#anaesthetic#retrolental fibroplasia#oxygen treatment#eye lens#high protein intake#kidney function#shark#urea#Ice Age#superoxide dismutase#superoxide
0 notes
Text
Unlock the secrets to clear vision with Prasad Netralaya! Our revolutionary eye care solution is specifically designed to tackle hereditary and genetic eye diseases. Say goodbye to blurry vision and hello to crystal-clear sight. With our cutting-edge technology and expert team, we're here to help you understand the genetic factors behind your vision problems. Take control of your eye health today and see the world in a whole new light with Prasad Netralaya!
0 notes
Text
Warnings for infertility, sub!johnny, dom!simon, oral sex, PIV sex, breeding, pregnancy mention 18+ MDNI
Thinking about trying for a baby with Simon but having issues convcieving so you both go to the doctors and get test done and find out Simon has an incredibly low sperm count and while its not impossible for you to get pregnant with Simons babe, it would be incredibly difficult. So you weigh up your options, talking about adopting and IVF, and while your both open to adopting you want to experience pregnancy but neither of you really want a random unknown donor who could have god knows kind of genetic and herititary disorders. You decide you want someone you know, someone you trust, eventually settling on Johnny. Hes Simons best friend after all and you both trust him immensely. When you go to ask him about he, hes happy to say yes all he has to do is jerk off into a jar and the doctors do all the rest. But then you inform him that no, you don't want to do it through doctors and stuff, you want him to fuck you and knock you up. Its less invasive that way, less stress on your body where you would be poked and proded and filled with hormones for egg extraction and stuff, and definitely far less expensive. He blushes a bright tomato red when you tell him this, stammering around an answer because he has always wanted to fuck you but you're Ghosts girl and he wouldn't do that to him and know hes been presented the perfect opportunity to do it. It stammers out a yes, not meeting Simons eyes, instead staring at your radiant smile.
Very soon after this, Johnny has you naked on his bed, legs spread as his head is buried between your thighs while Simon guides him with his hand and words, after all Simons 'gotta teach him how to fuck his girl right'. Simons fisting his cock as he watched you come undone under Johnnys tongue, eyes glazed over and switching between your look of pure pleasure and the way Johnnys laps at your clit and hole like a man starved and you were his first source of nourishment. After you've came twice from Johnnys tongue and fingers, Simon grips his hair by the roots and pulls his head up and Johnnys tongue lols out of his mouth and he pants like a dog, your cum soaking his chin and stubble and Simon has to stop himself from leaning down and licking the it and maybe even kissing Johnny to taste you on his lips (he decided in that moment, he would do that another time because there was going to be another time) and talks Johnny through fucking you. What angles you like, what pace to go at, how rough he can get with you and how you like for him to push down on your stomach when hes deep inside you. Then he sits himself on the chair facing the bed, hand wrapped tightly around his cock as he watches Johnny fuck you, matching Johnnys pace and barking out orders like they were on the field. The three of you cum at the same, Johnny pressed right against your cervix to ensure he gest his cum as deep inside you as possible (to help maximise your chance of getting pregnant of course and not for any other reason) and the moans you let out are harmonious and beautiful. Just 3 people reaching the same state of ecstaty.
And thats just the first time you fuck, after all it doesn't always work on the first try and maybe you'll continue on even after your pregnant.
#Cod x reader#Cod smut#Call of duty x reader#Call of duty smut#Ghoap x reader#Ghoap smut#Johnny mctavish x reader#Soap x reader#Johnny mctavish smut#Soap smut#Johnny soap mctavish x reader#Johnny soap mctavish smut#Simon riley x reader#Simon riley smut#Simon ghost riley x reader#Simon ghost riley smut#Ghost x reader#Ghost smut#Tw. Breeding#Tw. Pregnancy#tw. exhibitionist#Tw. Infertility
1K notes
·
View notes
Note
Hi! This is a request. Something along the lines of Reader sitting on Spencer Reid’s lap as he talks about his special interests and his hands happen to wander all over your body. Make it as smutty or fluffy as you’d like! Thank you!!
wandering • S. Reid
Make it as smutty or fluffy as you’d like, you say??😈😈 I say both. full disclosure, I did write him a bit more dom then my usual. Ty!
word count: 1185
———————————౨ৎ———————————
Spencer liked to talk. a lot.
It bothered people, very frequently actually- but you on the other hand? You thought it was charming. Spencer liked that about you, you were always willing to listen. No matter what station his train of thought was rolling through that day- you’d be there, head resting in your hands, nodding and commenting, your eyes never leaving his.
This particular day, his mind was set on rare neurological disorders. You were sat in his lap on the couch, fidgeting with the ends of his sleeves while he spoke. A nature documentary was playing on your tv, but neither of you were paying attention, so much so you had turned the volume off.
“Oh, another one-“ he grinned,resting his warm hands on your waist. “Metachromatic leukodystrophy. It’s genetic, actually- autosomal recessive.”
“Oh, what does that one do?” You queried, doing your best not to sound disinterested although you were preoccupied with his fraying sweater seams.
“Basically, our brains and nerves are very delicate. There’s a substance called lipids that build up frequently on the brain, spinal chord and peripheral nerves-“ he interrupted his own sentence to place a small kiss on the crook of your neck, sending warmth down through your collarbones. Despite the loving gesture, you frowned.
“That’s sounds scary.”
“It is, it is. Luckily, we all have enzymes whose sole jobs are to break down those lipids. People with Metachromatic leukodystrophy-“
You interrupted with a guess, raising your head to meet his eyes. “Don’t produce the enzymes?”
He grinned. “Exactly, love.”
“I guessed.”
“Well-“ he shrugged. “It was a good guess.” He pressed a kiss to the corner of your lips, going back to his rant.
“Oddly enough, it actually has similar symptoms to Kuru disease- that’s the one that causes tremors. Only lipids don’t eat away at the tissue,” his hands slowly slid up your sides, caressing your arms and trailing along the curve of your breasts. “..they just block it off.”
You giggled a little at the touch, face warming as you shifted in his lap.
“Stop it.” He said softly, with a smile, guiding your hips down. “It causes a lot of terrible symptoms, anyway. Loss of senses- the most interesting being an inability to detect pain.”
He sneaked another kiss to the side of your neck, a hand moving up to push your hair out of the way.
“It was discovered in the early 20th century, and three forms emerged. Infantile,” his hands slid down your sides, lips pressing quick, sloppy kisses to your jawline.
“juvenile,” as his hands slipped over your thighs, caressing the skin, “and adult.” As his hands expertly pushed your knees apart.
Your breath hitched. “Mhm, spence-“
He sighed through his nose. “Are you listening?”
“yeah, yeah, I am, just- keep going.”
His chin rested on top of your head as he firmly grabbed your hips, spinning you around so your forehead was against his chest, your legs straddling him.
“okay. Pay attention- back to MLD. The infantile form is, of course, the worst, it progresses the quickest and the symptoms are often the most brutal, particularly-“
His hands slid between your thighs, sending a rush up your core, and you pushed your head into his chest a little in a sad attempt of soothing your nerves.
“particularly seizures. Because of this, it’s misdiagnosed often, usually for some form of epilepsy.”
Was he really going to do this? While lecturing you about seizures? Jesus, this boy was going to kill you someday.
His fingers traced along the lace of your panties, one hand situated between the plush of your thighs, one on your waist. The contrast between the movements of his hands and the subject matter leaving his mouth was giving you whiplash, but you were so desperate for any kind of physical attention you let him continue speaking.
“There’s no cure, obviously, there rarely is for anything genetic and neurological.” He spoke, tone never faltering- even as his hand pushed your panties to the side, running along the slick of your folds and pressing a small circle to your clit- causing fireworks to erupt in your core and causing you to let out a long whine, muffled by the fabric of his shirt.
He pinched your side, gently, just as a reminder. “Shhh, love. Don’t you want to hear what I’m saying?”
you managed a shaky nod.
“Good.” He spoke simply, his fingers continuing to work expert circles into you.
“Anyway- before I was interrupted, I was going to say- there’s no cure, but there’s ways to keep the patient comfortable.”
At this point his voice was sure, constant and gentle, causing you to nearly have to strain to hear him correctly. His hands never faltered- and your muscles clenched, thighs tightening around him as the smell of his cologne enclosed your senses.
Your breath was quick, quieted whines and whimpers peaking through, although muffled by the thick material of his sweater. He continued. “Research, mainly in Europe, is proving stem cell treatment to be beneficial.. but that’s mostly in younger patients.”
Your breath hitched when his fingers just slightly trailed down, circling around your entrance and slowly pushing in as his voice persisted.
“a-ah!”
“Shush. You really need to listen, baby.”
His fingers pushed in and out of you, speed never falling even once. “There’s a drug, that was also developed in Europe- called Atidarsagene autotemcel.”
Your hips circled, his fingers curling as he worked you up to the edge. A choked moan escaped your lips, which he ignored.
“baby, cmon- I was saying, since metachromatic leukodystrophy affects the ARSA gene, the treatment takes hematopoietic stem cells from the patient and genetically modifies them to contain a fake, corrected ARSA gene-“
You moaned into his chest, your thighs clenching tighter around him- one hand flattening onto his back for purchase as his ministrations continued, pulling you closer to your inevitable climax.
“g-god, Spencer, can you just- please,”
His movements sped up. “Please, what? I don’t think you even know what you’re asking for, baby. You don’t have to worry, I don’t plan on stopping.”
You were lost for words, breath leaving your chest as his words began to blur together. You babbled something out, your back arching as fireworks lit up your nerves, pleasure washing over you in the midst of your climax.
“s-Spence!”
You pushed your forehead into his chest as his fingers worked you through your orgasm, his free hand coming up to gently hold the back of your head.
“shh, I know,” his hands withdrew from you, slipping out from your thighs and out from under your skirt. He grabbed your chin and allowed your lips to open, pushing his fingers into your mouth. “Here, taste yourself.”
He watched, desire in his eyes as you licked them clean, your cheeks hollowing. He slipped them out from your bruised lips and pressed another kiss to the top of your head.
When you lifted your still-trembling legs to get off his lap, he furrowed his brows, pouting.
“You’re leaving? I was just about to tell you about prions.”
———————————౨ৎ———————————
879 notes
·
View notes
Text
Facial Differences that You Should Consider Representing in Your Writing More
[large text: Facial Differences that You Should Consider Representing in Your Writing More]
As it has been said many times on this blog before, facial differences are a very wide spectrum - there’s thousands of conditions that cause it, and they’re often extremely different from each other. It’s an incredibly diverse category almost by definition. But…
In books, movies, and our inbox, it seems that a traumatic battle scar is the only facial difference that exists. I find this rather frustrating because I would like to see the real life diversity to be actually considered by writers when creating characters - and that’s exactly what this post is for. I hope that by making people just aware of the myriad of options they have, I can help a bit.
This isn’t to say that you shouldn’t write characters with scars, it’s to say that there’s more for you to consider. Just like not every physically disabled person has hip dysplasia and not every neurodivergent person has epilepsy, not every person with a facial difference has scars.
Of course, this list isn’t exhaustive - no such list exists, it would be like “list of every disability ever”, it simply can’t be done. This is just a dozen random facial differences that I would like to see incorporated into characters more often.
Facial paralysis Exactly what the name implies. There are many types of facial paralysis - complete, partial, bilateral, unilateral, chronic, acute, and it can affect the whole face, or only part of it. Sometimes it can cause problems with speech or dry eyes (mostly the latter), but it’s frequently just primarily a visual difference. A person with facial paralysis might be completely unable to make facial expressions at all if it’s severe, or have a lop-sided smile and inability to raise an eyebrow or control an eyelid like me. Causes include cranial nerve damage (especially the 7th nerve, which is called facial palsy), Bell’s palsy, Möbius syndrome, or multiple sclerosis! It can be congenital, like in my case, or acquired, like in most cases - mostly due to stroke. Here I would write something about the current media representation being good, bad, or what tropes to look out for but I don’t know a single character with it. So :-)
Anotia/microtia Microtia is a congenital facial difference that affects the outer ear(s) - as the name implies, they’re smaller than average; anotia means a complete lack of them. This usually will also result in being d/Deaf or hard of hearing in that ear, as the ear canal can be smaller or closed (depending on the “grade”). People with microtia who decide on using hearing aids will usually wear a bone-anchored hearing aid, which looks very differently from the “regular” HA; it’s worn with a headband. Microtia can be the only facial difference that a person has, but it can also be a part of Goldenhar syndrome, Treacher Collins syndrome (mentioned below), or hemifacial microsomia.
Congenital Trochlear Nerve palsy I have a subtype of this, and because it happens to have the most boring name in existence I have never seen anyone talk about it, certainly not see a character with it. So; CNIV palsy (again, an incredibly catchy name) is a disorder of one of the very easy to damage nerves that allow eyes to move. It causes constant double vision, severe strabismus, and progressive facial asymmetry. A person with CNIV palsy will have a 24/7 head tilt to the side and will have their chin tucked in, which causes said asymmetry - facial features on the side of the tilt will sag down, the eye will “sunk” in, and because it’s congenital, the jaw can grow to be misaligned (like mine). Over time, it causes neck pain and kyphosis, so add chronic pain to that. Trochlear nerve palsy can be congenital, acquired, traumatic, and even extremely rarely genetic (that’s me, allegedly <1 in a million). However, most acquired cases are only temporary, and “fix themselves” with the passage of time. Again, I would love to write something about CNIV palsy representation, but I’m confident it literally doesn’t exist : )
Sturge-Weber syndrome The most visible part of SWS - that you might be familiar with - are port wine stains. In this syndrome, they tend to be large and generally cover the forehead-eye area. Around 15% of people with any kind of port wine stain on their face have Sturge-Weber syndrome, and even more when it comes to larger ones. Most people with SWS will have epilepsy since childhood, and many will develop glaucoma (which causes blindness) if the PWS is around that eye. Hemiparesis (one-sided weakness) can also sometimes happen on the opposite side of the PWS. Here is a short article about media representation from a person with SWS.
Cystic Hygroma Also known as lymphangioma, it is a bump that mostly happens on a person’s lower face and/or neck. It’s almost always congenital and a result of a blockage in the lymphatic system (thus lymphangioma). Sometimes, if it affects the mouth or jaw, it may cause a speech disability where the person’s speech might not be fully understandable, or cause an airway obstruction; this generally means that the person has to have a trach tube in their neck to breathe. Here is a short article about living and growing up with cystic hygroma by Atholl Mills.
Congenital melanocytic nevus A complicated name for a specific kind of birthmark. Melanocytic means related to melanin, so it’s a black or brown birthmark that can show up on any part of the body and be of almost any size. Sometimes it can be hairy as well. While CMN doesn’t usually cause any problems, people who have it can have a higher risk of skin cancer, epilepsy, and brain tumors (if it's on the head). Here is a short article on representation - among other things - by a person with CMN.
Ptosis Ptosis is actually really common - I can almost guarantee that you have seen someone with it - but for some reason it never shows up in media, unless it’s to show that a character is under the influence or vaguely creepy. Ptosis is simply a drooped eyelid. It’s caused by damage to the third cranial nerve, which can be congenital, acquired, traumatic, etc. It’s very common in myasthenia gravis and CHARGE syndrome. In most cases ptosis is a visual thing, but it can sometimes cause problems - for me, it partially obstructs my vision and for some people who acquired it later in life that can cause pain (due to having to constantly lift the eyebrow). Ptosis is often misunderstood, and people tend to make bizarre assumptions about those of us who have it - even Wikipedia cites “looking sinister” as a symptom (not that I particularly trust Wikipedia as a source, but it shows the general public’s view quite well). In real life, we are normal people and all these “drunk/high/rude/evil” associations aren’t true at all.
Treacher Collins syndrome You have probably seen a person with TCS at some point, as it’s not that rare. This is a genetic, congenital disability that affects the development of the face. The bones of the jaw and cheeks are underdeveloped, eyes have a downturned shape, and microtia/anotia is often present as well. A lot of people with Treacher Collins are d/Deaf or hard of hearing. Sometimes, the small jaw might cause problems with breathing, which is why a lot of people with TCS will have a permanent tracheostomy tube in their neck. Similar to ptosis, eyes in TCS are often seen as “looking sad”, but that’s an incorrect assumption - that’s just how they look like. The main and only big representation of TCS in media is that one awful movie from a few years ago, that was literally just inspiration porn featuring an able-bodied actor based on a shitty book, made by an author with some sort of abled-person guilt. Very cool, don’t do that.
Crouzon syndrome Crouzon syndrome is a type of craniosynostosis; a congenital condition where a person’s skull fuses too early. There are other disabilities that can look somewhat similar, like Pfeiffer or Apert syndrome, but they are different!. CS will affect the person's skull - it will be taller than usual, eyes - they will be large and bulging, midface - it's often smaller than average and can look sunk in comparison to the jaw and forehead, and more. Sometimes people with Crouzon syndrome are d/Deaf or hard of hearing (very common with craniofacial differences), or experience long term effects of hydrocephalus, which happens fairly often. Here is a short article by Mikaela Moody about movie representation - and her piece on how it to be trans while having a facial difference, which I relate to a lot and wanted to share.
Phthisis bulbi Phthisis bulbi is something that I have mentioned on this blog before, as it logistically should be represented way more often in fiction than it currently is. It's also known as the “end-stage eye” which is a metal name. This is an ocular difference that can result after trauma to the eye. It can also result from a million other things, but trauma is apparently the most common thing to happen to an eye in fiction. With phthisis bulbi, the eye shrinks, sinks, and everything inside becomes stiff; this is permanent, and the eye isn't functional anymore - it's blind and unable to move. The only treatment is to have the eye removed, especially if it causes pain. If you're writing a character who got a Hot Sexy Scar over their eye and still has that eye, they probably should have this (and yes, the “shrunk and sunk” part is mandatory, you can't just make the eye lighter and call it a day).
Frontonasal dysplasia Frontonasal dysplasia is a congenital facial difference that affects the structure of the face. While it's a spectrum with a lot of variety, most people with FND will have hypertelorism (eyes spread widely apart), a flat and broad nose, and a cleft going through the middle of the nose. Other facial clefts (not necessarily just cleft lip) are also common. Sometimes, someone with it can also have cranium bifidum (meaning a brain/meninges that protrude through the skull, similar to how spina bifida works), or intellectual disability related to the potential absence of corpus callosum. Rarely, limb differences can also be a part of it; absent tibia, extra toes, or clubfoot. Again, I’m unaware of any representation of FND outside of “scary birth deformity” on medical shows =)
Parry–Romberg syndrome PRS is also known as progressive hemifacial atrophy, which is a much more descriptive name. It’s an acquired facial difference that people just get for unknown reasons, mostly before the age of 20 and usually between 5 and 15. Generally, PRS is considered to be slowly-progressing, but this can vary pretty widely between different people. As the name implies, it causes atrophy in the face, which affects everything from skin to fat and muscles to sometimes even bones. Some people will also experience skin darkening, alopecia (hair loss), or trigeminal neuralgia (very severe nerve pain) on the atrophied side. The difference between the two sides can be very pronounced, with a visible line between the halves showing up on the forehead. Again, no existing rep that I know of =)
And as always, I recommend this short PDF that in my opinion any writer who wants to include a character with an FD has to read. Additionally, you can also check our #face difference tag, this primer on facial difference, or this piece on making sure you’re not contributing to disfiguremisia.
Also apologies for the amount of “idk what to say about already existing rep because it literally doesn’t exist” but I hope it illustrates the problem =)
Happy Face Equality Week,
mod Sasza
#mod sasza#face difference#disabled character ideas#writing guide#writing resources#writing advice#writing help#face equality week#long post
899 notes
·
View notes
Text
eye strain warning
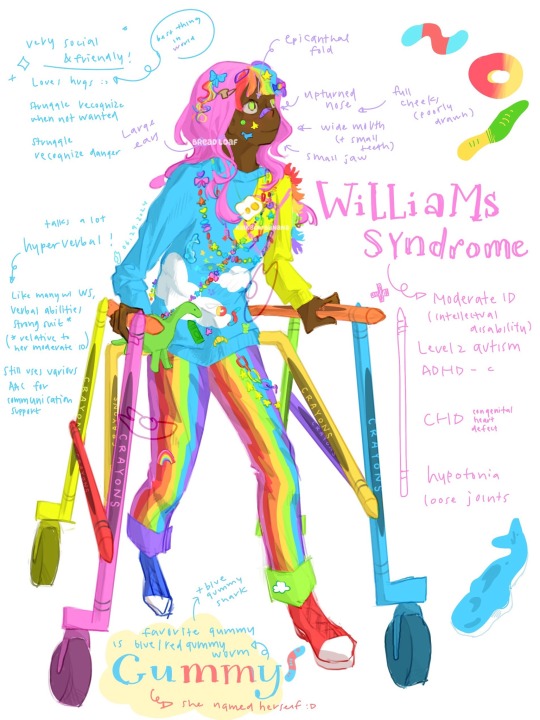
gummy 🌈🐬
[plain text: gummy 🌈rainbow emoji🐬dolphin emoji]
(^ shark emoji not blue enough)
[id: dark skinned black person with williams syndrome in decora kei fashion walk with posterior walker. person have pink hair with rainbow bangs n all sorts hair clips in hair & stickers on cheek. have many rainbow necklace include one with double yoke egg. wear blue sweater with white cloud where one sleeve is yellow horse with pink leash thing. there many pins on sweater include gummies (gummy shark, peach ring, gummy worm, gummy bear) & green crayons & others. she wear cross body green dino plushie (bag?). rainbow vertical stripe pants with rainbow n star chain. one shoe red one shoe blue. posterior walker made of different color crayons. there text around character describe her which be functionally described below. end id]
🌈🐬.
girl (complicated gender) with williams syndrome n love decora kei fashion & bright colors (she call them happy colors/excited colors)!! she has lotssss of bows n head pieces n hair clips n necklaces n bracelets n other decoration & big wardrobe with bright colored clothing! she love wear different outfits but it consistently decora kei.
she love gummy candy & named herself after them >:) blue/red gummy worm & blue gummy shark her favorites (blue gummy shark also my favorite. to look at.)
williams syndrome (also known as williams-beuren syndrome) is genetic developmental disorder micro-deletion of some of chromosome 7. for gummy, WS lead her have moderate intellectual disability (ID) & global developmental delay, level 2 autism, ADHD-c; congenital heart defects (CHD); hypotonia (low muscle tone), & loose joints.
like many people with WS, gummy very friendly & social! she love hugs & talking to people & talk lot & very physical in show affection! but also often struggle tell when other people not want be social / be social with her, be called “a lot” & “too much,” which lead her have trouble make n keep friends n make her sad—even tho WS make her extra outgoing, she also still get sad n mad n not hide it. she also struggle with danger awareness & often treat strangers like would with friend, n it been something that her support team very focused on work with her entire life because this lead her be very easily taken advantage of n be put in danger.
also like many ppl with williams syndrome, language & verbal abilities her strong suit—tho it’s relative to her moderate ID, so one shouldn’t expect she write speak communicate like average person without struggle. her words more simple, n still need many help for communication, including various form of AAC & aide person.
she has aides that pretty much 24/7 present because WS & moderate ID but working on skills so can be more independent! it something she been work very hard on entire life n she quite proud of progress.
she has many classic facial features associate with williams syndrome, like epicanthal folds at eye, upturned nose, wide mouth & small teeth, small jaw, full cheeks (badly drawn), n large ears.
70% or more people with WS have some sort cardiovascular problem, n so do gummy. she has supravalvar aortic stenosis (narrowing of aorta) which form of congenital heart defect (CHD). hers not very severe n be closely monitored.
she also have hypotonia & loose joints due to WS & uses posterior walker full time to get around. she really like her posterior walker, it shaped like many crayons :D also wear SMOs but forgot write it so oops
art fight character profile
[reblog welcome but please no repost]
#disabled#disability#decora kei#decora fashion#art#artist on tumblr#oc#original character#art fight#artfight#art fight 2024#eye strain#eye strain tw#kidcore#williams syndrome#autism#level 2 autism#intellectual disability#slug scribbles#facial difference#mobility aid#posterior walker#tw eye strain#long post#slug art
539 notes
·
View notes
Note
bro I can’t stop thinking about chase with a nerdy doctor reader who is basically the female Spencer Reid, goes of on tangents about the most random things that she somehow knows about and he is so happy to just sit there and listen 😩

𝐨𝐮𝐭𝐩𝐮𝐭. (𝐫.𝐜𝐡𝐚𝐬𝐞)
you like to ramble, Chase likes to listen.
fem!reader ☆ 1.1k ☆ masterlist. ☆ guess who’s backkkk
You don’t always notice when you're talking too much. It’s not intentional—it’s just that your brain moves faster than your mouth can keep up with, and when you latch onto something fascinating, you have to share it.
Right now, that something is the patient in Room 312.
You adjust your coat and push a stray strand of hair out of your eye, flipping through the patient’s file while Chase leans against the counter beside you. His posture is relaxed—arms crossed, weight shifted to one side—but his eyes are on you, steady and observant.
“This is so interesting,” you murmur, barely containing your excitement as you review the preliminary lab results. “I mean, it’s tragic for the patient, obviously, but from a medical standpoint, this is an incredibly rare case. Look—this deletion on chromosome 15? That could indicate Prader-Willi syndrome, but given the patient’s lack of speech development, the ataxic gait, and the characteristic happy demeanor, I think it’s more likely Angelman syndrome.”
You glance up, half-expecting Chase to be looking at the clock or zoning out like most people do when you go on a tangent.
Instead, he’s watching you.
He tilts his head slightly, a hint of a smirk tugging at the corner of his mouth. “And what makes you think that?”
Encouraged, you straighten and turn the file around, pointing to the genetic test results. “Well, it all depends on which parent the deletion came from. Both Angelman and Prader-Willi syndromes result from imprinting errors on chromosome 15. If the deletion is inherited from the father, it causes Prader-Willi syndrome. But if it’s inherited from the mother, it results in Angelman syndrome.”
Chase hums in acknowledgment, his gaze still locked on you, but you’re too deep in thought to notice the way he’s studying your face rather than the test results.
“The cool thing about imprinting disorders,” you continue, “is that they show how genes aren’t just about inheritance but also about which parent they come from. It’s not just about the presence or absence of a gene—it’s about whether that gene is supposed to be active in a particular parental copy. The same genetic region can cause two completely different disorders depending on whether the missing part came from the mother or father. Isn’t that wild?”
You pause, catching yourself.
You’ve been talking non-stop for at least two minutes.
Most people don’t last this long.
Your excitement fades slightly as you glance at Chase, expecting polite disinterest. Instead, he’s still looking at you, arms still crossed, that small smirk still lingering.
Your face heats up. “Uh—sorry. I tend to… ramble,”
He exhales a quiet chuckle. “I noticed,”
You chew the inside of your cheek, looking away. “You could’ve stopped me, you know,”
“Why would I do that?”
You glance back at him, surprised by his tone—warm, easy, almost fond.
His smirk softens into something more sincere, and you suddenly feel very aware of how close he’s standing. Close enough that you can smell his cologne—something clean and subtle, like cedar and soap.
You quickly look down at the machine running the genetic test. The results are almost ready, the sequence data processing line by line.
A small beep signals the final printout.
You grab it, scanning the page with an eager intensity that momentarily pushes Chase’s gaze from your mind. “A maternal deletion,” you murmur, eyes widening. “It is Angelman syndrome,”
Chase straightens slightly, stepping closer to glance at the results over your shoulder. “And that means…?”
“It means we need to tailor the treatment accordingly. Angelman patients benefit from seizure management, physical therapy, and specialised communication support since they often have minimal verbal speech—” You stop yourself, pressing your lips together.
There you go again.
“Sorry,” you mumble. “Rambling again,”
Chase shakes his head, smiling. “No, keep going. You were saying?”
You blink, caught off guard.
He actually wants to hear more?
“…Right,” you continue hesitantly. “So, one of the main issues in Angelman syndrome is the loss of function of the UBE3A gene in neurons. Normally, the maternal copy of UBE3A is the only active one in the brain because the paternal copy is silenced. So when there’s a deletion on the maternal side, the patient essentially loses all functional UBE3A expression in their neurons, which leads to the neurological symptoms—seizures, developmental delays, lack of speech,”
You pause again, gauging his expression. He’s not just listening—he’s engaged.
You exhale softly, almost disbelieving.
“…Most people don’t let me talk about this stuff,” you admit.
Chase shrugs. “Most people are missing out,”
Your breath catches for just a moment.
Before you can respond, there’s a soft knock at the door, and you both turn as House steps in. “I’m gonna guess by the look on both your faces that the test was positive,”
You straighten, holding out the test results. “Yep. The patient has Angelman syndrome due to a maternal deletion on chromosome 15,”
House nods approvingly. “Good. Go and tell the parents that their child will have the mental capacity of an 8 year old forever,”
—
The patient’s parents sit across from you in the consultation room, their hands clasped together anxiously. The mother looks exhausted, her eyes red-rimmed, and the father’s knuckles are white from gripping his knee.
You take a deep breath, softening your voice. “We have a diagnosis for your son,”
Chase stands beside you, his presence steadying as you walk the family through the diagnosis. You explain Angelman syndrome carefully—what it means, how it happens, what treatments and support are available.
And when the mother, voice trembling, asks, “Is there any hope? Will he ever speak?”
You hesitate, choosing your words carefully. “Angelman syndrome affects speech development, but many children learn to communicate in other ways—gestures, pictures, assistive technology. With the right support, he will find ways to express himself,”
Chase steps in then, his voice calm and reassuring. “And because we caught it early, you’ll be able to get him the right therapies sooner. Seizure management, physical therapy, and specialised communication support will all be extremely useful,”
You blink, surprised.
You hadn’t expected him to remember that part.
The mother swallows thickly, nodding, and the father squeezes her hand. “Thank you,” he murmurs. “Thank you for explaining it so clearly,”
You smile gently. “It’s what I’m here for,”
—
Later, as you walk out of the consultation room, Chase nudges your arm.
“You did good in there,” he says.
You huff a small laugh. “We did good,”
He tilts his head, considering. “Yeah. But I meant you,”
You glance up at him, and for a second, the usual teasing glint in his eyes is replaced with something softer. Something that makes your heart skip a beat.
“…Thanks,” you say quietly.
He smirks, stepping back, slipping his hands into his pockets. “By the way,” he adds, “I think you almost finished your whole genetics lecture before we got interrupted. You’ll have to tell me the rest later,”
You narrow your eyes. “You’re making fun of me,”
Chase grins. “Maybe a little,”
You roll your eyes, but you can’t help the small, warm smile tugging at your lips.
Because for the first time in a long time, you don’t feel like you’re too much.
You feel understood.
And when Chase walks away, glancing back at you with that unreadable smile, you wonder if maybe he understands you more than anyone ever has.
163 notes
·
View notes
Text
lYeshphyr noticing the majority of Toba's physical features come from lYeshphyr's own sire:




sire + dam = offspring
only thing toba truly genetically got from Kovah is some kind of personality disorder and also the ability to just fuck up terribly at killing someone and then being traumatized by them and just fucking off forever because of it and then killing themself
#as a reminder lYeshphyr's stark lightness is a like medical-magical sort of thing its like a pigment disorder#lYeshphyr actually has red and gold eyes. the brown eyes on toba are from lYeshphyr's sire#lYeshphyr doesnt have a consistent 'look' to carry on genetically due to being a chimera#so like Toba is a dragon. not a 1/4th siren- just a full dragon#taking lYeshphyr's sire's genetics because he was a dragon#that lYeshphyr just has but doesnt really present just carries#same with lYeshphyr's dam. the only child he has that reflects how he looks is Y#who is the offspring of lYeshphyr and his twin and thus a new type of creature alltogether as the natural offspring of 2 unnatural#species#and is genetically basically non existent. not that the physical embodiment of everything and nothing would be like. having sex#Y does not sleep or eat or do much at all
4 notes
·
View notes
Text


New Lundehund just dropped! Felix Junior Nilasson B3 made the quality requirement by a good margin and gained full registration today! He's the fourth of the Bs and fifth project dog overall (by my count) to enter the studbook.
The judge noted he has a slightly deep stop, but excellent proportions and volume of body (light and lean) and six sufficiently developed toes on each paw. In terms of health, he's HD B, PL 0, and eye screened clear, no signs of IL.
Nilas' grandmother was a Lundehund-Buhund cross, born in 2016. Lundehunds are being outcrossed to combat issues related to their severely restricted gene pool, such as infertility and a rare genetic disorder that causes 30% of deaths in the breed. The project is a collaboration between the breed club, kennel club, and our leading veterinary and genetic resource centers.
#lundehund outcross project#ik many of you already know this project well but added info for those that dont#look at this incredibly cool and good thing that is happening#Norrbotten-xes are hitting F2 as well these days with litter 2 expected this fall#ive been following this since the start in 2013 and i tear up every time they make a new registration#so many people have worked so hard for so long to make this happen#this is how you do successful outcrossing
154 notes
·
View notes
Text


hypermobile i. midoriya, t. iida, s. aizawa, k. bakugo
in which the mha boys have a partner with eds (ehlers danlos syndrome). ehlers danlos syndrome is a genetic connective tissue disorder that can cause symptoms like unsupported joints and joint hypermobility.
deku
gets so concerned whenever you get a subluxation
researches every holistic treatment he possibly can
and recommends them to you whenever you ask for recommendations
super gentle if you ask him to relocate something
like if you dislocated something
if you sprain something??
this man is CARING for you
carries you everywhere, brings you everything you need, the whole nine yards
if you asked him to do something like tape up your joints he gets so excited
like a little puppy being offered a treat
iida
sometimes he can be a little overprotective trying to make sure you don't get hurt
but he's just trying to look out for you
another man who doesn't mind carrying you around
always has an eye on you
you can never hide a subluxation or flare up or anything from him
he always knows
don't ask how, he just does.
aizawa
the most patient man on earth
always has painkillers on him for you
awful at cooking but it you're too exhausted to cook he'll order you some food or ask present mic to make something for the two of you
notices immediately if you're acting off
a great calming person to be around
you never feel like you have to be exciting around him
you can just relax
and take care of yourself
and he would not judge <3
bakugo
acts annoyed when you need him to take care of you
but he's secretly eating that shit up
he loves being ur knight in shining armor
like just something about you relying on him makes his heart race
lectures you about not taking care of yourself enough
like you could be doing everything right but he'll still tell you to take better care of yourself
he's just worried about you
taglist - @justmylvr @lwcedribbons @im0nsaturn @n3r0-5352 @dvartefox @failurewater @f0reverfaded @t0asty1 @iv-vee @mp3nai @straows
ⓒ luvseraph
#mha x reader#mha fluff#bnha x reader#bnha fluff#mha headcanons#bnha headcanons#izuku x reader#iida x reader#aizawa x reader#bakugou x reader#mha chronic illness#bnha chronic illness#seraph mha.#seraph writes.
108 notes
·
View notes
Note
So… I have a biology degree and Theo’s eye has me thinking. There is a genetic disorder called Alobar holoprosencephaly or Cyclopia that results in a child being born with only one eye right in the middle. Is this what happened to him?
It’s pretty rare but it would be enough of an explanation for him to be able to go out in public
Oh wow that's so interesting, I've never heard of that before.
The concept I had with Theo was "The only monster in a human school who tried to hide that fact".
I love your concept too but I feel like it would give a different meaning to his character. With him I want things to be a bit more exaggerated and story-ish you know. Like something you'd see in a kids book but it took a turn and now the main character is a down bad stalker.
Giving him an actual disorder like that would make him more real and human which I love but it would probably be more fitting for another character.
I hope that made sense lol
124 notes
·
View notes
Text
As an Ao3 author, I love giving headcanons that'd probably anger a certain side of the Batman fandom, but I personally don't care because it makes great angst and, again, I'm an Ao3 author and chronically ill!
First up! Dick Grayson, I like the idea of him having ADHD, of course, BUT... joint hypermobility syndrome.
(Joint Hypermobility Syndrome: Joint hypermobility syndrome is a connective tissue disorder. Thick bands of tissue (ligaments) hold your joints together and keep them from moving too much or too far out of range. In people with joint hypermobility syndrome, those ligaments are loose or weak. If you have joints that are more flexible than normal and it causes you pain, you may have joint hypermobility syndrome.)
Chronic pain fits him, don't ask, because as the eldest child with chronic pain and hypermobiltiy syndrome, trust, he has that look in his eye that he's been walking on swollen knees for the past twelve hours, had three mental breakdowns, and is still pushing through because SOMEBODY has to deal with this bull.
That's also the reason he wears freakin' spandex-- only, it's for compression! He wears compression items to help with swelling and pain TRUST, and let me have this because the math maths (it probably doesn't, but let me have this.)
He's got chronic fatigue, he's gotten used to popping dislocated joints back into place, Bruce was so confused how he dislocated and sprained so many bones so quickly when out as Robin. It's genetic, of course, Bruce finds. But he has money, and Dick powers through it all! Till he develops arthritis in his early thirties/ late twenties and actually hates everything because WHAT AND WHY--
---
Next up! JASON TODD! I have no proof, evidence, and it doesn't have to make sense but I like giving him asthma sometimes for the angst potential of if he didn't have it, he wouldn't have died in the explosion.
He didn't die from said explosion, nor JUST the smoke inhalation, but because he had an asthma attack, on the ground, bones broken, unable to breath because his inhaler did NOT survive the blast, if he even had it on him.
And that's why he wears helmet with so, so many filters in it now...
Also, being a street kid who struggles to even get his medication that keeps him alive? Peak angst, being to poor to afford your medication because the American healthcare system is actually trashy garbage.
R.I.P. Jason Todd, you would've loved clean air--
---
ANEMIC TIM DRAKE! But I up you, Tim Drake with Postural Orthostatic Tachycardia Syndrome (POTS)
(POTS: Postural orthostatic tachycardia syndrome (POTS) is a condition that causes your heart to beat faster than normal when you transition from sitting or lying down to standing up. It’s a type of orthostatic intolerance.)
Read ONE SINGLE FIC/ SERIES with this and I've loved it since because what do you mean he randomly falls asleep anywhere? No, forget your canon, he passed out and people think he just fell asleep... NOpe, he passed out, sorry random lady he was on a date with!
(The majority of people are AFAM but we aren't ready for my trans Tim headcanons yet either.)
(You’re at a higher risk of developing POTS after experiencing the following stressors:
Significant illnesses, such as viral illnesses like mononucleosis or serious infections.
Physical trauma, such as a head injury.)
Ngl, my dude gets a LOT of physical trauma (and mental--) also, losing a spleen? Surgery and at risk of viral illnesses? I'm sorry, but I need him to suffer more because I like when Tim Drake suffers horribly.
Now, despite having this condition, I am no expert, but also his caffiene/ energy drink addiction is from chronic fatigue, he shouldn't drink it, it's not healthy or good for him, but he stopped caring between the spleen loss and whatever the "Drake" run he did was because what even was that name?--
---
Damian is autistic and I will DIE ON THAT HILL--
No, I won't explain and you can't make me.
---
#headcanons#batman#bruce wayne#tim drake#dick grayson#jason todd#damian wayne#chronically ill#chronic illness#chronic pain#chronic fatigue#pots#pots syndrome#hypermobility#asthma#angst
147 notes
·
View notes