#Also would like to make it known that Leo has autism
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text

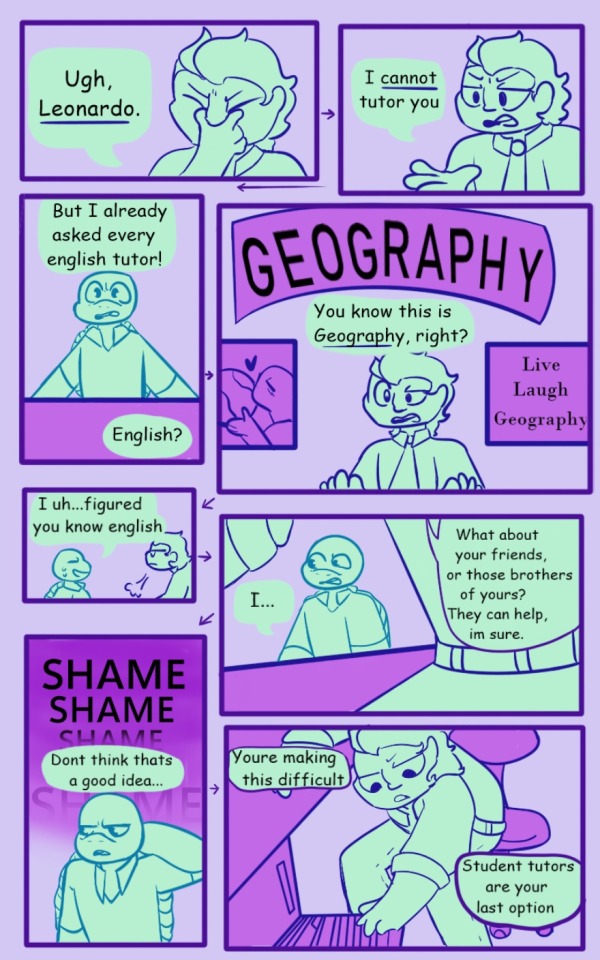

I had this idea that Koya becomes Leo’s tutor in mutant mayhem and i couldn’t let it go.
I’ll do more, but I like these pages and I’ve never made comics before so yippee
#tmnt#mutant mayhem#mm leonardo#Koya tmnt#she’ll show up eventually but rn she’s a mention#fan comic#my art#this came to me in a fever dream#Will it be cannon compliant? yes and no#Also would like to make it known that Leo has autism#and Koya is an undiagnosed neurodivergent
45 notes
·
View notes
Note
As the anonymous author of the famed (75 notes) What I Think Would Fix the Fates Royals asks, I now present to you:
Fates Royals Ranked by How Much Gender They Have (and also this time I include Azura)*:
Elise: You would think she's just a girl but she hides at least 15 genders under her bed alongside her contraband sweets. Nobody knows where she's getting all these..it's alarming
Xander: Xander has one solid gender. No one is quite sure what it is but he's definitely got a total of one. As you can see from his being so high on the list with only one gender, this family isn't very high on them.
Hinoka: She has like 89.5% of a gender and that gender is lesbian.
Ryoma: His gender is part Hoshidan, part his beautiful, illustrious hair when it's not in that weird headpiece. That is to say, one part is very deeply instilled in his personality, the rest is left to the imagination, you never see it but you know it exists. His gender would be sort of enigmatic if it wasn't SO in your face…known but unknowable, y'known?
Camilla: Has about 75% of a gender that can very loosely be described as being a woman. It's close enough that she doesn't bother explaining it beyond that but like there's 25% something else that she doesn't really touch.
Sakura: Whatever gender she has she does not think she's doing it very well. She's actually doing the best out of anyone because she's sweetiepie :)
Takumi: Takumi has got like half a gender. He had to move the rest of it out to make room for his crushing inferiority complex. Actually no, I think his gender IS having an inferiority complex.
Leo: Taking note of Takumi having only half of gender, decided he must become even less gender. This failed, he has the same thing going on now just in the opposite direction. Put them together and you now have every form of gender angst imaginable.
Corrin: No matter which Corrin you select at the start of Fates they both have just the vaguest hint of gender, dedicated to whatever meshes best with their siblings at the moment. Their gender is loving their family and having fun and also the inexplicable horror of existing in a nonhuman body and the alienation they feel because of it. Also autism.
Azura: They have so little gender that I consistently forget that they're supposed to be canonically a woman. You're telling me that if you could just sit by bodies of water and sing a little song and do cool shit all day you'd care about gender?? Yeah right.
*Ranking is NOT on gender they are, as they are all gender in some way. It’s about how much gender is in their gender. Also none of this is that serious because I could literally reverse the list and still make a case because they're my sillies :)
.
28 notes
·
View notes
Note
Re: ableism w/Symphony Donnie: Definitely some internalized ableism but I think that’s unfortunately due to not many people knowing what exactly neurodivergence looks like and how people with it processes things differently.
Like, honestly, my biggest gripe was the recording and even that, for the SPECIFIC context of this story and Donnie as a character, it makes sense. Does it make it right? No, but if Donnie never had to think about these things before, for him it’s the same as recording everything to protect his family. Just something he does.
Also, even though my heart broke with Reader’s at her realization, MULTIPLE times reader has said Donnie says what he means and even at the beginning with the “I like you” thing I was like, “Girl, I’m going to need you to define the relationship with him.”
And I think, with Leo, even when writer’s do write him as neurodivergent, what I’ve read always has him as the he better masker whether it’s explicitly said or not. Idk if Symphony Leo is neurodivergent or not but STILL, reader has picked up that he’s good with masking which usually comes off as charming or “easy breezy beautiful cover girl”.
Idk, maybe because I know a lot of people like Donnie irl but if anything I was more frustrated at the obvious miscommunication between both of them than him directly, because as reader said, she projected her feelings on to him when he’s been super direct with his intentions.
Basically, there are sometimes where I wish people would just realize that processing the same thing between two people doesn’t always look the same and that one isn’t necessarily bad.
well-said, anon-chan!
edit: this got SPOILER!! HEAVY!! for chap. 22 and also soooo long so i'm going to tuck it under a cut. but here's some meta on symphony to explore this a bit since it's something that's very important to me and also... pretty critical to the fic itself! i don't typically like explaining myself outside of the text and letting the fic itself speak but. hm. i suppose i shall let it slide for today!
as you all have hopefully noticed by now, as an author, i like to be. hm. more subtle with things. i prefer to tuck things away versus having things be blatant in the text. and this is kind of coming back to bite me a little with donnie and his neurodivergence, i suspect.
i've tried pretty hard to make it contextually obvious that donnie's autistic. i've all but used the word. the way he behaves and communicates is heavily autism-coded.
meanwhile, the story is from viola-chan's pov, and she's neurotypical-coded (well. as much as i, an adhd-riddled autistic cat in a trenchcoat can manage).
as a result, she doesn't... pick up on donnie's problems with communication. not right away. but here, in this chapter, we see where she finally figures out what their issue has been the entire time:
…Oh. Oh god. He really doesn’t get it. You’d known, of course, that Donnie wasn’t great with people. That he doesn’t communicate well. He doesn’t pick up on cues, or use them himself. No wonder he’s always so frank in his language, you realize. No wonder he’s so comforted by the firm rigidities of science. No wonder he looked so lost. No wonder he was so perplexed.
then, she puts that into practice by being specific and precise with how she talks. and we see that she now knows how to communicate with him in a way that works for both of them. and it works for them:
God; it’s like—a breath of fresh air, you think, staring at him in a little bit of awe. It’s so easy to talk to him, now that you’re just… letting it all out. Being honest. Frank. Infuriating that you hadn’t done this earlier. Feeling your irritation deflate, you nod. “…Okay. You just—need an explanation. Clarification.” “Yes, please,” Donnie gushes, fretting a little.
it's going to take some work. she still takes things he says personally and extrapolates past them (the whole "leo being an important person" thing). but she immediately nips it in the bud and is like. no. we're not doing that anymore. so, going forward, her relationship with donnie is one that's built on learning how to develop this open communication.
of course, it's not perfect, because they're human. donnie twisting her arm into still talking to him by calling in the favor is shitty behavior. a desperate bid to keep someone close that, for some reason, he can't imagine being without. not cool. the recordings of them having sex were shitty behavior to us, people who Know Better. but when violist-chan said 'hey, that's not cool, don't do that' and donnie was given a reason why not to, he just says ok. he might not understand ("but i record everything"). but he acknowledges that there's a concern there, and he agrees to be more conscientious in the future (having a consent sheet).
now then, let's look at leo's behavior in comparison.
donnie's biggest fault was that he didn't know to check in and make sure they were on the same page with everything. leo's fault, on the other hand, is purposeful, manipulative, and cruel. his open admission that he's been manipulating her from the beginning. manipulating donnie. lying to her.
to me, this is much, much worse than what donnie did. even knowing that at some point he starts developing friendly feelings towards her—and some of their interactions were indeed genuine!—i'm with violist-chan here. i'm not going to be digging through every one trying to parse out which ones were real and which ones were him being a dickhead. they're all tainted by the stain of betrayal.
also. because it has come up in a different ask that i will be publishing probably tomorrow bc of spoiler reasons: someone said something to the effect of 'why didn't he just not say anything? he could have taken that to his grave. how selfish'. i will remind you of a conversation between violist-chan and leo that happened in the previous chapter:
“Most of all, he’s honest,” you keep going, tangling your fingers together, staring down at the way they knot at your waist. “If he says something, I can take it at face value. There’s no hidden meaning. Nothing deeper. If he says something feels good, I know it feels good. If he says he likes something, he likes it. If he doesn’t like it, he doesn’t like it. If he asks for something, I don’t need to ask if he’s sure. He asks, so he’s sure. It—It’s a breath of fresh air. If I want to know what he’s thinking, really thinking, all I have to do is ask. And...” [...] Leo’s still as stone for a few moments longer, looking at you like he’s trying to decide if he wants to say something; but finally he relaxes and comes back to you himself. Reaching out, he flicks your forehead, causing you to wince and rub at it.
i think... leo maybe wouldn't have ever said anything about it. but then you said this. how donnie matters to you because he's honest. there's nothing deeper with him. it's all at face value. you never have to worry about what he's doing, what he's thinking. and that i think... really messed with leo. because he knows he hasn't been honest with you. you can't trust what he says at face value. you do have to worry about what he's doing. and for you to say that that's the main thing you love about donnie—it messed with him. so, even though he knew it would jeapordize the relationship with you, even knowing he wanted to put this off for as long as he could, even though, even though, he decides he has to tell you. he has to come clean.
so even though it feels like shitty, selfish behavior... it's actually him trying to do right by her for a change. to conform to what she looks for in a relationship (both romantic and platonic). it just... didn't go over so well, predictably. most people don't like hearing that not one, but two of their most precious relationships were built on a foundation of misunderstandings or lies.
side note. i do headcanon leo as having adhd that primarily manifests itself as an inattentive form. i don't suspect it has much to do with his behavior here... save perhaps for some possible rsd being triggered when violist-chan is like 'ok actually go fuck yourself i'm out of here.' i don't find it particularly relevant to the discussion of ableism, in this context.
so anyway. long post aside. it's... interesting to me. to see people saying 'actually fuck both donnie and leo equally!!! bleh bleh bleh!!!!' i don't know that it's. hm. active ableism. i'm certainly not accusing anyone of the sort. but it is, at the very least, indicative to me that there are a lot of people who don't read into the text as deeply as perhaps i would like on certain character traits, if i had a magic wand to wave.
....and also perhaps just ableism, haha.
43 notes
·
View notes
Note
Leo/Frank/Reyna with an autistic reader?
Autistic Reader
((I unfortunately don't know much about Autism but I did my best! I did do some research so I hope it's alright!))
Leo Valdez
-Leo does his best to be supportive but he has a million things going through his brain. Unfortunately you like things to be done at their exact time and get anxious when they aren’t.
-”Leo, we’re already five minutes late!” you stress out pacing outside his room. Leo does make his way out, getting his jacket on. But when he goes out and sees you so stressed out he honestly feels bad. He just gets so absorbed in his own work that he forgets about time.
-However Leo decides right there and then that he never wanted to be the cause of your stress ever again. He makes multiple alarms for himself to block out his time. Just as you were about to go complain to Leo about being late, again, you hear him talk by the front door.
-“Come on love we don’t want to be late do we?” he gives that dorky grin that makes your heart flutter. He really was a dork but you do go over giving him a light kiss that makes him go bright red.
-He isn’t perfect though, he often messes up with realizing you take things very literally. Which he works his best on, but he was known for making jokes and such! He’d never mean it maliciously though!
-The worst scenario with that was when you were getting ready to join the ares cabin in sword training and Leo called “break a leg!” The stare you gave him really made him realize just how bad he messed up. He quickly starts to explain what the phrase means as he feels guilty right away.
Frank Zhang
-Frank knew anxiety could get bad, he had to deal with it a lot himself. You two had bonded over that when you were younger after all. And now Frank was trying to help you meet his new friends.
-Of course he knew it’d be a lot to meet six other people who all had their own unique personality… So he had warned the group ahead of time that you two might sneak off for a bit to help you relax, promising it wasn’t because of the group.
-Everyone was very understanding. Frank could see you were getting a bit overwhelmed and went to your side smiling softly “Did you want to take a break?” he asks, keeping his voice calm and you nod, taking a shaky breath as you look at the railing of the boat.
-Frank knew you were never one to make eye contact so he never bothered you about it. “Here, there’s a good spot over here.” He leads you over where the chatter dies out and you get to enjoy seeing the ocean.
-You take a few breaths helping yourself calm down as Frank waits, standing at the railing while he waits. He knows when to give you space and you couldn’t have asked for a better boyfriend than him. After calming down a bit you feel guilty about running off from a party that was supposed to be about you making friends…
-”Hey, don’t feel guilty. They all understand.” he promises lightly sitting down beside you as if he read your mind. “Can I hold your hand?” he asks gently. You can’t help the soft smile forming on your face as you nod, holding your hand out for Frank to hold which he gladly takes. You can’t help but think how lucky you are.
Reyna Ramírez-Arellano
-Reyna is very observant, maybe it’s her combat skills but she just knows when something is wrong. She could tell the moment you don’t like something, the moment you’re stressed, or when you’re upset. She could really read you like a book.
-But what she did have problems with is telling your other emotions, which was unfortunate since you had a hard time explaining how you were feeling too. You were also very blunt and honest but she loved that.
-It was annoying having to deal with the other roman soldiers who would go around subjects to spare her or others feelings. She just wanted the truth and you would deliver. She was working on some paperwork and looked over to you.
-“What do you think of Octavian?” she asks curiously looking at you with a raised brow. You huff at that “I think he’s a jerk and I hate him for sacrificing my stuffed animal.” you say as if talking about the weather, making Reyna grin a bit at that she really did love how honest you were.
- She had to work out something to help you with your emotions, something that would help the both of you. She wanted to be a good girlfriend and be there to support you. But she knew that she couldn’t do it alone so she asked the other seven to help her come up with ideas.
-She should have just gone to Annabeth first as she printed out something called the emotion wheel. It was a wheel with different emotions on it that would then branch out to more detailed explanations like going from sad, to discourage. Something you could take one step at a time. It’d be perfect.
~Masterlist & Rules~
Like my writing? Please consider sending me a Ko-fi! ☕
#pjo#pjo x reader#hoo#hoo x reader#pjo fluff#leo valdez#leo valdez x reader#frank zhang x reader#frank zhang#reyna ramirez arellano#reyna x reader
143 notes
·
View notes
Text
UT POKÉMON TEAMS
Came up with this idea after finding my binders full of Pokémon cards and the autism blew my back out so now you're getting Undertale characters' Pokémon teams, starting with Sans. WARNING: I've put way too much thought into this.

At first, I wanted the teams to follow specific types. Then I thought "Hey, that's stupid actually, and pretty limiting." So here are the Pokémon I think Sans would have as a trainer:

1. Gengar: Sans shares this Pokémon with Chara and Kris. Gengar has a combined affinity for travelling in shadows, levitating, pulling pranks, and smiling like a freak. It's said to be able to move between dimensions, esepcially in its Mega form. It's a ghost poison type too, since some people compare the theorized "Karma" ability Sans has during his Bad Route battle to being poisoned. It's also fat and only 4'11 so it's the perfect Pokémon for this man. They're both short, round, spooky, silly, and smiley.
2. Snorlax: Snorlax is a sleeping giant that is great competitively, it represents the apparent laziness of Sans. Some people would probably pair him with Slaking, but Slaking is too human-looking to me, and its previous evolutions don't make sense for Sans to train. I could sooner imagine him with a Munchlax than a Vigoroth. Snorlax is also cute and sweet-looking, and sort of round and cartoonish to match Sans's design better. It's often found sleeping in "inconvenient" locations, like Sans. Plus, it only evolves with high friendship. It is supposedly incredibly lazy, but when pushed to show serious effort, it "displays awesome power".
3. Dusknoir: This Pokémon shares the grim reaper/hooded skeleton look with this Sans. It is said to pick up radio signals from "another world" (which is obviously the Afterlife in Pokémon, but Sans himself is theorized to be from another world). Its first evolution, Duskull, resembles a hooded skeleton that simply enjoys frightening children. Its final, powerful, intimidating evolution better fits the aura Sans has if he's pushed to actually fight. It also only has one eye, reminiscent of Sans's one glowing eye during his battle. It is known for taking souls to the afterlife, or "home".
4. Gholdengo: This money-themed Pokémon is based on Sans's habit of selling things. I figured this ghost type fit better than other moneyzthemed Pokémon like Meowth since Sans seems to make money through some tax-avasive, illegitimate means in Undertale. Even Papyrus isn't sure where Sans gets all of his gold to pay for things. Like Sans, Gholdengo is also able to make friends easily and gets along with everybody. It also has some big Papyrus energy, so I thought Sans would like it for that reason.
5. Glalie: Glalie looks like Sans and shares the ice typing with his environment in Snowdin. It evolves from a mysterious little gremlin, Snorunt, that also appears to be wearing a jacket/hoodie. It is able to immobilize foes and keep them from escaping, similar to how Sans can freeze time and the player's SOUL when he wants to knock you around. This Pokémon also has its laid-back side... sort of. It apparently eats its frozen prey "at a leisurely pace."
6. Luxray: I wanted to include a Pokémon that was based on space, but most of them were too out-there for Sans' team, like Gothitelle, Klefable, and the Legendary Cosmog (we'llget to Legendaries later). I finally found one I liked. Yes, Luxray is based on space stuff, specifically the constellation Leo. It is also based on a Lynx, said to be able to see through walls, kinda like how Sans can break the 4th wall and see through the player's cheating or other nonsense. From its Pokédex entry: "When its eyes gleam gold, it can spot hiding prey--even those taking shelter behind a wall." Apparently, this ability takes a lot out of it, so Luxray sleeps a lot to store up energy.
Our final Pokémon associated with Sans are the Legendary Dialga and Mythical Hoopa.

Legendary: Dialga, the time Pokémon. You know why this is here. It's blue and can control time. It's also associated with a "sibling", Palkia, who bends space, and the third, more mysterious Giratina (which kinds sounds like Gaster to me...).
Mythical: Hoopa is a mysterious, mischievous Pokémon that can travel between dimensions, teleport, and use its rings like wormholes. It has two forms: the first form is small and harmless-looking, but still a prankster. The second form is extremely powerful and uses its rings to warp space-time and to control and summon powerful Legendary Pokémon. It's first form is small, stocky, and cartoony, like Sans. Its second form is a powerful secret that, once unleashed, can cause massive destruction. Together with Dialga, this Pokémon's yellow mixes with Dialga's blue to give us the two colours of Sans's eye when he uses his full power in battle.
5 notes
·
View notes
Text
world building cause twn doesn't pt. 2: nilfgaard!
pt. 1 on the northern realms here
okay i'm making this because 1 witcher netflix is the most convoluted and confusing thing i've ever seen and does literally no world building and 2 special interest make autism brain go brr.
about this series
this is gonna be a multi part series about the witcher universe but this is all about nilfgaard!
ciri's timeline in twn encompasses the entirety of the first northern war, beginning with the attack on cintra and ending with the battle at sodden
the show ended in 1264 when we saw geralt meet ciri
this is just covering the human portions of nilfgaard. i'll talk about elven allied groups like the scoiatael later.
colour code cause i fucking love colour codes - already happened/introduced, probably s2, important background info, stuff that might be in the prequel, extras
background
the witcher takes place on the continent, which is mainly divided between south and north
the north is a collection of many kingdoms while the south is basically just nilfgaard and its many territories, dependencies, provences, and vassal states.
some of these conquered areas include toussaint, vicovaro, nazair, and mettina
nilfgaard loves invading the north. a lot. like this is the driving force of most of the plot in the witcher.
basic info
nilfgaard an insanely powerful absolutist monarchy, ruled by an emperor who has a huge collection of talented mages, spies, commanders, and advisors
as of ciri's timeline in twn, the emperor is emhyr var emreis, or, to those on more intimate terms with him: the white flame dancing on the graves of his foes

[ID: middle aged white man with slicked back shoulder length greying black hair. he is wearing a black dress with a red and black embroidered shirt underneath. he is wearing a gold medallion around his neck, has black leather boots, and is holding a silver goblet. end ID]
emhyr is crazy important, both as a character and to the politics of the witcher. he's also a member of the house of emreis, which i'll go into detail on in a bit.
he is also a major walking spoiler, so i won't talk about him in the context of twn or the books
nilfgaard is divided between the "heart" of the empire, also known as lower alba or simply nilfgaard, and the conquered territories, dependencies, provinces, etc
for all of nilfgaard's imperialism, it does allow these areas to retain a lot of their original cultural identity, to the point where someone from vicovaro would not really consider themself nilfgaardian
this works out because nilfgaard would not consider a vicovarian nilfgaardian either
lower alba
lower alba is the home of "real" nilfgaardians, and is also where the capital city is located
theres a bit of racism and racial purity here: lower albans consider themselves superior to the rest of humans due to their elven ancestry
this elven ancestry is also why nilfgaard is far more sympathetic to nonhumans than the north and uses a language similar to hen llinge (elder speech)
there are a LOT of notable albans, so i'll just keep it to the important ones and my favourites: carthia van canten aka cantarella, morvran voorhis, stefan skellen, the house of emreis, and vattier de rideaux
the capital, known as the city of golden towers or simply nilfgaard, is home to the imperial palace, where the emperor spends most of his time
i say most because there is also a summer residence at loc grim palace
now that we know the basics of the core empire, let's visit the other territories!
toussaint
the duchy of toussaint is one of the most important nilfgaardian states, and definitely the most beautiful. it's main economy is in wine
toussaint actually has no secret service or military, something quite rare on the continent. it does however, have a large system of knights errant that love chivalry
the capital is beauclaire, which is where the duke/duchess live
as of twn, its ruler is the duchess anna henrietta. i'll let you all make your own assumptions about the lovely annarietta
also for some reason in toussaint, people have 2 names that are smushed together. so anna henrietta becomes annarietta, sylvia anna becomes syanna, carolina roberta becomes caroberta etc
annarietta is also distantly related to emhyr, her great grandfather is the half brother of emhyr's father
the most notable toussaintois are the mages fringilla and artorius vigo

here's fringilla in twn. [ID: young black woman in a long sleeve grey-blue cloak. her hair is pulled back and she is looking slightly up and to the right with a blank expression. end ID]
vicovaro
"THERE ONCE WAS A MAID FROM VICOVARO..."
okay vicovaro is vassal state near the southernmost part of the empire, but we know it more for the people from it than what it actually is
there is an actual ruler, but the state is largely controlled by two key houses: the var anahid family and the dyffryn family
the capital is vicovaro, but the houses have their own land. we don't really hear about the var anahids, but the dyffyn house controls dyffra
notable vicovarians include assire var anahid and cahir mawr dyffryn aep ceallach. cahir in twn is right there.

[ID: young white man in black armour. he has an angular face and brown slicked back hair. he is scowling]
mettina
okay mettina is a bit confusing since it is the shared name for three different places. the first is the administrative unit mettina, which includes the provence mettina (2) and the provence maecht. in the provence there is also the capital city mettina (3).
tor lara aka the tower of the swallow is in mettina, and not much else tbh
maecht was the home of duny (that little man) for an unspecified number of years

[ID: young white man with dark curly hair. his face is dirty and sweaty and he is frowning slightly]
"wait! i thought duny was the urcheon of erlenwald, and that's in cintra!" don't... don't think too hard about duny. he lived in mettina for a while and took a trip to cintra where he met pavetta.
ebbing
for all intents and purposes, ebbing is an autonomous state, although nilfgaardians do have a hand on the wheel
includes salm, a technically sovereign provence, but is de facto dependent on ebbing
ebbing is most notably home to stygga castle, the one time fortress for the school of the cat, and bounty hunter leo bonhart
also, roegner of ebbing, pavetta's father, is from here
nazair
nazair is kinda the least important of the more important nilfgaardian dependencies
it was independent for a while but was conquered by cintra under queen calanthe and then nilfgaard under emperor emhyr
its main industries are cinnabrite and silver, both luxury goods
the only mildly important nazairi is becca of nazair, ciri's 6 times great grandmother
other minor areas
alba, toussaint, ebbing, and vicovaro are really the only important nilfgaardian areas, although mettina and nazair are mentioned quite a bit. borders change a lot, especially with an imperialist power, but this is the general list of nilfgaardian areas as of the first northern war
regions - daerlan (notable for military), eiddon (owned and ruled by alban spy vattier de rideaux), liddertall, magne, rowan, ruach, slopes (home to haern caduch, the bear school fortress), tarnhann, winneburg, and ymlac
provences - angren provence (contains dol angra, a profitable trade route), cintra (1264-1268), etolia, gemmera, geso, mag turga, mettina (contains kingdoms mettina and maecht), and nazair
vassals - cintra (after 1268), ebbing, toussaint, and vicovaro
tl;dr: the most important part of nilfgaard is lower alba, which is surrounded by many dependencies including toussaint, vicovaro, nazair, and mettina.
thank you for reading! i'm definitely gonna make more parts and will link them here when i do!
#the witcher#twn#wild hunt#the witcher netflix#jaskier#geralt#geraskier#tw3#geralt x jaskier#yennefer#yennefer of vengerberg#witcher#geraskefer#geralt x jaskier x yennefer#mine#gen tag#lore tag#haven't got a fucking queue
148 notes
·
View notes
Text
Quarantine Harry Potter Fanfiction *READING LIST*
I’ve spent the past months reading copious amounts of fanfiction and now my amount of AO3 bookmarks is absurd. I really need to share these because if I don’t I think I might implode. Drarry-centric but not all!
These are in no particular order nor is there a particular time frame that these were all posted. I have a little bit of everything in here just you wait.
On Punching Gods and Absentee Dads by Enigmaris
56 Chapters, 247k Words, Complete, no slash, T Rating
Marvel, Norse Mythology, Harry Potter Crossover
TW: Past Abandonment
Harry finds out that his dad is alive, has been the whole time. Instead of being overjoyed, Harry's disgusted. His dad left earth and abandoned his friends. Every painful thing he's ever gone through can be traced back to one man. Now Harry's got super strength he can't control and an almost unnecessary amount of magical power. His dad might be living it up with the Avengers now but not for long. With the help of his friends, Harry comes up with a plan for revenge. Get ready Avengers, Harry's out to punch a god.
We’re starting off strong with a Marvel crossover fanfic wow. Who knew that crossovers could be done tastefully as 2013 Wattpad kind of ruined it for us. However, this fic changed my mind! This fic is funny as fuck and is just a goodass time. I love a good multi-chapter fic (as you’ll soon see) and this one is a showstopper.
The Man Who Lived by sebastianL
42 Chapters, 254k Words, Complete, Draco/Harry, E Rating
TW: Major Character Death, Graphic Deptictions of Violence
Draco breaks a cup, and one thing leads to another. A story of redemption, tattoos, dreams, mistakes, green eyes, long conversations, and copious amounts of coffee.
With all of the Black Lives Matter protests happening right now, I think that this fic is super relevant. Draco has moved to New York City and is working as a receptionist at a tattoo shop and a mentor for inner city kids, but he accidentally gets forced to work out his differences with Harry, who at this point hates his guts. This fic is pretty serious, tackling themes of mental health, suicide, and police brutality. Every OC in this story is completely lovable and I cried my eyes out many times. When people ask me for a fic reccomendation this is the one I give people. Dare I say that this is my all-time favorite fic.
Warm Bodies by Betty_Hazel
Work in Progress, 37 Chapters as of 6/12/2020, 108k Words, Draco/Harry, E Rating
TW: D/s Dynamics, Graphic Porn, Dubious Relationship with Food
Draco Malfoy has spent his whole life wanting to go down on his knees for other men, and that's by far the least of the depraved things he fantasises about. He's wanted it all for so long that he's stopped believing that there might be someone out there who might be able to give it all to him; it comes as something of a surprise to find that maybe Harry Potter can, and that maybe Harry's looking for something too.
ALRIGHT MY PORN LOVERS THIS ONE IS FOR YOU! Don’t lie I know you’re horny. Somehow this fic is so fucking gorgeous and sweet yet so sinfully hot. It’s literally two boys who have never felt like their emotional needs have been satisfied learning to help and love each other like how much more wholesome does it get. I mean it’s all fine and wholesome until you get to the kinky sex which is WONDERFULLY WRITTEN MIGHT I ADD! I always say that if porn can make you feel something other than just horny, you’ve found a winner, and this story does just that.
Definitely check all the tags and I mean all the tags before you read this, but this is definitely one of my favorite porn with plot stories.
Running On Air by eleventy7
17 Chapters, 75k Words, Complete, Draco/Harry, T Rating
TW: No Archive Warnings
Draco Malfoy has been missing for three years. Harry is assigned the cold case and finds himself slowly falling in love with the memories he collects.
Might I just say that classics are considered classics for a reason. This is one of those stories that has the vibe of high school summer after senior year where all you do is try to escape reality and figure out your place in the world. While the plot is wonderful and the characters are great, I think what shines the brightest from this story is the writing style. It’s so enchanting and poetic with the best one-liners that make your heart hurt. On my AO3 bookmark i captioned it, “This just ripped my soul in half and restitched it together again,” and I still stand by that.
Lokison (Series) and How To Train Your Godling (Series) by sifsshadowheart
Main Story (Lokison): 33 Chapters, 244k Words, Completed, Harry/Various Characters, E Rating
14 Spinoffs/ Sequel Stories, Completed, Harry/Various, Various Ratings
Norse Mythology, Harry Potter, Percy Jackson, Various Fandoms Crossover
TW: Major Character Death, Graphic Violence, Underage Sex, Spiralling Mental Health
James and Lily Potter had a secret, one which led to Thanatos saving young Harry from a dreary life with the Dursleys and changed the face of the Second British Wizarding War before it ever began.
This story feels much more like a 12 season television show than a two hour movie if you know what I mean. The plot is pretty slow going but the character development and interation makes it worth it. The story blends the lore and events of the HP and PJO to make a completely new story without making it feel like a goddamn recap. The reader follows Harry from when he’s young all the way into adulthood and it’s a fun time to watch him grow as a character and bond with his parental figures. Also some of the spinoffs are really wild and I never would have thought of the pairings but they just work somehow?? My personal favorite spinoff is the Pirates of Caribbean/Calypso and Leo arc like HELLO?! hot pirates. The total word count of the two series is 465k so beware it takes a hot second to chug through this one.
This Worship of an Extinct Fire by Lomonaaeren
Oneshot, 30k Words, Draco/Harry, M Rating
TW: Graphic Depictions of Violence, Emotional and Physical Abuse, Deppression
Unspeakable Draco Malfoy has planned for nearly six months how to take down Thomas Linwood, a man who has discovered the secret of converting wizard bodies to pure magic. He was prepared for anything--except the discovery of the missing Harry Potter in Linwood's compound.
This one, I don’t know how it’s not considered a classic. I’ve seen it floating around on drarry tumblr and wow is it good. I especially like the detailed magic system and mechanics that Draco is investigating. How the author managed to have so much detailed and gracefully planned out backstory in 30k words is beyond me. Also gentle Dracoo Malfoy is my favorite Draco Malfoy :) absolute angel mode.
Little Compton Street (One Rainy Night in Soho) by LLAP15 and Writcraft
Oneshot, 66k Words, Draco/Harry, Past Sirius/James, E Rating
TW: Implied/Referenced Homophobia, Light D/s Dynamics, References to Cancer, References to HIV/AIDS
Draco is lonely, Harry hates the press and it won’t stop raining in London. Harry discovers a magical street that’s close to disappearing forever and Draco realises he’s one rainy night in Soho away from finding everything he’s been searching for.
This fic is, in every sense, a masterpiece. Especially for pride month, the story surrounding LGBTQIA+ activism, the AIDS Epidemic of the 80s, and the gentrification of historically queer communities is one that should be read by everyone. Every single place, OC, and historic event has real world ties and is historically accurate, making this fic even more enchanting. Everything about this fic is graceful and slow burning I can’t help but fall in love with it. I’ve only seen this fic once on HP tumblr, but I feel like it should be considered a classic as it is truly a moving piece. This fic is one of the biggest reasons why I became so enthralled with LGBT history and am writing a fic that takes place in a wizarding version of the AIDS epidemic.
Sensitive Touch by Raserwolf
45 Chapters, 194k Words, Complete, Draco/Harry, E Rating
TW: Racism and Racial Slurs, Homophobic Slurs, Ablism and Ablist Slurs, Rape and Sexual Assault, Sensory Overloads and Mental Breakdowns, Extreme Bullying and Hate Crime, Past Abuse, Anxiety Disorders, PTSD wow this is a long list
When Draco Malfoy encounters a struggling and frustrated Harry desperately trying to tie his shoes after a meltdown in the Great Hall, his curiosity regarding the incident leads him to seek the help of the two people closest to Harry: Ron and Hermione.
After even they are shocked to hear the extent of Harry's issues, though Hermione had her suspicions, he discovers more about the man than he ever thought he knew before.
As a Neurotypical, I found this fic to be absolutely wonderful. I don’t know much about the typical traits of those who are one the autism spectrum and how they affect their everyday lives, but from what I was reading in the comments from those who are on the spectrum or who have family who are, this fic was pretty accurate and realistic. Harry, who lives with aspergers, goes without a known diagnosis until 8th year and it’s just heightened by his PTSD and anxiety and ugh I just want to hug the boy. The story follows Harry and Draco and the rest of the 8th year gang through the year and has multiple arcs in which the wizarding world are just dumbass bitches who can’t fucking seem to accept people for who they are. Not only is Harry on the spectrum but he’s also Desi with a purpose and not just mentioned and forgotten which is wonderful. The boys go through a lot of trauma in the story but there’s also a lot of teeth-rotting fluff that I live for. This is one of the fics that I have read and reread because I love it so much.
This definitely is not my full list I have a ton more stories in my bookmarks if you are curious. I’ll probably post a part two to this just cause I have so much and read so often. These, however, are definitely the biggest highlights.
#harry potter#draco malfoy#drarry#fanfic#fanfiction#fanfiction rec#fanfiction recommendation#fanfiction rec list#fanfic rec#drarry fanfic#drarry fanfiction#harry potter fanfiction#harry potter fanfic#harry potter fanfic rec#marvel#mcu#marvel harry potter#marvel crossover#crossover fanfiction#crossover fanfic#archive of our own#ao3#norse crossover#norse mythology fics#fanfic masterpost#the problem is that i only read fanfiction now#i have an addiction#get me therapy#fanfic reading#reading list
44 notes
·
View notes
Text
Shattered Part 2: A ROTTMNT Fanfiction
Summary: The Best intentions don’t always don’t always have the Best results.
Word Count: 2545
Pairing: NONE
Rating: G
A/N I base Donatello’s struggles and Autism on my own experience and those of my family members who also have Autism. Also don’t be too mad at Leo, he’s trying
also I tried for HOURS to make a link to the previous chapter. I gave up, i’m sorry. I can’t even edit this thing after I post it to fix it, so this is it i’m sorry
Believe it or not, a family of mutants can have a normal morning.
For eleven year old Leo, that involved a bowl of Lou Jitsu Cereal, drowned in sugar (because the cereal was three years past its expiration date), and a morning of cartoons along his brothers. All crowded around the new projector Donnie had set up a few days ago. Which was a blessing, seeing as up until then they had to make do with an old rabbit antenna tv set that was always green.
Raph laughed loudly at the cartoons antics just as Donnie joined them, a plate of plane toast in his hands and his newly built tablet shoved under his arm, “Alright who has it?”
‘Has what?” Leo said without looking away from the screen
“My headphones,” As usual, even though Donnie was only eleven he spoke as though everyone else was the biggest idiot in the world. Leo never took offense though, if anything he thought it was flattering to be considered that stupid, “It’s 10:00 which means its time for my Ted Talk hour. I need my headphones back.”
Mikey finally tore his eyes away from the screen before popping up to his feet, ‘Oops! Sorry D, hold on,” he put his bowl precariously on a stack of magazines before hurrying away.
“See? No worries D.” Leo gave his brother one of his smiles, only to be returned with a scowl
“Leo, he took my headphones.”
“He borrowed them.”
“He took them without permission, I took me weeks to get all the parts I needed from the dump.”
Leo knew where this was headed, and unfortunately Raph was a little too wrapped up In the Looney Toons to pay attention to them. He set his bowl down as well before walking over, “D,” he thought carefully about what he was going to say, “He took them, but he didn’t’ do it to hurt you. You know, that right?”
Donnie glared at him, but Leo could see the anger and frustration slowly fading from his eyes. It had taken Leo a while to figure out how to calm Donnie down, usually facts did the charm. Information, something irrefutable, a word he had learned from Don, and thankfully Donnie was more forgiving of Mikey then the rest of them.
And it worked like a charm, Donnie took a deep breath,” Yeah…yeah, I know…” he exhaled a slowly breath, “he was curious…”
“Only cause he’s never seen a set of Bluetooth headphones before. Or headphones at all.”
Again, Donnie went silent, then nodded, “Maybe…I should make him a pair too.”
“I bet he’d like that. And if you want to go ahead and make us a third official unofficial twin robot-”
For the first time Donnie smiled, “That would be a triplet, would you and Raph like a pair too?”
“yes!’ Raph called from his spot without looking. Mikey hurried back into the living space, headphones in his hands with a guilty look on his face, “I’m sorry D, I cleaned them off with those wipes you like.” He held them out to him,” I’m sorry.”
Donnie again took a small breath and Leo worried that maybe he hadn’t calmed down enough but instead Donnie took the headphones back, “Just ask next time.”
“I will.” Mikey glanced over to Leo before walking back over to their cartoon morning. IT helped that Leo knew Mikey was truly sorry, but out of all their family members he was sure Mikey understood Donnie’s situation the least. That was something he had to fix soon before he did something Donnie couldn’t forgive. Leo smiled back at Donnie, “See?”
“Yeah,” Don’s eyes fell back on the purple headphones in his hands. Leo knew they were more than just a frivolous gizmo. They not only hooked up to everything electronic in the lair that had audio but also acted as noise filtering headphones when there was too much noise stimulation for Donnie to handle. ��I didn’t mean to get worked up thanks Leo.”
“No prob.” And with that the morning almost seemed redeemable. Until Leo gave Donnie a pat on the shoulder with a large grin, “See? Aren’t you happy I’m always around to defuse you?” before he went back over to his breakfast, enjoying a morning he would forget by the next morning.
Leo didn’t notice the pain that filled Donnie’s eyes, or how Donnie stood completely still for several moments before scrubbing at his eyes and hurrying back to his room. Just like no one noticed the muffled sobs that came from his room for a few moments
Just like Leo didn’t ‘noticed Donnie changed after that day
-now-
Believe it or not, Leo did not like always being right. Well, he enjoyed being right most of the time. It was a sensation he never tired of. But sometimes being right wasn’t a great reward.
Especially after last night.
The red slider turtle squeezed his eyes shut, focusing on the sound of a gurgling coffee pot and overwhelming smell of the rancid bean drink. It wasn’t his favorite smell, but one of Donnie’s favorite things in the world. Responsible for many late nights, it was a personal joke for him to try and hide Donnie’s coffee maker wherever he could. Mostly to see his official unofficial twin tear the lair apart in a half-awake rage to find it. He didn’t’ much feel like laughing right now. Right now, he just wanted to make his brother coffee.
“-but I still don’t’ get how the Soup Minister found the Soup Princess- “
“You gotta pay attention Raph, Lou Jitsu was in a love triangle with Minister Minestrone and Princess Pumpkin - Yo Leo! What are you doing up this early? Are you putting dirt in Donnie’s coffee again? You know he hates that.”
For a moment Leo couldn’t bring himself to turn around, instead he focused on the brown liquid dripping to the coffee pot, “I’m not putting dirt in it.”
“fertilizer again? Seriously? That made him sick last time- “
Leo turned around, “I’m not making him dirt, or anything! I’m just making him coffee.” For a moment, he felt better to see Raph’s face slowly fade into confusion. Satisfied, in a way he didn’t like, “you ok man? You look awful?”
“Do I? Gee I hadn’t noticed, I was just up half the night with Donnie weeping in my arms then the other half cleaning up his room while he slept in my bed, so no Raphie I bet I do look awful.”
Raph blinked at him, others might have thought his inability to comprehend his words was because of a limited intelligence, but Leo knew better. Raph was capable but morning brain could take down anyone. Finally, it seemed to hit the largest brother, “Is Donnie ok?”
“NO, he’s not, he came home trashed his room, and came to room in mumbling about some weird facts. When I tried to talk to him, he just fell apart.”
“Where’s he now?”
“Sleeping, he cried but after a while he just pulled away and curled up on my bed. I thought it was better to let him sleep there. I checked on his room, a breaking mess even by Splinters standards I picked up whatever I could. I only got done recently then I came in here.” Uh oh, he could feel the anger coming back, building in his stomach,” I told you something was wrong. I TOLD YOU something bad would happen! And now- “Leo paused, taking a breath, sometimes he forgot to do that when he was riled up, “Now he’s home, with a black eye, and I don’t know what’s going to happen when he wakes up- “
“This isn’t’ dirt is it?”
For a moment, Leo almost forgot whey he was so mad. In unison the three brothers turned towards the sputtering coffee pot to where said Donnie was standing, giving them all a confused if not suspicious look “Which one of you heathens made this?” Before exhausted eyes fell on Leo, “It was you wasn’t’ it? I got sick last time when you put fertilizer in my coffee- “
“I- “ok shock over, “NO its just coffee I promise D.”
Donnie narrowed his eyes at him, before looking back to his coffee mug. Sniffing it, “Ok I trust it for now, but if I end up getting poisoned again, I will NOT be happy. Now, if you will excuse me, I have A LOT of work to do.” Before exit the room
For a moment, the remaining group could only stand there, before Mikey spoke up, “Um, yeah Leo he’s a total mess.”
“I-He- “it wasn’t often he was at a loss for words, but it was known to happen. Instead he waved at Raph and Mikey, “Just give me a minute!” before running out of the room. By the time he reached Don’s bed room, Don had already set his cup down and was picking up one of the boxes, “I supposed I should thank you for cleaning this up, soooo consider this that.”
“No problem.” Back in the bed room and the remains of everything Donnie had destroyed last night. Now that he was more awake, he could see that, thankfully, the monitors and more complex equipment was undamaged, but Don’s personal computer anything else had been broken in one way or another. Don’s loft bed had even been knocked over, “I guess you had a rough night?”
“I guess.” Donnie picked through the box before looking to Leo for the first time since he entered the room,” Have you seen my phone?”
Leo thought back to that night before reaching into his satchel, “I found it in here last night, I’m sorta surprised you didn’t’ have it on you.”
“Thanks.” Donnie took the phone from him before setting it on his desk, calmly pulling out the head piece of his bust, and slamming the large piece of metal over phone a dozen or so times with such ferocity Leo leapt back to avoid the showing of metal and glass. He jumped back so far, he collided with the chest of his oldest brother who had come to investigate the noise, “What the hell just happened?!”
“Uh, “Leo wasn’t’ quite sure himself, “I think Donnie just destroyed his phone with his own face.”
“Would you two calm down,” Donnie called from his spot, “I have extras and it backed up to my server.”
Calming down would have been fun, except he had once seen Donnie yell at a kitten for looking at his phone. But instead he gave Raph a pat on the stomach, “I’ll take care of this go ahead.’” Except when he turned to walk back into the room, Raph grabbed his shoulder and yanked him out of the space hard enough to make Leo yelp in surprise. Spinning him till Leo was facing him, two giant hands on his shoulders as Raph glanced back into the bed room then to him, “Look I know you want to help Donnie, and that you’re way better at this then I am, but doesn’t it seem like you should leave him alone before he treats your face like his phone?”
“I know Donnie’s a little unpredictable sometimes, but I can handle him. It’s a twin thing, if there’s anyone who can help him chill out it’s Leon.”
Raph gave him a look that clearly said, ‘do you REALLY have this or are you just saying that to make me go away’ but did so anyway. For a few moments, Leo stood at the doorway as Donnie puttered around the boxes. Donnie glanced at his direction with enough heat to stop him. He probably would have stepped closer except Donnie still had a death grip on his bust and it was becoming more and more likely by the second. So instead he took a different approach, “Have you eaten yet Don?”
“I’ll eat later, there’s too much work to do.”
“I can see that.” He took a step deeper into the room again, “Do you want to talk about it?”
“No.”
That was about what he expected. Leo moved over to lean on Don’s desk. Without really thinking about it, he drifted his hand out to land on his brothers’ shoulder, “D, bro its me. It’s Leon Neon. You can talk to me ok man? Why don’t you tell me what happened at the Yokai Mart? Did you get mad at someone? Did you get lost- “
“I said no, now let it go. I went out, came back and now I’m working. End of story. Why don’t you go calm someone else down?”
A flush of shame filled him, of course Donnie had heard him say that. But he shook it off, “Come on you know I have to talk that way to Raph he doesn’t get you like I do.”
“Yeah you get me, you can read my mind, you can defuse me. Now leave, I have a room to rebuilt”
“Yeah it needs to be rebuilt because you destroyed it, don’t you understand that?!”
Don’s shoulder jerked free of his hand and turned to him, “I understand, Leo because I did it. I know what I did. If it had been or Mikey or even, you none of you would have given it a second thought. But because I have Autism, everyone’s freaked out. So, they have to send in the bomb squad.”
“Hey, I’m just trying to help, you’re the one who blew up- “
Before Leo could finish his thought, and to be honest he wasn’t sure wanted to before Donnie’s hands came up and shoved him hard in the chest. The red slider turtle stumbled back, his shell hitting the desk to his right with a crash before falling onto the ground. His head was spared any contact with the ground, but he looked at Donnie with shock, only to be met with the same shocked expression “Leo-I-I’m sorry are you alright?”
“Yeah, just a little bruised.” He was about to climb to his feet when Donnie quickly took his hand and yanked him up hard enough to make him stumble. He danced for a little bit to keep standing before turning his attention back to Donnie, his eyes swimming in tears. “D- “
“Can you please go now? I don’t want talk anymore.”
“I- “Leo paused,” Donnie- “he wanted to argue. He wanted to stay. He wanted to assure Donnie that he was fine, that he was still here to help him. But now his brother was trembling so hard he was afraid he would fall apart altogether. And he knew if he tried to hold him like he did last night, it would only make things worst.
Donnie didn’t want comfort, or a shoulder to cry on
He wanted to be alone.
“Ok. I’ll go. I’m sorry,” Leo took several steps back, unwilling to let his brother out of his sight incase he changed his mind and asked Leo to stay. But he knew better, “I love you bro.” he said before leaving through the curtain.
A moment later he heard Donnie burst into tears for the second time in twenty-four hours.
And he was left helpless
Part 1
Part 3
#shattered#rottmnt#rise of the teenage mutant ninja turtles#fanfiction#undercoverwizardninjaturtle#leo#leonardo#donnie#donatello#autism
168 notes
·
View notes
Note
Based on that one anons statement about the rottmnt fandom, I just wanted to say how cool it is about having a pretty well-experienced tmnt fan in the fandom... if that makes sense LOL Like, you have a lot more things to say and a better understanding on how people are in fandoms. It's hard to put into words, sorry. But it just makes the whole rottmnt fandom feel more chill whenever you give your thoughts and opinions. I always enjoy reading what you have to say. Much Love! 💕
Awww, THANK YOU. That really helps my confidence levels here, since I get anxious often about all my rambling.
And I do everything I can to not stir up too much ugliness that others can bring, because I remember being a fan in my teens and twenties and feeling so sure of everything. I see how easy that feeling is now with constant Social Media and immediate connection that I didn't have at that age. I got to grow up floating through the slowly growing fandom with each version. And the specifics would change but the interactions, the headcanon wars, those never changed. Every single petty argument has been done and I've seen it.
Sometimes I'll try to get between a fight but my words mess up and I have to just back away and watch fans hurt each other over.
For example, there were always heated disagreement over the Raph and Mikey dynamic in different versions but it exploded with 2012. See, after 2012 ended and our love affair waned, we really got into the different kinds of ways siblings acted... and to be honest I as an only child hated parts of the dynamic to the point where I wrote an entire AU full of love and apologies- but I also kept looking at the equally valid concerns of fans who saw nothing wrong and who kept saying it was normal. I had to take all sides into account because I didn't have experience. Which is what I seek in general. And then people began blatantly attacking fans who wanted to discuss the "abuse" aspect. It disturbed me. The fans headcanoning the unhealthy family dynamic struck back in defense and everything got really really bad. It went from "let's talk about the writing of these characters and how we the fans interpret it" to "if you think the characters are like this, you are wrong and deserve physical violence brought upon you" and it hurt to scroll through the tags for a while.
And then it seemed to fade as other arguments popped up, echoing the decades past, and when Rise happened, there was a little bit of disagreement over how it portrayed a family. Nothing vicious. And there was agreement across the board that Michelangelo was obviously portrayed and treated with more love and care, finally showing his ADHD artistic and psychic sensitive side since Mirage and Archie. So that right there brings fans together. Seeing Donnie with autistic traits that aren't stereotypical is also joining the fans, and part of me, as an ADHD Autistic, is both joyously elated and nervously worried because I desperately need to see both Donnie and Mikey with accurate representation regardless of whether or not canon confirms anything.
Like, I spent a decade headcanoning Mikey as autistic, just with very different traits, and I wound up writing a post on Don and Mike representing the varied circular twisting spectrum. And then other autistic fans brought up traits in Leo and Raph, all versions. And nowadays when I read fanfics written by autistics featuring autistic Leo or Raph, that nervous joy rears its head because I just want All Four to represent. And now that I with fellow advocate scholars are looking into ADHD as being on the Mobius spectrum of autism, there's a world of What Else Do The Ninja Turtles represent? coming into the fandom that before were less known due to smaller circles.
So, I love that you appreciate my insights, as random and ranty as they are. I do my best to ignore the fans who don't like my rambles (I got told "for once in your life just shut the fuck up" when they hadn't mentioned my being a problem before, and somehow it felt like my nerves were shivering taught strings caught on wire and it's still a vile sensation). I don't search for praise but I'll take it all when I get it.
I feel like the Rise fandom has some of the most creative, beautiful ideas for all sorts of AU What If stories, because there's the entire history of the franchise to bring in and pay tribute to. That's part of why I'm still here. The main part is, you know, sticking with my biggest autistic special interest that I've clung to since I was nine.
#Tmnt#thirty years with the ninja turtles#ninja turtles and the love of fans#rise of the teenage mutant ninja turtles#rottmnt spoilers#untitled rottmnt fanfic#yay angst#fandom history#tmnt fandom#i love this fandom#fandom grandma#tmnt history#my fandom friends#my fanfics#my fanfic#i created this tumblr because of michelangelo#neuropsychology of michelangelo#michelangelo is adhd and autistic like me#donatello is autistic obviously but so is michelangelo#the ninja turtles are autistic#the 2012 tmnt are all autistic#the 2012 tmnt are autistic#tmnt 2012 i'm looking at you#2003 mikey deserved better
17 notes
·
View notes
Text
Bias Game
This was so hard because my biases are not in stone!
I was tagged by: @heart-bleeding-autism-angel
Rules: List 10 biases and then answer the following questions
Kyuhyun (Super Junior)
Leo (VIXX)
Wonho (Monsta X)
Yuta (Nct)
Taeyong (Nct+ SuperM)
Yesung (Super Junior)
Hyesung (shinwa)
Youngjae (Got7)
Lucas (SuperM+WayV)
Hoshi (Seventeen)
Questions:
Between 1 and 4, who would you rather kiss?
This is so hard! um I am going to go with Yuta because he lips look really soft and kissable, if that makes sense.
Between 2 and 7, who would be your best friend?
Hyesung, because I think he would give good advice because he has seen and experienced more.
Between 5 and 10, who has a better voice?
Talking wise it is Taeyong because I find that his voice makes me happy and all smiley. Singing wise it is Hoshi because I love the uniqueness in his voice.
Between 1 and 8, who is the funniest?
Kyuhyun, he is known as the evil maknae for a reason.
Between 6 and 9, who would you date?
Lucas because his is closer to my real age and I like that he is dorky.
Between 4 and 8, who is the best dancer?
Even though Youngjae is a really good dancer but Yuta is the main dancer for a reason.
Between 3 and 5, who would you most likely to marry?
Probably Wonho because I feel like he would be the husband to encourage his wife to pursue her dreams and goals. I also feel like he would hype up his wife.
Between 1 and 7, who would you nurse when you’re sick?
Between Kyuhyun and Hyesung, I would be scared if Kyuhyun offered to help. so I am going with the safer option: Hyesung. Even though I would love to have both of them sing to me while I was sick.
Between 6 and 8, who would you rather have a vacation with?
Yesung if the vacation was suppose to be romantic because I feel like he is a very romantic person. In any other situation Youngjae, I feel like he would make any vacation really fun.
1 note
·
View note
Text
OC Ask Answers
I’ve been looking around at a bunch of random OC Ask prompts and been fleshing out my characters a little bit more with them here’s some of the answers. Some characters I can answer a lot more about and others I don’t know that much about yet. If anyone would like to know more about any of my characters I’d be happy to try and answer them. Gabby M.
Rooftop stargazing or meadow cloud watching?
-Definitely rooftop stargazing. Gabby loves watching the night sky she likes winding down from her work nights by watching the stars. Even though there’s a lot of light pollution in Origia, it’s so much smaller compared to the continents on earth that they got a bunch of stars in their night sky and Gabby really enjoys watching it. They also have two moons and that can lead to a bunch of fun astrological events.
Who will they take advice from, no matter what it is? Who won’t they take advice from, no matter what it is?
-Gabby almost always listens to Aeri. Aeri’s just got a certain confidence that Gabby is really drawn to, when they first met it changed Gabby’s life for the better and that’s caused Gabby to have a lot of trust in her. Meanwhile, Gabby will almost never listen to Ultra-Dude. He’s just not very competent in their eyes. They worked together for a little bit as part of the Ultra Wing when Gabby first got their powers but Ultra-Dude was always overconfident and self-absorbed so Gabby doesn’t put a lot of faith in him, often deferring to Officer Wheeler instead of Ultra-Dude.
Do they like fast food, or fancy restaurants? / What’s their dream job? Or do they simply not dream of labour?
-Gabby loves fast food. They work at a pizza delivery place and uses their teleportation to beat out the machine’s delivery speed. While working there, they often sneak some food despite the fact they get free food anyways. Since there’s a basic income everyone gets and their job can easily be done by the auto-trucks and drones, they don’t have to work anymore than they want to so Gabby’s really happy and enthusiastic about working there.
Does your OC believe in blood being thicker than water? (meaning family relationships and loyalties are the most important)
-Gabby’s definitely not a believer in this. They almost never interact with their family and are constantly with their chosen family. Their roommate Jake is one of their closest friends. Aeri originally was just a really flirty-type of friendship but that’s grown into an actual relationship. And Gabby and Taylor while still very new in their friendship, it will definitely grow as time moves on.
If you, the creator, met them, would you two get along?
-Oh my gosh, I hope so! Gabby was kind of originally a self-insert OC but as I’ve written them more and more they’ve definitely grown out of that and into their own character. So I feel like we’d have a lot in common as a result of that but it would still be fun. We’re both trans and I feel like that’s always a great starting place for friendships.
How would they fare in the zombie apocalypse?
-Assuming they had their powers, Gabby would do just fine. They could camp out on rooftops and with the vast cityscape that is Blanksford, they would be plenty of places to hide, and they could always teleport away if there was any trouble.
Madi V.
Are they open about their autism? Do they know they have it? Do they prefer to keep it to themselves rather than disclose?
-Neurodivergency isn’t treated the same in the Blanksford universe as it is in ours. It’s definitely not as stigmatized and understood a lot better. Madi does know she’s somewhat neurodivergent but doesn’t let it stop her or affect her life that much. She’ll keep it to herself in most situations but isn’t actively trying to hide it. She’s great with artistic tasks and gets along well with her CyVoice companion Blaine.
What was their childhood like?
-Madi’s parents divorced when she was 11. Her mother Rache really didn’t want to stay in Blanksford after the Blanksford Broadcast, her father Leo didn’t take it seriously and didn’t want to leave the life they had. Rache fought for custody but ultimately Leo convinced her that Madi really wouldn’t do well with the big life change. Madi didn’t have many friends but the few she did have, she really enjoyed being around. Madi’s father wasn’t very outward with his love for Madi and while she grew up their relationship became a lot worse. Madi never really talked with her mother after the divorce, but eventually they do get back in contact.
Aeri
What does your OC’s voice sound like?
-I like to imagine Aeri would be voiced by Ashly Burch. She’s my favorite voice actress and I loved her as Chloe Price in Life is Strange. But even her other roles like Ash Graven from Final Space and Aloy from Horizon: Zero Dawn sounds amazing and I really think would match up with Aeri as a character.
Do they wear makeup?
-Aeri is almost always wearing some make-up, she doesn’t have an abundance of self-confidence but she really tries her best to appear as though she does. The make-up she uses is very durable and doesn’t come off easily since she’s constantly flying around the city and doesn’t want it to be too affected.
Tell me about their thoughts on romance— are they in a relationship? Do they want to be? Are they a sappy, hopeless romance, or more of a “love is dead, romance is stupid” type?
-Normally Aeri’s been kind of loose cannon. Just dating to have a good time with new people and not so much looking for anything. Her relationship with Gabby is her longest relationship so far. She’s still very flirtatious with other people and constantly teases Gabby about it, but their relationship is doing surprisingly well for the both of them despite how different they are. She’s constantly caught off-guard by how much Gabby seems to be genuinely into her and will try to avoid a lot of the romance of their relationship because she’s just so unfamiliar with it, but Gabby’s patient with her and it’s slowly advancing.
Can they fight?
-Aeri’s not a great fighter but she knows how to handle herself and isn’t afraid to fight dirty to buy herself time to get out of a tough situation. Her powers of Aerokinesis can help her a bit, but she mostly tries to avoid fights despite how much trouble she can get into.
Taylor Che
Would they like to be famous? / How confident in themselves are they? Are they insecure, self-assured, or way too vain?
-Taylor’s really not that confident, but she’s found herself as one of the best sources for information about the supers in Blanksford. After that she even got powers of her own and is now very often caught in the spotlight. So while she never intended to be as known as she is, she’s doing her best to remain honest and true to her ideals. Before she got her powers she took a lot of pride in her blog about the supers and was able to justify her popularity based on her ability to have interesting takes and actually trying to ask the right questions. But now that her blog has gotten even more popular, she’ll occasionally doubt herself and wonder if her popularity is only based upon the fact the lucked into her superpowers.
Are they religious?
-No, there’s not really as much organized religion anywhere in Origia. There’s still a few that do and they’re free to worship, but Taylor isn’t one of them.
---
I didn’t expect to do this many when I started but I was having fun and ended up doing a lot more than I originally intended. I’ll probably do this again sometime soon because of how much I enjoyed it.
0 notes
Note
(P1)I know for your tarot guide you are planning a section on court cards but I still want to ask about them. I was at a local pagan meeting, specifically this was a tarot study group. I was talking to someone about how I have serious trouble with court cards. They said, well, how do you feel about people? And I said something like, I don't know, I'm not good at people. And he said well that's why you struggle with court cards, their just like people, figures in your life or parts of you...
(P2) they didn’t really give me more than that to go off of….well I still have problems with people, and with court cards!! I ended up getting diagnosed with autism a few months ago…which explains why I’m not so great with people. So how the heck can I relate with these court cards!? If I get them I just stare blankly. I can describe the rote meaning of the card but I can’t do more than that with it. It’s hard to interpret… is there anything you can recommend?
Yes, absolutely! There’s a variety of approaches to the court cards that don’t require a “people” based approach. You can approach them through their elements plus their numerology, their title’s approach to the element, their elemental mixtures, and even a zodiacal approach. This got long so under a readmore it goes.
Numerology + Elements
I’m a big fan of taking numerology into account if only because it helps one identify greater patterns within the spread. When I learned numerology, the system is for numbers greater than 9, you reduce them by adding the two digits together. This makes the Pages, number eleven, become twos. The Knights, number twelve, become threes. Queens as number thirteen become fours, And Kings as number fourteen become fives.
T(here’s another numerology idea that when you reach the teens, you take it as a more mature or experiences version of its ones digit. I.e. Pages as number eleven are more matured ones. This isn’t the system I use so I won’t discuss it much only because of a lack of familiarity but it’s still important to note you can use this approach too.)
With this approach, we get the following breakdown
Page of Wands = 2 + Fire = communication, crossroads, choice, balance, duality, choice + passion, desire, motivation, spirituality
Knight of Wands = 3 + Fire = growth, creativity, expression + passion, desire, motivation, spirituality
Queen of Wands = 4 + Fire = stability, structure, foundation, rigidity, stagnation + passion, desire, motivation, spirituality
King of Wands = 5 + Fire = challenge when overcome leads to beginning of a new cycle and mastery + passion, desire, motivation, spirituality
Page of Cups = 2 + Water = communication, crossroads, choice, balance, duality, choice + emotions, subconscious, dreams, empathy, intuition
Knight of Cups = 3 + Water = growth, creativity, expression + emotions, subconscious, dreams, empathy, intuition
Queen of Cups = 4 + Water = stability, structure, foundation, rigidity, stagnation + emotions, subconscious, dreams, empathy, intuition
King of Cups = 5 + Water = challenge when overcome leads to beginning of a new cycle and mastery + emotions, subconscious, dreams, empathy, intuition
Page of Swords = 2 + Air = communication, crossroads, choice, balance, duality, choice + communication, ideas, power, thought, intellect
Knight of Swords = 3 + Air = growth, creativity, expression + communication, ideas, power, thought, intellect
Queen of Swords = 4 + Air = stability, structure, foundation, rigidity, stagnation + communication, ideas, power, thought, intellect
King of Swords = 5 + Air = challenge when overcome leads to beginning of a new cycle and mastery + communication, ideas, power, thought, intellect
Page of Pentacles = 2 + Earth = communication, crossroads, choice, balance, duality, choice + growth, material things, self esteem, wisdom, nurturing
Knight of Pentacles = 3 + Earth = growth, creativity, expression + growth, material things, self esteem, wisdom, nurturing
Queen of Pentacles = 4 + Earth = stability, structure, foundation, rigidity, stagnation + growth, material things, self esteem, wisdom, nurturing
King of pentacles = 5 + Earth = challenge when overcome leads to beginning of a new cycle and mastery + growth, material things, self esteem, wisdom, nurturing
Their Title + Elements
Each title/rank of the tarot court has a differing focus and purpose. When you combine these with their elemental and suit associations you can get a really good idea of what the court card is all about!
Pages - Pages are messengers and initiators. They are just beginning to learn their suits. Thus, they have an aspect of youthfulness about them. This has historically associated them with children but when dealing with a person-based approach, it can also just indicate a youthful spirit. Pages are kind of like the Fools of the major arcana but in a specific area, just beginning to learn how to master their area of focus.
Knights - These are the knights of the Holy Grail, seeking the Grail of Knowledge of their respective suits. They go out into the world seeking answers. Thus they are constantly trying to express their suits, bringing them out into the physical world. The knights wear their suits on their sleeves and often aren’t subtle.
Queens - Queens are nurturers. They try to create environments where their suits can flourish. They are fond of stability as such. Stability and constancy make for better growth. The queens are more of a surrounding influence, more subtle to notice than the knights by far, but also more mastered of their suits.
Kings - Kings are the masters of their suits. They have wrestled with them until they’ve learned them inside and out. The kings as such represent maturity and wisdom in specific areas. The Kings in turn challenge us to become more mature and to master these suits, asking us to make their commitment to knowledge. They challenge and push us so that we become stronger and better in these areas.
Elemental Expressions
In the Golden Dawn tradition, the court cards represent different sides of the elements within their suits. If you’re strongly inclined towards the occult associations of the elements, this method could prove useful to you.
The Pages represent mixtures of earth and their respective element. Earth is solid, fertile, and generative. I’ve seen the Page of Fire described as fire’s generative property, the Page of Cups as crystallized snow, the Page of Swords is the air trapped within the earth, and the Page of Disks is the fertility of the earth.
The Knights represent mixtures of air and their respective elements. They’re expansive and mobile. The Knight of Wands is smoky, the Knight of Cups is like steam, the Knight of Swords is air unrestrained always moving and spreading outwards, and the Knight of Pentacles is the fruits of the earth.
The Queens are water plus their respective elements. They’re flowing and adaptive. The Queen of Wands is the “receptivity” of fire, its movement and shifting color. The Queen of Cups is the depth of water, hidden and secretive. The Queen of Swords is the rain-filled and darkened sky. The Queen of Pentacles is described as the earth’s fertility but more the actual earth itself than what is beginnig to grow like the Page is.
The Kings are fire plus their respective elements. The King of Wands is pure fire, hungry and destructive but transformative. The King of Cups is the stormy destructive side of water, its wrath and fury that leaves us washed pure and clean. The King of Swords is the Wind sweeping unrestrained across the earth, powerful and free. The King of Pentacles is the embodiment of the earth’s creative prowess.
Zodiacal Approach
You can also approach the court cards from the zodiacal perspective if astrology is your thing. When doing a zodical approach, I’ve seen slight variations on which rank gets associated with which quality. In the Golden Dawn tradition if we simplify it, the Knights are associated with the Fixed zodiac signs of Wands as Leo, Cups as Scorpio, Swords as Aquarius, and Pentacles as Taurus. In the Golden Dawn Tradition, this makes the Kings the Mutable signs making Wands as Sagittarius, Cups as Pisces, Swords as Gemini, and Pentacles as Virgo. This leaves the Queens as the Cardinal signs of Wands as Aries, Cups as Cancer, Swords as Libra, and Pentacles as Capricorn. The Pages are not assigned zodiacal associations for reasons I haven’t read because I am not that invested in Golden Dawn stuff. > >” However, this is probably the best known system and the most written on system.
This isn’t the only system I’ve seen, though. I’ve also seen the Knights be the Mutable signs and the Kings as the Fixed signs.This eaves the Queens still as the Cardinal signs. Additionally, I know the tradition of the zodiacal associations my mom learned is different from these because she uses the Queen of Swords as a signifier because in her learning, the Queen of Swords is associated with Aquarius. But Aquarius is a fixed sign so her tradition assigns the fixed signs to the queens.
You’re probably looking at this and going well, if I were to use this method then, which one is best? I’ll be honest, I haven’t read the Golden Dawn justifications for the system it has. From what I know of the signs and modalities, however, I’m not sure I agree with it in full. But that’s another post in and of itself to argue over. In any case, I’d recommend the Golden Dawn if only because it’s the most well-written on system afaik and therefore you’d most likely find resources to help you. So as a recap, if using the Golden Dawn system, that would leave you with the followingKnight of Wands - LeoQueen of Wands - AriesKing of Wands - SagittariusKnight of Cups - ScorpioQueen of Cups - CancerKing of Cups - PiscesKnight of Swords - AquariusQueen of Swords - LibraKing of Swords - GeminiKnight of Pentacles - TaurusQueen of Pentacles - CapricornKing of Pentacles - Virgo
Putting these all together
And just to make sure this is actually useful, here’s a way of putting these together. I’m going to select the Knight of Cups because I can.
So if we look at the Knight of Cups, we have plenty to work with: Water as an element as well as its mixture with Air, the suit of Cups, his rank as Knight, his number, and even his zodiacal association.
The Knight of Cups is a numerological three when reduced. It takes the lessons of the two and ones and combines.them so that things may be /expressed/. What is the knight expressing? They are expressing emotions, intuition, dreams, and the realm of the subconscious. They are a mixture of water and air making them ever-moving and potentially volatile form too much expansion of the emotions. Too much too fast. This is because they’re so actively seeking as they are a Knight but they lack the experience and maturity of the Queen and King to know how to handle the emotions they’re seeking out. They express emotions especially by wearing their heart on their sleeve. Zodiac-wise, they are Scorpio. Scorpio is intense and secretive. At its worst, Scorpio can sting itself to death. At its best, however, it turns into a protective and noble eagle, using its insights to help others. As this is a Cups card, this help would come in the realm of emotions.
So overall, we’re getting a picture of an emotionally intense individual. Emboldened by lessons learned as a Page, the Knight is now delving deeper into the realm of the subconscious. They often move too fast though and in their reversed form they bring out emotions they cannot handle. They have expanded far too quickly. Upright, they’re expanding their scope at the right pace. Growing, wearing their heart proudly on their sleeve. Reversed, this brings danger as they’re lashing out at people. Upright, it symbolizes the willingness to be emotionally genuine and vulnerable. Upright, they are noble and helpful, a protective force to those struggling with troubling emotions. They help give us the courage to delve into our subconscious and express our own emotions.
Hopefully some of this helps?
19 notes
·
View notes
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://ift.tt/2yiM0Yd" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don’t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody.
Source: http://chriskresser.com November 08, 2017 at 04:12PM
1 note
·
View note
Text
You think you know....
It is an often repeated fallacy that there is no research that supports the supposition that vaccines can cause autism. This talking point is most often repeated by medical personnel and public health officials who have simply never been told that these studies exist, and in some cases by those who refuse to read the information when it is offered to them, so they continue to labor under the false assumption that vaccine autism causation is merely an “internet rumor” or a result of one paper that was published in 1998.
This untruth was again testified to during the HHS Committee hearings
In fact, the first research paper to offer evidence that vaccines may cause autism was THE first paper ever written on autism. In the 1930’s, Child Psychiatrist Leo Kanner discovered 11 children over the course of several years who displayed a novel set of neurological symptoms that had never been described in the medical literature, where children were withdrawn, uncommunicative and displayed similar odd behaviors. This disorder would become known as “autism.” In the paper, Dr. Kanner noted that onset of the disorder began following the administration of a small pox vaccine. This paper, was published in 1943, and evidence that vaccination causes an ever increasing rate of neurological and immunological regressions, including autism, has been mounting from that time until now.
Autistic Disturbances of Affective Contact
Leo Kanner, Johns Hopkins University, 1943
“Since 1938, there have come to our attention a number of children whose condition differs so markedly and uniquely from anything reported so far, that each case merits – and, I hope, will eventually receive – at detailed consideration of its fascinating peculiarities.”
All of Kanners cases were born after, and began to appear following, the introduction of Eli Lilly’s new form of water soluble mercury in the late 1920s used as an anti-fungal in forestry, a wood treatment product in the lumber industry and as a disinfectant and anti-bacterial in the medical industry under the name of “Thimerosal” that was included in vaccines.
For further information on the early evidence of a vaccine/connection, I recommend reading Dr. Bryan Jepson’s book, “Changing the Course of Autism: A Scientific Approach for Parents and Physicians,” as well as Mark Blaxill and Dan Olmseted’s new book “The Age of Autism: Mercury, Medicine, and a Man-made Epidemic.”
As I testified to at the hearing, there is abundant research supporting the vaccine autism link. I have included 49 research papers for your review, and only included research published in the last ten years or so. This is by no means a complete list, but it one that I have been compiling for the last few years as relevant research came to my attention. I have ONLY included autism related information, not research on other vaccine injuries of which there are many.
As you can see, the medical professionals testifying that there is no scientific support for the vaccine/autism causation theory are uninformed about the current state of the science. When vaccination decisions are made based on an uninformed opinion, it means serious potential damage to the patient, and because of the law preventing lawsuits for vaccine injury, it also means that the uninformed medical professionals making bad recommendations CANNOT be held accountable in any way for giving the patient bad information.
Parents want to know if their child can develop autism from their vaccines. If they believe that the answer is yes, and the risk of brain injury from vaccination is higher than their risk from a disease, it is their right to decline vaccination for themselves and their children with out coercion.
Patients MUST be able to make their own informed vaccine decisions, because often, they know more about potential vaccine risks that even top public health officials do.
1. Hepatitis B Vaccination of Male Neonates and Autism
Annals of Epidemiology , Vol. 19, No. 9 ABSTRACTS (ACE), September 2009: 651-680, p. 659
CM Gallagher, MS Goodman, Graduate Program in Public Health, Stony Brook University Medical Center, Stony Brook, NY
PURPOSE: Universal newborn immunization with hepatitis B vaccine was recommended in 1991; however, safety findings are mixed. The Vaccine Safety Datalink Workgroup reported no association between hepatitis B vaccination at birth and febrile episodes or neurological adverse events. Other studies found positive associations between hepatitis B vaccination and ear infection, pharyngitis, and chronic arthritis; as well as receipt of early intervention/special education services (EIS); in probability samples of U.S. children. Children with autistic spectrum disorder (ASD) comprise a growing caseload for EIS. We evaluated the association between hepatitis B vaccination of male neonates and parental report of ASD.
METHODS: This cross-sectional study used U.S. probability samples obtained from National Health Interview Survey 1997-2002 datasets. Logistic regression modeling was used to estimate the effect of neonatal hepatitis B vaccination on ASD risk among boys age 3-17 years with shot records, adjusted for race, maternal education, and two-parent household.
RESULTS: Boys who received the hepatitis B vaccine during the first month of life had 2.94 greater odds for ASD (nZ31 of 7,486; OR Z 2.94; p Z 0.03; 95% CI Z 1.10, 7.90) compared to later- or unvaccinated boys. Non-Hispanic white boys were 61% less likely to have ASD (ORZ0.39; pZ0.04; 95% CIZ0.16, 0.94) relative to non-white boys.
CONCLUSION: Findings suggest that U.S. male neonates vaccinated with hepatitis B vaccine had a 3-fold greater risk of ASD; risk was greatest for non-white boys.
2. Porphyrinuria in childhood autistic disorder: Implications for environmental toxicity
Toxicology and Applied Pharmacology, 2006
Robert Natafa, Corinne Skorupkab, Lorene Ametb, Alain Lama, Anthea Springbettc and Richard Lathed, aLaboratoire Philippe Auguste, Paris, France, Association ARIANE, Clichy, France, Department of Statistics, Roslin Institute, Roslin, UK, Pieta Research,
This new study from France utilizes a new and sophisticated measurement for environmental toxicity by assessing porphyrin levels in autistic children. It provides clear and unequivocal evidence that children with autism spectrum disorders are more toxic than their neurotypical peers.
Excerpt: "Coproporphyrin levels were elevated in children with autistic disorder relative to control groups...the elevation was significant. These data implicate environmental toxicity in childhood autistic disorder."
Abstract: To address a possible environmental contribution to autism, we carried out a retrospective study on urinary porphyrin levels, a biomarker of environmental toxicity, in 269 children with neurodevelopmental and related disorders referred to a Paris clinic (2002–2004), including 106 with autistic disorder. Urinary porphyrin levels determined by high-performance liquid chromatography were compared between diagnostic groups including internal and external control groups. Coproporphyrin levels were elevated in children with autistic disorder relative to control groups. Elevation was maintained on normalization for age or to a control heme pathway metabolite (uroporphyrin) in the same samples. The elevation was significant (P < 0.001). Porphyrin levels were unchanged in Asperger's disorder, distinguishing it from autistic disorder. The atypical molecule precoproporphyrin, a specific indicator of heavy metal toxicity, was also elevated in autistic disorder (P < 0.001) but not significantly in Asperger's. A subgroup with autistic disorder was treated with oral dimercaptosuccinic acid (DMSA) with a view to heavy metal removal. Following DMSA there was a significant (P = 0.002) drop in urinary porphyrin excretion. These data implicate environmental toxicity in childhood autistic disorder.
3. Theoretical aspects of autism: Causes—A review
Journal of Immunotoxicology, January-March 2011, Vol. 8, No. 1 , Pages 68-79
Helen V. Ratajczak, PhD
Autism, a member of the pervasive developmental disorders (PDDs), has been increasing dramatically since its description by Leo Kanner in 1943. First estimated to occur in 4 to 5 per 10,000 children, the incidence of autism is now 1 per 110 in the United States, and 1 per 64 in the United Kingdom, with similar incidences throughout the world. Searching information from 1943 to the present in PubMed and Ovid Medline databases, this review summarizes results that correlate the timing of changes in incidence with environmental changes. Autism could result from more than one cause, with different manifestations in different individuals that share common symptoms. Documented causes of autism include genetic mutations and/or deletions, viral infections, and encephalitis following vaccination. Therefore, autism is the result of genetic defects and/or inflammation of the brain. The inflammation could be caused by a defective placenta, immature blood-brain barrier, the immune response of the mother to infection while pregnant, a premature birth, encephalitis in the child after birth, or a toxic environment.
4. Uncoupling of ATP-mediated Calcium Signaling and Dysregulated IL-6 Secretion in Dendritic Cells by Nanomolar Thimerosal
Environmental Health Perspectives, July 2006.
Samuel R. Goth, Ruth A. Chu Jeffrey P. Gregg
This study demonstrates that very low-levels of Thimerosal can contribute to immune system disregulation.
Excerpt: "Our findings that DCs primarily express the RyR1 channel complex and that this complex is uncoupled by very low levels of THI with dysregulated IL-6 secretion raise intriguing questions about a molecular basis for immune dyregulation and the possible role of the RyR1 complex in genetic susceptibility of the immune system to mercury."
Abstract Dendritic cells (DCs), a rare cell type widely distributed in the soma, are potent antigen presenting cells that initiate primary immune responses. DCs rely on intracellular redox state and calcium (Ca2+) signals for proper development and function, but the relationship between these two signaling systems is unclear. Thimerosal (THI) is a mercurial used to preserve vaccines, consumer products, and experimentally to induce Ca2+ release from microsomal stores. We tested ATP-mediated Ca2+ responses of DCs transiently exposed to nanomolar THI. Transcriptional and immunocytochemical analyses show murine myeloid immature and mature DC (IDCs, MDCs) express inositol 1, 4, 5-trisphosphate and ryanodine receptor (IP3R, RyR) Ca2+ channels, known targets of THI. IDCs express the RyR1 isoform in a punctate distribution that is densest near plasma membranes and within dendritic processes whereas IP3Rs are more generally distributed. RyR1 positively and negatively regulates purinergic signaling since ryanodine (Ry) blockade (1) recruited 80 percent more ATP responders, (2) shortened ATP-mediated Ca2+ transients >2-fold, (3) and produced a delayed and persistent rise (≥2-fold) in baseline Ca2+. THI (100nM, 5min) recruited more ATP responders, shortened the ATP-mediated Ca2+ transient (≥1.4- fold) and produced a delayed rise (≥3-fold) in the Ca2+ baseline, mimicking Ry. THI and Ry, in combination, produced additive effects leading to uncoupling of IP3R and RyR1 signals. THI altered ATP-mediated IL-6 secretion, initially enhancing the rate of but suppressing overall cytokine secretion in DCs. DCs are exquisitely sensitive to THI, with one mechanism involving the uncoupling of positive and negative regulation of Ca2+ signals contributed by RyR1.
5. Gender-selective toxicity of thimerosal.
Exp Toxicol Pathol. 2009 Mar;61(2):133-6. Epub 2008 Sep 3.
Branch DR, Departments of Medicine and Laboratory Medicine and Pathobiology, University of Toronto, Ontario, Canada.
Abstract A recent report shows a correlation of the historical use of thimerosal in therapeutic immunizations with the subsequent development of autism; however, this association remains controversial. Autism occurs approximately four times more frequently in males compared to females; thus, studies of thimerosal toxicity should take into consideration gender-selective effects. The present study was originally undertaken to determine the maximum tolerated dose (MTD) of thimersosal in male and female CD1 mice. However, during the limited MTD studies, it became apparent that thimerosal has a differential MTD that depends on whether the mouse is male or female. At doses of 38.4-76.8mg/kg using 10% DMSO as diluent, seven of seven male mice compared to zero of seven female mice tested succumbed to thimerosal. Although the thimerosal levels used were very high, as we were originally only trying to determine MTD, it was completely unexpected to observe a difference of the MTD between male and female mice. Thus, our studies, although not directly addressing the controversy surrounding thimerosal and autism, and still preliminary due to small numbers of mice examined, provide, nevertheless, the first report of gender-selective toxicity of thimerosal and indicate that any future studies of thimerosal toxicity should take into consideration gender-specific differences.
6. Comparison of Blood and Brain Mercury Levels in Infant Monkeys Exposed to Methylmercury or Vaccines Containing Thimerosal
Environmental Health Perspectives, Aug 2005.
Thomas Burbacher, PhD [University of Washington].
This study demonstrates clearly and unequivocally that ethyl mercury, the kind of mercury found in vaccines, not only ends up in the brain, but leaves double the amount of inorganic mercury as methyl mercury, the kind of mercury found in fish. This work is groundbreaking because little is known about ethyl mercury, and many health authorities have asserted that the mercury found in vaccines is the "safe kind." This study also delivers a strong rebuke of the Institute of Medicine's recommendation in 2004 to no longer pursue the mercury-autism connection.
Excerpt: "A recently published IOM review (IOM 2004) appears to have abandoned the earlier recommendation [of studying mercury and autism] as well as back away from the American Academy of Pediatrics goal [of removing mercury from vaccines]. This approach is difficult to understand, given our current limited knowledge of the toxicokinetics and developmental neurotoxicity of thimerosal, a compound that has been (and will continue to be) injected in millions of newborns and infants."
7. Increases in the number of reactive glia in the visual cortex of Macaca fascicularis following subclinical long-term methyl mercury exposure.
Toxicology and Applied Pharmacology, 1994
Charleston JS, Bolender RP, Mottet NK, Body RL, Vahter ME, Burbacher TM., Department of Pathology, School of Medicine, University of Washington
The number of neurons, astrocytes, reactive glia, oligodendrocytes, endothelia, and pericytes in the cortex of the calcarine sulcus of adult female Macaca fascicularis following long-term subclinical exposure to methyl mercury (MeHg) and mercuric chloride (inorganic mercury; IHg) has been estimated by use of the optical volume fractionator stereology technique. Four groups of monkeys were exposed to MeHg (50 micrograms Hg/kg body wt/day) by mouth for 6, 12, 18, and 12 months followed by 6 months without exposure (clearance group). A fifth group of monkeys was administered IHg (as HgCl2; 200 micrograms Hg/kg body wt/day) by constant rate intravenous infusion via an indwelling catheter for 3 months. Reactive glia showed a significant increase in number for every treatment group, increasing 72% in the 6-month, 152% in the 12-month, and 120% in the 18-month MeHg exposed groups, and the number of reactive glia in the clearance group remained elevated (89%). The IHg exposed group showed a 165% increase in the number of reactive glia. The IHg exposed group and the clearance group had low levels of MeHg present within the tissue; however, the level of IHg was elevated in both groups. These results suggest that the IHg may be responsible for the increase in reactive glia. All other cell types, including the neurons, showed no significant change in number at the prescribed exposure level and durations. The identities of the reactive glial cells and the implications for the long-term function and survivability of the neurons due to changes in the glial population following subclinical long-term exposure to mercury are discussed.
8. Neuroglial Activation and Neuroinflammation in the Brain of Patients with Autism
Annals of Neurology, Feb 2005.
Diana L. Vargas, MD [Johns Hopkins University].
This study, performed independently and using a different methodology than Dr. Herbert (see above) reached the same conclusion: the brains of autistic children are suffering from inflammation.
Excerpt: "Because this neuroinflammatory process appears to be associated with an ongoing and chronic mechanism of CNS dysfunction, potential therapeutic interventions should focus on the control of its detrimental effects and thereby eventually modify the clinical course of autism."
9. Autism: A Brain Disorder, or A Disorder That Affects the Brain?
Clinical Neuropsychiatry, 2005
Martha R. Herbert M.D., Ph.D., Harvard University
Autism is defined behaviorally, as a syndrome of abnormalities involving language, social reciprocity and hyperfocus or reduced behavioral flexibility. It is clearly heterogeneous, and it can be accompanied by unusual talents as well as by impairments, but its underlying biological and genetic basis in unknown. Autism has been modeled as a brain-based, strongly genetic disorder, but emerging findings and hypotheses support a broader model of the condition as a genetically influenced and systemic. These include imaging, neuropathology and psychological evidence of pervasive (and not just specific) brain and phenotypic features; postnatal evolution and chronic persistence of brain, behavior and tissue changes (e.g. inflammation) and physical illness symptomatology (e.g. gastrointestinal, immune, recurrent infection); overlap with other disorders; and reports of rate increases and improvement or recovery that support a role for modulation of the condition by environmental factors (e.g. exacerbation or triggering by toxins, infectious agents, or others stressors, or improvement by treatment). Modeling autism more broadly encompasses previous work, but also encourages the expansion of research and treatment to include intermediary domains of molecular and cellular mechanisms, as well as chronic tissue, metabolic and somatic changes previously addressed only to a limited degree. The heterogeneous biologies underlying autism may conceivably converge onto the autism profile via multiple mechanisms on the one hand and processing and connectivity abnormalities on the other may illuminate relevant final common pathways and contribute to focusing on the search for treatment targets in this biologically and etiologically heterogeneous behavioral syndrome.
10. Activation of Methionine Synthase by Insulin-like Growth Factor-1 and Dopamine: a Target for Neurodevelopmental Toxins and Thimerosal
Molecular Psychiatry, July 2004.
Richard C. Deth, PhD [Northeastern University].
This study demonstrates how Thimerosal inhibits methylation, a central driver of cellular communication and development. Excerpt:
"The potent inhibition of this pathway [methylation] by ethanol, lead, mercury, aluminum, and thimerosal suggests it may be an important target of neurodevelopmental toxins."
11. Validation of the Phenomenon of Autistic Regression Using Home Videotapes
Archives of General Psychiatry, 2005
Emily Werner, PhD; Geraldine Dawson, PhD, University of Washington
Objective To validate parental report of autistic regression using behavioral data coded from home videotapes of children with autism spectrum disorder (ASD) vs typical development taken at 12 and 24 months of age.
Design Home videotapes of 56 children’s first and second birthday parties were collected from parents of young children with ASD with and without a reported history of regression and typically developing children. Child behaviors were coded by raters blind to child diagnosis and regression history. A parent interview that elicited information about parents’ recall of early symptoms from birth was also administered.
Setting Participants were recruited from a multidisciplinary study of autism conducted at a major university.
Participants Fifteen children with ASD with a history of regression, 21 children with ASD with early-onset autism, and 20 typically developing children and their parents participated.
Main Outcome Measures Observations of children’s communicative, social, affective, repetitive behaviors, and toy play coded from videotapes of the toddlers’ first and second birthday parties.
Results Analyses revealed that infants with ASD with regression show similar use of joint attention and more frequent use of words and babble compared with typical infants at 12 months of age. In contrast, infants with ASD with early onset of symptoms and no regression displayed fewer joint attention and communicative behaviors at 12 months of age. By 24 months of age, both groups of toddlers with ASD displayed fewer instances of word use, vocalizations, declarative pointing, social gaze, and orienting to name as compared with typically developing 24-month-olds.
Parent interview data suggested that some children with regression displayed difficulties in regulatory behavior before the regression occurred.
Conclusion This study validates the existence of early autistic regression.
UPDATE: Since the Poling Case, this has become a popular link, so I will update it with more research and better information so that you can actually find and read the articles. Below is a partial list that I will keep adding to.
12. Blood Levels of Mercury Are Related to Diagnosis of Autism: A Reanalysis of an Important Data Set
Journal of Child Neurology, Vol. 22, No. 11, 1308-1311 (2007)
M. Catherine DeSoto, PhD, Robert T. Hitlan, PhD -Department of Psychology, University of Northern Iowa, Cedar Falls, Iowa
Excerpt: “We have reanalyzed the data set originally reported by Ip et al. in 2004 and have found that the original p value was in error and that a significant relation does exist between the blood levels of mercury and diagnosis of an autism spectrum disorder. Moreover, the hair sample analysis results offer some support for the idea that persons with autism may be less efficient and more variable at eliminating mercury from the blood.”
Abstract
The question of what is leading to the apparent increase in autism is of great importance. Like the link between aspirin and heart attack, even a small effect can have major health implications. If there is any link between autism and mercury, it is absolutely crucial that the first reports of the question are not falsely stating that no link occurs. We have reanalyzed the data set originally reported by Ip et al. in 2004 and have found that the original p value was in error and that a significant relation does exist between the blood levels of mercury and diagnosis of an autism spectrum disorder. Moreover, the hair sample analysis results offer some support for the idea that persons with autism may be less efficient and more variable at eliminating mercury from the blood.
13. Developmental Regression and Mitochondrial Dysfunction in a Child With Autism
Journal of Child Neurology / Volume 21, Number 2, February 2006 Jon S. Poling, MD, PhD, Department of Neurology and Neurosurgery Johns Hopkins Hospital
This article showed that 38% of Kennedy Krieger Institute autism patients studied had one marker for impaired oxidative phosphorylation (mitochondrial dysfunction), and 47% had a second marker.
Excerpt: "Children who have (mitochondrial-related) dysfunctional cellular energy metabolism might be more prone to undergo autistic regression between 18 and 30 months of age if they also have infections or immunizations at the same time.”
14. Oxidative Stress in Autism: Elevated Cerebellar 3-nitrotyrosine Levels
American Journal of Biochemistry and Biotechnology 4 (2): 73-84, 2008
Elizabeth M. Sajdel-Sulkowska, - Dept of Psychiatry, Harvard Medical School
Shows a potential link between mercury and the autopsied brains of young people with autism. A marker for oxidative stress was 68.9% higher in autistic brain issue than controls (a statistically significant result), while mercury levels were 68.2% higher.
Excerpt: The preliminary data suggest a need for more extensive studies of oxidative stress, its relationship to the environmental factors and its possible attenuation by antioxidants in autism.”
15. Large Brains in Autism: The Challenge of Pervasive Abnormality
The Neuroscientist, Volume 11, Number 5, 2005.
Martha Herbert, MD, PhD, Harvard University
This study helps refute the notion that the brains of autistic children are simply wired differently and notes, "neuroinflammation appears to be present in autistic brain tissue from childhood through adulthood." Dr. Herbert suggests that chronic disease or an external environmental source (like heavy metals) may be causing the inflammation.
Excerpt: "Oxidative stress, brain inflammation, and microgliosis have been much documented in association with toxic exposures including various heavy metals...the awareness that the brain as well as medical conditions of children with autism may be conditioned by chronic biomedical abnormalities such as inflammation opens the possibility that meaningful biomedical interventions may be possible well past the window of maximal neuroplasticity in early childhood because the basis for assuming that all deficits can be attributed to fixed early developmental alterations in neural architecture has now been undermined."
Abstract
The most replicated finding in autism neuroanatomy—a tendency to unusually large brains—has seemed paradoxical in relation to the specificity of the abnormalities in three behavioral domains that define autism. We now know a range of things about this phenomenon, including that brains in autism have a growth spurt shortly after birth and then slow in growth a few short years afterward, that only younger but not older brains are larger in autism than in controls, that white matter contributes disproportionately to this volume increase and in a nonuniform pattern suggesting postnatal pathology, that functional connectivity among regions of autistic brains is diminished, and that neuroinflammation (including microgliosis and astrogliosis) appears to be present in autistic brain tissue from childhood through adulthood. Alongside these pervasive brain tissue and functional abnormalities, there have arisen theories of pervasive or widespread neural information processing or signal coordination abnormalities (such as weak central coherence, impaired complex processing, and underconnectivity), which are argued to underlie the specific observable behavioral features of autism. This convergence of findings and models suggests that a systems- and chronic disease–based reformulation of function and pathophysiology in autism needs to be considered, and it opens the possibility for new treatment targets.
16. Evidence of Toxicity, Oxidative Stress, and Neuronal Insult in Autism
Journal of Toxicology and Environmental Health, Nov-Dec 2006.
Janet Kern, Anne Jones, Department of Psychiatry, University of Texas Southwestern Medical Center at Dallas, Dallas, Texas, USA
"This article discusses the evidence for the case that some children with autism may become autistic from neuronal cell death or brain damage sometime after birth as result of insult; and addresses the hypotheses that toxicity and oxidative stress may be a cause of neuronal insult in autism... the article discusses what may be happening over the course of development and the multiple factors that may interplay and make these children more vulnerable to toxicity, oxidative stress, and neuronal insult."
Abstract
According to the Autism Society of America, autism is now considered to be an epidemic. The increase in the rate of autism revealed by epidemiological studies and government reports implicates the importance of external or environmental factors that may be changing. This article discusses the evidence for the case that some children with autism may become autistic from neuronal cell death or brain damage sometime after birth as result of insult; and addresses the hypotheses that toxicity and oxidative stress may be a cause of neuronal insult in autism. The article first describes the Purkinje cell loss found in autism, Purkinje cell physiology and vulnerability, and the evidence for postnatal cell loss. Second, the article describes the increased brain volume in autism and how it may be related to the Purkinje cell loss. Third, the evidence for toxicity and oxidative stress is covered and the possible involvement of glutathione is discussed. Finally, the article discusses what may be happening over the course of development and the multiple factors that may interplay and make these children more vulnerable to toxicity, oxidative stress, and neuronal insult.
17. Oxidative Stress in Autism
Pathophysiology, 2006.
Abha Chauhan, Ved Chauhan
This study provides a helpful overview of the growing evidence supporting the link between oxidative stress and autism.
Excerpt: "Upon completion of this article, participants should be able to: 1. Be aware of laboratory and clinical evidence of greater oxidative stress in autism. 2. Understand how gut, brain, nutritional, and toxic status in autism are consistent with greater oxidative stress. 3. Describe how anti-oxidant nutrients are used in the contemporary treatment of autism."
18. Thimerosal Neurotoxicity is Associated with Glutathione Depletion: Protection with Glutathione Precursors
Neurotoxicology, Jan 2005.
S. Jill James, PhD [University of Arkansas].
This recent study demonstrates that Thimerosal lowers or inhibits the body's ability to produce Glutathione, an antioxidant and the body's primary cellular-level defense against mercury.
Excerpt: "Thimerosal-induced cytotoxicity was associated with depletion of intracellular Glutathione in both cell lines...The potential effect of Glutathione or N-acetylcysteine against mercury toxicity warrants further research as possible adjunct therapy to individuals still receiving Thimerosal-containing vaccines."
19. Aluminum adjuvant linked to gulf war illness induces motor neuron death in mice
Neuromolecular Medicine, 2007
Christopher Shaw, Ph.D. [Department of Ophthalmology and Program in Neuroscience, University of British Columbia, Vancouver, British Columbia, Canada]
This study demonstrates the extreme toxicity of the aluminum adjuvant used as a preservative in vaccines.
Excerpt: "testing showed motor deficits in the aluminum treatment group that expressed as a progressive decrease in strength measured...Significant cognitive deficits in water-maze learning were observed in the combined aluminum and squalene group...Apoptotic neurons were identified in aluminum-injected animals that showed significantly increased activated caspase-3 labeling in lumbar spinal cord (255%) and primary motor cortex (192%) compared with the controls. Aluminum-treated groups also showed significant motor neuron loss (35%) and increased numbers of astrocytes (350%) in the lumbar spinal cord.
20. Environmental mercury release, special education rates, and autism disorder: an ecological study of Texas
Health & Place, 2006
Raymond F. Palmer, University of Texas Health Science Center
This study demonstrated the correlation between environmental mercury and autism rates in Texas.
Excerpt: "On average, for each 1,000 lb of environmentally released mercury, there was a 43% increase in the rate of special education services and a 61% increase in the rate of autism. The association between environmentally released mercury and special education rates were fully mediated by increased autism rates. This ecological study suggests the need for further research regarding the association between environmentally released mercury and developmental disorders such as autism."
21. Autism Spectrum Disorders in Relation to Distribution of Hazardous Air Pollutants in the SF Bay Area
Environmental Health Perspectives – Vol. 114 No. 9, September, 2006
Gayle Windham, Div. of Environmental and Occupational Disease Control, California Department of Health Services
284 ASD children & 657 controls, born in 1994 in Bay Area, were assigned exposure levels by birth tract for 19 chemicals. Risks for autism were elevated by 50% in tracts with the highest chlorinated solvents and heavy metals. The highest risk compounds were mercury, cadmium, nickel, trichloroethylene, and vinyl chloride, and the risk from heavy metals was almost twice as high as solvents.
Excerpt: “Our results suggest a potential association between autism and estimated metal concentrations, and possibly solvents, in ambient air around the birth residence.”
22. A Case Series of Children with Apparent Mercury Toxic Encephalopathies Manifesting with Clinical Symptoms of Regressive Autistic Disorder
Journal of Toxicology and Environmental Health, 2007
David A. Geier, Mark R. Geier
This study reviewed the case histories and medical profiles of nine autistic children and concluded that eight of the nine children were mercury toxic and this toxicity manifested itself in a manner consistent with Autism Spectrum Disorders.
Excerpt: "...these previously normally developing children suffered mercury toxic encephalopathies that manifested with clinical symptoms consistent with regressive ASDs. Evidence for mercury intoxication should be considered in the differential diagnosis as contributing to some regressive ASDs."
Abstract
Impairments in social relatedness and communication, repetitive behaviors, and stereotypic abnormal movement patterns characterize autism spectrum disorders (ASDs). It is clear that while genetic factors are important to the pathogenesis of ASDs, mercury exposure can induce immune, sensory, neurological, motor, and behavioral dysfunctions similar to traits defining or associated with ASDs. The Institutional Review Board of the Institute for Chronic Illnesses (Office for Human Research Protections, U.S. Department of Health and Human Services, IRB number IRB00005375) approved the present study. A case series of nine patients who presented to the Genetic Centers of America for a genetic/developmental evaluation are discussed. Eight of nine patients (one patient was found to have an ASD due to Rett’s syndrome) (a) had regressive ASDs; (b) had elevated levels of androgens; (c) excreted significant amounts of mercury post chelation challenge; (d) had biochemical evidence of decreased function in their glutathione pathways; (e) had no known significant mercury exposure except from Thimerosal- containing vaccines/Rho(D)-immune globulin preparations; and (f) had alternate causes for their regressive ASDs ruled out. There was a significant dose-response relationship between the severity of the regressive ASDs observed and the total mercury dose children received from Thimerosal-containing vaccines/Rho (D)- immune globulin preparations. Based upon differential diagnoses, 8 of 9 patients examined were exposed to significant mercury from Thimerosal-containing biologic/vaccine preparations during their fetal/infant developmental periods, and subsequently, between 12 and 24 mo of age, these previously normally developing children suffered mercury toxic encephalopathies that manifested with clinical symptoms consistent with regressive ASDs. Evidence for mercury intoxication should be considered in the differential diagnosis as contributing to some regressive ASDs.
23. Attention-deficit hyperactivity disorder and blood mercury level: a case-control study in chinese children
Neuropediatrics, August 2006 - P.R. Kong [Department of Pediatrics and Adolescent Medicine, The University of Hong Kong].
This study demonstrates that blood mercury levels are higher for children with ADHD.
Excerpt: "There was significant difference in blood mercury levels between cases and controls, which persists after adjustment for age, gender and parental occupational status. The geometric mean blood mercury level was also significantly higher in children with inattentive and combined subtypes of ADHD. High blood mercury level was associated with ADHD. Whether the relationship is causal requires further studies."
24. The Changing Prevalence of Autism In California
Journal of Autism and Developmental Disorders, April 2003
Mark F. Blaxill, David S. Baskin, and Walter O. Spitzer
This study helps to refute the supposition made by some researchers that autism's epidemic may only be due to "diagnostic substitution".
Excerpt: "They have suggested that 'diagnostic substitution' accounts for an apparent increase in the incidence of autism in California that is not real. This hypothesized substitution is not supported by proper and detailed analyses of the California data."
25. Mitochondrial Energy-Deficient Endophenotype in Autism
American Journal of Biochemistry and Biotechnology 4 (2): 198-207, 2008
J. Jay Gargus and Faiqa Imtiaz Department of Physiology and Biophysics and Department of Pediatrics, Section of Human Genetics, School of Medicine, University of California, Irvine, Arabian Diagnostics Laboratory, King Faisal Specialist Hospital and Research Centre
Abstract
While evidence points to a multigenic etiology of most autism, the pathophysiology of the disorder has yet to be defined and the underlying genes and biochemical pathways they subserve remain unknown. Autism is considered to be influenced by a combination of various genetic, environmental and immunological factors; more recently, evidence has suggested that increased vulnerability to oxidative stress may be involved in the etiology of this multifactorial disorder. Furthermore, recent studies have pointed to a subset of autism associated with the biochemical endophenotype of mitochondrial energy deficiency, identified as a subtle impairment in fat and carbohydrate oxidation. This phenotype is similar, but more subtle than those seen in classic mitochondrial defects. In some cases the beginnings of the genetic underpinnings of these mitochondrial defects are emerging, such as mild mitochondrial dysfunction and secondary carnitine deficiency observed in the subset of autistic patients with an inverted duplication of chromosome 15q11-q13. In addition, rare cases of familial autism associated with sudden infant death syndrome (SIDS) or associated with abnormalities in cellular calcium homeostasis, such as malignant hyperthermia or cardiac arrhythmia, are beginning to emerge. Such special cases suggest that the pathophysiology of autism may comprise pathways that are directly or indirectly involved in mitochondrial energy production and to further probe this connection three new avenues seem worthy of exploration: 1) metabolomic clinical studies provoking controlled aerobic exercise stress to expand the biochemical phenotype, 2) high-throughput expression arrays to directly survey activity of the genes underlying these biochemical pathways and 3) model systems, either based upon neuronal stem cells or model genetic organisms, to discover novel genetic and environmental inputs into these pathways.
26. Bridging from Cells to Cognition in Autism Pathophysiology: Biological Pathways to Defective Brain Function and Plasticity
American Journal of Biochemistry and Biotechnology 4 (2): 167-176, 2008
Matthew P. Anderson, Brian S. Hooker and Martha R. Herbert Departments of Neurology and Pathology, Harvard Medical School/Beth Israel Deaconess Medical Center, Harvard Institutes of Medicine, High Throughput Biology Team, Fundamental Science Directorate, Pacific Northwest National Laboratory, Pediatric Neurology/Center for Morphometric Analysis, Massachusetts General Hospital/Harvard Medical School, and Center for Child and Adolescent Development, Cambridge Health Alliance/Harvard Medical School
Abstract: We review evidence to support a model where the disease process underlying autism may begin when an in utero or early postnatal environmental, infectious, seizure, or autoimmune insult triggers an immune response that increases reactive oxygen species (ROS) production in the brain that leads to DNA damage (nuclear and mitochondrial) and metabolic enzyme blockade and that these inflammatory and oxidative stressors persist beyond early development (with potential further exacerbations), producing ongoing functional consequences. In organs with a high metabolic demand such as the central nervous system, the continued use of mitochondria with damaged DNA and impaired metabolic enzyme function may generate additional ROS which will cause persistent activation of the innate immune system leading to more ROS production. Such a mechanism would self-sustain and possibly progressively worsen. The mitochondrial dysfunction and altered redox signal transduction pathways found in autism would conspire to activate both astroglia and microglia. These activated cells can then initiate a broad-spectrum proinflammatory gene response. Beyond the direct effects of ROS on neuronal function, receptors on neurons that bind the inflammatory mediators may serve to inhibit neuronal signaling to protect them from excitotoxic damage during various pathologic insults (e.g., infection). In autism, over-zealous neuroinflammatory responses could not only influence neural developmental processes, but may more significantly impair neural signaling involved in cognition in an ongoing fashion. This model makes specific predictions in patients and experimental animal models and suggests a number of targets sites of intervention. Our model of potentially reversible pathophysiological mechanisms in autism motivates our hope that effective therapies may soon appear on the horizon.
27. Heavy-Metal Toxicity—With Emphasis on Mercury
John Neustadt, ND, and Steve Pieczenik, MD, PhD
Research Review
Conclusion: Metals are ubiquitous in our environment, and exposure to them is inevitable. However, not all people accumulate toxic levels of metals or exhibit symptoms of metal toxicity, suggesting that genetics play a role in their potential to damage health. Metal toxicity creates multisystem dysfunction, which appears to be mediated primarily through mitochondrial damage from glutathione depletion. Accurate screening can increase the likelihood that patients with potential metal toxicity are identified. The most accurate screening method for assessing chronic-metals exposure and metals load in the body is a provoked urine test.
28. Evidence of Mitochondrial Dysfunction in Autism and Implications for Treatment
American Journal of Biochemistry and Biotechnology 4 (2): 208-217, 2008
Daniel A. Rossignol, J. Jeffrey Bradstreet, International Child Development Resource Center,
Abstract: Classical mitochondrial diseases occur in a subset of individuals with autism and are usually caused by genetic anomalies or mitochondrial respiratory pathway deficits. However, in many cases of autism, there is evidence of mitochondrial dysfunction (MtD) without the classic features associated with mitochondrial disease. MtD appears to be more common in autism and presents with less severe signs and symptoms. It is not associated with discernable mitochondrial pathology in muscle biopsy specimens despite objective evidence of lowered mitochondrial functioning. Exposure to environmental toxins is the likely etiology for MtD in autism. This dysfunction then contributes to a number of diagnostic symptoms and comorbidities observed in autism including: cognitive impairment, language deficits, abnormal energy metabolism, chronic gastrointestinal problems, abnormalities in fatty acid oxidation, and increased oxidative stress. MtD and oxidative stress may also explain the high male to female ratio found in autism due to increased male vulnerability to these dysfunctions. Biomarkers for mitochondrial dysfunction have been identified, but seem widely under-utilized despite available therapeutic interventions. Nutritional supplementation to decrease oxidative stress along with factors to improve reduced glutathione, as well as hyperbaric oxygen therapy (HBOT) represent supported and rationale approaches. The underlying pathophysiology and autistic symptoms of affected individuals would be expected to either improve or cease worsening once effective treatment for MtD is implemented.
29. Proximity to point sources of environmental mercury release as a predictor of autism prevalence
Health & Place, 2008
Raymond F. Palmer, Stephen Blanchard, Robert Wood University of Texas Health Science Center, San Antonio Department of Family and Community Medicine, Our Lady of the Lake University, San Antonio Texas, Chair, Department of Sociology
This study should be viewed as hypothesis-generating - a first step in examining the potential role of environmental mercury and childhood developmental disorders. Nothing is known about specific exposure routes, dosage, timing, and individual susceptibility. We suspect that persistent low-dose exposures to various environmental toxicants, including mercury, that occur during critical windows of neural development among genetically susceptible children (with a diminished capacity for metabolizing accumulated toxicants) may increase the risk for developmental disorders such as autism. Successfully identifying the specific combination of environmental exposures and genetic susceptibilities can inform the development of targeted prevention intervention strategies.
30. Epidemiology of autism spectrum disorder in Portugal: prevalence, clinical characterization, and medical conditions
Developmental Medicine & Child Neurology, 2007
Guiomar Oliveira MD PhD, Centro de Desenvolvimento da Criança, Hospital Pediátrico de Coimbra; Assunção Ataíde BSc, Direcção Regional de Educação do Centro Coimbra; Carla Marques MSc, Centro de Desenvolvimento da Criança, Hospital Pediátrico de Coimbra; Teresa S Miguel BSc, Direcção Regional de Educação do Centro, Coimbra; Ana Margarida Coutinho BSc, Instituto Gulbenkian de Ciência, Oeiras; Luísa Mota-Vieira PhD, Unidade de Genética e Patologia moleculares, Hospital do Divino Espírito Santo, Ponta Delgada, Açores; Esmeralda Gonçalves PhD; Nazaré Mendes Lopes PhD, Faculdade de Ciências e Tecnologia, Universidade de Coimbra; Vitor Rodrigues MD PhD; Henrique Carmona da Mota MD PhD, Faculdade de Medicina, Universidade de Coimbra, Coimbra; Astrid Moura Vicente PhD, Instituto Gulbenkian de Ciência, Oeiras, Portugal. *Correspondence to first author at Hospital Pediátrico de Coimbra, Av Bissaya Barreto, 3000-076 Coimbra, Portugal. E-mail: [email protected]
Abstract: The objective of this study was to estimate the prevalence of autistic spectrum disorder (ASD) and identify its clinical characterization, and medical conditions in a paediatric population in Portugal. A school survey was conducted in elementary schools, targeting 332 808 school-aged children in the mainland and 10 910 in the Azores islands. Referred children were directly assessed using the Diagnostic and Statistical Manual of Mental Disorders (4th edn), the Autism Diagnostic Interview–Revised, and the Childhood Autism Rating Scale. Clinical history and a laboratory investigation was performed. In parallel, a systematic multi-source search of children known to have autism was carried out in a restricted region. The global prevalence of ASD per 10 000 was 9.2 in mainland, and 15.6 in the Azores, with intriguing regional differences. A diversity of associated medical conditions was documented in 20%, with an unexpectedly high rate of mitochondrial respiratory chain disorders.
1 note
·
View note
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://traffic.libsyn.com/thehealthyskeptic/RHR_-_A_Three-Step_Plan_to_Fix_Conventional_Healthcare.mp3" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don’t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody.
0 notes
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://traffic.libsyn.com/thehealthyskeptic/RHR_-_A_Three-Step_Plan_to_Fix_Conventional_Healthcare.mp3" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don���t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody. RHR: A Three-Step Plan to Fix Conventional Healthcare published first on https://chriskresser.com
0 notes