#which adhd symptom does this fall under
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
China blocked Tumblr because of pornography and censorship problems in 2013.
Text
huge fan of that bit my brain does where as soon as i start working i have the skin tearing urge to make some kind of art and then i get home and it's fucking honk shoo time baby
#my bed when i get home like eyes emoji#👀#like that#which adhd symptom does this fall under#same shit happens when i work remote like the soul sucking is just part of the contract#rambling
16 notes
·
View notes
Text
Zack's ADHD
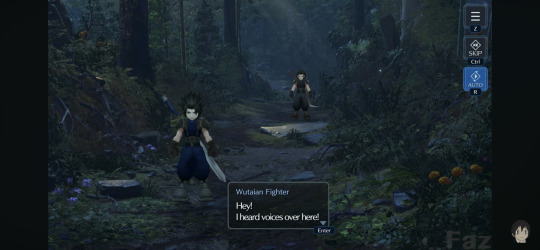
Zack fair has ADHD. That's something I see tons of people acknowledge that I myself agree with, but a lot of it feels very shallow/surface level? I mostly see people talk about his diffculty paying attention, but never really explore a lot of the other symptoms of ADHD that he very clearly has. In general, ADHD has symptoms that can be put in two categories. These being inattentiveness and Hyperactivity/Impulsive behavior. I'm going to try to go into each symptom I've seen him display. Going through things that fall under inattentiveness since that's what most people focus on first and foremost! Obviously, Zack has a short attention span. The opening of Crisis core has Angeal setting him back on track multiple times, and has to remind him of his mission. That bleeds into another symptom of ADHD, which is having a hard time listening to or following instructions.
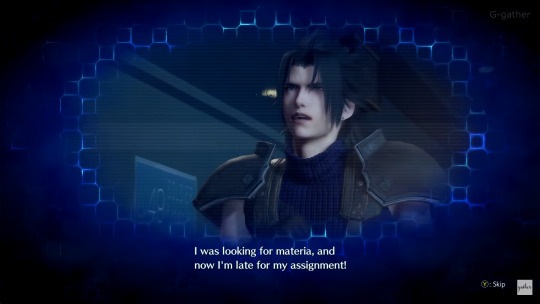
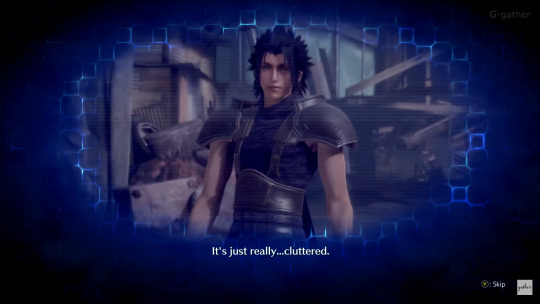
Another few symptoms of ADHD under inattentiveness is being disorganized, forgetful, and making careless mistakes. Zack has shown to fit under all of these things in DMW scenes. One in particular features him both losing materia AND forgetting his sword.

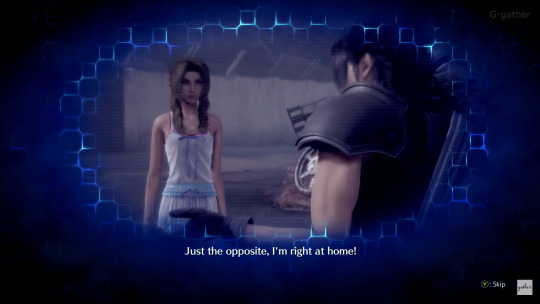
Again, we see that he's a messy person when he's talking to Aerith in another DMW scene.

Now I'm going to go into the symptoms that fall under Hyperactivity. Some of the most talked about symptoms he exhibits are a lack of ability to stay still, excessive physical movement, and excessive talking. Noteably too, people with ADHD can have difficulty controlling the volume of their voice, or how fast they speak. For example here, Zack is told right before to calm down by Angeal, and immediately proceeds to talk loudly (giving away their position.)
Circling back to the previously mentioned symptoms, trouble staying still and excessive movement are some of the few things I feel people notice first in correlation to ADHD, but never really think about what it really is in the context of ADHD. Zack tends to do squats when he's excited. It's a repeated motion he does to calm himself down and/or focus. Sound familiar? that's because it's stimming. Interupting conversations lines up with ADHD, and is something Zack does in-game too!
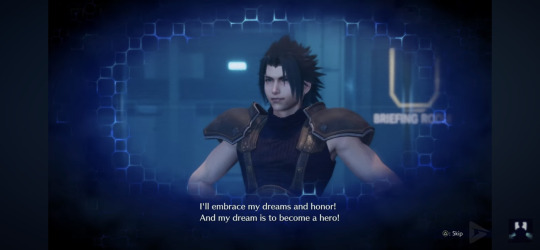
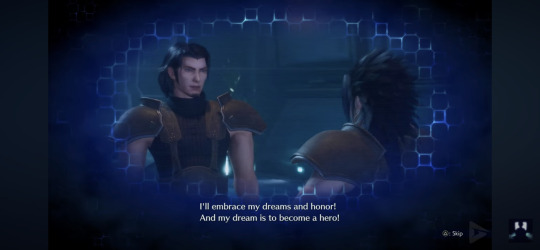
Here he interupts Angeal's speech (and gets a fond smile in turn. I will bring this up later for something else). Zack is impulsive by nature, and tends to rush into things without a clear plan. He has a very absent sense of danger sometimes as well. All of which fall under the Hyperactivity category of ADHD symptoms.
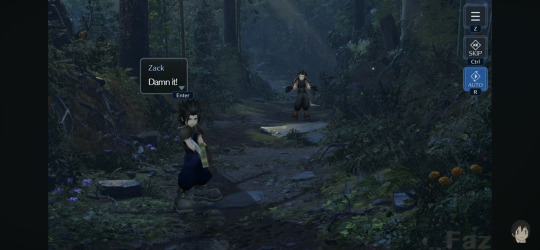
The symptoms I see in Zack that hardly a soul has acknowledged though, is him being easily frustrated or irritated. ADHD makes it hard to regulate emotions, and Zack showcases this a lot throughout Crisis Core. For Zack, this sometimes seems to fall under under Rejection Sensitive Dysphoria, which is common in people with ADHD. It's a discomfort and difficulty regulating feelings of failure or rejection. For Zack, this also takes the form of confusion/frustration/annoyance. However, in most instances of him taking criticism, he mostly manages to move past his and take the criticism/corrections to improve himself. Funnily enough, you can see his quick frustration/irritatrion in the very first cutscene when Angeal jumps down to elaborate on the parts of the mission he missed because Zack jumped a bit too soon due to his eagerness (more impulsivity). Zack gets angry due to this interuption to the task he was focused on, and becomes cheerful as soon as he is able to get back to his task. The frustration with interuption and being quickly upset is interesting. There are more instances of this kind of behavior, and it all really feels like it falls under this umbrella of him struggling to regulate his emotions. This also goes hand in hand with his stimming, since it isn't just the frustration/anger he has difficulty managing. His excitement and stress is something we also see him have difficulty managing, and can be tied into a lot of the other aspects of ADHD I have discussed here! Zack gets frustrated again later when Angeal ends the training simulator, and puts an end to the task he had been hyperfocused on.
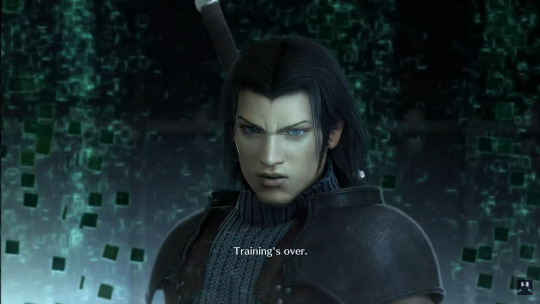
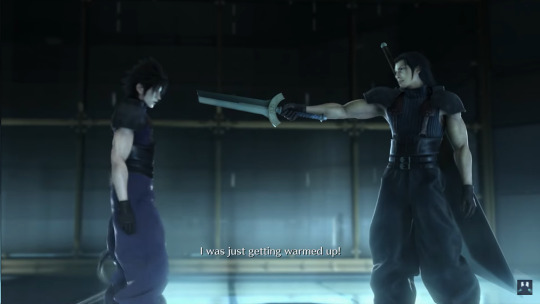
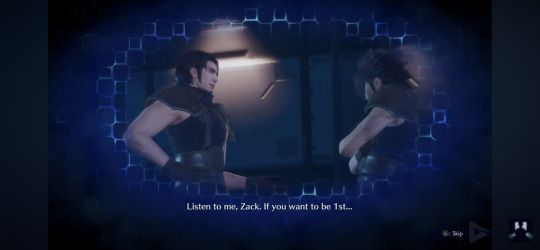
It's an irrational anger, but it makes more sense when read through this lense. Zack was excited and hyperfocusing on his mission. He charged ahead without hearing or understanding the full objective, and almost got hurt (in the context of the training sim). The sim was ended before Zack felt it was "finished", which resulted in a frustration he expressed outwardly. His hasty behavior and exciteability is a core character trait, but makes far more sense if you read him as a character who lives with ADHD. How he is written and how other characters interact with him is interesting to watch as well! One thing in particular I love a lot is Angeal's treatment of Zack's ADHD tendencies. For being in the military, which is a very unforgiving enviornment, Angeal shows quite a lot of compassion for Zack's ADHD tendencies. Things that would normally get him into trouble are instead corrected rather gently! Angeal consistently repeats instructions to Zack when he needs it, and keeps a firm hand when he guides Zack through missions. He never tells Zack to sit still. He never berrates him for his interjections (Zack going "And? And and and?"). The only time he really scolds Zack is when he's doing something that may endanger them.
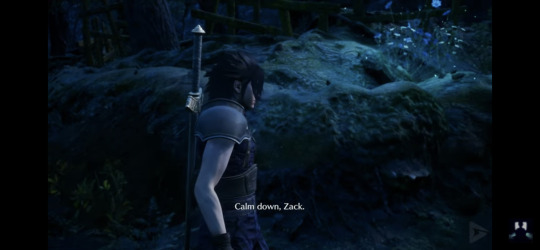
For example, here they're on a mission that requires stealth. Zack being loud isn't normally a problem, but here, they need to be relatively quiet in order to achieve their goal. Angeal is compassionate and understanding when Zack is... doing things that are very ADHD coded. As mentioned earlier, Angeal doesn't get upset when Zack interupts him. Instead, he just smiles. It's likely Angeal was the one who taught Zack to do squats to stim, actually. In the Ever Crisis version of Crisis Core, Angeal says this to Zack. Although it's not necessarily canon, it's still entirely plausible and just. Very wholesome.

More of Angeal's tolerance for Zack can be seen here, when Zack's attitude slips after being criticized, and Angeal pays it no mind. (Again, his rejection sensitive dysphoria plays a part in having him react rudely)



Again, you need to keep in mind that despite their closeness, Angeal is still both his mentor and superior. He doesn't have to be as patient with Zack as he is in-game, but he does so anyway because... that's just how he is. Angeal cares a LOT about his loved ones, and Zack is included in this. He shows a lot of love to this little guy! I think it's nice, because I love seeing characters with ADHD being treated with consideration by others. It's something I wish people did more IRL, really. Lots of ableism surrounding aspects of ADHD that aren't as easy to romanticize and considered "annoying", so having Angeal respond to them with understanding makes me incredibly happy. Altogether I just absolutely love Zack as a character. I love reading him with ADHD since I have it myself. I just want people to see the depth to it more though, since there's more to it than just "he's high energy and gets distracted". You get to understand his actions or irrational behavior a lot more when you dive past the surface of his writing. Big, massive, enormous fucking thanks to my bestie @rune-rapier for letting me bounce ideas to and from him!! He helped me get a lot of these scenes in here to analyze, and brought up a LOT of points that made it in this post, and made it a lot easier for me to word.
#this took forever#i started working on this... what? 3 hours now?#have to say. truly outdid myself this time LMAO#big fan of how it became an angeal appreciation post. semi accidental. FDSLKGELKFGJE#i just want people to understand that he isnt. being ableist or anything.#he's doing his job.#tag time!!!!#final fantasy 7#crisis core#ff7 crisis core#angeal hewley#zack fair#ff7 angeal#ff7#final fantasy vii#ffvii angeal#zack ff7#ff7 zack#zack fair has adhd#adhd#rejection sensitive dysphoria
290 notes
·
View notes
Text
(Tw for talk of r/fakedisordercringe, ableism, fake claiming, harassment, etc.)
I have had it with r/fakedisordercringe. This subreddit is filled with content that is both ableist and harmful to the neurodivergent community. The posts mock autistic people, systems, people with ADHD, etc. suggesting that people are faking or exaggerating their symptoms for attention. First of all, it's incredibly harmful to assume that someone is faking a disorder just because they don't fit into your narrow view of what that disorder looks like. Autism, for example, is a spectrum disorder, which means that there are a wide variety of ways that it can present itself. Just because someone doesn't exhibit all of the classic symptoms that you associate with autism doesn't mean that they're faking it. (Tell me you're an aspie supremacist without telling me you're an aspie supremacist /hj)
The reasoning that the users of this subreddit often use tend to fall under these categories:
"They don't experience *insert disability* the same way that I do, so they must be faking"
"They post too frequently about their disability, so they must be faking"
"They support self diagnosis, so they must be faking"
"They use xenogenders/neopronouns, so they must be faking"
etc.
Has it ever crossed your mind that maybe not everyone is the same? That not everybody's disability is the same? /nbh
The idea that someone can determine whether or not another person is truly autistic or has a mental disorder based on a few online interactions (or even just a post!) is absurd. Not every autistic person or people with other disorders fits the stereotype of what people expect, and it's not up to strangers on the internet to decide who is "legitimate" and who is not.
As an autistic person, I'm tired of constantly having to defend myself and my experiences. I'm tired of seeing people with disabilities being reduced to nothing more than punchlines for jokes.
A few days ago someone in a youtube comment section accused me of faking being autistic, by saying something along the lines of "Self diagnosed ahh". First off, not everybody can safely access diagnosis. You are so incredibly privileged if you think everyone can. Somebody being undiagnosed does NOT immediately mean they are faking. Second off, I am literally professionally diagnosed.
I am tired of r/fakedisordercringe and the hate, misinformation, and stigma it perpetuates.
Leave disabled people ALONE.
#tw fakedisordercringe#tw ableism#tw fakeclaiming#actually autistic#pro self dx#rant#neurodivergent#nonspeaking autistic#autism#aac user#nonspeaking#disabled#disability
810 notes
·
View notes
Text
3. Difficulty Waking Up with ADHD
More than 80 percent of adults with ADHD in my practice report multiple awakenings until about 4 a.m. Then they fall into “the sleep of the dead,” from which they have extreme difficulty rousing themselves.
They sleep through two or three alarms, as well as the attempts of family members to get them out of bed. ADHD sleepers are commonly irritable, even combative, when roused before they are ready. Many of them say they are not fully alert until noon.
4. Intrusive Sleep with ADHD
Paul Wender, M.D., a 30-year veteran ADHD researcher, relates ADHD to interest-based performance. As long as persons with ADHD were interested in or challenged by what they were doing, they did not demonstrate symptoms of the disorder. (This phenomenon is called hyperfocus by some, and is often considered to be an ADHD pattern.) If, on the other hand, an individual with ADHD loses interest in an activity, his nervous system disengages, in search of something more interesting. Sometimes this disengagement is so abrupt as to induce sudden extreme drowsiness, even to the point of falling asleep.
Marian Sigurdson, Ph.D., an expert on electroencephalography (EEG) findings in ADHD, reports that brain wave tracings at this time show a sudden intrusion of theta waves into the alpha and beta rhythms of alertness. We all have seen “theta wave intrusion,” in the student in the back of the classroom who suddenly crashes to the floor, having “fallen asleep.” This was probably someone with ADHD who was losing consciousness due to boredom rather than falling asleep. This syndrome is life-threatening if it occurs while driving, and it is often induced by long-distance driving on straight, monotonous roads. Often this condition is misdiagnosed as “EEG negative narcolepsy.” The extent of incidence of intrusive “sleep” is not known, because it occurs only under certain conditions that are hard to reproduce in a laboratory.
-
231 notes
·
View notes
Text
Some Musings on Plurality and Mental Health (had a conversation about this earlier today, but we've also been thinking about it generally for a while, so hey, why not, post time) Something that frequently tends to get lost in the noise of discourse but is, imo, actually pretty relevant to system community spaces of all kinds, is the realization that many (I'd venture to say most) systems of any kind, origin, dx, whatever, often have concurrent struggles with mental health issues of one kind or another. Not every system or every person who experiences multiplicity in a significant way has a Textbook Case dissociative disorder (or even a diagnosable dissociative disorder at all, depending on your framework for thinking about what does and does not fall under the scope of the label). But also, that doesn't necessarily mean they aren't dealing with significant mental health challenges: - A lot of systems are queer in one way or another, and many have had to deal with the dangers and insecurity and heartbreak of being queer in our current society. - A lot of systems are autistic/dyslexic/have ADHD/have other kinds of processing differences that have affected many years of their lives, especially if they went through any kind of education system that tried to force their brains into something different, told them they were broken, and facilitated social isolation in one way or another. - A lot of systems, even those without dissociative disorders, have other mental health diagnoses. Depression, anxiety, personality disorders, schizophrenia and related disorders, etc. - A lot of people overall have undergone traumatic experiences in their lives at some point (or multiple points), which we all know have significant aftereffects on mental and emotional health. Also, there's multiple global crises that have been going on for a while, of which the COVID pandemic is just one example, which means a lot of new and exacerbated mental (and physical!) health issues for a lot of people in the last few years. So, what's the relevance of all this?
To us, it's yet another reminder that the idea of an easy division between "disordered system" and "non-disordered system" is frankly illusory. For anyone whose experiences of multiplicity/systemhood/plurality/etc are a significant part of their lives and functioning, that relevance will extend to their struggles with mental health, regardless of whether the mental health issues they're having fall under DID/OSDD or not. Control over switching, new or worsened in-system conflicts, system members being differently impacted by traumatic experiences, degree of dissociative disconnect vs ease of internal communication and memory sharing, system members experiencing and presenting symptoms of mental health issue differently, dysphoria over external-body-vs-internal-self mismatches, increased dissociation overall as a collective coping mechanism.... all of this is stuff that lies at the intersection of any mental health issues and systemhood, potentially, not just "DID/OSDD + its associated classical presentations and etiology". If a parogenic system fell into heavy depression over the quarantine, they might start experiencing more negative dissociative symptoms, and they'd also have to figure out how to navigate the mental health support system (such as it is) while plural. If someone with PTSD from trauma in adulthood decides to look into daemonism for comfort, and finds themselves more and more feeling like a system, they may or may not qualify for DID but they will still be contending with healing-from-trauma-while-a-system. If a system without memory barriers or other apparent issues gets long COVID and has their whole lives upended from new disability, their presentation may start looking more like a dissociative disorder. None of these examples are necessarily exactly the same as having DID or OSDD (...depending on how you define the scope of those diagnostic labels, which is a complicated question all of its own), but they're within a spectrum of related experiences that involve both mental health disorder and plurality in an intertwined way. Which, I guess, is a long way of saying: There is no specific diagnostic category or label that someone has to fit in order to be suffering and need support--and that includes systems as well as singlets.
#system stuff#tw mild syscourse#long post#kinda rambling but thought there were some interesting ideas in there worth putting out there just in case
86 notes
·
View notes
Text
A small ramble about Eclipse's therapy
Okay, so this is all copy-pasted from Discord where I was going through it minute by agonizing minute and just rambling my little heart out

This episode. Specifically this one. Ramble under cut.
Reminders before I talk about this! Eclipse is confirmed to have ASPD in canon. I also have ASPD. I do know things on that topic because of this unfortunate fact. For some in-depth things on Eclipse's sociopathy, I suggest popping over to these two analyses! Eclipse Is a Sociopath - Traits of ASPD
Eclipse obviously doesn't even want to be here, we know this from the very start when Moon is literally shoving him to get him into the room
Eclipse attempts (and fails) to intimidate both Moon and Solar. First with the comment about Lunar, which was meant to get under Moon's skin but when he didn't get a reaction he brushed it off with a 'whatever'. Next with the stand-off with Solar "Name is Solar" Technically correct, as we know from earlier episodes that his name is "Solar Eclipse" and Lunar is "Lunar Eclipse" The 'eclipse brothers' (Which is only further supported by the fact that a blood moon is a type of eclipse) Of course, we all know this was not the answer Solar was wanting. (Solar gets his own petty revenge by dragging the process out. Moon also gets petty revenge by mocking Eclipse. This is honestly a good reminder that they all came from the same base personality.)
Eclipse was flabbergasted. Absolutely gobsmacked. Shook When Moon told him upfront that he does need therapy. I think this stems partly from the fact that this is Moon and Moon has never tried to do something that would benefit Eclipse And then just being told what he already knows by someone else probably caught him off guard. He doesn't want to go to therapy because he thinks that therapy means he is weak. We already know how Eclipse feels about being weak and needing to rely on others for literally anything. We see this on a lesser extent with Solar who doesn't ask for anything because he doesn't want to be seen as a burden.
I do think it's important that he calls Solar the 'inferior version' right after calling him the 'better version' of himself. He called Solar better than him and then immediately change his words. Possibly because he can't stand the fact that Solar actually is better than him. Not necessarily in what one thinks of when we do comparisons like that, but more of Solar's more stable than Eclipse. He has a family to lean back on. . . unlike Eclipse. The one person that Eclipse cared about (at one point but now claims to hate) now hates Eclipse but loves Solar, which is just. . . another version of Eclipse. And that knowledge has to be painful, even for Eclipse.
It's also possible that Eclipse actually does think that Solar is inferior due to the common mindset that socio/psychopaths tend to have about 'normal people' around them. We pity people on a superficial level for being held back by fickle things like emotions and guilt, while also blatantly ignoring our own issues that make our own lives 582390458234098x harder due to the packaged deal that is ASPD
(To briefly summarize the "package deal" - along with socio/psychopathy toss in Anxiety Disorders, Paranoia, Dissociation/Derealization Issues, PTSD, ADHD/ADHD-symptoms, and Depression)
Back to the analysis
Eclipse immediately starts to mock Earth's office. He tends to mock Earth a lot in the past, because she's a very reactive character. It also used to be a lot easier to make her insecure. Someone who is insecure isn't going to press a hostile party for conversation/information.
Earth, like the girl-boss she is, calls him out. Kudos to Earth
Okay let's step back from Eclipse a second because MOON This is probably the worst possible timing for him to bring Eclipse in for a therapy appointment and he knows it and even though Earth says it's fine he's still apologizing and genuinely sorry and I think that's a huge step from how he was falling apart a little bit ago and slipping back into what Old Moon was Moon's also always had a soft spot for Earth (Big brother syndrome except Moon is technically the youngest sibling)
Okay back to Eclipse. After a failed attempt to get under Earth's skin he goes for Moon again. The man really do be flabbergasted that the two most reactive people he knows aren't giving him the reaction he wants.
And then back to Earth. He honestly spends the first bit just trying to get a reaction out of everyone because that's what he's good at. He's exasperated when Earth starts asking him questions, and gives her his normal sarcastic a-hole response. He's purposefully unnerving and trying to make both Earth and Moon uncomfortable because he doesn't want to be there.
He skirts around the abandonment question, which just lets everyone in the room know that he does indeed feel abandoned. He deflects the question honestly horribly in my opinion. "Abandoned, why would I feel abandoned?" Proceeds to list off reasons that he would feel abandoned but phrases them as questions. Sir? Try harder.
Moon plays a common tactic when dealing with unwilling peoples. "The sooner you play along the sooner you can leave." Common courtroom/interrogation tactic. Gives a goal to work toward while also implying that they're willing to stick around for as long as the person in the room is willing to bullcrap them. This may be a familiar tactic to the audience because parents love using this when teens are lying to them. So do teachers. "Just tell us what we want to hear and then we can be done. But if you sit here in silence then I'll sit here in silence with you."
Reminds me of parole. A lot of people who've gotten in trouble with the powers that be are required to participate in active therapy if they want to get out of a heavier charge. It's a common requirement of plea deals
Watch me ramble Back on track
Plsplspls and then Eclipse says the same thing I FORGOT HE SAID IT CUT ME SOME SLACK IM TYPING AS I WATCH THIS FOR THE SECOND TIME ITS BEEN A WHOLE DAY I've got the adhd my memory is not that good sir
I'm only 6 minutes in are you bored yet
Earth does irritate him by making assumptions about him that are wrong. It's a small blow to the pride. He's not acting like he doesn't care, he just doesn't care. And then he just starts bullcrapping so I'm gonna call him out on his bullcrap
He didn't just care about the star
Someone who doesn't care isn't going to be hurt by rejection so lets go over the list
Getting back to Moon. Remerging their code which is where he felt like he was supposed to be. Moon shoved him away, rejected him, and that made him upset
Lunar. Lunar wasn't just a means to an end because Lunar had just the right traits, the right level of whatever to make Eclipse care about him. Think of it like this. Eclipse was barely offended by Bloodmoon attacking him and ditching him. But he went out of his way to blow Lunar up because Lunar, in his eyes, betrayed him
The star to an extent. He cared less about the star itself and more about being able to make a world perfect for him and those around him. He was a Lawful Evil type back then (Dances in DnD language)
Eh that's honestly all I can think of off the top of my head. I'd argue he also cared about Sun to an extent because he used to be Moon, but probably not as much these days lol But yeah CUT THE CRAP ECLIPSE GRRR WHOO LOW SELF ESTEEM "You'd all just immediately try to find a way to kill me" He really do think that everyone would just go out of their way to kill him even if he was existing peacefully. He's half right
Sun didn't really want anything to do with it. Solar was just going along with it because Moon's his best friend (and Solar himself is insecure whoo). Earth isn't confrontational. Ruin (who probably brought eclipse back, btw where did he disappear to we haven't seen that cockroach for a while) didn't hop on the kill Eclipse train until after he was 'kidnapped', and we all know how sus that was. Lunar, yeah, but that's Lunar. Moon also was immediately like "omg kill this guy" but also, that's just Moon. Like I have talked about how self-centered those two are before, haven't I? Monty also wanted to kill Eclipse on sight but he's literally worse than Moon so he don't really count. Monty is literally an awful person who is only semi-decent because of Earth
Eclipse describes his death to Earth as if she wasn't literally there. Again. Reactions. As well as the weird complinsult which she has no idea how to process. Is it an insult? Is it a compliment? It's both honey. It's both. Take it or leave it. Once again frustration and insecurity at the lack of control Eclipse has ove everything. From being monitored, to being brought back, to literally being in a brand new body that he had no say in. The physical lack of control bleeds into the mentality that he has no control over anything, including his own thoughts and emotions. And what's sad is it's kind of true. . . he can't even control his own actions some of the time because of the directives. That just makes him feel paranoid and hopeless, and while he doesn't say it explicitly, it shows. He doesn't think he can change in his mentality because he can't change anything else around him either. That's part of why he thinks therapy is pointless.
10:30 This is where I argue he takes off his metaphorical mask. Not because he trusts Earth, but he's trying to see where her breaking point is. She's been patient and kind and making an attempt to be understanding and it's curious because no one has ever just sat there and asked him questions and let him ramble. He's trying to make her uncomfortable still, but he's also curious. This is a button that has never been presented to him before, how many times can he press it before it's taken away from him. At first he's thinking about his answers, calculating his responses, but it feels honest.
12:20 And then he realized that he was getting ahead of himself and that he was just rambling because he's never had someone to talk to and he stops. Whether it's because it's something he doesn't want her to know, or Moon to know, or it's just something he isn't ready to say out loud yet, he changes topics.
And then he's back to deflecting and getting the focus off of him and poking at Earth again
(Side note: Earth calls him an idiot in a roundabout way and it made me giggle both times watching it)
"You would take more pride in-" Pauses video Gestures frantically PRIDE UGH THE FALLING POINT OF A SOCIOPATH IS OUR PRIDE Yes he would take more pride in it being about information gathering. He'd probably be more complicit if it were for that purpose instead of 'inner healing' because going to therapy is a BLOW TO HIS PRIDE IM Ignore me as I go insane Presses play
Eclipse breaking the fourth wall like-
He's very cynical about the idea of trust and it's because the few times he put his trust in someone/thing it's failed him. AND THEN MORE DEFLECTION ECLIPSE PLEASE- Just stay on topic I'm begging you I know it's hard but LET ME HARVEST YOUR BRAIN MAN STOP DEFLECTING
He's so gobsmacked when Earth claims that we aren't defined by who makes us. Which must be hard to hear for Eclipse because for a while there his entire identity was defined by the fact that he was made by Moon and left behind.
He presses Earth for further detail about this and it makes me wonder if this was the first time he's ever heard or conceptualized this
It's fun to hear Eclipse (I think for the first time) finally verbally disown Sun and Moon. "I don't care to make it right anymore. They've cast their stone and now I'm stuck in my own ship." AKA They had their chance to give him a chance time and time again and each time they shunned him. Why would you go back to someone who has only caused you pain? Eclipse is in a similar situation with Sun/Moon that Lunar is in with him. Part of him wants to be back with them because he was made from them, they will always be part of him just how Eclipse will always be part of Lunar. Violence begets more violence.
I do think it's interesting how Eclipse doesn't acknowledge that he blew up Lunar and it's probably because he didn't blow up Lunar. The Eclipse before him did. Just like how Moon didn't reject him, the Moon before did. (I'll come back to that later)
Earth has to point out that Lunar got ka-boomed and then Eclipse laughs "Oh yes, I did, right." Because, again, he didn't. The Eclipse before him did. It feels like he's trying to avoid taking accountability for that (and good on him because he's technically innocent it's not his fault he has the corrupted memories of a dead man)
HOWEVER ON THAT NOTE
It does feel like with every day that passes by those memories become more of who he is now, and he's slowly accepting them as part of his own identity because he's kind of stuck with them. If you woke up in a random place and someone handed you a broom and said 'you're bob the janitor' and that's all you knew you'd probably believe it (/ref)
(If someone gets that reference I will love you forever)
"Do you really. . . not care about him?" - Earth Eclipse: Doesn't answer the question, answers a question with a question which is DEFLECTING
Sir? You do too still care don't you?
"It's kind of hard to empathize with you" - Earth Me: Runs up chat to grab something
"a normal person cannot relate to a sociopath because our life experiences are so vastly different. You (general you) will never be able to understand what it’s like to be physically unable to care about someone to the point that it hurts because you want to care. And a socio/psychopath will never be able to understand on a visceral level what it’s like to be able to connect with another person or be able to feel things all the time or to do the right thing simply because something compels you to and not because you had to ask yourself “is this morally good or bad behavior” because you just know" - Me four days ago
Do find it interesting how Eclipse has no comment when Earth says he doesn't like her He probably likes her just fine, if I'm being honest. Probably likes her more than most other characters. He's just kinda a jerk and likes to press her buttons because it's funny
When she does manage to hit something right on the nail "It must be scary, right?" And "You just never have a sense of control" He makes a kinda-joke "Are we just going to keep talking about how sad we are" to change the topic AND SHE LAUGHED SHE LAUGHED AT HIS JOKE 👑 Ma'am you dropped this
I do personally Eclipse's sense of humor because it's pretty on point with my own, but I also really enjoy people being uncomfortable with it as well because that's half the fun. So I'm getting a small amount of dark enjoyment of Earth being uncomfortable at the boom joke

((Earth did awesome considering the circumstances. I can respect the fact that she is communicating her own emotional and mental needs even while dealing with someone who's not exactly pleasant for the general populace. She's gotten a lot better at setting boundaries))
Eclipse walks out because he's irritated with Moon. It's a power play. "I may have been forced to be here, but you can't make me sit and listen to you." He honestly had no idea what Moon would have said at the moment, and I also don't think that it would have been the best timing for Moon to drop that on him. They need a calm environment where neither of them is worked up to start touching that topic. Also MOON He's apologizing for something that isn't even his fault and while I can respect that, I almost wish he wasn't taking the blame for something a past self did. Just like how Eclipse is trying not to take accountability for what dead-man Eclipse did. They're two people who have been hurt by the actions of their predecessors and are playing out a game that was set into motion long long before their time. Now the only question that remains is who is Romeo and who is Juliet
Anyway that was the episode
Am taking inquiries and demands as well as bounties for my head
#sun and moon show#earth and lunar show#tsams moon#tsams fnaf#eclipse tsams#tsams earth#tsams solar#tsams#eclipse analysis#tsams analysis#alex talks#video analysis
22 notes
·
View notes
Text
Several months ago I saw some truly reductive and ignorant comments about rejection sensitive dysphoria on here and they've stayed bothering me.
RSD is NOT a medical condition; it is a set of symptoms that can be present in ADHD and AuDHD folks, but does not constitute its own diagnosis. After a lifetime of having to interpret neurotypical communication and actions that don't inherently make sense to us to determine if we are safe and correct in what we're doing, some of us have developed a set of trauma responses about being rejected, or worrying that we are/will be.
I saw someone call RSD a tiktok trend which they reduced to, "People with ADHD experience rejection sometimes," and I wanted to reach through their screen and throttle them. An RSD episode is not a typical reaction to rejection; unless a sudden and almost total loss of sense of self and self esteem is "normal". I don't think the feeling of dread and impending doom and failure is "normal". The instant loss of so many of my coping skills and the feeling like the world is going to end or fall apart of I don't "fix" the situation (get un-rejected) definitely isn't "normal".
I'm pretty sure I started forming this symptom set when I was a toddler; one of my "canon events" involves an incident with some church women when I was in Sunday school at about age 3 or 4 and I can see the same panic and desperation in my response then that I see when I'm having a bad RSD episode now. That feeling of powerlessness and panic driving you to do anything and everything just to end the situation is still so tangible to me, 32 years later.
And there's no one out there with coping techniques for me to learn. No real advice or treatment. I just have to go on doing my best until the next episode knocks my feet out from under me. Then I do my best to keep from hurting the people I care about while the absolutely unhinged parts of me try to figure out how to "fix" the situation.
This symptom set and the difficulty in regulating it has become the greatest force of destruction in my own life that doesn't come from outside threats. The list of friendships I, during an episode, or just the reaction itself has ended grows longer every year. All of my lowest depressive points and all of my most manic phases have come from this.
Even now, part of my mind is trying to renegotiate the end of my last relationship to an audience of no one and it's only just starting to feel less intense and imperative that I do so.
This is not the normal response to real and perceived rejection. And it's way too real to be dismissed as some social media pop psych topic of the month or whatever when it's basically Godzilla to my brain's downtown Tokyo. Fuck the neurotypicals and self hating NDs who say otherwise.
12 notes
·
View notes
Text
Deltarune; Neurodivergent HC

requested by @pulsar-ray (sorry its late /g)
characters: spampton, swatch and tasque manager

Spampton
Dysgraphia and Dyslexia majorly struggles with writing numbers and letters often written backwards never consistent with sizing and lines always curve random or misplaced capitalization uses the trick of writing a line under 6 or 9 to indicate which is which but still mixes it up at times only left and right trick that words is the "lefty loosey, righty tighty" rhyme, the L hand trick doesnt work for him will mix up words that are very similar uses numbers for letters both cuz cool typing quirk and mixes them up (3 and E, B and 8 etc)
Meares-Irlen Syndrome. wears glasses to help with his sight struggles reading large blocks of text as they look like patterned lines and can cause headaches very light sensitive very different prescriptions in each eye including slight colour distortion has trouble with distance, depth perception and hand-eye coordination frequent headaches
Autistic-Spec/ASD might have autistic spectrum disorder? definitely has a range of the symptoms and traits.
Swatch
ASD definitely on the autistic spectrum. hates the use of "functioning" labels. has a sound sensitivity and prefers being indoors in the city to avoid the loud city noise. loves organizing and categorizing things by colour. delayed verbal responses
Dyscalculia Can count just fine for the most part but begins to struggle with larger numbers. Has difficulty reading strings of numbers verbal and visual math equations? not near this one. does however count money just fine. struggles with subtraction and counting backwards from high numbers can be very slow when anything involves numbers at times due to things taking a little extra time to process for him.
Dyspraxia never ask him to catch something, literally cannot, will drop it, it will fall and break if breakable. delayed physical reactions, tends to be off balance and will stumble and likely fail to catch himself if he jumps. the person who trips over themself when running, probably done so a lot as a kid and prefers just walking and keeping movements small and in one place. does bump into things sometimes, especially bumps into the wall when turning a corner but usually only when hes not fully focused on where hes going.
Synesthesia every single colour has its own flavour and sound and/or smell shapes have specific colours and sounds to them isnt sure how to describe it but can point it out sometimes will say something like "this colour sounds high pitched" or "this shape has a smooth feel"
Tasque Manager
ADHD misplaces things hyperfocused on one thing at a time but will attempt to multi-task lots of movement, even when in idle mode she is never perfectly still despite popular belief, concentrates just fine on tasks, she just cant multi-task very well, can only handle a few things at a time and likely will become side tracked but still makes progress on tasks. tries a lot to schedule herself and stick to a list of tasks, swatch more often than not helps her out with this.
Hyperlexia very fast reader often helps swatch with number related issues always has a word for something very good memory when it comes to numbers and words, possibly includes a photographic memory and/or "dictionary-like" memory. MUCH better at writing/typing out things than verbal communication. tends to repeat specific words, mostly when speaking but not entirely in a "stumbling over the word" kind of way probably has a book collection stored somewhere. yes swatch organized the books for her.
Synesthesia different colours emulate a taste or smell to her certain textures and flavours have a colour to her different sounds have different shapes and colours to them she can get very descriptive about it at times if youre curious. it goes on.
if you have anything to add or would like to share your own headcanons feel free!
the inbox is always open!
#swatch deltarune#spamton deltarune#deltarune hc#deltarune#deltarune headcanon#swatch hc#swatch#swatch dr#swatch nd headcanon#spamton headcanon#spamton#spamton g spamton#spamton nd headcanon#tasque manager#deltarune tasque#deltarune chapter 2#deltarune tm#tasque manager deltarune#tasque manager headcanon#tasque manager nd headcanon#nd headcanons#neurodivergent#neurodivergencies#neurodivergent headcanon#bees hc#hc request#requested hc#request
39 notes
·
View notes
Note
Not sure if you’ve answered this/talked about this before, but would you say that the whole “must have severe trauma before age 9 to have DID/OSDD/etc” treated as law by some of the community is as rigid of a criteria as the textbooks say? Is it possible to form alters later in life?
Honestly, despite people making it out to be an issue of the phrasing of textbooks, out of all of the books on trauma and dissociation that I have read, none have ever actually been as rigid as the plural community's own standards are. The textbooks which people are so quick to disregard as rigid are infinitely more nuanced than syscoursers make them out to be if people would just read them.
They use terminology like "such as", "usually", "almost always", but rarely ever use words like "never" or "always". I like the way textbooks approach the subject far more than the average syscourser does.
On the age range, it's a lot more complex than a strict cut-off number could ever really describe. For ages researchers have debated on what that number should be, I've seen as low as 6 and as high as 14. It gets messy when we consider factors such as delayed brain development, as well as onset of symptoms that can be tied directly to DID and amnesia (symptoms may be attributed to a wide variety of other things instead of DID, which makes it difficult to say definitively, "yes this is a 100% sign of DID at such-and-such age"). How can we tell when exactly an alter really formed, when many stay hidden until much later or are commonly known to not exactly be distinct until well into adolescence or adulthood?
I think that when people think of alter formation, there is a tendency to believe that they split off immediately with a full personality and fleshed out details or that you will notice them there, which isn't really the typical picture of DID. It's more common for alters to start off as just different emotional or functional states without their own identity, and may not have a seperate voice or super seperated memories or behaviors until later down the line. It's more common for alters, especially in childhood, to be more fluid and gradually become more dissociated and seperated over time. This can make it seem like alters are "forming" for the first time in the teen years or in adulthood, when actually they split off much earlier but just weren't all that developed or elaborate.
Being a covert disorder, even if signs of DID and alters are present at younger ages, people don't often really notice them or they explain them away with other things (such as ADHD or an overactive imagination).
Personally, I prefer it when people avoid using rigid language in discussions where the subject is more complex than that - It's accurate to say, for example, "DID comes from severe childhood trauma, usually from under the age of 9", because that's the picture most people with DID will fall into from what we know from decades of DID research. However, to say "The trauma must always be from before the age of 9" seems a bit silly when many professionals still debate on what the exact number is and we state it as if we know this as the absolute truth and like every human being develops at the exact same rate. If someone does not believe they fit this picture, also, they may say "Well, then I cannot have DID" and avoid looking into recovery and treatment, which isn't very helpful to anybody.
When "alters forming later in life" is very much tied to subjective experiences and how each individual system defines "forming", as well, I think it's a bit odd to debate about. People get too fixated on numbers and rules, in my opinion.
18 notes
·
View notes
Note
Hey just for your info, neurodivergent is an umbrella term that encompasses any difference to do with the brain, so Mattie already qualifies as neurodivergent just based on having cerebral palsy!! A lot of people seem to use neurodivergent as shorthand for just ADHD and autism, but the person who coined it specifically wanted it to be as inclusive as possible, so while ADHD and autism definitely fall under it, so does anything from schizophrenia and personality disorders to stuff like cerebral palsy and multiple sclerosis. Sorry if this comes off as overbearing and annoying, I just wanted to get this info out there!!
I am aware of this, I explained it terribly, I'm so sorry!
I have cerebral palsy myself, and part of why I don't have an autism diagnosis is because they can't separate the autism from the brain damage; it's not a clear-cut thing, which leaves things rather undefined. I could be autistic, or it could just be the brain damage. Who the hell knows?
I also meant it in regards of cerebral palsy not really having clear symptoms. The physical stuff, kind of, but plenty of medical professionals have told me that they cannot just give a list of symptoms or an idea of what CP looks like in response to how it manifests in personality, despite knowing that the scarring has an effect on that since there aren't many studies on that and it's hard to judge. They can guess based on the location of the scar if they find it in a scan, but that's it.
While I know that autism and ADHD can be just as varied, it's certainly easier to research and find lists of symptoms than for someone with CP, especially as the information about the condition focuses on the muscles, as that's what the condition mostly affects.
Mattie's health is based on my own, which is a jumbled mess, so while I can tell you my own symptoms and what hers will be, it's not like Charlie who just point-blank tells you they're autistic in chapter 3 (if you make the right choices), it's more subtle and less clear-cut.
13 notes
·
View notes
Note
Hey I saw your post about questions about autism and that you were open to receive them. I hope this ask isn’t bothering you in any way or seems insulting. If so, I’m incredibly sorry.
Recently, I’ve had my suspicions that I might be on the spectrum. I highly empathize with the aspects of sensitivity to external stimuli (specifically noise and light), I believe some of my habits such as consistently tapping and moving my feet, and repeating back what others say.
I have an audio processing disorder and I am also transgender. (I’m aware that these two things have a correlation with being autistic.)
However, I feel like I don’t suffer any of the social problems that having autism can bring. Do you have to have these social interaction problems? Would a doctor take me seriously with my concerns?
there is a difference between traits and diagnostic criteria. The main manuals for diagnostic criteria are the DSM (by the APA) and the ICD (by the WHO). I prefer the ICD, because I am not American, it is freely available online, and its autism section is very detailed with divisions that actually make practical sense.
Here is the link: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/437815624
You can read it yourself, but the required features for the DX according to the ICD-11 are essentially as follows:
Limitations in initiating and maintaining social communication, and reciprocal social interactions. (for example, having trouble starting conversations, feeling like its very effortful to keep them going, having a lot of one-sided interactions where you do all the talking, etc)
Repetitive behaviour, interests, and activities (stimming, special interests, "black-and-white thinking" all fall under this)
These symptoms becoming obvious during childhood
These symptoms resulting in significant difficulties in personal, family, social, educational, occupational or other important areas of functioning (basically it means you have extra trouble working, at school, with friends, family)
So, basically, while there are a LOT of autistic traits there are only two that matter for a diagnosis: social ability and repetitive behaviour.
based on what you say, you may have the repetitive behaviour but you dont feel like you have the social ability part. It is possible that you do have social difference, there are several reasons why you might not realise that for example if you put a lot of effort into socialising as if common with presentations associated with femininity, or if all of your friends and family are more neurodivergent than average, or some other reason.
Or you might not be autistic. There are other neurodivergent conditions that have repetitive behaviour. I believe ADHD involves some, and the people with ADHD I know tend to be a bit more confident in their social ability (unless they are very generally anxious people which they frequently are, but comparatively...)
An important thing to remember is that diagnosis is not important or necessary for everyone. a lot of us grow up developing relatively functional "systems" for how to get around the gap between our behaviours and those of the neurodivergent population. And the state of support systems are so poor in most places that it may end up being a lot of money and time for very little benefit. I would recommend seeing a doctor about it if you feel you would benefit from accommodations at work or at school and these accommodations require a diagnosis in your country. Or if a diagnosis would be free in your country. I got formally diagnosed and I definitely needed it to progress, but I know that not everyone does. The community will largely be accepting if you feel you would like more informal support.
I am not a professional and this is not professional advice.
#not yet a professional#not YET#but when I am i will not be allowed to post things like this#autism#neurodivergence
5 notes
·
View notes
Text
#it's not even that someone on tiktok was annoying about adhd. it's that NTs on tiktok pretend to have adhd or autism or some other disorder#so that they can feel Special:tm: and thus end up making those disorders sound ridiculous with their complete misunderstanding of what thos#disorders are actually like. and because young people have no fucking critical thinking skills anymore they don't recognize it
lmao yeah so this is the exact thing i was talking about, actually! the way mental illness and disability commonly find themselves talked about in particular circles on social media (with very little critical thought being put towards an understanding of categories of ‘brain behaviour’ as socially constructed around a fulcrum of hegemony & the atomisation of quirks posited in deliberately vague language as ‘symptoms’ with the sense that X + Y = Z rather than Z being a collective term encompassing behaviours under which X or Y might fall, and Z is a taxonomical tool rather than an explanation) should (and in some circles, has) provoked discussion of the actual purpose of these categories, but instead it turns into a pissing contest about whose autism or ADHD or whatever else is or isn’t Valid.
like, this response is the exact thing i was describing in the original post, such that i’m genuinely baffled as to how you managed to read this and come away thinking i was on your side. the assumption that you can “know” whether or not an individual’s self-identification as one category or another is “true” (or else, as you say, stemming from a desire to feel “special”) presumes access to a person’s interiority that you are neither able nor entitled to have. the “truth” of a disability, or a mental illness, does not exist. i am not an ontologically autistic person; i am a person with a cluster of behaviours and predispositions that have been grouped together and classified as autism to the purpose of articulating my position in relation to a hegemonic state that we call neurotypicality. describing myself as autistic helpfully clarifies that position both in terms of understanding myself & in understanding the world around me and how i interact with it/it interacts with me, but that doesn’t mean i believe i’m describing an objective property. assigning legitimacy to objective truth over usefulness within a social constructionist worldview is a nonsense; and it leads to exactly what i described above, ie. the belief that a certain demographic of people are “faking” or else misattributing their personal quirks to particular labels of disability and/or mental illness and thus don’t deserve to be taken seriously when articulating themselves as such, which in turn means that anyone self-describing as such is worthy of dismissal.
i’m 100% sympathetic to conversations about hierarchies of social functionality within disability wherein - for example - some autistic people will effectively ‘punch down’ on other autistic people whose autism puts them in a position of greater social alienation, but the conversation to be had there is to do with how a greater proximity to the platonic ideal of neurotypicality causes people to essentially cash in what little social currency they can garner from that proximity at the expense of those who lack it. an autistic person who is eg. able to hold down a job, go about their day unassisted, live independently may well - rhetorically or otherwise - reinforce the social structures which keep autistic people who are not capable of those things in states of social alienation, but playing games of who is and isn’t “really” autistic overlooks the fulcrum of the relation ie. proximity to hegemony in favour of turning to the Autism Litmus Test & reifying the category as an objective description of an objective reality in the process.
please have like a basic understanding of antipsych before commenting on my posts lmfao
vast swathes of young people becoming more and more empowered to voice reactionary sentiments towards all kinds of disabled people because their internet circles collectively decided that someone on tiktok was annoying about their adhd
#so many WILD generalisations happening here. young people want to feel special. young people have no critical thinking skills.#anything to back those assertions up? at all?#antipsych
14K notes
·
View notes
Text
What Does a Dual Diagnosis Mean?
If communities come to realize the effects of substance use, then the provision of rehabilitation services must become significant issues in addressing better and healthier lives for those concerned.

A dual diagnosis is a term used in the healthcare field to describe a situation in which a person's simultaneous experience of both a mental health illness and a drug and alcohol use problem. This complicated situation can exacerbate both illnesses' symptoms, resulting in a challenging cycle. Comprehending dual diagnosis is essential for successful therapy since treating one condition alone frequently results in setbacks, highlighting the necessity of comprehensive treatment to promote long-term healing.
What is Dual Diagnosis?
Dual diagnosis, often known as co-occurring disorders, refers to people who have both a mental disease and a drug use disorder (SUD). A cycle that complicates diagnosis, treatment and recovery might result from the interactions between these two disorders. For example, someone who is depressed could use alcohol as a self-medication, but this may worsen their symptoms of depression. Similarly, people with anxiety disorders may abuse medications in an effort to manage their symptoms, only to discover that their substance use issue causes their anxiety.
Understanding the Components of Dual Diagnosis:
Substance use disorder and mental health condition are the two basic components of dual diagnosis. It's critical to dissect each of these elements in order to comprehend the idea more fully.
Mental Health Disorders
Many problems that impact a person's emotions, thoughts and behavior are included in the category of mental health disorders. Anxiety, depression and bipolar illness are a few of the more severe disorders that fall under this category. Among the mental health conditions that are most frequently observed in people who have multiple diagnoses are:
Depression: Characterized by chronic dissatisfaction, loss of interest in activities and a sense of hopelessness.
Anxiety Disorders: Including generalized anxiety disorder, panic disorder, and social anxiety, marked by excessive fear or worry.
Bipolar Disorder: A condition that causes extreme mood swings that including emotional highs (mania or hypomania) and lows (depression).
Schizophrenia: A severe mental disorder that affects how a person thinks, feels, and behaves, often involving delusions and hallucinations.
Post-Traumatic Stress Disorder (PTSD): Severe anxiety, flashbacks and uncontrolled thoughts about the traumatic experience are often the cause of it.
Substance Use Disorders
The abuse or dependency on drugs, alcohol or other substances is referred to as a substance use disorder (SUD). It can vary from sporadic abuse to full-blown addiction, in which the user is unwilling to give up even after being made aware of the harmful effects. Typical drugs used in SUDs include:
Alcohol: The most commonly abused substance worldwide, leading to a range of physical and mental health issues.
Opioids: Including both prescription painkillers and illegal drugs like heroin, opioids are highly addictive and can result in significant health deterioration.
Stimulants: substances that are often abused such as cocaine, methamphetamines or prescription drugs (like Adderall) prescribed to treat ADHD.
Marijuana: Marijuana usage, while usually considered to be less dangerous, can nevertheless develop to dependence and worsen mental health disorders.
The Connection Between Mental Health and Substance Use
Substance use problems and mental health are intimately related. Studies reveal that about 50% of those with mental illnesses will also develop drug use disorders at some time in their life and vice versa. Given that one of these disorders frequently makes the other worse, their interaction can be complicated. They interact in the followingimportant ways: Self-Medication: People who suffer from depression, anxiety or other mental illnesses may use medications or alcohol to help them cope with their symptoms. This is especially prevalent in those who believe that conventional treatment choices such as counseling or medication are unachievable or useless. Substance-Induced Mental Health Issues: Drug or alcohol abuse over an extended period of time can change brain chemistry and cause the emergence of new mental health problems. For example, excessive alcohol use can result in sadness, yet abusing stimulants can lead to anxiety or paranoia. Shared Risk Factors: Individuals are more vulnerable to developing mental health disorders and substance misuse due to genetics, trauma and environmental factors.
Signs and Symptoms of Dual Diagnosis
The individual mental health and drug use problems involved can have a substantial impact on the symptoms of dual diagnosis. But there are certain clear indicators that someone may be dealing with a mental health problem in addition to a drug use disorder: Changes in behavior or mood: Sudden or serious changes in mood, anxiety or irregular sleep habits may indicate co-occurring mental health disorders and drug abuse. Social withdrawal: Isolating from friends, family or social activities may indicate depression or anxiety coupled with substance use. Neglect of responsibilities: Missing deadlines for job, school or family responsibilities can be a warning sign, especially when substance abuse is involved. Substance tolerance and withdrawal: suffering withdrawal symptoms while abstaining from drugs or alcohol, building a tolerance to them and needing more to have the same impact. Compulsive use despite negative consequences: Continuing to use drugs or alcohol even when it is causing harm to mental or physical health, relationships or daily life. Physical symptoms: People may exhibit symptoms such as inexplicable exhaustion, fluctuations in weight or repeated medical illnesses associated with substance abuse and mental health problems.
Why is Dual Diagnosis Complex?
Dual diagnosis is particularly complex for several reasons: Mutual Reinforcement: Addiction to substances and mental health conditions may worsen one another. Treatment is made more challenging by this cyclic pattern since treating one problem without addressing the other frequently results in relapse. Difficulty in Diagnosis: Differentiating between a person's symptoms caused by substance abuse or mental illness can be difficult. For example, anxiety might be a sign of drug withdrawal or it could be a side effect that caused the drug usage. Stigma: Dual-diagnosis individuals frequently experience double stigma. Mental illness and addiction are already highly stigmatized in society and those who occur together may face much more bias or social exclusion than others.
Treatment Approaches for Dual Diagnosis
Treatment for dual diagnosis involves a comprehensive, integrated strategy that treats both the mental health and drug use disorders. Potential treatment methods are as follows: Integrated CareThis involves a coordinated treatment plan where both the mental health and substance use disorders are treated simultaneously. This approach is more effective than treating each condition separately, as the interaction between the two is acknowledged and addressed holistically. MedicationMedication such as mood stabilizers, antipsychotics or antidepressants may be administered, depending on the particular mental health issue. Methadone and buprenorphine are two other drugs that can be used to treat substance use disorders, especially opioid dependency. TherapyTherapy can help people understand the root causes of their substance use and develop strategies to maintain sobriety. Cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT) are commonly used to help people manage their mental health conditions and develop healthier coping strategies. Support GroupsPeer support is an essential component of rehabilitation and organizations like Mental Health Support Groups and Alcoholics Anonymous (AA) or Narcotics Anonymous (NA) may offer a feeling of accountability and community. Holistic ApproachesHolistic methods including mindfulness, meditation, physical activity and dietary counseling are also commonly included in therapies to support patients in maintaining their sobriety and mental health.
Challenges in Diagnosing Dual Diagnosis
The symptoms of substance use disorders and mental illnesses frequently overlap, making dual diagnosis detection difficult. For example, if a person with anxiety disorder drinks alcohol as a coping mechanism, they may exhibit symptoms that are exclusive to alcohol use without treating the underlying anxiety. Similar to how drug abuse may mimic or conceal the signs of mental health conditions, it can be challenging for medical professionals to determine which problem initially occurred or the most effective course of action for the patient. Many people with dual diagnoses receive wrong diagnoses at first because medical providers may just treat the drug use disorder without recognizing there is a mental health problem present as well. This could end in a cycle of relapse and insufficient therapy.
Importance of Early Intervention
Recovery chances are higher if a dual diagnosis is detected and treated early. If left untreated, dual diagnosis can exacerbate mental health symptoms, promote drug abuse and have a variety of negative effects such as marital problems, health concerns, and legal troubles. But many people with dual diagnosis may manage their diseases and have happy, productive lives if they receive prompt and appropriate care.
Conclusion
The complicated relationship between mental health and drug use problems makes dual diagnosis particularly challenging. The secret to long-term healing is an integrated, individualized treatment strategy that takes care of both problems at the same time. Early detection and treatment may greatly enhance results by giving people the resources and encouragement they require to take control of their mental health and attain sobriety.
1 note
·
View note
Text
Skip to main content

Home
Conditions
Back
Conditions
View All
ADD/ADHD
Allergies
Arthritis
Atrial fibrillation
Breast Cancer
Cancer
Crohn's Disease
Depression
Diabetes
DVT
Eczema
Eye Health
Heart Disease
HIV & AIDS
Lung Disease
Lupus
Mental Health
Multiple Sclerosis
Migraine
Pain Management
Psoriasis
Psoriatic Arthritis
Rheumatoid Arthritis
Sexual Conditions
Skin Problems
Sleep Disorders
Ulcerative Colitis
Drugs & Supplements
Back
Drugs & Supplements
Drugs
Supplements
Pill Identifier
Interaction Checker
Well-Being
Back
Well-Being
Aging Well
Baby
Birth Control
Children's Health
Diet & Weight Management
Fitness & Exercise
Food & Recipes
Health & Balance
Healthy Beauty
Men's Health
Parenting
Pet Health
Pregnancy
Sex & Relationships
Teen Health
Women's Health
Symptom Checker
Find a Doctor
More
Back
More
News
Blogs
Podcasts
Webinars
Newsletters
WebMD Magazine
Best Hospitals
Support Groups
Privacy & More
Subscribe
Log In
Search
Subscribe
Epilepsy
Epilepsy Guide
Help When Epilepsy Treatment Doesn't Work
Medically Reviewed by Christopher Melinosky, MD on May 12, 2023
Written by Katherine Kam
7 min read
What Is Refractory Epilepsy?
If your doctor says you have refractory epilepsy, it means that medicine isn't bringing your seizures under control. You might hear the condition called by some other names, such as uncontrolled, intractable, or drug-resistant epilepsy.
Your doctor can try certain things to help keep your seizures under better control. For instance, they might try different combinations of drugs or a special diet.
Your doctor may also put a device under your skin that sends electrical signals to one of your nerves, called the vagus nerve. This may cut the number of seizures you get. A Neuropace device is a reactive neurostimulator that detects seizures and shocks the brain to stop them.
Surgery that removes a part of the brain that causes your seizures may also be an option. With any of these treatments, you may still need to take epilepsy medicine throughout your life.
It's natural to feel anxious when the doctor tells you your epilepsy isn't getting better with the medicine you're taking. You don't have to go through it alone, though. It's important to reach out to family and friends to get the emotional support you need. You might also want to join a support group, so you can talk with other people who are going through the same things you are.
Featured
Tests and a Diagnosis for Epilepsy
Common Types of Seizures
Types of Epilepsy
Causes
Doctors don’t know why some people have refractory epilepsy and others don't. You can have refractory epilepsy as an adult, or your child might have it. About 1 in 3 people with epilepsy will develop it.
Symptoms
The symptoms of refractory epilepsy are seizures despite taking anti-seizure medication. Your seizures could take different forms and last from a few seconds to a few minutes.
You may have convulsions, which means you can't stop your body from shaking.
When you have a seizure, you may also:
Black out
Lose control of your bowels or bladder
Stare into space
Fall down suddenly
Get stiff muscles
Bite your tongue
Getting a Diagnosis
Your doctor has several ways to diagnose refractory epilepsy. They may ask you questions such as:
How often do you have seizures?
Do you ever skip doses of your medicine?
Does epilepsy run in your family?
Do you still have seizures after taking medicine?
Your doctor may also give you a test called an electroencephalogram. To do this, they'll place metal discs called electrodes on your scalp that measure brain activity.
Other tests might include a CT scan of your brain. It's a powerful X-ray that makes detailed pictures of the inside of your body.
You might also need to get an MRI of your brain. It uses magnets and radio waves to make pictures of your brain.
If you need surgery to treat refractory epilepsy, these tests can help doctors find out where your seizures are starting.
Your doctor will most likely want you to report your symptoms regularly. They may try several drugs at different doses.
Questions for Your Doctor
What might be causing my seizures?
Which tests are needed to diagnose refractory epilepsy?
Should I see an epilepsy specialist?
What treatments are available for refractory epilepsy?
What precautions should I take to avoid getting injured during a seizure?
Are there any limits on my activities?
Treatment
Medications. Your doctor may take a second look at the drugs you're taking. They may suggest another medicine, either alone or combined with other drugs, to see if it helps you have fewer seizures.
Many drugs can treat epilepsy, including:
Brivaracetam (Briviact)
Cannabidiol (Epidiolex)
Carbamazepine (Carbatrol, Tegretol)
Cenobamate (Xcopri)
Clobazam (Sympazan)
Divalproex (Depakote)
Dilantin (Phenytek)
Eslicarbazepine (Aptiom)
Felbamate (Felbatol)
Gabapentin (Neurontin)
Lamotrigine (Lamictal)
Levetiracetam (Keppra)
Oxcarbazepine (Trileptal)
Perampanel (Fycompa)
Potiga (Ezogabine)
Primidone (Mysoline)
Rufinamide (Banzel)
Tiagabine (Gabitril)
Topiramate (Topamax)
Vigabatrin (Sabril)
Zonisamide (Zonegram)
Surgery. If you still have seizures after trying two or three anti-epilepsy drugs, your doctor might recommend brain surgery.
It can help a lot if your epilepsy only affects one side of your brain. Doctors call that refractory partial epilepsy.
A surgeon removes the area of your brain that's responsible for your seizures.
It's natural to worry about brain surgery and to wonder if it will affect the way you think or if you'll seem like a different person afterward. Talk with your doctor about what to expect if you choose the surgery or if you don't, so you can weigh the risks and benefits. A lot of people who have the surgery say that getting free of seizures -- or at least making them less common and less intense -- makes them feel much better.
The surgeon usually operates on an area of your head that's behind your hairline, so you won't have noticeable scars.
After it's done, you'll probably need to stay in an intensive care unit of the hospital for a few days. After that, you'll move to a regular hospital room, where you may need to stay for up to 2 weeks.
You should take it easy for a while after you get back home, but you'll probably be able to return to a normal routine in 1 to 3 months. Even with the surgery, you might need to take seizure medication for a few years. You might need to stay on the drugs for the rest of your life.
Talk to your doctor about any side effects you might have from the surgery. You can ask them to put you in touch with other people who've had the surgery, so you can better understand what to expect.
Diet. The ketogenic diet helps some people with epilepsy. It's a high-fat, low-protein, no carb diet. You have to start it in a specific way and follow it strictly, so you need a doctor's supervision.
Your doctor will watch closely to see whether or when you can lower any of your medication levels. Because the diet is so specific, you may need to take vitamin or mineral supplements.
Doctors aren't sure why the ketogenic diet works, but some studies show that children with epilepsy who stay on the diet have a better chance of reducing their seizures or their medications.
For some people, a modified Atkins diet may work, too. It's slightly different from the ketogenic diet. You don't have to restrict calories, protein, or fluids. Also, you don't weigh or measure foods. Instead, you track carbohydrates.
People with seizures that are hard to treat have also tried a low-glycemic-index diet. This diet focuses on the type of carbs, as well as the amount that someone eats.
Electrical stimulation, also known as neuromodulation. This technology works directly on your nerves. It changes or controls nerve activity by sending electrical signals or medicine to a specific area. Methods include:
Cortical stimulation. Temporary electrodes are placed on the surface of your brain. The doctor sends a signal through them at a level low enough that you won’t notice. If it helps, they can be replaced with permanent electrodes for continuous stimulation.
Closed-loop stimulation. The doctor implants a device under your scalp and within your skull. It’s connected to two electrodes placed either on the surface of your brain, in the brain, or both. The electrodes record your brain waves. When the neurostimulator detects seizure-like activity, it sends a small electrical current to your brain that can stop, shorten, or maybe prevent the seizure.
Deep brain stimulation. The doctor implants thin electrodes deep into certain areas of your brain and a pulse generator under your collarbone. Wires under your skin connect the two. The pulse generator sends signals to disrupt abnormal patterns of brain activity.
Vagus nerve stimulation (VNS). The doctor puts a device that looks like a heart pacemaker under your left collarbone. It connects to the vagus nerve in your neck through a wire that runs under your skin. The device sends a current to the nerve, which may cut down on the number of seizures you get or make them less intense.
Clinical trials. You may want to ask your doctor if you could take part in a clinical trial. These trials test new drugs to see if they're safe and if they work. They're often a way for people to try new medicine that isn't yet available to everyone.
Taking Care of Yourself
Stress can sometimes trigger seizures. Talking to a counselor is a great way to find solutions to manage your stress.
Try going to a support group, too. You can talk with people who know what you're going through and who give advice from their own experience.
What to Expect
Even though you have refractory epilepsy, it's still possible to get your seizures under control. It may be a matter of switching to a different treatment.
Your doctor may find a different drug combination that helps. Getting electrical stimulation of the vagus nerve means fewer seizures for about 40% of people who try it. And if a brain surgeon can remove the part of the brain that's causing seizures, the seizures may stop, or at least happen less often and become less intense.
Getting Support
As you are finding out what works best, you'll need a strong network of family and friends who can offer emotional support, especially if your seizures prove hard to control. Having a trusted person to listen to you can be a great comfort when you're going through something tough.
Ask your doctor for information on support groups in your area. You can also find out about support groups by going to the website of the Epilepsy Foundation.
SourcesUpdate History
Share
Print
Save
View privacy policy, copyright and trust info
More on Epilepsy

Understanding Epilepsy Basics
What Is Epilepsy Surgery?
Everyday Tips for a Child With Focal Onset Seizures
Recommended

FEATURED
Related Links
Epilepsy News
Epilepsy Reference
Epilepsy Slideshows
Epilepsy Videos
Epilepsy Medications
Find a Neurologist
Brain & Nervous System
Children's Health
Drug Interaction Checker
Juvenile Myoclonic Epilepsy
Lennox-Gastaut Syndrome
Sign up for our free Good Health Newsletter
Get wellness tips to help you live happier and healthier
Subscribe
By clicking Subscribe, I agree to the WebMD Terms & Conditions & Privacy Policy and understand that I may opt out of WebMD subscriptions at any time.
Follow WebMD on Social Media
Download WebMD App

Policies
About
For Advertisers
Privacy Policy
Cookie Policy
Editorial Policy
Advertising Policy
Correction Policy
Terms of Use



© 2005 - 2024 WebMD LLC, an Internet Brands company. All rights reserved. WebMD does not provide medical advice, diagnosis or treatment. See additional information.

0 notes
Text
AuDHD Annotated Bibliography as of fall 2024. MH
Methodology
The purpose of this annotated bibliography is primarily to broaden the understanding of AuDHD literature and media that is publicly accessible for myself and other interested peeps. The formatting style originates from MLA with some differences based on my own preferences (and the fact I’m not in academia anymore so this is not being graded or peer reviewed). Organization of this AB has also been changed to my personal preferences.
I also want to say that this AB’s focus is primarily research/expression for adults. Some of the content is primarily for adults diagnosed/discovered their neurodiversity later in life. I acknowledge that there is a lot of content on social media (Instagram, tiktok, etm.) but I do not consider these sources to be open access because many of them require an account to view media and the rules around what content is allowed seems to be mercurial.
Posts on here that do not have blurbs mean that I have not fully read the content yet and is basically TBR. If you have an open access media you would like to be added to this list please feel free to contact me and I will evaluate it for addition!
Blog posts
“Support for dual diagnosis (autism + adhd).” Neurodiverse Couples Counseling Center, https://www.neurodiversecouplescounseling.com/audhd Accessed 29 Aug 2024.
Audience is significant other of someone who has AuDHD and new AuDHDers (adults). They sometimes cite their sources and do not use the disease-based model. They use multimedia – pictures, videos, as well as written. The venn diagram is not as good as Dr. Neff’s. Explanation of co-occurrances between ADHD and autism does not feel fleshed out. *they do not cite the studies they discuss in the section of how pregnancy could be connected to autism.
I appreciated that under treatment approaches they say expressly “Please know that the goal of behavior therapy must NOT be to turn you into a neurotypical person. It is to help you find ways to cope while living in an allistic world and be TRUE TO YOURSELF!” [italics in original].
*Clarified that autism and adhd could not be dual diagnosis until publication of DSM 5 which acknowledges the wide range of symptoms clients can experience.
ADDitude Editors "'A living contradiction:' the AuDHD experience" ADDitude, https://www.additudemag.com/audhd-autism-adhd-experience/ Accessed 4 Sept. 2024
Relatively brief, sources cited. Anecdotes from people's lived experience having autism and ADHD. There are a nice variety of perspectives-- some people talk about adhd conflicting with autism, others find that they compliment each other. One anecdote is from the mother of an AuDHD child, multiple anecdotes from people diagnosed later in life.
Hinze, Emma, et al. ��Understanding AuDHD strengths.” Attwood & Garnett Events https://attwoodandgarnettevents.com/what-is-the-neurodiversity-affirming-movement/ Accessed 29 Aug 2024.
References cited. Provides a list of strengths as well as misconceptions about AuDHD. Website appears to be informative- has posts on the neurodiversity-affirming movement, autism in women and girls, autism and ptsd in adults, etc. Also host master classes for “professionals, parents and those on the spectrum.”
Peer Reviewed Articles
Craddock, Emma “Being a woman is 100% significant to my experiences of ADHD and autism: Exploring the gendered implications of an adulthood AuDHD diagnosis.” Qualitative Health Research, 2024. https://www.open-access.bcu.ac.uk/15499/1/QHR_final_accepted_version_190424.pdf Accessed 29 Aug 2024.
This article discusses the gendered omission of women and girls from autism and adhd diagnoses and the theoretical and practical implications of the co-occuring conditions. This research aims to “bridge the gap” since previously late diagnosed ADHD and late diagnosed autism have been researched but not both together.
This study was among 6 participants who were white women between the ages of 34-55 in the UK. Two had PhDs, four worked full-time and two were unemployed. The study used Interpretative Phenomenological Analysis (IPA) and interviews were conducted via email, which was a much more autistic-friendly approach.
Some women identified being weird and also having to perform femininity, learning to be social was considered important but could be somewhat overlooked if the woman performed well in school. Women internalized their experiences and masked for normalcy as well as femininity. Some said that due to autistic inability to read social queues or adhd inattention to situations could lead to bullying and later SA. Gendered masking weighed heavily on women due to sensory sensitivities such as wearing bras, high heels, and other clothes they wore to mimic other women’s style of dress. One woman said that she had trouble advocating for herself, her coworkers and boss did not see her struggles so it felt like a burden to let others around her know that she was not doing well. All participants said being undiagnosed was a traumatizing experience, that they knew they were different but not knowing why led to negative self judgement. The women also said that there was a lack of post-diagnosis support, leaving them to process the information by themselves.
*I liked that it touched on - barriers around AuDHD includes lack of descriptive language to this day. Women are often dismissed when trying to get diagnosed and are diagnosed later than men. A woman with a diagnosis often dismissed when she states that she is AuDHD or otherwise neurodivergent.
Craddock, Emma “Raising the voices of AuDHD women and girls: Exploring the co-occuring conditions of autism and ADHD.” Disability & Society vol. 39, no. 8, pp. 2161-2165, https://www.tandfonline.com/doi/pdf/10.1080/09687599.2023.2299342 Accessed 29 Aug 2024
Hamilton, Inga “An Autistic Aesthetic of Connectivity.” Ought: The Journal of Autistic Culture, vol. 5, iss. 2., 2024. https://scholarworks.gvsu.edu/cgi/viewcontent.cgi?article=1169&context=ought Accessed 29 Aug 2024.
McKay, Erin, et al. “Proactive inhibitory control as a cognitive contributor to social difficulties in adolescents with ADHD traits.” Neurodiversity, vol. 2, pp. 1-13. https://journals.sagepub.com/doi/pdf/10.1177/27546330241258329 Accessed 29 Aug 2024.
This article looks at social difficulties between people with ADHD, people with ADHD with social difficulties, autistic people, and a small set of people with AuDHD. The conclusion of this article (that was most interesting to me) was that social difficulties are subtly different between people with ADHD and people with Autism. The subset of individuals with AuDHD they include because of their own interest and the authors note that the group with AuDHD is very small as a limitation.
Rosqvist, Hanna Bertilsdotter, et al. “Naming ourselves, becoming neurodivergence scholars.” Disability & Society, 2023. https://doi.org/10.1080/09687599.2023.2271155 Accessed 29 August 2024.
Websites
Neff, Megan Anna, Neurodivergent Insights https://neurodivergentinsights.com/
Some things are behind a paywall but has good blog posts and nice venn diagrams of what traits overlap between different neurodiversities. Author identifies as AuDHD, discussed in some blog posts. Some posts are also about mental illness, appreciate the intersection. Cites sources.
Ought: The Journal of Autistic Culture. https://scholarworks.gvsu.edu/ought/
This peer-reviewed journal (obviously) focuses on autistic experiences, it includes pieces and articles from/about people with other neurodivergent experiences including AuDHD.
#neurodivergent#neurospicy#audhd#actually autistic#neurodiversity#neurodivergence#actually audhd#peer reviewed
0 notes
Note
Also really glad to see that your blog is cluster-B safe! Despite what I said in my other asks about me feeling hesitant to label myself as nebularomantic due to it falling under the aro umbrella and me not relating to aros at all (but also not relating to allos because most of them draw a very hard line between platonic and romantic love and their experience of it is very alien and foreign to me and has actually led to some very unpleasant social interactions in the past), I do relate to the experience very much and I am pretty sure it's caused by the combination of all my personality disorders.
I also have diagnosed ADHD and used to be considered autistic as well (that was later changed to a misdiagnosis and now I'm considered ADHD with a lot of autistic traits) but for me, the problems with differentiating between platonic and romantic love seems to be directly caused by my 3 diagnosed personality disorders specifically. I have Schizotypal, Borderline and Avoidant. And like if I had just one of them this wouldn't be happening, I think, and maybe even the killer combo itself wouldn't be that much of a problem but I also have a lot of symptoms of NPD. Which isn't that weird, cluster B disorders tend to kinda overlap and while most of my BPD friends don't show NPD traits, coincidentally my one friend with NPD does have a lot of BPD symptoms. But yeah I have a fair share of NPD traits as a cherry on the top of my BPD cake, and when that combines with my STPD and my AVPD, it creates this unholy concoction. Oh yeah and the asexuality was probably the last nail in the coffin because if I could feel sexual attraction I might be able to differentiate platonic and romantic based on my sexual feelings. But alas I am not sexually attracted to anyone at all, I just think that all bodies look cool as all hell and I am an admirer of the human form. People and the diversity of the human experience, both physical and psychical, always moves me to tears because people are just so beautiful and perfect aaaand sorry got carried away by the star bright perfection of humanity again.
your reasoning is exactly why nebularomanticism is not specifically an "autistic" label, but a neurodivergent one!
cluster b disorders are so unfairly demonized. this is totally a place where that will not be tolerated towards any personality disorders (or anyone at all.)
personally, mine is because of my autism- but I do have some NPD traits also (enough to make my life a more difficult, but not enough to be diagnosed.....) which may have something to do with it. i naturally don't have many friends, but if i do want a friend, it is strictly in the "acquaintance" category, and i just want the company, without the strong emotional connection. i've had friends who i care deeply about, but that same platonic love for those people..... could just as well be called romantic. if i were to date one of those people, my behaviour towards them wouldn't change- because it's the same feeling, with the same behaviors (TO ME). i don't understand the difference between taking a friend out to the movies, and taking your boyfriend on a date to the movies. that should be the same thing.... right? hahaha
it is interesting to me that some people do feel a real difference with those two types of "love."
thank you for sharing your experiences! i do agree a lack of sexual attraction may cause some difficulty in differentiating those feelings too. i can see what you mean.
humanity is beautiful! one of the reasons i made this blog was to have a place for all sorts of people to be able to share their feelings. it's been nice hearing from you!
#sorry for not answering this with the other ask!#it was late at night and i was tired.#thank you for sharing your experience!#ask#nebularomantic#cluster b#aromantic#asexual
1 note
·
View note