#tourette syndrome treatment
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s website traffic is steadily declining.
Text
Best Tourette syndrome Treatment - Aware Gleneagles Global Hospitals
Our Neuroscience team at Aware Gleneagles Global Hospital is fully equipped to effectively address a wide range of neurological diseases, establishing us as a premier centre for Neurological Disorders in Hyderabad. Our facility is outfitted with state-of-the-art technology and staffed by a dedicated team of highly skilled neurologists and surgeons. Supported by well-trained nursing assistants and Para-medical staff, we are committed to providing exceptional, patient-cantered care for individuals with neurological conditions. Furthermore, we specialize in the treatment of cerebellar ataxia and Tourette syndrome, two specific neurological disorders. Our team of experienced neurologists possesses in-depth knowledge and expertise in managing these conditions effectively, ensuring optimal care for patients.
We are dedicated to delivering excellent neurological care and look forward to contributing to the well-being of patients. Our highly qualified and skilled neurologists provide comprehensive care, guiding patients from initial evaluation to accurate diagnosis and personalized treatment. Understanding the individuality of each patient, we create customized treatment plans that address their specific needs. Additionally, we offer expert advice on incorporating dietary and lifestyle changes to enhance overall well-being, support recovery, and prevent nerve diseases.
Address: 8-16-1, Nagarjuna Sagar Rd, Laxmi Enclave, Bhagya Nagar, Bairamalguda, L B Nagar, Hyderabad, Telangana India
Phone.no: 9840911421
Website: https://awaregleneaglesglobalhospitallbnagar.com/top-best-specialities/neurology-hospital-in-hyderabad/
cerebellar ataxia treatment | Tourette syndrome
Nerve diseases | neurological diseases
0 notes
Text

Examining Tourette Syndrome Treatment Effectiveness.
It is crucial to consult with a healthcare professional for personalized advice and to explore other evidence-based treatments available for managing Tourette Syndrome Treatment by CT Marijuana. Learn how medical cannabis may provide relief from tics and associated symptoms. For more details visit our website.
0 notes
Text
No, I love the fandom too much, so I have to brazenly create another character...

Anyway, yes, meet the next OS, this is Kimberly, and she ended up in a psychiatric hospital due to lingering Tourette's syndrome. While most people with this diagnosis experienced a decline after a peak at 17-18 years of age, for her it continued until she was 20 and didn't stop, which is why her relatives decided to leave her for psychiatric treatment

And yes, of course I ship her with Campbell. What can you do to me, I'm just taking a break from work like that x'>
51 notes
·
View notes
Text
WHAT CREEPS ARE AUTISTIC? + SUPPORT LEVELS

A/n: this are the pastas I personally think are autistic and why because I am autistic and I'll pass down the autism.
ATTENTION: Most of these don't have relation to my other headcanons, is just for good fun. The only one that really applies to my other headcanons is Jane. Cody and Toby can be implied but not really mentioned

Jane: I'm projecting
Cody (xvirus): because I said so
Hoodie/Brian: Because he's literally me
Toby: Because he already has ADHD and tourettes so he might as well get the whole pack
Bloody Painter: I'm projecting²
Sally: Because autism is coquette and she's too
Eyeless Jack: Because why not?
These are the autism support levels
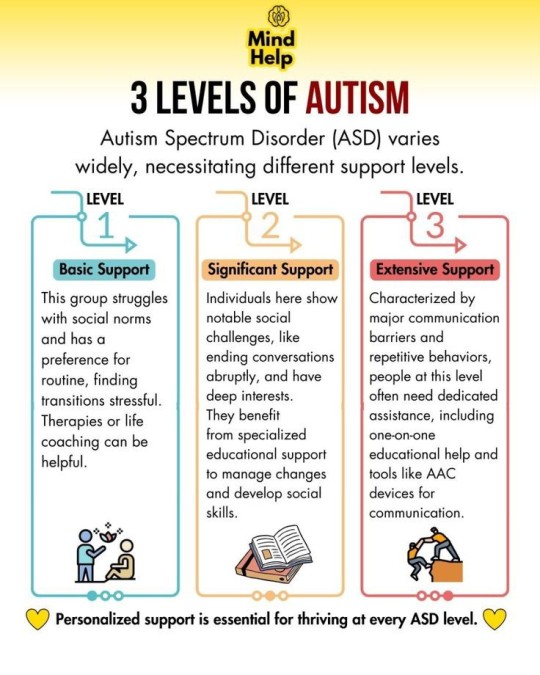
This is not set in stone, levels can fluctuate during the week/month based on how stressed the autistic person is or how well therapy/treatment is going. A person can also be between 2 levels, I myself am between level 1 and 2, because of my high masking. I have great social difficultys but can do day to day activities (mostly) fine, although on paper I'm level 1. Support levels can also be defined by concomitant disabilities, specially if they're intellectual (down syndrome, learning delay, etc)
Ok so now to the actual reasons
Jane: She's literally the embodiment of autism in afab people lmao. Her straightforward way of speaking, black and white thinking and strong sense of justice and difficulty forming connections are all very autistic traits. She's level 1 of support, 2 on bad days
Cody: High interest in microbiology = hyper focus + special interest. Bedsides I don't see him as "social" he prefers to be alone which could be either esquizoid personality disorder, autism or both. I'll go with both. He doesn't understand humans neither really like to be with them. They're level 2 (almost 3) support
Toby: Many psychological Disorders are accompanied with others, much like a pay one get three deal, tourettes, ADHD and autism are pretty common together. It is not always that "social difficultys" are tied to shyness or isolation, it can also be pushyness and a hyper personality much like Toby's personality. He's level 1
Hoodie/Brian: In my head he's schizophrenic AND autistic. Which really makes his paranoia worse, autism already make you hear things people filter out (like electricity) this together with auditory hallucinations makes him have really bad meltdowns. He's level 3 of support but with all the bullshit he's been through he's forcing himself to be level 1, he don't manage it very well so he acts like a level 2
Bloody Painter: isn't really specified why he's bullied in the og as far as I remember and many autistic folks are bullied for no reason. His passion for painting and drawing can be seen as an hyper focus /special interest. Also his hate from loud places and crowds can be because of sensory overload. Helen also has a personality similar to mine when I was younger so why not haha. He's level 2 of support
Sally: Is pretty rare that girls are diagnosed with autism below the age of 16. So I'll give a little representation here. Her love for pink and typically girly things to the point of looking like a stereotype can be read as her special interest. Autistic girls are often more naive than the average girl of the same age, which more often than not leads to abuse/bullying, so one more point there. Not much else besides the "I want her to be autistic because I wish I was diagnosed much younger". She's level 1 support.
Eyeless jack: He's the embodiment of sensory issues, bedsides I see him as pretty socially inept, not that he doesn't like to socialize, He just don't really know how (like me). Also I see his medical skills as being a side product of his Human body special interest. He's level 2 support
#creepypasta#creepypasta headcanon#slenderverse#jane the killer headcanons#jane the killer#x virus#cody x virus#x virus headcanons#hoodie headcanons#hoodie marble hornets#brian marble hornets headcanons#brian marble hornets#bloody painter headcanons#bloody painter#sally willians headcanons#sally creepypasta#sally headcanons#autism#autism headcanon#actually autistic
27 notes
·
View notes
Text
Port Mafia masterlist
Bold = oneshot
Chuuya:
S/O who had a fight with their parents and is crying
Reacting to S/O switching to customer service voice
With an S/O who suddenly initiates random physical contact
With an S/O who is professional at work but their apartment screams cuteness
With a rough S/O who has a heart of gold
With an S/O who had a rough day and just wants to cuddle
Comforting S/O who had an episode in public
With an S/O who can alter reality
Comforting reader who couldn’t sleep after watching a scary show
With an S/O similar to Ootori Emu
Reacting to S/O saying ‘when we have kids I can’t wait to take them trick or treating’
Soukoku in love with the same reader
Meeting S/O’s ex-fiancée
Reacting to S/O wearing lingerie (SFW)
With an S/O who's like present!Dazai
Ice skating with him
With an S/O who's scared of using their ability
No time to die
Boyfriend headcanons
First kiss headcanons (+ the Flags)
Blue Skies, Tainted Sorrow (Stormbringer!Chuuya)
With a female S/O who demands princess treatment
Unrequited love Part 2 Part 3 (final)
Tears to Shed
Akutagawa:
With a fem! S/O who has tourette syndrome
Reacting to S/O wearing lingerie (SFW)
Mori:
With an S/O who's scared of using their ability
#silverbladexyz#Port Mafia masterlist#bsd x reader#bsd x gender neutral reader#bsd x female reader#bsd x you#bsd x y/n#bungou stray dogs x reader#chuuya x reader#akutagawa x reader#mori ougai x reader
75 notes
·
View notes
Note
I'm back with another drug history request. How about abilify/aripiprazole?
Sometimes I look up a drug I think is going to be boring and it turns out wildly interesting (dextromethorphan). Sometimes I look up a drug I think is going to be super interesting, and it turns out to be kind of meh (aripiprazole).
Aripiprazole is an atypical antipsychotic. It is also sometimes called a second generation or even a third generation depending on who you talk to. It is used for treating schizophrenia, bipolar disorder, irritability due to autism, as an adjunct treatment for major depression, and tourettes syndrome.
First generation "typical" antipsychotics came out in the 1950s. They block dopamine in the brain. This helps to decrease "positive" symptoms of psychosis, such as hallucinations and delusions, but they can cause sedation and movement disorders which can be permanent.
Second generation "atypical" antipsychotics came out in 1994 and have a lot of different mechanisms of action, usually involving dopamine and serotonin. These decrease "positive" symptoms but also decrease "negative" symptoms like avolition and social withdrawal. These generally have side effects that are more metabolic in nature, such as weight gain and increased blood sugar levels.
Sometimes, dopamine stabilizing medications like aripiprazole and brexpiprazole are lumped in with second generation (they have a similar side effect profile), and sometimes they are put into their own category.
Aripiprazole was discovered in 1995 by Japanese scientists. It was approved in the US as a daily pill in 2002. In 2015 it became available as a once-monthly injection for people who had trouble remembering (or being willing to) to take pills daily.
Today it is the 99th most commonly prescribed medication in the USA.
19 notes
·
View notes
Text
How Common is Neurodivergence?

[image id: poster of "How Common is Neurodivergence?.” There are 12 circles and five small images: an image of a brain, speech bubbles, an infinity sign, a person reading, and a person surrounded by arrows and balls. Each of the 12 circles has a percentage representing how common a particular form of neurodivergence is written in Open Dyslexic font. Full transcript, more information, and references under the cut.]
More Information
Forms of neurodivergence represented here are focused on neurodevelopmental disorders.
These percentages are representative of percentage in general population and do not reflect percentages within neurotypes which are often higher due to co-occurrence being the norm, rather than the exception, within neurodevelopmental disorders; for example, 33-45% of people with ADHD will also have dyslexia (Butterworth & Kovas, 2013), whereas only 10% of the general population are dyslexic (British Dyslexia Association [BDA], 2023).
Certain neurodivergencies are often underrepresented and under-reported, so the percentages are likely to be higher; for example, one study suggests that rates for FASD in the UK may be as high as 17% (McQuire et al., 2019).
Some of the neurodivergencies represented here are umbrella terms and percentages given are representative of all forms of neurodiversity belonging to that term; for example, SpLds include dyslexia which is at a rate of 10% (BDA, 2023) and dyscalculia which is at 3-7% (Haberstroh & Schulte-Körne., 2019). Tic Disorders at 1% are another example here, as this is inclusive of Tourette Syndrome which is at 0.6%, and around 1 in 5 individuals exhibit tics at some point during childhood (Cavanna et al., 2017).
______________
Transcript in Full
1% Intellectual Disability
10% Language Disorder
4% Speech Sound Disorder
5% Stuttering
7.5% Social (Pragmatic) Communication Disorder
1.7% Autism
5% ADHD
10% Specific Learning Disorder (SpLD)
5% Developmental Co-Ordination Disorder (DCD)
3-4% Stereotypic Movement Disorder
1% Tic Disorders
3.6% Fetal Alcohol Spectrum Disorders (FASD)
______________
Sources
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th Ed., Text Rev.).
Arvidsson, O., Gillberg, C., Lichtenstein, P., & Lundström, S. (2018). Secular changes in the symptom level of clinically diagnosed autism. Journal of Child Psychology and Psychiatry, 59(7), 744–751.
Attention-deficit/hyperactivity disorder (ADHD). PsychDB. (2022, November 29).
Autism spectrum disorder (ASD). PsychDB. (2022, May 19).
Butterworth, B., & Kovas, Y. (2013). Understanding neurocognitive developmental disorders can improve education for all. Science, 340(6130), 300–305.
Cavanna, A. E., Coffman, K.A., Cowley, H., Fahn, S., Franklin, M. E., Gilbert, D.L., Hershey, T.G., Jankovic, J., Jones, M., Leckman, J.F., Lehman, R., Mathews, C.A., Malaty, I., McNaught, K., Mink, J.W., Okun, M.S., Rowe, J.A., Scahill, L.D., Scharf, J.M., Schlaggar, B.L., Stewart, E., Walkup, J.T., Woods, D.W.. (2017). The spectrum of Tourette Syndrome and TIC disorders: A consensus by Scientific Advisors of the Tourette Association of America. Tourette Association of America.
British Dyslexia Association. (2023). Dyslexia. British Dyslexia Association.
Dyspraxia at a glance. Dyspraxia Foundation. (2023).
Haberstroh, S., & Schulte-Körne, G. (2019). The Diagnosis and Treatment of Dyscalculia. Deutsches Arzteblatt International, 116(7), 107–114.
Ketelaars, M. P., Cuperus, J. M., van Daal, J., Jansonius, K., & Verhoeven, L. (2009). Screening for pragmatic language impairment: The potential of the Children’s Communication Checklist. Research in Developmental Disabilities, 30(5), 952–960.
May, P. A., Baete, A., Russo, J., Elliott, A. J., Blankenship, J., Kalberg, W. O., Buckley, D., Brooks, M., Hasken, J., Abdul-Rahman, O., Adam, M. P., Robinson, L. K., Manning, M., & Hoyme, H. E. (2014). Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics, 134(5), 855–866.
McQuire, C., Mukherjee, R., Hurt, L., Higgins, A., Greene, G., Farewell, D., Kemp, A., & Paranjothy, S. (2019). Screening prevalence of fetal alcohol spectrum disorders in a region of the United Kingdom: A population-based birth-cohort study. Preventive Medicine, 118, 344–351.
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E., Vamvakas, G., & Pickles, A. (2016). The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study. Journal of Child Psychology and Psychiatry, 57(11), 1247–1257.
Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442.
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry, 164(6), 942–948.
Prevalence and Therapy Rates for Stuttering, Cluttering, and Developmental Disorders of Speech and Language: Evaluation of German Health Insurance Data. (2021). Frontiers in Human Neuroscience, 15(645292), 1–13.
Social (pragmatic) communication disorder. PsychDB. (2021, March 29).
Stereotypic movement disorder. United Brain Association. (2022, August 8).
Wren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language, and Hearing Research, 59(4), 647–673.
UCL. (2013, April 19). Learning disabilities affect up to 10 per cent of children. UCL News.
#neurodiversity#neurodiverse stuff#neurodivergent#neurodivergence#actually autistic#actually audhd#autism#audhd#adhd#dyspraxia#disability#disabilties#neurodevelopmental#intellectual disability#communication disorder#stuttering#asd#motor disorders#dcd#actually dyspraxic#dyspraxic#tics#tourettes#splds#dyslexia#dyscalculia#dysgraphia#fasd
364 notes
·
View notes
Text
#tic disorder#tic disorders#tourettes#tourette syndrome#transient tic disorder#chronic motor tic disorder#chronic vocal tic disorder#persistent motor tic disorder#persistent vocal tic disorder#poll#polls#disability#neurodivergent
34 notes
·
View notes
Text
House would spend 5 minutes with me, I'd see him use a cane so I'd feel fine complaining that I'm in pain due to my physical disability, then I'd tic and jerk my head or smthn and House would ask me if I just felt that, I'd say yeah I have tourettes. He'd be like oh, diagnosed? and I'd be like no but it's pretty fuckinf obvious isn't it and then he'd put me under 10 tests and diagnose me with 300 invisible tumors syndrome and put me on 18 kinds of treatments all at once and change the diagnosis 5 times and change my treatments double that amount and he'd nearly kill me before concluding that it is, in fact, tourettes and I will not die within a week and I said goodbye to all my loved ones in vain but hey at least he'd officially diagnose what my physical disability is :D
11 notes
·
View notes
Text
#neurodivergent#autism spectrum disorder#autistic#adhd#bipolar disorder#ocd#dyslexia#dysgraphia#dyscalculia#tourette syndrome#anxiety disorder
12 notes
·
View notes
Note
Hey, I saw your post on things that can give you tics and what can’t and I have a few questions.
About 1/2 a year ago I developed tics, and I mean BAD. Happened over the course of a few days and it hit me like a damn semi (mainly because I’m in middle school in a small town and people are assholes, they’ve chilled out by now though).
A few months ago I went in to see a professional psychologist (at least I think that’s what he was, it’s something along the lines of that), when I got my results back I was told that the only things I had were minor ADHD, depression, and severe social anxiety. I was told that literally all of my major issues (unable to stay still, randomly going nonverbal, inability to make eye contact, and the tics) were because of the anxiety and now I’m seeing a bunch of posts like yours and I really don’t know who to believe.
Could you maybe provide me with a few articles so I can figure, like, figure a few things out?
(Also I would like to add that I have 41 tics as of current)
Hope I’m not being too too much of a bother/rude! Have a good day/night/afternoon.
(One more thing, I am writing this on 2 hours of sleep so anything I said that was stupid/grammar mistakes can be blamed on that)
First!
I can't diagnose you, but in my almost (haven't graduated from uni yet) professional opinion would to get a Cunningham blood panel test for PANS/PANDAS/BGE.
The sudden onset paired with periods of mutism (inability to speak) along with tics sounds like the source could be brain inflammation in the very early stages.
If a blood test rules this out, it could just be the classic Tourettic Triad of symptoms of ADHD/OCD/ASD but this would also need to be diagnosed by a neurologist. Reading about tics is not enough to give yourself a diagnosis- it is a neurological disorder and not the same as self diagnosing ADHD or autism. People can DIE from misdiagnosed tics.
Unfortunately, especially those who are AFAB, are likely to be misdiagnosed and have a harder time being diagnosed with a tic disorder or Tourettes than AFAB counterparts.
The fact that you weren't sent to a neurologist to evaluate your symptoms is medical neglect and you deserved better.
Second-
The argument that anxiety can't cause tics really comes from the fact that there are NO studies to prove anxiety causes tics. There are no studies to say they don't, because there is no clinical or scientific evidence that they do in the first place. It's sort of like asking "use scientific studies to prove to me that Santa Claus doesn't exist" .. You can't find those studies because everyone already knows Santa Clause doesn't exist so no one does a study on that in the first place. In this scenario, anxiety tics and Santa Claus are the same thing.
All studies agree that anxiety can worsen EXISTING tics, but none say that anxiety alone c a u s e s tics. Those are two very very different things. Ticcing when anxious does not mean being anxious makes you tic, it means that being anxious worsens and makes noticable tics that you already have.
What I can give resources to though, are genuine Tourettes and Tic Disorder websites:
#tics#actually tourettic#anxiety tics#tics and tourettes#tourettes#tourettes syndrome#pans/pandas#motor tics#vocal tics#tic disorders#tic disorder
19 notes
·
View notes
Note
your post made about detoxes reminds me of someone who posted in this Tourette’s Syndrome facebook group about how their kid has been on a “parasite cleanse” and has had an extreme increase in tics asking if the two could be related. I asked what medicine specifically. It was a naturopath-prescribed treatment where all but one ingredient was documented toxic to children. The child had no indication of parasites but the the naturopath insisted on a parasite cleanse to “cover all bases”.
The treatment might not even have been what caused the increase in tics, it could’ve been coincidental. But the company called cellcore that provides this treatment is so sketchy. The language just sets off so many alarm bells in my head. The attitude is always “well the worst that will happen is no change if it’s bogus” and I’m just exasperated bc whenever I bring up the potential harm especially regarding children I get such pushback.
I know my mom fell into this trap too when I was a kid and it’s such a slippery slope from a “healer” promising they’ll fix you and then all the sudden when it’s not working and there’s so much money down the drain it’s you, the sick child’s fault it’s not working and you aren’t healed because you aren’t “willing to believe” it will work. I don’t know, I was just glad to see a post addressing this in part. ���️

Parents of disabled children are truly some of the fuckin worst. They get it in their heads that they've been slighted by god in some way, so they take it out on the children that are even more reliant on them than your average kid; by neglecting them and ignoring their disability altogether, or pumping them full of every drug known to man and ✨️then some✨️
When reading about their diagnosis is literally Right There. Bare minimum. (Something neither of my parents did as well for any for my diagnoses)
Detoxes and cleanses are so extremely damaging.
7 notes
·
View notes
Text
Book an Appointment for Tourette Syndrome Treatment
Marijuana has potential benefits in treating Tourette Syndrome. Some individuals with Tourette Syndrome have reported reduced tics and improved symptoms with the use of medical marijuana. However, further research is needed to fully understand its effectiveness and safety. It is crucial to consult with a healthcare professional for appropriate guidance and to explore all available treatment options book an appointment for Tourette Syndrome Treatment.
1 note
·
View note
Text
By: Colin Wright
Published: Feb 6, 2024
This morning, The Free Press published a testimony from yet another gender medicine whistleblower, Tamara Pietzke, who described the medical malpractice she witnessed firsthand at a MultiCare hospital in Washington state. Although observing the harsh realities and ethical concerns posed by gender ideology for the past five years has somewhat callused my emotions on this issue, reading Pietzke’s personal account was utterly shocking.
Pietzke shares stories of three patients that led her to question the ethics of “gender-affirming care” for minors expressing distress over their “gender.”
The first case involved a 13-year-old girl with a profoundly troubling history, described by Pietzke as “one of the most extreme and heartbreaking life stories I’ve ever heard.” The girl suffered from a history of severe abuse by her mother, multiple sexual assaults, and was diagnosed with “depression, PTSD, anxiety, intermittent explosive disorder, and autism.” During their initial meeting, the girl showed Pietzke “extremely sadistic and graphic pornographic videos on her phone.” She also explained her tendency to mentally “age regress” to that of a little girl and watch Teletubbies while “sucking on pacifiers.” She had also been expelled from school for threatening to blow it up. Despite all this, the girl’s guardian sought a recommendation letter from Pietzke for the girl to start testosterone treatment.
After expressing her serious concerns about the advisability of medically transitioning this mentally distressed girl, Pietzke’s program manager insisted that her traumatic history should not prevent her from beginning her hormonal transition. Subsequently, the girl was quickly transferred from Pietzke’s care to a new “gender-affirming” therapist.
Another case involved a troubled 16-year-old girl, recently identifying with “they/he” pronouns and seeking testosterone. Three years later, she claimed to have a “xenogender,” identifying as a “wounded male dog.” Pietzke’s colleagues suggested this wasn’t anything to be concerned about.
The last patient, a female who transitioned at 17, sought relief for her Tourette syndrome, depression, anxiety, and gender dysphoria. Despite now having facial hair and a permanently deepened voice, her mental health issues remain.
It is obvious to most of us what an abhorrent medical scandal all of this is. These children have severe mental issues likely resulting from extreme childhood traumas, yet because they have uttered the word “gender,” all of their problems are suddenly attributed to a singular cause—gender dysphoria. And the only proposed solution is to permanently alter their healthy bodies with hormones and surgeries.
While all of this is unequivocally insane, Pietzke recounts a moment that both resonated with and enraged me. After encountering “gender-affirming care” in practice, she grew concerned. Being the diligent healthcare worker that she is, Pietzke sought to expand her knowledge on the subject by researching gender-affirming care online. Like any honest truth-seeker on this topic, she was “horrified” by what she discovered.
She learned that puberty blockers and cross-sex hormones are not FDA-approved for treating gender dysphoria and learned about their numerous side effects. She learned about the absence of good evidence supporting the psychological benefits of hormone treatments. She learned of the link between gender dysphoria and factors such as autism, mental health issues, trauma, and abuse. She learned that gender dysphoria is influenced by social contagion. She also learned about European countries that have either banned or imposed restrictions on medical transitions for minors after conducting systematic reviews of the evidence.
Confronted with these startling findings, Pietzke decided to raise a question during a mandatory online training session on gender-affirming care.
When the leader of the training brought up hormone treatments, I shakily tapped the unmute button on Zoom and asked why 70 to 80 percent of female adolescents diagnosed with gender dysphoria have prior mental health diagnoses. She flashed a look of disgust as she warned me against spreading “misinformation on trans kids.” Soon the chat box started blowing up with comments directed at me. One colleague stated it was not “appropriate to bring politics into this” and another wrote that I was “demonstrating a hostility toward trans folks which is [a] direct violation of the Hippocratic Oath,” and recommended I “seek additional support and information so as not to harm trans clients.” As soon as I closed my laptop, I burst into tears. I care so deeply about my clients that even thinking about this now makes me cry. I couldn’t understand how my colleagues, who are supposed to be my teammates, could be so quick to villainize me. I also wondered if maybe my colleagues were right, and if I had gone insane. [my emphasis]
This resonated deeply with me because it mirrored the treatment I received from most of my former friends, colleagues, and acquaintances when I began to ask very calm and clear questions about the “sex spectrum” and other concepts related to gender ideology that made no sense to me. Before I ever wrote publicly on this topic, I privately tormented over it for nearly two years, very seriously questioning whether I had lost my mind.
I’ve known people who had episodes where they’d burst into fits of rage and shout venomous insults at friends and family. But the next day, when confronted about those outbursts, appear confused and deny any recollection of their actions. Was I now that person? Was I having similar psychotic outbursts followed by amnesia? I asked myself these questions earnestly, because only something like that seemed to have the power to explain the negative treatment I was suddenly receiving from those around me. I couldn’t rule out my own insanity, and Occam’s Razor seemed to suggest that it was much more likely that I was the sole crazy one instead of everyone else.
It took considerable time for me to convince myself I was totally sane, but I thankfully got there.
The most profoundly sinister aspect of this cult ideology, aside from the practice of “gender-affirming care” itself, is its ability to drive even the most rational and principled among us to the mental brink of questioning our own sanity. It will require more whistleblowers like Tamara Pietzke and Jamie Reed to jolt people’s consciences awake, but fortunately, once someone confronts the reality of gender ideology honestly, they cannot turn away.
That’s because we’re the sane ones.
#Colin Wright#gender ideology#queer theory#gender affirming care#gender affirming healthcare#gender affirmation#medical malpractice#medical corruption#medical transition#we're the sane ones#religion is a mental illness
13 notes
·
View notes
Note
Hey there, do you have some cool sources on other types on involuntary movement that are not tics?
Yes, I do! Here is a list of involuntary movements, a simple description, and links to resources on them:
Akathisia -> an inability to remain still
StatPearls article
cleveland clinic article (very good)
Akinesia -> the loss of spontaneous, voluntary muscle movement
StatPearls article (free article)
healthline article
Athetosis -> slow, continuous, involuntary writhing movements commonly affecting arms and hands
healthline article
Chorea -> rapid, chaotic movements that seem to flow from one body part to another
NINDS article
StatPearls article
Dystonia -> sustained or repetitious muscular contractions; often produces abnormal posture
mayo clinic article
NINDS article
StatPearls article
Hemiballismus -> sudden, intermittent, flinging, or ballistic high amplitude movements commonly affecting proximal limb muscles
StatPearls article
Myoclonus → sudden, brief, involuntary muscle twitches
mayo clinic article
NINDS article
StatPearls article
Parkinsonism -> a clinical syndrome characterized by slowness, rigidity, tremor, and postural instability
StatPearls article
parkinson's disease vs parkinsonism
types of parkinsonism (parkinson's UK)
types of parkinsonism (parkinson's foundation)
Stereotypies -> repetitive, rhythmic movements with typical onset in early childhood
stereotypies in adults
medlink article
Tardive Dyskinesia -> uncontrollable and repetitive movements of the tongue, lips, face, trunk, and extremities
webmd article
Tics -> sudden, rapid, recurrent, and nonrhythmic movements or vocalizations
mayo clinic article on tourette syndrome
NINDS article on tourette syndrome
child mind institute article on tics and tourette
Tremor -> rhythmic back-and-forth or oscillating involuntary movements
NINDS article
classification of tremor
(at request I can find Tumblr or blog posts talking about personal experiences with some of these movements)
Basic definitions come from this article: https://www.psychiatrist.com/pcc/effects/drug-induced-abnormal-involuntary-movements-prevalence-and-treatment/
#asks answered#anon asks#involuntary movements#akathisia#akinesia#athetosis#chorea#dystonia#hemiballism#hemiballismus#myoclonus#parkinsonism#stereotypies#tardive dyskinesia#tics#tremor#links
25 notes
·
View notes
Note
I'm so tired of trenders telling me "You're just upset because people aren't suffering in the same way you are, thats a really horrible way to think" when I tell them that you need to have dysphoria to be trans and anyone who doesn't and says they're trans is a trender
I'm not angry that they don't have dysphoria as I'd never wish the pain of having gender dysphoria onto someone, I'm more angry that they are pretending to have dysphoria or pretending to be trans and go on stupid rants about how non dysphoric trans people are valid and when providing "proof and research" its a fake article made by another trender and not someone with scientific proof
I don't get why people only call out others who fake DID, autism, depression, tourettes syndrome or something like that (which of course it is very wrong to fake those things and they definitely deserve to be called out) but then they never call out people who fake being transgender
Because we live in an age now where instead of seeing trans people as transsexuals who alter and change their sex, they think we are just masculinised females and feminised males, their argument relies entirely on “let people do what they want with their bodies” - they see it as body modification like getting tattoos, piercings and cosmetic surgeries. While on one hand, that line of thinking does have its place because bodily autonomy is a fundamental human right. But it’s still repackaged transphobic notions, just saying it in a progressive way. That’s why we have moved away from terms like sex change and transsexual, they want us to accept it’s all just cosmetic and not really altering the sex but hormone replacement literally does alter it on a chemical level hence why you have to accept the common “health risks” of a male or female when you sign the consent form. There isn’t that much diff in terms of treatment for most conditions between males/females unless it’s sexual organ based but there is still some nuance to it. Males have higher risk of thickened blood and heart disease, females have higher risks of blood pressure issues and stroke. These things are important to be mindful of cause the risks change when one takes HRT. The body doesn’t function like their birth sex any longer.
And I’ve had similar things said to me too about oh don’t be upset they’re not suffering like you. Like I’m not, I’m just saying we are not the same and grouping people who lack any of the conditions that make one trans with us is more harmful than anything else.
8 notes
·
View notes