#medical insurance companies suck
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Text
I’ve seen a few posts recently talking about how important it is for us to share our tips for dealing chronic illness with each other, and I’ve realized that as a freakishly avid community enthusiast, I’ve been falling down on the job. So, I present
Wellplacedbanana’s Ridiculously Long List of Tips for All Things Chronic Illness (Curated Over 8+ Years):
Infusion Centers
Headed to an infusion center to get that sweet sweet (expensive as hell) live-saving medication pumped directly into your veins? Here’s what I do.
Bring headphones or earplugs. Most infusion centers try to maintain a semblance of quiet for the patients, but it can get loud fast—beeping IVs, pulse ox monitors, loud families, codes. Some infusion centers do pods of multiple people and some do individual bays, so this can affect noise levels.
Drink lots of water before if you have to get an IV placed. Don’t worry too much about bringing a water bottle because they’ll give you one when you get there. (Of course, if you have something like POTS and need more intense hydration, bring the damn water bottle.) If you’re not hydrated and they can’t find a vein, they’ll call in the ultrasound tech, and they’ll bring the longest IV needle you’ve ever seen. It hurts. Drink water.
Bring a book or your Switch or something else to entertain you, but don’t expect to actually do it. I tried bringing papers to edit the first time because I was like “Oh it’s an hour and a half of uninterrupted free time. I can get so much done!” I was wrong. The nurses are constantly checking in for vitals, the unit can be loud, and I spent the whole time trying not to vomit everywhere. Different infusions will have different side affects. Knowing what yours might be will help you plan for what you want to bring. Knowing how long your infusion will be can also help. Most infusion centers have to keep you 20-45 minutes after your first dose of a new medication to make sure you don’t have an allergic reaction, so factor that into your time too.
If you’re in a pod with other patients who’re friendly and if you feel up to it, don’t be afraid to talk with them. Lots of them are lonely, bored, interested in other people, etc. I met an elderly Thai lady one time who had been there for three hours and would be there for another four AFTER I left. We talked about her husband and her kids, and she listened to me talk about punctuation as style in prose. It made me feel less alone in the medical system and helped distract me from the nausea.
Conversely, if you don’t want to interact with anyone, snap on those headphones and block everything out. The nurses will get your attention if they need you. Don’t worry about staying lucid. Your job is to get the infusion and do what’s best for you.
You can bring snacks if you want, but most units/centers will have something to munch on or can order you something from the cafeteria if you’re at a hospital. Also the medication and the smells in the unit always make me nauseous, so it’s kind of a waste for me to bother pulling together food before I leave. You can always eat before or plan to get something on the way back. Going through a drive thru to get something with protein is my go to.
If possible, schedule your next appointment while you’re there. I have to go every three months, so I schedule the next one while I’m there, and then I never have to make any fucking phone calls. Phone calls are the worst.
My last and most important tip: ask the nurses when you need something. Blankets, water, snacks, pain meds, the lights turned off. If they can’t do it, they’ll tell you. They’d rather have you ask and have to say no, then you be uncomfortable. Don’t suffer if there might be a solution.
Dealing with Shitty Doctors
There are shitty doctors everywhere, in every specialty and every hospital system. It sucks, and you can do your best to avoid them, but most chronically ill patients will have to put up with one at some point. Here are my suggestions:
If they’re refusing to acknowledge one of your symptoms is a problem (won’t order tests, won’t refer you out, won’t ask any questions), tell them it’s affect your Activities of Daily Living. ADLs are one of the ways doctors measure severity of symptoms and quality of life. ADLs are the absolutely essential things you need to do to be a functioning human: eat, shower, get dressed, brush your teeth. ADLs are a trigger word for most doctors. Physical therapists and occupational therapists were created specifically to help patients achieve their ADLs. If you’re having severe joint paint, say it’s affecting you’re ability to shower and dress in the morning. If you have intense fatigue, say you’re too tired all the time to cook food to eat or even brush your teeth before bed. Tell them your symptoms are affecting your quality of life and your ability to function daily. This won’t always work, but it’s a good starting place. (A side note: if you have have to submit an insurance appeal for something that was denied, citing ADLs as a reason to receive the treatment/medical equipment/doctors visit, will often spur them into action. Sometimes, it’ll just make them ask more questions, but questions are better than flat out denial. This was a very helpful tactic when I was trying to get my manual wheelchair approved. I told them I was unable to complete my ADLs and it was affecting my quality of life, and they eventually came around. It’s also important to remember that ADLs are only the most base tasks that you need to live. Driving, working, socializing—those aren’t included in ADLs, and insurance especially will laugh in your face if you try to say you need medical equipment for something like that.)
Lots of doctors, consciously or unconsciously, will judge how you’re actually feeling by your mood in an appointment. I had a pediatric neurologist who couldn’t be convinced that my pain was at an 8 because I would laugh with my mom in the waiting room. Eight months in, I started getting real quiet, not talking, crying when he talked, all that shit, and he was so fucking flummoxed. He was like “what changed?? Are you depressed??” And I had to remind him that I was thirteen with a severe shoulder inure that hurt every time I breathed. Doctors will judge you based on how you look and how you present. It’s horrible, but it’s true. Present to them in the way that represents what they’d expect to see for your symptoms.
Whatever you do, don’t say anything (or send any snappy messages) that might be considered aggressive until you are absolutely, 100% positive you will never ever have to see them again. I’ve had a few doctors that said ridiculously horrible things to me. It’s tempting to send them a message about how shitty they’ve been or how much they’ve hurt you, but it won’t help. Shitty doctors have fragile egos and they don’t like to be challenged. They won’t take this well, and they’ll mark you as attention seeking, emotional, mentally unstable—you name it. When your other doctors call to ask questions about symptoms, etc, they’ll start talking shit, and everything gets complicated. This might sound dramatic to anyone who hasn’t seen it happen, but honestly, the medical system abuses emotion and mental illness to discard patients that aren’t afraid to advocate for themselves, and this is one of the least immoral ways they do it.
Remember that you don’t owe your doctors anything (except basic human decency). If they ask you to do something and you can’t or don’t want to, don’t. My psychiatrist was really fixated on me getting a light box to cure my depression. I did Not want to do that, so I didn’t. Sometimes, your doctors won’t move on to further treatment or tests until you try it, but most of the time you can say, “that’s not something I’m able to do right now. Let’s explore further options,” and they’ll move on.
Remember that learning to advocate for yourself takes years of practice. Just do your best, and try not to blame yourself for the ways you get mistreated. Therapy is the best investment I’ve ever made for this. It’s helped me learn how to advocate and how to process medical trauma.
Medication
For gods sake, take the as needed medication when you have a migraine or if you’re nauseous. Don’t punish yourself.
This might seem like a no brainer, but if you’re traveling and you’re going to take your medication bottles with you, put them in a ziplock bag. They will definitely open in your suitcase, and you’ll have to pick Levothyroxine out of your socks.
If a medication gives you icky side effects, tell your doctor and ask if there’s something that doesn’t do that. For me personally, it’s hard to find medication that works at all, so I often get stuck with things that make me feel like shit. But it doesn’t hurt to ask. Sometimes new medications come out or they dig up old ones.
Some medications come in dissolvable tablets or suppositories. They’re not fun, but if you have trouble swallowing pills, this is a good way to go. Again, communicate with your doctor about these things. I know that there are Scopolamine patches for nausea too. I’ve never used them before, but it might be worth looking into if need easy nausea relief.
All Things Wheelchair
Man, wheelchairs suck, but they’re also amazing. If you find yourself using one, you’ll encounter a steep learning curve.
If you’re not super buff when you first start, it’ll seem impossible to go up even a slight incline. Your arms will get stronger the more you move around, but it might take time. I eventually bit the bullet and started doing personal training. I’m lucky that I can afford it, and I know it’s not an option for everyone, but if you can, find a trainer who won’t saying anything shitty and who’s willing to accommodate. I worked with a queer-owned gym to find someone I was comfortable with. We do upper body strength training, and it gives me a chance to move my body more often. I still can’t go up big hills, but I feel infinitely more mobile. Give yourself time to adjust to the new strain on your body, even if you don’t do training for it. You’ll be sore in the beginning. Ice and heat will be your friends after long days. If your wrists start hurting a lot, you’re not wheeling correctly, and you should ask your doctor for a referral to PT or OT. Oh and your hands will be fucked for the first few weeks. I bought special wheelchair gloves to try to combat this, but it just made it harder for me to maneuver. Now I only use the gloves if it’s cold, if I’m going down hills, or in the rain/snow. (But seriously, if you’re going down steep hills, use traction gloves.)
Learn to pop a wheelie as soon as possible. It’s such a helpful skill. If you get good enough, you’ll be able to get up over single steps and traverse shitty pavement.
If your wheelchair has a cushion, then it has a cushion cover. Wash it.
Time for the grossest part: cutting hair out of your caster wheels. I hate this. I hate it so much. It’s fucking disgusting, but you have to do it. It’ll fuck up your wheels and make it harder to maneuver. Also it’s just gross to have all that nasty hair hanging out by your feet. Get yourself a long pair of thin scissors and cut all that hair out every week or every two weeks. If you don’t have long hair or live with people who have long hair, then you might be able to wait longer. You should also sanitize your hand rims while you’re at it. Hand sanitizer or Clorox wipes are great for this.
You’ll notice that it’s fucking impossible to carry shopping baskets or suitcases if you use a manual chair. Some people try to balance them on their laps or wedge them onto their footplates, but it’s pretty precarious. I got these weird peg things that attach to the frame. You can place a basket or your bag on it and still keep your hands free. Here’s the link for the ones I got, but it depends on your make and model, so do some research and call some different companies before buying anything. Also, make sure to measure the distance between the two sides of your frame to make sure a basket will be able to balance on the two pegs. Your frame might be too wide for this. Mine is, but I bought a special basket to take to the store that’s wide enough to reach across.
Lots of people will offer to push you. Some won’t even offer; they’ll just grab on and take you in whatever direction. It’s insanely invasive and dehumanizing. Don’t be afraid to put on your breaks if someone does this. I can stand and take small steps, so sometime I just get up and stare at them. You can also buy covers for your handles that have spikes so people can’t grab them. I know some wheelchair users who like it when people offer to push them. That’s good too! Take the help if you want it. Just remember to prioritize your safety and comfort. I had a big debate with another disabled person about whether it was infantilizing for someone to offer to hold open the door for us. I’m firmly on the side that they can offer, and I can say no, and they can listen, and then we can both appreciate the moment of shared humanity between us. They did not agree. Disabled people fight and disagree all the time because we’re not all carbon copies of each other. That’s okay! Just be respectful.
Getting a customized manual wheelchair was one of the single most stressful things I had to deal with. Insurance doesn’t like to pay for them because it’s about 3-12k, depending on the specifications and add-ons. But it’s also been the most liberating thing I’ve done since getting my mobility stripped from me. I’m not sure how it works for everyone, but I got a referral from my doctor to a custom wheelchair company. From there, they took measurements, discussed needs, and showed me different models. It’s going to be really really difficult to know what you want the first time. There’s a lot of different brands and customizations, so do your research and talk in depth with whoever’s making your chair. Ultra lite rigid frames are my favorite because they’re usually only 15-40 pounds, and the wheels can come off to make it even lighter. However, rigid frames don’t fold together in the middle like classic manual wheelchairs that you might find at a hospital or get at a rental company. They can be difficult to fit in the backseat of a car or in some trunks, so make sure to measure any cars you ride in regularly. Some people prefer to have tilted wheels so they can turn easier. Some people don’t want anything to do with that. Depending on your mobility and the people in your life, you might choose not to add push handles to your chair. I added some to mine because I often get dizzy, and it’s helpful to have handles in case I need someone to push me out of the crosswalk or into the shade. People who are highly independent and extremely strong might not want push handles because they won’t need help up steep hills. I like my handles a lot; however, my chair back is shorter than a standard wheelchair because it helps increase range of motion when I’m wheeling, so my push handles are lower than normal, and anyone who wants to push me has to hunch a bit to reach. Again, do your research and talk to your rep before making final decisions. Some companies will let you test out the chairs they have on hand to see what you like. It’s important to work with a wheelchair company you really like because you’re literally putting you life in their hands. I’ve had better luck with smaller, locally-owned companies, but you can’t always get referrals there, and not every town has them. Here’s my tip to you: Numotion sucks ass. Avoid them. My branch of Numotion seems to be an outlier; I’ve had really good experiences with them. But most of the time, its impossible to get ahold of anyone, their hours are few and random, and their customer service reps are rude. But! After you’ve completed your order form—gotten measurements and found customizations—they’ll submit it to insurance. This is the tricky part. I went through four appeals, before I got mine approved. Luckily, I had insurance through my mom’s job, and after the last appeal, her company told the insurance that they had to pay for it. This won’t be the case with everyone. Be diligent with your appeals. Have your doctors write specific, clear letters about why you need it, including information about all the customizations and add-ons. It’s likely that they’ll only pay for the base chair, and you’ll have to pay out of pocket for any extra things. Another note: most insurance companies will only pay for a new chair once every five years (if they approve the first one at all), so be sure that the chair you pick out will work for you for at least the next five and a half years.
I had an advisor in college tell me something devastating once: there is no AAA for wheelchairs. I’d broken a caster wheel and gotten stuck on a university sidewalk in 102 degree heat, and she was telling me about her own experiences getting stranded after one of her tires popped. She’s right; if you’re wheelchair breaks, you’re stuck wherever you are without any backup. Carry your phone with you. Tell your friends or family where you’re going before you leave. Familiarize yourself with the wheelchair repairs shops in your area. Sometimes places like bike shops will be able to help you fix smaller things. I always carry an Allen wrench with me in case I need to take a part off. And don’t worry; you’ll find that if something does go wrong, people are far more willing to help than you’d expect. One of the sculpture professors in the art department found me that day and went back to his workshop to get all his tools. He brought me water and sat in the sun while he tried to fix my wheel, and when he couldn’t, he offered to drive me wherever I needed to go. This man was a tenured professor with a prestigious MFA, and he was running late for a party where he was supposed to be handing out awards. You’ll find lots of good people when things inevitably go to shit.
Going along with the last point, your wheelchair will break, and you will have to send it into the shop to get repairs. If you can, invest in a cheap manual chair that you can use in emergencies. If you live with other people, you can buy a transport chair for cheaper, but you’ll need someone around to push you because it won’t have hand rims.
If you’re new to wheelchair use, give yourself space to feel all the emotions. When I first started, I had been using an office chair(!) to get around. My mom would push me from my bed to the bathroom and then back to bed while we waited to get a rental. I was so relieved when I got my own chair that I pushed everything else down. It took months to allow myself to be sad about all the things I couldn’t do anymore and be angry about all the inaccessible infrastructure that America has. Don’t push it down. Talk to a therapist or find people in the community to discuss it with. (If I choose to talk about my frustrations with friends, I always start with “I need to vent right now, and I’m grateful you’re willing to listen to me, but I’m not looking for any solutions to this at the moment,” or “can you give me some suggestions to work around these things that are frustrating me?” This gives my friends insight into what I need, instead of making them guess. It keeps us both from getting frustrated, and I highly suggest it, especially if you or your friends have trouble navigating social situations/expectations.)
Hand Controls
Hand controls are great option for your car if you’re unable to use your feet to drive. I got mine about a year back, but it was tricky and really confusing at first.
First thing you need to know: you can’t get hand controls without a prescription from a specialist. Usually a certain type of occupational therapist. You can look up driving rehab OTs in your area, but there aren’t many of them, and lots of the time you’ll have to drive several hours to see one. There’s usually a long wait list as well. (And of course, a lot of them don’t take insurance.)
If you’re able to find someone who’s certified, they’ll do an intake appointment and assess your physical abilities and needs. Sometimes, they’ll do the assessment and decide you aren’t fit to use hand controls. This can be for a multitude of reasons, including impaired mental cognition and slow reaction time, issues with hand or arm mobility, or there might be a better way to adapt a car for you. Again, it varies greatly on the person, and I’m not an OT, so I don’t know all the ins and outs. If you pass the assessment, and they view you got to drive with hand controls, you’ll be required to do a certain amount of training where you practice using different equipment. Some OTs will know what you need to use right away, and others will have you try different things out to see what fits best. There’s a lot of types of hand controls and a lot of adaptations that can be done to a car, so it really depends on the person. My training was only about 15 hours (plus independent driving practice), but it’ll depend on whether this is your first time ever driving, if you’ve driven without hand controls before, and if you have any other medical issues that might make it hard for you to adapt. Once you’ve completed the training and received your certificate from the OT, they’ll write a prescription to send to a shop that does specialty car adaptation. Kind of like wheelchairs, the shop you go to is very important. Ask your OT if they have any favorites in the area. Insurance never covers this, and some shops will way overcharge you if you’re not careful. My hand controls were about 3k out of pocket, but it was definitely worth it. It would’ve been a lot more to add other adaptations like a lift or a ramp, but sometimes you can buy used accessible vans for cheaper than adding it to your own car. Something to know: you’re usually able to turn your hand controls on and off. So if your friend needs to borrow your car, or you need to let a mechanic test drive it, you can disable to hand controls and allow someone else to use the foot pedals as normal.
Overall, it’s a very long, very expensive process, so plan ahead and be prepared to wait and pay.
Navigating Raising a Kid with Chronic Illnesses
I don’t have any kids, but my mom was my sole caretaker growing up, and I can offer you some of her thoughts. You have to remember that no matter what age your kid is, chronic illness is an impossible thing for them to deal with, and yet they have to deal with it anyways. Sometimes, there’s no good way to comfort a child who’s in 10/10 pain, or who’s about to undergo a life-altering procedure. All you can do is your best. Communicate. Offer support. Give affection. Make your love unconditional. I was a very angry teenager. I was angry with my mom that she couldn’t fix it, and I was angry with my doctors for the way they treated me. There were days where I would yell and sob and refuse to take my meds, and there where days where I would stare at the wall and not respond to anything. It drove my mom up the wall. She’s used to fixing things, and this was one of those things she couldn’t even help. I know she stills holds a lot of guilt for this, but she shouldn’t. She did her best. You’re doing your best too. You can’t fix everything. That being said, here are her suggestions:
Therapy, therapy, therapy. They might hate it, but some day, they’ll thank you. Remember that not every therapist is right for every patient. If your kid wants to switch to a different therapist, let them. It’s better than them sitting and not speaking the whole session.
Lots of kids with developing rare undiagnosed diseases will go through this vicious cycle where they get a new symptom, get sent to a specialist, get dismissed, and then develop a new symptom and start the process all over again. It’s not easy. My mom was a fan of throwing Pity Parties. Every once in a while, when the grind of it all started making us feel hopeless, she’d take me to the store and say, “pick out snacks and drinks. We’re going to throw a pity party, gorge on sugar, watch Lord of the Rings, feel bad for ourselves, and tomorrow, we’ll dust ourselves off and try again.” It helped. It was good to know that sometimes you can let life feel unfair, and it was even better to know that the next day it would be easier to try again.
A lot of being chronically ill as a kid is getting decisions stripped from you and having unexpected negative experiences. My mom would try to do spontaneous things every once in a while to remind me that not all surprises are bad. Instead of driving straight home after school one Friday, she took me to Starbucks without saying anything. After an MRI, she stopped at an art fair and let me pick out a necklace. We would go to the library after I spent the day in the hospital. Sometimes, she’d call my aunts while I was at school to come over and play card games on the weekends. And she was really big on giving me choices in everything. She never made me agree to new (non-lifesaving) treatment. Ever. If she really wanted me to do it, we’d talk it over and come to an agreement that made us both happy. Sick kids are forced into adulthood early; they know how to make calculated, logical decisions when needed. Let them be a part of their own healthcare. (They should also be given the chance to make rash, stupid decisions that have no bearing on their health.)
Keep track of everything. Doctors, meds, ER visits, PT exercises, diets they’ve tried for GI issues, everything about the surgeries they’ve undergone. Some day, you’ll need it. Or your kid will grow up into a chronically ill adult, and they’ll need it.
Talk to their school counselor about getting a 504 or IEP. Even if they’re not struggling. I was a super academically minded kid; I didn’t struggle to understand new concepts or complete homework correctly. But eventually it became hard for me to attend class and finish assignments. Having an IEP saved me. 504s are a lot easier to get (a lot less paperwork, less testing, less pushback from admin), but they’re not legally binding. If you want something concrete and all-encompassing, go for the IEP. IEPs are also really helpful when trying to get accommodations in college. You can also start with a 504 and switch to an IEP later. While we’re on the subject of school: remember that education is important, but school is not the end all be all of your child’s life. What should matter the most to you is that they end up safe and happy. I didn’t graduate high school; I took a proficiency test my junior year and dropped out. It was the best choice I could’ve made at the time, but it was still tough for my mom. I ended up going to college, and now I have a pretty solid job, but every kid will be different. Their mental and physical health is the most important. School is a huge huge huge stressor. Don’t make it harder for them than it already is.
Dating
God dating sucks enough on its own, but adding in chronic illness and disability just makes it a shit show. I don’t have a lot to offer on this other than you shouldn’t settle for anyone who doesn’t respect you, treat you with love and compassion, and accept every part of you for what it is. People will say rude shit. They’ll be nasty, fetishizing, infantilizing, dismissive. Some won’t be able to put up with all the things that come along with being ill. I sound like a broken record, but find a good therapist who can help you voice your needs and expectations clearly. Remember that you never have to go on a date if you don’t want to. Participate as you see fit. Throw it all out if you want.
I don’t have enough time to go into my tips for intimacy/sex and disability, but I’ll give you the highlights.
Communicate. Make it very clear what you’re able to do, what you’re interested in doing, and what you don’t want.
There are lots of ways to have sex. If you’re both having fun, being safe, and engaging consensually, then you’re doing it right. Don’t let abled bodied people tell you the way it should be done. There are lots of accessibility friendly toys to invest in, too.
As weird as it might sound, don’t be afraid to take breaks. Keep water near by. If you have POTS, keep salt or electrolyte tablets on hand. If you have to stop to vomit or go to the bathroom, don’t let it shame you. Go at your own pace and take care of your body.
Misc
Having seizures on a college campus: Most universities have a policy that if you lose consciousness while on campus, they have to call an ambulance. You are not required to ride in the ambulance. You can decline, and the paramedics will make you sign a form before leaving. If you’re still actively having seizures, then they’ll take you anyways, but you probably won’t be in any shape to try to decline. If you’re having seizures regularly, tell your professors. It’ll freak them the fuck out, so warn them ahead of time. It makes the whole thing a lot less awkward when you collapse in the aisle during a lecture. Related to that: communicate with your professors about all your accommodations and emergency health needs. They really honestly appreciate it when you talk to them about this stuff. Even if they have a big class and don’t remember you, it’s good to send them an email and introduce yourself. Hopefully, you’ve also talked to your college’s Disability Resource Center. If not, go do that. Now. (There’s a whole lot of shit that I have to say about campus accessibility and disability resource centers, but I’m not gonna go into it right now.) Also, wear your medical alert bracelet. I know they suck, but it sucks more for someone to be digging through your pants pocket while you’re seizing to try to find your wallet. And keep your emergency contact info pinned up somewhere in your dorm. I used to put mine on the fridge and point it out to my roommates at the beginning of term. It can take a while for RAs to pull yours up, so it’s best to make sure it’s easily accessible.
Remember that you do not function like a normal person. There is no wrong way to solve one of your problems. If you need to put a stool in your bathroom to sit at while you brush your teeth, do it. I got an extra tall stool to sit at while I cook at the stove because my wheelchair is too short. (Cooking in a wheelchair is another thing I could talk about forever.) If you need to wear a sleep mask on the bus because the light makes your migraine worse, do it. People can look at you funny all they want. Like I said, I rolled around my house in an office chair while I waited for a rental wheelchair. What I’m trying to say is find things that work and implement them, even if they’re non traditional.
Here’s what I pack in my bag for an ER visit: headphones, phone charger, book, zofran, Naproxen, water bottle, wallet with cash, socks, and sleep mask to block out the waiting room lights. If I’m expecting to be admitted, then I’ll pack more, but I try to keep it light if it’s just triage and a visit with the ER doctor. Sometimes I’ll stuff a granola bar or some almonds in there too.
My biggest tip for surviving hospital stays is to get out of your room (if possible). Go on walks around the unit. Some hospitals have little courtyards patients can sit in. If you’re in peds, go visit the rec room, even if it’s awkward. Their activities are usually meant for the younger kids, but it can be fun to connect with other people your age, and you’ll thank yourself later when you’re stuck in bed at 3am. Also, tell your friends to come visit you. Not everyone will be able to, but most people are happy to come hang out for an hour or two. It’ll help; I promise.
Clean your room every few weeks. Dear god, clean your room. I have trouble with executive functioning and finding energy to do housekeeping type stuff, but I get more depressed when my room is gross. So clean your room. Especially if you have hypersomnia/sleep excessively.
Don’t force yourself to use a pill organizer. I know everyone says it makes it easier, but I get overwhelmed when I have to refill it, and then I just don’t end up taking my meds. If it doesn’t work for you, don’t do it. If it does, then do it!
Don’t buy the self help books your therapist recommends unless you’re actually interested in reading them. It’ll just sit on your shelf and make you feel guilty for not being good enough.
Mental illness is tightly bound to physical illness. Try to be an active listener in your body. Sometimes, when I’ve been feeling really nauseous, my PSTD symptoms will get triggered over nothing, and it’ll frustrate the fuck out of me because it seems like it’s happening over nothing. I try to track when my emotional state is worse to see if it’s correlated to my physical symptoms. This helps curb the frustration and guilt. Sometimes it makes me dissociate more. It’s a balancing act. Just do your best.
Hobbies are so so so important. Make sure to give yourself time to work on them! And there are a million ways to adapt the activities you love if you’re having trouble, so don’t afraid to do some research. I know they have crochet hook grips for people with arthritis or loose grips, and there are super intense magnifying glasses for people who like to cross stitch and are having trouble seeing the tiny ass holes. I have a color blind friend who sends us pictures of paint to see if it’s the shade he wants. Very occasionally, you’ll come to the conclusion that there’s a hobby you can’t adapt. Let yourself be sad. I can’t hike anymore and it sucks. I can’t go tide-pooling either, and its not like if I just work really hard I’ll be able to do it some day. Life is shit, and sometimes you have to let things go. Be angry, be sad, tell people to fuck off if they try to turn you into inspiration porn, but also remember that there are lots of other cool things out there to try.
Going along with the hobby thing: take the time to learn ASL if you’re having trouble with your hearing or if you often go nonverbal. One of my friends had to get hearing aids last year, and we offered to learn with them, but they were hesitant because it feels like a non necessity to them. Something selfish that would take up all our time. If you think it’ll help, you should grant yourself the time to learn. Capitalism makes us think that we shouldn’t engage in activities unless we gain money or power from them, but that mindset will kill you. Your life will be infinitely easier if you learn ASL online with your partner or friends or siblings.
Look up Spoon Theory. It’s not a helpful metaphor for everyone, but most people in the community talk about it, so it’s good to be familiar with it.
Don’t be afraid to go out and find community! Find support groups, look up wheelchair sports if you’re into getting sweaty, brave the awkwardness of starting conversations with other patients in the clinic. I’m wholly and completely of the idea that humans are innately good. There are lots of interesting chronically ill/disabled people who’re looking for connection. Insurance companies and other medical entities rely on us feeling isolated, alone, and uniformed to continue making money and hold power. It’s important that we share with and support each other.
I know a lot of this is basic stuff, but it’s helpful to have reminders, and if you’re new to the whole song and dance, then it’s nice to get a sneak peak. There are a million things I didn’t get to, but this was what was on the top of my brain.
Also, I’m not the collective voice of every chronically ill person in the world. My experiences are not yours and they’re not everyone else’s. What works for me, might not work for you. Be kind.
#thanks to @thenarrativefoil for reminding me that we need to share with each other!!#if you have any suggestions for dealing with gastroparesis please hmu#I’m still waiting for my gastric emptying scan but I’d like to try out some of y’all’s tips#hopefully some of this is helpful to someone#chronic illness#chronic pain#disability#seizures#nausea#wheelchair user#ptsd#mental health#hand controls#medical insurance companies suck#therapy#so much talk of therapy#spoonie#if this is helpful to anyone I’ll make another
122 notes
·
View notes
Text
To everyone curious about fic updates…. I promise they will be updated soon. Back in December I had issues with multiple client’s health insurance and became extremely burnt out and overwhelmed by the process of fighting with insurance companies (fuck united most of all, all my homies hate united). It triggered a chronic illness flare so bad that all I’ve been able to do is go to work and sleep. I’ve written when I had energy but that hasn’t been much so it’s been like trudging through the mud to do much of anything.
I’ve had tonsillitis on and off for almost 2 months straight folks… and my own insurance is dicking me around about getting properly treated for it. Plus getting a tonsillectomy in your 30s fucking sucks so I’ve just been living with it. America is a dumpster fire. Hopefully there’s something for both Play Dead and Ego Death by the weekend. Much love and gratitude to everyone who’s been supporting my writing 💜
#personal update#fic writing#fan fic writing#fan fiction#ego death fic#play dead fic#trust and believe that mental health and medical professionals hate insurance companies just as much as patients… they suck
34 notes
·
View notes
Text
Nothing takes the wind out of your sails like FINALLY getting an ADHD diagnosis after literal decades of fighting for it, then having insurance deny the meds that might finally give me some sanity and stability.
Hey insurance providers: fuck you.

2 notes
·
View notes
Text
yes, doctors suck, but also "the medical ethics and patient interaction training doctors receive reinforces ableism" and "the hyper competitive medical school application process roots out the poor, the disabled, and those who would diversify the field" and "anti-establishment sentiment gets applications rejected and promotions requests denied, weeding out the doctors on our side" and "the gruesome nature of the job and the complete lack of mental health support for medical practitioners breeds apathy towards patients" and "insurance companies often define treatment solely on a cost-analysis basis" and "doctors take on such overwhelming student loan debt they have no choice but to pursue high paying jobs at the expense of their morals" are all also true
none of this absolves doctors of the truly horrendous things they say and do to patients, but it's important to acknowledge that rather than every doctor being coincidentally a bad person, there is something specific about this field and career path that gives rise to such high prevalence of ableist attitudes
and I WILL elaborate happily
#theres so much that contributes to this#and its such a traditional field that any change takes ten years to take effect even when its not as controversial as disability rights#ive no lost love for doctors as a whole#but the deeper causes here need to be examined to understand how this problem manifested and what can be done to fix it#disability#chronic illness#ableism#premed#medicine#salt baby talks
22K notes
·
View notes
Text
I'm sharing this across all my media platforms. Please, even if you don't donate, help get her story out. I didn't mention this in the story but our employer isn't working with her to give her the benefits they offer such as short and long term disability and sick pay. In fact, they denied her short term disability.
#help#charity#fundraising#medical debt#insurance companies can go suck dicks#we need universal Healthcare#donatetoday#donations#help a family
0 notes
Text
Sometimes people tell me I'm a good person. I'm not a good person by nature, or by default. I'm a good person because I've decided that it's important to me to act like one, on a daily basis, forever.
My actual nature is that I want power. I want power and I want my life to be easy and I want other people to be forced to be nice to me even if they hate me. I want other people to have to suck up to me, I want to watch people who I know hate me suffer through the indignity of having to suck up to me. I want to hurt people who hurt me. I want all of these things in the same exact deeply recognizable way that a gorilla or a chimpanzee does. I watch those documentaries and I recognize myself, intimately. The fact that I can behave like a good person in spite of that has taken me a long time and a lot of effort to achieve.
What you feel isn't as important for your "goodness" as what you do. And you get good at what you practice. So practice your skills at being polite, pleasant, kind. Practice gently interrupting negative behaviors--whether that's someone's negative behaviors directed towards themselves, or directed towards someone else. The idea that we have to be inherently without sin is such Christian garbage. It's psychological gibberish. We want things! We want everything! That is normal and human and the key is not acting on every bad feeling you have.
I have taken my insatiable desire for power and to manipulate people and I have used it for good. I have learned how to manipulate people into coming to the doctor and taking their blood pressure medication and being honest about their recreational substance use. I have taken my psychology education and I have used it to craft a persona that makes people feel at ease. I go home at the end of the day exhausted, because maintaining a persona for ten hours straight is exhausting, but I do it happy, because I manipulated the people I work with into feeling better and having brighter days. I manipulated my patients into feeling good about their achievements and recognizing where we need to do things differently.
The hard part is that when the mask slips, people find it not just off-putting but deeply upsetting. When I explain things like "I have thought very carefully about how I would conduct a career in domestic terrorism because I would genuinely like to bomb the headquarters of most American insurance companies, but I don't see a way to do it without getting caught and either killed or spending the rest of my life in prison, and at the moment I consider that an unacceptable outcome," people go from "ha ha! my wacky colleague" to "Jesus Christ, I didn't realize there was something actually wrong with you."
Anyway, don't make your kids read the extended works on Machiavelli at twelve, my dad thought he was helping me but all he accomplished was making me sad I'll never be a king.
2K notes
·
View notes
Text
Maybe it isn't that I actually hate medical professionals? They just suck and are weird sometimes, and a lot of them shouldn't be practicing, but I don't hate them as a group, like, personally.
What I hate is their ability to make my life harder in ways that are often completely opaque to me, and a lot of the crap things they do are not really possible to challenge. And I hate the fact that holding them responsible fort dogshit behavior in any way that will actually benefit me is almost always impossible.
And I also hate the fact that they have to do stupid things sometimes because that's how the system is set up, and those things sometimes mean patients actually get harmed. They aren't fond of that part either! They don't want the system to be the way it is! But they don't have a choice, so sometimes people like me get forced by bureaucracy into doing things that are re-traumatizing. And I can't imagine that feels good for them at all, knowing that their patients are sometimes only "consenting" because that bureaucracy will not let them be helped in any other way. Which isn't consent at all. I imagine that must be pretty traumatizing for them, too, sometimes.
If it were easier to actually access medical care without tremendous delays in this country right now I would have much less trouble finding providers who are good at what they do and are not horrible people, and who have clinic staff who can do their fucking job.
Oh and I also don't appreciate how evasive and unwilling to commit they are out of fear of being held to an answer that turns out to be inaccurate, but I can't make an informed decision about my own care unless they give me at least some information about probabilities and trajectories and typicalities. Genuinely, how the fuck am I supposed to navigate that shit. I get that some patients are really fucking difficult, but I should be able to get a special stamp on my file or something that says I understand that sometimes medicine isn't an exact science and the best answers that my doctors can give may not always prove to be accurate in the long term. I know they don't like being in that situation either.
A lot of medical professionals are fucking assholes, and unfortunately the ones who are not are still hamstrung by a system set up to actively prevent people from getting care.
I miss my old doctor. He gave no shits about anything that wasn't the patient. He prescribed scheduled meds based on what the patient needed and not based on fear of consequences potentially being imposed on him by the punitive patient-hostile drugs-are-bad moral panic machine developed to force suffering people into buying more dangerous drugs off the street in order to prevent far fewer people from maybe getting high off of drugs that at least weren't laced with lethal substances. (The purpose of a system is what it does.) Did he get sanctioned and become locally unhireable? Unfortunately yes he did. Does he now provide concierge care to rich people? Yes he does. He found a way to make it work, God bless him.
Everything about the medical system in this country is fucked. Hospitals, doctors, nurses, pharmacies, pharmacists, pharmacy techs, phlebotomists, clinic administrative staff, insurance companies, medical schools and schooling, licensing boards, drug advertising to both providers and patients, pharmaceutical reps, researchers, research, publishing, medical trials, pharmaceutical companies, manufacturers and distributors, medical equipment, charting software, billing and billing codes, diagnostic criteria, charity and low income services, accessible transportation, home care, the lack of independent individual patient advocates, dietitians and nutritionists, access to physical and occupational therapy and physical and occupational therapists, the massive bigotry of every kind rampant in every corner of the medical field, social work, senior care and assisted living, deprioritization of informed consent and harm reduction, disability applications, inaccessibility of medical records, especially psychiatric notes which are specifically allowed to be withheld from patients, lack of continuity of care for disadvantaged people, care that is equitably accessible to disabled people, telemedicine, patient portals, phone systems, clinic hours, every single aspect of inpatient and outpatient psychiatry, facility security, all sorts of things going on with therapists who are nevertheless probably the least malicious group of people in this entire charade, aaaaaand patients themselves.
Also hospital toilets that are too tall and make it literally physically impossible for me to poop while I'm there waiting for somebody to come out of surgery. I just needed to take a crap, guys. You didn't need to make the toilets so tall that my feet didn't even touch the floor. It is very clean but there is no shitting for short people at St Francis.
348 notes
·
View notes
Text
Okay, lets go through this apparent list of positives that Biden is in favor of.
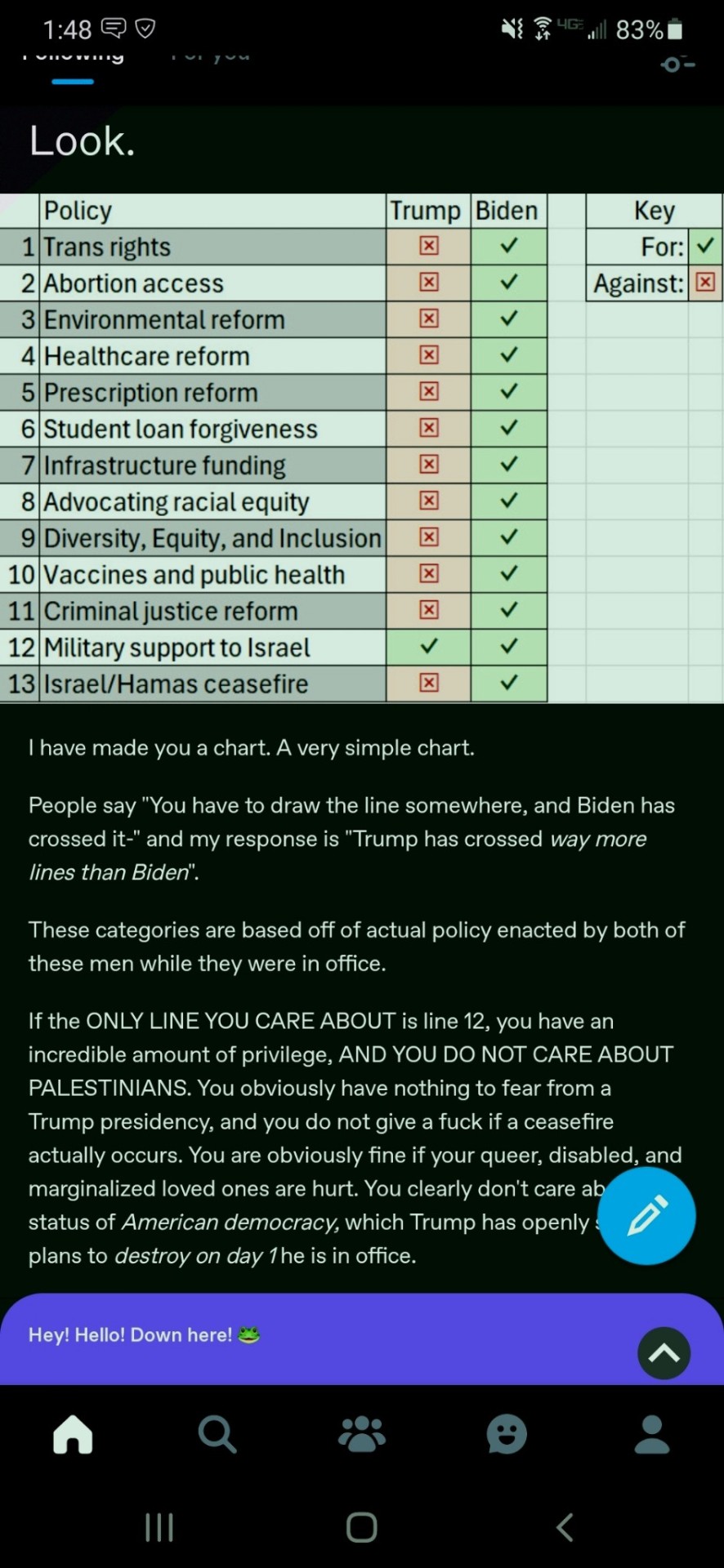
Trans Rights: There have been multiple laws within states to fully close off especially trans kids rights to medical treatments and more. This is extremely current. Biden puts in minimal effort to look like he's doing anything at all for trans and queer rights, and there haven't really been any efforts aside from doing one or two proposals that immediately get shot down, and he's more than okay with that, hence why there's no longer really any push for this shit still. If you're trans, you can't piss in Utah without the risk of getting a fine right now. Even though these are state laws, the fact that there's been nearly zero effort federally to address this besides the title IX rule, speaks a lot about priorities in this area.
Abortion Access: Are we just forgetting the whole Roe V Wade getting overturned thing that happened in 2022? Are you really trying to say that this is good for abortion access? Abortion access has gotten actively worse.
Environmental Reform: Biden has endorsed extreme oil drilling projects and in general oil companies still love him! Not to mention the train crashes which we'll get to later.
Healthcare Reform: Covid-19 is still around and is sadly predicted to stay around for a long while. Healthcare is still private and a competitive field in the US and that causes major issues as well. If you look this up, you see articles titled along the lines of "Biden has lowered the cost of insurance" and meanwhile it just dropped in 2020 once during the pandemic but has been growing in cost.
Prescription Reform: Reading into this, not much has changed, which isn't surprising under genocide Joe. Drugs in the US are still higher than anywhere else in the world, and with healthcare issues still abundant, this is still a big issue.
Student Loan Forgiveness: Student debt is still extremely high in the US, and while Biden has rolled out some plans for forgiveness, it's a fraction of the debt, and he primarily uses the whole thing to win over swing states. This is a dangling carrot that provides very little overall.
Infrastructure Funding: Train crashes from 2020-present, worldwide, but notice the amount of US crashes! Neat! Quite literally just look up train crashes in the US during his presidency, there's too many to link here. It is also important to remember that Biden signed a bill to prevent rail strikes, preventing a lot of pressure to the government and the economy, which would have been a GOOD THING. Seriously, this guy has fucked up our environment and our rights in multiple ways.
Advocating Racial Equity: Structural racism within the US is still a huge problem, Biden hasn't addressed much. Also people are still in cages on the Mexico/US border (Which has been maintained by every president in office since it was established), with a very recent crackdown on the border.
Diversity, Equity, and Inclusion: Just. Look at the racial equity and trans rights sections above. Biden does the bare minimum, loves focusing on swing states, and all around uses the ol' carrot on a stick.
Vaccines and Public Health: Once again look above at sections on healthcare, abortion access, and prescription reform. Its bad. Remember how Covid-19 vaccines aren't being continued for free?
Criminal Justice Reform: This is just structural slavery still. Disproportionate amounts of black people are incarcerated, police are still heavily funded under Biden. He does not care about reforming the justice system, he even supports cops breaking up campus protests! Cool!
Military Support for Israel: Yup! Both sides suck! Biden has a very long history of sure hating Arabic countries though! He's done nothing but ship weapons and participate in the genocide of Palestinian people. Would Trump also do this? Yes. Does this mean this is an issue you should just drop and call a non-issue? No, what the hell are you talking about.
Israel/Hamas Ceasefire: Netanyahu has no plans to accept any actual ceasefire, yet Biden still provides weapons and support. Wow! That sure is weird? I wonder if Biden really cares about a ceasefire or how he just looks publicly.
Biden is not a good president, much less a good human being. You provided such a flimsy chart with zero resources or support behind you, and it just feels like people are just making shit up at this point. Get your heads out of the liberal cesspool you grew up in.
#This one got long#Please feel free to correct me especially in regards to anything concerning foreign policies @ people not from the US#As someone who lives here in the US I don't have the lived experiences that come with this shit nation constantly fucking up the globe#Liberals are unable to imagine a better world#Stop calling Biden some kind of amazing president. He's funding a genocide and has effectively been asleep at best during his time#And been doing much worse while he's actually been doing anything#He is not some sleepy old dude he's a war criminal and a person who has enacted great harm towards many many people
176 notes
·
View notes
Text
shout out to people who know there’s something wrong but can’t convince a doctor to actually look into it instead of just treating the symptoms and hoping it goes away
shout out to people who have multiple conditions that interact in unexpected ways and/or get mistaken for one condition
shout out to people who have to constantly convince doctors that just because a certain test came back normal doesn’t mean nothing’s wrong
shout out to people who don’t have access to a doctor that specializes in a field related to their condition and have to make do with whoever is available
shout out to people who got called a hypochondriac for years before finally finding a doctor who would listen and take them seriously
shout out to people who got told for so long that they were faking it for attention that they started to actually believe it despite knowing deep in their hearts something was wrong
shout out to people who are scared to speak up about health problems they’re having because of the stigma surrounding them
shout out to people who never talk about their pain and constantly mask it out of fear of being a burden to others
shout out to people who do talk about their pain and get told to just suck it up
shout out to people who have to fight their insurance companies tooth and nail every time they receive even the most basic medical procedures, and start an all-out war with those companies to get lifesaving treatments
shout out to all the people disenfranchised by the medical system. I love you all.
395 notes
·
View notes
Text
A Guide for Writing Ed's Top Surgery!
I'm getting my top surgery on July 3 (whoo!!!) and I'm using this as an opportunity to gather info for fic purposes. I love writing Ed as a trans man, and I love everyone else who writes and draws him as trans, so I wanted to share the notes I'm taking to help others who want to draw or write Ed's top surgery experiences! I'll update this as we go in sections (pre-op, the surgery itself, and initial recovery).
This is all just my experience with getting a double-incision with free nipple grafts surgery, and it's from a US perspective. Your mileage may vary and this definitely isn't meant as a medical guide. If you're having your own top surgery listen to your surgeon, not me.
Pre-op guide below the cut!
In the months before his surgery:
Getting insurance approval for top surgery in the US, depending on where you live, can be incredibly frustrating, dehumanizing, and painful. Ed will need at least one letter from a therapist or other mental health provider, and he'll probably feel very frustrated about being treated like a child who is unable to make his own medical decisions. I had several insurance denials, needed to switch insurance companies (currently having to settle for one that's more expensive in every other way but will at least approve this surgery), and needed three (fucking 3!!) letters from mental health professionals to get my approval. Hard to overstate how much it sucked and how much it makes you feel like the people writing state and insurance laws see you as a stupid child. Ed will very likely have Lingering Issues about this experience.
Ed will need an initial consultation to confirm he's a good candidate for surgery. Mine was quick and easy!
Once he gets his approval, or once he decides to pay out-of-pocket, he'll get his surgery date! Depending on his clinic, this could be years away or it could be as soon as a couple months out, so anything is realistic for your story. You could lean into the joy of a date that's sooner than he'd expected or he could be frustrated by the whole process grinding to a halt.
His pre-op appointment:
The pre-op appointment is when Ed will meet his surgeon and get the details for his surgery date. Mine was almost two weeks before my surgery. He'll also receive packets of information and his post-op check-up dates. If he smokes, he should be tobacco-free by this date.
This is when Ed and Stede will be able to ask any last-minute questions. Ed can ask here if the surgeon will be willing to give him heart-shaped nipples, but they'll probably say no
This appointment is also when Ed will be struck by the reality of having post-operative drains and not being able to shower for a week. This will be deeply upsetting for him
Ed will probably be very nervous for this appointment (what if something goes wrong and he can't get his surgery?) but he'll be relieved and comforted by the whole experience. The mood in the whole plastic surgery center, for me, was downright fucking jubilant, all the nurses who saw my name on the chart were congratulating me and telling me how happy they were for me! This WILL make Ed cry
The week before his surgery:
It begins to sink in that Ed is about to have major surgery. He's excited, of course, but he'll be a little nervous too! Stede will need to give him lots of cuddles and promise to take good care of him
They'll need to make lots of Ed's favorite comfort foods to freeze so he has something to eat when he can't raise his arms well enough to cook
Ed should practice doing things without lifting his arms above his shoulders. He'll have a great time stomping around and pretending to be a dinosaur
He'll want to prepare a selection of comfy clothes he can wear without raising his arms. Stede's robes will be perfect
The biggest struggle for Ed during his recovery will be the boredom. Stede should help him build up a stock of video games, books, Lego sets, sketchbooks, and model building kits to keep his hands and brain busy!
They should prepare Ed's sickbed. He might be more comfortable sleeping upright on the couch or in an armchair propped up by pillows. He'll have to see how he feels after surgery and what positions are most comfortable, so getting both the couch and their bed ready is a good idea!
At some hospitals, including mine, you won't know what time to arrive at the hospital for your surgery until the day before, when they'll call you to let you know (they do this based on surgery room flow to ensure you arrive at the right time). Ed will find this stressful; Stede will HATE it.
Ed may need to shower with a special antiseptic skin wash the night before and the morning of his surgery. He will not enjoy having to get up at the asscrack of dawn to shower
The night before Ed's surgery, he and Stede should pack bags, just in case. Top surgery is an outpatient procedure, but just in case anything goes wrong and Ed has to stay overnight, it's good to be prepared. A change of comfy clothes, a book, and Ed's Nintendo Switch are good things to pack. Ed will also love taking a stuffed animal to keep him company after Stede can't go any further with him (and he can use the plushie to cushion the seatbelt on the car ride home).
Ed's super excited and everything's set for him! Good luck, Ed! 🥳
53 notes
·
View notes
Note
how do you feel about all the anti doctor rhetoric on tumblr and beyond? i feel like it comes from a place of misunderstanding and hurt over the failing healthcare system :/
I’m perhaps not the best person to answer this, because much of tumblr is American and I am not (I am from a country with fully public healthcare, and work as a doctor in Australia where there’s a mix of public/private care but I’ve only ever worked in the public system).
However, I think it’s multi factorial, with some causes being justified and others not so much.
A lot of anger towards the health system is very much justifiable - particularly in the US where health care is precarious and so expensive even if you have insurance coverage.
But that anger is wrongly directed at doctors, and generally the lowest paid doctors - family medicine, paediatrics, and emergency - because we’re one of the more visible facets of the system. People think we are very wealthy, but the bulk of the money seems to go to insurance companies and hospital admin, not to us. In fact, hospital admin in every country bend over backwards to avoid paying doctors for their actual labour.
(Once, in response to a patient’s parent asking me if they had to pay for their clinic appointment, i accidentally responded “I don’t know, I don’t think so. They don’t pay me for this.” by which i meant that i don’t get paid any extra for clinics but i did have to clarify that they were, like, paying me for the day overall. And also it was a public hospital so I was able to confirm after that no, they didn’t have to pay.)
Most people just don’t understand the way insurance works, or how little of that money goes to doctors. What I really wish I could broadcast to everyone is how little residents/registrars make. I made about 50k USD equivalent as an intern - which is nothing to sneeze at but I had just completed 8 years of university and was over $200,000 in debt from med school. A cop in my city makes about $75k USD, which is 25k USD (about 40k AUD) MORE per year than an intern doctor does.
Another reason for a lot of anti-doctor sentiment is that people really have been let down by the medical system. It can be complex, hard to navigate, and there are some legitimately bad doctors out there. There are also a lot of nurse practitioners replacing doctors in many roles, and while they’re a great resource, they just don’t get the same amount of training.
I believe that there are people who have been dismissed, particularly women, fat people, and trans people. By older doctors especially, and for women by male doctors, but also by younger and female doctors at times. This is mainly because as much as no one wishes to acknowledge it, doctors are human. And some humans suck ass. It takes effort to overcome one’s own biases but we are explicitly taught to work on that and to not let any biases we may hold impact our patients.
The common ideas and reasons given for hating doctors that “POTS isn’t taught in med school” or “med schools don’t teach about endometriosis” are completely untrue for most schools these days, though. I started med nearly a decade ago (yikes!) and we were taught about both these things! It’s not the 1980s anymore! “we never really researched the female body” WAS true but we are very much catching up on that now! There is some great work on endometriosis in particular being done in BC. However, trust in the medical system was justifiably lost (for these and many other reasons) and it will take a long time to gain that back.
There is a third factor, though, which i think is fully unjustified, and that’s the (often right wing led but adopted by the left as well) push to delegitimize academics. Covid really lit a fire under this one, and since then there’s been so much distrust towards science and scientists because we’re the “elite” in our “ivory towers” (so typed from my scrubby little city apartment). It’s often pushed by politicians who stand to gain votes, or influencers who want to sell you spirulina flakes or whatever the current trend is. There’s an intentional moving behind pushing this, but there are a few factors for people believing it.
It’s partially anti-intellectualism, because no one likes thinking that someone else might possibly be more educated on a subject. I do also think there is an element of sexism and racism - medicine and science are becoming lower paid and less trusted as more women and POC gain entry.
There’s also the fact that people don’t want to hear that sometimes things that are good for them aren’t fun. No one wants to get a vaccine because that hurts. Its much more pleasant to believe that getting a massage and drinking raw milk and rubbing lavender oil into everything is the TRUE cure, that doctors don’t want you to know about, because believing that lets you indulge in things that feel good while believing you’re doing good - which people love, even when it’s false.
This was much longer than I wanted it to be and doesn’t cover all the reasons! But this covers a few factors.
16 notes
·
View notes
Text
Andrew Perez at Rolling Stone:
EARLIER THIS WEEK, two Democratic senators announced they have requested a criminal investigation into Supreme Court Justice Clarence Thomas — regarding, in part, a loan for a luxury RV provided by a longtime executive at UnitedHealth Group, one of America’s largest health insurers. Thomas apparently recused himself in at least two cases involving UnitedHealth when the loan was active, according to a Rolling Stone review. Yet, he separately chose to participate in another health insurance case and authored the court’s unanimous opinion in 2004. The ruling broadly benefited the industry — shielding employer-sponsored health insurers from damages if they refuse to cover certain services and patients are harmed. Thomas’ advice to patients facing such denials? Pull out your checkbook.
While UnitedHealth was not a party to the case, the company belonged to two trade associations that filed a brief urging the Supreme Court to side with the insurers. “As we saw so starkly this term, Supreme Court decisions can have sweeping collateral implications: If the court rules in favor of one insurance giant, for instance, it tends to be a boon for all the other insurance giants, too,” says Alex Aronson, executive director at the judicial reform group Court Accountability. “That was the case here, and it’s a perfect example of why justices shouldn’t accept gifts — especially secret ones — from industry titans whose interests are implicated, whether directly or indirectly, by their rulings.” The public had no way of knowing about Thomas’ RV loan at the time of the decision: The loan was only exposed by The New York Times last year. Senate Democrats investigating Thomas believe that much or all of the loan, for a $267,230 motor coach, was ultimately forgiven. Sens. Sheldon Whitehouse (D-R.I.) and Ron Wyden (D-Ore.) recently requested the Justice Department investigate whether Thomas reported the forgiven portion of the loan on his tax filings, after he failed to disclose it in ethics forms.
Meanwhile, Thomas’ health insurance opinion has had wide-ranging, long-lasting ramifications, according to Mark DeBofsky, an employee benefits lawyer and former law professor. “It hasn’t been rectified. The repercussions continue,” DeBofsky tells Rolling Stone. “People who are in dire need of specific medical care, and [their] insurance company turns around and says, ‘That care is not medically necessary,’ and there’s an adverse outcome as a result of the denial of the treatment, or hospitalization, or service — there’s no recompense for what could have been an unnecessary death or serious injury.” Since last year, the Supreme Court has faced an unprecedented ethics crisis, with much of the focus aimed squarely at Thomas. ProPublica reported that Thomas received and failed to disclose two decades worth of luxury gifts from a conservative billionaire, Harlan Crow, who allegedly provided free private jet and superyacht trips to Thomas and his wife; bought a house from Thomas and allowed the justice’s elderly mother to live there for free; and paid for at least two years of boarding school tuition for Thomas’ grandnephew.
[...] Federal law requires Supreme Court justices to recuse themselves in any case where their “impartiality might reasonably be questioned.” The justices decide for themselves when such a move is necessary — and when they do withdraw from a case, they rarely say why. Thomas does not appear to have explained his decision to withdraw from the two matters that directly involved UnitedHealth. Thomas did not take similar steps in Aetna Health Inc. v. Davila, a case that broadly affected the health insurance industry. He instead authored the court’s opinion, which expanded insurers’ favorite tool for limiting liability: ERISA. Congress passed the Employee Retirement Income Security Act, commonly known as ERISA, in 1974 to protect employee benefits. The law is relatively vague when it comes to “welfare benefits,” and contains a broad preemption clause. The courts have filled in the blanks — including in the Aetna Health case — with distressing results for patients. Half of Americans have employer-sponsored health insurance coverage; nearly all of these plans are governed by ERISA.
Rolling Stone exposes how SCOTUS Justice Clarence Thomas received a $267K RV from a health insurance executive.
#Clarence Thomas#SCOTUS Ethics Crisis#SCOTUS#Ethics#Ron Wyden#Sheldon Whitehouse#UnitedHealth Group#Health Insurance#Employee Retirement Income Security Act#Harlan Crow
21 notes
·
View notes
Text
i think the way that people talk about therapy and therapists on this website is alarming. yes, a lot of therapists are bad and the healthcare system in the united states sucks. but therapy as a practice isn't designed to make you "normal". it's designed to increase autonomy and coping strategies. therapists might refer you or give you ideas to other places to go to change your material conditions but the reason therapists don't do that isn't because they hate you. it's because it's an ethical violation that creates transference and codependence. it's just not what talk therapy is for. and yeah, therapists are obligated to report you if you express suicidality. and a lot of therapists won't even do that unless they're slamming the emergency button, basically. my therapist and i agreed, together, to keep autism out of my medical record and code only my general anxiety diagnosis so i wouldn't be opened up to medical discrimination. i have a therapist friend who codes everybody as having adjustment disorder for the same reason. even in my classes they say the DSM is not law and there's always nuance. therapists are also people, often deeply empathetic people, who are also trying to work around a fucked system of insurance companies and for-profit care and while i understand ire towards them especially for people who've had negative experiences, i think it's misplaced
12 notes
·
View notes
Text
lrb i've also had that experience with insurance companies denying my psych meds because it wasn't their preferred medication. insurance denied my viibryd bc they didn't want to pay for it, so my psych and i had to come up with a list of other meds i've tried that didn't work. obvs it's not as dire as meds for seizures, but without my viibryd i am either so hypomanic i can't focus on anything or i'm actively suicidal.
i no longer have insurance. i fall into a gap where i "make too much money" to qualify for medicaid, but i don't make enough to pay for rent + groceries + the car payment + the car insurance + health insurance from the "affordable" healthcare marketplace. but when i was insured, i was regularly encouraged to fudge things when it came to getting what i needed from the insurance company.
it fucking sucks here, man.
9 notes
·
View notes
Note
hi! anon who asked about an autism dx last time. i have update that the doc enabled accomodations services which alleviates some stress, but she discussed the next steps being 1) to fork out money that I don't have to get a dx or 2) go on a waiting list to get 'officially' assessed. i was wondering from a what the pros and cons of getting ASD on your record are if you don't mind me asking? in how drs treat you and workplaces? ty for your advice and yr overflowing patience w the asks you get!!
to me, the only pro would be if you needed an accommodation, or set of accommodations, and had no other way to get them (no other applicable diagnoses, no way to leverage needs in a job contract etc). under social conditions of ever-increasing ableism, even any accommodations you manage to argue for with a formal dx will be a pyrrhic victory at best, because they'll be contingent upon the institution recognizing you as "special needs" and therefore possibly costly/inconvenient/less important than your (seemingly-)abled colleagues.
my autism dx allowed me to live in the dorms in college (on a quiet floor, in a single room, as outlined in my accoms. plan) and manage major sensory triggers in public spaces (quizzes and tests in a separate room; ability to leave the classroom for extended periods when sensorily overwhelmed). it was what legitimized me to my college's disability services, even as my entire constellation of dx's led them to demand "are you sure you're ready to live here? to be a student? to be in higher education? do you need [insert paternalistic suggestion here]?". talk to any disabled student/worker and they'll tell you that disability services/HR suck major ass. they're there to protect the company, and their bureaucracy is designed to break you down so you'll cost them less money. the purpose of an official dx in these contexts is to get a foot in the terrible, heavy, often-useless door, and nothing else.
in regard to medical professionals, it varies. i have stuff on my chart that's more stigmatized than autism, so i'm not the best person to ask about how autism may individually impact my treatment. but like, as a rule, you can expect to be listened to less/taken less seriously with something like autism on your records, which you likely already knew. this doesn't mean you're doomed never to have good medical care - my current people are Mad/disability/ND-affirming and abolitionist. but it took me a while to get here, and i have this constellation bc i have insurance and connections etc. consider what you want showing up if you ever need to go to the ER, or to a new dr. it is oftentimes easier to ask for what you need specifically rather than associate it with a diagnosis, for all the usual epistemic injustice reasons.
here's what i'd do in this situation: i'd sit down with my supervisor(s) and be like, okay, here's the stuff i need. how much of this is possible/what are you able to provide workarounds for? don't bring formal accoms into it. don't even bring disability into it. i've told people "i get weird about [noise/lights/etc] haha, sorry to be annoying but could you ___?". when you name yourself as the "weird" "problem," express deference, and play it for laughs, you can get quite a bit. it doesn't always work, though, or doesn't work long-term, in which case i'd say the waitlist would be your best bet.
10 notes
·
View notes
Note
my friend it seems desolate when you hear bad news like desantis's idea but a pharmacist can't refuse to fill a prescription from a doctor? that's super not allowed. and roe v wade being overturned is terrible but prescribing hormones for adults is a different story--especially in cases where someone already has a prescription, it's hard to take that away. there was a bill passed recently in my state preventing minors from getting any medical gender affirming care but even then there was a caveat excluding people who were already prescribed hormones
I don't know why you thought this was a helpful response to my very valid fears, but this comes across as condescending.
I don't live in Florida; Florida isn't the only state in this country where it sucks to exist while trans. And I do know my state laws.
In fact, any pharmacist or pharmacy in the state of South Carolina can refuse to fill my valid testosterone prescription based upon their personal beliefs at any time, and there isn't a thing I can do about it; and this is super allowed, because it is in fact, the law and has been so for over a year.
Actually, I can be refused "nonemergency" care based on a medical providers "conscience" at any time; it's fully legal, and they are protected by state law and so can't be reprimanded or terminated for it.
And this does not only apply to gender affirming care--it applies to abortion care, birth control, STI prevention/treatment, sterilization, insurance coverage of procedures from companies based within the state, etc. I speak of Roe and gender affirming care together often because they both affect my life and health, and the legal battles genuinely are connected.
Not only do I know of transmasc people locally who have struggled to find pharmacies where they can pick up their prescriptions, I also know of people who've been refused birth control prescriptions. I know one person who was refused a tubal ligation after giving birth. I know of at least one instance where a pediatrician refused to accept a child as a patient because the child has two moms.
Anyway, your state isn't the same as every state and my concerns are absolutely real even if they aren't the same as the ones you face.
50 notes
·
View notes