#it entirely is based on each individual person and how their disorder affects them
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Celebrities use Tumblr as well.
Text
I really wish people would stop confusing bipolar and borderline personality disorder and/or acting like one condition is more debilitating than the other
#one disorder is not worse than the other#it entirely is based on each individual person and how their disorder affects them#you can’t make general statements like ‘x is clearly worse than y because of xyz symptoms’#and it’s not a competition anyway#why do we need to have one worse than the other#bpd#bipolar tag#bipolar disorder#mental health
11 notes
·
View notes
Text
Treatment of Substance Abuse at NuLifeLineCare Rehab

Struggling with substance abuse or addiction can feel like navigating a never-ending maze, but there is always a way out. The journey to recovery may seem troubling, but with the right treatment and support system in place, it is entirely possible to break free from the chains of addiction. In this blog post, we will explore the various treatments available for substance abuse, ranging from evidence-based therapies to holistic approaches and medication-assisted treatments. Join us as we delve into the world of substance abuse treatment and discover how individuals can reclaim their lives from addiction.
Understanding Substance Abuse
Substance abuse is a complex issue that involves the harmful use of drugs or alcohol, leading to negative consequences in various aspects of a person’s life. It goes beyond just recreational use and develops into a pattern of dependency and compulsive behavior problems. Individuals struggling with substance abuse often find themselves unable to control their consumption, even when faced with adverse effects on their health, relationships, and daily functioning.
The underlying causes of substance abuse can vary from genetic tendencies to environmental factors such as trauma, stress, or peer influence. Additionally, mental health disorders like depression or anxiety can also contribute to the development of substance use disorders. Understanding substance abuse requires recognizing it as a chronic disease that affects brain function and behavior.
It’s crucial to approach individuals dealing with substance abuse with empathy and understanding rather than judgment. By clearing up on the complexities surrounding addiction, we can better support those in need and guide them towards effective treatment options tailored to their specific circumstances.
Types of Substance Abuse Treatment
Substance abuse treatment comes in various forms tailored to meet individual needs. One common type is inpatient treatment, where individuals stay at a specialized facility for an extended period to receive intensive care and support.
This option provides a structured environment away from triggers that may lead to substance use.
On the other hand, outpatient treatment allows individuals to continue living at home while attending therapy sessions and receiving support. It offers flexibility for those who have work or family commitments but still need help overcoming substance abuse. Both inpatient and outpatient treatments can be effective depending on the severity of the addiction and personal circumstances.
Therapies such as cognitive-behavioral therapy (CBT) and motivational interviewing are evidence-based approaches used in substance abuse treatment. These therapies help individuals understand their behaviors, develop coping strategies, and make positive changes in their lives. Additionally, holistic approaches like yoga, meditation, and acupuncture are gaining popularity for addressing the physical, emotional, and spiritual aspects of recovery.
Remember that each person’s journey to recovery is unique, so finding the right combination of treatments is key to success.
Holistic Approach to Treat Substance Abuse
When it comes to treating substance abuse, holistic approach focus on healing the individual as a whole — mind, body, and spirit. These approaches go beyond just addressing the addiction itself and consider other factors that may contribute to substance abuse.
Holistic treatments often include therapies like yoga, meditation, art therapy, acupuncture, and nutritional counseling. These methods aim to promote overall well-being and help individuals develop coping mechanisms for stress and triggers without relying on substances.
Combined activities that support mental health and emotional stability can be instrumental in recovery. By addressing underlying issues such as trauma or co-occurring disorders through holistic means, individuals can learn how to manage their emotions in healthier ways.
The goal of holistic treatment is not only to overcome addiction but also to improve one’s quality of life in all aspects. Embracing a holistic approach can empower individuals to make positive changes that benefit their overall health long-term.
The Role of Medication-Assisted Treatment
Medication-assisted treatment (MAT) is a crucial component in the comprehensive approach to treating substance abuse. It involves using medications in combination with counseling and behavioral therapies to provide a holistic solution.
MAT can help manage withdrawal symptoms, reduce cravings, and normalize brain chemistry affected by substance abuse. This approach can significantly increase the chances of successful recovery for individuals struggling with addiction.
The medications used in MAT are carefully prescribed by medical professionals based on individual needs and substance use history. They work to address the biological aspects of addiction while also supporting the psychological and emotional aspects through therapy.
It’s important to note that MAT is not a one-size-fits-all solution; it should be tailored to each person’s unique circumstances and treatment plan. By integrating medication with other therapeutic interventions, individuals can better focus on their recovery journey without being hindered by overwhelming withdrawal symptoms or intense cravings.
Medication-assisted treatment plays a vital role in helping individuals break free from the cycle of substance abuse and move towards a healthier, more fulfilling life.
Overcoming Barriers to Seeking Treatment
Seeking treatment for substance abuse can be troubling, and many individuals face barriers that prevent them from reaching out for help. One common barrier is the stigma surrounding addiction, which can make people feel ashamed or judged if they admit they need assistance.
Another obstacle to seeking treatment is the fear of withdrawal symptoms and the unknown journey of recovery. It’s essential to remember that healthcare professionals are there to support you through every step of the process.
Financial concerns also play a significant role in deterring individuals from seeking treatment. However, there are various resources available, including insurance coverage and sliding scale payment options at many facilities.
Additionally, lack of social support or fear of losing relationships can hinder someone from seeking help. Building a strong network of understanding and encouraging individuals can make a significant difference in overcoming these barriers.
Aftercare and Relapse Prevention
After completing a substance abuse treatment program, it’s crucial to have a plan in place for aftercare and relapse prevention. This phase is where the real work begins as you transition back into your daily life. Establishing a strong support system can make all the difference in maintaining your sobriety.
Attending follow-up counseling sessions or support groups can help keep you accountable and provide ongoing guidance. It’s important to continue practicing the coping skills learned during treatment to navigate triggers and cravings effectively.
Engaging in healthy activities like exercise, meditation, or hobbies can help reduce stress and improve your overall well-being. Avoiding old environments or relationships that may trigger substance use is essential in preventing relapse.
Remember, recovery is a journey, and setbacks may happen. The key is to stay committed to your goals and seek help when needed. By staying proactive and focused on your recovery, you can build a solid foundation for long-term sobriety.
Conclusion
Treating substance abuse requires a comprehensive approach that addresses the physical, psychological, and social aspects of addiction. With various types of addiction treatment options available, individuals struggling with substance abuse can find the help they need to overcome their addiction and lead a healthier life. It’s important to remember that seeking treatment is not a sign of weakness but rather a courageous step towards recovery. By utilizing evidence-based therapies, holistic approaches, medication-assisted treatment, and aftercare strategies, individuals can increase their chances of long-term sobriety.
Remember that overcoming substance abuse is a journey filled with challenges, setbacks, and victories. It’s crucial to have support from healthcare professionals, family members, and peers throughout this process. No matter how difficult it may seem at times, recovery is possible with dedication and perseverance. If you or someone you know is struggling with substance abuse, don’t hesitate to seek help at NuLifeLineCare Rehab and start the path towards healing today.
For more information, call us on 08958305058
Or visit: https://nulifelinecare.org/
#drugsfreeindia#saynotodrugs#nashamuktbharat#nashamuktbharatabhiyaan#nmba#bestrehabcentre#rehabilitation#nashamuktikendra#bestrehabindehradun#uttarakhand#fightagainstdrugs#fightagainstaddiction#nomoredrugs#addictionawareness#addictionrecovery#recovery#nasha_ab_nahi#bandkaronasha#dehradun#addiction#bestnashamuktikendra#nulifelinecarerehab
0 notes
Text
Helping: The Role of Delhi's Rehabilitation Centers — A Lifeline in Recovery of Mental Health.
Rehabilitation Centres in Delhi introduce the critical phase into the entire treatment and recovery process of patients with any type of mental illness or substance abuse disorder. Here, one can expect a recovery plan that includes medical support, therapy, and other relevant care activities for the affected individuals to get treatment for life rebuilding. This paper describes the role of Rehabilitation Centres in Delhi, the treatment services provided, and their role in long-term recovery.
Understanding Rehabilitation Centres Rehabilitation centers are specialized units that provide intensive treatment and support to patients recovering from mental health disorders, substance abuse, or both, which is the case in many situations. These centers are fully equipped with a multidisciplinary team of psychiatrists, psychologists, therapists, and other support staff to provide holistic care in Delhi.
Rehabilitation centers focus on helping patients overcome their challenges and give them new ways to take back control over their lives and develop the skills needed to maintain long-term recovery.
Why Rehabilitation Centres in Delhi Are Essential The quick life in Delhi entails a lot of challenges, with diversified populations and hence immense challenges to mental health and addiction issues. The rehabilitation centre Delhi provides a highly structured environment where the patient is left with no opportunity but to engage their whole self in the process of recovery, far from the stressors and triggers of usual life.
Those are some of the main benefits from centres:
It involves comprehensive care, which includes detoxification, therapy, medication management, and life skills training. These rehabilitation centers provide a very conducive environment for recovery, and the patients are in the company of people who understand their plight and are always willing to assist however they can.
Personalized Treatment Plans – Each patient is given a personalized treatment plan based on their condition. This will increase the chances of full recovery and long-term abstinence.
Aftercare Support – Nearly all of Delhi's rehab facilities also administer aftercare treatment to their patients. Aftercare treatment consists of additional therapy sessions, self-help group sessions and relapse prevention sessions that will enable patients to further fortify their condition even after being discharged from the facility.
Types of Rehabilitation Centres in Delhi There are quite a few types of rehabilitation centers in Delhi, each catering to different needs. Inpatient Rehabilitation Centers: These are structured environments with 24/7 care in which the patient is required to reside and engage in intensive treatments for their mental health or addiction problem.
Outpatient Rehabilitation Centres: The outpatient centres enable the patients to be treated from home. Patients with mild to moderate conditions who do not require 24-hour care can be enrolled in this type of centre.
Dual Diagnosis Centres: It is a type of centre designed for patients who have mental health disorders and substance abuse problems. It provides integrated care so that both problems are treated at a time.
Specialized Centers: A few rehabilitation centers in Delhi deal with specific populations, such as women, adolescents, or people grappling with disorders like eating disorders or PTSD.
How to Choose the Right Rehabilitation Centre in Delhi Selecting a rehabilitation centre that fits one's needs will start them well on their journey to recovery. Following are a few things to take into consideration:
Accreditation and Licensing: Check if the center has the accreditations and licenses from relevant authorities to ascertain that it meets the required standards of care.
Course of Treatment: Specific centers may offer a wide range of treatment approaches; others offer a combination of holistic therapy, medication-assisted treatment, and cognitive-behavioral treatment. Choose a treatment that will be best for you or your loved one.
Location and Facilities: Consider enrolling in a center that is located in a serene, peaceful environment to promote a smooth recovery process.
Success Rates and Reviews: Verify the success rates of the center and study the reviews of the patients. A high success rate of treatment and the good reviews given by patients explain more about that effective center.
Conclusion Rehabilitation centers in Delhi are assets for recovering mental health disorder and substance abuse. It is due to the comprehensive care, good environment, and individual treatment plans that these centres provide, which contribute critically towards helping a person take back control of their life. Therefore, in the event that you or anybody close to you is grappling with mental issues or issues of addiction, seeking help from a rehabilitation center in Delhi could just be the first step to a much healthier and enhancing life.
0 notes
Text
The Role of Homeopathy in Managing Thyroid Disorders and Diabetes
Thyroid disorders and diabetes are two of the most common endocrine system diseases affecting millions worldwide. The conventional treatments for these conditions often involve a lifetime of medication and regular monitoring. However, many individuals are exploring alternative therapies, like homeopathy, for a more holistic approach to managing these chronic conditions.
Understanding Thyroid Disorders and Diabetes
Before diving into how homeopathy can help, it’s essential to understand the basics of these conditions:
Thyroid Disorders: The thyroid is a small gland located in the neck that produces hormones regulating metabolism. Thyroid disorders, such as hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid), can disrupt various bodily functions, leading to symptoms like fatigue, weight changes, and mood swings.
Diabetes: Diabetes is a metabolic disorder characterized by high blood sugar levels. It occurs when the body either doesn’t produce enough insulin (Type 1 Diabetes) or becomes resistant to insulin (Type 2 Diabetes). Diabetes can lead to serious complications, including heart disease, nerve damage, and kidney problems.
How Homeopathy Works
Homeopathy is a natural form of medicine based on the principle of “like cures like.” It involves using highly diluted substances to stimulate the body’s self-healing mechanisms. Homeopathic remedies are individualized, meaning the treatment is tailored to the patient’s specific symptoms, personality, and overall health.
Homeopathy for Thyroid Disorders
Homeopathy offers a non-invasive way to manage thyroid disorders by focusing on the underlying cause rather than just the symptoms. Homeopathy treatment for thyroid includes several common remedies for thyroid conditions, such as:
Calcarea Carbonica: Often used for hypothyroidism, especially in patients who are overweight, easily fatigued, and sweat excessively.
Iodum: Typically prescribed for hyperthyroidism, particularly for individuals who experience weight loss despite a good appetite, restlessness, and palpitations.
Natrum Muriaticum: Used for thyroid conditions where symptoms include depression, dryness of the skin, and a craving for salt.
These remedies aim to restore balance to the thyroid gland, helping to regulate hormone production and alleviate symptoms.
Homeopathy for Diabetes
Homeopathy treatment for diabetes can be an adjunct therapy for managing the condition, particularly in the early stages or alongside conventional treatment. Some of the commonly used homeopathic remedies for diabetes include:
Syzygium Jambolanum: Known for its ability to reduce blood sugar levels, this remedy is often used in patients with Type 2 Diabetes.
Phosphoric Acid: Helpful for diabetes-related fatigue and mental exhaustion.
Uranium Nitricum: Used for patients with a history of diabetes in the family, who experience symptoms like increased thirst, frequent urination, and weight loss.
The individualized nature of homeopathy means that the treatment plan considers the patient’s overall health, lifestyle, and emotional state, offering a more comprehensive approach to managing diabetes.
Benefits of Homeopathy for Thyroid and Diabetes Management
Holistic Approach: Homeopathy treats the person as a whole, addressing physical, mental, and emotional well-being.
No Side Effects: Homeopathic remedies are natural and safe, with minimal to no side effects, making them suitable for long-term use.
Personalized Treatment: Each treatment is tailored to the individual’s unique symptoms and health condition, ensuring a more effective approach.
Support for Conventional Treatments: Homeopathy can be used alongside conventional medicine, potentially enhancing overall treatment efficacy and improving quality of life.
Conclusion
While homeopathy may not entirely replace conventional treatments for thyroid disorders and diabetes, it serves as a powerful complementary approach that addresses the root causes and supports the body’s natural healing processes. Dr. Anubbha’s Homeopathy Clinic is dedicated to offering the best homeopathy treatment for thyroid and diabetes, tailored to each patient’s specific needs.
As the best homeopathy doctor in Hyderabad, Dr. Anubbha provides personalized care, ensuring that your treatment plan is customized to align with your unique health requirements. Whether you’re dealing with hypothyroidism, hyperthyroidism, or diabetes, Dr. Anubbha’s expertise in homeopathy offers a safe, gentle, and effective alternative for managing these chronic conditions.
0 notes
Text
The Power of Talk Therapy: 5 Types of Psychotherapy Explained

Talk therapy, also known as psychotherapy, is one of the most powerful and effective tools for treating mental health issues. It involves talking with a psychiatrist in Indore or another mental health professional about your thoughts and feelings to help you gain insight into yourself and find solutions to problems. There are many different types of talk therapy, each designed to address specific needs. Here we will explore five common types of psychotherapy: Cognitive Behavioral Therapy (CBT), Interpersonal Psychotherapy (IPT), Dialectical Behavior Therapy (DBT), Acceptance and Commitment Therapy (ACT), and Eye Movement Desensitization and reprocessing (EMDR).
Cognitive Behavioral Therapy is based on the idea that our thoughts influence our emotions which then affect how we behave in certain situations. CBT helps people identify negative thought patterns that can lead to unhealthy behaviors or emotional reactions so they can be replaced with more positive ones. This type of therapy focuses on problem-solving skills by helping patients become aware of their thinking errors so they can make better decisions in life going forward.
Interpersonal Psychotherapy focuses on relationships between people rather than individual psychological processes as CBT does; it helps individuals develop better communication skills within their personal relationships such as family members or romantic partners through understanding interpersonal dynamics at play between all involved parties. IPT also works towards improving self-esteem while teaching coping mechanisms for dealing with stressors associated with everyday life events like job loss/change etc.
Dialectical Behavior Therapy combines cognitive behavioral techniques alongside mindfulness strategies which focus on acceptance instead of trying to change things out right away. DBT emphasizes developing healthy ways of managing difficult emotions such as anger management, impulse control; building healthier boundaries, etc. It’s often used when traditional therapies have been ineffective due to its ability to create lasting changes quickly without compromising quality care given throughout the entire process.
Also Read: OCD Treatment in Indore
Acceptance & Commitment Therapy's primary aim is to foster greater awareness of an individual's behavior patterns by using mindfulness practices combined with motivational interviewing techniques - this allows patients to see what triggers them emotionally before reacting impulsively, thus allowing people to take back control over their own actions/responses accordingly. ACT teaches us to accept ourselves regardless of any flaws we might have, while simultaneously pushing forward and pursuing goals despite any potential obstacles that may come up ahead of the journey itself. EMDR stands for Eye Movement Desensitization Reprocessing – it’s commonly used to treat trauma-related disorders, PTSD, panic disorder, phobias.
0 notes
Text
Abuse of Children Portrayed in Film
I like to use movies as an escape from the harshness of the real world and one of the things that I have learned about in my education is the effects on children when they are mistreated. I have a Masters Degree in Developmental Psychology and one of the hardest classes for me to handle was Abnormal Development in Children and Adolescents. We covered everything from dealing with dyslexia and ADHD to surviving severe abuse and loss at a very early age. We had guest speakers that ranged from people who had escaped genocide as children, to individuals who had been sold into prostitution by their parents, to people who had suffered severe abuse from their parents or guardian. I have heard stories that will stick with me forever and that is nightmare fuel that I don't want to share.
Because of my background education, I take note of the treatment and behavior of children and adolescents in the movies that I watch. There have been many great movies over the years that have depicted the suffering of children and it has always been difficult for me to deal with. There are more well known examples of films that focus on suffering but throw in more of a "sometimes we all suffer, even the children" message that demonstrate that kids aren't immune to great travesties (basically any film about The Holocaust). There are also well known films that show children "coming of age" through hardship (Annie 1982, Oliver! 1968) but end perfectly. There is a more current series of films that focuses entirely on a boy discovering a fantasy world that was robbed from him when his parents were murdered by a tyrant (Harry Potter series). But in this list I want to review some lesser known films that show examples of abuse. Even after all that I have seen and heard, the following list of films have affected me personally for one reason or another. Sometimes the children in these films endure and overcome their situation in the end. Sometimes these children do not survive or sadly remain in their misfortunes. To me, this can make the movie all the more powerful because of the incredible amount of pathos that endangering a child character can add. It can also make it a heart wrenching experience that is painful to watch. Here are some powerful films in which children suffer and the struggle is one of the main plot lines of the movie:
SPOILER WARNING AND VIEWER DISCRETION ADVISORY!!! I AM GOING TO GIVE AWAY THE PLOT TO THESE FILMS AND IT SHOULD GO WITHOUT SAYING THAT SOME OF THE PLOTS ARE DISTURBING!!! EITHER WATCH THE FILM IF YOU DON'T WANT SPOILERS OR CHECK OUT THE FOLLOWING SUMMARIES IF YOU WOULD RATHER JUST HEAR WHAT HAPPENS SO YOU KNOW IF YOU WANT TO WATCH OR NOT!!!
-----------------------------------------------------------------------------

Sybil (TV Movie) 1976
I just recently saw this film after I had heard of the story in my abnormal development class almost 10 years ago. It is the story of a woman who developed multiple personalities to deal with a childhood in the care of an undiagnosed schizophrenic mother. The movie stars Sally Fields and is based on a true account of Shirley Ardell Mason and her treatment by psychologist Cornelia Wilbur. The acting in the film is overdramatic at times, but it definitely reminded me of some of the actual old videos of Shirley Mason and her sudden strange switches in personality when she was scared or anxious. Dr. Wilbur used hypnosis to actually introduce Mason to her alternate personalities and she was able to recognize her disassociative identity disorder and overcome it. It still hurts me to think that this person was mentally wounded so deeply by her parents that it basically shattered her into pieces in an effort to make sense of things.

Leon: The Professional 1994
I mention this film a lot because it is a heartwarming story of an assassin teaching a young orphan how to murder. It is the breakout role for Natalie Portman and it is just amazing. Leon is a "cleaner" that lives next door to an abusive and addictive family with a troubled girl named Mathilda. The father gets in trouble with the mob and some enforcers come by and slaughter most of the family while Mathilda is getting groceries. She returns during the massacre and realizes what is happening so continues next door and pleads for shelter. Leon takes her in and teachers her the trade and protects her from the men who want to finish her off. The movie was written and directed by Luc Besson and stars Jean Reno, Gary Oldman, and Natalie Portman. The suffering that this girl endures because of her parent's addictions hurts me, yet I have seen and enjoyed this film many times. I recommend watching when in the mood to be deeply affected by the trials of a little girl and the killer who protected her.

Kids 1995
This film came out when I was early in high school and bothered me greatly. It is a story by Harmony Korine, and one of his many attempts to capture the hopeless lives of unmotivated and unsupervised teens. These are young teens having unprotected sex, stealing money to do drugs, and attacking people in the park. I did not really go to these kinds of parties when I was that age (or ever really) and it has bothered me to think that adolescents would partake in this kind of behavior. It is hard for me to believe that these kids had the ability to mentally comprehend the consequences of their actions and some of the characters end up contracting HIV from each other. I would not recommend the film because it is a depressing day in the life that no youth should have.

Gummo 1997
I would not call this a good movie and I wouldn't really recommend it. It is another work by Harmony Korine and really details the depravity that can occur with unsupervised youths living in low socio-economic conditions. This movie is just depressing and motivated me to find something to motivate me into action. I got into both psychology and teaching, which has served me well for the past 20 years. It was this film that showed me how low the bar for quality of life could be, and I guess for that I am thankful. However, I still wouldn't recommend it.

Happiness 1998
This movie I didn't see right away but noticed it at the video store on many occasions. I final watched it when I was about 25 on the recommendation of a friend and one particular storyline greatly disturbed me. It is basically the story of 3 sisters that feel they should be happy and project a face of happiness, yet they are miserable and have horrible lives. One sister in particular is married to a psychiatrist who turns out to be a pedophile that rapes the friends of his young son. At one point rather early on in the movie, this man confesses to his son that he raped the boy's friends and that he would do it again. The son is so confused that he asks his father why he never raped him. It is so disturbing to me because I know the boys that were assaulted will be forever damaged and this boy who was not actually raped will be mentally scarred as well. The fact that there are people in the world that would harm children that way, recognize what they had done, and then know they didn't have the self control to stop themselves from doing it again is horrifying to me.

Lilya 4-Ever 2002
This film is deeply disturbing and I highly recommend never watching it. I will spoil it for you now so you never have to see it if you don't want. A 16-year-old girl named Lilya lives with her mother. The mom gets a boyfriend and the couple move to America and abandons Lilya with a neglectful aunt. The aunt movies into the old apartment of her sister and Lilya is forced to move out and become a prostitute to make money. A boy comes along and convinces her to move to Sweden to escape her life. When they arrive, this boy sells her to a pimp and she becomes a teenage sex slave. She almost escapes, but is then captured and beaten almost to death. She escapes again and this time commits suicide so she won't be recaptured. This movie is awful and changed my mind about giving every film a chance. I wish I could forget this film, but I can't. Perhaps it is just not for me, but this film presentation is definitely an experience that you won't soon forget.

The Kite Runner 2007
I read this book in my twenties and saw the film in my thirties and both affected me greatly. A well-to-do boy and his friend are in a kite battle competition and the friend is beaten and raped when he goes to retrieve a fallen kite. The well-to-do boy denies knowing what happened to his friend (he does know) and basically shames and abandons him. This action haunts the well-to-do boy for the rest of his life. How the boy who was raped is basically falling prey to blaming the victim is heartbreaking, and the lifetime of guilt of the other boy is pitiable. Neither boy was the actual attacker yet they both were the ones that suffered.
---------------------------------------------------------------------------
There are many other examples of movies along these lines and could be found if you feel like suffering. I can't say that I would recommend them because they are very difficult to watch. Beyond just dealing with the content, it is rare to find child actors who can actually portray somebody who has truly suffered. The mix of bad acting and a depressing plot can make for a terrible movie going experience. The genre of movie involving suffering does exist, though, and it could be enjoyed (?) by some. Just not generally by me.
#harmony korine#gummo#kids#the kite runner#suffering#psychology#depressing movies#introvert#introverts#happiness#lilya 4 ever#leon the professional#movies
253 notes
·
View notes
Text
The Psychological Horror Manhwa “Killing Stalking” is not a Romance, but an Emotional Series Depicting the Codependent Relationship Between Two Ill Individuals
Content Warning!!: contains mentions of sexual abuse (rape) and mental illness.
Killing Stalking is an immensely twisted webcomic series, mainly popular within the Yaoi community for its boy on boy focused plotline. The story follows characters Yoon Bum (Bum), a shy, scrawny young man with a haunting past filled with abuse, and Oh Sangwoo (Sangwoo), a younger man who also has a quite damaging upbringing but masks it perfectly with his vibrant, extroverted personality. After being saved from a rape attempt during his time serving in the military, Bum develops a crush on his saviour, Sangwoo, from which an unhealthy obsession starts to arise and he eventually finds himself locating and breaking into the man’s home one day when he’s out. When he does, he discovers a terribly injured woman being held captive in his basement, and with further evidence, soon comes to the realization that his crush is actually a serial killer -- hence the name “Killing Stalking,” as Sangwoo kills and Bum stalks. For a very specific reason though, Sangwoo decides not to kill the man that had been stalking him, and instead holds him hostage in his custody. From here, the story goes into exceeding depth of the abnormal, toxic, and manipulative relationship the two form during their time spent together. By just the mere description of it, it’s a bit concerning to know that a large portion of readers still support Sangwoo and Bum’s relationship. In other words, they believe they truly loved each other and that the story was not only horror fiction but a romance as well. One could easily come to this conclusion by basing their relationship on the few parts within the novel where they showed affection towards each other -- for example when Bum allows Sangwoo to hug him to sleep when he suffered through the night, or my personal favourite, when Sangwoo buys Bum a stuffed frog keychain after finding out that he had an affinity for such creatures. But we cannot simply dismiss the underlying factors of their relationship because of some cute things they did that made our heart melt -- Sangwoo still abused Bum at his leisure which makes those moments quite meaningless in the sense of it all. What Sangwoo and Yoonbum shared can’t be classified as “love,” because even with their peculiar bond and endearing moments, the psychological damage they both endured played a bigger part in the way they perceived each other.
Many toxic relationships start out lovely and glamorous until the couple have become comfortable enough to start revealing some bad habits, but in Sangwoo and Bum’s case, they were already off to a bad start, as the reason they remained with each other was solely for reasons pertaining to their poor mental health.
At the time Sangwoo saved Bum in the military, Bum still suffered from Borderline Personality Disorder (BPD) -- a disorder he inferrably developed due to the fact that he grew up being constantly physically and sexually abused by the people around him. People with this illness may easily develop an infatuation for a person who shows them even the least bit of care; It can reach the point where they begin to idolize them and see them almost as a perfect human being -- which is exactly how Bum viewed Sangwoo after he helped him to escape a rape attempt. The likely specific term for what Sangwoo was to Bum is a Favourite Person (FP). To an individual suffering from Borderline Personality Disorder, their FP is everything -- their self-worth, identity and emotional dependency all rely on this one person, making them the center of their lives. In contrast to this sincere fondness, the only reason Sangwoo kept Bum alive was because of the man’s resemblance to his late mother -- the one person in his life who he truly loved. While his father was abusive and negligent, his mother tried her best to care for her son even while her own mental stability wasn’t so great either. Even though it was implied that he was responsible for the murder of both his mother and father in high school -- getting away with it scotch-free because of how perfectly executed his plan was -- he still shared a special bond with the woman, allowing her existence follow and continue to torutue him mentally as he grew older. When he saw Yoonbum, he felt as if she had been somewhat resurrected, or at least he could pretend so by dressing him up in his mother’s clothes and making him cook and do the chores; He also played the husband role by abusing and assaulting Bum just as his father did to his mother -- mostly just out of his own nature. Sangwoo had his own issues, “mommy issues,” and he initially needed to keep Bum alive so he could fulfill his own longing desires. Knowing the man’s character though, things wouldn’t end there and instead headed down a very gruesome and frightful path.
The very reasons that the two were drawn to each other we’re even more evident the longer they lived under the same roof. While Yoonbum continued to recall the perfect image he had of Sangwoo in his head, Sangwoo continued to manipulate the man in order to satisfy his own needs. A healthy relationship cannot be based on deceit, because one person will end up victimized instead of loved.
Oh Sangwoo is a sadistic sociopath with a history of kidnapping, abusing, raping and torturing innocent people, and because of his illness, he shows feels and shows no remorse for his actions and even proceeds to kill off his victims as they pleaded in objection. What some people don’t understand is that when Sangwoo met Bum, the only reason he treated him differently was not because he thought of him as special, but because he had a personal agenda that included making Bum think that was the truth and that he was indeed the favoured victim among many. It’s no surprise with the man’s manipulative personality that he would enjoy planting a lie in Bum’s head to make him stay and continue to do as he says, and this is confirmed whenever he returned back to his old destructive habits even after showing the man acts of affection. Yes, Sangwoo spared Bum’s life, clothed him and fed him, but as their bond grew, his narcissistic attitude was still more apparent than ever.
Upon meeting Bum for the first time, Sangwoo didn’t hesitate to aggressively break his ankles to prevent his mobility, he left the man within the dark confinement of his basement for a certain period of time before letting him out only after he had gained his trust. He made him sit in a chair to wash dishes and make dinner because he could no longer stand. Sangwoo also constantly dragged Bum down with derogatory words and statements every chance he could get, this included calling him a “retard,” and referring to him as a “disgusting” and “filthy” human being. As confirmed by the author, Sangwoo is also heterosexual, which is further proved by the homophobic remarks he made towards a significantly older man who was sexually attracted to him while murdering him with Bum’s aid. This fact alone is another one that should justify a strong point that demonstrates the true hostility of their relationship -- Yoonbum never gave his consent to have sex with Sangwoo, nor did he allow it to happen because “he wanted it.” He specifically used phrases such as, “No,” “Stop,” and “It hurts,” implying that sometimes there was no mutual agreement when they had sex and Sangwoo had actually raped him several times.
People with Borderline Personality Disorder have been reported to have difficulties seeing the faults in their partner -- this explains why Bum still held on to him. He chose to stay when he had the chance to escape, and with tears rolling down his face from excruciating pain he still told Sangwoo he loved him. In a scene where Bum is left alone with the police as they investigate the suspicions they have surrounding him, he questions them saying, “Could you kiss somebody like me? Could you love somebody like me?” As he believes nobody but Sangwoo could answer yes to those two questions, convinced that Sangwoo really does have feelings for him. It’s saddening to know that the poor man had successfully been lured into a trap, and because of his mental health it would be much harder for him to realize it.
To the readers that think, “Sangwoo and Yoonbum needed each other,” -- You’re not completely wrong. They did need each other in the way that they found somewhat of a saneness from each other’s presence, each using one another to each other’s benefit. But being together at the same time built on their insanity, as the presence of Sangwoo’s mother seemed to grow even more prevalent with Bum, who resembled her, also in the picture, and Yoonbum growing so unhealthily attached to Sangwoo that he constantly feared of abandonment and turned the sociopath into the only source of his happiness. They needed each other, but not for the right reasons. They were attached to each other, but there was no love, otherwise it would reflect throughout the story. One of the most debate-worthy scenes that challenge this fact is when Sangwoo is reported by an old lady in the hospital, the one that had ended his life, that he was calling out Bum’s name throughout the night as he lay in his deathbed. Those were his final words, and Yoonbum’s final word was also Sangwoo’s name before he was very well implied to have been hit by a car while he chased an illusion of the man he “loved.” Even I almost felt that this was solid proof that even through the tough and terrible of their relationship, deep inside, the two really were in love but could not express it in the right way due to their mental health issues -- after all, what someone makes of their final moments before death is much more meaningful than most of what they've done in their life entirely. But I came to realize that the only way I could support this relationship would be if they had met in an alternate universe where they did not suffer from such dreadful childhood trauma that made them into the hurting individual they had become before meeting each other. As difficult as it is for me to picture the two with different partners, it would be best if the two had not met at all as they only fed into the severity of their conditions.
121 notes
·
View notes
Note
im 31, and after over a decade of trying to figure out what is wrong with me, my therapist and I are finally thinking it’s ADHD. i’ve had a gut feeling about it for a while and every ADHD post is relatable. now the problem is finding an place that does adult assessments and is affordable (no insurance). do you have any tips on going through the assessment as an adult? and if i can’t afford it, and can’t get medication. how do i ever become the productive focused person i want to be? thanks.
Sorry in advance for the long post... I put the most relevant bits in bold for a TL;DR version.
I know getting diagnosed as an adult can seem daunting, but you shouldn’t worry too much. While ADHD was once viewed as something that only affected children, it is now widely recognized as a lifelong disorder and you shouldn’t have to fear being dismissed because you weren’t diagnosed early in life. It’s extremely helpful that you have been seeing a therapist, and they also think you have ADHD. Ask them to send over their notes when you do go to the doctor.
As for how to get diagnosed - I’ll start by saying I hate the way American healthcare is set up, as medication and healthcare in general are expensive. I have to move frequently for me and my husband’s jobs (we both work in hospitality, and as the saying goes, “You have to move out to move up!”). Because most (all?) ADHD medications are a Schedule II drug (highly regulated but still legal), I have to get rediagnosed in every new state. I always bring my past history, but most doctors want to complete testing as they are monitored for prescribing stimulants and can lose their license if found to be providing this medication without ample documentation. (All of this to say - I have been through the procedure many times as an adult.) Depending on the state, some doctors also require bloodwork and an EKG to ensure you are healthy enough to receive the medication (although some will accept past test results if done recently enough.) Also depending on the state and doctor, they may have additional requirements. In Florida, my doctor wanted a multitude of tests, and asked for a sleep study to ensure the medication wasn’t causing poor sleep. In California, as part of the Kaiser HMO system, I was required to do periodic drug tests to ensure I wasn’t also using street drugs, and to check that the Adderall was in my system (as a test that I was using it as prescribed, and not selling it). Some states are much easier – Utah, Alabama and West Virginia all were able to diagnose me in one appointment and prescribed the medication same day. Last, a General Practitioner won’t typically prescribe it and will direct you to a psychiatrist. Even if you did have insurance, most don’t cover psychiatrists or if they do, it comes with a different deductible (because obviously mental health isn’t part of regular health (heavy sarcasm)). After diagnosing, you have to meet with the doctor once a month to get the prescription refilled – due to the Schedule II status, they can’t have it on an auto-refill like other medications and they need to ensure you aren’t abusing it or having negative side effects. (although the one good thing to come out of COVID is that it normalized tele-health appointments, since an in-person meeting with a doctor once a month can be difficult to schedule). Even though I have health insurance, I typically pay out of pocket $120 a month for my visit with the doctor, and after insurance and a coupon I pay $73 for two medications (Adderall & Vyvanse). I’m fortunate now to be able to afford that expense – at the times in my life where I couldn’t, I would request a 30 day supply of the more affordable pills and only take medication on days where I couldn’t function without it (such as doing large amounts of paperwork) and try to use learned behavior techniques the rest of the time, to stretch out my resources.
As far as what goes into the actual diagnosis – doctors most commonly use a questionnaire about your daily life to assess you. Here is a link to commonly-used questionnaires: https://www.additudemag.com/adhd-assessments-and-tests/.
I know I just made it seem very daunting to get diagnosed and on a medication, but I want to be honest with you about what the process looks like, and again, depending on where you live it can be done in one session. Now that is out of the way, let me give you some information that is more helpful:
If you can, skip asking a regular GP for a referral and make an appointment directly with a psychiatrist. This will save you the extra cost of the doctor’s appointment, just to be told someone else will help. Many places have low cost mental health centers and ADHD falls into that realm, so I would check out what is available in your city. Before making an appointment, confirm the following:
- Do they diagnose ADHD?
- Do they prescribe medication? (Therapists don’t prescribe, only psychiatrists, and some will not prescribe ADHD medication at all so it’s important to be clear that it is your intention to receive medication if diagnosed)
- What tests do they require for diagnosing, and prescribing medication? (Some places may have more or less requirements, and it can even vary within a city or state. This way you will know if it’s something you can afford at the time.)
Talk with the doctor about your specific situation, and what medications are affordable without insurance. Adderall, for example, is past the 10 year exclusive patent and now has a generic version available. It comes in quick release and slow release, depending on your needs. You can also talk to the doctor about a prescription to both quick and slow release, so you take the correct medicine based on your needs for that day (marathon work day? Slow release that extends over the entire day. Afternoon project – quick release that lasts for four hours). Vyvanse is great but doesn’t have a generic version and is insanely expensive without insurance (to the tune of $350+). Use the GoodRX app to find deals on medication without insurance (Adderall is about $15 for a month supply with this app). There are a ton of drug options so look up the pricing during the doctor’s visit, so you can confirm that you can afford what they prescribe. Also keep in mind that getting a prescription filled is the same cost whether you get 1 pill or 30 (a fact I learned the hard way when getting a 10 pill prescription filled once.)
If you read all that and thought, Thanks but no thanks, here are some other options:
- My psychiatrist in Florida recommended that I take Rhodiola Rosea supplements in addition to medication, as it has clinically proven positive effects on ADHD symptom control. I found it on Amazon. Omega-3 fatty acid supplements are also proven effective.
- If you’re interested in this sort of thing, here is a super comprehensive study of various dietary supplements and behavior modifications that work or don’t work for ADHD: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4968082/
- Practicing meditation is a great way to relax your body (increased stress, while helpful for short-term tasks, can make ADHD symptoms worse long term) and train your mind to hold onto singular, important thoughts (people’s names, why you walked into the kitchen, etc). I use the Waking Up app and love it – there are also many free options in the App Store and on YouTube.
- Regular exercise is another great way to manage ADHD symptoms, as it gives your body a natural serotonin and dopamine boost, two important chemicals your body has trouble producing and absorbing naturally.
- Caffeine is a great, easily accessible stimulant that has a focusing and calming effect on ADHD individuals. My doctor actually asked my parents to give me coffee each morning before school when I was a child, before we moved onto prescriptions.
- Often, there are other factors that go along with ADHD, such as anxiety and/or depression. Getting this under control can go a long way in managing ADHD as well. I’m not sure if you have any issues with those, but it can be helpful to treat both if you do. The medication Wellbutrin is used to treat depression and also has mild stimulants, which would be helpful for both conditions. It isn’t a Schedule II drug, so you can probably ask your doctor for a 3 or 6 month prescription.
- There are a ton more mind hacks and learned behavioral mechanisms you can try – read some of my other posts for suggestions.
Of course, I have to give the legal disclaimer – all of this is based on my personal experience, I’m not licensed in the medical field in any way and only a doctor can give you proper advice for your body and situation, and what medications will be most helpful. 😊
#adhd#adhd diagnosis#actuallyadhd#actuallyadd#executive dysfunction#neurodivergent#adhd advice#getting diagnosed#going to the doctor
13 notes
·
View notes
Text
Acne: Benefits, Treatment, and Cost
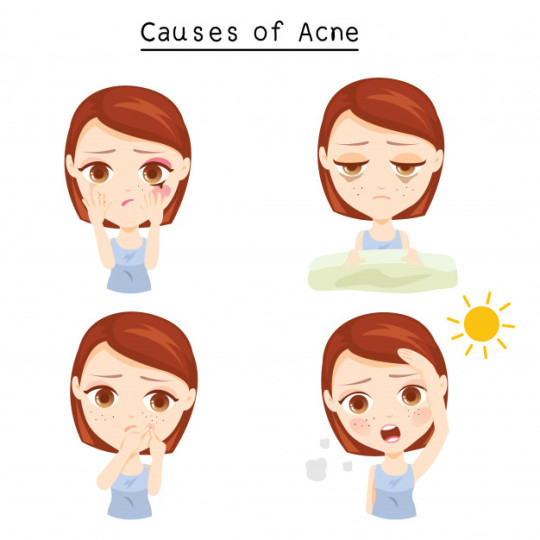
Acne, or in simpler terms, pimples, and zits, is an increasingly common skin disorder today. Affecting mostly the younger age group, the causes of acne include hormonal changes, diet, stress, a hot/ humid environment, or even certain oral medications. When the acne on one’s face becomes severe or progresses to the later stages, it causes extreme scarring. These scars are difficult to be rid of and can cause high emotional distress as well as impact self-esteem.
However, thanks to advanced science and technology today, acne treatment has become an actual possibility. Those suffering from acne can now choose to have their acne treated and their scars removed. In today’s article, we’ll be covering everything one needs to know about acne treatment in Mumbai, its benefits, costing, and more! Let’s get right into it, shall we?
What Causes Acne?
First and foremost, we need to know what causes acne. Acne occurs when the tiny holes in our skin aka the hair follicles get blocked. Here’s how: sebaceous glands are glands that lubricate the skin and prevent it from drying out by producing an oily substance called sebum. When acne occurs, these glands produce excess sebum which mixes with dead skin cells and as a result, clogs the follicles.
What Causes Acne Scars?
After the acne pimples subside, acne scars are a result of the fibrosis of the skin tissues healing. Acne scars are also caused by popping zits and pimples. Acne, if untreated, can leave behind dark marks and pits. Initially, the skin left behind by acne looks and feels different from the skin on your face. But, over time, the body replaces the area with skin that closely matches the rest of the skin on your face and body. Acne scars fade and heal depending on the size of acne, type of scar, depth, and other personal health factors.
Basic Treatments for Acne
The primary and basic treatments for acne include oral medications and topically applied creams. While some of these medications control sebum secretion and reduce bacterial inflammation, the others work towards controlling active acne. Some basic treatments help to fade out marks and scars as well. However, it is important to note that these medications and creams are prescribed based on an individual’s particular skin condition and medical history. If you’re looking for acne treatment in Mumbai, we recommend you consult with a dermatologist or skin specialist and only use the medications they prescribe after an examination.
Advanced Treatments for Acne
In some cases, acne can be advanced and chronic. In order to tackle the skin condition at its worst, doctors recommend certain modern techniques and procedures. Let’s take a look at them.
1. Medical Clean Up
Blackheads and whiteheads not only impact the aesthetic appearance of the face but if left untreated, can go on to form painful acne. The medical clean-up procedure, as the name suggests, refers to cleaning off blackheads, whiteheads, and comedones from the face. The process involves a combination of thorough cleaning, moisturization, chemical peeling, and extraction on the face. One can expect softer, smoother, and blemish-free skin after the process.
2. Medical or Chemical Peels
Medical or chemical peels are an age-old process that involves applying lactic acid to the skin. Lactic acid or the chemical peels help in removing dead skin cells allowing the production of new cells and collagen to be formed. The type of chemical peel is advised to you by your dermatologist as per your skin type and condition. The procedure entails causing a controlled injury on the skin which leads to wound healing, causing new smoother skin to grow. The process highly helps in improving skin texture, reducing scars, and ultimately, getting softer, beautiful-looking skin.
3. Laser Spot Reduction
Laser technique involves the use of Q-Switch NDYAG lasers to lighten the spots and marks left behind by acne. The laser beam is highly precise, targeting only the spots and marks, leaving out other areas of the skin unaffected. The laser-targeted areas are seen to be lighter in tone post-treatment with no evidence of any scars and marks. The procedure is entirely safe and it’s advised to undergo this treatment under the supervision of a qualified professional with efficient equipment.
4. Microneedling
Considered as one of the most effective treatments for reducing acne scars, micro-needling, or skin resurfacing involves the use of a derma pen. A dermapen is a small electric device with multiple pins on its head. These pins are pricked into the skin to create hundreds of tiny holes. The process causes controlled damage, resulting in collagen production and getting the desired results.

Cost of Treatment
Acne conditions can vary from individual to individual, and naturally, so will the treatments and their intensity. Below are some indicative prices of acne treatment in Powai available at our clinic InUrSkin:
1. Medical Face Cleanup - Rs. 1000/- onwards
2. Medical or Chemical Peels - Rs. 1300/- onwards
3. Laser Spot Reduction - Rs. 1000/- onwards
4. Microneedling Treatment - Rs. 2000/- onwards
You can prevent Acne breakouts by following simple steps of anti-acne regimen mentioned in my blog here - https://www.inurskn.in/be-spot-on-with-your-anti-acne-regimen/.
Acne is one such skin condition where the earlier you seek help, the better. Acne, if treated in time and at its early stages, can prevent you from a lot of worry in the long run. Be certain to consult with a dermatologist to work out how advanced your acne condition is and which treatment is best for your skin. Are you looking for a skin specialist to do acne treatment in Mumbai? Consult online with Dr. Sejal Saheta’s expertise and experience at The Personal Touch - our Online DoctorCare service. We’re a dermatology clinic with 15+ years of total experience offering the best services in cosmetology and dermatology. Dr. Sejal has extensive experience in conducting acne treatment in Powai and always offers appropriate solutions to her patients. You can be rest assured - we, at The Personal Touch, only advise and recommend what’s best for you and your skin.
About INURSKN:
Built on more than a decade of experience of Dr. Sejal Saheta, we are an honest and affordable skin & hair care clinic. Our goal is to make each patient comfortable and happy with their appearance with the least amount of intervention. InUrSkn is equipped with the latest technology, from lasers for skin rejuvenation and skin lightening to more traditional skin polishing machines. Located in Powai, Mumbai we are easily accessible from both central and western suburbs. In case we have been able to help you achieve your health and beauty goals, please do review us at:
On Practo: http://prac.to/vkpj
On Google: https://goo.gl/zHfACo
Disclaimer:
This article is one in a series of articles on skin conditions by Dr. Sejal Saheta – MD, DNB – Dermatology and Venereology. The objective of this series is to educate the reader and help them take precautions against various skin conditions they come across on an everyday basis. These articles are not meant to be used by patients for self-diagnosis or for avoiding proper medical treatment. The images used in the above blogs are just for the visual representation of the treatment results may vary from patient to patient.
1 note
·
View note
Text
Bullseye: Dissociative Identity Disorder
I’m kinda musing about Bullseye having a type of identity disorder after both the whole history of taking the roles of others and fanon interpretations around him. On one hand I can see how it fits but on the other it’s not quite perfect either which on the other hand is typical of DID in irl. So, I’m gonna look at this a little closer and see what I think.
As a disclaimer, I’m not a psychologist and I know that the entire DID diagnosis is in fact contested in psychology. This will be a long post.
TL;DR: there is evidence to say, more than enough for head canons, that Bullseye does have a from of DID together with comorbidity in other diagnoses. However, nothing on panel makes this absolutely clear due the absence of a clear definable alter contrasting to a core personality. He does however have a poor sense of self and identity.
But let’s start with what DID is and isn’t.
DID symptoms include "the presence of two or more distinct personality states" accompanied by the inability to recall personal information, beyond what is expected through normal forgetfulness. Other DSM-5 symptoms include a loss of identity as related to individual distinct personality states, and loss referring to time, sense of self and consciousness. In each individual, the clinical presentation varies and the level of functioning can change from severely impaired to adequate.
The symptoms of dissociative amnesia are subsumed under the DID diagnosis but can be diagnosed separately. Individuals with DID may experience distress from both the symptoms of DID (intrusive thoughts or emotions) and the consequences of the accompanying symptoms (dissociation rendering them unable to remember specific information). The majority of patients with DID report childhood sexual or physical abuse, though the accuracy of these reports is controversial.
Furthermore, DID is often comorbid with borderline personality and other diagnoses like substance abuse, anxiety, depression, PTSD, schizophrenia and bipolar disorder; and significant trauma.
In the comorbid category we find traits and actual diagnoses Bullseye has been given in canon.
Netflix Bullseye was canon borderline, as an interpretation of his comic self. While, it has not been state in the 616, it was the attempt to reconcile the mental health disorders that Bullseye obviously has from his violent mood swings with strong emotions, his distorted sense of self, tendency to fixate on people and unstable relationships. The Netflix show wasn’t perfect in it’s handling of it, especially in how BAD Dex’s psychiatrist was at their job, but showed a tragic side of the diagnosis if accompanied by the worst possible circumstances and a comorbid diagnosis of ASPD.

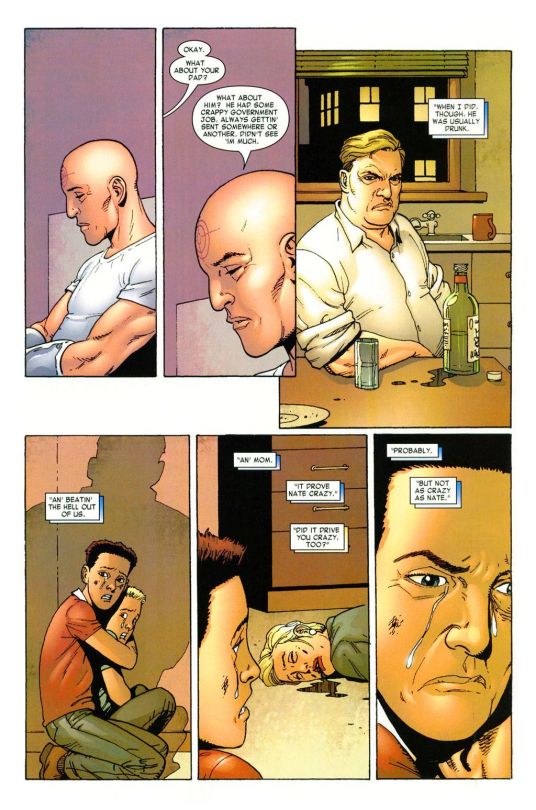
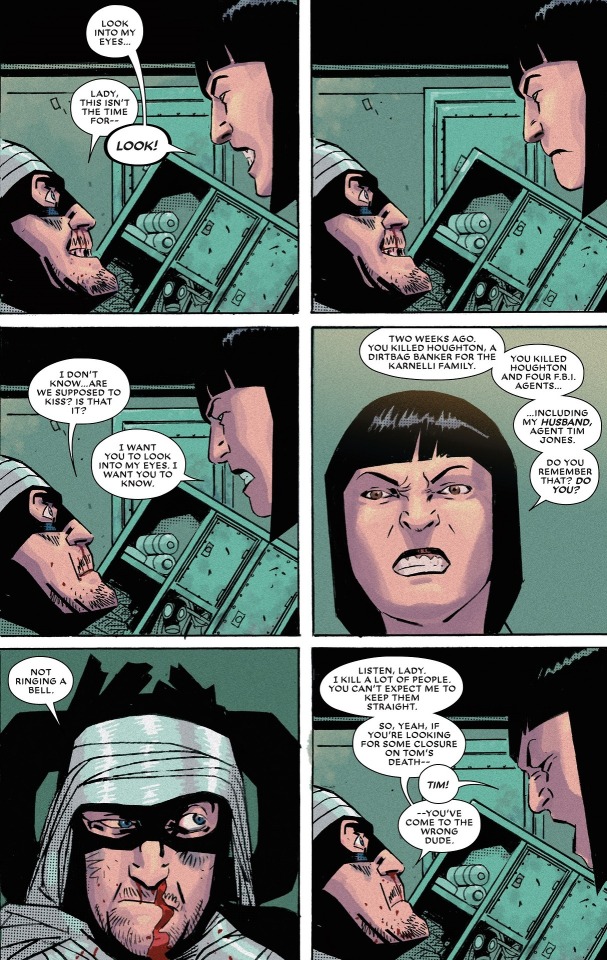
As for comics Bullseye, he was been on panel stated to have bipolar disorder (foolkiller), tumor induced hallucinations and brain damage (DD), ASPD/Psychopathy base on ‘scary frontal lobe’ (DD), and multible depictions of public breakdowns, nightmares and in a future timeline depression that lead to suicide (End of Days). He’s seen to have frequent suicidal ideation in 616, most prominently in Elektra where he begs her to kill him, but he’s self-destructive and suicidal in frequent appearances.
In Dark Avengers he was medicated, taking a anti-psychotic called Clozapine, which is primarily used to treat schizophrenia and Schizoaffective disorder. It’s not clear if this was his usual medication or a situational one.
He does meet the criteria of the latter rather well in verse.
Schizoaffective disorder: (SAD)
The diagnosis is made when the person has symptoms of both schizophrenia (usually psychosis) and a mood disorder—either bipolar disorder or depression—but does not meet the diagnostic criteria for schizophrenia or a mood disorder individually.
But to circle back into the issue of DID, we’ve already crossed of that, yes, Bullseye has mental health issues that are co-morbid with DID and shares traits with it. However, going into the actual criteria.
Does he have alters or a loss of identity tied to disassociation?
The former is actually harder to prove, unless you actually postulate that the persona of Bullseye is an alter, in it self, to a core personality that his traumatized and depressed as seen in his multiple more private breakdowns. Alters are usually more aggressive than the core personality, theoretically built to protect the core personality when it disassociates from harm, danger and abuse.
In that sense, Bullseye does fit the bill if you postulate a split between it and Lester/Dex/Benjamin. You do have enough trauma, both early childhood abuse and repeated adult, and other mental disorders to facilitate such a split of identity. This fits the criteria of DID.

As for the other common criteria of memory issues that is associated with the dissassociation aspect of DID.
There is no evidence however that he suffers from dissociative amnesia regarding what he does in his different personas, though he does state that he forgets things that he doesn’t find important and when confronted with information about himself he simply doesn’t recall. He doesn’t find this unusual however or worthy of remarking on. He frequently forgets people’s names too.
However, it is debatable if this is in fact beyond forgetfulness for a professiopnal assassin with a history of head trauma and shallow affect when it comes to empathy, which are key to imprint certain types of memories.
This is though from the perspective of Bullseye, the alter - if we postulate he does have DID - we normally meet on panel, and since his past life prior to Bullseye is shrouded in mystery it could be that this is no deliberate misdirection and concealment, but actual inability to recall. This could then meet the criteria of “inability to recall personal information” that is central in DID.
It could be that the ‘Bullseye’ alter does not know who the core personality is or any definable personal information, thus he lies to protect that personality. Thus the multiple choice backstory, the many names he uses, and theatrical nature of the Bullseye persona.
Regardless, this will inevitably become fanon as canon doesn’t have enough information to say either way.
However, we do have the on panel reoccurring issue of him dressing up as other heroes and seeming to suffer various gradients of confusion, stress and issues around his own identity.
Most blatantly in Daredevil, when he and Matt switched costumes and ultimately took on each others roles, seemingly both dissociating their identities in the ‘role-play’ they were engaging in.

Bullseye has traits of this in his other roles where he delves deep into some else’s life and tries to relive it (Punisher Max but even early Elektra with his obsession with her), and complains that being put in someone else's costume makes him feel a loss of identity and increasing his stress, resulting in a need to be ‘me’ and incresed violence (Dark Avengers as Hawkeye).
This all point to the weak construction of identity and his distorted sense of self. Bullseye relies on outside marks to know who he is, such as his costume, his role, and the direction of others.
That last part is supported by his need to have a steady employer and sense of purpose that has, he admits as much to the Kingpin and placed a lot of his sense of security in being the Kingpin’s assassin for the short time he was in that role. And he was repeatedly returned to him, looking for goals and order in his life.

In itself, this is a symptom of both BPD and SAD as well as DID. We see that mirrored in Netflix Dex who needs a ‘Northstar’ to find a way to function. Initially using his psychiatrist, then Julie Barnes, then the FBI and finally Wilson Fisk to determine who he was and what he was supposed to do.

Even 616 Bullseye cares what the Kingpin thinks of him and DD uses that to hurt him. And as in both verses, the Kingpin does not care for him but merely uses him, finding him weak-willed, a disapointment and stupid, thus easy to manipulate but prone to messing up jobs.
Now together, this can just point to a mood disorder together with identity issues needing outside order, leadership and framework to function and becoming psychologically distressed and confused when these are absent during times of high stress. Then on top of it being prone to nervous breakdowns and psychotic episodes. This can in itself be BPD, Bipolar with comorbid tendencies, Schizoaffective disorder and a multiple overlapping disorders.
However there are traits that imply that DID is a possible comorbidity with the preexisting diagnoses and disorders he seems to have. There is no singular disorder that fits all of his mental health issues; Bullseye is 100% comorbid. DID is a diagnosis that is one of the most comorbidity carrying in the DSM-5; it averages with 6-7 comorbid mental health disorders.
As a summary, the door is open to interpret him with or without dissociative identity disorder.
TL;DR:
Could Bullseye have Dissociative Identity Disorder?
Yes.
Does Bullseye have Dissociative Identity Disorder?
It’s not possible to tell.
Do writers intend Bullseye to have Dissociative Identity Disorder?
Seemingly, not. As the on panel diagnoses are ASPD + Bipolar Disorder or Borderline Personality.
Can I still headcanon it?
Of course.Especially since DID is notoriously hard to diagnose and considered one of the ‘hidden’ disorders.
24 notes
·
View notes
Text
TAFAKKUR: Part 255
DO NOT UNDERESTIMATE SMALL THINGS
Who does not want to know the future? Is it not one of our impossible dreams to obtain advance information about tomorrow? Events developing in time have such a complicated structure that small things can make all the difference. For example, a small mutation in one (or couple of) gene(s) leads to cancer, which can be a devastating disease. Today, we cannot make long-term predictions; we do not know when the next earthquake is going to take place or how stock market prices will continue to rise and fall. Life is full of these unknown and unpredictable events.
In modeling atmospheric convection in the 1960s, a meteorologist and mathematician at MIT, Edward Lorenz, came up with a mathematical model showing that small perturbations in input parameters result in huge deviations in output, the “butterfly effect.” In other words, in theory, a butterfly flapping its wings in China could bring about a storm in New York City. This is another way to express sensitive dependence on initial conditions. Getting up two minutes late, one may end up missing the bus, which in turn costs one the job interview. As a result of pushing the brake pedal one second earlier a person’s life can be saved. Such slight changes in daily actions are actually signs of how tiny changes are relevant with our lives and how sensitive the future is to the present. Such dependence is called nonlinearity and many scientific problems, such as the well-known Navier-Stokes equations, have been awaiting a solution because of this complexity. In contrast to a deterministic approach, which is based on the idea that the knowledge of the past enables one to make future prediction, a nonlinear (or chaotic) approach claims that the future is not that straightforward.
In contrast to what we used to believe, chaos does not mean complete disorder. Some complicated long-term events may have a hidden order. Being bound by time prevents us from knowing the future. It is in this sense, that time can be said to be another dimension, so that together with the other three, our living environment is formed. To be able to control or observe time-dependent events, the individual of this four-dimensional space may need to move outside of time. To understand this idea better we may analyze the well-known butterfly example. the behaviors of three different variables are very irregular, complicated and chaotic. However, when the same motions are transformed into another space where time is hidden, what we see is an interesting order between these three variables.
Chaos and spiritual life
The human being’s spiritual life is also sensitive to small changes. We are continuously exposed to our personal desires and Satan’s whispers. One small sin is an invitation to worse ones which eventually accumulate and trouble the soul. Similarly, every good deed, no matter how small, has the potential to become a ticket to paradise. It just depends upon the situation in which it was performed and the level of sincerity in our heart. Giving water to a thirsty dog is not an extraordinary act, but in the particular case mentioned in a tradition of the Prophet Muhammad, peace be upon him, this sincere act was significant enough to purify a very sinful person, while another went to hell because of letting a cat starve. In another tradition, the Prophet says, “When a person first commits a sin, it falls as a black dot in (the clean slate of) his heart; if he refrains, repents, and seeks forgiveness, it is however erased; if, on the other hand, he were to persist in sin, the dot will gradually expand until it covers the entire heart.” The Prophet then explained, “This is the state of sealing the hearts that God warned (us) of in the Qur’an: Nay the sins they have accumulated have covered their hearts like a seal” (Mutaffifin 83:14). Likewise, in his Risale-i Nur collection Nursi says, “Sin, penetrating the heart, will blacken and darken it until it extinguishes the light of belief. Within each sin is a path leading to unbelief. Unless that sin is swiftly obliterated by seeking God’s pardon, it will grow from a worm into a snake that bites the heart.”1 Likewise, initial tiny scruples can grow exponentially and destroy hope in the heart in an unexpected way. Nursi explains this in the following way:
O you afflicted with involuntary evil thoughts and fancies, such things resemble a misfortune. The more you dwell on them, the more they grow. If you ignore them, they dwindle away; if you exaggerate them, they swell; if you belittle them, they die down. If you fear them, they become grave and make you ill; if you do not fear them, they become slight and remain hidden. If you do not know their real nature, they persist and become established; if you recognize their nature, they disappear.
. . .
Satan first casts a doubt into the heart. If the heart does not admit it, he offers a blasphemy and causes the mind to recall some unclean memories and pictures, some ugly scenes that resemble blasphemy. This causes the heart to despair. People experiencing such thoughts think that they are acting wrongfully toward their Lord and so feel great agitation and anxiety. To free themselves, they flee from the Divine Presence and want to plunge into heedlessness and forgetfulness.
From the human being’s perspective, each time-dependent event can have very complicated consequences but it always bears God’s signature and His divine order. He is the only One Who knows the future, as stated in the verse: “They said, 'Why hasn't a miracle come down to him from his Lord?’ Say, ‘Only God knows the future.’ Therefore, wait, and I will wait along with you” (Yunus 10:20). It may not be possible to see tomorrow, but we should be aware that each small change we make affects our future. Many scholars lived in such a way that they were always carefully watching their hearts to take immediate action on small deeds or scruples. For every event or option we face, the decision is up to us to, like whether we smoke or not, whether we lie or not, whether we get up early or not and so on. These sets of small decisions play a role in terms of the future we do not know. Although they are small, they have such a big impact and should not be underestimated. Even reading this article was one of these small things you had the choice to do or not to do!
#allah#god#prophet#Muhammad#quran#ayah#islam#muslim#muslimah#help#hijab#revert#convert#hadith#sunnah#religion#reminder#dua#salah#pray#prayer#welcome to islam#how to convert to islam#new convert#new revert#new muslim#revert help#convert help#islam help#muslim help
1 note
·
View note
Text
Therapy For Anxiety As Well As Stress And Anxiety.
Stress And Anxiety Therapy & Therapy.
Content
Smart Area Home Heating: A Sustainable Service Sustaining The Energy Change.
Taking Care Of Splitting Up Anxiety In Dogs.
Xmases: 7 Ways To Maximize An Extremely Various Household Xmases

Silverline - this is a. totally free personal helpline providing details, friendship and also guidance to older people which is available 24 hr a day, everyday of the year. Every Mind Issues - this is a national project run by the NHS which offers you great deals of useful recommendations on mental health and wellbeing, access to resources and also an application to help track your mood. Resources have likewise been established particularly to sustain you with the important things you may be fighting with during Coronavirus. >> more information of direct-therapy Frequently Asked Questions plus are held on the internet and are around half a hr long, with time to ask concerns at the end of every session. The Coronavirus outbreak has had a big impact on our daily lives.
How Augmented Reality Is Helping Teens Address Anxiety ARPost - ARPost
How Augmented Reality Is Helping Teens Address Anxiety ARPost.
Posted: Mon, 11 Jan 2021 09:10:00 GMT [source]
Reducing or quiting each gear, will certainly decrease and stop the OCD's control of you. By acting upon each cog, you will be repossessing control of your life, from the OCD. Others do not have these devastating ideas, however may really feel very uncomfortable and become increasingly anxious and also troubled if they don't do what their head is informing them to do. SilverCloud- an on the internet course to assist you better handle anxiety, stress and anxiety and anxiety.
Smart Area Heating: A Sustainable Service Sustaining The Power Shift.
Progressively, as you overcome each obsession, you can begin to move up the power structure, relocating onto a much more difficult/distressing thing each time up until you have gotten over the most traumatic one. After identifying what you do you can list them all using theHierarchy of Feared Situations as well as price them according to just how distressing every one is or would be if you could not do what you feel obliged to do. The simplest means to begin is to maintain a diary of your routines/ compulsions for one week utilizing theOC Rituals Diary.
youtube
The even more we attempt NOT to think of something, the more it keeps turning up right into our heads. We need to maintain the stress up and maintain lowering, but it simply keeps popping back up right into our face. It might nudge us from time to time, yet that's ok, we can simply let it be. What our team believe deep down about ourselves, others as well as the world, influences and distorts the means we make sense of everyday life. Even if we believe something bad could take place, doesn't mean that is exactly how it truly is! We are checking out life and also situations with those extremely altered lenses. We can make positive changes in each tiny cog in this "savage gears of OCD" layout.
Taking Care Of Splitting Up Stress And Anxiety In Dogs.
Pure O is the main style of the Network 4's program, Pure, which follows 24-year-old Marnie, that is bombarded by invasive ideas of an extremely sexual nature. Drug therapies can additionally be utilized effectively in mix with ERP. The most usual medicine is a kind of antidepressant known as selective serotonin reuptake preventions. These boost degrees of a substance called serotonin in the mind. One of the most usual is worrying about contamination from dust or germs. Please be aware that as a result of the flow of time, the information offered on this page might be out of date or otherwise unreliable, and also any kind of views or opinions revealed might no longer be relevant. Some technological elements such as audio-visual as well as interactive media might no longer function.
If you disable this cookie, we will not have the ability to save your preferences. This suggests that every single time you see this web site you will need to make it possible for or disable cookies again. Purely Essential Cookie ought to be allowed at all times to make sure that we can conserve your choices for cookie setups. https://direct-therapy.org.uk uses cookies to ensure that we can give you with the best individual experience possible.
Christmas: 7 Methods To Take Advantage Of A Very Different Household Xmases
It's entirely easy to understand to really feel anxious with all unpredictability bordering the pandemic, or stressed with being removed from good friends or family members. They'll assist you to discover and also recognize a few of the ways you're really feeling, and deal practical methods you can aid yourself. Worn out as well as incapable to rest one evening, I finally admitted to myself that I required assistance. I researched regional therapists through a site called the Counselling Directory site as well as located someone suitable.
You will certainly discover exactly how they affect you and most importantly, what can be done to alter them.
It intends to break overwhelming issues down into smaller sized components, making them much easier to handle.
While past occasions and also experiences are considered throughout the sessions, the emphasis is more on current issues.
During how to choose Counselling for Depression , your therapist will certainly assist you recognize any unfavorable thought patterns you have.
Unlike a few other therapies, CBT is rooted in today as well as seeks to the future.
He had produced transgenic mice to over-express this healthy protein in their T-cells, one of the main cells responsible for the advancement of autoimmune illness, yet located the computer mice showed a lot more anxiousness than normal. When he and also his group evaluated the genetics shared in the animals' T-cells, they uncovered one genetics particularly was particularly active.
Is Cognitive Behavioural Treatment (cbt) Right For You?
Two days later on, we started our sessions and also I started to fight back versus OCD, first of all by speaking openly as well as truthfully. Saying your worst ideas out loud and also having an expert empathise and wish to explore them with you, instead of decline you, modifications everything. One half of my mind was advising me to stand up and leave, to examine, on the premise that I had actually done something absolutely dreadful. The opposite side was fighting back, assuring me that no, I had not done anything that can harm one more person, and also reminding me that I required to be expert and also not humiliate myself. I was chairing a conference for one of one of the most vital initiatives of my career, bordered by people with extremely hectic journals.
At what age does anxiety peak?
Adults ages 30 to 44 have the highest rate of anxiety of this age group, with around 23% of people this age reporting an anxiety disorder within the past year.
We give evidence-based information, advice and assistance to those influenced by Obsessive-Compulsive Condition. This phase will certainly give details regarding some of the related problems that may be co-morbid with OCD. You can support the work of OCD-UK by coming to be a member from just ₤ 2 a month. Obtain involved in the work of OCD-UK with volunteering or support the work of our charity via fundraising. Find out more concerning the suggested therapies for OCD, consisting of just how to access NHS or exclusive treatment. This section has lots of info, advice and also includes to assist during this time around. Having OCD is hard, not only for the individual, but likewise for those that love and also take care of individuals with OCD.
#cognitive behavioral therapy online#cognitive behavioral therapy techniques#cognitive behavioral therapy near me#cognitive behavioral therapy examples#cognitive behavioral therapy definition#cognitive behavioral therapy nhs#cognitive behavioral therapy for anxiety
1 note
·
View note
Text
WHAT IS MUSIC THERAPY? WHAT CAN MUSIC DO FOR MENTAL DISORDERS?

Hi everyone, today I want to shed some light on an extremely relevant topic that I’m sure has touched so many of us: music therapy and mental health.
In a modern society struggling with mental health is becoming more and more common. As a matter of fact, according to a study conducted worldwide by the Mental Health Organization, more than 300 million people suffer from depression. Additionally, more than 60 million people suffer from bipolar affective disorder, and 23 million people suffer from schizophrenia and other psychoses. Music has been used for self-regulation of moods and emotions for a very long time. The matter has also been subject of many investigations and studies. Through these studies, it has been possible to see all the benefits music has on physical, psychosocial and physical health. Additionally, extremely relevant are the studies conducted on the application of music as a therapeutic tool in the treatment or management of mental health disorders such as depression for instance.
There are several approaches where music has been used to promote therapy and health. The first one is Neurologic Music Therapy. This treatment is administered by an accredited music therapist with a certificate in neurologic music therapy. This approach is based on the rehabilitation of brain and behavior functions, concentrating mostly on cognitive speech, language, and sensorimotor disorders. This therapy consists of exercises to facilitate functional non-musical outcomes and to train abilities in cognition and psychosocial functions such as speech and language, motor control, emotional growth, and social skills. Another approach used is Music Therapy. This treatment is administered by a qualified and trained music therapist. The approach uses the music experiences of the patient to promote, maintain and restore health. The experiences are broadly categorized into active experiences that involve singing, playing instruments, improvisation or composition of music. The second category is receptive experiences. This involves adjunctive activities such as listening to live recorded music, for instance, relaxing music, meditating, practicing movement, drawing or reminiscing. Music therapy is focused on facilitating well-being, social relationship building, self-awareness, self-expression, communication, and personal development. The third approach is the Music Medicine. This term was developed in the 90s but sometimes it is used to describe uses of music that do not involve therapeutic process and client-therapist relationship. However, Music medicine is strictly related to music listening protocols for pain reduction, anxiety reduction, relaxation, mood induction, emotional well-being, to induce sleep and boost alertness.
It has been studied that music therapy can be helpful for many different issues that could be either physical or mental conditions. Indeed, it has been seen how music stimulates the senses and provokes a series of therapeutic responses that could lead to having feelings of familiarity, predictability and even security. Music therapy is used to help clients with mental disorders to communicate and express themselves when words fail to do that. This treatment has suggested that specific parts of the human brain are affected by elements of music. Particularly, it has been seen that for instance, some rhythmic paths appear to calm the mind and the body of the patients. In fact, it is thought that music therapy works in different ways depending on the issues that are addressed. For instance, some researches have shown that music with a strong and fast rhythm can affect the heart rate and the breathing path. This way music is broadly used as an aid with relaxation and to reduce muscle tensions. It has been also studied that music can promote the release of endorphins which are practically natural painkillers. This therapy is also helpful in assisting people in releasing negative memories and feelings. Last but not least, it has been found that music can help change behaviors and thus it can be used to reduce behavioral issues.
After all this information a question appears logic: What happens during a music therapy session? Music Therapy sessions are similar to other forms of therapy. Initially, the therapist establishes a therapeutic relationship and alliance with the patient. This will contribute to making the session of therapy a comfortable space where clients can address their issues, express themselves and work towards therapy goals. When these first vital steps are made, the therapy will involve the use of listening to music and making instrumental or vocal music and discussing the patient’s reactions during these experiences. The approach set by music therapists is also something interesting and relevant. Indeed, they normally use instrumental and vocal music strategies to help the client reach their therapy goals. For each patient it will be chosen a specific musical selection and some particular music-making activities. All of this will be based on the individual’s preferences and needs. Hence, music therapy initially involves assessment, treatment planning and evaluation which allows the therapist to select and modify them as needed based on the patient’s progress. As mentioned, these approaches may be active or receptive. Indeed, when the patient is asked to make music, that is an active technique. On the other hand, when the client is asked to listen to music and respond to it with body movements or analysis, that is when the receptive technique is used. Some patients may also be asked to write songs. Additionally, these techniques can be used during either an individual session or in group therapy settings.
Another crucial point about music therapy is that Music Therapists must be well trained in order to do their job properly. Hence, the patient must be careful in choosing the right therapist. Indeed, one of the therapist’s primary ethical duties is to consider carefully the possible risks intrinsic to each type of music experience and to share this knowledge with the patient. This will aim to protect the client and their safety, promoting their agency in the therapeutic process. Additionally, one of the primary responsibilities of the music therapist is to design and facilitate the therapeutic methods and the variations to support their patients while they face life’s trials. A good therapist has also to identify new options for acting and build on personal and collective capacities toward enhanced health and wellbeing.
Additionally, the patient should also take into consideration that every therapy session could carry some risks as well. For instance, during a group session that promotes cohesion among adults seeking mental health treatment, the patients may experience embarrassment from using their voices. Additionally, this experience might evoke unconscious memories and associations of unpleasant or even traumatizing nature. Moreover, when young patients engage in performing pre-composed music, such as a music group they might feel accomplished and proud of their work. Although, they might also experience intense anxiety, dissatisfaction and humiliation if the musical parts do not fit together. Another example is when an abused teen works with a therapist while composing an original song or instrumental piece. The energies brought to bear through musical tensions and resolutions or the moods evoked by the sonic qualities of certain instruments might be incongruous with the client’s lyrics. This may distort the patient’s inner experiences which could lead to complicating the therapeutic process. Additionally, some other risks related to music listening could include overstimulation and confusion. This could also be a major issue for those patients who experienced a brain injury or who have neurologic disorders that impact their use of the sensory input. Moreover, there is always a risk of physical injury as the listener takes in music to guide their movement schemes when dancing for self-expression or to release stress.
Furthermore, since I have experienced depression and since music has always helped me to stay balanced, I thought to shed some light on how music therapy could be useful to prove it is a valid option to treat this condition. I myself, have used music to heal when I was in need. Indeed, I can now say that music has been the fulcrum of my entire life, easing my pain during my worst years. Back in 2001, in my elementary school years, my struggle with depression and anxiety began. During those years I was bullied by my classmates and my teachers. My battle against bullies, depression, and anxiety, specifically panic attacks, went on for years and now I’m still dealing with the side effects of all that I had to endure. However, despite the pain I suffered, there is a bright side to these painful experiences: they made me discover how powerful music can be. As a matter of fact, that was during elementary school that I discovered my passion for music and in the last year of middle school I found out how powerful music can be and how it can be used to the advantage of people who suffer from mental disorders. While I was going through the harassments of bullies, music became my biggest source of happiness and escapism, to the point that I could not live without it. I started then listening to music to ease my pain and to escape from all the things I was going through. At the age of 12, I discovered that playing an instrument could give as many benefits as listening to music. Therefore, I took some guitar lessons, given the fact that I had always wanted to play an instrument. When I was in the 10th, 11th and 12th grade I took singing lessons, which helped me become more confident and raise my self-esteem. Thanks to these courses, I made music my major emotional outlet, and my safe space where I could release all my anger, frustration, rage, pain and where I could express myself. Hence, I could say that I experienced both receptive and active experiences and I can say that both of them have been extremely helpful. As a matter of fact, still, today when depression kicks in, I turn to music and it instantly gives me the relief I need.
Thanks for your attention✨ G✨
#music therapy#music#mental health#music saves lives#music is medicine#article#therapy#mental disorders#music blog#music helps#personal story#my story#reblog#music lovers#music is so powerful#powerful music#mental health and music#music addict#music heals#writers#tumblr writing society#writing about music#power of music#modern society#neurologic music therapy
17 notes
·
View notes
Text
An In-depth Response to JK Rowling from a Transman
**CW: transphobia, suicide, surgery, discrimination, assault**
Let me first say that we should not allow this conversation to derail the progress and momentum of the Black Lives Matter movement. Though race and sexuality intersect in many fascinating and important ways, it is important to allow the voices of our BlPOC to be heard and amplified for as long as it takes for meaningful, sweeping changes to be made in our society. That being said, I would be remiss if I did not take the time to process and respond to the conversation you have chosen to bring to the table.
TLDR: To JK’s assertion that trans women threaten the political and biological class of ‘women’, Acknowledging that trans women are women is not the erosion of a political and biological class. It is strengthening those classes by accepting the women who, despite all threats of assault or death, stand by their identity and celebrate womanhood.
Let me also begin by saying thank you. For surviving, for persisting, for blessing the world with the gift of magic. The books-which-need-not-be-named were and are pillars of my childhood, identity, and life philosophy. I will never stop finding solace in the pages of those books.
Before we can continue the conversation, I need to introduce myself. I am a (relatively) young white transman and former D1 softball player. I chose to defer physical transition but came out socially as a transman in my sophomore year and was one of the few openly trans NCAA athletes at the time. I was also a student, and spent a large portion of my collegiate career studying LGBTQ+ issues and how they connect to human psychology. My senior capstone was a paper titled “Transmen and Suicide: Unique Contributors to a Disproportionately High Suicide Attempt Rate.” This involved both an in-depth literature review of trans research and theory as well as an independent collection and analysis of transman testimonies. The year after graduation was spent as a Lab Coordinator for the Sexual Orientation and Gender Identity: Health and Human Rights Lab at the University of Texas at Austin which does phenomenal sociological and psychological research on queer youth in particular. This is not to say that I am an expert, but rather to make it clear that I, too, have spent years researching the fraught topics of gender and sexuality.
Thank you for referring to my trans brothers as “notably sensitive and clever people.” We do try to use the unique empathy granted by being seen and treated as both women and men. Most of us grew up as girls and have been targeted by the misogyny and sexism that you reference; we try to use those experiences to inform our responses and opinions to societal issues. I, specifically, am going to use my lived experiences to respond to your essay. There are some points with which I agree and appreciate your recognition - freedom of speech, the importance of nuanced conversation, and the fact that both women and trans people are at disproportionate risk of violence and must be safeguarded. There are other points with which I take umbrage and will address one by one.
JKR: “It’s been clear to me for a while that the new trans activism is having (or is likely to have, if all its demands are met) a significant impact on many of the causes I support, because it’s pushing to erode the legal definition of sex and replace it with gender.”
Response: Let’s be clear: trans activists - at least the majority of us - are not trying to erase sex as a definition. Instead, we are asking that the parameters be reconsidered to make space for intersex people and who have biologically transitioned. Your points about the biological differences in treatments for MS are well taken. Ignoring intersex people and focusing on only the binary sexes male and female, you’re right. There are often sex differences in diseases and health disorders. But the problem is that we don’t always know what drives those differences; if they’re based on hormones, physical bodies, or something else entirely. Intersex and trans people, if they choose, now have the medical capability to change their hormones and physical bodies to the extent that they can be classified as male or female.
I’m not going to give you a full explanation on sex as an expression of levels of hormones, chromosomes, and physical organs. I’m sure you already know that both biological men and women have varying amounts of the same hormones, and that hormone replacement therapy can and does give trans men and women the hormonal levels that correspond to each definition. I have been taking testosterone for just under 2 years and, for all intents and purposes, have the chemistry of a biological man. In the same way, surgeries can and do affect physical biology and organ makeup, from removal or reconstruction of a penis or vagina to the removal of ovaries and uterus entirely.
This creates a gray area as to how to medically treat diseases like MS in trans people. We’re still learning, and I’ll be the first to admit that. What I can say is that there are many binary trans people who are not trying to replace legal definitions of sex with gender, but rather are trying to expand the legal definitions of sex to those who, for all intents and purposes, are biologically male or female.
JKR: “I’m concerned about the huge explosion in young women wishing to transition and also about the increasing numbers who seem to be detransitioning (returning to their original sex), because they regret taking steps that have, in some cases, altered their bodies irrevocably, and taken away their fertility. Some say they decided to transition after realising they were same-sex attracted, and that transitioning was partly driven by homophobia, either in society or in their families.”
Response: I would very much like to see the studies that you are referencing in this “huge explosion” of detransitioning individuals. If you’re referencing the article by Lisa Littman, it is definitely worth noting that her study was a) descriptive rather than empirical and b) based on the testimonials of parents and not the actual trans youth.
According to a different and arguably more experienced researcher, Dr. Johanna Olsen, regret and detransitioning as you talk about it are extremely rare. I encourage you to watch her video below and read over some of the other research she is and has been doing.
Even if we were to listen to descriptive research such as Littman’s and assume that there are people who wish to detransition, the lack of fertility you’re talking about is not universal and, as with people assigned female at birth, varies. According to recent studies, trans men who wish to reproduce biologically can take a break from testosterone while carrying their children and resume afterwards. So far, there are no negative side effects for the children of transmen.
What should also be considered, especially in youth, is that hormone blockers are entirely reversible. But puberty is not. When trans children are put on hormone blockers, they are essentially delaying permanent puberty and taking time to examine whether it’s right for them. Access to medical care such as hormone blockers are essential to trans youth because it does give them time to figure out their identity before going through the male or female puberty that affects them.
I have not seen any cases of transition driven by homophobia, but would like to note that working to make parents less homophobic and transphobic seems to be a better use of time than arguing against the right of many trans youth who do need access to medical intervention.
JKR: “The argument of many current trans activists is that if you don’t let a gender dysphoric teenager transition, they will kill themselves. In an article explaining why he resigned from the Tavistock (an NHS gender clinic in England) psychiatrist Marcus Evans stated that claims that children will kill themselves if not permitted to transition do not ‘align substantially with any robust data or studies in this area. Nor do they align with the cases I have encountered over decades as a psychotherapist.’”
Response: This point is one of the more frustrating parts of your article because it is using one medical professional’s opinion to ignore a horrifying truth. Trans adults and youths experience suicidality and depression at staggering rates. While I cannot comment on studies in the UK, here in the US the lifetime suicide ideation rates for trans adults is 81.7%. The attempt rate is 40.4%, almost 10x the national average of 4.6%.
And those are just the statistics of the people who survived long enough to participate in the study. Denying the real threat of suicidality in trans youth is not only saddening - it is actively harmful.
JKR: “The allure of escaping womanhood would have been huge. I struggled with severe OCD as a teenager. If I’d found community and sympathy online that I couldn’t find in my immediate environment, I believe I could have been persuaded to turn myself into the son my father had openly said he’d have preferred.”
Response: This is one of the most frequent arguments I see for people denying trans men their identity. My own mother has suggested that I transitioned to escape sexism. To this, I respond that choosing to transition does not provide an escape to discrimination and harrassment. I was well aware, when choosing to come out and transition, of the statistics of discrimination I was entering. I was well aware that it might mean the loss of my athletic scholarship, the dismissal of the team of sisters that I played on, It was not a matter of escaping sexism, but rather a matter of being my most authentic self. Even if you dismiss my own personal experience, I would point to the trans women who actively transition and give up their male privilege in exchange for the trials and tribulations of womanhood. Either way, I can assure you that the suicidality trans people experience makes the “choice” to transition no more of a choice than raising your hands because a gun is pointed at your head.
JKR: “ I want to be very clear here: I know transition will be a solution for some gender dysphoric people, although I’m also aware through extensive research that studies have consistently shown that between 60-90% of gender dysphoric teens will grow out of their dysphoria”
Response: I appreciate your recognition of our reality! I would love to see the studies that present a 30% difference. In my experience, those of us that lived long enough to see adulthood have not grown out of dysphoria, even if we’ve learned coping strategies to make it bearable. And again, hormone blockers for teens allow the opportunity for them to grow however they need to without permanent changes being made.
JKR: “So I want trans women to be safe. At the same time, I do not want to make natal girls and women less safe. When you throw open the doors of bathrooms and changing rooms to any man who believes or feels he’s a woman – and, as I’ve said, gender confirmation certificates may now be granted without any need for surgery or hormones – then you open the door to any and all men who wish to come inside.”
Response: Once again I cannot speak to the politics or legislation of the UK. What I can say is that “bathroom bans” on trans people that require us to use the fitting room/bathroom/locker room of the sex we were assigned at birth lead to significant sexual and physical assault on trans people, which already face a disproportionate risk (as you mentioned). I personally have been fortunate enough to have not been physically assaulted when I was trying to go to the bathroom, but have been harassed in both mens and womens bathrooms (which I varied between during my transition, depending on how well I thought I was passing). Many of my friends are not as lucky.
JKR: “But, as many women have said before me, ‘woman’ is not a costume. ‘Woman’ is not an idea in a man’s head. ‘Woman’ is not a pink brain, a liking for Jimmy Choos or any of the other sexist ideas now somehow touted as progressive.”
Response: The implication that trans women - who are literally dying to be acknowledged as women - putting on a “costume” is flagrantly offensive. I am choosing to believe that you did not intend this implication and instead are confusing sex and gender. In which case,would refer you to the seminal work Gender Trouble: Feminism and the Subversion of Identity by Judith Butler. According to her, gender is literally a performance that one chooses to express. Transwomen define their gender and femininity as individuals, and do not choose to go through the grueling process of changing their biological sex because they like Jimmy Choos. The gender ‘woman’ is not a “pink brain” but rather an identity that can be inwardly cultivated and outwardly expressed. The sex ‘woman’ or female is an amalgamation of complex physiological systems that, as we’ve already discussed, can be altered.
JKR: “I refuse to bow down to a movement...”
Response: There is undeniably a movement, a “cancel culture” that dismisses nuanced conversation. I, like you, am concerned about the erosion of free speech and the expression of alternative points of view in nuanced discussions such as this one. But this movement is not specific to trans people and should not be described as such. Most trans activists and researchers that I know are not asking you to “bow down.” We’re asking you to come to the table and have an open mind. We’re asking you to use your huge platform to help trans people (as you clearly want to) without harming them (as you clearly have).
JKR: “...that I believe is doing demonstrable harm in seeking to erode ‘woman’ as a political and biological class and offering cover to predators like few before it.”
Response: This is the crux of the “TERF wars”. The refusal to accept trans women as women. To this, I would simply say: Acknowledging that trans women are women is not the erosion of a political and biological class. It is strengthening those classes by accepting the women who, despite all threats of assault or death, stand by their identity and celebrate womanhood.
#long post#essay#jk rowling#response#harry potter#transmen#ftm#mtf#transphobia#transwomen#trans#LGBT#terf#terf wars
5 notes
·
View notes
Text
ATTENTION, AWARENESS, AND LEARNING [sources: click, click, click, click, click]
the original plan was to have this as the initial section of my meta about Bucky’s memory (what he remembers vs. what he forgot, essentially) but: 1) i realized that was going to be a massive thing and splitting it might be in my best interest, and 2) memory does not exist without learning and learning does not exist without attention so, really, exploring each step individually might not be a bad idea after all. other than the linked sources, this meta will also build on what i have already discussed regarding the process of brainwashing that underlies the functioning of the Winter Soldier: here. on the other hand, whereas the topic of this meta is not memory, all of these cognitive processes are deeply enmeshed and therefore do not exist as categorically separated as this text may make them look like — these are conceptual separations only (despite the little fancy numbered topics, i end up talking of attention + learning + memory all at the same time), and a degree of overlap will always exist.
1. ATTENTION starting with the concept that we cannot learn about what we do not pay attention to, then it makes all the sense to ask: what does the Winter Soldier pay attention to? and the answer is: to whatever HYDRA commands him to. the hypnosis protocols (explored in the brainwashing meta) have the purpose, exactly, to fixate his attention on fulfilling the mission goal(s), whatever they may be, at expense of everything else — which, in turn, means that if, he’s not paying attention to, say, his surroundings and the people who are with him, he won’t be able to learn about, and posteriorly remember, this sort of details.
this brings me to the “i remember all of them” line in “Captain America: Civil War” — which Sebastian Stan himself has already stated was something Bucky said in the spur of the moment, something that Tony wanted to hear while having him literally in a choke-hold. no, he doesn’t remember all of them, much as this is a heartbreaking line with big cinematic impact. i personally headcanon that Bucky remembers Howard Stark, based on the fact that this is someone he met and got to know in the 40s — which is information that comes from the long-term memory, not equally affected by the mind wiping + cryostasis as short-term memory (which i shall explore in more detail in the future memory meta). even so, it’s not clear recollection — more like remembering what that particular mission was about, and remembering faces that, back then, the Soldier could not recognize but that, in retrospect, he’s able to make sense of. i also headcanon that a similar logic applies to the mission referenced in “Captain America: The Winter Soldier”, where Natasha talks of how he shot the man she was guarding through her, and it applies as well to the highway scene in the same movie. for these three missions, long-term knowledge and/or an intense emotional tone allowed for the Soldier’s attention to be highly focused on Howard/ Natasha/ Steve respectively, spanning beyond what the hypnosis protocol dictates. nonetheless, memories of these missions are fragmented and he remembers the associated emotions that these three persons evoked, more than any coherent dialogue or details of that moment.
in regard to the other targets/ missions, Bucky remembers conceptual information essentially (e.g., the target’s name, what day it was, what the mission briefing required him to do), considering that these targets held no previous meaning to him. because these conceptual details were what his attention was focused on. so, for example, he may be able to remember who was the target assassinated on a specific day and in which way this was done, but he won’t be able to remember what the person was wearing or what their face looked like or who were the handlers for that mission. not only he didn’t pay attention to these details but they would have been wiped in post-mission, anyway. the only memory traces that stay are those which already existed and those that HYDRA allowed him to effectively learn — and these, again, are reduced to information that was necessary for carrying out the mission successfully.
what consequences does all of this have, once Bucky breaks free from HYDRA? first, what he was allowed to pay attention to is what he is now able to remember, as discussed. and then, it means that his attention span undergoes a big change as soon as it’s “free”, so to speak. now he doesn’t have anyone dictating what to pay attention to — and, whereas this is a good thing, it also implies that the world is suddenly perceived as chaotic. because now he’s suddenly aware of everything that the Soldier never noticed — he perceives faces and colors and shapes and sensations and all else, and this can easily get overwhelming (even the good things).
again, i will complement/ explore this better in the memory meta, but this is why, in post-HYDRA, Bucky struggles with actions that require short-term and working memory — not only because these brain areas were affected by the wiping, but because his span of attention itself is all over the place. not in the sense of attention deficit disorder, per se, but because there is so much stimulation happening at the same time that he isn’t used at all to be aware of (and now add to this the fact that he is also a man out of his time, as much as Steve, and there is so much to learn anew in this modern world). depending on his general state of mind, his coping may vary from dissociation (just downright shut down everything because he currently has no mental energy to process any of it, so he withdraws instead) to actively trying to process the information he’s being given (and try to understand and make sense of it, and currently being mentally stable enough to pay attention and learn and keep up with all of it).
nonetheless, this process will frequently be a bumpy one. for example, he will try to pay attention to everything and, in the end, retain none of it exactly because he was so scattered, or he will (consciously or not) direct his attention to one thing only and everything else that is going on will go completely over his head. with this said, and roleplay-wise, you should expect things like your muse having to repeat something before he actually gets it and commits it to memory, or that he won’t be able to follow what your muse is talking about if there is a lot being conveyed in a short period of time (because, by the time your muse finishes, he’s already forgotten what was said at the start, or, instead, he focused on what was said first and didn’t follow anything else), or that your muse expects him to be paying attention but in the meantime something else captured his interest and, by the time your muse realizes, Bucky has gone over to the other side of the street to pet this cute cat while leaving your muse talking alone. exceptions to this are situations that are an actual mission or resembling of it, aka situations with a very well defined goal and where he has very clear instructions to adhere to — exactly because this is what he was trained, for 70 years, to focus on and pay attention to.
2. AWARENESS again. awareness and attention are two conceptually different things — but with a great degree of overlapping and interdependence. awareness, in particular, refers to directly knowing and perceiving, feeling or being cognizant of events. it’s the state of being conscious of something. so… is it possible to pay attention without being aware? technically yes, and i see this as a particularity of the Winter Soldier, actually. because if you ask him, during a mission: what is your target doing right now? — he knows, he’ll tell you, because he is paying attention to said target. but is he aware of what he’s doing, as in, does he realize he’s about to kill a human being and what this implies at every level? he isn’t. he’s doing it because he was commanded to do it, and weapons don’t question the hand that pulls the trigger. this is possibly the most drastic change that happens in post-HYDRA, because he finally becomes aware — finally regains a sense of being conscious of his actions (and shoutout to Sebastian’s terrific acting at the end of that helicarrier scene in CA:TWS, because with his eyes only he can so clearly depict this change — this moment when the Soldier becomes aware of what he is doing to Steve). and let me redirect to another of my previous metas, re: the dehumanization of the Winter Soldier, because this shift in awareness relies entirely on the human being vs. weapon/asset mindsets: here.
in post-HYDRA, then, this comes laced with everything i already discussed about attention. the increased capacity to pay attention to the world, once the hypnosis protocol is discontinued, comes hand-in-hand with this rise in awareness — paying attention to the sunlight like you never did before, and being aware that sunlight feels warm on your skin and being aware that, in turn, this is a pleasant sensation. unlike attention, however, gaining awareness brings Bucky a whole lot more demons to deal with — because it makes him conscious of what the Soldier has done and what it implies and, at the same time, it makes him conscious of what was done to him — and this dichotomy fuels a very toxic, very difficult to undo, cycle of guilt/shame vs. paranoia. on the other hand, whereas i don’t want to go into much detail about empathy right now, this also allows him to grow very compassionate and very mindful of his actions — because he knows what the Soldier is capable of, and because he never wants any of it to happen again as far as he can help it. which is why, for example, in my writing post- CA:TWS, a pervasive theme is that Bucky is way more scared of the harm that he can potentially do to others than what can be done to him.
and a smol extra note, once more based on Seb’s acting because this man’s body language is a heavens-sent: despite everything stated above, i don’t personally believe that the Winter Soldier is completely unaware of what he’s doing. this is speculative, obviously, and no more than my own headcanon, but i really don’t think he is. he’s trained to not question it, and most of the time he doesn’t actively question it (possibly, the only time this happens is the whole “the man on the bridge” moment), but he’s not completely ruthless either — on the contrary. the highway scene in CA:TWS is a perfect example, because we can see how uncaring he is re: his own well-being (hopping off the rail like he does and landing on that car like a ton of bricks, with zero care for his own body), but we don’t see him shooting/massacring any civilians even though he so easily could. he’s solely focused on Black Widow at that point and, yes, this is likely because it’s what the hypnosis protocol dictates his attention be given to, but i personally believe it also comes out of an unconscious desire to do no harm — that belongs not to the Soldier, but to James Buchanan Barnes. one more topic for a future meta!
3. LEARNING so… i actually feel like there isn’t much left to say about this topic in particular, given how i have already been tapping at it during the two previous ones. the Winter Soldier’s learning relies on two big strategies: classical/ Pavlovian conditioning and operant conditioning (both of which i have explored in the brainwashing meta). and a whole lot of repetition, till he learns what HYDRA wants him to learn — and anything else he casually/ autonomously learns and that is considered unnecessary is taken care of via mind wiping. the biggest implication of this is that, in post-HYDRA, Bucky is a bit like a child learning about the world for the first time. not only he’s in a modern world where so much is new and he doesn’t know about it, but his learning process relies basically only in association of stimuli + punishment or reinforcement. in post-HYDRA, he starts doing trial-and-error in an autonomous manner, he starts doing vicarious learning (i.e., learning through observing other people), he starts learning things by accident in the sense that he wasn’t even trying to but it happened anyway, he starts learning by imitating and doing what others do.
which brings me to another roleplay thing, and one that i often joke about but that, in fact, happens for real — the fact that all this makes Bucky rather gullible. for example, he will see some modern contraption that he never got to see/use before and he logically won’t have a clue about it, and he will likely believe what he’s told about it — because he has no other reference, because he trusts the person who’s telling him this, because this is how he’s learned things for the past decades. he’s used to being taught, more than to learn on his own, and he’s used to the things he’s taught being the only truth that matters, in typical HYDRA fashion. the difference is that he now is aware of what he’s being told, so if you tell him “go and assassinate the prime-minister” he will obviously know what this is about and why this isn’t a good idea, to say it mildly. also, this doesn’t make him completely oblivious, in the sense of believing everything he’s told blindly and without a sense of criticism — because, yes, he’s got a shitty memory but he can sill use logic and rationality — so if you tell him to cook a sundae in the microwaves he’ll tell you to go screw yourself, because sundae is ice cream and ice cream melts. on the other hand, popular references are the thing that confuse him the most and that are hardest to learn, exactly because they don’t carry this inherent sense of concrete logic — so if you tell him that YEET! is the new way to say good morning nowadays, chances are he’ll start telling it to everyone from there on until he’s taught properly about it.
to conclude, i just wanna mention yet again the connection with attention — because the limitations i have already discussed obviously have an impact on Bucky’s capacity to learn, in post-HYDRA. generally speaking, this capacity is reduced when compared to the Soldier — not only due to brain damage, but also because the Soldier was exceptionally prepared, through hypnosis, to learn any minimal details deemed necessary (for example, this is how he learned the 16 new languages that add to English and German that he already knew --- this specific headcanon: here). so, it’s not like he now sucks at learning, rather it was the Soldier that was (forced to be) way above the standard level. now in normal conditions, this capacity is more scattered and it fluctuates along with his span of attention — which, in turn, fluctuates along with his mental health status. but he is a curious person and he wants to improve and to learn more, either on his own or with help, and this intrinsic motivation is very important when it comes to adapting to a new life/new world.
5 notes
·
View notes
Text
Examination of Anomalous World Experience (EAWE)
The EAWE is the companion interview to the EASE that focuses on the person's experiences with the world, rather than with the self. There are 6 domains: Space and objects, which deals with the person's experience with space and physical objects, with disorders including hallucinations, distortions of spatial relationships, and experiences of seeing the same object in multiple ways at the same time (called "contamination" on the Rorschach test); time and events, which deals with the person's experience with time, with disorders involving time speeding up or slowing down, time breaking up or becoming fragmented, and constant anticipation of something major about to happen; other persons, which deals with the person's experience of other people, with disorders including disruptions of the sense of ego boundaries with other people, referential ideation based on actions or words by other people, and loss or lack of the ability to naturally understand social situations and social cues leading to attempts to compensate through increased focus or concentration; language, which deals with reduced fluency and disruption of prose in one's native language, distortions in the person's expression which causes others to misunderstand the person, problems with concrete and abstract concepts, and distraction by individual words and phrases leading to the person having difficulty following what they are reading or listening to; atmosphere, which deals with the person's overall feeling-state of the world, with disorders including derealisation (particularly The Truman Show-style derealisation), objects no longer having normal meaning, hyper-awareness of things that normally stay in the background of awareness, apophanous mood, and a sense of radical changes in the very structure of the universe itself; and existential orientation, which deals with radical changes in a person's worldview, dealing with such things as rejecting society's conventions and rules, being extremely open to believing new ideas, and grandiosity which involves the person considering others to be inferior, like insects compared to them.
Domain 1: Space and objects
Abnormal intensity or persistence of visual perceptions: Visual stimuli appear more or less intense or take longer to leave perception after ending.
Increase in intensity of visual perceptions:* Visual stimuli seem more intense, such as light being brighter or colours stronger.
Decrease in intensity of visual perceptions:* Visual stimuli seem less intense.
Recurrence or prolongation of visual stimuli: Even after visual stimuli are gone, person continues to see them. Also called palinopsia.
Blindness or partial blindness: Vision is experienced as being blurry or partially or wholly absent.
Blurred vision.*
Partial seeing: Person sees only part of an object.
Transitory blindness: Visual field is experienced as either partly or entirely absent.
Disturbances involving verticality (accuracy) of visual perceptions:* Mis-seeing objects or perceiving visual stimuli that is actually absent.
Visual illusions:* Person mis-sees something, mistaking it for something else.
Visual hallucinations:* Person experiences seeing something when nothing is there. Can seem only partially external.
Visual pseudohallucinations:* Like visual hallucinations, but person while experiencing it recognizes its lack of basis in reality.
Visual fragmentation: Objects or scenes appear broken up.
Object fragmentation: Cannot perceive objects as a whole.
Break-up of a scene: The world becomes fragmented, with different things appearing disconnected or unrelated to one another.
Captivation of attention by isolated details: Person attracted to certain details as if spellbound.
Disorganisation or disturbed object stability: Visual perception of things becomes fluid and unstable.
Disorganised object contours: Object contours are distorted.
Loss of perceptual stability (fluidity or contamination): Things seem to change their form or nature before the person's very eyes. Multiple forms of a single object may be perceived simultaneously in the same place, like a "photographic double exposure".
Changes in quality, size, or shape of visual perceptions:
Changes in color of visual perceptions: Things seem to be a different color from what they normally are.
Micropsia/macropsia: Things seem bigger or smaller than they actually are.
Dysmegalopsia: Things seem bigger on one side and smaller on the other than they actually are.
Metamorphopsia: Objects have a different but stable form than how they actually are.
Other distortions.
Disturbances of perceptual distance or object juxtaposition: Distances and/or relative positioning of objects to each other is distored.
Objects seem closer or farther away:* Objects are closer or farther than they appear.
Disturbance of relative spatial relationship (juxtaposition) of objects: The relative positioning of objects is distorted, including in the perception of 2 objects one of which is closer, with the closer one appearing farther away and the farther away one appearing closer. May have difficulty determining what is in the background or foreground.
General disturbances in estimation of distance: Person struggles to estimate how far away they are from something.
Distorted experiences of space: Space itself seems distorted.
Diminished perspectival orientation: Experiences space as isotropic, sees the world as if standing from nowhere in particular or everywhere at once.
Loss of topographical orientation: Feels disoriented in familiar places.
Loss of spatial integrity or structure: Feels as if space is inconsistent, as if pouring a jug of water down on the floor below results in the water falling onto the floor above or as if a path leads somewhere that should be geometrically impossible.
Loss of dimensionality: Perceives the world in only 2 dimensions.
Experience of infinite space: Person is overwhelmed by the magnitude of space in their location.
Figure/ground reversal: Person sees the space between objects rather than the objects themselves.
Affective experience of space:* Space feels threatening or strange, takes on a negative feel.
Abnormal intensity or persistence of auditory perceptions: Sounds seem more or less intense or last longer than they should.
Increases in intensity of auditory perceptions:* Sounds seem louder or more intense.
Decreases in intensity of auditory perceptions:* Sounds seem quieter or less intense.
Heightened awareness of background auditory sensations: Overly aware of sounds that should remain in the background, that are less relevant than other more important sounds.
Recurrence or prolongation of auditory stimuli: Sounds last longer than they should or recur.
Disturbances involving veridicality (accuracy) of auditory perceptions:* Mis-hearing sounds or hearing sounds that aren't there.
Auditory illusions:* Mis-hears sounds as something else.
Auditory hallucinations:* Hears sounds that aren't there, in a way that seems at least somewhat external to the person.
Auditory pseudohallucinations:* Like auditory hallucinations, but person is aware during the experience that they are false.
Other changes in quality of auditory perceptions: Experiences distortions in pitch, timbre, or other qualities of some or all sounds.
Problems localizing sounds: Has trouble pinpointing where sounds are coming from.
Disturbances of other senses:* Other senses, such as smell, taste, or touch, experience distortions.
Tactile disturbance:* Distortions in the sense of touch.
Gustatory disturbance:* Distortions in the sense of taste.
Olfactory disturbance:* Distortions in the sense of smell.
Synesthesia or abnormal concomitant perception:* Stimulus in one sense brings in involvement of another sense.
Splitting-off or isolation of sensory perceptions: Stimulus is perceived as having nothing to do with what is producing the stimulus, like another person's voice seems to have nothing to do with the person who is speaking.
Disturbances in recognising or identifying an object of perception: Fails to recognise what they are seeing or hearing, even when it is familiar to them.
Loss of boundaries with, or demarcation from, the physical world: Person experiences difficulty determining where their body ends and the rest of the world begins.
Domain 2: Time and events
Time or movements appear to change speed: This does not only occur when a person is bored, excited, or is engaged in activity.
Time or movements seem speeded up.*
Time or movements seem slowed down.*
Time or movements seem (somehow) both speeded up and slowed down.
Discrepancy between internal and external time:* Experiences discrepancy between the time that passes for their own actions versus the time for the rest of the world.
Internal time seems slower than external time:* Feels as if they are moving or thinking very slowly relative to the rest of the world.
Internal time seems faster than external time:* Feels as if they are moving or thinking much faster than others and the rest of the world.
Disruption of dynamic organisation of time: Seems like time no longer flows like it should. Here, there is a disruption of the unity of the present moment with the retention (immediate previous moment, "primary remembrance") and the protention (immediate next moment, "anticipation"), as described by philosopher Edmund Husserl.
Time feels as though completely stopped, static, infinite, disappeared: Feels as if time has stopped or ceased to exist.
Time as disjointed or fragmented: Each moment feels disconnected from the last and the next, as if time itself has become staccato, just a sequence of photographs, each having nothing to do with the next or last one.
Disorientation in time: Person becomes confused about the passage of time, with difficulty understanding how time flows and when to engage in events, and even what time of day it is.
Feeling limited to or isolated in the present moment: Person feels as if they newly come into being as a wholly different person with each passing moment of time.
Various bizarre experiences of time: Feels as if time is going backward, as if they are stuck in a Groundhog Day loop, as if they control time, as if they are present in multiple periods of time at once, or other bizarre experiences.
Disturbed anticipation: Disturbance of the expectation of the immediate next moment in time.
Perpetual anticipation: Constantly feels as if something very big is imminent, right about to happen. Called also ante festum experience or trema ("stage fright").
Constant surprise due to inability to anticipate future events: Is constantly surprised by mundane events that would normally be expected immediately beforehand, due to the inability to anticipate.
Feeling that "anything could happen": Feeling that literally anything, from the probable through the highly unlikely to the impossible, could happen, while not caring what that is.
Protention (future directedness) collapses: Feels as if they cannot move into the imminent next moments in a smooth, flowing way.
Disturbed awareness of the expected future:* The conception of the future beyond the imminent is distorted or feared in some way.
Future seems nonexistent.*
Future seems unimportant or irrelevant.*
Future seems threatening.*
Premonitions.*
Disturbed experiences of memories or of the past:
Past seems cut-off.*
Past seems vague or obscure.*
Past disappears or seems non-existent.*
Past seems accelerated:* Feels as if the memories are all condensed into a single moment.
Past seems slower:* Feels as if memories are all drawn out and elongated in time.
Intrusiveness of the past:* The past seems to limit the person, what they can do.
Erosion of distinction between past and present:* Confused about whether the person is remembering something or if they're actually doing something right now.
Past seems disjointed: What happened in the past seems all out of order, all disconnected from each other, or otherwise disjointed.
Domain 3: Other persons
Lack of social understanding or interpersonal attunement (hypoattunement): Person feels they cannot smoothly engage with other people at all; may feel like they must study and follow explicit rules to interact successfully with other people.
Loss of social common sense: Feels they cannot naturally grasp what other people do or how the conversation has gone.
Bodily/proprioceptive loss of attunement: Feels they are outward and cannot time their mannerisms and other actions properly (e.g. may not know when to begin speaking after another person has finished, or when to greet a person as they walk past them).
Specific difficulty understanding non-verbal communication: Has difficulty reading body language, tone of voice, and other forms of non-verbal communication.
Sense of remoteness from others:* Feels cut off from other people.
Alienated strategies for understanding others: Feels they have to engage in intellectual-style analysis of social situations to understand what they mean and what to do.
Alienated scrutinising of others' behaviour: Aware they tend to analyze social situations to know what they mean, like a zoologist out in the field doing in situ study of animals.
Algorithmic approach to social understanding/interaction: Person attempts to create algorithms, a set of formal rules, to use to guide them in social situations.
Sense of inferiority, criticism, or mistrust in relation to others:* Tends to feel threatened and criticized in social situations, making it hard to interact comfortably.
Feelings of self-consciousness, self-criticism:* Tends to be overly aware of flaws in their appearance, interaction, etc.
Feelings of social paranoia or social anxiety:* Feels people they're interacting with or are around them are constantly focusing on and judging them.
Pervasive mistrust of others:* Tends to feel other people are out to "get" them.
Torment or distress due to generalised social insecurity: Mere presence of others feels extremely burdensome and unbearable, as if by their very presence they endanger the person's cold self.
Interference by voices:* Feels like voices prevent them from interacting normally with people.
Disturbance of self-other demarcation: Feels like they have a hard time telling what thoughts, ideas, actions, sayings are in them, and what are in other people.
Hyperattunement: Feels like they can read minds.
Unusual influence over others: Feels like they can mind control other people.
Pathological openness: Feels like their innermost thoughts and feelings are open to being read by others.
Experiences of being controlled: Feels like they're being mind-controlled.
Merging or fluid psychological boundaries: They feel mixed up or confuse their thoughts and feelings with those of other people. May feel like there is no clear boundary between themselves and other people.
Universal merging with others:* Feels like there are no individuals, but everyone is part of the same hive mind or other collective consciousness.
Uncertain personal identity/attitudes:* Feels confused about their identity when around others.
Uncertain physical boundaries: Has difficulty telling where their body ends and other people's bodies begin.
Experience of being imitated: Feels like other people are imitating them deliberately to mess with them or make fun of them, in a way that seems strange to them.
Difficulties with the gaze: Has trouble with eye contact
Intrusiveness of the gaze of the other: Feels like other people's gazes are very intrusive and make them uncomfortable, often leading to avoidance of eye contact.
Feeling of exposure through one's own eyes: Feels like eye contact exposes their innermost thoughts and feelings to the other person.
Intrusiveness of one's own gaze: Feels like their own gaze is intrusive and unbearable for others.
Dehumanisation of the eyes of others: When making eye contact, the other person does not seem to be human or alive, with their eyes and body parts being seen as like inanimate objects.
Eyes as cosmic portals: Feels like the eyes of others (or one's own in the mirror) are windows into another world or dimension.
Unspecific uneasiness with gaze: Feels uneasy with eye contact without specifying the reason.
Depersonalisation of others: Depersonalisation, but of other people rather than oneself.
People seem dead:* Feels as if other people are dead (even though they're alive, up and moving around).
People seem unreal/false/illusory: Other people seem like they don't really exist or are fraudulent copies of themselves, without objective reality.
People seem mechanical: Other people seem like they are mere robots without a soul.
Persons dominated by a single characteristic: Focuses on a single characteristic of other people, and feels as if it defines the other person's entire being, like the other person is nothing more than that characteristic.
Heightened intensity, aliveness, or reality of others:* People seem more alive and energetic than normal, which feels fishy.
Changes in quality or tone of others' appearance: Other people look or seem strangely different from how they normally are.
People seem familiar in a strange way: Of people they've never met before, it strangely feels like they know the other person from somewhere. Like deja vu, but with people.
People seem unfamiliar in a strange way: Of people they know well, it strangely feels like they don't know the other person at all. Like Jamais vu, but with people.
People seem disgusied:* Feels like other people aren't actually those other people, but are people disguised as those other people.
People seem threatening in a strange way:* There is something about other people that makes it seem like they are a threat.
General/unspecified changes in the physical appearance of others: Something about how the other person looks, like maybe their eyes or face, seems strangely different from before.
People seem as if communicating something special or unusual (beyond the obvious): Other people seem to be dropping hints intended for the person, with the intent of the other people's speech being very different from what is said.
Paranoid significance:* The hint seems to express dislike or threats toward the person.
Grandiose significance:* The hint seems to signify the person's superiority or special powers.
Metaphysical significance: The hint seems to signify impending Doomsday or perhaps a cataclysm that has fundamentally altered the universe.
Unknown/unsalatable significance: The person cannot express the meaning of the hint.
Anomalous behavior/attitudinal responses to others: Person is aware they are acting strangely differently toward other people, often due to paranoia or not understanding social situations like they used to.
Active withdrawal:* Person tends to want to be alone and shut others out.
Oppositional/rebellious behaviour:* Person tends to want to act counter to other people.
Social disinhibition:* Person aware they disregard social norms when they interact.
Compulsive interpersonal harmony:* The person feels very eager to please and will do anything to avoid conflict with others.
Extreme compliance: Automatic obedience or imitation of others, echopraxia.
Compulsive clownery/entertainment of others: Feels like they must always crack jokes or clown around, in a way that turns out wooden or stilted to other people.
Domain 4: Language
Basic disruptions of standard verbal comprehension: Difficulty comprehending speech or writings.
Meaning/sound dissociation: Difficulty putting the representations of words with their meanings when heard or read.
Distraction via semantic possibilities: Gets caught up on all the different senses of a word or a statement that was just heard or read.
Distraction by individual words: Gets focused on individual words instead of the message as a whole.
Unspecified difficulty understanding: It's difficult to understand what they're hearing or reading.
Difficulty understanding emotional/expressive aspects of speech:* Has a hard time with understanding the intonations in what people say.
Specific changes in standard feel or meaning of words: Becomes focused on words because they feel different than they did before.
Focus on sound or appearance of words/phrases:* Very aware of how words sound or appear.
Unconventional semantic determination via signifier or fragments of words: Determines words' meanings by how they or parts of them look, rather than by the conventional meaning.
Words seem arbitrary/absurd: Is often so distracted by how arbitrary words seem that they do not attend to conversations
Words or language seems alive: Words take on a life of their own or feel like physical objects
Egocentric linguistic reference: Self-referencing ideas coming from the specific words or grammar that a person uses, but NOT the content of what they're saying.
Unconventional word choice, grammar, tone, or cryptic discourse: Says things in an unusual manner that often confuses people, which may be at least somewhat willful.
Cryptic, telegraphic, or ungrammatical speech: Speaks in a cryptic manner or using sentences structures that violate the grammar of the language they're speaking (even though they are a native speaker, for example), which may be experienced as intentional.
Stock words: Tends to overuse a certain few words or phrases to the point where they acquire many meanings beyond the conventional, causing their speech to feel stilted.
Made-up words (neologisms) or unconventional usage: Aware of using made-up words or using words in ways that differ greatly from their meanings.
Mannerisms and stilted speech: Tends to use very formal registers to say things in situations that would normally call for more casual speech.
Disturbed fluency: Has a hard time expressing self using language.
Unavailability of words: Cannot find the right words.
Unfocused or disorganised thoughts preclude verbal expression: Aware they have difficulty speaking because they cannot get their thoughts "straight", that is, their thinking has become so digressive or otherwise difficult to understand that they cannot express themselves.
General discordance between the intended expression and the expressed: Aware of inability to express themselves in a way that accurately expresses what they meant to say; little things in the expression keep being off to the point the listener or reader may be left with a different impression.
Disturbed relevance: Aware of having a hard time remaining on a single line of thought while talking or writing.
Derailment:* Aware that they have a tendency to lose track of what they're saying or writing.
Tangential responding: Aware that they make off-topic answers to questions.
Disturbance of linguistic engagement or purposefulness: Aware they speak in such a strange way that they are not engaging.
Aprosody (lack of emotional intonation):* Aware their speech lacks the normal intonation.
Echolalia: Feels a need to repeat what the other person says.
Speech feels autonomous: Feels like they are not in control of their speaking or writing
Anomalous experience of the abstract and the concrete: Has difficulty using the abstract and the concrete appropriately
Difficulty with or dislike of abstract concepts.
Abstract rendered in unusually concrete terms.
Specific or concrete meanings rendered in unusually abstract or general terminology.
Hyperabstract or vague discourse.
Ineffability; inability of language to describe or express (may include temptation to remain silent): Feels language cannot fully express what they mean to say.
Language inadequate to express unusual circumstances:* Feels their experiences are so unusual language becomes inadequate to describe them.
General feeling of the inadequacy of the language: Feels language is inadequate to describe even normal experiences, or otherwise sees the use of language as a waste of time.
Alienation from self-description: When they provide a narrative of one's life, they have difficulty with even recognising the person back them as themselves.
Domain 5: Atmosphere
Derealisation of the world: Sense of disconnection or unreality of the world
Remoteness or barrier (plate-glass feeling):* Feels cut off from the world.
Decreased intensity or substantiality:* The world seems flat.
Deanimation:* The world seems lifeless.
Falseness: The whole world feels like it is a stage.
Loss of enticement quality:* Nothing has any appeal.
Static quality, stillness, or morbid intellectualism: Looks at the world in a very static or geometric way.
Nonspecific/other derealisation* The world feels strange in some way.
Loss of affordances: Objects and events no longer have their normal meaning and are seen simply as fixtures on the world.
Inanimate things seem alive or intentional.*
Heightened intensity/hyperrealization:* The world feels somehow more alive, colorful, and intense than normal.
Deja vu experiences: Things feel familiar somehow or like they've happened before.
Jamais vu experiences: The familiar becomes unfamiliar and novel.
Perplexity: Reality becomes confusing
Confusion of realms: Difficulty distinguishing the internal, mental realm and the physical realm.
Unreal interferes: Delusions or imaginations interfere with the ability to live in the world.
World experienced as incoherent, disoriented: The world is no longer a fixed stable place of meaning, but has become confusing and incoherent.
Perplexing hyperawareness of tacit dimension: Things that would normally stay in the background of perception come to the foreground and are the focus of attention.
Anomalous manner of ascribing or perceiving meaning: The way the person derives meaning from things changes greatly
Meaning imposed on object by subject: Person tends to give their own idiosyncratic meaning to things
Meaning inherent in the object itself: The idiosyncratic meaning is perceived as soon as the object comes into perspective and is seen as intrinsic to the object.
Proliferation of meanings from the object: Perceiving the object causes an uncontrollable emergence of associations, that is, things that it reminds the person of.
Anomalous forms of meaning: Meaning given to objects tend to be very atypical, often in terms of the concrete and the abstract.
Physical or literalist instantiation of abstract meaning: Things like thoughts and feelings become hard and concrete, like they were physical objects in themselves.
Anomalous classification: Tends to classify different things together using unusual criteria
Intensified awareness of patterns or trends:* Increased tendency to see patterns in things.
Anomalous sense of causal relationships: Cause and effect become distorted.
Actions or events seem controlled by an external force or will.
Actions or events seem predetermined or planned.
All-inclusive self-consciousness/ontological paranoia: Keeps feeling like they are being watched, focused on
Diminished ontological independence of experienced world/subjectivism: The world lacks independence from the mind.
Subjectivism/solipsism: The person feels like they are the only mind in the universe and that they are the ones who build up the universe and bring things and people into being.
Double bookkeeping: Aware of two different realities, one real and physical, the other imaginary and delusional.
Influencing physical reality: Feels like their thoughts control the world
Pseudomovements of objects/persons: When the person is moving, it feels like things or people are moving in conjunction with them.
Revelatory or pseudorelevatory (apophanous) mood: There is something different, special, or unusual about the world, but the person cannot grasp it, filling them with wonder.
Uncanny particularity: Something seems peculiar about various mundane happenings in the world, like they signify something bigger happening behind the scenes.
Self-referentiality: Sees mundane things as referring back to themselves in one of various ways, listed below.
Paranoid significance:* Suggests someone is trying to harm them.
Grandiose significance: Suggests they are superior or special in some way.
Metaphysical significance: Suggests the entire universe has radically changed, with the implication that it is the person who is response, or the message is directed specifically toward them.
Unknown/unsalatable significance: The nature of the significance is unknown.
Unspecifiable strangeness: Something has changed, the person can sense it, but they don't know exactly what.
Quasi-mystical experiences: Amazed at the very existence of the world.
Mystic union with the world:* Feels especially connected and united with the world, but not in a way that suggests their ego boundaries have been compromised.
Mere being: Struck by the sheer existence of everything.
Experiences of the end of the world: Feels like the world is ending.
Anomalies of mood or affect: The person has entered into an unusual mood state.
Emptiness, numbness, indifference, lack of spontaneous response to the world.*
Feeling of emotional/affective blockage (in the sense of being unable to express).*
Pervasive, nameless anxiety with fear of annihilation.*
Basic irritation, restlessness, anger (nonemotional dysphoria).*
Detached euphoria. Feels euphoric, but in a way that is very disconnected, different than the euphoria in a manic state which tends to involve increased energy and actions toward goals.
Despair, demoralization, hopelessness.*
Abnormalities of mood constancy.*
Mood or emotion is abnormally present:* Feels like the mood lasts beyond the events or thoughts that triggered it.
Mood or emotion is abnormally labile:* Mood keeps changing
Incongruity of mood or emotion.
Mood or emotion inappropriate to the current situation: Has moods or emotional reactions one would expect to what's going on.
Moods or emotions are mutually contradictory: Very high level of ambivalence about how they feel about things.
Domain 6: Existential orientation
Rejection of society or convention: The person generally chooses to live according to their rules in disregard of societal norms.
Disinclination for human society: Person rejects society and would prefer to live as a misfit.
Antagonomia: Tends to act in ways that directly oppose societal values.
Idionomia: Person feels radically unique.
Extreme indifference or openness: Person is very open to all possibilities in a way suggesting they are detached from the normal concerns of life.
Attitude of indifference, insouciance, lack of concern: Expresses "callous indifference" and that nothing really matters, in a way suggesting cold detachment, different from the way indifference is typically expressed in mood disorders where there is a strong emotional component.
Conceptual freedom/anything goes: Feels like anything could happen: as far as they're concerned, for example, apples could just as easily start falling up from trees rather than down.
Pervasive disbelief, skepticism, or curiosity are the obvious, taken-for-granted: Constant tendency to question everything that society takes for granted.
Absolute certitude: The person is absolutely sure about their unusual interpretation of the world, and does not believe that it will ever be refuted.
Feeling of being special or superior: Person feels superior or like they have a special role to play in the universe.
Feeling of extraordinary insight:* Person feels as if they and they alone understand the mysteries of the world.
Messianic duty:* Person feels as if they are a savior the world is depending on.
Intellectual/spiritual grandiosity (with invidious comparison): Person feels as if they are much much more highly advanced and evolved than all other people, whom they view as vastly inferior.
Impossible responsibility or guilt:* Person feels guilty over things they could not have done.
Sense of loss of freedom or individuality: Feels as if they are controlled by outside forces.
Adherence to abstract, intellectualistic, and/or autonomous rules: Person follows self-imposed "rational" rules that are quite idiosyncratic.
Existential or intellectual change:* Person suddenly is absorbed by things like religion or philosophy.
Feeling of centrality: Person feels as if the universe revolves around them.
Decentering of the self relative to universe: Feels as if they are not really real, like they truly exist apart from the universe.
*Indicates experience that can also occur in other primary psychotic or mood disorders outside the schizophrenia spectrum, such as delusional disorder, major depressive disorder, or bipolar disorder.
3 notes
·
View notes