#exercise for stroke
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr Inc. is using 66 technologies for its website.
Text

Stroke Prevention Made Easy: Essential Tips for a Healthy Life
A stroke occurs when blood flow to the brain is interrupted, either by a blockage or a burst blood vessel, leading to brain damage. It's a leading cause of death and disability worldwide, but the good news is that many strokes are preventable.
Recognizing the Risk Factors
Several factors increase the risk of stroke, including high blood pressure, smoking, obesity, and a sedentary lifestyle. Family history and age are also significant contributors. However, adopting healthy habits can greatly reduce these risks.
Embrace a Healthy Diet and Active Lifestyle
A balanced diet rich in fruits, vegetables, whole grains, and lean proteins is essential. Reducing salt intake helps manage blood pressure, while avoiding excessive sugar and unhealthy fats can prevent obesity and diabetes—both major stroke risk factors.
Regular exercise, such as brisk walking, swimming, or cycling, strengthens the heart and improves circulation, further lowering stroke risk. Aim for at least 30 minutes of moderate activity most days of the week.
Supplements for Stroke Prevention
Certain supplements can support brain health and circulation. Omega-3 fatty acids, found in fish oil, help reduce inflammation and maintain healthy blood vessels. Coenzyme Q10 and magnesium can also support cardiovascular health. For those recovering from a stroke, these supplements may assist in the rehabilitation process.
Commit to a Healthier Lifestyle
Preventing stroke requires a commitment to a healthy lifestyle. By eating well, staying active, and considering the right supplements, you can significantly lower your risk and lead a life of vitality and wellness.
This post is intended to inform, educate, and recommend Neolife Supplements, an exclusive range of quality products, based on Nature backed by Science. You can interact with me by asking topical questions or suggesting areas you want to be treated. Please read and share this content with others who might find it relevant to their needs.
Solution::
Introducing: Omega-3 Salmon Oil Plus
Omega-3 Salmon Oil Plus. Works for the Heart, Brain, Joints, and more. It is clinically proven to support Heart and Cardiovascular health, Omega-3 Salmon Oil Plus may also promote youthful brain function, healthy flexible joints, and healthy eyes, ideal for pregnant women to support feutal eye and brain development. Omega-3 Salmon oil Plus has been clinically tested in humans and the results have been published in some of the world's most prestigious scientific journals.
Visit and Order Now: https://shopneolife.com/okieteekine/shop/atoz
For more information on how Neolife product range can benefit you and;
Inquiries for recommended product pairing with Omega-3 Salmon Oil Plus, for Stroke.
Call or WhatsApp:+234.8056.229.954
Model Visuals Courtesy: Pixabay
#Here are 20 optimized tags for your blog post on stroke:#stroke prevention#stroke risk factors#healthy lifestyle#prevent stroke#brain health#stroke supplements#diet for stroke#exercise for stroke#stroke recovery#heart health#stroke awareness#omega-3 benefits#CoQ10 for stroke#blood pressure management#reduce stroke risk#cardiovascular health#natural stroke prevention#stroke and diet#stroke and exercise#stroke support.
0 notes
Text

dont ask me what this pose is idk and also im still trying ta figure out howta draw him orz
#ppl draw him soooo cool its awesme#spacie scribbles#cotl#cult of the lamb#narinder#cotl narinder#this was a fun exercise ^_^#i kind of just turned my brain off and put strokes on screen#did some fun shading here!!#theres a bunch of errors but -#ill live lmao
1K notes
·
View notes
Text
I'm not listening to a white person on what's racist or insensitive to brown people. read orientalism by edward said before talking to me or my son ever again
#“the take away was literally not a writing exercise” 1. it was 2#2. cant you white bitches do that on a different post#3. telling indians what is and isnt dismissive of what they go through is hmm. what is it called#4. fuck your saviour complex#5. you guys ARE incredibly dismissive of the global south. our lives are just fiction no what you bitches “warn” about is already happening#wanna talk about how american overconsumption is contributing to the climate crisis? or are you too pussy for that#sorry i dont want my post about how i dont want my people to die in heat strokes to be hijacked. be serious for once in your lives#“sci fi writers have been warning about this” cool! wonder where they got that from#plagiarising gayatri spivak cause i hate her. can the subaltern speak or is that too much for your cracker sensibilities
205 notes
·
View notes
Text

Getting back into the swing of making stuff just for the fun of it! Here's my palm-sized painting of Patrick's house.
#patrick star#spongebob squarepants#painting#acrylic#spongebob backgrounds are SO fun#i struggle to incorporate brush strokes in my paintings#so it makes a really fun and cute exercise#i love how textured and physical all the early spongebob stuff is#you can see the hands at work
12 notes
·
View notes
Text

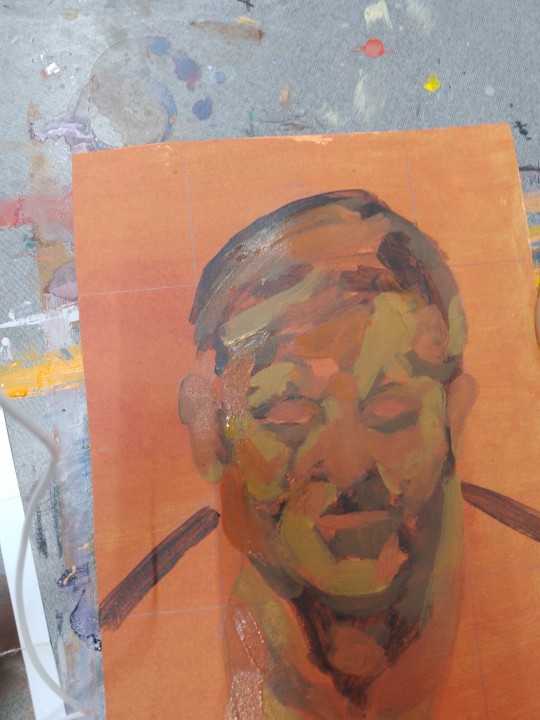
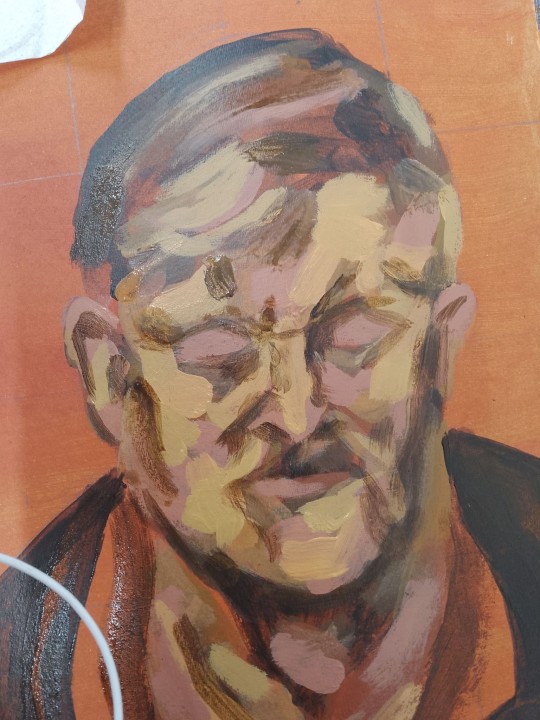
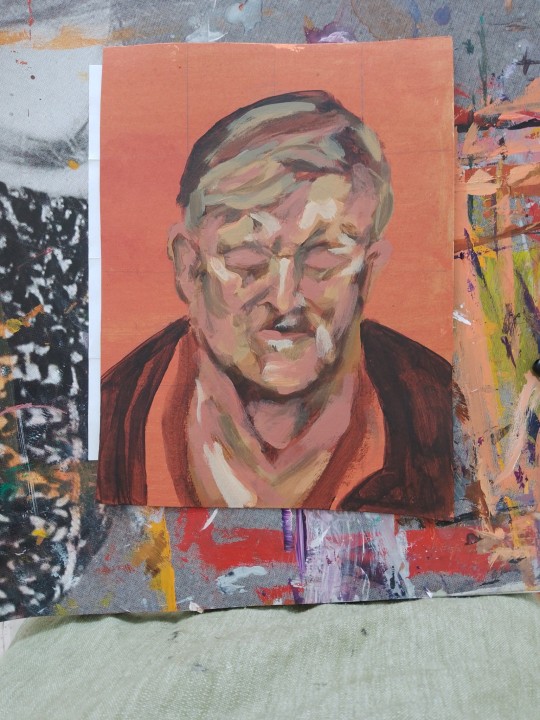


art update fr april part 2/2
#oh just paint a lucian freud they said. just mix skin colour frm 6-8 different tubes not counting varnish water or slowing agent they said.#like itll be a good exercise. idk wth im doing#all of this is progress frm 5 hrs total. i probably spent the first full hour drawing my grid and face in pencil bc i did NOT want to start#like it was too daunting lol. and then the following 2-3 hrs it's still like WHAT AM I DOING I MESSED IT ALL UP#and then you add more depth w dark and light and go like oh. maybe this can still be salvaged after all in time lol ok#it's still a wip i'll continue adding to it next week. apparently when you paint the bg is when i'tll all suddenly click and look solid?#heres to hoping lol. ive never felt more like a painter tho. close up included bc there are like a million brush strokes in there#my reproduction looks nothing like the original guy posing fr his portrait but itsure does look like. some guy in 3D surely#my art#sorry if the positioning is all over the place. those colours did not want to be accurately captured on camera fr
6 notes
·
View notes
Text

...
2 notes
·
View notes
Text
Pros of the butterfly stroke:
-makes you feel STRONK
-stretch out your back
-technically fastest (only when done well)
-subtle flex on the other folks at the gym
Cons of the butterfly stroke:
-as soon as you lose momentum you feel like a pathetic floundering sloth that fell in the pool
-you lose momentum quickly on account of it is the butterfly stroke
-done poorly is just really slow and awkward
-who thought this was a good idea
5 notes
·
View notes
Text
hey anon who sent the "you said i could stay with you if i needed a bed" prompt how do you feel about Tayala being involved (i had Ideas for it but they're.... set in an AU where the Inquisitorius didn't find Bode, lol)? it wouldn't be shippy between Cal and her, and obviously the spyscrapper would be the main focus
#ramblings#i'm hitting the au trying to fully form inside my brain. no. vague strokes ONLY#this is an exercise in writing ficlets. short scenes. i swear i used to be able to do that#you don't have to reply to this post if you don't want to reveal your user; you can send me another anon
4 notes
·
View notes
Text
rgg was real for insinuating treasurers are batshit insane
#snap chats#dangerous combo i was thinking about mine this morning but i also opened my canvas and forgot i had plans to draw jo yesterday#and im not mustering the will to make the post ive wanted to make for months in that I Think They'd Get Along#i think they should have bursts of violence together itd be a healthy team building exercise#theyd get along until mine found out jo left his baby in a locker and then i think we're watching the bloodiest beat down of the century#either that or the roast of the century. he might not be swinging but he's still doing maximum emotional damage#jo aint even denying that shit either he gonna let mine kick the shit outta him cause he knows he deserves it#but yeah very funny neither of them got proper education in economics yet they're left to manage funds#yeah i trust these *orphaned bitches to do my taxes. whats the worst that could happen#*technically jo aint an orphan hes a runaway but he still parentless im running with it#they'd both also get a stroke over aoki and daigo being an item. for one reason or another#ive compared mine to aoki but now the cursed option of comparing him to his dad#mental illness really does take you places you never wouldve imagined otherwise i need to be put down#i must draw them together but i cant think of anything.... very awful...#all i can imagine is sawashiro in goofy j-drama scenarios with the arakawas... its just too easy to imagine#esp after all ive done is watch tsutsumi in cutesy dramas and movies.... actual darlings for charas he plays. sometimes#im getting off topic ok bye
5 notes
·
View notes
Text
The Impact of Smoking and Other Harmful Habits on Vascular Health
Smoking is a highest cause of vascular disease and can significantly raise the risk of heart attack strokes and other vascular conditions. Sedentism, poor diet and excessive alcohol consumption are all harmful habits that can harm vascular health.
At the Vascular Center, we understand the critical role that lifestyle habits play in preventing and managing vascular diseases. Quitting smoking is one of the most effective ways to improve vascular health and reduce the risk of complications.
Smoking can damage the blood vessels, causing them to narrow and stiffen over time. This can reduce blood flow and increase the risk of blood clots, which can lead to heart attacks, strokes and other complications. Smoking also increases the risk of peripheral artery disease (PAD), a condition in which the blood vessels in the legs narrow and restrict blood flow to the muscles.
Quitting smoking can reduce the risk of these and other vascular conditions significantly. According to studies, the risk of heart attack and stroke can be comparable to that of a nonsmoker within a few years of quitting smoking. This emphasizes the significance of quitting smoking as soon as possible.
Other risk factors for cardiovascular disease include a sedentary lifestyle and a poor diet. Regular physical activity can help improve vascular health by strengthening the heart and blood vessels, lowering inflammation and increasing blood flow. A healthy diet high in fruits, vegetables and whole grains and low in saturated and trans fats can also improve vascular health.
Excessive alcohol consumption can also be detrimental to vascular health. Alcohol can raise blood pressure, cause heart muscle damage, and increase the risk of blood clots. Moderate alcohol consumption can help reduce the risk of these complications.
At the Vascular Center, we work with our patients to identify and address any lifestyle factors that may be contributing to their vascular disease. We offer support and resources to patients who want to quit smoking, eat healthier, and exercise more. We also provide comprehensive medical treatment options for vascular conditions, including medication, minimally invasive procedures and surgery.
Summary
Cigarette smoking and other unhealthy lifestyle choices can have a significant impact on vascular health. Smoking cessation, a healthy diet and increased physical activity can all help reduce the risk of vascular disease and improve overall health. If you are concerned about your vascular health, make an appointment with one of our specialists at the Vascular Center. We can collaborate to create a tailored plan to help you achieve optimal vascular health.
#vascular disease#smoking#harmful habits#lifestyle changes#vascular health#heart attacks#strokes#blood vessels#peripheral artery disease#healthy diet#exercise#alcohol consumption#medical treatment#minimally invasive procedures#surgery#Vascular Center
3 notes
·
View notes
Text
Save me zofran pls save me
#chronically ill phoenix#god forbid i do a *5 minute* workout#based on a scan a few years ago i have fibromuscular dysplasia in my middle cerebral artery#and so my working theory is that whenever my blood pressure goes up#from stuff like exercise or anxiety or even standing bc of the pots#that it triggers a migraine which also can cause the nausea#i see my neuro on Friday and it's one of the things i want to talk to her about#kinda want to ask to get another cta just to like make sure that is what it is#since it was just an incidental find when it showed up a few years ago and so it wasn't fully confirmed#and atp i just want to know if it is that bc if so i need to be more aware of stroke risks and stuff#but if it isn't then maybe i can stop stressing out as much that I'll have a stroke bc of it#but also the neuro appt is first gonna be about the jerking and twitching bc it's driving me up the wall
1 note
·
View note
Text
tell me how I'm supposed to resist practicing until my fingers hurt when I'm deeply anxious and malagueña is in the back of my guitar book. i could hyperfixate all day
#i'm on a hot streak with guitar today too; some of the chord recognition practice is really starting to pay off#a lot of these practice excerpts are really pretty easy now that i can be like o yea its my friend the a minor chord#yea i know where my fingers go for this one! and the next one and the next one#i gotta practice to get smoother and pay attention to my musicality#and i still fall flat on my face trying to do rest strokes esp when the next note is on the next string#but maybe my teacher was right it's a good idea to go back to the exercises after awhile in the solo book#i'm curious to see what he has to say about position playing bc i think the way this book explains it is terrible#but it's easy to put into practice at least for a few phrases at a time like the example pieces#like. the notes stay put unless you change the tuning. so it's just a matter of moving your hands around so the reach isn't ridiculous#just like on piano we don't always have to have our thumb on middle c#anyway! i can't see myself playing fast enough for tremolo just yet but i LOVE malagueña and latin guitar in general so maybe i'll learn#maybe this will be the piece i learn it for#i love the cadenza with the melody in the bass note and the rising tension of the repeated notes in the treble it's so dramatic#love love love! to the extent that i have ignored everyone and everything in my life for an hour and a half#don't ask about that
1 note
·
View note
Text
It can be quite difficult to live with a chronic ailment, however, if you work out and follow a fitness regime, then the standard of your life can improve. The reason why is that physical activity has been proven to be one of the most effective ways to address patients’ symptoms, improve their mood, and have a higher quality of life.
0 notes
Text
Supper Last Night, Stroke Therapy
1 note
·
View note
Text
John McLaughlin's Alternate Picking Techniques for Guitar
Please watch Video above for Detailed Info: Hi Guys, Today, two exercises for building jazz fusion 16th note double timed improvised guitar lines in the way that John McLaughlin exploits the alternate picking guitar technique. This is a “Line builder” that builds through connecting concepts together and becoming familiar with them as you do so. For Example: Arpeggios, Chromatics,…

View On WordPress
#alternate picking#chromatics#down stroke#Examples#explained#guitar exercises#guitar lesson#how to#improvised line#jazz fsuion#jazz fusion music#jazz improvisation#John Mclaughlin#liquid lines#music#pedagogy#pentatonics#speed#this is the way I do it#up stroke
0 notes
Text
thinking about low sodium and dehydration and pots and hating exercise bc it makes me feel bad actually and—
#GIRL I KNOWWWWWWW EXERCISE HELPS W MY MENTAL HEALTH AND PHYSICAL HEALTH TRUST ME I KNOOOOWWWWWW#grrrrrrrrrrrrr#like i hate all of this bc it probably is just dehydration and being out of shape BUT WHAT IF IT ISNT#and i dooooooont wanna say that out loud bc. i dont wanna like#be complaining over nothing but liiiiiiiiike#my grandpa literally like. suffered basically something like a stroke bc of low sodium#and him and my mom have like. lower than normal blood pressure im pretttyyyyy sure#so its. JGIGIGGGGHHG#i hate it here#bc i felt soo sleepy and then i had gatorade and bam i felt like a person again#in a way that water did not help#BUT OBVIOUSLY INSTAGRAM REELS DONT ACTUALLY MEAN SHIT#rambles#winter stfu
0 notes