#epithelial
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Kazakhstan’s Minister of Communications and Informatics has blocked the Tumblr site because it contained 60 sites of terrorism, extremism, and pornography in 2015.
Text
I had to try my own spin on it after sharing the song last night.
This is what I did instead of sleeping:
Crywolf & Echos - Epithelial (Prophetic Nightmares Cover)
I don't usually sing in my work, and even when I do it's layered with effects. So, sharing something so raw and real is a tad uncomfortable.
Nevertheless, I hope you enjoy.
#music#prophetic nightmares#my music#ambient#crywolf#echos#epithelial#cover#cover song#unofficial#SoundCloud
44 notes
·
View notes
Text
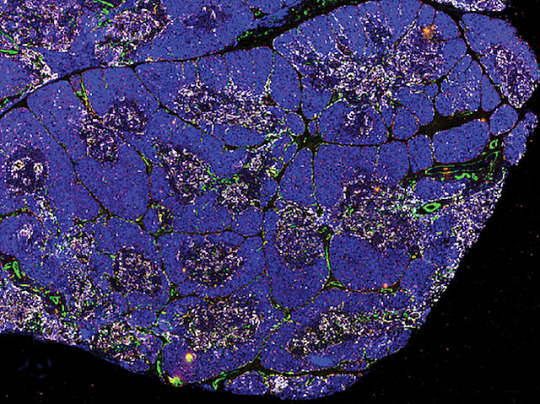
Nurturing T cells
The organ in your chest called the thymus – where the immune system's T cells mature – is composed of a number of cell types, including epithelial cells, vital for T-cell development. This study characterises epithelial stem cells and reveals their capacity to self-renew and organise, providing insight for prolonging T-cell activity as it declines with ageing and for tackling thymic disorders
Read the published research paper here
Image from work by Roberta Ragazzini and colleagues
Epithelial Stem Cell Biology & Regenerative Medicine Laboratory, The Francis Crick Institute, London, UK
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Developmental Cell, August 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#immunofluorescence#biology#immune system#T cells#thymus#ageing#epithelial#stem cells
13 notes
·
View notes
Text
Diverse Epithelial Lymphocytes in Zebrafish Revealed Using a Novel Scale Biopsy Method
Abstract Zebrafish (Danio rerio) are a compelling model for studying lymphocytes because zebrafish and humans have similar adaptive immune systems, including their lymphocytes. Antibodies that recognize zebrafish proteins are sparse, so many investigators use transgenic, lymphocyte-specific fluorophore-labeled lines. Human and zebrafish lymphocyte types are conserved, but many aspects of…
0 notes
Text
« We found that wounded epithelial cells can send bioelectric signals to neighboring cells over distances more than 40 times their body length with voltages similar to those of neurons. The shapes of these voltage spikes are also like those of neurons except about 1,000 times slower, indicating they might be a more primitive form of intercellular communication over long distances. »
0 notes
Text
SciTech Chronicles. . . . . . . . .Mar 18th, 2025
#pattern#eastward-shift#Mississippi#Tennessee#bioelectricity#epithelial#microelectrode#calcium#AI#age-related#Biobank#saliency#RNS#Wearable-LLM#PTSD#EEG#Observatory#hydrothermal#magma#steam
0 notes
Text
scall hot . send help!
1 note
·
View note
Text
if they really wanted me to stop pulling dry lip skin off before it heals they wouldn't make it the most satisfying thing in the world
7 notes
·
View notes
Text
dude i have to wake up in 6 hours and im really tired but i have homework due in 9 hours that i know i will not wake up early enough to do so i have to do it right now
#pain of a college student#man i did not miss these sleepless nights#staring at the layers of epithelial cells and forgetting the difference between stratified and basal again#this bird speaks#this bird studies
12 notes
·
View notes
Text
i'm sorry but it's very funny to get mad that people are yelling at you for making a post actively socially shaming tumblr users for being too uncool to smoke, like you were trying to make the subject of those middle school dare PSAs real for the first time ever
#'actually i was just SURPRISED' then why'd you make a post about how annoyed you were that people were claiming not to smoke in a poll.#sorry man. many people enjoy not paying large amounts of money in exchange for lung epithelial lesions#there was a whole reasonably successful public health campaign for a while and everything#i agree that people can be too cruel about smoking but 'incredulity that you're upset that only 30% of respondents claim to smoke' is#not really the same thing as that.#in many countries the rate of tobacco use is in fact well below that. i'm not sure what you expected to happen here.#box opener
9 notes
·
View notes
Text
scheduling a pee break in the middle of microscopy class to check the donmar announcement
#lie i will be totally engrossed in epithelial cells of the stomach and forget probably :(#macbeth#donmar warehouse
4 notes
·
View notes
Text

Follow that Cargo!
Analysing the details – including both spatial and organisational – of molecular cargo being transported through the secretory pathway in fruit fly epithelial cells using a vesicle tracking software tool called MSP Tracker
Read the published research article here
Image from work by Jennifer H. Richens, Mariia Dmitrieva and Helen L. Zenner, and colleagues
MRC-Laboratory of Molecular Biology, Francis Crick Avenue, Cambridge Biomedical Campus, Cambridge, UK
Image contributed by the authors under a Creative Commons Attribution 4.0 International (CC BY 4.0) licence
Published in PLOS Biology, April 2025
You can also follow BPoD on Instagram, Twitter, Facebook and Bluesky
6 notes
·
View notes
Text
As an oral surgeon, do you remember the development of the pre-maxilla?
The premaxilla is a crucial component of the upper jaw during the embryonic stage of development. It develops from the fused lower portions of the medial nasal processes and carries two central and two lateral incisors. The premaxilla stabilizes the facial skeleton and is comparable to the keystone of a masonry arch. Defective development of the premaxilla can lead to malformations of the mouth…

View On WordPress
#Canalis sinuousus#Cleft lip#Cleft palate#Embryonic development#Endognathion#Epithelial remnants#exognathion#Fusion#Globulo-maxillary cyst#Malformations#Maxilla#Maxillary processes#Medial nasal processes#Mesognathion#Nasolabial cyst#Nasopalatine duct cyst#Ossification#Pharyngeal arches#Premaxilla#Stomodeum
1 note
·
View note
Text
youtube
#Tumor microenvironment#cancer cells#stromal cells#immune cells#extracellular matrix#fibroblasts#macrophages#T cells#hypoxia#angiogenesis#vascularization#inflammation#oxidative stress#epithelial-mesenchymal transition#metastasis#cytokines#growth factors#exosomes#immune evasion#drug resistance.#Youtube
0 notes
Text
Do you think fate would be a creature, kind of like God? Something unknowable to us but also we are unknowable to them. We can pretend to understand as they may do us. Too macroscopic for us to see and study all of them at once. Us too microscopic for them to see and study us either. You know homeostasis, how things aim to be dynamically unchanged? Our pH, temperature, so many things where we are just a tiny sliver, a tiny line, a thin border, like our own skin. We can only live in our skin, and isn't it terrifying to realize how thin that is? Doesn't it make sense we can be dynamically unchanged? Going through the same cycle because some part of us fears a death that will happen? Afraid we will not be? But some things can be a positive feedback loop, for better or worse. Building muscle is a positive feedback loop, in my mind. Pregnancy. Death too, in a sense. It is not always some that will be good for you, but something can change. I am not the same person I was last year. That person is dead. Yet, do I fear that death? I don't know. So what if fate was like that? Afraid that things skewing off of fate's path would bring its end not knowing that just a different version of them will leave? What if things skewing was uncomfortable for it, like an itch, a hiccup, and so they go to stop it, not Willing to grow or evolve. But what if, what if it did? For a second? For a day? What if fate gets tired and for once, for once, it can rest and see what happens. For once, it knows it can't know everything. Wouldn't that be nice?
#my post#I just think it's fun to think about#kind of like to all the microbiomes and somatic cells and everything else we are composed of#most of the time they are at our mercy. we are the gods to them. neither of us can fully understand each other#that epithelial cell will never understand my existence and I will never understand theirs#but isn’t it nice to try?#isn’t that part of what science is about?#to me it is#i hope I get the chance to finish my degree one day#i miss it#i should learn about apoptosis again#does the cell fear its death or accept it#does it views its death as the greater good?
0 notes
Text
0 notes
Text
0 notes