#anaphylactic shock treatment
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text
Anaphylactic Shock: Understanding and Reacting to a Life-Threatening Emergency
Learn to recognize and respond to anaphylactic shock with this comprehensive guide. Discover causes, symptoms, and emergency steps, including using an epinephrine auto-injector. Be prepared to save lives with essential insights on managing severe allergic

View On WordPress
#allergic reaction treatment#allergy emergency response#anaphylactic reaction#anaphylactic shock#anaphylactic shock emergency#anaphylactic shock management#anaphylactic shock treatment#anaphylaxis#anaphylaxis first aid#anaphylaxis medical care#anaphylaxis prevention#anaphylaxis response steps#anaphylaxis symptoms#causes of anaphylaxis#epinephrine auto-injector#how to treat anaphylactic shock#how to use epinephrine injector#recognizing anaphylaxis#severe allergic reaction#what to do during anaphylaxis
0 notes
Text
Sicktember 2024 Prompt-Based Resources to Help You Get Started! 💚

**Sicktember 2023 prompt-based resources can be found [Here]
Hangovers
What is a hangover [niaaa.nih.gov]
15 hangover horror stories [buzzfeed.com]
7 ways to cure your hangover [health.harvard.edu]
How to Write a Drunk Character [allwritealright.com]
Over Indulgence
Dealing with Food hangovers [health.usnews.com]
4 Ways to Stop Digestive Discomfort [michiganmedicine.org]
I Ate Too Much. Now What Do I Do? [osfhealthcare.org]
Is It Possible… Stomach Explode? [popsci.com]
Campus/Con Crud
Crushing the Campus Crud [hercampus.com]
So What is Con Crud [granitcon.com]
Coming Down With the Crud [bmhsc.org]
Rogue Organs
What Is Appendicitis? [hopkinsmedicine.org]
Gallbladder Removal [nhs.uk]
Tonsillectomy [mayoclinic.org]
Spleen Problems and Removal [nhs.uk]
Dizziness/Vertigo
Understanding Vertigo [on.bluecross.ca]
Types of Vertigo [acare.abbott.com]
Dizziness vs. Vertigo [cornerstonephsio.com]
Medieval Treatment
Medicine in the Middle Ages [ncbi.nlm.nih.gov]
6 Medieval Medical Practices [guavahealth.com]
Healing Power of Maggots/Leeches (Modern) [mountainview-hospital.com]
When Medicine was Humorous [merryfarmer.wordpress.com]
Mononucleosis
About Mono [cdc.gov]
Mono For Teens [kidshealth.org]
How to Test for Mono [mountsinai.org]
Sick People Food
What People Around the World Eat When Sick [businessinsider.com]
Sick Day Foods Across the Globe [nyubiteclub.com]
8 Best Foods to Eat When Feeling Sick [forbes.com]
Toxin/Poison
Poisons and Toxins [sciencelearn.org]
Poisoning. What The Doctors Do [thedoctorwillseeyounow.com]
Common HouseHold Poisons [cincinnatichildrens.org]
FAQs Carbon Monoxide Poisoning [cdc.gov]
Brain Fog/Spaced Out
What is Brain Fog [everydayhealth.com]
Understanding Brain Fog [henryford.com]
Causes of Zoning Out [verywellhealth.com]
Aches And Pains
What Causes Body Aches When Sick? [uclahealth.org]
5 Tips For Writing About Physical Pain [louiseharnbyproofreader.com]
Hypochondriac tendencies
Illness Anxiety Disorder [my.clevelandclinic.org]
Signs You May be a hypochondriac [centerforanxietydisorders.com]
10 Health Anxiety Myths [happiful.com]
How To Write Anxiety [writerscookbook.com]
Anaphylactic Response
What is Anaphylaxis [betterhealth.vic.gov.au]
Anaphylactic Shock: What You Need to Know [healthline.com]
Waiting Rooms
What happens in the emergency department [advocatehealth.com]
Triage and Emergency Assessment [ncbi.nlm.nih.gov]
Setting Description: Emergency Waiting Room [writershelpingwriters.net]
Summer Flu
Can You Get the Flu in the Summer? [verywellhealth.com]
Leisure Sickness [avogel.ca]
Catching a Cold When It’s Warm [newsinhealth.nih.gov]
Heart Condition/Cardiac Arrest
Types of Heart Attacks [www.healthline.com]
Common Heart Conditions [summahealth.org]
What Does a Heart Attack Feel Like? [health.clevelandclinic.org]
How to Describe a Heart Attack in a Story [writingtipsoasis.com]
Pulling a Ferris Bueller
Define Pulling a Ferris Bueller [urbandictionary.com]
Ferris Bueller’s Day Off Summary [gradesaver.com]
10 Things Ferris Bueller Taught Us [dailyedge.ie]
A Note From the Mods [Tumblr Post]
Sick While Traveling
Take Steps to Stay Healthy While Traveling [cdc.gov]
Motion Sickness [sciencefocus.com]
How to Remove Vomit From Car Interior [wikihow.com]
Sick on Vacation Tips [apartmenttherapy.com]
Hospital Bed
How to Write a Hospital Scene [writersdigest.com]
Hospital Bed Components & Safety [robsonforensic.com]
9 Way to Help When Someone is Hospitalized [upstate.edu]
First Aid Kit
Make a First Aid Kit [redcross.org]
Travelers First Aid Kit [hopkinsmedicine.org]
Health Plan and First Aid for College [uh.edu]
Flushed Cheeks
Causes of Facial Flushing [verywellhealth.com]
What Can Cause Flushed Skin? [medicalnewstoday.com]
Doctor's Note
Obtaining a Dr Note for Work [inhersight.com]
How to Get A Dr. Note for School [solvhealth.com]
#sicktember#sicktember 2024#resources and advice#links#prompt based links#hangovers#stomach ache#campus/con crud#cold and flu#rougue organ#dizziness/vertigo#medieval treatment#mononucleosis#sick people food#bland diet#toxin/poison#body aches#anaphylaxis#waiting room#summer flu#heart condition/heart attack#k on#yui hirasawa#sick fics#sick character#writing resources#sick fic tips
205 notes
·
View notes
Text
Writing Notes: Food Allergies

Food allergies - the body’s abnormal response to specific proteins found in food. These proteins normally are harmless but cause a reaction in some people. They can occur when food is either eaten or touched.
Many people use the term ‘‘food allergy’’ to describe what is actually a food intolerance.
A food intolerance is a reaction to food that does not involve the immune system.
Lactose intolerance is a common food intolerance, while celiac disease is a food allergy.
Eight foods cause 90% of all food allergies. These are:
milk
eggs
peanuts
tree nuts (walnuts, cashews, pecans, almonds, etc.)
fish
shellfish
soy
wheat
When the body encounters an allergen, it releases large amounts of histamine.
The release of this chemical is responsible for allergic symptoms.
Symptoms of food allergy can range from mildly annoying to dangerous and life threatening.
These symptoms include:
tingling of the mouth
tingling or numbness in arms or legs
skin rash or hives
itching
abdominal cramps
vomiting
diarrhea
breathing difficulties
sudden drop in blood pressure (hypotension)
swelling of the tongue
swelling of the face and throat
loss of consciousness
death
The most serious symptom of food allergy is anaphylaxis.
Anaphylaxis, also called anaphylactic shock, is a sudden and potentially life threatening allergic reaction in which the whole body reacts to an allergen.
During anaphylaxis, the airway constricts, making breathing difficult.
Swelling of the throat may block airways as well.
Vomiting and diarrhea may occur.
The face may swell and the skin may become itchy with a rash or hives.
The heart may race and the heartbeat may become irregular.
Treatment for an allergic reaction is administration of an antihistamine drug.
The most common antihistamine is diphenhydramine hydrochloride; found in over-the-counter drugs, such as Benadryl, and in some prescription drugs.
If taken immediately, antihistamines can stop or moderate an allergic reaction.
In cases of a severe allergy or anaphylaxis:
an injection of a strong antihistamine called epinephrine (also known as adrenaline) may be used.
An auto-injectable form of epinephrine (Epi-Pen) that looks similar to a large ballpoint pen can be carried at all times if a person has a history of severe allergy.
If a severe allergic reaction occurs, the auto-injector is held against the skin and the medication is self-administered as a shot.
Epinephrine is a strong antihistamine; it often can stop anaphylaxis symptoms.
Source ⚜ More: Notes & References ⚜ Writing Realistic Injuries ⚜ On Allergy
#writing reference#writeblr#dark academia#spilled ink#writers on tumblr#literature#writing inspiration#writing notes#writing prompt#poets on tumblr#writing ideas#creative writing#fiction#medicine#food#allergy#pierre-auguste renoir#writing resources
88 notes
·
View notes
Text
I get disability memes on my Pinterest feed but after getting one for ER Drs/nurses that I found concerning, I kept seeing more and more like it and I went down a rabbit hole. I know it's one of the most stressful jobs someone can have and I really appreciate the medical staff that have been kind to me. These things are definitely made by the types of people who haven't been.
I think it's important because memes are kind of a way to let off steam but they mean what they're saying. They're not just jokes but they're framed in a way that they can say it more comfortably. Sometimes they're just straight up admitting to crimes and malpractice. It's like when someone says something that crosses a line in a joking tone so that if you feel attacked they insist it's just a joke and you're taking it too seriously. But my life is constantly in the hands of these people and I've been mistreated time and time again by medical personnel
I'm gonna go through them because honestly I hate them and there are a lot of repeating themes
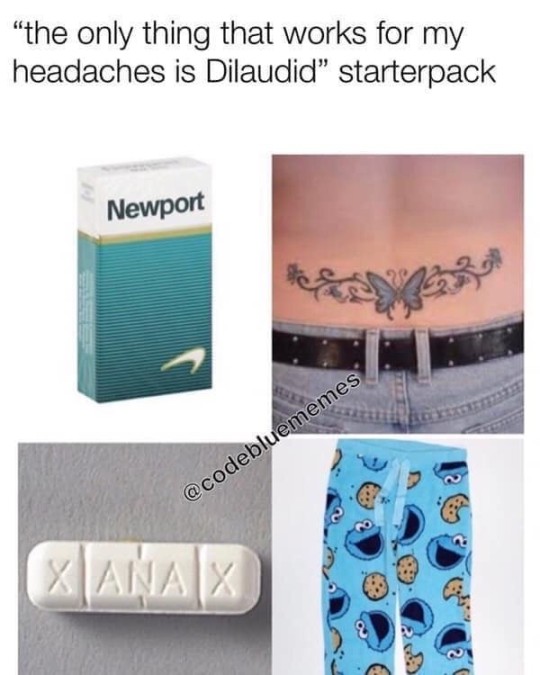
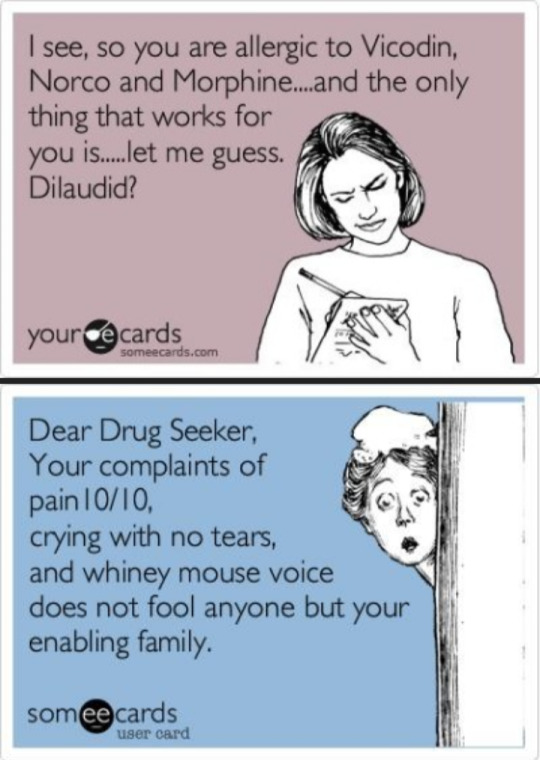
These are extremely common. The focus of the meme being that a whiny patient is asking for pain medication that they clearly don't need. Something commonly mentioned in these is disbelief that the patient has an allergy because it's common for someone trying to get drugs to claim they have an allergy.
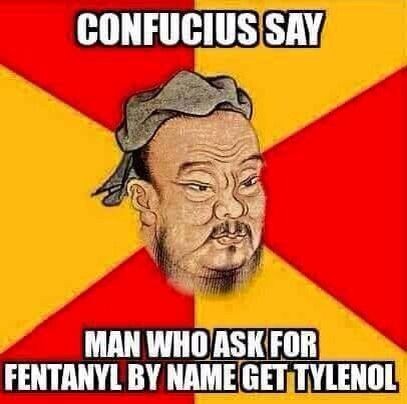
Also the Confucius one is both ableist and racist so double whammy I guess!
I've dealt with people I know are silently assuming this of me. I'm allergic to NSAIDs- deathly allergic and at risk for asphyxiation or anaphylactic shock. Medical staff sometimes have this attitude of "we know when you're faking your pain" (no really I had one say this shit on my post about this) and that has traumatized me immeasurably because they'd rather me wait for 4+ hours in some of the worst pain of my life than risk the possibility of me being an awful scheming mustache twirling addict.
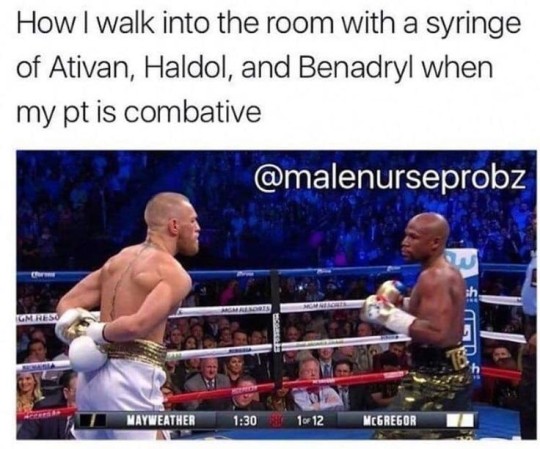

This category is just as common. "I don't like you so I'm going to drug you". That's more fucked up than they seem to think it is.

Then there's the category of "you're a whiny little bitch and I don't believe a word out of your mouth". Which contributes heavily to medical malpractice and abuse
Again these are doctors and nurses making these, people responsible for treating patients with care and dignity and respect. Especially if they want any in return

Aaaaand this one is just a crime. One that's happened to me actually- reporting examinations that never happened to get rid of me because I was such a nuisance (crying, hardly coherent, drenched in sweat, 9/10 pain on arrival)
And then there are the ones like "don't mess with me because i handle your treatment/meds 💕". Things like "the way you treat me is the deciding factor for how fast I'm going to get your painkillers 😊". Which to me is just... evil?
I've never in my life mistreated medical staff but people in a lot of pain get mean sometimes. It's a survival instinct actually- for aggression to accompany pain or panic. Not that it's ever okay but it isn't personal
These are just a few examples really, there are so fucking many of these with this awful, cruel, cynical tone. There are some funny ones that aren't mean or degrading towards patients but so many of them are and in nearly every one I see a mean spirited healthcare worker that I've encountered at some point who damaged me in ways I will never psychologically recover from
#chronic illness#chronic pain#disability#actually disabled#cfs#chronic fаtiguе ѕуndrоmе#spoonie#fibromyalgia#me/cfs#cfs/me#cripplepunk#cpunk#long covid#medical ableism#ableism
366 notes
·
View notes
Text
Smarty IV (Rafe Cameron x OC)

SYNOPSIS: smart girl isn’t as smart as rafe cameron.
WARNINGS: mature content; dark!rafe, toxic relationship, domestic violence, verbal abuse, blackmail, jealousy, general violence, manipulative behavior, explicit language, substance abuse & addiction, use of guns, mentions of past crimes, obsession
series masterlist
masterlist

“i wish you could just give me one day, laia…” rafe sighed loudly into to the empty space in front of him, fingers tensing around the steering wheel before dropping to his lap. “just one day where you aren’t being a total bitch.”
a scoff escaped my throat, the sound coupled with a roll of my eyes. it took everything to bite my tongue, memories of the last time i called him a bitch reason enough to do so.
“because i didn’t want you talking to the bitch–the girl, you were fucking while i was away?” i corrected myself immediately. it was out of character to call other women such derogatory names, but the word flowed so easily off my tongue. “the one that we just argued about a few days ago?”
“jesus christ, all she did was say ‘hi’! she was working!”
“she could have been lying on the floor dying of anaphylactic shock, rafe. i don’t give a fuck.” i shoved the car door open and jumped out before turning back to face him. “i told you not to talk to her.”
slamming the door shut, i left my boyfriend in the truck by himself as i trudged down the dock to where he keeps his boat. the sky was a clear blue and the sun was beaming down onto the earth, the warm yellow light leaving a sheen of sweat on my skin that was only amplified by the humidity. it was a beautiful day, calm waves and a stunning horizon in the distance gracing the view of onlookers surrounding the dock, but i couldn’t begin to appreciate it.
i tried giving rafe the silent treatment after finding out about his indecent activities, but he was never one to let that go on for very long.
after the fourth day of avoiding all contact with him, he made an appearance at my front door with little patience for my attitude. he gave no room to argue when he told me to get dressed and dragged me out to his car a few minutes later. i didn’t fight back because i knew it would make no difference.
he took us to the island club, and that girl happened to be working today. i’ve never been one to be jealous of rafe talking to other girls, but the fact that she got to fuck him before i did enraged me beyond comprehension. the scoff of annoyance that left my body as she greeted the two of us was out of my control. i didn’t notice that i had been mean-mugging here until rafe told me to ‘fix my face’ when she walked away.
the entire car ride after our lunch together was filled with a tense silence; one that remained until we arrived at the dock and was broken by him.
“i don’t wanna argue with you, laia. i was just being nice.” rafe tried to hold a hand out for me to board the boat, but i paid it no mind. hopping over the gap between the ledge of the yacht and the water, i made my way to the front with my boyfriend dragging his feet behind me.
“i gave you four days of peace, rafe.” my eyes cut him with the sharpness of the hunting knives he keeps in his basement. raising a finger, i point it directly into his broad chest. “you insisted on coming to bother me knowing that i’m mad at you. on top of that, you took me to the place that girl works! so no, you don't get to complain about me being a bitch.”
i take a seat on the right side of the steering wheel, eyes trained on the water in front of us. the blonde sighs loudly, the bass of it filled with frustration.
we remained silent for an amount of time that i’m sure was longer than necessary, but i refused to be the first to break it. rafe stops the boat a couple nautical miles away from where we were originally, the dark blue water surrounding all sides of us.
“baby?” rafe locks the wheel in place before take a seat next to me. i feel his eyes burning into my figure, gazing hotter than the summer sun beaming down onto us.
“yes, rafe?” the answer to his call was released with a tired sigh. i was genuinely upset about what happened, and hearing him talk was beginning to give me a headache.
my boyfriend takes a seat next to me, reaching over to pull me closer. he ignores my protests as he sits me on his lap and wraps his arms around my waist snugly, resting his chin on my shoulder.
“you know i love you, right?” the vibrations of rafe’s chest traveled through my back as he spoke. “i didn’t mean to make you upset. i haven’t thought about her in forever, i really was just being polite…”
it took everything in me not to roll my eyes.
he just told a blatant lie, right to my face. if he hadn’t thought about her in forever, why did she text him just a few days ago? if they hadn’t been in contact recently, then she wouldn’t have thought they were still on speaking terms. on top of that, there was no reason for him to speak to her–politeness be damned. he knew i was mad–and why i was mad–but chose to acknowledge her anyway.
it was a habit of rafe’s to take me out on dates, buy expensive gifts, and sing praises about how much he loves me whenever i was upset with him. he thought i didn’t notice, but after all this time it was hard not to pick up on the pattern. there’s only so many times shopping sprees and worship will make someone forget why they were upset in the first place.
“okay.” my voice was edged with irritation. i tried my best to disguise it with indifference, but there was nothing rafe didn’t notice when it came to me.
“okay?” i could feel him turn his head to look at me, the side of my face burning hot from his fiery gaze.
“yes, okay, rafe.” the reply was snippier than i meant for it to be. “i love you, too–what do you want me to say?”
a puff of air escaped through his nose; a sign of his own temper flaring up. i could feel his arms flex against me for a second before settling in their natural state.
“well; i’d like it to sound like you mean it, first of all.” the sass in his voice was evident. “i’ve already apologized, like, forty times. it happened, laia–i’m sorry that i slept with her. i’m sorry that i acknowledged her existence today. what else do you want from me?”
“you slept with her, rafe!” i swiveled my own head to meet his eyes directly, the familiar sight matching the ocean below us in color. “you can apologize forty-thousand times–i don’t give a fuck! that is so…beyond…i don’t know what you want from me, either.”
throwing his arms off, i rose to my full height before turning to face him with folded arms.
he stood up as well, head towering far above mine. i stumbled forward from being pulled back into his body, a pair of strong hands gripping my hips keeping me in place. there was no point in trying to back away–it wouldn’t make any difference when he would just put me right back where i was.
it was obvious that he was really sorry, but it was also clear that he wasn’t too happy about me not accepting his apologies. usually, i would let things go just so we didn’t have to argue. this time was different–he didn’t like that.
“if i could go back in time and un-fuck her, i would.” the wet muscle of his tongue poked out from his plush lips before returning to its place. “but i can’t. we were on a break that you wanted! it’s in the past now, laia, alright? do you think picking fights and ignoring me is gonna change what happened?”
i blinked up at him slowly. mouth sewn shut, i wasn’t really sure how to respond to that.
he was right; picking fights wasn’t going to change anything. my anger was genuine, but it had dissipated over the days that i’d isolated myself from him. i was mostly trying to make a point on how he couldn’t get away with doing things that hurt me and then expect to shower me in praise to receive my forgiveness.
shrugging as a reply, i turned my head away from him to face the horizon. my head was snapped back in his direction by a set of fingers sinking into my jawline. rafe’s eyes held the same softness they alway did when they held me in their gaze, but his exasperation was clear as the sky above.
“you look at me when i’m talking to you. do you think that’s going to fix things?” my throat bobbed at the scolding, his stern voice covering my skin in goosebumps inappropriate for the warm temperature of the nature that surrounds us. shaking my head no silently, i give him my honest answer. “right, okay…so are you acting out for attention? what are you trying to do?”
i shrugged again. the blond chuckled from above, amused by my sudden loss of words.
“i’m trying to show you that you can't just…say you love me and expect me to let shit go.” i said. “you took it way too far this time, rafe.”
“okay, so you wanna break up?”
i furrowed my brows at him, head jerking back in surprise. the question caught me off guard. he looked down at me expectantly and watched my eyes open and shut rapidly as i blinked away the shock.
“i never said that.” my head shook in denial at the accusation. “if i wanted to leave you, i would have done it before any of this ever happened.”
“so if you don’t want to break up, what the fuck are you still mad for?” i wasn’t sure if he was genuinely confused or angry; most likely overcome with both feelings. “tell me what it’s gonna solve when i’ve already apologized and i stopped talking to her before you even came back from school because i knew that i wanted you, not her. it’s not gonna solve anything, right?”
i hate it when he makes points. it made me feel stupid whenever he called me out and happened to be right–like right now. there were no plans for me to leave him; if i wanted to then i would have done it a year ago before i left for school. obviously i wanted us to work out, i loved him.
it was more of a point to make for myself than him. rafe gets away with most things, simply because i hate fighting with him. if it meant that things would go back to normal, i would let it go–even when it hurt me. i couldn’t let him just walk all over me anymore, that’s what i was trying to prove.
instead, it’s making me feel like i’m being difficult.
it was embarrassing. it shouldn’t be, but i could feel my skin heat up from the emotion washing over me in a thick layer that overpowered the sun above.
rafe took my slice as agreeance and nodded his head in understanding. bringing his face closer, i could feel his nose brush against mine, the gesture leaving a ticklish feeling in its wake.
“we’re adults, baby.” his warm breath landed against my lips as he spoke in a gentle voice. “that silent treatment shit is childish and you know i don’t like it. it’s over now, okay? just let it be over–let’s just focus on each other. that outside stuff isn’t important; just us.”
closing the minimal space between us, rafe presses his lips to mine. my eyes flutter shut at the familiar feeling. it was short and sweet; he pulled away before it went any further in order to gage my reaction. not seeing any resistance, the blond returns to the contact.
rafe’s lips open slightly, just wide enough for him to lick at the seam of my lips. i follow his lead, lips allowing him the access to slide his tongue into my mouth. the hand at my waist pulls me in so close that you’d think he wants me to live in his skin.
the feeling of his tongue against mine was pure sweetness, the taste of him something i missed more than i thought. nothing about it was sloppy, it was passionate and slow. the way he would pull away just slightly with my lip in tow, low eyes watching as it snapped back into place before he captured it again in a kiss.
rafe groans when try to pull away, the sound followed by the hand resting on my face relocating to the back of my head to tangle itself in my hair. he deepens the kiss, teeth smacking together just barely as allows himself to be a little rougher.
humming in protest, i place a firm hand against his chest to separate us. my head pulls back when my boyfriend attempts to chase after my evading lips.
“just us.” i whisper, repeating the words that left his mouth just a moment earlier.
something in the back of my mind set off alarm bells at the way rafe smiled, the look in his eyes unsettling in the strangest way, but I tuned them out in favor on focusing on the way his lips felt on mine.
#rafe cameron#rafe cameron x pogue!reader#rafe cameron x reader#drew starkey#rafe cameron x kook!reader#rafe cameron x oc#obx fanfiction#outer banks#obx1#obx2#dark!rafe cameron#obx3#cleoluvrr fics
271 notes
·
View notes
Note
is it effective to use Furosemide for post-spay seroma in dogs or cats?
GV here.
No. Furosemide is a powerful diuretic designed to reduce overall total blood volume and/or induce urine production in urgent or emergent scenarios such as congestive heart failure, certain types of shock including anaphylactic, certain severe edemas, and oliguric or anuric kidney failure. It's never the *only* thing you do, either. In each of those scenarios you would be throwing a book of treatments at the animal. Also, furosemide runs the risk of being quite damaging to the kidneys even when used properly and is not designed to be used to stop normal, non-life-threatening inflammatory processes. Just getting rid of the fluid in a post-spay/post-surgical seroma is not going to get rid of any specific discomfort and definitely not a life-threatening problem, nor will it address the underlying issue (typically a combination of the body's reaction to the suture + excessive movement +/- infection).
23 notes
·
View notes
Text
This afternoon I had one of the worst doctors appointments ever, which is saying something, but at least I didn’t have a panic attack this time.
So in no particular order, I was told:
I obviously present feminine - in response to asking me my pronouns (they also gestured to my outfit, cane, and decorated rucksack, so I’m burning all of this and never wearing it outside again)
There’s nothing they can do as I’ve tried everything they can offer
To stop taking my meds as they’re not working, but no attempts to offer me anything new
That said medications aren’t even down as repeat prescriptions as they’re all for ‘acute treatment’ (note that I’ve been on these for almost two years for most of them)
Told that there’s no point me doing anything about my gender identity as the waiting lists are too long, and I wouldn’t be classed as a priority
That because I’m unemployed it doesn’t matter that I don’t sleep properly because it’s not like I need to get up for anything
The only place in the country that does immunology tests won’t test me as I’m not actively in anaphylactic shock so I need to find my own ways to treat my symptoms
When asking me about why I’m unemployed, they asked if it was due to pain, I said yes, but also because I don’t have the right qualifications because I had to drop out when I got sick, and they said ‘how sick? And how was it serious enough to drop out’ - I guess they completely forgot that I am permanently sick as in disabled ??
#dores world 🌍#disability#disabled#chronic illness#chronic pain#chronic fatigue#disabled life#actually disabled#spoonie life#doctors suck#doctors appointment
25 notes
·
View notes
Note
great allergy post btw!!
I think its easy to say good allergies aren’t that bad because they’re avoidable and the symptoms aren’t really chronic in the same sense that typical disabilities are. But my god the social effects! Having to bring your own food everywhere and be mindful about traveling and plane rides constantly is really draining after a while, especially with very common allergens like gluten or meat or egg. Like it’s crazy to me that most people can just eat whatever (like random food trucks in particular because damn I wish) because I’ve never gotten to do that
also the comorbidities! asthma alone accounts for a long term impact of allergen exposure.
people do not care to understand the severity of anaphylaxis and I've even been in first aid trainings where all they did was pass the Epi-Pen trainer around. a certain popular public charter [R.E.D.A.C.T.E.D] doesn't even mandate allergy certification through the first aid/cpr provider they choose. (a majority of first aid/cpr courses I've taken are phenomenal with allergy training fwiw)
ANYWAYS here are the signs and symptoms of anaphylaxis and what to do if you or someone is experiencing them!
If you or someone you know is experiencing anaphylaxis, call emergency services immediately. Do not delay care. If you're unsure, call anyways. Symptoms can be rapid or within 2 hours of exposure.
Do not delay care after administering epinephrine (Epi-Pen, Adrenaclick, Auvi-Q, etc), it is only temporary, hospital care is necessary.
Do not assume that someone with an allergy has an epinephrine injector, especially in places where you have to pay for healthcare.
If someone goes unresponsive and is not breathing during an allergic reaction, start CPR (adult | child+infant) immediately.

Image description: an infographic from the Food Allergy & Anaphylaxis Connection Team titled "SIGNS AND SYMPTOMS OF ANAPHYLAXIS"
Anaphylaxis (an-a-fi-LAK-sis) is a serious allergic reaction that comes on quickly and has the potential to become life-threatening. The most common anaphylactic reactions are to foods, venom, medications, and latex. Anaphylaxis signs and symptoms that may occur alone or in any combination after exposure to an allergen include:
MOUTH: itching, tingling, swelling of the lips/tongue/palate (roof of the mouth)
THROAT: hoarseness, tightening of throat, difficulty swallowing, hacking cough, stridor (a loud, high-pitched sound when breathing in)
LUNGS: shortness of breath, wheezing, coughing, chest pain, tightness
GUT: abdominal pain, nausea, vomiting, diarrhea
CNS/BRAIN: anxiety, panic, sense of doom
EYES/NOSE: runny nose, stuffy nose, sneezing, watery red eyes, itchy eyes, swollen eyes SKIN: hives or other rash, redness/flushing, itching, swelling
CIRCULATION/HEART: chest pain, low blood pressure, weak pulse, shock, pale blue color, dizziness or fainting, lethargy (lack of energy)
Symptoms involving the throat, lungs, and circulation/heart are marked with asterisks, indicating immediate and potential life-threatening symptoms.
Consult with a board-certified allergist for an accurate diagnosis and management plan.
Although the majority of individuals experiencing anaphylaxis have skin symptoms, some of the most severe cases have no rash, hives, swelling
EPINEPHRINE is the first-line of treatment for anaphylaxis Antihistamines, inhalers, & other treatments should only be used as secondary treatment. Always carry two epinephrine auto-injectors at all times.
When you, or someone you know, begin to experience symptoms, CALL 9-1-1 IMMEDIATELY!
FAACT Food Allergy & Anaphylaxis Connection Team
AWARENESS • ADVOCACY • EDUCATION www.FoodAllergyAwareness.org
(513) 342-1293 Fax (513) 342-1239
P.O. Box 511 West Chester, OH 45071 [email protected]
[end ID]
106 notes
·
View notes
Text
PLEASE DONATE IF YOU CAN!
I'm a struggling dialysis patient. On Feb 1, 2022 I went into anaphylactic shock and nearly died while at treatment.. Just asking for a little help. Anything is a blessing.

gofundme.com/account-overdrawn-need-help
#donation#donate#help#please help#financial aid#financial assistance#crowdfunding#michael jackson#king of pop#kingofpop#mj#mjj#mjfam#3t#tjjackson#dialysis#fundraiser#mutual assistance
24 notes
·
View notes
Text
playing open heart after watching house md is so funny to me because dr ramsey just tore mc a new one for annie going into anaphylactic shock because of the treatment but like…that’s step one of any dr. house case is to almost kill the patient to rule out the initial treatment theory…chill dude she’ll be fine
#i jest obviously theres a reason house is known for medical malpractice#hate crimes md#playchoices open heart#open heart#house md#my posts
6 notes
·
View notes
Text
People used to think I was a picky eater but I actually have what is refered to as a hypersensitivity, meaning it will make me sick and/or give me a migraine if I eat these foods. It's different from an allergy as it's not an anaphylactic reaction, good since it means I won't go into shock, and it probably won't kill me but bad since there's no treatment other than avoiding it. I was trying to save money by shopping at a discount grocery store but as it turns out a lot of that stuff is not labeled correctly and actually contained the stuff I was sensitive to. Long story short I ended up with multiple GI bleeds that the doctors couldn't find a reason for. Since I've cut out all the known issue veggies, tomatoes, bell pepper, and spicy peppers, I've had a lot less issues, but it means I have to avoid foods that have the ingredient "spices" listed.
i mean this in the gentlest way possible: you need to eat vegetables. you need to become comfortable with doing so. i do not care if you are a picky eater because of autism (hi, i used to be this person!), you need to find at least some vegetables you can eat. find a different way to prepare them. chances are you would like a vegetable you hate if you prepared it in a stew or roasted it with seasoning or included it as an ingredient in a recipe. just. please start eating better. potatoes and corn are not sufficient vegetables for a healthy diet.
149K notes
·
View notes
Text
9 Anaphylactic Shock Nursing Care Plans to Save Lives
Anaphylactic shock is a severe, life-threatening allergic reaction that demands immediate, coordinated intervention. Prompt recognition and rapid treatment are crucial to prevent respiratory failure, cardiovascular collapse, and death. Nursing care plans for anaphylactic shock provide a structured, evidence-based approach to manage this emergency. This guide outlines nine comprehensive nursing…
0 notes
Text
Food Allergies vs. Food Sensitivities: What's the Difference?

Food allergies can seem brutal. They can also be quite dangerous, causing issues like skin reactions and anaphylactic shock, where your tongue and throat swell, making a trip to the emergency room necessary. (1) Most people experience food allergies soon after consuming a specific food, like nuts or seafood. Still, food sensitivities can be mistaken for allergies and if not treated, won’t go away. Fortunately, there are some treatments and steps you can take today to understand the difference and how to test for various food sensitivities that remove the guesswork.
Food allergies
Your immune system’s job is to fight off foreign invaders that could be dangerous. Sometimes your body can get confused, and your immune system tries to protect you from something that may not be harmful, like specific foods. When you consume these items, you may get hives, difficulty breathing, airway swelling, and low blood pressure. (2) For anyone who has had this experience, it can be a frightening event. When your body releases histamine, it causes inflammation, and you can end up with a life-threatening reaction.
Common foods that cause allergies
Some typical foods cause more issues than others regarding allergies. There could be more, but we will round up the top foods that have the most historic problems for people who suffer from food allergies. (3)
Eggs
Milk
Fish
Nuts
Shellfish
Peanuts
Wheat Soy
Now, you may be thinking this doesn’t look like an issue because you don’t consume these foods. You may not realize how many of these are labeled as ingredients in condiments or other pre-packaged foods. Many marinating sauces and dressings contain soy, so if you feel a little off after eating a steak or salad, that could be why. It’s important to read labels carefully when shopping.
Food sensitivities
Food sensitivity is a digestive response rather than an immune reaction. That’s why you may not feel well after consuming dairy or gluten. You may experience issues like, bloating, cramping, fatigue, headaches, sinus issues, and joint pain. (4)
Food sensitivities can be hard to diagnose because they may mimic other issues and get grouped in with those. Some doctors hear complaints regarding digestive problems and tell the patients they have general IBS and write a prescription for the latest pharmaceutical. If this helps, and often it doesn’t, it merely covers up the symptoms and does nothing to find the root cause of the issue.
Causes for food sensitivities
If you think you have food sensitivity, it’s crucial to understand what causes it to fix the problem. The general thought is that people who experience these sensitivities don’t make enough digestive enzymes to break down a specific ingredient. (5) There are also gastrointestinal issues that make people more prone to food intolerances, like celiac disease.
When you have food sensitivity, your body is reacting to that food and can’t absorb the nutrients or has a negative reaction to them. Unlike food allergies, many people experience sensitivities to foods they’ve eaten in the past. These can even be healthy foods, like strawberries or broccoli.
How to identify trigger foods
Now that you understand the difference between a food allergy and sensitivity, you need to know how to spot the foods causing you issues. If you think you are having intolerances but can’t pinpoint which foods, it can cause a ton of frustration. You want to properly uncover the food culprit so you can rotate them or eliminate them from your diet for a while.
One of the ways you can do this is to try an elimination diet. That means removing one food at a time to see how your body feels. You could start with dairy and not consume it for one to two weeks, and see if your symptoms go away. Then remove gluten, and so on after that. Once you feel better, you can add them back one at a time until you uncover the trigger foods that cause the problem.
Easy way to pinpoint food sensitivities
Rather than taking weeks to months to figure out why you feel so bad when you eat, there is a simple and effective way to know which foods you need to remove. A food sensitivities test is quick and easy. A simple finger stick that you can perform in the comfort of your home measures 96 food antigens. You’ll also get a detailed report to help you improve your diet and remove the irritants causing you to feel bad. A phone consultation is included to help you understand the report and learn how you can navigate these issues to feel like yourself again.
The usual suspects
There are some foods that many people should avoid for better overall health. Some so-called foods today are packed with chemicals and unhealthy ingredients.
Gluten: Gluten can trigger an autoimmune response called celiac disease, which can cause damage to your small intestine. (6)
Sugar: Sugar can cause multiple issues, including digestive problems and inflammation.
Dairy: Dairy causes bloating and cramps for many people.
Processed foods: Processed foods are unhealthy for everyone and we should remove them from our diets as much as possible.
Feeling better soon
Since food sensitivities can be experienced soon after eating, you can also feel better when you know what foods to remove from your diet. A quick test can reveal what you should avoid. The interesting fact about sensitivity is that you may not need to eliminate the food forever. Some people can add foods they enjoy back into their diets once they feel better.
You also want to improve your overall diet with nutrient-dense foods that aren’t on your food sensitivities report. Consuming foods like bone broth, coconut oil, and fermented foods can improve your gut health, helping with sensitivities.
We have more resources on our website to help you understand how you can have a healthy lifestyle and heal many common conditions with a natural approach. Be sure to contact your chiropractor in Macomb MI to learn how to be a wellness warrior or for more information about holistic medicine.
#chiropractor in macomb mi#chiropractic care macomb mi#top ranked chiropractor in macomb mi#affordable chiropractor in macomb mi
0 notes
Text
In-Pulse CPR, Inc, incorporated in 2012 in Tampa FL is an American Heart Association Training Center offering a large amount of community classes at over 50 class sites in Tampa Florida, Minneapolis Minnesota, Nashville Tennessee, and Harrisburg PA. We also provide smaller private classes throughout these states. At In-Pulse CPR (www.inpulsecpr.com) we are committed to classroom excellence for the thousands of healthcare as well as non-healthcare students who have attended our classes.
We have a goal to perfect our classroom training to be the best Cardiopulmonary Resuscitation (CPR) provider in the state. We have over 30 instructors and hundreds of Mankins to provide training for all group sizes. Do you need to comply with bus driver or CPR in schools' mandates? We can help. Ask us about the schools and counties we work with.
Discover the In-Pulse CPR difference. It doesn't matter if you are a healthcare professional, a teacher, childcare provider, businessman or woman, laborer, student, parent, or just a neighbor. It is important that you are prepared for a cardiac emergency. Being prepared can make the difference between life and death.
At In-Pulse CPR, we feel that you CAN learn a lot from a "dummy". We offer a variety of open enrollment classes and times in multiple locations. These CPR certification sessions, first aid courses, bloodborne pathogen trainings and more can provide the training you need. We also offer onsite private classes for your group. Every class includes adult, child, and infant CPR training, including the treatment of an airway obstruction, recognition of an impending emergency, and clear instruction in the use of an automated external defibrillator or AED.
First Aid training is also available and includes but is not limited to: soft tissue injuries, bone and muscle injuries, medical emergencies (including diabetic emergencies), anaphylactic shock (including how to use an epi-pen) and environmental emergencies.
All of our instructors with In-Pulse CPR come with years of experience in the medical field and offer real life experiences to help trainees better understand the importance of CPR certification.
0 notes
Text
Since you know, we're all airing out our grievances with insurance companies, Cigna
I was dying from Lyme disease (which despite what the internet says can be deadly without treatment) and they refused to cover treatment so I had to pay $5,000 out of pocket to get the treatment to save my life
When I collapsed at work they refused to cover any section of the ER bill
I have been fighting with them for three years to get back MRI's and it took ending up in the ER and losing my job for them to finally approve the MRI's
I have had pneumonia for several weeks now and they are refusing to cover treatment due to it essentially not being bad enough
And I need to go see an allergist since I've been having symptoms of the start of anaphylactic shock so who knows if they'll cover that
Fuck insurance companies
0 notes
Text
Anaphylactic Shock Following Black Ant Sting: A Case Report by Deng Jingqi by Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
We present a case of a 36-year-old male patient who developed anaphylactic shock following a black ant sting. The patient exhibited respiratory depression and subsequent respiratory arrest, which posed a diagnostic challenge. The proximity of the patient to a large comprehensive hospital facilitated timely management. However, the lack of availability of essential emergency medications, such as adrenaline, in resource-limited settings like Sierra Leone hinders prompt treatment. This case emphasizes the potential underestimation and delayed intervention in cases of anaphylactic shock caused by encounters with large ants, which are not uncommon.
Keywords: Anaphylactic shock, Black ant bite, Respiratory depression, Resource-limited settings
Introduction
Anaphylactic shock resulting from encounters with insects has been reported in various regions worldwide, including the Americas, Australia, Asia, and Europe, but limited reports exist from West Africa. This case highlights the challenges in promptly diagnosing anaphylactic shock, particularly when respiratory depression and respiratory arrest occur. The patient's proximity to a large comprehensive hospital played a crucial role in facilitating immediate medical intervention. However, the unavailability of essential emergency medications, such as adrenaline, in resource-limited settings like Sierra Leone can lead to delayed treatment. It is important to recognize that cases of anaphylactic shock caused by encounters with large ants may be underestimated and not receive timely medical attention.
Case
A 36-year-old Chinese male patient presented to the Emergency Department of Sierra Leone China Friendship Hospital at 12:47, Dec 2ed, 2022. The patient reported being bitten on the toe by a large black ant (Figure 1) around 12:00. Approximately 10 minutes after the bite, the patient collapsed and complained of dizziness and difficulty breathing. On examination, his blood pressure was 83/55 mmHg, heart rate was 90 beats per minute, and oxygen saturation was 85%. The patient appeared cyanotic, and decreased breath sounds were auscultated bilaterally in the lungs. There were no visible skin lesions at the site of the ant bite. At 13:06, the patient became confused, and his oxygen saturation further declined. By 13:15, he experienced respiratory arrest. Patient's past medical history is unremarkable and there are no known drug allergies.
Resuscitation measures were promptly initiated. At 13:00, a 500 mL Ringer's lactate solution was administered to establish intravenous access. Intravenous dexamethasone 10 mg was given at 13:10, followed by manual bag-valve-mask ventilation and intravenous (IV) administration of adrenaline 0.3 mg at 13:15. Additionally, intramuscular promethazine 12.5 mg was administered at 13:20. The maximum heart rate recorded following adrenaline administration was 180 beats per minute. By approximately 13:20, the patient regained spontaneous breathing, his complexion improved, and he regained consciousness. On reassessment, his blood pressure was 125/85 mmHg, and heart rate was 95 beats per minute. The patient remained stable and asymptomatic for one day and was subsequently discharged.
The large ant that stung the patient.
Discussion
The patient's presentation is consistent with anaphylactic shock caused by an allergic reaction to the black ant bite. While the standard symptoms of anaphylactic shock include skin symptoms, respiratory symptoms, cardiovascular symptoms, gastrointestinal symptoms, neurological symptoms, and general symptoms, this case exhibited some atypical features. These atypical symptoms may not be immediately recognized as anaphylaxis without a high index of suspicion. In this case, the patient also reported nausea, profuse sweating, and a feeling of impending doom, which are consistent with the general symptoms of anaphylaxis. Additionally, the patient exhibited cyanotic skin, indicating compromised oxygenation, which can be observed in severe anaphylactic reactions.1
In the management of anaphylactic shock, the use of adrenaline is considered a cornerstone of treatment. Adrenaline acts as a potent vasoconstrictor, bronchodilator, and cardiac stimulant, effectively counteracting the severe systemic vasodilation, bronchoconstriction, and cardiovascular collapse associated with anaphylaxis. Intramuscular (IM) administration is the recommended initial route for adrenaline administration in the management of anaphylaxis, especially in non-hospital settings or when IV access is not readily available. The preferred site for IM injection is the mid-anterolateral aspect of the thigh.2 In this case, the decision to administer adrenaline via IM injection may have provided a faster route of delivery. At the onset of the patient's presentation, there was no initial diagnosis of anaphylactic shock, and the availability of adrenaline was not established. The subsequent administration of adrenaline via IV route resulted in an increased heart rate.
The limited resources in Sierra Leone, including the unavailability of adrenaline, further complicated the management of this case. Its absence in the hospital posed challenges in providing immediate and appropriate treatment. The use of alternative medications, such as intravenous dexamethasone and supportive measures like manual bag-valve-mask ventilation, was necessary in this situation. It is essential to increase awareness and preparedness among healthcare professionals in managing anaphylactic reactions, particularly when presented with atypical symptoms such as respiratory depression and respiratory arrest.3, 4 This case emphasizes the need for education and training to ensure early recognition and prompt management of anaphylactic shock, even in resource-limited settings.
Conclusions
This case highlights the challenges in promptly diagnosing and managing anaphylactic shock, particularly when respiratory depression and respiratory arrest occur while without skin injury or symptom. Prompt recognition and immediate medical intervention are crucial in preventing adverse outcomes. Healthcare professionals should be prepared to handle anaphylactic reactions, even in resource-limited settings, by ensuring the availability of essential emergency medications. Increased awareness and education can improve the recognition and timely treatment of anaphylactic shock caused by encounters with large ants.
Disclosure: The authors declare no conflicts of interest and received no funding for this report.
#Anaphylactic shock#Black ant bite#Respiratory depression#Resource-limited settings.#Resource-limited settings#Journal of Clinical Case Reports Medical Images and Health Sciences.
0 notes