#Traumatology
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
#osteosynthesis#trauma#surgery#traumatology#orthopedics#fracture#orthopaedics#surgeon#ortopedia#orthopedic#vet#scoliosissurgery#scoliose#spine#escoliosis#escoliosebrasil#orthopedicsurgery#veterinary#osteosentez#ortopedi#orthopedia#doctor#osteosynthese#orthopaedicsurgery#scoliosis#residencia#pek#anklefracture#fraktur#traumasurgery
0 notes
Text
A 12 Day- Old Female Infant Diagnosed with Pelvic Osteomyelitis in the Pediatric Emergency Department by Mehmet Ali Oktay in Journal of Clinical and Medical Images, Case Reports

Abstract
Osteomyelitis (OM) is a bacterial disease that is very rare in newborns and has devastating consequences. Neonatal OM is seen in 1-3 in 1000 babies. We presented a 12-day-old female baby who was brought to the Pediatric Emergency Department (PED). Because she could not move her leg. She did not have fever and septic appearance and had a history of hospitalization in Neonatal Intensive Care Unit; acute phase reactants were high and radiological imaging performed gradually was consistent with OM. Our patient is the youngest patient who was diagnosed with pelvic OM upon admission to the PED. Earlydiagnosis and treatment prevent complications and sequels. Keywords: Osteomyelitis; newborn; pediatric emergency
Introduction
Osteomyelitis often occurs secondary to the hematogenous spread of microorganisms into the blood-rich metaphysis of the developing bone. When left untreated, it leads to complications such as joint destruction and decreased range of motion [1]. Osteomyelitis (OM) of the hip is rare in newborns. Signs and symptoms are quite different compared to older children. This may cause difficulties/delays in diagnosis and permanent disability [2]. Successful management of OM in the neonatal period has been associated with rapid correct diagnosis and adequate correct treatment [2, 3]. The incidence of OM in the pediatric age group is 1/5000 cases. About 50% of pediatric OM cases are under the age of five. The incidence of neonatal OM is 1-3/1000 cases [3]. Although there are studies on patients diagnosed with osteomyelitis while staying in neonatal intensive care unit (NICU) [1, 4, 5], cases diagnosed upon PED (Pediatric Emergency Department) admission are very rare [6]. In this article, the youngest case in literature who went to the PED and was diagnosed with pelvic and acetabulary OM is presented.
Case Report
A 12-day-old girl, born from the first pregnancy of a 28-year-old mother, was admitted to the PED with complaints of restlessness and inability to move her right leg. The day before the application, it was stated by her mother that she did not move her leg, that she was agitated when forced to move, and could not be consoled. The baby did not have a history of fever or trauma, her feeding was good, and her urine and defecation were normal. From her history, it was learned that she was born at 36 weeks and 3 days of gestation and had intrauterine growth retardation compatible with 31 weeks gestational age, and she was born by emergency cesarean section due to preeclampsia. The patient, who was hospitalized in the NICU due to temporary tachypnea of the newborn after birth, was discharged on the sixth postnatal day. During the follow-up in the NICU, umbilical catheterization was not applied to the patient. She had not received antibiotic treatment and no growth was detected in blood cultures taken before discharge.
At her evaluation in the Pediatric Emergency Department triage area, she was a restless baby with a good general appearance. Vital signs; body temperature was 37°C, heart rate was 140/min, respiratory rate was 42/min, pulse oximetry was 98%, and mean arterial pressure was 45 mmHg. There was no pathological finding in the physical examination, and it was observed that the patient's discomfort increased due to the position given to the hip and leg while changing the diaper. While abducting the right thigh from the hip in the supine position, there was limited range of motion compared to the left. No swelling or redness was detected on the joint surface.
Laboratory and radiological examinations were planned for the patient with a preliminary diagnosis of septic arthritis. In laboratory tests: hemoglobin (Hb) 14.6 g/dL, RBC (Erythrocyte) - 3.361 x10.e6/uL, hematocrit (Hct) 40.04%, white blood cell (WBC) 16.82 x10.e3/uL, neutrophil percentage 59.8%, C-reactive protein (CRP) 25.9 mg/L, erythrocyte sedimentation rate (ESR) 51 mm/hr, procalcitonin (PCT) 2.95 ng/mL, IL-6 145.6 pg /mL detected. On direct radiographs of the lower extremity and pelvis, the right femoro-acetabular distance was observed to be increased (Figure 1). Long bone radiographs were normal. In the superficial tissue ultrasound (US) performed for the right hip joint, bilateral hip joints were compared with each other, and no significant effusion was observed on the right side. The patient was consulted to the Orthopedics and Traumatology department with a preliminary diagnosis of septic arthritis. MRI was requested from the patient for the differential diagnosis of septic arthritis.

Figure 1: There is an increase in the right acetofemoral distance compared to the left.
Bilateral hip MR imaging showed “The right femoral head is small and irregular in appearance, and an area of pathological signal change in the right femur proximal metaphysis, medullary bone marrow, and solid periosteal reaction in the lateral proximal section is observed. Widespread edema was observed in the surrounding muscle planes, fascial surface and subcutaneous adipose tissue adjacent to the hip joint. In addition, medullary bone marrow edema was observed in the right acetabulum (osteomyelitis). Areas of pathological signal changes consistent with diffuse edema are observed in the right obturator externus, pectineus, quadriceps muscles, gluteal muscle planes and iliacus muscle (myositis). Minimal free fluid was observed in the right hip joint space. Findings were primarily evaluated as compatible with osteomyelitis and myositis.” (Figure 2).

Figure 2: Osteomyelitis in the proximal metaphysis of the femur
Due to the history of hospitalization in the intensive care unit, the patient was diagnosed with OM secondary to hematogenous spread and, according to the age, to include possible infectious agents, vancomycin (15mg/kg/dosex3), ceftazidime (30 mg/kg/dose x 3), fluconazole loading (12 mg/kg/dose)) and maintenance (6 mg/kg/dose) treatment was started. Blood culture was taken before antibiotic treatment. Our patient, who received antibiotic doses only one day before the operation, was operated on the postnatal 13th day.
The patient was operated by the Orthopedics and Traumatology department and the intra-articular pus was drained. From the material; joint fluid culture, fungal culture, tuberculosis PCR, ARB staining, fungus search was sent. There was no growth in the blood culture, but because of the growth of ceftazidime-resistant Klebsiella pneumoniae in the joint fluid culture, ceftazidime was discontinued and meropenem (20 mg/kg/dosex3) treatment was started. Fluconazole was discontinued on the 8th day because there was no growth in the fungal culture. The patient was discharged with oral trimethoprim-sulfamethoxazole treatment after 25 days of vancomycin and 27 days of meropenem treatment. Trimethoprim-sulfamethoxazole was discontinued 22 days after discharge. The regression of the inflammation was seen in the MRI taken under the control of the outpatient clinic. verbal consent was obtained from the patient's parents for the publication of the article.
Discussion
This case demonstrates the importance of detailed investigation of newborn infants admitted to PED. Although OM in newborns is rare, there are difficulties in diagnosing and treating it. High suspicion is required for early diagnosis and observation of clinical signs is very important.
Risk factors for osteomyelitis in newborns are stated as immature host-defense mechanisms, invasive intervention such as umbilical catheterization. It has been shown that half of the cases diagnosed with neonatal OM have a history of umbilical catheterization. It has been observed that the pregnancy and delivery history of the mother is also important in the development of OM, and maternal complications such as maternal hypertension, preeclampsia, ablatio placentae, infection are present in approximately half of the infants who develop OM [7]. Particular attention should be paid to the evaluation of newborn cases, especially in PEDs where is crowded and the number of patient admissions is high. Newborns are among the patients at risk for PED and require special care. Application complaints and prenatal, natal and postnatal history should be questioned in detail. It was observed that the mother of our case had preeclampsia during pregnancy, but umbilical catheterization was not applied to the baby.
In studies conducted in newborns with neonatal osteomyelitis, the most common sites of involvement were reported as femur, humerus, and tibia, respectively [1, 4, 8]. The pelvis is a rare site of hematogenous disseminated OM for neonates. Pelvic OM constitutes 2.3% of all childhood osteomyelitis cases [3]. Our case also had pelvic (acetabular) OM, which is a rare site of OM involvement. Involvement was also demonstrated in the proximal region of the right femur.
Pelvic OM was defined in three cases at 5, 15, and 18 days in the neonatal period [3, 9, 10]. In the literature, it has been observed that mostly cases hospitalized in the NICU were diagnosed with osteomyelitis [1, 3, 4, 8-10]. As far as we can find in the literature, a 4-week-old case with a diagnosis of distal tibial OM and culture of GBS has been reported, just like our case [6]. Our case is the youngest OM case diagnosed in the emergency department, except for the case in the literature. The clinical features, presentation symptoms, cultures and risk factors of cases diagnosed with neonatal osteomyelitis in the literature are shown in (Table 1)
Table 1: Comparison of cases with neonatal osteomyelitis in the literature.
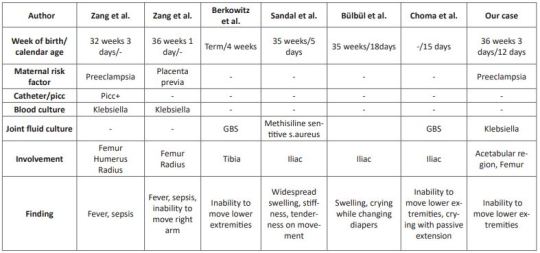
Clinical symptoms are related to the bone or joint area involved in newborns. Swelling and local inflammation findings are common findings in the neonatal osteomyelitis group. Systemic findings such as fever are seen in fewer of these cases. A highly variable rate of fever was found in 9.1-76.5% of patients with extensive neonatal osteomyelitis. In addition, it has been shown that the WBC count, CRP and ESR levels are high in the cases [1, 4, 8, 11]. In our case, there was no fever, but there were complaints of inability to move her right leg and restlessness. Laboratory parameters were high and consistent with the literature. In cases with osteomyelitis, direct radiographs can guide the correct diagnosis, exclude other diagnostic possibilities, or provide clues for underlying pathological conditions [12]. Soft tissue swelling on plain radiographs can be seen within days of the onset of infection. It can also show periosteal reaction, lytic lesions, joint effusions and destructive bone changes 7-10 days after the onset of infection [13]. US findings begin with nonspecific swelling in the soft tissues adjacent to the bone. US can show thickening and elevation of periosteal and subperiosteal fluid collections as early as 3 days [14]. In a study comparing osteomyelitis groups, it was shown that the diagnostic value of US was statistically higher in the newborn group compared to the other groups, regarding the capacity of detecting subperiosteal abscesses [11]. In our case, however, an increased femoro-acetabular distance was observed on direct X-ray, but no finding was found on US. This supports the view that the primary step in the pediatric emergency department in patients with suspected osteomyelitis should be started with direct X-ray as recommended in the literature.
MR imaging is the most useful imaging technique for evaluating suspected OM, allowing early detection of osteomyelitis and assessment of the extent of involvement and disease activity. MRI is very sensitive in detecting OM 3-5 days after the onset of infection [12]. As seen in our case, it still remains the gold standard. However, we recommend hospitalization in order not to miss the newborn cases because MRI is difficult in emergency conditions.
In infants, osteomyelitis and septic arthritis often coexist. While Staphylococcus aureus is the most common organism causing osteomyelitis at all ages, GBS and Escherichia Coli are important pathogens to be considered in newborns [6]. Culture is found to be negative in 22-50% of the cases [15]. Antibiotics to be used in neonatal OM should be effective against these pathogens [16]. In our case, treatment with antibiotics covering these pathogens was applied and Klebsiella pneumoniae growth was observed in the pus culture.
We think that even with rapid diagnosis and aggressive treatment, there are orthopedic sequelae and inadequate treatment increases the risk of chronic osteoma [16], therefore, in cases who apply to the pediatric emergency department with these complaints, early diagnosis and treatment of neonatal OM should be planned in a timely manner to minimize long-term sequelae.
In conclusion, a detailed anamnesis should be taken and a careful physical examination should be performed in newborns who present to the PED with limited range of motion at joints. Neonatal OM cases mostly consist of cases diagnosed while staying in the NICU. Pelvic involvement is rare and our case is the youngest pelvic OM case diagnosed in the PED.
For more details : https://jcmimagescasereports.org/author-guidelines/
#Osteomyelitis#newborn#pediatric emergency#Pediatric Emergency Department#OM#PED#catheterization#RBC#C-reactive protein#hematocrit#Traumatology#Mehmet Ali Oktay#JCMICR
0 notes
Text
personal little reference i mocked up for sherlock and john :p
#i hesitated to post this for a while because i didn’t want to get flamed for any inaccuracies but#i put a lot of research into traumatology and translated those specifics into something more suitably stylized#so it’s an honest attempt and ah ha yeah please don’t ‘uhm actually-‘ me LOL#the scars on sherlock’s back are odd but that’s on bbc sherlock alright i copied the wound pattern from a screencap#tw scars#cw scars#my art#the @ is my insta#fanart#fanartist#art#sherlock#bbc sherlock#sherlock holmes#john watson#johnlock#benedict cumberbatch#martin freeman#gen
289 notes
·
View notes
Text
the er is so full someone please save me

#it's either the flu or traumatology adjacent stuff (which i hate)#and people get so mad for the wait times but... it's full already#what do they want? squeeze themselves into another patient's bed?
2 notes
·
View notes
Text
being a medical student or working in the medical field is so traumatizing cause on moment its like ur making toast with nutella and ur brain is like hey remember when [the most traumatizing moment to ever happen] happened and youre just like …. yeah
#the most traumatizing floors ive ever been on have been pediatric traumatology#and then second place pediatric oncology#third is gyno when there are minors as patients … man.#when i had to comfort the pregnant ten year old who was catatonic 😟#i would never want to return to pediatric traumatology tho#plus the lead coats were heavy and hurt my back
1 note
·
View note
Text
And it paints the hospital floor a nice and children friendly shade
blood is so cool
76K notes
·
View notes
Text

Journal of orthopedic case reports publishes Images in Orthopaedics Case Reports Journal, Orthopaedics Journal, Case Reports in Orthopaedics etc. Journal of Orthopaedics and Traumatology Case Reports provides an equal platform to orthopaedic based medicine as well as personal experience and every case report should reflect these important concepts.
#Journal of Orthopaedics#Journal of orthopedic case reports#Traumatology Case Reports#Images in Orthopaedics Case Reports Journal#Case Reports in Orthopaedics
0 notes
Text
.𖥔 ݁ ˖𝐄𝐘𝐄𝐋𝐄𝐒𝐒 𝐉𝐀𝐂𝐊 𝐇𝐄𝐀𝐃𝐂𝐀𝐍𝐎𝐍𝐒 ꒷꒦ ๋࣭ ⭑

★ Jack speaks fluent German as he’s from Germany!
★ Since relying on his other senses, they have heightened significantly over time. He heavily relies on his touch especially due to having to bandage/stitch/treat wounds.
★ Has very sharp teeth, which is very useful to him as it’s easier to bite into kidneys, as well as any kind of organ for that matter.
★ Jack’s body is unable to digest actual food. His only source for food is organs directly from humans, which he hates having to rely on.
★ He chooses to eat kidneys because it’s the least disgusting organ to him. After years of consuming them though, he’s gotten used to the taste.
★ Very knowledgeable in both medicine and traumatology. He’s really good at identifying the injuries the creeps return with, especially major ones, to which he knows exactly how to treat. He’s almost a professional!
★ Spends a lot of time reading. He mainly reads medical related books, but he’ll occasionally read novels. It’s his favorite pastime.
★ Actually knows how to knit! He used to previously take classes when he was still human. He often knits bandages for him to use to wrap the other’s wounds.

★ He cannot stay in front of the sunlight for too long as his skin will begin to blister and burn if he does. He’s pretty much similar to a vampire in a sense.
★ Growls in his sleep. It’s a very faint growling though, so you’d have to be very close to him to hear it. He denies it.
★ Has a soft spot for animals. There was a time where he found an injured kitten in the forest. He quietly took it in and took care of it until it was at full health again.
★ His height is around 6’9.
★ One of the most reserved and quiet pastas. He speaks when absolutely necessary, and when he does, he likes to focus on the topic being discussed. He’s not the type to switch the subject. Other than that, he’s normally just listening to the voices or conversations of others.
★ Has a monotone voice. It’s hard to tell if whether or not he’s upset at times.
★ Not a very emotional person.
★ Jack is the one who gathers his own medical supplies. He feels as though it's his own responsibility to do so.

#creepypasta#creepypasta headcanon#creepypasta headcanons#eyeless jack#crp#slenderverse#slenderverse headcanons#headcanons#jack nyras#self indulgent!
152 notes
·
View notes
Text
Fuck it I'm gonna say it, Dragons Rising 2 coming out literally a few days after I went to therapy and got signed up for traumatology because of textbook symptoms of PTSD and/or CPTSD, with Lloyd now having panic attacks and implied PTSD too, Bonzle being another trans allegory after Sora, AND Arin being even more autistic coded, really made me feel seen. I love this show so much
#when one of my special interest shows make me feel seen like that#ninjago#lego ninjago#dragons rising#dragons rising 2#ninjago dragons rising#ninjago spoilers#dragons rising spoilers
285 notes
·
View notes
Text
Long live the pathology book, reading that caused me to self-diagnose, suffer through, and then miraculously survive 5 different types of cancer and at least 2 deadly infections all within a week.
Since then, I accepted that one day, I'm going to drop dead and there's nothing I can do about it. But all the other days? I'm going to live.
being in medical school is turning me into a hypochondriac dhjshdksh whaddya mean you can drop dead from infective endocarditis without any prior symptoms or only innocuous mild symptoms ehjsdjksjsls whaddya mean autopsies show that in 10% of deaths in younger populations theres evidence of infective endocarditis dhskdjskks im gonna scream
#when in med school#you are going to realize that everything is out there to kill us#especially our own body#i still don't understand how we don't drop dead a moment after we are born#it's a miracle that we live#and im amazed by this miracle every day#how many people survive despite all odds#the human body is terrifying but also amazing and beautiful in its working#but that being said#there's probably a reason i am in traumatology#less things here to be hypochondriac about
70 notes
·
View notes
Text
I posted this on reddit, but I've seen some gnarly posts about Venezuela here, so I'll post it here too.
"I'll try to answer all of them. I don't know if I can explain like you're 5 because I'm autistic af and English is not my first language, but I hope I can make myself understood.
I condemn practically everything about the government. In Venezuela, on average, only four out of 10 operating rooms in the country's main hospitals are operative, and the shortage of supplies in emergency rooms is around 37%, while in operating rooms it reaches 74%. As for my own experience, I have Classical Ehlers-Danlos Syndrome, I had a shoulder subluxation and I still do, and I went to the Victorino Santaella hospital in my country, there's little personnel, to the point that in the area for traumatology you could see dry blood on the floor because there just wasn't enough people to clean it up. Not a little bit of blood, but a lot. If you want decent medical attention, you will have to pay a bunch of money.
I had a strangulated umbilical hernia, which again, is something that commonly happens with the EDS. My dad had to spend 4000$ dollars on the operation, which for us, is a unachievable amount of money. He had to sell his car, and beg his job for the rest of the money, because the car was old asf and only covered about 200$.
Many people say the government is progressive, it is not. In Venezuela the LGBTQ community has absolutely no rights, it's incredibly difficult for trans people to change their documents or access hormonal treatment. Abortion is not legal here, not even in rape cases, gay marriage isn't legal either, and domestic violence largely goes unpunished.
The minimum wage is around 3 dollars, my dad works in transit so he earns minimum wage, because I have so many medical emergencies he has to make illegal driving licenses in order for me to get treatment. It is incredibly hard for my mom to find a job.
If you want an overview of the whole political situation, this thread can explain it better than I can:

This also explains many of the faults with the government, really, there are too many, I can't count them all.
There’s also no freedom of speech in Venezuela due to Nicolas Maduro’s oppression. All the news channels that are available are on his side. CNNE was removed from Venezuela after doing a documentary on Maduro and also was DW. Our only way to inform ourselves are socials, and most venezuelans are speaking through there.
Maduro's government is not a socialist government anymore, it paints itself that way to outsiders, but it is not. Money that should be going to public institutions is not going to those institutions, hence why the hospitals are in such dire state and you have to pay for private clinics in order to get appropriate care. I don't know if you're familiar with the CLAP bags, The Local Supply and Production Committees (CLAP) is a distribution program of some basic imported foodstuffs promoted by the Venezuelan government since 2016 in which the communities themselves organized in committees supply and distribute priority foods through a modality of delivery of products, house by house at first, later distributed in a local of the community. The problem with these is that they're frequently infected with weevils, maggots, and even if they look "good" on the outside, they can be infected with bacteria and give you food poisoning. Worse is, some people are entirely reliant on these.
They're supposed to protect our indigenous people, but a Venezuelan indigenous leader who opposed the incursion of armed groups and illegal mining was shot twice while in a neighborhood in the capital of Amazonas state. Maduro is also the richest man in Venezuela.
In the protests that occurred in 2017, around 150 people died thanks to the armed forces and colectivos (paramilitaries on the side of the government), police came out with tanks (idk the name exactly in English) and ran over people who were peacefully protesting. Right now, I believe there has been 11 people confirmed injured, though there's probably more, since hospitals are asking for resources to treat the injured.
I think most of these payment methods are only available in Venezuela, but I saw a Paypal here and there, if you can help I'd thank you so much:

As for the self-sufficiency, I don't know. As I said, I'm 17 and heavily reliant on my parents. This country's also really not accessible for disabled people, I cannot go down stairs and have to walk with a cane, there's rarely a place where elevators are functioning properly: ironically, especially in hospitals. In the hospital Victorino Santaella, my dad has to carry me through a bunch of stairs, he has a bunch of hernias in his back so that's obviously no good for him. I'm also at heavy risk of fainting, so yeah.
Also: I don't know how the housing situation is in Venezuela statistic-wise, but for the young adults, is impossible to get a house. Houses can cost up to 100.000$ and more, the average job will pay enough for you to eat, buy toilet paper, basic needs and that's about it.
My friends, who were studying university, couldn't finish cause they had to get a job in a supermarket or bakery in order to be able to support their parent economically. It's horrible.
We also have no running water, when we do it's brown, our power goes off all the time and I have no health insurance"
Do I support María Corina? Or the opposition? I'm skeptical about them, they're still politicians, and Machado is a Zionist. I'm worried about idolizing these figures, deeply. But there's no alternative guys.
For gringos saying that we are supporting fascists, and whatnot. We have literally no other option. This didn't start with US sanctions, it just got WORSE with them. But these sanctions are a symptom, not the root of our problem.
Please, listen to venezuelan voices. If you're really a leftist, just a bit of research will be enough to convince you that this is NOT even a socialist government anymore.
#anarchocommunism#anarchopunk#anarchy#anarchist#anarcho syndicalism#socialism#venezuela libre#free venezuela#venezuela#politics#cripplepunk#cripple punk#is it ACAB until it's Venezuela?
70 notes
·
View notes
Text



Simon Riley realizes how much touch starved he is due to his physical therapy.
Pairing: OC (Female, Dr Eavanson) x Simon "Ghost" Riley
w.c: 2.5k
Warning: Fluff, a little twisted Simon I guess, a small sexual inuendo. English it's not my first language.
••••••••••••••••••••••••••••••••••••
Due to his work, Simon Riley is a man accustomed to looking death in the eye, but his skill has helped him dodge it, avoid it, and even mock it to the face a few times.
But what he could not escape, no matter how hard he tried, was the pain.
Although adrenaline and satisfaction also accompanied him, sometimes, when he and his team completed a mission.
But those pleasant sensations went away when the pain knocked on the door. It was always there, like the shadow of a bad thought.
At least it reminded him that he was still alive, and not just another «Ghost» wandering through the valleys of violence.
A few months ago, while he was deploying a mission to capture one of many criminal gangs in Afghanistan, Simon and his team were cornering the leaders when suddenly one of those damned people managed to hit a bullet in his right shoulder, almost hitting his shoulder blade.
It was incredible how such a small object could transmit such a heartbreaking sensation that reached half of his body.
Fortunately, that did not prevent the capture of those scum, but the price of pain was quite expensive to pay.
The pain is what brought him here, in a seat in the waiting room of your medical office. Although the doctor successfully removed the bullet, the impact affected several muscles in his shoulder which prevented him from handling his weapons with the mastery that characterizes him. Therefore, they gave him a medical leave to recover, away from the battlefield.
Simon snorted in annoyance at the memory of his superiors demanding him to take the leave. They also recommended a doctor specialized in traumatology in his homeland, in England, who could carry out his therapy.
As hard as it was to accept it, he knew he needed therapy, so his body would be in optimal condition, just like before.
-Mr. Riley? -The receptionist, a middle-aged woman behind her desk, caught his attention- You can now go into the office, Dr. Eavanson is waiting for you.
Simon stood up from his seat and walked to where the woman indicated. He carried his hands in his pockets as she knocked lightly on the door and then opened it.
Simon didn't know what to expect, he thought you were a gray-haired man who was in charge of this office.
But there you were, a mirage of a delicate figure behind your desk visualizing something on the computer. Seeing you again, Simon felt something tense inside him, the receptionist closed the door behind her, leaving the two of you alone.
You raised your gaze to where he was and smiled kindly at him, Simon didn't know what to do, he was frozen, for a second he thought you had caught him and knew all the paralyzing sensation you caused him in just a few moments. "What's happening to me?" he thought to himself.
-Mr. Riley, right? -Finally, your welcoming voice broke the walls of silence. Simon was able to escape from his trance to nod slightly.
-It's nice to meet you, I'll take care of you today. I was reviewing the X-ray plates of your shoulder along with the medical file, I see that you have an injury in the supraspinatus muscle. Is that correct? -You got up from your seat and took a few steps to approach your new patient, Simon, but he, the lituanent who led a group of soldiers with the same strength and violence as he possesses, and who had experience in fighting against equal or worse subjects...
He took a step back at your approach, as if it were by instinct.
You realized that gesture, and then looked at him a little strangely.
Simon cursed himself inwardly. He was acting like a stupid teenager, or worse, like an antisocial who doesn't know how to deal with people, he had to do something.
-Yes. -He answered, finally while composing himself- That's right. The doctor who treated me in the camp made the same diagnosis... And therefore assigned me a series of therapies.
He almost let out a sigh of relief when he saw your face lose the signs of strangeness that you had shown a few seconds ago.
It was strange, normally he didn't pay attention to what others thought of him.
His mind began to search for an answer to the question that formed inside him. Why was it different with you?
-That's right. -You affirmed with the same smile.-Fortunately, in cases like his, recovery is guaranteed if you undergoes a series of therapies.
Simon nodded as he listened... while he used an effort to contain the desire of his eyes to travel something further below the borders of your face, he didn't want you to notice him doing that, while you looked at him straight in the eye.
-But first, I have to examine you. Could you undress and sit down on the stretcher, please? -Suddenly all of Simon's thoughts fell silent, as you pointed with your head to the stretcher that was on the right side of the room. And a coat rack to hang clothes.
«Shit» when he saw you he had totally forgotten that he had to undress in front of the doctor who was going to treat him.
He just didn't take into account that it was going to be someone like you.
In those microseconds where he tried to dilute his little panic, he glanced at you while you were checking something on your iPod.
You didn't seem to give the matter any big importance, anyway, for you it was just another body to check.
But for him, it was a body formed by years of work, but it was also full of tattoos and scars, in which each trace of them contained hundreds of stories. Some he still knew by heart, others... Not only were they too obvious, but the memory was also very present.
But the problem wasn't him, he wasn't embarrassed at all by his appearance, the problem was you... He didn't know how you were going to react to seeing a body like his, nor... Nor if you were going to like it.
He couldn't just stand there either.
Simon started by removing his black jacket, feeling the bother sensation by his right shoulder, then finishing with his long-sleeved shirt of the same color. He hung them on the clothes rack, and proceeded to sit on the strecher, feeling it soft at the same time he heard the squeal beneath him.
He assumed that was what announced to you he was ready for the evaluation. You put your iPod on your desk and went straight to where he was.
There, Simon's eyes escaped from their prison to be able to quickly and discreetly explore a little more of what he had already been able to capture.
You were smaller than him, without a doubt, even when he saw you sitting at the desk he realized. You barely reached the height of his chest.
His honey-colored eyes lowered a little more, until they met your neck. It was firm, not willing to allow your head to look down at any eventuality, and the skin that protected it looked so soft and delicate.
Simon wondered how many times you had covered it, not only from the cold weather, but to protect it from the curious glances the love marks made by some lucky indiscreet lover to whom you allowed such audacity.
Although you were not carrying any by now, he made sure of that.
His eyes lowered further, and found the protective layer that was your white coat and the blue uniform, those in your profession usually wear.
He did not deny he was only a little disappointed, since his imagination would have to cooperate to draw the shapes hidden beneath the layers of fabric.
But it did not matter, the best part was in front of him, totally accesible to his sight.
Your face.
-Well, I am going to examine the state of your shoulder with a series of movements to evaluate its condition - You announced, while you positioned yourself in front of him.- It is important that you let me know if you feel any pain, since that way I will know what type of therapy will be the most appropriate for you, okay? -You looked into his eyes to get his approval, Simon looked back at you and nodded.
-Okay.
-Perfect, let's get started.
You took the wrist of his right arm, and raised it slightly while your other hand gently rested on Simon's affected shoulder.
-I'm going to move your arm in a circular motion.-You announced again to begin to make the movements, gently.- From one to ten on a pain scale, how do you feel it?-She ask him.
Nothing could prepare him when he felt the touch of your soft fingers on his rough skin. He had to use an effort to contain the small exaltation that his body emitted.
Until you began to move his arm in a circular motion.
The sensation that the movements caused on his affected shoulder reminded him of the reasons why he was right now here, the pain was not as intense as the days after his operation. But it was still very annoying, he tried not to let the pain be reflected in his gestures.
-Seven. -He confessed.
-Perfect. -You snapped. You left his arm in the original position.- I'm going to repeat the procedure with another exercise, the conditions are the same. -You assured him with your voice that he felt as velvety in his ears.
You took his right arm wrist again, except this time you gently bent his arm until you were directing his hand towards his left shoulder, where your other hand was resting.
To do this, you had to put your arm around Simon's back, who was a significantly larger person than you.
But the one who was aware of all this was him, who felt his breathing stop for a moment, as he felt your delicate arm surround the skin of his back, which he felt was getting warmer and warmer.
While your chest was only centimeters away from coming into contact with his skin.
After months and months of combat, where many times he faced each other in hand-to-hand combat, using the power of his strength to weaken the enemy or using his perfect technique in the execution of weapons, where many times his opponents responded with scratches, bruises, blows, or even bullets, like the last time.
This was the first time he felt how physical contact with another person... did not imply some kind of harm to him.
And suddenly he realized, he realized after all these events how much he needed at least some small kind touch after the sea of violence he subjected himself to day after day.
He felt his heart ache a little below his chest.
Simon looked back at you, and imagined how he took advantage of the position to take you in his arms and place you on his lap, while you allowed his mouth to finally capture yours in an almost suffocating way, but you responded in the same expectant way as he did.
-From one to ten on a pain scale, how do you feel? -Your voice takes him out of the perfect imagination in which he was submerged, he answered quickly to pretend he never imagined such scenes with you just a few seconds ago.
-Six.
-Perfect. -You answered with your warm smile.
And so the first therapy session with you passed, where Simon had to honor his good sense of self-control, and for the first time in his life he realized he was almost on the verge of losing it.
-Very well Mr. Riley, you can put your clothes back on now. -You kindly indicated while looking into his eyes, Simon did as you asked, surprised that time had passed so quickly- As I suspected, the injury from your wound does not present a depth that supposes a serious magnitude, fortunately -You went to your desk to record with your computer the physical examination that you performed in detail- Therefore, you have been prescribed two sessions of physical therapy including interferential therapy for five weeks starting next Thursday.
Next, you removed two copies of the prescription from the printer. You gave a copy to Simon, who was already dressed and in front of the desk, which he took very willingly.
-On the prescription, write down two painkillers that will help you a lot with the pain and the necessary doses.-You indicated.- That's all for today, we'll see each other next Thursday, Mr. Riley, take care, and if you have any questions, you have my phone number that you can call- You assured, then getting up from your chair and offering him your hand as a momentary farewell, which Simón gladly took.
Since it was the last trace of contact with the one he would have to survive until his next meeting.
-Thank you very much for everything, Dr. Eavanson. See you next Thursday.- He said in farewell, then opening the door that separated him from the outside world... From you.
Darkness had already fallen over the city, and Simon was inside his apartment with the light off, on his bed, ready to finally rest. He had already taken the medicine you recommended, and for the first time in months, his shoulder was no longer bothering him so much in this position.
With his head on his pillow, he began to think on today's events.
After thinking for a while, he discovered that what happened a few hours ago had never happened to him before, until he was under your touch.
And he didn't understand why, certainly the last mission was one of the longest he had had in his career, where the only people he saw daily were his teammates.
It is true that he couldn't remember the last time someone had touched him in such a delicate and kind way.
And well, he had already gone on long missions before... And he had also touched other women in the past, and they had touched him too.
But none of them caused him the slightest bit of what you did. Even though they had only known each other for less than half an hour.
And after thinking, and thinking without coming up with any logical answer, he simply stopped looking for an answer, and dedicated the last moments of his day to enjoying the beautiful moments he spent with you in the walls of your doctor's office.
And with that he posed a question that perhaps would never have a clear answer: How would you react... if Simon lost the self-control he had left?
What would you think of all the things he had done with you inside his mind without you knowing?
Without a doubt, he was going to attend all his therapies.
•••••••••••••••••••••••••••••••••••••••••
I'll be glad for any sugestion 💘.
M A S T E R L I S T
38 notes
·
View notes
Text
Marine Academy chapter 8
Note: Chapter 8 on 28. Akainu X OC. OS is called Murphy.
THIS CHAPTER IS NSFW ! It's soft but still NSFW.
Please, do not forget, English is not my mother language and translate this kind of scene is pretty hard for me, sorry !
Marine Academy Part 1 Chapter 8
"Left on a mission, no return date".
Murphy reread for the hundredth time the letter written in hurry by Sakazuki an hour after his second departure. It was not planned at all.
She was supposed to take her physical exam at the end of the third semester and spend the evening with him to tell him how catastrophic her sword handling was.
The blonde had nearly failed her exam, within one point, allowing her to validate her semester, only thanks to the intense training session the previous weekend with Sakazuki.
Murphy still remembered how, the next morning, before she started the exam, a soldier she had once seen around Sakazuki, had discreetly gave her this letter. She had learned later that indeed, about ten second years had been called on a mission with the third years. This choice had been made at the last minute. Sakazuki had no choice but to write this letter in hurry during the night before leaving, to inform her.
It had been five long months since he had left. Once again, no letter or call but she now understood why.
But the moment had been particularly badly chosen given the events of the day before he left, when they had exchanged their kiss after training. And as usual, she had smiled at him and left , leaving him under the stars on the training ground. But when she remembered that he had responded vigorously to her kiss after a few seconds, it reassured her.
She stuffed the letter in her pocket, took a deep breath and pushed open the doors.
The jury was waiting for her, sitting on a bench. Murphy took a seat behind the desk, took out her thesis and began reading it.
Once the physical and theorical exams were over, she had entered the fourth semester where she was beginning scientific research.
Her semester had focused mainly on the theory of the various medical specialties and she had to select a topic from one of the specialties to develop a second-year dissertation. It was obviously only the first steps of real scientific research, but the blonde had invested herself body and soul in this file. She had obviously chosen a problem related to emergencies.
"Emergency care in patients with a Logia-type devil fruit, approach and particularities." Murphy began in front of the particularly attentive jury.
Her presentation lasted half an hour, as requested. Her file was clear, supported by scientific data and her experience during her various internships since entering the Academy.
"Thank you." Concluded one of the jury members whom she recognized as the head doctor of traumatology at the Marineford's Grand Hospital Marineford. She left the room in silence, letting the jury fill out their evaluation form discreetly.
When she closed the doors behind her, Claire, and Emma who had already made her presentation the day before, were waiting for her impatiently.
[...]
"Another bottle!" Emma yelled throughout the tavern.
The waiter arrived immediately, placing a bottle of sake in the center of the table, skillfully picking up the other empty bottles.
The brunette's descent was now known to the entire Academy, she was unbeatable. Claire, however, remained close to her, ready to grab her hair in case of an emergency exit... Murphy, for her part, was content to watch the scene, laughing, her yellow cocktail in her hand.
"Well, ladies." The brunette began in a brief moment of lucidity, as she tried to open the bottle with her bare hand.
"I want to congratulate us all on our exams! And good luck to our brilliant friend Claire, who is going to start her very last semester and cowardly abandon us."
The redhead had also finished her fifth semester exams and was going to start the final semester of the third year before finishing her studies at the Marine Academy.
The dorm would seem particularly empty without Claire's wisdom and calm.
As they were clinking glasses together, enjoying these last moments together, a soldier invited himself to the table of the three students. Emma had already grabbed her new bottle, ready to smash it on the soldier's skull, but was held back by Claire.
"Good evening Murphy. I was asked to warn you of Sakazuki's return. They arrived at the port half an hour ago."
Emma's eyes lit up, a psychopathic smile on her lips. "Murphy, do you hear that? It's time to wrap things up, my dear! Otherwise he'll slip through your fingers as soon as he finds another pretty blonde at the port!" The brunette yelled, drinking her glass of sake in one go.
The blonde, embarrassed by her friend's yelling throughout the tavern, hid her face in her hands. But she couldn't hide the smile that had just appeared on her lips at the announcement of Sakazuki's return.
"Murphy! Murphy! Murphy!" The brunette continued to yell throughout the tavern, quickly followed by complete strangers who were just as drunk as she was. Claire rolled her eyes at the whole mess and made discreet signs to the blonde to invite her to leave through the back before things got completely out of hand.
Murphy didn't need asking twice. She took her bag and slipped discreetly out of the tavern. The cold of the night bit her skin, she had forgotten her jacket in the bar. She jogged down the streets to warm up and stopped in front of the window of a store that was strangely still open at this hour.
She widened her eyes when she recognized the storefront.
"Jackpot!" The blonde said as she slipped inside. Her heart warmed in an instant when she smelled the aroma of cakes. Murphy bought two slices of cake, thanked the vendor and set off again at full speed through the streets. The snow was starting to fall. After a good ten minutes of running, which for her was an achievement despite the intensive training she had received from Sakazuki, she slipped through the back door of the large building.
She knew this parallel and discreet path from sneaking up with Sakazuki. She finally arrived in front of his bedroom door, a few snowflakes still in her hair, her dress slightly soaked with alcohol or snow, she wasn't sure.
Her hand hit the door twice, trying not to drop the box of cakes. She hoped that the man had come back directly from the port and hadn't been delayed, so that she could take refuge near her radiator.
No response. Murphy pressed her ear to the door and heard the shower water running. He probably hadn't heard it. The young woman tried to operate the handle and miraculously, it wasn't locked. The blonde slipped into the room, announcing her arrival anyway.
"Sakazuki! It's Murphy! I'm coming, I'm freezing!" The blonde said, putting the box of cakes on the coffee table. She heard the shower water turn off.
In the meantime, she curled up in front of the radiator, sighing with relief when the gentle heat warmed her frozen hands. "I hope you don't mind me coming in, but it's freezing outside and we're not all made of magma..." She continued, laughing.
She felt the man behind her approaching. Murphy turned to greet him but stopped short. He was half-naked, a simple towel around his hips, soaking wet. One of his legs was covered with a scar that had barely healed. His face was closed, no emotion appeared.
This cold face was no longer familiar to her. As they spent time together his features had softened, he had lowered his guard little by little and she no longer felt like she was facing a robot. But that cold face transported the blonde two years back to their first meeting.
She hesitated for a moment. Maybe she had crossed the line? Like Emma had told her, maybe he had met another pretty blonde on a port and their whole story (which was not that long after all) was already in the past for him after these five long months of absence…
"If I bother you I can come back later". Murphy whispered as she slowly got up. She felt like a hummingbird facing a cat ready to jump on her.
"I brought you a cake for your birthday." She continued, pointing at the snow-covered box on the coffee table. Smoke was coming out of Sakazuki's soaked chest, who still hadn't moved.
"I know your birthday was last month but since you weren't there I thought we could still..." The blonde didn't have time to finish before the soldier jumped on her.
She reflexively stepped back, her back lightly hitting the radiator. She felt the man's torso fall on top of her. The young woman found herself completely lying on her back on the carpet, at the foot of the sofa. She felt soldier's body envelop her, his warmth covering every inch of her skin, his right arm sliding down her back to press their two bodies together, his left hand getting lost in her blonde hair. And finally his lips pressed to hers, ardently asking for the right of entry. The man's burning body warmed her frozen body.
She responded in a few seconds to the man's burning kiss, her hips sticking to those of Sakazuki, her back arching under his caresses.
Her heart exploded at this mixture of emotions. Fear and surprise had given way to a burning pleasure of finding the man again and the desire to stay glued to his skin for hours. His kisses migrated to her neck, allowing her to breathe briefly. His left hand went down to her chest, passing under her dress. She shivered as she felt the man's powerful and warm hand caress her while he devoured her neck. As she felt herself completely weak and giving herself body and soul to the man, she stopped for a second, her forehead pressing against his.
"On the bed." She ordered.
She then felt her body take off from the ground quickly. She found herself almost standing, still in the arms of the man who continued to devour her, going from her lips to her neck. She wrapped her legs around his hips. He put his right arm on the woman's buttocks to better support her. He carried her to her room and did not let go of her for a single second as he laid her down on the bed, their lips remaining sealed. She took advantage of the fact that he was above her to lower her hands to her towel which she untied in a second. The proximity of the blonde's hands made him shiver. He hurried to take off the woman's dress for good, admiring the blonde's immaculate skin for a moment. His face went down to her chest while his hand went down to the woman's intimacy. Another burst of heat invaded the young woman when he caressed her. She buried her hands in his hair, her body burned with pleasure.
"Saka..." She whispered.
The blonde's murmur of pleasure excited the man who could not wait any longer. She was perfect, offered in front of him, and begging him. He could not hold back any longer and entered her slowly, his excitement at its peak as she screamed his name with pleasure with each of his thrusts. He felt all control leave him as she screamed his name, arching under him.
She obsessed him, he had dreamed of this moment since she left, his needs guiding him further and further into his fantasies. Holding out for so long without being able to touch her had been a real battle, he had to manage alone all this time, and this night was going to be the realization of all his fantasies. He gave one last thrust, releasing himself inside her at the same time as her as she screamed his name in a final orgasm. He collapsed on top of her carefully, pulled the covers up over them, taking her in his arms so she wouldn't get cold and let sleep take them.
7 notes
·
View notes
Note
Where did Stork learn to pilot if he spent most of his life in the Wastelands? Are there flight schools on Terra Merbia that accept merbs like him?
Prefer to think of him as self-taught. He mastered the art of piloting on his own, relying solely on old books, prehistoric airplane simulators, and own experience, formed from a lot of trial and mistakes.
Don't think any flight schools would accept such desperate merbs, given that Terra's surface is not very tolerant of the likes of Stork (remember my headcanon about the capture of merbs by humans). For this reason, merbs will never choose a skimmer: it creates a huge risk of sudden kidnapping in the sky. In addition, without proper preparation, it is very easy to fall from it. In the conditions of a difficult merbian life, there was no guarantee that the main parachute would open the first time, and this is already a direct path to traumatology.
I'm still inclined to believe that they prefer more reliable ways of navigating the sky instead. The most optimal solution is for aircraft with closed cabins, equipped with advanced protective equipment in order to minimize various risks. At the very least, this makes them a much stronger choice in favor of most merbs, which is especially important in the conditions of the heavenly element (it may also be one of the reasons Stork was previously afraid to leave Condor). Often, merbs make work trips to transport necessary goods, or go on regular business trips to perform other important tasks. Driving skimmers is strictly prohibited, and may result in a fine or community service (However, under other circumstances, my Hector would often break these rules).
In later episodes, Stork gradually learned to overcome his cowardice, which could make him the first merb to not only break one of the main stereotypes about his people, but also become a real phenomenon in the world of aviation. Although he has no formal training, he is one of the most talented pilots in Atmos, and without him, the squadron would never have achieved the results we saw in the show. His contributions are invaluable and having him on board is partly the key to their success. Nevertheless, the real test of running the Condor continues to be dealing with the crew, getting them to all agree on a course of action, and the endless stream of crises that arise.
You know, it's pretty funny that I'm the one who gets asked almost all of the Stork-related questions :D. At this rate, he'll be my OC soon, lol.
9 notes
·
View notes
Note
aaron for the ask game 🫶
ofc don't we love to break his ass 😈
How I feel about this character
have to admit, was not a die hard fan at first, but i also wasn't a hater at all. i think coming out of the tripping-balls adventure that was the trilogy, from Neil's pov, you just can't help not having Aaron on your radar, yk? but the second time, and all the times after that... ohohoho what a delight!! his one-liners are as bomb as his twin's - he is an overflowing pot of trauma and it is so so sooo yummy - man's is MOTIVATED - he's so fun to play with and put in the torture labyrinth - he is good at Exy - and his Barbie doll goes with almost everyone! he is my sweet, sweet boyo, and perhaps one of the Foxes' i most resemble? so much potential to unlock fr. we haven't even looked at the iceberg below, trust me.
All the people I ship romantically with this character
MY SPECIALTY. We got:
Kevin - Katelyn - Kevin & Katelyn & Thea - Kevin & Thea - Jean - Jeremy - Jean & Jeremy - Seth - Kevin & Seth - Matt - Matt & Seth - Matt & Kevin - Neil (crack) - Allison - Robin - and i think that's enough, rizzleman
My non-romantic OTP for this character
i think Matt? oh and Kate.
My unpopular opinion about this character
i don't see him going into Pediatrics. i'm thinking smth more like orthopedic surgery, or traumatology/ER? maybe oncology, even. he likes bones i feel. don't look into that. like obviously he'd be good with kids, and he would ace it in that department, but i just don't think it's what he likes best.
One thing I wish would happen / had happened with this character in canon
neilaaron bestfriendisms.
17 notes
·
View notes
Text
New Year's Eve part. 21
You know the rules, and so do I. See the rest of the saga on @corneille-but-not-the-author and @hel-phoenyx 's blogs <3
TW hospital
I know this hospital rather well. So many hours wandering in these corridors... Of course, they wouldn't let us see them until they're stabilized. I know some of the nurses in ER and traumatology, because I often have had accidents and injuries from 15 to now, with my bike y'know, and during my famous year on the streets, got a few broken bones. The nurses told me about a concussion. Because of a brick.
Heh. Headshot.
...
It will be funny when Sigi's walking out of here.
Tyr isn't doing way better. He is obviously thinking about his friend. He stays still, doesn't even try to sit somewhere. He looks so aloof. Doesn't even notice my antics.
Shit, you know what? I'm out. I send a text to Egill for him to join me here, just to chill over there.
I'm trying to keep my cool but inside I'm boiling. Last time I got there in that context, Tyr lost his hand.
I don't want to lose my boyfriend.
I don't want to lose Sigi I love him too much for him to die...
"Damn, you surely look bald", I shout as soon as I see my brother. "How's it going, my favourite cancer patient?"
I can't hug him. What a shame.
"Welp, I beat skin cancer but the bastard was found in my stomach. But I beat him once", he chuckles. "Still have xeroderma, though."
"Some things never change", I smile. "Missed you."
"Missed you too."
He makes his drip roll as he walks slowly towards me. He seems tired, and is skinnier, but overall? Better than I thought he would. I offer him my arm, but that kid is mad proud.
"You look distraught, Dom."
"My boyfriend is here. Concussion. He is unconscious."
"That's rough, buddy", he comments. "How did it happen?"
"A brick in the head during a protest", I say. "To be fair it's... It's not a good day."
"You betcha."
***
Egill, Tyr and I are now playing in a dark corner, away from any solar light, with a small ball and a nursery rhyme. Tyr has seen Fenrir. The man is stabilized. That's... reassuring.
And apparently, for Sigi, we got more scared than hurt. Won't have any sequela, but they will keep him for a few days in observation.
I've shed enough tears in this fucking place.
"I think you can see him now", Egill finally says, breaking our rhythm. "It will cheer him up."
"You think?" But before I can get giddy for that, I sigh loudly. "I might run into his parents. They don't know about us."
"What, they're like, observant Muslims?" he laughs. "Ya'Allah Masuda with who are mingling with? It's enough to have Amine and Qamar in our family!"
"In my humble opinion", Tyr replies, "the Warsowar are Christian. I am not sure what kind, but regarding how the mayor stigmatises Islam..."
"You got a point", I say. "It's a Polish surname, right? They must be Catholic."
"Heh, not necessarily", Tyr pursues.
"You know what? If you're not going I'm meeting asap my future BIL. No offense Tyr, but I know you since I'm able to walk so it has less of an impact", Egill declares as he seizes the ball.
***
I follow my brother after he puts on his protective gear, and we walk as we are bantering like siblings do. I love my siblings, you know? That's my babies. My baby siblings.
Even if Qamar is getting married in May but hey, I digress.
One thing about the Lulea: I got that white-passing, Qamar is visibly an Arab and a Muslim, and my brothers... Egill was more visibly racialised with his thick curly black hair and his designer stubble, but even now he is like a hairless mole you wouldn't say he is white. And Sigsteinn is pale as fuck but that's on his unspecified illness (Lou Gehrig's Disease, so far? we are actually still in the blur).
So...
Hm.
Yep.
If we run into the mayor and his wife, I don't know what we will do but we will surely do something.
I mean I helped the mayor find his glasses while on my date with Sigi, but I'm not sure my face stuck in his memory.
And I don't know how to answer the "who are you" question. Don't want to put my darling in a difficult situation.
We find the room.
"I think he already has visits", Egill notices. "If you don't go, I go."
"Egill we..."
"Wa'Allah Masuda since when are you getting cold feet from that sort of stuff? Where's my big sister who's just YOLO-ing through life?"
I snort.
"I'm scared to mess things up with Sigi..."
"Relax. From what you've said about him, he kinda match your freak. Or at least he is not bothered by your silliness." He smiles warmly. "It'll be fine. And you'll eventually meet his family so the sooner the better."
And fuck it he has me. I am perhaps stupid and impulsive. But that's me. I blunder all the time. Sigi loves me, so he loves that part of me. And I love Sigi. It's a hard time for him, so I have to be there. To help.
"I'm going first", I say.
And so I do.
To meet with two middle-aged persons. A man, with glasses, the guy I helped. The mayor. His father.
And a woman, holding Sigi's hand, with a cross on her neck. His mother.
Egill enters just after me.
"Heyyyyyyyy- llo sir, madam", my brother immediately greets. "Well that's awkward."
Sigismund is awake, but visibly confused and tired. With a huge bandage around his head. My heart breaks at this sight.
"Who are you?" the father asks. Yep. He doesn't recall me. I really don't like how he stares at me with his cold blue eyes.
"I'm Domhildr", I almost yell, pretty embarrassed with myself. "This is my brother Egill. I'm..."
"Oh, I know you", the woman says softly. "You're Sigismund's friend."
At these words, Sigi turns his gaze to me. His eyes widen.
"Yes, yes I am!" I want to disappear. I hate how those persons are dissecting me.
Well.
Perhaps.
Wearing one of my bimbo skirts and a crop top wasn't my best move.
"I learnt through one of his colleagues he got hurt and I got really worried and-"
"I'm glad Sigismund has such great friends", the mother continues. "You perhaps want some time together without us..."
Mister Warsowar doesn't look happy about it, even if he smiles. Yep. He doesn't like me. That's good because I don't like him neither.
"Sarovar, we should maybe go talk to a doctor to let Sigismund and his friend alone for a bit..."
"Yes, we should", he agrees with that fake warmth I find oddly off-putting. "We will be back soon, son."
Egill remains silent. He perhaps tries not to be seen. Well, it seems to work. They leave the room. Egill closes the door. I jump to Sigi's bedside.
"What are you doing here", my boyfriend mutters, visibly not quite grasping what's happening.
"I'm your girlfriend and you're at the hospital, you dummy", I say while trying to hold back tears. "I learnt and I got worried. I needed to make sure you're okay."
And in from of his silence, I continue:
"I'm happy it's not that bad... wa'Allah Sigi I thought I lost you!"
"You're not the one who got the brick in the head", he softly answers.
He tries to look reassuring but it doesn't feel right.
"Well I should perhaps get going", Egill says. "Have fun, loverbirds."
Now we're alone. I look him in the eyes, holding his hand. He lowers his gaze.
"You perhaps just put me in an... unfortunate situation with my parents, you know, Domhildr?"
"Would you rather have me not coming, darling?" I smile faintly. "I'm also in your life to take care of you, y'know. Would you have it any other way?"
He thinks for a bit, before exhaling.
"You're too cute, I can't stay mad at you", he lightly chuckles.
"I knowwww right?"
I stroke his hand without another word for a bit.
"But if you want me not to come tomorrow and the day after, say the word. Otherwise, I'm here tomorrow with strawberries."
"You're impossible..." but he smiles more sincerely.
"I know, but you love me."
"Yes, I indeed love you", Sigi says as he squeezes my fingers with tenderness.
"And I love you too."
4 notes
·
View notes