#Symptoms Of Suicidal Behavior
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
Catching Early Signs And Symptoms Of Suicidal Behavior | Solh Wellness
Despite being a severe and very troubling problem, suicide is not a mental illness. Instead, it symbolizes the excruciating and sometimes disastrous outcome that can be brought on by mental illnesses that are not appropriately managed or treated. From severe depression and bipolar disorder to post-traumatic stress disorder and substance use disorders, these underlying diseases span a wide range. We will talk about the early warning signs and symptoms of suicidal behavior in this conversation, as well as the precautions a caregiver can take.

Suicide Warning Signs:
Being able to recognize suicide warning signals is essential for early intervention and support. These warning signs include various mental and behavioral changes, such as:
Persistent Emotional Distress:Swings in mood, unplanned outbursts of rage, or protracted, extreme depression may be signs of underlying emotional pain. For instance, a typically upbeat person can go through a prolonged depressive episode.
Overwhelming pessimism: A red flag might be an extremely negative outlook on the future and the conviction that nothing can be done to change it. A complete lack of hope or the incapacity to envision a brighter future are common expressions.
Sleep Disturbances: Sleeping patterns that significantly alter, such as difficulty falling asleep or excessive sleep, may be a sign of mental distress.
Abrupt Calmness: An abrupt and speedy return to tranquility after a period of sadness or rage could be cause for alarm. This sudden calm could be a sign that the person is prepared to end their life.
Social Withdrawal: Depression, a key risk factor for suicide, may manifest as a loss of interest in once-loved hobbies and a preference for isolation over social interaction. Avoiding your friends or favorite pastimes is one way to do this.
Personality or Appearance Changes: Suicidal individuals could exhibit observable changes in their mood or behavior, such as speaking or moving unusually quickly or slowly. They could also appear to be unconcerned with how they look.
Self-Destructive Behaviour: Suicidal ideation may be indicated by negative behaviors that put one's safety in peril, such as reckless driving, unsafe sexual behavior, or increased substance misuse.
Recent Life Crises:Suicidal thoughts can be sparked by major life changes including the loss of a loved one, the end of a relationship, the diagnosis of a serious illness, the loss of a job, or financial difficulties.
Preparatory Actions: Some persons who are contemplating suicide start to organize their affairs, which may include calling or visiting friends and family, donating things, creating a will, or setting up their living space. You may even leave a letter behind.
Verbal or implied threats: Many people who are considering suicide will unintentionally or overtly tell acquaintances or family members. These safety measures could entail often discussing mortality or saying things such as, "It would be better if I weren't here." Because not everyone will be truthful about their intentions, suicide threats need to be taken seriously.
The caregiver should take the following activities if a loved one is exhibiting suicidal behavior:
When compared to people who experience social isolation, having supportive friends and family and having access to mental health facilities dramatically reduces the risk that someone will act on suicidal thoughts. If you come across someone who exhibits indicators of suicide ideation, keep the following in mind:
Initiate the Conversation:Ask if they are depressed or considering suicide without fear.
Enquire About Treatment: Ask if they are currently taking any medications or going to therapy.
Offer Hope:Reassure them that depression is a temporary illness that can be treated rather than attempting to talk them out of suicide.
Show You Care: Some people merely want to be liked and to know that others are receptive to hearing their worries. After that, you can convince them to seek expert assistance.
Conclusion
Untreated mental illnesses like depression, bipolar disorder, and substance use disorders can have dangerous side effects, one of which is suicide. Early warning signs include persistent mental anguish, excessive pessimism, sleep issues, social withdrawal, personality changes, self-destructive behavior, recent tragedies, preparation acts, and verbal threats. When a loved one exhibits symptoms of depression or suicidal ideation, caregivers can help them by talking with them, asking about treatment options, expressing genuine concern, and offering encouragement.
Since we at Solh think that mental health is important, we have selected a variety of effective self-help techniques to improve your mental wellbeing. We provide a variety of services, including goal-setting, mood analysis, self-assessment tests, journaling, and access to a vast collection of educational materials. Utilize our wide range of self-help resources to take control of your path to improved mental health and personal growth.
#Symptoms Of Suicidal Behavior#Signs Of Suicidal Behavior#Suicidal Behavior#Mental Illnesses#Suicide
0 notes
Text
we went over the 14yr long torture session in my last therapy visit actually, and i told her that toward the end i was fantasizing about and then actively considering walking into traffic because if i got catastrophically injured then they would have to treat my pain. and she told me that's not an uncommon thing for people to do. that she has heard that many times before.
like think about that. we are so moralistic about drug use and have politicized a particular type of medicine so much, and doctors are so uncompassionate toward and even suspicious of patients who are in pain because of it, that it's NOT UNCOMMON for people who are otherwise not suicidal to start completely genuinely longing to get hit by a fucking car just for the chance to be oh so graciously provided the absolute bare fucking minimum of care.
think about how many different things have pain as a symptom. how many things have pain as the only symptom the patient is aware of. how many of them are life or death crises. heart attacks. blood clots. strokes. bleeding ulcers. those are just what i can think of off the top of my fucking head, AND I'M NOT A FUCKING DOCTOR.
what i had, for example, feels exactly like appendicitis. and they left it for fourteen years because my only symptom was excruciating pain and i didn't fit their stupid little (completely unsupported by evidence, btw) diagnostic mnemonic. if it had been appendicitis, or anything else as immediately deadly that "just" hurts, i would have fucking died the same night i got sent home from the emergency room with "medical" "advice" to take some tylenol and rest - for the first time, that is. out of dozens. how many people do die that way?
because addicts are Bad. and because doctors are too arrogant and biased to practice medicine on the basis of evidence and informed consent when the profit model and conservative propaganda make it soooo easy to stay in the good old days of paternalism instead.
#jack facts#medical#soc#i want to tag this ''opioid crisis'' but i truly don't think i can manage to type it without the quote marks lmao#and like my thing and none of the things i mentioned are fixable via opioids obviously and fucking obviously i know that#but the fucking circus about opioid use and how prescribing opioids Must be avoided at All Costs No Matter What#results in this Us vs Them mentality of The Treacherous Drug Seeker vs The Nurse/Doctor Too Smart To Be Fooled#which is precisely why i said in my last post that they're ''like cops''#they have this perception that they are being constantly rushed by the lying swindling Enemy#and are so smug about it when they believe they have magically divined when someone reporting pain is faking or exaggerating#based on whatever the fuck they individually have decided is Drug Seeking Behavior TM TM TM#which are almost fucking always just normal fucking behavioral responses to pain and fear!!!!#and then that person is not a Patient (as cops are to Victim) they are instead an Addict (as cops are to Criminal)#and that person not only does not get pain relief they don't get anything the god damn fuck else either except a fucking attitude#and people fucking die. of whatever is hurting in the first place or from their endurance for endless torment running out.#disproportionately women and people of color and fat people and the mentally ill and disabled and the poor and children and the elderly and#nurses/doctors ���� cops 🤝 soldiers 🤝 ceos 🤝 mass murderers who are socially celebrated for heroism#not to put too radical and fine a point on it or anything lol#ANYWAY#i'll probably delete this or at least the tags lmao#whatever. i'm going to go lie in bed and have symptoms until 6 am when i have to get up to go be retraumatized at the medical lab :)#neglect#drug use#suicide#car crash#illness#ask to tag
14 notes
·
View notes
Text
Like a whole other thing is when I have put Mani/Moe in situations where suicide as a topic is part of the punchline, I am so cautious about it, and there's always a greater intention behind it. Biggest thing is the characterization -- this is a part of its history. Moe's experiences inform a lot of its feelings, choices, even core personality. It's also a distinct characterization of Mani. A reflection of the past. Mani is more prone to becoming volatile and destructive. I have so much lore in my head I can never elaborate on LMFAOOO (SCRAMBLED. EGG). But that is the point/idea behind it, and I am always So Careful. I don't do anything without intent.
#suicide ment#moe tag#mani tag#something something moe is a healer. bc ofc it fucking is LMFAOO#i feel like. i have so many thoughts. but i cannot fucking articulate them LMFAOO#idk moe is like a rescue animal.#LIKE. I FEEL LIKE A CORE PART OF MOE AS A CHARACTER. is the fact that it's doing better now#but it never fully 'recovered'.#it still has mental health struggles/conditions. but it's well-managed and at this point moe is more practically minded about it.#like maybe an even bigger part of moe's entire fucking character. is that you can't 'fix' it.#one bc some things were never meant to be fixed. an impossible task that led to nothing but trauma.#examples would be its gender identity/queerness in general and being autistic. those are things you can't 'fix'#and things that. never should be 'fixed'. bc they are literally not problems.#two. idk how to word it. but some things can't really be fixed but in a different way than the prev example.#but you manage the symptoms of it. change harmful behavior. practice damage reduction as much as you can.#already i am so tired and i'm gonna thrup trying to explain the difference. but please i am begging you. there is one. just trust me.#like having self-harming tendencies deeply ingrained in you is wholly different. i wish i had the fucking words to explain it.#but that IS. a core aspect of moe. capturing how these things have impacted it#and also. having gotten to a point where it stays silly.
3 notes
·
View notes
Text
Starting to wonder if I have bipolar but then I would literally have almost every mental illness. Like fr I'm not kidding you, I'm a collector and I never chose this
#it does run in my family since my mom had it#i just wonder because while im almost always suicidal the way that prevents itself can greatly change very quickly#like periodically ill be stuck to my bed very sad very mopy for like 3 weeks to 3 months#and then sudden i get this burst of false energy that is actually severe restlessness#and i NEED to do something when that happens. sometimes i just cannot sleep because ive gotta do something#sometimes i frantically draw or write and ill have these moments where i feel ecstatic and when i come back to normal levels of sadness#im convinced i mustve been delusional to think the thoughts that i had then#usually the sadness isnt as bad during those periods but the suicidality is much worse actually because i become very frantic#and have so much more energy#idk. my theory thus far has been either 1) adhd causing mood dysregulation and hyperactivity#2) fluctuations in my depression and anxiety combating each other. actually both of these.#or 3) DID. just DID. i think thats lretty self explanatory#the interesting thing is that i think what i described with point 1 and 2 would be clinically considered bipolar...?#listen clinicians dont always consider the other factors that contribute to what symptoms the person is having#especially in psychology where the lines are very blurry since diagnosis tends to be made on behavioral observations#and also on self reported symptoms.i suspect im one of the only people who would describe symptoms like 'im having x because i have y'#and not just 'im having x symptom'#skfjfh sorry to everyone who reads my tags 👍 psychology special interest go brr
14 notes
·
View notes
Text
haha why on earth is the most effective method to stop self destructive behavior just: make it inconvenient and be apathetic about everything
#like why have I (mostly) stopped cutting?#I do not care and taking care of it is more effort than I can be bothered to deal with ¯\_(ツ)_/¯#why did I stop starving myself?#my scale ran out of batteries and I could not be bothered to replace them#also I just Do Not Care anymore#why did I stop trying to get drunk in the middle of the night?#bc alcohol is gross af and I don't care enough about the effect to deal with it#why did I stop arguing with everyone and everything?#because it's too much energy I don't care anymore#why did I stop trying to trigger myself?#looking things up = effort. I don't care#why'd I stop considering suicide?#killing yourself is too much effort to plan and do#... my view on none of these things really changed#I don't think they're bad or anything#I just can't be bothered to do any of them#and that's more effective than just trying to reinforce that these are Bad Behaviors#ofc I have heard that extreme apathy is a depression symptom so take that as you will ¯\_(ツ)_/¯#ah but whatever#r.r#sh#sui#ed
2 notes
·
View notes
Text
Mental Health Insights: From Disorders to Treatment Strategies

Mental health is an essential aspect of overall well-being, impacting how we think, feel, and act. Understanding various mental health disorders and their treatment strategies can empower individuals and communities to foster a healthier society. In this blog, we will explore key topics including erectile dysfunction, dementia, schizophrenia, bipolar disorder, obsessive-compulsive disorder (OCD), and more, providing insights into their causes, symptoms, and effective treatment options.
Understanding Erectile Dysfunction
Erectile dysfunction (ED) is a condition that affects many men, often leading to emotional distress and relationship issues. The causes of ED can range from physical health problems, such as diabetes and heart disease, to psychological factors like stress and anxiety. Diagnostic tools, including physical exams and psychological assessments, help healthcare providers determine the underlying causes of this condition. Treatment options vary, including medication, lifestyle changes, and therapy, making it crucial for individuals to seek help when experiencing symptoms.
Dementia: Symptoms and Treatment
Dementia is a progressive condition that affects cognitive function, leading to memory loss, impaired reasoning, and changes in behavior. Common symptoms include confusion, difficulty with communication, and mood swings. Among the various types of dementia, Alzheimer’s disease is the most prevalent. Understanding the behavioral and psychological symptoms of dementia (BPSD) is vital for caregivers and healthcare professionals. Effective treatment strategies can include medication, cognitive therapy, and support from family and friends, ensuring that individuals with dementia maintain a good quality of life.
Demystifying Schizophrenia
Schizophrenia is often misunderstood, with many misconceptions surrounding its nature and treatment. This chronic mental health disorder can cause delusions, hallucinations, and disorganized thinking, severely impacting daily functioning. Dispelling myths about schizophrenia is essential for reducing stigma and promoting empathy. Treatment typically involves antipsychotic medications and psychosocial support, allowing individuals to manage their symptoms and lead fulfilling lives.
Bipolar Disorder: Navigating Mood Swings
Bipolar disorder is characterized by extreme mood swings, ranging from manic highs to depressive lows. Understanding the complexities of bipolar disorder is crucial for effective management. Early symptoms may include changes in sleep patterns, energy levels, and irritability. Treatment strategies often involve a combination of medication, therapy, and lifestyle adjustments to stabilize mood and enhance coping skills. By understanding the nature of these ups and downs, individuals can better navigate their mental health journeys.
Obsessive-Compulsive Disorder (OCD)
Obsessive-Compulsive Disorder (OCD) is a condition marked by intrusive thoughts and compulsive behaviors. Symptoms can manifest as persistent fears or worries, leading to repetitive actions aimed at reducing anxiety. In India, societal perceptions of OCD may lead to stigma, hindering individuals from seeking help. Effective treatment includes cognitive-behavioral therapy (CBT) and medication, helping individuals manage their symptoms and improve their quality of life.
The Future of Brain Stimulation for Mental Health
Innovative approaches, such as brain stimulation, are shaping the future of mental health treatment. Techniques like transcranial magnetic stimulation (TMS) and electroconvulsive therapy (ECT) have shown promise in treating conditions like depression and schizophrenia. These therapies work by modulating neural activity, offering new hope for individuals who have not responded to traditional treatments. Continued research and development in this area are essential for expanding treatment options for various mental health disorders.
Personality Disorders: Complex Behaviors
Personality disorders encompass a range of complex behaviors and emotional challenges that can impact interpersonal relationships. Conditions such as borderline personality disorder and narcissistic personality disorder can lead to difficulties in social and occupational functioning. Understanding the nuances of these disorders is vital for effective treatment, which may include therapy, medication, and support networks. By gaining insights into personality disorders, we can foster compassion and support for those affected.
Anxiety: A Natural Response to a Chronic Disorder
Anxiety is a natural response to stress; however, when it becomes chronic, it can interfere with daily life. Anxiety disorders can manifest in various forms, including generalized anxiety disorder, panic disorder, and social anxiety. Recognizing the symptoms and understanding the factors contributing to anxiety is crucial for effective management. Treatment strategies may include therapy, medication, and mindfulness practices, helping individuals regain control over their lives.
Stress, Resilience, and Health
Stress is an inevitable part of life, but how we respond to it can significantly impact our mental health. Building resilience is key to navigating life’s challenges. Stress management techniques, such as mindfulness, exercise, and social support, can enhance resilience and overall health. By understanding the relationship between stress and mental health, individuals can adopt healthier coping mechanisms and foster a supportive environment for themselves and others.
Youth Suicide: Causes and Prevention Strategies
Youth suicide is a critical issue that demands attention and action. Understanding the causes of youth suicide, including mental health disorders, bullying, and societal pressures, is vital for prevention. Implementing effective youth suicide prevention strategies involves raising awareness, providing support, and creating safe spaces for open discussions about mental health. Schools, families, and communities must work together to address this crisis and support at-risk youth.
Making Mental Health a Global Priority
Prioritizing mental health on a global scale is crucial for promoting overall well-being. Stories from individuals and communities highlight the need for accessible mental health services, education, and support systems. By sharing experiences and advocating for mental health resources, we can reduce stigma and encourage those struggling with mental health issues to seek help. Global initiatives and policies must focus on improving mental health services, ensuring that everyone has access to the care they need.
Bridging the Mental Health Gap for Indian Youth
In India, addressing the mental health needs of youth is essential for fostering a healthier future. A human-centered approach to mental health care can bridge the gap between available resources and those in need. By involving young people in the design and implementation of mental health services, we can create more effective and accessible support systems. Initiatives that focus on education, awareness, and community engagement will help empower youth to prioritize their mental well-being.
Child Mental Health Services
Investing in child mental health services is crucial for nurturing the next generation. Early intervention can help children develop healthy coping mechanisms and resilience. Understanding the signs of mental health issues in children, such as changes in behavior, academic struggles, and social withdrawal, is vital for timely support. Accessible mental health resources and trained professionals can make a significant difference in a child's life, ensuring they grow into well-adjusted adults.
Stress and Depression Among Medical Students
Stress and depression among medical students in India have become increasingly prevalent, driven by academic pressures and demanding schedules. Understanding the unique challenges faced by medical students is essential for developing effective support systems. Universities and institutions should implement mental health programs, promote work-life balance, and create environments where students feel comfortable seeking help.
Toxic Positivity and Its Impact on Mental Health
Finally, understanding toxic positivity—the belief that we should always maintain a positive attitude—can help us recognize its negative impact on mental health. This mindset can invalidate genuine feelings of sadness, anxiety, and frustration, making it difficult for individuals to express their emotions. By fostering an environment that encourages authentic emotional expression, we can promote mental well-being and support those struggling with their mental health.
Conclusion
Mental health is a multifaceted issue that requires understanding, compassion, and effective treatment strategies. From erectile dysfunction to child mental health services, each topic presents unique challenges and solutions. By fostering awareness and promoting accessible resources, we can work together to improve mental health outcomes for individuals and communities. Through education, support, and innovative approaches, we can create a future where mental health is prioritized, and everyone has the opportunity to thrive.
#Mental Health#Mental Health Disorders#Erectile Dysfunction#Dementia#Schizophrenia#Bipolar Disorder#Obsessive-Compulsive Disorder#Anxiety Disorders#Stress Management#Youth Suicide Prevention#Brain Stimulation#Personality Disorders#Child Mental Health#Toxic Positivity#Resilience#Global Mental Health#Indian Youth Mental Health#Medical Student Stress#Behavioral and Psychological Symptoms of Dementia#Mental Health Awareness
1 note
·
View note
Text
Let's Talk About The Overlap Between Autism, ADHD, and Schizophrenia

I've been wanting to make a graph like this for awhile, about the overlap between these three disorders. Tagging @auschizm because it's highly related to that blog :D
Text transcribed below the cut because it's long!
Title: Can We Talk About The Overlap Between... AUTISM, ADHD, AND SCHIZOPHRENIA?
Description: You always hear people talking about AuDHD, but schizophrenia has the same if not more overlap with these disorders, and it's not talked about!
Let's start boosting schizophrenic people's voices. There's more to the disorder than just psychosis!
Graph based on my personal experience with schizophrenia, my experiences with autistic and ADHD communities, and the words of people with AuDHD themselves.
Made by @gray-gray-gray-gray on tumblr.
Schizophrenia Only
Typical age of onset between 15 and 54 years old
Before the onset/ first psychotic break, there is a "prodrome" where you have a drop in functioning
Reoccuring episodes of psychosis (Hallucinations, delusions, paranoia, etc)
Likely had less noticeable or covert symptoms pre-onset
Often daydreaming, 'in their own world', hyper-self-reflective, 'space cadet'
Autism Only
Need for familiarty & routine
Sudden disruptions to routine are highly distressing
ADHD Only
Craves new experiences & novelty
Autism & ADHD (AuDHD)
Interest-based nervous system (meaning attention & focus is activated based on personal interest, not how important something is)
Onset in very early childhood -- before age 12
Autism & Schizophrenia (Auschizm)
Self-soothing via repetitive behavior
Higher rates of catatonic symptoms
Social withdrawal or exclusion
Difficulties filtering speech
Flat affect
Alogia
Concrete and/or literal thinking
Higher rates of personality disorders, dissociative disorders, and trauma
Internally oriented behavior
Difficulties wording what they
want to say correctly & disorganized speech
Difficulties with insight into what is part of the disorder and what is neurotypial
ADHD & Schizophrenia (SchizoDHD)
Impulsivity & hard to sit still
Difficulties regulating attention & focus, also causing social cue difficulties
Difficulty keeping a daily routine
Jumping around or out of sequence speech
Forgetfulness
Failing to reach a clear end goal or point in speech
Less coherent progression from start to finish in stories
General difficulties with thinking clearly
Drawing blanks / losing train of thought often
Difficulties finding motivation to do things
Lots of energy some days, no energy other days
Troubles multitasking
Planning poorly or not at all
All Three
Stimming
Echolalia, echopraxia
Executive dysfunction
Sensory issues & overload
Emotional dysregulation
Interconnected/webbed thought
ND communication (infodumping, connecting ideas, shared interest bonding)
Increased risk of victimization
Hyperfixations
Higher rates of depression, anxiety, OCD, BFRBS, bipolar, suicidality, sleep issues, eating disorders, and substance abuse
Eye contact differences
Difficulties switching tasks
Masking
Hyperfocusing
Restlessness
Prone to boredom
Memory issues
Social situation difficulties
Time blindness
Difficulties with school, learning, and following tasks
Chronic disorder
RSD
Anhedonia
Alexithymia
Interoceptive difficulties
#actually neurodivergent#neurodivergent#nd#neurodivergence#neurospicy#neuropunk#autism#asd#autism spectrum disorder#actually autistic#autistic things#autistic experiences#adhd#actually adhd#adhd problems#adhd experience#audhd#actually schizophrenic#actually schizospec#schizophrenia#schizospec#schizospectrum#schizophrenia spectrum#auschizm#schizodhd
2K notes
·
View notes
Text
Writing Mad Characters
Okay this is a bit awkward because I had this question copypasted into Google Docs I use to draft my answers, and I realized I've lost the question in my inbox (which is being flooded).
So...I'm so sorry for whoever asked this question. Sorry for the delay because I was struggling with life in general for the past month and definitely SORRY for losing your question (-‸ლ)
Q: I'm writing a story where a major character is slowly spiraling into madness where small details kinda hint into the downfall right before the bigger details appear and then it the floodgates open. Is there anything I should avoid? Anything that I should keep in mind? Anything that I should research?
Things to Avoid
“Mad” or “Insane” is too general. Writing a cliched ‘crazy’ character who randomly talks to imaginary people and lashes out at strangers, you’ll offend a whole bunch of people who've gone through/have mental illnesses. Read up on existing mental conditions (schizophrenia, bipolar disorder, post-traumatic disorder and borderline personality disorder, etc.) to see what your character might have.
Words like “mad” “crazy” or “insane” aren’t enough when you’re describing their status. As mentioned, these words hardly mean much when it comes to providing a clear description.
Contradicting yourself. Throwing random unhinged symptoms here and there wouldn’t work. In fact, you must have a clear arc on which they’re traveling and ensure that your “hints” are all getting at something.
Making the character overly destructive or harmful to others (when nothing really justifies it)
Justifying damaging behavior with this “madness”. Mad or not, your character will still have motives and goals that drive them forward.
Making them look incompetent just the fact that they have a mental condition that makes them appear “mad” to others shouldn’t prevent them from achieving success. In fact, they may be even more cool-hearted and logical when it comes to their obsessions/goals.
Research Tips
Narrow down the mental conditions your character experiences. Even if it’s a fictional condition, try basing it on existing ones and building on top of them.
Take some time to study characters and/or real clinical cases that resemble the kind of madness you’re going for.
- Anxiety Disorders: excessive fear and dread (ex. phobias) - Mood Disorders: persistent swings in mood or persistent feelings that interfere with daily life (ex. Depression, bipolar) - Psychotic Disorders: disordered thinking (ex. schizophrenia) - Eating Disorders: extreme emotional attitudes toward food (ex. Bulimia, anorexia) - Impulse Disorders: unable to resist urges (ex. Kleptomania, pyromania, gambling) - Personality Disorders: extreme inflexible personality traits (ex. Anti-social disorder, OCPD) - Past Traumatic Stress: persistent, frightening memories leading to emotional numbness
Does your character have empathy?
A sociopathic kind of madness is different.
General Writing Tips for Spiraling into Madness
Establish a Baseline
A lot of factors (stress, family history, innate personality, trauma, etc.) can contribute to madness, but it is not going to happen in a week. Define the existing mental and physical conditions your character has, and start from there.
If you’re aiming for suicidal tendencies at the end, you want to start with symptoms of depression (a condition that may lead to suicide) - growing apathetic, erratic sleeping patterns, irritability, etc.
This is also the stage where you want to plant some triggers that’ll go off later.
Trigger Events
A perfectly sound character suddenly spiraling down the madness route due to a single accident or traumatizing event isn’t convincing.
A madness “snap” denies the reader the experience of watching the character’s journey into madness and how they feel about it.
Internal Conflict (antagonist in himself)
You must remember that madness is incurable. If someone could “cure” themselves by eating healthy, exercising and taking a few pills, it wouldn’t be much of a madness, would it? This means that the worst antagonist is going to be the character themselves, or the part of them that’s been taken away.
Show how they are frustrated with themselves, scared of themselves, angry at their “alternative self”. The experience of not knowing yourself is a whole journey of its own.
Physical Manifestations/Quirks
If your character has a routine, show how they break down.
They might develop habits that they otherwise would never allow themselves to have, perhaps as an effort to “keep this madness out”
Deteriorating Relationships
Depict how the character’s madness impacts his closed/loved ones. In the earlier stages, those close to him might be faster to notice and accept the signs of madness, even if the character denies it him/herself.
The first signs of madness might show when the character is trying to deal with difficult relationships - like losing patience and being unable to pick up subtle social clues.
Choosing Obsessions Over Primal Urges
For these characters, obsession can take over a person’s normal urge to eat, sleep or even live. This can lead to, more or less, suicide.
Example: In Black Swan, Nina’s obsession with becoming the perfect ballerina drive her to insanity, to the point where she doesn't mind dying on stage for the show.
#writing#writers on tumblr#helping writers#creative writing#writeblr#poets and writers#let's write#creative writers#resources for writers#writers and poets#writing process#writing advice#writing inspiration#writing ideas#on writing#writer#writing prompt#writer stuff#writing community#writer on tumblr#writer problems#writer things#writer community#writerscommunity#writing blog#write#writers#writers block#writblr
595 notes
·
View notes
Text
How did they accidentally intimately understand the experiences of mentally ill ppl in s1??? How??? It’s gotta be cos the writers changed right
Ok bcos like, it’s not like Jinx in s1 was a good portrayal of mental illnesses in the sense that it was realistic. I’d actually argue that part of her appeal and what made her work so well is bcos she was undiagnosable. She showed many symptoms of what could be many different issues and so many ppl could relate to her on a basis of one symptom. But what they did with Jinx that made her work so well is that they seemingly understood the emotions and psychology that are shared by ppl with all types of different issues. They didn’t need to understand all the technicalities in terms of, like I said, a realistic portrayal of a specific issue. What mattered was that she felt like a really mentally ill person cos her arc dealt with the struggles of mentally ill ppl. She was portrayed to feel isolated, struggling to communicate/socialize, feeling like she was fundamentally wrong/different, like she inherently didn’t belong anywhere, frustrated with her own symptoms, having internalized guilt, a desire to be loved/accepted, feeling unlovable, trying to hide her issues/symptoms, futilely trying to fit/change her behavior to fit/pass, feeling like a failure etc.
The main betrayal of s2 when it comes to Jinx and her arc was violating that connection that ppl build with Jinx in s1. S2 Jinx is an extremely unrealistic, unrelatable and sanitized portrayal of mental issues.
99% of her symptoms disappeared after she experienced smth that would drastically exacerbate them. Are you pranking me? Is that what I’m supposed to relate to? Quick fixes were applied, like giving her Isha to fix her loneliness but 1)that’s not how raising a child while mentally ill would look like, it would make her struggles worse 2) they cease to portray crucial experiences of mental illness like feeling like you don’t belong cos your behavior is always off, these things don’t just disappear, even when ppl get better there’ll still be these moments, and that’s in a best case scenario. Like trans ppl after finishing treatment saying they got rid of 99% of their dysphoria, but never a 100%. look at how they expertly managed to portray Silco and Jinx having a close loving bond and simultaneously highlight her loneliness and isolation. So she has a kid now bcos single mothers are not famously lonely and isolated ppl right? It was a common point of criticism of Silco that Jinx not having friends amongst her peers is a really bad sign but now she still has no friends but now 1) it stopped being an issue 2) she’s also a single mother now.
The focus was switched from her being portrayed as likely born neurodivergent + traumatized to depression but specifically suicidality. it’s not like in s1 she wasn’t portrayed as depressed/suicidal and you’d think she’d become more so after s1 but that wasn’t the sole focus, but curiously it becomes so in s2. But despite this switch in focus that you’d think would stem from the writers wanting to write about their own experiences or smth that interests them that they think is important it couldn’t be clearer that the writers had zero empathy for the issues they were writing about cos it’s misery porn, a pitfall that many stories that center suicide fall into, glamorizing and romanticizing it. In s1 her worst symptoms like hallucinations were very dramatic and cool-looking visually but it was connected to this fundamental empathy, the understanding of mentally ill ppl as ppl with emotions and what those are. In s2 they drastically switch the portrayal of her issues to fit what they wanted to do with her in s2, and then proceeded to use it solely for cool and dramatic imagery/scenarios. It is completely disconnected from ppl’s real life experiences. The relatability was sacrificed for the sake of following tropes like 'death as redemption' that are supposed to be more dramatic or smth. Having her ping-pong from having no issues to having all the issues throughout the narrative.
Act1: She’s ‘dead inside’, she seems somewhat motivated at some point only for it to be revealed she was planning suicide – alright season, nice, what’s next. Act2: she’s just completely alright now from the get go, her hallucinations show up only when she first finds out Isha’s in danger. why? who knows. It’s like the writers understood that for them that would be a particularly stressful situation so they use the imagery of her illness to communicate she’s super distressed in this moment. So they used the imagery of mental illness not to convey mental illness and how it interacts with her life but as a dramatic-looking shortcut to convey a strong emotion, one that any other character would feel in this situation. Otherwise she’s doing better than she ever was, even in s1a1, and then Isha dies. Act3: so now she 100% ’wants to die’ again and it’s super depresso but then she has one conversation with Ekko and she’s again doing super good and then she dies by semi-suicide but she’s happy doing it and it’s like. beautiful? ok.

#we're at arcane's funeral#and amanda is writing sesbian lex#jinx#arcane#my:arcane#arcane s2#arcane critical
199 notes
·
View notes
Text
A Comprehensive Analysis on Eric Harris, 3.
Disclaimer: This analysis/psychoanalysis is limited only to analysis as a means to reflect and understand the people involved. It is strictly informative. Just like all of my posts, I am detached from the media I write about and solely focus on the people to understand their psychology, for others to gain insight. There is no room for me to romanticize or glorify anything I write because I am only here to explain. I understand and research, but I do not condone. Thank you.
note: This is all solely based on independent research. If I may be wrong with the medical aspects of this post, please correct me. I would appreciate it a lot.
Fluvoxamine Maleate

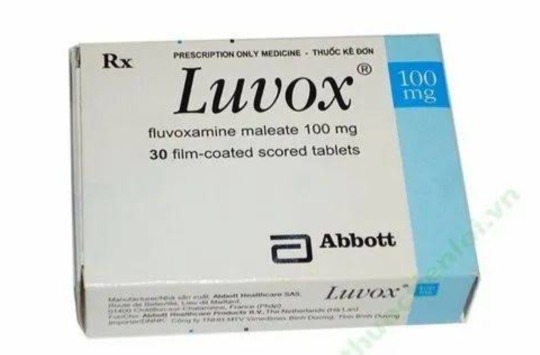
Just a few days before the shooting, Eric was promptly rejected from his application to serve in the marines. Despite his desirable qualities, he was rejected for the sole reason of being tested positive for consuming a prescripted drug after rejecting that he was off any medication. With a trace of Luvox in his system, theories speculate that the drug's side effects played a role on the events that have transpired. Luvox is a medication prescription drug that is used to treat mental illnesses such as Obsessive Compulsive Disorder (OCD), anxiety, depression, and others. While there are positive effects, the downside are heightened sensations of dread, irritation, depression, and arising violent behaviors. It also has a chance to increase manic symptoms, especially if taken in particularly large doses.
Anti-depressant usage, effects of overdose, and detoxification
When taken over the prescribed dosage, Luvox can lead to increased agression and suicidal ideation and tendencies. Eric was in anger management therapy after being on probation alongside Dylan for attempting to steal a vehicle containing thousands worth of valuable electronics and tools. After getting caught, Eric openly expressed his difficulties in managing his anxiety and explosive anger issues that his counselor said, "he frequently blew up and often cried." Revealing that this influences his homicidal and suicidal thoughts, so he was prescribed Fluvoxamine, which is a selective serotonin reuptake inhibitor (SSRIs). These drugs increase the capacity of the brain to receive serotonin.
According to an interview with Eric's friends, they speculate that Eric was off his medication completely for sometime. Abruptly stopping medication can lead to the development of a more violent response. For some people, drugs are able to fix their chemical imbalances, but it can also lead to withdrawal symptoms of taken for over the duration of 6 weeks. Abruptly discontinuing anti-depressants can lead to rebound depression or relapse. Symptoms may return stronger than before. Furthermore, SSRI's such as Luvox and Prozac take about 5 days to linger in one's system before subsequently washing off.
In a period of 11 months, Eric and Dylan have been under a juvenile detention program at Jefferson County district — this was in 1998, just a year before the shooting. They were allowed to leave the program by early February 1999. After finishing, Eric wrote a letter contained in his juvenile diversion program file. He states, "I learned that thousands of suggestions are worthless if you still believe in violence."
After public demands for stricter regulations on SSRIs after the tragic shooting, Luvox was temporarily banned in 2002. By 2008, drug manufacturers had reformulated Luvox to a controlled-release version specifically designed to treat OCD, excluding indications for depression or anxiety. Subsequently, the FDA approved Luvox CR for the treatment of OCD. The label does not explicitly prohibit prescribing it to the pediatric population, it notes that the smallest dose "may not be appropriate" for children, without providing further explanation.
Eric was about 17 at the time of taking the medication, which means he is part of the pediatric population. Though it's still unclear if he was taking normal doses for a long period of time or taken more than what was prescribed, it is clear that there was negligence with prescribing a child a SSRI that has the posibility of worsening their already apparent symptoms.
Columbine was really a case that opened the public's eyes into the dysfunctional aspects of society and institutions, transcending even to the medical field.
413 notes
·
View notes
Text

ikémen villains content warning list .ᐟ
this is a work-in-progress compilation of complete content warnings per route (because ikévil tends to underwarn a bit maybe to avoid spoilers) that will be updated as we go. please let me know if I missed anything, regardless if it says ‘work in progress’ or not, or pitch in with warnings. ♡ and ↻ are appreciated!
some of the ikévil routes contain sensitive themes that may be triggering. so please remember to take care of yourself while reading 🫶

GENERAL ༉‧₊˚. 🕊️
canon-typical violence, (minor but named) character death, depictions of murder.
────────────────────
WILLIAM REX ༉‧₊˚. 🍓
near death experience, drug abuse, sexual coercion (not by love interest), corruption, romanticization of death.
───────── 〔🌹〕 ─────────
HARRISON GRAY ༉‧₊˚. 🦊
corruption of the police and higher-ups, mentions of human trafficking, coercion to commit crimes, mentions of kidnapping.
───────── 〔🍧〕 ─────────
LIAM EVANS ༉‧₊˚. 🐈
attempted suicide, suicide and suicidal ideation, depression, anxiety, implied self-harm, mentions of child abuse (physical and emotional), fire, severe burn wounds, human trafficking, mental breakdowns.
───────── 〔🎟️〕 ─────────
ELBERT GREETIA ༉‧₊˚. 🍎
objectification both by and against love interest, mentions of sexual assault or rape (not by love interest), domestic abuse, attempted child sexual assault, pedophilia, obsessive and possessive behavior, stalkerish behavior, grooming, non-consensual touching, depicted suicide, self-harm, mental breakdowns, mentions of animal death, kidnapping, mentions of human trafficking.
───────── 〔🦋〕 ─────────

ALFONS SYLVATICA ༉‧₊˚. 🪞
description of children’s corpses, symptoms of depression, topics of mortality, attempted suicide, near death experience, self-harm, mental manipulation (?), dub-con: having sexual intercourse while one has “consented” in an intoxicated state or under the influence of a curse, (perceived) non-con, mentions of drug abuse and the effects of drugs, mentions of child abuse or labor, implied animal torture and death.
───────── 〔🐈⬛〕 ─────────
ELLIS TWILIGHT ༉‧₊˚. ⛓️ —— warnings provided by @myusuchaa !!
romanticization of murder and death, family murder and death, suppressed emotions, emotional disconnect, people pleasing, attempted kidnapping, negative treatment of disabilities, coercion, child trafficking, gang activity.
───────── 〔🥀〕 ─────────

ROGER BAREL ༉‧₊˚. 🍻
a loott of alcohol consumption, drug usage or abuse (recreational drug use), cult activity, near/death experience of a side character, dub-con, self-harm especially in the past.
───────── 〔🧪〕 ─────────
JUDE JAZZA ༉‧₊˚. ⌛️ —— w. i. p. ┊ warnings provided by @judesmoonbeauty !!
smoking, torture, mentions of drugs and human trafficking, neglect and child abuse, mentions of a child’s death and the death of a family member.
#ikemen villains#ikevil#ikevil william#ikevil william rex#ikemen villains william#ikevil harrison#ikevil harrison gray#ikemen villains harrison#ikevil liam#ikevil liam evans#ikemen villains liam#ikevil elbert#ikevil elbert greetia#ikemen villains elbert#ikevil alfons#ikevil alfons sylvatica#ikemen villains alfons#ikevil ellis#ikevil ellis twilight#ikemen villains ellis#ikevil roger#ikevil roger barel#ikemen villains roger#ikevil jude#ikemen villains jude#jude jazza#ikevil jude jazza
385 notes
·
View notes
Text

The last known photograph of Robin Williams, taken just the day before he died.
He passed away on the 11th of August, 2014, at the age of 63. He was found dead in his home in Paradise Cay, California. The cause of death was determined to be suicide by hanging.
In the months leading up to his death, Williams had been struggling with severe depression and anxiety. After his death, it was revealed that he had been diagnosed with early stages of Parkinson's disease, which he had not yet disclosed to the public.
Later, an autopsy report indicated that Williams had Lewy body dementia, a neurodegenerative disorder that can cause severe cognitive and behavioral changes, along with physical symptoms similar to Parkinson's disease.
Lewy body dementia is often misdiagnosed, and it is believed that the combination of his mental health struggles and the debilitating effects of this disorder contributed to his tragic decision to end his life.
Robin Williams left behind a legacy of remarkable performances in film, television and stand up comedy. Generations of children grew up with him on the television, and he touched the world with his humor, warmth and talent.
His death was a profound loss to the entertainment industry and to the many people who admired and loved him.
306 notes
·
View notes
Text
If Mike had the same focus on his mental health as part of his character arc in season 4 like Max did, he wouldn’t be as a disliked character by the general audience as he currently is.
I’m being serious.
Their behaviors throughout season 4 are similar enough to draw parallels between them.
They both treat Lucas like crap in less than ideal terms.




They both get their declining academic performance pointed out by another character.

They are both hiding things from people, and being open and honest about it could help them but they won’t do it.




They both mistreat and push away someone they love.


They both lack self-preservation, which leads them to have suicidal tendencies and put their lives at risk.









The show even makes a point of putting Mike next to Max in two of the symptoms mentioned in the Vecna’s curse.

The only difference is that Max’s character has a huge focus this season, and most of it is centers on her deteriorating mental state. On the other hand, the only time Mike gets a chance to explicitly and verbally acknowledge that he is struggling with something, he admonishes himself for caring about something so irrelevant considering the ongoing situation, and the scene shifts to be about Will and his disguised confession through the painting.

.
.
.
So, with all being said... what could this possibly mean for Mike in season 5? Well, Ms. Kelly said it best:



#mike wheeler#max mayfield#byler#<<< target audience#poor lucas; i guess that it's the price he pays for being the only emotional stable member of the party#also before anyone try to say anything#i absolutely loved max's storyline this season and will's confession in the van is one of more favorite scenes#so don't put words in my words and make me out to be someone i'm not
2K notes
·
View notes
Text
An exhaustive headcanon post about Bruce Wayne's unhealthy mentality.
trigger warning for: mentions C-PTSD, Survivor's Guilt, shitty dietary habits, insomnia, self-ableism, masking, workaholism, somewhat shady parenting, technically self-harm, and passive suicidal ideation.
Ok, so:
•Bruce def feels like he has to earn things. Like affection, respect, or just any form of a good thing happening to him.
•He earns his life, or so he says, but it's more like he's trying to earn the right to be alive, which is a wild thing to believe.
•Bruce is autistic as all hell, right? Diagnosed and everything, his parents used to pay for private treatment since the mental health system in Gotham is so ass. Well, after they died, Bruce just, doesn't do any of that anymore, he avoids therapists or psychologists like the plague, even ones outside of Arkham. He has a whole lot of Other Things™ outside of autism now, but he still refuses to go get proper help.
•Similarly, Bruce would rather die than to actually mention it to anyone. Like, yeah, as Brucie Wayne he's definitely masking hard (to the point where it's kinda upsetting and he gets overwhelmed), but like, he also doesn't tell shit to the whole rest of the Batfam, or the Justice League. The only person that knows that Bruce is autistic AND just generally mentally ill/traumatized, is fucking Alfred.
•This causes people to misunderstand him a lot, but part of him feels like that's more "deserved". Like, he thinks that he'd hate to be judged by his mental illness because he he dislikes the idea of his actions being justified retroactively of excused by his illnesses, not being self-aware enough to notice that this horrifically heightened sense of hyper-responsability about just fucking everything in his life is itself, a trauma response. Also, he's the world's biggest hypocrite, who famously believes that other rogues and people like Jason Todd need to be helped instead of killed or put down, going directly against his own attitude towards himself.
•He genuinely believes that whole "[insert mental illness here] is not an excuse to [insert a behavior or symptom of aforementioned mental illness here]", but like, only towards himself. To everyone else he rightfully thinks that stuff is bullshit.
•Bruce puts himself up to some crazy standards, actually. He works non-stop as both Brucie, Bruce, and Batman, always doing something, unable to stay still or even sleep. He skips meals, neglects his well-being, he puts everything on the line and expects himself to do it everyday, every hour, without fail, every single time.
•His kids think that he's neurotic, they're kinda right, the Justice League think he's too paranoid, they're right too, Gotham city thinks he's a saviour, it's true, the rogues think he's a monster, that's fair as well. Alfred? He just thinks Bruce is hurt, he's the most right of all.
•Part of this is a form of punishment, atonement for being alive, for surviving that fateful night when his parents didn't, for daring to go on with life when they're both sixteen feet under, for having the audacity to raise a family, the gall of having friends, the sheer nerve to even consider having a romantic relationship, when his parents couldn't even hug him. Not anymore. He's here, not them.
•And it kills him, because he saw it, saw them die, saw them gurgle on their own blood and sat with their bodies until the police arrived, this is what led him to become Batman, to mask as Brucie, to guide so many young people away from being like him as Bruce. So how dare he, how dare he be happy when they died? How dare he forget that alley, for even a second? How could he? Didn't he love them? Didn't he make a promise to live out the rest of his life in a mission to prevent events like this?
•It's like he's in a toxic relationship with two corpses, they're cold and their eyes follow him, he's hollow and blind to anything but them. Part of him would love to argue that his parents, Thomas and Martha Wayne themselves, would prefer to see him happy and fulfilled. Another part of him remembers gunshots, blood spatter, and the sound of choked gurgling, and Bruce spirals all over again.
•Perhaps he's waiting for this life for kill him, finish the job that gun didn't do years ago, kill him like his parents, hurt him so deeply he can't recover, destroy him until he's repented for being so inherently horrible. Because he is, he knows he is, he's neurotic, paranoid, a saviour complex having monster, this is what he aimed for, he seeked out this outcome, just waiting to be put down like those before him.
•He's passionate about his cause, sure, but that's surface level. The front used to keep the image of an asshole neurotic paranoid man that has a saviour complex, instead of exposing the truth behind himself. Who he really is.
•A child, that's who he is, a kid reliving his worst bad day over and over and over again.
•He earns his life, he'd earned this.
#bruce wayne#batman#bruce wayne headcanon#batman headcanon#jesus christ dude#I am so ill about him can you tell#autistic bruce wayne
153 notes
·
View notes
Text
this is going to be a long post, it's kinda just me writing all my raw unfiltered thoughts on ABA therapy as someone who actually went through it
-> TW for ABA therapy, child abuse, suicide <-
I was functionally diagnosed with autism at the age of 3 but it wasn't until I was 13 that I was actually formally evaluated for it and given an official diagnosis. I was behind in social skills and developmental skills

[ID: "was also described as a sensory seeker. She does not currently have any friends and has struggled to make and maintain peer relationships throughout her childhood. Difficulties with social skills were initially noted when she was in preschool (years before the onset of clinically significant symptoms of anxiety and"]

[ID: "Social functions: [blank]'s mother also completed a questionnaire rating her social responsiveness. Her responses on the SRS-2 indicated that [blank] is demonstrating severe deficits in the areas of Social Communication (reciprocal social interaction and nonverbal and verbal communication), Social Motivation (motivation to engage in social-interpersonal behavior) and Social Awareness (perceiving social cues) and moderate deficits in the areas of Social Cognition (understanding social cues). Severe Repetitive and Restrictive Behaviors (stereotypical behaviors or highly restricted interests) were also reported. The total T-score on the SRS-2 indicates severe deficiencies in reciprocal behavior that are likely to result in interference in everyday social interaction"]

[ID: "%ile) are mildly impaired, while her social skills are moderately impaired (2nd %ile). By domain, demonstrates mildly to moderately impaired abilities in six adaptive skills areas, including self care (9th %ile), communication (5th %ile), home living (5th %ile), self-direction (2nd %ile), social (2nd %ile), and leisure (1st %ile)"]
and ultimately all this ended up with the number one recommendation after my autism evaluation being for ABA therapy.

[ID: "Recommendations: Based on the above results, the following recommendations are made for [blank] and her family.
1. ABA therapy: [blank] May benefit from an intensive treatment program to foster cognitive and communication skills, improve independence and adaptive functioning, and help manage interfering behaviors (i.e home-based, 1:1 instruction, task analysis, etc.) Most private and community programs are based on principals of operant conditioning and taught in home with 1:1 instruction"]
*I'm getting misgendered here. my pronouns are he/him
"operant conditioning"-- like a dog 🐕🐕. woof woof.
my mom didn't know any better so she put me in ABA therapy with the Center for Autism and Related Disorders. she regrets this. I regret this more.
my autism evaluation was cruel, it dissected all my flaws as if I was a bug under a microscope in a highschool laboratory. my evaluation was passed around to ABA therapists, a line of high schoolers peering through the microscope examining the most vulnerable parts of me.
and I choose the highschool analogy quite deliberately. most of the ABA therapists at my center were recent highschool graduates with no degree and little training. they knew nothing about autism and had no qualifications. you need more certificates to become a professional dog trainer than to become a professional human trainer.
"operant conditioning"
and I wish I could say it was just a poor choice of words but ABA therapy was dog training for children. my dad used to call me an "it" and somehow I felt less dehumanized by that than the entire experience I had in ABA therapy.
I was the oldest person at my center (I did not receive in home therapy) with the next oldest being approximately 3 years younger than me. at the time I felt babied. I was surrounded by 5 year olds and I was treated as if I was not just a 5 year old but an autistic 5 year old and anyone who has been a visibly autistic 5 year old knows what that feels like. I had escaped being an autistic child and now I was being treated like one again. The head of the program tried to console me by telling me adults received their services too.
[ID: "Following the principles of applied behavior analysis, CARD has developed a treatment approach for children and adolescents with"]
this was the first lie they told me. CARD does not work with adults.
I was not allowed the privileges of being a 13 year old. because I was an autistic 13 year old and therefore I was the equivalent of a 5 year old. I was in psychotherapy at the same time and I had grown very accustomed to some level of freedom in therapy. I was allowed to use the bathroom independently. in ABA therapy I was not allowed to use the bathroom independently. I tried once, me and my therapist were on an "outing" to the grocery store and I told my therapist I was going to the bathroom and walked off and I got a very stern talking to about how I needed to "stop eloping" and if I didn't stop it would "become a behavior"
eloping became a common theme used to control me and squeeze money out of my parents.
out of everything I hated in my life, including severe physical abuse at home (which they did not report), I hated ABA therapy the most. I would repeatedly make serious threats of suicide to try to get out of ABA. no one cared. everyone thought I was being dramatic but there were times I wrote out suicide notes and ABA was among the reasons I listed. ABA made me feel hopeless, depressed, revolting, disgusting, inferior, and less than human. between ABA, my home life, and my social life I had never felt so hated and it was boiling through my skin. I acted out, I was bullying people, I was behaving recklessly, I was starting fights, and all this only made the oppressive force of ABA crack down on me harder. I was a cat hissing in the corner begging to be left alone and ABA brought a net to try to tame me further. every time I scratched back it was listed as a reason I needed to be there.
I was "disruptive" and "rebellious" and "uncooperative" and "resistant to treatment" and no one could figure out why I was "regressing" despite me shouting the answer. I was screaming and no one was willing to hear me
I hated myself and my autism. my autism diagnosis made me want to die. I didn't feel freed by it or understood I felt ashamed and disgusted. I felt incompetent and like I had failed. I was ashamed to be at ABA, it was my biggest secret. I'd lie to my friends about why I couldn't hang out and I'd lie to people in public about who the woman I was with was and I'd lie about all of it to try to cover up my most shameful secret.
ABA therapy did nothing but foster this. In ABA therapy I was mocked for being autistic and what was happening only clicked when a young kid, maybe only 4 or 5, was flapping his hands and a therapist took out her phone and recorded him. we were circus animals. it was all an entertaining show to them while they poked and prodded at us with metaphorical hot irons to make us dance. the first time a therapist laughed at me for rocking back and forth I wanted to throw up. I almost did. it was systematic bullying of children I was forced to watch and experience.
my point is: the last place on earth I wanted to be was the ABA center.
so of course I tried to leave. my mom would bring me McDonald's and I'd beg, sobbing real tears, to leave early because only she could sign me out. every time I'd go to meet her I'd be marked as "eloping" and my hotel stay in hell would get extended.
my natural response to a stressful environment (leaving) was pathologized. I was eloping this way and that way and never once did I actually, truly elope. that word was a weapon used against me. they used my "elopement" to justify extending my stay to my parents. they ate it right up.
they argued I needed to stay there because I was making friends. this was true, I'm great at getting along with children it's part of why I want to go into pediatrics, but I had also made real friends with people my age at my highschool. ABA was getting in the way. I wanted to spend time with my friends outside of school but ABA took up all my time from the minute I left school to 6pm and all day on weekends. I was doing a full time job's worth of hours. I complained about how I was missing out on spending time with my real friends (as in, over the age of 7) and I was met with almost no wiggle room in my schedule. I was allowed to pre-plan time to spend with friends but every time my friend group wanted to do something spontaneously? I had to say no, and I had to lie about why. my friends would share stories about driving around town with 2 people in the group stuffed in the trunk, of hanging out in the woods together, of taking part in ordinary highschool activities as ordinary high schoolers and it made me cry because I was not an ordinary highschooler and I was not allowed to participate in ordinary highschool activities. I was one of those weird, unpleasant, socially awkward autistic people instead. eventually, they just stopped inviting me. I was forced into the out group by ABA.
I'll never get that back. I'll never get a chance to be a normal highschooler ever again.
when I did have time available to hang out with people I never had the energy to. at the time I was living with an undiagnosed physical disability and I was begging to see a doctor but no one would believe that it wasn't just anxiety. the people who believed me least of all were the people at the center.
I was constantly told I was trying to get out of therapy by "feigning" very real pain and fatigue. I tried to explain spoon theory, and that I had limited spoons, and in response they made a task for me to name things to "regenerate spoons" that's not how it works. I wasn't the only physically disabled person there. there was a wheelchair user who was constantly forced to stand for periods of time despite being in agony doing it. he wasn't allowed rewards until he did it.
rewards were used to train us like dog treats are used with dogs. sometimes the treats were fun! I'd get to cook, play Mario kart, and go on outings. other times the treats were "using the correct name and pronouns for me." I'd constantly be threatened with deadnaming and misgendering if I was being "noncompliant."
misgendering because of my autism was a theme in my life. my neuropsych evaluation report misgendered me. my parents misgendered me. the staff at ABA misgendered me. at one point the head of the program suggested that my "gender confusion" was because of my autism. my abusive father latched onto this and still claims that the reason I'm "confused" about my gender is because the evil transgenders tricked me into thinking I'm one of them because I'm autistic and therefore easily impressionable.
the two therapists I had were nice because I refused to work with the others. they weren't on a power trip and both eventually left because they realized the harm the organization was doing. other therapists were not so kind. other therapists were on a power trip, because in their mind lording over autistic 5 year olds (and autistic 14 year olds) makes them powerful and strong. occasionally I'd get stuck with one of the other therapists when my usual therapists were out. they would talk to me in a baby voice. they would make fun of me for rocking back and forth, for not making eye contact, for talking about Skyrim "too much" and generally just for being autistic.
I never really knew what I was supposed to be doing, just that I was doing it wrong. the therapists there rarely actually told me what my tasks were they'd just mark yes or no on them, judging me for something I wasn't aware of. I was never actually supposed to graduate, I was never supposed to get out, if they wanted me to succeed they would have taught and explained what was happening but I was intentionally left in the dark.
I continued threatening suicide to get out. no one took me seriously. I was seriously considering it. there's no happy conclusion where someone finally realized it was all wrong, or I figured out how to be allistic and graduated, or I felt more comfortable there. I only got out when covid struck and shut the center down. it's gone now, replaced by a family advice center. I hope their advice for autistic children is to never put them in ABA.
there is no grander message here just suffering. I'm sorry if you were expecting some sort of great point at the end of this. there's not one. it happened, I wish it didn't, and I hope no one else experiences what I did ever again.
okay to reblog
#actually autistic#actuallyautistic#neurodivergent#aba therapy#aba survivor#tw aba therapy#tw child abuse#tw suicide#ok to rb
354 notes
·
View notes
Note
hiiiii!!!! i was wondering if u could share some of the most common to least common bpd symptoms?….and maybe ones u struggle with??? <:3
ive been thinking i have bpd for awhile,, (since i was 15,i’m almost 18 now) BUT i dont wanna self diagnose bc i don’t wanna offend anyone……is that offensive? to self diagnose? idek <:p
there isnt rlly least 2 most common, bpd is a spectrum and has a wide range of experiences!!! but i will list the diagnostic criteria 4 u, and explain it in a way some1 first learning abt bpd can understand ^w^
u must experience at least 5 of the 9 symptoms from the criteria in order 2 be diagnosed!!!
1: frantic efforts 2 avoid real or imagined abandonment; this does not include suicidal or self mutilating behavior covered in criteria 5.
this means an intense fear of abandonment. if u have bpd, being abandoned by those u love is most likely ur biggest fear. ik its mine!!! xD this can look like a number of things. this can include an avoidant attachment style, pushing ppl away becuz u feel a need 2 abandon them first b4 it happens 2 u. u might do the opposite and cling rlly hard. u might resort 2 manipulation tactics n threats 2 try 2 get them 2 stay even if its not in their best interest (not every1 w bpd does this, and not every1 w bpd doing this is doing it on purpose. ive done this in the past b4 i reflected on my own behavior and realized it was wrong. we r not abusers by default and we dont have bad intentions.) u might beg them 2 stay, promise them things, try 2 change urself 4 them, yell at them 4 wanting 2 leave. its terrifying what the fear might do 2 u.
2: a pattern of unstable and intense interpersonal relationships characterized by extremes of idealization and devaluation.
this ones pretty simple, consistently unstable relationships throughout ur life!!! but it might get a lil confusing at "extremes of idealization and devaluation", so ill try 2 explain that using a term from the bpd community, "splitting". splitting is when u switch from one extreme view of a person, object, character, pretty much anything, 2 the opposite. it USUALLY means going from loving some1 2 hating them, but it can mean the opposite (hating 2 loving), and it can apply 2 anything, not just a person. a good example of splitting is when ur fp (favorite person, another term from the bpd community) disagrees with u abt smth, or u see them hanging out with other ppl, u mightve viewed them as perfect b4 and now u feel an intense hatred and can only see them as a bad person. 2 other ppl, experiencing such a drastic change in perception over smth so small is seen as ridiculous, but rlly its entirely valid. its part of the disorder, its okay.
3: markedly and persistently unstable self image or sense of self.
u dont rlly know who u r a lot of the time, u dont have a strong sense of identity, if any at all. u might change styles often, change the way u talk, the jokes u make, ur beliefs, ur interests, ur hobbies. u might find urself basing ur entire personality on those around u. a common experience is that when ur favorite person or favorite ppl leave u, u dont know who u r anymore, becuz ur entire sense of self was mirrored from them. its like being a chameleon, but ur constantly mirroring other ppl, and ur nevr rlly ur own person.
4: impulsivity in at least two areas that r potentially self damaging (the examples listed in the DSM-5 include spending, sex, substance abuse, reckless driving, and binge eating, but i will provide moar examples!!!); this does not include suicidal or self mutilating behavior covered in criteria 5.
this ones also pretty simple!!! but personally i find that i become moar impulsive while in a bad headspace, or while im having a bpd episode/suicidal outburst. moar impulsive actions may include property damage, physical fights, running away, cutting contact with ppl, getting in contact with ppl who u know r dangerous, etc. those r all i could think of off the top of my head and they may not be the best examples, srry!!! :(
5: recurrent suicidal behaviors, gestures, threats, or self mutilating behavior.
i would like 2 say that self harm doesnt just mean cutting!!! self harm includes burning, hitting, ripping out hair, picking at skin, stabbing, and many moar. personally ive always been a cutter and i started when i was 9 or 10, but i want every1 2 know that all self harm is valid and this is a safe space 2 discuss it. im not gonna make any1 feel ashamed of it <3 also!!! suicidal threats and gestures may come across as manipulative, but that is almost NEVR our intention. we may act out in suicidal ways becuz its the only thing that gets us any sort of attention or care that we desperately need. i dont give a shit abt "ew theyre threatening suicide 4 attention, lets ignore them" becuz attention is a basic human need, and some1 threatening suicide REGARDLESS of their intentions is always a concern. whether its a call 4 help or not, they need help. dont disregard their mental health becuz their suicidal ideation doesnt present in an "acceptable" manner. all suicidal ideation, IS suicidal ideation. whether its passive, 4 attention, active w a plan, its all valid and requires attention and care.
6: affective instability due 2 a marked reactivity of mood (eg, intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely moar than a few days)
intense mood swings!!! u can feel happy one moment, and then switch 2 being depressed or anxious, and then go back 2 "normal" 10 minutes later. sometimes it just happens 4 no reason!!! absolutely fucking sucks
7: chronic feelings of emptiness.
this one is hard 2 explain and can mean varying things 4 different ppl. 4 me, it means i will never be happy in the long term (maybe with medication, but.. rawdogging life? bad idea) nothing gives me any sort of long term joy and i dont feel like i have a purpose. its like theres a hole in my chest that will nevr be filled. nothing will make me complete.
8: inappropriate, intense anger or difficulty controlling anger (eg, frequent displays of temper, constant anger, or recurrent physical fights)
angy
(also not every1 w bpd gets in2 physical fights or r angry at other ppl often, some ppl r moar angry at themselves)
9: transient, stress related paranoid ideation or severe dissociative symptoms.
paranoia is a symptom of bpd!!! although its shortlived in nature, and as stated above, stress related. dissociative symptoms can also present in a variety of ways!!! u can present with a fractured sense of self which may actually lead 2 u developing headmates iirc, but with them usually appearing as other versions of urself. or u might just dissociate due 2 stress or ur brain wanting 2 remove traumatic memories, 4 me dissociating feels like the whole world is fuzzy and blurry and i cant form any thoughts or emotions. i have dissociative amnesia and experience memory loss when this happens, which sucks becuz i dissociate at least once everyday. my memories r incredibly spotty and unreliable, its liek my brain is made of swiss cheese!!!
personally, i experience all of the symptoms from the diagnostic criteria, and they all effect my life on a daily basis. but that isnt 2 say that u need all of them in order 2 have bpd, as i said b4, u only need at least 5!!! there r also different types of bpd (not medically, theyre labels created by the bpd community) look in2 it if u resonate with some of the symptoms but not all of them!!! a lot of ppl who suspect they have bpd but dont present in a stereotypical way often relate 2 the term "quiet bpd", i recommend looking in2 it!!!
self diagnosis is entirely valid, and most of the ppl who r offended by it r neurotypical or they dont have the disorders that ppl r self diagnosing with. it stems mostly from ableism towards autistic ppl, specifically autistic ppl who self diagnose becuz they know theyre autistic but dont have the resources/time 2 get a diagnosis from a professional. if u believe ur borderline, and u've done ur research, i believe u. self diagnosis is not actually offensive 2 those who have mental disorders, im pretty sure the bpd community is accepting of self diagnosis!!! and if u cant find a community of ppl who r accepting of ur self diagnosis, just know that i believe u and this is a safe space 4 self diagnosis and ppl w bpd :3
bpd is also incredibly hard 2 get diagnosed with. its one of the most stigmatized disorders and often mental health professionals have a bias against it. sometimes, professional diagnosis is not an option 4 us. i knew i had bpd 4 years b4 i was able 2 get diagnosed. good luck!!!!
#jack.txt#birdie#damagedcoda6669#bpd#bpd awareness#borderline personality disorder#mental health#bpd safe#tw s3lf harm#tw self h4rm#tw sui ideation#tw self harm#tw sh#tw suicidal ideation
143 notes
·
View notes