#Rheumatoid Lung
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Hackers stole 65M passwords from Tumblr in 2013.
Text
i got an answer from my biological half aunt on my mom’s maternal side! bio grandma is still alive and my half aunt said no one in the family knew about my mom and that she’s in a bit of shock about it…
also we have a family history of heart murmurs, breast cancer, protein s deficiency, ehlers danlos syndrome and something really fucked up called malignant hyperthermia which is possibly fatal if you receive the wrong kind of anesthesia and it can happen AFTER safely receiving it the first time
#aaaand my bio grandpa’s side of the family graciously gifted us with bipolar#schizophrenia#autism#and lung cancer….#oh yea don’t forget the ibs and rheumatoid + psoriatic arthritis#really just a grab bag of genetic bullshit#i’ve got bipolar and graves’ disease to worry about from my dad too
0 notes
Note
hello!! could i request Dan Heng, Blade, Jing Yuan and Gepard with a chronically ill s/o? just some fluff and comfort :)
thank you!! have a lovely day <3
HSR x chronically ill!Reader
includes: Blade, Gepard, Jing Yuan, Dan Heng
a/n: hii!! I’m not sure what type of chronic illness you wanted the reader to have so each character has a different chronically ill reader, I hope that’s ok! blade's was kind of self-indulgent because i got arthritis (though no where as severe as the reader's is depicted) im so sorry if some of the illnesses arent 100% accurate word count: 1.4k (in total)
Blade x Reader with rheumatoid arthritis
: ̗̀➛ you were diagnosed with rheumatoid arthritis in every joint in your body. this meant that the pain in your joints would only get worse with time. of course, you had your good and bad days. on good days, the pain was minimal, to the point you wouldn't feel a thing. but on bad days, the pain in your shoulders made it difficult to carry bags, lift things, and particular bad days made it near impossible to get even changed. somedays, the pain in your hips were uneven and made you limp. Blade didn't really understand it at first; you were fine one day and looked terrible the next. it took him a while but he eventually understood that your arthritis came and went.
: ̗̀➛ one particular bad day, you could only lay down, feeling uncomfortable in your own body, a constant spike of pain present. breathing felt difficult, and you felt yourself tearing up just trying to sit up. the minutes it takes to even sit up right felt more like hours. sometimes, the pain killers wouldn't work as they should, and unfortunately, this was one of those days.
: ̗̀➛ Blade enters your room and you quickly turn your head to face him, and immediately regret it due to the pain. he knows it's one of those bad days; your eyes watery, the awkward position you were sitting in, and the look on your face just begging him to make the pain go away. it's difficult for him to comfort you with words so he goes to get some heating pads, food for you to eat, etc... anything he can really. he'll hold you close, minimal movements, letting you lay on him. in the silence between you two, he can't help but wish that at the very least, you could achieve the eternal peace he was chasing after.
Gepard x Reader with asthma
: ̗̀➛ as the captain of the silvermane guards, he has to keep fit and he’d like you, his lover, to at least do some morning runs with him. he knows that you have asthma, but he didn’t think a morning brisk would do anything awful. as long as you managed your symptoms, it was all fine! there usually arent any problems either, to the point your inhaler was often forgotten at home during these runs.
: ̗̀➛ unfortunately, perhaps you were trying to go faster for Gepard knowing he usually slowed down for you or something but you were definitely pushing yourself more than you could handle. your breaths drew short, not enough oxygen getting to you leaving you lightheaded as you continued to run. Gepard ran a bit in front of you, or at least he did. you watched as the distance between you and him grew farther and farther, and your running got slower until it came to a halt. leaning against a wall, you tried to catch your breath but you honestly couldn’t tell if you were breathing at all. the pain coming from your chest felt like too much, you had a hard time pushing air in and out of your lungs.
: ̗̀➛ Gepard ran back, retracing his steps, when he saw you were no longer with him. he found you hunched over, leaning against a wall, looking like you were hyperventilating. rushing to your side, he quickly recognizes that you were having an asthma attack. scooping you into his arm, he quickly runs back to your home. he may look calm due to the fact he is able to hide his fears, he’s a captain after all, but he’s panicking on the inside. the way home is blurry; you aren’t focused on what’s happening around you, only feeling your chest going up and down yet it didn’t feel like you were breathing. it felt as if there was something blocking your airway, causing everything to feel sort of stuck. Gepard grabs your inhaler and shakes it, before giving it to you. the effects don’t happen immediately which worried Gepard, but you eventually were able to breath, at least a little. he takes you to a hospital to get checked up immediately after. it’s when you’re getting checked does the realization that he came so close to losing you sink in. Gepard is clingier the week after that; holding your hands more (even when he’s working), kissing you almost every chance he gets, holding you before bed, etc… he’ll never forget to bring your inhaler on your morning runs after that.
Jing Yuan x Reader with diabetes
: ̗̀➛ low blood sugar is more than being shaky; no matter how long you’ve been diabetic, you’ll never get used to the god awful feeling of dread that occurs. Jing Yuan cares about your health, and he’s got the books and notes to prove it. usually, diabetes doesn’t get in the way of your life besides watching what you eat, having to keep fit, but it’s manageable.
: ̗̀➛ certain occasions like today, unfortunately, you wake up to a shaky feeling crawling up your body. it was early morning, Jing Yuan slept looking peaceful by your side. you forced yourself up and reached over to the meter as quietly as you could. after loading the strip into the device, you pricked your finger- a feeling you will never like. the number 40 glowed on the screen, glaring at you. you knew you had to wake Jing Yuan up because you really didn’t think you could go anywhere feeling like this. you felt awful nudging him awake, interrupting his sleep. all you have to do is show Jing Yuan the 40 and he’s beelining to the kitchen for some juice. when you finish drinking the juice, Jing Yuan holds; your head on his chest and his arms wrapped around you.
: ̗̀➛ your apologies to Jing Yuan for waking him fall to deaf ears as he’s rebutting everything you’re saying. many “nothing to be sorry about”s and “it’s not your fault”s could be heard. 15 minutes later, you prick your finger and show Jing Yuan a glowing 97. he goes to grab you a sandwich and after you finish eating, you two go back to bed. you lean on his shoulder, his hand cradling the side of your head, his chin laid on the top of your head, the two of you drift back to sleep holding each other.
Dan Heng x Reader with osteoporosis
: ̗̀➛ the path of the Trailblaze was not one without danger and Dan Heng was afraid you’d to be hurt in the crossfire though. you were diagnosed with osteopenia which eventually led to osteoporosis, which meant your bones were brittle. you hated it, this meant you were a liability to the astral express when trailblazing and often had to sit out during anything that had the slightest bit of danger. once, you asked if you could just have March’s shield on you at all times but even that proved ineffective in the long run.
: ̗̀➛ today, the astral express crew was visiting Herta for the Trailblazer to check out the simulated universe. Dan Heng quickly finished off the enemy before rushing to your side. it looked terrible, your arm was bent out of place and you couldn’t find it in yourself to say a thing. when you tried to move, a dreadful grinding sound occurred which made you nauseous. Dan Heng alerted the rest of the express crew before they all brought you to the medical department. thankfully, it wasn’t anything irreversible but throughout the treatment, you couldn’t help but feel like a big burden, getting hurt easily.
: ̗̀➛ once everything is fine and all you needed was time to heal, Dan Heng pulled you into a tight hug, whispering a few “thank god you’re fine”s and a “i was so worried.” usually you’d love his clingier side but it felt like pity. and god, it made you feel awful. no one else on the express would get hurt as easily as you. you push Dan Heng away, feeling terrible that you were such a burden, you quickly brief over how you feel. he grabs your wrist, looking you straight in your eyes, and loudly stated every reason you were not a burden because of your osteoporosis. from how you could take care of yourself to helping the express in ways non-physical like talking your way into less community service when the astral express crashed into a stadium. Dan Heng pulled you into a hug saying one last time, “you aren’t a burden.”
#honkai star rail#honkai star rail x reader#chronically ill reader#blade#hsr blade#blade hsr#blade x reader#gepard#gepard hsr#gepard x reader#gepard landau#jing yuan#hsr jing yuan#jing yuan x reader#dan heng#dan heng hsr#dan heng x reader#xieni's requests#this took forever to finish#i accidentally deleted it twice and had to rewrite
214 notes
·
View notes
Text
Help a disabled, neurodivergent, interracial family get back to the US for medical treatment
After three bouts of COVID and other medical issues over the past six years here in the Philippines, my health has deteriorated to the point at which I'm worried I won't get to watch my little girl grow up unless I can get back to where I can use my Medicare and VA benefits for various surgeries and treatments.
Unfortunately, even with all y'all's help, @thesurestthing and I are still in debt from the two-year ordeal of fixing our daughter's stateless status, so we can't do this on our own. My little sister started a fundraiser for us, and there are a couple of other ways to help, as well. If you can't help, please reblog. Thank you! (The PayPal link takes the lowest fees, but whatever works for you is best!)
If you want more details, they're under the cut:
Six years ago, while still grieving the deaths of my adult sons and a painful breakup, I moved from the US to the Philippines with just what I could carry, in large part because it's actually possible to survive here on the pittance US disability pays. I had kind of given up on life and figured I would sort of drift off eventually. I wasn't going to kick my own bucket, mind you; I just wasn't going to try very hard to keep living. And I figured I'd just pass away someplace beautiful.
Soon after I got here, though, @thesurestthing (also American) started messaging me from the states, told me she was going to come to the Philippines and be my girlfriend (even though I told her no at first), and eventually joined me here. We had a baby under lockdown, and got married.
So now I had something to live for. (And most of y'all know the drama with the error on El's birth certificate that left her stateless and took almost two years and a lot of money to get fixed.)
But I have had health scare after health scare over the past few years, including three bouts of COVID (some of you remember the month I spent hooked up to an oxygen machine), two bouts of pneumonia, a persistent two-year foot infection that took surgery to clear up (and is going to require another surgery to keep cleared up), damage to my heart and scarring in my lungs from long covid, a literal hole in my throat that is growing bigger, a spine injury, joint injuries, osteo and rheumatoid arthritis, a traumatic brain injury that affects my memory and concentration, adhd, bipolar disorder, autism, and other issues.
(Not even getting into the dental stuff--Hope to be able to get that done before we go back, here where it's cheaper, because Medicare doesn't cover that.)
I'm terrified that I won't be alive to watch my little girl grow up unless I can get someplace where I can use my Medicare and VA health benefits.
An old friend of mine is a social worker and on the school board in a small Minnesota city with its own VA clinic, and has offered to help us get settled in there, but we still have to find a place to live (suitable for a couple that includes a physically disabled adult, and who have a toddler), some basic household goods, some cheap used transportation, and need to survive for a couple of months while Zoey looks for work.
Given our situation in general and the fact that right now my disability is our only income, we're probably looking at having to pay at least six months (or possibly an entire year) of rent up front in order to get anyplace to lease to us.
We can't stay with friends because every single stateside friend we have with a spare room also has a cat--and I have an anaphylactic allergic reaction to cats, meaning that I will literally die if I'm around a cat for too long. I've had to go to the ER because I slept in a room that had a blanket in the corner that a cat had momentarily lain on. The only way I can be around cats is if I'm on massive doses of immunosuppressive drugs, which, well... The whole issue here is that I keep getting deathly ill, so suppressing my immune system even more is a non-starter. Oh, and Fel D 1, the protein secreted in cat dander, saliva, and waste, can stay even on hard surface for up to two years, and even longer on porous surfaces.
Again, if we weren't still in so much debt from El's birth certificate debacle, we might be able to do this at least mostly on our own. But as things stand, we can't do it on our own. We need your help.
If you read all of this, thank you very much. And again, if you can't give, please reblog.
For more medical details, check my Rob Gets Medical tag. For more details about Eleanor's birth certificate saga, check my Baby El tag.
132 notes
·
View notes
Text
With cold and flu season fast approaching, I want to post herbal recipes I am finding. These are not mine, and not medical advice!!!
Plant Origins of Thieves Oil
Clove: clove buds originate from the evergreen tree Syzygium aromaticum or Eugenia caryophyllata. These flower buds contain up to 20 percent essential oil, and are incredibly pungent, thanks to the major active chemical component called eugenol.
Rosemary: rosemary is a popular herb that comes from a small evergreen plant that belong to the mint family. It is native to the Mediterranean region, and possesses strong anti-inflammatory properties .
Eucalyptus: eucalyptus trees are native to Australia, Tasmania, and nearby islands. They’re the popular plant exclusively enjoyed by koala bears, and come in many different species. The oil is derived from the leaf of the eucalyptus tree, and is commonly used in cold remedies.
Cinnamon: cinnamon oil and the dried spice cinnamon both come from the bark of the true cinnamon tree (Cinnamomum zeylanicum). Essential oils that come from the leaf, bark and root of the cinnamon tree are much different, but the most common used version in Thieves oil is the cinnamon leaf. The active component in cinnamon bark essential oil is cinnamaldehyde.
Lemon: lemons come from a small tree in the Rutacea family. Lemon essential oil is derived by cold-pressing the peel of the lemon fruit, which is rich in different phytonutrients and beneficial compounds.
Thieves Oil Recipe
As long as you have all of the necessary essential oils on hand, you can easily make your own version of Thieves oil at home.
Ingredients: Master Blend
80 drops of clove essential oil
70 drops of lemon essential oil
40 drops of cinnamon essential oil
30 drops of eucalyptus essential oil
20 drops of rosemary essential oil
Method:
Combine all of the above essential oils in a dark amber coloured 15 milliliter (0.5 fluid ounce) glass bottle. Make sure you store it a cool, dry place, away from heat and light.
Benefits and Uses of Thieves Oil
This thieves oil recipe can be used to address certain health ailments, check out the benefits and uses below! Not medical advice
1. Relief from Aches and Pains
This Thieves oil recipe is loaded with plenty of anti-inflammatories to ease muscular and joint aches and pains. Rosemary and eucalyptus oil have actually been found to relieve rheumatoid arthritis, as well as muscle and joint aches and pains. You can dilute Thieves oil in a carrier oil (like jojoba oil, almond oil or grapeseed oil) to be used topically on the ache or pain. Typically the ratio is 1 drop essential oil to 4 drops carrier oil.
2. Immune System Support
Thieves oil was used to protect the “thieves” from the Black Plague, so you can be rest-assured that this oil provides some hefty immune support. Clove and rosemary essential oils are powerful antibacterials and anti-fungals. They’ve both been shown to have significant anti-microbial effects against dangerous bacteria like Staphylococcus epidermidis, Escherichia coli, and Candida albicans.
Massage the blend on your feet, lower back, neck and behind your ears for daily immune support. You can also diffuse Thieves oil to allow the essential oil molecules to enter your blood stream after they’ve entered your lungs! To get Thieves oil into your lungs is to diffuse the oil in a diffuser. Diffuse 15-20 drops of Thieves oil for 15 minutes, 3-4 times a day.
By live life fruit.
#witchcraft#witchy vibes#witch aesthetic#witchy#witchblr#witchythings#witches#witch#spells#witchcore#spellcraft#spellwork#spellcasting#witch tips#witchy herbs
70 notes
·
View notes
Note
Okay so magic as something the body sees as a threat/danger to the body...
And this ask may return in varying levels as I refine it and get a better understanding of the subject
What if the body had a low-level immune response to using magic--like it isn't at an autoimmune disorder (yet, possibly)? Would there be a fever to try and purge whatever it is (that the body can't find)? Or would it immediately start escalating to an auto-immune response?
Okay, I love this question. So to answer it, I'm gonna have to 1) explain the immune system and how autoimmune disprders work, and 2) figure out how magic can be physical in a way for the immune system to respond to it.
So first off, your immune system has two main parts: innate (you're born with this) and adaptive (you develop this). Adaptive is the important one here. It deals with B cells, T cells, antibodies, stuff like that. It is specific, regulated, and has a memory. It also has to have tolerance. Tolerance is when these immune cells recognize the self and don't attack. Autoimmune disorders are the failure of this ability. Cells can't distinguish the self from the non-self, so they develop an immune response to your own cells. So to answer the first part, any attack on the self is an autoimmune disorder. There's not really an in-between.
The reason behind autoimmunity is largely unknown and too grand for this tumblr post (it's a lot of genetics stuff, as well as environment), so we're gonna fast foward a bit to what happens when your immune system attacks you. I will note though, that autoimmune disorders are most common in young adult females (probably something to do with hormones at that age, like estrogen).
ANYWAYS, so...what's going to happen is that the immune cells start attacking your cells and killing them. If the beta cells of the pancreas are killed, thats Type 1 Diabetes. If the joints are attacked, that's Rheumatoid Arthritis. There's also Lupus, Scleroderma, Sjögren, etc. I'm not going to get into all of this here, but you get the point: DISEASE.
What are some symptoms related to autoimmune disorders? That's complicated because there are so many and they act on so many types of cells, that the symptoms are specific to each disease. But, I like Systemic Lupus Erthematosus because it has a lot of systemic symptoms due to the body attacking your DNA. These include: a rash on the cheeks (malar rash), arthritis, inflammation of serosal surfaces (like oral mucosa), kidney injury, psychosis, seizures, oral ulcers, and a decrease in cell types (like RBCs and WBCs). This can cause a low grade fever, photosensitivity, fatigue, muscle aches, loss of appetite, inflammation of the heart and lungs, and poor circulation to the fingers and toes.
Now onto the next part: magic autoimmune disorder. So we're going to assume that using magic goes along with having a certain type of cell. We'll call this a magicyte. We can say this cell type is increased in the blood when the user is doing magic stuff.
In our hypothetical, the immune system can no longer recognize magicytes as self and begins to attack and kill these cells. This will probably lead to a decreased ability or even an inability to do magic (like how people with DM1 can't make insulin). We can also say that there may be a low-grade fever due to immune system activation. Remember how I said adaptive immunity is specific? Well, that's good because it probably won't do much else. Lupus is really bad because DNA is attacked, so that fucks with a lot of cells. As long as magicytes are the only targets of this response, the person will probably only lose their ability to do magic. Systemic stuff like fever will probably appear after they attempt to use magic (thus increasing the number of those cells and increasing immune response).
I hope this answered your question, and thanks for the ask :))
#med student#medical school#medicine#med school#biology#med studyblr#immune system#autoimmine disease#lupus#questions#superpowers
7 notes
·
View notes
Text
Rheumatoid Arthritis
When to suspect – A patient with rheumatoid arthritis (RA) will typically have constitutional symptoms, morning stiffness, elevated acute phase reactants, and a small-joint arthritis affecting the hands and feet. Joint erosions appear late in the disease process.
●Evaluation – A diagnosis of RA requires an examination of the extremities to detect the presence of synovitis, which will typically present as a symmetric polyarthritis affecting the metacarpophalangeal (MCP), metatarsophalangeal (MTP), and proximal interphalangeal (PIP) joints.
In a patient suspected of having RA, both MRI and ultrasound can be used to determine the presence of synovitis when the physical examination is not clear.
●Diagnosis
•Use of serologies – In a patient who presents with a symmetric polyarthritis, the presence of rheumatoid factor (RF) or anti-citrullinated peptide antibodies(ACPA) confirms the diagnosis of RA. However, these tests have limited value as a screening tool or to evaluate patients with a syndrome atypical for RA, since both may appear in patients with other rheumatic or inflammatory diagnoses.
(I got this part from a simple Google search: Rheumatoid factor (RF) testing for rheumatoid arthritis (RA) has a sensitivity of 60–90% and a specificity of 85%. For early RA, RF sensitivity is estimated to be around 41–66%, while for established RA, it's 62–87%. The specificity accounts for 43–96%, with most studies reporting specificity higher than 70%.)
•Use or radiologic studies – Plain radiographs demonstrating the presence of joint erosions confirms the diagnosis of RA. However, erosions are a late finding of RA, and their absence does not rule out RA.
•Classification criteria – The 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria were not designed to establish a diagnosis of RA, although they are often used for this purpose. It is important to remember that these criteria may not identify RA in all patients, particularly after the initiation of immunosuppressive therapies.
●Differential diagnosis – Some infections, malignancies, and rheumatic diseases may present with synovitis that can mimic RA. Noninflammatory diagnoses, such as osteoarthritis (OA), carpal tunnel syndrome, and hypermobility syndromes, may present with joint pain or dysfunction in the absence of synovitis.
Epidemiology and risk factors – Involvement of the musculoskeletal system other than joints (e.g., bone and muscle) and of nonarticular organs (e.g., skin, eye, lungs, heart, and others) occurs in approximately 40 percent of patients with rheumatoid arthritis (RA) over the course of the disease. Risk factors for systemic, extraarticular disease include the presence of rheumatoid factor (RF), anti-citrullinated peptide antibodies (ACPA), and smoking. Extraarticular involvement in RA is associated with increased severity of disease, with overall morbidity, and with premature mortality.
●Constitutional symptoms – Constitutional and systemic symptoms and findings may include generalized aching, stiffness, and constitutional symptoms such as fevers, weight loss, and fatigue; these features sometimes antedate the onset of articular disease by several months.
●Osteopenia – Bone loss in RA is common. It may be generalized, resulting from immobility, the inflammatory process, and treatment effects of glucocorticoids; periarticular, due to local inhibition of bone formation by immune cells; or focal, due to degradation of juxtaarticular bone by activated osteoclasts. In the absence of antiresorptive therapy, all patients with RA can be expected to lose bone mineral. The generalized and periarticular osteopenia that affects all patients with RA should lead to a low threshold for therapy to prevent bone loss.
●Sarcopenia – Muscle weakness is a common symptom in RA. It may have several, often additive, causes. These include synovial inflammation, drug-induced muscle disease, myositis, and vasculitis.
●Weight gain – Body composition is frequently altered in patients with RA, with changes of increased body fat mass and reduced lean body mass (sarcopenia), even at normal body mass index. Altered body composition contributes to reduced physical function and cardiometabolic risk and may be attenuated by formal exercise interventions and control of the underlying inflammatory disease.
●Cutaneous manifestations – The most common of the cutaneous manifestations of RA is the rheumatoid nodule. Other cutaneous manifestations may arise when rheumatoid vasculitis is present or may be due to dermal infiltration of neutrophils. Atrophic skin over involved joints is sometimes present.
●Ocular manifestations – Symptoms of ocular and/or oral dryness are the hallmarks of Sjögren's disease, which may occur in association with RA. Eye involvement in RA also may include episcleritis, scleritis, peripheral ulcerative keratitis, and, less frequently, uveitis.
●Pulmonary manifestations – Pulmonary involvement in RA may include pleurisy and parenchymal lung diseases (e.g., interstitial fibrosis, pulmonary nodules, bronchiolitis obliterans, and organizing pneumonia), as well as lung disease caused by drugs or other agents used to treat RA or as a result of infectious complications resulting from immunosuppression.
●Cardiac manifestations – Cardiac involvement, such as clinically apparent pericarditis and myocarditis, and the presence of rheumatoid nodules in the pericardium, myocardium, or valvular structures are uncommon in patients with RA, although there is an increased risk of coronary artery disease, heart failure, and atrial fibrillation (AF). Vascular disease can take several forms in patients with RA. Vasculitis of small to medium blood vessels can occur, and higher-than-expected rates of coronary artery, peripheral vascular, and cerebrovascular disease are also seen.
●Kidney manifestations - Direct effects of RA on the kidney are rare. Membranous and mesangioproliferative glomerulonephritis are the most commonly reported nephropathies. Rheumatoid vasculitis may also occur. Drug toxicity is much more common.
●Neurologic manifestations – A range of neurologic abnormalities may be associated with RA, which can involve the peripheral or central nervous systems and which can result from local or systemic factors. Carpal tunnel syndrome is the most common neurologic manifestation, and a compressive myelopathy or radiculopathy can also occur. Patients with rheumatoid vasculitis may experience subtle or more severe neurologic disease.
●Hematologic manifestations – Anemia is commonly present in patients with active RA. Other hematologic abnormalities, including neutropenia, which is present in Felty syndrome and in large granular lymphocyte (LGL) leukemia (LGL syndrome), may require therapeutic interventions, while reactive thrombocytosis and eosinophilia generally parallel disease activity and do not themselves require treatment. Cytopenias related to the drugs used to treat RA also may be seen.
●Principles and goals of therapy – In patients with rheumatoid arthritis (RA), affected areas may be irreversibly damaged or destroyed if inflammation persists. Thus, prompt diagnosis, early recognition of active disease, and measures to quickly achieve and maintain control of inflammation and the underlying disease process, with the goal of remission or low disease activity, are central to modifying disease outcome. The application of these principles in the management of patients with RA, together with the development and use of newer and more potent drugs, has resulted in significant improvement in the outcomes of treatment.
●Care by a rheumatologist – An expert in the care of rheumatic disease, such as a rheumatologist, should participate in the care of patients suspected of having RA and in the ongoing care of patients diagnosed with this condition. The treatment of patients with RA by a rheumatologist is associated with better disease outcomes compared with care rendered primarily by other clinicians.
●Nonpharmacologic measures – Nonpharmacologic measures, such as patient education, psychosocial interventions, and physical and occupational therapy, should be used in addition to drug therapy. Other medical interventions that are important in the comprehensive management of RA in all stages of disease include cardiovascular risk reduction and immunizations to decrease the risk of complications of drug therapies.
●Initiation of DMARD therapy soon after RA diagnosis – We suggest that all patients diagnosed with RA be started on disease-modifying antirheumatic drug (DMARD) therapy as soon as possible following diagnosis, rather than using antiinflammatory drugs alone, such as nonsteroidal antiinflammatory drugs (NSAIDs) and glucocorticoids (Grade 2C). Better outcomes are achieved by early compared with delayed intervention with DMARDs.
●Tight control of disease activity – Tight control treatment strategies to "treat to target" are associated with improved radiographic and functional outcomes compared with less aggressive approaches. Such strategies involve reassessment of disease activity on a regularly planned basis with the use of quantitative composite measures and adjustment of treatment regimens to quickly achieve and maintain control of disease activity if targeted treatment goals (remission or low disease activity) have not been achieved.
●Pretreatment evaluation – Laboratory testing prior to therapy should include a complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), aminotransferases, blood urea nitrogen, and creatinine. Patients receiving hydroxychloroquine (HCQ) should have a baseline ophthalmologic examination, and most patients who will receive a biologic agent or Janus kinase (JAK) inhibitor should be tested for latent tuberculosis (TB) infection. Screening for hepatitis B and C should be performed in all patients. Some patients may require antiviral treatment prior to initiating DMARD or immunosuppressive therapy, depending upon their level of risk for hepatitis B virus (HBV) reactivation.
●Adjunctive use of antiinflammatory agents – We use antiinflammatory drugs, including NSAIDs and glucocorticoids, as bridging therapies to rapidly achieve control of inflammation until DMARDs are sufficiently effective. Some patients may benefit from longer-term therapy with low doses of glucocorticoids.
●Drug therapy for flares – RA has natural exacerbations (also known as flares) and reductions of continuing disease activity. The severity of the flare and background drug therapy influence the choice of therapies. Patients who require multiple treatment courses with glucocorticoids for recurrent disease flares and whose medication doses have been increased to the maximally tolerated or acceptable level should be treated as patients with sustained disease activity. Such patients require modifications of their baseline drug therapies.
●Monitoring – The monitoring that we perform on a regular basis includes testing that is specific to evaluation of the safety of the drugs being used (table 1); periodic assessments of disease activity with composite measures; monitoring for extraarticular manifestations of RA, other disease complications, and joint injury; and functional assessment.
Table 1:

●Other factors affecting target and choice of therapy – Other factors in RA management that may influence the target or choice of therapy include the disabilities or functional limitations important to a given patient, progressive joint injury, comorbidities, and the presence of adverse prognostic factors.
Rheumatoid factor can also be positive in diseases other than rheumatoid arthritis:

Pathophysiology – Rheumatoid factors (RFs) are antibodies directed against the Fc portion of IgG. Normal human lymphoid tissue commonly possesses B lymphocytes with RF expression on the cell surface. However, RF is not routinely detectable in the circulation in the absence of an antigenic stimulus. How chronic infections and rheumatic diseases lead to increased RF in serum is uncertain.
●Possible physiologic function – Whether RF has a physiologic function is uncertain, though some potentially pathogenic and other potentially beneficial activities have been suggested.
●Disorders associated with RF positivity – RF is detected in the setting of various rheumatic diseases, in infections, in other inflammatory diseases, and in some healthy people.
●No role as a screening test – Measurement of RF has little value as a screening test to diagnose or exclude rheumatic disease in either healthy populations or in those with arthralgias.
●Role in prognosis - Although, in aggregate, seropositive disease and higher titers of RF are associated with more severe RA, measurement of RF has limited prognostic value in the individual patient with RA. When RF is combined with other clinical data (such as joint count, anti-citrullinated peptide antibodies [ACPA] results, and C-reactive protein measurement), prediction can be improved but is still limited.
4 notes
·
View notes
Text
“Collette Roe,” 29 (USA 1975–1978)
A study published in the Southern Medical Journal documented multiple deaths from myocarditis after legal abortion between 1975 and 1978 (all of which were counted through the CDC’s abortion mortality data). One of them was a 29-year-old whose warning signs were ignored until it was too late.
“Collette” had suffered from tuberculosis as a child (although she had recovered since then). Three months before her fatal abortion, she’d been diagnosed with rheumatoid arthritis despite her age. But what should have made any medical professional reconsider an elective operation was what had happened only a month before the abortion date.
Collette had been admitted to the emergency room suffering from chest pain on the left side. It had been diagnosed as a lung inflammation called pleurisy, but before the abortion she said she had chest pain again. She should have been thoroughly examined to be sure that she was a condition for elective surgery and to check the cause of her pain. But instead of being treated as the alarming red flag that it was, Collette’s chest pain was written off as merely a sign that she was anxious— not over the operation she was about to have or even her recent ER visit, but assumed to be about the pregnancy itself. Her pain should have been seen as a genuine health concern, not dismissed as a figment of her imagination.
Collette was given paracervical anesthesia and the abortion was carried out. Immediately after, she had trouble breathing and orthopnea, which is a known sign of heart failure or other serious problems. She became tachycardic and was given the working diagnosis of a pulmonary embolism. Treatment was started, but Collette went into full cardiorespiratory arrest only five hours after the abortion. All attempts at resuscitation failed.
As the autopsy showed, it was no wonder that Collette had been in so much pain. She had suffered pericarditis, prominent myocarditis, focal myositis and interstitial pneumonitis. Myocardial edema was present with fiber necrosis. Her pericardial cavity contained about 150 ml of bloody fluid. However, there was no evidence of a pulmonary embolism. Not only were the red flags ignored, but Collette had also been misdiagnosed and treated for the wrong complication in her last day of life.
Before any elective operation, let alone one with so many serious risks, any client should have received a careful pre-op examination before they were put on the operating table. Collette needed real medical attention, not abortion.
(See Case 3)
#tw negligence#tw abortion#victims of roe#unsafe yet legal#tw misdiagnosis#tw ab*rtion#tw murder#abortion#pro life#abortion debate#death from legal abortion#unidentified victim
5 notes
·
View notes
Text
What are the Types and Treatments for Arthritis?

Many of us aim to move freely without discomfort throughout our lives. However, life’s challenges often include maintaining stable health as our bodies undergo wear and tear, leading to pain and discomfort.
When it comes to mobility, one prevalent condition worldwide is Arthritis, causing concern for many. Yet, Expert Orthopedic Doctors associated with the Leading Arthritis Treatment Hospital in Bangalore assure that successful methods exist today to manage this condition..
A bit of awareness and taking care at the right time can help a lot
Understanding Arthritis
The Best Knee Specialists in Bangalore at Suguna Hospital describe Arthritis as a condition that causes swelling and tenderness in one or multiple joints throughout the body. As your age or with certain health issues like high blood sugar levels, this condition may worsen.
Different Types of Arthritis
Arthritis isn’t restricted to a particular age but is commonly noticeable in later stages.
Some of the common types are:
Osteoarthritis – Affecting joints in your Hands, Knees and Spine.
Psoriatic Arthritis – Caused due to a very complicated skin disease called Psoriasis, this condition can be very challenging.
Reactive Arthritis – This causes joint pain and swelling. It is caused either due to infection or malfunction of key organs of your body including the intestines, genitals, or urinary tract.
Rheumatoid Arthritis – This is a chronic inflammatory disorder. In addition to affecting the different joints, it can deeply impact premier organs like heart, lungs and eyes.
When to See a Doctor? Experts recommend seeking immediate medical attention if you notice specific symptoms, like
Stiff joints
Acute pain in the joints
Difficulty in moving or standing
Swelling observed in or around the joints
Redness observed in the joints
Treating ArthritisManaging Arthritis requires a systematic approach. It’s crucial not to overlook persistent symptoms as mere discomfort. Ignoring these signs can lead to costly consequences.
Your treatment is based on how severe is your condition and can include:
MedicationsDepending upon the type of Arthritis diagnosed, your medications may include:
Ointments
Steroids
Physiotherapies and light workouts to begin with
SurgeryThis is the last resort which your doctors might recommend only if there are no signs of improvement after persistent medication. Some of the types of surgeries successfully performed include,
Joint Repairs
Joint Replacements
Overcome Arthritis and lead a pain-free, confident life. Avoid welcoming Arthritis! Consult the top Arthroscopy Surgeon in Bangalore at Suguna Hospital for a safe and successful journey ahead.
#Arthritis#Rheumatoid arthritis#Osteoarthritis#Psoriatic arthritis#Ankylosing spondylitis#Lupus arthritis#Reactive arthritis#Infectious arthritis#Septic arthritis#Arthralgia#Joint pain#Inflammatory arthritis#Non-inflammatory arthritis#Arthritis symptoms#Arthritis treatment#Arthritis medications#Arthritis diet#Arthritis exercises#Arthritis prevention#Arthritis relief#Arthritis diagnosis#Arthritis causes#Arthritis risk factors#Arthritis and genetics#Arthritis and weather#Arthritis and stress#Arthritis support groups#Arthritis research#Arthritis specialists#Arthritis in hands
5 notes
·
View notes
Photo
DID YOU KNOW THAT? Smoking is one of the most provocative environmental factors for the development of rheumatoid arthritis.
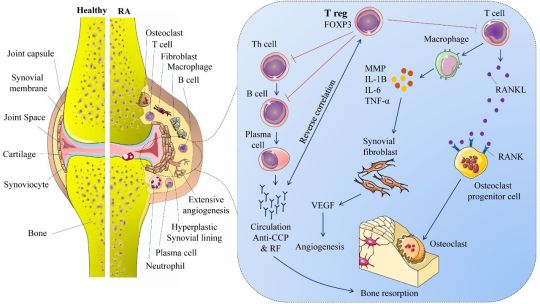
Why? Smoking --> lung inflammation --> activation of enzymes like peptidylarginine deaminase --> changes arginine into cyclic citrullinated peptides --> immune system makes anti-CCP antibodies --> complement is fixed in the tissues --> destruction
The relationship is dose-dependent and risk goes down after quitting.
Image belongs to Iranshahi et al, IJMBPH (2018)
9 notes
·
View notes
Text
The Myth of Normal: Trauma, Illness and Healing in a Toxic Culture (Gabor Maté, 2022)
“The gender gap in health is real, if underappreciated.
Women are more subject to chronic disease even long before old age, and they have more years of poor health and disability.
“Women have it worse,” a leading U.S. physician wrote recently, pointing out that women are at much higher risk of suffering chronic pain, migraines, fibromyalgia, irritable bowel syndrome, and autoimmune conditions like rheumatoid arthritis.
As noted in chapter 4, rheumatoid arthritis strikes women three times more often than it does men, lupus afflicts women by a disproportionate factor of nine, and the female-to-male ratio of multiple sclerosis has been rising for decades.
Women also have a higher incidence of non-smoking-related malignancies. Even when it comes to lung cancer, a woman who smokes has double the chance of developing the disease.
Women also have double men’s incidence of anxiety, depression, and PTSD. (…)
Early childhood mechanisms of self-suppression are reinforced by persistent, gendered social conditioning.
Many women end up self-silencing, defined as “the tendency to silence one’s thoughts and feelings to maintain safe relationships, particularly intimate relationships.” This chronic negation of one’s authentic experience can be fatal.
In a study that followed nearly two thousand women over ten years, those “who reported that, in conflict with their spouses, they usually or always kept their feelings to themselves, had over four times the risk of dying during the follow-up compared with women who always showed their feelings.”
As at home, so on the job. Another study showed that for women with non-supportive bosses, the squashing of anger—a natural adaptation to an environment in which to self-express would be to risk the loss of employment—increased the risk of heart disease.
Recall from chapters 5 and 7 this array of self-abnegating traits that predispose to disease: a compulsive and self-sacrificing doing for others, suppression of anger, and an excessive concern about social acceptability.
These personality features, found across all autoimmune conditions, are precisely the ones inculcated into women in a patriarchal culture.
“I was denying myself as a person, denying my own desires, my wants,” the first responder Liz said.
“I was not paying attention to what I needed. Everyone else was far more important. My job was way more important than any concern that I had. I wasn’t listening to myself in any regard.”
That “not listening to self” in order to prioritize others’ needs is a significant source of the health-impairing roles women assume.”
18 notes
·
View notes
Text
A terminally ill federal inmate wants to be released so he can die outside of prison. He's been refused, so he's applying for MAID
After more than four decades in a federal prison, Ed Speidel is fighting for a compassionate release so he can die outside, in a halfway house, rather than in his jail cell.
But after being rejected for parole and refused an appeal, he now fears he will die a painful death, struggling to breathe behind bars.
"My biggest fear is dying in jail. I don’t want to die in jail," said Speidel in a phone interview with CTV News from an office in the Matsqui Institution, a medium-security prison in Abbotsford, B.C.
The 62-year-old suffers from end-stage chronic obstructive pulmonary disorder (COPD) along with chronic pain and rheumatoid arthritis. Tests show his lungs have only 19 per cent function compared to healthy adults.
"I have days where I have a real hard time breathing and it's like choking, like you're starved for air," said Seidel.
He requires oxygen 24 hours a day. Yet just prior to his phone interview with CTV, he said he had to struggle to get staff to provide him with a portable oxygen unit to make the trip to the room where the interview would take place.
Speidel, who uses a walker and spends most of his time in his cell, says he is in no way a threat to the public.
"I was a s**thead. (I did) robberies. But I didn't hurt anyone," he said. "I have done 41 years. I’ve done my time. Nothing is being served by keeping me here."
At a parole hearing in July 2022, he asked for parole by exception – more commonly referred to as compassionate or geriatric parole – due to his failing health, age and time served. He was not represented by a lawyer and was turned down.
He obtained legal support early this year. Lisa Crossley, who works with Prisoner Legal Services in Vancouver, says the case is bolstered by a note from a doctor in the institution, recommending that the parole board consider compassionate release for Speidel given his progressive health condition.
But the motion on for an expedited hearing of his review on July 8 was rejected. Speidel is now working through an application for a medically assisted death, though he says it's not really his preference.
"For the vast majority of people, if you are terminally ill, what risks do you really pose? I think that should be asked and there should be more options for people for some type of release," Crossley told CTV News.
Still, Crossley says, she will continue to push for an expedited regular parole hearing, and for another appeal for a compassionate release. She believes it is the first case of its kind in the country that will highlight the plight of older prisoners who are ill.
"It is a matter of public importance that affects many people in federal prison," said Crossley.
AGING AND AILING INMATES
Of the 6,886 prisoners now in federal jails as of 2023, more than 1,700 (25.6 per cent) are 50 and older and are classified as aging offenders.
Surveys show that prisoners age more rapidly due to their past lifestyles, high rates of substance abuse and the stress of imprisonment.
There are higher rates of diseases that come with age including cancer, diabetes, lung disease and dementia.
Ivan Zinger, the correctional investigator of Canada, says a review, conducted in 2019 worried him.
"We saw an inordinate amount of prisoners who were either terminally ill or had dementia or Alzheimer's, who had severe mobility restrictions, who were bedridden. And all these individuals, you scratch your head, saying, 'What are they doing in a prison setting?'" he said in an interview from his office in Ottawa, Ont.
"Prisons and penitentiaries were never designed to be nursing homes or long-term care facilities or hospices. And this is what they've turned out to be. And it's just not acceptable," Zinger added.
In a statement sent to CTV News, Correctional Service of Canada officials said they could not comment on specific inmates or their cases, but wrote that the agency "acknowledges that challenges exist in addressing the multiple needs of aging offenders, but remains committed in its efforts to continue to develop strategies in meeting those needs.''
The Parole Board of Canada, meanwhile, is responsible for making decisions about exceptional paroles and when offenders don't pose a risk to the public. In an email to CTV News, PBC officials wrote that the board granted 29 paroles by exception to all age groups between 2019 and early 2023. Of those, 13 were prisoners aged 60 and older.
That amounts to about four compassionate releases per year and proves, says Zinger, that the corrections system is not offering enough medical compassionate releases.
"Each year, up to 40 incarcerated individuals die in Canadian penitentiaries of 'natural causes,' usually terminal illnesses,” he noted. “The fact of the matter is none of these individuals benefited from a compassionate release, even though their death was expected or imminent.”
Meanwhile, studies show the cost of keeping a geriatric offender in prison can be two to four times higher than housing them in a halfway home with medical support.
Zinger points to other jurisdictions, like in the U.S. and Europe, which are building secure nursing homes for inmates, where they can be transferred after they turn 65 or develop chronic or fatal illnesses.
In Canada, there are at least five secure halfway homes that accept or are just starting to accept aging inmates, with about four dozen beds. Haley House, in Peterborough, Ont., has 10 beds and is hoping to open a second home with 10 more beds this fall. Still, the case manager, Jeff Morgan, writes that existing facilities don't "come close to meeting the needs of aging offenders that are coming out of federal institutions, or are due to be released."
COMPASSIONATE PAROLE OR MAID?
With no indication he will get out any time soon, Speidel has applied for medical assistance in dying (MAID), and is awaiting a medical assessment. The process usually takes three months or less.
He says he'd much prefer dying a natural death in a supervised halfway house. But his next regular parole hearing could be in 2024.
"What it looks like is that it's easier to kill myself here, with their (medical) help, than it is to try and convince them to let me back out. And I don't understand why," Speidel said.
CTV reported earlier in 2023 that there has been a small but noteworthy increase in MAID deaths among inmates, at rates higher than those in most other countries that allow assisted death.
The 2019 report by the Zinger also warned that without better planning for aging and ailing prisoners, there would be a surge of requests for MAID.
"Canada’s correctional authority should not be seen to be involved in enabling or facilitating any kind of death behind bars. It is simply incongruent with CSC’s obligation to protect and preserve life," he wrote.
Yet Speidel’s case suggests this is exactly what is happening.
He wants parole to die on his own. But the road to approval for MAID may come more easily – a problem his lawyer says needs to be addressed.
“Are we comfortable with it being the case that people can apply for made and be granted it within a month?” said Crossley. ”If you're eligible for MAID, you meet all those requirements, do you really pose such a risk to the community that you shouldn't be eligible for some kind of release as well?” she added.
For Speidel, it is a simple, binary choice.
"I sure hope I get out because if I don't, I will take MAID. I'm not going to sit here, unable to breathe, until I'm laying on the floor choking," he said.
from CTV News - Atlantic https://ift.tt/wQad7ns
5 notes
·
View notes
Text
What are the Different Types and Treatments of Arthritis?

Leading a beautiful life doesn’t come without challenges. Our body goes through a lot of stress and grind in the process and there comes a stage when it needs more attention and care than ever before.
The Best Orthopedic Doctor in Bangalore at United Hospital explains that the wear and tear, our body is subjected to, leads to pain in the ankles and knees. Sometimes, it can get pretty hard to walk!
Are we welcoming Arthritis in this case?! Well, in the worst case, unfortunately, we may be. However, experts indicate that there is no need to panic. With rapid advancements in medical science, there is not just hope, but more confidence that we can defeat Arthritis.
It is all about being aware of what Arthritis exactly is and taking precautions at the right time that could be the best beginning to arrive at a successful solution.
Understanding Arthritis?
Experts at United Hospital, a dedicated Orthopedic Centre in Bangalore focusing on Arthritis care, explain that Arthritis is a medical condition involving swelling and tenderness of one or more joints. It may worsen with age and is a prevalent cause of discomfort among senior citizens
Types of Arthritis
Arthritis can affect individuals of any age, but the elderly are more vulnerable.
Some of the common forms of Arthritis are:
Osteoarthritis - It is a condition that affects joints in your Hands, Knees, Hips and Spine.
Psoriatic Arthritis - This a condition that develops in people due to a very challenging skin disease called Psoriasis.
Reactive Arthritis – This causes joint pain and swelling triggered by an infection in prominent parts of your body — most often your intestines, genitals or urinary tract.
Rheumatoid Arthritis – This is a chronic inflammatory disorder which can affect more than just joints including premier organs like lungs, heart, eyes and blood vessels.
Some of the other conditions faced notably by the elderly include Ankylosing Spondylitis.
Symptoms of Arthritis
The most common signs and symptoms of arthritis involve the joints. Hence, it is important to seek an expert opinion if you observe one or more of the following symptoms:
Pain in the joints.
Stiffness felt in the joints.
Swelling observed in or around the joints.
Redness observed in the joints.
Difficulty in moving.
Treatment for Arthritis
Arthritis, if untreated, can be a really painful thing to handle. However, what really matters is the right type of medical attention at the right time and from the right source. Your treatment is based on how severe is your condition and can include:
Medications
Depending upon the type of Arthritis diagnosed, your medications may include:
Non-steroidal anti-inflammatory drugs.
Creams and Ointments.
Steroids
Physical therapies and exercises.
Surgical Interventions
In case you do not get any relief from the above medications your doctor might recommend surgical interventions to bring you back to your routine lifestyles in quick time. Some of the types of surgeries performed include,
Joint Repairs
Joint Replacements
Joint fusions
Let’s say Goodbye to Arthritis forever and welcome a painless life. For many of us, life may begin at 40, but so does Arthritis! Hence, if you are wondering as to, “Which is the Best Orthopaedic Clinic near me to treat Arthritis”? feel free to connect with United Hospital.
#orthopaedic clinic near me#orthopaedic doctor in Bangalore#orthopedic hospital in Bangalore#bone doctor near me#bone hospital near me#joint replacement surgery in Bangalore#knee replacement surgery in Bangalore#total hip replacement#total hip arthroplasty surgery Bangalore#orthopaedic services Bangalore#Arthritis symptoms#Arthritis treatment#Types of arthritis#Rheumatoid arthritis#Arthritis pain relief#Arthritis causes#Arthritis management#Natural remedies for arthritis#Arthritis inflammation
2 notes
·
View notes
Text
It’s been awhile...
This will be quite the read, so I’ll keep it all under the cut, with a slight trigger warning. I am talking about my personal life and what I’ve been dealing with. Thank you for being understanding and taking the time to read this post. I love you all. ♡
✧・゚: *✧・゚:* *・゚✧*:・゚✧
I know none of you were probably expecting this. I mean, to be completely honest, I wasn’t expecting this either. However, after still getting many messages in my inbox and love on the content I’ve posted, even though I haven’t been around in... roughly two plus years, I wanted to make a post/announcement for everyone. This is to kind of explain what’s been going on in my life and what my plans are for this blog. Thank you all so much for the continued love and support during my absence.
So, to start off. Why have I been gone so long? Well, that’s a very, very long story that involves a lot of trauma and my personal life, so I’ll keep it as brief as possible. I dealt with a string of abusive relationships, many different jobs, moving several times (and by “several times”, I mean that I moved about 7 or 8 times within a year, including between different states), losing friends, trying to better my health, re-discover who I am, and so much more...
I’m not going to get into the details of my relationships or anything like that, but I would like to briefly talk about my health. I’ve finally gotten the chance to see doctors to get confirmed diagnoses, rather than simply wonder if I have something or not. As of right now, besides the mental illnesses I was already well aware of, I had a diagnosis that confirmed I have rheumatoid arthritis, or RA for short. For those of you that don’t know, it’s an autoimmune disease. I’ll post a link that will give you guys basic info about it so I don’t make this post even longer than it needs to be. To put it into simple terms, however, it’s a chronic autoimmune disease that mostly affects joints. RA occurs when the immune system, which normally helps protect the body from infection and disease, attacks its own tissues. The disease causes pain, swelling, stiffness, and loss of function in joints. Having a diagnosis is relieving but it’s also added a lot of stress to my life. I also have had 2 cancer scares now. The first scare (my lungs), which I got testing for, was clear. But now, on my second one (my thyroid), not so much. I have to wait a year to get retested to make sure nothing has gotten worse. It’s a lot, I know, but something I wanted to open up to you guys about.
Link: https://www.niams.nih.gov/health-topics/rheumatoid-arthritis#:~:text=Rheumatoid%20arthritis%20(RA)%20is%20a,loss%20of%20function%20in%20joints.
I also wanted to take the chance to reintroduce myself. I was still me before, but a lot of things about me were the choices of controlling ex’s, and not my own. So, hey there. My name is Stormi. I’m a 24 year old who is non-binary, born female, with no preference to pronouns. You can refer to me however you’d like, and I’ll be happy regardless. I enjoy listening to music, drawing, reading, writing, making crafts, playing video games, watching videos on YouTube, playing Dungeons & Dragons and so much more. It’s hard to encapsulate the person that I truly am over a post, but I still want to give you guys a little bit of an insight into who I truly am.
As for my plans on this blog... I’m not quite sure. I want to start writing and posting again, I do. But my health complicates that a bit. I think I will, but I won’t take it quite as seriously. What I mean by that is not that I won’t care, but I won’t be stressing myself out with it as much as I used to. I think I’m going to delete every single ask that I have in my inbox, re-work my character masterlist and a few other things and let you guys know when requests are open. When that happens, please feel free to request! Just be patient and give me some time to get to them. Also, in regards to NSFW content, I think the only thing I’m going to be accepting is probably headcanons. Don’t get me wrong, I like my smut just as much as the next person, but it’s really difficult for me to write it at times. I also worry that everything will end up being too similar.
Anyways, if you made it through this entire post, then thank you so much. It really means a lot to me. You all have been wonderful to me over the years, and I hope you all are excited about my gentle return to the world of tumblr. Even if you guys don’t have any requests, feel free to get into my inbox just to talk. As I’ve said before, my blog is a safe space for everyone. Thank you, I love you all :) ♡
8 notes
·
View notes
Text
Rarely do I talk about real life stuff here, but I need to scream this at the top of my lungs.
We got a package from my mother today with stuff for our impending family addition (third trimester, here I come!). In it was the three blankets pictured below, as well as three newborn hats and booties.
She MADE these for us. My mother has Rheumatoid Arthritis and Sjögren's Syndrome and Fibromyalgia and some days, she can barely move in her own house because of swelling and pain and she still made all these things for the baby. And it just makes my heart soar to the sky and straight into space to burn in the sun. I'm so touched.
I can't wait to let my baby cuddle up in these and tell them their grandma made them, special, just for my little Bubs.



#pregnancy musings#it's one part hormones and one part The Thing From March 2023 and one part just being a mushy pile of emotions#goodness help me I'm going to cry forever
3 notes
·
View notes
Text

Nicotine addiction is a severe issue that claims the lives of 6,000,000 people each year. So, it is time we educate our young and old folks on the damaging implications of smoking. 🚭
-According to researchers, since the 1950's smoking has had a causal link to lung cancer, heart disease, stroke, diabetes, and chronic obstructive pulmonary disease (COPD), which includes emphysema and chronic bronchitis. Smoking also raises the risk of TB, eye illnesses, and poor immunity system issues such as rheumatoid arthritis. Stop believing in the myth that vape or cigars are any better alternatives to cigarettes.
- The World No Tobacco campaign was established in 1987 by World Health Organisation (WHO) to increase awareness about tobacco products on people, public health, communities, and our environment. This year we focus on the theme "We Need Food, Not Tobacco," intending to change the minds of tobacco farmers to engage in planting sustainable alternate crops.
- A nicotine addiction can only cause illness, death and misery for you or your loved one. So, to protect yourself and your family from this disaster, you must quit smoking. @heartitout offers to support your quitting journey with our specialized experts trained to help all addicts. We want to see every human have a healthy heart and a happy smile. Talk to us today-https://heartitout.in/
2 notes
·
View notes
Text
How will ayurvedic medicine heal Arthritis?

Ortho Veda oil has shown excellent results in recovering from arthritis problem whose major symptoms are:
1) Inflammation
2) Pain
3) Swelling
4) Aching
5) Stiffness
The word” arthritis “ itself indicates joint inflammation. It is the loss of cartilage that gives rise to inflammation, intense pain and mobility issues to the person and that can spread across other connecting issues which are ligaments and tendons.
Researchers point out 100 types of arthritis that can happen at any age , pertaining to nutritional deficiency , sedentary habits, and alcoholism.
Types of Arthritis
-----------------------------------
Let’s understand the selected major types of arthritis damaging the physical mobility and mental health are:
1) Inflammatory arthritis
For unexplained reasons, several people have been diagnosed with inflammatory arthritis. It gives rise to swelling, pain and stiffness. Without experiencing injuries or cuts, one can get affected with inflammatory arthritis in several joints. Damage is done to the surface and also to the bones. Examples are rheumatoid arthritis, reactive arthritis, psoriatic arthritis and ankylosing spondilytis
2) Degenerative
Degenerative arthritis is characterized by loss of cartilage from the surface of the bones which actually holds the bones together, causing lubrication and smooth movement.
3) Connective tissue disorder
In this type of arthritis, one experiences destruction in the tendons and ligaments apart from cartilage. It can further damage the connecting tissues of skin, lungs and kidney. The examples of connective tissue disorder are:
1) Scleroderma
2) Lupus or SLE
3) Dermatomyosytis.
4) Sjogren’s
4) Metabolic
This type of arthritis occurs in the form of deposits of uric acid crystals in the area of joints due to disorder in the urinary system. And it leads to development of gout arthritis. It is one of the major signs noted in diabetic persons in the form of sudden pain and swelling.
5) Septic
It is the result of bacterial or fungal infection that can affect the knee and hip area of the body. Infection from the external sources like injury or surgery, reaching the joints and bones through the blood
6) Childhood
It is a juvenile rheumatoid arthritis which can do permanent damage to the bones.
For any of the above mentioned types of arthritis , Ortho Veda oil will be highly effective.
Lakhs of people have realized the value of Ortho Veda oil within a few days of use.

Key factors that determine the positive impact of this veda oil are:
1) Composition : Cow milk, Black sesame oil, Wild asparagus, camphor and eucalyptus are the major ingredients. No chemicals added. The composition is 100% natural and ayurvedic
2) Ortho Veda oil price: Ortho Veda oil price in India is cost effective. You can buy it easily from SKinRange online store at a moderate price. You can also get from Amazon at a discount right now.
3) Recovery effects: a) It will boost blood circulation and warmth in the affected area.
b) It will reduce swelling and inflammation.
c) It will produce relief from pain.
d) It will prevent cartilage loss.
e) It will boost lubrication and flexibility in joints.
4) Certification : Ayush Certified vata massage oil.
5) Side effects if any:No side effects found.
Direction of using this ayurvedic oil
Apply and massage the oil on the affected area as many times a day.
In order to boost immunity, strength, flexibility and longevity of bones and joints, you must eat vitamin D, C and calcium enriched foods along with Omega 3 fatty acids and zinc. Further, you must keep the habit of practicing exercise or yoga for keeping your joints and bones active.
#health#ayurvedicoil#arthritis#joint pain#joint pain relief#skinrange#ayurvedictreatment#essential oils
6 notes
·
View notes